
Gateway Community Health Provider Manual September 2010
Gateway Community Health Provider Manual September 2010 1 Table of Contents Table of Contents................................................................................................................................2 Section I Introduction ................................................................................................................................ 5 Purpose of the Manual..............................................................................................................5 About Gateway ..........................................................................................................................5 Mission Statement.....................................................................................................................6 Contact Information ...................................................................................................................6 Choice within Gateway Community Health ........................................................................6 Eligibility and Enrollment ......................................................................................................7 Intake Assessment ..............................................................................................................7 Section II Network Management & Provider Relations ................................................................................. 9 Introduction ..................................................................................................................... 9 Network Contracting Process ..............................................................................................9 Credentialing ................................................................................................................. 11 Fair Employment Practices (FEP) Process and Application ......................................... 12 Criminal Background Checks .......................................................................................... 14 Model Payment System (MPS) – Title XIX .................................................................... 14 Provider Sanctions............................................................................................................ 19 Section III Information Management/Claims Processing ........................................................................ 22 Introduction ........................................................................................................................ 22 Claims Submission Methods................................................................................................. 22 Electronic Claims Submission .......................................................................................... 22 Claims Processing ............................................................................................................ 23 Coordination of Benefits (COB) ........................................................................................ 23 ICD-9-CM Codes/Billing Codes........................................................................................ 24 Filing Limits/Forms ................................................................................................................. 24 Explanation of Benefits/Remittance Advise ..........................................................................27 Claims Appeal Process.......................................................................................................... 28 Fraud and Abuse .......................................................................................................... 28 Section IV Financial Management ............................................................................................................30 Introduction ........................................................................................................................ 30 Ability to Pay ...................................................................................................................... 30 Claims Verification .................................................................................................................. 31 Medicaid False Claims Act ............................................................................................... 32 2 Section V Clinical Services .......................................................................................................................34 Introduction .........................................................................................................................34 Emergency Procedures ..........................................................................................................34 Person Centered Planning ................................................................................................34 Crisis Planning .................................................................................................................. 39 Advanced Directives ...............................................................................................................40 Coordination of Care ...............................................................................................................41 Psychiatric Consultations on a Medical Floor..................................................................42 Targeted Case Management .................................................................................................43 Requirements for Community Living Support Staff and Respite Workers....................47 Verification Guidelines for Community Living Support Staff and Respite Workers......49 Section VI Utilization Management .................................................................................................................50 Introduction .........................................................................................................................50 Definitions.................................................................................................................................50 Authorization Process .............................................................................................................52 Utilization Guidelines and Management ........................................................................... 53 Inpatient Hospitalization and Partial Hospitalization Clinical Appeals ...........................54 Discharge Day in a 24 Hour Setting .................................................................................. 57 Residential Reconsideration Review................................................................................. 57 Section VII Quality Improvement ................................................................................................................ 59 Introduction .........................................................................................................................59 Contact Information .................................................................................................................59 Incident Reporting ................................................................................................................... 59 Death Reporting............................................................................................................ 59 Sentinel Events ..................................................................................................................60 Residential Monitoring.............................................................................................................61 Monitoring of Consumer Funds.............................................................................................. 62 Emergency Preparedness......................................................................................................63 Vehicle Safety ............................................................................................................... 64 Section VIII Compliance .............................................................................................................................. 66 Provider Monitoring & Site Visits ............................................................................................ 66 Medicaid Claims Audit ............................................................................................................67 Anti-Kickback Law ........................................................................................................ 68 Section IX Member Services/Customer Services ..................................................................................... 69 Introduction .........................................................................................................................69 Customer Service/Member Service Functions ................................................................. 69 Cultural Competency ..............................................................................................................70 Limited English Proficiency ................................................................................................ 73 3 Section X Introduction .....................................................................................................................................77 Grievance and Appeals .....................................................................................................77 Section XI Recipient Rights ....................................................................................................................... 79 Introduction .........................................................................................................................79 Section XIII Miscellaneous .......................................................................................................................... 80 Preliminary Death Report Form ........................................................................................... 81 Report of Recipient Death..................................................................................................... 82 Sentinel Event Report ............................................................................................................ 86 Glossary .............................................................................................................................88 Section XIII Addendums ............................................................................................................. 108 PIHP/CMHSP Encounter Reporting HCPCS and Revenue Codes ............................108 Medicaid Application ....................................................................................................... 108 Medicaid Provider Manual .............................................................................................. 108 Michigan Department of Community Health Approved Diagnosis Codes................. 108 Person Centered Planning Best Practice Guideline .................................................... 108 Consumerism Best Practice Guideline ......................................................................... 115 Self-Determination Policy & Practice Guideline ........................................................... 119 Housing Best Practice Guidelines .................................................................................. 131 4 Section I Introduction The following document comprises the Gateway Community Health (Gateway) Provider Manual. Gateway also issues and distributes periodic bulletins and written notices as changes are implemented to the policies and/or processes described in the manual at its provider meetings, on the Gateway on-line provider portal or through email. These bulletins and written notices are immediately effective when distributed or as otherwise indicated, and replace and take precedence over similar material, previously distributed. An inventory of these bulletins and written notices is maintained in and can be accessed by contacting the Provider Service Department. These bulletins and notices are incorporated into the online version of the manual on an annual basis. This manual serves as a ready reference tool for professional providers. Please be advised that this manual does not replace or eliminate any provider requirements or obligations contained in individual provider contracts and in all instances is to be interpreted in accordance with the terms and requirements contained in those contracts. Any discrepancies between this Manual and individual provider contracts shall be resolved in favor of the terms of such contracts. Purpose of the Manual Gateway Community Health developed this manual to supply providers with details on the structure, policies and procedures of Gateway. We recommend that providers and their staff read this manual and reference it as necessary. About Gateway Community Health Gateway Community Health, Inc. is a Michigan non-profit corporation, operating as a Manager of a Comprehensive Provider Network (MCPN) in Wayne County, Michigan. Gateway is funded by the Detroit-Wayne County Community Mental Health Agency (DWCCMHA). The Michigan Department of Community Health, in their revised plan for procurement, required Detroit-Wayne County Community Mental Health Agency to develop a vertically integrated network of Provider of Specialty Service Networks (PSSN) to ensure choice for persons receiving publicly funded mental health services. The Managers of Comprehensive Provider Networks are the Agency PSSNs. The MCPNs under the Detroit-Wayne County Community Mental Health Agency are to provide mental health and substance abuse services for persons with, or at risk for, serious emotional disturbance, severe mental illness, developmental disabilities, substance abuse, and MIChild beneficiaries. The system is designed to give individuals, within the identified populations, greater choice and involvement in their treatment. 5 The cornerstones of this system are: (1) providing choice; (2) Person-Centered Planning principals; and (3) maximizing the use of and developing new communitybased services. Services are provided through the Managers of Comprehensive Provider Networks, Substance Abuse Coordinating Agencies, and other Agency contractors. As a MCPN, Gateway contracts with DWCCMHA. MCPNs were established to develop and manage a comprehensive network of providers who meet the needs of individuals with or at risk of developing severe mental illness, serious emotional disturbance or developmental disabilities. The ultimate goal of the Detroit-Wayne County Community Mental Health Agency and each MCPN is to provide choice and access to quality care and services in a cost-efficient manner. MCPNs are not managed care plans and not insurance companies. Mission Statement Gateway Community Health will ensure access to a contracted network that provides comprehensive, culturally competent mental health and substance abuse services for children, adults, seniors and their families. These services will support recovery, independence, collaboration and empowerment within the home and community. Contact Information Address: 3011 West Grand Boulevard Suite 2000 Detroit, Michigan 48202 Toll Free: (800) 973-GATE (4283) Main Telephone: (313) 262-5050 TDD: (313) 875-4065 Choice within Gateway Community Health As stated in the definition of an MCPN, Gateway does not directly provide services or supports. Gateway is responsible for contracting and overseeing qualified, competent, Medicaid-approved providers to meet the needs described in the Person-Centered Plan. To meet this requirement, Gateway currently has contracts with many approved provider sites offering a wide array of services. Once a provider is selected the beneficiary will have choice, within certain limits, regarding the specific staff person providing the service or support. Choice may be limited by such things as caseload size and availability of other comparable staff within that provider location. In addition to the choice of staff and the choice of provider sites, the beneficiary has the option of choosing another MCPH on a monthly basis. 6 Eligibility and Enrollment This section contains information on how to determine eligibility and enroll a beneficiary into the system for Detroit-Wayne County Community Mental Health Agency under Gateway Community Health ELIGIBILITY To be eligible as a Gateway Community Health consumer, the individual must be a Wayne County resident with or at risk of developing a serious mental illness. Please refer to the glossary for definitions on serious emotional disturbance and serious mental illness. Based on the Michigan Mental Health Code, services are available to eligible persons regardless of ability to pay. ENROLLMENT Providers may check an individual‘s MCPN assignment via the web-based MH-WIN system if they have access to this system. If the provider does not have access to MHWIN, they may contact Pioneer Behavioral Health at 1-866-690-8257 or Gateway‘s Customer Service Department at (313) 262-5050 to request this information. If the member is not enrolled in an MCPH, the intake assessment must be completed via the intake e-form process. Enrollment and Re-enrollment process: 1. Providers must call Pioneer at 1-866-690-8257 in order to begin the enrollment process. 2. Pioneer will ascertain whether the consumer meets initial eligibility. 3. Consumers who meet initial eligibility will be defaulted into the MCPN of their choice. 4. Consumers presenting in a crisis situation will be re-enrolled into their previously assigned MCPN, if applicable. 5. Consumers presenting on a routine basis will be re-enrolled to their previous MCPN or the MCPN of preference if applicable. 6. The MCPN start date will be the date Pioneer receives the information allowing them to make a determination of initial eligibility (usually the first day) 7. Providers are to conduct an assessment and complete the eligibility E-form on the MH-WIN system and submit the form electronically. 8. An enrollment form should be completed and signed by the consumer and/or guardian and mailed to the Detroit-Wayne County Community Mental Health Agency. 9. All provider calls related to enrollment are to be routed to Pioneer for disposition. Intake Assessment 1. Providers are to complete the Intake Assessment Form on all Persons presenting for services who are either: New to the system or Are in the system but do not have an MCPN Assignment (Check MH-WIN) 7 2. 3. 4. 5. This form may be completed hard copy, but the information MUST be entered by the provider completing the intake assessment directly onto MHWIN using the Intake E-form process. Pioneer will no longer accept hard copy (paper) versions of this assessment. Important: Indicate the MCPN Affiliation by checking the appropriate box on the top of the form on page 1. Maintain a log of all assessments submitted indicating Person‘s name and the date the information was submitted. Providers must perform and document an ability to pay determination and billing determination for identification of first and third payor parties during the intake assessment, and at least annually thereafter. 8 Section II Network Management & Provider Relations Introduction The Network Management Department is responsible for maintaining all contracts and requirements for contracted providers. The Provider Relations Department serves as liaisons to the provider network. Applications for becoming a panel provider are available on the website at www.gchi.org or by contacting the Provider Relations Department. Contact Information: Lynch Travis Director, Provider Relations 313-263-2368 [email protected] H. Michael Falconer Director, Network Management 313-263-2398 [email protected] Barbara Tamachaski Provider Information Changes 313-263-2414 [email protected] Sharon Tye Provider License, Insurance and other Required Information Updates 313-263-2352 [email protected] Darlene Williams Provider Applications & Liaison 313-263-2464 [email protected] Network Contracting Process Any entity interested in becoming a panel provider for Gateway must follow the network‘s contracting process. Application Process - all applicant providers are required to complete an application to be considered for panel provider status. All requests are handled by the Network Management Department. The applicant provider is required to complete the application in its entirety and submit to the Provider Relations Liaison along with the required documentation as listed in the application. Only when the application is complete will it be reviewed by Network Management. Network Management will review submitted applications for consideration as a panel provider. 9 The review will take into consideration the applicant‘s history of service to the target population, the need for service in the applicant‘s geographic area, provider rates, recipient rights, quality of care, results of a site visit and other pertinent information available at the time of the review. Network Management forwards providers who are recommended for contracts to the Chief Executive Officer (CEO). The CEO reviews and either approve and executes the contracts, or deny the recommendation. Applicants will be issued written notice within approximately five (5) business days of the decision regarding the status of their application. Applications may be approved, pended or denied at this point. Approved applicants will receive a fully executed contract, their provider number and claim submission information. Denied applicants will be issued a notice within five (5) business days of the decision. Denied providers will be given an opportunity to request reconsideration of the decision within thirty-days (30) of the date of the denial letter. Request for Reconsideration - Applicants who have been denied a contract with Gateway are afforded the opportunity to request reconsideration of the decision. Applicant provider has 30 days from the date of the notification to file such request. Applicant must submit their request in writing to the Director of Network Management. Applicant must indicate reason for the request and any other documentation that may be necessary for further review. The Director of Network Management, or designee, will notify the applicant of the receipt of their request for reconsideration within 7 days. The reconsideration applicant will be notified of the final disposition within approximately 7 days of the determination. Applications may be pended by Network Management Workgroup or the CEO based on several factors which could include requests for additional information, contracted providers who are on plans of correction. The Director of Network Management, or designee, is responsible for informing the provider of the network‘s decision regarding a contract. Documentation of all applications, committee notes and contracts shall be the responsibility of the Director of Network Management and maintained within the Network Management Department. All applications and applicant information will be kept on file for a minimum of two (2) years. Once approved for contract, providers are contract document based on the type of service(s) to be rendered. Providers are then invited to a provider orientation meeting to become acclimated to the network‘s policies and procedures. Providers are given appropriate information regarding billing/claims, network processes and procedures, recipient rights information and other information the provider needs to operate with the network. 10 Provider contracting is secondary to meeting the needs of the consumer. There will be occasions where contracts will be issued outside of the normal Network Management structure due to an emergency or urgent situation in an effort to appropriately treat or place a consumer. The provider must be licensed for the type of service that will be rendered to the consumer in order to bill for those services (for example, licensed to service the mentally ill population if placing in an Adult Foster Care Home). They must meet minimum contracting requirements including the minimum liability insurance requirement. For out-of-network providers, a Letter of Agreement may be issued that is specific for one consumer. Credentialing The Director, Network Management is responsible for oversight regarding the credentialing of providers which includes the initial credentialing through the contracting process and continued re-credentialing. Providers that are not credentialed are notified by the Director of Network Management or Pioneer Behavioral Health. It is the policy of Gateway that all contracted service providers are appropriately credentialed to provide such services as listed in their Gateway contract. Gateway utilizes various methods to assure credentialing of service providers as an organization or in the case of children‘s services, individually. Gateway seeks to develop and maintain a network that provides a continuum of care that allows members to be served in the most appropriate levels of care and in the least restrictive environment. Careful evaluations of programs and individuals that are credentialed based on accreditation and licensure for service specific populations is paramount. Administrative credentialing is performed and involves verification of the following: Good standing with the State of Michigan and Federal regulatory agencies Lack of Medicaid and Medicare sanctions Current State of Michigan licensure and/or certification if applicable Professional and general liability insurance coverage as noted in the contract Compliance with contractual requirements regarding malpractice claims history Completion and submission of all required application documents pertaining to current accreditation Wayne County Fair Employment Practices certificate Not presently debarred, suspended, proposed for debarment, declared ineligible, or voluntarily excluded from covered transactions by any federal department or agency Prompt and effective response to any Recipient Rights findings, grievances, or other complaints, or service delivery concerns 11 Participate as appropriate in on-going administrative and clinical/service delivery monitoring and continuous quality improvement efforts Fair Employment Practices (FEP) Process and Application All contracted providers are required to maintain a current Fair Employment Practices Certificate through Wayne County. Applications can be obtained from Wayne County‘s web site at www.epurchasing.waynecounty.com or by calling Wayne County at (313) 224- 5021. You can also contact Gateway Provider Relations Department. The applications must be submitted to Human Relations Division, 600 Randolph, 5th Floor, Detroit, Michigan 48226. Their fax number is (313) 224-6932. Providers must submit a renewal application within 6 months of the expiration date of the current certificate. Providers who fail to maintain a current Fair Employment Practices Certificate will be subject to the Network‘s Scope and Severity Process up to and including termination of the contract. Accreditation The following organizations will satisfy site requirements for all programmatic, outpatient and residential services covered by accreditation (attestation that the accreditation covers all services is required): The Joint Commission Healthcare Facilities Accreditation Program (HFAP) of the American Osteopathic Association (AOA) Accreditation Association of Ambulatory Healthcare (AAAH) Council on Accreditation (COA) Commission on Accreditation of Rehabilitation Facilities (CARF) National Committee for Quality Assurance (NCQA) Pioneer Behavioral Health (the Agency‘s contracted Credentialing Verification Organization, CVO) Organizations accredited by one of the above mentioned bodies or holding a State of Michigan licensure or certification where State of Michigan standards meet or exceed accreditation standards, and wishing to supply traditional outpatient services must also meet the following: The medical director and clinical director (the person clinically responsible for the program) successfully completes verification of selected credentialing elements; All physicians associated with the organization successfully complete verification of selected credentialing elements. 12 For evaluation standards for non-accredited facilities, please refer to Gateway‘s credentialing policy. Child Mental Health Professional credentialing All providers who have staff providing services to children must have their staff credentialed through Pioneer Behavioral Health as a Child Mental Health Professional. Providers must submit all credentialing information to Pioneer Behavioral Health upon hiring. Staff will be credentialed according to the requirements defined for the Child Mental Health Professional. Initial credentialing is done within 90 days of hire. Pioneer maintains a database of all credentialed staff. Staff must be re-credentialed every two years and must maintain 24 hours per year of continuing education units. Contracted Providers are responsible for the following: Maintaining updated written policies and procedures which guide the credentialing process for employment Decisions on credentialing and re-credentialing of practitioners A list of individuals who are credentialed and the type of credential Maintaining files that include the documentation that supports the credential including A dated resume Evidence of primary source verification Relevant education Relevant training including 24 hours per year of ongoing population specific (SMI, SED, DD) in-service training and/or continued education related to the provision of services, supports, treatment and UR/UM activities License/certification/registration Current competence Documentation of certification to provide special assessments services or processes (e.g., Child & Adolescent Functioning Assessment ScaleCAFAS) For physicians: Professional and general liability insurance Reports from the National Practitioner Data Bank and Healthcare Integrity & Protection Data Bank Checking Medicaid exclusion status Ensuring all health care professionals are credentialed at a minimum of every two years. 13 All entities receiving Federal funds have an affirmative duty to check the program exclusion status of individuals and entities prior to entering into employment or contractual relationships, or run the risk of civil money penalties. All health care providers must check relevant Federal internet websites (http://www.epls.gov/epls/search.do. and http://exclusions.oig.hhs.gov/search.aspx) prior to hiring or contracting with individuals or entitles and periodically for the participating/exclusion status of current employees and contractors. All employees, contractors, and consultants hired to provide professional or direct care services to Persons receiving mental health services must be in good standing with the law (e.g. not a fugitive from justice, a convicted felon or an illegal alien). Criminal background checks must be completed on potential employees. Annual criminal background checks must be performed on all employees and other personnel who have regular contact with consumers on behalf of the applicant‘s company in order to be considered for contracting with Gateway. Model Payment System (MPS) – Title XIX Purpose - To maximize Title XIX (Medicaid) reimbursement for Personal Care Services provided to Medicaid eligible recipients in licensed residential settings and coordinate benefits for consumers. Title XIX is a Supplemental Income given to Providers for care of consumers who are not receiving payment from a network for personal care or community living supports to care for consumers (non-specialized residential consumers). The Provider must be licensed and meet minimum requirements of the Department of Consumer and Industry Services (DCIS). Provider must also have an agreement with the Gateway to process Title XIX for eligible consumers. Eligible Care Providers - Providers must be licensed and meet minimum requirements of the Department of Consumer and Industry Services (DCIS) and Department of Community Health (DCH) as defined and contained therein, Act 117, Public Acts of 1973, as amended and Act 218, Public Acts of 1979, as amended, for residential settings such as: homes for the aged, adult foster care family home, adult foster care small group home, adult foster care large group home, adult foster care congregate facility, foster family home, foster family group home, and child caring institutions and enrolled in the Model Payment System. 14 Medicaid (MA) Designated Case Manager: case manager must be either a Qualified Mental Retardation Professional (QMRP) as defined in 42 CFR 483.430, or a Qualified Mental Health Professional (QMHP) as defined in Michigan‘s Medicaid Mental Health Clinic Provider Manual, Chapter III. Personal Care Services: services provided in accordance with an individualized plan of service that assist a recipient by hands-on assistance, guiding, directing, or prompting of Personal Activities of Daily Living (PADL) in at least one of the following activities: EATING/FEEDING: the process of getting food by any means from the receptacle (plate, cup, glass) into the body. This item describes the process of eating after food is placed in front of an individual; TOILETING: the process of getting to and from the toilet room for elimination of feces, and urine, transferring on and off the toilet, cleansing self after elimination, and adjusting clothes; BATHING: the process of washing the body or body parts, including getting to or obtaining the bathing water and/or equipment, whether this is in bed, shower or tub; GROOMING: the activities associated with maintaining personal hygiene and keeping one‘s appearance neat, including care of teeth, hair, nails, skin, etc; DRESSING: the process of putting on, fastening and taking off all items of clothing, braces and artificial limbs that are worn daily by the individual, including obtaining and replacing the items from their storage area in the immediate environment. Clothing refers to the clothing usually worn daily by the individual; TRANSFERRING: the process of moving horizontally and/or vertically between the bed, chair, wheelchair and/or stretcher; AMBULATION: the process of moving about on foot or by means of a device with wheels; ASSISTANCE WITH SELF-ADMINISTERED MEDICATION: the process of assisting the client with medications that are ordinarily self-administered when ordered by the client‘s physician. Process and Procedure Upon placement of a non-specialized mental health recipient into a residential foster care setting, the case manager shall insure that any need for personal care services are identified in the consumer‘s plan and according to Medicaid (MA) standards. In addition, the case manager shall take the required action(s) to further insure that payment(s) for personal care services are issued, and all payment problems are resolved. 15 Consumer must have active Medicaid during the effective dates of service. Consumer must need on-going personal care services to be Title XIX eligible. Personalized services are provided in accordance with an individualized plan of service that assist a recipient with hands-on assistance, guiding, directing, or promoting of personal Activities of Daily Living in a least one of these activities: Eating/Feeding, Toileting, Bathing, Grooming, Dressing, Transferring, Ambulation and Assistance with SelfAdministered Medication. Personal care tasks are not required to be performed each day. However, in a monthly payment program, personal care services must be continuous and on-going during that calendar month for payment. Responsibility of the Case Manager Case Manager should develop a Service Plan/Plan of Service when the recipient is admitted to the foster care facility to establish Title XIX eligibility funding. The Case Manager will complete an assessment form at the time of the initial placement and annually thereafter. The Service Plan should be developed jointly with the recipient and foster care provider using the DWCCMHA‘s form. Personal Care Services must be ordered by a Case Manager and be approved by their supervisor, to be eligible for payment. The Case Manager must complete a 3803 Form. The 3803 Form must be approved (signed by the supervisor). If the supervisor is not available, the 3803 form may be signed by a Registered Nurse. Approval must be completed within three (3) business days. The Case Manager will submit the original 3803 form to the Title XIX Specialist at Gateway within seven (7) days of placement. The Case Manager must review and sign off on the provider log kept at the provider site at least once each month to ensure that personal care services are being delivered. The Case Manager must re-evaluate the consumer within 365 days of the last order date to determine if the consumer still requires Personal Care Services. Provider should notify Case Manager and Title XIX Specialist within 24 hours regarding any consumer who moves, becomes hospitalized, leaves home permanently, or dies. A new order/form is required when: A recipient moves; A recipient has never lived in a non-specialized residential setting; A substantial change (clinically) has occurred; Recipient transfers from DHS or another Community Health Services provider or MCPN; 16 Title XIX eligibility has lapsed (3803 Form is expired) after 365 days or approval of services has not been obtained within 15 days after order has been signed and dated. Instructions for completing the 3803 Form Name: Agency Number: Move in Date: Date of Birth: Sex: SSN#: FIA: Medicaid ID #: Diagnosis: Type of Guardianship: County: Placement facility: Phone Number: Address: Medicaid Provider ID Number: Global Assessment of: End Date Reason: Parent/Legal Guardian Name: Treatment/training (PPB): Objective: Type of Facility: Provide/Assist: Guide/Direct: Full legal name of consumer Consumer‘s member number Date consumer entered the home Consumer‘s date of birth Male or Female Recipient‘s Social Security Number FIA/DHS Case Number ID number as it appears on the recipient‘s Medicaid Card Clinical diagnosis using ICD-9-CM classification Consumer‘s guardianship, if any County of residence Name and address where the recipient lives Telephone number of the facility Address of the facility Provider ID Recipient‘s GAF Score Functioning Leave Blank Consumer‘s Parent(s) or Legal Guardian Type of treatment for the consumer (usually Rehabilitation is stated for mental health) Check one Level of care of recipient Check this column if the recipient is totally dependent upon staff to perform the task for him/her, or is partially dependent and needs physical assistance, meaning ―hands on service‖ Check this column if the recipient can perform the task him/herself but requires verbal direction in the form of prompts or reminders When the Title XIX Specialist receives the 3803 Form from the Case Manager, the Title XIX Specialist will enter the authorization into the AuthentiCare System. Once this process is completed, the provider is able to bill monthly for the personal care services. Provider of services must maintain a service log that documents specific days on which personal care services were delivered consistent with the recipient‘s individual plan of services. 17 Providers are required to use MI AuthentiCare. MI AuthentiCare is a paperless billing system for Adult Foster care (AFC) providers. The system provides automated electronic billing for facility services provided through the Department of Human Services (DHS), formerly Family Independence Agency (FIA) and Community Mental Health Service Program Boards (CMH). Providers do not bill Gateway. Gateway consumers in an AFC home who are receiving services through one of the Primary Providers (the eight partner agencies for the Gateway Network) must be authorized by the Network. Therefore, if there are consumers who have been put on Title XIX through FIA/DHS, they must be end dated from FIA/DHS and enrolled on the AuthentiCare System through Mental Health (CMH). Providers cannot bill through MI AuthentiCare before the end of the month. Providers can only bill for services at the beginning of the next month for services in the previous month, which is after services have been provided. Providers can bill within 370 days from the date of service. The provider may call or use the website to bill for the client. Providers will no longer receive the FIA 2353 invoice. The MI AuthentiCare system takes the place of this form. Providers will need their Identification (ID) Number and Pin Number when completing their billing, as well as information on clients that they are billing for, such as the Medicaid ID number and the dates that the consumer was in the AFC home. If a client leaves the AFC home during the month, the provider should contact the case manager. The case manager will contact the Title XIX Specialist to end date the client from the Authenticare system. If a provider bills for services that are not rendered, the provider will be responsible to reimburse the Michigan Department of Community Health. Provider Agreement The FIA-1625 is a two-part form that must be completed by AFC providers prior to enrollment. No authorization can take effect prior to the date of this agreement. The agreement is in effect until there is a change of licensee or facility name in which case a new agreement must be obtained. The provider sends the original to Gateway. Gateway sends the form to the Medicaid Payment Division in Lansing for provider enrollment. Once Gateway has been informed the provider has been enrolled, Gateway will contact the provider with their enrollment number. The FIA-AFC licensing system is computerized and provides a Data Base for linking with the Model Payment System. This data base is automatically updated weekly to reflect licensing changes. When an AFC provider is enrolled, the licensing data is confirmed from the data base. However, Termination of a license automatically end dates the license eligibility on the MPS. 18 Duplicate Payments of Title XIX Funds Providers cannot receive payment for personal care services from Gateway while at the same time receiving payment for personal care services under the Model Payment System. When this error occurs, the following steps should be taken: Title XIX Specialist/ Case Manager will notify PCS LANSING immediately and identify what happened in a written statement and includes pertinent information. This statement should be forwarded to: DCH, Bureau of Finance P. O. Box 30668 Lansing, MI 48909-8168 Over Payment and Recoupment The Network is responsible for correctly determining eligibility of payments of service program needs and the amount of those payments. When an overpayment is discovered, corrective action must be taken to prevent further overpayment and to assure the overpayment is recouped. Providers are responsible for correctly billing for personal care services which were authorized and actually delivered. Title XIX Specialist ends the authorization immediately through AuthentiCare and sends an Overpayment Letter to Provider. If notified by DCH Program office that repayment has not been made by provider, Title XIX Specialist will follow up with provider. The Adult Foster Care Provider must write an explanation for overpayment and enclose the repayment of funds. (Un-cashed warrant or personal check made out to STATE OF MICHIGAN). PROVIDER SANCTIONS At the sole discretion of Gateway, action may be taken when there is evidence that a Provider is out of compliance with the terms and conditions of the Agreement and/or with other regulatory requirements or statutes. The following is a list of the sanctions available to Gateway. They do not have to be issued progressively. Depending upon the nature of the violation, an immediate termination of the Agreement may be levied. Corrective Action Plan: A letter identifying the specific violation(s) will be presented to the Provider along with a request for the Provider to prepare a written plan of correction (CAP). 19 The CAP must include a specific target date for meeting compliance, details regarding actions to be taken to correct the deficiency and the person responsible for assuring the correction is achieved. The CAP must also include provisions for ongoing monitoring to assure continued compliance. Gateway will inform the Provider of the acceptance of the CAP, in full or in part. Gateway may request the Provider make revisions to the CAP. Suspension of Referrals: This action would be taken as the result of identified health, safety, or well-being issues of consumers. The suspension may be made for a specific Provider program that is not in compliance. A suspension of referrals is generally taken along with a corrective action plan. Written notice to the Provider will specifically identify the condition that resulted in the suspend referral suspension, the required corrective action(s) and a target date. Withholding of Funds: A Provider will be notified that payment will be withheld along with the reason for the withholding. The Provider must meet the required conditions for the release of the withheld funds. Failure to meet Medicaid Provider Services standards and repeated failure to submit timely, related would be an example of when this sanction may be used. Removal of Consumer(s) Termination of the Agreement Immediate Termination or Suspension: At Gateway‘s sole discretion, any of the following events shall/may result in the immediate termination or suspension of the Agreement: The withdrawal, expiration or non-renewal of Agency required credentialing of Contracted Provider; The bankruptcy or receivership of Contracted Provider, or an assignment by Contracted Provider for the benefit of creditors; The loss or limitation of Contracted Provider's liability insurance; A reasonable determination by the Agency or Gateway that Contracted Provider's continued management and delivery of the Covered Services could result in harm to Persons; The debarment or suspension of Contracted Provider from participation in any governmental sponsored program, including, but not limited to, Medicare or Medicaid; The indictment or conviction of Contracted Provider for any crime; Change of control of Contracted Provider to an entity not acceptable to the Agency or Gateway; or Disapproval of the Contracted Provider by the MDCH or any other governmental entity, to the extent such approval is required in connection with the funding for Covered Services delivered hereunder. 20 As per the Agreement, Contracted Provider shall provide immediate notice to the Agency and Gateway, upon Contracted Provider's knowledge of any of the aforesaid events. 21 Section III Information Management/Claims Processing Introduction It is the policy of Gateway to manage its core operations including claims processing per the contract standards of Detroit-Wayne County Community Mental Health Agency. This information is to serve as a guide regarding claims processing and procedures. Providers receive compensation for services rendered to Gateway consumers through the submission of claims or encounter data depending on the terms of the provider contract. Providers must be contracted with the Network to be eligible for reimbursement for services rendered. Please refer to the Network Contracting Process. For submission of claims for services that require prior authorization, providers must contact Gateway to receive an authorization letter, which will include the following: The period of authorization (start date of authorization and ending/lapse date) The service category or codes to be used in billing. The number of units of services authorized Claims Submission Methods Based on the type of provider, claims are submitted in different fashions: Residential Providers (Providers of Personal Care and Community Living Supports in a residential setting) - Residential Providers submit claims for services rendered utilizing a 3806 form. This can be done via a paper form or an electronic version of the 3806. Outpatient Provider Agencies - Agency providers can submit claims for services utilizing the CMS-1500 form for authorized professional outpatient services. Hospitals - Hospitals will submit claims for services rendered utilizing the CMS1500 form for authorized professional/physician services and the UB-04 (CMS-1450) claim form for authorized hospital admissions. Electronic Claims Submission Providers with sufficient capacity and capabilities can submit claims through the use of a HIPAA compliant electronic data file format called the ANSI ASC X12N 837 Format. Residential providers can submit services electronically through the use of the 3806 DDE (direct data entry) system. The information required to complete electronic and paper claims is the same; however, electronic claims may require providers to input information into different fields. Software vendors typically provide instructions for entering the information. 22 For submission of claims using the ANSI ASC X12N 837 Format, please contact BayArenac Behavioral Health at 1-800-288-5309. For submission of claims using the 3806 DDE form, please contact Gateway‘s Provider Service Team at 313-262-5040. Claims Processing Providers must be issued a provider identification number specific to Gateway before submission of claims for processing. Any provider who submits claims without including their unique provider identification number will have those claims returned without being processed for payment. Please note: the National Provider Identifier (NPI) number currently does not replace the provider identification number assigned by Gateway, however plans are underway to use the NPI number exclusively. Providers must include the DWCCMHA member eligibility number on the claim in order for the claim to be processed. If it is not correct or not included on the claim, the claims edit process will issue a rejection and the claim will not process for payment. For those services that require prior authorization, the complete authorization number must be included on the claim in order for the claim to be processed. Inaccurate authorization numbers will cause the claim to be rejected. It is the provider‘s responsibility to obtain authorization for those services that require prior authorization before services are delivered. Coordination of Benefits (COB) Providers are required through contract (or Letter of Agreement) to coordinate benefits appropriately. Prior to submission of claims, providers must identify and bill consumer‘s other sources of coverage for care as well as determining a consumer‘s ability to pay. Gateway funds are the funds of last resort. Failure to coordinate benefits appropriately is a violation of the contract and Medicaid guidelines. The provider must make every attempt to seek reimbursement from other third party payers before seeking payment from the network including exhausting all levels of appeals with third party payers. Third parties must be billed timely. All third party claims for coordination of benefits must be submitted on paper with the Explanation of Benefits (EOB) from the other insurance company attached. An electronic printout of the provider‘s data system is not acceptable for COB. No electronic billing is accepted for COB. Claims received without the EOB are returned to the provider using the send back letter indicating this requirement. All COB claims are reviewed by a claims specialist to determine if additional payment from the network is necessary. 23 If the provider was reimbursed by the third party equal to or exceeding the contracted amount with the networks, there is no amount due to the provider, this includes copays and deductibles. The provider may not hold a Medicaid eligible member liable for any costs, charges, fees or other liabilities in the event that the network becomes insolvent, or payment is not made by the State, Detroit-Wayne County Community Mental Health Agency or any other entity. The provider is required by contract to assist eligible consumers in applying for and maintaining Medicaid coverage. Eligibility changes must be reported to the consumer‘s case manager. Link to the Medicaid Application can be found in the Addendum section of this manual. ICD-9-CM Codes/Billing Codes Procedure Codes: All claims must be Health Insurance Portability and Accountability (HIPAA) compliant. Only procedure codes approved by the Michigan Department of Community Health and in the contracted providers benefit array may be utilized. Any code that requires a modifier must include such modification in order for the claim to be processed. Revenue Codes: Hospitals are paid on a per diem basis and must include the appropriate revenue code according to the type of unit. (Refer to appropriate coding manual for description of revenue codes.) MDCH code list is listed in the Addendums section of this manual. ICD-9-CM codes: The claim must include a primary diagnosis code that is listed on the Michigan Department of Community Health‘s list of approved diagnosis code edits for reimbursement. Codes submitted that are not on this list will cause the claim to reject for invalid diagnosis code. This list is available in the Addendums Section of this manual. Filing Limits/Forms Providers are encouraged to submit claims as soon as the service has been provided. Providers shall submit claims for Covered Services to Gateway in a manner and format prescribed by Gateway, and claims must be submitted no more than ninety (90) days after the date of service and no later than two (2) months after the end of the Agency fiscal year, whichever is sooner. Payment for any claims not submitted within such time period shall be denied, except under circumstances relating to good faith efforts to coordinate benefits with other third party payors. Corrections or additions to claims shall be accepted by Gateway only if made within thirty (30) days from receipt of the initial claim. 24 Claims subject to third party reimbursement shall be submitted to Gateway within ninety (90) days of Contracted Provider's receipt of third party reimbursement, but in no event later than one year from the date of service. Claims must be submitted to: Bay Arenac Behavioral Health Gateway Claims Dept. P.O. Box 5559 Saginaw, MI 48603 Clean claims received by Gateway claims processing department will be processed within 30 days of receipt. Clean claim means a claim or an encounter submitted on a CMS-1500, CMS-1450 (UB-04) or 3806 claim form for Covered Services rendered by Contracted Provider with descriptive service and Consumer information that: Identifies the owner and facility that provided treatment or service including matching identifying numbers, or any affiliation status Identifies the Person with accurate identifiable information Lists the date and place of service Is a claim for Covered Services for an eligible Consumer If necessary, substantiates the Medical Necessity and appropriateness of the service provided Includes any applicable prior authorization number Identify services rendered using proper procedure and diagnosis codes Include additional information when required by Gateway Is certified by the Contracted Provider to be true, accurate, and prepared with the knowledge and consent of the Contracted Provider. Completion of Paper Claim Forms: Be sure the dates are within the appropriate boxes on the form Use only black ink Handwritten claims must be legible Keep a copy for your records Forms that do not meet the above requirements cannot be processed and will be returned to the provider unprocessed. For completion of the 3806 form: Provider Number: Enter the provider identification number assigned by Gateway. Provider Name: Enter the provider name of the facility where the consumer is located. Provider Address: Enter the address of the facility. Bill Through: Enter the month and year of the billing period. 25 Provider Phone: Enter the provider phone number. Member #: Enter the member identification number. Name (Last, First): Enter the member‘s last name and the member‘s first name. Authorization #: Enter the authorization number as provided on the Letter of Authorization. Primary ICD9: Enter the primary ICD9 diagnosis of the member. Secondary ICD9: Enter the secondary ICD9 diagnosis of the member if applicable. Service Code: Enter the HCPCS, CPT or Revenue code being billed for services rendered for the member as agreed in the provider‘s contract. Days In.: Enter the number of days the consumer is in the facility. Days Absent: Enter the number of days the consumer was not in the facility. Total Days: Add together the days in column and the days absent column. Per Diem x Days In: Enter the amount derived from this calculation. Payment is only made for actual days of service, not vacant bed days. Net Bill: Is the total amount billed minus any coordination of benefit payments to the provider. 1 through 31: Place a ―V‖ on the box for circumstances/dates when the member is in residence. Signature of the Provider: A representative of the provider organization must sign this form. Date: Enter the date this form was signed. Mandatory: All items are required for all claims. If the item is left blank, the claim cannot be processed. Summary for completion of a CMS 1500 (HCFA 1500): Line #1 Mark appropriate box, Medicare, Medicaid, etc. Line #1a Insured‘s I.D. number (consumer‘s unique member ID on the authorization) Line #2 Patient‘s name (Member Name) Line #3 Patient‘s date of birth and sex Line #5 Patient‘s address Line #6 Patient‘s relationship to insured Line #9 Complete this section if there is another insurance company Line #10 Patient‘s condition related to Line #12 & 13 Signature on file and current date Line #21 Diagnosis – ICD-9-CM code Line #24a Dates of service Line #24b Place of service Line #24d Billing codes Line #24f Dollar amount of charges Line #24g Number of days/units being claimed 26 Line #25 Line #28 Line #29 Line #30 Line #31 Line #32 Line #32a Line #33 Federal Tax ID Number (SSN or EIN) Total charge Amount paid (Use if another insurance company or the company has made partial payment or there is an ability to pay. EOB from other insurance must accompany claim upon submission for payment Balance due Your signature and date Name and address where services were rendered NPI number of #32 Billing name, address and provider number assigned by Gateway NPI number of #33 Line #33a . If the adjudication process determines that a paper claim is not clean, the claim will be returned with a form indicating the area or areas needing to be addressed. Provider must correct claim and resubmit for payment Claim is processed by Gateway claims processing department. Explanation of Benefits/Remittance Advise Providers will receive an Explanation of Benefits (EOB) that details every claim submitted unless the claim was returned for not meeting minimum criteria for claims processing. The EOB will accompany the provider‘s payment. The following are claims edits currently part of the claims processing procedure: ANR - Authorization Not Required - the code billed has been paid without an authorization CNC - Coverage Not Current - referring to the members eligibility with Gateway & indicating that the member was or is enrolled, but not on this date of service CNE - Client Not Enrolled - indicates that the member became eligible after the date of service billed COB - Third Party Primary - the payment is based on another insurance which is primary DBP - Denied, Bill to Primary- a third party carrier must be billed prior to payment consideration DPC - Denied by Primary Carrier - EOB received with claim indicates primary carrier denied of which we also will deny DS - Duplicate Claim - denied due to previously processed claim to same vendor, date of service, and service code category INV - Invalid Client ID - the member number billed is not found on the system PCR - Paid at Contracted Rate - the procedure billed was reimbursed per the rate indicated in the providers contract LN - Too Long from Service to Claim - the date of service billed is beyond the parameters set by the provider‘s contract for timely billing 27 MAX - Billed Max Units - procedure is set up on system to pay a designated number of units for a date of service and claim was received billing more than this amount PA - Paid as Claimed – claim paid as billed PAR - Prior Authorization Required - authorization for the service billed must be obtained PLA - Paid Less than Claimed - paid at contracted amount which is less than billed amount QAL - Quantity Over Approved Limit - units are already used for the authorizationnot enough units in the authorization to cover services billed SNB - Service Not in Benefit Plan - the code billed does not appear in the provider‘s contract of billable services VOID - Void Claim - previously paid claim line has been voided and money is taken back Resubmitting a claim Providers should only resubmit a claim for the following reasons: The paper claim was returned with a Claim Send Back Form describing claim defects that must be corrected The electronic claim file was not processed The claim was denied Providers should not submit claims that have already been processed and paid even if the claim did not pay as intended or authorized. These claims will need to be reviewed by Provider Service for possible reconciliation. Claims Appeal Process For claims denied based on processing guidelines (denials that do not involve medical necessity criteria) the provider must submit a request in writing to the Provider Service Team ([email protected]) within 60 days of the rejection. Provider must submit all necessary information required to assist in the review of the appeal. Provider Service will review the appeal and respond to the provider in writing within 30 days of receiving the request for appeal. If the decision is to process the claim, the provider has 30 days to submit the claim to Provider Service for processing. Please note: this does not apply to claims that were rejected for not being a "clean claim" such as rejections for invalid member ID or service not in benefit plan. When the provider has all the necessary information to submit a clean claim, the Provider can resubmit. Fraud and Abuse Gateway is committed to the prevention of fraud and abuse. Examples include: Billing for nonexistent or unnecessary medical services Billing for professional services rendered by personnel lacking appropriate credentials to provide the service 28 Double Billing - billing Medicaid and another insurance company for the same procedure It is Gateway‘s policy to vigorously enforce all Federal and State statutes related to the filing of false claims. If Gateway has reason to believe a Provider may have committed fraud or abuse, the Quality Improvement or Compliance department, or designee, will conduct a thorough review including reviewing claim forms, medical records, progress notes, staffing levels and attendance records and other documents as necessary. The absence of substantive documentation of the delivery of billed services will be construed as presumptive evidence that such services were not delivered and will be considered as evidence of possible fraud or abuse or violation of the Medicaid False Claims Act. Gateway is required to report to the appropriate agencies if there is suspected fraud or abuse. If the fraud and abuse allegation is substantiated, Gateway will require repayment of involved funds and will review the Provider for further contract sanctions up to and including termination. 29 Section IV Financial Management Introduction Gateway is committed to maintaining accurate and complete financial information relative to payment for services provided to eligible Consumers. Ability to Pay It is the policy of Gateway to monitor contract providers regarding ability to pay determination parameters as prescribed within the Michigan Mental Health Code and, as applicable, Medicaid regulations. Providers are to establish guidance and implement protocol for Provider‘s staff and subcontractors for the collection of ability to pay information for uninsured and under insured Consumers. Gateway has adopted the following, as allowable under applicable Federal laws, regulations, and waivers, as their operational oversight procedures regarding compliance with the requirements of Chapter 8 of Michigan‘s Mental Health Code regarding evaluating the ability to pay of consumers who are uninsured or under insured: The fee determination/ability to pay process should be completed by the Gateway provider appointed to perform that role during the first appointment or as soon as practical after the start of services. For a consumer who receives inpatient services on a voluntary basis, the hospital shall perform its statutory duty to determine the responsible parties‘ insurance coverage and ability to pay as soon as practical after the individual is admitted. Consumer fees shall be reassessed annually or at re-entry, which ever is first or if there is any substantial change in the consumer‘s financial status. Providers shall charge responsible parties for that portion of the financial liability that is not met by insurance coverage. Providers shall not impose charges in excess of ability to pay or impose an undue financial burden on the individual or the individual‘s family members. An individual shall not be denied services because of the inability of responsible party to pay for services. As stated in the Mental Health Code, ―If an individual is covered, in part or in whole, under any type of insurance coverage, private or public, for services provided directly by or by contract with the department or a community mental health services program, the benefits from that insurance coverage are considered to be available to pay the individual financial liability, notwithstanding that the insurance contract was entered into by a person other than the individual or notwithstanding that the insurance coverage was paid for by a person other than the individual.‖ 30 If the responsible party believes the figures used to determine their ability to pay are not appropriate to their current income status or do not appropriately reflect their ability to pay, they may request a new determination of ability to pay. The responsible party has a right, by means of an administrative hearing, to contest an ability to pay determination. There must be notification to D-WCCMHA or the Michigan Department of Community Health (MDCH) on the appropriate MDCH form. If the responsible party willfully fails to provide relevant insurance coverage information or if the responsible party willfully fails to apply for affordable and available insurance benefits that cover the cost of services provided to the individual by Gateway with funds received from MDCH or D-WCCMHA, the responsible party‘s ability to pay shall be determined to include the amount of insurance benefits that would be available. If the amount of insurance benefits is not known in a case described in this section, the responsible party‘s ability to pay shall be determined to be the full costs of services. After determination of the responsible party‘s ability to pay, providers are required to deduct the ability to pay amount determined above from the amount billed to Gateway. Claims Verification It is the policy of Gateway that all providers submit claims for reimbursement in accordance with all federal, state and local standards. All reimbursed services are subject to review for conformity and accepted medical practice and coverage limitations. Post-payment reviews of paid claims may be conducted to assure that the services, the rendering provider network and setting, were appropriate and comply with the policy. Post-payment review also verifies that services were billed appropriately (e.g., correct procedure codes, modifiers, quantities, etc. and that third party resources were utilized to the fullest extent available (i.e. Coordination of Benefit and Ability to Pay). Examples of parameters for claims verification methodology to be used by Gateway include, but are not limited to: Claims verification of services delivered to persons with serious mental illness including both adults and children. Claims verification of services representative of array of covered services provided by the agency under review. Sample selection based on information from the claims system (Note: at times, the Agency may choose the sample based on their concerns as the Agency retains oversight of the complete process). Claims verification of samples up to 100% of claims/services rendered by any provider for which such verification is in the sole discretion of Gateway determined to be appropriate. A verification process that includes on-site reviews and interviews with members as deemed appropriate by Gateway. 31 Advance notice (optimally two (2) days) to the provider receiving the audit or verification process. Confirmation of the following through an on-site record review based on claims/invoices/encounter data submitted: Services claimed are listed in Chapter III of the Medicaid Provider Manual Services claimed were identified in the Person-Centered Plan Services claimed were documented as provided within the member‘s record Prerequisite services were provided when required Dates of service on submitted documentation match dates of service in onsite record Services were provided by qualified staff with appropriate signature Notification to the provider about deficiencies found and what follow up is required including a Plan of Action or Plan of Correction. Notification to the Agency of any Plans of Correction. Set time frames for follow-up visits. Utilization of the Network‘s Scope and Severity Protocol for assessing provider performance deficiencies and imposing remediation sanctions. Remedies/sanctions may include, but are not limited to: A written Plan of Action or Plan of Correction A ban on new referrals Holding of claims during an investigation period Reimbursement of funds Reporting to appropriate licensing/law enforcement agencies Termination of contract The False Claims Act applies when a company or person: Knowingly presents (or causes to be presented) to the Federal Government a false or fraudulent claim for payment, Knowingly uses (or causes to be used) a false record or statement to get a claim paid by the Federal Government, Conspires with others to get a false or fraudulent claim paid by the Federal Government, Knowingly uses (or causes to be used) a false record or statement to conceal, avoid, or decrease an obligation to pay or transmit money or property to the Federal Government. The government is no longer required to prove that a physician or another claimant had a specific intent to violate the law. If Gateway has reason to believe a provider may have committed fraud or abuse, the Compliance Department, or a designee, will conduct a thorough review of claim forms, medical records, progress notes, staffing levels, attendance records and other documents as necessary. 32 The absence of documentation of the delivery of billed services will be considered evidence that such services were not delivered and will be considered as evidence of possible fraud or abuse or violation of the Medicaid False Claims Act. If the fraud and abuse allegation is substantiated, Gateway will require repayment of involved funds and will review the contract and implement contract sanctions up to and including termination of the contract(s) 33 Section V Clinical Services Introduction Gateway is responsible for managing a wide array of clinical services. Gateway staff manages inpatient psychiatric hospitalizations and partial hospitalizations, residential placement, ACT, Skill Building and Home-based services. Emergency Procedures Gateway emergency services are available 24 hour per day, 365 days per year by calling (313) 262–5050 or (800) 973-4283. The phone is answered by Gateway‘s Customer Services Department who can assist you in a crisis/emergency situation either with information and referral and/or direct transfer to the delegated crisis screening staff. The policy and procedures are as follows: All members requiring screening for inpatient hospitalization will have this service available face-to-face, as needed, within the 30-minute, 30-mile contract standard. Appropriately trained staff shall complete all such screenings and all dispositions shall be made within three (3) hours of the referral. Gateway strives to ensure the health and safety of the people and communities we serve, ensure continuity of clinical care for the people we serve, and meet contractual performance standards with the Detroit-Wayne County Community Mental Health Agency. Residential Emergency Contact Procedures Contact Gateway at 313-262-5050 or 1-800=973-4283 24 hours per day, 365 days per year. All emergencies are communicated to Gateway and the primary provider Case Manager. A supervisor should always be available. If the situation is emergent and you are not able to reach an appropriate provider staff, contact Gateway at 800-973-4283 or 313262-5050. In cases of an immediate, life-threatening medical or psychiatric concern, the Direct Care Staff should first employ all lifesaving measures and/or call the Fire Department, Police Department, Ambulance (e.g. call 911), or transport the person to the nearest Emergency Room (depending on the specific circumstances). The Direct Care staff should then notify the appropriate primary provider case manager and Gateway. For psychiatric, behavioral and non-medical emergencies (such as violation of behavioral agreement or failure to respond appropriately to staff on duty) it is the goal of Gateway Community Health to keep the individual stable and in the community as much as possible. 34 Towards this goal, we request the Provider and/or the Direct Care Staff should, using their best judgment of the situation, to first contact the responsible clinical staff using the directions above. Clearly state: Your name and name of provider/home Gateway Member‘s name The nature of the concern (briefly) The staff directly involved with the case may be referred to a clinical care coordinator to receive recommendations on how to best deal with the situation and may, in some cases, be able to avoid the need for removing the individual from the setting. If there is a need for a face to face psychiatric screening, a referral will be made to the appropriate screening agency; Detroit Receiving Hospital Crisis Center for adults and Children‘s Hospital of Detroit for children. For medical matters (such as resident illness, physical symptoms/complaints) the resident should be taken to the hospital. For medication refusal, complete an Incident Report and follow the Detroit-Wayne County Community Mental Health Agency guidelines for Incident Reports and deliver them as instructed (see below). Incident Reports: All Incident Reports are to be completed and faxed, within 24 hours, to the DWCCMHA ORR at (313) 833-2043, the QI department at (313) 263-2453 or (313) 263-2513, and the responsible CMHC. Evacuations: In situations resulting in the need to evacuate the living site, it is expected that each provider has emergency plans in place. Once the situation has been stabilized and all residents are safely accounted for, notice should be given to Gateway Community Health using the Incident Report process described above. Any emergency contact with Gateway should be referred to 800-973-4283 or 313-262-5050. Person Centered Planning It is the policy of Gateway that Person Centered Planning techniques and philosophy will be utilized when developing Individual Plans of Service for services and supports offered by Network contracted providers. Person Centered Planning is a highly individualized process designed to respond to the expressed needs/desires of the person. Each person has strengths and the ability to express preference and to make choices. The person‘s choices and preferences shall always be honored and considered, if not always granted. Each person has gifts and contributions to offer to the community, and has the ability to choose how supports, services and/or treatment may help them utilize their gifts and make contributions to community life. Person-Centered Planning processes maximize independence, create community connections, and work towards achieving the person‘s dreams, goals and desires. A person‘s cultural background shall be recognized and valued in the decision- making process. 35 The Person Centered Plan is that person‘s vision of what he/she would like to be and do. The plan is not static, but rather it changes as new opportunities and obstacles arise. It contains the listing of services and supports agreed upon during the PersonCentered Planning process. It describes the goals, the supports needed specific to amount, scope, frequency and duration, who is responsible for working on the goal and the target date for goal completion. Capacity Building - focuses on the person‘s gifts, talents, and skills rather than deficits. It builds upon the person‘s capacities and affords opportunities which will reasonably encourage the person to engage in activities that promote a sense of belonging in the community. Person Centered Focus - the focus is continually on the person for whom the plan is being developed, and not on plugging the person into available slots in a program. The person‘s choices and preferences must be honored. Network Building – the process brings together people who care about the person, and are committed to helping the person articulate their vision of a desirable future. They learn together and invent new courses of action to make the vision reality. Outcome Based – the plan focuses on increasing any or all of the following experiences which are valued by the person: 1. Growing in relationships or having friends. 2. Contributing or performing functional/meaningful activities. 3. Sharing ordinary places or being part of their own community. 4. Gaining respect or having a valued role which expresses their gifts and talents. Community Accountability – the plan will assure adequate supports when there are issues of health and safety, while respecting the person‘s dignity as a fully participating member of the community. Standards Persons have the right (regardless of age or level of care setting) to direct the planning for support services and/or treatment, and shall be informed of this right at admission and again during the process used to plan their care. Prior to the development of the Individual Plan of Service, the person will be allowed to express a preference for which individuals to involve in the preplanning and planning process. This may include involvement of specific family members, advocates, or other professional staff who are supporters of the person. Plans of service shall be developed in a manner that promotes the person‘s strengths, needs, abilities, and preferences. For people participating in programs where a ―brief therapy‖ protocol is employed, these standards still apply and the person will be given the opportunity to involve family or other community persons, as they may desire. Services must be delivered in a manner that is flexible and accommodating to the needs of the person and their support network, particularly in regard to meeting times. 36 Person-Centered Plans shall use adequate supports to safeguard persons in the community, while respecting their dignity. Whenever the person‘s Person-Centered Plan would cause them to be at risk for harm to self or others, issues of health and safety shall take priority. Complaints made regarding the failure to use a Person-Centered Planning approach shall be accommodated by offering the right to appeal. If the person is not satisfied with the results of the appeal, complaints shall be investigated by the Office of Recipient Rights. The appropriate staff will assess the person‘s degree of satisfaction with their ability to participate in the treatment planning process through such tools as satisfaction questionnaires or other feedback methods. Person-Centered Planning (PCP) Practice Guidelines - Essential Quality Elements Person-Centered Planning is a process in which the person is provided with opportunities to reconvene any or all of the planning processes whenever he/she wants or needs. The process encourages strengthening and developing natural supports by inviting family, friends and allies to participate in the planning meeting(s) to assist the person with his/her dreams, goals and desires. The development of natural supports shall be viewed as an equal responsibility of the supports coordinating agency and the person. The supports coordinating agency, in partnership with the person, is expected to develop, initiate, strengthen and maintain community connections and friendships through the Person-Centered process. The person is provided with the options of choosing external independent facilitation of his/her meeting(s) as part of the pre-planning process, unless the person is receiving short-term outpatient therapy only or medication only. Before a Person-Centered Planning meeting is initiated, a pre-planning meeting occurs. In pre-planning, the person chooses: Dreams, goals, desires and any topic about which he/she would like to talk; Topics he/she does not want discussed at the meeting; Who to invite; Where and when the meeting will be held; Who will facilitate; and, Who will record; All potential support and/or treatment options (array of mental health services including Medicaid-Covered Services and Alternative Services and Mental Health Code-required services) to meet the expressed needs and desires of the person are identified and discussed. Health and safety needs are identified in partnership with the person. The plan coordinates and integrates services with primary health care. The person is provided with the opportunity to develop a crisis plan. Each Individual Plan of Service must contain the date the service is to begin, the specified amount, scope, frequency, duration and who will provide each authorized service. Alternative services are discussed. 37 The person has ongoing opportunities to express his/her needs and desires, preferences, and to make choices. This includes: Accommodations for communication, with choices and options clearly explained, shall be made. To the extent possible, the person shall be given the opportunity for experiencing the options available prior to making choice/decision. This is particularly critical for persons who have limited life experiences in the community with respect to housing, work or other domains. Persons who have court-appointed legal guardians shall participate in PersonCentered Planning and make decisions that are not delegated to the guardianship papers from the court. Persons are provided with ongoing opportunities to provide feedback on how they feel about the service, support and/or treatment they are receiving, and their progress toward attaining valued outcomes. Information is collected and changes are made in response to the person‘s feedback. Each person is provided with a copy of his/her Individual Plan of Service within 15 business days after the meeting. When a person is in an urgent/emergent situation, the goal is to get the person‘s crisis situation stabilized. Following stabilization, the person and supports coordinating agency will explore further needs for assistance and if required, proceed to a more in- depth planning process. The Individual Plan of Service can be redone or amended prior to the annual date due to significant change(s) or to meet the wishes of the person. The person must be notified of their right to appeal/dispute the recommendations in the PCP at the time of the PCP meeting. Such notification shall be documented in the medical record. Staff engaged in completing PCPs shall have evidence of ongoing training in PersonCentered Planning available in their personnel records. Family-Centered Services are required for all children, and the following criteria must be met: Service delivery shall concentrate on the child as a member of the family, with the wants and needs of the child and family integral to the plan developed. Parents and family members of minors shall participate in the Person-Centered Planning process unless: The minor is 14 years of age or older and has requested services without the knowledge or consent of parent, guardian or person in loco parentis within the restrictions stated in the Mental Health Code; The minor is emancipated; or The inclusion of the parent(s) or significant family members would constitute a substantial risk of physical or emotional harm to the person or substantial disruption of the planning process as stated in the Mental Health Code. Justification of the exclusion of parents shall be documented in the clinical record. 38 Crisis Planning It is the policy of Gateway that those Persons receiving services shall be offered an opportunity to work with their treatment team to develop a crisis plan which could be implemented when needed. The purpose is to establish guidelines for clinical staff in utilizing the Crisis Plan as part of the Person-Centered Planning Process in the development and implementation of an Individualized Plan of Service and to assist consumers in contingency planning for crisis situations, this may occur due to stress or decomposition. A Crisis Plan is a plan of action to be implemented in the event of a medical or psychiatric emergency. This plan is also a plan of prevention. Although a Crisis Plan is not mandatory, the offer to complete a Crisis Plan is required by the Michigan Department of Community Health (MDCH) and the Detroit-Wayne County Community Mental Health Agency (DWCCMHA). A Crisis Plan is a part of the Person-Centered Planning Process. An emergency situation is a situation wherein the individual can reasonably be expected, in the near future, to physically injure himself, herself, or another person; is unable to attend to food, clothing, shelter or basic physical activities that may lead to future harm; or the individual‘s judgment is impaired leading to the inability to understand the need for treatment resulting in physical harm to self or others. Contractors/subcontractors contracted with Gateway shall have a policy and procedure regarding Crisis Planning. Consumers shall receive information regarding the development of a crisis plan. Contractors/subcontractors contracted with Gateway shall offer individuals receiving mental health services the opportunity to develop a crisis plan whenever necessary and minimally as a part of the Person-Centered Planning Process. Consumers shall make the decision to develop a crisis plan or decline developing such a plan. The Crisis Plan will include all of the following elements: Those symptoms that would indicate to others that they need to take action in the consumer‘s behalf. How the consumer has handled this crisis in the past to help them feel safe, healthy, and have a better quality of life. Medications the consumer is currently taking, those that might help in a crisis and those that should be avoided. Treatments that the consumer prefers and those that should be avoided. Actions that others can take that would be helpful in the crisis. Actions by others that should be avoided during the crisis. Past and present supports available to the person. Consumer should have input into the handling and preventing of the crisis situation. 39 Services and supports must be based upon health and safety needs, as well as personal preference. Health and safety of someone must always be considered and protected. A Crisis Plan shall not take the place of a Safety Contract. Who the consumer would want to take this action. The Crisis Plan shall be reviewed and revised as necessary but minimally on an annual basis. Advanced Directives Gateway ensures the right of their members to issue advance directives. Network providers who provide 24-hour care will seek out these directives from the members and offer referral information on ways members can issue these directives. Providers will have policies in place that outline their implementation of advance directives. Advance Directive is a legal document allowing a person to give directions about future medical care or to designate another person(s) to make medical decisions if he or she should lose decision-making capability. Advance directives may include living wills, durable powers of attorney, or similar documents describing the preferences of the member. Providers of services will have available information and referral to appropriate sources to assist those members who wish to initiate an advance directive. During the intake process providers will, whenever possible, ask the member at intake if they have an Advance Directive in place. Members who are dying will be counseled during treatment about advance directives. Particular attention will be paid to advance directives in developing pain treatment or pain management plans. A copy of the Advance Directive will be kept in the clinical record, and any cases of dying individuals that are transferred to another provider will include the directive in the transferred paperwork. The issue of advance directives must be addressed in the personcentered plan when the plan includes pain treatment or pain management. Information and referral to an appropriate source will be made available to those members inquiring about issuing an advance directive. This right extends to all adults or their designated decision-maker and is not limited to those with a diagnosed terminal illness. Network providers including those in 24-hour care settings will have a policy in place for making decisions about withholding resuscitative services, or forgoing or withdrawing lifesustaining treatment which is based on the member‘s advanced directive. The policy will identify the service provider‘s position on initiating or removing life-sustaining treatment. 40 Those providers whose policy is never to withhold resuscitation will inform the member and/or their families of this policy. Gateway Community Health Provider contracts will reflect the requirement of advance directives where necessary. Coordination of Care It is the policy of Gateway that community mental health services shall be coordinated with primary health care services, Medicaid Health Plans (MHPs), Substance Abuse Coordinating Agencies, Individual Practitioners, Public Health Agencies and other General Health Care Providers, utilizing the Person-Centered Planning (PCP) process. This is a Network policy that applies to Gateway and their Contracted Service Providers. Gateway and their contracted providers shall meet or exceed the following: Ensure coordination of care utilizing the PCP process, which clearly defines the services and supports needed to achieve individualized goals. Ensure the Person-Centered Planning Process clearly defines respective responsibilities and health–related services when persons are jointly served. Ensure full access to complaint/grievance/appeal processes, which enforce each Person‘s IPOS/PCP rights. Ensure adherence to this policy, including development, implementation and monitoring of any policies and procedures be carried out with competent regard for cultural, ethnic, gender and community values, and sensitivity for cultural diversity. Develop internal procedures that describe the step-by-step process of Coordination of Care with Primary Health Care Providers and Medicaid Health Plans. Ensure the development, implementation, and monitoring of procedures to coordinate care with substance abuse contractors (individual practitioners, public agencies, and/or their designees) for Persons who are receiving ongoing services and supports. Ensure referral to the appropriate community resources when services requested by the Person are not available on site. Provide information to Persons receiving services, their guardians and parents of minor recipients about the availability of family planning and health information. 41 This information shall include a statement that receiving mental health services does not in any way depend upon requesting family planning services or health information services. Maintain updated information regarding licensure, controlled substance and Drug Enforcement Administration registration information for physicians. Ensure procedures are developed and implemented for notifying the Medicaid Health Plan, consulting with practitioners prior to prescribing medication, and sharing complete and updated medication records. Receive referrals from Medicaid Health Plans for person‘s under the age of 21, as a result of the Early Periodic Screening Diagnostic and Treatment assessment Psychiatric Consultations on a Medical Floor Gateway reimburses for psychiatric consultations on a medical floor for an eligible Gateway Medicaid member per the requirements of the Detroit-Wayne County Community Mental Health Agency contract. The physician must be appropriately credentialed through the hospital‘s credentialing process where services are provided. Gateway will allow for one psychiatric consultation and one follow up consultation without requiring prior authorization. Services after these initial sessions are to be preauthorized by Gateway. Covered Codes – Gateway is responsible for payment of the following codes: 9925199260 and 90862 in accordance with Medicaid Standards and Medicaid Fee Screens. Contracting process may take place after services have been rendered to consumers as this service may require an immediate psychiatric consult to determine mental status. The Physician must still meet contracting requirements before reimbursement can be made. Upon receipt of the required information, Gateway will determine if the physician has been disbarred from participating in any Medicaid programs. Physicians are issued an agreement to sign. This agreement must be in place before payment to the physician can be made. Upon completion of the contracting process, physician will be issued a provider number which is needed to bill for services. The physician will be sent a copy of the agreement. Claims processing - Physician or designee will be educated on submission of a HCFA 1500 form to the claims processing department. Clean claims will be paid in accordance with contract standards and within 45 days of receipt of the claim. Claims should be submitted within 60 days from the date of service and in accordance with Medicaid standards. 42 Targeted Case Management Providers of Targeted Case Management must demonstrate the capacity to provide all core requirements specified below and have sufficient number of staff to meet the needs of the target population. Case management services are to be delivered in accordance with the requirements of Chapter Three Section 13 of the Michigan Department of Community Health Medicaid Provider Manual. The determination of the need for targeted case management services must occur at the completion of the intake process and through the person-centered planning process for consumers receiving services and supports. Justification as to whether case management is needed must be documented in the consumer‘s record with alternative recommendations when appropriate. Targeted case management is a covered service that assists beneficiaries to design and implement strategies for obtaining services and supports that are goal-oriented and individualized. Services include assessment, planning, linkage advocacy, coordination and monitoring to assist beneficiaries in gaining access to needed health and dental services, financial assistance, housing, employment, education, social services and other services and natural supports developed through the person-centered planning process. Targeted case management is provided in a responsive, coordinated, effective and efficient manner focusing on process and outcomes. A primary case manager must be a qualified mental health or mental retardation professional (QMHP or QMRP); or if the case manager has only a bachelor‘s degree but without the specialized training or experience they must be supervised by a QMHP or QMRP who does possess the training or experience. Services to a child with serious emotional disturbance must be provided by a QMHP who is also a child mental health professional. Services to children with developmental disabilities must be provided by a QMRP. Targeted Case Management services must be available for all children with serious emotional disturbance, adults with serious mental illness, persons with a developmental disability and those with co-occurring substance use disorders who have multiple service needs, have a high level of vulnerability, require access to a continuum of mental health services and/or are unable to independently access and sustain involvement with needed services. Core Requirements Assuring that the Person-Centered Planning process takes place and that it results in the individual plan of service. Assuring that the plan of service identifies what services and supports will be provided, who will provide them, and how the Case Manager will monitor (i.e., interval of face-to-face contacts) the services and supports identified under each goal and objective. 43 Overseeing implementation of the individual plan of service, including supporting the consumer‘s dreams, goals, and desires for optimizing independence; promoting recovery; and assisting in the development and maintenance of natural supports. Assuring the participation of the consumer on an ongoing basis in discussions of his plans, goals, and status. Identifying and addressing gaps in service provision. Coordinating the consumer‘s services and supports with all providers, making referrals, and advocating for the consumer. Assisting the consumer to access programs that provide financial, medical, and other assistance such as Home Help and Transportation services. Assuring coordination with the consumer‘s primary and other health care providers to assure continuity of care. Coordinating and assisting the consumer in crisis intervention and discharge planning, including community supports after hospitalization. Facilitating the transition (e.g., from inpatient to community services, school to work, dependent to independent living) process, including arrangements for follow-up services. Assisting beneficiaries with crisis planning. Identifying the process for after-hours contact. Assessment: The provider must have the capacity to perform an initial written comprehensive assessment addressing the consumer‘s needs/wants, barriers to needs/wants, supports to address barriers, and health and welfare issues. Assessments must be updated when there is significant change in the condition or circumstances of the consumer. The individual plan of services must also reflect such changes. Documentation: The consumer‘s record must contain sufficient information to document the provision of case management, including the nature of the service, the date, and the location of contacts between the Case Manager and the consumer, including whether the contacts were face-to-face. The frequency of face-to-face contacts must be dependent on the intensity of the consumer‘s needs. The Case Manager must review services at intervals defined in the individual plan of service. The plan shall be kept current and modified when indicated (reflecting the intensity of the consumer‘s health and welfare needs). A consumer or his/her guardian or authorized representative may request and review the plan at any time. A formal review of the plan shall not occur less often than annually to review progress toward goals and objectives and to assess consumer satisfaction. Monitoring: The Case Manager must determine, on an ongoing basis, if the services and supports have been delivered, and if they are adequate to meet the needs/wants of the consumer. Frequency and scope (face-to-face and telephone) of case management monitoring activities must reflect the intensity of the consumer‘s health and welfare needs identified in the individual plan of services. All eligible consumers shall be informed of case management services. 44 All eligible consumers shall be offered a choice of Case Managers when available. Case Managers shall clearly document the consumer‘s eligibility for case management services in their evaluation and assessment. Case Managers shall document in the Individual Plan of Service (IPOS) the case management services that the consumer and support system are to receive. The IPOS shall be in the form of goals, objectives, and interventions. Case Managers shall document in the IPOS the exploration and use of natural supports and community resources in assisting the consumer and his or her support system to achieve their desired goals. Case Managers shall document in the IPOS the amount, scope, frequency and duration type of case management services that will be provided, including the frequency of direct face to face monitoring contracts, which shall occur as necessary and no less than monthly. Case Managers shall document in the IPOS the interval at which the IPOS shall be reviewed. They shall also document the amount, scope frequency and duration of the services to be received in terms the consumer can understand. Case Managers shall review the IPOS at the interval identified on the IPOS. This review shall include progress toward goals and objectives, appropriateness of treatment goals/objectives, consumer and his or her support system‘s satisfaction with case management services, and the consumer and support system‘s ongoing appropriateness for case management services. This review shall be documented in the case record. Case Managers shall document in the IPOS services that are not available and the alternative services that will be provided. Case Managers shall deliver case management services as identified in the IPOS. This delivery of services shall be clearly documented in the case record. Individual Plan of Service. The Contracted Provider shall participate in the preparation of an IPOS for each Gateway designated Consumer and to implement all applicable goals and objectives. The IPOS shall detail the specific plan for Covered Services the Consumer will receive from the Contracted Provider while in the Contracted Provider's care, custody and supervision. The Contracted Provider shall furnish all Covered Services identified as being the responsibility of the Contracted Provider in each individual Consumer's IPOS. The IPOS shall detail the nature of the service needs, as well as time frames and measurable outcomes associated with goals and expectations in the IPOS. The IPOS shall also detail the Contracted Provider‘s role in meeting the identified goals. The plan for the Consumer‘s movement back into the Consumer's family setting, or semiindependent, independent, or other living arrangement in the least restrictive setting shall be included in the IPOS and carried forward wherever possible and appropriate. 45 Each Consumer‘s IPOS is incorporated into this Agreement by reference, included in the scope of Contracted Provider‘s Covered Services under this Agreement, and shall represent part of the Contracted Provider‘s contractual obligations herein. Each IPOS, and any amendment to the IPOS, must be pre-approved in writing by Gateway or its designee in order for Covered Services to be eligible for payment to Contracted Provider hereunder. The Contracted Provider shall obtain and maintain a copy of the current IPOS for each Consumer at the Contracted Provider‘s Residential Facility in addition to the home records. Any Consumer‘s IPOS shall be made available to Gateway upon request. Contracted Provider shall maintain these records for a period of at least six (6) years. Case Managers shall monitor on an ongoing basis the welfare and safety of the consumer. This shall be documented in the case record. Minimally this will include one face-to-face contact per month in their living environment. Case Managers shall be supported by the Contracted Provider or Subcontractor, and not limited, in the information they provide about the availability of, and access to, the full array of services and supports available to the consumer and his or her support system. Case Managers shall demonstrate coordination with the consumer‘s primary care physician regarding health issues/problems/concerns. For consumers age 21 or under, Case Managers shall demonstrate informing the consumer with Medicaid insurance and his or her support system of the availability of EPSDT services, and shall link the consumer and his or her support system to these services, when appropriate. For consumers age 21 or under, Case Managers shall demonstrate coordination with the consumer‘s primary care physician regarding EPSDT services. The Contracted Provider or Subcontractor must maintain an up-to-date resource manual that can be conveniently accessed and used by the Case Managers. The resource manual shall be updated on a yearly basis and shall include a listing of informal and formal community resources. The listing for the resource shall include the types of services provided, eligibility criteria, and names and locations of the referral source. Case Managers shall receive a minimum of 24 hours of training per year in the area of case management and/or supports coordination specific to the population they work with. Training will encompass sessions on the Gateway Case Manager Technical Assistance Manual. The Contracted Provider or Subcontractor shall maintain a record of these training hours. The Contracted Provider or subcontractor shall maintain consumers‘ records consistent with Gateway and Detroit-Wayne County Community Mental Health Agency‘s policies and procedures. 46 Consumer‘s records shall be reviewed on an ongoing basis as part of the Contracted Provider or Subcontractor‘s quality assurance/quality improvement program. The Case Manager will identify for consumers the after-hours clinical contact information. The Case Manager assists and coordinates the discharge plan with the hospital discharge planner and the outpatient treatment team. If a residential placement is needed or requested, the hospital treatment team representative or provider Case Manager will contact Gateway residential placement staff and fax a placement packet. The Case Manager for children‘s services obtains a placement packet on children to be placed in a child caring institution. The packet is forwarded to the children‘s placement manager for review. Final decisions for placement of children in child caring institution are made in Gateway‘s Children Unit. The Case Manager will communicate information regarding consumers to Gateway Community Health Clinical Care Managers and assist in coordinating/developing crisis plans. Requirements for Community Living Support Staff and Respite Workers Individuals who provide CLS must: Be at least 18 years of age. Be able to practice prevention techniques to reduce transmission of any communicable diseases from themselves to others in the environment where they are providing support. Have a documented understanding and skills in implementing the individual plan of services and report on activities performed. Be in good standing with the law (i.e. not a fugitive from justice, a convicted felon, or an illegal alien). Be able to perform basic first aid and emergency procedures. Have successfully completed the Medication I, Medication II, Working with People I and Working with People II modules of the Direct Care Staff training Be trained in Recipient Rights annually. Be an employee or contractor of a Gateway contracted provider of Community Living Supports in an Unlicensed Setting (H0043). Additional requirements: a. Background checks: Must have a valid driver‘s license for at least 3 years and currently be insured Drivers must have appropriate class license for driving vans, school buses or larger trucks, as applicable (consumers cannot be used as drivers) 47 b. c. d. e. f. g. No major violations in the last 3 years o DWI, DUI, OUI, OWI, refusing to take a substance test, driving with an open container of alcohol, negligent homicide or manslaughter using a motor vehicle, operating a vehicle while in the commission of a felony, aggravated assault with a motor vehicle, permitting an unlicensed person to drive, reckless driving, fleeing or evading the police/roadblock, resisting arrest, speed contest, hit and run (bodily injury or property damage), failure to report an accident, illegal passing of a school bus, or leaving the scene o Staff that transport members cannot have any drunken driving offenses on their record, even if it was a misdemeanor charge. No more than 8 points, broken down as follows: o Maximum of 1 moving violation in the last 3 years in combination with one at fault accident, or o Maximum of 2 moving violations in the last 3 years with no atfault accidents or o Maximum of 2 at-fault accidents in the last 3 years with no moving violations Contracted providers must check driving record and criminal record before they can start work and every year thereafter. o See Attachment F for additional background check information CPR/First Aid: Certification must be obtained within 30 days of starting work. Certification will last to the expiration date identified by the trainer. The expiration dates need to be tracked by the staffing agency as part of their routine personnel procedures. Recipient Rights (RR) Training: The standard is within 30 days for new hires and annually thereafter TB test and blood borne pathogens (BBP) training: The standard is within 30 days of hire and annually thereafter. Other Requirements: Photo ID Social Security Card I-9 form (citizenship) At this time, finger printing is not required for Community Living Support Staff, Family Friend Respite workers, Respite workers, and/or Hospital Sitters. All of the above standards apply for Respite workers with the exception of Family Friend Respite workers. For staff working only as Family Friend respite workers the standards are as follow: Photo ID Social Security Card No background check is required for this class of worker 48 Verification Guidelines for Community Living Support Staff and Respite Workers Contracted providers of Community Living Support Staff and/or Respite shall take the following steps to ensure the Medicaid covered services and supports paid for and reported to Gateway were delivered appropriately: 1. White out is not to be used on timesheets. All timesheets shall be original documents and any errors need to have a single line drawn through them and need to be initialed by the person correcting the error. Timesheets are not to be pre- signed and copied. 2. Timesheets are not to be reused. 3. Timesheet must be dated and signed by the paid support staff. The consumer name and an authorized signature (typically the individual consumer or their family member will counter-sign the timesheets) must be on each timesheet. 4. A progress note is to be filled out that indicate what was done for/with the consumer during the time worked. This documentation should relate back to the specific reasons/ goals for the staffing identified in the Person-Centered Plan. 5. Consumer families need to fill out an “authorized signature” (for whoever will be countersigning the timesheets). This signature can then be used to verify signatures on timesheets. 6. Any unusual incidents, including but not limited to questionable reporting of time by paid support staff, shall be documented on an Incident Report form and submitted to both the Agency and Gateway per established guidelines. 7. Each paid support staff and persons completing the authorized signature form shall receive information about the False Claims Act, Whistleblowers‘ protections, and any contractor specific policies for detecting and preventing fraud, waste and abuse. Documentation that this information was shared must be kept as part of the personnel file for each paid support staff. 49 Section VI Utilization Management Introduction It is the policy of Gateway to authorize payment in an orderly and efficient manner for all medically necessary covered services requiring such authorization and identified during the Person-Centered Planning process. The authorization process is not intended to interfere with the timeliness of service delivery and the terms and conditions contained herein shall be interpreted strictly in accordance with the terms of individual provider contracts, and as applicable, the terms of the Michigan Department of Community Health Medicaid Provider Manual. Definitions (These definitions are applicable and take precedence over all others within this section of the Provider Manual): Administrative Non-Certification – An administrative communication, issued by a Gateway Director, that a particular service or LOC has not been requested for Certification or Authorization by Gateway in accordance with Gateway authorization request timeframes. Appeal - A request by a member, member-designated representative, or provider acting on a member‘s behalf, to review a medical necessity determination made in response to a request for services. Authorization - Approval for a specific covered service to be delivered as a covered benefit to a covered member. Payment is subject to member eligibility, provider licensure/certification and benefit limits at the time services are provided. A decision rendered by a qualified professional who has been delegated the authority by Gateway, to approve a request for covered clinical services as meeting the clinical care criteria of Medical Necessity. (DWCCMHA/MCPN Contract). When applicable to Medicaid services, Gateway authorization and approval decisions will be made according to level of care guidelines established and published by MDCH in its Medicaid Provider Manual. Authorized Services – Covered services determined by or on behalf of Gateway to be medically necessary and eligible for payment/reimbursement in accordance with the terms of the contract between the provider and the Network, and applicable Medicaid regulations. While all funded services require authorization by Gateway, only specific subsets require prior authorization. Authorized/Certified (or authorization/certification): Means that Gateway, or the representative whom it has designated to perform prior authorization/utilization management on its behalf, has screened the candidate and has approved the inpatient or partial hospitalization, the specialized residential or crisis residential level of care services or ACT, Skill Building or Home-based services to be medically necessary for the individual and has indicated so by providing evidence to the admitting facility. 50 Certification – Confirmation that a particular level of care of a covered benefit has been determined by Gateway, or someone acting on its behalf, to meet the medical necessity criteria prerequisite to authorization of payment. Any inpatient psychiatric admission not certified by or on behalf of DWCCMHA is not a benefit of the Medicaid program. (DWCCMHA/MCPN Contract) Clinical Care Coordinator - A Qualified Professional (Master‘s level clinician, Psychologist, Social Worker or Licensed Professional Counselor, with three years postgraduate experience with appropriate State Licensure licensed registered nurse who has been delegated the authority by Gateway, to review a request for covered clinical services as meeting the criteria of Medical Necessity. Clinical Non-Authorization - Confirmation by a physician that has been authorized by Gateway to do so that a requested service does not meet medical necessity criteria and is therefore subject to denial or other adverse decision. Concurrent Review - The process of determining the medical necessity of extending the delivery of a specific level of care, such as, for, e.g., inpatient hospital, state hospital, partial hospital, crisis residential, or specialized residential/child caring institutional services, ACT, Skill Building or Home-based services when such continued level of care has been requested and the previous authorization has expired. Denial of Authorization - An adverse authorization decision made by or on behalf of Gateway by an authorized health care professional with appropriate expertise, in the case of inpatient hospital, state hospital, partial hospital, crisis residential services, ACT, Home-based or Skill Building. Services. Inpatient Hospital and Partial Hospitalization Services First Level Appeal - The next level of appeal that can be requested following a Reconsideration Review. This level of appeal is performed by physicians authorized to do so on behalf of Gateway. Initial Inpatient Hospital and Partial Hospitalization Services Authorizations - The pre-authorization that permits the admission of the eligible individual into the level of care requested. Inpatient Hospital and Partial Hospitalization Services Reconsideration Review – The first level of appellate review of a denial of authorization for services. A Request for Reconsideration Review must be filed within thirty days of the Clinical NonCertification at issue. The clinical reconsideration is sent to a different physician for review and decision. Inpatient Hospital and Partial Hospitalization Services Second Level Appeal The next level of appeal that can be requested following a First Level Appeal. This level of appeal is performed by Detroit-Wayne County Community Mental Health Agency. 51 Gateway will send the case along with all supporting documentation to the Detroit-Wayne County Community Mental Health Agency for a final determination if the provider has requested the final level of appeal. Length of Stay (LOS) - The number of days that a member remains in a given level of care. (Operations) Level of Care (LOC) - The intensity of professional care required to achieve the treatment objectives for a specific episode of care. (Operations) Level of Care (LOC) Protocols - Severity of Illness/Intensity of Service Protocols provided by the Michigan Department of Community Health (MDCH) and DWCCMHA, each as amended from time to time, as part of a utilization management system, which are intended to monitor the appropriateness of mental health care. Severity of Illness refers to the nature and severity of the signs, symptoms, functional impairments, and risk potential related to the person's complaint. Intensity of Service pertains to the setting of care, to the types and frequency of needed services and supports, and to the degree of restriction necessary to safely and effectively treat the individual. (DWCCMHA/MCPN Contract) Pre-Authorization/Prior Authorization – Any authorization that is required and/or rendered prior to the delivery of particular services or levels of care. Physician – Any physician participating in the utilization review process as an authorized representative of Gateway. PREST – An independent review organization under contract with Gateway comprised of board certified psychiatrists with many specialty areas (i.e., children, elderly, etc.) Provider – as used in the portion of this policy entitled ―Inpatient Hospitalization and Partial Hospitalization Clinical Appeals,‖ means a provider of inpatient hospitalization or partial hospitalization services. Authorization Process Gateway is responsible for both the initial and, if applicable, (based on the service) ongoing concurrent authorizations for those members who meet eligibility criteria. These services require an authorization prior to services being delivered. Gateway is committed to using the highest standards of clinical expertise and managed care. The goal is to provide quality of care and outcomes for members of behavioral health services in the Gateway Community Health. Gateway clinical staff: Develop appropriate utilization management (UM) guidelines and protocols. Review prior authorization requests within established time frames per authorization guidelines. 52 Refine, edit, update and disseminate utilization management criteria to providers and other staff. Integrate utilization of diagnostic formulation, the clinical assessment, the treatment/service plan, and the results of assessments related to requests for prior authorization for appropriate and medically necessary services. The initial authorization/continued stay review process helps to ensure that appropriate services are delivered and that either anticipated progress is being made toward the established clinical goals or the treatment plan is adjusted accordingly. This step allows Gateway to obtain necessary information to document the medical necessity of ongoing care. To request authorization for inpatient services, providers must contact Gateway at 1-800973-4283 or 313-262-5050 24hours a day, 7 days a week. For outpatient services, providers will use the numbers above during normal business hours Monday thru Friday from 8:00 a.m. to 5:00 p.m. If the outpatient provider prefers, information with the request for authorization may be faxed to Gateway at 313-875-4715. For each eligible member for whom the provider has submitted an initial authorization request, there is an initial amount of each service that is authorized for the particular level of care, if the UM criteria is met. To obtain authorization or for re-authorization for additional services the provider should provide clinical criteria prior to the last anticipated authorized service date. This review will include, but is not limited to, the following information: Presenting problem Diagnosis Current symptoms Current level of functioning Prior psychosocial, psychiatric, and substance abuse history and prior treatment Mental status Medications (dosage and side effects) Medical complications and significant medical history Treatment plan and progress toward goals For outpatient authorizations the provider should provide the above information along with an IPOS. Decisions for inpatient decisions are rendered within 3 hours of the time requested. Outpatient authorization decisions are rendered within 3 business days of request. Utilization Guidelines and Management Gateway works proactively with providers to build consensus around the appropriate level of care and treatment plan. Gateway believes that the relationship between treatment standards and clinical judgment is one of assistance and collaboration rather than one of control. 53 To effectively authorize and review care, objective and measurable utilization management criteria based on sound clinical principals and processes have been developed and included in the Michigan Department of Community Health Medicaid Provider Manual. The elements of these service listings are the basis for the Gateway utilization management process. These criteria support fair, impartial and consistent utilization management decision making that services the best interest of our members. Gateway seeks to ensure that each member can access needed services with the appropriate provider, at the correct intensity of service and duration of care with special attention to involvement of, and collaboration with natural and community supports. Inpatient Hospitalization and Partial Hospitalization Clinical Appeals A clinical appeal is a request for a reconsideration of a determination that the requested inpatient hospitalization or partial hospitalization service does not meet medical necessity criteria. There are several levels of appeal available. The inpatient hospitalization and/or partial hospitalization Provider has up to 30 calendar days from the date of issuance of Gateway‘s written Clinical Non-Certification Notice to submit a written request for appeal. Requests received beyond the 30 day time frame will not be eligible for review. A failure to file a timely request for reconsideration and/or appeal of any Clinical Non-Certification determination that has been issued or upheld constitutes constructive agreement with such earlier Clinical Non-Certification and a withdrawal of the previous request for such services or level of care. 1. Reconsideration a. Standard Reconsideration When an adverse determination is made for continued stay in any inpatient hospitalization or partial hospitalization level of care requiring Pre-Authorization and the member is no longer in treatment at that level of care, a standard reconsideration review may be requested by the member, member representative or Provider. The Clinical Care Manager may request the medical record from the provider and forwards the request with relevant documentation to a physician. The member, member representative or Provider must request the reconsideration within 30 calendar days of the date of the written notification of the adverse determination. A Physician reviews pertinent information and makes a determination within 30 calendar days of receipt of the medical record. Notification of the determination will be sent to the member and facility in writing. 54 For cases where a non-authorization determination is upheld, the written notification includes the name of the Physician who rendered the determination, the clinical rationale, and a description of the First Level Appeal process. b. Expedited Reconsideration When an adverse determination is made for continued stay in any prior authorized level of care and the member is currently in treatment, the Care Manager upon request for reconsideration will forward the request for an expedited reconsideration, with relevant documentation, to a Physician. The member, member representative or Provider must request the expedited reconsideration within 2 days of the non-authorization decision. A Physician will attempt to contact the treating physician telephonically, to conduct the review within 2 business days of receipt of the request for expedited reconsideration. The Physician informs the treating physician of his/her determination at the time of the review and explains the first level of the clinical appeal process. Notification of the review determination is generally sent to the member and the treating physician (and/or facility) in writing within two business days of the review. For cases where a non-certification an/or non-authorization determination is upheld, the written notification includes the name of the Physician who rendered the determination, the clinical rationale, and a description of the First Level Appeal process. 2. First Level of Appeal a. Standard First Level Appeal A Standard First Level Appeal is offered when the standard reconsideration is upheld. The Care Manager may request the medical record from the Provider and forwards the request with relevant documentation to a Physician. The member, member representative or Provider must request the Standard First Level Appeal within 30 calendar days of the date of the written notification of the results of the reconsideration. A Physician reviews pertinent information and makes a determination within 30 calendar days of receipt of the medical record. Notification of the determination will be sent to the member and treating provider in writing. 55 For cases where a non-authorization determination is upheld, the written notification includes the name of the Physician who rendered the determination, the clinical rationale and a description of the Second Level Appeal Process. b. Expedited First Level Clinical Appeal An expedited First Level Appeal is offered when the expedited reconsideration is upheld. The Clinical Care Manager requests a copy of the medical record and forwards the request with relevant documentation to a Physician. The member, member representative or Provider must request the First Level Appeal within two (2) business days of receipt of the written notification of the results of the expedited reconsideration. Expedited First Level Appeal for admissions to any prior authorized level of care will be completed within two (2) business days of receipt of the requested clinical information. The Physician informs the attending or treating clinician (or designee) of his/her determination at the time of the review and explains the Second Level Appeal process. Notification of the review determination is sent to the member and the treating clinician (and/or facility, if applicable) in writing within two (2) business day of the review. For cases where a non-authorization determination is upheld, the written notification includes the name of the Physician who rendered the determination, the clinical rationale, and a description of the Second Level Appeal process. 3. Second Level Appeal If the member, member representative or Provider wishes to appeal the results of the First Level Appeal, a Second Level Appeal is conducted by the DetroitWayne County Community Mental Health Agency (DWCCMHA). In expedited cases, the member, member representative or Provider must request the Second Level Appeal within two (2) business days of receipt of the written notification of the results of the first level appeal. The DWCCMHA will make a determination in accordance with the clinical urgency of the request and the member‘s clinical condition. In standard cases, the member, member representative or provider must request the Second Level Appeal within 30 calendar days of the date of the written notification of the results of the first level appeal. The DWCCMHA will make a determination within 30 calendar days of receipt of the clinical information. The DWCCMHA will forward the results of the Second Level Appeal to Gateway who will notify the member and the treating clinician (and/or facility, if applicable) 56 of the review determination within two (2) business days of the determination. 4. A d m i n i st r a t i ve F a ir H e a r in g Medicaid recipients receiving Medicaid-covered services have the right to request an Administrative Fair Hearing at any time after the initial non-authorization determination is made. 5. Alternative Dispute Resolution Process Non-Medicaid recipients or Medicaid recipients receiving services not covered by Medicaid may access the Alternative Dispute Resolution Process after exhausting the Gateway and Agency appeal processes. The Alternative Dispute Resolution Process must be requested within ten (10) business days of notification of the results of the Gateway and Agency appeal processes. Discharge Day in a 24 Hour Setting This policy applies to all contracted facilities that provide 24-hour service (hospital, residential facilities, crisis residential facilities, child caring institutions, etc.) Provider is to follow guidelines as designated in the authorization policies specific to Gateway. Provider will be issued an authorization number for all authorized days/units, provided the consumer meets medical necessity criteria. Once the day of discharge has been determined, authorization will not include payment for the day of discharge in a facility that provides 24-hours of service. These include settings where the individual has been admitted for bed occupancy with the expectation that the individual will remain at least overnight, even when it later develops that the individual can be discharged or is transferred to another facility by 11:59 p.m. and does not use the bed overnight. Days of care provided to a consumer are in units of full days, beginning at midnight and ending 24 hours later. Medicaid covers the day of admission but not the day of discharge. If the day of admission and the day of discharge are the same, the day is considered an admission day and counts as one day. Unless there are extenuating circumstances, the discharge day will not be authorized. Residential Reconsideration Review Residential providers that do not agree with the level of care for their residents as determined by Gateway or the primary provider agency are invited to express their clinical concerns with Gateway through the Appeals department by completing a reconsideration request form. This form is available on the provider portal. It can also be requested through the appeals department. 57 This policy is intended solely to assist Gateway and its primary provider agencies in serving their consumers and expressly does not confer on the residential provider any legal standing or contractual rights of its own to appeal or otherwise contest any level of care determinations made by or on behalf of Gateway or its primary provider agencies. 58 Section VII Quality Improvement Introduction The mission of the Quality Improvement (QI) Department is to institute processes that assure systematic approaches are used to 1) determine the relevant standards and best practices, 2) the processes and activities to assess performance, 3) the measurement of performance against defined standards and/or best practices, and 4) the improvement strategies to improve performance and consumer outcomes. Further, to outline the systematic approach to achieve and measure performance improvement in all operations, both clinical and non-clinical, that impact consumers‘ access, health and safety, quality of life and satisfaction, person-centered planning, service-related processes and outcomes. QI also seeks to create, sustain and enhance a network of culturally aware providers who are committed to delivering quality supports following these same principles in a timely manner. Contact Information L. C. Smith, LMSW, Quality Manager – (313) 263-2452 Incident Reporting Any of the following circumstances and/or situations occurring in a Gateway Residential or Outpatient setting must be reported to Quality Improvement within 24 hours of occurrence. They are: 1. 2. 3. 4. 5. 6. Death of a recipient Physical illness requiring admission to a hospital Accidents requiring emergency room visits and/or admissions to hospitals Serious challenging behaviors not previously addressed in the IPOS Arrest or conviction of recipients Medication errors which could lead to adverse health outcomes All Incident Reports are to be completed and faxed, within 24 hours, to the DWCCMHA ORR at (313) 833-2043, the QI department at (313) 263-2453 or (313) 263-2513, and the responsible CMHC. Death Reporting Definition: The Death Reporting procedure is defined as a procedure to notify Gateway of a consumer‘s death and to process the death of Gateway consumers. 59 STANDARDS: 1. Contracted Providers are to report the death of a Gateway consumer within one (1) business day by calling the 24 Hour number: 1-800-973-4283. During the call the representative will complete the Preliminary Death Report form (see Section XI) using information provided during the call. 2. A Mental Health Professional (excluding Adult Foster Care Home Providers) will complete the Report of Recipient Death (see Section XI) and include all relative documentation/information within ten (10) business days of the consumer‘s death. The Report of Recipient Death should be faxed to GCH Quality Department (313-263-2453). 3. All deaths are Sentinel Events and, as such, require a Sentinel Event Report (see Section XI) to be completed by a Mental Health Professional (excluding the Adult Foster Care Home Provider), within three (3) business days prior to the Report of Recipient Death, or afterwards, depending on the information gathered during the completion of the Report of Recipient Death. The Sentinel Event Report should be faxed to the GCH Quality Manager, at 313263-2453. Sentinel Events It is the policy of the Gateway that occurrences of potential Sentinel Events, and substantiated Sentinel Events, involving Gateway consumers be reported, reviewed, investigated and subjected to a root cause analysis when appropriate. Follow-up action(s) are to be taken in a timely manner and compliant with regulatory and contractual guidelines. Sentinel Events: An unexpected occurrence involving death or serious physical or psychological injury, or the risk thereof. Serious injury specifically includes loss of limb or function. The phrase ―or risk thereof‖ includes any process variation for which a recurrence would carry a significant chance of a serious adverse outcome. Criteria to determine a Sentinel Event are: Death of recipient that does not occur as a natural outcome to a chronic condition (e.g., terminal illness) or old age; Serious illness requiring admission to a hospital (This does not include planned surgeries, whether inpatient or outpatient or admissions directly related to the natural course of the person‘s chronic illness, or underlying condition); Serious injury (including but not limited to an accident or suspected abuse) requiring emergency room or emergency care center visit and/or admission to a hospital. (This includes injuries of sufficient severity to require visits to a hospital and/or medical center urgent care clinics emergency rooms, and/or admissions to hospitals); 60 Serious challenging behaviors not already addressed in a treatment plan and that include significant (in excess of $100) property damage, attempts at self-inflicted harm or harm to others, or unauthorized leaves of absence, for, e.g., a person‘s escape from a locked protective treatment setting; person to person altercation requiring medical attention, person to person sexual assault or occurrence of sexual intercourse while in a locked protective treatment setting; An arrest or conviction of a felony or violent offense. (Police transport to a screening center on a petition is not an arrest). Medication error consisting of (a) wrong medication; (b) wrong dosage; (c) missed dosage; or (d) improperly administered dosage resulting in death or serious injury or the risk thereof. (It does not include instances in which consumers have refused medication.) Credible allegation of sexual abuse, neglect, or exploitation. The purpose of this policy is two-fold: 1. To achieve compliance with DWCCMHA's (the Agency's) "Sentinel Events" policy and peer review process in accordance with the Michigan Mental Health Code, Section 330.2200 and all applicable Federal, State, and Local standards; and 2. To accomplish the goals listed below. The goals of this policy are: 1. To have a positive impact in improving consumer care and preventing Sentinel Events; 2. To focus the attention of this organization on an incident or Sentinel Event to understand the causes that underlie the event, and to make changes in policy or procedures when needed. 3. To increase the general knowledge about incidents, critical incidents or Sentinel Events, their causes, and strategies for prevention. Residential Monitoring Gateway mandates that residential settings where members receive Covered Services are sufficient to ensure the health and safety of those members. Therefore, Gateway routinely monitors residential providers to assess compliance with health and safety standards, and, with any local, state, or federal standards that Gateway, in its sole discretion, deems applicable. Monitoring of Residential Provider Sites An Abbreviated Health and Safety Assessment is performed for all routine monitoring of contracted specialized residential settings where there are Gateway residents and is generally completed on a quarterly basis. 61 A Comprehensive Health and Safety Assessment is performed at least annually. Such assessments may, at the sole discretion of Gateway, be required for other residential settings. Gateway reserves the right to monitor more frequently as, in their sole discretion, they deem appropriate. Health and safety concerns and possible Recipient Rights violations are identified by the Quality Improvement Department and all other appropriate agencies. The assessment will include a face-to-face interview with a member and will include an evaluation of the level to which their health and safety needs are being identified and met. The assessment may include a review of the provider‘s written policy and records for the safeguard and control of Consumer funds. A copy of the assessment will be given to the home provider by the Designated Monitoring Agency. All completed monitoring assessments done within the month are due to Gateway by the 15th of the following month by the monitoring agency. A progress note reflecting the review agent‘s conversation with the consumer in the home, that the consumer‘s chart was reviewed, the date, time, and appropriate service code will be placed in the consumer‘s chart. The Quality Improvement Department or designee reviews all information to confirm the residential setting is or is not in substantial compliance with all rules and guidelines established by Gateway. If the residential site substantially meets health and safety criteria, routine monitoring will continue. If the residential setting does not meet these criteria, remedial action will be required, and a corrective action plan or, if circumstances require, a Plan of Correction is put in place. The cost of any such monitoring is allocated to the impacted provider. The Plan of Correction and implementation is monitored by the Quality Improvement Department or designee. The monitoring can be as frequent as necessary as identified by the Quality Improvement Department. It is the responsibility of the Gateway Quality Improvement Department to ensure all Plans of Correction are kept updated. Providers who are not compliant in implementing the required plans of correction will be subject to review utilizing the Scope and Severity Protocol for remediation due to their non-compliance with contract requirements. Gateway reserves the right to visit any contracted or approved residential setting at any time. All information is kept on file for a minimum of six years. 62 Associated Forms Comprehensive Health and Safety Assessment Abbreviated Health and Safety Assessment Unlicensed Health and Safety Assessment Provider Application Provider Contract Plan of Correction Emergency Preparedness Emergency Preparedness for residential providers and supports coordinators of persons in community settings is very important. All residential providers are required to have an emergency preparedness kit consisting of: 4 oz bottle of water for each consumer Diapers for incontinent consumers Batteries Battery operated radio Flashlights Hand sanitizer/wet wipes Rain ponchos Emergency medical charts List of emergency numbers First-aid kits – travel size Blood-borne pathogen kit Socks/gloves Snacks (such as cheese or peanut butter crackers) Blankets This kit is for use if there is an emergency that requires the staff and consumers to leave the home (i.e. Fire) and designed to meet the immediate needs of consumers until they are relocated. Providers are also required to maintain a three-day emergency food supply. This food supply is separate from the rest of the food supply and must be rotated on a regular basis to avoid the food from becoming out dated. Below is a sample of what the provider is required to have to feed consumers for three days due to an emergency such as a power outage. Emergency Food Supply (enough for 3 days without power) Manual can opener (somewhere in the residence) Powdered milk, which should be labeled grade A and pasteurized, may be used as a beverage in cooking and baking (emergency use only) Canned food Canned fruits Bottled water Items such as Vienna sausage, tuna fish, granola bars Peanut butter Crackers 63 Emergency Sample Menu Breakfast Cold cereal with milk Fruit cup Lunch Tuna/peanut butter sandwiches Chips, Juice or Kool Aid Dinner Canned beans SPAM or canned chicken Canned Fruit Ice tea Snack Peanut butter crackers Granola bars Providers must also maintain compliance with AFC Licensing rules in regards to consumer safety which consist of complying with: Fire Drills Evacuation Assistance Scores (E-scores) Evacuation Difficulty Index Score Protection Plans For specifics of this requirement, please see: www.michigan.gov/cis Go to: Family and Health Services, Adult foster Care, Appendix FA procedure for determining Evacuation Capability Forms for this rating can be found in the NFPA 1985 Life Safety Code handbook or can be purchased at www.nfpacatalog.org As part of the residential monitoring process, providers are monitored on a quarterly basis for compliance with emergency preparedness. If you have additional questions regarding this procedure, contact the Quality Improvement Department or your Provider Service representative. Vehicle Safety It is the policy of Gateway that all contracted providers and subcontractors and their employees who transport consumers will comply with the State of Michigan laws governing seat belt and child restraint seats. Unless an employee or a consumer has a written medical exemption from a licensed physician in their personnel file/case record, seat belts are to be worn by all drivers and passengers. (With the exception of those exemptions listed in Sections 257.710d and 257.710e of the Michigan Vehicle Code, Act 300 of 1949). In order to ensure compliance with State laws, Gateway requires contractors, subcontractors and their employees who transport members adhere to the following standards: Michigan Vehicle Code (Excerpt), Act 300 of 1949. In addition to the Michigan Vehicle Code, all staff and passengers in a 64 vehicle will wear seatbelts whenever the vehicle is in motion unless they have a written medical exemption from a licensed physician or as exempted in Sections 257.710d and 257.7103 of the Michigan Vehicle Code, Act 300 of 1949. Staff who transport consumers whether in their own personal vehicle or a contracted providers vehicle shall possess a valid, unrestricted driver‘s license and or chauffeur‘s license when necessary with current motor vehicle insurance, as well as, valid motor vehicle registration. Contracted providers and subcontractors shall have policy and procedures regarding transportation of consumers and vehicle safety. In the event that a consumer is wheelchair bound and is being transported in their wheelchair staff must ensure that the wheelchair is properly secured in the vehicle. In the event that a consumer displays a pattern of failing to utilize their seatbelt during transportation the Interdisciplinary Team will address this safety issue in the Individual‘s Plan of Service and Behavior Management Committee as appropriate. 65 Section VIII Compliance Gateway is committed to consumers, employees, contractual providers and the community to ensure business is conducted with integrity, in compliance with the requirements of applicable laws and sound business practices, and with the highest achievable standards of excellence. The Gateway Compliance Plan draws on recommendations from the following four major sources: 1. Federal regulators that include the Office of the Inspector General (OIG) of Health and Human Services (HHS) Guidelines. 2. National Legal Compliance experts 3. National Behavioral Health experts 4. National MBHO Accreditation experts The compliance plan provides a framework for Gateway to comply with applicable fraud and abuse statutes, regulations and program requirements. The key intentions of the Compliance Plan are to: Minimize organizational risk and improve compliance with the billing requirements of Medicare, Medicaid and all other applicable federal health care programs. Maintain adequate internal controls (paying special attention to the Agency‘s identified high risk areas. Reduce the possibility of misconduct and violations through early detection. Reduce exposure to civil and criminal standards. Encourage the highest level of ethical and legal behavior from all employees. Educate employees, contract members, Board Members, and stakeholders of their responsibilities and obligations to comply with applicable local, state and federal laws and regulations including licensure requirements, as well as, accreditation standards. Promote a clear commitment to compliance by taking action to uphold such laws, regulations and standards. Provider Monitoring and Site Visits Provider Monitoring and/or Audit visits will be conducted to determine compliance with licensing, contractual and regulatory facility standards. Providers must meet all standards that apply for all audits conducted. In some cases, compliance may be determined by a percentage of compliance, i.e. 95% or higher. In other cases, there must be 100% compliance. 66 New providers will receive reviews before a contract is finalized. Follow up reviews will be scheduled within six months of contract start date. All Providers will receive, at a minimum, an annual audit. Safety and environmental reviews will be conducted, as well as testing for compliance with the Michigan Mental Health Code, and any other related regulatory, and contractual obligations that may include review of staff personnel records training records and clinical compliance. As required, policies and procedures of the organization will also be reviewed. Member charts will be reviewed to determine if appropriate care is being rendered, recorded, and monitored as required. This will include the charts of the Clinical Provider and the AFC Provider, as appropriate. Staff training records will be reviewed to ensure all required training is being completed. AFC personnel audits will include areas such as: Direct Care Worker Training, Recipient Rights, Person Centered Planning, CPR, and First Aid. The Provider will receive Follow up visits, targeted at review of areas of deficiency, which will be conducted on a schedule dependent on the level of violation and type of audit. Providers will receive results of the follow up audits will in writing. Monitoring will also be repeated on a periodic basis to assure that identified corrections have been implemented and are effective, and/or to confirm and document ongoing compliance when no specific problems have been identified. Providers may also receive unannounced site visits by Gateway staff at any time. If a provider has been determined to be sufficiently non-compliant with contract terms or quality of care poses potentially high health, safety or other liability risks unannounced site reviews will be conducted in order to satisfy the concerns or questions as to compliance or performance. Providers must also meet requirements Medicaid Claims and Billing. Providers must be accurate in billing submissions to ensure appropriate billing practices are being utilized that are consistent with CMS, MDCH guidelines and any other contractual arrangements made with GCH. Other Provider documentation requirements include: consumer eligibility for services, whether or not the services provided were identified in the IPOS, if the billing units match case record documentation, staff providing service have appropriate credentials, and other items required by MDCH, D-WCCMHA and/or GCH. Providers will receive results of all audits in writing. Depending on the nature of the non-compliance/level of violation GCH may include the requirement for a submission of a Plan of Correction (POC). 67 The POC will be reviewed by Quality and/or Compliance Department staff. Submission and approval of a POC becomes a legal obligation of the provider under the provider contract. Patterns of deficiencies will be grounds for disciplinary action up to restriction or termination of contracts for network providers and suspension or termination of providers. In preparation for the audit, Providers are Required To: Have all requested charts present and available at the time of the audit. Allow adequate access to the Electronic Medical Records to the charts being audited to allow for the completion of the audit Designate a representative who will be responsible for assisting with the audit process as necessary, i.e. attempting to locate documents within the chart provided, and providing copies of documents requested The representative will, in the cases of identified deficiencies, provide written confirmation by initialing the audit form, and/or comment regarding any disagreement with findings. Gateway will: Furnish a list of the consumer charts to be audited (at least 1 day prior to the audit date.) Review records as they are presented during the audit. Additions to the record that are located in a staff office or other places, cannot be added when the audit has started. Review audit outcomes and coordinate with Finance staff if claims are found to be non-compliant (i.e. – no Treatment Plan, expired treatment plan, billed and paid units do not match service units documented. Antikickback Law Because Gateway and its providers are receiving Medicaid funds, the Federal legislation (Medicare and Medicaid Patient Protection Act of 1987, as amended 42 U.S.C. 1320a-7b.), also known as the ―Antikickback Law‖, is the law that applies. The Act prohibits individuals from soliciting or accepting anything of value including gifts, payments, services, favors or anything else that might appear to influence the actions of the individual. An offer of a gift by a provider to Gateway staff may be interpreted as an attempt to influence actions. That may not have been the intention, but if this action appears to be an attempt to influence, it is prohibited. Providers should never offer a gift of cash or financial instruments (e.g., checks, stocks) to Gateway staff. 68 Section IX Member/Customer Service It is the function of the Customer Service Unit to be the entry to Gateway Community Health (GCH) and to convey an atmosphere that is welcoming, helpful and informative to all individuals that contact the organization with consumer-related questions and issues. All callers will be served with respect, provided clear and concise information within the scope of the position of the Customer Service Representative who will also refer callers to others in or outside the organization as appropriate. In order to assure prompt access to consumer service, GCH has strict telephone service standards. The average speed of answer for customer service lines is 30 seconds or less. The abandonment rate for the customer service line is 5% or less. Members, providers or facilities wishing to initiate medical necessity determination procedures can contact Gateway‘s toll-free Customer Service Unit 7 days per week, 365 days per year. 24-Hour Customer Service Lines 313 - 262 - 5050 800 - 973 - 4283 TDD: 313 - 875 - 4065 The GCH Customer Service Unit will also provide information regarding grievance and appeals, Fair Hearings, local dispute resolution processes, Recipient Rights and claims issues. Customer Service Standards for Providers It is the function of the customer services unit to be the entry to your facility and to convey an atmosphere that is welcoming, helpful and informative. Functions: Welcome and orient persons to services and benefits available. Provide information about how to access mental health and other community services. Provide information about how to access the various rights processes. Help persons with problems regarding benefits. Assist people with and oversee local complaint and grievance processes. Standards: There shall be a designated unit called ―Customer Services‖. 69 There shall be a minimum of one FTE dedicated to customer services. There shall be sufficient staff to meet the needs of the people accessing the facility. There shall be a designated toll-free customer services telephone line and access to a TTY number. The numbers shall be displayed in the provider‘s brochures and public information materials. Telephone calls to the customer service unit shall be answered by a live voice during business hours. Telephone menus/trees are not acceptable. If messages are taken due to high volume, there must be a response to each within one business day. The hours of customer service unit operations and the process for accessing information from customer services outside of normal business must be publicized. All providers will have a customer handbook which shall contain the staterequired topics. Upon request, the customer service unit shall assist consumers with the grievance and appeals, and local dispute resolution processes. Customer Service Monthly Tracking Report is due by the 3rd of each month. Grievance and Appeal logs are due to Gateway by the 10th of each month. The Consumer Handbook that shall be used by Member Services on behalf of Gateway and the Primary Providers that are part of their contracted provider network shall be DWCCMHA‘s Consumer Handbook. The handbook is available by contacting DWCCMHA‘s Customer Service Department at (313) 833-2500. Upon request, Customer Service shall assist beneficiaries with the grievance, appeals, local dispute resolution processes, and coordinates as appropriate with Fair Hearing Officers and the DWCCMHA Office of Recipient Rights. Cultural Competency Gateway staff, contracted providers and subcontractors shall assure sensitivity, demonstrate accommodations and cultural competencies to individuals of diverse ethnic and cultural backgrounds in the provision of services. Culture: is broadly defined as a common heritage or set of beliefs, norms, and values shared by a group of people. There is great diversity within each broad category and individuals may identify with a given racial or ethnic culture to varying degrees. Others may identify with multiple cultures, including those associated with their religion, profession, sexual orientation, region, or disability status. Cultural Competency: is an approach to delivering mental health services grounded in the assumption that services are more effective when they are provided within the most relevant and meaningful cultural, gender-sensitive and age-appropriate context for the people being served. 70 In 2006, the United States Surgeon General defined cultural competence in the most general terms as ―the delivery of services responsive to the cultural concerns of racial and ethnic minority groups, including their languages, histories, traditions, beliefs, and values‖. Most of the time, the term cultural competence refers to sets of guiding principles, developed to increase the ability of mental health providers, agencies or systems to meet the diverse communities, including racial and ethnic minorities. Cultural Diversity: Refers to differences in race, ethnicity, language, nationality or religion among various groups within a community. Ethnic: A large group of people classed according to common racial, national, tribal, religious, linguistic, or cultural origin or background. Standards All contracted providers and their subcontractors shall have mechanisms in place to assure that sensitivity and accommodations are made for individuals with diverse ethnic and cultural backgrounds. Staff shall receive training in cultural competency. All contracted providers and their subcontractors shall have a policy that pertains to cultural competency. The Michigan Department of Community Health (MDCH) and the United States Department of Health and Human Services mandate that all supports and services will be provided in a manner that demonstrates cultural competency. The culturally competent system of care is developed based on utilization of several tools: The assessment The plan Implementation of the plan. Cultural Competency Guiding Principles as set forth below by Gateway are based on the premise that a culturally competent program is one that is sensitive to, and understanding of, cultural differences. Gateway requires that the implementation of an understanding of and sensitivity to cultural differences are reflected in program philosophy. A consumer driven system of care promotes consumer and family as the most important participants in service provision. Natural community support and culturally competent practices are viewed as an integral part of a system of care, which contributes to desired outcomes in a managed care environment. Culture is a predominant force in shaping behaviors, values and institutions; Cultural differences exist and have an impact on service delivery. Diversity is recognized and respected. Unique, culturally defined needs of various consumer populations will be respected. 71 Cultural Competence Standards: All contracted providers and subcontractors shall develop a comprehensive cultural competence plan and integrate that plan into the organizational structure that ensures attention to the following areas of practice: The contracted providers and subcontractors shall have and demonstrate a philosophy that reflect a comprehensive understanding of the dynamics of ethnic and cultural differences and that provides a framework for eliminating bias in service intervention and delivery. It is recommended that the contracted provider‘s and subcontractor‘s mission statement and goals recognize the cultural and ethnic diversity of the consumer populations it services and reflect a commitment to serve those groups sensitively and competently. The contracted provider‘s and subcontractor‘s governing boards shall provide overall guidance, and shall be accountable for the fulfillment of the Contractor‘s mission, operations and the goals for the consumers it serves. It is recommended the contracted provider‘s and subcontractor‘s board of directors and/or advisory committee have representation and input from individuals of different cultures and/or the ethnic groups reflective of the community it serves. The contracted provider‘s and subcontractor‘s board of directors shall have the opportunity to learn about issues of cultural diversity and how those issues effect the organization‘s contracted responsibility to provide high quality, culturally competent services. The contracted providers and subcontractors shall be knowledgeable about federal, state, county and city laws and regulations that relate to culturally diverse populations and address nondiscrimination policies and practices. The contractor shall implement activities to obtain consultation from organizations and/or outside experts that represent cultural and ethnic groups in the community served before finalizing programs and policies that may have cultural impact. The contracted provider shall ensure that its program brochures, annual reports, newsletters, special events, etc., reflect the diversity of the populations it services. Contracted provider documents, including policies and procedure manuals, shall reflect recognition of the cultural diversity of its staff and the consumer population it serves. The contracted provider shall incorporate a community based system of care which focuses on including familiar and valued community resources that are in tune with the consumers cultural beliefs and consistent with their needs. The contracted provider‘s outreach efforts and service delivery system shall reflect responsiveness to the racial, cultural, and ethnic community it serves. The contracted provider shall provide services that are geographically and culturally accessible. The contracted provider shall offer an avenue for the community it serves to express their views, give feedback and exchange and let their needs be articulated and included as an integral part of an on-going assessment of the contracted network and the service delivery process. 72 The contracted provider shall actively advertise positions in culturally diverse print and broad case media and through community information networks and organizations representing culturally diverse groups. The contracted provider shall document that staff are trained, provided continuing education opportunities, and practice culturally congruent interventions. The contracted provider shall have consistent opportunities for feedback and exchange from consumers concerning service delivery. Limited English Proficiency Gateway ensures that no individuals are denied benefits or subjected to discrimination by Gateway or contracted providers on the basis of limited English proficiency. Interpretation: Refers to the spoken word interpreted from one language into another by a third party. Limited English Proficient (LEP): An individual who is unable to speak, read, write or understand the English language at a level that permits him or her to interact effectively with English speaking people. Persons Eligible to be Served or likely to be Directly Affected: Are those people who are in the entity‘s service area, and who either are eligible for the covered entities‘ benefits or services, or otherwise might be directly affected by such an entity‘s conduct. Safe Harbor: Written translations must be provided under the following circumstances: Ensure that translated written material, including vital documents, are provided for each eligible LEP language group that constitutes ten percent (10%) or 3000, whichever is less, of the population of persons eligible to be served, or likely to be directly affected by the programs, services or supports required to be provided by the network and contracted providers. Ensure at minimum that vital documents are translated into the appropriate nonEnglish languages of persons for each LEP language group that constitute five percent or 1,000 whichever is less, of the population of persons eligible to be served, or likely to be directly affected by the programs, services, or supports provided by the Network and contracted providers. Translation of other documents, if needed, can be provided orally. Ensure that written notice is provided in the primary language of the LEP language group of the right to receive competent oral translation of written materials to eligible LEP language groups that constitute less than 100 persons eligible to be served, or likely to be directly affected by the programs, services, or supports provided by Gateway and its contracted providers. Service Area: The geographic areas, from which the Network and service providers draw or can be expected to draw, consumers. Translation: Refers to the written word, indicating materials written in one language and translated into another. 73 Vital Documents: Includes applications or consent forms, letters or notices regarding eligibility or participation criteria, and notices pertaining to reduction, denial or termination of services or benefits, that require a response from beneficiaries, and/or that advise regarding free language assistance. Large documents such as enrollment books may not need to be translated in their entirety. However, vital information contained in large documents must be translated. Gateway and contracted providers shall: Develop policies and procedures that accommodate individuals who have limited proficiency. Follow the Network‘s standards set in the Guidelines for Translations for MultiLanguage Materials or Products. Ensure all services, programs, or activities shall be accessible and usable to individuals with LEP. Provide adequate information to enable individuals with LEP to understand the types of services and benefits available. Conduct a thorough assessment of the language needs of the service area, following the federal safe harbor rules and identifying: The non-English languages that are likely to be encountered in its program and estimate the number of LEP individuals that are likely to be directly served by its program. The language needs of each client and record this information in the client‘s record. The points of contact in the program or activity where language assistance is likely to be needed. The resources that will be needed to provide effective language assistance and the location and availability of these resources. The arrangement that must be made to access these resources in a timely manner. Provide a range of language assistance which may include: Sign language interpreters for individuals with hearing impairments/limitations. Alternative formats such as large print or Braille for individuals with visual impairments/limitations. Oral language interpretation for individuals that are non-English speaking. Hiring bilingual staff trained and competent in interpreting. Testing self-identified bilingual staff for language proficiency. Hiring trained and competent staff interpreters. Contracting with outside interpreter service(s) for training and competent interpretation. Formally arranging for the services of trained and skilled voluntary community interpreter(s). Arranging for the use of a telephone language interpreter service. This may be used as a supplemental system or when a language encountered can not be accommodated by other resources. 74 Ensure the interpreter service is familiar with terminology used in the provision of mental health services. Ensure that vital documents are available in language(s) other than English in accordance with Federal safe harbor guidelines. Ensure access by, at a minimum, providing notices in writing, in the LEP individual‘s primary language, of the right to receive free language assistance in a language other than English, including the right to competent oral translation of written materials free of cost. Notice can be provided by, but not limited to: Use of language identification cards, which allow LEP beneficiaries to identify their language needs. A message on the card must invite the LEP person to identify the language he/she speaks. Identification must be included in the individual‘s record. Posting signs in regularly encountered languages (in accordance with Federal safe harbor guidelines) other than English in waiting rooms, reception areas, and other initial points of entry. These signs must inform applicants and beneficiaries of their right to free language assistance services and invite them to identify themselves as persons needing services. Translation of applications and instructional information and other written materials into appropriate non-English languages by competent translators. Uniform procedures for timely and effective communication between staff and LEP individuals. This includes instructions for English speaking employees to obtain assistance from interpreters or bilingual staff when receiving calls from, or initiating calls to LEP individuals. Inclusion of statements about services available and the right to free language assistance services in applicable non-English languages, in brochures, booklets, outreach, and recruitment information and other materials routinely disseminated to the public. Disseminate Limited English Proficiency policy to staff. Provide training to new employees and periodic training to other staff to ensure staff is: Knowledgeable and aware of LEP policy and procedures. Are trained to work effectively with interpreters. Understand the dynamics of interpretation between consumers and the interpreter Monitor its language assistance program periodically to assess: The current LEP makeup of its service area. The current communication needs of LEP applicants and consumers. Whether existing assistance is meeting the needs of such persons. Whether staff is knowledgeable about policies and methods of implementation. Whether sources of arrangements for assistance are still current and viable. 75 If modifications are needed. 76 Section X Grievance and Appeals Introduction It is the policy of Gateway that all consumers have the right to a fair and efficient process for resolving complaints regarding their services and supports. Purpose: To define appeals related to the actions of denial, reduction, suspension or termination of services and supports; and grievances about any matter other than an action, such as quality of care or relationships. To establish a structured grievance and appeal resolution process for consumers that promotes the resolution of consumer concerns, as well as support and enhance the overall goal of improving the quality of care. Grievance and Appeals Grievance means an expression of dissatisfaction about any matter other than an action. A grievance can be filed when a member of Gateway communicates dissatisfaction with Gateway or the contracted service providers. The Grievance and Appeals Coordinator is responsible for assuring effective coordination of all disputes, grievances and appeals; tracking and trending the data; assisting in the generation of regularly scheduled reports for review by the Executive Director and MQC; and ensuring avoidance of conflict of interest or purpose related to grievances, dispute, and appeals. A grievance can be submitted orally or in writing by the member themselves, or their legal representative. This can be done whenever a member verbalizes dissatisfaction. An informal grievance can be a phone call or a letter to the service provider or to Gateway Customer Service department at: 1-888-711-5465 Grievances may be filed 24 hours a day, 7 days a week Gateway and the contracted providers shall ensure the informal grievance process is initiated at the time a consumer is expressing dissatisfaction with services. This process shall include the following: Ensuring appropriate staff, who are not the subject of the grievance, immediately resolve the consumer‘s concerns. Ensuring professionals with the appropriate clinical expertise are consulted for all grievances which involve clinical issues of medical necessity. Logging of the date, time and resolution of the grievance. Informing the consumer of his/her right to file a formal grievance, if the informal grievance cannot be resolved. 77 A consumer may request assistance with their grievance from the service provider, Gateway or other person of their choice. Persons in AFC facilities can be assisted in completing the grievance form by their Case Manager and/ or their Service Provider or their assigned representative. There are interpreter and TTY/TTD services are available to help the consumer, if needed. Grievance forms must be available to all persons at Gateway service providers. When the service provider or Gateway Community Health receives the grievance, they must contact the complainant within one working day that their grievance was received. A letter titled ‗acknowledgement of grievance‘ must be sent confirming the receipt of the grievance within 5 days of the actual grievance being filed. This letter will come from the agency who received the grievance. The letter will specifically come from Grievance and Appeals Coordinator, or Gateway Customer Service staff. If the issue is moved to another department or supervisor, the information will be referred back to the Grievance and Appeals Coordinator. If the grievance is not resolved immediately the service provider or Gateway will make a decision about the grievance within 30 calendar days from the day the grievance was filed. A notification of resolution letter must be sent upon resolution of the grievance. The notification of the resolution letter will address other options that are available to if the consumer is not satisfied with the resolution. The whole grievance process should not exceed 60 days from the time the grievance was filed. Grievance information is kept separate from the consumer‘s clinical file. Documentation of the grievance from the service providers must be sent to Gateway‘s Grievance and Appeals Coordinator on a monthly basis by the 10th of the following month. The information is then aggregated and sent to Detroit Wayne County Community Mental Health Agency Grievance and Appeals Coordinator by the 15th of every month. 78 Section XI Recipient Rights Introduction Recipient Rights functions are the responsibility of the Detroit-Wayne County Community Mental Health Agency. All providers contracted with Gateway must have their employees trained in recipient rights within 30 days from hire and annually thereafter. Providers are to contact the Detroit- Wayne County Community Mental Health Agency‘s Office of Recipient Rights at (313) 833-2500 to register staff for training. Detroit-Wayne County Community Mental Health Agency Recipient Rights Policies can be obtained by contacting the Agency‘s Office of Recipient Rights at (313) 833-2149 or at www.gchi.org. 79 Section XII Miscellaneous [Remainder of page intentionally left blank] 80 GATEWAY COMMUNITY HEALTH PRELIMINARY DEATH REPORT Instructions: All deaths must be reported to Gateway Community Health Inc. (GCHI) by telephone within one business day of notification at the 24 hour number 1-800-973-4283. Do not fax, e-mail or leave a message. you must speak with someone. GCHI will provide D-WCCMHA, ORR the information and obtain a Death Log Number. Today’s Date: Community Mental Health: Type of Service: Case Manager: Consumer’s Name: Gender: Date of Birth: Male Female Age: Date of Death: Time: Social Security #: MCPN #: Location of Death: _____________________________________ *City: AFC Home: ______________________________________ Specialized or Personal Home: General Yes No City: Cause of Death (Check All That Apply): Diabetes Cancer Heart Disease Unknown at this time Renal Failure Stroke/Seizure Infectious Disease Other: Was Death Expected? Yes No Population: MI Child MI Adult Was Adult/Child Protective Services Notified? By Whom? Yes DD No Was Office of Children and Adult Licensing Notified? By Whom? Yes No Was Law Enforcement Notified? By Whom? Yes No AXIS I: AXIS III: Caller’s Name: Telephone#: Gateway Staff Name:________________________________ Telephone #: * D-WCCMHA- ORR must have the city the consumer died in prior to giving a death log number to Gateway. Gateway Quality Staff complete: D-WCCMHA ORR Staff: DL #: Gateway Community Health Quality Management Department Revised 08/16/2010 81 REPORT OF RECIPIENT DEATH (*MUST BE TYPED) Date of Report: Date of Death: SECTION I: Instructions: (TO BE COMPLETED FOR ALL RECIPIENTS) All deaths must be reported to the Agency's Office of Recipient Rights by telephone within one business day of Provider notification. This form and a copy of the Incident Report, if applicable, shall be mailed to the Agency's Office of Recipient Rights within 10 business days of telephone notification. If information is unavailable at the time the report is submitted, an amended report must be submitted. SEND THE LAST 3 PSYCHIATRIST, THERAPIST, CASE MANAGEMENT PROGRESS NOTES AND INDIVIDUAL PLAN OF SERVICE ALONG WITH THIS REPORT. PLEASE FAX THE REPORT AND DOCUMENTS TO QUALITY COMPLIANCE SPECIALIST AT 313-263-2513 OR 313-263-2453 1. Service Provider: __________________________ 2. Provider No.: ____________________________________ 3. Client Name: ______________________________ 4. D-WCCMHA Case Number: _________________________ 5. Place of Death: [ ] Detroit [ ] Other Wayne County: 6. Social Security Number: _____________________ 7. Sex: _____ 8. Race: _____ 9. Birth Date: ______________ 10. Program(s) in which client was active at time of death: Inpatient ] A.C.T. Outpatient Substance Abuse Residential Partial Day a) Admission Date: __________ Other (specify) b) Population: MI MI Child DD 11. Was the Treatment Plan developed by an Interdisciplinary Team? Yes ] No 12. Was the client hospitalized in a state facility within the past six months? Yes No If yes, name of facility Discharge Date: 13. Date of client's last treatment by Provider: ________________ ________________________________________ 14. When was death discovered by Provider? (date and time): ______________ _____________________________ 15. When did death occur? (date and time): _______________ __________________________________________ 16. Where did death occur? ___________________________________ __________________________________ (Location, including place and city) 17. Was the death expected? or unexpected? 18. Brief explanation of death: (If Incident Report was completed, please attach): (Attach extra sheets if needed.) 82 REPORT OF RECIPIENT DEATH (*MUST BE TYPED) SECTION II: 1. Current DSM Diagnosis (include all 5 Axis): A. AXIS I: AXIS II: AXIS III: AXIS IV (Specify Stressor(s), State Severity: AXIS V GAF: B. Alcohol/Substance Use: Write Diagnosis on AXIS I or AXIS III. If NONE, CIRCLE ―NONE‖ HERE 2. CAUSE OF DEATH: 3. RELEVANT PAST MEDICAL HISTORY INCLUDING MOST RECENT MED/SURG HOSPITALIZATION: 4. SUMMARY OF PSYCHIATRIC TREATMENT INCLUDING MOST RECENT PSYCHIATRIC HOSPITALIZATION, INCLUDING DATES: 83 5. SURGICAL PROCEDURES DURING PAST YEAR: 6. RECENT CHANGES IN MEDICAL STATUS: 7. SUMMARY OF MEDICAL CONDITION AND TREATMENT PRECEDING DEATH (IF TREATED IN A MEDICAL/SURGICAL FACILITY. INCLUDE DATE OF ADMISSION AND DISCHARGE): 8. MEDICATIONS (DOSE AND TIME ADMINISTERED): (A) LAST 24 HOURS (B) LAST 30 DAYS 9. CIRCUMSTANCES SURROUNDING DEATH, INCLUDING TREATMENT (Attach extra sheets if needed) Physician and/or Preparer‘s Signature and Telephone Number (If psychiatrist is on staff, physician‘s signature must be included) 84 REPORT OF RECIPIENT DEATH (*MUST BE TYPED) This page is being requested by a Gateway Community Health physician and Quality staff for the purposes of more in depth analysis of possible trends related to consumer deaths. SECTION III: Any Medical Condition: Yes No Did consumer have a Primary Care Physician? Yes No Name of PCP: Dates of contact with PCP in last 90 days? ______________________________________________ Was the consumer compliant with psychotropic and medical medications in the past 30 days? Weight: lbs. Was the consumer a Smoker? /km Yes Yes No Height: __________ Ft. __________ Inches No How many packs a day? ______________ (approximate) Did the consumer abuse Alcohol? Yes No Did the consumer abuse drugs other than alcohol? How often did the consumer drink? Yes No How long? Name of Substance(s) used? Did consumer ever participate in Outpatient Substance Abuse Treatment including AA/NA? Yes No Which Program? SEND THE LAST 3 PSYCHIATRIST, THERAPIST, CASE MANAGEMENT PROGRESS NOTES AND INDIVIDUAL PLAN OF SERVICE ALONG WITH THIS REPORT. PLEASE FAX THE REPORT AND DOCUMENTS TO QUALITY COMPLIANCE SPECIALIST AT 313-263-2513 OR 313-263-2453. 85 GATEWAY COMMUNITY HEALTH REPORTABLE SENTINEL EVENT FORM Sentinel Events must be reported by telephone or e-mail to Gateway‘s Quality Unit within one (1) business day. If you complete and send the Sentinel Vent Form within one (1) business day, you do not need to make the phone call or send the e-mail. To report by telephone, please call L.C. Smith at (313) 263-2452. If you do an e-mail notification, please e-mail [email protected]. This form must be typed, completed and submitted to Gateway‘s Quality Unit within three (3) business days of the notification. Fax this form to Gateway Community Health, Quality Manager – Special Programs, at (313) 263-2453. Initial Report Updated Report 1. Date of Report: 2. Date of Occurrence: 3. Name of MCPN/Service Provider: Gateway Community Health/ 4. Name of Person Receiving Services: 5. Is the person registered in CMH-Link? Yes No – Member ID#: 6. Date of Birth: 7. Social Security#: 8. Setting: Habilitation Support Waivers Services Targeted Case Management Supports Coordination Own Home w/Community Living Supports Children‘s Waiver Substance Abuse Residential Treatment Program ACT Program Home Based Program Wraparound Program Specialized Residential and/or Child Caring Institution (fill out lines below) Name of AFC or CCI: MDHS License#: 86 9. Type of Incident: Injuries that require ER visits, medi-center, urgent care clinics/centers and/or admission(s) to hospital(s) as a result of an incident resulting from abuse, neglect or accidents or loss of limb or function Arrest of recipient Conviction of recipient Death of recipient that did not occur as a result of the natural outcome to a chronic condition or old age Medication error(s) (wrong medication, wrong dosage, double dosage, or missed dosage resulting in risk of harm or adverse reaction(s) or the risk thereof) Physical illness requiring admission(s) to a hospital(s) (do not include planned surgeries, whether inpatient or outpatient OR admissions directly related to the natural course of the person‘s chronic illness or underlying condition) Serious challenging behaviors not already addressed in the IPOS (include property damage> $100.00, attempts at self-inflicted harm or harm to others, or unauthorized leaves of absence) 10. Detail Summary of Review: 11. Detail Summary o Findings/Decision: 12. Detail Summary of Action(s) Taken: 13. Detail Summary of Follow-up: Print Name of Staff Completing Report: Signature: Phone#: Fax#: Cellular Phone#: Date: E-Mail: Pager#: 87 Glossary Priority of Application. The definitions of terms contained in this glossary are general definitions that take precedence over any competing or ―common‖ meaning in every instance in which such term is capitalized in any document or correspondence, with the exception that: (a) Any such general definitions shall be subordinate to and replaced by any conflicting definitions contained in Gateway‘s, MCPN or other contracts, extensions, or expansions, the Michigan Mental Health Code, Medicaid regulation, MDCH or DWCCMHA written policy or procedure, to the extent that such definitions have been incorporated or are otherwise legally applicable to the topic addressed in any document or correspondence; and (b) Both the general and incorporated definitions referred to above shall be subordinate to and replaced by any specific definitions included in a particular text in any document or correspondence, and such case specific definitions shall take precedence over any competing general or incorporated definitions of such terms in those instances. To assist in understanding the context in which and sources from which these definitions were derived, when these definitions remain identical to those in the source materials, this is indicated by referring to that source in parenthesis. Acute Crisis Intervention Home - Short-term services provided in a protected residential setting under the supervision of a Qualified Mental Health Professional for developmentally disabled adults who also have mental illness and are experiencing an acute exacerbation of the illness. (DWCCMHA/MCPN Contract) Administrative Efficiencies - The ability to produce a desired effect in with a minimum of effort, expense, or waste as applied to management functions of the organizations. (DWCCMHA/MCPN Contract) Administrative Fair Hearing or Medicaid Fair Hearing - An impartial review process maintained by the MDCH to ensure that Medicaid beneficiaries or their legal representatives involved in a community Mental Health Services Program have the opportunity to appeal decisions of DWCCMHA or its representatives which result in the denial, suspension, reduction or termination of Medicaid covered services. A Medicaid beneficiary or any person entitled to services may request a hearing within 90 days of notice of the denial, suspension, reduction or termination of Medicaid-covered benefits. (DWCCMHA/MCPN Contract) 88 Administrative Request for Reconsideration - Any written dissatisfaction or disagreement by a provider following an adverse decision of a Provider Dispute and a desire to appeal the dispute to the next level, if permitted by Gateway and/or Consumer, as applicable. (Operations) Adult Foster Care Home - (Adults Ages 18 and Older) Adult Foster Care is a general licensed living arrangement that may accommodate one or more residents. Residents in this setting have mild to no maladaptive behaviors and may or may not require assistance with community living and self care tasks. Specialized services can be arranged and provided in this setting if indicated. (DWCCMHA/MCPN Contract) Adverse Action - A denial, suspension, reduction or termination of mental health services, except as ordered by a physician's determination of absence of medical necessity. (DWCCMHA/MCPN Contract) AFP - MDCH's required Application for Participation. (DWCCMHA/MCPN Contract) Appeal – In relation to recipient rights, a process established by MDCH to provide a mechanism for prompt reporting, review, investigation, and resolution of apparent or suspected violations of the rights guaranteed by the Michigan Mental Health Code. (MMHC) Assertive Community Treatment (ACT) - Assertive Community Treatment (ACT) is a comprehensive and integrated set of medical and psychosocial services provided on a one-to-one basis primarily in the client's residence or other community locations (non- office setting) by a mobile multidisciplinary mental health treatment team. The team provides an array of essential treatment and psychosocial interventions for individuals who would otherwise require more intensive and restrictive services. The team provides additional services essential to maintaining an individual's ability to function in community settings. This would include assistance with addressing basic needs, such as food, housing, and medical care and supports to allow individuals to function in social, educational, and vocational settings. (DWCCMHA/MCPN Contract) Authorization - A decision rendered by a Qualified Professional who has been delegated the authority by Gateway, to approve a request for covered clinical services as meeting the criteria of Medical Necessity. (DWCCMHA/MCPN Contract) Authorized Representative - An authorized representative is any individual designated by a member or appointed by a court to represent his or her interest, including but not limited to, a practitioner, spouse, parent, family member, or legal representative (such as a guardian, executor or attorney). (MMHC and Operational P&P) Authorized Services - Services deemed medically necessary and eligible for reimbursement based on the contract between the provider and the Network. 89 All funded services are authorized by Gateway, but only a specific subset of available services require prior authorization. (Operational P&P) Beneficiary - Persons who are Medicaid-eligible. (DWCCMHA/MCPN Contract) Best Value - A process used in competitive negotiated contracting to select the most advantageous offer by evaluating and comparing factors in addition to cost or price. (DWCCMHA/MCPN Contract) Capitation - Generally: a fixed amount paid per month for covered services to be provided to each member of a referenced class of eligible recipients for whom such services are medically necessary. (Operational) As applied to DWCCMHA/MCPN contracts: A fixed amount paid per month per Person to the MCPN for Covered Services. (DWCCMHA/MCPN Contract) Categorical Funds - Funds that are designated for a specific service, program and/or special population. (DWCCMHA/MCPN Contract) CCH -Contracted Community Hospital that provides acute inpatient and/or partial hospitalization services by contract with DWCCMHA. (DWCCMHA/MCPN Contract) Certification - Certification is a process of evaluating/screening clients to determine and approve appropriate and clinically necessary services for inpatient psychiatric admission, and other prior authorized services, which includes certifying appropriateness of all inpatient hospital and physician services related to the admitting mental health diagnosis, including laboratory and x-ray services, medications, etc. Any inpatient psychiatric admission not certified by the CMH is not a benefit of the Medicaid program. (DWCCMHA/MCPN Contract) CFAC -Consumer Family Advocate Council (DWCCMHA/MCPN Contract) CAFAS - Child and Adolescent Functional Assessment Scale (DWCCMHA/MCPN Contract) Child Mental Health Professional - One of the following: a) A person who is trained and has one year of experience in the examination, evaluation, and treatment of minors and their families and who is one of the following: i. A physician ii. A psychologist iii. A certified social worker or social worker; iv. A registered nurse; OR b) A person with at least a bachelor's degree in a mental health-related field from an accredited school who is trained, and has three (3) years of supervised experience, in the examination, evaluation, and treatment of minors and their families. OR c) A person with at least a master's degree in a mental health-related field from an accredited school who is trained and has one year of experience, in the examination, evaluation, and treatment of minors and their families. (DWCCMHA/MCPN Contract) 90 Children's Diagnostic and Treatment Service - A program operated by or under contract with a Community Mental Health Services Program, which provides examination, evaluation and referrals for minors, including emergency referrals, that provides or facilitates treatment for minors, and that has been certified by MDCH. (DWCCMHA/MCPN Contract) Clean Claim -A clean claim is one that can be processed in accordance with the claims processing requirements specified in the Provider Manual without obtaining additional information from the provider of the service or a third party. It does not include a claim from a provider who is under investigation for fraud or abuse, or a claim under review for medical necessity. (Operations; DWCCMHA/MCPN Contract) Clinical Appeal - A request by a member, member-designated representative, or provider to review an adverse medical necessity determination made in response to a request for services. The Clinical Appeal process is described in the Provider Manual. (Operations) CM - Case Manager/qualified primary case manager (DWCCMHA/MCPN Contract) CMH - Community Mental Health (DWCCMHA/MCPN Contract) CMHP - Child Mental Health Professional (DWCCMHA/MCPN Contract) CMS - Centers for Medicare and Medicaid Services (DWCCMHA/MCPN Contract) Community Mental Health Services Program (CMHSP) - A program operated under Chapter 2 of the Michigan Mental Health Code – Act 258 of 1974 as amended. Complaint - An oral or written statement made to the Office of Recipient Rights ("ORR") alleging violation of a Mental Health Code protected right. (DWCCMHA/MCPN Contract) Consumers - Recipients of services designated by two types: Primary and Secondary. Primary refers to the recipient of services. Secondary refers to family members of the primary recipient. (DWCCMHA/MCPN Contract) Co-Occurring Disorders - When used in the context of Persons, this term refers to cooccurring psychiatric and/or substance use disorders. (DWCCMHA/MCPN Contract) Contracted Provider - An individual or entity participating in the Provider Network pursuant to a contract with Gateway to provide Covered Services. (DWCCMHA/MCPN Contract) 91 Corrective Action Plan (CAP) - Refers to the written plan of action that a provider has been formally required by Gateway to develop/take to address/answer deficiencies formally identified as constituting material breaches of its contractual obligations. There are two applications of the term. It can refer either to (a) the Plan required to be developed and submitted by the provider for approval by Gateway or (b) a specific Plan directed by Gateway. A Corrective Action Plan will generally: 1. Address how corrective action will be accomplished for those enrollees and entities affected by the deficient performance/practice; 2. Address how the provider will identify other enrollees having the potential to be affected by the deficient performance/practice; 3. Address what measures will be put into place or systemic changes made to ensure that the deficient performance/practice will not recur; 4. Indicate how the provider plans (or, if a directed POC, how the provider will be required) to monitor its performance/practice to make sure that solutions are sustained. 5. Include dates when corrective action(s) will be completed. Covered Services under MCPN - Contract Specialty supports and services as described in Appendix B of DWCCMHA/MCPN contract, as amended. (DWCCMHA/MCPN Contract) Credentialing - The review process used by Gateway to determine if a practitioner, group, group or facility that has applied to participate in a provider network meets criteria for inclusion. This review process is described in the Gateway Manual (Operations) Crisis Residential (CR) - Short term intensive treatment services provided in a protected residential setting as an alternative to inpatient hospital admission when clinically appropriate for people experiencing acute psychiatric crisis diagnosed by a Qualified Mental Health Professional, as meeting criteria for an acute inpatient hospital admission. The mentally ill adult must have symptoms that can be stabilized in an alternative community setting. (DWCCMHA/MCPN Contract) Cultural Competency - The capacity of the network to address behavioral health needs of members in a manner that is congruent with their cultural, religious, ethnic, and linguistic backgrounds. A set of academic and interpersonal skills that allow individuals to increase their understanding and appreciation of cultural differences and similarities within, among, and between cultural groups. This requires a willingness, and ability to draw on community-based values, traditions, and customs, and to work with knowledgeable individuals of, and from, the community in developing targeted interventions, communications and other supports to address the unique needs of specific population groups. 92 An acceptance and respect for difference, a continuing self-assessment regarding culture, a regard for and attention to the dynamics of difference, engagement in ongoing development of cultural knowledge, and resources and flexibility within service models to work toward better meeting the needs of the minority populations. The cultural competency of an organization is demonstrated by its policies and practices. Customers In this Agreement, a potential recipient of Covered Services, which includes all people located in the defined service area. (Operations; DWCCMHA/MCPN Contract) Denial of Authorization - An adverse decision made by a psychiatrist regarding a request to authorize services, after appropriate evaluation of relevant clinical information. (DWCCMHA/MCPN Contract) Department of Human Services – DHS formerly FIA Dependent Living Setting - An Adult Foster Care facility b) A nursing home c) A Home for the Aged d) Child Caring Institution (DWCCMHA/MCPN Contract) Detroit-Wayne County Community Mental Health Agency (DWCCMHA) - The community mental health services program established and administered pursuant to provision of the State Mental Health Code, for the purpose of providing a comprehensive array of mental health services appropriate to the condition of individuals who are Wayne County residents, regardless of ability to pay. (DWCCMHA/MCPN Contract) Duplicate Claim - A claim with the same member number, date of service, provider and service/procedure as a previously paid claim. (Operations) Early On Program - Early On services are delivered to children ages 0 to 3 identified either with a developmental delay or developmental disability. Early On services provide infant mental heath services to families with children between the ages of 0 to 3, who have been identified as "at risk" for an out of home placement due to parenting problems such as substance abuse, mental illness, physical abuse, or neglect. Additional services include clinic-based and home-based services for children between the ages of 3 to 5. These services shall be designed and delivered in such a manner as a) to provide an aftercare option for children who were discharged from Early On services or infant mental health services due to reaching the age limitation; b) to provide a transitional option for children who were discharged from Early On services or infant mental health services due to achieving their treatment goals; c) to provide services to families with children ages 3 to 5, who have been identified as "at risk" for an out-of-home placement due to parenting problems such as substance abuse, mental illness, physical abuse or neglect. (DWCCMHA/MCPN Contract) 93 Effective Freedom - The realization of social citizenship and full community membership. Citizens are able to build upon basic freedoms – to effectively unlock the potential of liberty – by making choices, pursing personal goals, engaging in productive activity, establishing a wide range of associations and relationships, participating in community events, and living in real homes. (DWCCMHA/MCPN Contract) Emergency Situation - A situation in which an individual is experiencing a serious mental illness or a developmental disability, or a child is experiencing a serious emotional disturbance, and one of the following apply: 1. The individual can reasonably be expected within the near future to physically injure himself, herself, or another individual, either intentionally or unintentionally. 2. The individual is unable to provide himself or herself food, clothing, or shelter, or to attend to basic physical activities such as eating, toileting, bathing, grooming, dressing, or ambulating, and this inability may lead in the near future to harm to the individual or to another individual. 3. The individual's judgment is so impaired that he or she is unable to understand the need for treatment and, in the opinion of the mental health professional, his or her continued behavior as a result of the mental illness, developmental disability, or emotional disturbance can reasonably be expected in the near future to result in physical harm to the individual or to another individual. (DWCCMHA/MCPN Contract) Encounter -A face to face meeting between a covered person and health care provider where services are delivered. (Operations) A document submitted in a claim format specified by DWCCMHA that documents the services and costs of services provided to a consumer. (DWCCMHA/MCPN Contract) Enhanced Health Services - Those services beyond the responsibility of the Person's health plan, that are provided for rehabilitative purposes to improve the Person's overall health and ability to care for health-related needs. This includes nursing services, dietary/ nutrition services, maintenance of health and hygiene, teaching selfadministration of medication, care of minor injuries or first aid, and teaching the Person to seek assistance in case of emergencies. Services must be provided according to the professional's scope of practice and under appropriate supervision. Enhanced health services must be carefully coordinated with the Person's health care plan. (DWCCMHA/MCPN Contract) Early and Periodic Screening, Diagnosis and Treatment (EPSDT) - Federal regulations require state Medicaid programs to offer early and periodic screening, diagnosis, and treatment (EPSDT) to eligible Medicaid beneficiaries under 21 years of age. The intent is to find and treat problems early so they do not become more serious and costly. (DWCCMHA/MCPN Contract) 94 Executive Performance Oversight Committee (EPOC) - An internal committee tasked with reviewing the performance of contract providers against their contractual performance standards and recommending appropriate provider sanctions for noncompliance with contractual, policy, or procedural issues and issues related to member complaints/grievances, Recipient Rights violations, quality of care, or complaints of violations of state and federal laws and regulations. (Operations) Explanation of Benefit (EOB) - A statement mailed to providers explaining why a claim was or was not paid. (Operations) Facility - A residential building for the care or treatment of individuals with serious mental illness, serious emotional disturbance, or developmental disability that is either a state facility or a licensed facility. (DWCCMHA/MCPN Contract) Fee for Service (FFS) – A form of reimbursement for health care services in which a provider is paid a specific amount for a service rendered. (Operational) FIA - Family Independence Agency (DWCCMHA/MCPN Contract) Grievance - A process for expressing dissatisfaction with an actual or supposed circumstance regarded by the complainant as just cause for protest about mental health treatment/services/supports, managed and/or delivered by DWCCMHA network, made in accordance with the Mental Health Code, with available assistance of an ORR representative, as needed. (DWCCMHA/MCPN Contract) HCFA- Health Care Financing Administration, now known as the Centers for Medicare and Medicaid Services. (DWCCMHA/MCPN Contract) Health Insurance Portability and Accountability Act of 1996 (HIPAA) - Public Law 104- 191, 1996 to improve the Medicare program under the Title XVIII of the Social Security Act, the Medicaid program under the Title XIX of the Social Security Act, and the efficiency and effectiveness of the health care system, by encouraging the development of a health information system through the establishment of standards and requirements for the electronic transmission of certain health information. The Act provides for improved portability of health benefits and enables better defense against abuse and fraud, reduces administrative costs by standardizing format of specific healthcare information to facilitate electronic claims directly addresses confidentiality and security of patient information – electronic and paper-based, and mandates "best effort" compliance. HIPAA mandates, among others, that the following requirements must be implemented: 1- Data integrity, confidentiality, and availability guards. 2Access control (user-based, role-based, and availability). 3- Audit controls (user-based, role-based). 4- Data authentication (automatic log-off, unique user ID, password, PIN, biometrics, token, or telephone callback). 5- Unauthorized access guards 6Communications/network controls (access controls, encryption, integrity controls or message authentication) 95 7- Network controls (alarm, audit trail, entity authentication, event reporting, userbased, role-based, or context based access) (DWCCMHA/MCPN Contract) Individual - For the purpose of the DWCCMHA/MCPN contract, sub-contracts, and provider contracts: a person with mental illness, developmental disabilities, or substance use disorders (or a combination of disabilities), including persons who are Medicaid- eligible, as well as other mental health and substance abuse specialty services recipients who may be indigent, are self-pay, or have private insurance coverage. (DWCCMHA/MCPN Contract) Initial Assessment -Term used in substance abuse service. It is a process that collects sufficient information to determine a level of care based on at least the six dimensions of the American Society of Addiction Medicine Patient Placement Criteria. This initial assessment process also gathers enough information to determine an initial diagnostic impression using the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition. (DWCCMHA/MCPN Contract) Intensive Crisis Stabilization -The process of stabilizing an individual in acute crisis to avert a psychiatric admission or to shorten the length of an inpatient stay. (DWCCMHA/MCPN Contract) Intensive Crisis Stabilization Services - Structured treatment and support activities provided by a mental health crisis team, under psychiatric supervision and designed to provide a short-term treatment alternative to inpatient psychiatric services. Services should be used to avert a psychiatric admission or to shorten the length of an inpatient stay. (DWCCMHA/MCPN Contract) IPOS -Individual Plan of Service (DWCCMHA/MCPN Contract) ITT- Interdisciplinary Treatment Team (DWCCMHA/MCPN Contract) I-Team - Agency Inter-Divisional Team (DWCCMHA/MCPN Contract) Jail Diversion – Is a collaborative, integrated program utilizing a community's resources to divert a person with serious mental illness, serious emotional disturbance or developmental disability from possible jail incarceration when appropriate. (DWCCMHA/MCPN Contract) Length of Stay (LOS) - The number of days that a member remains in a given level of care. (Operations) Level of Care (LOC) - The intensity of professional care required to achieve the treatment objectives for a specific episode of care. (Operations) 96 Level of Care (LOC) DWCCMHA/MCPN Contract Protocols - Severity of Illness/Intensity of Service Protocols provided by the Michigan Department of Community Health ("MDCH") and DWCCMHA, each as amended from time to time, as part of a utilization management system, which are intended to monitor the appropriateness of mental health care. Severity of Illness refers to the nature and severity of the signs, symptoms, functional impairments, and risk potential related to the person's complaint. Intensity of Service pertains to the setting of care, to the types and frequency of needed services and supports, and to the degree of restriction necessary to safely and effectively treat the individual. (DWCCMHA/MCPN Contract) Limited English Proficiency (LEP) - Persons, who cannot speak, write, read or understand the English language in a manner that permits them to interact effectively with health care providers and social services agencies. (DWCCMHA/MCPN Contract) Linguistically Appropriate Services - Provided in the language best understood by the consumer through bi-lingual staff and the use of qualified interpreters, including American Sign Language, to individuals with limited-English proficiency. These services are a core element of cultural competency and reflect an understanding, acceptance, and respect for the cultural values, beliefs, and practices of the community of individuals with limited- English proficiency. Linguistically appropriate services must be available at the point of entry into the system and throughout the course of treatment, and must be available at no cost to the consumer. (DWCCMHA/MCPN Contract) MACMHB - Michigan Association (DWCCMHA/MCPN Contract) of Community Mental Health Boards Medicaid Abuse - This term, generally used in the context of Medicaid Fraud and Abuse, refers to provider practices that are inconsistent with sound fiscal, business or medical practices, and result in an unnecessary cost to the Medicaid program, or in reimbursement for services that are not medically necessary or that fail to meet professionally recognized standards for health care. It also includes recipient practices that result in unnecessary cost to the Medicaid program (42 CFR § 455.2). Medicaid Verification - The process described in the Provider Manual to verify that claims have been filed in accordance with all applicable federal and state legal requirements and any applicable local standards. MCO - Managed Care Organization (DWCCMHA/MCPN Contract) MCPN - Manager of a comprehensive provider network contracting with DWCCMHA. For each Manager of Comprehensive Provider Network Contract, MCPN shall include all parties to such agreement other than DWCCMHA. (DWCCMHA/MCPN Contract) 97 MCPN Manual -The manual developed and implemented by DWCCMHA, and adopted by the MCPN, that includes policies, procedures, forms, instructional materials, and other information as referenced and incorporated by individual provider contracts with Gateway and used to support and supervise/manage the Provider Network, in accordance with Agency guidelines. (DWCCMHA/MCPN Contract) MDCH - Michigan Department of Community Health, State of Michigan. The State division is responsible for funding a comprehensive array of specialty mental health services for persons with serious mental illness and children with severe emotional disturbances and specialty services for persons with developmental disabilities and to priority populations as defined in the Michigan Mental Health Code. (DWCCMHA/MCPN Contract) Management Services Council - A committee (however denoted) established by DWCCMHA in accordance with the terms of the DWCCMHA/MCPN contract, comprised of key Agency executives, to manage the Agreement between DWCCMHA and the MCPN. (DWCCMHA/MCPN Contract) Medicaid Eligible – An individual who has been determined to be eligible for Medicaid by the State of Michigan. (DWCCMHA/MCPN Contract) Medical Necessity -The clinical appropriateness of a course of treatment/ specific services suitable to the patient's need, based on the client's psychiatric status using approved clinical criteria and professional judgment. As defined by the MDCH, medical necessity refers to mental health and/or substance abuse services that are: 1. Necessary for screening and assessing the presence of a mental illness or substance (use) disorder, as defined by standard diagnostic nomenclature (i.e., DSM-IV or its successor); 2. Required to identify and evaluate a mental illness or substance (use) disorder that is inferred or suspected; 3. Intended to treat, ameliorate, diminish, or stabilize the symptoms of mental illness (or substance use) disorder and to prevent or delay relapse; 4. Expected to prevent, arrest or delay the development or progression of a mental illness (or substance use disorder) to prevent or delay relapse; 5. Designed to provide rehabilitation for the recipient to attain or maintain an optimal level of functioning according to his or her potential, (including functioning in important life domains, such as daily activities, social relationships, independent living, and employment pursuits); 6. Delivered consistent with national professional standards of practice, including standards of practice in community psychiatry, psychiatric rehabilitation and in substance abuse services, and/or empirical professional experience; 7. Provided in the least restrictive setting. (DWCCMHA/MCPN Contract) Mental Health Professional - A person who is trained and experienced in the areas of mental illness or mental retardation and who is any one of the following: 1) A physician who is licensed to practice medicine or osteopathic medicine in Michigan and who has substantial experience with mentally ill or developmentally disabled recipients for one year immediately preceding his/her involvement with a recipient under these rules; 98 2) A psychologist 3) A certified social worker 4) A registered nurse 5) A professional person, other than those defined in these rules, who is designated by the director in written policies and procedures. This mental health professional shall have a degree in his or her profession and shall be recognized by his or her respective professional association as being trained and experienced in the field of mental health. (DWCCMHA/MCPN Contract) Michigan Department of Consumer and Industry Services (MDCIS) - The State agency responsible for licensure and certification of Adult Foster Care (AFC) homes. (Michigan Code) MIChild - A health insurance program offered through the State of Michigan for the uninsured children of Michigan's working families; eligibility requirements are established by the State. (DWCCMHA/MCPN Contract) MRS - Michigan Rehabilitation Services, now known as the Michigan Department of Career Development—Rehabilitation Services. (DWCCMHA/MCPN Contract) Multicultural Services -Specialized mental health services for multicultural populations such as African-Americans, Hispanics, Native Americans, Asian and Pacific Islanders, and Arab/Chaldean-Americans. (DWCCMHA/MCPN Contract) Non-Categorical Funds - Funds that are not designated for any specific programs, services or special populations. (DWCCMHA/MCPN Contract) OBRA - Omnibus Budget Reconciliation Act of 1987; 1990 is federally mandated legislation establishing programs and a funding program that was developed in 1989. Office of Recipient Rights (ORR) - Division of DWCCMHA established in accordance with the Michigan Mental Health Code to ensure a uniformly high standard of protection of the rights of the recipients throughout the State. (DWCCMHA/MCPN Contract) Out-of-Area Services -These are services provided to Wayne County consumers by out-of-area service providers who are not part of the Detroit-Wayne County Community Mental Health Network. Typically, special "purchase of service" arrangements are negotiated with the out-of-area provider or responsible CMHSP for that area, to provide the service(s). While DWCCMHA's MCPNs are expected to have a countywide network, there may be occasions when the MCPN may need to secure such service provisions as out-of-area on a temporary time targeted basis. There are times when such services may have to be obtained out of state, however, these out-of-area and out of state services will need to be authorized, paid and monitored by the MCPN. Transportation should be provided when necessary. (DWCCMHA/MCPN Contract) 99 Out-of-Network Services - Services provided by a mental health professional who does not participate in the Provider Network. (DWCCMHA/MCPN Contract) Outreach - Efforts to extend services to those Persons who are under-served or hard-to reach that often require seeking individuals in places where they are most likely to be found, including hospital emergency rooms, homeless shelters, women's shelters, senior centers, nursing homes, primary care clinics and similar locations. (DWCCMHA/MCPN Contract) Participating (PAR) Provider - A participating (PAR) provider has an agreement with GATEWAY and/or its affiliated companies to provide mental health to Gateway members. Unless otherwise specified, in this policy the term PAR provider refers not only to institutions, but also to PAR individual professionals. (Operational P&P) PASARR - readmission screening and annual resident review are requirements of the OBRA program. Preadmission screening must be completed prior to placement of a person with mental illness in nursing homes. Annual review determines the need for continued nursing home care and whether specialized services for the mental illness are indicated. (DWCCMHA/MCPN Contract) Person - For the purpose of the DWCCMHA/MCPN contract, sub-contracts, and provider contracts, Person is an Individual with Serious Mental Illness/Severe Emotional Disturbance who qualifies for Covered Services and selects MCPN for such services. (DWCCMHA/MCPN Contract) Person-Centered Planning or PCP - Process for planning and supporting an individual receiving service that builds upon the individual's capacity to engage in activities that promote community life and that honor the individual's preferences, choices, and abilities through the Public Mental Health System. The person-centered planning process involves families, friends, and professionals as the individual desires or requires. (DWCCMHA/MCPN Contract) Policy Manuals of the Medical Assistance Program - The MDCH periodically issues notices or proposed policy for the Medicaid program. Once a policy is final, MDCH issues policy bulletins that explain the new policy and give its effective date. These documents represent official Medicaid policy and are included in the policy manual of the Medical Assistance Program. (DWCCMHA/MCPN Contract) Practice Guideline - MDCH-developed guidelines for PIHPs for specific service, support or systems models of practice that are derived from empirical research and sound theoretical construction and as applied to the implementation of public policy. MDCH guidelines issued prior to June 2000 were called "Best Practice Guidelines." All guidelines are now referred to as Practice Guidelines. (DWCCMHA/MCPN Contract) 100 Prepaid Inpatient Health Plan (PIHP) - Organization that manages specialty health care services under the Michigan Medicaid Waiver Program for Specialty Services. (DWCCMHA/MCPN Contract) Priority Population - Persons who are at risk for developing serious emotional disturbance (SED) serious mental illness (SMI) or have developmental disabilities (DD). For purposes of managing specialized treatment and support services, SMI and SED are defined by diagnosis, degree of disability and/or duration of illness. (DWCCMHA/MCPN Contract) Protected Health Information (PHI) – Is individually identifiable health information that is maintained or transmitted by a ―HIPAA covered‖ entity in any form or medium. Information is considered to be ―individually identifiable‖ if (i) it identifies the individual or (ii) there is a reasonable basis to believe that the information can be used to identify the individual. In addition to clinical information, individually identifiable health information may include demographic characteristics, such as name, address, age, or payment and billing details such as procedure code and diagnosis. (HIPAA) Provider - A legal entity or independent practitioner that provides covered services and supports as specified by Gateway. (DWCCMHA/MCPN Contract) Provider Applicant - Provider who is requesting to become a contracted provider of the Gateway Community Health. (Operational P&P) Provider Applicant Appeal Process - The internal process of reviewing the provider application information that originally was denied upon recommendation by the Network Management Workgroup. (Operational P&P) Provider Application Process - Process a potential provider must follow when requesting to become a contracted provider for the Gateway Community Health. (Operational P&P) Provider Dispute - A written communication by a provider, primarily indicating disagreement or expressing dissatisfaction with an administrative decision (Operations) Provider Network -The network of providers contracted by MCPN and all Contracted Providers to deliver Covered Services to Recipients. (DWCCMHA/MCPN Contract) Provider Service & Network Management Departments -The departments at Gateway that are responsible for recommending, processing, and executing provider contracting and Provider Service requirements. 101 Provider Sponsored Specialty Networks (PSSN) - Vertically integrated, comprehensive service entities that are organized and operated by affiliated groups of service providers that offer relatively complete "systems of care" for beneficiaries with particular service needs. DWCCMHA uses the term MCPN as an alternative to PSSN. (DWCCMHA/MCPN Contract) Psychiatric Partial Hospitalization Program - A nonresidential treatment program that provides psychiatric, psychological, social, occupational, nursing, music therapy, and therapeutic recreational services under the supervision of a physician to adults diagnosed as having serious mental illness or minors diagnosed as having serious emotional disturbance who do not require 24-hour continuous mental health care, and that is affiliated with a psychiatric hospital or psychiatric unit to which consumers may be transferred if they need inpatient psychiatric care. (DWCCMHA/MCPN Contract) QMRP -A Qualified Mental Retardation Professional is a person with specialized training or experience in treating or working with persons with mental retardation and is one of the following: 1. Educator with a degree in education from an accredited program. 2. Occupational therapist: a. A graduate of an occupational therapy curriculum accredited jointly by the Council on Medical Education of the American Medical Association and the American Occupational Therapy Association; or b. Is eligible for certification by the American Occupational Therapy Association under its requirements; or c. Has two years of appropriate experience as an occupational therapist and has achieved a satisfactory grade on an approved proficiency examination, except that such determination of proficiency does not apply to persons initially licensed by the State or seeking initial qualifications as an occupational therapist after December 31, 1977. 3. Physical therapist: a. Licensed as a physical therapist by the State b. has graduated from a physical therapy curriculum approved by the American Physical Therapy Association or by the Council on Medical Education and Hospitals of the American Medical Association c. Has two years of appropriate experience as a physical therapist, after December 31, 1977. 4. Physician of medicine or osteopathy, licensed by the State. 5. Psychologist with a master's degree from an accredited program. 6. Registered nurse: currently licensed by the State of Michigan 7. Social worker with a bachelor's degree in: a. social work from an accredited program; or b. in a field other than social work and at least three years of social work experience under the supervision of a qualified social worker. c. 102 8. Speech pathologist or audiologist (qualified consultant): a. Licensed by the State and is eligible for a certificate of clinical competence in speech pathology or audiology granted by the American Speech and Hearing Association; or b. Meets the educational requirements for certification, and is in the process of accumulating the supervised experience required for certification. 9. Therapeutic recreation specialist: a. Graduate of an accredited program; and b. Licensed or registered by the State. 10. Rehabilitation counselor: certified by the Committee on Rehabilitation Counselor for Certification. (DWCCMHA/MCPN Contract) QPIC - Quality Performance and Improvement Council (DWCCMHA/MCPN Contract) Qualified Health Plan (QHP) - A health plan (e.g., HMO, PPO, POS) in which a Medicaid recipient may belong. The QHP pays for mental health services when a consumer is Medicaid eligible, but does not meet the DD, SMI or SED requirements. (DWCCMHA/MCPN Contract) Qualified Mental Health Professional - A qualified mental health professional is licensed, certified or registered by the State of Michigan or a national organization to provide mental health services and clinical and administrative supervision. (DWCCMHA/MCPN Contract) Reasonable Access - (geographic access standard) Services are available within 30 miles or 30 minutes in urban areas or within 60 miles or 60 minutes in rural areas (DWCCMHA/MCPN Contract) Recovery - The over arching message of recovery is that hope and restoration of a meaningful life are possible, despite serious mental illness. Instead of focusing primarily on symptom relief, as the medical model dictates, recovery casts a much wider spotlight on restoration of self-esteem and identity and on attaining meaningful roles in society. (DWCCMHA/MCPN Contract) Respite - Respite services are those services that are provided in the individual's/family's home or outside the home to temporarily relieve the unpaid primary caregiver. Respite services provide short-term care to a child with a mental illness/emotional disturbance to provide a brief period of rest or relief for the family from day to day care giving for a dependent family member. Respite programs can use a variety of methods to achieve the outcome of relief from care giving including family friends, trained respite workers, foster homes, residential treatment facilities, respite centers, camps and recreational facilities. Respite services are not intended to substitute for the services of paid support/training staff, crisis stabilization and crisis residential treatment or out-of-home placement. (DWCCMHA/MCPN Contract) 103 Root Cause Action Plan - The ―Root Cause Action Plan‖ is the product of the Root Cause Analysis that identifies the strategies for implementation to reduce the probability of Sentinel Events occurring in the future. The Action Plan addresses responsibility for implementation, oversight, pilot testing as appropriate, timelines, and strategies for achieving improvements to reduce risk, including measurement of the effectiveness of the actions. (DWCCMHA/MCPN Contract) Root Cause Analysis - A structured and process-focused framework for identifying and evaluating the basis or causal factors involved in producing a sentinel event. The analysis should include the development of an action plan that identifies the steps that will be implemented to lessen the risk that similar events would happen to have happen. (DWCCMHA/MCPN Contract) Root Cause Analysis Administrative/Managed Care Component - The non peerreviewed portion (generally, but not limited to, the non-clinical portion) of the Root Cause Analysis shall be conducted by Gateway ‗s MQC Department upon referral by the Incident Review Committee (IRC), and by the legal entity or entities contracted with or subcontracted under Gateway Community Health to provide community mental health services/supports to affected Recipients. Screening - Means the CMH has been notified of the Person and has been provided enough information to make a determination of the most appropriate services. The screening may be provided on-site, face-to-face, by CMH personnel, or, over the telephone. (DWCCMHA/MCPN Contract) Second Opinion/Reconsideration - An additional clinical evaluation and decision provided in response to a request from an applicant, authorized representative or referring mental health professional, in dispute of an adverse decision when: 1) A specific request for inpatient hospitalization has been denied by a psychiatrist reviewer, and 2) Following a face-to-face assessment by a qualified professional, determination is made that no mental health service is needed and the applicant is referred outside DWCCMHA network to other human service resources. (DWCCMHA/MCPN Contract) Secondary Treatment - Secondary treatment services are those which are provided by professionals other than the treating clinician (for instance, a psychiatrist who performs a consultation or a social worker who conducts a daily living skills group at a partial hospitalization program), and individuals from relevant medical delivery systems, including Primary Care Physicians (PCPs). (Operational P&P) Sentinel Event - Unexpected occurrence involving death or serious physical or psychological injury, or the risk thereof. Serious injury specifically includes loss of limb or function. The phrase "or the risk thereof" includes any process variation for which a recurrence would carry a significant chance of a serious adverse outcome. (DWCCMHA/MCPN Contract) 104 Serious Emotional Disturbance - A diagnosable mental, behavioral, or emotional disorder affecting a minor that exists or has existed during the past year for a period of time sufficient to meet diagnostic criteria specified in the most recent diagnostic and statistical manual of mental disorders published by the American Psychiatric Association and approved by the MDCH, and that has resulted in functional impairment that substantially interferes with or limits the minor's role or functioning in family, school or community services. The following disorders are included only if they occur in conjunction with another diagnosable serious emotional disturbance: 1. A substance use disorder; 2. A developmental disorder; 3. A "V" code in the diagnostic and statistical manual of mental disorders. (DWCCMHA/MCPN Contract) Serious Mental Illness - Diagnosable mental, behavioral, or emotional disorder affecting an adult that exists or has existed within the past year for a period of time sufficient to meet diagnostic criteria specified in the most recent diagnostic and statistical manual of mental disorders, published by the American Psychiatric Association and approved by the MDCH, in functional impairment that substantially interferes with or limits one or more major life activities. Serious mental illness includes dementia with delusions, dementia with depressed mood and dementia occurs in conjunction with another diagnosable serious mental illness. The following disorders are included only if they occur in conjunction with another diagnosable mental illness: 1) A substance abuse disorder 2) A developmental disorder 3) A "V" code in the diagnostic and statistical manual of mental disorders. (DWCCMHA/MCPN Contract) Service Authorization - A process designed to help assure that planned services meet medical necessity criteria, and are appropriate to the conditions, needs and desires of the individual. Authorization can occur before services are delivered, at some point during service delivery or can occur after services have been delivered based on a retrospective review. (DWCCMHA/MCPN Contract) Stakeholder - An individual or entity that has an interest, investment or involvement in the operations of a Prepaid Inpatient Health Plan or affiliate. Stakeholders can include individuals and their families, advocacy organizations, and other members of the community that are affected by the Prepaid Inpatient Health Plan and the supports and services it offers. (DWCCMHA/MCPN Contract) State Hospital Services - An inpatient program operated by the Michigan Department of Community Health for the treatment of individuals with serious mental illness or serious emotional disturbance. (DWCCMHA/MCPN Contract) Sub-capitation -A fixed amount paid per month per enrolled consumer, which shares risk with affiliates or established risk-sharing entities. (DWCCMHA/MCPN Contract) 105 Substance Abuse - A maladaptive pattern of substance use manifested by recurrent and significant adverse consequences related to the repeated use of substances. If the primary diagnosis is mental illness, then the CMH will be the lead agency for the determination of necessary services, with coordination with the Substance Abuse Coordinating Agency. If the primary diagnosis is substance abuse, then the Substance Abuse Coordinating Agency will be the lead agency for the determination of necessary services, with coordination with the CMH. (DWCCMHA/MCPN Contract) Substance Use Disorders - Substance use disorders include Substance Dependence and Substance Abuse, according to selected specific diagnosis criteria given in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition. Specific DSM IV diagnoses are found in Attachment 7.0.1.1 of the department's contract with CMHSPs. Technical Advisory MDCH – developed document with recommended parameters (DWCCMHA/MCPN Contract) Technical Requirement - MDCH/PIHP contractual requirements providing parameters for PIHPs regarding administrative practice related to specific administrative functions, and derived from public policy and legal requirements. (DWCCMHA/MCPN Contract) TPL Third Party Liability – refers to any other health insurance plan or carrier (e.g., individual, group, employer-related, self-insured or self-funded plan or commercial carrier, automobile insurance and worker's compensation) or program (e.g., Medicare) that has liability for all or part of a recipient's covered benefit. (DWCCMHA/MCPN Contract) UM Designee - Person or entity designated by DWCCMHA to oversee the UM Plan. (DWCCMHA/MCPN Contract) UM Plan - A utilization management plan for the Provider Network, which includes comprehensive, written utilization management policies and procedures that evaluate the appropriateness and effectiveness of Covered Services provided by the MCPN and the Contracted Providers, and is approved by DWCCMHA. (DWCCMHA/MCPN Contract) Utilization Management (UM) - The process of evaluating the necessity, appropriateness and efficiency of health care services against established guidelines and criteria and the evaluation of the necessity, appropriateness, and efficiency of the use of health care services, procedures, and facilities. (Operations). Using established criteria to recommend or evaluate services provided in terms of medical necessity, effective use of resources and cost-effectiveness. (DWCCMHA/MCPN Contract) Utilization Review (UR) - Analysis of the patterns of service authorization decisions and service usage in order to determine the means for increasing value of services provided (minimize cost and maximize effectiveness/ appropriateness). 106 Urgent Situation - A situation in which an individual is determined to be at risk of experiencing an emergency situation in the near future if he or she does not receive care, treatment, or support services. (DWCCMHA/MCPN Contract) Wraparound Services - Wraparound services are an individually designed set of services provided to minors with serious emotional disturbance or serious mental illness and their families that includes treatment services and personal support services or any other supports necessary to maintain the child in the family home. Wraparound services are to be developed through an interagency collaborative approach and a minor's parent or guardian and a minor age 14 or older are to collaborate in planning the services. (DWCCMHA/MCPN Contract) Your Choice - The term originally designated by DWCCMHA for its program for the delivery of pre-paid behavioral health services through its MCPN contracts. (DWCCMHA/MCPN Contract) 107 Section XIII Addendums PIHP/CMHSP Encounter Reporting HCPCS and Revenue Codes -Link http://www.michigan.gov/documents/mdch/MHCodeChart10-01-07 210734 7.doc Medicaid Application – Linkhttp://www.michigan.gov/dhs/0,1607,7-124-5453 5530--,00.html Medicaid Provider Manual – Link http://www.mdch.state.mi.us/dchmedicaid/manuals/MedicaidProviderManual.pdf Michigan Department of Community Health Approved Diagnosis Codes – Link http://www.michigan.gov/documents/mdch/MHCodeChart_7-01-09_285851_7.doc Person Centered Planning Best Practice Guideline Attachment 4.5.1.1 to the contract between CMH and DCH I. Summary/Background The Michigan Mental Health Code establishes the right for all individuals to have their Individual Plan of Service developed through a person-centered planning process regardless of age, disability or residential setting. The Individual Plan of Service may include a treatment plan, support plan or both. In the past, Medicaid or other regulatory standards have governed the process of treatment or support plan development. These standards drove the planning process through requirements on the types of assessments to be completed and the professionals to be involved. Personcentered planning departs from this approach in that the individual will direct the planning process with a focus on what he/she wants and needs. Professionally trained staff will play a role in the planning and delivery of treatment and may play a role in the planning and delivery of supports. However, the development of the treatment or support plan, including the identification of possible services and professionals, is based upon the expressed needs and desires of the individual. The Michigan Department of Community Health (MDCH) has advocated and supported a family approach to service delivery for children and their families. This approach recognizes the importance of the family system and the fact that supports and services will impact the entire system. Therefore, in the case of minors, the child/family will be the focus of service planning and family members are integral to the planning process and its success. The wants and needs of the child/family will be considered in the planning and evaluation of supports, services and/or treatment. 108 Managed care strategies will play an important role in planning for and delivery of supports, services and/or treatment. Person-centered planning fits well with these strategies. Both strategies attempt to ensure that individuals are provided with the most appropriate services necessary to achieve the desired outcomes. When an individual expresses a choice or preference for a support, service and/or treatment for which an appropriate alternative of lesser cost exists, a process for dispute resolution and appeal may be indicated. This document provides guidelines for addressing dispute concerns. The literature describes specific methods for person-centered planning, including but not limited to, individual service design, Personal Futures Planning, McGill Action Planning Systems, Essential Lifestyle Planning, Planning Alternative Tomorrows With Hope, etc. This practice guideline does not support one model over another. It does, however, define the values, principals and essential elements of the person-centered planning process and it provides illustrations to its application. II. Values and Principles Underlying Person-Centered Planning Person-centered planning is a highly individualized process designed to respond to the expressed needs/desires of the individual. A. Each individual has strengths, and the ability to express preferences and to make choices. B. The individual's choices and preferences shall always be considered if not always granted. C. Professionally trained staff will play a role in the planning and delivery of treatment and may play a role in the planning and delivery of supports. Their involvement occurs if the individual has expressed or demonstrated a need that could be met by professional intervention. D. Treatment and supports identified through the process shall be provided in environments that promote maximum independence, community connections and quality of life. E. A person's cultural background shall be recognized and valued in the decisionmaking process. III. Practice Guidelines A. Essential Elements 1. The individual shall be given ongoing opportunities to express his/her needs or desired outcomes. This would include: a. Making accommodations for communication to maximize ability for expression; 109 b. The identification of outcomes of value for the individual; and c. Expectations of the service delivery system. 2. Potential support and/or treatment options to meet the expressed needs of the individual are identified and discussed with the individual. 3. The individual shall be given ongoing opportunities to express his/her preferences and to make choices. This would include: a. Choices and options shall be clearly explained. b. To the extent possible, the individual shall be given the opportunity for experiencing the options available prior to making a choice/decision. This is particularly critical for those persons who have limited life experiences in the community with respect to housing, work and other domains. c. Individuals who have court-appointed legal guardians shall participate in person-centered planning to the maximum extent possible and shall have authority not otherwise specifically delegated to the guardian. d. Parents and significant family members of minors are integral to and shall participate in the planning process unless: i. The minor is fourteen years of age or older and has requested services without the knowledge or consent of parents, guardian or person in loco parentis within the restrictions stated in the Mental Health Code; ii. The minor is emancipated; or iii. The inclusion of the parent(s) or significant family members would constitute a substantial risk of physical or emotional harm to the recipient or substantial disruption of the planning process as stated in the Mental Health Code. Justification of the exclusion of parents shall be documented in the clinical record. 4. Individuals are provided with opportunities to provide feedback on how they feel about the service, support and/or treatment they are receiving and their progress toward attaining valued outcomes. B. Illustrations of Individual Needs Person-centered planning processes begin when the individual makes a request to the Responsible Mental Health Agency (RMHA). The first step is to find out from the individual the reason for his/her request for assistance. During this process, individual needs and valued outcomes are identified rather than requests for a specific type of service. Since person-centered planning is an individualized process, how the RMHA proceeds will depend upon what the individual requests. This guideline includes a chart of elements/strategies that can be used by the person representing the RMHA depending upon what the individual wants and needs. Three possible situations are: 110 1. The individual expresses a need which would be considered urgent or emergent. When an individual is in an urgent/emergent situation, the goal is to get the individual's crisis situation stabilized. Following stabilization, the individual and RMHA will explore further needs for assistance and if required, proceed to a more in-depth planning process as outlined below. It is in this type of situation where an individual's opportunity to make choices may be limited. 2. The individual expresses a need or makes a request for a support, service and/or treatment in a single life domain and/or of a short duration. A life domain could be any of the following: a. Daily activities; b. Social relationships; c. Finances; d. Work; e. School; f. Legal and safety; g. Health; h. Family relationships; etc. 3. The individual expresses multiple needs which involve multiple life domains for support(s), service(s) or treatment of an extended duration. The following chart represents the elements/strategies that can be used depending on the kinds of needs expressed by the individual. IV. Assurances and Indicators of Person-Centered Planning Implementation It is the responsibility of the RMHA to assure that the Individual Plan of Service is developed utilizing a person-centered planning process. Below are examples of systemic and individual level indicators which would demonstrate that personcentered planning has occurred. The methods of gathering information or evidence may vary and include the review of administrative documents, clinical policy and guidelines, case record review and interviews/focus groups with individuals and their families. A. Systemic indicators would include, but not be limited to: 1. The RMHA has a policy or practice guideline which delineates how personcentered planning will be implemented; 2. Evidence that the RMHA informs individuals of their right to person- centered planning and associated appeal mechanisms, investigates complaints in this area, and documents outcomes; 3. Evidence that the RMHA's quality improvement system actively seeks feedback from individuals receiving services, support and/or treatment regarding their satisfaction providing opportunities to express needs and preferences and the ability to make choices; and 111 4. The RMHA's staff development plan includes efforts to ensure that staff involved in managing, planning and delivering support and/or treatment services are trained in the philosophy and methods of person-centered planning. B. Individual indicators could include but not be limited to: 1. Evidence the individual was provided with information of his/her right to personcentered planning; 2. Evidence that the individual chose whether or not other persons should be involved and those identified were involved in the planning process and in the implementation of the Individual Plan of Service; 3. Evidence that the individual chose the places and times to meet, convenient to the individual and to the people he/she wanted present; 4. Evidence that the individual had choice in the selection of treatment or support services and staff; 5. Evidence that the individual's preferences and choices were considered, or a description of the dispute/appeal process and the resulting outcome; and 6. Evidence that the progress made toward the valued outcomes identified by the individual was reviewed and discussed for the purpose of modifying the strategies and techniques employed to achieve these outcomes. V. Dispute Resolution/Appeal Mechanisms 1. If in the judgment of the person representing the RMHA, an individual requests inpatient treatment, or a specific mental health support or service for which appropriate alternatives for the individual exist that are of equal or greater effectiveness and equal or lower cost, to the RMHA should: a. Identify and discuss the underlying reasons for the request/preference; b. Identify and discuss alternatives with the individual; and c. Negotiate toward a mutually acceptable support, service and/or treatment. In the event that a mutually acceptable alternative cannot be reached, the person representing the RMHA should: 112 a. Document the individual's preference, the support, service and/or treatment the RMHA is offering, and the reason for not accepting that preference; b. Inform the individual of their right to appeal the decision as permitted in the Grievance and Appeal Technical Requirement attachment to the MDCH/CMHSP Managed Specialty Supports and Services Contract. This would include: i. His/her right to contact the recipient rights office for consultation, mediation or intervention in response to their request for a specific mental health support or service; ii. His/her right to request a second opinion as referenced in the Mental Health Code, if requesting inpatient treatment; and iii. His/her right to a Fair Hearing, if a recipient of Medicaid coverage. 2. If in the judgment of the RMHA, an individual's choice or preference for the inclusion or exclusion of a planning participant, meeting location or specific provider poses an issue of health or safety or exceeds reasonable expectations of resource consumption, the RMHA should discuss and identify the individual's underlying reason for that specific choice or preference and negotiate toward a mutually acceptable alternative that meets the outcomes intended. 3. If an individual is not satisfied with his/her Individual Plan of Service, the Michigan Mental Health Code allows the individual to make a request for review to the designated individual in charge of implementing the plan. The review shall be completed within 30 days and shall be carried out in a manner approved by the appropriate governing body. In addition, the individual has access to the appeal processes as defined in the Grievance and Appeal Technical Requirement of the MDCH/CMHSP Managed Specialty Supports and Services Contract. 4. If the individual believes that the opportunity for person-centered planning is not provided as specified in the manner above, it is the responsibility of the RMHA to inform the individual of his/her right to consult with the recipient rights office. 5. When there is a disagreement between an individual and the legal guardian or responsible parent, the RMHA staff should attempt to mediate between the two parties in order to provide an outcome which is acceptable to both parties. VI. Definitions Case Manager/Supports Coordinator: The staff person who works with the individual to gain access to and coordinate the services, supports and/or treatment which the individual wants or needs. 113 Emancipated Minor: The termination of the rights of the parents to the custody, control, services and earnings of a minor which occurs by operation of law or pursuant to a petition filed by a minor with the probate court. Emergency Situation: A situation when the individual can reasonably be expected in the near future to physically injure himself, herself, or another person; is unable to attend to food, clothing, shelter or basic physical activities that may lead to future harm or the individual's judgment is impaired leading to the inability to understand the need for treatment resulting in physical harm to self or others. Family Member: A parent, stepparent, spouse, sibling, child, or grandparent of a primary consumer, or an individual upon whom a primary consumer is dependent for at least 50 percent of his or her financial support. Guardian: A person appointed by the court to exercise specific powers over an individual who is a minor, legally incapacitated or developmentally disabled. Individual Plan of Service: A written Individualized Plan of Service directed by the individual as required by the Mental Health Code. This may be referred to as a treatment plan or a support plan. Minor: An individual under the age of 18 years. Person-Centered Planning: A process for planning and supporting the individual receiving services that build upon the individual's capacity to engage in activities that promote community life and honor the individual's preferences, choices, and abilities. The person-centered planning process involves families, friends, and professionals as the individual desires or requires. Responsible Mental Health Agency (RMHA): A Community Mental Health Services Program responsible for arranging and/or coordinating the provision of services for the individual. Urgent Situation: A situation in which an individual is determined to be at risk of experiencing an emergency situation in the near future if he or she does not receive care, treatment or support services. VII. Legal References: Mental Health Code Act, 258 MI. §§ 409-1-7 (1974 & Supp. 1996). Mental Health Code Act, 258 MI. §§ 700-g (1974 & Supp. 1996). Mental Health Code Act, 258 MI. §§ 707-1-5 (1974 & Supp. 1996). Mental Health Code Act, 258 MI. §§ 712-1-3 (1974 & Supp. 1996). 114 Consumerism Best Practice Guideline I. Summary This guideline sets policy and standards for consumer inclusion in the service delivery design and delivery process for all public mental health services. This guideline ensures the goals of a consumer-driven system which gives consumers choices and decision-making roles. It is based on the active participation of primary consumers, family members and advocates in gathering consumer responses to meet these goals. This participation by consumers, family members and advocates is the basis of a provider‘s evaluation. Evaluation also includes how this information guides improvements. II. Application A. Psychiatric hospitals operated by the Michigan Department of Community Health (MDCH). B. Centers for persons with developmental disabilities and community agencies operated by the MDCH. C. Children‘s psychiatric hospitals operated by the MDCH. D. Special facilities operated by the MDCH. E. Community Mental Health Services Programs (CMHSPs) under contract with MDCH. F. All providers of mental health services who receive public funds, either directly or by contract, grant, third party payers, including managed care organizations or other reimbursements. III. Policy This policy supports services that advocate for and promote the needs, interests, and well-being of primary consumers. It is essential that consumers become partners in creating and evaluating these programs and services. Involvement in treatment planning is also essential. Services need to be consumer-driven and may also be consumer-run. This policy supports the broadest range of options and choices for consumers in services. It also supports consumer-run programs which empower consumers in decision-making of their own services. 115 All consumers need opportunities and choices to reach their fullest potential and live independently. They also have the rights to be included and involved in all aspects of society. Accommodations shall be made available and tailored to the needs of consumers as specified by consumers for their full and active participation as required by this guideline. IV. Definitions Informed Choice: means that an individual receives information and understands his or her options. Primary Consumer: means an individual who receives services from the Michigan Department of Community Health or a Community Mental Health Services Program. It also means a person who has received the equivalent mental health services from the private sector. Consumerism: means active promotion of the interests, service needs, and rights of mental health consumers. Consumer-Driven: means any program or service focused and directed by participation from consumers. Consumer-Run: refers to any program or service operated and controlled exclusively by consumers. Family Member: means a parent, stepparent, spouse, sibling, child, or grandparent of a primary consumer. It is also any individual upon whom a primary consumer depends for 50 percent or more of his or her financial support. Minor: means an individual under the age of 18 years. Family Centered Services: means services for families with minors who emphasize family needs and desires with goals and outcomes defined. Services are based on families‘ strengths and competencies with active participation in decision-making roles. Person-Centered Planning: means the process for planning and supporting the individual receiving services. It builds upon the individual‘s capacity to engage in activities that promote community life. It honors the individual‘s preferences, choices, and abilities. Person-First Language: refers to a person first before any description of disability. 116 Recovery: means the process of personal change in developing a life of purpose, hope, and contribution. The emphasis is on abilities and potentials. Recovery includes positive expectations for all consumers. Learning self-responsibility is a major element to recovery. V. Standards A. All services shall be designed to include ways to accomplish each of these standards: 1. ―Person-First Language‖ shall be utilized in all publications, formal communications, and daily discussions. 2. Provide informed choice through information about available options. 3. Respond to an individual‘s ethnic and cultural diversities. This includes the availability of staff and services that reflect the ethnic and cultural makeup of the service area. Interpreters needed in communicating with non-English and limited English-speaking persons shall be provided. 4. Promote the efforts and achievements of consumers through special recognition of consumers. 5. Through customer satisfaction surveys and other appropriate consumer related methods, gather ideas and responses from consumers concerning their experiences with services. 6. Involve consumers and family members in evaluating the quality and effectiveness of service. Administrative mechanisms used to establish service must also be evaluated. The evaluation is based upon what is important to consumers, as reported in customer satisfaction surveys. 7. Advance the employment of consumers within the mental health system and in the community at all levels of positions, including mental health service provision roles. B. Services, programs, and contracts concerning persons with mental illness and related disorders shall actively strive to accomplish these goals: 1. Provide information to reduce the stigma of mental illness that exists within communities, service agencies, and among consumers. 2. Create environments for all consumers in which the process of "recovery" can occur. This is shown by an expressed awareness of recovery by consumers and staff. 3. Provide basic information about mental illness, recovery, and wellness to consumers and the public. C. Services, programs, and contracts concerning persons with developmental disabilities shall be based upon these elements: 1. Provide personal preferences and meaningful choices with consumers in control over the choice of services and supports. 117 2. Through educational strategies: promote inclusion, both personal and in the community; strive to relieve disabling circumstances; actively work to prevent occurrence of increased disability; and promote individuals in exercising their abilities to their highest potentials. 3. Provide roles for consumers to make decisions in policies, programs, and services that affect their lives including person-centered planning processes. D. Services, programs, and contracts concerning minors and their families shall be based upon these elements: 1. Services shall be delivered in a family-centered approach, implementing comprehensive services that address the needs of the minor and his/her family. 2. Services shall be individualized and respectful of the minor and family‘s choice of services and supports. 3. Roles for families to make decisions in policies, programs and services that affect their lives and their minor‘s life. E. Consumer-run programs shall receive the same consideration as all other providers of mental health services. This includes these considerations: 1. 2. 3. 4. 5. Clear contract performance standards. Fiscal resources to meet performance expectations. A contract liaison person to address the concerns of either party. Inclusion in provider coordination meetings and planning processes. Access to information and supports to ensure sound business decisions. F. Current and former consumers, family members, and advocates must be invited to participate in implementing this guideline. Provider organizations must develop collaborative approaches for ensuring continued participation. Organizations‘ compliance with this guideline shall be locally evaluated. Foremost, this must involve consumers, family members, and advocates. Providers, professionals, and administrators must be also included. The CMHSP [Community Mental Health Service Provider] shall provide technical assistance. Evaluation methods shall provide constructive feedback about improving the use of this guideline. This guideline requires that it be part of the organizations‘ Continuous Quality Improvement. VI. References and Legal Authority Act 258, Section 116(e), Public Acts of 1974 as amended, being MCL 330.1116, 1704, 1708. 118 Self-Determination Policy & Practice Guideline Michigan Department of Community Health Mental Health and Substance Abuse Services July 18, 2003 Introduction Self-determination incorporates a set of concepts and values that emphasize participation and the achievement of personal control for individuals served through the public mental health system. These concepts and values stem from a core belief that people who require support through the public mental health system must have freedom not only to define the life they seek, but to be supported to direct the assistance they require in pursuit of that life. Persons who rely on the public mental health system for necessary supports and services must have access to meaningful options from which to make choices, and be supported to control the course of their lives. Arrangements that support self-determination must be sponsored by the public mental health system, assuring methods for the person to exert direct control over how, by whom, and to what ends they are served and supported. Person-centered planning (PCP) is a central element of self-determination. PCP is the crucial medium for expressing and transmitting personal needs, wishes, goals and aspirations. As the PCP process unfolds, the appropriate mix of paid/non-paid services and supports to assist the individual in realizing/achieving these personally- defined goals and aspirations are identified. The principles of self-determination recognize the rights of people supported by the mental health system to have a life with freedom, and to access and direct needed supports that assist in the pursuit of their life, with responsible citizenship. The methods applicable to self-determination provide a route for the person to engage in activities that accompany a meaningful life. Activities that promote deep community connections, the opportunity for real work, ways to contribute to one‘s community, and participation in personally-valued experiences must be among the purposes of supports the person may need. These supports function best when they build upon natural community experiences and opportunities. The person determines and manages needed supports in close association with chosen friends, family, neighbors, and co-workers as a part of an ordinary community life. Person-centered planning and self-determination underscore a commitment in Michigan to move away from traditional service approaches for consumers of the public mental health system. 119 In Michigan, the flexibility provided through the Medicaid 1915(b) Specialty Services waiver, together with the Mental Health Code requirements of PCP have reoriented organizations to respond in new and more meaningful ways. Recognition has increased among providers and professionals that many consumers may not need, want, or benefit from a clinical regimen, especially when imposed without clear choice. Many provider agencies are learning ways to better support the consumer to choose, participate in, and accomplish a life with personal meaning. This has meant, for example, reconstitution of segregated programs into non-segregated intervention options that connect better with community life. However, the move away from predefined programmatic approaches and professionally managed models has many barriers. Conflicts of interest abound among many who manage the current system. Agencies and providers have obligations and underlying values that affirm the principles of choice and control. Yet, they also have long-standing investments in existing programs and services, including their investments in capital and personnel resources. Even when options are expanded, the choices currently available seldom dissolve the isolation of people with disabilities, reduce the segregation, nor necessarily promote participation in community life and the realization of full citizenship rights. The Department of Community Health is supportive of the desire of people who use the services of the public mental health system to have a full and meaningful role in controlling and directing their specialty mental health services and supports arrangements. At the same time, the Department knows that the system change requirements, as outlined in this policy and practice guideline, are not simple in their application. The Department is committed to continuing dialogue with stakeholders and to the provision of support, direction and technical assistance so the system may make successful progress to resolve technical difficulties and apparent barriers, to achieve real, measurable progress in the implementation of this policy. This policy is intended to clarify the essential aspects of arrangements that promote opportunity for self-determination, and define required elements of these arrangements. Purpose I. To provide policy direction that defines and guides the practice of selfdetermination within the public mental health system in order to assure that arrangements which support self-determination are made available as a means for achieving consumer-designed plans of specialty mental health services and supports. Core Elements I. Consumers are to be provided with information about the principles of selfdetermination and the possibilities, models and arrangements involved. Consumers shall have access to the tools and mechanisms supportive of self-determination, upon request. 120 II. Self-determination arrangements shall commence when the CMHSP and the consumer reach an agreement on a plan of specialty mental health services and supports, the amount of mental health and other public resources to be authorized to accomplish the plan, and the arrangements through which authorized public mental health resources will be controlled, managed, and accounted for. III. Within the obligations that accompany the use of funds provided to them, CMHSPs shall ensure that their services planning and delivery processes are designed to encourage and support consumers to decide and control their own lives. The CMHSP shall offer and support easily-accessed methods for consumers to control and direct an individual budget. This includes providing them with methods to authorize and direct the delivery of specialty mental health services and supports from qualified providers selected by the consumer. III. Consumers of services of the public mental health system shall direct the use of resources in order to choose meaningful specialty mental health services and supports in accordance with their plan as developed through a person-centered planning process. IV. Fiscal responsibility and the wise use of public funds shall guide the consumer and the CMHSP in reaching an agreement on the allotment and use of funds comprising an individual budget. V. Accountability for the use of public funds must be a shared responsibility of the CMHSP and the consumer, consistent with the fiduciary obligations of the CMHSP. VI. Realization of self-determination principles requires arrangements that are partnerships between the CMHSP and the consumer. They require the active commitment of the CMHSP to provide a range of options for consumer choice and control of personalized Provider Servicehips within an overall environment of person-centered supports. VII. In the context of this partnership, CMHSPs must actively assist consumers with prudently selecting qualified providers and otherwise support the consumer with successfully using resources allotted in an individual budget. VIII. Issues of health, safety and well-being are central to assuring successful accomplishment of a consumer‘s plan of specialty mental health services and supports. These issues must be addressed and resolved using the person-centered planning process, balancing consumer preferences and opportunities for self direction with CMHSP obligations under federal and state law and applicable Medicaid Waiver regulations. Resolutions should be guided by the consumer‘s preferences and needs, implemented in ways that maintain the greatest opportunity for consumer control and direction. 121 IX. Self-determination requires recognition that there may be strong inherent conflicts of interest between the consumer‘s choices and current methods of planning, managing and delivering specialty mental health services and supports. X. The CMHSP must watch for and seek to minimize or eliminate either potential or actual conflicts of interest between itself and its provider systems, and the processes and outcomes sought by the consumer. IX. Arrangements that support self-determination, allowing a consumer to choose, control and direct providers of specialty mental health services and supports are not themselves covered services under the Specialty Mental Health Plan. They are administrative mechanisms. Self-determination arrangements must be developed and operated within the requirements of the Prepaid Health Plan contract between the CMHSP and the State of Michigan and in accordance with federal and state law. Involvement in self-determination does not change a consumer‘s eligibility for particular specialty mental health services and supports. Policy III. Opportunity to pursue and obtain a plan incorporating arrangements that support self-determination shall be established in each Community Mental Health Services Program, for adults with developmental disabilities and adults with mental illness. Each CMHSP shall develop and make available a set of methods that provide opportunities for the consumer to control and direct their specialty mental health services and supports arrangements. IV. A. Participation in self-determination shall be a voluntary option on the part of the consumer. B. Consumers involved in self-determination shall have the authority to select, control and direct their own specialty mental health services and supports arrangements by responsibly controlling the resources allotted in an individual budget, towards accomplishing the goals and objectives in their plan of specialty mental health services and supports. C. A CMHSP shall assure that full and complete information about self-determination and the manner in which it may be accessed and applied is provided to each consumer. This shall include specific examples of alternative ways that a consumer may use to control and direct an individual budget, and the obligations associated with doing this properly and successfully. D. Self-determination shall not serve as a method for a CMHSP to reduce its obligations to the consumer, or to avoid the provision of needed specialty mental health services and supports. 122 E. A CMHSP shall actively support and facilitate a consumer‘s application of the principles of self-determination in the accomplishment of his/her plan of services. II. Arrangements that support self-determination shall be made available to each consumer for whom an agreement on a plan of authorized specialty mental health services and supports, along with an acceptable individual budget, has been reached. A consumer initiates this process by requesting the opportunity to participate in self-determination. For the purposes of self-determination, reaching agreement on the plan must include delineation of the arrangements that will, or may, be applied by the consumer to select, control and direct the provision of those services and supports. A. Development of an individual budget shall be done in conjunction with development of a plan of specialty mental health services and supports, using a personcentered planning process. B. As part of the planning process leading to an agreement about self-determination, the arrangements that will, or may, be applied by the consumer to pursue selfdetermination shall be delineated and agreed to by the consumer and the CMHSP. C. The individual budget represents the expected or estimated costs of a concrete approach to accomplishing the consumer‘s plan. D. The amount of the individual budget shall be formally agreed to by both the consumer and the CMHSP before it may be authorized for use by the consumer. A copy of the individual budget must be provided to the consumer prior to the onset of a selfdetermination arrangement. E. Proper use of an individual budget is of mutual concern to the CMHSP and the consumer. 1. Mental Health funds included in an individual budget are the assets and responsibility of the CMHSP, and must be used consistent with statutory and regulatory requirements. Authority over their direction is delegated to the consumer, for the purpose of achieving the goals and outcomes contained in the consumer‘s plan. The limitations associated with this delegation shall be delineated to the consumer as part of the process of developing the plan and authorizing the individual budget. 2. An agreement shall be made in writing between the CMHSP and the consumer delineating the responsibility and the authority of both parties in the application of the individual budget, including how communication will occur about its use. The agreement shall include a copy of the consumer‘s plan and individual budget. The directions and assistance necessary for the consumer to properly apply the individual budget shall be provided to the consumer in writing when the agreement is finalized. 123 3. An individual budget, once authorized, shall be filed with the consumer‘s approved plan of service. An individual budget shall be in effect for a specified period of time. Since the budget is based upon the consumer‘s plan of specialty mental health services and supports, when the plan needs to change, the budget may need to be reconsidered as well. In accordance with the Person-Centered Planning Practice Guidelines, the plan may be reopened and reconsidered whenever the consumer, or the agency, feels it needs to be reconsidered. 4. The individual budget is authorized by the CMHSP for the purpose of providing a defined amount of resources that may be directed by the consumer to pursue accomplishing their plan of specialty mental health services and supports. An individual budget shall be flexible in its use. a. The consumer may adjust the specific application of CMHSP-authorized funds within the budget between budgetary line items and/or categories in order to adjust his/her specialty mental health services and supports arrangements as he or she deems necessary to accomplish his/her plan. b. Unless the planned adjustment deviates from the goals and objectives in the consumer‘s plan, the consumer does not need to seek permission from the CMHSP nor be required to provide advance notification of an intended adjustment. c. When a consumer makes adjustments in the application of funds in an individual budget, these shall occur within a framework that has been agreed to by the consumer and the CMHSP, and described in an attachment to the consumer‘s selfdetermination agreement. When changes are made, these shall be promptly communicated to the CMHSP. d. If an adjustment in the use of the budget is intended for a service/support that does not serve to accomplish the direction and intent of the person‘s plan, then the plan must be appropriately modified before the adjustment may be made. The CMHSP shall attempt to resolve such situations in an expedient manner. e. The funds aggregated and used to finance an individual budget may be controlled by more than one funding source. Flexibility in the use of these funds is therefore constrained by the specific limitations of funding sources (e.g., Home Help, Vocational Rehabilitation, etc.) Consumers must be informed when some of the resources associated with accomplishing their plan of services and supports involve commitments from funding sources other than the CMHSP, and assisted to work within constraints that accompany them. 124 f. Funds allotted for specialty mental health services may not be used to purchase services which are not specialty mental health services, nor should contracts with providers of specialty mental health services be entered into if they are not fiscally prudent. 5. Either party -- the CMHSP or the consumer -- may terminate a self-determination agreement, and therefore, the self-determination arrangement. Prior to the CMHSP terminating an agreement, and unless it is not feasible, the CMHSP shall inform the consumer of the issues that have led to consideration of a discontinuation or alteration decision, in writing, and provide an opportunity for problem resolution. Typically this will be conducted using the person-centered planning process, with termination being the option of choice if other mutually-agreeable solutions cannot be found. In any instance of CMHSP discontinuation or alteration of a self-determination arrangement, the local processes for dispute resolution may be used to address and resolve the issues. 6. Discontinuation of a self-determination agreement shall not, by itself, change the consumer‘s plan of services, nor eliminate the obligation of the CMHSP to assure specialty mental health services and supports required in the plan. 7. In any instance of CMHSP discontinuation or alteration, the consumer must be provided an explanation of applicable appeal, grievance and dispute resolution processes and (where required) appropriate notice. IV. Assuring authority over an individual budget is a core element of selfdetermination. This means that the consumer may use, responsibly, an individual budget as the means to authorize and direct their providers of services and supports. A CMHSP shall design and implement alternative approaches that consumers electing to use an individual budget may use to obtain consumer-selected and directed provider arrangements. A. Within prudent purchaser constraints, a consumer shall be able to access any willing and qualified provider entity that is available to provide needed specialty mental health services and supports. B. Approaches shall provide for a range of control options up to and including the direct retention of consumer-preferred providers through purchase of services agreements between the consumer and the provider. Options shall include, upon the consumer‘s request and in line with their preferences: 1. Services/supports to be provided by an entity or individual currently operated by or under contract with the CMHSP. 2. Services/supports to be provided by a qualified provider chosen by the consumer, with the CMHSP agreeing to enter into a contract with that provider. 125 3. Services/supports to be provided by a consumer-selected provider with whom the consumer executes a direct purchase-of-services agreement. The CMHSP shall provide guidance and assistance to assure that agreements to be executed with consumer-selected providers are consistent with applicable federal regulations governing provider contracting and payment arrangements. a. Consumers shall be responsible for assuring those individuals and entities selected and retained meet applicable provider qualifications. Methods that lead to consistency and success must be developed and supported by the CMHSP. b. Consumers shall assure that written agreements are developed with each provider entity or individual that specify the type of service or support, the rate to be paid, and the requirements incumbent upon the provider. c. Copies of all agreements shall be kept current, and shall be made available by the consumer, for review by authorized representatives of the CMHSP. d. Consumers shall act as careful purchasers of specialty mental health services and supports necessary to accomplish their plan. Arrangements for purchasing services shall not be excessive in cost. Consumers should aim for securing a better value in terms of outcomes for the costs involved. Existing personal and community resources shall be pursued and utilized before using public mental health system resources. e. Fees and rates paid to providers with a direct purchase-of-services agreement with the consumer shall be negotiated by the consumer, within the boundaries of the consumer‘s authorized individual budget. The CMHSP shall provide guidance as to the range of applicable rates, and may set maximum amounts that a consumer may spend to pay specific providers. 4. A consumer shall be able to access alternative methods to choose, control and direct personnel necessary to provide direct support, including: a. Acting as the employer of record of personnel. b. Access to a provider entity that can serve as employer of record for personnel selected by the consumer. c. CMHSP contractual language with provider entities that assures consumer selection of personnel, and removal or reassignment of personnel who fail to meet consumer preferences. d. Use of CMHSP-employed direct support personnel, as selected and retained by the consumer. 126 5. A consumer participating in self-determination shall not be obligated to utilize CMHSPemployed direct support personnel or a CMHSP-operated or -contracted program/service. 6. All individuals selected by the consumer, whether she or he is acting as employer of record or not, shall meet applicable provider requirements for direct support personnel, or the requirements pertinent to the particular professional services offered by the provider. 7. A consumer shall not be required to select and direct needed provider entities or his/her direct support personnel if she or he does not desire to do so. IV. A CMHSP shall assist a consumer participating in self-determination to select, employ, and direct his/her support personnel, to select and retain chosen qualified provider entities, and shall make reasonably available, consistent with MDCH Technical Advisory instructions, their access to alternative methods for directing and managing support personnel. A. A CMHSP shall select and make available qualified third-party entities that may function as fiscal intermediaries to perform employer agent functions and/or provide other support management functions, in order to assist the consumer in selecting, directing and controlling providers of specialty services and supports. B. Fiscal intermediaries shall be under contract to the CMHSP or a designated subcontracting entity. Contracted functions may include: 1. Payroll agent for direct support personnel employed by the consumer (or chosen representative), including acting as an employer agent for IRS and other public authorities requiring payroll withholding and employee insurances payments. 2. Payment agent for consumer-held purchase-of-services and consultant agreements with providers of services and supports. 3. Provision of periodic (not less than monthly) financial status reports concerning the individual budget, to both the CMHSP and the consumer. Reports made to the consumer shall be in a format that is useful to the consumer in tracking and managing the funds making up the individual budget. 4. Provision of an accounting to the CMHSP for the funds transferred to it and used to finance the costs of authorized individual budgets under its management. 5. Assuring timely invoicing, service activity and cost reporting to the CMHSP for specialty mental health services and supports provided by individuals and entities that have a direct agreement with the consumer. 127 6. Other supportive services, as denoted in the contract with the CMHSP, that strengthen the role of the consumer as an employer, or assist with the use of other agreements directly involving the consumer in the process of securing needed services. C. A CMHSP shall assure that fiscal intermediary entities are oriented to and supportive of the principles of self-determination, and able to work with a range of consumer styles and characteristics. The CMHSP shall exercise due diligence in establishing the qualifications, characteristics and capabilities of the entity to be selected as a fiscal intermediary, and shall manage the use of fiscal intermediaries consistent with MDCH Technical Assistance Advisories addressing fiscal intermediary arrangements. D. An entity acting as a fiscal intermediary shall be free from other relationships involving the CMHSP or the consumer that would have the effect of creating a conflict of interest for the fiscal intermediary in relationship to its role of supporting consumerdetermined services/supports transactions. These other relationships typically would include the provision of direct services to the consumer. The CMHSP shall identify and require remedy to any conflicts of interest of the entity that, in the judgment of the CMHSP, interfere with the performance of its role as a fiscal intermediary. E. A CMHSP shall collaborate with and guide the fiscal intermediary and each consumer involved in self-determination to assure compliance with various state and federal requirements and to assist the consumer in meeting his/her obligations to follow applicable requirements. It is the obligation of the CMHSP to assure that the entities selected to perform intermediary functions are capable of meeting and maintaining compliance with the requirements associated with their stated functions, including those contained in relevant MDCH Technical Assistance Advisories. F. Typically, funds comprising a consumer‘s individual budget would be lodged with the fiscal intermediary, pending appropriate direction by the consumer to pay consumer-selected and contracted providers. Where a consumer selected and directed provider of services has a direct contract with the CMHSP, the provider may be paid by the CMHSP, not the fiscal intermediary. In that case, the portion of funds in the individual budget would not be lodged with the fiscal intermediary, but instead would remain with the CMHSP, as a matter of fiscal efficiency. Definitions Fiscal Intermediary: A fiscal Intermediary is an independent legal entity (organization or individual) that acts as a fiscal agent of the CMHSP for the purpose of assuring fiduciary accountability for the funds comprising a consumer‘s individual budget. A fiscal intermediary shall perform its duties as specified in a contract with a CMHSP or its designated sub-contractor. 128 The purpose of the fiscal intermediary is to receive funds making up a consumer‘s individual budget, and make payments as authorized by the consumer to providers and other parties to whom a consumer using the individual budget may be obligated. A fiscal intermediary may also provide a variety of supportive services that assist the consumer in selecting, employing and directing individual and agency providers. Examples of entities that might serve in the role of a fiscal intermediary include: bookkeeping or accounting firms; local ARC or other advocacy organizations; a subsidiary of a service provider entity if no conflict of interest exists. Qualified Provider: A qualified provider is an individual worker, a specialty practitioner, professional, agency or vendor that is a provider of specialty mental health services or supports that can demonstrate compliance with the requirements contained in the contract between the Department of Community Health and the CMHSP, including applicable requirements that accompany specific funding sources, such as Medicaid. Where additional requirements are to apply, they should be derived directly from the consumer‘s person-centered planning process, and should be specified in the consumer‘s plan, or result from a process developed locally to assure the health and well-being of consumers, conducted with the full input and involvement of local consumers and advocates. Consumer: For the purposes of this policy, ―Consumer‖ means the adult consumer of direct specialty mental health services and supports, and/or his/her selected representative. That is, the consumer may select a representative to enter into the selfdetermination agreement and for other agreements that may be necessary for the consumer to participate in consumer-directed supports and services arrangements. Where the consumer has a legal guardian, the role of the guardian in self-determination shall be consistent with the guardianship arrangement established by the court. A person selected as the representative of the consumer shall not supplant the role of the consumer in the process of person-centered planning, in accordance with the Mental Health Code and the requirements of the contract between the CMHSP and the Department of Community Health. Where a consumer has been deemed to require a legal guardian, there is an extra obligation on the part of the CMHSP and those close to the consumer to assure that it is the consumer‘s preferences and dreams that drive the use of self-determination arrangements, and that the best interests of the consumer are primary. A CMHSP shall have the discretion to limit or restrict the use of self-determination arrangements by a guardian when the planned or actual use of those arrangements by that guardian are in conflict with the expressed goals and outcomes of the consumer. Individual Budget: An individual budget is a fixed allocation of public mental health resources, and may also include other public resources whose access involves the assistance of the CMHSP, denoted in dollar terms. These resources are agreed upon as the necessary cost of specialty mental health services and supports needed to accomplish a consumer‘s plan of services/supports. 129 The consumer served uses the funding authorized to acquire, purchase and pay for specialty mental health services and supports that support accomplishment of the consumer‘s plan. Plan: A plan means the consumer‘s Individual Plan of Services and/or Supports, as developed using a person-centered planning process. CMHSP: For the purposes of this policy, a Community Mental Health Services Program is an entity operated under Chapter Two of the Michigan Mental Health Code, or an entity under contract with the CMHSP and authorized to act on its behalf in providing access to, planning for, and authorization of specialty mental health services and supports for people eligible for mental health services. Specialty Mental Health Services: This term includes any service/support that can legitimately be provided using funds authorized by the CMHSP in the individual budget. It includes alternative services and supports as well as Medicaid-covered services and supports. Choice Voucher System: The Choice Voucher System is the designation for set of arrangements that facilitate and support accomplishing self-determination, through the use of an individual budget, a fiscal intermediary, and direct consumer-provider contracting. Its use shall be guided by MDCH Technical Assistance Advisories which may be issued from time to time by the Department. Self-Determination: Self-determination incorporates a set of concepts and values that underscore a core belief that people who require support from the public mental health system as a result of a disability should be able to define what they need in terms of the life they seek, have access to meaningful choices, and have control over their lives. Within Michigan‘s public mental health system, self-determination involves accomplishing system change to assure that services and supports for people are not only person-centered, but person-defined and person-controlled. Self-determination is based on four principles. These principles are: Freedom: The ability for individuals, with assistance from significant others (e.g., chosen family and/or friends), to plan a life based on acquiring necessary supports in desirable ways, rather than purchasing a program. This includes the freedom to choose where and with whom one lives, who and how to connect to in one‘s community, the opportunity to contribute in one‘s own ways, and the development of a personal lifestyle. Authority: The assurance for a person with a disability to control a certain sum of dollars in order to purchase these supports, with the backing of their significant others, as needed. It is the authority to control resources. 130 Support: The arranging of resources and personnel, both formal and informal, to assist the person in living his/her desired life in the community, rich in community associations and contributions. It is the support to develop a life dream and reach toward that dream. Responsibility: The acceptance of a valued role by the person in the community through employment, affiliations, spiritual development, and caring for others, as well as accountability for spending public dollars in ways that is life-enhancing. This includes the responsibility to use public funds efficiently and to contribute to the community through the expression of responsible citizenship. A hallmark of self- determination is assuring a person the opportunity to direct a fixed amount of resources, which is derived from the person-centered planning process and called an individual budget. The person controls the use of the resources in his/her individual budget, determining, with the assistance of chosen allies, which services and supports he or she will purchase, from whom, and under what circumstances. Through this process, they possess power to make meaningful choices in how they live their life. Housing Best Practice Guidelines [From the contract between CMH, Community Mental Health, and DCH, Michigan Dept. of Community Health.] I. Summary This guideline establishes policy and procedure for ensuring that the provision of mental health services and supports are not affected by where consumers choose to live: their own home, the home of another or in a licensed setting. In those instances when public money helps subsidize a consumer‘s living arrangement, the housing unit selected by the consumer shall comply with applicable occupancy standards. II. Application A. Psychiatric hospitals operated by the Michigan Department of Community Health (MDCH). B. Regional centers for developmental disabilities operated by MDCH. C. Special facilities operated by MDCH. D. Residential placement agencies operated by MDCH. E. Community Mental Health Services Programs (CMHSPs) as specified in their master contract with MDCH. III. Policy 131 The Michigan Department of Community Health recognizes housing to be a basic need and affirms the right of all consumers of public mental health services to pursue housing options of their choice. Just as consumers living in licensed dependent settings may require many different types of services and supports, persons living in their own homes or sharing their household with another may have similar service needs. RMHA‘s [Responsible Mental Health Agency] shall foster the provision of services and supports independent [regardless] of where the consumer resides. When requested, RMHAs shall educate consumers about the housing options and supports available, and assist consumers in locating habitable, safe, and affordable housing. The process of locating suitable housing shall be directed by the consumer‘s interests, involvement and informed choice. Independent housing arrangements in which the cost of housing is subsidized by the RMHA are to be secured with a lease or deed in the consumer‘s name. This policy is not intended to subvert or prohibit occupancy in or participation with community based treatment settings such as an adult foster care home when needed by an individual recipient. IV. Definitions Affordable: is a condition that exists when an individual‘s means or the combined household income of several individuals is sufficient to pay for food, basic clothing, health care, and personal needs and still have enough left to cover all housing related costs including rent/mortgage, utilities, maintenance, repairs, insurance and property taxes. In situations where there are insufficient resources to cover both housing costs and basic living costs, individual housing subsidies may be used to bridge the gap when they are available. Habitable and safe: means those housing standards established in each community that define and require basic conditions for tenant/resident health, security, and safety. Housing: refers to dwellings that are typical of those sought out and occupied by members of a community. The choices a consumer of mental health services makes in meeting his or her housing needs are not to be linked in any way to any specific program or support service needs he or she may have. Responsible Mental Health Agency (RMHA): means the MDCH hospital, center or CMHSP responsible for providing and contracting for mental health services and/or arranging and coordination the provision of other services to meet the consumers‘ needs. 132 V. STANDARDS RMHAs shall develop policies and create mechanisms that give predominant consideration to consumers‘ choice in selecting where and with whom they live. These policies and mechanisms shall also: A. Ensure that RMHA-supported housing blends into the community. Supported housing units are to be scattered throughout a building, complex, or the community in order to achieve community integration when possible. Use of self-contained campuses or otherwise segregated buildings as service sites is not the preferred mode. B. Promote and support home ownership, individual choice, and autonomy. The number of people who live together in RMHA-supported housing shall not exceed the community‘s norms for comparable living settings. C. Assure that any housing arranged or subsidized by the RMHA is accessible to the consumer in compliance with applicable state and local standards for occupancy, health, and safety. D. Be sensitive to the consumer‘s cultural and ethnic preferences and give consideration to them. E. Encourage and support the consumer‘s self-sufficiency. F. Provide for ongoing assessment of the consumer‘s housing needs. G. Provide assistance to consumers in coordinating available resources to meet their basic housing needs. RMHAs may give consideration to the use of housing subsidies when consumers have a need for housing that cannot be met by the other resources which are available to them. VI. References and Legal Authority MCL 330.1116(j). VII. Exhibits Federal Housing Subsidy Quality Standards based on 24 CFR § 882.10. Housing occupied by a consumer of the Supported Community Living Program must meet the following minimum environmental standards as interpreted by MDCH based on 24 CFR § 882.10 [Housing Quality Standards]. Such housing standards shall serve as an example of standards that should be considered when seeking federally subsidized housing. 133 Every unit must have at least a living room, kitchen and bath. A one-room efficiency with a kitchen may be utilized provided there is a private bath. The ceilings, walls and floors of each room should be in good condition; cracks, bulges, holes, and floor coverings that might cause someone to trip are unacceptable as is lead paint. Each room must have at least one window that opens to the outside except for the bath where a working exhaust fan may substitute for a window. All windows designed to be operable and should open easily. All operable windows and doors that can be reached from the outside, a common public hallway, a fire escape, porch or other outside place that can be reached from the ground, must have a working lock. The living room should have at least two wall mounted electrical outlets, or one outlet and one permanent overhead light fixture. The kitchen should have at least one electrical outlet and one permanent light fixture; the bath at least one permanent overhead or wall light fixture. Both the kitchen and bath electrical outlets must have ground fault interrupters. Table, floor and ceiling lamps plugged into sockets and extension cords do not count; they are not permanent. Broken or frayed wiring, fixtures hanging from wires with no other firm support (such as a chain), missing cover plates on switches or outlets and badly cracked outlets are not acceptable. Both the kitchen and bath must have hot and cold running water. A bathroom sink may not be used in place of a kitchen sink and vice versa. The bathroom should have a tub or shower with hot and cold running water and a toilet that works. Single units must have at least two unobstructed means of egress. Units in apartment complexes should have an entrance from the outside or from a public hall so that it is not necessary to go through anyone else‘s living space to get into the unit. There shall be an operating smoke detector adjacent to each sleeping area with appropriate maintenance procedures in place to keep each detector continuously operational. If the unit is in an apartment building with elevators or stairwells, the former should be safe and work properly and the latter well lit and have railings. Any length of stairs (e.g., generally more than four steps), and porches, balconies or decks more than 30 inches above ground should have secure handrails attached. The building foundation should have no serious leaks and the plumbing and sewage systems must be served by an approved public or private water supply system. The roof should not leak and the gutters and downspouts, if present, should be securely attached to the building. 134 Roof leaks can usually be detected by checking for stains on the ceiling inside the building. The chimney should not lean or have big cracks or missing bricks, the water pipes should be in good condition with no leaks and no serious rust that causes the water to be discolored, the water heater should be equipped and installed in a safe manner, and the heating equipment should be adequate to provide sufficient heat to keep the unit warm during cold months. Spacer heaters (or room heaters) that burn oil or gas and are not vented to a chimney are not acceptable. Space heaters that are vented are acceptable if they provide sufficient heat. If the service site is a mobile home, it must be placed on the site in a stable manner so as to be free from hazards such as sliding or wind damage, and there must be at least one operating smoke detector in the home with appropriate maintenance procedures in place to keep it continuously operational. 135


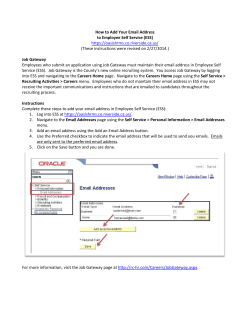







© Copyright 2026