
Comparing SFT and bio
ii50 (C) Subjective global assessment (SGA) SGA should be used to identify severe malnutrition in haemodialysis patients (Evidence level III). Rationale SGA is based on a combination of subjective and objective features from the medical history and physical examination. A modified version of the SGA has been used in the Canada/United States Peritoneal Dialysis Study (CANUSA) and DOPPS studies (see Appendix). It was demonstrated that lower values of the mSGA were associated with a higher mortality risk [16]. The investigators concluded that in haemodialysis patients malnutrition, as indicated by low values obtained with the mSGA, was associated with higher mortality risk [16]. In a prospective observational study, it was also shown that patients with the lowest SGA score had higher mortality and hospitalization rates [17]. In a direct comparison with the determination of body nitrogen content by means of in vivo neutron activation analysis it was demonstrated that SGA was able to differentiate severely malnourished patients from those with normal nutrition, but appeared not to be a reliable predictor of the degree of malnutrition [18]. (D) Anthropometry Anthropometry in MHD patients should be assessed immediately after dialysis (Opinion). Anthropometry (Mid Arm Circumference (MAC), Mid-Arm Muscle Circumference (MAMC) and four site Skin Fold Thickness (SFT) should be performed by the same individual on the nonfistula arm (Opinion). Rationale BMI, Four-site skin fold thickness (SFT), mid-armcircumference (MAC) and mid-arm-muscle-circumference (MAMC) are anthropometric screening methods to assess fat and lean body mass and may detect a potential risk for Protein and Energy Wasting (PEW). These are easy to use, widely available and cost effective tools to help assess nutritional status of patients on MHD but fluid status influences calculations. Four-site SFT, MAC and MAMC: these anthropometric measurements are important for overall nutritional assessment. Measuring muscle mass, MAC and MAMC, is essential to assess muscle mass. It is necessary to perform skin fold thickness at four sites to obtain an accurate assessment of total body fat: triceps, biceps, sub-scapular and ileac crest. The Frisancho Tables (1984) and Durnin and Womersley (1974) equations are used to calculate lean body mass and body fat percentage from obtained details (see Appendix for methods). D. Fouque et al. Comparing SFT and bio impedance analysis (BIA): Oe et al. [19] evaluated body composition [lean body mass (LBM), body fat (BF) and total body water (TBW)] using SFT and BIA techniques in 20 stable MHD patients pre- and post-dialysis. These authors showed a good agreement between the two techniques (R ¼ 0.93, P < 0.005) and proposed that BIA might be the preferred method, as BIA is not operator dependent and requires minimal training to assess fluid status. Kamimura et al. [20] also found that SFT measurements were comparable with BIA and remain interesting for routine body fat assessment. Ninety clinically stable MHD patients were studied; body fat measurements using SFT and BIA were similar (13.5 6.2 kg and 13.7 6.7 kg). Further research is recommended to obtain references for body composition assessment that are simple to use in the routine care of MHD patients. (E) Normalized protein nitrogen appearance (nPNA) Normalized PNA should be measured in clinically stable haemodialysis patients and be above 1.0 g/kg ideal BW/day (Evidence level III) (see Guideline 3). Rationale Normalized PNA provides an independent and less time consuming assessment of dietary protein intake. Nitrogen balance, the difference between intake and losses, is zero in the steady state or slightly positive. Both net protein breakdown under fasting conditions and dietary protein requirements are strongly influenced by body mass. In order to normalize PNA it should be related to body weight of the patient. When determining nPNA, patients should be stable and neither anabolic nor catabolic [21]. The protein equivalent of total PNA can be estimated from interdialytic changes in urea nitrogen concentrations in serum and urine (see Appendix). A recent study in more than 50.000 US adult haemodialysis patients reported that mortality was lowest for patients having a nPNA between 1.0 and 1.4 g protein/kg BW/day; furthermore, when patients had a decreased nPNA after a 6-month follow-up, the 18-month subsequent mortality increased [22]. PNA should however not be used alone to evaluate nutritional status, but rather as one of several independent measures when evaluating nutritional status. (F) Serum albumin and serum prealbumin Serum albumin should be above 40 g/l by bromocresol green method (Evidence level III). For other albumin assessment methods the target values should be adapted to the above (Opinion). Serum prealbumin should be above 0.3 g/l (Evidence level III) EBPG guideline on nutrition Rationale Serum albumin is recommended for routine measurement because a large body of literature is available, that defines normal serum albumin values and characterizes the clinical factors affecting serum albumin concentrations. Serum albumin, per se, is an indicator of visceral protein stores. During recent years the interactions between inflammation and malnutrition status became complex, as inflammation and dietary protein intake exert competing effects on serum albumin levels [23]. A number of publications demonstrate the relationship between serum albumin concentrations and outcome [24]. Hypoalbuminaemia is a predictor of future mortality [25–29] and cardiac disease [27] at the time of initiation of dialysis and at any time during dialysis treatment. Among 1411 patients enrolled in the HEMO study, those in the low albumin group had significantly greater prevalence of coronary heart disease [30]. Serum albumin should not fall below 40 g/l (measured by the bromocresol green method). Patients with a serum albumin level below 35 g/l have a relative mortality risk of 4 [31], or a 2-year survival of 20% as compared with a 2-year survival of 80% in those with a serum albumin greater than 40 g/l [23]. Serum albumin levels are not only affected by poor energy and protein intake, but also by other factors including inflammation, catabolic and anabolic processes, age, comorbidity, fluid overload (i.e. plasma volume) and urinary albumin losses [32,33]. Albumin synthesis is reduced during the acute phase response. The presence of acute or chronic inflammation limits the specificity of serum albumin as a nutritional marker. Measurements of serum albumin levels is inexpensive, easy to perform and widely available. Since there are currently more than fifty different methods for measuring serum albumin in laboratories, reference values should be known to all nephrologists especially when benchmarking is done in order to compare levels in between centres on the national or international level. The available literature suggests that prealbumin, also called transthyretin, may have unique validity among the panel of available biochemical nutritional indicators. However, no formal guideline was developed for serum prealbumin so far. Although predicting outcome, more mechanistic understanding of its functions is mandatory. Beside issues of reproducibility, costs inhibited implementation of prealbumin so far. Serum prealbumin is a more sensitive indicator for the nutrition status than albumin due to its shorter half life [34,35]. Prealbumin levels correlate strongly with serum albumin and have shown to provide prognostic value independent of albumin [36]. Because albumin is markedly influenced by inflammation as negative acute phase reactant its levels change more rapidly than prealbumin [37]. Therefore prealbumin is a good indicator of liver anabolic protein synthesis. The half life of serum ii51 prealbumin is approximately two days instead of 20 days for albumin [34,35]. Serum prealbumin levels lower than 0.3 g/l predict a relative mortality risk of 2.64 [36]. The patients 2-year survival rate was 50% with a serum prealbumin level <0.3 g/l and 90% in patients with a prealbumin level >0.3 g/l. Another cohort of 130 patients observed for 10 years demonstrated that each 0.01 g/l increase in serum prealbumin at enrolment was associated with a 9% decrease in the relative risk of death [38]. (G) Serum cholesterol Serum total cholesterol should be measured and be above the minimal laboratory threshold value (Evidence level III). Rationale and commentary Serum cholesterol is a component of the lipid profile, recommended for routine measurement, to assess the cardiovascular risk of a given haemodialysis patient [39,40]. Low (<1.5 g/l) or declining serum cholesterol concentrations are predictive of increased mortality risk [31,34,41–45]. Hypocholesterolaemia is associated with chronic protein–energy deficits and/or the presence of comorbid conditions, including inflammation. Individuals with low, low–normal (1.5–1.8 g/l), or declining serum cholesterol levels should be investigated for possible nutritional deficits as well as for other comorbid conditions. The relationship between serum cholesterol and outcome has been described as either ‘J-shaped’ or ‘U-shaped’ with increasing risk for mortality as serum cholesterol falls below approximately 2 g/l or rises above 2–3 g/l. Low levels of cholesterol are confounded by inflammation [45] and are influenced by the same comorbid conditions that affect other nutritional markers (e.g. serum albumin). Predialysis serum cholesterol correlates with serum albumin, prealbumin, creatinine and age [46]. If a patient takes lipid lowering drugs, these should be taken into account in the total cholesterol values. (H) Technical investigations Rationale For the assessment of malnutrition several technical tools are available such as bioelectrical impedance analysis (BIA), whole body dual energy X-ray absorptiometry (DXA), near infrared interactance (NIR) and in vivo neutron activation analysis. In addition the presence of malnutrition can be investigated by means of subjective global assessment. In vivo neutron activation analysis is considered the reference standard for the determination of protein ii52 malnourishment. In a sex- and age-matched study, Allman et al. [47] demonstrated that haemodialysis patients manifested a significantly lower total body nitrogen content, suggesting protein depletion. This observation was confirmed by Rayner et al in a larger group showing that nitrogen levels were more decreased in males (13%) than in females (4%). Later studies demonstrated that a significant proportion of haemodialysis patients had total body nitrogen depletion, expressed as a nitrogen index <80% being the ratio of measured nitrogen vs the predicted nitrogen for sex-, age- and height-matched controls [48–50]. This seems especially to be the case in older patients [48] and patients starting dialysis late i.e. at low levels of renal function [49]. Pollock et al. [48] demonstrated that patients with a nitrogen index of <80% had a relative risk of dying of 4.1 compared with patients with a higher index whereas Cooper et al. [51] found a hazard ratio of mortality of 1.6 per 10% of decline in nitrogen index. Several studies demonstrated that compared with in vivo neutron activation analysis, nutritional state analysis by means of anthropometry underestimated the presence of protein malnutrition in haemodialysis patients [47,50,52]. Studies comparing in vivo neutron activation analysis with BIA, DXA or NIR are lacking. DXA determines in a non-invasive way fat mass, fat-free mass and bone mineral mass and density from which body composition is computed. Thus, protein–energy nutritional status can be assessed. However, there are only limited data comparing DXA-determined body composition of haemodialysis patients with that of healthy subjects. Woodrow et al. [53] demonstrated that in comparison with control subjects patients on chronic haemodialysis have a significant reduction in lean tissue mass. In this study, the investigators also found similar reductions in fat-free mass with BIA, which were not found with skin-fold anthropometry. Data comparing nutritional status between haemodialysis patients and control subjects determined with BIA are scarce. Woodrow et al. [53] demonstrated with BIA a decrease in lean body mass in haemodialysis patients compared with healthy control subjects. Madore et al. [54] developed an impedance index with which they could demonstrate in a small group of haemodialysis patients that fat mass and lean body mass were significantly reduced in 50% of patients compared with the ideal value obtained from the NHANES II tables, suggesting the existence of malnutrition in these patients. Likewise, Maggiore et al. [55] demonstrated that haemodialysis patients after haemodialysis had lower body weight and a reduced phase angle compared with healthy controls. However, these investigators concluded that bioimpedance indexes were not reliable in detecting clinically overt lean body mass depletion albeit that phase angle was strongly related to patient survival [55]. Likewise, Woodrow et al. [56] found in patients with chronic renal failure compared with control subjects D. Fouque et al. larger errors with BIA and skin fold anthropometry compared with DXA, suggesting that the latter technique is the preferred one. Suggestion for future research Validation of the assessment of nutritional state by means of in vivo neutron activation analysis vs BIA, DXA and NIR. More frequent use of handgrip testing in clinical research studies. Guideline 2.2. Monitoring and follow-up of nutritional status Nutritional status should be followed using the following assessment tools (Opinion): (A) Dietary interviews (B) Body weight (C) nPNA, serum albumin and serum cholesterol The use of other technical investigations should be restricted to research purposes (Opinion). (A) Dietary interviews Stable and well-nourished haemodialysis patients should be interviewed by a qualified dietitian every 6–12 months or every 3 months if they are over 50 years of age or on haemodialysis for more than 5 years (Evidence level III). Malnourished haemodialysis patients should undergo at least a 24-h dietary recall more frequently until improved (Opinion). Rationale Dietary interviews are the best way to detect in time a reduced food intake before other objective malnutrition parameters start changing. Depending on staffing constraints a 3-day dietary recording or a 24-h recall of previous day intake should be performed, evaluated and findings must be noted in the patient’s care plan. During the same appointment any new dietary information can be implemented. Patients may need to be seen sooner if abnormal monthly blood tests require dietary intervention. Patients may request to visit the dietitian more often to alter parts of their dietary regimens or changes in their personal circumstances may indicate the need for additional information. Establishing a telephone help line and/or access to internet facilities enables dietitians and patients to communicate more frequently. The reasons for more frequent interviews in patients over 50 years of age and treated by haemodialysis for more than 5 years have been discussed in Guideline 1. EBPG guideline on nutrition ii53 Table 1. Significance of unplanned weight loss Unplanned weight loss in past 3–6 months (% body weight) Significance >10% of body weight 5–10% of body weight Clinically significant More than normal intra-individual variation (potentially significant)— early indicator of risk of malnutrition increased Within ‘normal’ intra-individual variation (small) <5% of body weight (B) Body weight Post dialysis body weight should be averaged over the month and percentage change in the average weight of the previous month, should be calculated (Opinion). Percent interdialytic weight gain (IDWG) should be based on ‘dry weight’ (post dialysis) (Evidence level III). Rationale It has been suggested that MHD patients should have been on MHD for 60 days as this can reflect ‘dry weight’ more accurately [12]. Ideal body weight (IBW) is the weight based on a range of BMI’s that yields the lowest morbidity and mortality rates. IBW may need to be adjusted in overweight and underweight patients. Unintentional weight loss during the previous 3–6 months period is more accurate as a risk factor for protein–energy malnutrition than BMI. This weight loss may be categorized according to the British Association of Parenteral and Enteral Nutrition (BAPEN) Malnutrition Advisory Group as in Table 1 [57]. Therefore, a simple cut-off of >10% weight loss during the last 3–6 months can be recommended for the diagnosis of malnutrition. Typically MHD patients are advised to keep IDWG between 2 and 2.5 kg. Current guidelines for daily fluid intake vary from 500 to 750 ml in addition to daily urine output. Thirst is dependent on dietary sodium (salt) intake and a high sodium intake will contribute to excessive IDWG and may not be the immediate result of food intake itself. Therefore, MHD patients must be advised to reduce their daily sodium (salt) intake to 5–6 g salt (Na 85–100 mmol). However, patients eating well also gain additional weight in between dialysis and this is due to the invisible fluid content of food. A ‘dry’ diet of 2100 Kcal can contain as much as 300–350 ml fluid and this adds to the daily fluid intake. It has been suggested by Sherman et al. [58] that IDWG could reflect nutritional intake. In a study of 860 randomly selected patients, a relationship between IDWG and nPCR was noted, a higher protein (g/kg) intake was associated with a higher IDWG, confirmed by a correlation analysis that dry weight and nPCR were independent factors (R ¼ 0.05). There was a small but significant positive association between IDWG and serum albumin concentrations: 3.78 vs 3.83 g/dl (P < 0.001) in patients with a <3% and >4.5% dry weight gain, respectively. Testa et al. [59] also found that dietary protein and energy intake was higher in patients with a higher IDWG of 4.5 1.5% during the 3 days interval. Dietary protein, energy and sodium intake were assessed from 3-day diet diaries from 32 patients, for each patient for 1 year. This study suggests that a stable IDWG may be a clinical indicator of adequate protein and energy intake and that the extent of IDWG was not directly related to blood pressure even in hypertensive patients. Some patients are afraid of gaining more then 2 kg in between dialysis treatment and this may affect their nutritional intake. Nutritional counselling is therefore important and should establish which patients eat well compared with those who do not and have a lower IDWG. Patients with large weight gains should nevertheless be challenged to assess what proportion is nutritive and non-nutritive fluid consumption. Staff should be aware of this when assessing compliance with dietary and fluid intake when discussing ‘individual ideal IDWG’ of 2 kg or less as this may be inappropriate for some patients. A percentage of dry body weight gain of 4–4.5% seems acceptable in patients with an optimal nutritional intake and observing salt restriction. Recommendation for future research Further studies are required to evaluate what constitutes an ‘ideal’ IDWG for the well nourished and what percentage is acceptable for hypertensive and cardiovascularly unstable MHD patients. (C) nPNA, serum albumin and serum cholesterol nPNA, serum albumin and serum cholesterol should be measured at presentation, 1 month after beginning of haemodialysis and three monthly thereafter in clinically stable patients (Opinion). In clinically unstable patients with a number of comorbidities, persistent inflammation, during periods of intensive dietary counselling and during therapeutic intervention the frequency of measurements should be increased to monthly intervals (Opinion). Rationale Albumin levels also reflect several non-nutritional factors which are frequently present in MHD patients, including inflammation and infection, urinary and dialysate losses as well as hydration status. Therefore, serum albumin alone is not a clinically useful measure ii54 for protein/energy nutritional status in MHD patients. Hypoalbuminaemia in MHD patients does not necessarily indicate protein–energy malnutrition, which also may not correlate with changes in other nutritional parameters. Normalized PNA is a valid estimate of protein intake, is well validated and simple to use in the clinical setting. It is important to monitor protein intake in MHD patients. However, there are limitations as well such as overestimation of dietary protein intake when the protein intake is <1 g/kg/day, possibly due to protein catabolism [60,61]. Normalizing PNA to body weight can be misleading in obese and volume overloaded patients. It is recommended that for individuals who are <90% or >115% of standardized body weight, the oedema-free adjusted body weight is used. Serum total cholesterol is part of the routine lipid profile measured in 3–6 month intervals according to changes in clinical status and during lipid modifying interventions [39]. Similar arguments apply for serum cholesterol as for serum albumin. Serum cholesterol may not correlate with changes in nutrition but also with changes in other nutritional parameters e.g. with those pointing to an activated acute phase reaction. Technical investigations are not recommended for routine follow up Rationale Changes in body composition reflecting nutritional status can be monitored with several techniques although the number of studies is limited and direct comparisons of these techniques with a gold standard are lacking. By means of in vivo neutron activation analysis a declining trend in the nitrogen index was found after 1 year in prevalent haemodialysis patients whereas the nitrogen index correlated with dietary calorie intake [48]. Pupim et al. [62] investigated nutritional parameters for 1 year in 50 incident haemodialysis patients including BIA every 3 months and DXA at the beginning and end of the year. BIA-derived fat mass as well as DXA-measured fat mass increased over time suggesting an improvement of nutritional status. This was not associated with a change in body mass of these patients, which was explained by a decrease in total body water. In prevalent chronic diabetic haemodialysis patients a decrease in DXA-determined fat mass was found after 1 year of treatment which was attributed to impaired nutritional status in these patients [63]. From these studies it can be concluded that technical tools can be used to monitor changes in body composition. Future research, however, should further clarify which method is the preferred one and with what intervals it should be applied. D. Fouque et al. References 1. Wiggins KL. Guidelines for Nutrition Care of Renal Patients. Renal Dietetic Practice Group, Am Diet Assoc, 3rd edn 2001; 1–101 2. Clinical practice guidelines for nutrition in chronic renal failure. K/DOQI, National Kidney Foundation. Am J Kidney Dis 2000; 35: S1–S140 3. Schoenfeld PY, Henry RR, Laird NM, Roxe DM. Assessment of nutritional status of the National Cooperative Dialysis Study population. Kidney Int Suppl 1983; 23: S80–S88 4. Thomas B. Manual of Dietetic Practice, Brit Diet Assoc, 3rd edn 2001: 30–37 5. Kloppenburg WD, Stegeman CA, Hooyschuur M, Van der Ven J, de Jong PE, Huisman RM. Assessing dialysis adequacy and dietary intake in the individual hemodialysis patient. Kidney Int 1999; 55: 1961–1969 6. Burrowes JD, Larive B, Cockram DB et al. Effects of dietary intake, appetite, and eating habits on dialysis and non-dialysis treatment days in hemodialysis patients: Crosssectional results From the HEMO study. J Renal Nutr 2003; 13: 191–198 7. Lou LM, Gimeno JA, Paul J et al. Evaluation of food intake in hemodialysis using a food consumption and appetite questionnaire. Nefrologia 2002; 22: 438–447 8. Kopple JD, Zhu X, Lew NL, Lowrie EG. Body weight-forheight relationships predict mortality in maintenance hemodialysis patients. Kidney Int 1999; 56: 1136–1148 9. Aparicio M, Cano N, Chauveau P et al. Nutritional status of haemodialysis patients: a French national cooperative study. French Study Group for Nutrition in Dialysis. Nephrol Dial Transplant 1999; 14: 1679–1686 10. Leavey SF, Strawderman RL, Jones CA, Port FK, Held PJ. Simple nutritional indicators as independent predictors of mortality in hemodialysis patients. Am J Kidney Dis 1998; 31: 997–1006 11. Leavey SF, McCullough K, Hecking E, Goodkin D, Port FK, Young EW. Body mass index and mortality in ‘healthier’ as compared with ‘sicker’ haemodialysis patients: results from the Dialysis Outcomes and Practice Patterns Study (DOPPS). Nephrol Dial Transplant 2001; 16: 2386–2394 12. Abbott KC, Glanton CW, Trespalacios FC et al. Body mass index, dialysis modality, and survival: analysis of the United States Renal Data System Dialysis Morbidity and Mortality Wave II Study. Kidney Int 2004; 65: 597–605 13. Chauveau P, Combe C, Laville M et al. Factors influencing survival in hemodialysis patients aged older than 75 years: 2.5-year outcome study. Am J Kidney Dis 2001; 37: 997–1003 14. Chumlea WC, Dwyer J, Bergen C et al. Nutritional status assessed from anthropometric measures in the HEMO study. J Renal Nutr 2003; 13: 31–38 15. Combe C, Chauveau P, Laville M et al. Influence of nutritional factors and hemodialysis adequacy on the survival of 1,610 French patients. Am J Kidney Dis 2001; 37: S81–S88 16. Pifer TB, McCullough KP, Port FK et al. Mortality risk in hemodialysis patients and changes in nutritional indicators: DOPPS. Kidney Int 2002; 62: 2238–2245 17. Kalantar-Zadeh K, Kopple JD, Block G, Humphreys MH. Association among SF36 quality of life measures and nutrition, hospitalization, and mortality in hemodialysis. J Am Soc Nephrol 2001; 12: 2797–2806 18. Cooper BA, Bartlett LH, Aslani A, Allen BJ, Ibels LS, Pollock CA. Validity of subjective global assessment as a nutritional marker in end-stage renal disease. Am J Kidney Dis 2002; 40: 126–132 19. Oe B, de Fijter CW, Oe PL, Stevens P, de Vries PM. Four-site skinfold anthropometry (FSA) versus body impedance analysis (BIA) in assessing nutritional status of patients on maintenance EBPG guideline on nutrition 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. hemodialysis: which method is to be preferred in routine patient care? Clin Nephrol 1998; 49: 180–185 Kamimura MA, Jose Dos Santos NS, Avesani CM, Fernandes Canziani ME, Draibe SA, Cuppari L. Comparison of three methods for the determination of body fat in patients on long-term hemodialysis therapy. J Am Diet Assoc 2003; 103: 195–199 Kopple JD, Jones MR, Keshaviah PR et al. A proposed glossary for dialysis kinetics. Am J Kidney Dis 1995; 26: 963–981 Shinaberger CS, Kilpatrick RD, Regidor DL, et al. Longitudinal associations between dietary protein intake and survival in hemodialysis patients. Am J Kidney Dis 2006; 48: 37–44 Kaysen GA, Chertow GM, Adhikarla R, Young B, Ronco C, Levin NW. Inflammation and dietary protein intake exert competing effects on serum albumin and creatinine in hemodialysis patients. Kidney Int 2001; 60: 333–340 Dwyer JT, Larive B, Leung J et al. Are nutritional status indicators associated with mortality in the Hemodialysis (HEMO) Study? Kidney Int 2005; 68: 1766–1776 Lowrie EG, Lew NL. Death risk in hemodialysis patients: the predictive value of commonly measured variables and an evaluation of death rate differences between facilities. Am J Kidney Dis 1990; 15: 458–482 Iseki K, Yamazato M, Tozawa M, Takishita S. Hypocholesterolemia is a significant predictor of death in a cohort of chronic hemodialysis patients. Kidney Int 2002; 61: 1887–1893 Foley RN, Parfrey PS, Harnett JD, Kent GM, Murray DC, Barre PE. Hypoalbuminemia, cardiac morbidity, and mortality in end-stage renal disease. J Am Soc Nephrol 1996; 7: 728–736 Owen WF, Jr., Lew NL, Liu Y, Lowrie EG, Lazarus JM. The urea reduction ratio and serum albumin concentration as predictors of mortality in patients undergoing hemodialysis. N Engl J Med 1993; 329: 1001–1006 Owen WF, Lowrie EG. C-reactive protein as an outcome predictor for maintenance hemodialysis patients. Kidney Int 1998; 54: 627–636 Beddhu S, Kaysen GA, Yan G et al. Association of serum albumin and atherosclerosis in chronic hemodialysis patients. Am J Kidney Dis 2002; 40: 721–727 Lowrie EG, Huang WH, Lew NL. Death risk predictors among peritoneal dialysis and hemodialysis patients: a preliminary comparison. Am J Kidney Dis 1995; 26: 220–228 Stenvinkel P, Barany P, Chung SH, Lindholm B, Heimburger O. A comparative analysis of nutritional parameters as predictors of outcome in male and female ESRD patients. Nephrol Dial Transplant 2002; 17: 1266–1274 Kaysen GA. Biological basis of hypoalbuminemia in ESRD. J Am Soc Nephrol 1998; 9: 2368–2376 Avram MM, Mittman N, Bonomini L, Chattopadhyay J, Fein P. Markers for survival in dialysis: a seven-year prospective study. Am J Kidney Dis 1995; 26: 209–219 Goldwasser P, Michel MA, Collier J et al. Prealbumin and lipoprotein(a) in hemodialysis: relationships with patient and vascular access survival. Am J Kidney Dis 1993; 22: 215–225 Chertow GM, Ackert K, Lew NL, Lazarus JM, Lowrie EG. Prealbumin is as important as albumin in the nutritional assessment of hemodialysis patients. Kidney Int 2000; 58: 2512–2517 Ingenbleek Y, Carpentier YA. A prognostic inflammatory and nutritional index scoring critically ill patients. Int J Vitam Nutr Res 1985; 55: 91–101 Mittman N, Avram MM, Oo KK, Chattopadhyay J. Serum prealbumin predicts survival in hemodialysis and peritoneal dialysis: 10 years of prospective observation. Am J Kidney Dis 2001; 38: 1358–1364 European Best Practice Guidelines in Haemodialysis (Part 1). Section VII. Vascular disease and risk factors. Nephrol Dial Transplant 2002; 17 [Suppl 7]: 88–109 ii55 40. K/DOQI clinical practice guidelines for management of dyslipidemias in patients with kidney disease. Am J Kidney Dis 2003; 41: 1–91 41. Piccoli GB, Quarello F, Salomone M et al. Are serum albumin and cholesterol reliable outcome markers in elderly dialysis patients? Nephrol Dial Transplant 1995; 10 [Suppl 6]: 72–77 42. Degoulet P, Legrain M, Reach I et al. Mortality risk factors in patients treated by chronic hemodialysis. Report of the Diaphane collaborative study. Nephron 1982; 31: 103–110 43. Iseki K, Miyasato F, Tokuyama K et al. Low diastolic blood pressure, hypoalbuminemia, and risk of death in a cohort of chronic hemodialysis patients. Kidney Int 1997; 51: 1212–1217 44. Goldwasser P, Mittman N, Antignani A et al. Predictors of mortality in hemodialysis patients. J Am Soc Nephrol 1993; 3: 1613–1622 45. Liu Y, Coresh J, Eustace JA et al. Association between cholesterol level and mortality in dialysis patients: role of inflammation and malnutrition. JAMA 2004; 291: 451–459 46. Cano N, Di Costanzo-Dufetel J, Calaf R et al. Prealbuminretinol-binding-protein-retinol complex in hemodialysis patients. Am J Clin Nutr 1988; 47: 664–667 47. Allman MA, Allen BJ, Stewart PM et al. Body protein of patients undergoing haemodialysis. Eur J Clin Nutr 1990; 44: 123–131 48. Pollock CA, Ibels LS, Allen BJ et al. Total body nitrogen as a prognostic marker in maintenance dialysis. J Am Soc Nephrol 1995; 6: 82–88 49. Cooper BA, Aslani A, Ryan M, Ibels LS, Pollock CA. Nutritional state correlates with renal function at the start of dialysis. Perit Dial Int 2003; 23: 291–295 50. Arora P, Strauss BJ, Borovnicar D, Stroud D, Atkins RC, Kerr PG. Total body nitrogen predicts long-term mortality in haemodialysis patients – a single-centre experience. Nephrol Dial Transplant 1998; 13: 1731–1736 51. Cooper BA, Penne EL, Bartlett LH, Pollock CA. Protein malnutrition and hypoalbuminemia as predictors of vascular events and mortality in ESRD. Am J Kidney Dis 2004; 43: 61–66 52. Rayner HC, Stroud DB, Salamon KM et al. Anthropometry underestimates body protein depletion in haemodialysis patients. Nephron 1991; 59: 33–40 53. Woodrow G, Oldroyd B, Turney JH, Tompkins L, Brownjohn AM, Smith MA. Whole body and regional body composition in patients with chronic renal failure. Nephrol Dial Transplant 1996; 11: 1613–1618 54. Madore F, Wuest M, Ethier JH. Nutritional evaluation of hemodialysis patients using an impedance index. Clin Nephrol 1994; 41: 377–382 55. Maggiore Q, Nigrelli S, Ciccarelli C, Grimaldi C, Rossi GA, Michelassi C. Nutritional and prognostic correlates of bioimpedance indexes in hemodialysis patients. Kidney Int 1996; 50: 2103–2108 56. Woodrow G, Oldroyd B, Smith MA, Turney JH. Measurement of body composition in chronic renal failure: comparison of skinfold anthropometry and bioelectrical impedance with dual energy X-ray absorptiometry. Eur J Clin Nutr 1996; 50: 295–301 57. Todorovic V, Russell C, Stratton R, Ward J, Elia M. A Guide to the Malnutrition Universal Screening Tool (MUST) for Adults. Brit Ass Parent Enteral Nutr (BAPEN) 2003. 58. Sherman RA, Cody RP, Rogers ME, Solanchick JC. Interdialytic weight gain and nutritional parameters in chronic hemodialysis patients. Am J Kidney Dis 1995; 25: 579–583 59. Testa A, Plou A. Clinical determinants of interdialytic weight gain. J Ren Nutr 2001; 11: 155–160 60. Lorenzo V, de BE, Rufino M et al. Caloric rather than protein deficiency predominates in stable chronic haemodialysis patients. Nephrol Dial Transplant 1995; 10: 1885–1889 ii56 61. Enia G, Sicuso C, Alati G, Zoccali C. Subjective global assessment of nutrition in dialysis patients. Nephrol Dial Transplant 1993; 8: 1094–1098 62. Pupim LB, Kent P, Caglar K, Shyr Y, Hakim RM, Ikizler TA. Improvement in nutritional parameters after initiation of chronic hemodialysis. Am J Kidney Dis 2002; 40: 143–151 63. Okuno S, Ishimura E, Kim M et al. Changes in body fat mass in male hemodialysis patients: a comparison between diabetics and nondiabetics. Am J Kidney Dis 2001; 38: S208–S211 Guideline 3. Recommendations for protein and energy intake Guideline 3.1. Recommended protein intake The dietary protein intake in clinically stable chronic haemodialysis patients should be at least 1.1 g protein/kg ideal body weight/day (Evidence level III). The achieved nPNA in a clinically stable chronic haemodialysis patient should be at least 1.0 g/ideal body weight/day (Evidence level III). Rationale The prevalence rate of protein–energy malnutrition in chronic haemodialysis patients ranges from 20% to 70% with an average of 40% [1–3]. A poor nutrient intake is the most frequent cause for malnutrition in MHD patients. Observational or interventional clinical trials have reported patients’ spontaneous intakes to be as low as 20–25 kcal/kg/day and/or 0.8–1.0 g/kg protein/day [4,5]. Although some patients may do well with slightly lower intakes than recommended, the general dialysis population should be advised to reach a minimal protein intake of 1.1 g protein/kg/day. Protein intake should be taken with a sufficient energy intake (e.g. 30–40 kcal/kg/day, see Recommendation 3.2) to guarantee an optimal metabolic balance. Protein requirements. There has been controversy regarding the optimal protein intake in MHD patients since clinical studies are scarce and their duration is usually too short (on average less than 10 days) to obtain valid conclusions. In healthy adults, metabolic studies include nitrogen balances during many days or weeks, and whole body as well as regional (at tissue level such as forearm) amino acid turnover studies. Values reported in these studies are expressed as a mean SD. However, when transferred to the general population, a mean experimental value of a minimal intake means that 50% of subjects will be covered whereas 50% will not be adequately covered by the proposed level. Since there is no method for identifying those patients who will not be in balance by eating this mean value, the World Health Organization defined a ‘population level’ by adding 2 SDs of the mean to the protein intake obtained through metabolic studies [6]. This ‘population level’ is therefore considered safe, since it will ensure that 97.5% of patients would get D. Fouque et al. enough protein to balance their needs. Consequently, this also implies that almost half of the subjects will be counselled to achieve a protein intake above their individual needs. This is the reason why a given subject can remain in metabolic equilibrium, e.g. in adequate nutritional status when receiving a protein intake less than recommended. For healthy young adults, the most recent recommendations have slightly increased the daily protein intake towards 0.8–0.85 g/kg body weight [6,7]. Furthermore, in a recent meta-analysis, it was not possible to recommend different values for elderly people, nor was it possible to find marked differences in requirement according to the nature of animal or vegetable protein [7]. Thus, a balanced intake of high quality animal protein and vegetable protein source should be proposed. Protein requirements in the normal population chronic haemodialysis. During routine haemodialysis, protein requirements do not appear to be sufficient for the following reasons. First, the dialysis treatment induces a loss of nutrients (glucose, amino acids, vitamins and trace elements) through the dialysis filter, which may even be more important today in response to the use of more porous membranes and/or more efficient techniques such as haemofiltration [8,9]. Second, the dialysis procedure itself is a catabolic event responsible for protein catabolism (fragmentation of albumin, release of pro-inflammatory cytokines, role of heparin) [9–15]. For example, in response to the rapid decrease in plasma amino acid at the start of the haemodialysis session, muscle proteolysis occurs in order to maintain an adequate plasma and cellular amino acid concentration [16,17]. This catabolic event may lead to muscle wasting over the long term. Feeding patients during the dialysis session through regular meals, special liquid feeding or parenteral administration has been shown to revert this catabolic state and should be used as frequently as possible [11,17,18]. Some authors have hypothesized that, during the non-dialysis days, the catabolic stress may not be present or even be replaced by an anabolic response [19]. Nutrient intake may vary according to the dialysis schedule: food intake was greater by approximately 10% on non-dialysis days than on dialysis days [5], an observation not confirmed by Kloppenburg et al. [20]. During a standard threeweekly dialysis schedule, food intake was recently reported to be spontaneously reduced by 40% on the last day of the long interdialysis interval, probably in order to avoid fluid overload [21].This last observation fits well with the previous report from Sherman et al. [22] showing that patients with a reduced interdialytic weight gain (<3% dry weight) had a mean nPNA of 0.94 g/kg BW/day, as compared with those who had an interdialytic weight gain >4% corresponding to a nPNA of 1.17 g/kg BW/day. Research data in dialysis patients indicate that in most metabolic studies performed in adult chronic dialysis patients, a protein intake of 0.8–0.85 g/kg BW/day or less was constantly associated with a EBPG guideline on nutrition negative metabolic balance [23–27]. When protein intake averaged 1.1 g/kg/day or more, most patients showed neutral or positive balance [23–27] but not all [28]. These observations have led many investigators to recommend a safety level of protein intake of 1.2 g/kg BW/day. After publication of previous nutritional guidelines in renal disease [29, 30], sporadic reports have challenged these recommendations, by reporting good nutritional status in patients eating less protein [31,32]. These observations may have been obtained in selected patients, and for the safety reasons detailed above, lower levels of protein intake should not be recommended for the general dialysis population. Protein intake and nutritional status in epidemiological studies in maintenance dialysis. In a cross-sectional survey of more than 7400 haemodialysis patients, Aparicio et al. [4] showed that serum albumin reached a plateau of 39.3 g/l for a PNA of 1–1.2 g/kg/day, but no superior serum albumin values were observed in patients with greater nPNAs. Additional data have recently been obtained from prospective epidemiological studies [33–35]. Ohkawa et al. [33] reported in 127 MHD patients that body composition, as assessed by CT scan, was maintained constant with a level of protein intake of 0.9–1.1 g protein/kg/day, and that there was no clinical or biochemical benefit for the patients eating more than 1.1 g protein/kg/day. Kloppenburg and colleagues performed a randomized cross-over trial comparing two levels of protein intake (0.9 vs 1.1 g/kg BW/day) for 40 weeks each in 45 haemodialysis patients [36]. They did not observe significant changes in nutritional parameters between the two diets which were comparable in terms of energy intake (28–30 kcal/kg BW/day). In a secondary analysis of the HEMO study, serum albumin was shown to be positively associated with protein intake (assessed by equilibrated normalized PCR) only between 0.4 and 1.0 g/kg/day, without further benefit on serum albumin for a nPCR > 1.0 [37]. Is a protein intake greater than 1.2 g/kg/day harmful in chronic haemodialysis? Although larger protein intakes may not improve nutritional status, they may possibly be associated with better survival: in a 2-year prospective follow-up of more than 1600 chronic haemodialysis patients in France, higher nPNA was associated with higher survival by univariate analysis [34]. More recently, the same group reported increased survival in patients with an nPNA between 1.24 and 1.46 g/kg BW/day, as compared with the quartiles having an nPNA lower than 1.24. Survival was not further improved in the upper quartile of patients taking 1.46 g protein and above [35]. In another recent 1-year prospective study, Kalantar et al. [38] reported an inverse relationship between PNA (mean value, 1.13 0.29 g/kg/day, range 0.5–2.15) and mortality or hospitalization rate in 122 patients adequately dialysed (Kt/V > 1.2). Protein intake and CKD mineral and bone disease. Elevated protein intakes are not dissociable ii57 from an increase in dietary phosphate, which has led some investigators to warn against a potential increase in vascular calcification. Most clinical trials have specifically addressed the question of dietary phosphate restriction only in CKD stages 2 and 3, well before end-stage renal disease (stage 5), in an attempt to prevent secondary hyperparathyroidism [39]. Once dialysis treatment is started however, the relationship between dietary phosphate and hyperphosphataemia is less straightforward, since bone metabolism and intestinal absorption become the focus of complex interactions and new therapeutic interventions [40]. In 39 patients undergoing a 80-week randomized cross-over trial, Kloppenburg et al. [36] reported that two different protein intakes (0.94 vs 1.15 g/kg IBW/day, estimated from food reports, corresponding to a nPNA of 0.9 and 1.0 g/kg/day, respectively) were not associated with different serum phosphate levels (1.88 0.40 vs 1.89 0.39 mmol/l, respectively). Serum phosphate was markedly influenced by the dialysis dose, being lower in the greater dialysis dose group (1.77 0.30 vs 2.01 0.41 mmol/l for Kt/Vs of 1.26 0.14 and 1.02 0.08, respectively), underlining the predominant importance of the dialysis dose over the protein intake in controlling serum phosphate and the phosphocalcic product. Many individuals may have a high serum phosphate without eating a large quantity of proteins, possibly from a greater intestinal fractional absorption of phosphate and the influence of vitamin D therapy, and these patients may better benefit from oral phosphate binders than from a reduction in their protein intake. In contrast, low serum phosphate is frequently associated with low protein intake in patients undergoing regular 4-h or shorter haemodialysis sessions. Indeed, Lorenzo et al. [41] reported that patients with a serum phosphate <4 mg/dl did eat 0.86 0.3 g protein/kg BW/day whereas those with a serum phosphate >4 mg/dl had a protein intake of 1.05 0.4 g/kg/day. Finally, and most importantly, there is no prospective clinical trial to show that the vascular risk associated with elevated serum phosphorus or calcium phosphate product occurs in response to a high protein intake. Protein intake and frequency of haemodialysis. The frequency of the dialysis sessions should be considered when analysing nutritional intake. Indeed, fear of overload or pulmonary oedema may significantly limit food intake during the interdialytic interval, particularly during the long 3-day period [21]. Switching patients to a daily haemodialysis program, either long noctural or short 2-h, has been reported to augment protein intake up to 40%, an increase that was sustained over 1 year and associated with improved serum albumin in almost all pilot studies [42]. The reasons for this improved nutrient intake is probably due to the lifting of the fluid restriction and other general limitations of food intake, especially for those nutrients containing phosphate and/or potassium. ii58 Protein intake and inflammation. Inflammation, which has been repeatedly reported in 20–50% of routine haemodialysis patients, may impair nutritional status by different mechanisms such as increased anorexia and/or protein catabolism [37,43]. Controversial debate occurs as to wether protein intake may reverse impaired nutritional status in the presence of chronic inflammation. In a randomized dietary intervention study, Leon et al. [44] showed that it was possible to increase serum albumin over 6 months in haemodialysis patients by simple dietary counselling, and this improvement also occurred when chronic inflammation was present. In an ancillary analysis of the HEMO study in more than 1000 MHD patients, Kaysen et al. [37] showed that serum albumin was independently influenced by either protein intake or inflammation status. Indeed, serum albumin correlated positively with protein intake (as assessed by ‘nPCR’) only for a protein intake <1.0 g/kg/day, with no further benefit above, and there was no inflammation impact on serum albumin for C reactive protein (CRP) values <13 mg/l [37]. These authors suggested that the independent effect of protein intake might positively impact on nutritional status of inflamed patients with a CRP > 13 mg/l. A comparable observation has been reported by Chauveau and colleagues [35] in a recent prospective cohort of more than 400 MHD patients. These authors showed that the 2-year survival of patients with a serum CRP > 10 mg/l was superior for the patients with a nPNA 1.2 g/kg/day. Thus, the relationship between chronic inflammation, dietary intake and nutritional status still remains unclear but may suggest that malnourished inflamed patients may benefit from increased protein intakes. Thus from these studies, it seems that nutritional status does not much improve when protein intake is 1.0–1.2 g/kg/day or above, whereas there might be a sustained protective effect on morbi-mortality for protein intakes slightly above these nutritional recommendations. These hypotheses should be confirmed in larger specifically designed prospective studies. Practically however, if an individual dialysis patient eats slightly less (0.9–1.0 g/kg/day) than recommended and presents with a stable nutritional status, in absence of superimposed disease or catabolic event, and until further survival studies become available, his/her protein intakes may be maintained under the recommended level unless clinical and/or biochemical nutritional indices worsen. Recommendation for further research Which PNA gives the best survival in chronic haemodialysis? Formula for normalizing PNA. Specific protein needs for malnourished HD patients (may differ from well-nourished patients). Effect of dialysis techniques on nutritional status (haemofiltration, daily dialysis, etc.) on appetite and D. Fouque et al. their relationship with appetite regulatory factors (leptin, ghrelin). Effects of higher protein intake on malnourished inflamed patients. Relationship between protein intake, vascular calcification and bone metabolism. Guideline 3.2. Recommended energy intake The recommended energy intake in a clinically stable chronic haemodialysis patient should be 30–40 kcal/kg IBW/day, adjusted to age, gender and to the best estimate of physical activity level (Evidence level III). Regular physical activity should be encouraged, and energy intake should be increased proportionally to the level of physical activity (Opinion). Rationale Energy metabolism in chronic kidney disease. Energy metabolism may be impaired during CKD, in response to metabolic disorders such as insulin resistance and impaired triglyceride utilization, carnitine deficiency, hyperparathyroidism, metabolic acidosis, chronic inflammation and the haemodialysis procedure itself [45]. However, except in severely sick patients, these abnormalities do not seem to greatly affect resting energy expenditure (REE) [45– 50]. Indeed, even if some activities or treatments impact on energy metabolism in CKD, this will occur for only short periods of time in the entire nycthemere and the resulting overcost may not significantly alter the daily energy expenditure (DEE) [6,51]. Energy expenditure has even been shown to be reduced in CKD patients as compared with control subjects [51,52]. The main reason for altered energy metabolism seems therefore to be a predominant deficit in energy intake rather than an increase in energy expenditure. Indeed, many reports in MHD showed energy intake being as low as 20–22 kcal/kg BW/day [53–56]. When normalized by lean body mass, REE may be more elevated in MHD than in peritoneal dialysis for yet unexplained reasons [57], but this normalization does not reflect a general consensus until now [45,53]. How to estimate daily energy expenditure? Estimation of daily energy expenditure (DEE) has been performed by different research tools including indirect calorimetry (sequential or continuous over 24 h or more), deuterated water, physical activity questionnaires, and Harris-Benedict or Schofield formulas [6,47,48,57–60]. Daily energy expenditure strongly depends on the active metabolic mass, e.g. lean body mass, but is independent on fat mass [48]. Since excess energy intake is rapidly stored in fat tissue in the body, the optimal daily energy intake (DEI) in a stable adult equals his/her daily energy expenditure. A detailed individual calculation of DEI firstly includes the estimation of resting energy expenditure (REE) also EBPG guideline on nutrition ii59 called basal metabolic rate, strongly influenced by thermic conditions including ambiant temperature, and thyroid function. Resting energy expenditure (REE) can be estimated as follows: lifestyle (AF of 1.4), will have a DEE of approximately 1500 kcal/day, e.g. 30 kcal/kg/day. A 30-year very active male, weighting 80 kg with a height of 1.80 m, will have a REE of 1900 kcal/day, and his DEE will be 1900 1.7 ¼ 3230 kcal, e.g. 40 kcal/kg/day. 3.2.1 By the use of the Schofield tables reported by the WHO [6]: Males Females 18 30 years 15:3 BW þ 679 14:7 BW þ 496 30 60 years 11:6 BW þ 879 8:7 BW þ 829 > 60 years 13:5 BW þ 487 10:5 BW þ 596 The WHO recommendations obtained through the Schofield tables (see equation 3.2.1) have been recently challenged, and newer studies have reported measured daily energy expenditure to be even lower by 8–14% and 16–20% in sedentary adult women and men, respectively [62,63]. Elderly people have a decline in REE in response to a 3% loss of lean body mass per decade and their activity factor was estimated to be low, at about 1.45. In the most recent dietary reference intakes released by the Food and Nutrition board (Institute of Medicine, Washington, USA), to determine someone’s energy requirement, the DEE is estimated for a 30-year old adult and then reduced by 7 and 10 kcal/year for age above 30 [63]. Blanc et al. [59] reported that the WHO recommendations led to a 10% overestimation of daily energy expenditure in elderly women (mean age, 75 year), underlining the need for further research in larger cohorts of patients. Thus, from the most recent publications in the field, it seems that energy requirements could be lower than previously reported. Finally, there is a metabolic adaptation to a reduced energy intake, which includes a decrease in resting energy expenditure, both from a loss of active lean body mass, but also through an improved efficiency of energy metabolism, as recently showed by Friedlander et al. [64]. Thus, even though their energy intake does not reach the recommended values, malnourished patients may still benefit from a relative increase in their nutritional intake, from spontaneous or supplemental oral intake, or from oral or parenteral sources during the dialysis session [11,18,65]. where REE is expressed in kcal/day and body weight (BW) in kg 3.2.2 By the use of Harris-Benedict equations as follows: For men: REE ¼ 66 þ (13.7 BW) þ (5 H) (6.8 A) For women: REE ¼ 655.1 þ (9.6 BW) þ(1.8 H) (4.7 A) where REE is expressed in kcal/day, body weight (BW) in kg, height (H) in cm and age (A) in years. 3.2.3 By the use of Black equations [61] as follows: For men: REE ¼ 259 BW0.48 H0.50 A0.13 For women: REE ¼ 230 BW0.48 H0.50 A0.13 where REE is expressed in kcal/day, body weight (BW) in kg, height (H) in m and age (A) in years. The third important and highly variable determinant of daily energy expenditure (DEE) is physical activity. To obtain the optimal DEE, REE should be multiplied by an activity factor, which greatly depends on the type and the duration of professional and recreational activities. This factor is generally comprised between 1.3 and 2, with a mean of 1.5 in most publications [59] with an upper limit of 2.2 in case of extemely high physical activity, an uncommon condition in routine dialysis (see [6] for detailed calculations). Thus, daily energy expenditure (DEE) can be estimated as follows: Daily energy expenditure (i.e. daily energy requirement): DEEðkcal=dayÞ ¼ 1:51 REE 1 activity factor could vary from 1.2 to 2 (see text for comments) Examples: A 40-year male weighting 75 kg, with a height of 1.75 m will have a REE of about 1700 kcal/day. If he develops a moderate but significant activity, his DEE will be 1700 1.5, e.g. 2550 kcal per day, equal to 34 kcal/kg/day. A frail elderly woman, aged 75, with a weight of 50 kg and a height of 1.60 m and a very sedentary How to estimate daily energy intake? Since energy intake in excess of expenditure is rapidly stored as fat in a stable well-nourished haemodialysis patient, the optimal energy intake equals his/her daily energy expenditure. In contrast to protein, estimation of energy intake can only be done by monitoring intake and not by collecting any fluid parameter. There are a lot of difficulties in performing diet collections, among which dietitian availability and patient training, knowledge and perception of exact food intake, time consumption and cost. Precision of food reports are limited and may artefactually underestimate patients’ true energy intake, the magnitude of underestimation being greater in patients with larger BMIs, in both men and women [58]. From a recent analysis from 40 MHD patients, Kloppenburg et al. [66] measured basal metabolic rate and obtained self reports of energy intake. Whereas in general, the daily energy expenditure cannot be lower than 1.2-1.3 REE (see above), these authors found that 60% of patients had an ii60 energy intake report lower than 1.27 REE. Since these patients did not present with symptoms of chronic malnutrition, the authors suggested that daily energy intake was notably underestimated. The underreporting of energy intake could be improved by increasing the number of dietary interviews: it has been shown that at least four different 3-day dietary interviews separated each by 1 month were necessary to reduce the intraindividual variability of reports [67], the impact of dialysis or non-dialysis day schedule [5], but 5–7 days appear optimal [20]. In addition, a 7-day collection is more conform with reality of intakes, since there is in some patients an important spontaneous intake reduction the ‘seventh-day’, e.g. the last day of the long interdialytic interval, [21]. Training should be performed, including spouse and/or relatives to help identifying nutrient type and size of servings since patients are not able to clearly identify the different sources of nutrients [44]. Finally, it should be emphasized that energy intake cannot be derived from other reported food components. Indeed, for a same amount of protein intake, the variability of energy intake between patients is too large to draw any reliable relationship between protein and energy intake [68]. Thus, physical activity determination and reported dietary energy intake will be the best estimate of patients’ needs. Is energy intake sufficient in MHD patients? After the publication of previous guidelines [29,30], there was some disagreement between the recommended values as compared with what was reported in observational studies [54–56]. Most epidemiological studies have reported energy intakes lower than recommended, and being as little as 20–25 kcal/kg BW/day. Thus, when clinical or biological indices of malnutrition are found in a given patient (see Guideline 2), a nutritional work-up should be rapidly performed. However, if there is no clear sign of ongoing malnutrition or (a) catabolic process or processes, a number of facts may partly explain the discrepancy between low reported energy intake and patient’s nutritional status. There could be a true inadequate energy intake that will lead to reduced physical activity, altered protein metabolism and muscle losses: this could be corrected by active nutritional support (see Guideline 5). Alternatively, individual energy expenditure was not correctly assessed, in case of a more reduced than estimated physical activity, which is frequent in chronically haemodialysed patients: thus the true energy needs are closer to 30 kcal/kg/day or may even be slightly less in elderly sedentary women (see above formules for calculation). A third event is the potential underestimation of energy intake through the food reports or dietary interviews, an occurrence recently confirmed in healthy adults [69] as well as in renal failure patients [45,53,66,70]. Energy intake can be markedly increased in MHD patients by administering oral supplements [71,72]. Daily amounts of 500 kcal could be delivered quite easily and the benefits related to these interventions D. Fouque et al. have been recently reported to be better than previously expected (see Guideline 5). Increasing the frequency of dialysis to daily sessions has allowed a generous increase in energy intake in recent reports [42,73]. These interventions have been associated with weight gain, both from fat and lean body mass. In summary, estimating energy needs and energy intake is a skilled task, and recent findings have underlined the following points: (1) there is a trend for lowering the daily energy requirements in healthy adults, particularly in women; (2) energy expenditure should be more closely matched to physical activity, which may be very variable between individuals, and particularly reduced in dialysis patients; (3) almost all methods for monitoring daily energy intake, even when used by a trained staff, do underestimate actual energy intake. Whether this information applies to dialysis patients is not fully known and may be the scope for further research. However, these points partly explain why, in routine practice, patients may do acceptably well despite recorded energy intakes lower than previously recommended. References 1. Cianciaruso B, Brunori G, Kopple JD et al. Cross-sectional comparison of malnutrition in continuous ambulatory peritoneal dialysis and hemodialysis patients. Am J Kidney Dis 1995; 26: 475–486 2. Marcen R, Teruel JL, de la Cal MA et al. The impact of malnutrition in morbidity and mortality in stable haemodialysis patients. Spanish Cooperative Study of Nutrition in Hemodialysis. Nephrol Dial Transplant 1997; 12: 2324–2331 3. Park YK, Kim JH, Kim KJ et al. A cross-sectional study comparing the nutritional status of peritoneal dialysis and hemodialysis patients in Korea 1999. J Renal Nutr 9: 149–156 4. Aparicio M, Cano N, Chauveau P et al. Nutritional status of haemodialysis patients: a French national cooperative study. French Study Group for Nutrition in Dialysis. Nephrol Dial Transplant 1999; 14: 1679–1686 5. Burrowes JD, Larive B, Cockram DB et al. Effects of dietary intake, appetite, and eating habits on dialysis and non-dialysis treatment days in hemodialysis patients: cross-sectional results From the HEMO study. J Renal Nutr 2003; 13: 191–198 6. Energy and protein requirements. Report of a joint FAO/WHO/ UNU Expert Consultation. World Health Organ Tech Rep Ser 1985; 724: 1–206 7. Rand WM, Pellett PL, Young VR. Meta-analysis of nitrogen balance studies for estimating protein requirements in healthy adults. Am J Clin Nutr 2003; 77: 109–127 8. Ikizler TA, Flakoll PJ, Parker RA et al. Amino acid and albumin losses during hemodialysis. Kidney Int 1994; 46: 830–837 9. Combarnous F, Tetta C, Cellier CC et al. Albumin loss in on-line hemodiafiltration. Int J Artif Organs 2002; 25: 203–209 10. Raj DS, Zager P, Shah VO et al. Protein turnover and amino acid transport kinetics in end-stage renal disease. Am J Physiol Endocrinol Metab 2004; 286: E136–E143 11. Veeneman JM, Kingma HA, Boer TS et al. Protein intake during hemodialysis maintains a positive whole body protein balance in chronic hemodialysis patients. Am J Physiol Endocrinol Metab 2003; 284: E954–E965 12. Gutierrez A, Alvestrand A, Wahren J et al. Effect of in vivo contact between blood and dialysis membranes on protein catabolism in humans. Kidney Int 1990; 38: 487–494 EBPG guideline on nutrition 13. Ikizler TA, Pupim LB, Brouillette JR et al. Hemodialysis stimulates muscle and whole body protein loss and alters substrate oxidation. Am J Physiol Endocrinol Metab 2002; 282: E107–E116 14. Lofberg E, Essen P, McNurlan M et al. Effect of hemodialysis on protein synthesis. Clin Nephrol 2000; 54: 284–294 15. Veeneman JM, Kingma HA, Boer TS et al. The metabolic response to ingested protein is normal in long-term hemodialysis patients. Am J Kidney Dis 2004; 43: 330–341 16. Raj DS, Welbourne T, Dominic EA et al. Glutamine kinetics and protein turnover in end-stage renal disease. Am J Physiol Endocrinol Metab 2005; 288: E37–E46 17. Lim VS, Ikizler TA, Raj DS et al. Does hemodialysis increase protein breakdown? Dissociation between whole-body amino acid turnover and regional muscle kinetics. J Am Soc Nephrol 2005; 16: 862–868 18. Pupim LB, Flakoll PJ, Brouillette JR et al. Intradialytic parenteral nutrition improves protein and energy homeostasis in chronic hemodialysis patients. J Clin Invest 2002; 110: 483 19. Lim VS, Yarasheski KE, Flanigan MJ. The effect of uraemia, acidosis, and dialysis treatment on protein metabolism: a longitudinal leucine kinetic study. Nephrol Dial Transplant 1998; 13: 1723–1730 20. Kloppenburg WD, Stegeman CA, Hooyschuur M et al. Assessing dialysis adequacy and dietary intake in the individual hemodialysis patient. Kidney Int 1999; 55: 1961–1969 21. Bellizzi V, Di Iorio BR, Terracciano V et al. Daily nutrient intake represents a modifiable determinant of nutritional status in chronic haemodialysis patients. Nephrol Dial Transplant 2003; 18: 1874–1881 22. Sherman RA, Cody RP, Rogers ME et al. Interdialytic weight gain and nutritional parameters in chronic hemodialysis patients. Am J Kidney Dis 1995; 25: 579–583 23. Kopple JD, Shinaberger JH, Coburn JW et al. Optimal dietary protein treatment during chronic hemodialysis. Transactions – Am Soc Art Int Org 1969; 15: 302–308 24. Ikizler TA, Greene JH, Yenicesu M et al. Nitrogen balance in hospitalized chronic hemodialysis patients. Kidney Int 1996; 57: S53–S56 25. Borah MF, Schoenfeld PY, Gotch FA et al. Nitrogen balance during intermittent dialysis therapy of uremia. Kidney Int 1978; 14: 491–500 26. Lim VS, Flanigan MJ, Zavala DC et al. Protective adaptation of low serum triiodothyronine in patients with chronic renal failure. Kidney Int 1985; 28: 541–549 27. Rao M, Sharma M, Juneja R et al. Calculated nitrogen balance in hemodialysis patients: influence of protein intake. Kidney Int 2000; 58: 336–345 28. Slomowitz LA, Monteon FJ, Grosvenor M et al. Effect of energy intake on nutritional status in maintenance hemodialysis patients. Kidney Int 1989; 35: 704–711 29. Clinical practice guidelines for nutrition in chronic renal failure. K/DOQI, National Kidney Foundation. Am J Kidney Dis 2000; 35: S1–S140 30. Toigo G, Aparicio M, Attman PO et al. Expert working group report on nutrition in adult patients with renal insufficiency (Part 2 of 2). Clin Nutr 2000; 19: 281–291 31. Uribarri J. The obsession with high dietary protein intake in ESRD patients on dialysis: is it justified? Nephron 2000; 86: 105–108 32. Lim VS, Flanigan MJ. Protein intake in patients with renal failure: comments on the current NKF-DOQI guidelines for nutrition in chronic renal failure. Semin Dial 2001; 14: 150–152 33. Ohkawa S, Kaizu Y, Odamaki M et al. Optimum dietary protein requirement in nondiabetic maintenance hemodialysis patients. Am J Kidney Dis 2004; 43: 454–463 34. Combe C, Chauveau P, Laville M et al. Influence of nutritional factors and hemodialysis adequacy on the survival of 1610 French patients. Am J Kidney Dis 2001; 37: S81–S88 ii61 35. Chauveau P, Bourdenx J, Montaudon D et al. Interaction between nutrition and inflammation in the Bordeaux study of inflammation in chronic hemodialysis patients (BICHE): 2 years follow-up. J Am Soc Nephrol 2004; 15: Abs 36. Kloppenburg WD, Stegman CA, Kremer Hovinga TK et al. Effect of prescribing a high protein diet and increasing the dose of dialysis on nutrition in stable chronic haemodialysis patients: a randomized, controlled trial. Nephrol Dial Transplant 2004; 9: 1212–23 37. Kaysen GA, Greene T, Daugirdas JT et al. Longitudinal and cross-sectional effects of C-reactive protein, equilibrated normalized protein catabolic rate, and serum bicarbonate on creatinine and albumin levels in dialysis patients. Am J Kidney Dis 2003; 42: 1200–1211 38. Kalantar-Zadeh K, Supasyndh O, Lehn RS et al. Normalized protein nitrogen appearance is correlated with hospitalization and mortality in hemodialysis patients with Kt/V greater than 1.20. J Renal Nutr 2003; 13: 15–25 39. K/DOQI clinical practice guidelines for bone metabolism and disease in chronic kidney disease. Am J Kidney Dis 2003; 42: S1–S201 40. Locatelli F, Cannata-Andia JB, Drueke TB et al. Management of disturbances of calcium and phosphate metabolism in chronic renal insufficiency, with emphasis on the control of hyperphosphataemia. Nephrol Dial Transplant 2002; 17: 723–731 41. Lorenzo V, Martin M, Rufino M et al. Protein intake, control of serum phosphorus, and relatively low levels of parathyroid hormone in elderly hemodialysis patients. Am J Kidney Dis 2001; 37: 1260–1266 42. Fouque D, Guebre-Egziabher F, Laville M. Advances in anabolic interventions for malnourished dialysis patients. J Ren Nutr 2003; 13: 161–165 43. Kaysen GA, Chertow GM, Adhikarla R, et al. Inflammation and dietary protein intake exert competing effects on serum albumin and creatinine in hemodialysis patients. Kidney Int 2001; 60: 333–340 44. Leon JB, Majerle AD, Soinski JA et al. Can a nutrition intervention improve albumin levels among hemodialysis patients? A pilot study. J Renal Nutr 2001; 11: 9–15 45. Cuppari L, Avesani CM. Energy requirements in patients with chronic kidney disease. J Ren Nutr 2004; 14: 121–126 46. Monteon FJ, Laidlaw SA, Shaib JK et al. Energy expenditure in patients with chronic renal failure. Kidney Int 1986; 30: 741–747 47. Ikizler TA, Wingard RL, Sun M et al. Increased energy expenditure in hemodialysis patients. J Am Soc Nephrol 1996; 7: 2646–2653 48. Tabakian A, Juillard L, Laville M et al. Effects of recombinant growth factors on energy expenditure in maintenance hemodialysis patients. Miner Electrolyte Metab 1998; 24: 273–278 49. Schneeweiss B, Graninger W, Stockenhuber F et al. Energy metabolism in acute and chronic renal failure. Am J Clin Nutr 1990; 52: 596–601 50. Cuppari L, de Carvalho AB, Avesani CM et al. Increased resting energy expenditure in hemodialysis patients with severe hyperparathyroidism. J Am Soc Nephrol 2004; 15: 2933–2939 51. Veeneman JM, Kingma HA, Stellaard F et al. Oxidative metabolism appears to be reduced in long-term hemodialysis patients. Am J Kidney Dis 2005; 46: 102–110 52. Avesani CM, Draibe SA, Kamimura MA et al. Decreased resting energy expenditure in non-dialysed chronic kidney disease patients. Nephrol Dial Transplant 2004; 19: 3091–3097 53. Kloppenburg WD, de Jong PE, Huisman RM. Low calorie intake in dialysis patients: an alternative explanation. Am J Kidney Dis 1999; 33: 1202–1204 54. Rocco MV, Paranandi L, Burrowes JD et al. Nutritional status in the HEMO Study cohort at baseline. Hemodialysis. Am J Kidney Dis 2002; 39: 245–256 ii62 55. Thunberg BJ, Swamy AP, Cestero RV. Cross-sectional and longitudinal nutritional measurements in maintenance hemodialysis patients. Am J Clin Nutr 2005; 34: 2005–2012 56. Schoenfeld PY, Henry RR, Laird NM et al. Assessment of nutritional status of the National Cooperative Dialysis Study population. Kidney Int 1983; 23: S80–S88 57. Neyra R, Chen KY, Sun M et al. Increased resting energy expenditure in patients with end-stage renal disease. J Parenter Enteral Nutr 2003; 27: 36–42 58. Livingstone MB, Black AE. Markers of the validity of reported energy intake. J Nutr 2003; 133 [Suppl 3]: 895S–920S 59. Blanc S, Schoeller DA, Bauer D et al. Energy requirements in the eighth decade of life. Am J Clin Nutr 2004; 79: 303–310 60. Schofield WN. Predicting basal metabolic rate, new standards and review of previous work. Hum Nutr Clin Nutr 1985; 39 [Suppl 1]: 5–41 61. Black AE, Coward WA, Cole TJ et al. Human energy expenditure in affluent societies: an analysis of 574 doubly-labelled water measurements. Eur J Clin Nutr 1996; 50: 72–92 62. Alfonzo-Gonzalez G, Doucet E, Almeras N et al. Estimation of daily energy needs with the FAO/WHO/UNU 1985 procedures in adults: comparison to whole-body indirect calorimetry measurements. Eur J Clin Nutr 2004; 58: 1125–1131 63. Trumbo P, Schlicker S, Yates AA et al. Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein and amino acids. J Am Diet Assoc 2002; 102: 1621–1630 64. Friedlander AL, Braun B, Pollack M et al. Three weeks of caloric restriction alters protein metabolism in normal weight, young men. Am J Physiol Endocrinol Metab 2005; 289: E446–E455 65. Pupim LB, Flakoll PJ, Ikizler TA. Nutritional supplementation acutely increases albumin fractional synthetic rate in chronic hemodialysis patients. J Am Soc Nephrol 2004; 15: 1920–1926 66. Kloppenburg WD, de Jong PE, Huisman RM. The contradiction of stable body mass despite low reported dietary energy intake in chronic haemodialysis patients. Nephrol Dial Transplant 2002; 17: 1628–1633 67. Laville M, Fouque D: Nutritional aspects in hemodialysis. Kidney Int Suppl 2000; 76: S133–S139 68. Black AE, Bingham SA, Johansson G et al. Validation of dietary intakes of protein and energy against 24 hour urinary N and DLW energy expenditure in middle-aged women, retired men and post-obese subjects: comparisons with validation against presumed energy requirements. Eur J Clin Nutr 1997; 51: 405–413 69. Slimani N, Bingham S, Runswick S et al. Group level validation of protein intakes estimated by 24-hour diet recall and dietary questionnaires against 24-hour urinary nitrogen in the European Prospective Investigation into Cancer and Nutrition (EPIC) calibration study. Cancer Epidemiol Biomarkers Prev 2003; 12: 784–795 70. Avesani CM, Kamimura MA, Draibe SA et al. Is energy intake underestimated in nondialyzed chronic kidney disease patients? J Renal Nutr 2005; 15: 159–165 71. Allman MA, Stewart PM, Tiller DJ et al. Energy supplementation and the nutritional status of hemodialysis patients. Am J Clin Nutr 1990; 51: 558–562 72. Stratton R, Bircher G, Fouque D et al. Multi-nutrient oral supplements and tube feeding in maintenance dialysis: a systematic review and meta-analysis. Am J Kidney Dis 2005; 46: 387–405 73. Galland R, Traeger J, Arkouche W et al. Short daily hemodialysis rapidly improves nutritional status in hemodialysis patients. Kidney Int 2001; 60: 1555–1560 D. Fouque et al. 4. Recommendations for vitamins, minerals and trace elements administration in MHD patients Due to insufficient evidence from clinical trials for recommending administration of vitamins, the following information only reflects the expert’s opinion and cannot be considered as a clinical guideline but a recommendation. 4.1. Vitamins Abnormal renal metabolism, inadequate intake and/or gastrointestinal absorption and dialysis losses, account for vitamin deficiencies amongst dialysis patients. Losses are even greater with high-flux and high-efficiency dialysis. Vitamin deficiency progresses slowly depending on body stores, nutritional intake and chronic dialysis losses. Vitamin status in individual patients depends on age, gender, actual vitamin intake, previous supplementation, dialysis losses, residual renal function, time on dialysis and types of dialysers in addition to impaired metabolism. Ideally vitamin supplements should be tailored to individual needs. Overt clinical manifestations include depressed immune system, neuropathy and impaired amino acid and lipid metabolism, mild scurvy and other abnormalities. The most frequently observed vitamin disturbances concern water soluble vitamins and these may be supplemented daily or administered after dialysis, three times weekly, which promotes compliance. In a recent prospective cohort study, the DOPPS evaluated the relative risk (RR) for hospitalization and mortality in 16 345 MHD patients from 308 randomly selected renal centres in Europe, Japan and USA [1]. There were large regional variations in the percentage of patients who received various multivitamin types of water soluble vitamins. In Europe, this ranged from 3.7% in the United Kingdom to 6.4% in Italy and 37.9% in Spain; it was 5.6% in Japan as compared with 71.9% in the US. Possible reasons for these large variations may be due to differences in cost, health insurance coverage, patient’s preferences and patients and medical staff health beliefs regarding efficacy as several short-term studies have in the past not shown benefits. The DOPPS evaluation showed a 16% reduction in the relative risk for mortality in MHD patients taking water soluble vitamins [2]. However, only a prospective randomized controlled trial would prove that water soluble vitamin supplementation improves outcomes. The authors meanwhile proposed that while awaiting further more robust evidence, prescription of water soluble vitamin supplements, being of minimal medical risk, could be proposed to the patients [1]. If administered, watersoluble vitamin supplements should be taken or infused at the end of the dialysis session. Patients should be discouraged to purchase regular vitamin EBPG guideline on nutrition ii63 and mineral supplements over the counter as requirements differ from those for healthy people, and some formulas include vitamins that are not recommended in maintenance dialysis. 4.1.1 Water-soluble vitamins Thiamine (B1) A daily supplement of 1.1–1.2 mg thiamin hydrochloride is recommended Rationale. Thiamine deficiency is responsible for beriberi, a rare condition in MHD patients. Vitamin B1 deficiency may also be evoked in case of atypical neurological symptoms (Wernicke encephalitis). Thiamine is strongly removed during haemodialysis. Thiamine plasma concentration may not reflect its biological activity. Thiamine intake in MHD patients can range from 0.6 to 1.5 mg/day depending on individual food consumption, and is mainly contained in pork meat, beer and dried vegetables [3]. Patients with a poor nutritional intake, as may occur in the elderly, are most likely to benefit from supplementation. Thiamine has been administered in amounts up to 300 mg/week in patients undergoing high-flux haemodialysis [4]. Presently, all renal multivitamin formulas include thiamine, from 1.5 mg (NephroviteÕ , Dialyvite3000Õ , DiatxÕ , USA, RenavitÕ , Germany), 3 mg (RenaxÕ , USA) to 50 mg (DialvitÕ , Switzerland) per tablet. Riboflavin (B2) A daily supplement of 1.1–1.3 mg is recommended Rationale. Although it is well cleared during haemodialysis, not tightly bound to proteins, riboflavin deficiency is uncommon. A supplement of 1.1–1.3 mg is equal to the recommended daily allowance of healthy people and is sufficient to supplement inadequate nutritional intake and dialysis losses [3]. Riboflavin is contained in milk, bread and cereals, lean meat and egg. Presently, all renal multivitamin formulas include riboflavin, from 1.7 mg (NephroviteÕ , Dialyvite3000Õ , USA, RenavitÕ , Germany), 2 mg (RenaxÕ , USA) to 10 mg (DialvitÕ , Switzerland) per tablet. Pyridoxine (B6) A daily supplement of 10 mg hydrochloride is recommended as pyridoxine Rationale. There is evidence that plasma and red cell pyridoxine levels are low in MHD patients. Although the pyridoxine recommended dietary allowance in healthy adults is 1.3–1.7 mg, the use of erythropoietin (EPO) may increase requirements because of increased erythropoiesis. Some drugs and other substances interfere with pyridoxine metabolism, an additional cause for deficiency. A decreased level of pyridoxine may be associated with hyperhomocysteinaemia, but the benefit of supplementation is as yet unclear [3,5]. Pyridoxine is contained in yeast, cereal buds, green vegetables, egg yolk and meat. A supplement of 10 mg/day is recommended as this is the lowest pyridoxine hydrochloride dose that has consistently normalized pyridoxine deficiency and the transamination activation index of stable MHD patients. Pyridoxine supplementation given to correct hyperoxalaemia or hyperhomocysteinaemia is still a controversial issue. High doses of pyridoxine hydrochloride (200–600 mg daily) should be avoided as these have been associated with peripheral neuropathy. Presently, all renal multivitamin formulas include pyridoxine, 10 mg (NephroviteÕ , Dialyvite3000Õ , USA, RenavitÕ , Germany), 15 mg (RenaxÕ , USA), 40 mg (DialvitÕ , Switzerland) and 50 mg (Diatx ZnÕ , USA) per tablet. Ascorbic Acid (vitamin C) A daily supplement of 75–90 mg is recommended. Rationale. Vegetables and fresh fruit are the main sources of vitamin C but these foods are often restricted or need to be avoided in a potassium restricted diet, resulting in an inadequate intake. In addition, vitamin C is inactivated by heat during cooking. Vitamin C is readily removed by dialysis as reported by Wang et al. [6]. Serum levels fell by 30–40% after a single dialysis session and losses from 80 to 280 mg per dialysis session have been reported [3]. Vitamin C deficiency contributes to a mild form of scurvy sometimes seen in MHD patients, may lead to abnormal amino acid metabolism and disturbances in folic acid metabolism. Although high-flux dialysis techniques increase vitamin C losses, Descombes et al. [4] reported normal plasma ascorbate values in patients receiving 500 mg vitamin C at the end of the dialysis session thrice weekly. Vitamin C supplements appear to improve functional iron deficiency and hence the response to EPO [7–9]. Vitamin C supplementation may help to relieve muscle cramps. In a double blind randomized trial, 60 MHD patients, divided into four groups, daily received either vitamin E (400 mg), vitamin C (250 mg), either vitamins or a placebo for 8 weeks [10]. Muscle cramps significantly improved in patients receiving both vitamins E and C (97%), vitamin E alone (54%), vitamin C (61%) as compared with only 7% of placebo-treated patients [10]. More recently, Deicher et al. [11] reported that, in MHD patients followed for 30 months, total vitamin C plasma levels were predictive of mortality, with a risk of dying at least three times greater in the plasma vitamin C tertiles <60 mmol/l, suggesting to keep patients plasma vitamin C levels above this target. Further studies are required to explore safety, to what extend patients are vitamin deficient, and whether other dialysis factors may increase removal. High doses of vitamin C (e.g. superior to 500–1000 mg daily) should however be avoided in MHD patients because of tissue oxalate deposition in response to increased ii64 D. Fouque et al. serum oxalates not cleared by the failing kidney. Presently, renal multivitamin formulas generally include vitamin C, e.g. 50 mg (RenaxÕ , USA), 60 mg (NephroviteÕ , Diatx ZnÕ , USA, RenavitÕ , Germany), 100 mg (Dialyvite3000Õ , USA) and 200 mg (DialvitÕ , Switzerland) per tablet. vitamin B12 equal to the requirement, e.g. 2.4 mg/day, seems safe. Presently, most but not all renal multivitamin formulas include vitamin B12, 6 mg (NephroviteÕ , DialyviteÕ , USA, RenavitÕ , Germany), 12 mg (RenaxÕ , USA) and 1 mg (Dialyvite3000Õ , USA) per tablet. Folic Acid (Folate, vitamin B9) A daily supplement recommended. of 1 mg folic acid is Rationale. In MHD patients, folic acid levels may be reduced in serum and red blood cells and induce megaloblastic anaemia. Folic acid is contained in yeast, liver, green vegetables, fruit and meat. Because of impaired intestinal absorption, ethanol or drug interaction and dialysate losses, particularly with high flux/high efficiency dialysis [12], it is prudent to prescribe 1 mg folic acid/day to prevent deficiency. This may be insufficient to lower elevated plasma homocysteine levels as the administration of 5–10 mg/ day has shown a plasma homocysteine reduction by 30–50% [3]. Indeed, the National Kidney Foundation Task Force on Cardiovascular Disease issued a report with recommendations for treatment of hyperhomocysteinaemia [13]. It was recommended that MHD patients should receive daily 5 mg folic acid, 50 mg pyridoxine and 400 mg vitamin B12, to reduce serum homocysteine levels and protect against cardiovascular disease. Presently, all renal multivitamin formulas include folic acid, 0.8 mg (RenavitÕ , Germany), 1 mg (NephroviteÕ , DialyviteÕ , USA), 3 mg (Dialyvite 3000Õ , USA, DialvitÕ , Switzerland) and 5 mg (Diatx ZnÕ , USA) per tablet. B12 (cobalamin) A daily supplement of 2.4 mg vitamin B12 is recommended. Rationale. Vitamin B12 or cobalamin, combined with the gastric intrinsic factor, are necessary factors for an optimal folate metabolism, a normal nonmegaloblastic erythropoiesis and to avoid nervous system demyelinization observed in pernicious anaemia. Cobalamin is found in sufficient amounts in meat, liver, seafood, milk and egg yolk. Vitamin B12 undergoes an enterohepatic cycling. Most MHD patients present plasma levels of cobalamin in the normal range, whether they receive vitamin B12 supplements or not. Administration of vitamin B12 has been shown to improve or correct nerve conduction velocity in MHD patients having low vitamin B12 plasma levels [14]. Vitamin B12, when administered for 1 mg monthly, is also efficient in decreasing serum homocysteinaemia by 10% [15]. Since there is no clear report of vitamin B12 toxicity even for high vitamin B12 doses, i.e. 2.5 mg three times weekly [16], and because some dialysis patients have an intake below the daily requirements, a daily supplement of Niacin (vitamin B3, nicotinamide, nicotinic acid, vitamin PP) A daily supplement recommended. of 14–16 mg niacin is Rationale. Niacin is contained in meat, fish, dry vegetables, coffee and tea. A deficit in niacin store results in signs of pellagra, a dermatosis associated with diarrhea and dementia, as soon as 50–60 days after a complete dietary niacin removal. However, pellagra has never been reported in a chronic dialysis patient. Niacin undergoes a rapid metabolic clearance and does not seem to be cleared by dialysis. Pharmacological niacin doses improve lipid profile by increasing serum HDL and decreasing LDL cholesterol fraction and serum triglycerides. Since many MHD patients have limited intakes of food containing niacin, it is recommended to supplement patients with the required allowance of normal adults, e.g. 14–16 mg daily. Recently, niacin, given at about 1000 mg daily has been reported to efficiently decrease serum phosphate by 20% in hyperphosphataemic MHD patients, by inhibiting intestinal phosphate transport [17]. A mild thrombopenia was recently reported as a side effect of this treatment dose in maintenance dialysis [18]. High doses of niacin have been alternatively proposed for controlling dyslipidaemia and reduce cardiovascular risk in non-renal patients [19]. Side effects of high-dose niacin (1000–1500 mg daily) include flushes and impaired glucose metabolism [20]. Thus, high doses of niacin should be prescribed with great caution in dialysis patients, since no long-term clinical trial has been performed in these patients. Presently, many renal multivitamin formulas include niacin, 20 mg (NephroviteÕ , DialyviteÕ , Dialyvite3000Õ , Diatx ZnÕ , RenaxÕ , USA, RenavitÕ , Germany) per tablet. Biotin (vitamin B8) A daily supplement of 30 mg biotin is recommended. Rationale. Major sources of biotin (vitamin B8) include yeast, egg yolk, liver, soybean, mushrooms and cauliflower. Biotin deficiency may be responsible for depression, somnolence, hyperesthaesia, anorexia and dermatosis, symptoms often present to a certain extent in MHD patients. In renal patients, a decrease in intestinal biotin absorption has been reported, as well as a plasma biotin decrease during the dialysis session [3]. Furthermore, food intakes that are low in protein are also low in biotin and do not meet the minimal daily biotin requirement. An adequate biotin EBPG guideline on nutrition intake has been proposed at 30 mg/day, and for the aforementioned reasons, it seems prudent to recommend this value also to MHD patients. Clearly, further studies are needed to better address the biotin needs in maintenance dialysis. Presently, many renal multivitamin formulas include biotin, 150 mg (NephrocapsÕ , USA) and 300 mg (DialyviteÕ , Diatx ZnÕ , NephroviteÕ , RenaxÕ , USA, RenavitÕ , Germany) per tablet. Pantothenic acid (vitamin B5) A daily supplement of 5 mg pantothenic acid is recommended. Rationale. Pantothenic acid is widely spread in many food including liver, kidney, fresh vegetables and egg yolk. It plays an important role in b-oxidation, free fatty acid and amino acid oxidation and protein acylation. To date, there is no clear information on pantothenic acid stores for MHD patients. Pantothenic acid is cleared by dialysis, and although no data are yet available, newer more efficient techniques might increase pantothenate losses. Since diets low in protein may not provide the adequate daily needs (5 mg/day), it is recommended that MHD patients take a supplement of 5 mg/day. Further research is warranted on pantothenic acid dialysate losses and stores in dialysis patients. Presently, many renal multivitamin formulas include pantothenic acid, 5 mg (NephrocapsÕ , USA) and 10 mg (NephroviteÕ , DialyviteÕ , Diatx ZnÕ , RenaxÕ , USA, RenavitÕ , Germany) per tablet. 4.1.2 Fat-soluble vitamins Vitamin D is not considered in this section as its metabolism, effect and administration in MHD patients depend on phosphocalcic metabolism and bone status, and has been the focus of a recent set of guidelines [21]. Vitamin A (retinol) A daily intake of 700–900 mg is recommended. Vitamin A supplements are not recommended. Rationale. Vitamin A is found in dairy products, fish oil, liver, spinach and carrots. Vitamin A is necessary for night vision and epithelium maintenance. Serum plasma levels of vitamin A are elevated in patients with chronic kidney disease. Vitamin A is not removed during MHD and deficiencies are rare and mostly related to inadequate nutritional intake. Vitamin A toxicity includes hypercalcaemia, anaemia and hypertriglyceridaemia. In order to prevent vitamin A toxicity, supplements containing larger amounts than 700–900 mg/day should not be given to MHD patients. Patients receiving total parenteral nutrition (TPN) may require vitamin A supplements, but not greater than 700–900 mg/day [3,5]. ii65 Vitamin E (alpha-tocopherol) A daily supplement of 400–800 IU is recommended in secondary prevention of cardiovascular events and for preventing recurrent muscle cramps. Rationale. Vitamin E is a strong antioxidant and cell membrane protector. Vitamin E is mainly found in vegetable oils (corn, sunflower and soybean) and wheat germs. Vitamin E plasma levels are not influenced by the dialysis session, and no vitamin E is found in the spent dialysate. There is no decrease in vitamin E plasma levels in long-term MHD patients [22]. The potential benefits of vitamin E supplementation were addressed in a large randomized controlled trial (Secondary Prevention with Antioxidants of Cardiovascular disease in End-stage renal disease, SPACE). A total of 196 MHD patients with preexisting cardiovascular disease were randomly assigned to either a treatment group (97 patients) receiving 800 IU vitamin E or a control group (99 patients) receiving a placebo. Patients were followed up for a median of 519 days. The primary end point was myocardial infarction, ischaemic stroke, peripheral vascular disease, unstable angina. Sixteen percent of patients on vitamin E vs 33% on placebo proceeded to a primary endpoint and 5.1% on vitamin E vs 17.2% on placebo suffered from myocardial infarction, both reductions being highly significant in favour of the use of vitamin E [23]. Vitamin E supplementation appears to be effective in reducing the incidence of leg cramps. Roca et al. [24] compared the effect of quinine and vitamin E in 40 patients with a history of leg cramps who were randomized to either quinine 325 mg or vitamin E 400 IU taken daily at bedtime for 2 months. Quinine and vitamin E were equally effective in reducing cramps as compared with the wash-out period, but due to potential toxicity of quinine, vitamin E should be recommended as treatment of choice [24]. As shown previously for vitamin C in the Khajehdehi et al. trial [10], vitamin E (400 mg daily) alone or in combination with vitamin C (250 mg daily) was able to alleviate muscle cramps significantly when patients receiving both vitamins E and C (97%) or vitamin E alone (54%) whereas only 7% of the placebo group patients improved [10]. Presently, some but not all renal multivitamin formulas include vitamin E, 30 IU (Dialyvite3000Õ , USA) and 35 IU (RenaxÕ , USA) per tablet. Vitamin K A daily intake of 90–120 mg is recommended. There is no need for vitamin K supplementation, except in patients receiving long term antibiotic treatment or those with altered coagulant activity; a daily amount of 10 mg vitamin K may be temporarily administered. Rationale. Vitamin K is contained in green leaves vegetables (cabbage, spinach) and cow milk. ii66 Vitamin K undergoes intestinal reabsorption through enterohepatic cycling, which may be reduced during oral antibiotic administration. Vitamin K (K for Koagulation in german) is essential in promoting synthesis of II, VII, IX and X coagulation factors but also of some coagulation inhibitors such as factor C, S and Z. Vitamin K is a cofactor for the g-carboxylation of glutamate in proteins (GLAproteins) such as the matrix GLA-protein and osteocalcin, explaining a potential role of vitamin K deficiency in patients with bone fractures. In addition, high plasma vitamin K levels have been associated with soft tissue calcifications in MHD patients and elevated serum parathormone values were found in patients with a low plasma vitamin K level [25]. The daily recommended allowance for healthy individuals is 90–120 mg [26]. There is no evidence that MHD patients suffer from vitamin K deficiency. Patients who are treated with antibiotics for prolonged periods and who have a poor nutritional intake may benefit from a 10 mg/day vitamin K supplement. Patients receiving TPN may require 7.5 mg vitamin K per week [5]. 4.2. Minerals Phosphate (phosphorus) A daily intake of 800–1000 mg phosphate is recommended. Dietary education improves phosphate control. Dietary phosphate control should not compromise protein intake. Rationale. Dietary phosphate intake should be restricted in MHD patients to avoid hyperphosphataemia leading to secondary hyperparathyroidism. The consequences and treatment of hyperphosphataemia are well known and have been reviewed recently in the context of the management of renal bone disease [21,27]. Foods with a high protein content may contain 12–16 mg phosphate per gram protein, with dairy products having the highest ratio. Thus, a protein intake of 80 g (optimal for a MHD patient weighing 70 kg) will bring about 1100 mg phosphate daily. Since 40–80% of the oral phosphate load will be absorbed, depending on vitamin D administration, the net phosphate gain for two days will be 800–1700 mg. Because one standard haemodialysis session can only clear 500–700 mg phosphate, this will result in a positive phosphate balance, an increase in calcium–phosphate product, an increase in serum parathyroid hormone and a greater cardiovascular risk [21]. However, compromising protein intake at the expense of phosphate restriction should be avoided. Foods high in protein but with the least amount of phosphate should preferably be prescribed through a detailed dietitian interview. Hyperphosphataemia should be treated by intensive counselling, by increasing phosphate binders and D. Fouque et al. by reviewing the dialysis regimen as appropriate. It has recently been shown in a randomized dietary intervention trial that MHD patients who received extra counselling on the phosphate content of food and a detailed report of their own phosphocalcic laboratory parameters, they reduced their serum phosphate and calcium phosphate product by 23% (P < 0.01 for both parameters) after 6 months of intervention [28]. More frequent dialysis sessions (e.g. short daily or long nightly schedules) have been reported in pilot studies to improve control of hyperphosphataemia despite increased protein and phosphate intake [29]. Longer duration of dialysis (‘t’ from Kt/V) also helps to improve control serum phosphate, as well as increasing the dialysis membrane surface. Calcium The total intake of elemental calcium should not exceed 2000 mg/day including calcium obtained from calcium-based phosphate binders. Rationale. Calcium intake may be limited due to dietary phosphate restriction (milk and dairy products). Overall, a mean food calcium intake is comprised between 500 and 800 mg/day. However, other sources of calcium include calcium-based phosphate binders, and thus the total daily intake of calcium could be much greater, leading to a positive calcium balance, vascular calcifications and episodes of hypercalcaemia. For these reasons, the total amount of oral calcium intake including calcium-based phosphate binders should not exceed 2000 mg daily, and non-calcium phosphate binders should be used if hyperparathyroidism is not controlled. The consequences and treatment of altered phosphocalcic metabolism have been extensively reviewed in recent guidelines regarding the management of renal bone disease and metabolism [21]. Sodium and fluid A daily intake of no more than 80–100 mmol (2000–2300 mg) sodium or 5–6 g (75 mg/kg BW) per day of sodium chloride is recommended. Interdialytic weight gain (IDWG) should not exceed 4–4.5% of dry body weight. Rationale. The importance of controlling interdialytic weight gain (IDWG) by restricting dietary sodium (and fluid intake) and the preference for using lower sodium dialysate, has been described in the Haemodynamic Instability Guideline 2.1. With progressive loss of urine output, sodium and fluid restrictions are vital to control extra cellular volume, blood pressure and to prevent excessive IDWG in anuric and oliguric MHD patients. By reducing the sodium load from diet and dialysate, the lesser urge for patients to quench their EBPG guideline on nutrition thirst improves compliance with fluid restriction and reduces IDWG. A reduction in sodium intake to 80–100 mmol/l (5–6 g salt) in addition to lowering the dialysate sodium concentration from 140 to 135 mmol/l appears to be sufficient to suppress thirst and hence excessive weight gain. This also benefits blood pressure control and might result in the withdrawal of antihypertensive treatment in some patients [30]. The majority of dietary sodium, 70–80%, is derived from salt and mono sodium glutamate added to food at home, in restaurants and food outlets or by food manufacturers. Examples of some convenience foods are: ready to eat meals, cured meat and fish products, canned and processed foods. The salt content of some staple foods such as breakfast cereals (i.e. cornflakes), bread, butter and margarine and sandwich fillings contribute significantly to dietary sodium intake. In anuric patients, each 8 g NaCl (140 mmol Naþ) requires 1 l of fluid intake to maintain normal serum sodium. Dietary Naþ intake (mmol) may be calculated from average daily fluid weight gain (kg) average serum Naþ concentration (mmol/l). An 80 kg dialysis patient with 4% IDWG, will have 12 g NaCl intake per day. Current guidelines for daily fluid intake vary from 500 to 1000 ml in addition to daily urine output to achieve an IDWG of 2–2.5 kg or 4–4.5% dry body weight. Some dialysis centres include the amount of ‘hidden’ fluid in food in fluid allowance prescriptions. Individual fluid allowances need to be adapted for patients living in warmer climates, during periods of hot weather, working in hot environments and as a result of clinical conditions (high fever). However, it is more efficient to carefully monitor salt rather than fluid intake, since as a response to salt intake, thirst will regulate the subsequent fluid ingested. All foods that are liquid at room temperature (18–208C) should be counted as fluid except oil and foods with a high fat or sugar content. Reducing sodium and fluid in addition to a potassium and phosphate restriction and ensuring that protein and energy intake is adequate, is difficult and a stepwise approach to educate the patient is most important. MHD patients must be advised to avoid those convenience foods that contain potassium chloride or other potassium containing additives to replace salt. ii67 for hyperkalaemia should also be investigated and corrected such as metabolic acidosis together with a review of drug therapies that contribute to hyperkalaemia such as angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, spironolactone, b-blockers, non-steroidal anti-inflammatory drugs and other contributing drug therapies. Tissue destruction (e.g. catabolism) as a result of trauma or weight loss releases potassium from intracellular space and results in hyperkalaemia in haemodialysis patients [31]. 4.3. Trace elements Iron (Fe) A daily intake of 8 mg Fe for men and 15 mg for women is recommended. Supplementary Fe should be given to all haemodialysis patients treated with an erythropoiesisstimulating agent (ESA), to maintain adequate serum transferrin and serum ferritin levels, aimed to achieve a target haemoglobin (Hb) concentration >110 g/l or a haematocrit >33%, except for those receiving the iron intravenously. Rationale. The Institute of Medicine (USA) published the Dietary Reference Intakes (DRI) in 2001 and recommended a daily iron allowance for adults of 8 mg for men and 15 mg for women [26]. Fe deficiency is common in MHD patients and is mainly due to blood losses during dialysis, frequent blood testing, blood remaining in dialysers and gastrointestinal bleeding. Iron absorption from food and oral supplements may be impaired due to increased gastric pH levels as a result of phosphate binder and antacid use. Oral Fe supplements should be taken between meals (at least 2 h after and 1 h before a main meal) to maximize Fe absorption and should not be taken with phosphate binders. Oral Fe supplements are known to cause adverse gastrointestinal effects and compliance with drug therapy may be compromised. Indeed, most MHD patients will receive Fe supplementation, intravenously or orally, as described in detail in the updated European Best Practice Guidelines for management of anaemia in patients with chronic renal failure [27]. Potassium In patients with a pre-dialysis serum potassium greater than 6 mmol/l, a daily intake of potassium of 50–70 mmol (1950–2730 mg) or 1 mmol/kg IBW is recommended. Rationale. Hyperkalaemia is a potential cause of sudden death in MHD patients. There are no warning signs and when pre-dialysis serum potassium levels approach 6 mmol/l, nutritional counselling to lower dietary potassium is indicated, in addition to Calcium ResoniumÕ or KayexalateÕ . However, other causes Zinc (Zn) A daily nutritional intake of 8–12 mg of elemental zinc (Zn) for women and 10–15 mg for men is recommended. Routine zinc supplementation is not recommended. A zinc supplementation of 50 mg Zn element per day for 3–6 months should be considered in haemodialysis patients with a chronic inadequate protein/energy intake and symptoms evoking zinc deficiency (impaired taste or smell, skin fragility, impotence, peripheral neuropathy). ii68 Rationale. Zinc deficiency is rare in western countries since zinc is absorbed in large quantities from protein rich foods such as red meat, fish and shellfish, milk and milk products, poultry and eggs. Zinc is albumin bound and plays an important role in protein, carbohydrate, energy, nucleic acid and lipid metabolism [32]. The Institute of Medicine (USA) recommends for healthy adults a daily zinc intake of 8 mg for women and 11 mg for men [26]. In the United Kingdom, recommendations are slightly different, 7 mg for women and 9 mg for men [33]. Matson et al. [34] and Kalantar-Zadeh et al. [35] recommend 12 mg of elemental zinc for women and 15 mg for men. Early signs of deficiency include defects in rapidly dividing tissues such as skin, intestinal mucosa and immune response, decreased taste acuity with a loss in taste buds, impotence, glucose intolerance and hyperlipidaemia. Taste and smell impairment associated with chronic uraemia contributes to anorexia leading to a reduced food intake that includes protein and may result in zinc deficiency [5]. Zinc deficiency in uraemic patients may contribute to peripheral neuropathy [36]. Oral iron supplements, calcium-based phosphate binders and corticosteroids may promote zinc deficiency. Although improvements in taste, smell, appetite, wound healing, immune response and sexual function have been reported when zinc supplements were prescribed, results were not supportive in several earlier studies. Most involved a small number of MHD patients, were of short duration whereas zinc concentration levels may vary due to different laboratory techniques. Zinc supplementation should be given for at least 3 months since shorter trials did not show expected improvements on taste [34] or immune system [36,37]. It was shown in a 3-month randomized crossover trial that zinc supplementation, 50 mg Zn element per day for 90 days significantly increased serum zinc level from low to normal and also increased nPCR and serum cholesterol [38,39]. In more observational reports, nerve conduction velocity improved with zinc supplementation [40] as well as sexual potency [41] but not all studies have confirmed this [42]. Zinc sulphate is a gastric irritant and should be taken with meals. Zn acetate, Zn aspartate and Zn chloride seem to be better tolerated even on an empty stomach [36,41]. Adding zinc to the haemodialysate may be considered if side effects associated with oral supplementation prohibit their use. During a randomized crossover study, serum zinc levels, taste acuity and nerve conduction velocity improved by adding zinc to dialysate during 12 weeks and achieving an increase in serum zinc from 10.1 1.3 to 23.1 0.7 mmol/l (N ¼ 13.8 1.9) [40]. Once this supplement was discontinued at the end of the 3 months supplementation, taste acuity reduced. Serum zinc levels lowered to baseline levels indicating that zinc supplementation should have been continued to maintain normal zinc levels. Presently, some but not all renal multivitamin formulas include zinc, 15 mg (Dialyvite3000Õ , USA), D. Fouque et al. 20 mg (RenaxÕ , USA) and 3000-ZincÕ , USA) per tablet. 50 mg (Dialyvite Selenium (Se) A daily intake of 55 mg of selenium is recommended. Routine selenium supplementation is not recommended. A selenium supplementation for 3–6 months should be considered in haemodialysis patients with symptoms evoking selenium deficiency (cardiomyopathy, skeletal myopathy, thyroid dysfunction, haemolysis, dermatosis). Rationale. Selenium is an essential trace element leading to an adequate glutathionine peroxidase (GPX) activity that protects cells from lipid peroxidation. Thyroid function regulation depends on selenium. The recommended intake for healthy males and females is 55 mg/day [26]. In case of acute oxidative stress, selenium needs may increase up to 100–150 mg/ day. Intestinal absorption is thought to be 50–65% [32]. The main sources of selenium are meat, fish, fat, vegetables and cereals. However, selenium content of food depends on the selenium content of local soil on which crops have grown or animals have grazed. A severe cardiomyopathy has been reported in the region of Keshan, China, where there is an extreme lack in selenium in earth and food, leading to very low selenium intake (<15 mg/day) and low serum selenium in humans. This cardiac disease is reversed by administering a selenium supplement. Other clinical symptoms of altered selenium metabolism include skeletal muscle dystrophia, haemolysis and dermatosis. Low serum selenium in CKD and MHD patients are not uncommon. There is no recommendation for selenium supplementation for CKD patients but if prescribed, selenium levels should be monitored closely, as selenium is excreted by the kidney and not removed by dialysis [5]. Selenium supplementation might be helpful in partially improving thyroid function in MHD patients. In a randomized control trial, Napolitano et al. [43] administered selenium to stable MHD patients. Ten patients received sodium selenite supplements orally, 500 mg three times weekly for the first 3 months followed by 200 mg three times weekly for the next 3 months, whereas five patients received a placebo. Selenium supplementation was well tolerated and a significant increase in serum selenium was observed as well as an improvement in thyroid function tests (i.e. a reduction in TSH) and an improvement in immune parameters in patients receiving selenium. No side effect was reported [43,44]. In a small pilot trial, Richard et al. [45] administered selenium intravenously as sodium selenite in six MHD patients, 50 mg at the end of the dialysis session three times weekly for the first five weeks then 100 mg for the next 15 weeks. This treatment was able to increase serum selenium levels and restore glutathione peroxidase activity to normal. EBPG guideline on nutrition ii69 Presently, some renal multivitamin formulas include selenium, 70 mg per tablet (Dialyvite3000Õ and RenaxÕ , USA). Table 2. Recommended dietary intake and supplements of vitamins and trace elements in adult haemodialysis patients (opinion) Vitamins Daily recommendation Thiamine hydrochloride (B1) Riboflavin (B2) Pyridoxine hydrochloride (B6) Ascorbic Acid (C) Folic Acid (B9) Cobalamine (B12) Niacin (B3, nicotinamide, nicotinic acid, PP) Biotin (B8) Pantothenic acid (B5) Retinol (A) 1.1–1.2 mg supplement 1.1–1.3 mg supplement 10 mg supplement 75–90 mg supplement 1 mg supplement 2.4 mg supplement 14–16 mg supplement Alpha-tocopherol (E) Vitamin K Minerals and Trace elements Phosphorus Calcium Sodium Potassium Iron Zinc Selenium 30 mg supplement 5 mg supplement 700–900 mg intake (no supplement) 400–800 IU supplementa 90–120 mg intake (no supplement) 800–1000 mg intake 2000 mg intake including calcium from phosphate binders 2000–2300 mg intake i.e. 5–6 g sodium chloride 50–70 mmol intake (1950–2730 mg) or 1 mmol/kgb 8 mg (men) and 15 mg (women) intakec 10–15 mg (men) and 8–12 mg (women) intake (no supplement)d 55 mg intake (no supplement)e a For secondary prevention of cardiovascular events and muscle cramps. b Only in hyperkalaemic patients, otherwise liberal intake. c In case of EPO treatment, supplemental iron is to be added, either orally or parenterally. d In case of malnutrition or symptoms of zinc deficiency, a trial of 50 mg Zn/day for 3–6 months could be considered (see text). e In case of symptoms of zinc deficiency, a trial of selenium for 3–6 months could be considered (see text). References 1. Andreucci VE, Fissell RB, Bragg-Gresham JL et al. Dialysi Outcomes and Practice Patterns Study (DOPPS) Data on Medication in Hemodialysis Patients. Am J Kidney Dis 2004; 44 [Suppl 2]: S61–S67 2. Fissell RB, Bragg-Gresham JL, Gillespie BW et al. International variations in vitamin prescription and association with mortality in the Dialysis Outcomes and Practice Patterns Study (DOPPS). Am J Kidney Dis 2004; 44: 293–299 3. Chazot C, Kopple JD. Vitamin metabolism and requirements in renal disease and renal failure. In Nutritional Management of Renal Disease, Kopple JD, Massry SG Eds, 2nd edn, Lipincott Williams and Wilkins, Philadelphia, USA: 2004; 315–356 4. Descombes E, Hanck AB, Fellay G. Water soluble vitamins in chronic hemodiualysis patients and needs for supplementation. Kidney Int 1993; 43: 1319–1328 5. Wiggins KL. Renal Care: Resources and practical applications. Renal Dietitians Dietetic Practice Group: Am Diet Ass 2003: 51–52 6. Wang S, Eide TC, Sogn EM et al. Plasma ascorbic acid in patients undergoing chronic haemodialysis. Eur J Clin Pharmacol 1999; 55: 527–532 7. Giancaspro V, Nuziello M, Pallotta G et al. Intravenous ascorbic acid in hemodialysis patients with functional iron deficiency: a clinical trial. J Nephrol 2000; 13: 444–449 8. Lin CL, Hsu PY, Yang HY et al. Low dose intravenous ascorbic for erythropoietin hypo-responsive anaemia in diabetic haemodialysis patients with iron overload. Ren Failure 2003; 25: 443–453 9. Keven K, Kutley S, Nergizoglu G et al. Randomized, crossover study of the effect of vitamin C on EPO response in hemodialysis patients. Am J Kidney Dis 2003; 41: 1233–1239 10. Khajehdehi P, Mojerlou M, Behzadi S et al. A randomized double blind placebo controlled trial of supplementary vitamin E, C and their combination for treatment of haemodialysis cramps. Nephrol Dial Transplant 2001; 16: 1448–1451 11. Deicher R, Ziai F, Bieglmayer C, Schillinger M, Horl WH. Low total vitamin C plasma level is a risk factor for cardiovascular morbidity and mortality in hemodialysis patients. J Am Soc Nephrol 2005; 16: 1811–1818 12. Lasseur C, Parrot F, Delmas Y et al. Impact of high-flux/ high-efficiency dialysis on folate and homocysteine metabolism. J Nephrol 2001; 14: 32–35 13. KDOQI Clinical Practice Guidelines in cardiovascular disease in dialysis patients. Am J Kidney Dis 2005; S3: 16–153 14. Rostand SG. Vitamin B12 levels and nerve conduction velocities in patients undergoing maintenance hemodialysis. Am J Clin Nutr 1976; 29: 691–697 15. Kaplan LN, Mamer OA, Hoffer LJ. Parenteral vitamin B12 reduces hyperhomocysteinemia in end-stage renal disease. Clin Invest Med 2001; 24: 5–11 16. Mangiarotti G, Canavese C, Salomone M et al. B12 in maintenance hemodialysis patients receiving massive supplementation of vitamin B12. Int J Artif Organs. 1986; 9: 417–420 17. Takahashi Y, Tanaka A, Nakamura T et al. Nicotinamide suppresses hyperphosphatemia in hemodialysis patients. Kidney Int 2004; 65: 1099–1104 18. Rottembourg JB, Launay-Vacher V, Massard J. Thrombocytopenia induced by nicotinamide in hemodialysis patients. Kidney Int 2005; 68: 2911–2912 19. Grundy SM, Vega GL, McGovern ME et al. Diabetes Multicenter Research Group. Efficacy, safety, and tolerability of once-daily niacin for the treatment of dyslipidemia associated with type 2 diabetes: results of the assessment of diabetes control and evaluation of the efficacy of niaspan trial. Arch Intern Med 2002; 162: 1568–1576 20. Canner PL, Furberg CD, Terrin ML, McGovern ME. Benefits of niacin by glycemic status in patients with healed myocardial infarction (from the Coronary Drug Project). Am J Cardiol 2005; 95: 254–257 21. K/DOQI clinical practice guidelines for bone metabolism and disease in chronic kidney disease. Am J Kidney Dis 2003; 42 [4 Suppl 3]: S1–S201 22. Chazot C, Laurent G, Charra B et al. Malnutrition in long-term haemodialysis survivors. Nephrol Dial Transplant 2001; 16: 61–69 23. Boaz M, Smetena S, Weinstein T et al. Secondary prevention with antioxidants of cardiovascular disease in end stage renal disease (SPACE): randomised placebo-controlled trials. Lancet 2000; 356: 1213–1218 24. Roca AO, Jarjoura D, Blend D et al. Dialysis Leg Cramps. Efficacy of quinine versus vitamin E. ASAIO J 1992; 38: M481–M485 25. Kohlmeier M, Saupe J, Shearer MJ, Schaefer K, Asmus G. Bone health of adult hemodialysis patients is related to vitamin K status. Kidney Int 1997; 51: 1218–1221 26. Trumbo P, Schlicker S, Yates AA et al. Dietary references intakes for energy, carbohydrate, fiber, fat, fatty acids, ii70 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. 45. D. Fouque et al. cholesterol, protein and amino acids. J Am Diet Assoc 2002; 102: 1621–1630 Locatelli F, Aljama P, Barany P. European Best Practice Guidelines Working Group. Revised European best practice guidelines for the management of anaemia in patients with chronic renal failure. Nephrol Dial Transplant 2004; 19 [Suppl 2]: 1–47 Ford JC, Pope JF, Hunt AE, Gerald B. The effect of diet education on the laboratory values and knowledge of hemodialysis patients with hyperphosphatemia. J Renal Nutr 2004; 14: 36–44 Galland R, Traeger J, Arkouche W, Cleaud C, Delawari E, Fouque D. Short daily hemodialysis rapidly improves nutritional status in hemodialysis patients. Kidney Int 2001; 60: 1555–1560 Krautzig S, Janssen U, Koch KM et al. Dietary salt restriction and reduction of dialysate sodium to control hypertension in maintenance haemodialysis patients. Nephrol Dial Transplant 1998; 13: 552–553 Beto JA, Bansal VK. Medical nutrition therapy in chronic kidney failure: integrating clinical practice guidelines. J Am Diet Assoc 2004: 104: 404–409 Thomas B. Manual of Dietetic Practice. Brit Diet Ass, 3rd edn, London, 2001: 182–183 Dietary Reference Values for Food Energy and Nutrients for the United Kingdom. Department of Health Report on Health and Social Subjects 1991; 41: 1–210 Matson A, Wright M, Oliver A et al. Zinc supplementation at conventional doses does not improve the disturbance of taste perception in HD patients. J Renal Nutr 2003; 13: 224–228 Kalantar-Zadeh K, Kopple JD. Trace elements and vitamins in maintenance dialysis patients. Adv Renal Repl Therapy 2003; 10: 170–182 Kouw PM, Jonings CH, de Vries PMJM et al. Effects of zinc supplementation on zinc status and immunity in haemodialysis patients. J Trace Elem Electrolyte Health Disease 1991; 5: 115–119 Turk S, Bozfakioglu S, Ecder ST et al. Effects of zinc supplementation on the immune system and on antibody response to multivalent influenza vaccine in hemodialysis patients. Int J Artif Organs 1998; 21: 274–278 Jern NA, VanBeber AD, Gorman MA et al. The effects of zinc supplementation on serum zinc concentration and protein catabolic rate in HD patients. J Renal Nutr 2000; 10: 148–153 Chevalier CA, Liepa GL, Murphy MD et al. The effects of zinc supplementation on serum zinc and cholesterol concentrations in HD patients. J Renal Nutr 2002; 12: 183–189 Sprenger KBG, Bundschau D, Lewis K et al. Improvement of uremic neuropathy and hypogeusia by dialysate zinc supplementation: a double blind study. Kidney Int 1983; 24 [Suppl 16]: S315–S318 Mahajan SK, Abbasi AA, Prasad AS et al. Effect of oral zinc therapy on gonadal function in HD patients. Ann Intern Med 1982; 97: 357–361 Rodger RS, Sheldon WL, Watson MJ et al. Zinc deficiency and hyperprolactinaemia are not reversible causes of sexual dysfunction in uraemia. Nephrol Dial Transplant 1989; 4: 888–892 Napolitano G, Bonomini, Bomba G et al. Thyroid function and plasma selenium in chronic uremic patients on hemodialysis treatment. Biol Trace Element Research 1996; 55: 221–230 Bonomini M, Forster S, De Risio F et al. Effects of selenium supplementation on immune parameters in chronic uraemic patients on haemodialysis. Nephrol Dial Transplant 1995; 10: 1654–1661 Richard MJ, Ducros V, Foret M et al. Reversal of selenium and zinc deficiencies in chronic hemodialysis patients by intravenous sodium selenite and zinc gluconate supplementation. Time-course of glutathione peroxidase repletion and lipid peroxidation decrease. Biol Trace Elem Res 1993; 39: 149–159 Guideline 5. Treatment of malnutrition 5.1. Dietary intervention Malnourished haemodialysis patients should receive nutritional counselling (Evidence level III). In hospitalized patients counselling should be started within 3 days of referral. A daily follow-up should be performed when patients are at high nutritional risk and weekly when at low risk (Opinion). Rationale and commentary Regular dietary counselling is an important part of the overall nutritional management of MHD patients. A qualified dietitian is trained to apply specific counselling techniques and these are aimed at behavioural change strategies to empower the patient to make successful changes in his/her diet. A ‘renal’ diet is complex as the intake of several nutrients requires modification during the different stages of chronic kidney disease and once again when the mode of dialysis changes or the patient is transplanted. Thus a MHD diet requires changes in the intake of protein and energy, sodium and fluid, potassium, calcium and phosphate and also in mineral and vitamin requirements. Early intervention during regular follow up may prevent nutritional inadequacies and could avert malnutrition. Several investigators studied the effect of regular nutritional counselling regarding nutritional intake of MHD patients. Removing some of the reasons for inadequacies considerably improved intake without the need for nutritional supplements. Sehgal et al. [1] investigated barriers to protein nutrition among MHD patients in a cohort of 298 patients from 22 dialysis units. Four parameters were assessed: nutritional status (serum albumin and PNA); potential medical barriers (poor appetite, difficulty in chewing, inadequate dialysis, bioincompatible dialysis membranes and comorbidity); behavioural barriers (knowledge of the protein content of food and dietary noncompliance) and socio-economic barriers (expense of foods with a high protein content, lack of support with shopping and cooking). It was concluded that three medical factors (poor appetite, inadequate dialysis and comorbidity), two behaviour factors (lack of knowledge and low interdialytic weight gain, IDWG) and one socio-economic factor (need for help with shopping and cooking) were independently associated with poor nutritional intake of MHD patients. Leon et al. [2] showed that frequent nutritional counselling by trained dietitians and tactfully removing existing barriers to food optimizes dietary protein and energy intake that leads to improved serum albumin, even in the presence of chronic inflammation. EBPG guideline on nutrition Akpele and coll. compared in a pilot study in 40 patients on haemodialysis for at least 6 months intensive dietary counselling vs the prescription of nutritional supplements [3]. The difference in rate of change in serum albumin (3.5 g/dl at onset) was measured [3]. The dietary goal was 1.2 g protein/kg IBW/day and 30–35 kcal/kg IBW/day. Twenty-six patients received nutritional supplements and 14 dietary counselling only. Patients receiving intensive counselling showed greater benefit than those receiving supplements. Indeed, albumin concentrations rose by 0.06 g/dl/month in the non-supplemented group vs 0.04 g/dl/month in the supplemented group [3]. A possible reason for this smaller change in the supplemented group was non-compliance and ageusia, anorexia, gastro intestinal side effects (diarrhoea), fear of weight gain, taste fatigue and preference for whole foods. Sharma et al. [4] surveyed 106 Indian MHD patients and found that patient’s diets changed over time on dialysis to a lower protein and energy intake than originally prescribed. Intakes were also compromised on dialysis days also adding to an increasingly poorer nutrient intake [4]. Dietary counselling and continuous monitoring therefore play an important role in malnutrition prevention. Steiber et al. [5] analysed nutritional intakes of CKD patients on admission in a general hospital. Less than 25% of patients with chronic renal failure (pre-dialysis, HD and CPD) achieved a 75% intake of the recommended diets. By knowing factors that can predict poor oral intake at referral, patients at risk could be identified earlier and their nutritional loss during hospitalization decreased. Similarly, it was shown that MHD patients only received 80% or less of recommended intake when hospitalized over 1 week [6]. Thus, it is now clear that malnutrition can start or deteriorate in hospital. Early aggressive intervention from the start of hospitalization should be initiated within 3 days of referral with a daily follow up for high and weekly follow up for low risk patients. 5.2. Oral supplements and enteral feeding Nutritional supplements should be prescribed if nutritional counselling does not achieve an increase in nutrient intake to a level that covers minimum recommendation (see Guideline 3) (Evidence level III). Products specifically formulated for dialysis patients should be prescribed in preference to standard supplements for non-renal patients (Evidence level III). Enteral tube [naso-gastric or percutaneous entero-gastrostomy (PEG)] feeding using disease specific formulas for dialysis patients should be prescribed if attempts to increase dietary intake with oral supplements fail and nutritional status does not improve (Evidence level IV). ii71 Rationale The development of several feeding methods such as PEG tube feeding and Intradialytic Parenteral Nutrition (IDPN) and the development of diseasespecific commercial products for oral (flavoured), enteral (no added flavour) and parenteral feeding have greatly modified the application of nutritional support for MHD patients during the past years. Oral or enteral nutritional support is less expensive than parenteral nutrition. Standard products for oral and enteral nutritional support contain a mixture of whole protein and/or amino acids, glucose polymers, fat components and added vitamins, minerals (including phosphate) and trace elements. It is preferable to use specific formulated products for dialysis patients containing more protein and energy (1.5–2.0 kcal/ml) and less potassium and phosphate if patients are hyperphosphataemic and/or hyperkalaemic [7]. Some of the oral supplements contain a non-sweet glucose polymer without addition of other nutrients or flavours. These are presented as a powder or as a concentrated liquid and are suitable to be added to food and drinks to improve energy intake without significantly altering the taste. Few clinical trials have been conducted about the provision of oral nutritional support to dialysis patients [7] and are limited in patient number and by short duration. Results have been affected due to early withdrawal from the trials when patients experienced side effects such as nausea or diarrhoea and when non-compliant with prescribed amount of nutritional supplement(s) [3]. Using essential amino acid tablets (15 tablets daily for 3 months), Eustace et al. [8] reported non-compliance as high as 50% at 3 months of oral supplement, underlining the necessity for more research on supplements specifically designed for MHD patients. A recent systematic review and meta-analysis of 18 studies (five randomized and 13 non-randomized controlled trials) on the use of multi-nutrient oral supplements and tube feeding in MHD patients by Stratton et al. [7] showed that oral and enteral nutritional support improves protein and energy intake, increases serum albumin concentrations by 0.23 g/dl (P < 0.05) and improves total energy intake. There is still insufficient data on the clinical effect on MHD patients and specifically malnourished patients to determine from which regimen they would benefit most. Clinical benefits of oral nutritional supplements. A number of studies have investigated the effect of oral supplements on the nutritional parameters of MHD patients [3,8–15]. Ivarsen et al. [15] and Eustace et al. [8] studied the effect of amino acid supplements on albumin changes in MHD patients. Providing 19 stable, well-dialysed and wellnourished MHD patients a daily protein supplement containing 7.8 g amino acids (4.8 g were essential) for 3 months in addition to their usual MHD diet, ii72 no improvement in nutritional parameters was shown, although intracellular amino acid concentration improved significantly [15]. In a randomized double blind trial, Eustace et al. [8] studied the benefits of a supplement containing a daily total of 10.8 g essential amino acids (EAA) in 29 MHD and 19 peritoneal dialysis (PD) patients with a mean three months prestudy serum albumin of 3.8 g/dl or less. Patients were taking five tablets (e.g. 3.6 g EAA), three times daily with food for 3 months. Serum albumin concentrations increased by 0.22 0.09 g/dl (P ¼ 0.02) in MHD patients but did not change significantly in the PD group. Patients with lower serum albumin concentrations improved more. No improvement was seen in serum amino acid concentrations. Non-compliance with prescribed supplements and gastrointestinal side effects can affect the outcome of oral nutritional support as shown by Akpele et al. [3]. In this pilot study of 41 MHD patients, 26 patients were given a commercial renal-specific nutritional supplement in addition to their regular dietary intake for an average of 6–7 months. The expected increase in protein and energy intake however was not achieved and several factors contributed to the lack of compliance such as taste impairment, anorexia and gastrointestinal side effects such as nausea, diarrhoea, fear of weight gain, taste fatigue and preference to whole food. These investigators concluded that patients may benefit from a choice in a selection of different nutritional products with different consistency and flavour to boost their protein and energy intake [3]. Changing the timing of taking the prescribed nutritional supplement can improve compliance. Cockram et al. [11] compared the gastrointestinal symptoms, bowel habits, routine blood chemistries, urea kinetics and nPNA in 79 patients over a three week period using three products: one standard and two special formulas (one with and one without a fructooligosaccharide – FOS) developed for renal patients. The investigators found that the two specialized formulas resulted in lower serum phosphate levels and a decrease in the calcium–phosphate product. Patients taking the product containing FOS had less constipation [11]. Caglar et al. [10] studied 85 malnourished MHD patients who were given a commercial nutritional supplement containing 475 kcal and 16.6 g protein for oral use on haemodialysis days to ensure compliance, for a period of 9 months. Serum albumin concentration rose significantly from 3.33 0.32 to 3.65 0.26 mg/dl (P ¼ 0.002) during 6 months of supplementation. The changes in BMI (from 25.8 6.1 to 27.1 5.4) and estimated dry body weight (from 73.1 15.3 to 76.1 16.2 kg) were not statistically significant. The mean SGA score improved by 14% from baseline by the end of the study (P ¼ 0.02) [10]. The effect of two different oral nutritional supplements both providing daily an additional 16 g protein and 500 kcal on improving body weight and serum albumin levels was studied by Sharma et al. [14]. Forty seven malnourished MHD patients in India with a BMI of less than 20 and a serum albumin D. Fouque et al. concentration of less than 40 g/l were selected and 40 completed this trial after 1 month of thrice weekly dialysis. Twenty-six patients received oral supplements containing 16 g protein and 500 kcal either as a commercial supplement (CS) or a low cost home made blend (HP Blend) after the dialysis session was completed, for 1 month [14]. Patients were also prescribed a diet with 1.2 g protein and 35–45 kcal/kg BW/day followed by regular counselling. The control group received counselling only. A significant improvement in serum albumin concentration (P ¼ 0.03) was seen in the supplemented HP Blend and the CS group even after 1 month compared with the control group. The HP Blend and control group gained the same amount of dry weight (2 kg). Patients however were young, without comorbidities and with baseline BMIs of 17.9 or less [14]. Kuhlman et al. [12] showed in a small and short study that specific protein and energy supplements for CKD patients taken as a sip feed in addition to a prescribed MHD diet with a total intake of 1.5 g/kg protein and 45 kcal/kg/day, resulted in a sustained weight gain of 1.2 0.4 kg during a 3-month period in underweight patients with a mean BMI of 17.6. Adding a glucose polymer daily to the regular MHD diet was investigated by Allman et al. [9] and Milano et al. [13]. Both investigators reported the absence of gastrointestinal side effects and the products were well tolerated. In the first trial, Allman et al. randomly prescribed 100–150 g glucose polymer equivalent to 400–600 kcal/day to 9 patients in addition to their usual diet (protein intake: 1.16 0.28 g/kg and energy: 30 10 kcal/kg) for 6 months vs no supplement in the control group. The supplemented patients gained 3.1 2.3 kg (P < 0.005), 1.8 kg as body fat and 1.3 kg as lean body mass indicated by changes in anthropometry. BMI rose from 21.3 to 22.9 and this weight gain was maintained 6 months after stopping the supplement [9]. In the second trial, Milano et al. [13] studied the effect of a 100 g glucose polymer supplement (380 kcal) daily in 21 MHD patients in addition to their usual diet. This amount increased their energy intake to at least 34 kcal/kg/day. After 6 months of supplement, their mean weight increased by 2.4 kg (range 0.6–6.3 kg) but assessed by anthropometry, this weight gain appeared to be predominantly fat. This gain was maintained for 6 months after cessation of the supplement [13]. Clinical benefits of enteral tube feeding. If the provision of oral supplements in addition to intensive counselling is unsuccessful, tube feeding should be proposed. Renal specific formulas may be used to maximize protein and energy supply, while controlling excessive amounts of fluid, phosphate, potassium and unnecessary vitamins usually contained in standard feed products. Sayce et al. [16] analysed serum albumin and anthropometry in eight malnourished MHD outpatients who received PEG feeding for 3–15 months. Energy dense renal formula tube feeds were prescribed based on EBPG guideline on nutrition individual requirements. The feed was administered as a bolus or by means of continuous pump feeding overnight. Two anuric patients required changes in their feeding regimens due to fluid overload. The amount of tube feed was reduced even further during the 3-day weekend interval when fluid overload was likely to occur. After 3 months, mean dry weight increased from a mean of 43.0 to 48.3 kg (P ¼ 0.01). Mid upper arm circumference increased from 20.2 to 24.8 cm (P ¼ 0.02) and triceps skinfold thickness from 17.7 to 19.8 mm (P ¼ 0.03). Serum albumin rose from 29.5 to 36.5 g/l (P ¼ 0.01). It was concluded that home enteral feeding using PEG access is effective and safe in improving and maintaining nutritional status in malnourished MHD patients. Frequent monitoring with provision of additional support throughout the feeding period is paramount. Holley et al. [17] performed a retrospective analysis of a small cohort of 10 MHD patients (mean age 66 years) who received nasogastric or PEG enteral feeding for 1–36 months. Seven out of ten patients had suffered a cerebrovascular accident; two patients were in intensive care units. In five patients, tube feeding was supplementary to a normal nutrition and provided 50% of protein and energy of their requirements to achieve a protein intake of 1.0–1.3 g protein/kg BW and 30– 35 kcal/kg per day. Serum albumin rose from 2.8 to 3.3 g/dl (P ¼ 0.04) by the end of the feeding period, but no significant weight gain was reported. Eight out of ten patients had at least one episode of hypophosphataemia (<2.0 mg/dl in four of the eight patients) which was resolved by replacing the regimen from the renal to a standard formula and by using phosphate supplements [17]. Although retrospective and of limited size, these results should encourage well designed prospective studies in MHD patients. Recommendations for further research What is the optimal composition of oral supplements (taste, concentration, electrolyte composition, vitamin and trace content)? What is the optimal schedule and delivery rate of oral and enteral supplements? What are the indications, optimal duration and complications of PEG in MHD patients? Is it possible to improve patient’s appetite with specific oral supplements? 5.3. Intradialytic parenteral nutrition When intensive dietary support, oral supplements and enteral nutrition have failed, a course of parenteral nutrition is recommended (Evidence level IV). Intradialytic parenteral nutrition (IDPN) is recommended in malnourished patients only if spontaneous nutrient intake is >20 kcal/kg IBW and 0.8 g protein/kg IBW/day. Otherwise, total parenteral nutrition infused over the entire day is indicated (Opinion). ii73 Rationale and commentary There are many speculative reasons that intravenous nutrition may improve patient’s nutritional status. In the particular case of maintenance dialysis, the fact that patients will be referred three times weekly with vascular access allowing additional nutrient infusion theoretically simplifies applicability, delivery and compliance to parenteral nutrition. On the other hand, time to exposure for nutritional support is rather short (standard 10–15 h weekly) as compared with total parenteral nutritional support used in intensive care units or at home for patients with intestinal failure. Hence, non-renal nutritionists often question the efficacy of IDPN. In addition, IDPN is more expensive than any oral or enteral nutrition. The key questions are: do patients have a spontaneous intake great enough to supplement through a limited delivery related to the intermittent pattern of intradialytic parenteral nutrition (e.g. greater than 20 kcal and 0.8 g protein/kg IBW/day), and how will IDPN interfere with spontaneous patient’s intake throughout metabolic and appetite alterations? Several retrospective analyses, prospective trials and reviews have addressed the various aspects of IDPN [18–28]. From a metabolic point of view, one haemodialysis session dramatically decreases the plasma amino acids and as a consequence, blunts intracellular muscle protein synthesis. In addition, in response to the rapid plasma amino acid decrease at the start of the haemodialysis session, muscle proteolysis occurs in order to maintain an adequate plasma and cellular amino acid concentration [29]. These events result in a clear catabolic state at the end of the dialysis session [30–32]. In the long term these catabolic modifications may lead to muscle wasting. Feeding patients by parenteral route during the dialysis session has been shown to revert this acute catabolic state by maintaining a normal plasma amino acid concentration [30]. Recently, Pupim et al. [33] reported that a brief 15 min cycling exercise at the beginning of the dialysis session dramatically improved the anabolic effect of the IDPN supplement. However, it is less clear if these beneficial effects are associated with long-term improvement in patient’s nutritional status and morbi-mortality. Indeed, protein metabolism may be modified during the nondialysis days, and to some extent, compensate for the dialysis-induced acute catabolic state. In more prolonged surveys, improvement in serum albumin [22,24] and patient’s spontaneous intake has been reported [23,24,27] but few studies were adequately designed and to date, evidence is low. Thus, long-term randomized studies should address the potential effect of IDPN on nutritional status and morbimortality of MHD patients. The ongoing Fines study, the largest prospective randomized controlled trial addressing the efficacy on oral and intradialytic nutritional support in malnourished MHD patients ii74 will provide evidence for indication and limits of nutritional support in these patients [18]. 5.4. Anabolic agents In case of severe malnutrition resistant to optimal nutritional intervention, a course of androgens should be considered in MHD patients for three to 6 months (Evidence level II). Androgens should be administered weekly or bimonthly (Evidence level II). Patients should be monitored at regular intervals for side effects (hirsutism, voice change, priapism, alteration in plasma lipids, liver tests and prostatic markers) (Evidence level II). Patients with a known prostate cancer should not receive androgens (Evidence level II). Rationale In healthy adults the body protein mass is maintained at equilibrium by a subtle tuning between anabolism and catabolism that is regulated through independent signals. Among anabolic factors (which promote growth in childhood, and maintenance of protein mass in adults), growth hormone (GH) and insulinlike growth factor (IGF)-1 have been studied in-depth in many disorders, including CKD. Many acute administration studies and most mid-term (3–6 months) treatments with recombinant GH have reported beneficial metabolic, nutritional and body composition changes [34–45]. Long-term administration of recombinant GH has not been studied in CKD adults, and potential side-effects may occur, such as hyperglycaemia, hypertriglyceridaemia, and sodium retention. Recombinant GH treatment is only approved in short stature CKD children and helps to catch-up growth. However, GH is not currently approved in adult MHD patients. Recombinant IGF-1, which also exerts acute anabolic responses in malnourished dialysis patients [46], is only approved for the specific Laron nanism, a GH receptor deficient disease. Thus, except for pituitary insufficiency, a treatment by recombinant GH to improve nutritional status cannot yet be proposed to adult dialysis patients. Androgens are well-known anabolic compounds. It should be emphasized that with age and CKD, a relative androgen insufficiency may be present, underlining a potential cause for muscle loss in males. Recently, it has been reported that non-renal male patients with coronary disease and low plasma testosterone levels did benefit from low-dose transdermal testosterone treatment, which improved their coronary symptoms [47]. In elderly patients without known kidney disease, a 6-month administration of low doses of testosterone to reach supranormal plasma levels significantly increased muscle mass and strength [48]. In kidney patients, androgens have D. Fouque et al. been largely utilized before the era of erythropoietin to correct anaemia and reduce the number of blood transfusions. However, since the release of recombinant EPO in the 1990s, androgens were left apart and it is only since recently that their anabolic properties were rediscovered [48–54]. In a randomized controlled trial, Johansen et al. [52] assessed body composition and strength while administering nandrolone decanoate, 100 mg intramuscularly weekly for 6 months in 29 MHD patients. Body composition was monitored by dual energy X-ray absorptiometry and functional status by treadmill, walking, and stair-climbing times. Nandrolone decanoate induced a 4.5 kg lean body mass gain (P < 0.01) and a fat loss of 2.4 kg (P < 0.01) from baseline. There was a reduction in reported symptoms of fatigue and a decrease in walking and stair climbing times in the nandrolone group. No changes in serum cholesterol or triglycerides were reported in either group. Dose adjustment was done in two women who complained of acne and amenorrhea [52]. In elderly MHD patients receiving EPO, Gascon et al. [54] administered nandrolone decanoate, 200 mg intramuscularly weekly for 6 months in 14 patients who were withdrawn from EPO, whereas 19 patients continued to receive regular EPO treatment. Patients receiving nandrolone gained weight (from 68.2 9.1 to 70.3 8.6 kg; P < 0.05) and muscle mass (P < 0.05) [54]. Haemoglobin improved from 9.6 1.0 to 11.0 1.4 g/dl (P < 0.01) in the nandrolone group, whereas no change was observed in the EPO group who received 6000 3900 IU EPO weekly. Serum albumin decreased from 4.0 0.3 to 3.6 0.5 g/dl (P < 0.05) in the EPO group, whereas it did not change in the nandrolone group. During nandrolone treatment, although serum triglycerides increased from 144 78 to 180 76 mg/dl (P < 0.05) and HDL-cholesterol decreased from 39 13 to 32 11 (P < 0.05), Lp(a), a strong predictor of cardiovascular risk, decreased from 26 23 to 9 8 mg/dl (P < 0.005) [54]. Thus, it is not clear in MHD patients if androgens impair lipid metabolism to the point of increasing long-term cardiovascular risk, which should be weighted against the risk of rapidly worsening malnutrition. In another retrospective study by Pai and colleagues [50] in which five women received 25 mg nandrolone decanoate intramuscularly weekly for 3 months, no side effect was reported. Serum albumin significantly rose from 29 to 33 g/l (P < 0.05) in the study of Pai et al. [50] and from 32 to 38 g/l (P < 0.001) in the prospective randomized trial reported by Navarro and colleagues [51]. The dose of nandrolone administered in these studies ranged from 100 mg twice monthly for 3 months to 200 mg weekly for 6 months. Potential side effects include voice change and hirsutism in women, prostatic markers in men and abnormal liver tests and change in lipid metabolism in all and regular follow-up should be done accordingly [55,56]. Thus, in moderate EBPG guideline on nutrition amounts for 3–6 months, nandrolone improved body composition in MHD patients. Recommendation for further research Larger randomized controlled trials of androgens administration should be performed in various degrees of malnutrition in MHD patients, in order to characterize a likely dose-response, the optimal duration and frequency of administration and to monitor potential side-effects. Test the efficacy of a combined intervention of androgens and exercise training on body composition and nutritional status of malnourished MHD patients Measure the effects of a combined intervention by androgens and supplemental nutrition (either oral, enteral or parenteral) on body composition and nutritional status of malnourished MHD patients 5.5. Other interventions: daily dialysis A 6–12 month trial of daily dialysis (either short daily or long nocturnal) should be considered as a rescue therapy in unstable patients undergoing difficult haemodialysis sessions with symptoms of malnutrition or malnourished patients with poor appetite after a negative nutritional workout (Opinion). ii75 Table 3. Serum albumin level before and at the end of daily dialysis programs in pilot maintenance dialysis adult patients trials (SDHD: short daily haemodialysis; NHHD: nocturnal home haemodialysis) Reference Treatment Nb S. albumin (g/l) Patients At start At the end Woods et al. [67] Buoncristiani et al. [68] Pinciaroli [69] Kooistra and Vos [70] Galland et al. [61] Lugon et al. [71] Pierratos et al. [57] McPhatter et al. [72] O’Sullivan et al. [66] Cacho et al. [73] SDHD SDHD SDHD SDHD SDHD SDHD NHHD NHHD NHHD NHHD 72 50 22 13 10 5 12 9 5 5 39 39 35 42.2 39 40 41.2 34 36.3 43.0 43.5 44 42.6 43.2 42 43 41.4 41 36.8 43.8 Whether those nutritional changes are beneficial over the long term is not known and should be the subject to future well-designed randomized trials. Indeed, one recent systematic review on the benefits of daily nocturnal haemodialysis, although clearly showing improved blood pressure and left ventricular hypertrophy, did report mixed effects on quality of life, anaemia control and phosphocalcic metabolism [65]. Authors asked for harder endpoint events such as mortality or cardiovascular morbidity before this strategy could be more largely diffused. Rationale References Since almost 10 years, daily haemodialysis pilot trials in Europe and North America have reported nutritional and metabolic effects in MHD patients [57–73]. Different schedules as well as durations have been proposed, such as six 2-h morning sessions to seven 8-h slow nocturnal sessions weekly. Interestingly, although nutrition was not the primary cause for enrolling patients in these programs, most reported unexpected improvements in appetite, clinical and biological nutritional parameters. Table 3 reports the change in serum albumin before and after switching from standard haemodialysis thrice weekly to daily dialysis. The improvement appeared greater in studies in which patients disclosed lower albumin levels, except for one [66]. In studies where nutritional status and dietary intake were followed, increase in food intake was best explained by an increase in well-being, a reduced interdialytic weight gain, a decrease in phosphate binders and KayexalateÕ , which are known to decrease appetite [61]. Another possible explanation, yet unproved, could be a better clearance of catabolic molecules and/or anorectic compounds. Thus, daily dialysis allows freeing patients from dietary restrictions and, at least for some months, may be viewed as a rescue therapy in malnutrition states. 1. Sehgal AR, Leon J, Soinski JA. Barriers to adequate protein nutrition among haemodialysis patients. J Renal Nutr 1998; 8: 179–187 2. Leon JB, Majerle AD, Soinski JA, et al. Can a nutrition intervention improve albumin levels among hemodialysis patients? A pilot study. J Renal Nutr 2001; 11: 9–15 3. Akpele L, Bailey JL. Nutrition counseling impacts serum albumin levels. J Renal Nutr 2004; 14: 143–148 4. Sharma M, Rao M, Jacob S et al. A dietary survey in Indian hemodialysis patients. J Renal Nutr 1999; 9: 21–25 5. Steiber AL. Clinical indicators associated with poor oral intake of patients with chronic renal failure. J Renal Nutr 1999; 9: 84–88 6. Laville M, Fouque D. Nutritional aspects in hemodialysis. Kidney Int 2000; Suppl 76: S133–S139 7. Stratton RJ, Bircher G, Fouque D et al. Multinutrient oral supplements and tube feeding in maintenance dialysis: a systematic review and meta-analysis. Am J Kidney Dis 2005; 46: 387–405 8. Eustace JA, Coresh J, Kutchey C et al. Randomized doubleblind trial of oral essential amino acids for dialysis-associated hypoalbuminemia. Kidney Int 2000; 57: 2527–2538 9. Allman MA, Allen BJ, Stewart PM et al. Body protein of patients undergoing haemodialysis. Eur J Clin Nutr 1990; 44: 123–131 10. Caglar K, Fedje L, Dimmitt R, et al. Therapeutic effects of oral nutritional supplementation during hemodialysis. Kidney Int 2002; 62: 1054–1059 ii76 11. Cockram DB, Hensley MK, Rodriguez M, et al. Safety and tolerance of medical nutritional products as sole sources of nutrition in people on hemodialysis. J Renal Nutr 1998; 8: 25–33 12. Kuhlmann MK, Schmidt F, Kohler H. High protein/energy vs. standard protein/energy nutritional regimen in the treatment of malnourished hemodialysis patients. Miner Electrolyte Metab 1999; 25: 306–310 13. Milano MC, Cusumano AM, Navarro ET et al. Energy supplementation in chronic hemodialysis patients with moderate and severe malnutrition. J Renal Nutr 1998; 8: 212–217 14. Sharma M, Rao M, Jacob S et al. A controlled trial of intermittent enteral nutrient supplementation in maintenance hemodialysis patients. J Renal Nutr 2002; 12: 229–237 15. Ivarsen P, Frystyk J, Pedersen EB. The pattern of intracellular free amino acids in granulocytes from hemodialysis patients change to an oral protein supplement (granulocyte amino acids after protein in HD patients). Clin Nephrol 1999; 52: 110–118 16. Sayce H, Rowe P, McGonogle R: Percutaneous endoscopic gastrostomy feeding in hemaodialysis out-patients. J Human Nutr Diet 2000; 13: 333–341 17. Holley JL, Kirk J. Enteral tube feeding in a cohort of chronic hemodialysis patients. J Renal Nutr 2002; 12: 177–182 18. Cano N. Intradialytic parenteral nutrition: where do we go from here? J Renal Nutr 2004; 14: 3–5 19. Foulks CJ. An evidence-based evaluation of intradialytic parenteral nutrition. Am J Kidney Dis 1999; 33: 186–192 20. Chertow GM, Ling J, Lew NL et al. The association of intradialytic parenteral nutrition administration with survival in hemodialysis patients. Am J Kidney Dis 1994; 24: 912–920 21. Kopple JD. Therapeutic approaches to malnutrition in chronic dialysis patients: the different modalities of nutritional support. Am J Kidney Dis 1999; 33: 180–185 22. Capelli JP, Kushner H, Camiscioli TC et al. Effect of intradialytic parenteral nutrition on mortality rates in endstage renal disease care [see comments]. Am J Kidney Dis 1994; 23: 808–816 23. Piraino AJ, Firpo JJ, Powers DV. Prolonged hyperalimentation in catabolic chronic dialysis therapy patients. J Parenter Enteral Nutr 1981; 5: 463–477 24. Hiroshige K, Iwamoto M, Kabashima N et al. Prolonged use of intradialysis parenteral nutrition in elderly malnourished chronic haemodialysis patients. Nephrol Dial Transplant 1998; 13: 2081–2087 25. Guarnieri G, Faccini L, Lipartiti T et al. Simple methods for nutritional assessment in hemodialyzed patients. Am J Clin Nutr 1980; 33: 1598–1607 26. Wolfson M, Jones MR, Kopple JD. Amino acid losses during hemodialysis with infusion of amino acids and glucose. Kidney Int 1982; 21: 500–506 27. Cano N, Labastie-Coeyrehourq J, Lacombe P et al. Perdialytic parenteral nutrition with lipids and amino acids in malnourished hemodialysis patients. Am J Clin Nutr 1990; 52: 726–730 28. Navarro JF, Mora C, Leon C et al. Amino acid losses during hemodialysis with polyacrylonitrile membranes: effect of intradialytic amino acid supplementation on plasma amino acid concentrations and nutritional variables in nondiabetic patients. Am J Clin Nutr 2000; 71: 765–773 29. Raj DS, Zager P, Shah VO et al. Protein turnover and amino acid transport kinetics in end-stage renal disease. Am J Physiol Endocrinol Metab 2004; 286: E136–143 30. Pupim LB, Flakoll PJ, Brouillette JR et al. Intradialytic parenteral nutrition improves protein and energy homeostasis in chronic hemodialysis patients. J Clin Invest 2002; 110: 483–492 D. Fouque et al. 31. Raj DS, Welbourne T, Dominic EA et al. Glutamine kinetics and protein turnover in end-stage renal disease. Am J Physiol Endocrinol Metab 2005; 288: E37–E46 32. Bohe J, Rennie M. Muscle protein metabolism during haemodialysis. J Renal Nutr 2006; 16: 3–16 33. Pupim LB, Flakoll PJ, Levenhagen DK et al. Exercise augments the acute anabolic effects of intradialytic parenteral nutrition in chronic hemodialysis patients. Am J Physiol Endocrinol Metab 2004; 286: E589–E597 34. Kopple JD, Brunori G, Leiserowitz M et al. Growth hormone induces anabolism in malnourished maintenance haemodialysis patients. Nephrol Dial Transplant 2005; 20: 952–958 35. Kotzmann H, Yilmaz N, Lercher P et al. Differential effects of growth hormone therapy in malnourished hemodialysis patients. Kidney Int 2001; 60: 1578–1585 36. Johannsson G, Bengtsson BA, Ahlmen J. Double-blind, placebo-controlled study of growth hormone treatment in elderly patients undergoing chronic hemodialysis: anabolic effect and functional improvement. Am J Kidney Dis 1999; 33: 709–717 37. Iglesias P, Diez JJ, Fernandez-Reyes MJ et al. Recombinant human growth hormone therapy in malnourished dialysis patients: a randomized controlled study. Am J Kidney Dis 1998; 32: 454–463 38. Garibotto G, Barreca A, Russo R et al. Effects of recombinant human growth hormone on muscle protein turnover in malnourished hemodialysis patients. J Clin Invest 1997; 99:97–105 39. Blake PG: Growth hormone and malnutrition in dialysis patients. Perit Dial Int 1995; 15: 210–216 40. Ikizler TA, Wingard RL, Breyer JA et al. Short-term effects of recombinant human growth hormone in CAPD patients. Kidney Int 1994; 46: 1178–1183 41. Schulman G, Wingard RL, Hutchison RL et al. The effects of recombinant human growth hormone and intradialytic parenteral nutrition in malnourished hemodialysis patients. Am J Kidney Dis 1993; 21: 527–534 42. Ziegler TR, Lazarus JM, Young LS et al. Effects of recombinant human growth hormone in adults receiving maintenance hemodialysis. J Am Soc Nephrol 1991; 2: 1130–1135 43. Hansen TB, Gram J, Jensen PB et al. Influence of growth hormone on whole body and regional soft tissue composition in adult patients on hemodialysis. A double-blind, randomized, placebo-controlled study. Clin Nephrol 2000; 53: 99–107 44. Ericsson F, Filho JC, Lindgren BF. Growth hormone treatment in hemodialysis patients – a randomized, double-blind, placebo-controlled study. Scand J Urol Nephrol 2004; 38: 340–347 45. Kotzmann H, Riedl M, Pietschmann P et al. Effects of 12 months of recombinant growth hormone therapy on parameters of bone metabolism and bone mineral density in patients on chronic hemodialysis. J Nephrol 2004; 17: 87–94 46. Fouque D, Peng SC, Shamir E et al. Recombinant human insulin-like growth factor-1 induces an anabolic response in malnourished CAPD patients. Kidney Int 2000; 57: 646–654 47. English KM, Steeds RP, Jones TH et al. Low-dose transdermal testosterone therapy improves angina threshold in men with chronic stable angina: a randomized, double-blind, placebo-controlled study. Circulation 2000; 102: 1906–1911 48. Ferrando AA, Sheffield-Moore M, Yeckel CW et al. Testosterone administration to older men improves muscle function: molecular and physiological mechanisms. Am J Physiol Endocrinol Metab 2002; 282: E601–E607 49. Bhasin S, Woodhouse L, Casaburi R et al. Testosterone dose-response relationships in healthy young men. Am J Physiol Endocrinol Metab 2001; 281: E1172–E1181 EBPG guideline on nutrition 50. Barton Pai A, Chretien C, Lau AH. The effects of nandrolone decanoate on nutritional parameters in hemodialysis patients. Clin Nephrol 2002; 58: 38–46 51. Navarro JF, Mora C, Macia M et al. Randomized prospective comparison between erythropoietin and androgens in CAPD patients. Kidney Int 2002; 61: 1537–1544 52. Johansen KL, Mulligan K, Schambelan M. Anabolic effects of nandrolone decanoate in patients receiving dialysis: a randomized controlled trial. JAMA 1999; 281: 1275–1281 53. Johnson CA. Use of androgens in patients with renal failure. Semin Dial 2000; 13: 36–39 54. Gascon A, Belvis JJ, Berisa F et al. Nandrolone decanoate is a good alternative for the treatment of anemia in elderly male patients on hemodialysis. Geriatr Nephrol Urol 1999; 9: 67–72 55. Teruel JL, Aguilera A, Avila C et al. Effects of androgen therapy on prostatic markers in hemodialyzed patients. Scand J UrolNephrol 1996; 30: 129–131 56. Teruel JL, Lasuncion MA, Rivera M et al. Nandrolone decanoate reduces serum lipoprotein(a) concentrations in hemodialysis patients. Am J Kidney Dis 1997; 29: 569–575 57. Pierratos A, Ouwendyk M, Francoeur R et al. Nocturnal hemodialysis: three-year experience. J Am Soc Nephrol 1998; 9: 859–868 58. Vos PF, Zilch O, Kooistra MP. Clinical outcome of daily dialysis. Am J Kidney Dis 2001; 37: S99–S102 59. Kooistra MP, Vos J, Koomans HA et al. Daily home haemodialysis in The Netherlands: effects on metabolic control, haemodynamics, and quality of life. Nephrol Dial Transplant 1998; 13: 2853–2860 60. Lacson E, Jr, Diaz-Buxo JA. Daily and nocturnal hemodialysis: how do they stack up? Am J Kidney Dis 2001; 38: 225–239 61. Galland R, Traeger J, Arkouche W et al. Short daily hemodialysis rapidly improves nutritional status in hemodialysis patients. Kidney Int 2001; 60: 1555–1560 62. Goffin E, Pirard Y, Francart J et al. Daily hemodialysis and nutritional status. Kidney Int 2002; 61: 1909–1910 63. Schulman G. Nutrition in daily hemodialysis. Am J Kidney Dis 2003; 41: S112–115 64. Maduell F, Navarro V, Torregrosa E et al. Change from three times a week on-line hemodiafiltration to short daily on-line hemodiafiltration. Kidney Int 2003; 64: 305–313 65. Walsh M, Culleton B, Tonelli M et al. A systematic review of the effect of nocturnal hemodialysis on blood pressure, left ventricular hypertrophy, anemia, mineral metabolism, and health-related quality of life. Kidney Int 2005; 67: 1500–1508 66. O’Sullivan DA, McCarthy JT, Kumar R et al. Improved biochemical variables, nutrient intake, and hormonal factors in slow nocturnal hemodialysis: a pilot study. Mayo Clin Proc 1998; 73: 1035–1045 67. Woods JD, Port FK, Orzol S et al. Clinical and biochemical correlates of starting ‘‘daily’’ hemodialysis. Kidney Int 1999; 55: 2467–2476 68. Buoncristiani U, Fagugli R, Pinciaroli M et al. Control of aneamia by daily dialysis. J Am Soc Nephrol 1997; 8: 216A 69. Pinciaroli M. Results of daily hemodialysis in Cantanzaro: 12-year experience with 22 patients treated for more than one year. Home Hemodial Int 1998; 2: 12–17 70. Kooistra MP, Vos J. Daily home hemodialysis: towards a more physiological treatment of patients with ESRD. Semin Dial 1999; 12: 424–430 71. Lugon J, Reimbold S, Pereira C et al. Improvement in dialysis adequacy and quality of life by in-center daily hemodialysis. J Am Soc Nephrol 1997; 8: 165A 72. McPhatter LL, Lockridge RS, Jr, Albert J et al. Nightly home hemodialysis: improvement in nutrition and quality of life. Adv Ren Replace Ther 1999; 6: 358–365 73. Cacho C, Ferrara K, Guthrie B et al. Slow Intensive Home Hemodialysis (SIHD): the University Hospitals of Cleveland experience. Nephrol News Issues 2000; 14: 36–41 ii77 Guideline 6. Metabolic acidosis Mid-week predialysis serum bicarbonate levels should be maintained at 20–22 mmol/l (Evidence level III). In patients with venous predialysis bicarbonate persistently <20 mmol/l, oral supplementation with sodium bicarbonate and/or increasing dialysate concentration to 40 mmol/l should be used to correct metabolic acidosis (Evidence level III). Rationale In two epidemiological studies a U-shape relationship between serum bicarbonate levels and mortality has been demonstrated in haemodialysis patients [1,2]. Lowrie et al. [1] reported from a retrospective analysis in over 12 000 haemodialysis patients an increased risk of dying if serum bicarbonate levels were <17.5 or >25 mmol/l. Recently, this was confirmed in the DOPPS study, in which a rise in mortality was present if predialysis bicarbonate level was <17 or >27 mmol/l [2]. In the latter study, it was demonstrated that serum bicarbonate levels between 20.1 and 21.0 mmol/l faced the lowest risk for mortality and levels of 21.1–22.0 the lowest risk of hospitalization. From these epidemiological data it can be concluded that predialysis serum bicarbonate levels of 20–22 mmol/l seem to be optimal. Although in a number of studies the effect of metabolic acidosis on nutritional status in haemodialysis patients has been investigated, their outcome is inconclusive as only a small number of patients were investigated, the follow-up was short and few randomized prospective trials are available. In a singleblind crossover study design, Williams et al. [3] demonstrated that 27% of patients had metabolic acidosis defined as pH < 7.36 when treated with a 30 mmol/l bicarbonate dialysis solution. When the bicarbonate content of the dialysate was increased to 40 mmol/l, all patients had a pH > 7.36 which appeared to be associated with a rise in triceps skinfold thickness but no change in serum albumin or other nutritional parameters. When using a 40 mmol/l bicarbonate dialysis solution, it seems prudent to monitor post-dialysis venous bicarbonate to avoid post-dialytic alkalaemia. In two small prospective studies, it could be demonstrated in haemodialysis patients [4] and patients with chronic renal failure [5] that metabolic acidosis (serum bicarbonate levels <21 mmol/l) could be corrected by oral sodium bicarbonate supplementation (serum bicarbonate levels in both studies after treatment >24 mmol/l). This resulted in a rise in serum albumin levels, but no other changes in nutritional parameters. In both studies it was shown that after correction of metabolic acidosis nPNA decreased. Verove et al. [5] did not find a difference in daily protein intake. Likewise, Movilli et al. did not find a change in protein intake [6] or urea kinetics and ii78 serum proteins [4] after the correction of metabolic acidosis. In a longitudinal observational study of 248 patients it was also observed that correction of metabolic acidosis by increasing the dialysate bicarbonate concentration to 39 mmol/l resulted in a fall in MPNA whereas serum albumin and SGA did not change [7]. Thus, several authors have concluded that in moderate to severe metabolic acidosis protein catabolism is present resulting in a rise in MPNA which then does not reflect daily protein intake only [4–8]. The existence of increased protein turnover in acidotic haemodialysis patients was indeed shown by studies with radiolabelled leucine [9]. Likewise, it was demonstrated that net daily acid gain was higher in acidotic haemodialysis patients [10]. Uribarri et al. [11] found in the HEMO study a negative correlation between serum total carbon dioxide levels and MPNA, and concluded that this could be attributed to a high protein intake in the patients with more severe metabolic acidosis as there were no signs of abnormal nutritional parameters in these patients. Thus, in patients with persistent metabolic acidosis protein intake may be assessed to see whether a high protein intake could contribute to the acidosis. In one randomized prospective study, treatment of acidotic haemodialysis patients with oral sodium bicarbonate and increasing the bicarbonate dialysate concentration to 40 mmol/l caused a rise in serum bicarbonate levels without any effect on serum albumin and other nutritional parameters [12]. In this study, however, oral supplementation and increasing dialysate bicarbonate only resulted in a rise of serum bicarbonate levels to 20 mmol/l, which could be too low to see positive effects on nutritional outcome. Kooman et al. [13] demonstrated in acidotic haemodialysis patients that oral sodium bicarbonate supplementation resolved metabolic acidosis, caused a rise in serum branched-chain amino acids but did not affect nutritional parameters. Similar findings have been obtained in children [14]. In summary, it may be concluded that correction of metabolic acidosis to serum bicarbonate levels at around 20–22 mmol/l should be aimed for to reduce the risk of mortality and morbidity, to increase serum albumin levels and to reduce protein catabolism. References 1. Lowrie EG, Lew NL. Death risk in hemodialysis patients: the predictive value of commonly measured variables and an evaluation of death rate differences between facilities. Am J Kidney Dis 1990; 15: 458–482 2. Bommer J, Locatelli F, Satayathum S et al. Association of predialysis serum bicarbonate levels with risk of mortality and hospitalization in the Dialysis Outcomes and Practice Patterns Study (DOPPS). Am J Kidney Dis 2004; 44: 661–671 3. Williams AJ, Dittmer ID, McArley A, Clarke J. High bicarbonate dialysate in haemodialysis patients: effects on acidosis and nutritional status. Nepholr Dial Transplant 1997; 12: 2633–2637 D. Fouque et al. 4. Movilli E, Zani R, Carli O et al. Correction of metabolic acidosis increases serum albumin concentrations and decreases kinetically evaluated protein intake in haemodialysis patients: a prospective study. Nephrol Dial Transplant 1998; 13: 1719–1722 5. Verove C, Maisonneuve N, El AA, Boldron A, Azar R. Effect of the correction of metabolic acidosis on nutritional status in elderly patients with chronic renal failure. J Renal Nutr 2002; 12: 224–228 6. Movilli E, Bossini N, Viola BF et al. Evidence for an independent role of metabolic acidosis on nutritional status in haemodialysis patients. Nephrol Dial Transplant 1998; 13: 674– 678 7. Blair D, Bigelow C, Sweet SJ. Nutritional effects of delivered bicarbonate dose in maintenance hemodialysis patients. J Renal Nutr 2003; 13: 205–211 8. Bastani B, McNeely M, Schmitz PG. Serum bicarbonate is an independent determinant of protein catabolic rate in chronic hemodialysis. Am J Nephrol 1996; 16: 382–385 9. Graham KA, Reaich D, Channon SM, Downie S, Goodship TH. Correction of acidosis in hemodialysis decreases wholebody protein degradation. J Am Soc Nephrol 1997; 8: 632–637 10. Sepandj F, Jindal K, Kiberd B, Hirsch D. Metabolic acidosis in hemodialysis patients: a study of prevalence and factors affecting intradialytic bicarbonate gain. Artificial Organs 1996; 20: 976–980 11. Uribarri J, Levin NW, Delmez J et al.Association of acidosis and nutritional parameters in hemodialysis patients. Am J Kidney Dis 1999; 34: 493–499 12. Brady JP, Hasbargen JA. Correction of metabolic acidosis and its effect on albumin in chronic hemodialysis patients. Am J Kidney Dis 1998; 31: 35–40 13. Kooman JP, Deutz NE, Zijlmans P et al. The influence of bicarbonate supplementation on plasma levels of branched-chain amino acids in haemodialysis patients with metabolic acidosis. Nephrol Dial Transplant 1997; 12: 2397–2401 14. Mak RH. Effect of metabolic acidosis on branched-chain amino acids in uremia. Pediatr Nephrol 1999; 13: 319–322 Appendices Formulas (body weight, nPNA, dialysis dose, residual renal function) Body weight: definitions BW: body weight—should be assessed in patients wearing stocking feet and light indoor clothing with accurate scales, calibrated on a regular basis. Ask the patient to remove coat, jacket and heavy objects such as coins, keys, whichever is appropriate. ABW: actual body weight—the patient’s present body weight at the time of the observation. SBW: standard body weight—normal weight of healthy Americans of similar sex, age, height and skeletal frame size, obtained through the NHANES II Tables [1]. USB: usual body weight—the patient’s weight obtained through history or previous measurements, considered to be stable over time. efBW: oedema free body weight, corresponding to ‘dry weight’—obtained post-dialysis in HD patients EBPG guideline on nutrition ii79 based on clinical judgement wether the patient still presents clinical oedema. Estimating height in elderly and physically disabled patients [2] AefBW: adjusted oedema-free body weight—should be used in order to calculate the optimal dietary intake of protein and energy. It may avoid recommendations for too large intakes that may induce overproduction of waste products increasing uraemic symptoms. When patient’s body weight will improve towards standard body weight value, adjustment of body weight will not be necessary anymore. If possible use recent documented (i.e. passport details) or self reported height, although patients tend to overestimate height which decreases with advancing age. AefBW ¼ efBW þ ðSBW efBWÞ 0:25 where SBW obtained from NHANES II Tables [1]. Height Height should be measured as follows: ask the patient to remove shoes, to stand straight with feet together, buttocks, shoulder blades and head against the measuring device or wall and looking straight ahead. The measuring device will indicate length in meters/centimetres. The practitioner should not depend on self-reporting as patients tend to overestimate height which decreases with advancing age. Alternative height measurements Length forearm (ulna), knee height and arm demispan. In older people, the measurement of height to calculate BMI does not take into account bone loss (osteoporosis) that results in reduced height. Using alternative measurements such as knee height compensates for age-related changes. Arm demispan can be used for people with curvatures of the spine, with infirmity and confusion. Length of forearm (ulna) (Fig. 1) Ask the patient to bend the left arm if possible, palm across the chest, fingers pointing to opposite shoulder. Using a tape measure, measure the length in centimeters to the nearest 0.5 cm between the point of the elbow (olecranon) and the mid-point of the prominent bone of the wrist (styloid process). Use Table 1 to convert ulna length (cm) to height (m). Knee height (Fig. 2) Measure left leg if possible. The patient should sit on a chair, without shoes, with knee at a right angle. Hold tape measure between 3rd and 4th finger with zero reading underneath fingers. Place your hand flat across the patient’s thigh, about 4 cm behind the front of the knee. Extend the tape measure straight down the side of the leg in line with the bony prominence at the ankle (lateral malleolus) to the base of the heel. Measure to the nearest 0.5 cm. Note the length and use Table 2 to convert knee height (cm) to height (m). Fig. 1. Estimating height from ulna length (permission from MAG BAPEN, www.bapen.org.uk). Source: Malnutrition Advisory Group (MAG) British Association of Enteral and Parenteral Nutrition (BAPEN), 2003 (www.bapen.org). Demispan (Fig. 3). Demispan should not be used in patients with severe or obvious curvature of the spine (kyphosis or scoliosis). Table 1. Estimating height from ulna length (permission from MAG BAPEN, www.bapen.org.uk) HEIGHT (m) HEIGHT (m) HEIGHT (m) HEIGHT (m) Men (<65 years) Men (>65 years) Ulna length (cm) Women (<65 years) Women (>65 years) Men (<65 years) Men (>65 years) Ulna length (cm) Women (<65 years) Women (>65 years) 1.94 1.87 32.0 1.84 1.84 1.69 1.65 25.0 1.65 1.61 1.93 1.86 31.5 1.83 1.83 1.67 1.63 24.5 1.63 1.60 1.91 1.84 31.0 1.81 1.81 1.66 1.62 24.0 1.62 1.58 1.89 1.82 30.5 1.80 1.79 1:64 1.60 23.5 1.61 1.56 1.87 1.81 30.0 1.79 1.78 1.62 1.59 23.0 1.59 1.55 1.85 1.79 29.5 1.77 1.76 1.60 1.57 22.5 1.58 1.53 1.84 1.78 29.0 1.76 1.75 1.58 1.56 22.0 1.56 1.52 1.82 1.76 28.5 1.75 1.73 1.57 1.54 21.5 1.55 1.50 1.80 1.75 28.0 1.73 1.71 1.55 1.52 21.0 1.54 1.48 1.78 1.73 27.5 1.72 1.70 1.53 1.51 20.5 1.52 1.47 1.76 1.71 27.0 1.70 1.68 1.51 1.49 20.0 1.51 1.45 1.75 1.70 26.5 1.69 1.66 1.49 1.48 19.5 1.50 1.44 1.73 1.68 26.0 1.68 1.65 1.48 1.46 19.0 1.48 1.42 1.71 1.67 25.5 1.66 1.63 1.46 1.45 18.5 1.47 1.40 ii80 For bed bound patients, those with severe disabilities and those with kyphosis or scoliosis, it is preferable to use forearm (ulna) length to estimate height. The patient should stand as this makes taking the measurement easier. Locate and mark the mid-point of the sternal notch (V at the base of the neck). Ask the patient to raise the right arm until it is horizontal with the shoulder (give assistance if necessary; make sure the wrist is straight). D. Fouque et al. Place a tape measure between the middle and ring finger of the patient’s right hand, with zero at the base of the fingers. Extend the tape measure along the length of the arm to the mid-point of the sternal notch and note the measurement to the nearest 0.5 cm. Use Table 3 to convert demispan length to height (m). Ideal body weight estimation (Tables 4 and 5). Body mass index (BMI). BMI is calculated from the weight (kg) divided by the square of the height (m). BMI of maintenance dialysis patients should be maintained in the upper 50th percentile (BMI for men and women of at least approximately 23.6 and 24.0 kg/m2) The World Health Organization describes the condition of low BMI as thinness which is divided into three grades: Grade 1: BMI 17.0–18.49 (mild thinness) Grade 2: BMI 16.0–16.99 (moderate thinness) Grade 3: BMI < 16.0 (severe thinness) The Malnutrition Advisory Group (MAG), a standing committee of the British Association for Parenteral and Enteral Nutrition [2] has recommended Fig. 2. Estimating height from knee height (permission from MAG BAPEN, www.bapen.org.uk). Source: Malnutrition Advisory Group (MAG) British Association of Enteral and Parenteral Nutrition (BAPEN), 2003 (www.bapen.org). Fig. 3. Estimating height using demispan (permission from MAG BAPEN, www.bapen.org.uk). Source: Malnutrition Advisory Group (MAG) British Association of Enteral and Parenteral Nutrition (BAPEN), 2003 (www.bapen.org). Table 2. Estimating height (in meter) from knee height (permission from MAG BAPEN, www.bapen.org.uk) Men (18–59 years) 1.94 1.93 1.92 1.91 1.90 1.89 1.88 1.87 1.865 1.86 1.85 1.84 1.83 1.82 1.81 Men (60–90 years) 1.94 1.93 1.92 1.91 1.90 1.89 1.88 1.87 1.86 1.85 1.84 1.83 1.82 1.81 1.80 Knee height (cm) 65 64.5 64 63.5 63 62.5 62 61.5 61 60.5 60 59.5 59 58.5 58 Women (18–59 years) 1.89 1.88 1.875 1.87 1.86 1.85 1.84 1.83 1.82 1.81 1.80 1.79 1.78 1.77 1.76 Women (60–90 years) 1.86 1.85 1.84 1.835 1.83 1.82 1.81 1.80 1.79 1.78 1.77 1.76 1.75 1.74 1.73 Men (18–59 years) 1.80 1.79 1.78 1.77 1.76 1.75 1.74 1.73 1.72 1.71 1.705 1.70 1.69 1.68 1.67 Men (60–90 years 1.79 1.78 1.77 1.76 1.74 1.73 1.72 1.71 1.70 1.69 1.68 1.67 1.66 1.65 1.64 Knee height (cm) 57.5 57 56.5 56 55.5 55 54.5 54 53.5 53 52.5 52 51.5 51 50.5 Women (18–59 years) 1.75 1.74 1.735 1.73 1.72 1.71 1.70 1.69 1.68 1.67 1.66 1.65 1.64 1.63 1.62 Women (60–90 years) 1.72 1.71 1.70 1.69 1.68 1.67 1.66 1.65 1.64 1.63 1.625 1.62 1.61 1.60 1.59 Men (18–59 years) 1.66 1.65 1.64 1.63 1.62 1.61 1.60 1.59 1.58 1.57 1.56 1.555 1.55 1.54 1.53 Men (60–90 years 1.63 1.62 1.61 1.60 1.59 1.58 1.57 1.56 1.55 1.54 1.53 1.52 1.51 1.49 1.48 Knee height (cm) 50 49.5 49 48.5 48 47.5 47 46.5 46 45.5 45 44.5 44 43.5 43 Women (18–59 years) 1.61 1.60 1.59 1.585 1.58 1.57 1.56 1.55 1.54 1.53 1.52 1.51 1.50 1.49 1.48 Women (60–90 years) 1.58 1.57 1.56 1.55 1.54 1.53 1.52 1.51 1.50 1.49 1.48 1.47 1.46 1.45 1.44 EBPG guideline on nutrition ii81 Table 3. Estimating height (in meter) using demispan (permission from MAG BAPEN, www.bapen.org.uk) Men (16–54 years) Men (>55 years) Demispan (cm) Women (16–54 years) Women (>55 years) Men (16–54 years Men (>55 years Demispan (cm) Women (16–54 years) Women (>55 years) 1.97 1.90 99 1.91 1.86 1.75 1.69 82 1.69 1.65 1.95 1.89 98 1.89 1.85 1.73 1.68 81 1.67 1.64 1.94 1.87 97 1.88 1.83 1.72 1.67 80 1.66 1.63 1.93 1.86 96 1.87 1.82 1.71 1.66 79 1.65 1.62 1.92 1.85 95 1.85 1.81 1.69 1.65 78 1.63 1.61 1.90 1.84 94 1.84 1.80 1.68 1.64 77 1.62 1.59 1.89 1.83 93 1.83 1.79 1.67 1.62 76 1.61 1.58 1.88 1.81 92 1.82 1.77 1.65 1.61 75 1.59 1.57 1.86 1.80 91 1.80 1.76 1.64 1.60 74 1.58 1.56 1.85 1.79 90 1.79 1.75 1.63 1.59 73 1.57 1.55 1.84 1.78 89 1.78 1.74 1.62 1.57 72 1.56 1.54 1.82 1.77 88 1.76 1.73 1.60 1.56 71 1.54 1.52 1.81 1.75 87 1.75 1.71 1.59 1.55 70 1.53 1.51 1.80 1.74 86 1.74 1.70 1.58 1.54 69 1.52 1.50 1.78 1.73 85 1.72 1.69 1.56 1.53 68 1.50 1.49 1.77 1.72 84 1.71 1.68 1.55 1.51 67 1.49 1.47 1.76 1.71 83 1.70 1.67 1.54 1.50 66 1.48 1.46 Table 4. Fiftieth (50th) Percentile of Standard Body Weight for Men (NHANES 1 and II); reproduced with permission from Frisancho et al. The Amercian Journal of Clinical Nutrition [1]. Table 5. Fifthieth (50th) Percentile of Standard Body Weight for Women (NHANES 1 and II); reproduced with permission from Frisancho et al. The Amercian Journal of Clinical Nutrition [1]. Age Age 25–54 years 55–74 years 25–54 years Weight (kg) Weight (kg) Height (cm) Small frame Medium frame Large frame Small frame Medium frame Large frame 157 160 163 165 168 170 173 175 178 180 183 185 188 64 61 66 66 67 71 71 74 75 76 74 79 80 68 71 71 74 75 77 78 78 81 81 84 85 88 82 83 84 79 84 84 86 89 87 91 91 93 92 61 62 63 70 68 69 70 75 76 69 76a 78a 77a 68 70 71 72 74 78 78 77 80 84 81 88 95 77 80 77 79 80 85 83 84 87 84 90 88 89 a Value estimated through linear regression equation. nutritional measurements should be height, weight and recent weight loss. The BMI categories are: BMI < 18.5 chronic protein–energy undernutrition probable BMI 18.5–20.0 chronic protein–energy undernutrition possible BMI > 20.0 chronic protein–energy undernutrition unlikely Classification of BMI. Significance: (normal individuals) from Wiggins [3] <16 <18.5 Severely underweight underweight 18.5–24.9 Within normal weight range 25–29.9 Overweight 30–34.9 Obesity class I 35–39.9 Obesity class II >40 Obesity class III 55–74 years Associated with health problems May be associated with health problems for some people ‘ideal’ or healthy weight range associated with lowest risk of illness and mortality for most people May be associated with health problems in some people Associated with increased risk of health problems such as heart disease, hypertension, diabetes Associated with increased risk of health problems such as heart disease, hypertension and diabetes Extreme obesity Height (cm) Small frame Medium frame Large frame Small frame Medium frame Large frame 147 150 152 155 157 160 163 165 168 170 173 175 178 52 53 53 54 55 55 57 60 58 59 62 63* 64* 63 66 60 61 61 62 62 63 63 65 67 68 70 86a 78 87 81 81 83 79 81 75 80 76 79 76 54 55 54 56 58 58 60 60 68 61a 61a 62a 63a 57 62 65 64 64 65 66 67 66 72 70 72a 73a 92 78 78 79 82 80 77 80 82 80 79 85a 85a a Value estimated through linear regression equation. Calculating BMI in amputees [3]. IBW needs to be adjusted by taking into account the weight of body segment(s) that is/are amputated. Adjustments of body weight can be made from knowledge of missing limbs segments. Upper limb: whole arm 5% (upper arm 2.7% and fore arm 1.6%, hand 0.7%) Lower limb: whole leg 16% (thigh 10.1%, lower leg 4.4%, foot 1.5%) To measure full body weight equation Estimated full body weight ðkgÞ measured weight ¼ 100 ð100 % weight of amputationÞ Change in body weight over the previous 6 months Unintentional weight loss over the previous 3–6 months is categorized as 10 % of body weight: clinically significant, 5–10% of body weight: more than normal intraindividual variation, <5% of body weight: within ‘normal’ intraindividual variation. ii82 D. Fouque et al. A cut-off of >10% weight loss during the last 6 months is recommended to be used in the diagnosis of malnutrition [4]. Body surface. Body surface area should be estimated according to Gehan and George method [5] BSA ¼ 0:235 BW0:51456 BH0:42246 Body water. Total body water (TBW), necessary for the calculation of the correct dialysis dose, can be estimated by the Watson formulas (2): Vmale (L) ¼ 2.447 þ 0.3362 BW (kg) þ 0.1074 BH (cm) 0.09516 age (years) Vfemale (L) ¼ 2.097 þ 0.2466 BW (kg) þ 0.1069 BH (cm) Normalized protein equivalent of total nitrogen appearance nPNA. By the use of protein nitrogen appearance (PNA), formerly called protein catabolic rate (PCR), the dietary protein intake can be estimated in patients with neutral nitrogen balance (i.e. in patients, who are neither anabolic nor catabolic). In order to normalize PNA, it should be related to the body weight of the patient, leading to nPNA. In order to optimize the diet of patients with renal disease, the dietary protein intake has to be controlled. In stable patients (non-catabolic, non-anabolic) nPNA reflects the dietary protein intake and can be calculated based on UNA (urea nitrogen appearance in the urine and/or in the dialysate, respectively) for the following reasons: 1. In patients with a neutral nitrogen balance, the nitrogen intake is identical with the loss of nitrogen (that is the total nitrogen appearance: TNA) 2. As nitrogen in protein accounts for 16% of the protein’s weight, the protein equivalent of nitrogen appearance (PNA) can be calculated by total nitrogen appearance (TNA).as: PNA ¼ 6:25 TNA 3. There is a linear relationship between TNA and UNA. The ratio between UNA and TNA, however, depends on the dietary intake of protein as well as the status and treatment of the patient [2] 4. In order to normalize PNA to body weight, the K/DOQI Nutrition Work Group recommends the use of the following formula [4]: nPNA ¼ PNA AefBW where AefBW is the adjusted, oedema free body weight, see above PNA is calculated by using spKt/V and C0. Different formulas are used for different days of the week (5) in a two-BUN, single-pool, variable-volume model: Beginning of the week PNA ¼ C0/[36.3 þ (5.48)(spKt/V) þ (53.5)/(spKt/V)] þ 0.168 Midweek PNA ¼ C0/[25.8 þ (1.15)(spKt/V) þ (56.4)/(spKt/V)] þ 0.168 End of week PNA ¼ C0/[16.3 þ (4.3)(spKt/V) þ (56.6)/(spKt/V)] þ 0.168 where C0 ¼ predialysis blood urea nitrogen (BUN) spKt=V ¼ single pool Kt=V In patients with considerable residual renal function, C0 should be replaced by C00 : C00 ¼ C0 ½1 þ ð0:79 þ 3:08=ðKt=VÞÞ Kr=V where Kr is residual renal clearance in ml/min [4]. Residual renal function: glomerular filtration rate (GFR) Residual renal function should be expressed as equivalents of glomerular filtration rate (GFR). One accepted method in both PD and HD patients is to estimate GFR from the mean of urea and creatinine clearance [6], normalized to 1.73 m2 using the Gehan & George method [5] for calculating body surface area (BSA). The collection time in haemodialysis patients is identical with the interval between two dialysis sessions. The plasma concentration of urea and creatinine used in the following formula are determined at the beginning and end of the collection. As in pre-ESRD and peritoneal dialysis patients, the bladder must be empty at the beginning of the collection (i.e. at the end of the dialysis) and must be completely emptied at the end of the collection (i.e. before the next dialysis starts): Uurea Ucreat þ GFR ¼ prePurea þpostPurea prePcreat þpostPcreat Uvol 1:73 BSA t derived from: Uurea 0:5 ðprePurea þpostPurea Þ Ucreat þ 0:5 ðprePcreat þpostPcreat Þ Uvol 1:73 BSA t GFR ¼ 0:5 with 0.5 (prePurea þ postPurea) ¼ average concentration of urea in the plasma between dialysis sessions and 0.5 (prePcreat þ postPcreat) ¼ average concentration of creatinine in the plasma between dialysis. prePurea, plasma urea concentration before dialysis at end of collection; postPurea, plasma urea concentration after dialysis at beginning of collection; prePcreat, plasma creatinine concentration before dialysis at end of collection; postPcreat, plasma creatinine concentration EBPG guideline on nutrition after dialysis at beginning of collection; Uurea, urine urea concentration; Ucreat, urine creatinine concentration; Uvol, urine volume; t, time of collection between dialysis sessions. In order to be more precise, the post-dialysis concentrations should be replaced by the post-rebound concentrations, which can be calculated as follows [7]: Post-rebound concentration for urea: post td=ðtdþ35Þ rebound ¼ pre pre where td, dialysis time in minutes; pre, concentration before dialysis before collection; post, concentration immediately after dialysis. Post-rebound concentration for creatinine: post td=ðtdþ70Þ rebound ¼ pre pre where td, dialysis time in minutes; pre, concentration before dialysis before collection; post, concentration immediately after dialysis. Dialysis dose For MHD it is recommended to calculate the equilibrated Kt/V (eKT/V) instead of the single pool Kt/V (sp(Kt/V) from pre- and post-HD blood samples taken under standard conditions (see below). The eKt/V takes into account the urea rebound post dialysis resulting from redistribution of peripheral pools. Haemodialysis dose should be quantified as equilibrated Kt/V (eKtV) based on the regional blood flow two-pool model [8,9]: ii83 for central venous catheter. using sterile technique withdraw any heparin/saline from the arterial port withdraw 10 mL of blood collect blood sample (b)Post-dialysis blood sampling procedure: As recirculation of dialysated blood in the arterial line or rebound of urea can significantly influence the value of urea, the sampling technique must be performed in a standardized way leading to reproducible results. In following the techniques explained below, the sample will be drawn after possible recirculation but before rebound of urea from peripheral compounds. 1. Turn off dialysate flow or reduce to minimum, decrease ultrafiltration rate to 50 ml/h 2. Decrease blood flow to 50–100 ml/min for 15 s proceed with slow pump or stop pump technique Slow flow sampling technique 3. draw blood sample with pump running at 50–100 ml/min 4. stop blood pump and complete disconnection procedure Stop pump sampling technique 5. stop the blood pump 6. clamp arterial and venous blood lines; clamp arterial needle tubing 7. sample blood either from arterial sampling port nearest to patient or from the arterial needle tubing after disconnection from the arterial blood line 8. blood is returned to the patient, complete disconnection procedure eKt=V ¼ spKt=V ð0:6 spKtV=TÞ þ 0:03 ðwith an arteriovenous accessÞ The value for single pool Kt/V (spKtV) should be derived from urea kinetic model or alternatively from the natural logarithm equation to estimate spKtV [10]: spKt=V ¼ lnðR 0:008 tÞ þ ð4 3:5 RÞ dBW=BW where R, post-HD/pre-HD BUN ratio; T, treatment time in hours; dBW, intradialytic weight lost (corresponding to ultrafiltration); BW, end session body weight. Standard conditions for blood sampling Methods procedure derived from the K/DOQI guidelines [4,11]. (a) Pre-dialysis blood sampling procedure: for arteriovenous graft or fistula: obtain the blood from arterial needle before connecting the tube or flushing the needle, avoid dilution of the sample by saline and/or heparin LABORATORY METHODS Serum Albumin The gold-standard for determining serum albumin levels are immunological methods. Serum albumin levels determined by established methods like the bromcresol green (BCG) or bromcresol purple (BCP) method differ from those obtained by immunological methods due to limitations in methodology [12]. Comparing the values of albumin in plasma and serum, measured by the same method, identical values are found. However, differences are found between the bromcresol green and the bromcresol purple method. Uremic toxins as well as certain medications (e.g. phenylbutazon, clofibric acid) [13] influence the measurement. In general, bromcresol green methods overestimate albumin levels [14] compared with bromcresol purple [15] and nephelometry [16]. Bromcresol purple, on the other hand, generally underestimates albumin values [12,17]. Thus the evaluation of the ii84 serum albumin level must take into account the different normal ranges of the applied laboratory methods. Bicarbonate Plasma bicarbonate is estimated from total CO2 measurements. It is thus mandatory to use fresh D. Fouque et al. blood samples because CO2 might be lost leading to significant underestimation of plasma bicarbonate [18]. One must also keep in mind that total CO2 levels assessed by electrode-based methods are an average 4 mmol/l higher compared with plasma bicarbonate concentrations determined by enzymatic assays [19]. EBPG guideline on nutrition The plasma bicarbonate, calculated from pCO2 by using the Henderson-Hasselbach equation, gives: ðpH6:1Þ cHCO 3 ðmmol=lÞ ¼ 0:0307 pCO2 ðmmHgÞ 10 C-reactive protein C-reactive Protein (CRP) has been used as a marker of inflammation for many years. In this respect, levels in the range of 5–300 mg/l have been of interest, which are detected by the common laboratory methods. Standard immunological methods like immunonephelometry and immunoturbidimetry should detect levels at least above 5 mg/l. New assays allow the detection of even lower CRP levels in the range of 0.1–10 mg/l. These so called ‘high sensitive-CRP-assays’ (hs-CRP) are needed to assess the risk of atherosclerosis [20–22], as already only slightly elevated CRP levels below 5 mg/ l have been found to be associated with increased risk of cardiovascular disease [23]. TECHNICAL ASSESSMENT Subjective global assessment (SGA) The SGA was developed for use in assessing the nutrition of general surgery patients [24]. It is recommended also for patients on dialysis, because it is a valid clinical assessment of nutritional status and is strongly associated with patient survival. Remind that the overall SGA classification is not simply a numerical store. It does strongly depend on the clinical judgement of the examiner. He has to consider whether the patient’s status is improving or deteriorating, this information may lead to different ‘scores’ given in each section. The SGA is based on history and physical examination [24]. It focuses on gastrointestinal symptoms (anorexia, nausea, vomiting, diarrhoea), weight loss in the preceding 6 months, and visual assessment of subcutaneous tissue and muscle mass. Scores are subjectively rated on a four-point or seven point scale [4]. The use of the seven point scale is recommended because of its greater sensitivity and its use in large epidemiological studies such as the CANUSA study [25]: Severe malnutrition: 1 or 2, Moderate to mild malnutrition: 3 to 5, Mild malnutrition to normal nutritional state: 6 to 7. SGA was found to be related to other markers of nutritional status in dialysed [26] and non-dialysed uraemic subjects [27] as well as to mortality [28]. Anthropometry Skinfold thickness (SFT) should be measured by someone experienced in the use of skinfold callipers. The measurement is taken at four different sites ii85 Table 6. Equivalent body fat content (in% body weight) obtained from the sum of four (biceps, triceps, subscapular and suprailiac) skinfold measurements. Reproduced with permission from Durnin and Womersley. British Journal of Nutrition [32]. Skinfolds Men (y) Women (y) (mm) 17–29 30–39 40–49 50þ 16–29 30–39 40–49 50þ 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90 95 100 105 110 115 120 125 130 135 140 145 150 155 160 165 170 175 180 185 190 195 200 205 210 4.8 8.1 10.5 12.9 14.7 16.4 17.7 19.0 20.1 21.2 22.2 23.1 24.0 24.8 25.5 26.2 26.9 27.6 28.2 28.8 29.4 30.0 31.0 31.5 32.0 32.5 32.9 33.3 33.7 34.1 34.5 34.9 35.3 35.6 35.9 12.2 14.2 16.2 17.7 19.2 20.2 21.5 22.5 23.5 24.3 25.1 25.9 26.6 27.2 27.8 28.4 29.0 29.6 30.1 30.6 31.1 31.5 31.9 32.3 32.7 33.1 33.5 33.9 34.3 34.6 34.8 12.2 15.0 17.7 19.6 21.4 23.0 24.6 25.9 27.1 28.2 29.3 30.3 31.2 32.1 33.0 33.7 34.4 35.1 35.8 36.4 37.0 37.6 38.2 38.7 39.2 39.7 40.2 40.7 41.2 41.6 42.0 12.6 15.6 18.6 20.8 22.9 24.7 26.5 27.9 29.2 30.4 31.6 32.7 33.8 34.8 35.8 36.6 37.4 38.2 39.0 39.7 40.4 41.1 41.8 42.4 43.0 43.6 44.1 44.6 45.1 45.6 46.1 10.5 14.1 16.8 19.5 21.5 23.4 25.0 26.5 27.8 29.1 30.2 31.2 32.2 33.1 34.0 34.8 35.6 36.4 37.1 37.8 38.4 39.0 39.6 40.2 40.8 41.3 41.8 42.3 42.8 43.3 43.7 44.1 17.0 19.4 21.8 23.7 25.5 26.9 28.2 29.4 30.6 31.6 32.5 33.4 34.3 35.1 35.8 36.5 37.2 37.9 38.6 39.1 39.6 40.1 40.6 41.1 41.6 42.1 42.6 43.1 43.6 44.0 44.4 44.8 45.2 45.6 45.8 46.2 46.5 19.8 22.2 24.5 26.4 28.2 29.6 31.0 32.1 33.2 34.1 35.0 35.9 36.7 37.5 38.3 39.0 39.7 40.4 41.0 41.5 42.0 42.5 43.0 43.5 44.0 44.5 45.0 45.4 45.8 46.2 46.6 47.0 47.4 47.8 48.2 48.5 48.9 49.1 49.4 21.4 24.0 26.6 28.5 30.3 31.9 33.4 34.6 35.7 36.7 37.7 38.7 39.6 40.4 41.2 41.9 42.6 43.3 43.9 44.5 45.1 45.7 46.2 46.7 47.2 47.7 48.2 48.7 49.2 49.6 50.0 50.4 50.8 51.2 51.6 52.0 52.4 52.7 53.0 Source: Durnin JV, Womersley J. Body fat assessed from total body density and its estimation from skinfold thickness: measurements on 481 men and women aged from 16 to 72 years. British Journal of Nutrition 1974; 32: 77-97. (biceps, triceps, subscapular and suprailiac). For each skinfold, the mean of three measurements is taken. The sum of four different skinfold sites allows to estimate patient’s body fat in percent body weight (Table 6). Mid-upper arm circumference (MAC) should be measured on the non-dominant, non-fistula arm. The arm should be bent at the elbow at an angle of 908. The midpoint between the acromion and olecranon process should be ascertained by measurement and marked. The MAC at this point should be measured three times and the mean taken. ii86 D. Fouque et al. Table 7. Mid-arm muscle circumference (MAMC) for adult men and women from USA (from NHANES I study [33]); measurements made in the right arm. Reproduced with permission from Bishop CW, Bowen PE, Ritchey SJ. The Amercian Journal of Clinical Nutrition [33]. Age (years) Men 18–24 25–34 35–44 45–54 55–64 65–74 Women 18–24 25–34 35–44 45–54 55–64 65–74 50th Percentile (cm) 27.2 28.0 28.7 28.1 27.9 26.9 20.6 21.4 22.0 22.2 22.6 22.5 Source: Bishop CW, Bowen PE, Ritchey SJ. Norms for nutritional assessment of American adults for upper arm anthropometry. American Journal of Clinical Nutrition 1981; 34: 2530–39 [ref. 33]. Mid-arm muscle circumference (MAMC, Table 7) should be calculated as the MAC in cm minus (triceps skinfold thickness ). There are no agreed cut off points for MAC, TSF or MAMC for the diagnosis of malnutrition in either the normal population or patients with chronic renal failure. Frisancho’s tables provide standards for mid-arm muscle circumference in normal subjects [29,30] whilst norms have also been published for the dialysis population [31]. Handgrip strength Muscle strength is best evaluated by muscle dynanometry of the handgrip strength which has been related to protein stores assessed by neutron activation analysis in non-uraemic subjects [34]. In pre-ESRD patients handgrip strength was strongly related to lean body mass determined by DEXA, anthropometry, and creatinine kinetics and the strongest factor related to malnutrition defined by SGA [27]. In dialysis patients handgrip strength was reduced in malnourished patients determined by SGA [35]. References 1. Frisancho AR. New standards of weight and body composition by frame size and height for assessment of nutritional status of adults and the elderly. Am J Clin Nutr 1984; 40: 808–819 2. Todorovic V, Russell C, Stratton R, Ward J, Elia M. A Guide to the ‘Malnutrition Universal Screening Tool’ (‘MUST’) for Adults. Brit Ass Parenter Enteral Nutr (BAPEN) 2003, pp. 1–23. 3. Wiggins KL. Renal care: resources and practical applications. Renal Dietitians Dietetic Practice Group. J Am Diet Assoc 2001; 1–101 4. Clinical practice guidelines for nutrition in chronic renal failure. K/DOQI, National Kidney Foundation. Am J Kidney Dis 2000; 35: S1–S140 5. Gehan EA, George SL. Estimation of human body surface area from height and weight. Cancer Chemother Rep 1970; 54: 225–235 6. Van Olden RW, Krediet RT, Struijk DG, Arisz L. Measurement of residual renal function in patients treated with continuous ambulatory peritoneal dialysis. J Am Soc Nephrol 1996; 7: 745–750 7. Tattersall JE, DeTakats D, Chamney P, Greenwood RN, Farrington K. The post-hemodialysis rebound: predicting and quantifying its effect on Kt/V. Kidney Int 1996; 50: 2094–2102 8. Daugirdas JT. Simplified equations for monitoring Kt/V, PCRn, eKt/V, and ePCRn. Adv Ren Replace Ther 1995; 2: 295–304 9. Leblanc M, Charbonneau R, Lalumiere G, Cartier P, Deziel C. Postdialysis urea rebound: determinants and influence on dialysis delivery in chronic hemodialysis patients. Am J Kidney Dis 1996; 27: 253–261 10. Daugirdas JT. Second generation logarithmic estimates of single-pool variable volume Kt/V: an analysis of error. J Am Soc Nephrol 1993; 4: 1205–1213 11. NKF-K/DOQI Clinical Practice Guidelines for Hemodialysis Adequacy: update 2000. Am J Kidney Dis 2001; 37: S7–S64 12. Joseph R, Tria L, Mossey RT et al. Comparison of methods for measuring albumin in peritoneal dialysis and hemodialysis patients. Am J Kidney Dis 1996; 27: 566–572 13. Calvo R, Carlos R, Erill S. Underestimation of albumin content by bromocresol green, induced by drug displacers and uremia. Int J Clin Pharmacol Ther Toxicol 1985; 23: 76–78 14. Carfray A, Patel K, Whitaker P, Garrick P, Griffiths GJ, Warwick GL. Albumin as an outcome measure in haemodialysis in patients: the effect of variation in assay method. Nephrol Dial Transplant 2000; 15: 1819–1822 15. McGinlay JM, Payne RB. Serum albumin by dye-binding: bromocresol green or bromocresol purple? The case for conservatism. Ann Clin Biochem 1988; 25: 417–421 16. Blagg CR, Liedtke RJ, Batjer JD et al. Serum albumin concentration-related health care financing administration quality assurance criterion is method-dependent: revision is necessary. Am J Kidney Dis 1993; 21: 138–144 17. Maguire GA, Price CP. Bromcresol purple method for serum albumin gives falsely low values in patients with renal insufficiency. Clin Chem Acta 1986; 155: 83–87 18. Kirschbaum B. Spurious metabolic acidosis in hemodialysis patients. Am J Kidney Dis 2000; 35: 1068–1071 19. Bray SH, Tung RL, Jones ER. The magnitude of metabolic acidosis is dependent on differences in bicarbonate assays. Am J Kidney Dis 1996; 28: 700–703 20. Rifai N, Ridker PM. High-sensitivity C-reactive protein: a novel and promising marker of coronary heart disease. Clin Chem 2001; 47: 403–411 21. Blake GJ, Ridker PM. High sensitivity C-reactive protein for predicting cardiovascular disease: an inflammatory hypothesis. Eur Heart J 2001; 22: 349–352 22. Cotton F, Thiry P, Hsain AB, Boeynaems JM. Analyzer transfer of a broad range high-sensitivity C-reactive protein immunoassay. Clin Lab 2001; 47: 405–409 23. Ridker PM, Cushman M, Stampfer MJ, Tracy RP, Hennekens CH. Inflammation, aspirin, and the risk of cardiovascular disease in apparently healthy men. N Engl J Med 1997; 336: 973–979 24. Detsky AS, McLaughlin JR, Baker JP et al. What is subjective global assessment of nutritional status? J Parenter Enteral Nutr 1987; 11: 8–13 EBPG guideline on nutrition 25. Adequacy of dialysis and nutrition in continuous peritoneal dialysis: association with clinical outcomes. Canada-USA (CANUSA) Peritoneal Dialysis Study Group. J Am Soc Nephrol 1996; 7: 198–207 26. Enia G, Sicuso C, Alati G, Zoccali C. Subjective global assessment of nutrition in dialysis patients. Nephrol Dial Transplant 1993; 8: 1094–1098 27. Heimburger O, Qureshi AR, Blaner WS, Berglund L, Stenvinkel P. Hand-grip muscle strength, lean body mass, and plasma proteins as markers of nutritional status in patients with chronic renal failure close to start of dialysis therapy. Am J Kidney Dis 2000; 36: 1213–1225 28. Chung SH, Lindholm B, Lee HB. Influence of initial nutritional status on continuous ambulatory peritoneal dialysis patient survival. Perit Dial Int 2000; 20: 19–26 29. Frisancho AR. New norms of upper limb fat and muscle areas for assessment of nutritional status. Am J Clin Nutr 1981; 34: 2540–2545 ii87 30. Frisancho AR. Triceps skin fold and upper arm muscle size norms for assessment of nutrition status. Am J Clin Nutr 1974; 27: 1052–1058 31. Nelson EE, Hong CD, Pesce AL, Peterson DW, Singh S, Pollak VE. Anthropometric norms for the dialysis population. Am J Kidney Dis 1990; 16: 32–37 32. Durnin JV, Womersley J. Body fat assessed from total body density and its estimation from skinfold thickness: measurements on 481 men and women aged from 16 to 72 years. Br J Nutr 1974; 32: 77–97 33. Bishop CW, Bowen PE, Ritchey SJ. Norms for nutritional assessment of American adults for upper arm anthropometry. Am J Clin Nutr 1981; 34: 2530–2539 34. Windsor JA, Hill GL. Grip strength: a measure of the proportion of protein loss in surgical patients. Br J Surg 1988; 75: 880–882 35. Qureshi AR, Alvestrand A, Danielsson A et al. Factors predicting malnutrition in hemodialysis patients: a crosssectional study. Kidney Int 1998; 53: 773–782







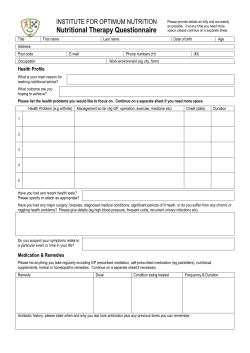


© Copyright 2026