
ADM issi ON Assess
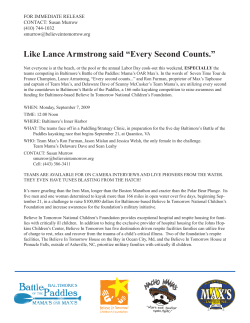
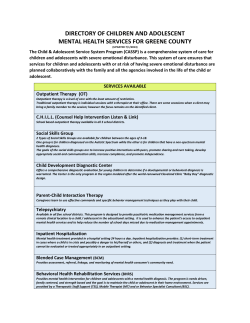
ADMISSION Assessment & Care Planning Dementia & Mental Capacity Information Day to Day Recording Sample Pack Daily Reporting & Communication Comprehensive Care Planning System Optional / Nursing Information Jo Turner (Manager) Chester Lodge Mandatory Assessments/Records Less admin more care... … a comprehensive care planning system, easy for staff to use … it promotes the opportunity to ensure that all care plans are individualised and person centred. During the last three inspections CQC were happy with every one of our care plans … the nurse assessors from the local PCT have commented about the high quality of our care plans and that all of the information they require is accurately recorded and easy to find. The documentation guide helps staff to understand the relevance of each form and how each can be used to evidence that the outcomes are being met … Respite Contents ADMISSION 21.076 Pressure Ulcer Assessment 19 21.049 Pre Assessment 4 21.078 Bedrail Assessment 20 21.026 Hospital Transfer Record 5 21.079 General Risk Assessment 21 21.050 Re-Assessment 5 21.080 General Risk Evaluation 21 21.051 Admission 5 Optional / Nursing Information Assessment & Care Planning 21.081 Pain Chart 22 21.052 Support Plan 6 21.082 Wound Chart 22 21.053 Care Plan 7 21.083 Depression Scale 23 21.054 Care Plan Evaluation 7 21.084 Medication Record 23 21.055 Activity Plan 8 21.089 Dependency Profile 24 21.056 Activity Plan Evaluation 8 21.085 Observations and Monitoring 25 21.057 Social Activity 8 21.086 Diabetic Chart 25 21.058 Social Activity Comments 8 21.088 Fluid Balance 25 21.087 Repositioning Chart 25 21.090 Deterioration Scale 26 Dementia & Mental Capacity Information 21.059 Personal History 9 21.060 Support Network 9 21.061 Mental Capacity Assessment 10 21.062 Deprivation of Liberty 10 21.063 Lasting Power of Attorney 11 21.064 Future Wishes 11 Day to Day Recording 21.065 Personal Care 12 21.066 Bowel Chart 12 21.098 Bristol Stool Chart 12 21.067 Food Chart 13 21.068 Weight Chart 13 21.069 Body Chart 14 21.070 Epilepsy Chart 14 21.071 Oral Assessment Tool 15 21.072 Record of Behaviour 15 Daily Reporting & Communication 21.091 Keyworker 27 21.092 Communication Sheet 27 21.093 Multidisciplinary Notes 27 21.094 Doctors Notes 28 21.095 Family Communication 28 21.096 District Nurse Notes 28 20.768 Daily Report 29 20.025 Daily Report - Single 29 20.019 Nursing Report 29 Respite 20.929 Respite Booklet 30-31 Mandatory Assessments/Records 21.075 Manual Handling 16 21.074 Falls Risk Assessment 17 21.073 MUST Tool 18 21.097 MUST Poster 18 21.077 Infection Risk Assessment 19 2Email: [email protected] Phone: 01604 646 633 ADMISSION Dementia & Mental Capacity Information Day to Day Recording Mandatory Assessments/Records Standex Systems have been providing care planning systems to the care sector for over 40 years. Part of an international group with over 18,000 satisfied clients which includes 2,500 in the UK alone. Standex in the UK specialise in providing care planning systems to care homes, nursing homes, hospices and hospitals. At Standex Systems Ltd we always strive to be ahead of your documentation needs. By keeping a close eye on the requirements of the Care Quality Commission, we are able to develop and update care planning systems in line with the regulations. As a company we provide a wide range of filing and storage solutions to compliment our care planning system to create a one stop shop for your care planning needs. Assessment & Care Planning Company Overview Optional / Nursing Information Daily Reporting & Communication Respite Other product ranges available: • Files & Storage • Waste & Laundry Fax: 01604 644 646 • Treatment Trolleys • Medication Trolleys Web: www.standexsystems.co.uk 3 ADMISSION Assessment & Care Planning Dementia & Mental Capacity Information Day to Day Recording Mandatory Assessments/Records Optional / Nursing Information Daily Reporting & Communication Respite 21.049 Pre Assessment • Demographics, medical history, medication, allergies, resus status. • Holistic Assessment (including a section about whether service user has mental capacity at time of assessment). • LPA details if applicable. • Infection status. • Reasons for acceptance/ non acceptance. • This form allows evidencing that the needs, wishes , preferences and decisions of the service user are placed at the centre of assessment, planning and delivery of care, treatment and support. Whilst promoting independence. In line with Outcome 1: Respecting and involving people who use services. • The very first form that is used before the service user has even entered the home. It evidences that safe and appropriate care is given because individual needs are established from when they are referred. It can be recorded that all aspects of their individual circumstances, and their immediate needs are recorded prior to admission (or non admission as the case may be). In line with Outcome 4: Consent to care and treatment 4Email: [email protected] Phone: 01604 646 633 ADMISSION Dementia & Mental Capacity Information Day to Day Recording • Hospital Transfer Record should be used if the service user is taken into hospital. • Provides ambulance crew and staff at the hospital with vital information regarding the service user’s health and support required. • The principal concern of the care home is to maintain the service user’s well-being, provide optimal care during the transfer period, and to deliver the service user safely to the receiving unit. • The care home can keep the top copy for their records, the 2nd and 3rd copies can be given to the hospital and ambulance crew for their records. • You may attach photocopied care plans and the latest daily report if you feel this will better inform nursing staff of support required. • In line with Outcome 6: Cooperating with other providers. Assessment & Care Planning 21.026 Hospital Transfer Record Mandatory Assessments/Records 21.050 Re-Assessment Optional / Nursing Information • A smaller version of Pre-Assessment to document any changes in service user’s condition on return to the home. • Can document whether the home can still cater for service user’s needs. Daily Reporting & Communication Respite 21.051 Admission • Service user details on admission. • Designed to go in front pocket of the file where it can be seen quickly and easily. • Quick ‘at a glance’ view of service user’s details. Fax: 01604 644 646 Web: www.standexsystems.co.uk 5 ADMISSION • Based on Roper, Logan and Tierney’s Activities of Daily Living with further categories for a more robust assessment. • Any problems trigger a care plan. • This can be done on a monthly basis or more frequently if needs change. Here we have the review section where the service user/advocate can sign to say they have been involved in the assessment. • The holistic assessment looks at Cognition, Psychological, Physical, Social and End of Life. • Can be used to evidence that the following outcomes are being met: • Outcome 1: Respecting and involving people who use services. • Outcome 2: Consent to care and treatment • Outcome 4: Care and welfare of people who use services • Outcome 5: Meeting nutritional needs • Outcome 7: Safeguarding people who use services from abuse • Outcome 9: Management of medicines • Outcome 10: Safety and suitability of premises • Outcome 21: Records Respite Daily Reporting & Communication Optional / Nursing Information Mandatory Assessments/Records Day to Day Recording Dementia & Mental Capacity Information Assessment & Care Planning 21.052 Support Plan 6Email: [email protected] Phone: 01604 646 633 ADMISSION Assessment & Care Planning Dementia & Mental Capacity Information 21.053 Care Plan Day to Day Recording Mandatory Assessments/Records • Generated from the Support Plan. • Looks at need, goal and support required. • Each plan needs to be person centred (blank for you to do this). • Our Documentation Guide gives you prompts for each area and encourages staff to think in a ‘person-centred way’. 21.053 Can be used to evidence that the following outcomes are being met: • Outcome 7: Safeguarding people who use services from abuse. • Outcome 8: Cleanliness and infection control. • Outcome 9: Management of medicines. • Outcome 11: Safety, availability and suitability of equipment. • Outcome 21: Records. Optional / Nursing Information • Outcome 1: Respecting and involving people who use services. • Outcome 2: Consent to care and treatment. • Outcome 4: Care and welfare of people who use services. • Outcome 5: Meeting nutritional needs. Daily Reporting & Communication Respite 21.054 Care Plan Evaluation • To be used to document the evaluation of the care plans. Fax: 01604 644 646 Web: www.standexsystems.co.uk 7 ADMISSION 21.055 Activity Plan Day to Day Recording Dementia & Mental Capacity Information Assessment & Care Planning • To be used as the care plan but specifically for social activity. • Useful for use by Social Activity Co-ordinators. • To be used to document the evaluation of the activity plans. 21.057 Social Activity • Can be used to plot dates of social activities. • There is a year on a form. Respite Daily Reporting & Communication Optional / Nursing Information Mandatory Assessments/Records 21.056 Activity Plan Evaluation 21.058 Social Activity Comments • Can be used to write comments about the social activity in conjunction with the activity care plans or on their own. 8Email: [email protected] Phone: 01604 646 633 ADMISSION Assessment & Care Planning Dementia & Mental Capacity Information Mandatory Assessments/Records • Personal Story. • Useful for reminiscence, especially in those with dementia. • Person-centred. Day to Day Recording 21.059 Personal History Optional / Nursing Information Daily Reporting & Communication Respite 21.060 Support Network • Quick glance document can be used to document service user’s support. • Can be used for any out of hours contacts such as Macmillan Nurse etc. Therefore supporting End of Life documentation. Fax: 01604 644 646 Web: www.standexsystems.co.uk 9 ADMISSION Assessment & Care Planning Dementia & Mental Capacity Information Day to Day Recording • To be used if a service user needs to make a decision and their mental capacity is in question. • Assists staff in assessing capacity in line with the Mental Capacity Act 2005. Respite Daily Reporting & Communication Optional / Nursing Information Mandatory Assessments/Records 21.061 Mental Capacity Assessment 21.062 Deprivation of Liberty • Will assist manager in deciding whether an application to deprive a service user of their liberty is required. • Document the outcome of the decision. 10Email: [email protected] Phone: 01604 646 633 ADMISSION Assessment & Care Planning Dementia & Mental Capacity Information Mandatory Assessments/Records • For details of any Written Lasting Power of Attorney and/or advocates. • Can document any Advance Decisions/refusal of treatment if they become incapacitated (i.e. advance care planning). Day to Day Recording 21.063 Lasting Power of Attorney Optional / Nursing Information Daily Reporting & Communication 21.064 Future Wishes Respite • Looks at wishes of the service user at end of life (ie advance care planning). • What is important? • What would they like to happen? • What would they not like to happen? • Worries, concerns and special wishes. • Also looks at what they wish to happen after death. Fax: 01604 644 646 Web: www.standexsystems.co.uk 11 ADMISSION 21.065 Personal Care Optional / Nursing Information Mandatory Assessments/Records Day to Day Recording Dementia & Mental Capacity Information Assessment & Care Planning • Used to replace a bath book. • Year on a form. 21.066 Bowel Chart • To record bowel movements and complications. • Uses Bristol Stool Chart (poster provided). 2011 Standex Systems Ltd DO NOT PHOTOCOPY FOR ANY OTHER REASON THAN LEGAL 39 Charter Gate Quarry Park Close - Moulton Park Ind. Estate Northampton - NN3 6QB Phone (01604) 646 633 Fax (01604) 644 646 Web www.standexsystems.co.uk System No: 21.120 Respite Daily Reporting & Communication Bristol Stool Chart The Bristol Stool Chart is designed to classify the form of human faeces into 7 categories. It was developed by Dr K W Heaton at the University of Bristol (1997) Type 1 Type 2 Type 3 Type 4 Separate hard lumps, like nuts (hard to pass) Type 5 Sausage-shaped but lumpy Type 6 Fluffy pieces with ragged edges, a mushy stool Type 7 Watery, no solid pieces ENTIRELY LIQUID Like a sausage but with cracks on its surface Soft blobs with clear-cut edges (passed easily) Like a sausage or or snake, smooth and soft Type 1 and 2 indicate constipation Type 3 and 4 are the ‘ideal stools’ especially the latter. Type 5, 6 and 7 tend towards diarrhoea. If the service user has a Type 7 stool then a sample should be considered. Please refer to your homes policy regarding isolation and infection control if the service user has a Type 7 stool Reproduced by kind permission of Dr KW Heaton, Reader in Medicine at the University of Bristol. 12Email: 21.098 Bristol Stool Chart • Reference guide for Bowel Chart. [email protected] Phone: 01604 646 633 ADMISSION Assessment & Care Planning Dementia & Mental Capacity Information Day to Day Recording 21.067 Food Chart • Enables detailed recording of food intake. • Sits above MUST Tool in system. Mandatory Assessments/Records Optional / Nursing Information Daily Reporting & Communication Respite 21.068 Weight Chart • Can document monthly weight on graph to show clearly any dips in weight (and vice versa). • New version will allow you to monitor as and when required (ie daily or weekly). • Year on form based on monthly review. Fax: 01604 644 646 Web: www.standexsystems.co.uk 13 ADMISSION Assessment & Care Planning Dementia & Mental Capacity Information Day to Day Recording • Can be used to map any bruising or markings that have no explanation but are a concern to staff. • Could also be used when service user is admitted to hospital and on their return as a safeguard for both service user and staff. Respite Daily Reporting & Communication Optional / Nursing Information Mandatory Assessments/Records 21.069 Body Chart 21.070 Epilepsy Chart • Allows recording of seizures. • An accurate and comprehensive record. 14Email: [email protected] Phone: 01604 646 633 ADMISSION Assessment & Care Planning Dementia & Mental Capacity Information Mandatory Assessments/Records • Scoring tool to ascertain condition of mouth. • Suggested actions on reverse to assist care planning. • Year on form based on monthly review. Day to Day Recording 21.071 Oral Assessment Tool Optional / Nursing Information Daily Reporting & Communication Respite 21.072 Record of Behaviour • Allows recording of any behaviour that may be deemed inappropriate and harmful. • Enables staff to clearly see patterns and triggers etc. Fax: 01604 644 646 Web: www.standexsystems.co.uk 15 ADMISSION Assessment & Care Planning Dementia & Mental Capacity Information Day to Day Recording Mandatory Assessments/Records Optional / Nursing Information Daily Reporting & Communication Respite 21.075 Manual Handling • Staff can clearly document which type of handling is appropriate for which movement. • Any constraints, environmental concerns etc can be recorded. • Year on form based on monthly review. 16Email: [email protected] Phone: 01604 646 633 ADMISSION Assessment & Care Planning Dementia & Mental Capacity Information Day to Day Recording Mandatory Assessments/Records Optional / Nursing Information Daily Reporting & Communication Respite 21.074 Falls Risk Assessment • Has questions and necessary actions to prevent the risk of falling. • Year on a form based on monthly review. • In Line with Outcome 4: Care and welfare of people who use services. By identifying risks staff can then state in the care plans how they will be managed and reviewed. Fax: 01604 644 646 Web: www.standexsystems.co.uk 17 ADMISSION • Enables MUST score to be documented. • Over two and a half years on a form based on monthly review. University Hospitals of Leicester NHS Trust by poster • Accompanied Ward: Site: with BMI, weight loss 'MALNUTRITION UNIVERSAL SCREENING TOOL' ('MUST') table and alternative measurements for quick Height Body Mass Index (BMI) Weight 3-6 months ago % Weight Loss reference. System No.: 20.952 Name: Hospital No: kg m Measured / Recalled Measured / Recalled PLEASE CIRCLE PLEASE CIRCLE Change in weight over last 3-6 months kg kg/m2 USE CHART TO CALCULATE FROM CURRENT WEIGHT AND HEIGHT (See bottom) Yes / No / Don't know Measured / Recalled / IF YES USE CHART TO CALCULATE % USING CURRENT AND PREVIOUS WEIGHT (see bottom) Don't know PLEASE CIRCLE 'Malnutrition Universal Screening Tool' ('MUST') Score Please circle score A BMI Less than 18.5kg/m2 = 2 ∨ 2 2 2 2 * Order a special diet if appropriate e.g. gluten free, pureed diet Between 18.5kg/m and 20kg/m = 1 1 1 1 1 * More than 20kg/m2 = 0 0 0 0 0 Assist with ordering suitable meal choices (suggest high energy/high calorie main courses and puddings and 'Chef's Specials') than 10% = 2 21.097More MUST Poster Between 5% and 10% = 1 2 2 2 2 * Encourage the patient to request additional items for snacks between meals 1 1 1 1 * Encourage milk and milky drinks Less than 5% = 0 0 0 0 0 * Offer 1 Build Up drink per day (savoury or sweet) Unless contraindicated e.g. renal disease, lactose intolerant, milk allergy or patients * Offer assistance with eating and drinking, when required. Instigate red tray if indicated * Treat underlying conditions such as nausea, vomiting, diarrhoea * Commence food and drink record charts for all meals and snacks 2 B % Unplanned weight loss over last 3-6 months C MEDIUM / HIGH RISK DATE 2 • Reference guide for MUST Tool Acute disease Patient acutely ill and there has been NO or likely showing BMI chart, Weight Loss effect score to be NO nutritional intake for > 5 days: table and alternative measurements. Total RISK: Low = 0 Medium = 1 High = 2 or more YES = 2 2 2 2 2 NO = 0 0 0 0 0 NO Please circle NOT NEEDED Refer to your ward dietitian if: * * * * * S I G N Nutritional care plan started? YES following low residue diets. Contact ward dietitian for advice REVIEW INTAKE AFTER THREE DAYS, if intake remains minimal, refer to your ward dietitian * Add scores to give RISK Record total score: If score 1 or more start Nutrition careplan (see right). If no improvement or if score > 4 refer to Dietitian * * 'MUST' score is 4 or more Enteral tube feeding is required NBM > 5 days 'MUST' score increases or there is no improvement on medium/high risk nutrition care plan Specialist advice is required following diagnosis, or a full nutritional assessment is required in response to clinical judgement Patient requires assessment and provision of a therapeutic diet e.g. allergy, metabolic Repeat 'MUST' weekly - if weight drops >1kg/week refer to your ward dietitian WEIGH PATIENT TWICE WEEKLY AND DOCUMENT ON WEIGHT CHART The ‘Malnutrition Universal Screening Tool’ (‘MUST’) is reproduced here with the kind permission of BAPEN (British Association for Parenteral and Enteral Nutrition). The ‘MUST’ was developed by 2011 Standex Systems Ltd DO NOT PHOTOCOPY FOR ANY OTHER REASON THAN LEGAL 39 Charter Gate Quarry Park Close - Moulton Park Ind. Estate Northampton - NN3 6QB the Malnutrition Advisory Group (MAG) of BAPEN and first produced in November 2003. Repeat 'MUST' weekly or if condition changes - using new weight and on discharge as part of discharge care planning Phone (01604) 646 633 Fax (01604) 644 646 Web www.standexsystems.co.uk System Number: 21.097 ‘MALNUTRITION UNIVERSAL SCREENING TOOL’ (‘MUST’) 'MUST' TOOL Estimating BMI category from mid upper arm circumference (MUAC) - use if you cannot measure service user’s actual weight or height Body Mass Index and Weight Loss Table STEP 1 - Body Mass Index (BMI) Score Measure height and weight to get BMI and document score in service user file. If unable to obtain height and weight, use the A BMIprocedures scoreshown (& below. BMI) Height (feet and inches) alternative Height (feet and inches) STEP 2 - Weight Loss Score The Nutrition screening tool is based on and 'MUST' andscore reproduced here Note percentage of unplanned weight loss document in service user file with kind permission of BAPEN (the British Association for Parenteral and Enteral Nutrition). Further information on 'MUST' is available on the BAPEN website www.bapen.org.uk B - Weight loss score SCORE 0 Wt Loss SCORE 1 SCORE 2 Wt Loss Wt Loss 5-10% <5% > 10% SCORE 0 Wt Loss < 5% 34kg 36kg 38kg 40kg 42kg 44kg 46kg 48kg 50kg 52kg 54kg 56kg 58kg 60kg 62kg 64kg 66kg 68kg 70kg 72kg 74kg 76kg 78kg 80kg 82kg 84kg 86kg 88kg 90kg 92kg 94kg 96kg 98kg 100kg 102kg 104kg 106kg 108kg 110kg 112kg 114kg 116kg 118kg 120kg 122kg 124kg 126kg < 1.7 kg < 1.8 kg < 1.9 kg < 2 kg < 2.1 kg < 2.2 kg < 2.3 kg < 2.4 kg < 2.5 kg < 2.6 kg < 2.7 kg < 2.8 kg < 2.9 kg < 3 kg < 3.1 kg < 3.2 kg < 3.3 kg < 3.4 kg < 3.5 kg < 3.6 kg < 3.7 kg < 3.8 kg < 3.9 kg < 4 kg < 4.1 kg < 4.2 kg < 4.3 kg < 4.4 kg < 4.5 kg < 4.6 kg < 4.7 kg < 4.8 kg < 4.9 kg < 5 kg < 5.1 kg < 5.2 kg < 5.3 kg < 5.4 kg < 5.5 kg < 5.6 kg < 5.7 kg < 5.8 kg < 5.9 kg < 6 kg < 6.1 kg < 6.2 kg < 6.3 kg 1.7 - 3.4 kg SCORE 1 Wt Loss 5-10% 5st 4lb > 3.4 kg SCORE 2 0 Wt SCORE Loss Wt Loss < 5% >10% <4lb The subject’s left arm should be bent at the elbow at a 90 degree angle, with the upper SCORE 1 Wt Loss 5-10% SCORE 2 Wt Loss > 10% 4 - 7lb > 7lb SCORE SCORE arm0half parallel to the1side ofSCORE 2 Wt Loss Wt Loss Wt Loss the body. Measure the distance <5%between the5-10% bony protrusion >10% on the shoulder (acromiom) Weight before weight loss (st lb) Weight (kg) Weight (kg) 5st 7lb <4lb 4 - 8lb kg > 3.6 kg >7lb 4lbof-the 7lb <4lband the point 5st>> 8lb 4lb 34 kg 1.8 - 3.6 <1.70 1.70 - 3.40 >3.40 elbow 5st 11 lb <4lb 4 - 8lb 8lb 1.9 - 3.8 kg > 3.8 kg - 8lb >8lb 5st> 8lb 7lb <4lb(olecranon 4lb process). 6st <4lb 4 - 8lb 36 kg 2 - 4 kg<1.80> 4 kg 1.80 - 3.60 >3.60 6st 4lb <4lb 4 - 9lb kg > 4.2 kg >8lb 4lb - 8lb <4lb 5st> 9lb 11 lb 38 kg 2.1 - 4.2 <1.90 1.90 - 3.80 >3.80 6st 7lb <5lb 5 9lb > 9lb 2.2 - 4.4 kg > 4.4 kg Mark the mid-point. >8lb 4lb 8lb <4lb 6st 40 kg 2.3 - 4.6 <2.00 2.00 4.00 >4.00 6st 11lb <5lb 5 10lb > 10lb kg > 4.6 kg 7st <5lb 5 - 10lb > 10lb 4lb - 9lb >9lb 6st 4lb <4lb kg > 4.8 kg 42 kg 2.4 - 4.8 <2.10 2.10 - 4.20 >4.20 7st 4lb <5lb 5 - 10lb > 10lb 2.5 - 5 kg > 5 kg 5lb - 9lb >9lb <5lb 6st 7lb 44 kg 2.6 - 5.2 <2.20 2.20 - 4.40 >4.40 7st 7lb <5lb 5 - 11lb > 11lb kg > 5.2 kg 7st 11lb <5lb 5 - 11lb > 11lb 5lb - 10lb >10lb 6st 11lb <5lb 46 kg 2.7 - 5.4 <2.30 2.30 - 4.60 >4.60 kg > 5.4 kg 8st <6lb 5 - 11lb > 11lb 2.8 - 5.6 kg 5.6 kg 5lb - 10lb >10lb 7st <5lb 48 kg 2.9 <2.40>> 5.8 2.40 - 4.80 >4.80 8st 4lb <6lb 6 - 12lb > 12lb - 5.8 kg kg >10lb 5lb - 10lb <5lb 7st 4lb 8st 7lb >6lb 6 - 12lb > 12lb 50 kg 3 - 6 kg<2.50> 6 kg 2.50 - 5.00 >5.00 8st 11lb <6lb 6 - 12lb > 12lb kg > 6.2 kg 5lb - 11lb >11lb 7st 7lb <5lb 52 kg 3.1 - 6.2 <2.60 2.60 - 5.20 >5.20 9st <6lb 6 - 13lb > 13lb 3.2 - 6.4 kg > 6.4 kg 5lb - 11lb >11lb 7st 11.lb <5lb 54 kg 3.3 - 6.6 <2.70 2.70 - 5.40 >5.40 9st 4lb <7lb 7 - 13lb > 13lb kg > 6.6 kg 9st 7lb <7lb 7 13lb > 13lb >11lb 6lb - 11lb 8st <6lb kg > 6.8 kg 56 kg 3.4 - 6.8 <2.80 2.80 - 5.60 >5.60 9st 11lb <7lb 7lb 1st > 1st - 7 kg > 7 kg 6lb 12lb >12lb 8st 4lb <6lb 58 kg 3.63.5- 7.20 <2.90 2.90 5.80 >5.80 10st <7lb 7lb 1st > 1st kg > 7.2 kg 10st 4lb <7lb 7lb - 1st 6lb - 12lb >12lb 8st> 1st 7lb <6lb kg > 7.4 kg 60 kg 3.7 - 7.4 <3.00 3.00 - 6.00 >6.00 10st 7lb <7lb 7lb - 1st 1lb > 1st 1lb 3.8 - 7.6 kg > 7.6 kg 6lb - 12lb >12lb 8st 11lb <6lbAsk the subject 62 kg 3.9 - 7.8 <3.10 3.10 - 6.20 >6.20 10st 11lb <8lb 8lb - 1st 1lb > 1st 1lb to let arm hang loose kg > 7.8 kg 11st <8lb 8lb - 1st 1lb 9st > 1st 1lb 6lbaround - 13lb <6lband measure 64 kg 4 - 8 kg<3.20> 8 kg 3.20 - 6.40 >6.40 the upper >13lb arm at 11st 4lb <8lb 8lb - 1st 2lb > 1st 2lb kg > 8.2 kg 7lb making - 13lbsure that>13lb <7lbthe mid-point, 9st 4lb 66 kg 4.1 - 8.2 <3.30 3.30 - 6.60 >6.60 the 11st 7lb <8lb 8lb - 1st 2lb > 1st 2lb 4.2 - 8.4 kg > 8.4 kg but not tight. 7lbis-snug 13lb >13lb <7lbtape measure 11st 11lb <8lb 8lb - 1st 3lb 9st > 1st7lb 3lb 68 kg 4.3 - 8.6 <3.40 3.40 - 6.80 >6.80 kg > 8.6 kg 12st <8lb 8lb - 1st 3lb 9st > 1st11lb 3lb kg > 8.8 kg 7lb - 1st.0lb >1st.0lb <7lb 70 kg 4.4 - 8.8 <3.50 3.50 - 7.00 >7.00 12st 4lb <9lb 9lb - 1st 3lb > 1st 3lb 4.5 - 9 kg > 9 kg >1st 0lb 7lb 1st 0lb <7lb 10st 72 kg 4.6 - 9.2 <3.60 3.60 - 7.20 >7.20 12st 7lb <9lb 9lb - 1st 4lb > 1st 4lb kg > 9.2 kg 12st 11lb <9lb 9lb - 1st 4lb 10st > 1st 4lb 7lb - 1st 0lb >1st 0lb <7lb 4lb kg > 9.4 kg 74 kg 4.7 - 9.4 <3.70 3.70 - 7.40 >7.40 13st <9lb 9lb - 1st 4lb > 1st 4lb 4.8 - 9.6 kg > 9.6 kg - 1st 1lb >1stto1lb 10st 7lb <7lbIf MUAC7lb 76 kg 4.9 <3.80 3.80 7.60 >7.60 is < 23.5cm, BMI is likely 13st 4lb <9lb 9lb 1st 5lb > 1st 5lb - 9.8 kg > 9.8 kg 13st 7lb <9lb 9lb - 1st 5lb 10st > 1st 5lb 8lb -2 1st 1lb >1st 1lb 11lb <8lbbe < 20 kg/m 78 kg 5 - 10 kg<3.90> 10 kg 3.90 - 7.80 >7.80 13st 11lb <10lb 10lb - 1st 5lb > 1st 5lb kg > 10.2 kg 8lb - 1st 1lb >1st 1lb 11st <8lb 80 kg 5.1 - 10.2<4.00 4.00 - 8.00 >8.00 14st <10lb 10lb - 1st 6lb > 1st 6lb 5.2 - 10.4 kg > 10.4 kg is > 32cm, to be - 1st BMI 2lbis likely >1st 2lb 4lb <8lbIf MUAC8lb 14st 4lb <10lb 10lb - 1st 6lb 11st > 1st 6lb 82 kg 5.3 - 10.6<4.10 >8.20 kg > 10.6 kg 4.10 - 8.20 > 30 kg/m2 14st 7lb <10lb 10lb - 1st 6lb > 1st 6lb kg > 10.8 kg 4.20 - 8.40 8lb - 1st 2lb >1st 2lb 11st 7lb <8lb 84 kg 5.4 - 10.8<4.20 >8.40 14st 11lb <10lb 10lb - 1st 7lb > 1st 7lb 5.5 - 11 kg > 11 kg 8lb - 1st 3lb >1st 3lb 11lb <8lb 86 kg 5.6 - 11.2<4.30 >8.60 15st <11lb 11lb - 1st 7lb 11st > 1st 7lb kg > 11.2 kg 4.30 - 8.60 15st 4lb <11lb 11lb - 1st 7lb 12st > 1st 7lb 8lb - 1st 3lb >1st 3lb <8lb kg > 11.4 kg 4.40 - 8.80 88 kg 5.7 - 11.4<4.40 >8.80 15st 7lb <11lb 11lb - 1st 8lb > 1st 8lb - 11.6 kg > 11.6 kg 9lb - 1st 3lb >1st 3lb 4lb <9lb 90 kg 5.8 <4.50 4.50 - 9.00 >9.00 15st 11lb <11lb 11lb - 1st 8lb 12st > 1st 8lb 5.9 - 11.8 kg > 11.8 kg 16st <11lb 11lb - 1st 8lb 12st > 1st 8lb 9lb - 1st 4lb >1st 4lb 7lb <9lb 92 kg 6 - 12 kg<4.60> 12 kg 4.60 - 9.20 >9.20 16st 4lb <11lb 11lb - 1st 9lb > 1st 9lb - 12.2 kg > 12.2 kg 9lb - 1st 4lb >1st 4lb 12st 11lb <9lb 94 kg 6.1 <4.70 4.70 9.40 >9.40 16st 7lb <12lb 12lb 1st 9lb > 1st 9lb 6.2 - 12.4 kg > 12.4 kg 9lb - 1st 4lb >1st 4lb <9lb 13st 96 kg 6.3 - 12.6<4.80 >9.60 kg > 12.6 kg 4.80 - 9.60 9lb - 1st 5lb >1st 5lb 13st 4lb <9lb 98 kg <4.90 4.90 - 9.80 >9.80 9lb - 1st 5lb >1st 5lb 13st 7lb <9lb 100 kg <5.00 5.00 - 10.00 >10.00 from ulna length - use if you cannot user’s actual 10lbheight - 1st 5lb >1st 5lb 13stmeasure 11lb service <10lb 102 kg <5.10 Estimating 5.10 -height 10.20 >10.20 10lb - 1st 6lb >1st 6lb 14st <10lb 104 kg <5.20 5.20 - 10.40 >10.40 10lb - 1st 6lb >1st 6lb 14st 4lb <10lb 106 kg <5.30 5.30 - 10.60 >10.60 Measure between the point of the elbow (olecranon process) and the 10lb - 1st 6lb >1st 6lb 14st 7lb <10lb 108 kg <5.40 5.40 - 10.80 >10.80 midpoint of the prominent bone of the wrist (styloid process) (left side 10lb - 1st 7lb >1st 7lb 14st 11lb <10lb 110 kg <5.50 5.50 - 11.00 >11.00 if possible). 11lb - 1st 7lb >1st 7lb <11lb 15st kg row<5.60 5.60 - 11.20 >11.20 Find the ulna length in cm in112 the white in the table below. 11lb - 1st 7lb >1st 7lb 15st 4lb <11lb Choose the appropriate height metres from the age and gender in 114inkg <5.70 5.70 - 11.40 >11.40 Height (m) the options above or below116 the white 11lb - 1st 8lb >1st 8lb 15st 7lb <11lb kg bar. <5.80 5.80 - 11.60 >11.60 Note: The black lines denote the exact cut off points (30, 20 and 18.5 kg/m ), figures on the chart have been rounded to the nearest whole number 11lb - 1st 8lb >1st 8lb 15st 11lb <11lb 118 kg <5.90 5.90 - 11.80 >11.80 11lb - 1st 8lb >1st 8lb <11lb 16st 120 kg <6.00 6.00 - 12.00 >12.00 11lb <11lb kg 1.89 <6.10 6.101.82 - 12.20 Men (<65 years) 1.94 1.93122 1.91 1.87 1.85 1.84 1.80 1.78>12.20 1.76 1.75 1.73 1.7116st 1.694lb 1.67 1.66 1.64 1.62 1.60- 1st 1.589lb 1.57 >1st 1.55 9lb 1.53 STEP 3 Height (m) 12lb <12lb kg 1.82 <6.20 6.201.76 - 12.40 Men (>65 years) 1.87 1.86124 1.84 1.81 1.79 1.78 1.75 1.73>12.40 1.71 1.70 1.68 1.6716st 1.657lb 1.63 1.62 1.60 1.59 1.57- 1st 1.569lb 1.54 >1st 1.52 9lb 1.51 Acutely ill and no nutritional intake or unlikelihood of no nutritional intake for more than 5 days Note: The black lines denote the exact cut off points (30,20 and 18.5 the nearest whole number. STEP 4 kg/m2), figures on the chart have been rounded to Ulna 12631kg 30.5 <6.30 - 12.60 Length (cm) 32 31.5 30 29.5 6.30 29 28.5 28 27.5>12.60 27 26.5 26 25.5 25 24.5 24 23.5 23 22.5 22 21.5 21 20.5 Weight (stones and pounds) Respite Current Weight Weight (stones and pounds) Daily Reporting & Communication Optional / Nursing Information Mandatory Assessments/Records Day to Day Recording Dementia & Mental Capacity Information COMPLETE ON FIRST SCREEN - DATE: Weight before weight loss (kg) Assessment & Care Planning 21.073 MUST Tool 2 Add scoresbyfrom step 1, 2 and 3 Ltd together to obtainwith an overall scoreHospitals for risk ofofmalnutrition “Derived from forms developed Standex Systems in conjunction University Leicester” STEP 5 Use management guidelines and/or local policy to develop care plan Plate 1 Composite LEICESTER HOSPITAL 1.51 1.49 1.48 1.46 1.49 1.48 1.46 1.45 20 19.5 19 18.5 Women (<65 years) 1.84 1.83 1.81 1.80 1.79 1.77 1.76 1.75 STANDEX Phone · Fax1.58 (01604) 6441.55 646 www.standexsystems.co.uk 1.73 ©2007 1.72 1.70 1.69 SYSTEMS 1.68 1.66 Ltd. 1.65 1.63(01604) 1.62 646 1.616331.59 1.56 1.54 1.52 1.51 1.50 1.48 1.47 Women (>65 years) 1.84 1.83 1.81 1.79 1.78 1.76 1.75 1.73 1.71 1.40 20XXX 07/08/06 18Email: 1.70 1.68 1.66 1.65 1.63 1.61 1.60 1.58 1.56 1.55 1.53 1.52 1.50 1.48 1.47 1.45 1.44 1.42 [email protected] Phone: 01604 646 633 ADMISSION Assessment & Care Planning Dementia & Mental Capacity Information Mandatory Assessments/Records • Evidences that systems are in place to monitor and manage infection control. Day to Day Recording 21.077 Infection Risk Assessment Optional / Nursing Information Daily Reporting & Communication Respite 21.076 Pressure Ulcer Assessment • • • • Waterlow Score. Body map. Year on a form based on monthly review. Waterlow Manual accompanies form. Fax: 01604 644 646 Web: www.standexsystems.co.uk 19 ADMISSION Assessment & Care Planning Dementia & Mental Capacity Information Day to Day Recording Mandatory Assessments/Records Optional / Nursing Information Daily Reporting & Communication Respite 21.078 Bedrail Assessment • Asks risk balance questions. • Staff get a recommendation via the Risk Matrix Tool. • Can document your rationale for using (or not), bedrails. • Consent signature column. 20Email: [email protected] Phone: 01604 646 633 ADMISSION Assessment & Care Planning Dementia & Mental Capacity Information Day to Day Recording 21.079 General Risk Assessment Mandatory Assessments/Records • One form per risk. • Trigger questions regarding level of risk and actions to be taken. • In the style of the care plans with tabs. • Can use evaluation form to evaluate plan without having to re-write. Can be used to evidence that the following outcomes are being met: • Outcome 10: Safety and suitability of premises. • Outcome 11: Safety, availability and suitability of equipment. • Outcome 21: Records. Optional / Nursing Information • Outcome 1: Respecting and involving people who use services. • Outcome 2: Consent to care and treatment. • Outcome 4: Care and welfare of people who use services. • Outcome 7: Safeguarding people who use services from abuse. Daily Reporting & Communication Respite 21.080 General Risk Evaluation • To be used to document the evaluation of the risk assessment. Fax: 01604 644 646 Web: www.standexsystems.co.uk 21 ADMISSION 21.081 Pain Chart Respite Daily Reporting & Communication Optional / Nursing Information Mandatory Assessments/Records Day to Day Recording Dementia & Mental Capacity Information Assessment & Care Planning • Numeric Pain Scale (for those who can verbalise pain). • Doloplus2 (for those with a cognitive impairment, ie dementia, who cannot verbalise their pain). • Can assess acute and chronic pain. • Body Map. 21.082 Wound Chart • One chart per wound for more detailed documentation. • Accompanies care plan if one is required. 22Email: [email protected] Phone: 01604 646 633 ADMISSION Assessment & Care Planning Dementia & Mental Capacity Information Mandatory Assessments/Records • Questions to ascertain whether service user has depression. • Soon to be one for those with cognitive impairment such as dementia. Day to Day Recording 21.083 Depression Scale Optional / Nursing Information Daily Reporting & Communication Respite 21.084 Medication Record • Document all medication on arrival including short term meds such as antibiotics and any changes to medications. • In line with Outcome 9: Management of medicines, where an upto date list of medicines taken by the service user needs to be documented when they first begin the service. Fax: 01604 644 646 Web: www.standexsystems.co.uk 23 ADMISSION Assessment & Care Planning Dementia & Mental Capacity Information Day to Day Recording Mandatory Assessments/Records Optional / Nursing Information Daily Reporting & Communication Respite 21.089 Dependency Profile • Scoring tool to ascertain dependency levels. • Can be plotted on graph to show patterns of dependency levels. • Can be used as evidence if applying for continuing healthcare funding (has the same domains). • Designed to be a monthly assessment and in line with Outcome 21: Records, it can be evidenced on that assessments are updated, monitored and reviewed to ensure records are kept and maintained for each service user. 24Email: [email protected] Phone: 01604 646 633 ADMISSION • To record temp, pulse, resps, blood pressure, fluid intake, output and input. • Can record any relevant comments. Day to Day Recording • Document time, blood sugar and insulin given. Dementia & Mental Capacity Information 21.086 Diabetic Chart Assessment & Care Planning 21.085 Observations and Monitoring 21.088 Fluid Balance Mandatory Assessments/Records • Document intake and output over 24 hours. • Two weeks on one form. Optional / Nursing Information Daily Reporting & Communication Respite 21.087 Repositioning Chart • Document repositioning of service user. • Two weeks on one form. Fax: 01604 644 646 Web: www.standexsystems.co.uk 25 ADMISSION Assessment & Care Planning Dementia & Mental Capacity Information Day to Day Recording Mandatory Assessments/Records Optional / Nursing Information Daily Reporting & Communication Respite 21.090 Deterioration Scale • Recommended by Dr Jo Hockley in line with Gold Standards Framework. • Can be used to record periodic review of deterioration and required action. 26Email: [email protected] Phone: 01604 646 633 ADMISSION Assessment & Care Planning • Enables keyworkers to document their notes. Dementia & Mental Capacity Information 21.091 Keyworker Day to Day Recording 21.092 Communication Sheet Mandatory Assessments/Records • Can be used for general communication purposes. • Can be used to replace the Communication book. Optional / Nursing Information Daily Reporting & Communication Respite 21.093 Multidisciplinary Notes • Enables the multidisciplinary team to document their notes. Fax: 01604 644 646 Web: www.standexsystems.co.uk 27 ADMISSION 21.094 Doctors Notes 21.095 Family Communication • Enables family to document any concerns they may have and any communication they wish to get across to staff. • Recommended by Dr Jo Hockley. Respite Daily Reporting & Communication Optional / Nursing Information Mandatory Assessments/Records Day to Day Recording Dementia & Mental Capacity Information Assessment & Care Planning • Enables Doctors to document the outcome of their visit. 21.096 District Nurse Notes • Allows District Nurses to document the outcome of their visit. 28Email: [email protected] Phone: 01604 646 633 ADMISSION Assessment & Care Planning • Sits at the back so can be changed very easily. • A form on which day to day occurrences should be recorded. • A3 in size. Dementia & Mental Capacity Information 20.768 Daily Report Day to Day Recording 20.025 Daily Report Mandatory Assessments/Records • Sits at the back so can be changed very easily. • A form on which day to day occurrences should be recorded. • A4 in size. Optional / Nursing Information Daily Reporting & Communication 20.019 Nursing Report Fax: 01604 644 646 Web: www.standexsystems.co.uk Respite • For use by nursing staff. • Sits at the back so can be changed very easily. • A form on which day to day occurrences should be recorded. • A3 in size. 29 30Email: [email protected] Phone: 01604 646 633 Respite Daily Reporting & Communication Optional / Nursing Information Mandatory Assessments/Records Day to Day Recording Dementia & Mental Capacity Information Assessment & Care Planning ADMISSION ADMISSION Assessment & Care Planning Dementia & Mental Capacity Information Day to Day Recording Mandatory Assessments/Records Optional / Nursing Information Daily Reporting & Communication Respite 20.929 Respite Booklet • The Standex System in condensed format for those who are having short term respite. 31 Web: www.standexsystems.co.uk Fax: 01604 644 646 Contact your local business manager for a no obligation care planning consultation for your care home. For any guidance or advice on all aspects of care planning, please contact our Nurse Advisor, Lucy Caldwell RGN on 01604 646 633 Lucy Caldwell Nurse Advisor Standex Systems Ltd 39 Charter Gate І Northampton NN3 6QB Tel.: + 44 (0)1604 / 64 66 33 І Fax: +44 (0)1604 / 64 46 46 Email: [email protected] www.standexsystems.co.uk The forms contained within this brochure are protected by english copyright law and should not be reproduced or copied for any reason other than legal requirements. Standex Systems Ltd 39 Charter Gate, Quarry Park Close, Moulton Park Industrial Estate, Northampton, NN3 6QB Phone: 01604 646 633 Fax: 01604 644 646 www.standexsystems.co.uk








© Copyright 2026