
T
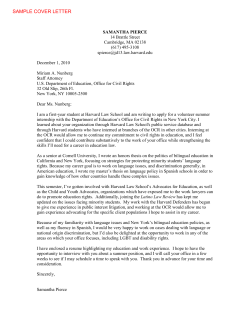
VOL UME 15 • N UMBER 11 Abdominal aortic aneurysms: Triple A, double trouble T he aorta is the largest artery in the body; it’s also the strongest. But size and strength are not enough to protect this crucial blood vessel; in fact, the aorta is one of the body’s most vulnerable arteries. Although many things can go wrong with the aorta, the most common is an aneurysm; it’s an unfamiliar term, but it’s a well-chosen name based on the ancient Greek word that means “to widen.” Any part of the aorta can develop a widening, or aneurysm, but most occur in the lower part of the artery as it travels through the abdomen, carrying blood to the legs (see figure). Abdominal aortic aneurysms (AAAs) are rare in young people, but the prevalence rises steadily in men above 55 and in women above 70. In all, men are 5 to Abdominal aortic aneurysm Normal abdominal aorta Renal arteries Kidney Aneurysm Iliac arteries © 2011 Harriet Greenfield Aneurysms are most likely to develop in the lower abdomen, below the arteries that carry blood to the kidneys and above the branches that supply the legs. 10 times more likely than women to have an AAA. While many are harmless, others can rupture, usually with deadly results. That’s why AAAs are responsible for at least 9,000 deaths in the United States each year, making them our 13th leading killer. Most victims are men over 65. Fortunately, though, new advances in diagnosis and therapy are dramatically improving the management of this age-old problem. The normal aorta The aorta is the body’s main blood vessel; it receives all the blood pumped out from the left ventricle of the heart. Because it lies in the chest, the first part of the artery is called the thoracic aorta; after leaving the heart, it ascends toward the neck, and then descends toward the abdomen. When the artery leaves the chest, it becomes known as the abdominal aorta. After traveling along the rear of the abdomen just in front of the spine for about seven inches, the abdominal aorta divides into the two smaller iliac arteries that carry blood to the pelvis and legs. In healthy adult men, the top of the aorta is about 3 centimeters (cm), or 1.2 inches, wide; as it runs through the body and distributes blood to the head and arms, it tapers to a width of about 2 cm (0.8 inches) in the abdomen. If a segment of the abdominal aorta widens by over 50%, to 3 cm or more, it is considered to be an aneurysm. Like all arteries, the aorta’s wall has three layers: a thin inner layer lined with endothelial cells, a middle layer composed of smooth muscle cells and elastic tissue, and an outer layer of supporting tissues. But the middle layer of the aorta distinguishes it from other arteries; it is composed of layer upon layer of elastic tissue, which makes it very thick and strong. It needs that strength to absorb june 2011 INSIDE Is sex exercise—and is it hard on the heart?. . . . . . . . . 5 Many men get exercised about sex—but how does this indoor activity rate as exercise? Medical memo: Cholesterol and prostate cancer. . . . . . . . 6 Scientists have come a long way in understanding how cholesterol affects the heart and blood vessels. They are just starting to puzzle out the relationship between cholesterol and the prostate. On call. . . . . . . . . . . . . . . . . . . 8 Excessive perspiration Deodorants are not a cure-all. What’s New Core Exercises Special Health Report from Harvard Medical School To order, call 877-649-9457 (toll-free) or visit us online at www.health.harvard.edu. Receive Harvard Health Publications’ free e-mail newsletter Go to www.health.harvard.edu to subscribe to HEALTHbeat. This free, weekly e-mail newsletter brings you health tips, advice, and information on a wide range of topics. You can also join in discussion with experts from Harvard Health Publications and folks like you on various health topics, medical news, and views by reading the Harvard Health Blog (www.health.harvard.edu/blog). CONTACT US Write to us at [email protected] For customer service, write us at [email protected] This Harvard Health Publication was prepared exclusively for Bulfinch Medical Group - Purchased at http://www.health.harvard.edu/ Abdominal aortic aneurysms (continued) Knowledge Is Power E d ito r ia l S ta f f Editor Harvey B. Simon, M.D. Editorial Assistant Kathleen Sweeney Laing Copy Editor Pat Cleary Art Director Heather Derocher Illustrator Harriet Greenfield Production Coordinator Nicole Wall e d ito r ia l boa r d Board members are associated with Harvard Medical School and affiliated institutions. Cardiology Patrick T. O’Gara, M.D. Endocrinology Gilbert H. Daniels, M.D. Gastroenterology Stanley J. Rosenberg, M.D. Internal Medicine Christopher M. Coley, M.D. Stephen E. Goldfinger, M.D. Russell S. Phillips, M.D. Neurology Colin McDonald, M.D. Oncology Marc B. Garnick, M.D. Orthopedics John M. Siliski, M.D. Otolaryngology Gregory W. Randolph, M.D. Preventive Medicine Edward L. Giovannucci, M.D. Psychiatry Greg L. Fricchione, M.D. Radiation Oncology William U. Shipley, M.D. Surgery David W. Rattner, M.D. Urology William C. DeWolf, M.D. Niall M. Heney, M.D. C US TOM E R S E RV I C E Call: 877-649-9457 (toll-free) E-mail: [email protected] Online: www.health.harvard.edu/customer_service Letters: Harvard Health Publications P. O. Box 9308 Big Sandy, TX 75755 -9308 Subscriptions: $32 per year (U.S.) Back issues: Harvard Health Publications ($5 each) P.O. Box 9309 Big Sandy, TX 75755-9309 Bulk StayWell Consumer Health Publishing subscriptions: One Atlantic Street, Suite 604 Stamford, CT 06901 888-456-1222 ext. 31106 (toll-free) 203-653-6266 [email protected] Corporate sales StayWell Consumer Health Publishing and licensing: One Atlantic Street, Suite 604 Stamford, CT 06901 [email protected] editorial correspondence E-mail: mens _ [email protected] Letters: Harvard Men’s Health Watch 10 Shattuck Street, 2nd Floor Boston, MA 02115 permissions Copyright Clearance Center, Inc. Phone: 978-646-2600 Online: www.copyright.com Published monthly by Harvard Health Publications, a division of Harvard Medical School Editor in Chief Anthony L. Komaroff, M.D. Publishing Director Edward Coburn © 2011 Harvard University. (ISSN 1089-1102) Proceeds support the research efforts of Harvard Medical School. Harvard Health Publications 10 Shattuck St., 2nd Floor, Boston, MA 02115 The goal of the Harvard Men’s Health Watch is to interpret medical information for the general reader in a timely and accurate fashion. Its contents are not intended to provide personal medical advice, which should be obtained directly from a physician. We regret that we cannot respond to inquiries regarding personal health matters. PUBLICATIONS MAIL AGREEMENT NO. 40906010 RETURN UNDELIVERABLE CANADIAN ADDRESSES TO: CIRCULATION DEPT., 1415 JANETTE AVENUE, WINDSOR, ON N8X 1Z1 E-mail: [email protected] the tremendous force of blood being propelled directly from the heart. And after absorbing the force when the heart pumps blood, the aorta gives some of it back: as the heart relaxes to refill with blood between beats, the elastic fibers in the aorta recoil, pushing the blood along its route to the rest of the body. The aorta expands with each heartbeat and narrows down again between beats. It’s a demanding routine, and over the years it can take quite a toll. In many older people, the elastic tissue in the aorta stiffens, making the artery less flexible; the process contributes to systolic hypertension and all its complications. And over time, the aorta itself can widen and weaken, developing into an aneurysm. Who gets an AAA? Age is a major risk factor. AAAs are rare before age 55, but they become increasingly common thereafter, affecting 4% to 8% of men above age 65. It’s not surprising that AAA is a disease of aging, since elastic tissue in the artery’s wall wears down with time, and the aorta is unable to replenish or repair this vital material. Even so, age alone does not account for the problem, since the aorta remains normal in the majority of senior citizens. Gender is another important risk factor. AAAs are much more common in men than in women, and they tend to occur about 10 years earlier in males than females. However, women face a higher risk of rupture and death than men with aneurysms of comparable size. Family history contributes in some cases. A sibling, parent, or child of a patient with an AAA has up to a one-infour chance of developing an AAA. Age, gender, and genes come with the territory, but other risk factors are reversible. Smoking is the most important; it quadruples the chance of developing an AAA. Hypertension is another important risk factor. Although older studies were mixed, a recent report linked AAAs with high total cholesterol 2 | Harvard Men’s Health Watch | June 2011 and low HDL (“good”) cholesterol levels. Surprisingly, perhaps, diabetes is not linked to AAAs. Age, male gender, family history, smoking, hypertension, and abnormal cholesterol levels—it’s a familiar recipe for atherosclerosis. Indeed, many people with AAAs also have atherosclerosis of their smaller arteries, especially the arteries that carry blood to the heart muscle and the leg muscles. It illustrates the fact that AAAs are localized manifestations of problems that involve the whole body. In fact, more than a third of patients with AAAs also have coronary artery disease. It also explains why surgical repair is so risky. Symptoms Most AAAs are clinically silent, producing no symptoms at all. But as aneurysms enlarge, they can produce pain in the abdomen or back. When such complaints occur, they are usually nonspecific, producing a pulsating sensation or gnawing ache deep in the abdomen or in the mid-back. Unfortunately, there is no mistaking the tragic event that people worry about most: rupture of an AAA causes severe abdominal and low back pain, a profound fall in blood pressure, and collapse. It’s a highly lethal event: 75% of victims die before they even get to the operating room, and of the remainder, only about half make it through surgery. Doctors often refer to AAAs as time bombs; it’s understandable, since they are often entirely silent until they burst with a big bang. But it’s now clear that even if AAAs are time bombs, they usually have long fuses—and doctors can detect them long before they explode. Diagnosis The simplest way for a doctor to detect an AAA is to feel a pulsating swelling in his patient’s abdomen, often just to the left of the belly button. As in so much of life, though, the easy way is not always a good way; except in thin people with sizable aneurysms, a doctor’s physical exam www.health.harvard.edu This Harvard Health Publication was prepared exclusively for Bulfinch Medical Group - Purchased at http://www.health.harvard.edu/ will miss most AAAs. Since only a minority of AAAs have enough calcium in their walls to show up on x-rays, an ordinary x-ray is not much help either. Fortunately, there is a simple, relatively inexpensive, entirely safe way to detect AAAs. Ultrasound will detect 95% of all AAAs, and it’s rare for the test to miss an AAA large enough to cause trouble. Because they are quick, easy, and accurate, ultrasound tests can be repeated to monitor the size of an AAA, thus identifying enlarging aneurysms at risk for rupture. In fact, ultrasound can detect an increase of as little as 3 millimeters in an aneurysm’s diameter. Newer tests such as computed tomography angiography (CTA) and magnetic resonance angiography (MRA) are also extremely accurate, but they are much more expensive and time-consuming than ultrasounds. In general, doctors reserve CTAs and MRAs for preoperative evaluations; patients receive an injection of dye for these tests. If ultrasounds are so accurate and AAAs so worrisome, shouldn’t everyone have the test as part of an annual physical? It’s the $64,000 question, and after extensive study, a general consensus has emerged. At present, most experts advise against universal screening, arguing that the problem is just not common enough to justify the enormous cost of mass testing. But targeted screening is another matter. The United States Preventive Services Task Force recommends a single screening ultrasound for men between the ages of 65 and 75 who have ever smoked. Medicare also covers screening for anyone with a family history of AAA. Needless to say, everyone with symptoms or physical findings at all suggestive of an AAA should have an ultrasound as promptly as possible. tests performed to evaluate other problems. Some are discovered by physical exam or as a result of routine screening. What’s next? Because AAAs are like time bombs, doctors and patients get very nervous about them. It’s understandable for a man to want his AAA repaired before it ruptures, but it’s not that simple. Far from being a quick fix, surgical repair is difficult and risky even when the aneurysm is intact and stable; in most hospitals, elective repair carries a mortality rate of 4% to 6%. It’s quite a dilemma, but there is a way out: doctors can now identify the AAAs at highest risk of rupturing. The key determinant is size (see chart, below). As an AAA gets larger, its walls get thinner and weaker, much as a balloon thins out as it’s inflated. An important study demonstrates the key role of an AAA’s diameter. Size* Annual risk of rupture 3–3.9 cm Less than 1% 4–4.9 cm 1% 5–5.9 cm 11% 6 cm or larger 25% *2.5 cm = 1 inch Even though small aneurysms carry some risk of rupture, a major review of seven trials covering over 4,100 patients concluded that repairing aneurysms smaller than 5.5 cm does not improve survival. But if small AAAs don’t warrant repair, they certainly require attention. Ultrasounds should be repeated every six to 12 months for small AAAs, and every three months for 5-cm AAAs. Aneurysms that expand by more than 0.5 cm over six months should be considered for repair, as should aneurysms that begin to cause pain. And every patient with an AAA should avoid all forms of tobacco exposure and reduce blood pressure What to do? Many AAAs are discovered accidentally and cholesterol levels if elevated (see in the course of abdominal imaging “Prevention and control,” page 4). www.health.harvard.edu Repairing AAAs AAAs rupture because their walls are thin and weak. Immediate surgery is the only treatment for a ruptured aneurysm, but even with prompt diagnosis and expert surgery, only about half the patients survive. To prevent a disastrous rupture, doctors can place a prosthetic graft inside the aneurysm, shoring up its walls. There are two very different ways to place an aortic graft. Conventional surgical repair in volves general anesthesia and a large abdominal incision. The surgeon clamps the aorta just above the aneur ysm, temporarily halting the flow of blood; since most AAAs are below the renal arteries, circulation to the kidneys is preserved. Next, the surgeon opens the aorta and places a Dacron tube within it. After stitching the graft in place, the surgeon closes the aorta, removes the clamp, and sews up the abdomen. It’s an effective procedure, but it’s a big operation. Even in the best of hands, a conventional AAA repair has a substantial risk of complications, including infection, bleeding, and even death, particularly since the typical patient is an older man with athero sclerosis. But in 1991, a new option became available, the endovascular stent graft. As doctors gained experience and improved the technique, they began using it more often; grafting is now performed somewhat more often than surgery in the United States. Like conventional surgery, an endovascular stent graft involves placing a reinforcement inside the aneurysm— but in this case, it’s a metal stent covered with a synthetic fabric. Doctors thread the graft up into the aorta through a thin catheter that they have inserted into the femoral artery in the groin. X-rays are used to monitor the progress of the catheter on a video screen; when the stent is in place, doctors expand it and then withdraw the catheter. Over time, the aneurysm shrinks down around the stent. June 2011 | Harvard Men’s Health Watch | 3 This Harvard Health Publication was prepared exclusively for Bulfinch Medical Group - Purchased at http://www.health.harvard.edu/ Endovascular repair can be performed under general, spinal, or even local anesthesia, and if all goes well, patients recover in just a few days. Endovascular AAA repair is an important option, but it’s technically demanding and requires a skilled medical team. The procedure can have complications of its own, including infections, bleeding into the space between the graft and the aorta, and migration of the graft itself. Which type of repair is best? It’s a crucial question, but there’s no simple answer. If you compare the results in the first weeks and months after AAA repair, endovascular stent graft is the clear winner. There are fewer early complications and deaths than with surgical repair. The endovascular procedure is more expensive, but hospitalizations are much shorter, and patients recover and return to normal function much sooner. Over time, though, the difference between the two approaches narrows. By two years, the overall survival is similar, and it remains so for at least six years. As the years pile on, though, patients with endovascular stent grafts are more likely to develop problems that require repeat procedures than patients with surgical grafts. Even without complications, all patients with grafts require careful monitoring, but endovascular grafts need more frequent imaging studies, including regular CT scans. Endovascular stent grafting is still a relatively new procedure, and with additional experience, outcomes are improving. Long-term, head-tohead randomized clinical trials will be necessary to decide which repair is best. But unless new data show a clear winner, individualized decisions will be important. Men with underlying conditions that boost the risks of surgery are likely to bene fit from endovascular repair. On the other hand, some aneurysms are not suitable for endovascular repair. The 4 | Harvard Men’s Health Watch | June 2011 skill and experience of the medical and surgical teams that are available to the patient can tip the balance one way or the other. And when there is little statistical difference between the two options, old-fashioned patient preference should guide the decision. At present, more than 60% of all AAA repairs in the U.S. are performed using the endovascular technique. Until new research is completed, the choice between surgical and endovascular AAA repair may seem difficult— but patients should be grateful that the choice is hard because there are two very good options. Prevention and control Modern imaging techniques make it easy to diagnose AAAs, new guidelines help doctors decide who to screen, and new techniques make AAA repair better and safer than ever. But prevention is the best medicine of all; how can men reduce the risk of getting an AAA and, failing that, how can they prevent a small AAA from enlarging enough to require repair or pose a risk of lifethreatening rupture? Until recently, the answer to these key questions was simple: avoid tobacco, control your blood pressure, and improve your cholesterol. Simple or not, these strategies remain essential. But as scientists learn more about the complex abnormalities that produce AAAs, they are beginning to explore new ways to control the process. To stay strong and resistant, the middle layer of the aorta’s wall depends on elastin, collagen, and other fiber-like proteins. Age, tobacco, and high blood pressure take a toll on these proteins, but they don’t attack the fibers directly. Instead, they stimulate enzymes that attack the aorta’s fibers; the most damaging group goes by the formidable name of matrix metalloproteinases (MMPs). As the MMPs break down elastin and collagen, they trigger inflammation, which adds insult to injury. As things progress, the muscle cells in the wall of the aorta begin to suffer, further weakening the artery, eventually causing it to widen and bulge out to form an aneurysm. New research is raising hope that it may be possible to interrupt this process and stabilize the aorta’s wall. Smoking cessation is the first requirement, both for preventing AAAs and for slowing the enlargement of established aneurysms. Blood pressure control is also vital. At one time, doctors hoped that beta blockers would be particularly helpful for reducing stress on the aorta, but clinical trials have not confirmed that these drugs can slow the growth of AAAs. More recently, attention has turned toward ACE inhibitors. Ani mal studies suggest these medications may slow enlargement of AAAs, and a large Canadian study linked ACE inhibitors, but not beta blockers or other antihypertensive medications, to a reduced risk of aortic rupture. More research is needed, but at present, doctors should strongly consider prescribing an ACE inhibitor for their AAA patients who need to have their blood pressure lowered. Doctors should also consider prescribing a statin for AAA patients, even if they don’t have high cholesterol levels. For one thing, many men with AAAs also have coronary artery disease and are at high risk for heart attacks. For another, statins appear to slow the enlargement of AAAs and to reduce the death rate, both in patients who have had their AAAs repaired and in those who have not. This apparent protection may depend more on the statin drugs’ ability to reduce MMP activity, fight inflammation, and reduce clotting than on their cholesterol-lowering action. Some other medications are of interest, but are highly experimental for treating AAAs. The antibiotic doxycycline inhibits MMP activwww.health.harvard.edu This Harvard Health Publication was prepared exclusively for Bulfinch Medical Group - Purchased at http://www.health.harvard.edu/ all AAAs; it is generally safe to watch small, painless aneurysms, but aneur ysms that are painful, enlarging, or 5.5 cm or larger are dangerous. At least 9,000 Americans will die from ruptured AAAs this year. The first goal of research was to prevent aneurysm rupture. Two successful methods, surgery and endovascular Now and then Abdominal aortic aneurysms are com- stent grafting, are now available, and mon, particularly in older men who about 40,000 Americans undergo are current or former smokers. A sim- these procedures each year. The next goal of therapy will be ple ultrasound exam can detect nearly ity, and in animal experiments it has protected against AAA formation. A recent study shows it can also suppress inflammation in human AAAs. The antibiotic roxithromycin and the diabetes drug rosiglitazone are also being investigated. to stop aneurysms from enlarging enough to require repair. New studies suggest scientists may be on the threshold of success. But even now, men can and should protect themselves the old-fashioned ways, by avoiding tobacco, controlling blood pressure and cholesterol, and by eating right and exercising regularly to prevent obesity. Men who achieve all this can safely regard AAA as the shorthand for a popular auto club, not a risk to health and life. Is sex exercise? And is it hard on the heart? t some time in his life, nearly every man gets exercised about sex. And as many men get older, they wonder if sex is a good form of exercise or if it’s too strenuous for the heart. These questions may sound like locker room banter, but they are actually quite important—and they now have solid scientific answers. Treadmill vs. mattress To evaluate the cardiovascular effects of sexual activity, researchers monitored volunteers while they walked on a treadmill in the lab and during private sexual activity at home. In addition to 13 women, the volunteers included 19 men with an average age of 55. About three-quarters of the men were married, and nearly 70% had some form of cardiovascular disease; 53% were taking beta blockers. Despite their cardiac histories, the men reported exercising about four times a week, and they reported having sexual activity about six times a month on average. Researchers monitored heart rate and blood pressure during standard treadmill exercise tests and during “usual” sexual activity with a familiar partner at home. All the sex acts concluded with vaginal intercourse and male orgasm. Disappointedly perhaps, the treadmill proved more strenuous. During www.health.harvard.edu sex, the men raised their heart rates only 72% as high as they did on the treadmill, and the average blood pressure during sex was just 80% as high as during maximal treadmill exercise. On an intensity scale of 1 to 5, with 5 being the highest, men evaluated treadmill exercise as 4.6 and sex as 2.7. Sex was even less strenuous for women in terms of heart rate, blood pressure, and perceived intensity of exertion. Sex as exercise Men seem to spend more energy thinking and talking about sex than on the act itself. During sexual intercourse, a Sex and survival A man’s heart may swell with love, but is sex swell for his heart? Possibly so, according to a report from the United Kingdom. Researchers evaluated 918 men who were in good general health when the study began. Each man provided information on the frequency of his sexual activity; over the next 10 years, the men who reported three or more orgasms per week enjoyed a 50% lower death rate than the men who ejaculated less often. A report from the Massachusetts Male Aging Study agrees that sex may be protective. The subjects were men between 40 and 70 who were randomly selected residents of the Boston area. A total of 1,165 men were eligible for the study and agreed to participate. None of the men had cardiovascular disease when they enrolled in the 17-year study; 213 of the men had erectile dysfunction and were analyzed separately. Among the 952 men with intact erectile function, men who had sex once a month or less were 45% more likely to develop cardiovascular disease than the men who had sex two or more times a week. The link between sexual activity and cardiac health was not explained by conventional cardiac risk factors or a man’s satisfaction with his relationships. Although the American and British findings are heartening, they do not prove that sex itself is protective. Another explanation is that sexual activity reflects a general satisfaction with life that is good for health. And it’s even more likely that the men who had sex infrequently may have been burdened by social isolation or by smoking, drinking, drug abuse, or diseases that impair libido and potency. Men who choose to discuss these studies with their partners need not dwell on these major caveats. June 2011 | Harvard Men’s Health Watch | 5 This Harvard Health Publication was prepared exclusively for Bulfinch Medical Group - Purchased at http://www.health.harvard.edu/ man’s heart rate rarely gets above 130 beats a minute, and his systolic blood pressure (the higher number, recorded when the heart is pumping blood) nearly always stays under 170. All in all, average sexual activity ranks as mild to moderate in terms of exercise intensity. As for oxygen consumption, it comes in at about 3.5 METS (metabolic equivalents), which is about the same as doing the foxtrot, raking leaves, or playing ping pong. Sex burns about five calories a minute; that’s four more than a man uses watching TV, but it’s about the same as walking the course to play golf. If a man can walk up two or three flights of stairs without difficulty, he should be in shape for sex. Sex as sex Raking leaves may increase a man’s oxygen consumption, but it probably won’t get his motor running. Sex, of course, is different, and the excitement and stress might well pump out extra adrenaline. Both mental excitement and physical exercise increase adrenaline levels and can trigger heart attacks and arrhythmias, abnormalities of the heart’s pumping rhythm. Can sex do the same? In theory, it can. But in practice, it’s really very uncommon, at least during conventional sex with a familiar partner. Careful studies show that fewer than one of every 100 heart attacks is related to sexual activity, and for fatal arrhythmias the rate is just one in 200. Put another way, for a healthy 50-yearold man, the risk of having a heart attack in any given hour is about one in a million; sex doubles the risk, but it’s still just two in a million. For men with heart disease, the risk is 10 times higher—but even for them, the chance of suffering a heart attack during sex is just 20 in a million. Those are pretty good odds. How about Viagra? Until recently, human biology has provided unintentional (and perhaps unwanted) protection for men with heart disease. That’s because many of the things that cause heart disease, such as smoking, diabetes, high blood pressure, and abnormal cholesterol levels, also cause erectile dysfunction. The common link is atherosclerosis, which can damage arteries in the penis as well as in the heart. Sildenafil (Viagra), vardenafil (Levitra), and tadalafil (Cialis) have changed that. About 70% of men with erectile dysfunction (ED) respond to the ED pills well enough to enable sexual intercourse. Sex may be safe for most men with heart disease, but are ED pills a safe way to have sex? For men with stable coronary artery disease and well-controlled hyperten- sion, the answer is yes—with one very, very important qualification. Men who are taking nitrate medications in any form cannot use ED pills. This restriction covers all preparations of nitroglycerin, including long-acting nitrates; nitroglycerin sprays, patches, and pastes; and amyl nitrate. For tunately, other treatments for erectile function—such as the vacuum pump, alprostadil injections, or urethral tablets—are safe for men with heart disease, even if they are using nitrates. Safe sex Sex is a normal part of human life. For all men, whether they have heart disease or not, the best way to keep sex safe is to stay in shape by avoiding tobacco, exercising regularly, eating a good diet, staying lean, and avoiding too much (or too little) alcohol. Needless to say, men should not initiate sexual activity if they are not feeling well, and men who experience possible cardiac symptoms during sex should interrupt the sexual activity at once. With these simple guidelines and precautions, sex is safe for the heart— but it should be safe for the rest of the body, too. Sexually transmitted diseases pose a greater threat than sexually induced heart problems. When it comes to sex, men should use their heads as well as their hearts. Medical memo Cholesterol and prostate cancer A sk men about their top health worries, and most will put cholesterol and prostate cancer high on the list. That’s understandable, since unfavorable cholesterol levels contribute to heart attack and stroke, the first and fourth leading causes of death in America, and prostate cancer takes about 32,000 lives a year. Still, while most men understand the 6 | Harvard Men’s Health Watch | June 2011 link between cholesterol and cardiovascular disease, few suspect a link between cholesterol and cancer. New research is beginning to change that. though low cholesterol levels could protect the heart, they might increase the risk of cancer. Indeed, a series of population studies from the 1980s reported a higher incidence of cancer in people with low cholesterol levEarly worries Back when scientists were nailing els. This research also sparked worry down the relationship between high about cholesterol-lowering drugs, cholesterol and heart disease, they which was heightened when the first were also raising concerns that al- statin was released in 1987. www.health.harvard.edu This Harvard Health Publication was prepared exclusively for Bulfinch Medical Group - Purchased at http://www.health.harvard.edu/ Medical memo (continued) Fortunately, both fears proved unfounded. On further analysis, it turned out that having cancer causes cholesterol levels to fall, not the other way around. Doctors call this “reverse causation”; people with cancer eat less and lose weight, so their cholesterol levels fall after they develop cancer. And decades of experience with statins show that these widely used drugs do not increase the risk of malignancy. Early hopes Now that early worries have been dispelled, research is starting to raise hope that reducing cholesterol levels may help reduce the risk of certain cancers. Just as the statin drugs once fueled concern, they have now taken the lead in raising hope. Although there is no conclusive evidence that statin therapy lowers the overall risk of cancer, many, but not all, studies suggest these medications may reduce the risk of prostate cancer, particularly the aggressive tumors that matter most (see Harvard Men’s Health Watch, May 2011). New hints Two recent papers raise the possibility that low blood cholesterol levels may protect the prostate along with the heart. The Prostate Cancer Prevention Trial (PCPT) did not set out to study cholesterol, but to evaluate chemoprevention with finasteride (Proscar, generic), a drug approved to treat men with benign prostatic hyperplasia (see HMHW, June 2009). Beginning in 1993, researchers assigned 18,882 men with normal digital rectal exams (DREs) and prostate-specific antigen (PSA) levels below 3.1 nanograms per milliliter to receive either a placebo or 5 milligrams of finasteride a www.health.harvard.edu day. At the end of seven years, 5,615 men who had been taking the placebo and had undergone a prostate biopsy were eligible for the new cholesterol study. Each volunteer had his cholesterol measured at the start of the study, enabling the scientists to compare cholesterol levels with the result of prostate biopsies. Men with cholesterol levels below 200 milli- Now that early worries have been dispelled, research is starting to raise hope that reducing cholesterol levels may help reduce the risk of certain cancers. grams per deciliter enjoyed a 59% lower risk of developing aggressive prostate cancers than men with higher cholesterol levels. There was no relationship between cholesterol and less aggressive prostate cancers. The apparent protective effect of low cholesterol remained valid even after the researchers accounted for other factors that may affect both cholesterol levels and prostate cancer risk, including obesity, exercise, and red meat intake. Unfortunately, statin use was not recorded. The second study also involved a new analysis of data from a completed trial, in this case the AlphaTocopherol, Beta-Carotene Cancer Prevention (ATBC) Study. Starting in 1985, 29,093 male Finnish smokers volunteered to take vitamin E (alpha-tocopherol), beta carotene, both vitamins, or placebo. The trial ended in 1993 with the sobering finding that beta carotene increased the risk of lung cancer. But the story did not end there. Instead, the researchers continued to observe the men until 2003, and then looked back at the volunteers’ original cholesterol results to see if cholesterol levels predicted the subsequent development of cancer. In this study of smokers, low total cholesterol levels were linked to an increased risk of cancer in the first nine years of follow-up but not in later years, which strongly indicates reverse causation—in other words, a cancer that had not yet been diagnosed was causing a reduction in cholesterol levels. On the other hand, high levels of HDL (“good”) cholesterol were linked to an 11% reduction in the risk of prostate cancer, suggesting that what’s good for the heart may also be good for the prostate. But since men with high HDL levels were also leaner, more physically active, and consumed more alcohol, it’s not clear if the apparent protection was due to HDL itself or to lifestyle factors. Perspectives Both of these 2009 studies are interesting, but neither is perfect. The PCPT study suggests that low total cholesterol levels may reduce the risk of aggressive prostate cancer, but it did not take statin use into account. The ATBC study suggests that high HDL cholesterol levels may be protective, but it did not show that the apparent benefit was due to HDL itself rather than to lifestyle factors that boost HDL. Medical research is like a jigsaw puzzle. These new studies add small pieces, but it will take years for scientists to complete the picture of how cholesterol levels affect the prostate. While doctors work on the puzzle, though, men may be glad to know that their heart-healthy choices may also be prostate-healthy. June 2011 | Harvard Men’s Health Watch | 7 This Harvard Health Publication was prepared exclusively for Bulfinch Medical Group - Purchased at http://www.health.harvard.edu/ on call with Harvey B. Simon, M.D., Editor Excessive perspiration Q Compared to the problems your readers ask about, Men’s Health Watch, October 2008). Anxiety is another my issue may seem silly. But I hope you’ll give me relatively common cause. Because generalized hyperhidrosis has so many some advice, since it really is very annoying. I’m troubled possible causes, it’s important to get a medical evaluaby excessive sweating. tion so any underlying problems can be tackled headAlthough it’s not a major illness, excessive sweat- on. If doctors can’t find any underlying problem, they ing is far from trivial. In fact, it can be very embar- may try to control the sweating with an anticholinergic rassing, and it can interfere with healthy interpersonal medication. Because these drugs have uncomfortable side effects (including dry mouth, constipation, and relationships. Call it by its medical name, hyperurinary retention), they must be used with care hidrosis, and your problem may get the respect and are generally reserved for very troublesome it deserves. sweating problems. Sweating itself is both normal and necessary. In localized hyperhidrosis, the excess sweating It’s one of the body’s two main ways of shedis restricted to confined areas of the body, typiding the heat that is a byproduct of our metabocally the palms, soles, and armpits. Underlying lism; the other is the conduction of heat from diseases are rarely responsible. Instead, common the skin to the surrounding air. When the air triggers include intense emotion (particularly is hot, it’s hard to dissipate heat by conduction. anxiety) and strong odors or flavors (particularly When the air is humid, sweat won’t evaporate, making heat loss by perspiration ineffective. So the spicy foods, citrus fruit, coffee, chocolate, and apples). discomfort of summer is not due to heat or humidity, Often, though, it’s not possible to pinpoint the cause of localized hyperhidrosis, but in all cases, heat makes the but both. Without sweating, we’d burn up. But people with problem worse. Localized hyperhidrosis can be hard to control. If hyperhidrosis sweat more than is necessary to regulate body temperature. Excessive perspiration comes ordinary antiperspirants don’t help, a prescription antiin two forms, generalized hyperhidrosis and local- perspirant containing 20% aluminum chloride hexahydrate (Drysol) may. But for some patients, the best ized hyperhidrosis. When heat, humidity, and exercise trigger sweat- remedy involves periodic injections of tiny amounts of ing all over the body, it’s a normal response to ther- botulinum toxin type A (Botox). Since your question doesn’t give details about your mal stress. But generalized sweating can also be a sign of metabolic disorders (such as an overactive sweating problem, it’s not possible to point you in a thyroid or diabetes), infections (ranging from the flu particular direction. And since I can’t offer specific to tuberculosis), or certain tumors (particularly lym- advice, I’m reduced to offering a generic tip for excesphomas). Generalized hyperhidrosis can also result sive sweating: stay calm—and, if possible, cool. from alcohol abuse (especially during alcohol withdrawal) or from a medication (the antidepressant venlafaxine, or Effexor, is an example). Hormonal events are an even more common cause, particularly menopause in women and androgen-deprivation therapy in men with prostate cancer (see Harvard A Send us a question for On call Visit the Harvard Men’s Letter blog online: www.health.harvard.edu/blog 8 | Harvard Men’s Health Watch | June 2011 Harvey B. Simon, M.D., Editor, Harvard Men’s Health Watch By mail: Harvard Men’s Health Watch 10 Shattuck St., 2nd Floor Boston, MA 02115 By e-mail: [email protected] (Please write “On call” in the subject line.) Because of the volume of correspondence we receive, we can’t answer every question, nor can we provide personal medical advice. This Harvard Health Publication was prepared exclusively for Bulfinch Medical Group - Purchased at http://www.health.harvard.edu/










© Copyright 2026