
O P T
An Independent Licensee of the
Blue Cross and Blue Shield Association.
APPENDIX G
OPTOMETRY & OPTICIAN GUIDELINES
Acknowledgement: Current Procedural Terminology (CPT®) is copyright 2014
American Medical Association. All Rights Reserved. No fee schedules, basic
units, relative values or related listings are included in CPT. The AMA assumes no
liability for the data contained herein. Applicable – ARS/DFARS Restrictions Apply
to Government Use.
NOTE:
The revision date appears in the footer of the document. Links within
the document are updated as changes occur throughout the year.
GENERAL CODING INFORMATION
Use of Modifiers for Identifying Specific Eye
•
Left and Right Eyes
When using modifiers to identify the specific eye treated you should use one
of the following immediately after the procedure code:
RT = Right
LT = Left
Each line should be coded separately using only one of the modifiers on
each line.
Each line should reflect 1 unit.
BCBSKS-Business Procedure Manual
Appendix G: Optometry and Optician Guidelines
Current Procedural Terminology © 2014 American Medical Association. All Rights Reserved.
NOTE: Codes published herein are current on the revision date and are subject to change.
Contains Public Information
Page G-1
Revision Date: April 2014
•
Left, Right, Upper, and Lower Eyelids
When using modifiers to identify the specific eyelid treated you should use
one of the following immediately after the procedure code:
•
E1 = Left upper eyelid
E2 = Left lower eyelid
E3 = Right upper eyelid
E4 = Right lower eyelid
Multiple Modifiers per Procedure Code
DO NOT use multiple modifiers on one line of service (i.e., RTE3; E1E2;
LTE3; RTLT). Doing so will not allow your claim to process and will delay
your payment.
Eye Examinations
•
Routine Eye Examinations (Standard Benefit)
One of the diagnoses from this list should be submitted in the 2300 HI01-2 or in
the first position of Box 21 for our system to recognize that the service is
routine.
Diagnoses Considered Routine
Disorders of refraction and accommodation
367.0
367.1
367.20
367.21
367.32
367.4
V72.0
Hypermetropia
Myopia
Astigmatism, unspecified
Astigmatism, regular
Aniseikonia
Presbyopia
Examination of eyes and vision
BCBSKS-Business Procedure Manual
Appendix G: Optometry and Optician Guidelines
Current Procedural Terminology © 2014 American Medical Association. All Rights Reserved.
NOTE: Codes published herein are current on the revision date and are subject to change.
Contains Public Information
Page G-2
Revision Date: April 2014
Procedure Codes
Routine Eye Examination Procedure Codes:
92002 Intermediate Eye Exam, New Patient
92004 Comprehensive Eye Exam, New Patient
92012 Intermediate Eye Exam, Established Patient
92014 Comprehensive Eye Exam, Established Patient
Please Note: The new BlueCare plans may cover routine exams under
the pediatric vision coverage for members up to age 19. Be sure to check
Availity for eligibility benefits regarding specific coverage.
Reimbursement
The reimbursement will be based on the MAP for the 92012, not on the code
billed.
Refraction 92015 with Routine Eye Examination
The refraction may be billed separately; however, the allowance for the
refraction will be content of service to the routine exam.
NOTE: For FEP – If the 92015 is done for a routine diagnosis code, it will
deny as non-covered (patient responsibility).
Number of Routine Eye Examinations per Benefit Period
Most patient contracts limit the routine eye exam benefit to one per
benefit year.
Other contracts limit this benefit to one every two years.
Please use the eligibility feature in Availity or call Customer Service at
(800) 432-0272 to ascertain the limit for a specific patient.
Contact lens examination, testing, fitting and three follow-up visits;
contact checks
Please Note: Please see Other Services/Contact Lens for Medical
Conditions, further in this section if you are dispensing a lens for a medical
condition.
BCBSKS-Business Procedure Manual
Appendix G: Optometry and Optician Guidelines
Current Procedural Terminology © 2014 American Medical Association. All Rights Reserved.
NOTE: Codes published herein are current on the revision date and are subject to change.
Contains Public Information
Page G-3
Revision Date: April 2014
Contact exam, testing, fitting and follow-up visits
If there is no vision hardware coverage these services are considered noncovered and are patient financial responsibility.
You do not have to bill the contact exam, testing, fitting, follow-up visits to
us, unless you want us to deny the service for benefit of notifying the
patient. If there is no hardware coverage, then you may bill the patient at
the time of service for the contact exam, testing, fitting, and follow-up visits.
Also, “Blue Shield Contact Exam, Testing, Fitting, Follow-Up Visits Patient
Financial Responsibility” Form is at the end of this section of the manual. It
is suggested that you keep the signed form in the patient’s file for future
reference if the patient questions whether they were informed.
If billing for this service and lenses are not dispensed, you should code
your claim as follows: 92310-92317.
Please Note: Some providers may consider the AMA-CPT procedure
codes of 92310, 92311, 92312, 92313, 92314, 92315, 92316, 92317 and
92325 to include the material. BCBSKS does not include the material
in these procedure codes.
We look at these codes as testing, fitting and follow-up only. Do not
include your materials; material should be coded with the appropriate “V”
HCPCS procedure codes.
If billing for this service and lenses are dispensed, you should code your
claim as follows:
92310 for the professional portion
Vxxxx for the lenses dispensed
If billing for a contact check, which is usually non-covered as stated under
contact exam without hardware coverage, you should code your claim as
follows and we will deny as patient financial responsibility if there is no
vision correction benefit:
92310 for the professional portion
Vxxxx for the lenses dispensed
BCBSKS-Business Procedure Manual
Appendix G: Optometry and Optician Guidelines
Current Procedural Terminology © 2014 American Medical Association. All Rights Reserved.
NOTE: Codes published herein are current on the revision date and are subject to change.
Contains Public Information
Page G-4
Revision Date: April 2014
Content of Service of Routine Eye Examination
The following services are considered part of the routine eye exam and
should not be billed separately:
Preparation of patient record with routine demographic information.
Analysis of power of present glasses, if any (manual or computerized
automatic lens analyzer).
Case history of symptoms, past medical/dental history, present
medications and familial eye/vision problems, etc.
Visual acuity testing at 20' (Snellen chart) and 14” to 16” (Near-point
Snellen card), both unaided and present glasses, if any.
Color vision testing with color plates, either monocularly or binocularly
(Ishara Color Vision Plates).
Tonometry, either by Schiotz indentation, MacKay-Marg Electronic
Applanation, Goldmann Applanation or Non-Contact Methods
(Tonometer).
Objective measurement of static (distance) refractive error by either
retinoscopy or computerized autorefractor (retinoscope or autorefractor).
(This service can be broken out on your claim and we will combine the
charge with the eye exam procedure code charge and only allow up to the
MAP for the exam procedure code or your charge whichever is the lesser.)
Blood pressure screening (sphygmonanometer).
Cover test for gross muscle imbalances (occluder).
Analysis of eye muscle movements, tracking and convergence (penlight).
External ocular examination of lids and adnexae (penlight).
Biomicroscopy of anterior segment-lid margins, corneas, iris, conjunctiva,
estimation of anterior chamber depth, lens clarity, shallow vitreous
(biomicroscope).
Ophthalmoscopy, direct or indirect, from posterior poles, optic discs,
maculas, and peripheral retinas (direct or indirect ophthalmoscope).
Subjective coordination of testing for measurement of lateral or vertical
imbalances as well as near focusing ability (phoroptor, trial lens set and/or
phorometer).
Screening fundus photography (fundus camera).
Photographs – including external ocular photography.
Screening for defects in central and/or peripheral field of vision (arc
perimeter, tangent screen or computerized auto field analyzer).
Ophthalmometry for measuring corneal curvature and for presence of
scarring and/or keratoconus (ophthalmometer).
BCBSKS-Business Procedure Manual
Appendix G: Optometry and Optician Guidelines
Current Procedural Terminology © 2014 American Medical Association. All Rights Reserved.
NOTE: Codes published herein are current on the revision date and are subject to change.
Contains Public Information
Page G-5
Revision Date: April 2014
•
Analysis of findings, consultation, determination of course of treatment and
writing of prescription.
Routine corneal topography.
Other routine eye examination services.
Determination of refractive state.
Medical Eye Examinations
Medical Diagnosis on Claim Form:
A medical diagnosis must be submitted in the 2300 HI01-2 or appear in the
first position in Box 21 of the claim form.
Valid Procedure Codes for Medical Eye Examinations
92002
92004
92012
92014
99201
99202
99203
99204
99205
99211
99212
99213
99214
99215
Refraction 92015 with Medical Eye Examination
This code may be billed separately, and reimbursement will be based on the
appropriate year MAP for the code.
Medical Eye Examinations for Patients with Diabetes
Diabetic Diagnosis Codes For All Policies:
One of the following must be submitted in the 2300 HI01-2 or in the first
diagnosis position in Box 21 of the claim form:
250.0 - 250.9
357.2
362.01
362.02
362.03
362.04
362.05
362.06
362.07
366.41
Diabetes mellitus
Polyneuropathy in diabetes
Background diabetic retinopathy
Proliferative diabetic retinopathy
Nonproliferative diabetic retinopathy
Mild nonproliferative diabetic retinopathy
Moderate nonproliferative diabetic retinopathy
Severe nonproliferative diabetic retinopathy
Diabetic macular edema
Diabetic cataract
BCBSKS-Business Procedure Manual
Appendix G: Optometry and Optician Guidelines
Current Procedural Terminology © 2014 American Medical Association. All Rights Reserved.
NOTE: Codes published herein are current on the revision date and are subject to change.
Contains Public Information
Page G-6
Revision Date: April 2014
•
Medical Emergency Eye Care
•
Medical Emergency Diagnosis on Claim Form:
A medical emergency diagnosis must be submitted in the 2300 HI01-2 or
appear in the first position in Box 21 of the claim form.
Other Medical Services
How to code your services for Medical Vision Correction Hardware Also
see “DISPENSING” further in this section of the manual
Contact Lens for Medical Conditions
Contracts that exclude coverage for contact lenses for routine vision
correction may cover lenses for the treatment of a medical condition. If the
diagnosis is on the approved diagnosis list you should apply the following:
Simple condition
Use 92002 through 92014 or the appropriate evaluation and
management code.
Use 92071 for the fitting of the bandage lens. Code 99070 (bandage
lens) will deny content of service when billed with 92071.
More complex conditions
Use E & M (99201 through 99215) or ophthalmology examination
(92002 through 92014) procedure code for the exam.
Use 92310 – 92317 for the fitting of the lens.
Use 92325 for the modification of the lens.
Use a V code for the supply of the lens.
Use 92072 for fitting of the lens when using a V code for dispensing
the lens.
BCBSKS-Business Procedure Manual
Appendix G: Optometry and Optician Guidelines
Current Procedural Terminology © 2014 American Medical Association. All Rights Reserved.
NOTE: Codes published herein are current on the revision date and are subject to change.
Contains Public Information
Page G-7
Revision Date: April 2014
Keratoconus
Valid Diagnosis Codes
Please submit one of the following diagnoses in the 2300 HI01-2 or in
the first diagnosis position in Box 21 of the claim form when billing for
care for this condition
371.60 Keratoconus, unspecified
371.61 Keratoconus, stable condition
371.62 Keratoconus, acute hydrops
Office Visit Procedure Codes for Keratoconus Patients
See Medical Eye Examination and the codes listed there.
Contact Lens Procedure Code for Keratoconus Patient Care
♦
♦
♦
Use 92072 for the fitting of the lens.
Use a V code for the dispensing of the lens.
Conventional soft contact lenses are not allowed for diagnosis of
keratoconus.
Medical Records for Keratoconus Claims
Medical records, in most cases, are not needed. You may send your
claims in without them and if, for some reason, we need them we will
request them.
Postoperative Care for Cataract Surgery
BCBSKS will cover these services when performed by an optometrist if
the surgeon does not bill the global fee for the surgery including pre
and postoperative care. Following are the guidelines for billing:
♦
♦
♦
♦
Use the appropriate procedure code for the surgery.
Use modifier 55 with the procedure code for the surgery.
The surgeon must use 54 modifier on his/her portion with the same
procedure code. If he/she does not, the claim will be denied as
already paid to another provider. (NOTE: Date of Service must
reflect Date of Surgery)
Units of service should equal 1 (2400 SV104 or Box 24G).
BCBSKS-Business Procedure Manual
Appendix G: Optometry and Optician Guidelines
Current Procedural Terminology © 2014 American Medical Association. All Rights Reserved.
NOTE: Codes published herein are current on the revision date and are subject to change.
Contains Public Information
Page G-8
Revision Date: April 2014
♦
♦
Date Assumed/Relinquished Care is submitted in the 2300 DTP
and actual number of days should be submitted in the 2300 NTE or
in Box 19.
Claim must show date of surgery (2300 DTP or Box 24A).
See Dispensing further in this section of the manual for
cataract diagnoses and other pertinent guidelines for vision
correction hardware.
Glaucoma Screening
G0117 Glaucoma screening for high-risk patients furnished by an
optometrist or ophthalmologist
G0118 Glaucoma screening for high-risk patients furnished under the
direct supervision of an optometrist or ophthalmologist
Both codes are considered content of the eye exam if performed on the
same date
If either procedure is performed by itself, it will be reviewed for possible
coverage based on payment criteria for 92002.
Pachymetry
Please see medical policy at BCBSKS website link below:
Pachymetry
Visual Fields
Gross Visual Fields: Considered content of service of the routine eye
examination and should not be billed separately.
Visual Fields (92081, 92082, 92083) codes are unilateral or bilateral;
which means units of service should reflect 1. When billing visual
fields for a medical condition in addition to a routine or medical eye
examination you must make sure that the line item of service points to the
correct diagnosis for coverage to be considered.
BCBSKS-Business Procedure Manual
Appendix G: Optometry and Optician Guidelines
Current Procedural Terminology © 2014 American Medical Association. All Rights Reserved.
NOTE: Codes published herein are current on the revision date and are subject to change.
Contains Public Information
Page G-9
Revision Date: April 2014
In the 2400 SV107 or Box 24E, the number placed here must correspond
to the position number of the medical diagnosis in the 2300 HI or Box 21
that supports the performance of the visual fields. (The medical diagnosis
that warrants the visual field being performed should be submitted in
2300 HI01-2 or the first position in Box 21; then the number “1” must be
indicated for the line billing the visual fields in the 2400 SV107 or Box
24E.)
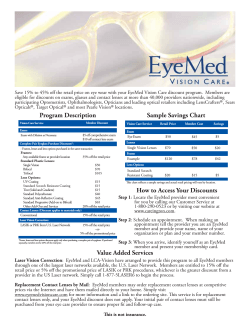
Example of diagnosis coding and line item indications:
21. DIAGNOSIS OR NATURE OF ILLNESS OR INJURY
1.
/ 365.11
2.
/ 367.1
24.
3.
4.
A
DATES OF SERVICE
From
MM DD
To
YY MM
DD
YY
021509
021509
22. MEDICAID RESUBMISSION CODE
/_______
23. PRIOR AUTHORIZATION NUMBER
/_______
B
C
D
E
F
G
H
I
J
K
Place
of
Service
Type
of
Service
PROCEDURES, SERVICES, OR SUPPLIES
DIAGNOSIS
CODE
DAYS
OR
UNITS
EPSDT
EMG
COB
$ CHARGES
RESERVED
FOR
LOCAL USE
11
11
92012
92082
2
1
Fundus Photography
Please see medical policy at BCBSKS website link below:
Fundus Photography
Fundus Photography Screening
This service will be denied as content of service of the eye examination
when billed with a routine diagnosis.
Do not use 92250 for fundus photography screenings. Screenings
should not be billed separately.
Fundus Photography with Interpretation and Report 92250:
This service will be considered for payment if the diagnosis is other than
routine.
If you are following a medical condition you may bill for this service
using 92250 if the service includes interpretation and report. The
report must be written and maintained in the patient’s file.
BCBSKS-Business Procedure Manual
Appendix G: Optometry and Optician Guidelines
Current Procedural Terminology © 2014 American Medical Association. All Rights Reserved.
NOTE: Codes published herein are current on the revision date and are subject to change.
Contains Public Information
Page G-10
Revision Date: April 2014
As of January 1, 2014, this procedure code is considered bilateral.
Therefore, if providing bilaterally or unilaterally, units of service should
be 001.
When 92250 for a medical condition in addition to a routine or medical
eye examination you must make sure that the line item of service
points to the correct diagnosis for coverage to be considered.
In the 2400 SV107 or Box 24E, the number placed here must
correspond to the position number of the medical diagnosis in the
2300 HI or Box 21 that supports the performance of the fundus photos.
(The medical diagnosis that warrants the fundus photos being
performed should be submitted in 2300 HI01-2 or in the first position in
Box 21; then the number “1” must be indicated for the line billing the
fundus photos in the 2400 SV107 or Box 24E.)
Computerized Corneal Topography: 92025
Please see the medical policy for this procedure code at the link below:
Corneal Topography/Computer-Assisted Corneal Topography/Photokeratoscopy
Optomap
The guidelines for fundus photography, as previously outlined in this section,
apply to Optomap or any similar equipment.
Photodynamic Therapy
This service should be coded with 67221
This service is considered for reimbursement for age related macular
degeneration (AMD).
Services for other diagnoses are subject to medical review.
BCBSKS-Business Procedure Manual
Appendix G: Optometry and Optician Guidelines
Current Procedural Terminology © 2014 American Medical Association. All Rights Reserved.
NOTE: Codes published herein are current on the revision date and are subject to change.
Contains Public Information
Page G-11
Revision Date: April 2014
Lacrimal Duct Implants
Temporary Implant
A4262
Type of service 9
Indicate three digit units of service
Insertion of Implant
68761
Type of service 2
Indicate three digit units of service
Permanent Implant
A4263
Indicate three digit units of service
Reimbursement
Full MAP will be allowed for the plugs
Full MAP will be allowed for the first insertion
½ MAP will be allowed for the second insertion
Ophthalmic Diagnostic Imaging:
92132 – Scanning Computerized Ophthalmic Diagnostic Imaging, anterior
segment, with Interpretation and Report, unilateral or bilateral. This code
is considered Experimental and Investigational (E/I).
Please see Medical Policy Scanning Computerized Ophthalmic
Diagnostic Imaging for:
92133 – Scanning Computerized Ophthalmic Diagnostic Imaging,
posterior segment, with Interpretation and Report, unilateral or
bilateral, optic nerve.
92134 – Retina
Vision Therapy
Most member policies do not cover this service. Please call the Benefit
Information Department to determine if your patient has the coverage.
BCBSKS-Business Procedure Manual
Appendix G: Optometry and Optician Guidelines
Current Procedural Terminology © 2014 American Medical Association. All Rights Reserved.
NOTE: Codes published herein are current on the revision date and are subject to change.
Contains Public Information
Page G-12
Revision Date: April 2014
Dispensing
•
Assignment of Benefits (pertains to Opticians only)
BCBSKS does not offer CAP contracts to opticians, hearing aid dispensers,
private duty registered nurses or private duty licensed practical nurses since
there are so few patient contracts that cover their services.
Your patients cannot assign the payment of the benefits to you.
•
•
Materials
The AMA-CPT procedure codes of 92310, 92311, 92312, 92313, 92314,
92315, 92316, 92317, and 92325 - 92326 include the material by AMA-CPT
definition.
BCBSKS does not include the material in these procedure codes.
We look at these codes as testing, fitting and follow-up only. Do not include
your materials; they should be coded with the appropriate
“V” HCPCS procedure codes.
Coverage
Most patients’ contracts only cover lenses, frames or contact lenses when there
has been cataract surgery or other medical conditions.
Medical and Routine Vision Correction
Valid Procedure Codes
Lenses, Frames, Contact Lenses
Use current HCPCS codes and nomenclature listing for appropriate
V-code for lenses, frames, and contact lenses for all claims
submissions for dispensing. When using code V2781, please indicate
whether it is for bifocals or trifocals, otherwise claim will be returned
asking for clarification. If billing two lenses, use the appropriate code
as one line item and indicate two units.
BCBSKS-Business Procedure Manual
Appendix G: Optometry and Optician Guidelines
Current Procedural Terminology © 2014 American Medical Association. All Rights Reserved.
NOTE: Codes published herein are current on the revision date and are subject to change.
Contains Public Information
Page G-13
Revision Date: April 2014
Eye Glass Lenses Guidelines
•
Dispensing
Use AMA-CPT for the professional fee for dispensing for all claims
submissions for dispensing. Do not include the charge for the material
in this fee.
Use appropriate HCPCS “V” procedure codes, remembering to code the
number of units per lens if more than one of the same power.
Coverage after Cataract Surgery
Some BCBSKS contracts will cover vision correction hardware after there has
been cataract surgery.
Diagnoses Codes for After Cataract Surgery
379.31
743.35
V43.1
•
Subluxation of lens
Congenital aphakia
Organ or tissue replaced by other means (lens) pseudophakos
An initial pair of eyeglasses, frames, and lenses (or contact lenses) is
reimbursed only when surgery for age related, congenital, or traumatic
cataracts has been performed to correct visual defects resulting from
aphakia or pseudophakia. Reimbursement will only be made for the above
diagnoses.
When cataract surgery is performed on only one eye, reimbursement will still
be made on the Frames, but only on the lens for the eye on which the
surgery was performed.
These guidelines are not applicable to routine vision hardware
benefits.
Content of Service for Dispensing:
Shipping and handling
Taxes
Fitting
Measuring
Other dispensing services
BCBSKS-Business Procedure Manual
Appendix G: Optometry and Optician Guidelines
Current Procedural Terminology © 2014 American Medical Association. All Rights Reserved.
NOTE: Codes published herein are current on the revision date and are subject to change.
Contains Public Information
Page G-14
Revision Date: April 2014
•
Date of Service
When dispensing frames and/or lenses the date of service must be the date the
items were dispensed, not the date when they were ordered.
•
Deluxe Items
See “Deluxe and Cosmetic Vision Correction Waiver” form at the end of this
section.
•
S0500 Disposable Contacts
This code should not be used for any other type of lenses. Indicate number
of lenses being dispensed in the units field of the claim form.
20 lenses = 020 units of service
6 lenses = 006 units of service
On a claim attachment indicate the number of days, weeks, or months
supply.
•
V Codes for Non-Disposable Contacts
You should use the appropriate V code(s) from the HCPCS Listing
•
V2710 Slab Off Prisms
This service can be considered for separate reimbursement.
Code one line of service with modifier 50 for bilateral procedure.
BCBSKS-Business Procedure Manual
Appendix G: Optometry and Optician Guidelines
Current Procedural Terminology © 2014 American Medical Association. All Rights Reserved.
NOTE: Codes published herein are current on the revision date and are subject to change.
Contains Public Information
Page G-15
Revision Date: April 2014
Blue Cross and Blue Shield of Kansas, Inc
*Independent Licensees of the Blue Cross and Blue Shield Association.
DELUXE and COSMETIC WAIVER for MEDICAL CONDITION
Eyeglasses and Contact Lenses
This form does not apply to Boeing patients.
The provider must document in the patient record the discussion with the patient regarding the following
services.
ITEM
CHARGE
ITEM
CHARGE
Deluxe Portion of Frame
$
Metal Suspension
$
Oversizing
$
Engraving/Monogramming
$
Beveling
$
Photochromatic Tint
$
Facets
$
Tints (excluding Rose 1-2)
$
Roll and Polish
$
Disposable Sunglasses
$
Frosting
$
Scratch Resistant Coating
$
Lip
$
Disposable Lenses Portion
$
Nylon String Mounting
$
Contact Lens Tint
$
Grooving
$
Progressive Lenses Portion
$
Notching
$
Other (identify item)
$
Drilling
$
Other (identify item)
$
Dispensing Deluxe/Cosmetic Portion
$
Subtotal This Side
$
Subtotal This Side
$
Subtotal Left Side
$
Grand Total
$
BCBSKS, Inc. benefits for vision correction services have some limitations. They will only reimburse for the standard appliance
and if I choose to have deluxe or cosmetic service, I understand that I am financially responsible for those differences as outlined
above. I realize that the standard item is available but it is my choice to have the more deluxe or cosmetic item(s). I also
understand that the provider of the item(s) has the option to request this amount at the time the item is ordered, at the time it is
delivered or at their normal billing time. The arrangements made to pay this amount are solely between myself and the provider
of the item(s). I understand that BCBSKS, INC. has any involvement.
Patient Signature
Date
Provider Please:
Keep original in patient’s file.
Give copy to patient.
Send copy with claim.
Use V2799 NOC used for Deluxe/Cosmetic portion with one total sum for this on the claim form. On claim attachment indicate
the following: V2799 = deluxe/cosmetic portion
4. Use V2020 for the standard frame portion.
5. Use appropriate dispensing, lens, and other covered services procedure codes from AMA-CPT and HCPCS for the
remainder of the services or items.
6. Always use modifier 22 when submitting any claim attachment.
1.
2.
3.
15-344 08/03
BCBSKS-Business Procedure Manual
Appendix G: Optometry and Optician Guidelines
Current Procedural Terminology © 2014 American Medical Association. All Rights Reserved.
NOTE: Codes published herein are current on the revision date and are subject to change.
Contains Public Information
Page G-16
Revision Date: April 2014
REVISIONS
02/01/2011
Changed revision date to “February 2011” from “June 2010.”
Page G-13 –
• Under bulleted code 92132, added a sub-bullet:
This code is considered Experimental and Investigational (E/I).
Units of 002 should be used if billing for bilateral procedure.
• Under bulleted code 92134, changed second sub-bullet to “001 units,” added
“or unilateral,” and deleted “procedure.” Previous text read:
Page G-15 –
Under bullet “Lenses, Frames, Contact Lenses,” added the following verbiage:
When using code V2781, please indicate whether it is for Bifocals or Trifocals, otherwise claim
will be returned asking for clarification.
06/13/2011
Changed revision date to “June 2011” from “February 2011.”
Page G-12 –
Under bullet, “Computerized Corneal Topography: 92025,” removed the three
sub-bullets (listed below), and added the link to the corresponding medical policy.
Use modifier 22 when submitting any claim attachment.
07/14/2011
This service will be denied as content of service of the eye examination when billed
with a routine diagnosis.
The service will be considered for reimbursement if billed with a medical diagnosis.
Changed revision date to “July 2011” from “June 2011.”
Page G-8 –
Under “Post Operative Care for Cataract Surgery,” 4th bullet did read:
♦
Units of service must reflect the number of post-op care days assumed. (Date of
surgery counts as day #1.)
Added a new 5th bullet.
The final bullet on the page did read:
♦
04/09/2012
Claim must show date of service range ("From and To" in Box 24A) that equals the
number of units indicated in Box 24G.
Changed revision date to “April 2012” from “July 2011.”
Changed copyright date in the footer for Current Procedural Terminology to 2011.
Previous copyright date was 2010.
Page G-3 –
Under “Eye Examinations” the third bullet on page G-3, the refraction will now be
content of service to the routine exam.
The third bullet did read:
Refraction 92015 with Routine Eye Examination
The refraction may be billed separately; however, the allowance for the combined charges
(examination and refraction) will not exceed the maximum allowable payment for the routine
eye examination.
BCBSKS-Business Procedure Manual
Appendix G: Optometry and Optician Guidelines
Current Procedural Terminology © 2014 American Medical Association. All Rights Reserved.
NOTE: Codes published herein are current on the revision date and are subject to change.
Contains Public Information
Page G-17
Revision Date: April 2014
REVISIONS
4/09/2012,
continued
6/22/2012
Page G-8 –
Under 3rd arrow bullet “Contact Lens Procedure Code for Keratoconus Patient
Care”, a third sub-bullet was added. This information was published in the Blue
Shield Report S-2-11 newsletter, dated March 7, 2011.
Changed revision date to “June 2012” from “April 2012”.
Page G-7 –
Under bullet titled “Simple condition such as abrasion”, the second bullet was
changed. The word code was changed from 92070 to 92071, “and dispensing”
was deleted, and the word “bandage” was added.
Previous verbiage read:
Use 92070 for the fitting and dispensing of the lens.
Under bullet titled “More complex conditions”, added a fourth bullet.
Page G-8 –
Under bullet, “Keratoconus”, a link to the medical policies was added.
Page G-9 –
Under “Pachymetry”, verbiage was deleted and a link to the medical policies was
added.
Previous wording:
Pachymetry will not be allowed when scientifically demonstrated effect upon
management of a disease is not documented. As an example, if the diagnosis of
glaucoma is established the results of a pachymetry test would not be of value for
clinical management.
Page G-13 –
Deleted information on Ophthalmic Diagnostic Imaging.
The section did read:
6/27/2012
Ophthalmic Diagnostic Imaging:
92132 – Scanning Computerized Ophthalmic Diagnostic Imaging with
Interpretation and Report, unilateral or bilateral.
This code is considered Experimental and Investigational (E/I).
92133 – Scanning Computerized Ophthalmic Diagnostic Imaging, posterior
segment with Interpretation and Report, unilateral or bilateral, optic nerve.
92134 - Retina
This service is covered for 365.00 through 365.9 Glaucoma
Units of 001 should be used if billing for bilateral or unilateral.
Other diagnoses must be submitted with modifier 22 and medical records. Claims
without medical records will be denied.
Page G-3 –
Under the third bold bullet titled “Refraction 92015 with Routine Eye
Examination”, a note was added for clarification of FEP processing.
BCBSKS-Business Procedure Manual
Appendix G: Optometry and Optician Guidelines
Current Procedural Terminology © 2014 American Medical Association. All Rights Reserved.
NOTE: Codes published herein are current on the revision date and are subject to change.
Contains Public Information
Page G-18
Revision Date: April 2014
REVISIONS
6/27/2012,
continued
1/31/2013
Page G-8 –
The word “conventional” was added to the third bullet under “Contact Lens
Procedure Code for Keratoconus Patient Care”.
Changed the revision date to “January 2013” from “June 2012”.
Changed the copyright date for Current Procedural Terminology to 2012.
Updated links within the manual.
Throughout the manual, added corresponding electronic loop and segment
information to all references to HCFA 1500 claim form box numbers.
Page G-2 –
Removed “(Excluding Boeing)” from the “Eye Examinations” heading.
Page G-4 –
Removed the bullet at the bottom of the page:
• See Boeing Traditional for their guidelines.
Page G-5 –
Removed “(other than Boeing)” from the title at the top of the page.
Page G-9 –
First bullet on the page, change the word “Accepted” to “Assumed”, added the
word “Care”.
Old wording:
♦ Date Accepted/Relinquished and actual number of days should be in box 19 or the
electronic narrative.
Page G-14 –
Under the sub-bullet, “Lenses, Frames, Contact Lenses”, at the bottom of the
page, added the final sentence, “If billing two lenses….”
Pages G-16-19 –
Deleted all instructions for Boeing.
The section did read:
Boeing
•
Boeing Routine Eye Examinations
Boeing Procedure Codes and Diagnoses
These products follow the same coding guidelines as regular BCBSKS claims.
Applicability of CAP Contract to Boeing Vision Exam
When a provider is CAP contracting the CAP write-off amounts apply, whether the
provider is Boeing Vision Exam (BVE) or not.
Content of Service for a Boeing Routine Eye Examination
Boeing Traditional:
The following services are considered part of the routine eye exam and should not be
billed separately.
Preparation of patient record with routine demographic information.
Analysis of power of present glasses, if any (manual or computerized automatic lens
BCBSKS-Business Procedure Manual
Appendix G: Optometry and Optician Guidelines
Current Procedural Terminology © 2014 American Medical Association. All Rights Reserved.
NOTE: Codes published herein are current on the revision date and are subject to change.
Contains Public Information
Page G-19
Revision Date: April 2014
REVISIONS
1/31/2013,
continued
analyzer).
Case history of symptoms, past medical/dental history, present medications and familial
eye/vision problems, etc.
Visual acuity testing at 20' (Snellen chart) and 14” to 16” (Near-point Snellen card),
both unaided and present glasses, if any.
Color vision testing with color plates, either monocularly or binocularly (Ishara Color
Vision Plates).
Tonometry, either by Schiotz identation, MacKay-Marg Electronic Applanation,
Goldmann Applanation or Non-Contact Methods (Tonometer).
Objective measurement of static (distance) refractive error by either retinoscopy or
computerized autorefractor (retinoscope or autorefractor). (This service can be broken
out on your claim and we will combine the charge with the eye exam procedure code
charge and only allow up to the MAP for the exam procedure code or your charge
whichever is the lesser.)
Blood pressure screening (sphygmonanometer).
Cover test for gross muscle imbalances (occluder).
Analysis of eye muscle movements, tracking and convergence (penlight).
External ocular examination of lids and adnexae (penlight).
Biomicroscopy of anterior segment-lid margins, corneas, iris, conjunctiva, estimation of
anterior chamber depth, lens clarity, shallow vitreous (biomicroscope).
Ophthalmoscopy, direct or indirect, from posterior poles, optic discs, maculas, and
peripheral retinas (direct or indirect ophthalmoscope).
Subjective refraction for correction of distance and ear refractive errors (phoroptor or
trail lens set).
Subjective coordination of testing for measurement of lateral or vertical imbalances as
well as near focusing ability (phoroptor, trial lens set and/or phorometer).
Screening fundus photography (fundus camera).
Screening for defects in central and/or peripheral field of vision (arc perimeter, tangent
screen or computerized auto field analyzer).
Ophthalmometry for measuring corneal curvature and for presence of scarring and/or
keratoconus (ophthalmometer).
Analysis of findings, consultation, determination of course of treatment and writing of
prescription.
Comprehensive biomicroscopy for contact lens evaluation.
Keratometry for contact lens evaluation
Fluorscein study for contact lens evaluation
Anatomical measurements for contact lens evaluation.
Fitting of diagnostic lenses.
Follow-up visits
Corneal photography to determine curvature of cornea for contact lenses.
There are several levels of service involved with both of these procedures. It is the
minimal level that is being considered content of service.
Boeing Contact Lens Examination, Testing, Fitting and 3 Follow-Up Visits
These are considered content of service of the routine eye exam.
If a provider is contracting with BVE, the contact exam, testing, fitting, and 3 follow-up
visits are included in the routine vision exam (92002-92014).
We prefer that you not separately bill this service.
If for some reason you find it necessary to submit a charge for this service you should
code it in the following manner:
92499 and include on claim attachment the following: "92499 = contact exam, testing,
BCBSKS-Business Procedure Manual
Appendix G: Optometry and Optician Guidelines
Current Procedural Terminology © 2014 American Medical Association. All Rights Reserved.
NOTE: Codes published herein are current on the revision date and are subject to change.
Contains Public Information
Page G-20
Revision Date: April 2014
REVISIONS
1/31/2013,
continued
fitting and 3 follow up visits.
Use modifier 22 when submitting any claim attachment.
•
Boeing Medical Eye Examinations
Boeing processes these services under the medical portion of the member’s contract.
BCBSKS coding guidelines are used for Boeing medical eye examinations and are addressed
earlier in the BCBSKS section of the manual.
•
Boeing Hardware
Boeing Frames
If you are contracting with the Boeing Vision Network Hardware, you have agreed to give
a 15% discount off of your retail price, with the balance being patient responsibility.
Do not take the 15% off your charge on the claim. We will do that for you.
Boeing will allow $70.00.
Balances are patient responsibility.
Boeing Lenses
The primary contractor has a schedule of fees that they will allow for lenses and contacts
under the Boeing contract. These allowances may vary depending on the type of lens
provided.
The appropriate “V” procedure codes should be used.
If billing for disposable lenses, modifier DL should be used with the “V” procedure
code.
Balances are patient responsibility.
3/06/2013
Changed revision date to “March, 2013” from “January, 2013”.
Page G-7 –
Under “Other Medical Services” bullet, a second sentence regarding code 99070
was added to second sub-bullet () under “ Simple condition such as abrasion”.
5/01/2013
Changed revision date to “May, 2013 from “March, 2013”.
Page G-1 –
Under “Use of Modifiers for Identifying Specific Eye”, added a final bullet on the
page, “Each line should reflect 1 unit.”
Page G-4 –
Under the third bullet, the single code listed (92310) was changed to a range of
codes.
Page G-5 –
The third from the last bullet on the page was added.
Page G-6 –
A fourth bullet was added at the top of the page.
BCBSKS-Business Procedure Manual
Appendix G: Optometry and Optician Guidelines
Current Procedural Terminology © 2014 American Medical Association. All Rights Reserved.
NOTE: Codes published herein are current on the revision date and are subject to change.
Contains Public Information
Page G-21
Revision Date: April 2014
REVISIONS
5/01/2013,
continued
Page G-7 –
• Under the large bullet, “Medical Eye Examinations” (page G-6), the final bullet
of the section was deleted (which appeared on page G-7).
Deleted verbiage:
Number of Medical Eye Examinations with Retinal Examination for Diabetic Patients
per Benefit Period:
One medical eye exam with retinal examination for diabetic patients per benefit period is
allowed.
• Also deleted the words, “such as abrasion”, from the “Simple condition” subbullet.
• Added the code “92325” to the second bullet under the “More complex
conditions” sub-bullet.
Page G-8 –
Under “Contact Lens Procedure Code for Keratoconus Patient Care” (third
bullet), first sub-bullet, replaced code range “92310 – 92317” with a single code,
“92072”.
Page G-9 –
Deleted all verbiage under “Pachymetry”; now directed to medical policy on the
BCBSKS website.
Deleted verbiage:
BCBSKS considers this service medically necessary, one per lifetime in relation to
glaucoma evaluation, as an adjunct tool for those at high risk for glaucoma and/or
corneal disorders.
Pachymetry will not be allowed when scientifically demonstrated effect upon
management of a disease is not documented. See medical policy at link below.
http://www.bcbsks.com/CustomerService/Providers/MedicalPolicies/policies.htm
Routine Glaucoma Screening using Pachymetry
The use of pachymetry for routine glaucoma screening is considered investigational
and is a provider write-off unless a Policy Memo No. 1 Limited Patient Waiver is
signed prior to the service. GA modifier should be used with code to indicate waiver
on file.
Waiver for FEP – For FEP patients the waiver is only accepted for services
considered not medically necessary. This means in the case of pachymetry used
for routine glaucoma screening the service would be a provider write-off even if a
waiver were signed prior to the service being rendered.
Procedure Codes for Pachymetry
BCBSKS-Business Procedure Manual
Appendix G: Optometry and Optician Guidelines
Current Procedural Terminology © 2014 American Medical Association. All Rights Reserved.
NOTE: Codes published herein are current on the revision date and are subject to change.
Contains Public Information
Page G-22
Revision Date: April 2014
REVISIONS
5/01/2013,
continued
76514
Diagnostic Ultrasound – Head and Neck – Corneal pachymetry,
unilateral or bilateral (determination of corneal thickness)
Valid Diagnosis Codes for Non-Routine Pachymetry
Please use one of the following diagnoses by submitting the diagnosis code in the
2300 HI01-2 or in the first diagnosis position of Box 21 of the claim form when
billing for care for this condition.
High-risk glaucoma indicative diagnoses codes
Corneal disorders
364.53
364.77
365.00
365.01
365.02
365.03
365.04
365.10
365.11
365.12
365.13
365.14
365.20
365.23
366.11
367.0
367.1
367.20
371.20
371.21
371.22
371.23
371.57
371.58
996.51
Page G-9 –
Second sub-bullet under “Visual Fields”, replaced verbiage to state that “units of
service should reflect 1”.
Deleted verbiage:
Visual Fields (92081, 92082, 92083) codes are unilateral or bilateral; which means units of
service are not necessary and will not be recognized when processing claims:
Page G-10 –
Under “Fundus Photography”, added link to the medical policy on the BCBSKS
website.
BCBSKS-Business Procedure Manual
Appendix G: Optometry and Optician Guidelines
Current Procedural Terminology © 2014 American Medical Association. All Rights Reserved.
NOTE: Codes published herein are current on the revision date and are subject to change.
Contains Public Information
Page G-23
Revision Date: April 2014
REVISIONS
5/01/2013,
continued
Page G-12 –
Under second sub-bullet, “Permanent Implant A4263”, removed first sub-bullet,
“Type of service 9”.
Deleted verbiage:
Type of service 9
Page G-14 –
Changed the word “most” to “some”. Deleted first sub-bullet under “Coverage
after Cataract Surgery”.
Deleted verbiage: (in bold)
Most BCBSKS contracts will cover vision correction hardware after there has been cataract
surgery.
Contact lenses are covered in place of glasses.
Page G-15 –
Deleted third sub-bullet under “S0500 Disposable Contacts” (third bullet).
Deleted verbiage:
6/3/2013
Use modifier 22 when submitting any claim attachment.
Changed revision date to “June 2013” from “May 2013”.
Page G-7 –
Changed wording of the first bullet under “ Simple condition” sub-bullet.
Old wording:
Use 92002 through 92014 for the evaluation and management service.
Changed wording of the second and third bullets under “ More complex
conditions” sub-bullets, and separated the second bullet into two bullets.
Old wording:
Use 92310 – 92317. 92325 for the fitting of the lens.
Use a V code for the dispensing of the lens.
1/27/2014
Page G-11 –
Changed the link so it links to the medical policy page, rather than the medical
policy itself.
Changed revision date to January 2014 from June 2013. Updated CPT copyright
to 2014.
Page G-3 –
Added note to include routine exam coverage under pediatric vision coverage to
age 19, and reference to Availity to check eligibility regarding coverage.
BCBSKS-Business Procedure Manual
Appendix G: Optometry and Optician Guidelines
Current Procedural Terminology © 2014 American Medical Association. All Rights Reserved.
NOTE: Codes published herein are current on the revision date and are subject to change.
Contains Public Information
Page G-24
Revision Date: April 2014
REVISIONS
3/04/2014
4/15/2014
Page G-11 –
Changed verbiage to include units of service 001 for bilaterally or unilaterally
billing procedure code 92250.
Page G-12 –
Added section on Ophthalmic Diagnostic Imaging.
Page G-12 – Modified section on Ophthalmic Diagnostic Imaging to include
Medical Policy update for codes 92133 and 92134.
Page G-2 – Removed invalid diagnosis (367.2 Astigmatism)
BCBSKS-Business Procedure Manual
Appendix G: Optometry and Optician Guidelines
Current Procedural Terminology © 2014 American Medical Association. All Rights Reserved.
NOTE: Codes published herein are current on the revision date and are subject to change.
Contains Public Information
Page G-25
Revision Date: April 2014









© Copyright 2026