
Balloon catheter ablation to treat paroxysmal atrial fibrillation:
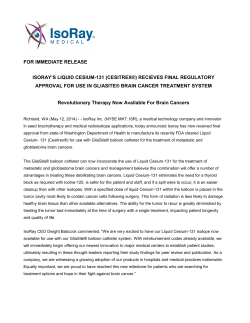
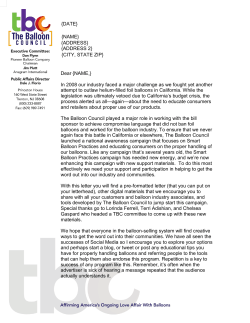
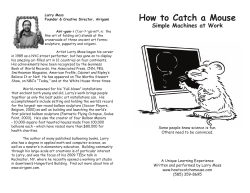
Balloon catheter ablation to treat paroxysmal atrial fibrillation: What is the level of pulmonary venous isolation? Vivek Y. Reddy, MD,* Petr Neuzil, MD,† Andre d’Avila, MD,* Margaret Laragy, BS,* Zachary J. Malchano, MS,* Stepan Kralovec,† Steven J. Kim, MS,‡ Jeremy N. Ruskin, MD* From the *Cardiology Department, Homolka Hospital, Prague, Czech Republic, †Cardiac Arrhythmia Service, Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts, and ‡St. Jude Medical, Inc., Minnetonka, Minnesota. BACKGROUND Unlike the initial balloon ablation catheters that were designed to deliver ablation lesions within the pulmonary veins (PVs), the current balloon prototypes are fashioned to deliver lesions at the PV ostia. OBJECTIVE Using electroanatomical mapping, this study evaluates the actual location of ablation lesions generated by cryobased, laser-based, or ultrasound-based balloon catheters. METHODS In a total of 14 patients with paroxysmal atrial fibrillation, PV isolation was performed using either a cryoballoon catheter (8 patients), laser catheter (4 patients) or ultrasound balloon catheter (2 patients). Patients underwent preprocedural computed tomographic/magnetic resonance imaging. An intracardiac ultrasound catheter was used to aid in positioning the balloon catheter at the PV ostium/antrum. In all patients, sinus rhythm bipolar voltage amplitude maps (using either CARTO with computed tomographic/magnetic resonance image integration or Introduction Electrical pulmonary venous (PV) disconnection is an effective means to treat patients with paroxysmal atrial fibrillation (AF).1– 8 Because of the technical difficulties associated with point-to-point ablation using a standard spot ablation catheter with the left atrium (LA), there has been a significant effort in developing alternative ablation catheter designs to quickly and easily isolate PVs. The first such device tested clinically was an ultrasound balloon ablation catheter that delivered energy in a radial fashion at the level of the diameter of the balloon, hence necessitating that the balloon catheter be placed within the PV when delivering energy.9 This balloon design was suboptimal because the level of electrical isolation typically excluded the proximal Supported in part by the Deane Institute for AF and Stroke Research, and an NIH K23 award (HL68064) to Dr. Reddy. Drs. Reddy and Neuzil have received research grant support from Cryocath Technologies, Inc, Cardiofocus, Inc, Biosense-Webster, Inc, and St Jude Medical, Inc. Dr. Kim is an employee of St Jude Medical, Inc. Address reprint requests and correspondence: Dr. Vivek Y. Reddy, Cardiac Arrhythmia Service, Massachusetts General Hospital, 55 Fruit Street, GRB-109, Boston, Massachusetts 02114.E-mail address: [email protected]. (Received May 4, 2007; accepted November 1, 2007.) NavX mapping) were generated at baseline and after electrical PV isolation as confirmed by use of a circular mapping catheter. RESULTS Electrical isolation was achieved in 100% of the PVs. Electroanatomical mapping revealed that after ablation with any of the 3 balloon catheters, the extent of isolation included the tubular portions of each PV to the level of the PV ostia. However, the PV antral portions were left largely unablated with all 3 balloon technologies. CONCLUSION Using the current generation of balloon ablation catheters, electrical isolation occurs at the level of the PV ostia, but the antral regions are largely unablated. KEYWORDS Catheter ablation; Balloon catheter; Cryoablation; Laser; Focused ultrasound; Electroanatomical mapping; Atrial fibrillation (Heart Rhythm 2008;5:353–360) © 2008 Heart Rhythm Society. All rights reserved. portions of the vein, so PV triggers of AF located at this region would not be included in the ablation lesion.10 Also, from a safety perspective, the intravenous location of the energy delivery resulted in PV stenosis. Since this first-generation device, balloon ablation catheters have evolved considerably.11 There are now 3 major balloon-based ablation devices at various stages of clinical evaluation: (1) cryoballoon ablation, (2) endoscopic laser ablation, and (3) high-intensity focused ultrasound (HIFU). Each of these has been fashioned to be placed at the PV ostia so as to theoretically isolate the veins outside their tubular portion. In this study, detailed electroanatomical mapping (EAM) was performed after balloon ablation using each of these 3 ablation strategies in patients with paroxysmal AF to assess the true anatomical location of electrical PV isolation. Methods All procedures were performed after written informed consent according to institutional guidelines at the Massachusetts General Hospital and Homolka Hospital. In a total of 50 patients with paroxysmal AF in whom at least 1 membrane-active antiarrhythmic drug had failed, we performed 1547-5271/$ -see front matter © 2008 Heart Rhythm Society. All rights reserved. doi:10.1016/j.hrthm.2007.11.006 354 Heart Rhythm, Vol 5, No 3, March 2008 Figure 1 Catheter cryoballoon ablation system. A: The balloon ablation catheter is shown inflated after having been advanced through a deflectable sheath (in black). The balloon catheter has a central lumen through which a guidewire can be advanced (as shown). B: Occlusion of the targeted PV ensures circumferential balloon–tissue contact, and consequently electrical PV isolation. By injecting contrast through the balloon catheter central lumen, the left superior PV is highlighted without evidence of periballoon contrast leak. C: In another example, ICE was also helpful to both identify the position of the balloon catheter as well as to assess for periballoon leak. In this image, the back face of the balloon catheter is seen occluding the left inferior PV—flow from the left superior PV is seen on color flow Doppler. ICE ⫽ intracardiac echocardiography; PV ⫽ pulmonary vein. catheter ablation using either a cryoablation, laser, or HIFU balloon ablation catheter. The cohort of patients discussed in this report represents the 14 patients within this group who underwent detailed LA-PV EAM both before and after ablation. Ablation procedures Procedures were performed either with conscious sedation or under general anesthesia. After standard femoral vascular access, dual transseptal punctures were performed with fluoroscopic and intracardiac ultrasound (Acunav, SiemensUltrasound, Mountain View, California) guidance. Intravenous heparin was instituted before the transseptal puncture. EAM of the LA-PVs was performed at baseline using either a magnetic EAM system (CARTO, Biosense-Webster, Inc, Diamond Bar, California) or an electrical impedance-based EAM system (NavX, St Jude Medical, Inc, Minnetonka, Minnesota). In selected patients, custom software was used to register and project the electrical information onto a patient-specific volumetric 3-dimensional image derived from preacquired computed tomographic (CT) or magnetic resonance (MR) imaging. Bipolar electrogram voltage amplitude data were displayed. After baseline mapping, electrical PV isolation of all PVs was performed using 1 of the 3 balloon ablation technologies as detailed below. Intracardiac echocardiography (ICE) was used to aid in balloon catheter positioning at the various PV ostia. Electrical PV isolation was established using a circular 10-pole or 20-pole multielectrode mapping catheter (Lasso, Biosense-Webster, Inc) to verify both entrance and exit conduction block. Cryoablation The cryoablation balloon system is a deflectable catheter with a balloon-within-a-balloon design wherein the cryo refrigerant (N2O) is delivered within the inner balloon (Figure 1). There is a constant vacuum applied between the inner and outer balloon to ensure the absence of refrigerant leakage into the systemic circulation in the event of a breach in the integrity of the inner balloon. The cryoballoon catheter used was 23 mm in diameter. The deflated balloon catheter is deployed through a 12F deflectable sheath. Once within the LA, the inflated balloon is positioned at the PV ostium (with ICE guidance) to temporarily occlude blood flow from the targeted PV. Each balloon-based cryoablation lesion lasts 4 minutes. Laser ablation The laser ablation catheter system incorporates an endoscopic visualization capability using a 2F endoscope positioned at a proximal location in the balloon (Figure 2). A deflectable sheath is also used to deliver this 12F balloon catheter. Once in the LA, the 20-, 25-, or 30-mm-diameter balloon is inflated and positioned at the PV ostia under ICE guidance. The endoscope allows the operator to visualize the internal face of the balloon and identify areas of balloon–tissue contact (blanched white) versus blood (red). An optical fiber that projects a 90° to 150° arc is advanced and rotated to the desired location for energy delivery. Once the proper location is identified, a diode laser is used to deliver laser energy at 980 nm (5.5 to 6.5 W/cm for 60 to 120 seconds/lesion). HIFU ablation The HIFU catheter is a 14F system that, once inflated, consists of a fluid-filled balloon in front of a smaller CO2 filled balloon (Figure 3). Energy from a radially directed ultrasound transducer reflects off this air–fluid interface to project forward and concentrate energy to deposit just beyond the face of the balloon. Contact with the atrial tissue is Reddy et al Balloon Isolation of Pulmonary Veins 355 Figure 2 Endoscopic laser balloon ablation system. A: The balloon ablation catheter is shown inflated after having been advanced through a deflectable sheath (in blue). An aiming beam is projected from an optical fiber as an arc that can be rotated and advanced/retracted. When the proper location is selected, the laser energy is transmitted via this same optical fiber. The mini-endoscope is located at the proximal end of the balloon catheter (near the white light) and is facing forward. B: ICE is helpful to identify the position of the balloon catheter relative to the vein; in this image, the balloon is at the ostium of the left superior PV, as well as straddling the ostium of the left inferior PV. C, D: Two examples of the images seen through the endoscope. Red represents blood, and white represents the blanched balloon–tissue contact. The green arc of the aiming beam is manipulated to select the locations to deliver the laser energy. The endoscopic field of view is partially obstructed (as outlined by the dotted lines) by the central lumen of the balloon catheter. Abbreviations as in Figure 1. not necessary for ablation with this catheter. This deflectable catheter is delivered using a nondeflectable 14F sheath. ICE was used to verify proper positioning of the catheter. Lesions were delivered using either a 20- or 25-mm-diameter balloon catheter for 40 to 60 seconds per lesion. Results Of the 50 patients who underwent balloon catheter ablation, preablation and postablation EAM was performed on 8, 4, and 2 patients with the cryoablation, laser, and HIFU balloon catheters, respectively. The average LA size was 43.6 ⫾ 3.9 mm for the complete patient cohort and 41.5, 46.8, and 45.5 mm for the patients treated with the cryoballoon, laser balloon, and HIFU balloon catheters, respectively. The majority of the patient cohort (9 of 14, 64%) had 4 relatively distinct PVs: 4 and 2 patients had either a discrete left common PV or right middle PVs, respectively. The individual details for these patients are shown in Table 1. Respective examples of use of each of the balloon ablation catheters are shown in Figures 1 to 3. Electrical isolation of the PVs was achieved in 54 of 54 veins, as verified by using a circular mapping catheter placed just inside (that is, within the first 2 to 3 mm) of the respective PVs. To determine the extent of this electrical isolation, electroanatomical bipolar voltage amplitude substrate mapping of the LA-PVs was performed at baseline and postablation (Figures 4 to 6). Regardless of the balloon ablation energy source, the extent of isolation included the tubular portions of each PV. For a quantitative analysis, the bipolar voltage amplitudes of the electroanatomical points acquired from each pair of ipsilateral veins was calculated. The preablation and postablation amplitudes of the left PVs were 0.5 ⫾ 0.8 mV (number of electroanatomical points measured per patient ⫽ 56 ⫾ 20) and 0.1 ⫾ 0.2 mV (number of points ⫽ 61 ⫾ 34), respectively. For the right PVs, the preablation and postablation amplitudes were 0.8 ⫾ 0.9 mV (number of 356 Heart Rhythm, Vol 5, No 3, March 2008 Figure 3 High-intensity focused ultrasound balloon ablation system. A: Shown in this schematic of the HIFU catheter is the reflective interface created by the anterior fluid-filled balloon (in blue) and the posterior CO2 gas-filled balloon. The radially directed ultrasound energy is reflected forward to create a circumferential zone of concentrated ablative energy just beyond the fact of the balloon. B: An ICE catheter is placed within the coronary to visualize the HIFU catheter positioned at the ostium of the left inferior PV. As shown, the balloon catheter does not need to be in contact with the LA-PV tissue for effective ablation. HIFU ⫽ high-intensity focused ultrasound; LA ⫽ left atrium; other abbreviations as in Figure 1. electroanatomical points measured per patient ⫽ 60 ⫾ 40) and 0.1 ⫾ 0.1 mV (number of points ⫽ 46 ⫾ 20), respectively. But as shown in Figures 4 to 6, the antral portions of the PVs were not ablated with the balloon ablation catheters. There were no complications in the patients studied in this report. During a mean follow-up of 461 ⫾ 109 days (range 309 to 609), 4 of 14 patients had clinical recurrences of atrial fibrillation (Table 2). This included 2 patients who had undergone cryoballoon ablation and 2 patients who had undergone laser balloon ablation. Because of the frequency of clinical symptoms, 2 of these patients (the 2 cryoballoon ablation patients) underwent repeat catheter ablation. In both of these patients, the repeat procedure revealed resumption of electrical conduction into the PVs. Focal ablaTable 1 tion using standard radiofrequency ablation isolated the PVs in both of these patients, and there was no inducible AF with rapid atrial pacing or during the infusion of Isuprel (up to 20 g/min). Discussion The key findings of this study are: (1) the 3 balloon ablation catheter designs are all capable of electrically isolating the PVs outside the tubular portions of the PVs at the level of the PV ostia, and (2) the PV antra are left largely unaffected by this ablation stratagem. The importance of PV isolation during catheters ablation of paroxysmal AF has been established as a result of several key clinical observations.1– 8 First was the initial description that the PVs harbor foci that initiate AF, and that in indi- Individual patient information PV sizes (mm) Patient no. Ablation energy source Balloon diameter(s) (mm) LA size (mm) Mapping system 1 2 3 4 5 6 7 8 9 10 11 12 13 14 Cryo Cryo Cryo Cryo Cryo Cryo HIFU HIFU Cryo Laser Laser Cryo Laser Laser 23 23 23 23 23 23 20 20, 23 20, 25, 23 25, 20, 41 43 39 48 37 37 43 48 43 46 47 44 47 47 EiEAM MEAM MEAM EiEAM EiEAM EiEAM EiEAM EiEAM MEAM EiEAM EiEAM MEAM EiEAM EiEAM 25 25 30 30 25 LSPV LIPV 21 19 LCPV 26 15 21 19 18 20 27 14 18 14 18 15 19 20 17 19 19 17 15 18 14 22 RSPV RIPV 22 26 16 20 18 13 23 25 16 18 20 21 21 21 15 19 21 23 12 15 17 21 19 18 19 16 20 19 RMPV 6 9 Cryo ⫽ cryoablation; EiEAM ⫽ electrical impedance-based electroanatomical mapping; HIFU ⫽ high-intensity focused ultrasound; LA ⫽ left atrium; LCPV ⫽ left common pulmonary vein; LIPV ⫽ left inferior pulmonary vein; LSPV ⫽ left superior pulmonary vein; MEAM ⫽ magnetic electroanatomical mapping; PV ⫽ pulmonary vein; RIPV ⫽ right inferior pulmonary vein; RMPV ⫽ right middle pulmonary vein; RSPV ⫽ right superior pulmonary vein. Reddy et al Balloon Isolation of Pulmonary Veins 357 Figure 4 Level of electrical isolation using the cryoballoon ablation catheter. Shown are baseline and postablation bipolar voltage amplitude maps of the LA-PVs. After registering the magnetic electroanatomical mapping data with the patient’s 3-dimensional magnetic resonance image, the voltage amplitude electrogram information was projected onto the 3-dimensional image. In the color range shown, red represents low amplitude (ⱕ0.1 mV) and purple high amplitude (ⱖ1 mV). Abbreviations as in Figure 3. viduals with paroxysmal AF ablation of these foci could eliminate AF. However, direct targeting of these foci fell out of favor for 2 reasons: (1) it was difficult and time consuming to evoke these PV triggers during any given procedure, so it was common to see clinical recurrences from a different focus either within the same PV or from another PV, and (2) excessive ablation within the veins caused PV stenosis. This initial approach was followed by a strategy of routine electrical isolation of all PVs in any given patient. Although initially performed within the tubular portions of the PVs in a segmental fashion using a circular mapping catheter to guide the procedure, this was again followed by clinical recurrences from foci just proximal to the ablation line (as well as PV stenosis). Accordingly, the procedure has now evolved to an extraostial ablation strategy involving placement of the lesions outside the PVs, a procedure that is somewhat facilitated by the use of EAM systems. Although this current approach to ablation of paroxysmal AF has a good efficacy and acceptable safety profile, it remains a technically difficult procedure requiring skilled operators. This has prompted the intense development of catheter systems to rapidly and safely isolate the PVs. But this has not proven to be an easily tractable problem, in large part because of the complexity of the PV anatomy. The variability in both PV shape and anatomy is well established.12–14 Instead of round PVs that join the LA chamber in a perfectly orthogonal manner, the PVs have an oval configuration, often combine with the ipsilateral vein before joining the LA proper, and typically have an oblique angle with which they join the LA. In addition, the junction of the PVs with the LA is not distinct and often includes an antrum that may include a large portion of the posterior LA.14 In fact, some investigators contend that the complete posterior LA must be ablated or otherwise electrically excluded to achieve the best clinical outcome.15 Three balloon catheter technologies using different ablation energy sources have evolved to negotiate this anatomical complexity. The cryoablation balloon catheter is advanced to each PV ostium, and forward pressure is applied to completely occlude blood flow. Because the cyrorefrigerant is delivered to the whole face of the balloon, any tissue in contact with the balloon is ablated. This can be safely performed because experimental and clinical results have shown that cryothermal ablation is associated with minimal risk of PV stenosis.16,17 On the other hand, the diode laser balloon catheter uses a strategy involving an endoscope to allow the operator to visualize balloon–tissue contact, and an adjustable lasing element to tailor the lesion to the appropriate location.18 By varying the location of this adjustable aiming beam, a series of arcs of laser energy are applied to the tissue at only the desired locations. This provides a greater flexibility to both the location of the 358 Heart Rhythm, Vol 5, No 3, March 2008 Figure 5 Level of electrical isolation using the laser and HIFU balloon ablation catheters. A: Using the electrical impedance-based electroanatomical mapping system, the LA-PV anatomy was constructed and the projected bipolar voltage amplitude maps are shown after ablation using the laser balloon catheter (left, anterior view; right, posterior view). B: Similarly, after ablation using the HIFU catheter, posterior views of the baseline and postablation voltage maps are shown. Abbreviations as in Figure 3. energy deposition and the total amount of energy applied to each site; for example, a greater amount/duration of energy could be applied anteriorly along the ridge between the left-sided PVs and LA appendage than that applied along the posterior wall near the course of the esophagus. Alternatively, because the HIFU balloon ablation catheter is designed to concentrate the energy beyond the face of the balloon surface, contact with the tissue is not required for ablation. Ablation with this technology can be performed in a piecemeal fashion with the HIFU balloon catheter delivering a series of sequential lesions as it is precessed about the long axis of the PV.19 –21 This is feasible because HIFU energy is associated with minimal thromboembolic risk even when sonicating directly into blood. The results from the present study show the actual location of the ablation lesion set when using these 3 balloon technologies. As shown, all PVs can be isolated at the level of the PV ostia and, importantly, outside their tubular portions. However, it must also be noted that in large part, the PV antra are not ablated. The clinical impact of not addressing this tissue in the lesion set is unknown. Despite the lack of effect on the antra, the preliminary clinical experience with these balloon ablation catheters in patients with paroxysmal AF has revealed an approximately 70% arrhythmia-free success rate at 1 year, a result similar to that seen with radiofrequency ablation.17,18,21 Despite the relatively small number of patients in this series, it is interesting to note the results of the patients re-studied for clinical recur- rences. The cause of the recurrences was not PV antral or other extrapulmonary triggers, but rather a resumption of electrical continuity with the PVs. This again speaks to the importance of the adequacy of the level of PV isolation.22 Indeed, as shown in Figure 7, the level of isolation seen during point-to-point radiofrequency ablation is similar to that seen with the balloon ablation catheters. Thus, for patients with paroxysmal AF, it remains an open question whether ablation beyond the level of the PV ostium is really necessary. It should be noted that for each of these balloon systems, there is the potential for modifying these devices to allow for a more extensive LA ablation zone. The most intuitive initial step is to simply increase the diameter of the ablative balloon element. However, the preliminary clinical experience with this approach has been disappointing in large part because the atrial tissue is less distensible than initially expected. When larger cryoballoons or laser balloons were used, circumferential contact with the tissue, a known requirement for efficacy with these balloon systems, could not be achieved. Because of the poor compliance of the atrial chamber, it seems that a better alternative will be to make the balloons more compliant to the tissue, a concept currently being explored in second-generation systems. The HIFU system, on the other hand, does not need tissue contact to be effective. But to easily use this technology to ablate the PV antra, it will be necessary to improve the navigability of this catheter. For example, by incorporating Reddy et al Balloon Isolation of Pulmonary Veins 359 Figure 6 Level of electrical isolation after standard radiofrequency catheter ablation. In a patient with paroxysmal AF, electrical PV isolation was performed using a 3.5-mm irrigated-tip radiofrequency ablation catheter under electrical impedance-based electroanatomical mapping guidance to place an extraostial ablation lesion set. Shown are the baseline (A) and postablation (B) voltage amplitude maps of the LA-PVs. Abbreviations as in Figure 3. an EAM capability (whether magnetic-based or electrical impedance-based) into the catheter, it may be possible to stitch together a series of ablation lesions incorporating the PV antra as the balloon is widely precessed about the orifice of each vein. Unlike patients with paroxysmal AF, there is considerable evidence that catheter ablation of persistent/permanent AF may require ablation beyond electrical isolation of the PVs. Particularly for those patients with permanent AF, it seems necessary to perform a staged ablation strategy involving linear ablation, ablation of sites of complex fractionated electrograms, and ablation within the coronary sinus and right atrium.23 It is less likely that the balloon ablation paradigm of electrical PV isolation alone would be adequate for these patients. Further clinical work is necessary to investigate these hypotheses. Limitations Because of the complexity of the LA-PV anatomy, it is difficult to quantify the level of PV isolation beyond that described in this report. However, this does not detract from the main conclusion of this investigation, namely that balloon ablation incorporates electrical isolation of the PV ostia but not antra. Table 2 Patient follow-up Patient Duration of AADs Clinical Repeat no. follow-up (days) discontinued? recurrence? procedure? 1 2 3 4 5 6 7 8 9 10 11 12 13 14 609 595 593 574 552 529 408 390 394 394 396 395 310 309 Yes No Yes Yes No Yes Yes Yes Yes No Yes No Yes No AADs ⫽ antiarrhythmic drugs. No Yes No No No Yes No No No No No Yes No Yes Yes Yes No No 360 Implicit in this study is the assumption that catheter ablation using these balloon catheters is technically easier to perform than point-to-point using a standard spot ablation catheter. However, this assertion must be proven in a comparative study. This report does not address the ability to make permanent isolating lesion sets. It has been shown that in paroxysmal AF patients with post–radiofrequency ablation clinical recurrences, PV reconnection is a critical factor. As shown by the patients with clinical recurrences, the predictors of achieving permanent PV isolating lesions with the balloon-based ablation catheters remain to be identified in future evaluations. Conclusion When treating patients with paroxysmal atrial fibrillation, balloon ablation catheters are able to isolate the PVs outside the level of the tubular vein. However, the current generation of balloon ablation catheters leaves the veins’ proximal antral regions unablated. References 1. Haissaguerre M, Jais P, Shah DC, et al. Electrophysiological end point for catheter ablation of atrial fibrillation initiated from multiple pulmonary venous foci. Circulation 2000;101:1409 –1417. 2. Jais P, Weerasooriya R, Shah DC, et al. Ablation therapy for atrial fibrillation (AF): Past, present and future. Cardiovasc Res 2002;54:337–346. 3. Chen S-A, Hsieh M-H, Tai C-T, et al. Initiation of atrial fibrillation by ectopic beats originating from the pulmonary veins: electrophysiological characteristics, pharmacological responses, and effects of radiofrequency ablation. Circulation 1999;100:1879 –1886. 4. Marrouche NF, Dresing T, Cole C, et al. Circular mapping and ablation of the pulmonary vein for treatment of atrial fibrillation: Impact of different catheter technologies. J Am Coll Cardiol 2002;40:464 – 474. 5. Oral H, Knight BP, Tada H, et al. Pulmonary vein isolation for paroxysmal and persistent atrial fibrillation. Circulation 2002;105:1077–1081. 6. Gerstenfeld EP, Guerra P, Sparks PB, et al. Clinical outcome after radiofrequency catheter ablation of focal atrial fibrillation triggers. J Cardiovasc Electrophysiol 2001;12:900 –908. 7. Pappone C, Rosanio S, Augello G, et al. Mortality, morbidity, and quality of life after circumferential pulmonary vein ablation for atrial fibrillation. J Am Coll Cardiol 2003;42:185–197. Heart Rhythm, Vol 5, No 3, March 2008 8. Ouyang F, Bansch D, Ernst S, et al. Complete isolation of left atrium surrounding the pulmonary veins: New insights from the double-lasso technique in paroxysmal atrial fibrillation. Circulation 2004;110:2090 –2096. 9. Natale A, Pisano E, Shewchik J, et al. First human experience with pulmonary vein isolation using a through-the-balloon circumferential ultrasound ablation system for recurrent atrial fibrillation. Circulation 2000;102:1879 – 1882. 10. Saliba W, Wilber D, Packer D, et al. Circumferential ultrasound ablation for pulmonary vein isolation: Analysis of acute and chronic failures. J Cardiovasc Electrophysiol 2002;13:957–961. 11. Keane D. New catheter ablation techniques for the treatment of cardiac arrhythmias. Card Electrophysiol Rev 2002;6:341–348. 12. Wittkampf FH, Vonken E, Derksen R, et al. Pulmonary vein ostium geometry analysis by magnetic resonance angiography. Circulation 2003;107:21–23. 13. Kato R, Lickfett L, Meininger G, et al. Pulmonary vein anatomy in patients undergoing catheter ablation of atrial fibrillation: Lessons learned by use of magnetic resonance imaging. Circulation 2003;107:2004 –2010. 14. Ahmed J, Sohal S, Malchano ZJ, et al. Three-dimensional analysis of pulmonary venous ostial and antral anatomy: Implications for balloon catheter-based pulmonary vein isolation. J Cardiovasc Electrophysiol 2006;17:251–255. 15. Kanj MH, Wazni OM, Natale A. How to do circular mapping catheter-guided pulmonary vein antrum isolation: The Cleveland Clinic approach. Heart Rhythm 2006;3:866 – 869. 16. Sarabanda AV, Bunch TJ, Johnson SB, et al. Efficacy and safety of circumferential pulmonary vein isolation using a novel cryothermal balloon ablation system. J Am Coll Cardiol 2005;46:1902–1912. 17. Reddy VY, Neuzil P, Pitschner HF, et al. Clinical experience with a balloon cryoablation catheter for pulmonary vein isolation in patients with atrial fibrillation: One-year results. Circulation 2005;112:II491– 492. 18. Reddy VY, Neuzil P, Themisotoclakis S, et al. Long-term single-procedure clinical results with an endoscopic balloon ablation catheter for pulmonary vein isolation in patients with atrial fibrillation. Circulation 2006;114:II-747. 19. Wong T, Markides V, Peters NS, et al. Anatomical left atrial circumferential ablation to electrically isolate pulmonary veins using a novel focused ultrasound balloon catheter. Heart Rhythm 2006;3:370 –371. 20. Antz M, Chun KRJ, Ouyang F, et al. Ablation of atrial fibrillation in humans using a balloon-based ablation system: Identification of the site of phrenic nerve damage using pacing maneuvers and CARTO. J Cardiovasc Electrophysiol 2006;17:1242–1245. 21. Schmidt B, Antz M, Ernst S, et al. High intensity focused ultrasound for pulmonary vein ostium isolation– 6 months follow-up data. Circulation 2005; 112:II– 491. 22. Verma A, Kilicaslan F, Pisano E, et al. Response of atrial fibrillation to pulmonary vein antrum isolation is directly related to resumption and delay of pulmonary vein conduction. Circulation 2005;112:627– 635. 23. Haissaguerre M, Sanders P, Hocini M, et al. Catheter ablation of long-lasting persistent atrial fibrillation: Critical structures for termination. J Cardiovasc Electrophysiol 2005;16:1125–1137.






© Copyright 2026