
Tools for Identifying Emotional Intelligence
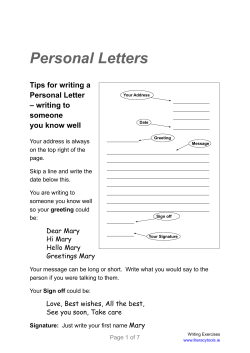
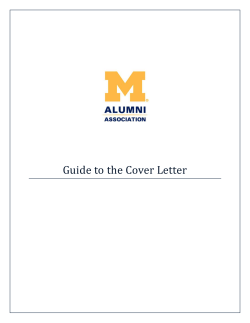
2012 Minnesota Alliance for Patient Safety Conference Breakout Session #3 Tools for Identifying Emotional Intelligence Thursday, Oct. 25, 2012 11:10 a.m. – 12:10 p.m. Presenter: Timothy B. McDonald, M.D. Session Objectives: 1. Understand the methodology for addressing communication styles. 2. List differences in communication styles. 3. Appreciate the importance of emotional intelligence in communicating patient harm events. Timothy McDonald, M.D., J.D. Timothy McDonald, M.D., J.D., is a physician-attorney who has been involved in quality and patient safety efforts at the University of Illinois Medical Center for the past decade. Until his recent promotion to assistant vice president for quality and safety for the entire University of Illinois, he served as the chief safety and risk officer for health affairs and the program director for the pediatric anesthesiology residency program. His focus has been on the principled approach to quality, medical liability and patient harm with an emphasis on the robust reporting of patient safety events, near misses and unsafe conditions. He has helped pioneer the medical center’s learner reporting process as a means of engaging learners from all professions and all specialties in safety and quality education. The principled approach to patient harm also includes a commitment to communicate within the health care team and with patients and families throughout the therapeutic relationship. It also involves a promise to investigate and by working with quality management create systems improvement following the detailed analysis of harm or near miss events or other gaps in quality metrics. His federally funded research has focused on all of these domains and their impact on improving the quality of care while mitigating medical liability issues, including the establishment of teaching methodologies for all levels and professions in health care. Tools for Assessing Communication Competence and Emotional Intelligence Timothy B McDonald, MD JD Professor, Anesthesiology and Pediatrics Chief Safety and Risk Officer for Health Affairs University of Illinois College of Medicine at Chicago University of Illinois Hospital and Health Science System Overview • Importance of Communication • Individual Differences in Communication Competence • Cognitive Complexity – Impressions of Liked and Disliked Others • Message Design Logic – Responses to Hypothetical Scenarios • Discussion/Q&A 2 Importance of Communication Conveying information Providing emotional support Coordinating and regulating behavior Minimizing malpractice risk Managing our own identities and those of others • Defining and redefining contexts, roles, identities, meanings, relationships • • • • • 3 Some more background Institute of Medicine: 1999 report that shook the medical world Some more background: the negative power of poor communication after harm occurs Institute of Medicine: 1999 report that shook the medical world Making Matters Worse More issues related to communication Part of the issue • February 2012, Volume 31, Issue 2 • Impact on the medical malpractice community Adding to the equation • Journal of Trauma, September, 2010 • 8% of physicians generate 34-40% of unsolicited patient complaints • Same 8 % generate 50% of risk management expenses • Physicians in bottom q-tile of patient satisfaction have 110% malpractice risk More value to communication • July 2011, Volume 30, Issue 7 • 50-60 of claims dropped once information shared 12 Creating a communication consult service Communications assessment tool Measures emotional intelligence Assesses cognitive complexity Identifies highly skilled communicators in complex social situations • Balances out the “special colleague” issue • • • • Individual Differences in Communication Competence • Some people are more skillful communicators than others. • Some communication tasks/situations are much more difficult than others – Easy: describe your apartment – Hard: disclose a medical error to a grieving family • Differences in skill most visible in hard situations 14 Disclosure Requires High Level of Skill • Disclosure situations are hard – Multiple, conflicting goals – High level of emotional arousal – High ego-involvement – Highly consequential • Critical to identify organization’s best communicators for Patient Communication Consult Service • Communication skill predicts malpractice risk 15 Our Approach to Assessment • The tasks you completed allowed us to make a preliminary assessment of your communication competence • We will explain how we analyzed your performance and how you performed • Measures we used have a long history • So first, a quick course in communication theory! 16 Constructivism: A general theory of communication competence • Represent the social world in terms of bipolar dimensions known as “constructs” • Cognitive complexity refers to the degree of differentiation, integration and abstractness of one’s interpersonal constructs • Cognitive complexity is correlated with communication skill/competence – More constructs => higher level of competence 17 Personal Constructs • Construct is a bipolar dimension for representing the social world – kind/cruel, fair/unfair, happy/unhappy, considerate/inconsiderate, genuine/fake • Quality of social perception increases as constructs increase in number, level of abstractness, and level of integration • Social skill increases similarly 18 Analogy #1: Image Resolution http://en.wikipedia.org/wiki/Image_resolution 19 Analogy #2: Color Depth 1 bit (2 colors) 8 bit (256 colors) 2 bit (4 colors) http://en.wikipedia.org/wiki/Color_depth 4 bit (16 colors) 16 bit (16,777,216 colors) 20 Analogy #3: Dimensionality of Data Increasing the number, level of abstractness, and level of dimensionality in scientific data has many benefits. 21 Benefits of Increasing Dimensionality • • • • • • More acute perception Greater insight Improved predictions Greater strategic understanding Greater success in achieving goals More effective action 22 Interpersonal Cognitive Complexity The number, level of abstractness, degree of integration of one’s dimensions for representing the social world 23 Benefits of Interpersonal Cognitive Complexity • Same benefits as increased dimensional data, plus: – More organized and integrated impressions of others – Greater ability to: • recognize others feelings and dispositions; integrate inconsistent information about others; understand others thoughts, feelings and motivations; produce effective messages, accurately and completely interpret others messages, structure conversational interactions (Burleson & Waltman, 1988) 24 Benefits (cont’d.) • More differentiated, abstract and organized system of constructs enables greater skill at: – Social perception – Impression organization – Information integration – Social evaluation – Social perspective taking – Message production 25 Measuring Interpersonal Cognitive Complexity • The Role Category Questionnaire (Crockett, 1965) • Thought to elicit a representative sample of respondent’s interpersonal constructs • Describe one liked and one disliked other – In as much detail as possible in 5 minutes each – Focus on habits, beliefs, mannerisms, not physical appearance • Impressions can be scored for: – Number of constructs (“differentiation”)** – Abstractness of constructs – Level of integration of constructs 26 Caveats • Only measuring interpersonal cognitive complexity (not measuring perception in other realms) • It is an imperfect measure • Not measuring you IQ or value as a human being! • Interpersonal cognitive complexity continues to develop over the entire lifespan. 27 Frequency Distribution of Number of Constructs (i.e. Cognitive Complexity) 25 23 Frequency 20 15 10 4 standard deviations above the mean! 8 7 4 5 2 0 10 20 30 40 50 0 0 0 60 70 80 1 90 0 0 100 More Number of Constructs 28 Frequency of Construct Distribution MHA Volunteers Constructs 3.5 3 2.5 2 Constructs 1.5 1 0.5 0 10 thru 20 20-30 30-40 40 and > 29 Comparison of Construct Frequency 25 20 15 Co Min 10 5 0 10 thru 19 20 thru 29 30 thru 39 40 thru 49 50 thru 59 60 thru 69 70 thru 79 80 thru 89 90 thru 99 30 Highly Complex Impression (liked other) • intelligent, intellectual, relaxed, down-to-earth, approachable, genuine, humble, caring, kind, thoughtful, loving, free spirited, respectful, hilarious, insightful, discerning, intuitive, composed, deferent, patient, deep, pensive, considerate, multifaceted, complex, worldly, ambitious, dedicated, shy, inspirational, friendly, reliant, trustworthy, talented, infectious, comforting, faithful, motivational, introspective, pondering, committed, loyal, fun, bohemian, adventuresome, generous, articulate (47 constructs) 31 Moderately Complex Impression (liked other) very positive, easy to get along with, has great organizational skills, has a great sense of humor and can make people laugh, is very polite to others, has good manners, is a caring person, is very giving, enjoys life, is very creative, is a good writer, follow through with was she sets out to do, is never late, likes good food and good wine, will give you the shirt off her back, knows how to love, loves animals, is not self centered, most always looks on the bright side, willing to be of service to others, is very generous and laughs a lot. (23 constructs) 32 Average Complexity Impression Funny, well read, thoughtful of others, a good selector of gifts of gifts for others, a very attentive father and grandfather, committed, very goal directed, personally able to sustain an effort in his work - self-motivated, a bit opinionated, has some hold over of self worth issues from his childhood which cause him to take things personally that he shouldn't, tends to project some of those type feelings to others. (13 constructs) 33 Low Complexity Impressions • Genuine and sincere, taking people at face value and giving them the benefit of the doubt until they prove otherwise. Strong work ethic and team oriented. (6) • Accepts blame, Acknowledges others achievements, Level headed, trustworthy (4) • Good Listener (1) (liked other) • Narcissistic moron (2) (disliked other) 34 Construct Abstractness • In increasing order of abstractness (Burleson & Waltman, 1988): – Physical descriptions – Role descriptions, e.g., name, age, gender – Descriptions of general behaviors or specific actions – Reports of specific or general beliefs and attitudes – Abstract dispositional and personality characteristics 35 Abstract & Concrete Constructs • Abstract – Open to new ideas, spiritual, contemplative, moral, bohemian, multifaceted, infectious, discerning, territorial, linear thinker, patriarchal • Concrete – Average build, dark brown hair, middle aged, tall, always on time, well groomed, nice, mean, hardworking 36 Highly Integrated Constructs • Focused on outcomes, but considers the means to the end equally important; not afraid to move forward, but does so in a well-informed manner; ready, aim, fire at a quick but calculated pace; earlier in career was ready, fire, aim. • He doesn't see the world as black or white but listens to everyone to see and understand their views. Even when he disagrees he is respectful and has a complete understanding of the other person's view point…He doesn't agree with me to just agree, he stands he ground but does it with grace and ease. 37 Development of Constructs over the Lifespan • From concrete to abstract • From few to many • From isolated to integrated • Life-long opportunity for learning, growth, development 38 Person-Centered Messages “…those which reflect awareness of and adaptation to the subjective, affective, and relational aspects of communicative contexts” (Burleson & Waltman, 1988, p. 15) 39 Cognitive Complexity and PersonCentered Communication • As cognitive complexity increases, people produce increasingly personcentered messages • As person-centeredness of message increases, others tend to perceive the message as more effective, comforting, persuasive, etc. 40 The Logic of Message Design • People differ in the way they reason from goals to messages • Developmental progression in basic concepts of language and communication – Expressive: language a medium for expressing thoughts/emotions – Conventional: Communication is a game played by social rules – Rhetorical: Communication is the creation and negotiation of social selves and situations 41 Expressive Design Logic • Premise: language is for expressing thoughts/emotions • Evaluative dimensions: Clarity of expression; openness; honesty; unimpeded signaling • Key message function: self-expression • Time orientation: reaction to prior event • Little attention to context • Subjective and associative; incoherent • Pragmatically pointless content • Message adaptation by editing only 42 Conventional Design Logic • Premise: Game played by social rules • Evaluative dimensions: Appropriateness; control of resources; cooperativeness • Message function: Secure desired response • Temporal organization: Present • Action and meaning context determined • Intersubjective and rule-focused coherence • Focus on rights and obligations • Saves face using politeness 43 Rhetorical Design Logic • Premise: creation of social selves/situations • Evaluative dimensions: flexibility; symbolic sophistication; depth of interpretation • Message function: Negotiate social consensus • Temporal organization: Movement toward desired context • Communication creates context • Explicit context-defining clauses and phrases • Focus on rights and obligations • Saves face by redefining context 44 Development of Competence • Increasing cognitive complexity • Increasing mastery of higher-level message design logic • Rhetorical messages and message producers tend to be evaluated more favorably than conventionals, who in turn are evaluated more favorably then expressives 45 30 Num. Constructs by Group Project MDL 29 18.0769 13.25 0 Mean Number of Constructs 10 20 One-way ANOVA, F(2, 41)= 4.25, p = 0.02 1 2 3 46 Num. Constructs by Disclosure MDL One-way ANOVA, F(2, 41)= 5.19, p = 0.01 19.5161 9.75 0 Mean Number of Constructs 10 20 30 31.6667 1 2 3 47 Goals of Disclosure Task? • Depends on timing! • Task goals? • Interpersonal/Relationship goals? 48 Error Disclosure Elements • Apology • Nature of error, harm • When, where error occurred • Causes and results of harm • Actions taken to reduce further injury • Actions to prevent recurrence • Describe error review process • Who will manage ongoing care • How system issues are identified • Ongoing communicator/patient advocate • Names and contact info • Offer counseling/support • Consider costs, patient’s bill Patient Communication Consult Service flyer, UIC Dept. of Safety and Risk Management 49 Four R’s of Apology • • • • Recognition Regret Responsibility Remedy Woods, M. S. (2004). Healing Words. 50 Communicating with Patients: Generic Do’s Introduce yourself by name and role Find a private/appropriate place to talk Sit down Frame the bad news with preliminary remarks Proper nonverbal behavior (posture, gesture, facial expression, volume, rate, distance) • LISTEN (silence is not bad) • Use plain language (no jargon) • • • • • 51 Do’s for Initial Disclosure • Do – Provide emotional support and reassurance • Acknowledge & name emotional states • Express empathy and regret about bad outcome (apologize) – Only provide solid facts – Express uncertainty as appropriate about event, cause, prognosis – Offer assurances of follow-up and reassure they will not be abandoned • We will investigate • We will be in constant communication • Provide contact information – Ask them questions about their current understanding – Provide opportunity for them to ask questions 52 Don’ts • Speculate or jump to conclusions or make unwarranted inferences (about cause or outcome) • Offer unsupported opinions • Prematurely admit fault or accept blame • Make promises you can’t keep • Finger-point • Digress into medical jargon 53 Example Bill and Beth? (As I sit down I say) My name is xxxx, I am a xxxxx here at MCR. I understand you are here with your daughter Mary while she has her GI procedure, correct? (Leaning towards them, calm, steady and caring/concerned eye contact) I realize you both have been sitting out here in the lobby while the Code Blue was announced overhead and you may have seen members of our healthcare team go into Mary's room. Please know that I can appreciate how you seeing that may have been quite alarming, and I want to candidly share the information that I have at this moment regarding what transpired. (As I put my hand on theirs keeping my body language and eye contact calm) First and foremost, please know that she is resting comfortably in the recovery suite at this time, and the nurse will come out in a moment to take you back to her. As you may be aware Mary was scheduled to receive moderate sedation during her procedure, and we monitor her vital signs closely during these circumstances. When the team determined she was not breathing adequately towards the completion of the procedure they called the Code Blue. We are committed to keeping you and Mary informed about what we unearth as we investigate this situation further. The involved provider will be speaking to Mary and you in a moment, and once we know more about precisely what happened we want to coordinate a followup care conference with you, Mary and the involved provider and staff as appropriate so that we can afford us with the opportunity to provide further information and answer any outstanding questions you may have. Does this sound like an acceptable plan at this time? I also want to give you my business card so that we may keep in touch throughout our review process. I want you both to know you can call me at any time if you have any concerns or questions for me. I am here to support you and Mary. I want you to know that we genuinely are dedicated to delivery world class care, and if there are any improvement opportunities that merit our attention we absolutely want to identify them. Do you have any questions for me at this time? Otherwise, let me check with the nurse and get you both back to see your daughter. 54 Example Mr. and Mrs ...., I'm xxxx a xxxx. I'm so sorry to tell you that there were some complications during Mary's procedure so that she was not breathing as deeply as she should have been. We have been able to get her breathing, heart rate and blood pressure back to normal ranges, but do not know for sure right now what her outcome will be. I know this must be a terrible shock to you. I'll certainly try to answer all the questions you undoubtedly have, but there may be some questions that I won't have any answers for right now. Is there anyone we can call that you would like to have with you? 55 Example Mary is doing well and is resting comfortably. She had a bit of struggle toward the end of the procedure, however, she received the care necessary to keep everything on the right track. We will give her a few minutes to get settled and you can go in and see her. 56 Example I regret that Mary had a bad cardiopulmonary event, and she had to be resuscitated because she was not breathing and her heart rate decreased to a very low level. Mary is OK now. This problem may have had something to do with the sedation given to Mary for the procedure. 57 Example Hello, are you X? I am X. I would like to update you on the procedure. Toward the end of the procedure Mary breathing stopped and her heart rate was very low. Currently her vital signs are in the normal range. 58 Example Bill and Beth, I need to discuss the outcome of the procedure that we just completed. And I'm afraid that I need to deliver some bad news. During the procedure Mary stopped breathing at one point and her heart rate dropped down to 30 beats per minute, which is well below what it should have been. We had to perform CPR on your daughter and we did get her breathing, pulse and blood pressure back to normal. We've transferred your daughter to the ICU and will have to wait to see what impact this will have on her brain's functioning. Our team, and I'm guessing you as well, have a lot of questions about what may have occurred during the procedure that led to this occurring. We'll be looking at the monitoring during the procedure as well as the amount of sedation given and any other factors that may have contributed to this happening to your daughter. And I want you to be assured that as we find out all of the facts, we'll be letting you know exactly what happened. This would be hard news for anyone, and I can only imagine how hard it is for you to hear this. How are you feeling right now? What can I do fo you? What other questions do you have for me? 59 Example …I'm sorry that this happened. It was my responsibility to manage the sedation and I administered too much of the sedative medication. I don’t know the extent of the damage if any from the sedation but I want assure you that I will be involved in helping her recovery and the hospital will assist with any recovery, including medical care and expenses, if need be… 60 Example I have made a mistake in caring for your mother. She received too much sedation during the case.…I am sorry for everything that has just occurred. I know that it is going to be difficult to process now and as we move forward. However, I would like to get your input and have you be a part of the process for change in the future. It may be too early to talk about this now, but my hope is that we can create a plan for change to avoid this in the future. Patient and family input is very helpful. Please, when you are ready, let me know if you would like to be a part of this change. I am going to discuss the case with other members of the team including the nurses, other physicians, and staff. I will ask for their input and advice as well. We will discuss what went well, what did not, and what is needed for future situations such as these. Again, I am very sorry for my mistake. I want to prevent this in the future and hope that you will be a part of the process of making that happen. Here is my contact information if you would like to talk about this further or have other questions. 61 References O’Keefe, D. J., Shepherd, G.J., & Streeter, T. (1982). Role category questionnaire measures of cognitive complexity. Central States Speech Journal, 33, 333-338. Burleson, B. R., & Waltman, M. S. (1988). Cognitive complexity: Using the role category questionnaire. In C. H. Tardy (Ed.), A handbook for the study of human communication: Methods and instruments for observing, measuring and assessing communication processes. Westport, CT: Ablex. Burleson, B. R. (2006). Constructivism: A general theory of communication skill. In B. B. Whaley & W. Samter (Eds.), Explaining communication: Contemporary theories and exemplars. Mahwah, NJ:Erlbaum. Burleson, B. R. (2003). Emotional support skills. In J. O. Greene & B. R. Burleson (Eds.), Handbook of communication and social interaction skills (pp. 551–594). Mahwah, NJ: Erlbaum. Crockett, W. H. (1965). Cognitive complexity and impression formation. In B. A. Maher (Ed.), Progress in experimental personality research (Vol. 2, pp. 47–90). New York: Academic Press. Delia, J. G., O’Keefe, B. J., & O’Keefe, D. J. (1982). The constructivist approach to communication. In F. E. X. Dance (Ed.), Human communication theory: Comparative essays (pp. 147–191). New York: Harper & Row. O’Keefe, B. J. (1988). The logic of message design: Individual differences in reasoning about communication. Communication Monographs, 55, 80–103. Woods, M. S. (2004). Healing words: The power of apology in medicine. Oak Park, IL: Doctors in Touch. 62








© Copyright 2026