
2014-2016 Home & Community Based Services Provider Manual i
2014-2016 Home & Community Based Services Provider Manual 5240 Fountain Drive Crown Point, IN 46307 www.nwica.com i Contents Home and Community Based Services Manual..........................................................................................1 Funding Sources and Eligibility .................................................................................................................1 Community and Home Options to Institutional Care for the Elderly and Disabled (CHOICE) ............................. 1 Social Services Block Grant-Title XX..................................................................................................................... 2 Title III: Funding Requirements (OAA) ................................................................................................................. 3 Older Hoosier Account Funding Requirements.................................................................................................... 3 HCBS Service Definitions ..........................................................................................................................4 Adult Day Services (AD1, AD2, AD3, ADST) ......................................................................................................... 4 Attendant Care Services (ATTC)........................................................................................................................... 7 Home Delivered Meals (HDM)........................................................................................................................... 10 Home Health Aide Services (HOHE) ................................................................................................................... 13 Home Health Supplies and Assistive Devices (ATCH, ATCM, SUPP)................................................................... 15 Home Repair/Maintenance Services (HCP) ....................................................................................................... 18 Homemaker Services (HMK) .............................................................................................................................. 20 Personal Emergency Response System (PRSI, PRSM) ........................................................................................ 22 Respite (RNUR, RHHA, RATT, RHMK)................................................................................................................. 24 Skilled Nursing (SKNU)....................................................................................................................................... 26 Transportation Services (TRAN)......................................................................................................................... 27 Standard Operating Procedures for HCBS ...............................................................................................29 Service Provision....................................................................................................................................33 Reimbursement to Providers..................................................................................................................42 HCBS Forms ...........................................................................................................................................45 CHOICE Invoice .................................................................................................................................................. 46 i SSBG Invoice………… ........................................................................................................................................... 47 Title IIIE Family Caregiver Invoice ...................................................................................................................... 48 Title IIIB In-Home Services Invoice ..................................................................................................................... 49 Transportation Invoice....................................................................................................................................... 50 HCBS Billing ...........................................................................................................................................51 Appendix A 455 IAC 2: Home & Community Based Services Rule...................................................................... 54 Appendix B: Indiana Division of Aging Incident Reporting Policy ..................................................................... 81 Appendix C: IHCP Bulletin BT200371 – Documentation Standards for HCBS .................................................... 91 Appendix D: Older Americans Act Title III C..................................................................................................... 106 Appendix E: CHOICE Guidelines ...................................................................................................................... 112 ii Home and Community Based Services Manual Funding Sources and Eligibility Community and Home Options to Institutional Care for the Elderly and Disabled (CHOICE) The Community and Home Options to Institutional Care for the Elderly and Disabled Program (CHOICE) is designed to change the way the state provides and delivers long-term care for older adults and persons with disabilities. Above all, the purpose of CHOICE is to enable older adults or persons with disabilities to live independently in their own homes or in community-integrated settings. It is further intended to allow older adults ready access to community resources in order to improve the quality of life of families and children, with an emphasis on seniors and persons with disabilities. The program is also intended to encourage more coordinated planning; to give increased attention to CHOICE participant views; to provide greater respect for participant preferences; and to value participant selection of providers as well as services. Choice Funding Requirements CHOICE funds are exclusively state dollars used to provide services for older adults and persons with disabilities enabling these individuals to maintain independence in their own homes and communities. Eligibility Requirements for Choice Funding To be eligible for CHOICE funding, the older adult or person with disabilities must: be a resident of Indiana; be at least 60 years of age or disabled; make complete and proper application for Medicaid; qualify under criteria developed by the CHOICE board as having an impairment that places the person at risk of losing independence; and have no assets or have assets that do not exceed the worth of five hundred thousand ($500,000) as determined by the FSSA DA. apply for Indiana Medicaid and receive and eligibility determination from the Division of Family Resources A person is at risk of losing independence if the person is unable to perform two or more activities of daily living as measured on the long-term care services eligibility screen. The use by or on behalf of the person of any of the following services or devices do not make the client ineligible for services under CHOICE: skilled nursing assistance; supervised community and home care services, including skilled nursing supervision; adaptive medical equipment and devices; and 1 adaptive non-medical equipment and devices. Financial Eligibility and Cost Share Requirements for Choice Funding CHOICE services are offered to all persons regardless of their income. Although there are no income restrictions on eligibility, there is a method of cost reimbursement applicable to individuals who can pay all or a portion of the cost of CHOICE services rendered. The cost share requirement: The client's cost share of the payment for services rendered shall be calculated by using the CHOICE Cost Share Worksheet, which includes the United States Department of Health and Human Services Poverty Income Guidelines. (For more information, consult the Community and Home Options to Institutional Care for the Elderly and Persons with Disabilities (CHOICE)). CHOICE is the funding of last resort for in-home and community-based services. If funding for a consumer’s services is available from any other source, that source must be used before CHOICE funding can be used. * A copy of the complete CHOICE Guidelines manual is included as Appendix E of this Service Provider Manual. Social Services Block Grant-Title XX The Social Services Block Grant (SSBG) was created for the purpose of consolidating federal assistance to states for social services into a single grant. States are given much flexibility in using social services grants and are encouraged to furnish services directed at particular objectives. The FSSA DA uses SSBG money to fund a compilation of in-home, community-based, and facility-oriented services targeted for low-income older adults and persons with disabilities. Eligibility Requirements for SSBG Funding To be eligible for SSBG funding, the older adult or person with disabilities client must meet the following requirements: The client must be a resident of Indiana. The client must have a documented determination of service need. A service need exists when the case management provider determines and documents that the client's functional status may be enhanced through the provision of appropriate services. The client must meet program income guidelines. If the client fails to meet the income guidelines but has a documented need for service due to abuse, neglect, exploitation, risk of institutionalization, and/or pending discharge from the hospital or nursing facility, the client may qualify for SSBG funded services as a no means-test client. Otherwise, the client must be determined to be in financial need by the case management provider. Financial need exists when the client's and the family's incomes fall below 300% of the poverty level listed in the current Department of Health and Human Services Poverty Guidelines. The client must meet program income guidelines through a declaration of income (the verbal indication of the source and amount of gross income). 2 Title III: Funding Requirements (OAA) Title III funds are federal dollars that are provided to the FSSA DA for allocation to AAAs and service providers to develop and implement services necessary to allow older adults to remain in their homes as long as possible, while enhancing their sense of dignity and worth. Eligibility Requirements for Title III Funding To be eligible for Title III funding, the client must be at least 60 years of age. Priority is given to serving those older adults who are in greatest economic need, social need, or both, with particular attention to low-income minority older adults, and to serving older adults residing in rural areas. Although there are no financial eligibility requirements for Title III, specific programs funded partially or fully with Title III dollars may have special financial eligibility requirements. For additional eligibility requirements, refer to Section 4 - Service Definitions. Older Hoosier Account Funding Requirements The Indiana legislature appropriates state dollars to the FSSA DA to assist with meeting the match requirements of various funding sources that support programs and activities for older adults. Programs under Title III, Title V, and Title VII of the OAA require that federal funds be matched by state and local funds. Eligibility Requirements for Older Hoosier Account Funding Eligibility requirements are the same as those of the funding source the Older Hoosier account dollars are used to match. Financial Eligibility Financial eligibility requirements are the same as those of the funding source the Older Hoosier account dollars are used to match. Older Hoosier accounts match a percentage of dollars provided by a particular funding source. Services provided would depend upon the funding source the Older Hoosier account dollars are used to match. 3 HCBS Service Definitions Adult Day Services (AD1, AD2, AD3, ADST) Applicable Rules and Regulations 455 IAC 1 & 2 – Home and Community Based Services rule; State of Indiana Medicaid Waiver Standards and Guidelines for Adult Day Services; Section 4003 of the Indiana Division on Aging Operations Manual; Section 7 of the Indiana Division of Aging Waiver Provider Manual ; Section 10038 of the Indiana FSSA CHOICE Manual; and NWICA all define service as: Service Description Adult Day Services are structured community based programs that provide a variety of health, social, recreational, and related supportive services for older adults and persons with disabilities in a protective setting during daytime and early evening hours. This service is designed to meet the needs of eligible persons through an individualized service plan including personal care and supervision, medical care, transportation to and from the site, and therapeutic and recreational activities. Adult Day Services also includes the provision of meals and snacks, as appropriate. Adult Day Services assess the needs of participating individuals and offer services to meet those needs. Adult Day Services are provided at 3 different, designated levels of services. The 3 levels of Adult Day Services include: Basic Adult Day Services (Level 1) which include the following: monitoring and/or supervision of all Activities of Daily Living (ADL’s) which are defined as dressing, bathing, grooming, eating, walking, and toileting with hands on assistance provided as needed; comprehensive, therapeutic activities; assurance health assessment and intermittent monitoring of health status; monitoring of medication/or medication administration; and the ability to provide appropriate structure and supervision for those with mild cognitive impairment. Enhanced Adult Day Services (Level 2) which include the following: assuring that Basic (Level 1) service requirements are met; providing hands-on assistance with 2 or more ADL’s or hands-on assistance with bathing or other personal care; health assessment with regular monitoring or intervention with health status; dispensing or supervision of the dispensing of medications to participants; psychosocial needs assessment and addressing needs including counseling for participants and caregivers; and provision of appropriate therapeutic structure, supervision and intervention for those with mild to moderate cognitive impairments. Intensive (Level 3) which includes the following: meeting Basic (Level 1) and Enhanced (Level 2) service requirements; hands on assistance or supervision with all ADL’s and personal care; one or more direct health intervention(s) as required; rehabilitation and restorative services including Physical Therapy, Speech Therapy, Occupational Therapies, coordinated or available; providing therapeutic intervention to address dynamic psychosocial needs such as depression or family issues effecting care; and providing therapeutic interventions for those participants with moderate to severe cognitive impairments. 4 Allowable Activities Supervision and assistance, when needed, with Activities of Daily Living and supervision of personal hygiene and personal care as determined in level of service assessment. Provision of individual and group social, health related, and recreational activities provided at the Adult Day Service site. Recreational activities should be activities that are included in a place of treatment related to specific therapeutic goals which can include a group exercise program and preventative health screening such as blood pressure checks and discussion groups. Activities that may be provided outside the program site, during service hours, if accompanied by a staff member, Those activities may include: 2 shopping trips per month (per client), when taken in a group; Medically related trips, when necessary, as documented in the care plan; a maximum of 4 specialized field trips each per month designed for client groups, such as attendance at concerts, plays, films, museums, or special events; and 1 nutritionally balanced meal per day (and a nutritional snack if the client is present for more than 3 hours). Activities Not Allowed Funding sources for adult day services will cover only those activities described as Allowable Activities. Provider Requirements Adult Day Service providers must be approved by the Indiana Division on Aging. The provider must be in compliance with the following requirements of the Indiana Medicaid Adult Day Services Standards and Guidelines: administrative structure requirements administrative responsibilities staff requirements facility and grounds requirements service requirements emergency preparedness documentation requirements service file documentation requirements activities requirements food service requirements meal requirements nutrition component requirements vehicle requirements Unit of Service ¼ hour = 1 unit Service Authorization Services must be provided in accordance with the Vendor Authorization issued by the NWICA Case Manager. Documentation Requirements Documentation as required by the Indiana Medicaid Adult Day Service Standards and Guidelines Documentation compliant with the Indiana Health Coverage Programs Provider Bulletin BT200371, Documentation Standards for Home and Community-Based Services Waiver Programs 5 NWICA monthly service progress report. Funding Source(s) Funding sources include SSBG, CHOICE, Older Hoosier Funds, Title III, Program income. 6 Attendant Care Services (ATTC) Applicable Rules and Regulations 455 IAC 1 & 2 – Home and Community Based Services Rule; IC 16-27-4 Licensure of Personal Service Agencies; Section 4007 of the Indiana Division on Aging Operations Manual; Section 7 of the Indiana Division of Aging Waiver Provider Manual; Section 10039 of the Indiana FSSA CHOICE Manual; and NWICA all define service as: Service Description Attendant Care Services are defined by law as services that could be performed by an impaired individual for whom the services are provided if the individual were not impaired; and that enable the impaired individual to live in the individual's home and community rather than in an institution; and to carry out functions of daily living, self-care, and mobility. The term includes the following: Assistance in getting in and out of beds, wheelchairs, and motor vehicles Assistance with routine bodily functions, including: bathing and personal hygiene; using the toilet; dressing and grooming; and feeding, including preparation and cleanup. The provision of assistance: through providing reminders or cues to take medication, the opening of preset medication containers, and providing assistance in the handling or ingesting of non-controlled substance medications, including eye drops, herbs, supplements, and over-the-counter medications; and to an individual who is unable to accomplish the task due to an impairment and who is: competent and has directed the services; or incompetent and has the services directed by a competent individual who may consent to health care for the impaired individual. Allowable Activities Attendant Care Services may include: Assistance, as specified in the plan of care, which may include the following: Personal Care and Grooming activities including bathing, oral hygiene, hair care, shaving, dressing, application of cosmetics, etc. under the following circumstances: Client does not require skilled transfer, skilled skin care or skilled assistance with dressing. Client’s skin is not broken or open There are no active chronic skin problems May include preventive care only such as massage of reddened areas, application of skin moisturizers, nonmedicated OTC lotions or solutions, reporting changes to supervisor, application of preventive spray to unbroken skin areas, which may be susceptible to breakdown. Mobility Transfer under the following circumstances: Client needs only standby assistance or assistance with adaptive equipment (such as gait belt, wheelchairs, tub seats, grab bars) Client is able to direct the transfer and assist with transfer to some extent Client DOES NOT require a mechanical lift such as a Hoyer lift. 7 Client has good balance, is NOT in a weakened state and has a low risk for falls Client is fully trained in use of adaptive/assistive devices as well as transfer in and out of a motor vehicle. Attendant Care does NOT transport Clients. May accompany Client to medical appointments and to other service ONLY if assigned on care plan and when all care provided in relation to the trip is non-skilled Assistance with ambulation under the following circumstances: Client is fully trained with adaptive equipment Skilled transfer is NOT required Client does NOT have any cast or need for special skin care Client generally independent and needs only stand-by assistance or assistance with a gait belt Nutrition Meal planning, preparation, and clean up Elimination Assisting with bedpan, bedside commode, toilet Incontinent or involuntary care Emptying urine collection and colostomy bags Safety Use of the principles of health and safety in relation to self and client Identify and eliminate safety hazards Practice health protection and cleanliness by appropriate techniques of hand washing, waste disposal, and household tasks Other Reminding client to self-administer medication Realty orientation and sensory stimulation Escorting client to medical appointments. Attendant Care shall NOT transport Clients. May accompany Client to medical appointments and to other service ONLY if assigned on care plan and when all care provided in relation to the trip is non-skilled Assistance with correspondence and bill paying. Incidental homemaker activities, which are not furnished in the absence of other attendant care services that are essential to the client’s health care needs to prevent or postpone institutionalization. Activities directly related to a client’s medical needs, furnished in conjunction with but subordinate to direct Client care, are described in the Homemaker Service – Section 4013 Activities Not Allowed occupied bed changes; bearing full weight of client during transfer; supervision of dispensing of medication by client or dispensing of medication for client; skin care on broken skin; passive range of motion exercises; assistance with crutch ambulation; bed baths; other activities that must be performed by a licensed health care professional; and nail care of diabetic clients. Attendant Care Services will not be provided to medically unstable clients as a substitute for care provided by a registered nurse, licensed practical nurse, licensed physician, or other health professional. Provider Requirements 8 Pursuant to state law, NWICA requires its providers of Attendant Care to be licensed either as a Home Health Agency or a Personal Service Agency. To provide services under CHOICE funding, the provider must also be certified as a Medicaid Waiver provider. Unit of Service ¼ hour = 1 unit Service Authorization Services must be provided in accordance with the Vendor Authorization issued by the NWICA Case Manager. Documentation Requirements Documentation required by the Indiana State Department of Health Documentation compliant with the Indiana Health Coverage Programs Provider Bulletin BT200371, Documentation Standards for Home and Community-Based Services Waiver Programs NWICA monthly service progress report. Funding Source(s) Funding sources include SSBG, Title III, CHOICE, and local funds. 9 Home Delivered Meals (HDM) Applicable Rules and Regulations Title IIIC of the Older Americans Act; 455 IAC 1 & 2 Home and Community Based Services Rule; Section 10043 of the Indiana FSSA CHOICE Manual; Section 8000 of the Indiana Division of Aging Operations Manual; Section 7 of the Indiana Division of Aging Waiver Provider Manual ; and NWICA all define services as: Service Description A Home delivered meal is a meal provided to a qualified individual at his/her place of residence. The meal is served as part of a program administered by the AAA and meets all the requirements of the Older Americans Act and State/Local laws. Home Delivered Meal Program Requirements The Home Delivered Meals provider shall deliver the meal that has been prepared by a NWICA contracted Meal Preparation/Catering vendor, to the eligible participant’s home. There shall be no more than a four-hour lapse of time between preparation time and meal delivery at the clients home. The Home Delivered Meals provider shall maintain the proper temperatures for the hot food at 135° F.; and cold foods at 40° F.; and shall maintain adequate sanitary practices for handling the food transit. The Home Delivered Meals provider shall be compliant with any and all pertinent rules and regulations as set forth by the Local Board of Health having jurisdiction in the area that the provider operates. The Home Delivered Meals provider must maintain appropriate insurance pertaining to the preparation and distribution of meals. The Home Delivered Meals provider must provide meals in accordance with the menu approved by the NWICA contracted Registered Dietician. Participant Contributions The Home Delivered Meals providers shall offer the opportunity for each client to contribute financially toward the cost of a meal. The Home Delivered Meals provider shall ensure a method to solicit and collect contributions that maintains client confidentiality. The contribution is considered program income. Program income records must be available upon request and reported to NWICA on a monthly basis. The Home Delivered Meals providers will ensure that all contributions are counted and recorded daily by two (2) people. All contribution records must be documented on the required client signature sheet. The client signature sheet and proof of deposit must be submitted to NWICA on a monthly basis. The Home Delivered Meals provider must have written fiscal policies and procedures regarding control of program income. The fiscal policies and procedures regarding program income must provide reasonable assurance that program income is correctly earned, recorded, and used to expand Home Delivered Meals services. In accordance with OMB Circular A-110, use of program income is limited to increasing meal service, providing supportive services related to improving nutritional status, and facilitating access to nutrition services. Program income must be verifiable in the provider’s general ledger. 10 Emergency Plans Emergency plans must be in place for all home delivered meal programs. The plan must include at least the following information: 1) Written procedures are in place: To contact staff, volunteers, caterers, etc. (e.g., telephone and cell numbers, phone tree) For weather-related emergencies. To determine program closings. To notify participants of program closings (e.g., radio, telephone). For facility and equipment breakdowns. When individuals are hurt or become ill. Identifying emergency service agencies to assist in meal delivery, rescue, or other matters. When key personnel are absent. 2) Staff is trained to assist older adults in an emergency situation: Participant files include emergency contact or caregiver designee information. Participants are provided printed information about the types of foods and other necessities to have on hand for emergencies. Home Delivered Meal Supplies for Service: In order to provide a home delivered nutritious meal to eligible participants some necessary supplies will be needed. These supplies will be provided by the NWICA contracted Meal Preparation/Catering vendor. Below are items that may be required for service; Condiment Approved Food Carry-out Containers Insulated Food Carrier Emergency Supply Pack Shelf stable meal packages will be available in the month (s) of December and January. The Nutrition Coordinator will organize a shelf stable meal request letter that will be sent out to all Home Delivered Meals vendors for amount submission. Once ordered, the supplier will deliver to all vendors in the six county region. Shelf stable meals are non-refrigerated and require minimal to no preparation and they are nutritionally packaged to meet the regulated one-third RDA. The shelf stable meals will supply clients with an emergency meal replacement due to state of an emergency and nutrition program closures. Allowable Activities Delivery of meals supplied by the NWICA contracted Meal Preparation/Catering vendor to the eligible participant’s home. 11 Activities Not Allowed Activities not covered under allowable activities. Meals provided to individuals not eligible for Older American’s Act funding. Eligibility/Target Population In order to receive home delivered meals the following criteria must be met: An individual must be 60 years of age or older Must be homebound or Must be isolated. Registered congregate meal participants who request a home delivered meal (s) due to a short-term illness or health condition Unit of Service 1 delivered meal = 1 unit Service Authorization Services must be provided according to the Vendor Authorization provided by the NWICA Case Manager. Documentation Requirements Client signature sheet and/or route log signed by driver. *Note: Medicaid requires client signatures. Monthly invoice must include: Signature information as described above Cash Match/Project Income and In-Kind supporting documentation Nutritional education, health information and surveys must be part of the home delivered meal program. Applicable Funding Sources Older American’s Act TIII, NSIP, CHOICE, Waiver 12 Home Health Aide Services (HOHE) Applicable Rules and Regulations Section 4012 of the Indiana Division on Aging Operations Manual; 410 IAC 7.9 Home Health Agencies – Definitions; 455 IAC 1 & 2 – Home and Community Based Services rule; IC 16-27-1 Licensure of Home Health Agencies; Section 10042 of the Indiana FSSA CHOICE Manual; and NWICA all define service as follows: Service Description Home health aide services include all health monitoring activities performed in the home, supervision of medication, and dressing changes under the supervision of a nurse as required by federal Home Health Agency standards. Allowable Activities Allowable Services include: Assistance with personal hygiene and grooming under the following circumstances Need for skilled skin care Need for skilled transfer Need for skilled assistance with dressing Consumer has poor balance, is in a weakened state and/or has a high risk for falls Consumer is at high risk for skin breakdown Ambulation Assistance under the following circumstances: Skilled transfers are required with the ambulation Mechanical lift device is used Consumer has poor balance, is in a weakened state and/or has a high risk for falls Consumer is still being trained in initial use of adaptive equipment Observation and reporting to nurse is needed when Consumer has a new cast Skilled skin care is needed Transferring Assistance under the following circumstances: Consumer unable to assist with transfer Mechanical lift device is used Consumer has poor balance, is in a weakened state and/or has a high risk for falls Consumer still being trained in initial use of adaptive equipment Need for skilled skin care May include use of a transfer belt or gait belt to assist, transfer from bed to chair (and back), use of a mechanical lift such as a Hoyer lift, transfer into and out of bathing areas (i.e. shower/tub) transferring onto and off the toilet and in and out of a motor vehicle. Assistance with positioning/turning as follows: Consumer is not able to identify to staff when his/her position needs to be changed Skilled skin care is required with position change Consumer has contractures requiring special positioning Consumer has communicable disease or draining wounds Therapeutic bed (Clinitron, Stryker, Circle) is used Consumer has casts or traction equipment Consumer is unconscious or dying Consumer is at risk for aspiration Assistance with range of motion as follows: 13 When prescribed by a nurse or other health care professional such as a physician or therapist. May include passive range-of-motion, or working with simple traction, fractures, casts, dislocations, paralysis, contractures, unconscious Consumer or technology-dependent Consumer Other activities as allowed by the Home Health Agency in compliance with federal requirements Activities Not Allowed Services outside the scope of practice for a Home Health Aide are not allowable under home health aide services. Provider Requirements Provider must be licensed by the Indiana State Department of Health. To provide services under CHOICE funding, the provider must also be certified as a Medicaid Waiver provider. Unit of Service ¼ hour = 1 unit Service Authorization Services must be provided in accordance with the Vendor Authorization issued by the NWICA Case Manager. Documentation Requirements Documentation required by the Indiana State Department of Health Licensure Documentation compliant with the Indiana Health Coverage Programs Provider Bulletin BT200371, Documentation Standards for Home and Community-Based Services Waiver Programs NWICA monthly service progress report Funding Source(s) Funding sources include Title III, SSBG, and CHOICE. 14 Home Health Supplies and Assistive Devices (ATCH, ATCM, SUPP) Applicable Rules and Regulations Section 4001 of the Indiana Division on Aging Operations Manual; Section 10037 & 10053 of Indiana FSSA CHOICE Manual; Section 7 of the Indiana Division of Aging Waiver Provider Manual; and NWICA all define services as: Service Description NWICA defines Home Health Supplies as supplies not covered under other funding sources such as private insurance, Medicare, or Medicaid. Supplies may include but are not limited to incontinence supplies, nutritional supplements, skin care ointment, medical gloves, etc. NWICA defines Assistive Device as an item which is used to increase, maintain, or improve functional capabilities. Such devices are intended to replace functional abilities lost to the individual because of his or her disability and must be used in performing Activities of Daily Living (ADL) or Instrumental Activities of Daily Living (IADL). For all individuals whose independence can be enhanced through the use of an Assistive Device, the following types of items may be approved. Adaptive eating utensils Adaptive kitchen utensils Adaptive telephones with large numbers Bath/shower chair: with or without transfer bench Dressing aids Gait belt Grab bars Hand held shower unit Medication reminder units Raised toilet seat Reacher/grabber Shampoo tray for bed bath Walker basket Walker wheels Wander devices: for individuals with dementia only Activities Not Allowed Devices that are covered by Medicare, Medicaid, or private insurance will not be approved. Funds may not be used to purchase assistive devices that are not of direct benefit to the individual. Funds cannot be used to purchase, repair, or otherwise pay for dentures, hearing aids or glasses. NWICA will not approve the following items: Appliances (non-adapted) Automobiles Batteries Blood pressure monitors Clothing 15 Computer/computer software Dentures/Dental Care Eating utensils (non-adapted) Exercise equipment Eye glasses Fans Furniture (non-adapted) Golf carts Health club memberships Hearing aids Heating pads Home maintenance/repairs/remodeling/new construction Hospital bed Kitchen utensils (non-adapted) Massage devices Mattresses Medical supplies Medicare and Medicaid covered items Medications (prescribed or over-the-counter) Modified secondary home entrance/exit Muscle stimulators Orthotics (prosthetic shoes, lifts, braces) Oxygen equipment Pads/Pillows/Cushions Physical therapy devices Ramp enclosure Repairs/modifications to items purchased by Medicare, Medicaid or private insurance Scales Scooter/carts for outdoor transportation Service/support animals Smoke alarms Support hose/stockings Swimming pool accessories Therapies Toothbrushes (non-adapted) A second wheelchair as a reserve/backup Provider Requirements Provider must be licensed by the Indiana Board of Pharmacy. To provide services under CHOICE funding, the provider must also be certified as a Medicaid Waiver provider. Unit of Service 1 supply or device = 1 unit. 16 Service Authorization Services must be provided in accordance with the Vendor Authorization issued by the NWICA Case Manager. Home Health Supplies and Assistive Devices must be approved by the Northwest Indiana Community Action (NWICA) and comply with all applicable medical and manufacturing standards. Items that do not appear on the above “approved” and “not approved” lists may be considered by NWICA. Determinations will be made based on the individual’s unique circumstances as they apply to the current definitions, policies and procedures. A denial letter must accompany requests for items generally covered by Medicare, Medicaid, or private insurance Documentation Requirements Documentation required by the Indiana Board of Pharmacy Licensure Documentation compliant with the Indiana Health Coverage Programs Provider Bulletin BT200371, Documentation Standards for Home and Community-Based Services Waiver Programs NWICA monthly service progress report The delivery date and type of any supply, and/or The installation/delivery date of any assistive device, and The maintenance date of any assistive device Funding Source(s) Funding sources include Title III, SSBG, and CHOICE 17 Home Repair/Maintenance Services (HCP) Applicable Rules and Regulations Section 4014 of the Indiana Division on Aging Operations Manual; and Section 10045 of the Indiana FSSA CHOICE Manual all define service as: Service Description Home Repair/Maintenance and minor home repair services are planned and monitored maintenance and minor repair activities essential to health and safety. Home Repair may be made to an owner or renter occupied single-family dwelling. The intent of the service shall be to make the dwelling habitable and shall not be done to improve the appearance of the property. Service activities shall be performed in order of priority. Repairs made to correct life threatening conditions and/or conditions that pose a health or safety hazard to the older adult or person with disabilities will be top priority. Allowable Activities The Home Repair and Maintenance Services program dollars shall be used only for repairs that directly correct and/or prevent health and/or safety hazards. Home Repair/Maintenance and minor home repair activities may include: plumbing, heating, and electrical malfunction repair or replacement; storm door, window, and screen repairs; gutter and roof patching; heavy cleaning; and broken step repairs; Health and safety alterations may include installation of: handrails; ramps; deadbolts; smoke detectors; locks; and window bar Ground maintenance services may include limited lawn moving, snow removal, and minimal yard cleanup to assure safe entrance and departure from the premises. Time spent in assessing the job, obtaining the supplies, performing planned activities, and cleaning up. Travel time between work sites. Activities Not Allowed Service providers will not be paid for such activities as: Billing for more than the actual time of each staff person delivering services, even when more than one client is simultaneously benefiting from the service; and Billing for home repair services which cannot be documented as avoiding a clear and present health/safety hazard. Services may not be provided for aesthetic purposes only. Provider Requirements 18 To provide services under CHOICE funding, the provider must also be certified as a Medicaid Waiver provider. If the Indiana State Department of Health implements a Personal Service Agency Licensure, all providers will need to be in compliance with these licensing requirements. Unit of Service ¼ hour = 1 unit Service Authorization Services must be provided in accordance with the Vendor Authorization issued by the NWICA Case Manager. Documentation Requirements Documentation compliant with the Indiana Health Coverage Programs Provider Bulletin BT200371, Documentation Standards for Home and Community-Based Services Waiver Programs NWICA monthly service progress report Funding Source(s) Funding sources include Title III, CHOICE, SSBG, Older Hoosier Funds, and local funds. 19 Homemaker Services (HMK) Applicable Rules and Regulations 455 IAC 1 & 2 – Home and Community Based Services Rule; IC 16-27-4 Licensure of Personal Service Agencies; Section 4013 of the Indiana Division on Aging Operations Manual; Section 7 of the Indiana Division of Aging Waiver Provider Manual; Section 10044 of the Indiana FSSA CHOICE Manual; and NWICA all define service as: Service Description Homemaker services offer direct and practical assistance with household tasks and related activities. Homemaker services assist the older adult person with disabilities who has experienced a loss in the ability to perform the instrumental activities of daily living to remain in a clean, safe, healthy home environment. Homemaker services are provided when the client is unable to meet these needs or when an informal caregiver is unable to meet these needs for the client. Allowable Activities Homemaker services provided for housekeeping tasks which may include: dusting and straightening furniture cleaning floors and rugs by wet/dry mop and vacuum sweeping; cleaning the kitchen, including washing dishes, pots, and pans; cleaning the outside of appliances and counters and cupboards; cleaning ovens and defrosting and cleaning refrigerators; maintaining a clean bathroom, including cleaning the tub, shower, sink, toilet bowl, and medicine cabinet, emptying and cleaning commode chair/urinal; laundering clothes in the home or Laundromat, including washing, drying, folding, putting away, ironing, and basic mending repair; changing linen and making beds; washing insides of windows; removing trash from the home; choosing appropriate procedures, equipment, and supplies; improvising when there are limited supplies, keeping equipment clean and in its proper place; and Homemaker services may provide assistance with meals/nutrition that may include: shopping, including putting food away; and making meals, including special diets under the supervision of a registered dietitian or health professional. Homemaker services may include completing the following essential chores or errands: grocery shopping; household supply shopping; prescription pick up; food stamp pick up; and assistance with correspondence Homemakers do not transport clients. Errand related tasks are completed on behalf of the client. 20 Activities Not Allowed Services requiring hands-on personal care or any activity that must be provided by a licensed health professional care service are not allowed. Homemaker services that benefit household members only. Provider Requirements Pursuant to state law, NWICA requires its providers of Homemaker services to be licensed either as a Home Health Agency or a Personal Service Agency. To provide services under CHOICE funding, the provider must also be certified as a Medicaid Waiver provider. Unit of Service ¼ hour = 1 unit Service Authorization Services must be provided in accordance with the Vendor Authorization issued by the NWICA Case Manager. Documentation Requirements Documentation required by the Indiana State Department of Health Personal Service Agency Licensure. Documentation compliant with the Indiana Health Coverage Programs Provider Bulletin BT200371, Documentation Standards for Home and Community-Based Services Waiver Programs NWICA monthly service progress report. Funding Source(s) Funding sources include Title III, SSBG, CHOICE, Older Hoosier Funds, and other local funds. 21 Personal Emergency Response System (PRSI, PRSM) Applicable Rules and Regulations 455 IAC 1 & 2 – Home and Community Based Services rule; Section 4001 of the Indiana Division on Aging Operations Manual; Section 7 of the Indiana Division of Aging Waiver Provider Manual; Section 10050 of the Indiana FSSA CHOICE Manual; and NWICA define the service as: Service Description Personal Emergency Response System (PERS) is an electronic device that enables individuals at high risk of institutionalization to secure help in an emergency. The system is connected to the person's phone and programmed to signal a response center once a "help" button is activated. Professionally trained PERS staff assesses the nature of the emergency and obtains appropriate help for the individual as necessary. Allowable Activities PERS services shall include the following approved, reimbursable activities when PERS is identified on the individual’s Service Plan: Installation and maintenance of PERS equipment in the participant’s home by appropriately trained staff. (PRSI; only one unit of PRSI may be authorized and billed for each authorized equipment type) PERS equipment which provides the participant with the ability to reliably activate an immediate emergency signal to the surveillance/response center. PERS equipment which has an uninterruptible power source. PERS equipment which is appropriate to the individual’s cognitive, physical, and medical condition. Information and training to the participant (and caregivers, as necessary) regarding the use of the PERS equipment. Continuous surveillance of signaling equipment for activated signals by the surveillance/response center 24 hours per day, 365 days per year. (PRSM; one unit per month of PRSM may be authorized and billed for monitoring of signaling equipment.) Scheduled testing of all in-home equipment at least every 30 days to ensure that equipment is functional. A telephone line monitor that ensures that telephone connections are maintained between the PERS equipment in the home and the surveillance/response center. A direct response to the participant within 60 seconds by surveillance/response center professional staff who has been trained in emergency response and who use an established response protocol over the PERS equipment and/or the telephone. An emergency telephone communication from the surveillance/response center in accordance with an established protocol to a local response network including friends, neighbors, police, fire, and/or ambulance, depending on the nature of the emergency. A response by professional staff who has been trained in emergency response and who use response protocols for each participant. Detailed documentation of responses to all activated signals. 22 Detailed technical and operations manuals which describe PERS elements, including PERS equipment specifications, installation, functioning, and testing, staff training requirements, emergency response protocols, and record keeping and reporting procedures. Service Limitations PERS services are limited to those individuals who live alone, or who are alone for significant parts of the day, who are alone for any period of time and have a written plan for increasing the duration of time spent alone as a means of gaining a greater level of independence, or who have no regular caregiver for extended periods of time, and who would otherwise require extensive routine supervision. PERS services are limited to individuals who are able to effectively utilize PERS equipment. Provider Requirements PERS providers comply with the following: All legal requirements set by the Federal Communication Commission Equipment must meet the Underwriters Laboratories, Inc. (UL) standards for home health care signaling equipment To provide services under CHOICE funding, the provider must also be certified as a Medicaid Waiver provider. Unit of Service PRSI ( Personal Emergency Response System Install) – one installation = one unit PRSM (Personal Emergency Response System Monitoring) – one unit of monitoring may be billed each month equipment is authorized by NWICA to be in the home Service Authorization Services must be provided in accordance with the Vendor Authorization issued by the NWICA Case Manager. Documentation Requirements It is required that the agency maintain a record that documents the date that the service is started, the dates that it is provided, and the date it is terminated. The provider shall maintain documentation of routine testing of equipment and shall present such documentation upon request by NWICA. The provider shall maintain detailed documentation of responses to all activated signals Documentation compliant with the Indiana Health Coverage Programs Provider Bulletin BT200371, Documentation Standards for Home and Community-Based Services Waiver Programs NWICA monthly service progress report Funding Source(s) Funding sources include SSBG, CHOICE, Older Hoosier Funds, Title III, and Program income. 23 Respite (RNUR, RHHA, RATT, RHMK) Applicable Rules and Regulations 455 IAC 1 & 2 – Home and Community Based Services rule; Section 4025 of the Indiana Division on Aging Operations Manual; Section 10052 of the Indiana FSSA CHOICE manual all define services as: Service Description Respite care services are those services provided temporarily or periodically to older adults or persons with disabilities to relieve the usual unpaid caregiver. Service may be provided in the client’s or caregiver’s home or in a nursing facility or other location, depending on the funding source involved and individual program requirements. Respite care is provided to assist a family in keeping an older adult or person with disabilities in the home. Allowable Activities Respite care services may provide: homemaker services; attendant care; home health aide services; skilled nursing services; or services provided in a facility. Activities Not Allowed services that duplicate any other service provided under the client’s plan of care. provision of services to an older adult or person with disabilities who is without a usual caregiver. Provider Requirements To provide services under CHOICE funding, the provider must also be certified as a Medicaid Waiver provider. Providers providing skilled services must be licensed by the Indiana State Department of Health. In 2006, the Indiana State Department of Health will be implementing a Personal Service Agency Licensure. All providers will need to be in compliance with these licensing requirements. Unit of Service 1/4 hour of allowable activity = 1 unit of service Service Authorization The NWICA case manager will provide the provider a vendor authorization specifying the client and service information. Documentation Requirements Documentation must include: The reason for the respite The location where the service was rendered 24 The type of respite provided Provider ensures the absence of the usual caregiver while respite services are being provided. Documentation required by the Indiana State Department of Health Personal Service Agency Licensure and/or Indiana State Department of Health Personal Service Agency Licensure. Documentation compliant with the Indiana Health Coverage Programs Provider Bulletin BT200371, Documentation Standards for Home and Community-Based Services Waiver Programs. NWICA monthly service progress report. Funding Source(s) Funding for respite care services may be available through SSBG, Title III, CHOICE, program income, and local funds. 25 Skilled Nursing (SKNU) Applicable Rules and Regulations Section 4012 of the Indiana Division on Aging Operations Manual; 410 IAC 7.9 Home Health Agencies – Definitions; 455 IAC 1 & 2 – Home and Community Based Services rule; IC 16-27-1 Licensure of Home Health Agencies; all define service as: Service Description Service provided by a Registered Nurse (RN) or Licensed Practical Nurse (LPN) to provide services such as blood draws, wound care, catheter changes, diabetic education, IV therapy, colostomy care, and medication set-up. Allowable Activities Activities allowable for licensed skilled nurses to provide including but not limited to the activities listed under service description. Activities Not Allowed Activities not required to be performed by an LPN or RN Activities which are allowable under other funding sources Provider Requirements A licensed home health agency employing licensed nursing staff Unit of Service ¼ hour = 1 unit Service Authorization Services must be provided in accordance with the Vendor Authorization issued by the NWICA Case Manager. Documentation Requirements Documentation required by the Indiana State Department of Health Licensure Documentation compliant with the Indiana Health Coverage Programs Provider Bulletin BT200371, Documentation Standards for Home and Community-Based Services Waiver Programs NWICA monthly service progress report. Funding Source Funding sources include CHOICE, TIII, and SSBG. 26 Transportation Services (TRAN) Applicable Rules and Regulations Section 4029 of the Indiana Division on Aging Operations Manual and Section 10055 of the Indiana FSSA CHOICE Manual define service as: Service Description Transportation Services ensure older adults and persons with disabilities (particularly those persons living in rural areas) access to services that help them remain independent. All Transportation Services shall comply with Federal Transit Authority (FTA), Federal Department of Transportation (DOT) and Indiana Department of Transportation (INDOT) rules and regulations as well as applicable codes, including the Americans with Disabilities Act (ADA) regulations for public transit. Allowable Activities A one-way trip for the purpose of healthcare, social activities, shopping, etc. for the purpose of assisting individuals to access services and remain independent. When demand exceeds services available, the provider shall prioritize the types of transportation that will be provided. Prioritization would be as follows: Trips for medical reasons Trips for nutritional purposes Shopping Socialization purposes Activities Not Allowed Activities not listed above Provider Requirements All providers must properly maintain vehicles which include: A standard list of items checked each day the vehicle in service is used. Procedures in place that require the vehicle be out of service until such corrections are made of specific items that would include: Brakes Fuel Emergency Equipment Seat belts All vehicles shall have an inspection every 6 months or as recommended by the vehicle manufacturer. Drivers providing service under the agreement must possess at least a Class C CDL with a passenger endorsement. If equipment dictates, drivers must possess the appropriate license to operate the vendor’s vehicles. In addition to standard insurance coverage, transportation vendors must have Ambulatory coverage in a minimum amount of $1.5 million, Wheelchair Accessible coverage in a minimum amount of $1.5 million and General Vehicle Liability in a minimum amount of $1 million. Policies must list NWICA as an additional insured. Vendor is responsible for submitting updated Certificates of Insurance as applicable. Unit of Service 27 1 one-way trip = 1 unit Service Authorization For transportation services provided with Title III funds, no NWICA service authorization is required for services provided by contracted providers. Transportation providers must ensure eligibility requirements (60 years of age or older) are met. For transportation services provided through CHOICE and/or SSBG, services must be provided in accordance with the Vendor Authorization issued by the NWICA Case Manager. Documentation Requirements Client demographic information and trip information entered into INsite/NAPIS on a monthly basis. Vehicle inspection reports and client intake forms must be available for review at the provider’s office. Funding Source(s) Funding sources may include Title III, CHOICE and SSBG depending on provider qualifications and contractual requirements. 28 Standard Operating Procedures for HCBS Provider Qualifications In order to become an approved provider of HCBS, an entity shall do the following: Under CHOICE a Service Provider must be Medicaid Waiver Certified; and meet the current minimum service provider requirements as specified; and Be a provider of an approved nursing facility level of care Medicaid waiver service or a home and community based service listed in 455 IAC 2-5-1. Appendix A Show proof of licensure or certification from the state of Indiana, if a license is required. Certify that, if approved, the entity will provide HCBS using only personnel who meet the qualifications defined in this manual. Retain, and have readily available, a copy of the most current executed signed provider agreement appropriate to the funding program and the provided service. Assure and document compliance with the executed provider agreement or contract and this rule. In order to maintain approved status as a provider of HCBS, an entity must do the following: Continue to maintain minimum standards set out in this manual. Successfully complete the renewal process, as determined by NWICA. Receive written notice of renewal to be maintained by the provider. Orientation and Training Service providers must maintain a written plan for orienting new staff. New program staff must receive orientation and training which includes at a minimum: introduction to the program, Vendor policies and procedures, maintenance of records and files (as appropriate), organizational standards and expectations for ethical behavior, confidentiality and, as appropriate, HIPAA compliance, and emergency procedures Direct care staff will also receive orientation and training including first aid, CPR, universal precautions, and the aging process. Issues addressed under the aging process may include, though are not limited to: cultural diversity dementia cognitive impairment mental illness abuse and exploitation communicable and infectious diseases communication techniques 29 food handling and sanitation Service providers must also maintain a written annual training plan which includes at least the following: Dates of training Topics of training Presenters Goals to be accomplished Staff required to attend Evidence of implementation of orientation and training plans must be available for review at the service provider’s offices. Personnel Policies and Procedures Employees must have access to service provider personnel policies and procedures. Personnel policies and procedures must include at least the following: Job Descriptions Service providers maintain written job descriptions for each position in the organization. Job descriptions include minimum qualifications for the position and major duties required of the position. Hiring procedures Service providers have a written procedure for conducting reference, employment and criminal background checks on each prospective employee or agent. Written hiring procedures prohibit employing or contracting with a person convicted of crimes including at least the following: A sex crime (IC 35-42-4) Exploitation of an endangered adult (IC 35-46-1-12) Abuse or neglect of a child (IC 35-42-2-1) Failure to report battery, neglect, or exploitation of an endangered adult or dependent (IC 35-46-1-13) Theft occurring within 10 years prior to the date of application for employment (IC 35-43-4; IC 16-27-25(a)(5) Murder (IC 35-42-1-1) Voluntary manslaughter (IC 35-42-1-3) Involuntary manslaughter (IC 35-42-1-4) Battery (IC 35-42-2) Service providers have a written procedure for conducting license verifications. The verifications include at least the following: Licensed professionals must be checked for findings through the Indiana Professional Licensing Agency. 30 All employees, regardless of their current status as a nurse’s aide or home health aide, must be checked for findings from the Indiana State Department of Health Nurse Aide Registry. Service providers can visit http://www.in.gov/services.htm to complete these searches online. Performance Evaluation Performance evaluations should be conducted with each employee at least annually. Procedures for performance evaluations should include a face to face meeting with the employee to discuss performance strengths and areas for improvement. Documentation of the annual performance evaluation should be maintained in the personnel file. Disciplinary Action/Performance Enhancement Each service provider has written policies and procedures regarding disciplinary action and/or performance enhancement. The policies and procedures list examples of infraction that will result in disciplinary action or performance enhancement actions. Examples include, but are not limited to, the following: Falsifying client records Breach of confidentiality Improper treatment of client Being under the influence of alcohol or illegal substance Stealing from client or vendor Excessive absenteeism Failure to report to work Availability of management staff Management staff or designated supervisory individuals are available during all hours of operation/service provision to consult with program staff, if necessary. Relatives as caregivers An individual who is a legally responsible relative of an eligible consumer (including a parent of a minor individual or a spouse) cannot provide services for that individual for compensation under the Agreement with NWICA except as otherwise stated in IC 12-10-10-9(b). Personnel Files Personnel files have documentation of the following: Employee/agent is at least 18 yrs old Direct care staff have current CPR certification Orientation/training documentation Reference checks Criminal background checks prior to service provision Current job description Current certification/licensing 31 Documentation that licensed professionals have been checked for findings through the Indiana Professional Licensing Agency AND that non-licensed employees have been checked for findings from the Indiana State Department of Health Nurse Aide Registry Proficiency testing Annual performance evaluations Current TB test or chest x-ray 32 Service Provision Receiving a Referral from NWICA Prospective consumers complete an initial screening to determine their level of need and their functional and financial eligibility for home and community based services under NWICA funding sources. If eligibility requirements are met, the consumer is referred to our Case Management department. Our Case Managers are trained and certified to assess each consumer’s situation and to assist the consumer in developing a Plan of Care designed to support the consumer’s independence and ability to remain in their home and community. The consumer and Case Manager develop a menu of services, and then the consumer receives a list of vendors who contract with NWICA to provide the desired services. Consumers choose their own vendors. They may make their selections by any process or criteria that they choose and the Case Manager is not permitted to influence that decision. Once the consumer has chosen their provider(s,) for services under our CHOICE, SSBG and TIII funding sources, the Case Manager prepares the Vendor Authorization. (See Sample on next page.) The Vendor Authorization indicates the approved services, dates and number of units. Services must be provided within the authorized dates and must not exceed the number of units as indicated. Units may not be moved from one month to another without written authorization from the Case Manager. When the Vendor Authorization is completed, the Case Manager sends a copy to each vendor selected by the consumer. For Aged and Disabled or Traumatic Brain Injury Medicaid Waiver Consumers, once the consumer has chosen their providers(s) for services under the Medicaid Waivers, the Case Manager prepares the CostComparison Budget (CCB). The CCB indicates the approved services, dates and number of units requested and is submitted to the state for approval. Once the CCB is approved at the state level, a Notice of Action is generated by the state and sent electronically to the AAA and all vendors with authorized services on the CCB. The vendor is able to open CCB notifications and Notices of Action simply by entering the last 4 digits of the consumer’s social security number which service providers should include in each client’s file. Vendors should not provide services to a consumer for whom they do not have a current Vendor Authorization or Notice of Action. Vendors who provide services without current authorizations run the risk of not receiving reimbursement for those services. Vendors should notify the consumer that their authorization to provide the services has ended and encourage the consumer to contact the case manager to discuss the situation. Any services provided other than as indicated on the Vendor Authorization or Notice of Action sent by the state will not be allowable; however, service providers have more frequent face to face contact with consumers than do Case Managers. If a service provider believes that services are not authorized appropriately, the provider should contact the Case Manager to discuss the situation further. NWICA appreciates this feedback from providers and believes that it strengthens our partnership as we mutually care for consumers. 33 34 35 Service Provider Policies Regarding Service Provision Vendors maintain written policies and procedures regarding service provision which include at least the following: Rights of service recipients Each service provider maintains a written statement of consumer rights. This statement is provided to consumers at the start of care and is reviewed with new employees at orientation. The statement includes at least the following rights. Receive Information. Each Participant has the right to receive information about the service provider, the provider’s policies and procedures, services, staff, and the consumer’s rights and responsibilities. Dignity and Privacy. Each consumer is guaranteed the right to be treated with respect and with due consideration for his or her dignity and privacy. Receive information on available service options. Each consumer is guaranteed the right to receive information on available service options and alternatives, presented in a manner appropriate to the consumer’s condition and ability to understand. Participate in decisions. Each consumer is guaranteed the right to participate in decisions regarding his or her health care, including the right to refuse treatment. Free from restraint or seclusion. Each consumer is guaranteed the right to be free of any form of restraint or seclusion used as a means of coercion, discipline, convenience or retaliation. Copy of records. Each consumer is guaranteed the right to request and receive a copy of his or her records, and to be informed of the procedure for requesting records. Free exercise of rights. Each consumer is free to exercise his or her rights, and that the exercise of those rights does not adversely affect the way the consumer is treated by the service provider. Freedom to Change Provider. Service providers shall not impose any limitation on the consumer’s freedom to change providers. Abuse, Neglect and Exploitation In Indiana, any person who has reason to believe that a consumer is a victim of abuse, neglect or exploitation is obligated to make a report to Child Protective Services (CPS), Adult Protective Services (APS) or to the police. "Reason to believe" means that the evidence available to that person, if presented to other individuals of similar background and training, would make those individuals think that the consumer has been abused or neglected. 36 The law (I.C. 12-10-3) requires all individuals with reason to believe a disabled adult is being abused, neglected, or exploited to make a report to Adult Protective Services (APS) and/or local law enforcement. Failure to make a report is considered a Class B misdemeanor. In Indiana a Class "B" misdemeanor conviction carries a penalty of imprisonment for a fixed term of up to one hundred eighty (180) days and a fine up to $1000.00. Service providers will also inform the case manager any time a report is made regarding the abuse, neglect or exploitation of a consumer of services under the agreement; however, it is still the service provider’s obligation to report to the appropriate authorities. Informing the case manager does not relieve the service provider of their duty to report. If you have reason to believe an individual is being abused, neglected or their safety is in jeopardy in anyway, you are required to report to proper authorities immediately. How to Make a Report to Adult Protective Services An APS report should be filed within the county where the endangered person lives as soon as possible upon indication that there may be a problem. When making a report to APS have as much of the following information as possible: The endangered adult’s name, address, phone number, age, and physical or mental capacity Alleged perpetrator’s name, address, phone number, and relationship to the endangered adult Nature and extent of the abuse, neglect, or exploitation Any additional information that may be helpful REMEMBER YOU DO NOT NEED TO DETERMINE IF THE ABUSE OR NEGLECT IS OCCURING BUT YOU ARE RESPONSIBLE AS A CITIZEN OF THE STATE OF INDIANA TO REPORT IT. ADULT PROTECTIVE SERVICES CONTACT INFORMATION: Lake County Referrals (219) 755-3863 Porter County Referrals (219) 326-6808 ext. 505 Jasper, Newton, Pulaski, and Starke County Referrals (219) 326-6808 ext. 420 Your local law enforcement agency can also be contacted. Wellness Checks by Local Law Enforcement If an emergency requires a wellness check, the consumer’s local police department should be contacted immediately and asked to conduct a “Wellness Check”. You will need the client’s name and address and any available contact information for caregivers or family members. Police will generally notify the requestor after visiting the individual. 37 Communicable/infectious disease An infectious disease is one in which an organism has invaded the body and has the potential of spreading into multiple systems. A contagious disease is one in which an organism can spread from one individual to another. Service providers will establish policies and procedures regarding infectious and contagious diseases for both employees and consumers. Discharge/Termination process Each service provider must establish a written service procedure which includes formal written notification of the termination of services and documentation in client files. The written notification must state the reason for the termination, the effective date, and advise about the right to appeal. Reasons for termination may include, but are not limited to the following: the client’s decision to stop receiving services; reassessment which determines a client to be ineligible; improvements/changes in the client’s condition so they no longer are in need of services; permanent institutionalization of client in an acute care or long term care facility The service provider becomes unable to continue to serve the client. Service providers are required, under the agreement, to give thirty (30) days advance notice of any termination of services initiated by the provider. Notice shall be provided to the client/caregiver and to the NWICA Case Manager. If the consumer initiates the termination of services, written notice from the vendor shall be provided to the Case Manager within 10 days of termination by the consumer. Transfer of records upon change of provider Pursuant to 455 IAC 2-8-3, if an individual changes providers for a home and community based service, the original provider shall transfer copies of all records related to the individual to the new provider: within five (5) calendar days; and in compliance with HIPAA regulations See Appendix A for the complete text of 455 IAC 2, Indiana’s Home and Community Based Services Rule. 38 Incident Reporting All vendors are required to comply with the Indiana Division of Aging Incident Reporting Policy. All reportable incidents and unusual occurrences shall be reported to the Indiana Division of Aging in the manner prescribed. See Appendix B for the text of the Indiana Division of Aging Policy. Service providers will also inform the case manager any time an incident report is made regarding a consumer of services under the agreement; however, it is still the service provider’s obligation to report to the appropriate authorities. Informing the case manager does not relieve the service provider of their duty to report. Service Areas Each Service Provider indicated in the application for a contract the areas in which they were willing to provide services. The agreement was issued with this understanding. If, for any reason, a Service Provider needs to change the service areas designated in their proposal/contract, a written request should be submitted to Quality Assurance. Staffing Service Providers agree to provide sufficient staffing to commit to the service(s) and time period(s) authorized on the Vendor Authorization. Service Providers agree to provide backup for their own staff in the event that a scheduled worker is unable to fulfill their assignment. Backup staff must meet the qualifications for the service that is authorized. Service Providers are required to promptly notify the client and the client’s Case Manager if any schedule disruption occurs. Consistent schedule disruptions may result in probation or suspension of the agreement. Minimum Visit Times Any service provider desiring to establish a minimum visit length longer than 2 hours must obtain written permission from NWICA. Staffing with more than one staff person When the safety of a staff person is a concern, the option of staffing with two persons for half the authorized time may be requested. (For example: service authorized for 2 hours every week could be provided by 2 people at once for 1 hour every week.) Request must be made to and approved by the consumer’s Case Manager. Procedure: Service Provider submits written request to Case Manager, explaining the extenuating circumstances contributing to the concern for the staff person’s safety. The Case Manager will contact the consumer to discuss the concerns and the proposed plan for service. If approved, the Case Manager will send the Service Provider a Plan of Care noting that service by 2 staff members at the same time will be allowable. 39 Progress Reports The Service Provider is responsible to notify the case manager regarding any changes in the consumer’s status, including, but not limited to: missed service; service refusal; consumer request for service termination; hospitalization; change in physical; mental or emotional state; death; change in living arrangements; unresolved consumer complaints or grievances; any other significant issues regarding the consumer and/or services. In addition to ongoing communication with the Case Manager which is documented in the consumer’s file, Case Managers may periodically request a progress report from the vendor. The Case Manager will specify, at the time of the request, what type of information they are requesting. Documentation Service providers maintain, in the provider's office, documentation of all services provided to an individual. Documentation related to an individual shall be maintained by the provider per HIPAA guidelines. Service Providers shall maintain the documentation required by the following: The Service Definition applicable to the services the provider is providing to an individual. The professional standards applicable to the provider's profession. The individual's plan of care. Client Files Client files contain at least the following information: Authorization for services The individual’s full name Telephone numbers for emergency services that could be required for the individual Documentation of coordination/communication between vendor and NWICA including case notes, progress reports, and other correspondence Evidence of client notification when the regular worker or appointment was changed. Case manager notification when the services were not provided as authorized. Consent by the individual or the individual’s legal representative for emergency treatment for the individual, if applicable Documentation, including but not limited to the following information, of all services rendered for the last 45 days: Changes in the individual’s physical condition or mental status during the last 45 days Any unusual event such as vomiting, choking, falling, disorientation or confusion, behavioral problems, or seizures occurring during the last 45 days The response of the provider to the observed change or unusual event All documentation of medication administered for the last 45 days, where applicable Documentation should be kept chronologically and must include the following information for verification of service claim: Date of Service 40 Arrival & departure time Tasks performed Tasks performed are appropriate to job description/scope of service Signatures of client and service provider Additional Notes Regarding Documentation All documentation errors must be corrected using the following, universally accepted, method of drawing a line through the entry (in ink). Do not obliterate the word, but enter the correct information, and initial and date the change. Signatures are required to authenticate all documentation of services rendered. While it is recommended that a full signature be used for each entry, each individual entry must be signed, including, at a minimum, the first initial and last name. If the first initial and last name is used, a master signature file must be maintained. The file must contain a complete (first and last name) signature and the corresponding initial and last name to be used for documentation purposes. If a service requires a certain licensure level, for example health services provider in psychology (HSPP) for level 1 behavior management, that individual must include his or her title or credential in the signature. The payer source must be identified on each piece of documentation for verification of billing. This clarifies which payer source the documentation supports for billing activity, for example: waiver, CHOICE, SSBG, and Title III. Most clients should not be receiving AAA payer/funds home health service and waiver services concurrently on a consistent basis. AAA payer/funds may be used for spend-down; however, home health service hours should be used next, followed by waiver services and finally AAA payer/funds hours to meet any needs not covered by the other programs. For clients receiving more than one service, the hours should be broken out and clearly credited to the appropriate payer source. (Indiana Health Coverage Programs Document Standards for Home and Community-Based Waiver Programs BT200371 December 19, 2003) See Appendix C. Rounding of Units Each service definition specifies the unit by which a particular service is billed. Certain units of service are billed in 15-minute increments and some are billed in 60-minute increments. There is no procedure for billing a partial unit of service. If a partial unit is rendered, units should be accrued to the end of the current month of service. At the end of the current month of service, partial units can be rounded to the next whole unit when calculation units of service provided. When rounding of units occurs at the end of the billing month, the following guidelines can be used by providers: 15-minute units of service: Any partial unit of service eight minutes of more is rounded up to a 15-minute unit of service. Any partial unit of service seven minutes or less must not be rounded up and therefore should not be billed. 60-minute units of service: 41 Any partial unit of service 30 minutes or more is rounded up to a 60-minute unit of service. Any partial unit of service 29 minutes or less must not be rounded up and therefore should not be billed. Quality Assurance & Quality Improvement Provider has a QA/QI system in place. The QA/QI system is reviewed and updated annually. The QA/QI system includes at least the following: A method for measuring consumer satisfaction Documentation of efforts to improve provision of services based on customer satisfaction results An annual assessment of the appropriateness and effectiveness of each service provided to an individual A method for analyzing data regarding reportable incidents and services provided Documentation of efforts to improve service provision to reduce occurrences of reportable incidents Reimbursement to Providers The State of Indiana transitioned to a new statewide accounting system on September 16, 2009. Reimbursement from NWICA is dependent on the State of Indiana's payment terms, which are described below. As allowed in the administrative code, the State of Indiana issues payments 35 days after the invoice date. We wanted to explain to you how this impacts our reimbursement times. (Please note that this only applies to Area Agency on Aging funding sources including CHOICE, SSBG, and Title III. This will not impact reimbursement for Community Services Intake services.) Currently, providers are required to submit invoices to us by the 5th business day of each month following the month in which services were provided. Invoices submitted to us by the 5th are processed into our system by the 20th and we invoice the State by the 20th of each month. If they wait 35 days to reimburse us, we will receive payment from them around the 25th of the following month. NWICA then issues checks to our providers on Friday of the same week we receive funds. This means that providers have waited approximately 60 days to receive payment for services rendered. In an effort to alleviate this cash flow problem, NWICA offers the opportunity to submit invoices twice each month per the following guidelines. A provider may choose to bill for services provided between the 1st and the 15th of the month. These invoices would be due to NWICA on the 20th of the month. A second invoice could then be submitted for services provided between the 16th and the last day of the month. These invoices would be due to NWICA on the 5th business day of the following month (please refer to the Provider Invoice Schedule on page 44). Whether a provider chooses to bill once or twice a month, invoices for all services provided during that month must be received at NWICA by the 5th business day of the following month. There will be no exceptions. Here are some additional suggestions that will help ensure timely payment: 42 Submit your invoices to NWICA in a timely manner. Make sure your invoices are complete and have all necessary documentation. This will minimize delays caused by adding unnecessary steps to the process. Check invoice folders on SharePoint regularly/often to ensure that any corrections necessary are submitted as soon as possible. (For instructions/more information on NWICA’s electronic billing via SharePoint, see page 51 below). We also need to be sure that providers understand that, though the Division of Aging says they’ll reimburse us at 35 days, in some cases it is taking longer than this. 43 Provider Invoice Schedule Services Provided Invoice Due Jan 1‐ 15 Jan 1‐31 Feb 1‐15 Feb 1‐28 March 1‐15 March 1‐31 April 1‐15 April 1‐30 May 1‐15 May 1‐31 June 1‐15 June 1‐30 July 1‐15 July 1‐30 August 1‐15 August 1‐31 Sept 1‐15 Sept 1‐30 Oct 1‐15 Oct 1‐31 Nov 1‐15 Nov 1‐30 Dec 1‐15 Dec 1‐31 Jan 20 Feb 5 Feb 20 March 5 March 20 April 5 April 20 May 5 May 20 June 5 June 20 July 5 July 20 August 5 August 20 Sept 5 Sept 20 Oct 5 Oct 20 Nov 5 Nov 20 Dec 5 Dec 20 Jan 5 NWICA transmits to State Feb 5 Feb 20 March 5 March 20 April 5 April 20 May 5 May 20 June 5 June 20 July 5 July 20 August 5 August 20 Sept 5 Sept 20 Oct 5 Oct 20 Nov 5 Nov 20 Dec 5 Dec 20 Jan 5 Jan 20 Anticipated Reimbursement to NWICA* March 10 March 25 April 10 April 25 May 10 May 25 June 10 June 25 July 10 July 25 August 10 August 25 Sept 10 Sept 25 Oct 10 Oct 25 Nov 10 Nov 25 Dec 10 Dec 25 Jan 10 Jan 25 Feb 10 Feb 25 No invoices will be processed after Feb – 5th bus. day March - 5th bus. day April – 5th bus. day May – 5th bus. day June – 5th bus. day July – 5th bus. day Aug – 5th bus. day Sept – 5th bus. day Oct – 5th bus. day Nov – 5th bus. day Dec – 5th bus. day Jan – 5th bus. day 44 HCBS Forms Invoices CHOICE SSBG Title III E – Family Caregiver Title III B – In-Home Services Title III B – Transportation 45 CHOICE Invoice 46 SSBG Invoice 47 Title IIIE Family Caregiver Invoice 48 Title IIIB In-Home Services Invoice 49 Transportation Invoice 50 HCBS Billing Invoices are due to NWICA by the 5th calendar day after the close of the calendar month in which services were delivered. For example, if services are provided to a consumer in June, the invoice is due to NWICA by July 5th. Invoices received after the 5th will not be processed. There will be no exceptions. Billing documents are submitted electronically to NWICA via SharePoint extranet system only (See below). Upon receipt of signed service agreement, NWICA facilitates SharePoint remote access and training for all vendors. Incorrect invoices will be returned to the service provider. Invoices returned for correction may be resubmitted. Incorrect invoices will be uploaded by NWICA to a designated file folder location on SharePoint. Returned invoices will include comments explaining any necessary correction(s). Resubmission of corrected invoices must occur before NWICA prepares claims each month – no later than the 15th calendar date of the month. Providers are expected to check their SharePoint folders frequently during invoice processing to ensure corrections are processed and submitted in a timely matter. Questions regarding returned invoices should be directed to NWICA’s Grants Management Accountant. Complete Monthly Invoice as follows: Complete Provider name, address and phone number. Complete Consumer name, address, phone number and social security number. Enter the Care Plan period from the current Vendor Authorization. Enter the current Case Manager’s name. Enter the Service Delivery Dates, i.e. May 1 – May 31, 2014. Enter the total number of units of service provided to the consumer during the service delivery period in the appropriate row. Multiply the units by the unit rate and enter the amount in the Total Claim column. Sign and date the invoice. Complete SharePoint Billing Procedures as trained (See below) Invoicing Via SharePoint All providers will be contacted by NWICA IT Staff to have training coordinated for NWICA’s electronic invoicing system. This individualized training will take the vendor’s software and hardware into account and should suffice in enabling providers to complete invoicing on an ongoing basis. Should any problems arise with this process post-training, a step-by-step guide is provided below that may assist with troubleshooting. If systematic issues with invoicing cannot be resolved utilizing this tool, the appropriate provider representative should contact NWICA IT staff to see about resolving the issue. Please note: NWICA IT staff will provide support related to the function of our applications but they cannot provide support for providers equipment. 51 Instructions for Converting Invoice Documents for SharePoint Uploading Separate all invoices to be scanned in by Funding Source. Scan them as organized in .PDF format to office computer. Open Invoice Document, click on File and select “PRINT” in the Windows Drop-down Menu. In the PRINT SET UP screen, click the drop-down menu (top-center of the PRINT SET UP screen) and select MICROSOFT OFFICE DOCUMENT IMAGE WRITER. Next to it click on Advanced and check “Print to File” option 52 at the bottom the selection. Click “OK” then click “Print” You will now be prompted to save the invoice (based on action taken in Step 3 above). When saving, be sure to add the “.tiff” extension to the name of the file (example: “OctoberInvoice.tiff”). Locate the newly created .tiff document on your computer, and upload to SharePoint. (See posted SharePoint instructions for more info on how to do SharePoint uploading) 53 Appendix A 455 IAC 2: Home & Community Based Services Rule (460 Code now relocated to 455 IAC) 54 55 56 57 58 59 60 61 62 63 64 65 66 67 68 69 70 71 72 73 74 75 76 77 78 79 80 Appendix B: Indiana Division of Aging Incident Reporting Policy INCIDENT REPORTING POLICY FOR THE DIVISION OF AGING DOCUMENT CONTROL Document Information Document Name: Agency/Division: Incident Reporting Policy Division of Aging Document Author: Date: REVISION HISTORY Version Date Changes 0.1 01-10-07 Creation 1.0 02-09-07 Added Document Control and Signature Sections Added Header and Footer 2.0 03-16-07 Revision Signatures Position/Title Signature Date Author (required) Sponsor (required) Stakeholder (required) 81 POLICY/PURPOSE STATEMENT It is the policy of the Indiana Division of Aging (DA) to ensure the health and safety of all individuals receiving services through the DA. This policy is established to identify and address both immediate and potential risks to the health and safety of individuals receiving services as specified in 455 IAC 2. This policy addresses incidents (reportable unusual occurrences). II. STANDARDS The DA ensures implementation of necessary safeguards to protect the health, safety and welfare of individuals. Anyone with knowledge of an incident that effects, or potentially effects, the individual’s health and safety shall submit an incident report through the DDRS/DA Incident Reporting system An initial report regarding an incident, allegation, or suspicion of abuse, neglect, or exploitation shall be submitted within twenty-four (24) hours of the incident or having knowledge of the incident. Providers of home and community-based services are required to submit an incident report for reportable unusual occurrences within forty-eight (48) hours of the time of the incident or becoming aware of the incident. Any staff suspected, alleged, or involved in incidents of abuse, neglect, or exploitation of an individual will be immediately suspended from duty pending investigation by the provider. DEFINITIONS ”Adult Protective Service” (APS) means the program established under IC 12-10-3. ”Aging staff” means any individual employed by the Division of Aging, or its designee. ”Case manager” means the certified and approved individual chosen by the individual and/or family to coordinate the individual’s service. ”Child Protective Services” (CPS) refers to child protection services established under IC 31-33. ”Day”, as used in this policy, refers to a calendar day The Division of Aging (DA) is the entity established in IC 12-10-1-2 to assist the constantly increasing number of aged in: (1) maintaining self-sufficiency and personal well-being with the dignity to which the years of labor entitle the person; and (2) realizing the aged person's maximum potential as a creative and productive individual. “Direct care staff” means a person or an agent or employee of a provider entity who provides hands-on services to an individual while providing any of the following services including, but not limited to: respite, attendant care, adult foster care, adult day services, assisted living, congregate care, supported employment, structured day program, residential based habilitation, transportation, health care coordination, occupational therapy, physical therapy, speech therapy, or behavior management. 82 “Division of Aging staff” means any individual employed by the Indiana Family and Social Services Administration Division of Aging. “Home and community-based services” or “HCBS” means supportive services provided within the limit of available funding to an eligible individual and includes, but is not limited to, the following: homemaker services, attendant care services under IC 16-18-2-28.5, respite care services and other support services for primary or family caregivers, adult day services, home health services and supplies, home delivered meals, transportation and self-directed attendant care services provided by a registered personal services attendant under the applicable statute to individuals in need of self-directed in-home care.. “Incident” means, for the purposes of this policy, a single episode (event) of a reportable unusual occurrence. An incident involves a situation in which an individual or individuals have experienced or are the subject of a reportable unusual occurrence. Multiple occurrences related to the same type of issue are considered separate incidents. A separate incident report shall be filed at the time each episode occurs. “Individual” means a person who has been determined eligible for services by the DA. If the term is used in the context indicating that the individual is to receive information, the term also includes the individual’s legal representative. “Legal representative” means any of the following: (1) A guardian. (2) A health care representative acting under IC 16-36-1. (3) An attorney in fact for health care appointed under IC 30-5-5-16. (4) An attorney in fact appointed under IC 30-5-5 who does not hold health care powers. (5) The personal representative of the estate of a resident of a long term facility or client of home care services as set forth in IC 12-10-13-3.3. “Provider” or “service provider” means an entity approved by the DA to provide an individual with agreed upon HCBS. “Reportable unusual occurrence” includes, but is not limited to, the following: Alleged, suspected, or actual abuse, neglect, or exploitation of an individual. Alleged, suspected, or actual assault or abuse by an individual. The death of an individual A residence that compromises the health and safety of an individual due to any of the following: A significant interruption of a major utility. An environmental, structural, or other significant problem. 83 Environmental or structural problems associated with a dwelling where individuals reside that compromise the health and safety of the individuals. A residential fire resulting in any of the following: Relocation. Personal injury. Property loss. Suspected or observed criminal activity by: a staff member, employee, or agent of a provider; a family member of an individual receiving services; or the individual receiving services; when the care of the individual is impacted or potentially impacted. Injuries of unknown origin. Suicidal ideation or a suicide attempt that had the potential to cause physical harm, injury, or death. A major disturbance or threat to public safety created in the community by the individual. The threat can be: toward anyone, including staff; and in an internal setting; and need not be outside the individual’s residence. Admission of an individual to a nursing facility, excluding respite stays. A significant injury to an individual, including, but not limited to, the following: A fracture. A burn greater than first degree. Choking that requires intervention. Contusions or lacerations. An injury that occurs while an individual is restrained. Police involvement when there is an arrest. A missing person. Inadequate staff support for an individual, including inadequate supervision, with the potential for endangering the health or welfare of the individual. “Sentinel Event” means an unexpected occurrence involving serious physical or psychological injury or the risk thereof. Serious injury specifically includes a loss of limb or function. The phrase "or risk thereof" includes any process variation for which a recurrence would carry a significant chance of a serious outcome. A distinction is made between an adverse outcome that is related to the natural course of an individual's illness or diagnoses or major loss of function, or risk thereof, that is associated with the treatment/supports, or lack of treatment/supports, for that condition or diagnosis. The following are considered Sentinel Events even if the outcome was not major permanent loss of function: Suspected or actual abuse, neglect or exploitation. 84 The unexpected death of an individual. Attempted suicide which results in physical harm and/or injury to the individual AND the need for around-the-clock care (regardless of what type of facility). Suspected rape, sexual assault or sexual exploitation against or by a person receiving services. Major disturbance or threat to public safety created in the community by the individual (the threat can be toward anyone including staff and can be in an internal setting – does not have to be on the street). Police involvement when there is an arrest of the individual. Serious physical harm and/or injury of known origin to the individual requiring in-patient hospitalization; Serious physical harm and/or injury to the individual of unknown origin (broken bones, serious lacerations, etc.); Significant change in physical and/or mental health status of the individual (significant increase in seizure activity, aspiration pneumonia, initial diagnosis of terminal disease, significant increase in behavioral issues, etc.); Adverse conditions where an individual is placed at significant risk, possibly due to failure of staff/provider to support the individual's needs (staff not being there when they are assigned to be, staff doing improper patient transfer techniques, etc.). Elopements / missing persons that put the individual and/or others at significant risk. “Support team” means the case manager, the individual who is or may be receiving services administered through the Division of Aging, and any other person or entity the individual chooses to develop a plan to safely reside in the community. PROCEDURES Identification of a Reportable Incident Responsible Entities Anyone with direct monitoring responsibilities including, but not limited to, the following individuals: Case Managers Division of Aging staff Direct care staff Other provider staff, agent, or officer Action Any individual who, as a result of service provision, oversight or monitoring, identifies a event or concern that is, or could be, a reportable unusual occurrence, including a Sentinel Event and/or a suspected or actual incident of abuse, neglect or exploitation, shall: Make a determination as to whether the incident or alleged incident represents: Suspected or actual abuse, neglect or exploitation and/or death; and/or A Sentinel Event; and/or 85 A “reportable unusual occurrence”; Reports such events in accordance with this policy and any other applicable state reporting requirements. Reporting Responsible Entities Anyone with direct monitoring responsibilities including, but not limited to, the following individuals: Case Managers Division of Aging staff Direct care staff Other provider entity staff, agent or officer Actions An initial report regarding an incident shall be submitted in accordance with this policy and as soon as the reporter becomes aware of or receives information about an incident. Incident reports involving suspected or actual abuse, neglect or exploitation, and/or a death, are reported within 24 hours of the occurrence or knowledge of the occurrence in the currently approved format. Incident reports involving Sentinel Events are reported within 24 hours of the occurrence or knowledge of the occurrence in the currently approved format. All other incidents are reported within 48 hours of the occurrence or knowledge of the occurrence in the currently approved format. All incidents (including incidents that are also Sentinel Events and/or events that meet the criteria for suspected or actual abuse, neglect or exploitation) are filed through the DDRS/DA Incident Reporting system. Specific requirements may also apply to incident reporting depending on the nature of the incident described below: APS or CPS Reporting: If an event or concern is found to meet the criteria for suspected or actual abuse, neglect or exploitation including the death of an individual, the incident is reported immediately by the individual with knowledge of the suspected or actual abuse, neglect or exploitation or death to APS or CPS as appropriate. The incident is reported in accordance with Indiana Criminal Code APS or CPS reporting requirements. 86 NOTE: Providers that employ a staff person involved in an incident shall suspend staff involved in the incident pending provider investigation. A narrative shall be provided to APS or CPS (as appropriate) and shall include the following: The name of the person contacted. The phone number of the contact. The county of the contact. No later than twenty-four (24) hours of the occurrence or knowledge of the occurrence, an incident report is also reported in the DA incident reporting system. The incident is coded as a Sentinel Event. A copy of the incident report shall be forwarded to: The individual or legal representative The service provider, if applicable The case manager APS/CPS, as applicable Any other applicable service provider identified The Area Agency on Aging, as applicable Local law enforcement when applicable Incident reports involving Sentinel Events (except incidents meeting the criteria for suspected or actual abuse, neglect or exploitation including the death of an individual, which should have been reported immediately by the individual with knowledge of the suspected or actual abuse, neglect or exploitation or death. See Section (3)(a)): Are reported within 24 hours of the occurrence or knowledge of the occurrence in the currently approved format. Are coded as a Sentinel Event incident and the type of the event is noted in the index section of the incident report within the automated system. A copy of the incident report shall be forwarded to: The individual or legal representative The service provider, if applicable The case manager APS/CPS, as applicable Any other applicable service provider identified The Area Agency on Aging, as applicable Local law enforcement when applicable If an incident initial report is received late and meets the criteria for a sentinel event, the incident will be coded as sentinel – no matter how late the report is. All other incidents: Are reported within 48 hours of the occurrence or knowledge of the occurrence in the currently approved format. Are coded as appropriate in the incident reporting system and the type of event noted in the index section of the incident report within the automated system. 87 A copy of the incident report shall be forwarded to: The individual or legal representative The service provider, if applicable The case manager Any other applicable service provider identified The Area Agency on Aging, as applicable Review of Incidents Responsible Entities DA Staff or designee Actions Initial incident reports will be reviewed within 7.5 working hours of receipt, by DA staff or designee (reviewer). The reviewer will determine if: appropriate notifications have been made, APS or CPS referral has been made, if required the incident meets criteria for a Sentinel Event formal follow-up reports are required The reviewer will request additional information from the submitter or the Case Manager when additional information is required to make these determinations. The reviewer will instruct the submitter to make notifications to APS, CPS, Case Manager or other entities when this has not been done. The reviewer will also notify APS or CPS when appropriate. The reviewer will review an individual’s incident history to identify trends or special needs, and may make recommendations for systemic changes. If the reviewer determines that the health, safety, and welfare concerns have been successfully resolved, the incident will be closed. If a feasible plan to resolve the incident is documented in the initial incident report, the reviewer will: Confirm implementation of the plan, through communications with the AAA, provider, family members, informal caregivers, and consumer, as appropriate; and Ensure the desired outcome was achieved (e.g. situation is resolved and individual’s health and welfare are safeguarded); and If the incident is resolved close the incident; or If the incident is deemed, by the reviewer, to not be resolved appropriately: Refer the incident to the DA Director or designee; and 88 Require additional follow-up reports until the incident is resolved. The reviewer will assign coding appropriate to the incident, including designating Sentinel Event status. The reviewer will ensure the incident information is included in the incident database. The reviewer will send notification of any report specific to a Sentinel Event to appropriate individuals within the Division of Aging, such as the Medicaid Waiver supervisor, Quality Assurance Liaison, Quality Assurance Specialist, ISDH and the Office of Medicaid Policy and Planning . The reviewer will send to the Case Manager notification of the need for follow-up reports. If the individual does not have a Case Manager, the Division of Aging will designate a DA staff person as responsible for follow up. In situations where it would be a conflict of interest for the Case Manager to perform follow-up activities, the Division of Aging will designate a DA staff person as responsible for performing these activities. Follow-up Activities Responsible Entities Case Managers Division of Aging Other provider entities Actions The provider of case management services or, in the event there is no case manager, the designated DA staff, must contact the individual and other support team members as needed, to discuss and address the incident and related issues and concerns. The provider of case management services or, in the event there is no case manager, the designated DA staff, shall submit an incident follow-up report summarizing steps taken and plans identified to resolve the initial incident, and the current status of the situation. The incident follow-up report will be submitted in the prescribed incident follow-up report format within seven (7) days of the date of the initial incident report, and every seven (7) days thereafter. Incidents that are not resolved within twenty-one (21) days of the date of the initial incident shall be referred to the DA Director or designee for additional action. Follow-up reporting shall continue every seven (7) days until the incident is deemed resolved by the DA. Follow-up incident reporting shall be copied to the Quality Assurance Specialist immediately upon receipt 89 The Quality Assurance Specialist within the Division of Aging responsible for Sentinel Event followup will take the steps necessary including communication with case managers, AAAs, other providers, family members and informal to verify or ensure that immediate threats to the individual’s health and welfare are addressed and resolved, and will document this in the individual’s Division of Aging incident record. All information required by the reviewer to be submitted must also be submitted to the individual or the individual’s legal guardian and to the provider of case management services. Weekly status reports of the open sentinel events will be reviewed by the Quality Assurance Liaison. On a monthly basis, the Quality Assurance Liaison will review the open incident reports requiring follow up. Through the weekly and monthly reports, the Quality Assurance Liaison will analyze, and track the incident reports, review for trends, review for appropriate corrective action and will make recommendations to the Sanctions Committee or Quality Improvement Executive Committee, as appropriate for sanctions or quality improvement procedures that should be implemented. Non-compliance with this policy may result in actions taken by the Division of Aging to include: Shall not authorize continuation of services to an individual or individuals by the provider Shall not authorize receipt of services by individuals not already receiving services from the provider at the time the determination is made that the provider did not implement a corrective action plan to the reasonable satisfaction of the Division of Aging 90 Appendix C: IHCP Bulletin BT200371 – Documentation Standards for HCBS 91 92 93 94 95 96 97 98 99 100 101 102 103 104 105 Appendix D: Older Americans Act Title III C From the U.S. Code Online via GPO Access [wais.access.gpo.gov][Laws in effect as of January 3, 2006][CITE: 42USC3030e] TITLE 42--THE PUBLIC HEALTH AND WELFARE CHAPTER 35--PROGRAMS FOR OLDER AMERICANS SUBCHAPTER III--GRANTS FOR STATE AND COMMUNITY PROGRAMS ON AGING Part C--Nutrition Services subpart i--congregate nutrition services Sec. 3030e. Grants for establishment and operation of nutrition projects The Assistant Secretary shall carry out a program for making grants to States under State plans approved under section 3027 of this title for the establishment and operation of nutrition projects(1) which, 5 or more days a week (except in a rural area where such frequency is not feasible (as defined by the Assistant Secretary by regulation) and a lesser frequency is approved by the State agency), provide at least one hot or other appropriate meal per day and any additional meals which the recipient of a grant or contract under this subpart may elect to provide; (2) which shall be provided in congregate settings, including adult day care facilities and multigenerational meal sites; and (3) which may include nutrition education services and other appropriate nutrition services for older individuals. (Pub. L. 89-73, title III, Sec. 331, as added Pub. L. 95-478, title I,Sec. 103(b), Oct. 18, 1978, 92 Stat. 1536; amended Pub. L. 102-375,title III, Sec. 313, Sept. 30, 1992, 106 Stat. 1238; Pub. L. 103171,Sec. 3(a)(13), Dec. 2, 1993, 107 Stat. 1990; Pub. L. 106-501, Title III,Sec. 312(c), Nov. 13, 2000, 114 Stat. 2252.) Amendments 2000--Par. (2). Pub. L. 106-501 inserted “, including adult daycare facilities and multigenerational meal sites” before semicolon. 1993--Pub. L. 103-171 substituted “Assistant Secretary” for “Commissioner” in introductory provisions and par. (1). 1992--Par. (1). Pub. L. 102-375 inserted “(except in a rural area where such frequency is not feasible (as defined by the Commissioner by regulation) and a lesser frequency is approved by the State agency)”after “week” and struck out before semicolon at end “, each of which assures a minimum of one-third of the daily recommended dietary allowances as established by the Food and Nutrition Board of the National Academy of Sciences-National Research Council”. Effective Date Subpart effective at close of Sept. 30, 1978, see section 504 of Pub. L. 95-478, set out as an Effective Date of 1978 Amendment note under section 3001 of this title. 106 Nutrition Projects for Elderly Under Prior Provisions, Qualified Under Successor Provisions, Eligible for Funds Under Such Provisions; Discontinuance of Payments for Ineffective Activities Operation of predecessor projects under successor provisions, see section 501(b) of Pub. L. 95478, set out as a note under section 3045of this title. From the U.S. Code Online via GPO Access [wais.access.gpo.gov][Laws in effect as of January 3, 2006][CITE: 42USC3030f] TITLE 42--THE PUBLIC HEALTH AND WELFARE CHAPTER 35--PROGRAMS FOR OLDER AMERICANS SUBCHAPTER III--GRANTS FOR STATE AND COMMUNITY PROGRAMS ON AGING Part C--Nutrition Services subpart ii--home delivered nutrition services Sec. 3030f. Grants for establishment and operation of nutrition projects for older individuals The Assistant Secretary shall carry out a program for making grants to States under State plans approved under section 3027 of this title for the establishment and operation of nutrition projects for older individuals which, 5 or more days a week (except in a rural area where such frequency is not feasible (as defined by the Assistant Secretary by regulation) and a lesser frequency is approved by the State agency),provide at least one home delivered hot, cold, frozen, dried, canned, or supplemental foods (with a satisfactory storage life) meal per day and any additional meals which the recipient of a grant or contract under this subpart may elect to provide. (Pub. L. 89-73, title III, Sec. 336, as added Pub. L. 95-478, title I,Sec. 103(b), Oct. 18, 1978, 92 Stat. 1536; amended Pub. L. 102-375,title III, Sec. 314, Sept. 30, 1992, 106 Stat. 1238; Pub. L. 103171,Sec. 3(a)(13), Dec. 2, 1993, 107 Stat. 1990.) Amendments 1993--Pub. L. 103-171 substituted “Assistant Secretary” for “Commissioner” in two places. 1992--Pub. L. 102-375 inserted “(except in a rural area where such frequency is not feasible (as defined by the Commissioner by regulation) and a lesser frequency is approved by the State agency)" after "week" and struck out before period at end, each of which assures a minimum of one-third of the daily recommended dietary allowances as established by the Food and Nutrition Board of the National Academy of Sciences-National Research Council”. Effective Date Subpart effective at close of Sept. 30, 1978, see section 504 of Pub. L. 95-478, set out as in Effective Date of 1978 Amendment note under section 3001 of this title. 107 From the U.S. Code Online via GPO Access [wais.access.gpo.gov][Laws in effect as of January 3, 2006][CITE: 42USC3030g] TITLE 42--THE PUBLIC HEALTH AND WELFARE CHAPTER 35--PROGRAMS FOR OLDER AMERICANS SUBCHAPTER III--GRANTS FOR STATE AND COMMUNITY PROGRAMS ON AGING Part C--Nutrition Services subpart ii--home delivered nutrition services Sec. 3030g. Efficiency and quality criteria The Assistant Secretary, in consultation with organizations of and for the aged, blind, and disabled, and with representatives from the American Dietetic Association, the Dietary Managers Association, the National Association of Area Agencies on Aging, the National Association of Nutrition and Aging Services Programs, the National Association of Meals Programs, Incorporated, and any other appropriate group, shall develop minimum criteria of efficiency and quality for the furnishing of home delivered meal services for projects described in section 3030f of this title. The criteria required by this section shall take into account the ability of established home delivered meals programs to continue such services without major alteration in the furnishing of such services. (Pub. L. 89-73, title III, Sec. 337, as added Pub. L. 95-478, title I,Sec. 103(b), Oct. 18, 1978, 92 Stat. 1536; amended Pub. L. 97-115,Sec. 10(e), Dec. 29, 1981, 95 Stat. 1601; Pub. L. 100-175, title I,Sec. 182(n), Nov. 29, 1987, 101 Stat. 967; Pub. L. 102-375, title III,Sec. 315, Sept. 30, 1992, 106 Stat. 1239; Pub. L. 103-171,Sec. 3(a)(13), Dec. 2, 1993, 107 Stat. 1990.) Amendments 1993--Pub. L. 103-171 substituted “Assistant Secretary” for “Commissioner”. 1992--Pub. L. 102-375 inserted “the Dietary Managers Association, “after “Dietetic Association,”. 1987--Pub. L. 100-175 substituted “National Association of Area Agencies” for “Association of Area Agencies”. 1981--Pub. L. 97-115 substituted “National Association of Nutrition and Aging Services Programs” for “National Association of Title VII Project Directors”. Effective Date of 1987 Amendment Amendment by Pub. L. 100-175 effective Oct. 1, 1987, except not applicable with respect to any area plan submitted under section 3026 (a)of this title or any State plan submitted under section 3027(a) of this title and approved for any fiscal year beginning before Nov. 29, 1987,see section 701(a), (b) of Pub. L. 100-175, set out as a note under section 3001 of this title. 108 From the U.S. Code Online via GPO Access [wais.access.gpo.gov][Laws in effect as of January 3, 2006][CITE: 42USC3030g-21] TITLE 42--THE PUBLIC HEALTH AND WELFARE CHAPTER 35--PROGRAMS FOR OLDER AMERICANS SUBCHAPTER III--GRANTS FOR STATE AND COMMUNITY PROGRAMS ON AGING Part C--Nutrition Services subpart iii--general provisions Sec. 3030g-21. Nutrition A State that establishes and operates a nutrition project under this chapter \1\ shall\1\ So in original. Title III of Pub. L. 89-73, as amended, contained parts and subparts, but not chapters. (1) solicit the advice of a dietitian or individual with comparable expertise in the planning of nutritional services, and (2) ensure that the project(A) provides meals that(i) comply with the Dietary Guidelines for Americans, published by the Secretary and the Secretary of Agriculture, (ii) provide to each participating older individual(I) a minimum of 33\1/3\ percent of the daily recommended dietary allowances as established by the Food and Nutrition Board of the Institute of Medicine of the National Academy of Sciences, if the project provides one meal per day, (II) a minimum of 66\2/3\ percent of the allowances if the project provides two meals per day, and (III) 100 percent of the allowances if the project provides three meals per day, and (iii) to the maximum extent practicable, are adjusted to meet any special dietary needs of program participants, (B) provides flexibility to local nutrition providers in designing meals that are appealing to program participants, (C) encourages providers to enter into contracts that limit the amount of time meals must spend in transit before they are consumed, (D) where feasible, encourages arrangements with schools and other facilities serving meals to children in order to promote intergenerational meal programs, (E) provides that meals, other than in-home meals, are provided in settings in as close proximity to the majority of eligible older individuals' residences as feasible, 109 (F) comply \2\ with applicable provisions of State or local laws regarding the safe and sanitary handling of food, equipment, and supplies used in the storage, preparation, service, and delivery of meals to an older individual, \2\ So in original. Probably should be “complies”. (G) ensures that meal providers carry out such project with the advice of dietitians (or individuals with comparable expertise), meal participants, and other individuals knowledgeable with regard to the needs of older individuals, (H) ensures that each participating area agency on aging establishes procedures that allow nutrition project administrators the option to offer a meal, on the same basis as meals provided to participating older individuals, to individuals providing volunteer services during the meal hours, and to individuals with disabilities who reside at home with and accompany older individuals eligible under this chapter,\1\ (I) ensures that nutrition services will be available to older individuals and to their spouses, and may be made available to individuals with disabilities who are not older individuals but who reside in housing facilities occupied primarily by older individuals at which congregate nutrition services are provided, and (J) provide \3\ for nutrition screening and, where appropriate, for nutrition education and counseling. \3\ So in original. Probably should be “provides”. (Pub. L. 89-73, title III, Sec. 339, as added Pub. L. 106-501, Title III, Sec. 313, Nov. 13, 2000, 114 Stat. 2252.) Codification Pub. L. 106-501, Sec. 313, which directed amendment of subpart 4 of part C of title III of the Older Americans Act of 1965 (Pub. L. 89-73)by striking section 339 and inserting this section, was executed in this subpart, which is subpart 3 of part C of title III of the Act, by repealing prior section 3030g-21, and inserting this section, to reflect the probable intent of Congress and the redesignation of subpart 4 of part C of title III of the Act as subpart 3 by Pub. L. 106-501,Sec. 312(b). Prior Provisions A prior section 3030g-21, Pub. L. 89-73, title III, Sec. 339, as added Pub. L. 102-375, title III, Sec. 317, Sept. 30, 1992, 106 Stat.1241, related to compliance with dietary guidelines prior to repeal by Pub. L. 106-501, title III, Sec. 313, Nov. 13, 2000, 114 Stat. 2252. See Codification note above. 110 From the U.S. Code Online via GPO Access [wais.access.gpo.gov][Laws in effect as of January 3, 2006][CITE: 42USC3030g-22] TITLE 42--THE PUBLIC HEALTH AND WELFARE CHAPTER 35--PROGRAMS FOR OLDER AMERICANS SUBCHAPTER III--GRANTS FOR STATE AND COMMUNITY PROGRAMS ON AGING Part C--Nutrition Services subpart iii--general provisions Sec. 3030g-22. Payment requirement Payments made by a State agency or an area agency on aging for nutrition services (including meals) provided under part A, B, or C of this subchapter may not be reduced to reflect any increase in the level of assistance provided under section 3030a of this title. (Pub. L. 89-73, title III, Sec. 339A, as added Pub. L. 102-375, Title III, Sec. 317, Sept. 30, 1992, 106 Stat. 1241.) Prior Provisions Prior sections 3030h to 3030l were repealed by Pub. L. 106-501,title III, Sec. 314(1), Nov. 13, 2000, 114 Stat. 2253. Section 3030h, Pub. L. 89-73, title III, Sec. 341, as added Pub. L.100-175, title I, Sec. 140(d), Nov. 29, 1987, 101 Stat. 945; amended Pub. L. 102-375, title I, Sec. 102(b)(6), (10)(C), Sept. 30, 1992, 106Stat. 1201, 1202; Pub. L. 103-171, Sec. 3(a)(13), Dec. 2, 1993, 107Stat. 1990, authorized a grant program for States. Section 3030i, Pub. L. 89-73, title III, Sec. 342, as added Pub. L.100-175, title I, Sec. 140(d), Nov. 29, 1987, 101 Stat. 945; amended Pub. L. 102-375, title I, Sec. 102(b)(7), title III, Sec. 318, Sept.30,1992, 106 Stat. 1201, 1241, defined “in-home services”. Section 3030j, Pub. L. 89-73, title III, Sec. 343, as added Pub. L. 100-175, title I, Sec. 140(d), Nov. 29, 1987, 101 Stat. 945, provided for the State agency to develop eligibility criteria. Section 3030k, Pub. L. 89-73, title III, Sec. 344, as added Pub. L.100-175, title I, Sec. 140(d), Nov. 29, 1987, 101 Stat. 946, required that funds available under former part D of this subchapter be in addition to funds otherwise expended. Section 3030l, Pub. L. 89-73, title III, Sec. 351, as added Pub. L.100-175, title I, Sec. 141(d), Nov. 29, 1987, 101 Stat. 946; amended Pub. L. 102-375, title VII, Sec. 708(a)(2)(C), Sept. 30, 1992, 106Stat. 1292; Pub. L. 103-171, Sec. 3(a)(13), Dec. 2, 1993, 107 Stat. 1990,authorized program of grants to satisfy special needs of older individuals. 111 Appendix E: CHOICE Guidelines CHOICE MANUAL Revised September 2012 Revised November 2007 Prepared by the Division of Aging Prepared by the Division of Aging 112 TABLE OF CONTENTS 10000 Overview of CHOICE.......................................................................................... 3 10001 Code of Ethics.................................................................................................... 4 10002 AAA Contracts for Administration of CHOICE Funds ..................................... 5 10003 Public Records Requests.................................................................................. 5 10004 CHOICE Eligibility Determinations ................................................................... 5 10005 CHOICE Waiting List.......................................................................................... 8 10006 CHOICE Reduction in Service and Participant Termination Policy................ 8 10007 CHOICE Cost-Sharing ....................................................................................... 9 10008 Individual Cap on CHOICE Funds................................................................... 10 10009 Funding of Last Resort.................................................................................... 10 10010 CHOICE Funds and Medicaid.......................................................................... 11 10011 Covered Services............................................................................................. 12 10012 CHOICE and Hospice Services ....................................................................... 13 10013 CHOICE and Self-Directed Attendant Care .................................................... 14 10014 CHOICE Fund Prohibited Uses ....................................................................... 17 10015 Unusual Occurrences/Incident Reporting...................................................... 18 10016 CHOICE Applicant and Participant Appeals .................................................. 18 10017 CHOICE Plan .................................................................................................... 18 10018 AAA CHOICE Reporting .................................................................................. 20 10019 Case Management ........................................................................................... 21 10020 Plan of Care...................................................................................................... 25 10021 Confidentiality.................................................................................................. 28 10022 Provider Requirements – General .................................................................. 28 10023 Provider Requirements – Organizational Chart Guideline. ........................... 30 10024 Provider Requirements – Personnel Records ............................................... 30 10025 Provider Requirements – Personnel Policies and Manuals.......................... 31 10026 Provider Requirements – Maintenance of Records of Services Provided ... 33 10027 Provider Requirements – Data Collection Standards.................................... 33 10028 Provider Requirements – Billing Standards................................................... 33 10029 Provider Requirements – Disclosure of Financial Information..................... 33 10030 Provider Requirements – Insurance............................................................... 34 10031 Provider Requirements – Quality Assurance and Quality Improvement System......................................................................................................................... 34 10032 Transfer of Individual’s Records Upon Change of Provider ......................... 35 10033 Provider Requirements – Procedures for Protecting Individuals................. 35 10034 Provider Requirements – Individual’s “No-Show” for a Service .................. 36 10035 Legally Responsible Individuals as CHOICE Providers................................ 36 10036 Provider Requirements – Coordination of Services and Plan of Care ......... 36 10037 Service Specific Provider Requirements – Adaptive Equipment Providers 37 10038 Service Specific Provider Requirements – Adult Day Services Providers .. 37 10039 Service Specific Provider Requirements – Attendant Care .......................... 37 113 10040 Service Specific Provider Requirements – Environmental Modifications ... 37 10041 Service Specific Provider Requirements – Family Caregiver Support......... 38 10042 Service Specific Provider Requirements – Home Health Services............... 38 10043 Service Specific Provider Requirements – Home Delivered Meals .............. 38 10044 Service Specific Provider Requirements – Homemaker ............................... 38 10045 Service Specific Provider Requirements – Home Repair and Maintenance Services....................................................................................................................... 39 10046 Service Specific Provider Requirements – Information and Assistance ..... 39 10047 Service Specific Provider Requirements – Legal assistance services ........ 39 10048 Service Specific Provider Requirements – Nutrition Education ................... 39 10049 Service Specific Provider Requirements – Outreach Services..................... 39 10050 Service Specific Provider Requirements – Personal Emergency Response Systems....................................................................................................................... 40 10051 Service Specific Provider Requirements – Pest Control Services ............... 41 10052 Service Specific Provider Requirements – Respite Care .............................. 41 10053 Service Specific Provider Requirements – Supplies ..................................... 43 10054 Service Specific Provider Requirements – Therapy Services ...................... 43 10055 Service Specific Provider Requirements – Transportation........................... 43 10056 Service Specific Provider Requirements for Self-Directed In-Home Care ... 44 10057 Provider Requirements – Warranties ............................................................. 45 10058 Provider Monitoring ......................................................................................... 46 10059 Provider Non-Compliance with Requirements .............................................. 47 10060 Provider Non-Compliance with Requirements That Endangers the Health or Welfare of an Individual Such That an Emergency Exists ....................................... 48 10061 Provider – Revocation of Approval................................................................. 49 10062 Provider Appeals ............................................................................................. 49 10063 HCBS Providers – Resolution of Disputes..................................................... 50 10000 20000 Overview of CHOICE The Community and Home Options to Institutional Care for the Elderly and Disabled (CHOICE) program provides case management services, assessment, and in-home and community services to individuals who are at least 60 years of age or persons of any age who have a disability due to a mental or physical impairment and who are found to be at risk of losing their independence. At least 20% of the AAA CHOICE service dollars shall be utilized for individuals under the age of 60 with disabilities. The CHOICE board has a range of oversight responsibilities as described in IC 12-10-11 and IC 12-10-10-11(b). The Indiana Family and Social Services Administration (FSSA), Division of Aging (DA) establishes CHOICE guidelines and procedures for the effective management of the 114 CHOICE program and provides a process for public input. The FSSA DA is responsible for publishing CHOICE guidelines and procedures as part of the FSSA DA Operations Manual (which are contained in this Section). Comments and recommendations specific to these guidelines are accepted annually from the public. The FSSA DA provides notice to the public of revisions in guidelines and procedures by publishing any revisions of CHOICE guidelines and procedures in the CHOICE Board meeting agenda and posting revisions of CHOICE guidelines and procedures before an official CHOICE Board meeting in the office of the FSSA DA. Comments and recommendations for revision may be given during any official CHOICE board meeting. 10001 Code of Ethics All CHOICE providers or agents (including AAAs and CHOICE service providers) shall abide by the code of ethics in this section (Authority IC 12-10-10, 455 IAC 1.2-21.-, 455 IAC 1-4-11) (1) A provider shall do the following: (A) Provide professional services with objectivity and respect for the independence, needs, and values of the individual receiving services. (B) Avoid discrimination on the basis of factors that are irrelevant to the provision of services, including, but not limited to race, creed, gender, age, or disability. (C) Provide sufficient objective information to enable an individual or the individual’s guardian to make informed decisions. (D) Accurately present the professional qualifications and credentials of the provider and of all employees and agents. (E) Require all employees or agents to assume responsibility and accountability for personal and professional competence in the practice of the person’s profession and provision of services under this article. (F) Require professional, licensed, or accredited employees or agents to adhere to accepted industry standards for the employee’s or agent’s area of professional practice. (G) Require all employees or agents to do the following: i Maintain the confidentiality of individual information consistent with the standards of this article and all other laws and regulations governing confidentiality of individual information, including the Health Insurance Portability and Accountability Act (HIPAA). ii Conduct all practice with honesty, integrity, and fairness. iii Fulfill professional commitments in good faith. iv Inform the public and colleagues of services only by use of factual information. v Refrain from the following: 115 (a) Advertising or marketing services in a misleading manner. (b) Engaging in uninvited solicitation of potential individuals who are vulnerable to undue influence, manipulation, or coercion. (H) evaluation. Make reasonable efforts to avoid bias in any kind of professional (I) Notify the proper authority of any conduct that may cause harm or undue influence toward a participant. This may include FSSA DA, Indiana State Department of Health, licensing authorities, accrediting agencies, employers, or the State of Indiana Attorney General. 10002 AAA Contracts for Administration of CHOICE Funds The FSSA DA contracts with the AAAs to administer CHOICE funds (Authority IC 12-10-10, 455 IAC 1-4-3, 455 IAC 1-4-11) (1) The FSSA DA enters into contracts with AAAs for the purpose of administering CHOICE funds. Contracts are effective for a period of two (2) years. (2) Contracted activities include but are not limited to: (A) budgeting; (B) case management; (C) oversight; (D) monitoring; (E) reporting; (F) quality assurance; and (G) submission of fiscal claims to the FSSA DA. 10003 Public Records Requests As a public agency, each AAA shall make public records available in accordance with Indiana’s Public Access Laws (Authority IC-5-14-3). The AAA shall ensure the provisions of IC-5-14-3, as well as HIPAA requirements regarding Protected Health Information (PHI) are followed when disclosing or making public records available. 10004 CHOICE Eligibility Determinations Individuals must meet specified eligibility requirements in order to participate in CHOICE. (Authority IC 12-10-10, 455 IAC 1-4-1,455 IAC 1-4-5, 455 IAC 1-4-7(d) and (e), 455 IAC 1-4-11) (1) The CHOICE case manager shall conduct an eligibility determination for individuals requesting services funded by CHOICE. In order to be eligible for 116 CHOICE funds an individual must: (A) B e at least sixty (60) years of age or disabled. i Age shall be verified as recorded on a birth certificate, driver’s license, passport or other official government document. Case manager shall document in case notes that age was verified using these documents; ii "Disabled" refers to an individual with a severe chronic disability that is attributable to a mental or physical impairment or combination of mental and physical impairments that is likely to continue indefinitely; (B) B e an individual at risk of losing their independence. i “Individual at risk of losing their independence” means the individual is unable to perform two (2) or more activities of daily living as determined through the use of an assessment. The long-term care services eligibility screen developed by the division shall be used by the case manager to assess the applicant's risk of losing his or her independence and to assist in the development of a plan of care if appropriate. (C) Have assets that do not exceed five hundred thousand dollars ($500,000). If applicant wishes to receive services but has assets in excess of five hundred thousand dollars ($500,000), applicant may continue to receive services, but obligation for payment is solely upon the client. i For applicants who have had a Medicaid determination within ninety (90) days of application for CHOICE, the case manager shall obtain asset information submitted to the Division of Family Resources (DFR) as part of the Medicaid eligibility determination process, from the FSSA DA CHOICE representative. (a) The FSSA DA CHOICE representative shall provide the countable resource amount for each of the following assets (resources) obtained from the ICES system: Checking and Savings Accounts Certificates of Deposit Individual Retirement Accounts (except MED Works) Stocks/Bonds/Mutual Funds Cash surrender value of life insurance (CSV) Vehicles Non-income-producing Real Estate Trust Funds ii For applicants who have not had a Medicaid eligibility determination within ninety (90) days of application for CHOICE, the case manager shall: (a) Assist the applicant with gathering and completion of information necessary for the applicant to submit an application for Medicaid to the DFR; and (b) Ensure the applicant has made application for Medicaid assistance prior to authorizing interim CHOICE services pending completion of the Medicaid eligibility determination as described in Section 12 of the Division of Aging Operations Manual. 117 (c) Upon completion of the Medicaid eligibility determination, the case manager shall obtain asset information from the FSSA DA CHOICE representative as described in (C)(i) above. (d) If applicant is denied Medicaid eligibility due to a failure to comply with the DFR requests, the applicant will be denied eligibility for CHOICE, as well. (e) If determination of eligibility has not been made within 90 calendar days of the Medicaid application being submitted to the DFR, the respective AAA shall contact the FSSA DA CHOICE representative for assistance. (f) For all CHOICE clients, who are not already a Medicaid client, the respective AAA shall have that individual’s Medicaid status reconsidered on an annual basis or upon a substantial change in financial or medical status. (g) Any applicant who is eligible for specific benefits and/or services from Medicaid but refuses those benefits and/or services from Medicaid will be ineligible for those specific benefits and/or services from CHOICE. iii The CHOICE applicant must complete and sign the CHOICE Asset Attestation Form (Attachment 1) attesting that the information obtained from the Medicaid eligibility determination process continues to accurately reflect their assets, including type and amount. (a) If the applicant’s assets have changed, the case manager shall refer the applicant to DFR for a Medicaid eligibility redetermination. iv shall: If the applicant has assets in excess of $500,000, the case manager (a) Inform the applicant of their obligation to assume responsibility for payment of CHOICE service costs; and (b) services. Determine if the applicant wishes to continue to receive CHOICE v If the individual wishes to receive, or continue to receive, CHOICE services, the case manager shall ensure the individual is billed for 100% of the cost of CHOICE services in accordance with CHOICE billing procedures. vi If the individual does not wish to receive, or continue to receive, CHOICE services, the case manager shall determine whether access to CHOICE services is essential to the individual’s health and welfare. (a) If the case manager believes lack of access to CHOICE services places the individual at risk of neglect or harm, the case manager shall: File an incident report documenting the circumstances; and Take no further action in regard to CHOICE services until the FSSA DA CHOICE representative makes a determination regarding how to proceed. The FSSA DA CHOICE representative shall make this determination within three (3) business days of notification by the case manager and shall notify the AAA in writing of their determination. 118 (b) If the case manager believes lack of access to CHOICE services does not place the individual at risk of neglect or harm, the case manager shall: Not authorize the individual to receive CHOICE services or shall ensure CHOICE services are terminated, as appropriate. 10005 CHOICE Waiting List AAAs are responsible for ensuring there is no CHOICE waiting list whenever feasible and, when necessary, for maintaining the waiting list for their service area, submitting required data and reports regarding the waiting list and monitoring individuals who are on the waiting list. (Authority IC 12-10-10, 455 IAC 1-4-3, 455 IAC 1-4-5, 455 IAC 1-4-11) The CHOICE waitlist is comprised of individuals who have been assessed and are waiting for Choice services. The I4A Waiting List Policy will provide written protocol for a unified procedure to place patients on and off of the waiting list. 10006 CHOICE Reduction in Service and Participant Termination Policy (Authority 455 IAC 1-4-7(e)(f)) CHOICE funding should be used after all other possible payment sources have been identified and all reasonable efforts have been employed to utilize those sources. The AAA shall reduce or disallow services that are paid by CHOICE in any of the following circumstances: a) When the assessed level of need diminishes as established by an assessment. b) When the AAA's CHOICE service funds are insufficient to meet the service commitment to current participants, all reasonable efforts have been made to secure resources to avoid service reductions, the AAA has stopped performing new assessments and care plans, and the AAA has adopted a fair and equitable policy for distributing service reductions among participants. c) When an individual receiving services becomes eligible under a Medicaid home and community-based services waiver and begins receiving those services that are allowable through the Medicaid program. d) When a current participant becomes eligible for in-home and community services from other sources for which he or she was not previously eligible and is receiving those services. e) When other resources become available in the community and the individual begins receiving those services that were not available at the time of the development of the previous care plan. f) If services needed by the applicant, as determined by the assessment, would be so costly that CHOICE payment for the needed services would cause the AAA to exceed the allowable cost per individual determined by the division. g) When the individual or his or her CHOICE representative refuses to receive services from other sources that would ensure that CHOICE is the funding of last resort. The AAA shall terminate services that are paid by CHOICE in any of the following 119 situations: a) When the individual's health or personal circumstances have improved so that he or she no longer needs in-home and community-based services to maintain his or her independence in a safe, non-institutional environment. b) When the health, welfare, or safety of the participant or of others who interact with the individual can no longer be reasonably assured. c) When the services being provided are detrimental to the individual's health. d) When the individual or his or her CHOICE representative has fraudulently obtained or misused CHOICE funded services. e) Upon the death of the individual receiving services. f) When the individual or his or her CHOICE representative refuses to comply with cost sharing under section 8 of this rule. g) When the individual or his or her CHOICE representative voluntarily requests termination. h) When the individual or his or her CHOICE representative refuses services necessary for his or her health and well-being. CHOICE Cost-Sharing AAAs are responsible for determining and implementing cost-sharing requirements for CHOICE. (Authority, IC 12-10-10, IC 12-10-11-8, 455 IAC 1-4-4, 455 IAC 1-4-8, 455 IAC 1-4-11) (1) Cost-sharing is not required for: Participants whose income does not exceed one hundred fifty percent (150%) of the federal income poverty level. (2) Cost sharing is required for participants with incomes over 150% FPL, unless the cost share of services would result in an income falling below 151% of the FPL. The participant is not obligated to pay the amount owed that would drop their income below this level. (A) Participants with incomes over 150% FPL and up to 350% may be charged a share of cost depending on their amount of income adjusted by allowable deductions as specified in the Division of Aging Cost Share document. The cost share increases by ½ of 1% for each 1% increase in the percent of poverty over 150% FPL. The increase and corresponding dollar amount is also displayed in the Division of Aging Cost Share document. (B) Participants with an income that exceeds three hundred fifty percent (350%) of the federal poverty level (FPL) adjusted by any allowable deductions as specified in Attachment 2, must pay 100% of the cost of CHOICE services except for case management, the initial assessment and the development of the plan of care. (C) The case manager shall determine the cost share amount by entering required income and service information into the FSSA DA data system. The data system automatically generates the cost share amount. 120 (3) AAA. The collection of each individual’s monthly cost share is the responsibility of the (A) If the cost share is equal to $9.99 or less annually, the AAA is not required to collect the cost-share from the individual. (4) Cost Share Billing statements will be generated monthly and sent to the appropriate CHOICE individuals by the AAA. (5) Cost share is not applied to case management, since this has been determined by the FSSA DA to be an administrative service and not a direct service. 10008 Individual Cap on CHOICE Funds CHOICE funds are subject to an individual cap. (Authority IC 12-10-10, 455 IAC 1-4-11) (1) The FSSA DA has established a maximum level of expenditures of CHOICE funds per individual (cap). The current cap amount per quarter is $13,517. (2) This cap is not to be applied monthly, but over a period of three (3) consecutive months to coincide with the period covered by the plan of care. (A) period. The cost of home modifications can be amortized over a twelve month (3) CHOICE case management is an administrative function of the AAA. It is excluded from the cost cap. (4) The maximum level of expenditure will be calculated as a single cost amount for the elderly and for persons with disabilities under sixty years of age. (A) (B) basis. This level of expenditure is calculated by the FSSA DA based on the Skilled Nursing Facility (SNF) Index, and is adjusted annually. The cap amount is provided to the AAAs by the FSSA DA on an annual 10009 Funding of Last Resort CHOICE funds may only be utilized after all other available sources of funding of home and community-based services (HCBS) have been accessed. CHOICE funding shall be used only after all other possible payment sources have been identified and all reasonable efforts have been employed to utilize those sources. (Authority IC 12-10-10, 455 IAC 1-4-7, 455 IAC 1-4-11) The AAA case manager shall conduct a review of all available sources of funding of home and community-based services other than CHOICE supports for each individual 121 determined eligible for CHOICE funds. The review shall include, but is not limited to: (A) Older Americans Act Funded HCBS such as Home Delivered Meals, respite and adult day care services; (B) Medicaid state plan HCBS such as home health services, durable medical (DME), non-emergency transportation, therapies, and targeted case management; (C) Medicaid HCBS waiver services such as those included in the AD Waiver, TBI Waiver, and DD Waiver; (D) Medicare services such as home health services and DME or special services provided by Medicare Advantage (HMO) plans; (E) Services funded by the Ryan White Program; (F) Services funded by the Vocational Rehabilitation Program; (G) Food stamps; (H) Services funded by the Veteran’s Administration; (I) Services funded by HUD; (J) Title III-E caregiver funds; and (K) Other sources of HCBS. 10010 CHOICE Funds and Medicaid Except as provided in subsections (1)(a)(ii) and (1)(B) below CHOICE funds may only be utilized after an applicant has been determined ineligible for Medicaid or if currently eligible for Medicaid, after a determination that the requested service(s) is not available from Medicaid. (Authority, IC 12-10-10, 455 IAC 1-4-7, 455 IAC 1-4-11) (1) CHOICE funds may not be authorized for any new client who has not applied for, or received, a Medicaid eligibility determination within the last ninety days. (A) A new client who has not applied for Medicaid eligibility determination within ninety (90) days of application for CHOICE, the case manager shall: i Assist the applicant with gathering and completion of information necessary for the applicant to submit a Request for Assistance (for Medicaid) to the DFR; and ii Ensure the applicant has made application for Medicaid assistance prior to authorizing interim CHOICE services pending completion of Medicaid eligibility determination. (B) CHOICE funds may be authorized for Medicaid applicants awaiting the outcome of a Medicaid eligibility determination. (2) CHOICE funds and Medicaid spend down: If an eligible individual meets Medicaid asset guidelines but has a spend down provision to satisfy, CHOICE services 122 may be utilized while the spend down amount is being met. (3) CHOICE funds may be authorized for Medicaid recipients following a determination by the case manager and/or FSSA DA that Medicaid state plan services and HCBS waiver services for which the individual is eligible do not meet the identified need for which CHOICE funds are being requested. (A) If the individual is a Medicaid recipient, the case manager must review whether the requested service is available or could be available under the Medicaid state plan or under a HCBS waiver in which the individual is enrolled. (B) If the requested service is denied by Medicaid (in the case of Medicaid state plan services) or by the HCBS waiver case manager or other HCBS waiver decision maker (in the case of HCBS waiver services), but an alternative service is authorized, the individual must access this Medicaid state plan or HCBS waiver alternative service. (1) CHOICE funds cannot be used to fund alternative and/or more costly services or supports as an alternative to one that is available from another funding source because of individual preference, convenience or other factors unrelated to need. For example, CHOICE funds may not be authorized to purchase a specific type of van modification when a less costly van modification that can meet the individual’s needs has been authorized from another funding source. (2) If the individual refuses to access the authorized or available Medicaid state plan or HCBS waiver service, the case manager must issue a CHOICE denial and notice of right to appeal in accordance with Section 100016. (C) If the requested service is denied by Medicaid (in the case of Medicaid state plan services) or by the HCBS waiver case manager or other HCBS waiver decision maker (in the case of HCBS waiver services), and an alternative service is not authorized or available, the service or support may be funded by CHOICE (subject to all other CHOICE funding restrictions.) (4) CHOICE participants determined ineligible for Medicaid must reapply for a Medicaid eligibility determination each time their circumstances change in a manner that could affect eligibility (e.g. result in a determination they are eligible for Medicaid). (A) The case manager shall assist the participant with gathering and completion of information necessary for the applicant to submit a Request for Assistance (for Medicaid) to the DFR and shall monitor the outcome of the Medicaid eligibility determination process. 10011 Covered Services CHOICE funds may only be used to purchase specified services. (Authority IC 12-10-10, 455 IAC 1-4-11,455 IAC 1.2-5-1(e)) CHOICE funded services are limited to: (A) Adaptive aids and devices. (B) Adult day services. 123 (C) Attendant care. (D) Case management services. (E) Environmental modifications. (F) Family caregiver support. (G) Home health services. (H) Home delivered meals. (I) Homemaker. (J) Home repair and maintenance services. (K) Information and assistance. (L) Legal assistance services. (M) Nutrition education / counseling. (N) Outreach services. (O) Respite care. (P) Therapy services. (Q) Transportation. (R) Self-directed attendant care services provided by a registered personal services attendant under the applicable statute to persons in need of self- directed inhome care. (S) Other services necessary to prevent institutionalization of eligible individuals when feasible as authorized on the plan of care. 10012 CHOICE and Hospice Services CHOICE participants may receive Medicare and/or Medicaid hospice services and CHOICE funded services and supports, but these services must be coordinated to ensure non-duplication of services and payment. (Authority, IC 12-10-10, 455 IAC 1-4-11) (1) The case manager, upon learning of an individual’s election (or plan to elect) the hospice benefit under Medicare and/or Medicaid, shall contact the individual and the hospice case manager to review the need to coordinate services. (A) Hospice services include a range of services designed to address the needs of individuals with a terminal illness. Services include: nursing services; medical social services; physician services; counseling services, including dietary and bereavement counseling; short-term inpatient care, including respite care; medical 124 appliances and drugs; home health aide and homemaker services; physical therapy; occupational therapy; and speech-language pathology services. In addition, Medicare covers any other service that is specified in the hospice plan of care, and for which payment may otherwise be made under Medicare. The most common hospice services in danger of duplication with CHOICE-funded services are home health aide and homemaker services. Hospice, except when provided as an inpatient service, provides intermittent services that do not include sitter or companion services. Services are not designed, for example, to provide care, to enable a caregiver to go to work. (B) The case manager must review the hospice plan of care and reduce CHOICE services that are duplicative of services contained in the hospice plan of care and terminate CHOICE-funded respite services, for as long as the individual remains enrolled in hospice. A CHOICE recipient may not refuse hospice services in order to continue to receive a comparable service funded by CHOICE. (C) When an individual elects hospice services, they may not receive paid respite services funded by CHOICE but instead must utilize hospice respite services, if not a duplicate service. (D) The CHOICE case manager and hospice case manager should explain to the individual the services covered through both programs and the reductions that are being made and the reasons for the reductions (e.g. to ensure non-duplication of services and payment). 10013 CHOICE and Self-Directed Attendant Care AAAs must inform CHOICE participants of their right to choose to self-direct personal attendant services. CHOICE participants may choose to self-direct personal attendant services as specified in this section. (Authority, IC 12-10-10, IC 12-10-17.1, 455 IAC 1-4-11) (1) CHOICE participants may choose to self-direct personal attendant services if they are an "individual in need of self-directed in-home care". (A) An ”individual in need of self-directed in-home care” means a disabled individual, or person responsible for making health related decisions for the disabled individual, who: i is approved to receive Medicaid HCBS waiver services or is a CHOICE participant; ii is in need of attendant care services because of impairment; iii requires assistance to complete functions of daily living, self-care, and mobility, including those functions included in attendant care services; iv chooses to self-direct a paid personal services attendant to perform attendant care services; and v assumes the responsibility to initiate self-directed in-home care and exercise judgment regarding the manner in which those services are delivered, including the decision to employ, train, and dismiss a personal services 125 attendant. (B) "Attendant care services" means those basic and ancillary services, which the individual chooses to direct and supervise a personal services attendant to perform, that enable an individual in need of self-directed in- home care to live in the individual's home and community rather than in an institution and to carry out functions of daily living, self-care, and mobility. (C) "Basic services" means a function that could be performed by the individual in need of self-directed in-home care if the individual were not physically disabled. The term includes the following: i vehicles. ii iii iv v vi Assistance in getting in and out of beds, wheelchairs, and motor Assistance with routine bodily functions. Health related services. Bathing and personal hygiene. Dressing and grooming. Feeding, including preparation and cleanup. (D) “Health related services" means those medical activities that, in the written opinion of the attending physician submitted to the case manager of the individual in need of self-directed in-home care, could be performed by the individual if the individual were physically capable, and if the medical activities can be safely performed in the home, and: i are performed by a person who has been trained or instructed on the performance of the medical activities by an individual in need of self- directed in-home care who is, in the written opinion of the attending physician submitted to the case manager of the individual in need of self-directed in-home care, capable of training or instructing the person who will perform the medical activities; or ii are performed by a person who has received training or instruction from a licensed health professional, within the professional's scope of practice, in how to properly perform the medical activity for the individual in need of self-directed in-home care. (E) "Licensed health professional" means the following: A registered nurse. A licensed practical nurse. A physician with an unlimited license to practice medicine or osteopathic medicine. A licensed dentist. A licensed chiropractor. A licensed optometrist. A licensed pharmacist. A licensed physical therapist. A certified occupational therapist. A certified psychologist. A licensed podiatrist. A licensed speech-language pathologist or audiologist. (F) "Ancillary services" means services ancillary to the basic services provided to an individual in need of self-directed in-home care who needs at least one (1) of the basic services (as defined in section 4 of this 126 chapter). The term includes the following: i Homemaker type services, including shopping, laundry, cleaning, and seasonal chores. ii Companion type services, including transportation, letter writing, mail reading, and escort services. iii Assistance with cognitive tasks, including managing finances, planning activities, and making decisions. (2) Individuals self directing their own care health related services must have the approval of their attending physician. (A) The case manager must maintain an attending physician’s written opinion in the individual’s case file regarding the opinion of the individual’s attending physician that the health related services could be performed by the individual if the individual were physically capable, and if the medical activities can be safely performed in the home, and: i are performed by a person who has been trained or instructed on the performance of the medical activities by an individual in need of self- directed in-home care and, in the written opinion of the attending physician, the individual in need of selfdirected in-home care is capable of training or instructing the person who will perform the medical activities; or ii are performed by a person who has received training or instruction from a licensed health professional, within the professional's scope of practice, in how to properly perform the medical activity for the individual in need of self-directed in-home care. (3) Responsibilities for self-directed care: (A) The individual in need of self-directed in-home care is responsible for recruiting, hiring, training, paying, certifying any employment related documents, dismissing, and supervising in the individual's home during service hours a personal services attendant who provides attendant care services for the individual. (B) If an individual in need of self-directed in-home care is less than twentyone (21) years of age or unable to direct in-home care because of a brain injury or mental deficiency, the individual's parent, spouse, legal guardian, or a person possessing a valid power of attorney may make employment, care, and training decisions and certify any employment related documents on behalf of the individual. (C) An individual in need of self-directed in-home care or an individual under subsection (B) and the individual's case manager shall develop an authorized plan of care. The authorized plan of care must include a list of weekly services or tasks that must be performed to comply with the authorized plan of care. (4) Parents of minor individuals, spouses, or other adults legally responsible relatives for the individual may not provide attendant care services for compensation under this legislation. 127 (5) Providers of CHOICE-funded self-directed care must comply with the requirements set forth in IC 12-10-17. (6) Upon request, the FSSA DA will provide to an individual in need of self-directed in-home care the following: (A) A list of personal services attendants who are registered with the division and available within the requested geographic area will be provided without charge, (B) A copy of the information of a specified personal services attendant who is registered with the FSSA DA. The division may charge a fee for shipping, handling, and copying expenses. (7) The individual in need of self-directed in-home care and the personal services attendant must each sign a contract, in a form approved by the FSSA DA, that includes, at a minimum, the following provisions: (A) The responsibilities of the personal services attendant. (B) services. The frequency the personal services attendant will provide attendant care (C) The duration of the contract. (D) The hourly wage of the personal services attendant. The wage may not be less than the federal minimum wage or more than the rate that the recipient is eligible to receive under a Medicaid home and community based services waiver or the community and home options to institutional care for the elderly and disabled program for attendant care services. (E) Reasons and notice agreements for early termination of the contract. (8) A personal services attendant who is hired by the individual in need of selfdirected in-home care is an employee of the individual in need of self-directed in- home care. The division and the AAA are not liable for any actions of a personal services attendant or an individual in need of self-directed in-home care. A personal services attendant and an individual in need of self-directed in-home care are each liable for any negligent or wrongful act or omission in which the person personally participates. 10014 CHOICE Fund Prohibited Uses CHOICE funds may not be used for some purposes or activities. (Authority IC 12-10-10, 455 IAC 1-4-7, 455 IAC 1-4-11) Choice funds may not be used to: (1) purchase services or supports available from another funding source, including but not limited to: Medicare, private long-term care insurance, Vocational Rehabilitation, Medicaid state plan and Medicaid HCBS waivers. (2) purchase real estate. 128 (3) provide care or services to an individual residing in an institution. However, funds may be used for assessment and plan of care development for current residents in institutions who could return to their homes if determined to be eligible for the CHOICE program. Assisted living facilities are not considered institutional settings. Home modification is an exception and will be acceptable for an individual residing in an institution if used to transition an individual back into the home. However, the individual would need to have been an active CHOICE client prior to the institutionalization. 10015 Unusual Occurrences/Incident Reporting Any person with direct monitoring responsibilities shall report all incidents that meet the definition of a reportable unusual occurrence in accordance with the requirements of Indiana FSSA DA Incident Reporting Policy. (Authority IC 12-10-10, 455 IAC 1.2-8-2, 455 IAC 1-4-11) All incidents classified as reportable unusual occurrences shall be reported to the DA, and to APS or CPS when applicable, and in accordance with the FSSA DA Incident Reporting Policy. Refer to the Indiana FSSA DA Incident Reporting Policy for definitions, policy and procedure. 10016 CHOICE Applicant and Participant Appeals CHOICE applicants have a right to appeal AAA decisions regarding eligibility or services to be provided. (Authority IC 12-10-10, 455 IAC 1-4-3, 455 IAC 1-4-11 IAC 1-4-10) Refer to Section 3007 of the Division of Aging Operations Manual. 10017 CHOICE Plan A CHOICE Plan must be submitted each year with the Area Plan or Area Plan Update. The CHOICE Plan must include procedures for making CHOICE program information available to applicants, participants and the public. CHOICE Plan Contents and Format: Section 1 – Intake and Referral Process Description of the referral and intake process, including eligibility determination protocols and method of eligibility notification. Section 2 – Assessment Process Description of the assessment process, format, and procedures used by AAA case managers including methodology for ensuring completion of ninety-day face-to-face assessments of CHOICE participants. Section 3 – Nursing Home Outreach Describe the outreach and follow up methods for offering assessments to current nursing home residents who apply for CHOICE. Section 4 – Hiring Practices Describe the methods of recruitment, screening, and hiring of staff. 129 Section 5 – Care Plan Development Process Description of the procedures used to develop the plan of care including a timeline for the development process from start to implementation of services. Also a description of the role the individual and/or their family play in the development of their care plan. Section 6 – Area and Community Support Services A list of all available long-term support services, both public and private, within the area. Section 7 – Case Management and Service Coordination Policies and procedures for the case management and service coordination. Section 8 – Coordinating CHOICE with Other Funding Sources Policies and procedures for coordinating CHOICE with Medicaid state plan services, HCBS waiver services and other funding sources for in- home and community-based services. Describe the methodology for determining priority funding, last resort funding, and preventing duplication of services among funding sources. Section 9 – QA/QI Plan Description of quality assurance (QA) and quality improvement (QI) plan for CHOICE services consistent with FSSA DA QA/QI requirements for HCBS. Section 10 – Plans of Care Evaluation and Monitoring Description of internal methods of evaluating plans of care to ensure participants are receiving quality services and direction. Describe how plans of care are selected for review, who conducts the monitoring, what criteria is used to evaluate the appropriateness of service and stewardship of funding, and the frequency of monitoring. Include policies and procedures for conducting QIPs internally and in collaboration with FSSA DA or its contractor. Section 11 – Follow up and Incident Reporting Description of processes and procedures for participant follow up and incident reporting. Section 12 – Mortality Reviews Policies and procedures for responding to mortality reviews conducted by FSSA in accordance with the FSSA DA Mortality Review Policy for HCBS. Section 13 – Cost Sharing Description of CHOICE cost sharing plan procedures, including cost share collection methods. Section 14 – Complaint and Appeal Procedures Description of complaint and appeal procedures, which include the process for notifying applicants or participants of the right to an administrative hearing, which incorporates the FSSA DA Complaint Policy for HCBS. 130 Section 15 – Waiting List Description of policies and procedures for operating, maintaining and clearing the AAA waiting list for CHOICE services in accordance with the requirements contained in these CHOICE Guidelines. Section 16 – Budget Budget Narrative and breakdown of spending in accordance with the contract between AAA and FSSA DA on the following categories: 1. A Breakdown of Proposed Spending on Consumer Services 2. Assessments 3. Care Plan Development 4. Reassessments 5. AAA Administration 6. Any Other Appropriate Costs Section 17 – Provider Selection Description of processes and procedures for selecting service providers. Including methods for ensuring a variety of CHOICE providers for participants to choose from. 10018 AAA CHOICE Reporting Before October 1 st of each year, the AAA is required to report both programmatic and fiscal information from the previous state fiscal year, July 1 to June 30, to the FSSA DA. FSSA DA uses the data to prepare a report for review by CHOICE Board and the Indiana General Assembly (Authority IC 12-10-10, 455 IAC 1-4-11). (1) Each AAA shall provide an annual report that details: (A) The amount of CHOICE funds spent; (B) Administrative expenses for CHOICE; (C) The use of CHOICE funds in supplementing the funding of services provided to individuals through other programs; (D) The waiting list for CHOICE including numbers of persons on the waiting list, movement off the waiting list and actions taken to clear the waiting list; (E) The number, capacity and types of participating CHOICE providers; (F) An examination of CHOICE participants’: i ii iii Demographic characteristics; Impairment and medical characteristics; Reportable unusual occurrences/incidents; 131 iv Grievances and Appeals; v Length of time receiving CHOICE services in 30 day increments; and vi The number of CHOICE participants leaving the CHOICE program by month, their reason for leaving and final disposition. (G) CHOICE participant outcomes; (H) have: A determination of the estimated number of CHOICE applicants who i ii and iii performed; (I) 100004); and one (1) assessed activity of daily living that cannot be performed; two (2) assessed activities of daily living that cannot be performed; three (3) or more assessed activities of daily living that cannot be Children’s CHOICE and CHOICE/TANF expenditures (see Section (J) The AAA will complete the cost share report generated from INsite and send to FSSA DA on a quarterly basis. (K) Choice data for each month must be entered into INsite by the 10th of the following month. 10019 Case Management Case Manager Qualifications ( Authority IC 12-10-10, IC 12-10-10-1, 455 IAC 1.2, 455 IAC 1-4-3, 455 IAC 1-4-11) Case managers must meet specific requirements regarding qualifications and certification in order to be eligible to perform CHOICE program-related duties. Case managers must be employees of the AAA formally assigned to carry out the AAA’s responsibility for case management. Case managers and applicants must meet the following qualifications: (A) Possess a degree or licensing as described below: i Bachelor's Degree in social work, psychology, gerontology, sociology, counseling, nursing; or ii A license as a Registered Nurse with one year of experience in human services; or iii A Bachelor's Degree in any other field with a minimum of two years, full-time direct service experience with the elderly or persons with disabilities. This experience must include assessment, plan of care development, implementation, and monitoring.; or iv A Master's Degree in a related field may substitute for the required experience. (B) A current limited criminal history obtained from the Indiana State Police Central Repository, as prescribed in 455 IAC 1.2-6-2. Applicants with any criminal 132 convictions including, but not limited to, the following may not be certified: i ii iii iv v vi vii viii ix (C) A sex crime (IC 35-42-4). Exploitation of an endangered adult (IC 35-46-1-12). Abuse or neglect of a child (IC 35-42-2-1). Failure to report battery, neglect, or exploitation of an endangered adult or dependent (IC 35-46-1-13). Theft (IC 35-43-4), except as provided in IC 16-27-2-5(a)(5). Murder (IC 35-42-1-1). Voluntary manslaughter (IC 35-42-1-3). Involuntary manslaughter (IC 35-42-1-4). Battery (IC 35-42-2). Applicants have the right to appeal adverse determinations. Criminal or Juvenile History Appeals: The subject of a record may initiate a challenge as to the accuracy/completeness of any entry on his/her record. For Indiana entries on the report, challenges should be directed to: Indiana State Police, Records Division, Indiana Government Center North, Room N302, 100 North Senate Ave., Indianapolis, IN 46204. For federal entries on the report, challenges should be directed to: FBI, Criminal Justice Information Services (CJIS) Division, ATTN: SCU, Mod. D-2, 1000 Custer Hollow Road, Clarksburg, WV 26306. All Other Criminal/Civil History Appeals: The local DCS office will provide contact information for the appropriate agency. Case Manager Certification The AAA makes decisions regarding certification based upon the submitted documentation. The decision regarding certification is sent to the candidate with a copy sent to the FSSA DA. Each AAA must certify case managers according to the following criteria: (A) The applicant’s compliance with and completion of all applicable provider requirements. (B) The applicant’s demonstrated qualifications and abilities to determine the needs of community alternatives to institutional placement available. Case managers must have knowledge of the disabilities/conditions of the persons served by CHOICE. (C) Be at least eighteen (18) years of age, competent to provide services, and demonstrate the ability to communicate. i Possess a current, valid state-issued driver’s license if the employee will be transporting an individual and provide proof of current insurance on the vehicle used to transport (1) CHOICE case managers must complete training specific to the CHOICE program before performing CHOICE program-related duties. (A) All case managers must attend the FSSA DA “Case Management Orientation” within the first six months of employment with an AAA and obtain at least 20 hours of additional training each year. (10 of which must be DA approved) 133 (B) Case Manager Orientation Training is exclusive to new case managers. Case managers who have already attended Case Manager OrientationTraining shall not be invited to attend a second time. Case Manager Non-Compliance CHOICE case managers who do not comply with CHOICE program requirements will be subject to corrective action up to and including decertification (Authority IC 12-10-10, 455 IAC 1-4-11) (1) A CHOICE case manager may be subject to corrective action and/or decertified for failure to comply with CHOICE requirements, including provider requirements specified in this Chapter. (A) Corrective action shall be initiated at the option of the AAA and may include, but is not limited to: i ii iii and/or iv Removal from an active caseload for retraining; Attendance at prescribed training sessions; One-to-one follow along by a case manager assigned by the AAA; Suspension for a prescribed period of time followed by any of (i) through (iii) above. A CHOICE case manager will be decertified (de-activated) as of the case manager’s last date of employment. A case manager shall NOT be decertified for a temporary absence, such as for maternity, medical, or family leave. Case Management Responsibilities and Standards (Authority IC 12-10-10, 455 IAC 1.2-17-7, 455 IAC 1.2–17-2455 IAC 1-4-11, 455 IAC 14-2, 455 IAC 1.2-8-1, 455 IAC 1.2-9-2) Each AAA is responsible for performance and oversight of “case management” functions for CHOICE and the standards by which case managers operate, which include: (A) Assessing the individual to determine functional impairment level and corresponding need for services; (B) Identifying all sources of funding, services and supports other than CHOICE. CHOICE is last resort funding. (C) Developing a plan of care that addresses the individual's needs; Case managers will ensure that “person centered planning” is utilized in the development of the individual’s CHOICE plan of care and while they receive services. (D) Reviewing and explaining to the individual/guardian the services that will be provided and obtaining all required signatures on the plan of care before submitting it to the Area Agency on Aging. Any plan of care requiring State approval will not be implemented prior to obtaining State approval. (E) Supervising the implementation of services for the individual; Case managers shall ensure a maximum response time between implementation of the initial plan of care and the first monitoring contact will be no more than thirty (30) calendar 134 days. Case managers will complete face-to-face contact with each individual a minimum of every ninety (90) days to assess the quality and effectiveness of the plan of care. (F) Advocating on behalf of the individual's interests; Case managers will communicate the individual’s needs, strengths and preferences to appropriate persons including CHOICE providers and other persons of the individual’s choosing. Case managers will regularly inform individual’s of their right to refuse treatment or seek a change to their plan of care. (G) Monitoring the quality of community and home care services provided to an eligible individual and ensuring that plan of care objectives are being met. Case managers will document within seven (7) days, in the chronological narrative, each contact with the individual and with the providers. (H) Determining the cost effectiveness of using in-home and community services as alternatives to traditional care or services. Case managers will monitor the services being provided to ensure good stewardship of the funding. (I) Reassessing the plan of care to determine the continuing need or termination of services. At least two of these face-to-face contacts per year will be in the home setting. Case managers will complete annual assessments and care plan updates with the individual in a timely manner to avoid gaps in service authorization. (J) Providing each individual/guardian with clear and easy to understand instructions for contacting the case manager. The case manager will also provide additional information and procedures for individuals who may need assistance or have an emergency that occurs before or after business hours. (K) Providing information and referral services to individuals in need of community and home care services; Case managers will provide, at a minimum but not limited to, a state information guide as provided by the Division of Aging to individuals on how to choose a provider and will assist the individual to evaluate potential service providers. (L) Performing record keeping and data collection activities, including the import and export of case records at a minimum of every seven (7) calendar days; Case managers will keep all files in a standardized format and sequence and provide the State ready access to all case manager documentation shall a request be made. (M) Providing community education regarding the case management system. (N) Establishing relationships with existing service providers and collaborating with the other service providers to coordinate services consistent with the participant’s plan of care. (O) Providing continuous supervision of case managers. Ensuring compliance with all DA issued manuals, as well as all federal, state, and local law, 135 and all FSSA policy, rules, regulations and guidelines. (P) Ensuring the case management system has access to administrative and support services. (Q) Facilitating and monitoring the formal and informal supports that are developed to maintain the individual’s health and welfare in the community. (R) Ensuring confidentiality of individual information. Case managers will maintain privacy and confidentiality of all individual records and follow all applicable guidelines set forth in this section regarding record access. (S) Performing an assessment and planning for discharge from an institutional setting. (T) Maintaining the highest professional and ethical standards. (U) Ensuring individuals have a free choice of service provider, and of case manager, and shall have the right to change any provider or case manager. Case managers will provide to individuals a list of potential providers the services offered. (V) Ensuring unusual occurrences/incidents made known to the case manager are reported and addressed in accordance with the FSSA DA Incident Reporting Policy for HCBS and in accordance with Indiana mandatory reporting requirements when applicable. (W) CHOICE. Conducting follow-up evaluations for individuals terminated from (X) home Coordinate services when other payer sources are providing care in the 10020 Plan of Care The case manager shall initiate a plan of care and work with the individual or his or her designated CHOICE representative, to develop the plan of care with respect to the individual’s unique needs and wishes. (Authority IC 12-10-10, 455 IAC 1-4-3, 4, 5, 6, 455 IAC 1.2-19-1, 455 IAC 1-4-11) The case manager shall initiate a CHOICE plan of care for each person eligible for CHOICE regardless of the applicant's income and assets, except when: (A) The applicant or his or her CHOICE representative does not want to proceed with the development of a plan of care; (B) The applicant or his or her CHOICE representative refuses to release the information that is necessary to develop a plan of care; and/or (C) The AAA does not have the resources, within the available funds, to develop and carry out a plan of care. 136 Preliminary Information Gathering The case manager shall have available or gather the following information concerning the participant prior to initiation of the plan of care: (1) The needs and wants of a participant or his or her designated CHOICE representative including their health, welfare, and request for self-directed care. (2) All services available regardless of funding source or community resource provider. (3) A list of service s the participant is eligible for and the funding available for each of those services. Plan of Care Development The plan of care shall be developed in collaboration with the individual or his or her designated CHOICE representative and shall include a formal description of goals, objectives, and strategies designed to enhance independence. CHOICE plans of care shall be developed within 14 calendar days of the date of the assessment, except when the AAA does not have the resources, within the available funds, to develop and carry out a plan of care. When funds are not available, development of a plan of care shall be deferred until such time as funds become available. When funding becomes available, the plan of care shall be developed within 14 days of availability of these funds. At that time the previous assessment shall be reviewed and revised, if needed, prior to completion of the plan of care. The long-term care services eligibility screen developed by the FSSA DA shall be used by the AAA to assess the applicant's risk of losing his or her independence and to assist in the development of a plan of care, if appropriate. The participant has the right to be involved in the formulation of the plan of care and shall be involved at every stage of decision making regardless of their care or living situation. The applicant, or their CHOICE representative, may decide whether family or others may participate in the development of the plan of care and updates that may follow. During the development of the plan of care, necessary communication assistance shall be provided at no cost to the participant. Each plan of care shall include services that may be funded by CHOICE when necessary to meet an individual’s assessed needs and subject to specific CHOICE fund limitations. Each plan of care must be developed in accordance with limitations specific to CHOICE funds. i CHOICE funds may be used for services authorized under the CHOICE program. ii Some services that may be funded with CHOICE funds require additional documentation to establish necessity and appropriateness of the service. iii CHOICE funds are the funding of last resort. iv CHOICE funds may not be authorized for any individual who has not applied for, or received, a Medicaid eligibility determination within the last ninety days. v There is an individual cap on CHOICE funds that must be applied 137 during plan of care development. (D) Each plan of care shall address: i The individual’s personal goals in key life areas including home life, health care, community participation and self-direction; ii The individual’s daily living needs and preventative health care needs as well as any other identified needs; iii The services needed to maintain independence. iv The cost of the services still needed. v The sources of all services and support available to meet the individual’s needs whether paid or unpaid, including the payment sources of those services and the no-cost or voluntary services that can be provided to meet the individual's needs. vi The requested and authorized CHOICE service(s) when necessary to meet an individual’s assessed needs and subject to specific CHOICE fund limitations. The plan of care shall specify for each authorized CHOICE service; (a) The frequency of the service(s); (b) The duration of the service(s); (c) The provider of the service(s); (d) Any special instructions specific to the service(s); and (e) Provisions for back-up services and emergencies. (E) The plan of care must be signed by the applicant or by his or her CHOICE representative. i If the case manager has reason to believe that an individual lacks the capacity to make a knowing and informed decision regarding his or her own care, the case manager shall consult with the individual's physician. The individual's physician shall make a determination regarding the individual's capacity to make a knowing and informed decision. If the physician determines that the individual lacks the capacity to make a knowing and informed decision regarding his or her own care, the plan of care and any revisions must be approved and signed by the individual's CHOICE representative. ii If the individual is physically unable to sign the application or plan of care, but has the capacity to make a knowing and informed decision regarding his or her own care, the individual may indicate his or her assent and authorize another to sign. iii There shall be documentation in the case file that the individual (and/or representative, if any) has reviewed and approved the plan of care. (F) Notwithstanding the fact that an individual needs a CHOICE representative, the case manager shall work and consult with the individual who will be receiving the services and shall take his or her preferences into consideration when developing a plan of care, to the extent that the individual's health or safety is not threatened. The case manager shall ensure the individual, individual’s legal representative if applicable, and providers of services regardless of whether the services 138 are CHOICE services or received from another sources, are provided with copies of relevant documentation. i Copies of relevant documentation shall include information on individual rights, an individual’s plan of care, how to file complaints with FSSA DA, and requesting appeals concerning issues and disputes relating to the services provided to the individual. ii A copy of the plan of care shall be given to the applicant/participant or his or her designated CHOICE representative upon completion of the plan of care, upon revision to the plan of care and at any other time upon request. 10021 Confidentiality (Authority P.L. 104-91) The AAA shall maintain individual case records for each individual who applies for or receives services. These records shall be maintained for a minimum of seven years after the individual’s termination from the program or other final action. The AAA shall maintain the confidentiality of CHOICE files and records at all times. Such files and records shall not be disclosed except: (1) (2) to the individual or their CHOICE representative; to a person representing the individual in an appeal from a CHOICE decision; (3) to the division or other state agencies for purposes of securing in-home and community services; (4) to an adult or child protective services investigator under IC 12-10-3 and IC 31-611-3; (5) under court order; or (6) as authorized by the individual or their CHOICE representative. The AAA shall use CHOICE records for purposes of the CHOICE program and for the coordination of other related services only. 10022 Provider Requirements – General CHOICE funded services may only be provided by authorized service providers. (Authority, IC 12-10-10, 455 IAC 1.2, 455 IAC 1-4-3, 455 IAC 1-4-11) (1) Each AAA shall arrange for the provision of individually needed CHOICE services through local provider agencies or individuals who are approved to provide CHOICE-funded services. (2) Providers of self-directed attendant care services funded under CHOICE are exempt from the following provisions, but are required to comply with Section 139 10013, Self-Directed Attendant Care. (3) In order to become an approved CHOICE provider of HCBS, an entity shall do the following: (A) Meet the current minimum service provider requirements as specified in this Chapter or show proof of licensure or certification from the state of Indiana, if a license is required. i Providers that are licensed and regulated by the Indiana State Department of Health (ISDH) shall be deemed approved for those licensed services. ii For services not licensed by the ISDH, the provider must meet all other requirements to provide the specified service(s). (B) consumers. Be certified and/or enrolled to provide services for CHOICE program (C) Certify that, if approved, the entity will provide HCBS using only persons who meet the qualifications specified in this Chapter. (D) Retain, and have readily available, a copy of the most current executed signed provider agreement or contract as applicable. (E) Assure and document compliance with the executed provider agreement or contract and the requirements of this Chapter. (F) Comply with the following: i Applicable federal, state, county, or municipal regulations that govern the operation of the agency. ii FSSA laws, rules, and policies. (G) Provide proof of the following: iii That insurance is in force as prescribed in 455 IAC 1.2-11-1 and 455 IAC 1.2-12-1(4). iv That any employee, agent, or staff of the provider agency meets all standards and requirements for the specific services the person will be providing. v That licensed health professionals are checked for findings through the Indiana professional licensing agency. vi That certified home health aides and/or certified nursing assistants are checked for finding on the aide registry through the Indiana professional licensing agency. (H) (H) Obtain a current limited criminal history obtained from the Indiana state police central repository, as prescribed in 455 IAC 1.2-15-2(b)(2), for each employee or agent involved in the direct management, administration, or provision of services before providing direct care to individuals receiving services. i Providers may not be, or may not employ or contract with, a person convicted of crimes including, but not limited to, the following: (a) A sex crime (IC 35-42-4). (b) Exploitation of an endangered adult (IC 35-46-1-12). 140 (c) Abuse or neglect of a child (IC 35-42-2-1). (d) Failure to report battery, neglect, or exploitation of an endangered adult or dependent (IC 35-46-1-13). (e) Theft (IC 35-43-4), except as provided in IC 16-27-2-5(a)(5). (f) Murder (IC 35-42-1-1). (g) Voluntary manslaughter (IC 35-42-1-3). (h) Involuntary manslaughter (IC 35-42-1-4). (i) Battery (IC 35-42-2). ii Criminal or Juvenile History Appeals: The subject of a record may initiate a challenge as to the accuracy/completeness of any entry on his/her record. For Indiana entries on the report, challenges should be directed to: Indiana State Police, Records Division, Indiana Government Center North, Room N302, 100 North Senate Ave., Indianapolis, IN 46204. For federal entries on the report, challenges should be directed to: FBI, Criminal Justice Information Services (CJIS) Division, ATTN: SCU, Mod. D-2, 1000 Custer Hollow Road, Clarksburg, WV 26306. All Other Criminal/Civil History Appeals: The local DCS office will provide contact information for the appropriate agency. (I) Obtain and submit a current document from the nurse aide registry of the Indiana State Department of Health verifying that each unlicensed employee or agent involved in the direct provision of services has no finding entered into the registry, if applicable, before providing direct care to individuals receiving services. (J) Ensure staff providing direct care for CHOICE participants: i Are at least eighteen (18) years of age. ii Are competent to provide services according to the individual’s plan of care. iii Demonstrate the ability to effectively communicate. iv Submit a copy of a current negative TB test or negative chest x-ray that is completed annually. v Possess a current, valid state-issued driver’s license if the employee will be transporting an individual. Provide proof of current insurance on the vehicle used to transport an individual that meets current Indiana requirements. (K) The provider shall maintain documentation that the provider meets the requirements and maintains the minimum standards set out in this Chapter for providing CHOICE-funded services. 10023 Provider Requirements – Organizational Chart Guideline. CHOICE providers shall maintain and make available an organizational chart. (Authority IC 12-10-10, 455 IAC 1.2-9-1,455 IAC 1-4-11) 10024 Provider Requirements – Personnel Records CHOICE providers shall maintain in the provider’s office, files for each employee or 141 agent of the provider. (Authority, IC 12-10-10, 455 IAC 1.2-14-1, 455 IAC 1-4-11) (1) The files for each employee or agent who provides direct care shall contain the following: (A) An annual negative tuberculin skin test or chest x-ray before providing services, updated in accordance with recommendations of the Centers for Disease Control. (B) Copies of the current, valid state-issued driver’s license and automobile insurance information, updated when the insurance is paid, if the employee or agent will be transporting an individual. (C) Limited criminal history information that meets the requirements of 455 IAC 1.2-6-2(3). (D) Verification of each training session attended by the employee or agent, including substantiation of the following: i ii iii iv The content. The length of the training session. Identification of the trainers. Dated signatures of the trainers and the employee. (2) The files for each employee or agent who does not provide direct care shall contain the following: (A) Limited criminal history information that meets the requirements of 455 IAC 1.2-6-2(3). (B) applicable. Professional licensure, certification, or registration, including renewals, as (C) Verification of each training session attended by the employee or agent, including substantiation of the following: i ii iii iv The content. The length of the training session. Identification of the trainers. Dated signatures of the trainers and the employee. 10025 Provider Requirements – Personnel Policies and Manuals CHOICE providers, who use employees or agents to provide services shall adopt, maintain and ensure compliance with personnel policies and manuals. (Authority IC 12-10-10, 455 IAC 1.2-15, 455 IAC 1-4-11) (1) A provider or its agent shall adopt, maintain, and follow a written personnel policy. The written personnel policy shall: (A) Be reviewed at least annually and updated as needed. 142 (B) Be provided to each employee or agent. (C) Include, but is not limited to, the following: i A procedure for conducting reference, employment, and criminal background checks on each prospective employee or agent. ii A prohibition against employing or contracting with a person convicted of crimes including, but not limited to, the following: (a) A sex crime (IC 35-42-4). (b) Exploitation of an endangered adult (IC 35-46-1-12). (c) Abuse or neglect of a child (IC 35-42-2-1). (d) Failure to report battery, neglect, or exploitation of an endangered adult or dependent (IC 35-46-1-13). (e) Theft (IC 35-43-4), except as provided in IC 16-27-2-5(a)(5). (f) Murder (IC 35-42-1-1). (g) Voluntary manslaughter (IC 35-42-1-3). (h) Involuntary manslaughter (IC 35-42-1-4). (i) Battery (IC 35-42-2). (D) A process for evaluating the job performance of each employee or agent at the end of the training period and annually thereafter, including a process for feedback from individuals receiving services from the employee or agent. (E) Disciplinary procedures. (F) A description of grounds for disciplinary action against or dismissal of an employee or agent. (G) A clear description of an employee’s rights and responsibilities, including the responsibilities of administrators and supervisors. (H) A procedure to ensure compliance with HIPAA regulations. (2) A provider or its agent shall adopt and maintain a job description for each position, including the following: (A) Minimum qualifications for the position. (B) Major duties required of the position. (C) The written personnel policy required by subsection (1). (3) A provider or its agent shall ensure compliance with and compile written policies and procedures specified in this section into a written operations manual. (A) The operations manual shall be regularly updated and revised not less 143 often than annually. (B) Upon the request of FSSA DA or its designee, the provider shall do either of the following: i Supply a copy of the operations manual to FSSA DA or its designee, or another state agency at no cost. FSSA DA will maintain the confidentiality of proprietary information, as deemed appropriate. ii Make the operations manual available to FSSA DA or its designee, or another state agency for inspection at the offices of the provider. 10026 Provider Requirements – Maintenance of Records of Services Provided A CHOICE provider or its agents shall maintain, in the provider’s office, documentation of all services provided to an individual. (Authority, IC 12-10-10, 455 IAC 1.2-16, 455 IAC 1-4-11) (1) A CHOICE provider or its agents shall: (A) Maintain, in the provider’s office, documentation of all services provided to an individual. (B) Analyze and maintain the documentation required by the following: i to an individual. ii iii CHOICE standards applicable to the services the provider is providing The professional standards applicable to the provider’s profession. The individual’s plan of care. (2) Documentation related to an individual and required by this article shall be maintained by the provider per HIPAA guidelines following the end of service provision by the provider or its agent to the individual or as specified in law or rule. 10027 Provider Requirements – Data Collection Standards CHOICE providers shall comply with data collection and reporting standards. (Authority IC 12-10-10, 455 IAC 1.2-9-4, 455 IAC 1-4-11) A provider or its agent shall utilize the INsite state-approved data collection system. 10028 Provider Requirements – Billing Standards CHOICE providers shall comply with billing standards. (Authority IC 12-10-10, 455 IAC 1.2-9-4, 455 IAC 1-4-11) 10029 Provider Requirements – Disclosure of Financial Information CHOICE providers shall comply with financial disclosure requirements specified in this Section. (Authority 455 IAC 1.2-10-1, 455 IAC 1-4-11) (1) (A) (1) A provider or its agent shall do the following: Maintain financial records in accordance with generally accepted 144 accounting and bookkeeping practices. (B) Be audited as follows: i Under the direction of the provider agreement or contract. ii According to state board of accounts requirements and procedures for the services contracted. http://www.in.gov/sboa/publications/ (2) A provider will, upon request, provide to the AAA and/or FSSA DA copies of audit findings. 10030 Provider Requirements – Insurance CHOICE providers shall secure insurance as specified in this Section. (Authority IC 12-10-10, 455 IAC 1.2-11-1, 455 IAC 1-4-11) A provider shall secure insurance to cover at least personal injury, loss of life and property damage to an individual caused by fire, accident, or other casualty arising from the provision of services to the individual by the provider. 10031 Provider Requirements – Quality Assurance and Quality Improvement System CHOICE providers or their agent shall have a written internal quality assurance and quality improvement system in accordance with this Section. (Authority IC 12-10-10, 455 IAC 1.2-9-5, 455 IAC 1-4-11) (1) A provider’s or its agent’s written internal quality assurance and quality improvement system shall be: (A) Focused on the individual. (B) Appropriate for the services being provided. (C) Ongoing and updated at least annually. (2) The system described in subsection (1) shall include at least the following elements: (A) guidelines. An annual survey of individual satisfaction, in accordance with contract (B) Records of findings for annual individual satisfaction surveys. (C) Documentation of efforts to improve service delivery in response to the surveys of individual satisfaction. (D) An annual assessment of the appropriateness and effectiveness of each service provided to an individual. (E) i (a) A written process for the following, if applicable: Analyzing data concerning the following: Reportable incidents. Reportable incidents are those incidents 145 specified in the Indiana FSSA DA Incident Reporting Policy. (b) Services provided. ii future incidents. Developing and reviewing recommendations to reduce the risk of 10032 Transfer of Individual’s Records Upon Change of Provider CHOICE funded services may only be provided by authorized service providers. (Authority, IC 12-10-10, 455 IAC 1.2-8-3, 455 IAC 1-4-11) If an individual changes providers for a home and community-based service, the case manager shall facilitate the transfer of pertinent records related to the individual to the new provider within five (5) calendar days while maintaining compliance with HIPAA regulations. 10033 Provider Requirements – Procedures for Protecting Individuals CHOICE providers shall develop procedures to protect individuals as specified in this section. (Authority, IC 12-10-10, 455 IAC 1.2-8-1, 455 IAC 1-4-11) (1) Each provider of services shall maintain specific written safety and security policies and procedures for an individual. (2) Each provider of services shall train all employees or agents in implementing written safety and security policies. (3) Each provider of services shall establish a written procedure providing for when and how to notify law enforcement, APS, or CPS, as deemed appropriate and emergency response agencies in an emergency or crisis. (4) Each provider of services shall establish a written procedure providing for scheduling and completion of evacuation drills when providing services in locations other than an individual’s own home (i.e. residential service providers and adult day services providers.) (A) Adopting procedures that shall be followed in an emergency or crisis, such as any of the following: a tornado, a fire, inclement weather. (5) Each provider of services shall establish a written procedure providing for: administrative action against; investigating an alleged violation by; disciplinary action against; and dismissal of an employee or agent of the provider; if the employee or agent is involved in the alleged, suspected, or actual abuse, neglect, exploitation, or mistreatment of an individual or a violation of an individual’s rights. (6) Each provider of services shall establish a written procedure for employees or agents of the provider to report violations of the provider’s policies and procedures to 146 the provider. (7) Each provider of services shall establish a written procedure for the provider or for an employee or agent of the provider, for informing: APS or CPS as applicable; an individual’s legal representative, if applicable; the appropriate ombudsman;any person designated by the individual; and the provider of CMS to the individual; of a situation involving the alleged, suspected, or proven abuse, neglect, exploitation, or mistreatment of an individual or the violation of an individual’s rights. (8) Each provider will inform individuals of their right to exercise any or all guaranteed rights without: restraint; interference; coercion; discrimination; or threat of reprisal; by the provider, employee, or agent. (9) Each provider of services shall establish and make available to the individual; the written protocol for reporting required reportable unusual occurrences to FSSA DA . (10) Each provider of services shall establish and make available to the individual receiving services a written protocol informing the individual about the right to file a complaint with FSSA DA and the process of filing a complaint with FSSA DA. 10034 Provider Requirements – Individual’s “No-Show” for a Service CHOICE providers shall report individuals who do not report to a location as scheduled for a service as an unusual occurrence in accordance with the requirements of Division of Aging Incident Reporting Policies and Procedures. (Authority IC 12-10-10,455 IAC 1.2-8-2, 455 IAC 1-4-11) 10035 Legally Responsible Individuals as CHOICE Providers CHOICE-funded services may only be provided by legally responsible individuals as specified in this section. (Authority IC 12-10-10) (1) Relatives of CHOICE participants who complete the FSSA DA training program established under IC 12-10-10-9(a) are eligible for reimbursement under CHOICE for the provision of homemaker and personal care services to those participants. (2) An individual who is a legally responsible relative of an individual in need of selfdirected in-home care, including a parent of a minor individual and a spouse, is precluded from providing attendant care services for compensation 10036 Provider Requirements – Coordination of Services and Plan of Care (Authority IC 12-10-10; 455 IAC 1.2-19-1; 455 IAC 1-4-11) 147 Procedure. 1) All entities responsible for providing service to an individual shall do the following: (A) Coordinate the services provided to an individual. (B) Share documentation regarding the individual’s well-being, as required by the individual’s plan of care. 10037 Service Specific Provider Requirements – Adaptive Equipment Providers CHOICE providers of adaptive equipment shall provide this equipment (see Section 4001 of DA Operations Manual). Providers must meet requirements contained in the CHOICE guidelines as applicable to the provider. Adaptive equipment may be funded by CHOICE if the individual has no other source of funding adaptive equipment. (Authority IC 12-10-10; 455 IAC 1.2-9-6; 455 IAC 1.2-9-6; 455 IAC 1.2-20-1; 455 IAC 1.2-20-1; 455 IAC 1-4-11) 10038 Service Specific Provider Requirements – Adult Day Services Providers CHOICE providers of adult day services shall implement services in accordance with the requirements of Section 4003 of the DA Operations Manual. Adult Day Services may only be funded by CHOICE if the individual has no other source of funding. Providers must meet requirements contained in the CHOICE Guidelines as applicable to the provider. (Authority IC 12-10-10; 455 IAC 1.2-9-6; 455 IAC 1.2-20-1; 455 IAC 1-4-11) 10039 Service Specific Provider Requirements – Attendant Care CHOICE providers of attendant care services shall implement services in accordance with the requirements of Section 4007 of the DA Operations Manual. Attendant care services may only be funded by CHOICE if the individual has no other source of funding. Attendant Care Services are a HCBS Waiver service. Providers must meet requirements contained in the CHOICE Guidelines as applicable to the provider. Providers must be licensed as either a home health agency or personal services agency unless certified by FSSA (Authority IC 12-10-10; 455 IAC 1.2-9-6; 455 IAC 1.2-20-1; 455 IAC 1-4-11) 10040 Service Specific Provider Requirements – Environmental Modifications CHOICE providers of environmental modifications shall implement services in accordance with the requirements of Section 4018 of the DA Operations Manual. 148 Environmental Modification Services may only be funded by CHOICE if the individual has no other source of funding. Providers must meet requirements contained in the CHOICE Guidelines as applicable to the provider. Environmental modifications are a HCBS Waiver service. (Authority IC 12-10-10; 455 IAC 1.2-9-6; 455 IAC 1.2-20-1; 455 IAC 1-4-11) (A) Reimbursement for Environmental Modification Supports has a lifetime cap of $15,000. Service and repair up to $500 per year, outside this cap, is permitted for maintenance and repair of prior modifications. (If the lifetime cap is fully utilized, and a need is identified, the case manager will work with other available funding streams and community agencies to fulfill the need.) 10041 Service Specific Provider Requirements – Family Caregiver Support Family Caregiver Support Program services may only be funded by CHOICE if the caregiver has no other source of funding. Providers must meet requirements contained in the CHOICE Guidelines as applicable to the provider. (Authority IC 12-10-10; 455 IAC 1.2-9-6; 455 IAC 1.2-20-1; 455 IAC 1-4-11) 10042 Service Specific Provider Requirements – Home Health Services CHOICE providers of home delivered meals shall implement services in accordance with the requirements of this Section. (Authority IC 12-10-10; 455 IAC 1.2-9-6; 455 IAC 1.2-20-1; 455 IAC 1-4-11) 10043 Service Specific Provider Requirements – Home Delivered Meals CHOICE providers of home delivered meals shall implement services in accordance with the requirements of Section 8006 of the DA Operations Manual. Home Delivered Meals may only be funded by CHOICE if the individual has no other source of funding. No more than two meals per day will be reimbursed under the CHOICE program. Providers must meet requirements contained in the CHOICE Guidelines as applicable to the provider. (Authority IC 12-10-10; 455 IAC 1.2-9-6; 455 IAC 1.2-20-1; 455 IAC 1-4-11) 10044 Service Specific Provider Requirements – Homemaker CHOICE providers of homemaker services shall implement services in accordance with the requirements of Section 4013 of the DA Operations Manual. Homemaker Services may only be funded by CHOICE if the individual has no other source of funding. Providers must meet requirements contained in the CHOICE Guidelines as applicable to the provider. 149 Providers must be licensed as a home health agency or a personal services agency through ISDH (Authority IC 12-10-10; 455 IAC 1.2-9-6; 455 IAC 1.2-20-1; 455 IAC 1-4-11) 10045 Service Specific Provider Requirements – Home Repair and Maintenance Services CHOICE providers of home repair and maintenance services shall meet specified requirements and develop and implement safety and security policies and procedures specified in Section 4014 of the DA Operations Manual Home Repair and Maintenance Services may only be funded by CHOICE if the individual has no other source of funding. Providers must meet requirements contained in the CHOICE Guidelines as applicable to the provider (Authority IC 12-10-10; 455 IAC 1.2-9-6; 455 IAC 1.2-20-1; 455 IAC 1-4-11) 10046 Service Specific Provider Requirements – Information and Assistance CHOICE providers of information and assistance services shall meet specified requirements and develop and implement safety and security policies and procedures specified in Section 4016 of the DA Operations Manual. Information and Assistance Services may only be funded by CHOICE if the individual has no other source of funding. Providers must meet requirements contained in the CHOICE Guidelines as applicable to the provider. (Authority IC 12-10-10; 455 IAC 1.2-9-6; 455 IAC 1.2-20-1; 455 IAC 1-4-11) 10047 Service Specific Provider Requirements – Legal assistance services CHOICE providers of legal assistance services shall meet specified requirements and develop and implement safety and security policies and procedures specified in Section 4017 of the DA Operations Manual. Legal Assistance Services may only be funded by CHOICE if the individual has no other source of funding. Providers must meet requirements contained in the CHOICE Guidelines as applicable to the provider. (Authority IC 12-10-10; 455 IAC 1.2-9-6; 455 IAC 1.2-20-1; 455 IAC 1-4-11) 10048 Service Specific Provider Requirements – Nutrition Education CHOICE providers of nutrition education services shall meet specified requirements and develop and implement safety and security policies and procedures specified in this Section. (Authority IC 12-10-10; 455 IAC 1.2-9-6; 455 IAC 1.2-20-1; 455 IAC 1-4-11) 10049 Service Specific Provider Requirements – Outreach Services CHOICE providers of outreach services shall meet specified requirements and develop 150 and implement safety and security policies and procedures specified in Section 4021 of the DA Operations Manual. Outreach Services may only be funded by CHOICE if the individual has no other source of funding. Providers must meet requirements contained in the CHOICE Guidelines as applicable to the provider. (Authority IC 12-10-10; 455 IAC 1.2-9-6; 455 IAC 1.2-20-1; 455 IAC 1-4-11) 10050 Service Specific Provider Requirements – Personal Emergency Response Systems Personal Emergency Response Systems providers must meet specified requirements to provide CHOICE-funded services. (Authority IC 12-10-10; 455 IAC 1.2-18-1; 455 IAC 1-4-11) Procedure. Personal Emergency Response System (PERS) is an electronic device which enables certain individuals at high risk of institutionalization to secure help in an emergency. The individual may also wear a portable help button to allow for mobility. The system is connected to the person’s phone and programmed to signal a response center once a “help” button is activated. The response center is staffed by trained professionals. (1) (A) Service Requirements/Allowable Activities: PERS consists of: i Device Installation service; and Ongoing monthly maintenance of device. (2) (A) (3) Service authorization requirements: The case manager authorizes PERS. Limitations/Exclusions (A) PERS is limited to those individuals who live alone, or who are alone for significant parts of the day, and have no regular caregiver for extended periods of time, and who would otherwise require extensive supervision. (B) Systems must meet Underwriters Laboratory (UL) and FCC regulations prior to installation. (C) All devices must meet applicable state and local requirements and regulations for licensure and/or certification for the type of system for which the contractor is providing. (4) (A) PERS providers must Meet all the provider requirements contained in the CHOICE guidelines 151 as applicable to the provider; (B) Be Qualified Contractors, Special Equipment Suppliers, Businesses, Agencies, Organizations, or Individuals; and (C) Be knowledgeable of applicable standards of manufacturing, design, and installation of the specific device installed. (5) Documentation requirements (A) PERS must be provided in accordance with the written Plan of Care addressing specific needs determined by the individual’s assessment. (6) (A) Billing requirements. PERS is billing depends on the funding source. 10051 Service Specific Provider Requirements – Pest Control Services CHOICE providers of pest control services shall implement services in accordance with the requirements of this Section. (Authority IC 12-10-10; 455 IAC 1.2-9-6; 455 IAC 1.2-20-1; 455 IAC 1-4-11) 10052 Service Specific Provider Requirements – Respite Care CHOICE providers of respite services shall meet specified requirements and develop and implement safety and security policies and procedures. (Authority IC 12-10-10; 455 IAC 1.2-9-6; 455 IAC 1.2-20-1; 455 IAC 1-4-11) Procedure. (1) Respite Care services are those services that are provided temporarily or periodically in the absence of the usual caregiver. (2) Respite Care may be provided in the following locations: in an individual’s home, in the private home of the caregiver, in an adult foster care home, or in a Medicaid certified nursing facility. (3) The level of professional care provided under respite care services depends on the needs of the client. (A) A client requiring assistance with bathing, meal preparation and planning, specialized feeding, such as a client who has difficulty swallowing, refuses to eat, or does not eat enough; dressing or undressing; hair and oral care; and weight bearing transfer assistance should be considered for respite home health aide under the supervision of a registered nurse. (B) A client requiring infusion therapy; venipuncture; injection; oral medication; Hoyer lift; wound care for surgical, decubitus, incision, and so forth; ostomy care; and tube feedings should be considered for respite nursing services. (4) Service Requirements/Allowable Activities: (A) Homemaker services 152 (B) Attendant care (C) Home health aide services (D) Skilled nursing services (E) Nursing facility services. (5) Service authorization requirements: (A) The case manager authorizes respite care, except when required to be provided in a nursing facility. i The case manager is required to receive prior authorization from the Indiana Family and Social Services Administration (IFSSA) with a completed Request for Approval to Authorize Services Form before Respite Care may be provided in a nursing facility. (6) Limitations/Exclusions (B) Respite care shall not be used as day/child care to allow the persons normally providing care to go to work. (C) Respite care shall not be used as day/child care to allow the persons normally providing care to attend school. (D) Respite care shall not be used to provide service to a member while member is attending school. (E) Respite care may not be used to replace skilled nursing services that should be provided under the Medicaid State Plan. (F) Respite care must not duplicate any other service being provided under the individual’s plan of care. (G) If an individual’s need for respite care services can be met by an LPN, but an RN provides the service, the service may only be billed at the LPN rate. (4) Respite care providers must - (A) Meet all the provider requirements contained in the CHOICE guidelines as applicable to the provider; (B) i ii iii iv Be a: Community Developmental Disabilities Agency; or Licensed Home Health Agency; or Medicaid Certified Nursing Facility; or Individual . (C) Family members who are providing care giving to the participant may not be paid to provide respites services (since respite services are designed to relieve the 153 caregiver during periods of brief absence from the individual). (D) Providers must be qualified to provide the “level” of respite care services authorized by the case manager, or by FSSA DA for NF services. (5) Documentation requirements (A) Respite care must be provided in accordance with the written Plan of Care addressing specific needs determined by the individual’s assessment. (B) Documentation must include the following elements: the reason for the respite, the location where the service was rendered and the type of respite rendered. For example, respite Home Health Agency (HHA). i Documentation should include date and time, and at least the last name and first initial of the respite care provider making the entry. ii If the person providing the service is a professional, the title of the individual must also be included. For example, if a nurse is required to perform the service then the RN title would be included with the name. (6) Billin g requirements. (A) Billing depends on the funding source. 10053 Service Specific Provider Requirements – Supplies CHOICE providers of supplies shall implement services in accordance with the requirements of this Section. (Authority IC 12-10-10; 455 IAC 1.2-9-6; 455 IAC 1.2-20-1; 455 IAC 1-4-11) 10054 Service Specific Provider Requirements – Therapy Services CHOICE providers of therapy services shall meet specified requirements and develop and implement safety and security policies and procedures specified in this Section. (Authority IC 12-10-10; 455 IAC 1.2-9-6; 455 IAC 1.2-20-1; 455 IAC 1-4-11) 10055 Service Specific Provider Requirements – Transportation CHOICE providers of transportation services shall meet specified requirements and develop and implement safety and security policies and procedures specified in this Section. (Authority IC 12-10-10; 455 IAC 1.2-12-1; 455 IAC 1-4-11) Procedure. (1) The following provider types may be certified to provide transportation services: (A) Qualified public and private carriers. (B) Qualified individuals. i Individual personnel providing transportation must meet the 154 following requirements. (a) Have a valid Operator’s license under IC 9-24-3 for individuals using private vehicles. (b) Have a valid Chauffeur’s license under IC 9-24-4 or an Indiana Public Passenger Chauffeur’s license when driving a vehicle designed to transport fewer than 15 people (IC 9-24-5). (c) Have a valid Indiana Commercial Driver’s license when operating a vehicle designed to transport a minimum of 15 people (IC 9-246). (d) Have a safe, legal driving record. (e) Have auto insurance, including liability insurance. (f) Have properly licensed and maintained vehicles. (2) An approved provider of transportation services or its agent shall do the following: (A) Maintain the vehicle or vehicles used in the provision of transportation services in good repair. (B) Retain and make available upon request, records of regular and appropriate maintenance. (C) i ii Assure the vehicle used for transportation services is properly registered: with the Indiana Bureau of Motor Vehicles; or in the state in which the owner of the vehicle resides. (D) Retain and make available upon request, documentation confirming the provider has the appropriate insurance as required under Indiana law. 10056 Service Specific Provider Requirements for Self-Directed In-Home Care CHOICE funded services may only be provided by authorized service providers. (Authority IC 12-10-10; IC 12-10-17.1; 455 IAC 1-4-3; 455 IAC 1-4-11) Procedure (1) An individual who is a legally responsible relative of an individual in need of selfdirected in-home care, including a parent of minor individual and a spouse, is precluded from providing attendant care services for compensation. (2) An individual may not provide attendant care services for compensation for an individual in need of self-directed in-home care services unless the individual is registered. (A) An individual who desires to provide attendant care services must register with the FSSA DA or with an organization designated by the division. 155 (B) The FSSA DA shall register an individual who provides the following: i A personal résumé containing information concerning the individual's qualifications, work experience, and any credentials the individual may hold. The individual must certify that the information contained in the résumé is true and accurate. ii The individual's limited criminal history check from the Indiana central repository for criminal history information under IC 10-13-3 or another source allowed by law. (a) The limited criminal history check and report must be updated every two (2) years (b) Individuals who have lived outside of Indiana the two years prior to registering will have to have a National criminal history check. iii If applicable, the individual's state nurse aide registry report from the State Department of Health. This subdivision does not require an individual to be a nurse aide. iv Three (3) letters of reference. v A registration fee. The FSSA DA establishes the amount of the registration fee. vi Proof that the individual is at least eighteen (18) years of age. vii Any other information required by the FSSA DA. (C) A registration is valid for two (2) years. (3) A personal services attendant may renew the personal services attendant's registration by updating any information in the file that has changed and by paying the fee required under subsection. (4) A personal services attendant who is hired by the individual in need of selfdirected in-home care is an employee of the individual in need of self-directed in- home care. (A) The division is not liable for any actions of a personal services attendant or an individual in need of self-directed in-home care. (B) A personal services attendant and an individual in need of self-directed in-home care are each liable for any negligent or wrongful act or omission in which the person personally participates. (5) The FSSA DA and any organization designated by the FSSA DA shall maintain a file for each personal services attendant that contains: (A) comments related to the provision of attendant care services submitted by an individual in need of self-directed in-home care who has employed the personal services attendant; and (B) the items described in subsection (2). 10057 Provider Requirements – Warranties Warranties are required for applicable CHOICE-funded services. 156 (Authority IC 12-10-10; 455 IAC 1.2-18-1; 455 IAC 1-4-11) Procedure. (1) All applicable services provided to an individual under the CHOICE program including, but not limited to: durable medical equipment; personal emergency response system; home modification; and vehicle modifications; shall supply a warranty effective for at least one (1) year from the date of new installation or the date the individual received the new item, whichever is applicable. 10058 Provider Monitoring CHOICE providers are routinely monitored to ensure compliance with applicable requirements of this Chapter. Primary monitoring of CHOICE providers shall be a function of the Area Agencies on Aging. (Authority IC 12-10-10; 455 IAC 1-4-11; 455 IAC 1.2, Section 4) Procedure. (1) FSSA DA periodically monitors CHOICE providers: (A) As stated in the current executed contract or provider agreement. (B) Upon receiving a complaint or report alleging a provider’s noncompliance with the requirements of the CHOICE program. i If a person other than an individual receiving service files a complaint, FSSA DA shall notify the person filing the complaint of completion of the following: (a) FSSA DA monitoring as a result of the complaint. (b) monitoring. Any corrective action by the provider as a result of FSSA DA (C) As frequently as deemed necessary by FSSA DA. (D) According to FSSA DA approved policy. (2) FSSA DA monitors compliance with the requirements of the CHOICE program through any of the following means: (A) Requesting and obtaining information from the provider. (B) On-site inspections. (C) applicable. Meeting with an individual or the individual’s legal representative as (D) Reviewing provider records and the records of an individual. (E) Following-up on completed inspections, as frequently as deemed 157 necessary by the FSSA DA, to determine compliance after submission of a corrective action plan by a provider to the FSSA DA. (3) The provider will submit to the FSSA DA any requested documentation within ten (10) days from the date that the provider receives a report of findings unless otherwise specified. (4) After an on-site inspection, FSSA DA shall issue a written report, which shall: (A) Document the findings made during monitoring. (B) Identify necessary corrective action. (C) Give the provider ten (10) days in which to complete the corrective action plan unless otherwise specified. (D) Identify documentation needed from the provider to support the provider’s completion of the corrective action plan. (E) Be submitted to the provider. (5) A provider shall do the following: (A) If requested, complete a corrective action plan to the reasonable satisfaction of FSSA DA within: i ii the time period identified in the corrective action plan; or another time period agreed upon by the FSSA DA. (B) Notify FSSA DA upon the completion of a corrective action plan. (C) Provide FSSA DA with all requested documentation. 10059 Provider Non-Compliance with Requirements CHOICE providers who do not comply with CHOICE program requirements will be sanctioned up to and including decertification. (Authority IC 12-10-10; 455 IAC 1-4-11; 455 IAC 1.2, Section 5) Procedure. (1) If a provider does not comply with the requirements of the CHOICE program or does not submit and complete an acceptable, approved corrective action plan to the reasonable satisfaction of FSSA DA within the time specified, FSSA DA shall not authorize either or both of the following: (A) The continuation of services to an individual or individuals by the provider if the services do not comply with the specified requirements. (B) The receipt of services by individuals not already receiving services from the provider at the time the determination is made that the provider did not implement a corrective action plan to the reasonable satisfaction of FSSA DA. 158 (2) The decertification process is initiated by the Area Agency on Aging and the FSSA DA will assist with the appeals process if necessary. (3) FSSA DA shall give written notice of FSSA DA’s action specific to provider noncompliance to the following: (A) The provider. (B) The individual receiving services from the provider. (C) The individual’s legal representative, if applicable. (4) The written notice shall include the following: (A) complied. The CHOICE program requirements with which the provider has not (B) The effective date, with at least thirty (30) days notice, of FSSA DA’s action specific to the non-compliance(s). (C) The need for planning to obtain HCBS for an individual or individuals. (D) The provider’s right to seek administrative review of FSSA DA’s action. 10060 Provider Non-Compliance with Requirements That Endangers the Health or Welfare of an Individual Such That an Emergency Exists CHOICE providers are subject to special and expedited sanctions when the provider’s noncompliance with CHOICE program requirements endangers the health or welfare of an individual such that an emergency exists. (Authority IC 12-10-10; 455 IAC 1-4-11; 455 IAC 1.2, Section 6) Procedure. (1) If a provider’s noncompliance with CHOICE program requirements endangers the health or welfare of an individual such that an emergency exists, as determined by FSSA DA or its designee, FSSA DA may enter an order for any of the following: (A) Termination of continued authorization for the provider to: i endangered; or ii serve any individual whose health or safety is being seriously provide any services under a HCBS program. (B) Denial of authorization for the receipt of services by individuals not already receiving services from the provider at the time FSSA DA determines that a provider’s noncompliance with this article endangers the health or safety of an individual. (2) Any action taken under subsection (1) shall remain in effect until such time FSSA 159 DA determines the provider’s noncompliance is no longer endangering the health or safety of an individual. (3) FSSA DA shall give written notice of an order under subsection (1) to the following: (A) The provider. (B) The individual receiving services from the provider. (C) The individual’s legal representative, as applicable. (4) The written notice shall include the following: (A) not complied. The requirements of the CHOICE program with which the provider has (B) A brief statement of the facts and the law leading to FSSA DA’s determination that an emergency exists. (C) The need to immediately obtain services that comply with this article for an individual or individuals. (D) The provider’s right to seek administrative review of FSSA DA’s action. (5) The order issued under subsection (1) shall expire on the earlier of the following: (A) The date FSSA DA determines that an emergency no longer exists. (B) Ninety (90) days. (6) During the pendency of any related proceedings under IC 4-21.5, FSSA DA may renew an emergency order for successive ninety (90) day periods. 10061 Provider – Revocation of Approval CHOICE provider approval may be revoked by the FSSA DA under specified circumstances. (Authority IC 12-10-10; 455 IAC 1-4-11; 455 IAC 1.2, Section 7) Procedure. (1) The FSSA DA may revoke the approval of a CHOICE provider for any of the following reasons: (A) The provider’s repeated noncompliance with CHOICE requirements. (B) The provider’s continued noncompliance with CHOICE requirements. (C) The provider’s noncompliance with CHOICE requirements that endangers the health or welfare of an individual. 10062 Provider Appeals 160 If a CHOICE provider has an executed contract or provider agreement to provide a service to an individual, the provider has the right to appeal decisions that adversely affect the service provider. (Authority IC 12-10-10; 455 IAC 1-4-11; 455 IAC 1.2-7-1) Procedure. (1) The service provider shall make a written request for an appeal hearing to the secretary of FSSA within fifteen (15) days of the date of an adverse decision. (2) The request must: (A) include a statement indicating with reasonable particularity the issue the service provider wishes to be reviewed; and (B) be signed and dated by the service provider. (3) Appeal proceedings will be conducted by a FSSA-appointed administrative law judge (ALJ) under IC 4-21.5. (A) Notice of the ALJ’s decision shall be sent also to any listed adversely affected party. 10063 HCBS Providers – Resolution of Disputes If a dispute arises between or among providers, the dispute resolution process set out in this section shall be implemented. Authority IC 12-10-10; 455 IAC 1.2-9-3; 455 IAC 1-4-11) Procedure. (1) The resolution of a dispute shall be designed to address an individual’s needs. (2) The parties to the dispute and the individual shall attempt to resolve the dispute informally through an exchange of information and possible resolution. (3) If these parties are not able to resolve the dispute within fifteen (15) calendar days, each party must document, in writing, the issues in the dispute, their positions and their efforts to resolve the dispute and the parties shall refer the dispute to FSSA DA or its designee for resolution in coordinating the individual’s needs. (4) The parties shall abide by the decision. (5) A party adversely affected or aggrieved by FSSA DA’s decision may request an administrative review of the decision under 455 IAC 1.2-7-1 within fifteen (15) calendar days after the party receives written notice of the recommendation. (A) Administrative review proceedings shall be conducted under IC 4-21.5. 161 Attachment 1: CHOICE Eligibility Asset Attestation Form Case manager – Record countable assets as determined by DFR on the basis of a Medicaid eligibility determination below or attaché asset print out from DFR. Date of determination Note: If more than ninety days old, the applicant must be referred to DFR for a new determination. I, (insert individual’s name) certify: 1) That the items listed as assets, truthfully represent my total and current assets. 2) That I will notify my case manager should my assets change prior to or at any time during receipt of CHOICE services. 3) That I will be responsible for paying for CHOICE services if my assets change and are determined to exceed the allowable limit of $500,000 and I did knowingly withhold such information. Signature of Individual or representative Date 162 Attachment 2: Cost-Sharing Detail Categories of income to be recorded in INsite: Interest Bearing Accounts Pension Social Security Retirement Social Security Disability SSI VA Benefit Child Support Alimony Earnings, Salaries, Tips Worker's Compensation Net Rental Income Deemed Value From Fixed Assets - Interest earned from any source, including the following: o saving and checking accounts o interest bearing accounts such as CDs, IRAs, stock/bonds - Net amount of any pension received by individual. These may be from former employment or a widow/widower. - Social Security pension. - Social Security Disability pension. - Supplemental Security Income check. - Veteran's Benefit. - Child support. - Alimony. Income of Parents or Spouse Disability Insurance Other Income Allowable Deductions from Income Recorded in INsite Health Insurance Premiums LTC Medical Care Psychological Care Medicare Premiums Unpaid Medical/Psych. Bills Individual-Paid Services Other Allowable Payments 163 Table 1: Cost Share Amounts Based on Final Income (Income minus Deductions) Percent Individual State Percent Individual State Percent Individual State of of of Share % Share Share % Share Share % Share Poverty Poverty Poverty % % % 151 0.0 100.0 219 34.0 66.0 287 68.0 32.0 152 0.5 99.5 220 34.5 65.5 288 68.5 31.5 153 1.0 99.0 221 35.0 65.0 289 69.0 31.0 154 1.5 98.5 222 35.5 64.5 290 69.5 30.5 155 2.0 98.0 223 36.0 64.0 291 70.0 30.0 156 2.5 97.5 224 36.5 63.5 292 70.5 29.5 157 3.0 97.0 225 37.0 63.0 293 71.0 29.0 158 3.5 96.5 226 37.5 62.5 294 71.5 28.5 159 4.0 96.0 227 38.0 62.0 295 72.0 28.0 160 4.5 95.5 228 38.5 61.5 296 72.5 27.5 161 5.0 95.0 229 39.0 61.0 297 73.0 27.0 162 5.5 94.5 230 39.5 60.5 298 73.5 26.5 163 6.0 94.0 231 40.0 60.0 299 74.0 26.0 164 6.5 93.5 232 40.5 59.5 300 74.5 25.5 165 7.0 93.0 233 41.0 59.0 301 75.0 25.0 166 7.5 92.5 234 41.5 58.5 302 75.5 24.5 167 8.0 92.0 235 42.0 58.0 303 76.0 24.0 168 8.5 91.5 236 42.5 57.5 304 76.5 23.5 169 9.0 91.0 237 43.0 57.0 305 77.0 23.0 170 9.5 90.5 238 43.5 56.5 306 77.5 22.5 171 10.0 90.0 239 44.0 56.0 307 78.0 22.0 172 10.5 89.5 240 44.5 55.5 308 78.5 21.5 173 11.0 89.0 241 45.0 55.0 309 79.0 21.0 174 11.5 88.5 242 45.5 54.5 310 79.5 20.5 175 12.0 88.0 243 46.0 54.0 311 80.0 20.0 176 12.5 87.5 244 46.5 53.5 312 80.5 19.5 177 13.0 87.0 245 47.0 53.0 313 81.0 19.0 178 13.5 86.5 246 47.5 52.5 314 81.5 18.5 179 14.0 86.0 247 48.0 52.0 315 82.0 18.0 180 14.5 85.5 248 48.5 51.5 316 82.5 17.5 181 15.0 85.0 249 49.0 51.0 317 83.0 17.0 182 15.5 84.5 250 49.5 50.5 318 83.5 16.5 183 16.0 84.0 251 50.0 50.0 319 84.0 16.0 184 16.5 83.5 252 50.5 49.5 320 84.5 15.5 185 17.0 83.0 253 51.0 49.0 321 85.0 15.0 186 17.5 82.5 254 51.5 48.5 322 85.5 14.5 187 18.0 82.0 255 52.0 48.0 323 86.0 14.0 188 18.5 81.5 256 52.5 47.5 324 86.5 13.5 189 19.0 81.0 257 53.0 47.0 325 87.0 13.0 190 19.5 80.5 258 53.5 46.5 326 87.5 12.5 191 20.0 80.0 259 54.0 46.0 327 88.0 12.0 192 20.5 79.5 260 54.5 45.5 328 88.5 11.5 193 21.0 79.0 261 55.0 45.0 329 89.0 11.0 194 21.5 78.5 262 55.5 44.5 330 89.5 10.5 195 22.0 78.0 263 56.0 44.0 331 90.0 10.0 196 22.5 77.5 264 56.5 43.5 332 90.5 9.5 164 197 198 199 23.0 23.5 24.0 77.0 76.5 76.0 265 266 267 57.0 57.5 58.0 43.0 42.5 42.0 333 334 335 91.0 91.5 92.0 9.0 8.5 8.0 200 201 202 203 204 205 206 207 208 209 210 211 212 213 214 215 216 217 218 24.5 25.0 25.5 26.0 26.5 27.0 27.5 28.0 28.5 29.0 29.5 30.0 30.5 31.0 31.5 32.0 32.5 33.0 33.5 75.5 75.0 74.5 74.0 73.5 73.0 72.5 72.0 71.5 71.0 70.5 70.0 69.5 69.0 68.5 68.0 67.5 67.0 66.5 268 269 270 271 272 273 274 275 276 277 278 279 280 281 282 283 284 285 286 58.5 59.0 59.5 60.0 60.5 61.0 61.5 62.0 62.5 63.0 63.5 64.0 64.5 65.0 65.5 66.0 66.5 67.0 67.5 41.5 41.0 40.5 40.0 39.5 39.0 38.5 38.0 37.5 37.0 36.5 36.0 35.5 35.0 34.5 34.0 33.5 33.0 32.5 336 337 338 339 340 341 342 343 344 345 346 347 348 349 350 351 92.5 93.0 93.5 94.0 94.5 95.0 95.5 96.0 96.5 97.0 97.5 98.0 98.5 99.0 99.5 100.0 7.5 7.0 6.5 6.0 5.5 5.0 4.5 4.0 3.5 3.0 2.5 2.0 1.5 1.0 0.5 0.0 165







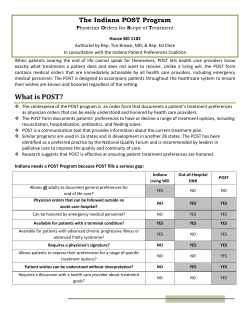


© Copyright 2026