
Personnel Policy Manual ! M. Alexandrunas, DMD-Grove City Dental Expressions, Inc.
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! Personnel Policy Manual M. Alexandrunas, DMD-Grove City Dental Expressions, Inc. ! ! ! Manuals and services are intended to provide a concise, practical guide to personnel administration and procedures, as well as an explanation of some of the common pitfalls that have caused substantial or recurring liability for employers. Manuals and services are not meant to substitute for legal advice, nor should they be viewed as a treatise on the laws, legal advice, or legal opinions of any kind. ! The information and references contained herein may be materially affected by legislative, regulatory, and judicial developments, and reflect interpretation of such at the time of publication. does not warrant its products and services to necessarily meet your individual requirements or that access to services may not be delayed or interrupted or that products or services will not be error-free. excludes and expressly disclaims all express and implied warranties not stated herein. Neither Bent Ericksen & Associates nor the authors assume any liability about the use of any of the policies or forms. The manual is sold with the understanding that the publisher is not rendering professional legal services. If legal advice is required, the services of a competent attorney should be retained . ! State and local laws vary significantly and are subject to change. It is the responsibility of the user to ensure that final policies comply with all current laws that apply to the employer’s operations. Before adopting any personnel policies, employers may want to have them reviewed by experienced legal counsel to assure compliance with all applicable laws. ! Throughout this manual, M. Alexandrunas, DMD-Grove City Dental Expressions, Inc may be referred to as GCDE. ! MISSION STATEMENT To the patients of Grove City Dental Expressions our main purpose is the best care for your oral health and well being. Our principal goal is to preserve your natural teeth. We use the most current dental procedure and products to maximize your restoration life expectancy. ! We provide exceptional dental care through our high-tech, high-touch philosophy. We will equip our office with state of the art equipment. Digital x-rays, an intra-oral camera and a powerful clinical software system will allow us to diagnosis and treatment plan better than ever. ! We seek out continuing education courses that matter to our patients. We are constantly attending new courses that engage and challenge our thinking, helping us to be one of the front runners of the dental industry. Implementation of these new idea’s is done quickly as to bring these new procedure and products to you our patients. ! Providing great customer service is the backbone to our practice. We understand that you have many options for your dental care. Dr. Alexandrunas and his staff have implemented many protocols to ensure that your visit is enjoyable and relaxing. We take the time that is needed to give each patient our individual attention and strive to learn about each patient on a personal level. Our management software aids in patient follow up and in the accuracy of your account. ! Our practice is growing and will continue to grow in this community because we care about you, our patient. We care about the high quality of dentistry we are providing and we are confident that our patients will continue to refer other great people so that they too can become part of Grove City Dental ! ! INTRODUCTION TO POLICIES This manual serves as a ready reference for doctor and employees. It is a summary of personnel policies and procedures, and employee benefits. It is designed to be a working guide for the administration of a consistent and fair personnel program. Please read it carefully and learn its contents. ! The policies are intended to: !Prevent misunderstandings that might arise from unwritten policies, inconsistently applied policies, or lack of proper communications !Eliminate the need to make hasty decisions in matters of personnel policies !Assure uniformity and fairness throughout the practice !Communicate to everyone within the employment relationship the rights and responsibilities of all ! The policies described are not an expressed or implied contract of employment between the employer and the employees and do not in any way imply or create any rights, contractual or otherwise. We reserve the right to modify, suspend, rescind, interpret and administer any of the policies, procedures, terms, conditions, and language of any or all parts of this manual. However, the “at-will” employment policy can be changed only by written notification signed by the employer. To be binding, the specific terms or benefits of any employment must be in writing and signed by the employer/manager. ! Examples of the types of employment decisions that are within the sole discretion of the employer include: "Hire and discharge "Compensation "Benefits "Discipline "Layoff "Work schedules "Work assignments "“Extenuating circumstances” and case-by- case decisions "Job responsibilities "Anything else that the employer may determine to be necessary for the safe, efficient, and economic operation of the business ! This policy manual replaces all earlier policy manuals, and takes precedence over all memoranda and oral descriptions of personnel policies, practices, and procedures. Outdated manuals should be removed and saved for later reference, if needed. ! You will be informed of any revisions to these policies as they occur. Please keep current with the changes by reading the manual periodically. As policies are updated the latest revision date will be shown at http:// dentist-grovecity.com/human-resources-manual/. ! 1 The policy manual is located in a place where it is easily accessible to everyone. Please familiarize yourself with these policies, and sign a copy of the Employee Acknowledgment Form (see Form #101). The form is also located at the end of the 900 section of this manual. If you have any questions, please feel free to ask. ! ! DISTRIBUTION OF MANUAL This Personnel Policy Manual is the property of the practice. A copy is located at http://dentistgrovecity.com/human-resources-manual/ for easy referral. Each employee is responsible for keeping up with recent changes to the manual. It will be necessary that it is reviewed yearly. Form #301 must be signed by each employee yearly stating they have reviewed the manual. ! ! OUR PHILOSOPHY Our aim is to provide each patient with the finest care in a professional environment that inspires trust and confidence. We have learned that a patient follows the doctor's recommendations in direct proportion to the level of trust perceived to exist between the doctor and the employees. We therefore encourage you to share your ideas, opinions, and feelings so we can be sure to keep open the channels of communication. ! A professional practice is a business that must be managed efficiently and profitably if we are to continue serving our community with quality treatment. We invite and appreciate your contributions and suggestions toward greater office efficiency. Our fees are fair and reflect the care and expertise with which we treat each patient. We strive: !To help our patients achieve the highest level of health possible !To be committed to excellence in all of our services to the patient !To treat the patient's needs with the highest level of care, skill, and comfort !To participate enthusiastically, honestly, and positively in all areas of the practice !To change, grow, and evolve with our profession and society !To enhance the lives of all those with whom we come in contact !To foster an environment that supports and encourages all the above !To maintain a safe and healthy environment for our patients and ourselves !To be part of the solution of any conflict or problem solving, to share our ideas and feelings, and to confront any issue in a win-win manner in order to maintain office harmony and teamwork ! ! EMPLOYMENT PRACTICES EMPLOYER—EMPLOYEE RELATIONS We believe that the strength and future growth of the practice depends directly upon the contributions made by every employee. We also know that high productivity and efficiency depend on individual job satisfaction and happiness. ! In our effort to implement fair and effective personnel policies, we pledge to: !Hire people based on their qualifications and potential contributions to the practice !Provide employees with avenues for addressing job-related concerns !Recognize each employee as an individual and valuable member of the team !Maintain safe and healthful working conditions !Conduct Performance Reviews periodically, so employees will know where they stand regarding their work performance and extend guidance and assistance as needed !Provide a competitive compensation package based largely on industry standards in the community and the quality of the employee’s work performance !Welcome your input and suggestions ! ! ! Your responsibilities are to: !Be professional and honest in all business dealings on behalf of the practice !Keep all business and proprietary information in strictest confidence. !Give a productive day's work commensurate with your individual skills and abilities !Be friendly and courteous to other employees and patients !Adhere to office policies !Address complaints or grievances through established channels (See Problem Resolution Procedure) The practice assumes responsibility to: !Schedule hours of work, and to make changes in the work schedule !Change work assignments or job classifications as needed !Change office policies as needed taking into consideration internal circumstances, competitive forces, and economic conditions !Dismiss, assign, supervise and discipline as necessary !Decide and act whenever it is in the best interest of the practice and employees ! NEW HIRE REPORTS The federal “Personal Responsibility and Work Opportunity Reconciliation Act” (PRWORA), requires all states to operate a child support enforcement program. Under PRWORA, all employers must report new hires to their state within 20 days of hiring. Employers may use W-4 or equivalent forms for new hire reporting purposes, at the employer’s option. Certain states encourage use of the forms developed for their own new hire reporting programs for ease of processing. ! ! ! The following information must be reported: ! 3 !200 ! ! ! EMPLOYMENT PRACTICES "Employee's full first and last names, social security number, home address and start of work date "Employer's name, address, account number, and Federal Employer Identification Number IMMIGRATION LAW COMPLIANCE All employers are required to comply with the federal immigration laws. In keeping with this obligation, all new employees must fill out an I-9 form and provide satisfactory evidence of identity and legal authority to work in the United States no later than three business days after beginning the new job. All offers of employment and continued employment are contingent upon presenting such proof. ! ! EQUAL OPPORTUNITY EMPLOYMENT POLICY ! ! “AT-WILL” EMPLOYMENT It is our policy to provide equal employment opportunities to qualified persons without regard to race, creed, color, gender, age (over 40), national origin, religion, physical or mental disability, medical condition, marital status, pregnancy, citizenship, veteran's status, and sexual orientation1 as required by state and federal laws. This will extend into all areas of the employment relationship, including promotions, wages, benefits, and all other privileges, terms, and conditions of employment. You are free to terminate your employment with the practice at any time, with or without a reason, and the employer has the right to terminate your employment at any time, with or without reason. Therefore, employment with the practice is not for a specified term and can be terminated “at-will" by either party. This employment policy includes all employees including those presently employed by the practice. No employee or representative of the practice, other than its owner, has the authority to enter into any agreement for employment for any specified period of time, or to make any agreement contrary to the foregoing. ! The “at-will” policy constitutes an integrated agreement with respect to the nature of the employment relationship. There are no other oral or collateral agreements regarding this issue. These provisions supersede all existing policies and practices and may not be amended or added to without the express written approval of the employer. ! ! BONDING OF EMPLOYEES Bonding is a precautionary measure to insure adequate protection of property, personnel, and assets. This measure helps insure employer and employees against the intentional or accidental loss of property, including embezzlement, caused by the bonded employee. Certain employees who have specific responsibilities within the office may be bonded. ! ACCOMMODATION OF INDIVIDUALS WITH DISABILITIES (This Policy Only Applies To Employers with 15 or More Employees) 1 Many states currently have laws that ban bias based on sexual orientation and those that do are increasing. Currently they include: California, Connecticut, District of Columbia, Hawaii, Massachusetts, Minnesota, Nevada, New Hampshire, New Jersey, Rhode Island, Vermont, and Wisconsin. Laws change constantly. Check with your local state Labor Board periodically regarding the protected classes in your state. ! 4 !201 ! ! EMPLOYMENT PRACTICES The practice complies with the Americans with Disabilities Act (ADA), and applicable state and local laws providing for nondiscrimination in employment against qualified individuals with disabilities. We will provide reasonable accommodation for such individuals in accordance with these laws. It is our policy to: "Ensure that qualified individuals with disabilities are treated in a nondiscriminatory manner during the pre-employment process and in all conditions of employment if hired. "Administer medical examinations (a) to applicants only after conditional offers of employment have been extended, and (b) to employees only when justified by business necessity, such as for a second medical opinion or a fitness-for-duty exam, or as part of a voluntary annual physical examination program. "Keep all medical-related information confidential in accordance with the requirements of the ADA and retain such information in separate confidential files. "Notify individuals with disabilities that we provide reasonable accommodation to qualified individuals with disabilities, by including this policy in the Employee Policy Manual and by posting the Equal Employment Opportunity Commission's poster on not discriminating against individuals with disabilities and other protected groups conspicuously throughout our facilities. ! Procedure for Requesting an Accommodation—qualified individuals with disabilities must make requests for reasonable accommodation. We will then meet with the individual to identify the precise limitations resulting from the disability and the potential accommodation the practice might be able to make. ! Items to consider are: The nature and cost of the accommodation, the practice’s overall financial resources, the effect on the other employees’ ability to perform their duties, and the overall impact on the practice. ! The employee will be informed of the decision. If the accommodation request is denied, the decision may be appealed by submitting a written request. After reviewing the appeal, we will notify the employee of the decision, which is final. ! ! HARASSMENT It is our policy to provide a work environment that is free from any form of sexual, religious, or other forms of illegal harassment. An annual Harassment can take many forms: actions that may be acceptable to one person may cause another to feel uneasy or uncomfortable. Jokes, name calling, etc., especially relating to protected characteristics are prohibited. Sexual harassment includes but is not limited to: verbal, physical, or visual behavior of a sexual nature; graphic or suggestive comments about an individual's dress or body, or actual or perceived sexual orientation; making unwanted sexual advances and requests for sexual favors where either (1) submission to such conduct is made an explicit or implicit term or condition of employment; (2) submission to or rejection of such conduct by an individual is used as the basis for employment decisions affecting such individual; or (3) such conduct has the purpose or effect of substantially interfering with an individual's work performance or creating an intimidating, hostile, or offensive working environment. ! Any incident of sexual, religious, race, age, nationality or other types of harassment, including threats, intimidation and assault to our employees or any other person by our employees or any other person, must be reported immediately to the person(s) listed on the Designated Name page which is the last page of this manual. The report should state the time, place, the type of harassment, the person or persons involved ! 5 !202 ! EMPLOYMENT PRACTICES and the name of any possible witnesses (see Problem Resolution Procedure in the Personnel Policy Manual and use the Problems/Concerns Report Form #111). A prompt investigation will be conducted as discreetly as possible. Confidentiality will be maintained with respect to a sexual harassment complaint. Only those with a need to know about such a complaint will be advised of its existence. The employee accused of prohibited conduct will have an opportunity to explain the conduct in question. Any person who has been found in violation of this policy shall be subject to appropriate disciplinary action, including letters of reprimand, suspension, demotion, termination, and the possibility of civil liability. It is the responsibility of every employee to conscientiously follow this policy. This policy will be reviewed annually with all employees. See Form #119. ! Employees who are dissatisfied with the resolution of the investigation should file a written complaint. No employee will be subject to any form of retaliation or discipline for pursuing a harassment complaint. ! ! HEPATITIS B VACCINATION Hepatitis B vaccination is made available to employees who are reasonably expected to be in contact with blood (or its products) in the performance of their duties (see Hepatitis B Information and Consent Form #108). The vaccination is made available within 10 days of the initial assignment to employees who have not already been vaccinated. The employer will pay the immunization expense. Employees who decline to have the vaccination will be asked to sign a formal statement of declination but may later change their mind (see Hepatitis B Vaccine Declination Form #109). (For more information on bloodborne pathogen compliance refer to the OSHA Manual or the Health and Safety Manual.) ! ! THE EMPLOYMENT SELECTION PROCESS Candidates for job openings are selected on the basis of merit, competence, experience and satisfactory character and employment references. Additional training is usually needed in order for any new employee to become effective on the job. The cost of this training can be expensive. It is, therefore, our policy not to hire anyone who would have to take an extended leave shortly after beginning employment. If an extended leave is requested by a new employee, the request may be denied and employment terminated. In order to maintain impartiality and fairness in employee relations, we do not hire relatives of employees when it would result in one family member working under the direct or indirect supervision or authority of another family member. ! Applicants and the information they have provided either on the employment application form, the resume, or during the interview will be thoroughly screened for accuracy. Any misrepresentation, falsification or omission of material information may result in a denial of an offer or, if the applicant is hired, be cause for immediate dismissal without any liability to the employer other than for payment of services actually rendered. ! ! During the screening process, we will review: !The employment application !Education and work experience !Prior work history ! 6 !203 ! EMPLOYMENT PRACTICES References License verification (if applicable) !Copies of certificate of training !Test results to ascertain skill and potential job performance (if applicable) !Compliance with the Immigration Reform and Control Act (IRCA) of 1986 !Results of a medical examination (if applicable) ! ! ! A word of caution in the treatment of job applicants and their references: It is important that we maintain good public relations throughout the screening and interviewing process with applicants. Therefore, it is our policy to look upon job applicants as potential patients and treat them with the same professional courtesy and consideration. ! ! MEDICAL EXAMINATIONS After a conditional offer of employment has been made, applicants may be required to pass a medical examination. These examinations will be paid for by the practice and are the property of the practice. Such records will be treated in a confidential manner and will be made available only to the employee, persons designated and authorized by the employee, relevant insurance companies, or the employee's certified healthcare practitioner. ! ! NEW EMPLOYEE ORIENTATION PROGRAM During your first few days of employment, you will participate in an orientation program. During this program, you will receive important information regarding the performance requirements of your position, basic personnel policies, your compensation, and benefits programs, plus other information necessary to acquaint you with your job. Your orientation will partially be structured with our New Employee Orientation Checklist (see Form #201). ! You will also be asked to complete all necessary paperwork at this time, such as medical benefits plan enrollment forms, beneficiary designation forms, and appropriate federal, state, and local tax forms. At this time, you will be required to present information establishing your identity and your eligibility to work in the United States in accordance with applicable federal law. ! We encourage you to ask any questions you may have during this program so that you will understand all the guidelines that affect and govern your employment relationship with us. ! You may be required to attend specific educational and training sessions to improve your skills or performance. The new employee will be able to participate in bonus and incentive programs after 90 days of satisfactory employment. ! ! ! EMPLOYEE PERFORMANCE REVIEW The evaluation of an employee's job performance is an ongoing process. The performance review serves as a guide to evaluate progress, areas for improvement, to plan further training and to establish and commit to future goals. The frequency of evaluations may vary depending upon the length of service, job position, ! 7 !204 ! EMPLOYMENT PRACTICES past performance, changes in job duties, or recurring performance problems. After the review, you will be required to sign the performance evaluation report simply to acknowledge that the items have been discussed with you and that you are aware of its contents. ! A salary review is usually given separately and on a different date than the performance review. ! REFERENCE REQUESTS ! It is our policy that all requests for information concerning current and former employees are handled in a consistent and appropriate manner. Such requests usually involve employment information, personal and business references, descriptions of job duties, etc. The procedure outlined below is to be followed by all employees who are approached, either formally or informally, and asked to provide information about present or former employees. ! All written, oral, or informal requests for information about employees or former employees are to be referred to the Office Manager. Consequently, no employee may provide (either on or off-the-record) any information regarding current or former employees to any non-employee. By following this policy, we can ensure that the information released about an employee is accurate, authorized, and representative of the practice’s position. ! In addition, to avoid charges of slander or defamation claims, employees and former employees are cautioned to be very careful about what they say about other employees, the employer, and the practice when they are away from the workplace. ! ! SERIOUS DISEASES Employees afflicted with a serious disease are to inform the employer as soon as possible. It is our desire to respond with compassion and understanding and at the same time safeguard everyone's interests, including the employees, patients, and the practice. The seriously ill employee must understand this obligation and provide the employer with the medical information needed to make basic work and health decisions. Information regarding an employee's serious disease will be kept confidential, unless law requires disclosure; or if in the opinion of the employer, it is necessary to protect the health and safety of the employee, employees, or others. OSHA outlines procedures for identifying at-risk tasks, use of protective equipment, handling, cleaning, and disinfecting contaminated work areas, equipment and protective clothing, providing hepatitis B vaccines, labeling areas and objects of potential exposure, employee training, and the creation and retention of medical and training records. ! Serious diseases include, but are not limited to, cancer, myesthenia gravis, heart disease, multiple sclerosis, hepatitis, tuberculosis, and Acquired Immune Deficiency Syndrome (AIDS). A certified healthcare practitioner's certification may be necessary for continued active employment. (Since the types of illnesses included under Americans with Disabilities Act are being modified periodically, check with your employer if you have any questions about a particular illness.) ! ! ! ! 8 !205 ! EMPLOYMENT PRACTICES PROBLEM RESOLUTION PROCEDURE ! The purpose of a resolution procedure is to ensure fair and equitable treatment for all employees. ! We are eager to learn of any condition that may be causing problems for you on the job. Such conditions cannot be corrected unless you make them known. A problem may involve work conditions, policies, alleged discrimination, harassment, or anything else that prevents a fair and productive work environment. ! You are encouraged to use the following procedure so a problem can be addressed and resolved as soon as possible. Please state the situation as clearly as possible, preferably in writing, within ten days after you become aware of the situation. Any complaints of harassment must be reported immediately to, either, the Practice Administrator, the designated person or the employer who will then follow through according to the harassment policy described earlier in this manual. ! Step 1. The Practice Administrator, Manager, or Designated Person (If not applicable, go to step 2) !The administrator checks the circumstances and provides a solution to the problem within five working days !In the event you are not satisfied that the problem has been resolved—proceed with Step 2 ! Step 2. The Employer " The employee brings the situation to the attention of the employer in writing within ten working days " The employer investigates the circumstances and returns a decision within five working days " The employer’s decision on a given issue does not set precedence for future decisions. ! ! ! 9 !206 HOURS OF WORK ! Your workdays and hours will be discussed in advance between you and the doctor. A copy of your schedule will be kept in your HR folder. You are responsible for reading the schedule and being available for work when required. The workdays and hours may be increased or decreased in response to the needs of the practice. ! Office requirements, due to unexpected emergencies and changes in planned procedures, occasionally make it necessary to work beyond the scheduled work hours. When overtime is required, you will be notified as much in advance as possible. The employer reserves the right to assign employees to jobs other than their usual assignments when required. ! Keeping Track Of Your Time—All Employees are responsible, individually, for recording their time on the punch clock when: !Reporting for work !Leaving for lunch !Returning from lunch !Leaving at the end of the day ! Attendance records whether on card or computer, are used as a means of recording hours worked and calculating pay. They record regular hours worked, meal periods, overtime, absences and PTO. Attendance records are legal documentation of hours worked and must not be removed, destroyed, falsified, defaced or removed from the premises. All non-exempt employees, whether salaried or hourly, must complete a weekly time record reflecting actual hours worked each day. Any mistakes or omissions on the attendance record are to be reported immediately to the office Manager using FORM #117 TIME CORRECTION WORKSHEET in this manual. Only then can the necessary corrections be made. ! Do not permit another employee to enter your time for you. Likewise, do not register another employee's time even if requested to do so. ! Do not sign in or start work earlier than 5 minutes before your normal starting time or sign out or stop work later than 5 minutes after your normal quitting time unless overtime has been approved in advance. This will give you a ten-minute “window” within which to check in or out without incurring overtime. Thereafter, for pay calculation purposes, time will be rounded off to the nearest one-tenth of an hour (e.g., one-tenth is 6 minutes; three-tenth is 18 minutes). Employees are not permitted to work on their own initiative before or after scheduled working hours or during non-paid meal periods or paid rest breaks. ! Time off with pay or any time for which you expect to be paid must be entered on your attendance record. All time off requests must be submitted in writing. See below for more information. ! Exchanging Hours—please do not exchange hours with another employee without prior written approval from the doctor. Authorization will not be granted unless it can be accomplished without overtime. ! ! ! 10 !44 ! PERSONAL TIME OFF ! ! WHAT CONSTITUTES TIME WORKED ! ! LEAVING PREMISES ! ! WHEN THE DOCTOR IS AWAY ! ! JOB ABANDONMENT You must get written approval before leaving the practice during work hours for personal reasons. Time spent receiving dental treatment must be recorded on the attendance record as personal time off. Time off during normally scheduled work hours will be deducted as vacation days. From your actual commencement of duties until the end of your workday, except for time spent at lunch or dinner, constitutes time worked. Getting ready and clean-up time, employee meetings in the beginning or during the day are also time worked. Arriving early, leaving late, or preliminary time spent in attending to personal matters such as grooming, changing clothes (unless required by the nature of the job), are not considered time worked. Do not sign in until you are ready to go to work. Likewise, do not work after you have signed off on the attendance record or computer time clock. For purposes of calculating overtime, time worked does not include paid time off. If you have to leave the premises for any reason during the regular work period, be sure to get written permission and record the time on your attendance record. When the doctor is away from the office and therefore not seeing patients, it provides the employees an opportunity to complete unfinished tasks. Check with the doctor or the authorized person, no later than the day before, to determine if your presence is required while the doctor is gone. For example, the clinical employees may be asked to take the time off and the administrative employees to come to work to answer the phone and get caught up, etc. If your presence is not required at the office, you may, with approval: "Take time off without pay "Take time off and be charged with time off you have earned but not used. Please indicate on your attendance record what type of benefit with which to charge the time off. An employee who is absent from work for three consecutive days without notification is considered to have resigned. If you request time off that is denied and take time off anyway, or, if you fail to return from an approved absence on the agreed upon date, the absence is considered to be job abandonment and treated as a voluntary resignation. ! ! ! 11 !45 ! ! ATTENDANCE AND PUNCTUALITY Absenteeism—To ensure that our patients receive the proper treatment, we must have adequate staff to handle the workload. Therefore, any absences from work regardless of the reasons2 are unacceptable and constitute an unsatisfactory work record (refer to Employee Relations: Responsibility and Conduct). New employees who miss a day of work within the orientation and training period will be subject to disciplinary action which could include termination. ! Failure to notify the employer properly of any absence may result in loss of compensation and may be grounds for disciplinary action (see Job Abandonment). Please call every day during an absence unless otherwise agreed upon. If you are absent for two consecutive working days due to a personal illness or disability, you may be required to provide documentation from your certified healthcare practitioner stating your ability to return to work. Absences longer than one week are converted to a leave of absence. ! Tardiness—If you are unable to report to work or find that you will be more than 15 minutes late, please notify the employer as far in advance as possible. In case of an unexpected absence, please notify the employer at least one hour before your shift is scheduled to begin. ! ! REST PERIODS Meal Period—You will be scheduled for an unpaid meal break after no more than five and one half hours of work. An employee may not work through a mandatory meal period and be allowed to shorten the work day by a corresponding period of time. There are two exceptions: 1) You may (with the employer’s permission) voluntarily agree to waive the right to a meal break, provided the work day is no more than 5.5 hours; 2) If the workday is more than six hours, a paid working meal period may be permitted if the nature of the work does not permit you to be released from duty (i.e. due to the patient schedule) and you have entered into a written agreement with the employer for a working paid "On Duty Meal Period” (see Form #416). If it is a non-patient day, and you do not take at least 1/2 hour break after 5.5 hours of work, that lunch period will be automatically deducted from your paycheck. You must take a 1/2 hour break after 5.5 hours of work on non-patient days. No exceptions. ! Rest Break—You receive a paid rest break of 10 minutes at approximately the middle of every four hours of work. The breaks may not be combined and added to the lunch period, nor can they be waived to shorten the work day. We ask that you take your breaks when they will not negatively affect patient care. For insurance purposes, we ask that you remain on office premises during rest breaks. 2 Exceptions to this attendance policy would be the serious medical conditions that are covered by the Family Medical Leave Act. Other exceptions covered by federal and state regulations may also apply. ! 12 !46 ! WAGES AND SALARIES ! ! OVERTIME PAY The practice will maintain a salary administration program that: "Allows for differences in individual ability, knowledge, and skill "Provides incentive to encourage each individual to strive for improved performance Overtime is paid according to the federal Fair Labor Standards Act and the State Wage, Hours, and Child Labor laws. ! Exempt employees are not required to be paid overtime pay. ! Non-Exempt employees are paid overtime regardless of method of payment (hourly, daily, or salary). When employees are paid a daily rate or salary, the pay is converted to an equivalent hourly rate for overtime calculation purposes. ! Overtime rate will be calculated at the rate of one and one-half times the employee’s regular hourly rate of pay on time worked in excess of 40 hours in a week or the daily number of hours required by your state3. ! Overtime is not paid twice for the same hours. Employers in states with daily overtime requirements need only pay overtime on the greater number of hours in the week of either the total daily number of overtime hours OR the weekly number of overtime hours. ! Commissioned non-exempt employees will be paid overtime based on their average hourly earnings for the week. The overtime rate will usually vary from week to week based on their fluctuating commissions. ! Time not included for overtime calculation purposes—paid time off is not included to determine hours worked for overtime pay purposes. ! Overtime is to be authorized in advance—employees are not permitted to work more than their regularly scheduled hours without prior approval and may not work on their own initiative before or after scheduled working hours or during non-paid meal periods or breaks. Violation of this policy may result in disciplinary action, up to and including discharge. If you work OT, you will receive a documented warning to be placed in your file. ! ! COMPENSATORY TIME OFF (COMP TIME) Comp Time, or make up time is not permitted. ! ! 3 Alaska, California, Puerto Rico and Nevada—8 hours in one day, (Nevada exemption: not applicable if, by mutual consent, the employee agrees to work 10 hours per day for 4 calendar days within any scheduled work week or if the employee earns 1½ times minimum wages); Florida—10 hours for manual laborers; Colorado—12 hours. Wage and Hour laws change, check state labor laws periodically to assure compliance. ! 13 !144 ! ! PAY SCHEDULE AND TIME SHEET Wages are based on an hourly rate, a daily rate, or a monthly salary. All corrections to an individuals time sheet must be submitted, in writing, prior to the close of the pay period. Please print, review for accuracy and sign off on your timesheet the last day you work in a pay period and give it to the proper person. ! Pay periods are biweekly. A sheet demonstrating the pay periods and pay dates will be distributed once a year. ! Please review your paycheck for errors. If you find a mistake, report it immediately, so it can be corrected using Form #117 provided in this manual. ! As a condition of further employment, you agree to bring questions or errors regarding pay calculations or any other concerns retarding payment of wages or reimbursement of expenses to the Office Manager and and the Payroll Coordinator to provide an opportunity for GCDE to address any errors. You must fill out FORM #117 to process corrections to your timecard correctly. To prevent misunderstandings later, any discrepancies must be reported within 5 days after receiving the check, or we will assume that no error has occurred and you will have no recourse later. ! ! ! INCENTIVE OR BONUS PAY Incentive or Bonus Pay is entirely up to the discretion of upper management and may be given or withdrawn at any time, for any reason, without notice, explanation or restitution. ! ! ! PAYROLL DEDUCTIONS State and federal payroll taxes will be withheld from your paycheck in accordance with state and federal laws. These deductions include State and Federal Withholding Tax, Social Security Tax (FICA), State Disability Insurance (SDI) taxes and any State and Federal Tax Liens. Other reasons for deductions may include United Fund, U.S. Savings Bonds, health insurance premiums for the employee or dependent coverage, garnishments (see Garnishment of Wages section of manual) for payment for goods or professional services received by the employee on behalf of self or a member of the family. ! New employees are required to fill out a Withholding Exemption Certificate (Form W4) on or before the day they begin work. If you fail to fill out Form W4, the employer is required to withhold the maximum amount of tax. A Form W4 remains in effect until a new amended form is submitted. ! You must file an amended Form W4 reducing the number of exemptions within ten days after: "The spouse for whom you had been claiming an exemption is divorced or legally separated from you or claims their own exemption on a separate certificate "The support of a dependent for whom you claimed exemptions is taken over by someone else or no longer furnishes more than half the support for the year ! 14 !145 ! "You find the income of a dependent relative is less than the legally allowable amount for the year, and you had not previously claimed an exemption for the dependent "You or your spouse will reach age 65 on or before January 1 of the next year "You or your spouse becomes blind "Your spouse dies You may file a new Form W-4, increasing the number of exemptions when: "Your spouse no longer claims his or her own allowance on a separate certificate (e.g., when a wife stops working, the husband may claim an extra allowance) "A child is born to or adopted by you "You begin to provide more than half of a dependent relative’s support for the current year "You find that the income of a dependent relative will be less than the exemption amount and you have not claimed an allowance for the dependent ! If you want to change the number of your exemptions or your marital status for income tax withholding purposes, complete the appropriate form available from the employer. ! An amended Form W-4 will be made effective by the first payroll period ending 30 or more days after you submit the form. ! Employer’s are required to submit the W4 Form to the Internal Revenue Service for review if you (1) claim 10 or more exemptions, or (2) claim total exemption from withholding and earn more than $200.00/week, or (3) the employer believes you have claimed an excessive number of dependents. ! ! REPORTING TIME PAY (SHOW UP PAY) ! ! WAGE AND TAX STATEMENT—FORM W-2 When you show up to work a regularly scheduled workday but are not provided with the expected amount of work and are sent home early, you will receive the amount legally required or two hours, whichever is less. If you work more than two hours but less than four hours, you will be paid a minimum of four hours pay. If you are sent home early and receive reporting time pay for time not actually worked, the time not worked is excluded when computing time for overtime purposes. This does not apply in cases of “acts of god” such as but not limited to: bad weather in which the local governing bodies declare a closure of roads (i.e. Level 3 storm), loss of electricity or power. See “Inclement Weather and inactive time pay” on pg. 17 ! You will receive two copies of Form W2 showing income taxes and social security taxes withheld for the year by January 31 of the following year. However, if you request a W-2 form before the January 31 deadline, it will be provided within 30 days of your written request or within 30 days of your final payment of wages, whichever is later. ! PAY ADVANCES We do not pay wages or salaries in advance. ! ! 15 !146 ! SALARY ADJUSTMENTS Wages are reviewed at least once a year. Wage adjustments are discretionary and based on performance, increased skills, and the individual’s contributions to the welfare and profitability of the practice (see Performance Appraisals). PAYROLL ADJUSTMENTS ! It is necessary to bring any questions or errors regarding pay calculations or any other concerns regarding payment of wages or reimbursement of expenses to the Office Manager and Payroll Coordinator to provide an opportunity for GCDE to address any errors. See Form #116 and Form #117. DIRECT DEPOSIT All employee's will have paycheck's direct deposited into the bank of their choice. It will be the employee's responsibility to provide a current voided deposit slip on the 1st day of employment. Exceptions will be considered at the employer’s discretion. ! LOST PAYCHECKS Each employee is responsible for his or her individual paycheck after it has been received. Please report a lost payroll check within 24 hours so we can initiate the “stop-payment” process. At the employer’s discretion, employees may have any related bank charges deducted from their following paycheck. ! ! JURY DUTY When called to serve on jury duty or as a witness, you are to submit a copy of the summons to the employer or your manager immediately. You are also required to submit certification from the court listing the actual days of service. ! If you are called to serve on jury duty, you will be given a Leave Of Absence. Wages will not be paid while on jury duty. ! If you are released before the end of the workday, you are to return to work for the balance of the day. The employer reserves the right to contact the court to request a release from jury duty. When serving jury duty, the employee is to ask for the "Court Phone Service." ! ! INCLEMENT WEATHER AND INACTIVE TIME PAY This policy establishes guidelines during periods of extreme weather conditions, emergencies or special circumstances. ! Unless an emergency closing is announced, all employees are expected to report to work. However, all employees are urged to use their own discretion in deciding whether they can commute safely to work. ! If the weather, or other emergency conditions, prevent employees from reporting to work on time or coming to work at all, you are required to notify the employer, or a person so designated, no later than 7:00 a.m. or earlier if possible on that day. ! ! 16 !147 There are times when unusual circumstances prevent employees from working. Inactive time may be caused by: "A failure by the employer to provide sufficient work "Equipment or material breakdowns "Other unexpected obstacles or emergency conditions beyond the control of the employer ! When unable to report to work because of weather conditions, or if inactive time is necessitated, the time off is without pay. Hourly paid employees have the option of using any paid time off they have earned. Calling the employer as soon as reasonably possible if the unusual circumstance prevents you from coming to work on time. ! ! ON-CALL HOURS/WAIT TIME Employees may be directed to be available on an "on-call" basis during their non-work hours due to unique potential staffing needs including but not limited to emergencies. When the time spent on-call is controlled by the employer and the employee is unable to use the time effectively for his/her own purposes, the specific time the employee is directed to be on-call will be considered as hours worked. Such time is technically referred to as "engaged to wait." During periods of on-call time during which the employee is completely relieved of her/his duties and restrictions are not placed on the employee's ability to use the non-work time effectively for her/his own purposes, the time involved is not part of hours worked. Such time is technically referred to as "waiting to be engaged." ! Paid on-call hours (engaged to wait) may be compensated at a different capacity work rate (refer to definition in this section). They are included for purposes of calculating overtime ! ! CONTINUING EDUCATION We firmly believe educational development is important. Employees are encouraged to take educational courses or training to increase their competence in the present job assignment and to prepare for future advancement. If you are asked to take a course for the betterment of the company during regularly scheduled hours and you refuse, and you are not needed at work to perform non-patient related tasks, you will not be paid for that day. You may choose to take vacation or personal time for that day instead, if you fall under the guidelines for vacation/personal time hours. ! Dress code for attendance is professional but comfortable attire. No jeans, cut-offs or tank tops please. ! Wages—you may or may not be paid for courses attended during or outside of your regular work schedule, as agreed upon in advance for course and compensation if any (see Different Capacity Work Rate). You will not be paid for courses you take to maintain licenses or certificates that are a condition of employment or for which you voluntarily attend outside your regular work schedule. Please submit in writing at least 2 weeks in advance, if you will be out for a course and missing a regularly scheduled work-day so that the appropriate substitute may be secured. ! Expenses—the employer will pay the expenses for the courses that have been agreed upon. Types of expenses to be considered may include: ! 17 !148 ! "Travel (Including mileage to/from airport, minus the mileage to/from your home; Air Travel, Cabs when applicable, Car Rentals and Flight) if it falls within your regular work hours, may be paid at the minimum wage rate. "Meals (3x/day; Any other snacks or drinks purchased outside those times are the responsibilty of the employee; Alcohol will never be purchased or reimbursed by Grove City Dental Expressions.) "Accommodations "Tuition "Salary (see Different Capacity Work Rate) "Supplies (when applicable) Gratuity-Grove City Dental Expressions will cover up to 15% of the gratuity related to meals or cabfare during travel or other times Grove City Dental Expressions covers the cost of an item. Anything over 15% will be the responsibility of the purchaser. ! Receipts for Reimbursement of Expenses—All receipts submitted to Accounts Payable to cover Parking, meals, etc must be itemized. Please request an itemized receipt. You may not be reimbursed for the particular expense if this receipt is not included. ! Instead of a dollar-for-dollar reimbursement, you may be allowed a per-diem amount to cover daily expenses. Otherwise, reimbursement for the agreed upon expenses may be obtained when the course is completed if, within 30 days of its completion, you submit to the employer the following: "Evidence of completion of the course "A verified statement of tuition paid and other costs "A detailed outline of information covered at the courses "Receipt of incurred expenses ! Copies of certificates and units earned will be maintained in your personnel file. ! Commitment to Work-If Grove City Dental Expressions incurs the expenses for a continuing education course totaling over $500 in tuition, meals, travel, accommodations or other expenses associated with a course, you may be required to sign a commitment letter. The commitment letter states you will continue working in your current position at GCDE for a minimum of 6 months following the last day of the course. If you resign or are fired prior to that day, you will owe back some of the monies GCDE paid towards your continuing education. This is done to prevent employees from taking a high expense course, paid at the expense by GCDE, and leaving shortly after. Thus GCDE would have paid for the benefits of the course but would not have received those benefits for a long enough time period. The total monies incurred by GCDE will be equally prorated for 6 months after the last date of the course. Example: course cost $1000, last day of course 2/10/10, employee leaves on 5/10/10, course cost due to employer from employee, $500. See form #115. This money would be due prior to the employee’s last day of work. If the money is not paid by the final paycheck, it will be deducted from the last paycheck. If the last paycheck is not high enough to cover the fees, you will be billed. If not paid in full within 30 days, the account will be sent to collections with a 33% up charge to cover the cost of the collection agency’s fees. ! ! 18 !149 Different Capacity Work Rate4 ! You may be paid a separate straight-time rate of pay for dissimilar types of work during the same workweek. Traveling to, or attending a seminar or workshop is considered dissimilar type of work than the work conducted during their normal workday. The time may therefore be paid at a different rate from their regular rate of pay while attending such seminars or workshops. To use this special rate, several conditions will be considered: " The hourly rate of pay will equal or exceed the minimum wage requirements. This new rate then becomes the special hourly rate of pay for this period. The hourly rate is 75% of the individuals regular hourly rate. This rate should not exceed $15/hour. The rate of pay will be decided upon prior to the date of the course, in writing. See Form #110. " No overtime will be paid for con-ed/travel hours. Hours paid under con-ed will show up separately on the employees paycheck and will not show up on the punch in/out clock. ! ! TRAVEL TIME One Day Travel—travel time incurred during or outside of the normal work hours will be counted as hours worked with the usual unpaid meal period deducted. The employer may also deduct the time the employee would normally spend commuting to the regular workplace. You will be paid at the different capacity rate mentioned above. ! Overnight Travel—travel time incurred during the normal work hours will be counted as hours worked (on both normal workdays and days that are normal days off). You will be paid at the different capacity rate mentioned above. In accordance with the FLSA and most state laws, you will not be paid for time spent outside the normal working hours while traveling as a passenger on a train, bus, airplane, boat, or automobile5. The time spent driving traveling between home or office to the point of departure, e.g. an airport or rail station, is paid. If leaving from home, the usual travel time between home and office will be deducted. ! LUNCH AND LEARNS Lunch and Learns consist of educational courses that may or may not apply directly to your job held during a normal work day during a regular scheduled lunch breaks. They are not mandatory but lunch is provided. These opportunities are designed to improve you professionally and maybe great team building experiences. You are required to clock in/out for these Lunch and Learns. You will not be paid for these Lunch and Learns as they are not mandatory. All employees are encouraged to participate. ! 4 Wage-Hour Opinion Letter No. 1649, C.H.H. 31,844 (1986); Accord 29 C. F. R. §§ 778.115 and 778.419, and Townsend v. Mercy Hospital of Pittsburgh, 689 F. Supp. 503 (W. D. Pa. 1988), aff’d, 862 F.2d 1009 (3d Cir. 1988). See also Letter of Chief Deputy Labor Commissioner James H. Curry dated March 9, 1990, and DSLE “Update” (May 1992). See 29 C. F. R. § 778.316. The rates must be for different type of work. 5 Some states, California for example, have more stringent laws regarding compensation for overnight travel. Check with your local state to insure compliance. ! 19 !150 ! RECERTIFICATION Several positions within the practice require the attainment of certain licenses or certificates. It is a job requirement that these be kept valid and current. Employees are responsible for maintaining a valid license by attending the necessary number of continuing education courses required for recertification at their own expense. ! If possible, please arrange to attend the courses that are given during the hours you are not scheduled to work or give at least two weeks notice of courses you wish to attend during your regularly scheduled working hours so that arrangements can be made for substitute personnel. ! Since certification is a requirement of the job, you will not receive wages for attending or be paid any lost wages or be reimbursed for related expenses. However, the employer may agree to pay for total or partial cost of the tuition for courses that have been mutually agreed upon. Alternatively, you may be required to pay the expenses and then be reimbursed after a mutually agreed upon time of continued employment with the practice. ! Upon completion of recertification, please provide us with a copy of the renewed license. The employer assumes no responsibility for employees who become delinquent in the number of units needed for recertification and who, consequently, lose their license. If employee does not have a license in good standing this will result in termination and employee voluntary resignation. ! ! ON THE JOB ACCIDENTS If you become unable to complete a workday because of an injury incurred while on the job, you will be paid for the balance of the day. The injury must be reported immediately. Refer to Workers’ Compensation and reporting injuries in the Employee Benefits section of this manual. ! 20 !151 BENEFITS CHART ! A written agreement with individual employees that contains terms that are different from those stated below takes precedence over any benefits listed in this manual. ! TYPE OF BENEFITS (For detailed information refer to the individual benefit pages in this section of manual) Workers' Comp. Insurance Unemployment Insurance ! ! Regular Employee Status ! Part! ! Full Part Time Time Time ! Per-Diem Employees ! Full Time ! ! Part Time Temp. X X More than 20 hrs/wk Less than 20 hrs/wk More than 20 hrs/wk Less than 20 hrs/wk X X X X X X X X X X X X X x X* X* Sick Leave/Well pay Holidays Paid Time Off Dental Benefits Bereavement Leave ! ! X X denotes eligibility * Change in Employee Status: Employees who change from a no-benefit, part-time status, to a part-time or full-time status that does provide benefits, become eligible for the benefits the date the change becomes effective. A change in status may result by a decision made by the employer or, by an employee having worked the number of hours regularly worked by employees in another status. ! ! ! ! ! ** As laws continue to change in this area, it is recommended that employers verify if short term disability insurance is required in their state. At this time, the following states are understood to require this insurance coverage: CA, HI, NJ, NY, PR, and RI. * HOLIDAYS FOR PART-TIME EMPLOYEES, see pg 30, PAID HOLIDAYS NOTE: Hawaii Health Care Act. Employers in the state of Hawaii must ensure that employee benefits meet the requirements of the Hawaii Prepaid Health Care Act (HPHCA). Hawaii clients see inserted addendum in the back pocket of this manual. ! 21 !244 EMPLOYEE CLASSIFICATION ! For purposes of employee benefits eligibility, employees are classified according to specific terms and definitions. However, all employees, including new employees, are “at-will” employees (refer to “At-Will” Employment Policy and Employment Agreement Form #101, page 65). The employee classifications are: ! New Employees—employees who are employed for less than ninety (90) calendar days are considered new employees. This initial time of employment is considered the orientation and training period. The duration of the orientation and training period can be extended at the employer's discretion. ! Except for vacation benefits, which accumulate starting at date of hire, new employees do not earn nor are they eligible for benefits during the orientation and training period. Upon satisfactory completion of the orientation and training period, they are: !Considered potentially qualified !Reclassified as a regular or temporary employee !Enrolled to participate in applicable benefit plan (refer to Employee Benefits Chart) and bonus systems !Informed of the above ! Former Employees who have been gone for less than 12 calendar months, at the employer's discretion, may be re-hired and receive full or partial seniority and benefits credit for service prior to the separation. The credits, and their time of commencement, are to be decided upon prior to beginning employment and the details stated in writing and signed by both the employer and the employee. ! Regular Full-Time Employees—employees who are paid either a salary or an hourly rate and who regularly work 36 hours within a workweek. ! Regular Part-Time Employees—employees who work less than the number of hours regularly worked by full-time employees are considered regular part-time employees. ! Temporary Full-Time Employees—employees whose service is intended to be of limited duration and who work the same number of weekly hours worked by regular full-time employees are considered temporary full-time employees. Temporary full-time employees are not eligible for benefits. ! Temporary Part-Time Employees—employees whose service is intended to be of limited duration and who normally work fewer hours than those worked by regular full-time employees. Temporary part-time employees are not eligible for benefits. ! Per-Diem Employees—employees who are paid a daily rate for the hours worked are considered per-diem employees. Per-diem employees typically receive a higher rate of pay than other employees. These employees receive higher wages in-lieu of certain employer-sponsored benefits. These benefits include, but are not necessarily limited to, vacation, sick leave, holidays, health insurance and dental benefits. ! Employees who transfer from Per-Diem status to Regular Employee status may be eligible for some or all of the benefits previously waived as a per-diem employee. If such a change in classification occurs, no ! 22 !245 portion of the employee’s service as a per-diem employee shall be credited for purposes of determining benefits (employee will be considered a new employee for benefit purposes). ! Employees who transfer from Regular Employee status to Per-Diem status will be treated as terminated for purposes of reconciling their benefit status. All vested benefits, if any, that are payable at termination will be paid to the employee. ! Exempt Employees—employees who are exempt from the minimum wage and timecard overtime provision of the Fair Labor Standards Act (FLSA) as amended are considered exempt employees. Such employees include employees who qualify as exempt executive, administrative, professional employees, outside sales persons, and computer programmer/analysts. ! Non-Exempt Employees—employees who are not exempt from the minimum wage, overtime and timecard provisions of the FLSA are considered non-exempt employees. ! Change in Employee Status—employees who change from part-time to full-time status receive new employee status and are subject to all policies pertaining to new employees (see above). For example, if full-time employees earn a one week paid vacation after one year of service, and three weeks after five years, the former part-time employee must complete one year of full-time service before earning a one week vacation, and five years before earning three weeks of paid vacation (refer to Employee Benefits Chart). At the time of the change, the employee will be paid for any unused benefits earned as a part-time employee and start earning credits as a full-time employee. ! Employees may be transferred to another assignment as a necessary element in the operation of the practice. ! ! ! ! ! ! ! ! ! ! 23 !246 ! ! ! EMPLOYEE BENEFITS DENTAL BENEFITS Specified regular employees (refer to the BENEFITS CHART) will be eligible to receive the following dental benefits with the provisions outlined below after 120 days of employment. Dental benefits cover the type of general dentistry that is normally performed within the practice. ! After 120 days of employment, an employee will receive $300 credit towards dentistry to be used on a calendar year basis at our office. This $300 is applied each January 1st regardless of when hired. This $300 cannot be redeemed for cash. All dentistry will be performed at 30% of the current fee schedule fees. (Example: A crown is $1200. This would be charged to the employee at 30%, so $360). All immediate family members of the employee would receive the 30% rate, but are not eligible for the $300 credit. Any procedures requiring lab expenditures exceeding $300, will be cost plus 20%. (Example: If Invisalign is $1200 for the lab fees; the cost to do Invisalign would be cost plus 20%: $1200 plus 20%=$1440.) ! If an employee has insurance, insurance will be billed. If the insurance fee schedule is higher then the our fee schedule, then employee will forfeit the difference and will not be reimbursed due to our agreements with the insurance companies. ! If employment is terminated for any reason while there is a negative balance in the Personal Dental Benefit Account, you will owe the balance. If arrangements for payment are not made prior to the final paycheck, the monies owed may be deducted from the final paycheck. If needed, continuation of treatment will be charged at the regular rate. The PDBA account can only be used for dental treatment while employed by the practice and any positive balance will not be paid at time of termination. ! LIFE INSURANCE ! Life insurance is not provided as a benefit at this time. ! MEDICAL BENEFITS ! Medical benefits are not provided at this time. ! 24 !247 ! ! ! ! EMPLOYEE BENEFITS SICK LEAVE/WELL PAY There is no paid sick leave. Vacation days must be used. If you are going to be sick, YOU are in charge of contacting a sub agency and arranging a sub. You must notify the Office Manager via a phone call ASAP. In order to provide optimal patient care, we must be fully staffed. ! Employees who claim protection under the Americans With Disabilities Act (ADA) or the Family Medical Leave Act (FMLA) are to notify the employer immediately. (Refer to Leave Of Absence policy in this section). ! New Employees-Any days taken off for any reason, including sickness, during the 120 day probation period, are seen as voluntary resignation unless prior written approval from the office manager. ! Notice of absence—employees who know in advance that they will be absent for health reasons must give advance notice, including the probable start date and duration of the absence. If a sudden illness makes it impossible for an employee to request unpaid sick leave before the workday begins, the employee should notify the person(s) listed on the Designated Name page which is the last page of this manual, no later than one hour before the start of the workday. Please state if the illness and the time off are taken under the provisions of The Americans with Disabilities Act (ADA). If an employee is too ill to place the call, have a relative or other responsible individual make the call. If the sickness occurs during regular scheduled work hours, you must take a vacation day. If the employee does not have any vacation days to use, you must take unpaid time off. Failure to follow this procedure will void the claim for paid leave and can be grounds for disciplinary action including termination. ! During an absence because of illness, you are to notify the employer daily of progress unless otherwise agreed upon. ! Physician’s Statement—if you are absent on sick leave more than two consecutive days please bring a certified healthcare practitioner’s certificate verifying the reason for your absence. The note should also state that you are able to perform your regular work assignment and state if there are any restrictions pertaining to your duties or the number of hours you can work. However, at the employer’s discretion, you may be required to bring a certified healthcare practitioner’s certificate verifying the medical reason for your absence, when you are absent for less than two days. ! Notice of an Employee's Return To Work after an illness needs to be given in advance so that scheduling adjustments can be made. ! PERSONAL DAYS ! There are no personal days. If you take off time, you must use vacation days or unpaid leave. ! ! RELIEF DAYS ! 26 !248 ! ! EMPLOYEE BENEFITS Pre-set days on the calendar decided by upper management. These days are given as paid days off that don’t count as vacation benefits or other paid time off. Hours incurred do not apply to OT pay as they are not physically worked. You will only get paid relief pay if you are regularly scheduled to work that day. If you are regularly scheduled to work that day, then the amount you will be paid is as follows. The amount of hours you are paid is an average of the prior 3 weeks of that same day. Example: if the relief day is a friday, the hours you are paid out are the average of the 3 prior fridays which you have worked. If you work every other friday and the day you are scheduled to work falls on a relief day, then you will be paid your average hours usually worked. If you are not scheduled to work on that day, even if you worked previous fridays, then you will not be paid. ! VACATION BENEFITS Starting May 1st, 2014. The previous system in place as of January 1st will be honored for employees who currently had one year of uninterrupted service by January 1st, 2014 for the year of 2014 only. ! ! Regular full-time employees after 120 days of uninterrupted service, will receive time off with pay annually for recreational purposes in acknowledgment of service rendered. This policy does not apply to associate doctors. All vacation requests of 3 or more days must be submitted in writing to the Office Manager at least 30 days prior. ! Each year, eligible employees (see Benefits Chart) are entitled to vacation time paid at their regular rate of pay (not including overtime or incentive/bonus pay) as outlined in the Vacation Benefit table below. ! ! Vacation Benefit for Regular Full-Time Employees Prior to successful completion of the orientation None and training period After 120 days of continuous service 2 vacation days per year After 12 months of continuous service 5 vacation days** per year After 36 months of continuous service 10 vacation days per year After 60 months of continuous service 15 vacation days per year ! ! * Continuous service is broken if employment has been terminated or otherwise interrupted for a period of thirty days. Exceptions may be made at the discretion of the employer. ** A vacation week constitutes the number of straight time hours worked in an average workweek. Straight time hours include all hours for which employees are not being paid overtime. If the practice is using a payroll service, vacation time is earned based on actual straight time hours worked as computed by the service. Therefore, earned vacation time is directly proportional to actual time worked during the year. ! Regular part-time employees are not eligible for vacation days. ! Vacation benefit accrual—upon successfully completing the orientation, training period and 120 days of continuous, uninterrupted service, employees will accrue the aforementioned vacation benefits (SEE ! 27 !249 ! ! EMPLOYEE BENEFITS ! CHART ABOVE). After 120 days of employment, the employee is eligible to use the vacation days earned at any time. Approval must be given for vacation time in order for proper patient care. It may be necessary for a sub to be trained in your absence. Amount of vacation time and vacation time approval is solely under the discretion of the Office Manager. ! Using accrued vacation—you are not eligible to use accrued vacation until after 120 days of continuous employment. You are required to use your accrued vacation benefit within the year after which it has been earned. Unused vacation time will be paid out at the end of the employee’s anniversary year unless carried over with special permission. If there are extenuating circumstances (i.e., when the absence may severely affect service during a critical period), you may carry all or part of the accrued vacation forward to the next year. However, you may not carry over more than four weeks of vacation at any time. Vacation time carried over in excess of four weeks will be paid on the following paycheck. ! Vacation approval—vacations must be taken at the time most convenient for the practice. All vacations must be approved in advance to assure that patient scheduling needs are met. Therefore, please submit your vacation request in writing with as much advance notice as possible. Conflicting requests will be decided in favor of the person with the most seniority in that position. ! Paid holidays that fall during employee vacation—if a paid holiday falls while an employee is on a paid vacation, eligible employees will be charged with one less vacation day. The unused vacation day may be taken at another time as the schedule permits (See When The Doctor Is Away). ! Office closed for vacation—you may be required to take vacation while the doctor is on vacation. If the employee goes on vacation when the doctor does, employees not eligible for vacation benefits may be required to cover the office during the vacation period. ! Employees returning from military service will earn vacation benefits based on their length of service from the date of hire, including time spent in the military (see Uniformed Services Employment and Reemployment Rights Act). ! Overtime—paid vacation time is not included as hours worked when computing overtime for the week. ! Split vacations—are permissible if scheduling permits. However, a request for vacation of less than a oneweek duration is not encouraged. ! Leave of absence—no vacation time is earned while on a leave of absence. Any earned and unused vacation time must be taken before the beginning of a leave of absence. ! Job abandonment—if you fail to return from vacation on the scheduled date, the failure to return will be considered job abandonment and treated as a voluntary termination. ! Retirement—any unused vacation will be paid to employees who are retired for reasons of age or disability or to the estate of a deceased employee. ! ! 28 !250 ! ! EMPLOYEE BENEFITS ! Vacation pay upon termination—any accrued and unused vacation time will be paid at time of separation. ! Eligible employees whose employment ends either voluntarily or involuntarily will receive payment of any credited vacation not taken. ! PAID HOLIDAYS ! The days below will be observed as paid holidays for full-time employees who have completed 12 months of continuous service. ! Paid Holidays ___ New Year’s Day* ___ Memorial Day* ___ Independence Day* ___ Labor Day* ___ Thanksgiving Day* ___ Christmas Day* ! ! When Observed January 1 Last Monday in May July 4 First Monday in September Fourth Thursday in November December 25 Regular full-time employees receive holiday pay equivalent to the straight time pay for the hours worked in a regular workday, up to 8 hours. Paid holidays are not to be counted as hours worked for overtime calculation purposes. Paid holidays will appear on a pay stub as holiday hours and will not be calculated on the punch clock. ! Eligible part-time employees (refer to Benefits Chart) receive an amount equivalent to their straight time pay. To qualify for holiday pay, the holiday must fall on a regularly scheduled workday. ! New Employees do not receive holiday benefits until they successfully complete the orientation and training period and 12 months of continuous service. ! Eligibility—to be eligible for holiday pay, you must work (or be on an excused paid absence, not including paid sick time) on the latest regularly scheduled workday before the holiday and the next regularly scheduled workday following the holiday. This policy does not apply to associate doctors. ! Holidays that fall on a regular scheduled day off—when a paid holiday falls on a regular scheduled day off, the employee will not receive pay for that day. ! Holidays that fall during a vacation—when a paid holiday falls while you are on a scheduled vacation, you will receive your regular pay under Holiday pay for the day. ! Holiday pay for an employee while on a leave of absence—employees on a leave of absence for any reason are not eligible for holiday pay. ! 29 !251 ! ! EMPLOYEE BENEFITS ! Holiday pay upon termination—employees who end their employment will not receive compensation for unused holidays. ! ! BEREAVEMENT LEAVE Eligible employees bereaved by the death of a family member will be granted time off without pay for up to a total of 3 workdays. ! All employees must notify the employer prior to taking any bereavement leave. At the employer’s discretion, additional unpaid leave may be granted. ! ! LEAVE OF ABSENCE The purpose for establishing leave of absence policies is to ensure that all leaves are granted on a fair and equitable basis to eligible employees. A leave of absence is defined as an excused absence without pay. ! A request for a Leave of Absence is to be submitted in writing (Form #409). Unless otherwise stipulated by state or federal regulations, the employer reserves the right to approve or deny any request for a leave of absence without giving a reason. ! SPECIFIC TYPES OF LEAVES: ! Types of Leave That Are Not Legally Mandated !Personal Leave Due To Illness Or Disability (applicable to employers with less than 50 employees) !Personal leave—exceptional circumstances not involving employment elsewhere ! Types of Leave That Are Legally Mandated !Medical Leave for Occupational Disabilities (see Worker’s Compensation and Medical Leave for Occupational Disabilities) !Personal leave due to a serious health condition of self, child, spouse or parent (see Family and Medical Leave Act (FMLA)) !Pregnancy Leave (see Pregnancy Leave Of Absence) !Jury or Witness Duty !Military Leave !Parental Leave ! Rules applicable for specific types of leave—employers with 50 or more employees must adhere to the regulations established by The Family and Medical Leave Act (FMLA). Equivalent state regulations that are the more stringent than FMLA take precedence. ! The Americans with Disabilities Act (ADA) relates to employers with 15 or more employees. Equivalent state regulations that are the more stringent than ADA take precedence. ! ! 30 !252 ! ! ! ! EMPLOYEE BENEFITS PERSONAL LEAVE OF ABSENCE DUE TO ILLNESS OR DISABILITY A medical leave may be granted to eligible employees who are temporarily unable to work due to illness or disability. For purposes of this policy, illness or disabilities include: inpatient or outpatient care in a hospital, hospice, or residential medical care facility. For disabilities associated with pregnancy, childbirth, and related medical conditions, refer to Pregnancy Leave Of Absence and The Family Medical Leave Act (FMLA) later in this section. ! Eligibility—after having completed 6 months of employment, regular full-time, regular part-time, and perdiem employees may request a leave of absence for medical reasons. Exceptions to the length of service requirement will be considered at the employer’s sole discretion. ! A Request for A Leave Of Absence—a request for a medical leave must be submitted in writing at least 30 days in advance or as early as possible for unforeseeable events. A healthcare provider's statement must be submitted in writing verifying the reason for the disability and the leave’s beginning and expected ending dates. The employer reserves the right to approve or deny any request for a leave of absence. ! If a leave is necessitated because of an illness or disability covered under ADA, please specifically state that you are requesting a leave covered by ADA. ! Length of Leave—a medical leave of absence may be granted for a period of up to four weeks. If four weeks proves to be insufficient, the time may, at the employer’s discretion, be extended to a maximum of 3 months. You will be required to use any accrued paid vacation, unused holidays or sick leave time before taking a medical leave. Any combination of medical leave and accrued paid time may not exceed the approved time for the leave. The total time of all absences related to the same medical condition is considered part of the same leave. ! If you are requesting an ADA leave, the employer may request a second opinion, to verify the length of time you will be on leave. The second opinion will be paid by the practice. ! Reporting on Progress—you are required to report directly to the employer every 30 days on your medical status and your continued intention to return to work. ! Salary and Benefits—the leave of absence is without pay and you do not accrue seniority while on a personal leave of absence. Benefits such as medical insurance, sick time, holidays and vacation times are not earned and do not accumulate during the leave. Subject to the terms, conditions, and limitations of the applicable plans, the employer will provide medical insurance benefits until the end of the month in which the leave begins. If insurance is to remain in force, you must pay the full share of the premium either through increased payroll deductions before the leave begins (when the need for the leave is foreseeable) or, if you prefer, through separate payments that are made by you to the employer every pay period. Please let us know your decision before the leave begins. If you do not pay the total amount of the premium, coverage will discontinue. ! ! ! 31 !253 ! ! EMPLOYEE BENEFITS ! Benefits such as sick time, holidays and vacation time are earned for the full month in which you work at least 50 percent of the time. Paid time off, such as vacation time or paid sick time, count as time worked. ! When you return from leave, benefits will again be provided according to the applicable policies and plans. ! Reinstatement to Work—so that your return to work can be properly scheduled, please provide at least 30 days advance notice in writing of the date you intend to return to work. If you take a leave because of a personal serious health condition, you must provide a note from your physician verifying that you are able to return to work and can assume your regular work duties. The letter must also state if there are any restrictions pertaining to duties or the number of hours you can work (see Medical Release To Work, Form #112). ! Unless applicable state or local laws require otherwise, reinstatement cannot be guaranteed to any employee returning from medical leave. Employees will be notified about any such right to reinstatement before their leave begins. We will endeavor to place employees returning from leave in their former position or in a position comparable in status and pay, subject to budgetary restrictions, the company’s need to fill vacancies, and the ability to find qualified temporary replacements. ! Accepting outside or supplemental employment while on a leave will result in the employee’s discharge. ! Voluntary Termination—you are considered to have resigned voluntarily: !When not returning to work on the scheduled day of return !When the purpose for requesting the leave was misrepresented !When the request for a leave of absence is denied and you take time off anyway !When no position is available at the end of the leave !When reporting requirements are not met !When your return would place an “unreasonable burden” on the employer ! ! PERSONAL LEAVE OF ABSENCE A personal leave may be granted to eligible employees who wish to take time off work to fulfill personal obligations due to an exceptional or emergency nature. ! Eligibility—regular full-time, regular part-time and per-diem employees may request a leave of absence for personal reasons. Eligible employees may request a leave after having completed 6 months of employment. Exceptions to the length of service requirement will be considered at the employer’s sole discretion. ! A Request for a Leave Of Absence—a request for a personal leave must be submitted in writing at least 30 days in advance or as early as possible for unforeseeable events. Your desire to return to work and a date of return must be agreed upon in writing. The employer reserves the right to approve or deny any request for a leave of absence. ! ! 32 !254 ! ! EMPLOYEE BENEFITS ! Length of Leave—a leave of absence may be granted for a period of up to four weeks. If four weeks proves to be insufficient, the time may, at the employer’s discretion, be extended to a maximum of 3 months. You will be required to use any accrued paid vacation, unused holidays or sick leave time before taking a personal leave. Any combination of medical leave and accrued paid time may not exceed the approved time for the leave. ! Reporting on Progress—you are required to report directly to the employer every 30 days on your status and your continued intention to return to work. ! Salary and Benefits—the leave of absence is without pay and you do not accrue seniority while on a personal leave of absence. Benefits such as medical insurance, sick time, holidays and vacation times are not earned and do not accumulate during the leave. Subject to the terms, conditions, and limitations of the applicable plans, the employer will provide medical insurance benefits until the end of the month in which the leave begins. If insurance is to remain in force, you must pay the full share of the premium either through increased payroll deductions before the leave begins (when the need for the leave is foreseeable) or, if you prefer, through separate payments that are made by you to the employer every pay period. Please let us know your decision before the leave begins. If you do not pay the total amount of the premium, coverage will discontinue. ! Benefits such as sick time, holidays and vacation time are earned for the full month in which you work at least 50 percent of the time. Paid time off, such as vacation time or paid sick time, count as time worked. ! When you return from leave, benefits will again be provided according to the applicable policies and plans. ! Reinstatement to Work—so that your return to work can be properly scheduled, please provide at least 30 days advance notice in writing of the date you intend to return to work. ! Unless applicable state or local laws require otherwise, reinstatement cannot be guaranteed to any employee returning from a personal leave. Reinstatement is at the employer's discretion. ! Accepting outside or supplemental employment while on a leave will result in the employee’s discharge. ! Voluntary Termination—you are considered to have resigned voluntarily: !When not returning to work on the scheduled day of return !When the purpose for requesting the leave was misrepresented !When the request for a leave of absence is denied and you take time off anyway !When no position is available at the end of the leave !When reporting requirements are not met !When your return would place an “unreasonable burden” on the employer ! ! ! ! ! 33 !255 ! ! ! ! EMPLOYEE BENEFITS MEDICAL LEAVE OF ABSENCE FOR OCCUPATIONAL DISABILITIES A leave of absence may be granted to employees who are temporarily unable to work due to a work-related injury or disability. Some states recommend that an employee on a medical leave of absence for occupational disabilities, be allowed to continued until s/he is “medically stable.” A decision to terminate leave will be based on all facts relevant to each employee’s situation. ! A Request for a Leave Of Absence—a request for a disability leave must be submitted in writing at least 30 days in advance or as early as possible for unforeseeable events. A healthcare provider's statement must be submitted in writing verifying the reason for the disability and the leave’s beginning and expected ending dates. Any changes are to be promptly reported to the employer. If you wish to return to work after the leave, please submit a statement to that effect before the start of the leave or you will be considered to have voluntarily resigned from employment. ! Length of Leave—based on legal requirements, a leave of absence will be granted for a period of up to 12 weeks or to the end of the disability, whichever comes first. If 12 weeks proves to be insufficient, an extended leave will be granted according to federal and state workers’ compensation regulations. ! You will be required to use any accrued paid vacation, unused holidays or sick leave time before taking a disability leave. Any combination of disability leave and accrued paid time may not exceed the approved time for the leave. The total time of all absences related to the same medical condition is considered part of the same leave. ! Leave of absence for occupational disabilities ends when: !The employee is released for full or partial duty. The employee must provide a physician’s statement in writing indicating the employee’s fitness to return to work !The employer receives satisfactory medical evidence that the employee is unable to return to work !The employee directly or indirectly informs the employer (for example, by accepting employment elsewhere, moving out of state, etc.) that he or she does not intend to return to the practice !The employee has been on a medical leave of absence for the approved time !If for business or economic reasons, the job is not available !When your return would place an “unreasonable burden” on the employer ! Reporting on Progress—you are required to report directly to the employer every 30 days on your status and your continued intention to return to work. ! FMLA—if the employer is covered by the Family Medical Leave Act (see FMLA in this section) a workers' compensation leave is designated as FMLA leave. Therefore, when applicable, the provisions of the FMLA govern health benefits continuation. ! Salary and Benefits—the leave of absence is without pay and you do not accrue seniority while on a personal leave of absence. Benefits such as medical insurance, sick time, holidays and vacation times are not earned and do not accumulate during the leave. Subject to the terms, conditions, and limitations of the ! 34 !256 ! ! EMPLOYEE BENEFITS ! applicable plans, the employer will provide medical insurance benefits until the end of the month in which the leave begins. If insurance is to remain in force, you must pay the full share of the premium either through increased payroll deductions before the leave begins (when the need for the leave is foreseeable) or, if you prefer, through separate payments that are made by you to the employer every pay period. Please let us know your decision before the leave begins. If you do not pay the total amount of the premium, coverage will discontinue. ! Benefits such as sick time, holidays and vacation time are earned for the full month in which you work at least 50 percent of the time. Paid time off, such as vacation time or paid sick time, count as time worked. ! When you return from leave, benefits will again be provided according to the applicable policies and plans. ! Reinstatement to Work—so that your return to work can be properly scheduled, please provide at least 30 days advance notice in writing of the date you intend to return to work. ! You must provide medical certification verifying that you are able to return to work and to perform safely and satisfactorily your regular work, or stipulate any restrictions pertaining to job duties or the number of hours you can work. ! Unless applicable state or local law requires otherwise, reinstatement cannot be guaranteed to any employee returning from a medical leave. You will be placed in your former position or in a position comparable in status and pay, subject to budgetary restrictions, the need of the practice to fill vacancies, and the ability to find qualified temporary replacements. ! Accepting outside or supplemental employment while on a leave will result in the employee’s discharge. ! Voluntary Termination—you are considered to have resigned voluntarily: !When not returning to work on the scheduled day of return !When the purpose for requesting the leave was misrepresented !When the request for a leave of absence is denied and you take time off anyway !When no position is available at the end of the leave !When reporting requirements are not met !When the length of the leave exceeds the allowable time (see above) !When your return would place an “unreasonable burden” on the employer ! PREGNANCY LEAVE OF ABSENCE ! The leave provisions referenced below are only applicable when required by state or federal law. ! A pregnancy disability leave is provided for employees who are temporarily unable to work due to a disability related to pregnancy, childbirth, or related medical conditions. (If more than 50 employees or the number specified by an applicable state family leave act if applicable to employers with less than 50 employees, see Family and Medical Leave Act (FMLA)). ! 35 !257 ! ! EMPLOYEE BENEFITS ! Reporting a Pregnancy—a health care provider’s statement must be submitted in writing verifying the expected pregnancy disability leave’s beginning and expected ending dates. Any changes in any of these dates are to be promptly reported to the employer. ! With a written request from your healthcare provider that you be transferred to a less strenuous or hazardous position, we will do our best to accommodate you. If we are unable to do so, and you are not able to continue your normal job responsibilities, you may be asked to go on a pregnancy leave. ! Health Hazards During Pregnancy Release Letter—pregnant employees may suffer personal injuries or problems with their pregnancy as a result of ergonomic risk factors. These may lead to premature delivery and reduced gestational age, low birth weight babies, and spontaneous abortion or miscarriage. If you continue to work during your pregnancy, it will be necessary for you to sign a release agreement taking full responsibility for any possible consequences due to work-related health hazards to yourself and the unborn child. The agreement reads: ! It is our understanding that you are pregnant and wish to continue working in your capacity as a ________________________________. You should be aware that scientific evidence indicates that a pregnant woman's exposure to x-ray radiation, as well as other types of health hazards, that is, chemical/ toxic hazards and strenuous physical requirements, may pose a significant risk to the fetus. There is a likelihood that you and your fetus will be exposed to at least some of these risks during your pregnancy if you continue to work at your present capacity. !Due to the office's limited staff, you may often be the only employee on duty who is qualified or available to perform tasks that could pose a health hazard. While we will attempt to limit your exposure, there will inevitably be times when you must perform the duties assigned to your job function. !You may request a transfer to another job assignment and, if a position is available and you are qualified, we will do our best to accommodate you. !If you decide to continue working for us as a _____________________________________ we will certainly allow you to do so, provided you and your physician deem it safe and you are willing to assume the risks associated with such possible health hazards. If you are willing to take full responsibility for any possible consequences in assuming such risk, other than illnesses or injuries that would normally be covered under Workers’ Compensation, please indicate so with your signature below. !You may request a pregnancy disability leave if you or your physician feels that continued performance of your responsibilities may present a hazard to you or the child. !Please feel free to consult with your physician and attorney before you sign this letter. Return the letter ! within ten days from the above date. Request for a Leave Of Absence—a request for a pregnancy disability leave must be submitted in writing at least 30 days in advance or as early as possible for unforeseeable events. If you wish to return to work after the leave, please let us know before the start of the leave or you will be considered to have voluntarily resigned from employment. (Use Leave Of Absence Application, Form # 409). A pregnancy leave will be counted against any FMLA entitlements (See FMLA later in this section.) ! ! 36 !258 ! ! EMPLOYEE BENEFITS ! Length of Leave6—when required by state or federal law, a leave of absence will be granted for a period of up to four7 (4) weeks. If the initial period of approved absence needs to be extended because of medical complications related to the pregnancy, the leave can be extended up to a total of three8 (3) months pending written verification from your certified health care professional. Any request for a pregnancy-related disability leave must be accompanied with a certified healthcare professionals statement verifying the disability and the leave’s beginning and expected ending dates. Since the leave is without pay9, you may, at the employer’s option, take any accrued paid vacation and/or sick leave to run concurrent with the pregnancy leave. ! A request for a leave of absence beyond the allotted time will be considered on the same basis as a request for a personal leave of absence. ! Reporting on Progress—you are required to report directly to the employer every 30 days on your health status and your intent to return to work. ! Pregnancy leave of absence ends when: !The employee is released for full or partial duty. The employee must provide a physician’s statement in writing indicating the employee’s fitness to return to work !The employer receives satisfactory medical evidence that the employee is unable to return to work !The employee directly or indirectly informs the employer (for example, by accepting employment elsewhere, moving out of state, etc.) that he or she does not intend to return to the practice !The employee has been on a medical leave of absence for the approved time !If for business or economic reasons, the job is not available ! Salary and Benefits—the leave of absence is without pay and you do not accrue seniority while on a personal leave of absence. Benefits such as medical insurance, sick time, holidays and vacation times are not earned and do not accumulate during the leave. Subject to the terms, conditions, and limitations of the applicable plans, the employer will provide medical insurance benefits until the end of the month in which the leave begins. If insurance is to remain in force, you must pay the full share of the premium either through increased payroll deductions before the leave begins (when the need for the leave is foreseeable) or, if you prefer, through separate payments that are made by you to the employer every pay period. Please let us know your decision before the leave begins. If you do not pay the total amount of the premium, coverage will discontinue. Benefits such as sick time, holidays and vacation time are earned for the full month in which you work at least 50 percent of the time. Paid time off, such as vacation time or paid sick time, count as time worked. 6 Since state laws change, check periodically with your State Labor Commission for the latest regulations regarding length of leave requirements. 7 8 9 California six (6) weeks; Puerto Rico – 8 weeks (4 before delivery and 4 after) California – four (4) months (88 working days if working 5 days per week) Puerto Rico – with pay and benefits ! 37 !259 ! ! EMPLOYEE BENEFITS ! When you return from leave, benefits will again be provided according to the applicable policies and plans. ! Returning From Pregnancy Leave—if you wish to return to work earlier than the date agreed upon at the start of the leave, the employer will reinstate you no later than the agreed upon date or earlier if possible. However, business reasons may prevent the employer from having you return before the agreed upon date. ! Reinstatement to Work—so that your return to work can be properly scheduled, please provide at least 30 days advance notice in writing of the date you intend to return to work. ! If you take a leave because of a personal serious health condition, you must provide a note from your health care provider verifying that you are able to return to work and can assume your regular work duties. The letter must also state if there are any restrictions pertaining to duties or the number of hours, you can work. (See Medical Release To Work Form #112). ! Unless applicable state or local laws require otherwise, reinstatement cannot be guaranteed to any employee returning from medical leave. Employees will be notified about any such right to reinstatement before their leave begins. We will endeavor to place employees returning from leave in their former position or in a position comparable in status and pay, subject to budgetary restrictions, the employer’s need to fill vacancies, and the ability to find qualified temporary replacements. ! Accepting outside or supplemental employment while on a leave will result in the employee’s discharge. ! Voluntary Termination—you are considered to have resigned voluntarily: !When not returning to work on the scheduled day of return !When not returning within the allowed time for a pregnancy leave (see Length of Leave above). !When the purpose for requesting the leave was misrepresented !When for business or economic reasons the job is not available !When reporting requirements are not met !When you have not supplied a written statement of your intent to return to work (must be provided with the request for a leave of absence) !When your return would place an “unreasonable burden” on the employer ! Leave For Adoption—pregnancy leave is interpreted to include situations "where the family unit is increased by adoption rather than natural birth.” The leave will be granted for a period of four weeks. This allows a parent to be at home with the child during the first few weeks of adjustment. If more time is needed a request should be submitted for a personal leave of absence (for other details refer to Pregnancy Leave and Personal Leave). ! ! BREASTFEEDING RIGHTS AND PUMPING MILK While not required by federal law, our female employees who choose to breastfeed are offered lactation rooms as feasible given our building accommodations or as required by state law, whichever provides the greatest benefit to our employees. This is intended to allow employees who are new mothers to return to ! 38 !260 ! ! EMPLOYEE BENEFITS ! work more easily and create goodwill and a more productive atmosphere. This time shall run concurrently with breaks if possible. If additional time is needed it can be taken as unpaid time off if, in the opinion of the business owner, it does not disrupt normal operations of the practice. ! ! UNEMPLOYMENT INSURANCE If employment is terminated, you may be eligible to receive unemployment insurance. The insurance provides financial assistance to employees who become unemployed through no fault of their own. Consequently, when employees are at fault, such as resigning voluntarily or being discharged for unprofessional conduct (refer to Responsibility and Conduct), they may lose eligibility for unemployment benefits. In order to receive unemployment benefits, a claim must be filed at the local office that administers the state's unemployment insurance law. ! ! STATE DISABILITY INSURANCE (CA., HI, N.J., N.Y., P.R., R.I. at this time. Other states may follow.) Employees who suffer from a non-work-related illness or injury may be entitled to State Disability Insurance (SDI). SDI provides low cost disability protection if an illness or injury not caused by the job prevents you from working. In the states in which SDI is required, a small percentage of each employee’s wages, up to the prevailing maximum, is deducted each pay period to finance this mandatory insurance. To initiate a claim, telephone the nearest State Disability office to request the necessary forms. During the waiting period before disability payments begin, you can take earned and unused sick leave. This will help to compensate for any lost wages during the waiting period. ! ! SOCIAL SECURITY As an employee of the practice, you are covered under the provisions of the federal social security law (FICA). If any employee's earnings stop because of death, disability, or retirement, then the employee and his or her family (if requirements are met) may be eligible for the lost earnings to be replaced in part from the fund. Social security insures basic retirement payments, Medicare, disability payments, death benefits for survivors, and burial allowance. The amount of deduction from your wages for social security taxes is matched by the practice. ! ! WORKERS' COMPENSATION Employees are covered by workers’ compensation insurance for work-related injuries or occupational diseases. Your employer pays this insurance. ! Benefits—workers’ compensation benefits provide medical, surgical, and hospital treatment, in addition to payment for loss of earnings that result from work-related injuries. Benefits include: !Cash benefits for both impairment and disability (disability payments cover certain physical problems, while impairment benefits cover disability and loss of wages) !Medical benefits within the legislated limits !Rehabilitation benefits, including both medical rehabilitation and vocational training for cases involving severe disabilities ! 39 !261 ! ! EMPLOYEE BENEFITS ! ! Compensation paid to an injured worker is decided by a rate set by law—usually a percentage of a regular weekly wage with a fixed maximum and minimum amount, subject to a total maximum limitation figure !Compensation payments typically begin from the first day of an employee’s hospitalization or after the third day following the injury if an employee is not hospitalized ! ! Reporting injuries—if you are injured while working, notify the employer immediately and fill out the Accident Report (Form #113), regardless of how minor the injury may be. Failure to report an accident can result in a violation of legal requirements, and can lead to difficulties in processing benefit and insurance claims. The practice will not pay for any medical treatment given before the employer was made aware of the injury. ! All injuries involving time off must be reported to the branch of government responsible for Workers’ Compensation matters. Serious injuries, illnesses, or deaths must be reported to the branch of the government responsible for Workers’ Compensation. The employer will file injury reports with the insurance carrier within five days after the injury occurs. Check the posted information for the name of the insurance carrier and the expiration date of the present insurance coverage. ! Our insurer regularly reviews and audits medical claims for indications of fraud. Persons who willfully make false statements or conceal material facts to obtain disability benefits may be punished by both imprisonment and fines. Employer do!263262262 ! ! es not discriminate or retaliate against employees who have filed legitimate workers' compensation claims ! Disclaimer notice—the employer or the insurance carrier may not be liable for the payment of any worker’s compensation benefits for any injury that arises out of an employee’s voluntary participation in any off-duty recreational, social, or athletic activity that is not part of the employee’s work-related duties. ! ! PARENTAL LEAVE FOR SCHOOL VISITS Some states have enacted laws that grant leave so employees can attend meetings or events at their children’s schools or day-care centers, although these requirements vary from state to state. School leave entitlements range from four to 40 hours per year; four, eight, or 16 hours per year are common requirements. A few states do not specify a leave allotment and instead require time off if an employee’s child has been suspended or is involved in other disciplinary or juvenile justice proceedings. Because of the variation with requirements, check with your local state bureau of labor for specific parental leave requirements. ! ! UNIFORMED SERVICES EMPLOYMENT AND REEMPLOYMENT RIGHTS ACT The 1994 Uniformed Services Employment and Reemployment Rights Act (USERRA), guarantees that employees who are activated for military duty, including Army, Navy, Air Force, Marine Corps, Coast Guard, and their reserves, be re-employed when they return to civilian life again. ! ! ! 40 !262 ! ! EMPLOYEE BENEFITS ! Returning employees must be reinstated to the same position and benefits to which they would have been entitled if continuously employed. This includes seniority, seniority-tied increases in vacation and sick-day accrual rates, pay raises based on longevity, and promotions based on longevity or length of service that they were reasonably certain to have achieved. ! USERRA requires that returning employees be "promptly reemployed." What is considered "prompt" generally depends on the circumstances and how long the employee has been on military leave. ! The only exceptions are: "If the total time of uniformed service exceeds five years, "If the returning employee does not notify the employer of his/her intent to return to employment within specified periods of time based on length of service and/or new or aggravated injury. "If a disability was incurred or aggravated by military service such that the returning employee is unable to perform the job responsibilities at the time of reinstatement. ! If a returning employee’s position was discontinued during a military leave, any severance pay that would have been paid is due upon his or her return. If the returning employee was on a recall list at the time he entered military service, he must be returned to the recall list upon completion of his service. ! ! Other Important USERRA Provisions: "All employers are covered, regardless of size, as is every employee, regardless of length of service or part-time status. The only exclusions are workers employed for brief, nonrecurring periods. "Service includes inactive and active duty for training, active duty and full- time National Guard duty. Absences required for examinations to determine fitness to perform military duty are also covered. "Employees must provide written or oral notice of their need for military leave unless military necessity prevents giving notice or it would be unreasonable or impossible to give notice. "Employers must not discriminate or retaliate against any person who applied for, serves, or has served as a member of a "uniformed service" including the Army, Navy, Air Force, Marine Corps, Coast Guard, and their reserves. "Employers must grant a leave of absence for up to five years to any person who is absent from a job because of military service. "Employers must place a returning employee in the position he or she would have held had employment not been interrupted by military service. ! ! ! 41 !263 ! ! POLICIES ! HEALTH AND SAFETY (If available, refer to the OSHA or Safety Manual for additional health and safety procedures.) It is our goal to provide a completely safe workplace for every one of our employees. Prevention of workinduced injuries and illness is our common goal for a safe and healthful working environment. ! We will comply with all applicable occupational safety regulations concerning employees exposed to blood or other potentially infectious materials. Universal precautions, engineering and work practice controls, and personal protective equipment will be utilized to limit the spread of diseases in the work place. A system of precautions will generally include elements such as: !Identification of tasks and jobs involving a risk of exposure to blood or other potentially infectious materials !The use of protective barriers, such as gloves and goggles, by employees who are exposed to blood or bodily fluids or who are required to handle contaminated items and to clean contaminated areas !Procedures for the handling and disposing of potentially infectious materials, clothing, and other items !Provisions for the cleaning and disinfecting of work areas or equipment contaminated with blood or bodily fluids with a suitable disinfectant !Procedures for providing hepatitis B vaccinations, when required, and post-exposure follow-up !Employee training and familiarization with appropriate work and emergency procedures !Labeling areas and objects of potential infection ! In most circumstances, you may not refuse to work because you are afraid of contracting a life-threatening illness from a co-worker or patient. Employees concerned about being infected with a serious disease by a co-worker, customer, patient, or other person, should convey their concern to their employer. ! Employees who refuse to work with or perform services for a person known or suspected to have a serious disease, without first discussing their concern with the employer, will be subject to discipline, up to and including termination. ! Safety and health program includes: !Providing safeguards – mechanical and physical !Conducting safety and health inspections to find and eliminate unsafe working conditions or practices, to control health hazards, and to comply fully with OSHA safety and health standards for every job !Training all employees in good safety and health practices !Providing necessary personal protective equipment and instructions for use and care !Developing and enforcing safety and health rules and requiring that all employees cooperate with these rules as a condition of employment !Investigating – promptly and thoroughly – every accident to find out what caused it !Correcting the problem so it will not happen again !Setting up a system of recognition and awards for outstanding safety service or performance ! ! 42 !88 ! ! POLICIES Everyone is responsible for safety. If you see an unsafe or hazardous condition, report it immediately. To avoid injuries, please observe the following important precautionary measures. ! When faced with an emergency: !Stay composed !Walk briskly if necessary !Do NOT run! ! When lifting: !Plan what you want to lift and don’t be in a hurry !Separate your feet a shoulder width apart to give you a solid base of support !Bend at your knees, not at the waist !Keep your back straight !Avoid twisting your body and point your toes in the direction you want to move !Lift with your legs, not your back ! Store materials and equipment safely and neatly; avoid clutter that might cause accidents. ! General housekeeping is everyone's responsibility. ! Report equipment defects to your employer immediately. Repairs are to be made by authorized maintenance personnel. Do not operate defective equipment. ! Do not climb on or into any shelving or fixtures. ! Wear safe and appropriate footwear. Walking barefoot is prohibited !Keep exit doors, fire exits, or electrical panels unlocked !Safety glasses must be worn in all applicable and requisite situations ! In The Event Of Fire—follow any specific procedures as outlined for your office or building: "Keep calm "Call the fire department; know the emergency phone number "Use stairways or other alternative exits; do NOT attempt to use the elevator "If trapped in the office, keep the doors closed and seal any cracks (with wet towels if possible) "Open or break a window for air and call for help; do not panic or jump ! The best rule of all...BE PREPARED. Be sure that: !All fire extinguishers are checked and in proper working condition !You know where each extinguisher is located !You are familiar with the right procedure for their use !You are familiar with all OSHA and safety and health requirements ! ! ! 44 !89 ! ! POLICIES ACCIDENTS OR INJURIES (For details, refer to the OSHA or safety manual) ! If you experience or witness an accident in which an employee, patient, or visitor sustains a personal injury, regardless of how serious, immediately report the situation to your employer. Likewise, employees who are exposed to occupational health hazards or suffer a job-connected health injury must report it immediately. Non job-related injuries that might be aggravated on the job or adversely affect job performance are also to be reported. Failure to report an accident or injury can result in a violation of legal requirements and can lead to difficulties in processing insurance and benefit claims. ! SAFETY SHIELDS Safety shields are to be worn during certain clinical and/or laboratory procedures, as required by law. The office will supply nonprescription safety shields for each employee's use. ! ! SMOKING Because of the overwhelming evidence that smoking is dangerous and injurious to a person's health, employees are encouraged not to smoke. However, we recognize that the decision to smoke or not to smoke is a personal one. ! Smoking, or carrying the scent of having smoked, is prohibited within the premises at all times. This policy is for the health and safety of all employees and our patients. Your cooperation is requested, as this policy must be rigidly enforced to comply with the health and safety requirements and to maintain proper insurance coverage for the building. ! CHEWING GUM Employees are not allowed to chew gum while on duty. The reason for this is, every now and then a staff member will chew gum with his/her mouth open, while talking to a patient. This is just plain rude. ! FOOD ! Food is never to be consumed in front of patients; nor is it to be left in their view. ! As with the rest of the office, it is everyone's responsibility to keep the area neat and clean. Dirty cups and utensils, old food, etc., must be cleaned or thrown away in order to keep it a pleasant place for all who use it. ! Beverages may be consumed at your desk provided they are in an appropriate container and cannot be easily spilled. There are to be absolutely no soda cans or bottles during office hours. Beverage containers of any type should never be placed on the same desk as a computer or other electronic equipment. ! ! ! 45 !90 ! ! POLICIES MAILBOX SYSTEM Each employee will have a mailbox to receive and distribute any and all written memo’s, mail, magazines, etc. All mail boxes should be kept empty as much as possible. It should never become a “storage bin” that never gets emptied. ! VOTING ! ! APPEARANCE You are expected to go to the polls before or after regular working hours. If that is not possible, you are to give at least two working days advance notice that time off during working hours is needed or we may not be able to provide you with voting time off. Unless required by state law, voting time is not time worked and will not be included for overtime calculation purposes. Employees are to wear professional, neat, clean, and tasteful clothing. Immoderate hairstyle, rings, ornaments, tattoos, ornamental piercings, or colors are unacceptable. Please keep nails neatly trimmed and clean at all times. Close contact with patients necessitates meticulous attention to personal and oral hygiene. For example, the smell of cigarette smoke or the eating of malodorous foods such as garlic and onions, may offend patients and coworkers. Any request for a deviation in the Appearance or Uniform Policy must be submitted in writing. However, such requests are not likely to be approved if they cause any potential undue hardship to the business, or do not meet the Safety or Uniform Policy requirements of the practice, or might infringe on other employees’ rights. ! Women—light jewelry is permitted. Unusual, large, or unprofessional jewelry is not permitted. ! It is preferred that hair be worn short or shoulder length. If hair is longer, it is to be tied back in a neat manner so as not to interfere with the performance of duties. ! Nails are to be manicured and their length should not interfere with the execution of duties. ! Make-up and perfume are to be kept to a minimum. ! Men—face to be shaved and/or mustaches, beards, and sideburns neatly trimmed. Hair is to be clean, well trimmed, and well groomed. ! Men and Women—shoes should not be made of cloth, but of real or synthetic leather that can be scrubbed, sprayed, polished and buffed. Shoelaces should be clean and in good condition. For certain positions, the employer must approve exceptions to this policy. ! ! UNIFORM POLICY We will provide, replace, and launder all uniforms that fall in the category of “personal protective equipment” as required by OSHA. (OSHA regulations are not within the scope of this manual—please refer to OSHA regulations and other regulatory requirements on the subject.) ! ! 46 !91 ! ! POLICIES You are responsible for purchasing, laundering and maintaining your own uniforms. All dental assistants and hygiene staff are to wear long sleeves, close toed shoes and protective clothing. We provide throw away gowns and protective glasses. Please refer to the OSHA manual for further information. ! SOLICITATION ! To prevent disruptions and in order to protect employees from interference in their work, demonstrating or selling a non-work related product during work hours is prohibited. Non-employees are prohibited from trespassing, soliciting, or distributing literature on office property. ! ! PERSONAL DATA CHANGES The employer must keep certain personnel records in order to comply with legislated record keeping and reporting requirements. These records are confidential and only available to authorized personnel. So that we can keep the records updated, please report any of the following changes when they occur: !Name !Address !Telephone number !Number of dependents (a new W-4 form must be completed for income tax withholding purposes within 10 days of the change if the change results in a decrease in the number of dependents) !Marital status !Education (courses completed and other training or skills acquired) !Selective service status !Physical or other limitations !Beneficiary designations for insurance, disability, pension, and profit sharing plans !Person(s) to notify in case of an emergency ! ! ! PERSONNEL RECORDS Employees are requested to help keep their record up-to-date by informing the employer of any changes in personal information—for example, home address, telephone numbers, tax withholding information, and emergency contacts. An employee can add a statement to qualify or counter information in their personnel files. The statement must be factual and directly relevant to the employee's performance or employment qualifications. ! A third party may subpoena employment records from a current or former employer. If employment records are subpoenaed, the employee must be notified and has the right to object to production of the records. ! Security and Confidentiality—the physical safety and privacy of personnel records must be secured at all times. Physical safeguards include locked files and/or special computer access codes. Entry to the files is strictly limited to authorized personnel only on a need-to-know basis. ! Inspection of Records—employees and past employees may inspect and copy certain documents in their personnel files. These inspections are limited to no more than twice in a 12-month period. A request for an appointment to review the file with the employer present must be submitted in writing to the Office Manager. ! 47 !92 ! ! POLICIES ! 1. The following types of records are available for review: "Employment applications and personnel action forms (including those for promotions, salary changes, and job title changes) "Form I-9, Employment Eligibility Verification Form, and other documents related to employment eligibility and identity "Form W-4 and related tax withholding information "Time cards and attendance records "Performance appraisals "Awards and commendations "Accident reports "Records regarding workplace exposures to toxic substances and any related medical information in employer's possession "Warnings, reprimands, and other documents related to disciplinary actions (excluding documents prepared in connection with ongoing investigations. See below) "Any reported problems or concerns reported by the employee (Form #422) "Medical records. (At employer’s discretion, medical records may be released to the employee’s physician rather than to the employee. See below for information on excluded medical documents.) "Workers' compensation information, including claims, injury reports, and medical reports "Fringe benefit enrollment and election forms, including designation of beneficiary forms "Pension and retirement enrollment and election forms "Emergency contact information; and biographical information ! 2. The following types of documents are not accessible to employees: "Pre-employment reference information, including letters, notes, and information provided by prior employers or from other relevant sources (information gained from public records will be made available to employee) "Medical records that the employee can obtain from his or her healthcare provider "Records relating to ongoing investigations of policy violations, prohibited conduct, or criminal offenses "Documents developed or prepared for use in grievance or court procedures ! ! ! ! NOTE: Documents will be retained in accordance the requirements of federal and state law. An employee can request copies of any documents that the employee previously had provided to employer or that had previously been provided to the employee. ! ! PARKING You may park behind the building in the municipal parking lot. Parking on the streets is typically limited to 2 hours at a time, per the Granville Police. Remember to lock your car, the practice will not be responsible for damage or theft to personal automobiles or property. ! 48 !93 ! ! ! POLICIES ! PRACTICE PROPERTY OR EQUIPMENT Property or equipment belonging to the practice may not be removed from the premises without written approval. You will be responsible for the proper care and return of all property and equipment assigned to your possession. Desks, lockers, computers or other storage devices, as well as any articles or information found within them, may be inspected by the employer or authorized personnel at any time, either with or without prior notice or consent. Personal use of office materials or postage is absolutely not permitted for any reason at any time. ! PURCHASING AUTHORITY ! No employee or other contract labor personal has purchasing authority unless given explicitly or else they will be personally financially responsible for all paid for yet unapproved items. The Office Manager’s are authorized to purchase items thru the office debit card. For an Office Manager, any item other than postage over the amount of $50 must receive approval using a CSW, Form #118 from the Chief Financial Officer (CFO). ALL EMPLOYEES OTHER THAN the Office O/M’s MUST submit a CSW for approval for ALL items of any value. Approval of a CSW must be sumitted to the CFO. ! ! OFFICE SECURITY The employer takes no responsibility for employees’ personal belongings that are lost, damaged, stolen or destroyed. ! Some employees are provided with a desk or a locker for their use during work. Prohibited materials, including weapons, alcohol, non-prescribed drugs or medications, may not be placed in a desk or locker. Perishable items should not be left for a prolonged period. ! Do not make duplicate office keys. Please notify the employer immediately if your key is lost. ! No outside agency, inspector, visitor, inquirer, salesperson, or ex-employee may enter the treatment rooms or office from the reception room without permission. ! Employees are not to discuss the security system or code with any unauthorized person. Violations will result in immediate dismissal. ! ! ! ! ! VIOLENCE PROTECTION POLICY In our effort to make our practice safe, we do not tolerate any type of workplace violence committed by or against employees. The following list of prohibited behaviors relevant to employees and clients is intended to be descriptive but not restrictive: "Causing physical injury to another person. "Making threatening remarks. ! 49 !94 ! ! ! POLICIES "Aggressive or hostile behavior that creates a reasonable fear of injury to another person or subjects another individual to emotional distress. "Intentionally damaging employer, employee or client property. "Possession of any type of weapon in the workplace. That includes someone who holds a license to carry a concealed handgun. The workplace applies to parking lots, buildings, cars, employees who are off the property but performing a task for the practice and/or employer sponsored recreational events (i.e., picnics, etc.). Any suspected violation will be acted upon as required by law. "Committing acts by, or related to sexual harassment or domestic violence. Any violations of this policy or any potentially dangerous situations must be immediately reported to management and can be cause for immediate dismissal. ! ! PERSONAL TELEPHONE AND CELL PHONE USE The office telephones are intended solely for business use and are not to be used for personal calls. Accordingly, receiving or making personal telephone calls on the office telephones of a non-emergency nature is not allowed without permission. No personal long distance or toll calls are to be charged to the employer's phone. For training purposes and to maintain quality communication with our patients, the phone lines may be monitored from time to time. Incoming personal calls, other than emergencies, cannot be taken during working hours. In such instances, messages will be taken in writing and routed to your mail box. Personal cell phone and/or integrated camera use is to be made away from the areas where patients are located and should be made or taken only during meal or break periods. Cell phones are to be turned off during periods the employee is not on a meal or rest break. Violation of this rule may result in a loss of bonus for that period. ! ! OUTSIDE EMPLOYMENT (MOONLIGHTING) You are expected to devote your full efforts to the interests of the practice during normal working hours and any additional hours that may be required. If you decide to work at another job, it must not divert your time, interests, or talents away from the satisfactory accomplishment of your work responsibilities. Outside employment is not a satisfactory reason for poor performance, absenteeism, tardiness, or refusal to work overtime. You are not eligible for a paid absence when the absence is caused by circumstances related to the second job. ! ! ! ! CONFIDENTIALITY AND NON-DISCLOSURE The practice makes available to each employee certain confidential information, including but not limited to patients' names, treatment histories, addresses, communications, files, bills and payment records; as well as office forms, manuals, etc. These items are of substantial value, highly confidential, and constitute the professional and trade secrets of the employer. They are provided and disclosed to the employee solely for use in connection with the employment. In adherence with HIPAA regulations and this confidential and non-disclosure policy, each employee shall: ! 50 !95 ! ! POLICIES Regard and preserve the information as highly confidential and the trade secrets of the employer, such information is not to be discussed away from the premises or within hearing distance of any patient or unauthorized person !Not disclose, nor permit to be disclosed, any of the information to any person or entity !Not photocopy or duplicate, and shall not permit any person to photocopy or duplicate, any of the information without employer's consent and approval !Not make use of the information for their own benefit or the benefit of any person or entity other than the employer !Continue to keep any information inviolate even after termination of employment ! ! When discussing confidential matters at the office, keep voices at a low level. Be particularly aware of what is said at the front desk and outside of the treatment rooms, as patients easily overhear it. ! Patients should not be exposed to discussion of internal office matters. For example, if a patient's ledger or chart cannot be located or there is a scheduling conflict, the patient does not need to be told this information. ! Employees are not to release personal information regarding present or former employees, that is, phone number, address, etc., without the employee's specific and prior approval in writing. ! Employees handling confidential information, including personnel files, are responsible for its security and extreme care is to be exercised to ensure that it is safeguarded to protect the practice, each employee, the suppliers, the patients, and the employer. Any employee who violates this confidentiality and disclosure policy is subject to disciplinary action up to and including discharge, and possible legal action. ! Although not intended to discourage employees creativity, any system, idea, or communication developed during your employment with the practice is the property of the practice and remains so even after termination. ! HEALTH INSURANCE PORTABILITY AND ACCOUNTABILITY ACT (HIPAA) (If available, refer to a HIPAA implementation and administration manual for detailed information on requirements imposed by the Act) ! The Health Insurance Portability and Accountability Act (HIPAA) is a federal law enacted to protect the individual's health coverage “portability” and to limit the use of eligibility restrictions and/or pre-existing condition exclusions. All group health plans with two or more employees and all insurance carriers that sell group health coverage are subject to HIPAA regulations. Important features include: "Small businesses with 50 or fewer employees are guaranteed access to health insurance. No insurer can exclude an employee or an employee's dependent from health insurance coverage based on health status. This is important because, previously, insurers commonly refused to cover small businesses if an employee or a dependent had a serious medical condition; "Guaranteed Renewal and Availability of Insurance. Once an insurer sells a policy to any individual or group, it's required, with a few exceptions, to renew coverage regardless of the health status of any member of the group. ! 51 !96 ! ! POLICIES "Guaranteed Access for Individuals. People who lose their group coverage (because they quit, are fired, or change jobs) are guaranteed access to individual coverage. The coverage is available without regard to health status and renewal is guaranteed; and "Pre-existing Conditions. Workers and their covered dependents covered by group insurance policies can't be excluded from coverage for more than 12 months because of a pre-existing medical condition. And, if the employee or dependent previously had coverage for that condition, the exclusion is reduced for each month of previous coverage, assuming that there wasn't a break in coverage of more than 63 days. For example, if an employee was covered for cancer treatment for six months under a previous plan, then the exclusion under the new plan can only be for six months. Employers must also comply with HIPAA privacy regulations and adhere to the Act’s electronic transaction standards. ! ! PERSONAL PROBLEMS ! ! COMPUTER, EMAIL, AND INTERNET USAGE Employees are encouraged not to bring their personal problems to work, but sometimes it is unavoidable. If there is a severe problem that affects your ability to perform, it is to be discussed with the doctor or practice administrator. You can expect to find understanding and help toward finding a solution in the best interest of all concerned. Personal problems are not to be discussed within hearing distance of patients, guests, or other employees. Computers, computer files, email, instant messaging, internet access, and computer software furnished to employees are the property of the company and intended for legitimate business use in the course of your assigned duties only. Internet access includes, but is not limited to: e-mail, FTP, telnet, web browsing, workplace blogs, and usenet or newsgroups that are accessed on or from the business premises. ! We strive to maintain a workplace free of harassment. To that end, employees may not use the business provided computer or Internet services to: engage in illegal, fraudulent or malicious conduct; send, receive or store offensive, obscene, or defamatory material; annoy or harass other individuals or send e-mail of a personal nature; distribute or store chain letters, jokes, solicitations or offers to buy or sell goods. No employee may use the business internet access to post opinions on the internet, particularly any opinion of a political or discriminatory nature. ! Some computer files or software may interact poorly with existing software and may contain harmful computer viruses. Therefore, software or files may not be downloaded from the internet without prior authorization. Likewise, the illegal duplication of software and its related documentation is not permitted. ! Employer's right to monitor and access all office files, internet, e-mail, and instant messaging usage—all computer and system files must be accessible to the employer and are subject to unannounced inspections. Therefore, your employer will keep copies of all Internet and e-mail passwords and unauthorized passwords are prohibited. ! Employees are to notify their employer or any member of management of violations of this policy. Employees who violate this policy will be subject to disciplinary action, including termination of employment. ! 52 !97 ! ! POLICIES ! ! MAINTENANCE—HOUSEKEEPING ! ! GARNISHMENT OF WAGES ! ! USE OF PRIVATE VEHICLE ! ! ALCOHOL AND DRUG ABUSE Clean and orderly surroundings have a positive bearing on employees morale and productivity. Patients are favorably impressed and attracted to an office that looks professional and well maintained. It is your responsibility to keep work areas neat and tidy and to correct or report any conditions that detract from the professional image of the facility. A garnishment is a court order requiring the employer to remit part of an employee's wages to a third party in payment of a debt. Garnishments involve the employer in your personal affairs and result in considerable administrative and financial responsibilities for the practice. You are encouraged to work out a satisfactory solution to any indebtedness so that a garnishment will not become necessary. Also any services or goods sold to employee or direct family member unpaid to employer, after 30 days will be withheld from the most current paycheck/deposit. See form If you use your own vehicle on practice business, you will be required to provide proof of adequate insurance coverage. Documentation showing insurance coverage is to be given to the employer each time your insurance is renewed. Employees are not to use cell phones, beepers, two-way pagers, and the like, while they are driving on practice business. Being under the influence of any drug or alcoholic beverage on the job poses a serious risk to employees’ and patients’ health and safety. Therefore, employees are strictly prohibited from the illicit use, possession, sale, conveyance, distribution, or manufacture of illegal drugs, intoxicants, or controlled substances. Illegal activity and substance abuse, both on and off the job, can lead to termination. ! In addition, employees are strictly prohibited from the abuse of alcohol and prescription drugs. Legally prescribed medications are only permitted within the practice to the extent that the uses of such medications do not adversely affect your job performance, your safety or that of others. If you are using a drug or a medically prescribed medication that is known or advertised as possibly affecting or impairing judgment, coordination, or other senses or which may adversely affect the ability to perform work in a safe and productive manner, it is your responsibility to advise the doctor of this fact before reporting to work. ! Drug and Alcohol Testing—if there is reasonable cause to suspect that you are under the influence of any illegal or non-prescribed drugs, you may be required to immediately submit to a medical examination and/or to submit to urine, blood, saliva, breath, and/or hair testing for drugs or alcohol. The reasonable cause may be related to appearance, behavior, speech, excessive absenteeism, frequent accidents, declining performance, or situations involving safety, security, accidents, and the retesting of workers who have completed or are in a rehabilitation program. Employee acceptance of medical examinations and testing is a condition of employment. Therefore, refusal to submit to a drug or alcohol test will be considered ! 53 !98 ! ! POLICIES equivalent to a confirmed “positive” test and will result in immediate disciplinary action which may include discharge. ! Inspections to Administer and Enforce Policy—in order to promote a safe, productive, and efficient work place, the employer reserves the right to inspect any articles and property in the employees’ possession. The inspection may include lockers, desks, boxes, packages, lunch boxes, containers, and any other object on practice property. ! Notification of Criminal Charges—any employee charged with alleged use or possession of drugs or convicted of a criminal drug statute must notify the employer in writing within five calendar days. ! Any violation of this Alcohol and Drug policy will result in adverse employment action up to and including dismissal and referral for criminal prosecution. ! Employee Assistance—employees with substance abuse problems are urged to seek help. Alcoholics Anonymous (AA) and Narcotics Anonymous (NA) provides information and support. Local chapters are listed in the telephone directory. ! ! ACCEPTING ENTERTAINMENT, GIFTS, FAVORS, AND GRATUITIES No employee shall solicit or accept any gift, gratuity, favor, entertainment, reward, or any other item of monetary value that might influence or appear to influence the judgment or conduct of the employee in the performance of his or her job. Employees can accept gifts or entertainment only in cases where the gifts or entertainment are of nominal value, are customary in the industry, will not violate any laws, and will not influence or appear to influence the employee's judgment or conduct at his or her employer's business. ! GRIEVANCE POLICY ! ! If an employee has a grievance, the it must be submitted in writing to the Office Manager and receive a signature and date by the Office Manager on it’s notice that such grievance was received. ! ! ! 54 !99 ! ! ! ! 1. ! ! 2. ! 3. ! 4. ! EMPLOYEE RELATIONS COMMUNICATING AND RELATING TO PATIENTS Patients' needs are NUMBER ONE in importance. You must leave your personal problems and troubles outside the office. Patients come to our office to improve their health and get out of pain. An atmosphere of warmth, cheerfulness, and caring must be conveyed. Indifference to patients' problems will not contribute to this atmosphere. REMEMBER PATIENTS' NAMES and use them often when talking with the patients. Refer to the patient as "Mr.", "Mrs.", "Miss", "Ms", unless the patient invites you to call him/her by their first name. Do not give patients nicknames or refer to them as "Hon", "Darlin", or other pet names. Your statements to patients must be in keeping with the practice policy and the dentist’s image. When talking to patients regarding their progress, be reassuring and tell them they have the very best dentist and are in good hands. Tell them to follow the dentist’s instructions and that the dentist will do everything possible to make the patient comfortable, answer his questions, etc. Nontreating personnel should never make personal recommendations or a diagnosis concerning patients' problems, causes or treatments. Rather, tell the patient to be sure to discuss the situation with the dentist. If necessary, walk the patient to the front desk and help them make an appointment for a consultation with the dentist. Relay both positive and negative comments to the dentist. This enables him to communicate better with patients, answer questions, and avoid misunderstandings. Feel free to relay positive "wins" expressed by our patients at staff meetings. It is vital that you have an understanding of the dental profession. We encourage you to learn all you can about dental care and its scientific approach to the restoration and maintenance of the human body. RESPONSIBILITY AND CONDUCT Certain standards of personal integrity and human behavior are an integral part of good character and respect for the rights of others. Unprofessional conduct disrupts the orderly flow of business, hurts morale, and lessens the quality of patient care. As we explained elsewhere in this manual, employment with the practice is at the mutual consent of the employee and the employer, and employment may be discontinued at-will, at any time, by either the employee or the employer, with or without cause or advance notice. Although we do not exercise a formal system of discipline, an employee may, at the employer's discretion, be given a warning and the opportunity to correct a problem before discharge. The employer reserves the right to take any disciplinary action as deemed appropriate. ! ! ! ! ! ! ! 55 !188 ! ! EMPLOYEE RELATIONS ! ! UNPROFESSIONAL CONDUCT Identifying every type of conduct or performance considered unprofessional is impossible. However, to offer some guidance, we provide the following examples of conduct and performance problems that could result in disciplinary action, including discharge: ! 1. Unexcused or repeated absence or tardiness. 2. Unauthorized personal telephone calls or attending to personal affairs during work hours. 3. Misuse of electronic email or internet communications system. 4. Working unauthorized overtime. 5. Destruction or negligent abuse of office property. 6. Refusal to work scheduled or emergency overtime. 7. Posting, removing, or tampering with posted notices without permission. 8. Leaving premises during working hours without authorization. 9. The use of any equipment owned by the practice for personal reasons without permission. 10. Mishandling, misappropriation, or unauthorized removal or possession of the funds or property of the employer or other employees. 11. The use of any practice-owned equipment, including computers without permission. 12. Personal behavior outside the office which could be harmful to the reputation of the practice. 13. Inability to establish rapport with employer, other employees, or patients. 14. Unsatisfactory work performance and/or attitude. Violation of any employer policy, including policies described in this manual, as revised from time to time. 15. Improper disclosure of confidential information or adherence to all HIPAA requirements, including information contained in employee records. 16. Falsifying or destroying any records, including timekeeping records. 17. Reporting to work or working while under the influence of alcohol or illegal drugs. 18. Possession of alcohol or illegal drugs while on duty or on the employer's premises. 19. Illegal activity and substance abuse, both on and off the job. 20. Disloyalty, insubordination, misconduct, and/or engaging in rude or discourteous conduct. 21. Refusing to accept a reasonable and proper assignment. 22. Recording information or tampering with another employee’s attendance record. ! 56 !189 ! ! EMPLOYEE RELATIONS 23. Falsifying, making inaccurate entries, or omitting requested information on the employment application form or other company records. 24. The employer’s good faith belief that employee has knowingly given false statement(s). 25. Dishonesty, theft or fraud. 26. Noncompliance with acts and rules of the State Board of Examiners. 27. The possession of firearms within the practice. 28. Failure to use assigned safety equipment or failure to abide by safety rules and policies. 29. Creating or contributing to unsanitary conditions (this includes eating at your desk, lab or other workstation not designated as an eating area). 30. Refusal to work on a patient without employer’s permission. 31. Sexual harassment, religious harassment, or other unlawful harassment of another person. 32. Establishing a competing business during the employment or engaging in work that creates a conflict of interest in the opinion of the employer. 33. Refusal to sign the Performance Review form or other required employment-related documents. 34. Discussing work-related issues within hearing distance of patients. 35. Failure to report to work without providing adequate notice as described elsewhere in this manual. ! POSSIBLE CONSEQUENCES: As explained elsewhere in this manual, employment may be discontinued at-will, at any time, by either party, with or without cause or advance notice. Therefore, the following disciplinary procedures are advisory and not binding on the employer. At the employer's discretion the employee may be 1) given a written or oral warning (see Employee Counseling Memo Form #114), or 2) suspended from duty without pay, or 3) discharged from employment. ! HANDBILLS AND SOLICITATION ! Handbills are notices or advertisements. No handbills will be distributed on practice property without prior approval of the owner and office manager. ! Solicitation is urging the employees/patients to do or buy something. Unauthorized solicitation is strictly prohibited. ! ! ! PERFORMANCE APPRAISALS Performance appraisals are vital for future planning and they provide a timely, fair, and objective measurement of performance against requirements. Each employee may receive a performance appraisal at least once a year (see Performance Appraisal Form #203). ! 57 !190 ! ! EMPLOYEE RELATIONS ! New employees may be given a performance appraisal during their 90th to 120th day of employement (see New Employee Progress Report Form #202). Performance appraisals may be performed if needed at anytime. ! Performance appraisals may generally be held at the chosen time, but may be conducted more or less frequently, depending on the business needs of the employer. Salary adjustments will not automatically be made at the time of the performance evaluation. ! Employees are advised at least three days before the scheduled performance appraisal. This gives the employer and employee an opportunity to prepare so that areas of mutual concern can be addressed. The performance appraisal is designed to: !Maintain and improve job satisfaction by letting the employees know the employer is interested in their job progress and personal development !Serve as a systematic guide to recognize needs for further training !Assure a factual, objective analysis of an employee's performance versus job requirements !Help to place employees in positions within the practice that will best use their talents and capabilities !Provide an opportunity to discuss job problems or interest !Serve as an aid in salary administration !Provide a basis for coordinating organizational and individual goals and objectives !Give recognition for superior performance where applicable ! The Performance Appraisal addresses job factors and behaviors that are observable, measurable, and specifically related to job performance. The factors to be considered are: !Quality of Work !Quantity of Work !Job Knowledge !Employee Relations !Patient/Employee/Doctor Relations ! 58 !191 ! ! ! ! ! ! ! ! ! ! JOB DESCRIPTIONS ! ! ! ! See Job Descriptions Manual— Features “essential” job functions for each Position to satisfy The Americans with Disabilities Act (ADA) ! ! 59 !32 SEPARATION FROM EMPLOYMENT ! Employees serve “at-will” and those who quit, are discharged, or fail to respond to a recall, will be regarded as separated from employment. ! Separations are classified as either voluntary or involuntary and will be processed in accordance with the separation policies and procedures that follow. ! Voluntary—a resignation initiated by the employee. We realize that occasionally an employee resigns to pursue other interests. Although you may resign at will, at any time, with or without cause or advance notice, you are requested to provide at least two weeks’ advance notice, in writing (see Form #300), whenever possible. ! Although an employee may give several weeks notice, the employer may find it inefficient, disruptive or undesirable to permit the employee to work for the period specified and reserves the right to accelerate the effective date of the resignation. Severance or in-lieu-of-notice pay may be awarded at the employer's discretion (see below). ! Unauthorized Leave—if you request time off that is denied, and take the time off anyway, that time off will be considered job abandonment and treated as a voluntary termination. ! If the practice is sold or acquired and you are offered a position with the new owner and choose not to stay, you will be considered to have voluntarily resigned. ! Involuntary—a permanent separation initiated by the employer due to: !Lack of work !Inability to perform satisfactorily the duties of the position !Reorganization and/or relocation !Unprofessional conduct !Practice being sold and employment terminated ! The above items are not intended to show all the possibilities that might result in involuntary release from employment (refer to Employee Relations section of manual). ! Exit Interview—employees will be asked to complete an exit interview questionnaire at the time of their departure (see Exit Interview Form #104, page 74). This questionnaire gives you a chance to communicate your views on your work, pay, benefits, management, and communication within the practice. If this form is not filled out in person, a certified letter will be sent to the address on file at the time of separation. ! ! REQUEST FOR VERIFICATION OF EMPLOYMENT Whenever an authorized company or individual requests employment-related information about a present or former employee, an authorization form must be signed by the employee or prior employee before any such information will be released (see Authorization to Give References Form #105, page 75). A copy of this form can be obtained by request. ! ! ! 60 !132 SERVICE LETTER ! In responding to other employers' requests for employment information about a former employee, the practice provides the individual's start and end date of employment and title of position(s) held. Additional employment information is provided only if the individual authorizes the release of such information by completing the Authorization To Give References Form (see Form #105). ! ! RETURN OF PROPERTY If you quit or are terminated, any property belonging to the practice must be returned at the time the last paycheck is provided. Items may include uniforms, keys, manuals, equipment, etc. Your cooperation is appreciated. Your final paycheck may be withheld until all property is returned to GCDE. ! CONSOLIDATED OMNIBUS BUDGET RECONCILIATION ACT OF 1985 (COBRA) (Applies to employers with 2010 or more employees) ! Employers who are covered under COBRA or corresponding state provisions, must permit eligible employees to continue medical insurance upon termination of employment, under an employer's group health plan. Essentially, the act requires that employees and their family members be allowed to purchase health care coverage at the employer's group rates for specified periods of time when an employee experiences a “qualifying event” that results in the loss of employer-provided coverage. The insurance premium is to be paid by the employee. If an employee is off on a FMLA leave, COBRA starts at the end of the leave. ! Qualifying events are any change in a worker's employment status, including voluntary or involuntary termination, retirement, or a reduction in hours, that would make the employee ineligible for group health insurance; an employee dying, divorcing, legally separating, or gaining entitlement to Medicare; or a dependent child's loss of coverage due to age. COBRA coverage is not required if an employee's loss of health coverage is due to a discharge for gross misconduct. ! Employees must notify the employer of qualifying events such as a divorce or legal separation or a child attaining the plan's maximum age for coverage. The employer will notify the plan administrator of qualifying events such as an employee's termination, reduction of work hours, death, or eligibility for Medicare. ! When they are notified of a qualifying event, the plan administrator will notify qualified beneficiaries of their right to elect COBRA continuation coverage. However, those family members who were not covered under the employer's regular group health plan prior to the qualifying event are not qualified beneficiaries and cannot elect continuation coverage. ! 10 While federal COBRA regulations apply to employers with 20 or more employees, thirty-eight states are currently known to have “COBRA expansion programs” which may extend coverage to employees for employers with less than 20 employees. Check with your local State COBRA requirements or call our office. ! 61 !133 ! PROPOSING NEW POLICIES & CHANGING POLICIES To ensure that our office runs smoothly, efficiently and that we all work as a team, no one is to change a policy or change the way something is done without written approval by Dr. Alexandrunas. ! If you have a great idea on how to do something better, more efficiently, etc., write it up on a Memo Form and put it in Dr. Alexandrunas’ slot in his mailbox or send it to Dr. Alexandrunas at [email protected]. Dr. Alexandrunas will read your proposed policy and if approved it will be written up in policy format and distributed to all staff and discussed at the next staff meeting. ! We definitely appreciate your ideas, enthusiasm and input, so feel free to suggest anything you think would help. ! When a policy is changed without everyone’s knowledge, things become confused and unorganized. Please follow the above procedure and refer other staff to it as needed. ! GENERAL POLICY MANUAL CONCLUSION The policies contained in this manual have been created for all employees and associates whether temporary or full time. The purpose is to give you a clear understanding of what is expected from you as well as our viewpoint of what the ideal practice should be. ! Without policy we have “gray areas”. One can get caught in a real mess when one doesn’t know what’s needed and wanted. ! Everyone forgets with time. In order to avoid any misunderstandings, it is recommended that all employees review this policy manual periodically. As with any policy, “I forgot” is not an acceptable excuse. Employees are required to review this manually annually and sign Form #102. ! These policies will remain in effect from this point forward unless Dr. Alexandrunas decides to amend or cancel any of them. You will be notified in writing if this occurs. Staff is always welcome to propose policy for their areas where it is found to be lacking. Just ensure you attach a request form to the proposed policy and route it through the office manager to the owner. ! ! ! ! ! ! ! ! ! ! 62 ! ! FOR REPORTING HARASSMENT: ! DESIGNATED NAME(S) Name: Company: Title: Address: Email: Phone Number: Michael Casey Grove City Dental Expressions PR Director 3111 Columbus St. Suite A Grove City, OH 43123 [email protected] 614-725-6879 Name: Company: Title: Address: Email: Phone Number: Karl Alexandrunas Grove City Dental Expressions Office Manager 3111 Columbus St Suite A Grove City, OH 43123 [email protected] 614-935-7677 ! FOR REPORTING INABILITY TO REPORT TO WORK: ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! 63 FORM #101 EMPLOYEE ACKNOWLEDGEMENT FORM ! Complete information below and give to each employee to read and sign. !! Employee’s Name: _______________________________ !Please read, sign and return this form by (date) !The policies described in this manual will be effective (date) . If you have any questions, please let me know immediately. ! Employer’s Signature: _______________________________ ! HR Director’s Signature: _______________________________ ! Please read the following and place your signature below. !! I understand that the policies and procedures described in the Personnel Policy Manual are not an expressed or implied contract of employment between the employer and me and should not be viewed as the basis of any contractual obligations of the employer. ! I further understand that I am free to terminate my employment with the practice at any time, with or without cause, and the employer has the right to terminate my employment at any time, with or without cause. Therefore, employment with the practice is not for a specified term and can be terminated at-will by either party. The “at-will” policy constitutes an integrated agreement with respect to the nature of the employment relationship that is final and fully binding; there are no other oral or collateral agreements regarding this issue. This employment policy includes all employees including those presently employed by the practice from this day forward. ! I have read, understand and agree to adhere to the policies in this manual and by continuing my employment, I confirm acceptance of these policies. ! ! Employee's Signature ______________________________ Date ________________ ! !! cc: Employee Employee’s Personnel File ! ! ! ! 64 ! FORM #102 EMPLOYEE ACKNOWLEDGEMENT FORM HR MANUAL YEARLY REVIEW Date__________________ Please read the following and place your signature below. ! ! ! Employee’s Name_______________________________________________________ ! ! I have read, understand and agree to adhere to the policies in this manual and by continuing my employment, I confirm acceptance of these policies. ! ! ! Employee's Signature ______________________________ Date ________________ ! ! HR Director’s Signature: _______________________________ ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! FORM #103 ! EMPLOYEE ACKNOWLEDGEMENT FORM FOR BALANCE ON LEDGER Please read the following and place your signature below. ! I hereby acknowledge if there is a balance over 30 days on my or my families account ledger for dental work, products or other services rendered by M. Alexandrunas, DMD-Grove City Dental Expressions, Inc. all or part of the monies owed will be deducted from my paycheck until the balance is paid in full. ! If bonus is not received, 25% of the balance will be deducted from my paycheck until the balance is paid in full. If bonus is allotted for that month, the entire sum of the monies owed will be taken from the bonus until my balance is paid in full (whether met that month or consecutive months). ! I also acknowledge that the final balance will be deducted from my final paycheck if I have not paid in full at the time of separation of employment. ! I have read, understand and agree to adhere to this policy. ! ! Employee's Signature ______________________________ Date ________________ ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! FORM #104 EXIT INTERVIEW FORM ! Employee Name______________________ Termination Date ______________________ Eligible for Rehire [ ] Yes [ ] No Job Title ______________________ Reason for Termination Voluntary Involuntary [ ] Another Position [ ] Attendance [ ] Personal Reasons [ ] Violation of Company Policy [ ] Relocation [ ] Lay Off [ ] Retirement [ ] Reorganization [ ] Return to School [ ] Position Eliminated [ ] Other_____________ [ ] Other_______________ 1. What are your primary reasons for leaving? ! 2. What did you find most satisfying about your job? ! ! 3. What did you find most frustrating about your job? ! ! 4. Were there any company policies or procedures that made your work more difficult? ! 5. Would you consider returning to this company in the future? ! 6. Would you recommend this company to a friend as a good place to work? ! ! 7. Is there anything the company could have done to prevent you from leaving? ! Employee Comments: Interviewer Comments: Employee's Signature ____________________ Date: ! HR Director’s Signature: _______________________________ ! ____________________ FORM #105 ! AUTHORIZATION TO GIVE REFERENCES I hereby give M. Alexandrunas, DMD-Grove City Dental Expressions, Inc.! authorization to furnish information TO: ____________________________________! ! ! ! ! ! ! ! ! (NAME, ADDRESS, CONTACT #)! about my employment record, including dates of employment, job title, a statement of the reason for the termination of my employment, work performance, abilities, and other qualities pertinent to my qualifications for employment, hereby releasing them from any and all liability for damages arising from furnishing the requested information. ! ! SIGNATURE OF EMPLOYEE:__________________________________________! ! Name: ________________________________________ Date: _________________! ! HR Director’s Signature: _______________________________ ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! FORM #106 ON DUTY MEAL PERIOD ! On-Duty Meal Period Agreement ! I, _________________________________ , understand and agree that the nature of my work as ! a ___________________________________________ prevents me from being relieved of all ! duties and requires me to remain on-duty during meal periods. I voluntarily agree to work an on- ! duty meal period. I understand that any on-duty meal period is to be recorded on my time ! records as time worked, and that I will be paid for such time. I further understand that I will be ! given the opportunity to eat a meal while on duty. ! I understand that I may revoke this agreement at any time by providing written notice in ! advance to my supervisor. As an option, I further understand that I may revoke this agreement ! by signing the revocation section below and returning this Agreement to my supervisor. I also ! understand that I may work on-duty meal periods after revoking this agreement by signing a new ! on-duty meal period agreement. ! ! ! ! Employee signature _________________________ Date_____________________________ ! ! ! Print employee’s name _________________________________________________________ ! ! SUPERVISOR’S SIGNATURE___________________________________________________! ! ! ! On-Duty Meal Period Agreement Revocation ! I revoke my On-Duty Meal Period Agreement. I acknowledge that this revocation is not ! complete until I sign below and return this form to my supervisor. I also further understand that ! this revocation only applies to meal periods to which I otherwise would be entitled after I submit ! this signed revocation to my supervisor. ! ! ! Employee signature ___________________________________________Date_____________ ! ! ! Print employee’s name __________________________________________________________! ! ! FORM #108 HEPATITIS B INFORMATION AND CONSENT !! Employee (please print) _______________________________________ Date ____________ !About Hepatitis B !The disease - Hepatitis b is an infection cause by a virus - HBV. The virus may survive for as long as a week on hand pieces, equipment, charts, or uniforms. Consequently, employees and their families risk exposure. !Most people afflicted with HBV recover completely. However, although you may recover, there is a 5-10% chance you will become a chronic carrier of the virus. You may not exhibit symptoms but will continue to carry the disease. You may develop chronic active hepatitis or cirrhosis. HBV has been know to aid in the development of liver cancer. HBV caused death in ½% of those afflicted. !The vaccine - immunization can prevent acute hepatitis. IT may reduce sickness and death from chronic active hepatitis, cirrhosis and liver cancer. There are two vaccines available. Heptavx produced from the plasma of chronic carriers, and Recombavax, a newer synthetic vaccine. Both are effective and sage. IF you agree, you will receive two doses and a booster over time. Full immunization usually occurs after the third dose. Some people may not develop immunity even after vaccination. !We have no evidence showing the vaccine has ever caused Hepatitis B. However, people who have been infected with HBV prior to vaccination may develop clinical Hepatitis in spite of immunization. The duration of immunity is not know at this time. !The side effects - these are rare. You may feel tenderness and redness at the site of injection; you may develop a low-grade fever. Rash, nausea, joint pain, and mild fatigue have also been know to occur. The vaccine should not be taken if you are pregnant. !Statement of consent - I have read the above statement about Hepatitis B disease and vaccine. I understand the benefits and possible risk involved. However, there is no guarantee that I will become immune or that I will not experience an adverse side effect from the vaccine. !I refuse to take the vaccine (Employee must sign “Hepatitis B Vaccine Declination” Form 109). _______________________________ I agree to take the vaccine._______________________ I have already received partial immunization on (date) ______________________________________ I have already received total immunization on (date) ________________________________________ To my knowledge, I am not pregnant. !! Employee’s signature ________________________________________ Date _____________ HR Director’s Signature: _______________________________ ! FORM #109 B VACCINATION DECLINATION FORM !I understand that, dueHEPATITIS to my occupational exposure to blood or other potentially infectious materials (OPIM), I may be at risk of acquiring hepatitis B virus (HBV) infection. I have been given the opportunity to be vaccinated with hepatitis B vaccine, at no charge to myself. However, I decline the hepatitis B vaccine at this time. I understand that by declining this vaccine, I continue to be at risk of acquiring hepatitis B, a serious disease. If, in the future, I continue to have occupational exposure to blood or other potentially infectious materials (OPIM), and I want to be vaccinated with hepatitis B vaccine, I can receive the vaccination series at no charge to me. !! 1. I have been advised that, in the course of my employment as a with M. Alexandrunas, DMDGrove City Dental Expressions, Inc., I may be exposed or have the potential for exposure to hepatitis B Virus (HBV). !2. The risks associated with receiving or not receiving the vaccination have been explained to me. !Employee's Last Name: _________________________________ Employee's First Name:_________________________________ !Position Title:____________________________ !! Employee Signature: __________________________________ !! HR Director’s Signature: _______________________________ !! !! !! !! !! !! !! !! ! Date:____________ ! FORM #110 ! DIFFERENT CAPACITY WORK RATE The hourly rate of pay will equal or exceed the minimum wage requirements. This new rate then becomes the special hourly rate of pay for this period. The hourly rate is 75% of the individuals regular hourly rate. This rate should not exceed $15/hour. The rate of pay will be decided upon prior to the date of the course, in writing. ! I, __________________________________(print name), will be attending the following course ! _____________________________________________________________________________ ! on_____________(date). ! The rate of pay for my incurred hours will be _____________________. ! Employee Signature: __________________________________ Date:____________ !! Supervisors Signature: _________________________________ Date: ____________ ! ! ! ! ! ! ! ! ! ! ! FORM #111 ! PROBLEMS / CONCERNS REPORT FORM ! Employee Date Position ! Directed to (check one): Manager/Administrator Employer ! The following is a statement of my problem / concern. I request that it be reviewed in accordance with the Problems Resolution Procedure in the Staff Policy Manual. ! The reason for my concern is: ! Witness/es who can confirm my statements: ! I believe the appropriate solution to my concern is: ! Employee’s signature_________________________________________ Date__________________ HR Director’s Signature: _______________________________ ! cc: Employee’s Personnel File Employee FORM #112 MEDICAL RELEASE TO WORK ! ! Employer’s Name M. Alexandrunas, DMD-Grove City Dental Expressions, Inc. ! Date____________ ! Employee Name____________________________________ Position________________________ ! The above named employee wishes to return to work after a period of medical leave of absence. Our concern is for the health and well being of all of our staff members. Please complete the following: ! Diagnosis ! Is employee ready to return to work and perform normal work duties? NOTE: Job Description attached. (Check one) Regular work duties with no restrictions Light duty with restrictions listed below No duty ! Please indicate any work restrictions ! Doctor’s signature__________________________________________ Date___________________ ! Doctor’s name (please print) ________________________________ Phone ! Reviewed and accepted by (signature of patient)__________________________________________ ! PLEASE RETURN THIS FORM TO EMPLOYER ! HR Director’s Signature: _______________________________ ! ! ! ! _____________________ cc: Employee’s Personnel File FORM #113 ACCIDENT REPORT FORM ! Employee___________________________________________ ! ! Position_______________________ Date and Time of Accident________________________ Location of Accident: Name of Witness______________________ ! Description of Accident (How accident occurred): Cause of Accident/Injury: Type of Illness/Injury: ! Medical treatment received: If yes, by whom? Doctor’s name/address/telephone: No Yes Employer-authorized treatment: No Yes No Yes ! Sick Leave/Unpaid Leave used? : ! First day of leave: Days sick leave used: Days unpaid leave used: Date returned to work: ! Preventive measures taken to prevent recurrence? Does an unsafe condition still exist? ! No Yes Employer’s signature________________________________________________ Date_____________________ HR Director’s Signature: _______________________________________ Date____________________ ! ! FORM #114 EMPLOYEE COUNSELING MEMO FORM ! Employee___________________________________________ Date Hired_______________________ ! Position___________________ Date(s) of previous documentation on file:_________________________ ! Today’s Date: ! Reason For Counseling (what happened? - be specific. Include, date, time): If more space is needed, attach separate documentation. Have both parties date and sign attached page(s). ! 2. Nature Of Disciplinary Action (if suspension, state if paid/unpaid, include beginning date and return date): 3. Corrective action expected of employee (Be specific, state date action must have been accomplished): Potential Consequences: Employee has been warned that failure to take appropriate corrective action or any future infraction will result in disciplinary action, which may include discharge. ! Employer initial here that employee has been warned of possible discharge: ! Employee's Comments: Employer/Manager’s Comments: Employer/Manager’s Signature Date My signature indicates that the above items have been presented and discussed with me and does not necessarily indicate that I agree with the reason(s) for the counseling. I recognize that I have five (5) days in which to submit any written comments I may have. My comments will then be attached to this form and placed in my Personnel File. Employee’s Signature Date HR Director’s Signature Date cc: Employee’s Personnel File Employee ! FORM #115 Commitment to Work Form ! Employee________________________________________Position_____________________________ ! Name of Course attending and dates______________________________________________________ ! Cost of course: Tuition_____________________Travel______________________ Accomodations_________________________ Total:__________________________ ! *Note: As per the HR Manual in regards to Gratuity: Grove City Dental Expressions will cover up to 15% of the gratuity related to meals or cabfare during travel or other times Grove City Dental Expressions covers the cost of an item. Anything over 15% will be the responsibility of the purchaser. ! All receipts submitted to Accounts Payable to cover Parking, Mileage, etc must be itemized. Please request an itemized receipt. You may not be reimbursed for the particular expense if this receipt is not included. I understand by agreeing to attend this seminar, at cost to my employer M. Alexandrunas, DMDGrove City Dental Expressions, Inc. I will work at least 6 months from the last date of the class or else have to pay back GCDE for tuiton fees, travel and accomodations on a prorated schedule. ! Signature of Employee_____________________ ! Signature of Employer_____________________ ! ! ! ! ! ! ! ! ! ! ! ! ! ! cc: Employee’s Personnel File, Employee Date:_______________________ Date:_______________________ FORM #116 PAYROLL ACKNOWLEDGEMENT FORM ! ! By signing this letter, and as a condition of further employment, I agree to bring questions or errors regarding timesheet errors, corrections or any other concerns regarding payment of wages or reimbursement of expenses to the Office Manager to provide an opportunity for Grove City Dental Expressions to address any errors. ! _________________________________________________________________________ Signature ! Date FORM #117 TIME CORRECTION WORKSHEET ! Employee Name__________________________________ Pay Period Start__________________________________ Pay Period End__________________________________ Date Time Recorded in Dentrix Actual Time to be Recorded Reason for Correction I have submitted the about time correction sheet and have noted the times and dates that need correction. The time corrections are correct and true to my knowledge. Employee Signature________________________________________ Date__________________________ Your Signature___________________________ To be signed by employee and manager after times have been corrected. I affirm that the above requested changes have been made and my time sheet for the above mentioned pay period has been corrected. ! ! Manager Signature________________________________________ Employee Signature________________________________________ ! Date__________________________ Date__________________________ ! ! ! FORM #118 Completed Staff Work (CSW) ! To: _____________________________ Date: _______________________ From: __________________________ Situation: _____________________________________________________________________________________ ____________________________________________________________________________________ Data: _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ Solution: _____________________________________________________________________________________ _____________________________________________________________________________________ ! ! ! ! ! ! ! ! ! ! ! FORM # 119 ! ! Granville Dental/Grove City Dental Expression Sexual Harassment Training ! I acknowledge that I have attended the Sexual Harassment Training course that has been provided by my employer Granville Dental/Grove City Dental Expressions. Additionally, I also understand the company policies surrounding sexual harassment and have knowledge of appropriate behavior in the workplace. It has also been explained to me how to submit a concern to my employer if any harassing situation arises and what information is needed to investigate the matter appropriately. Employee Signature____________________________________________________ ! Date___________________________________ Human Resource Director_______________________________________________ ! Date___________________________________ ! ! ! ! ! ! ! ! ! ! ! ! ! FORM #201 NEW EMPLOYEE CHECKLIST ! ! Employee Name: ______________________________________________________ _____ Welcome Letter !_____ Face Sheet !_____ At-Will Agreement !_____ Exhibit A: Job Description !_____ Exhibit B: Time Sheet Example !_____ Exhibit C: Pay Schedule !_____ HIPPA: Acknowledgement of Privacy Practices !_____ Hepatitis B Vaccine Acceptance and Declination Form (if applicable) !_____ W4 !_____ Ohio Exemption Form !_____ I-9 !_____ Copy of Driver’s License !_____ Copy of Social Security Card !_____ Direct Deposit Form !_____ Radiation Certification (if applicable) !_____ Hygiene License or other State Board License in good standings(if applicable) !_____ Payroll Acknowledgement Form !_____ HR Manual Acknowledgement Form !_____ Key Agreement Form ! Employees Signature __________________________________Date____________ ! HR Signature _________________________________Date_____________ ! ! ! FORM #2O2 NEW EMPLOYEE PROGRESS REPORT FORM ! Employee Date hired ! Current salary $ Date of last review ! Attendance Record: # of days absent since hired ! Has employee received any disciplinary warnings? Yes ! If yes, list date(s) of warnings ! Today’s date Next review # of days late since hired Needs Improvement No Satisfactory Job Knowledge (How well does employee demonstrate competence?) Quality of Work (What is employee’s quality of work?) Quantity of Work (Does quantity of work meet your standards?) Safety (Does employee work safely and follow safety rules?) Initiative (Is employee a "self starter"?) Dependability (Does employee follow instructions and do what is expected?) Conduct (Does employee follow policy and conduct him/herself professionally?) Attitude (Is employee’s behavior toward job and others acceptable?) Cooperation (Does employee work effectively as a team member?) Absence/Punctuality (Review attendance record above) Training (Has employee been fully trained?) ! ! ! ! ! ! ! ! ! ! Action plan for improvement (List what, how, and by when): Employer’s signature___________________________________ Employee’s signature__________________________________ HR Director’s Signature__________________________________________ Date ________________________ Date ________________________ Date______________________________ cc: Employee, Employee’s Personnel File FORM #2O3 EMPLOYEE PERFORMANCE APPRAISAL FORM ! Employee Date hired ! Current salary $ Date of last review ! Attendance Record: # of days absent since hired ! Has employee received any disciplinary warnings? Yes ! If yes, list date(s) of warnings ! Today’s date Next review # of days late since hired Needs Improvement No Satisfactory Job Knowledge (How well does employee demonstrate competence?) Quality of Work (What is employee’s quality of work?) Quantity of Work (Does quantity of work meet your standards?) Safety (Does employee work safely and follow safety rules?) Initiative (Is employee a "self starter"?) Dependability (Does employee follow instructions and do what is expected?) Conduct (Does employee follow policy and conduct him/herself professionally?) Attitude (Is employee’s behavior toward job and others acceptable?) Cooperation (Does employee work effectively as a team member?) Absence/Punctuality (Review attendance record above) Training (Has employee been fully trained?) ! ! ! ! ! ! ! ! ! ! Action plan for improvement (List what, how, and by when): Employer’s signature___________________________________ Date ________________________ Employee’s signature__________________________________ Date ________________________ HR Director’s Signature_______________________________ Date ________________________ cc: Employee Employee’s Personnel File FORM #300 ! ! VOLUNTARY RESIGNATION BY EMPLOYEE FORM ! Date: Employee: Social Security No.: Title: Date of Hire: Supervisor's Name: ! I, the undersigned, am voluntarily resigning from my position as (Title)_________________ with M.ALEXANDRUNAS, DMD-GROVE CITY DENTAL EXPRESSIONS, INC. ! My last day of employment with M.ALEXANDRUNAS, DMD-GROVE CITY DENTAL EXPRESSIONS, INC. will be (Specify Date)____________. I am resigning my position because: ! ! ! You may contact me at the following telephone number and address: ! ! After (Specify Date)____________ you can reach me at: Thank you for your attention in this matter. ! Employee Signature__________________________________ Date ____________ ! Received by: ________________________________________________________ (Name/Title) Date ! HR Director’s Signature: __________________________________________________________________________ ! Date ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! JOB DESCRIPTIONS Exhibit A! ! ! ! Position Title: Registered Dental Assistant (RDA) Employee Status: Non Exempt Reports To: Dr. Mark Alexandrunas Job Summary: To assist in the performance of quality, caring clinical dentistry; to become adept at assigned clinical procedures; to aid the doctor smoothly and unobtrusively. Perform clinical and technical procedures under the supervision of a licensed dentist. The RDA gets the patient ready, prepares the operatory and equipment and assist the doctor during examinations and treatment. Maintain awareness of comfort and safety needs of patients. Maintain equipment and inventory. Adhere to all required OSHA and health regulations. Coordinate, integrate and represent all facets of patient services. Meet and greet patients and make them feel welcomed and relaxed. Answer the telephone, schedule appointments, communicate with patients regarding financial and scheduling options, maintain patient records and coordinate patient flow. Manage and control the daily, weekly, and monthly schedule in order to meet the practice production and collection goals. Compile data and operate office equipment to maintain business records and reports. Qualifications: To perform this job successfully, the individual must be able to perform each essential duty satisfactorily. The requirements listed below are representative of the knowledge, skill, and/or ability required. Education and Experience: High school diploma or equivalent. This position requires ________ years of experience in the dental office. Knows how to administer CPR and first aid. Certificates, Licenses and Registrations: RDA license, X-ray license, CPR certificate (name any other licenses required). Knowledge: Can competently perform the clinical and technical dental procedures required of a Registered Dental Assistant. Can take quality x-rays, including FMX, Pano and anterior PA’s. Knows how to administer CPR and first aid. Knows how to take blood pressure, attach EKG leads to patients and understand readings of monitors. Thorough understanding of cross contamination and how to prevent it. Keeps informed and updated on OSHA regulations (OSHA officer). Must know and keep updated on federal and state labor law regulations (federal and state labor law officer). Oral surgery practice: Knows CDC guidelines. ! ! ! Skills: Knows how to work with: Autoclave, model trimmer, X-ray machine - Pano, Panoramic X-ray, X-ray processor, X-ray duplicator, ultrasonic, O2 and N2O, laser, Intra Oral camera, Laser, Vacupress, Paché gun, KCP 2000, Whip-Mix and hand pieces. Physical Requirements: The physical demands described here are representative of those that must be met by an employee to successfully perform the essential functions of this job. While performing the duties of this job, the employee is required to do detailed work, using arms, hands, and fingers to handle and feel object worked with. The employee intermittently is required to either sit, stand, walk, stoop, bend or reach throughout the day. Good eye-hand coordination and manual dexterity is needed. Specific vision abilities include close vision, color vision, peripheral vision, depth perception, and ability to adjust focus. Must be physically able to administer CPR. The employee may have to physically assist drowsy patients after anesthesia. May have to lift up to 25 pounds, roll a 90-pound anesthesia machine and a full 35-gallon drum of expended chemicals on wheels from one area to another. (When required by the Americans with Disabilities Act, reasonable accommodations may be made to enable individuals with disabilities to perform the essential functions.) Work Environment: The work environment characteristics described here are representative of those an employee encounters while performing the essential functions of this job. While performing the duties of this job, the employee is occasionally exposed to toxic or caustic chemicals and risk of radiation. The noise level is usually moderate. Since everyone within the practice works on a time schedule governed by patient’s appointments, the work and general environment can become somewhat hectic at times. Therefore, it is essential that the employee is able to, both physically and emotionally, effectively handle the normal anxieties associated with the job. Competencies: § Is able to “get along” well with fellow employees. Treats all with respect and courtesy § Can work well in teams of co-workers § Can accept constructive criticism § Has a desire and ability to work well with the public § Is organized, motivated, committed and self-directed § Has a positive attitude about the practice, the services provided and the products old. § Ability to communicate - expresses thoughts and ideas competently § Increases knowledge and skills through self-study and by attending courses and seminars. § Able to understand relevant concepts regarding duties and responsibilities § Has dependable job attendance and can be relied on to follow through with assigned task Authority: Record treatment information in the patient's chart. Enter type of treatment planned for next appointment and the amount of chair time, doctor time and assistant time needed. Dismiss patients. Please refer to Essential Essential Duties and Responsibilities section. Then make a mark or highlight each of the duties that you consider essential (most important). Essential Duties and Responsibilities: Direct Supervision Duties (doctor present): § Apply nonaerosol and noncaustic topical agents § Take impressions for diagnostic and opposing models § Remove postextraction and periodontal dressings § Place and remove elastic orthodontic separators § Assist in the administration of nitrous oxide § Hold anterior matrices § Remove sutures, arch wires, ligature ties § Take intraoral measurements for orthodontic procedures § Seat adjusted retainers or headgears. Check for loose orthodontic bands § Apply topical fluoride § Place and remove rubber dams § Perform mouthmirror inspection of the oral cavity, including charting of lesions, existing restorations and missing teeth § Place, wedge, and remove matrices § Obtain endodontic cultures § Dry canals with absorbent points § Test pulp vitality § Place bases and liners on dentin § Remove cement excess from supragingival surfaces of teeth § Size stainless steel crowns, temporary crowns, and bands § Temporary cementation and removal of temporary crowns and orthodontic bands § Place postextraction and periodontal dressings § Placement and ligation of arch wires. placement and removal of temporary sedative dressings § Perform coronal polishing Other Duties: § Seat patients in designated treatment rooms in a timely fashion § Take, process and mount xrays § Pour and trim study models § Review medical history, progress from the previous visit, if applicable, and the scheduled treatment plan with each patient § Inform the doctor when the patient is ready § Assist the doctor by passing instruments, aspirating intraoral fluids, mixing materials and medicaments § Record treatment rendered in the patient's chart and charge out all procedures § Escort patients to the business area for financial followup and rescheduling § Monitor incoming and outgoing lab cases § Take, develop, and mount full mouth xrays § Assures compliance with OSHA and health regulations § Check that lab cases have been received the day before treatment Daily Maintenance: § Turn on all lights, units, nitrous equipment and automatic processors each morning § Prepare all treatment rooms in advance for each patient § Decontaminate all treatment rooms and sterilize all instruments after each patient appointment § Change all chemical solutions, i.e., disinfectant soaks and sprays, sterilents, ultrasonic, presoak and xray processing § Maintain cleanliness of treatment rooms, dark room, lab and sterilizing area § Clean and flush vacuum traps § Clean and lubricate handpieces § Restock all treatment rooms and other clinical support areas § Clean sharp instruments and handles hazardous chemicals in a safe manner. § Decontaminate all treatment rooms and sterilize all instruments after each patient appointment § Change all chemical solutions, i.e., disinfectant soaks and sprays, sterilents, ultrasonic, presoak and xray processing § Maintain cleanliness of treatment rooms, dark room, lab and sterilizing area § Clean and flush vacuum traps § Clean and lubricate handpieces § Restock all treatment rooms and other clinical support areas Routine Maintenance: § General house cleaning (drawers, cabinets, carpet) § Clean x-ray-processing rollers § Order supplies § Maintain plaster trap and lab counter areas § All office personnel are required to assist with the general cleaning of the office, hallways and bathroom to keep a clean and orderly appearance Additional or different duties may be assigned from time to time. ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! Position Title: Dental Assistant ! Employee Status: Non-Exempt ! Reports To: (name of Manager/Supervisor) Dr. Mark Alexandrunas ! Job Summary: To assist in the performance of quality, caring clinical dentistry; to become adept at assigned clinical procedures; to aid the doctor smoothly and unobtrusively. Perform clinical and technical procedures under the supervision of a licensed dentist. The RDA gets the patient ready, prepares the operatory and equipment and assist the doctor during examinations and treatment. Maintain awareness of comfort and safety needs of patients. Maintain equipment and inventory. Adhere to all required OSHA and health regulations. ! Qualifications: To perform this job successfully, the individual must be able to perform each essential duty satisfactorily. The requirements listed below are representative of the knowledge, skill, and/or ability required. ! Education and Experience: High school diploma or equivalent. This position requires ________ years of experience in the dental office. Knows how to administer CPR and first aid. ! Certificates, Licenses and Registrations: X-ray license, CPR certificate. ! Knowledge: Can competently perform the clinical and technical dental procedures required of a Registered Dental Assistant. Can take quality x-rays, including FMX, Pano and anterior PA’s. Knows how to administer CPR and first aid. Knows how to take blood pressure, attach EKG leads to patients and understand readings of monitors. Thorough understanding of cross contamination and how to prevent it. Keeps informed and updated on OSHA regulations. ! Oral surgery practice: Knows CDC guidelines. ! Skills: Knows how to work with: Autoclave, model trimmer, X-ray machine - Pano, Panoramic X-ray, X-ray processor, X-ray duplicator, ultrasonic, O2 and N2O, laser, Intra Oral camera, Laser, Vacu-press, Paché gun, KCP 2000, Whip-Mix and hand pieces. ! Physical Requirements: The physical demands described here are representative of those that must be met by an employee to successfully perform the essential functions of this job. ! While performing the duties of this job, the employee is required to do detailed work, using arms, hands, and fingers to handle and feel object worked with. The employee intermittently is required to sit, stand, walk, stoop, bend or reach throughout the day. Good eye-hand coordination and manual dexterity is needed. Specific vision abilities include close vision, color vision, peripheral vision, depth perception, and ability to adjust focus. Must be physically able to administer CPR. ! The employee may have to physically assist drowsy patients after anesthesia. May have to lift up to 25 pounds, roll a 90-pound anesthesia machine and a full 35-gallon drum of expended chemicals on wheels from one area to another. (When required by the Americans with Disabilities Act, reasonable accommodations may be made to enable individuals with disabilities to perform the essential functions.) ! Work Environment: The work environment characteristics described here are representative of those an employee encounters while performing the essential functions of this job. ! While performing the duties of this job, the employee is occasionally exposed to toxic or caustic chemicals and risk of radiation. The noise level is usually moderate. Since everyone within the practice works on a time schedule governed by patient’s appointments, the work and general environment can become somewhat hectic at times. Therefore, it is essential that the employee is able to, both physically and emotionally, effectively handle the normal anxieties associated with the job. ! Competencies: Is able to “get along” well with fellow employees. Treats all with respect and courtesy Can work well in teams of co-workers Can accept constructive criticism Has a desire and ability to work well with the public Is organized, motivated, committed and self-directed Has a positive attitude about the practice, the services provided and the products sold. Ability to communicate - expresses thoughts and ideas competently Increases knowledge and skills through self-study and by attending courses and seminars. Able to quickly grasp relevant concepts regarding duties and responsibilities Has dependable attendance and can be relied on to follow through with assigned tasks ! Authority: Record treatment information in the patient's chart. Enter type of treatment planned for next appointment and the amount of chair time, doctor time and assistant time needed. Dismiss patients after treatment. ! An unlicensed dental auxiliary may not perform any of the following functions, unless authorized by a specific statute or regulation: Diagnosis for treatment planning Surgical or cutting procedures on hard or soft tissue Fitting and adjusting of correctional and Prosthodontics appliances Prescription of medicines Condensation, carving, or removal of permanent restorations, including final cementation procedures. Irrigation and medication of canals, tryin cones, reaming, filing, or filling of root canals. Oral prophylaxis procedures Taking impressions for Prosthodontics appliances, bridges, or any other structures, which may be worn in the mouth Administration of injectable and/or general anesthesia and acupuncture ! Please refer to Essential Duties and Responsibilities section. Then make a mark or highlight each of the duties that you consider essential (most important). ! Essential Duties and Responsibilities: ! Direct Supervision Duties (doctor present): Apply nonaerosol and noncaustic topical agents Take impressions for diagnostic and opposing models Remove postextraction and periodontal dressings Place and remove elastic orthodontic separators Assist in the administration of nitrous oxide Hold anterior matrices Remove sutures, arch wires, ligature ties Take intraoral measurements for orthodontic procedures Seat adjusted retainers or headgears Check for loose orthodontic bands Apply topical fluoride Place and remove rubber dams ! ! Other Duties: Seat patients in designated treatment rooms in a timely fashion Take, process and mount x-rays Pour and trim study models Review medical history, progress from the previous visit, if applicable, and the scheduled treatment plan with each patient Inform the doctor when the patient is ready Assist the doctor by passing instruments, aspirating intraoral fluids, mixing materials and medicaments Record treatment rendered in the patient's chart and charge out all procedures Escort patients to the business area for financial followup and rescheduling Monitor all incoming and outgoing lab cases Take, develop, and mount full mouth xrays Daily Maintenance: Turn on all lights, units, nitrous equipment and automatic processors each morning Prepare all treatment rooms in advance for each patient Decontaminate all treatment rooms and sterilize all instruments after each patient appointment Change all chemical solutions, i.e., disinfectant soaks and sprays, sterilents, ultrasonic, presoak and xray processing ! Maintain cleanliness of treatment rooms, dark room, lab and sterilizing area Clean and flush vacuum traps Clean and lubricate handpieces Restock all treatment rooms and other clinical support areas Clean sharp instruments and handles hazardous chemicals in a safe manner Routine Maintenance: General house cleaning (drawers, cabinets, carpet) Clean x-ray-processing rollers Order supplies Maintain plaster trap and lab counter areas ! Additional or different duties may be assigned from time to time. !! !! !! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! Position Title: Registered Dental Hygienist Employee Status: Non-Exempt Reports To: (name of Manager/Supervisor) Dr. Mark Alexandrunas and Karl Alexandrunas Job Summary: With gum disease rampant, the RDH is in a special position to provide our patients the most important health service possible. The hygienist assists the dentist in providing oral health to patients by cleaning, scaling and polishing teeth. Takes and processes X-rays. Records evaluation of mouth conditions and extent of prophylaxis on dental chart to provide dentist with information for more complete diagnoses and subsequent treatment if needed. Provides the patient with ongoing preventive oral care through patient education, treatment and reinforcement of the doctor's treatment plan. Adheres to all required OSHA and health regulations. Qualifications: To perform this job successfully, the RDH must be able to perform each essential duty satisfactorily. Keeps informed and updated on OSHA regulations. The requirements listed below are representative of the knowledge, skill, and/or ability required. (If additional qualifications are needed, enter it here on a copy of this job description). Education and Experience: High school diploma or equivalent. This position requires years of experience as hygienist. Knows how to administer CPR and first aid. Certificates, Licenses and Registrations: Valid X-ray certificate, current RDH license, to include expanded functions, CPR certificate. Skills: Scaling and root planing, appropriate use of Cavitron, Radiographic skills, administration of local anesthetic and Nitrous Oxide. If additional skills are needed, enter it here on a copy of this job description. Physical Requirements: The physical demands described here are representative of those that must be met by an employee to successfully perform the essential functions of this job. Reasonable accommodations may be made to enable individuals with disabilities to perform the essential functions. While performing the duties of this job, the employee is required to do detailed work, using arms, hands, and fingers to handle and feel object worked with. The employee intermittently is required to sit, stand, walk, stoop, bend or reach throughout the day. Good eye-hand coordination and manual dexterity is needed. Specific vision abilities include close vision, color vision, peripheral vision, depth perception, and ability to adjust focus. Must be physically able to administer CPR. The employee may have to physically assist drowsy patients after anesthesia. May have to lift up to 25 pounds, roll a 90-pound anesthesia machine and a full 35-gallon drum of expended chemicals on wheels from one area to another. Work Environment: The work environment characteristics described here are representative of those an employee encounters while performing the essential functions of this job. While performing the duties of this job, the employee is occasionally exposed to toxic or caustic chemicals and risk of radiation. The noise level is usually moderate. Since everyone within the practice works on a time schedule governed by patient’s appointments, the work and general environment can become somewhat hectic at times. Therefore, it is essential that the employee is able to, both physically and emotionally, effectively handle the normal anxieties associated with the job. Competencies: § Is able to “get along” well with fellow employees. Treats all with respect and courtesy § Can work well in teams of co-workers § Can accept constructive criticism § Has a desire and ability to work well with the public § Is organized, motivated, committed and self-directed § Has a positive attitude about the practice, the services provided and the products sold § Ability to communicate - expresses thoughts and ideas competently § Speaks and writes grammatically correct English § Increases knowledge and skills through self-study and by attending courses and seminars § Able to understand relevant concepts regarding duties and responsibilities § Maintains a professional demeanor in stressful situations § Ability to complete tasks within a specific time frame § Considers patients comfort an important priority § Has dependable job attendance and can be relied on to follow through with assigned tasks Authority: Decide on treatment needed for the present appointment and record treatment information in the patient's chart. Enter type of treatment planned for next appointment and the amount of chair time, doctor time and assistant time needed. Dismiss patients. Please refer to Essential Essential Duties and Responsibilities section. Then make a mark or highlight each of the duties that you consider essential (most important). Essential Duties and Responsibilities: Patient Treatment: § Greet and seat patients. Take xrays, develop, and mount, if necessary. § Evaluate gingival health and health of all oral tissue. § Perform oral cancer exam. Take blood pressure. § Administer nitrous oxide and oxygen. Classify patient's periodontal condition. § Scale, polish, and apply fluoride. § Periodontal soft tissue curettage. § Do root planing. § Do Perio probe and chart. § Recommend perio consultation; refer out to specialists. § Application of pit and fissure sealants. § Polish and contour restorations. § Polish appliances (partials, dentures, etc.). § Oral exfoliative cytology. § Take impressions for diagnostic and opposing models. § Application of nonaerosol and noncaustic topical agents. § Removal of postextraction and periodontal dressings. § Removal of sutures and ligature ties. § Take intraoral measurements for orthodontic procedures. § Check for loose bands. § Place elastic separators. § Test pulp. § Remove cement excess from subgingival surfaces of tooth. § Size stainless steel crowns, temporary crowns, and bands. § Temporary cementation and removal of temporary crowns and orthodontic bands. § Placement of postextraction and periodontal dressings. § Myofunctional evaluation. Patient Education: § Explain disease process and the role of bacteria in caries and periodontal health § Provide appropriate educational literature § Provide instruction on home care § Recommend intraoral aids § Evaluate hygiene booklets for patient distribution § Explain prevention to patients and parents of small children § Reflect and reinforce the doctor's philosophy Recording Patient Information: § Update medical history and screen for potential problems every six months, or after a threeyear absence. § Periodontal charting. § Chart lesions, existing restorations, and missing teeth. § Classify periodontal conditions and occlusal relations. § Charge out completed treatment. § Put recall stickers on the chart § Counsel patients for case acceptance. § Inform doctor of any special problems with oral hygiene. § Assist doctor during clinical exam and record findings and recommendations. § Record treatment rendered on patient's chart and initial. § Communicate to the front office: length of time needed for patient's next appointment or recall; when to schedule; what will be done (record on chart and code). General Duties: § Turn on equipment in the morning and off at night. § Set up treatment rooms for each patient. § Seat and dismiss hygiene patients. § Manage supplies, instruments, and the state of treatment rooms. § Disinfect patient chair, cuspidor, and counter tops. § Maintain the cleanliness of hygiene room and the functions of the equipment. § Clean, sterilize, and set up instruments. § Sharpen instruments. § Restock hygiene room. § Clean and lubricate handpieces. § File charts and offer assistance to the front office. § Implement and monitor recall system. § Call patients who are overdue for recall. § Help clinical assistant if needed. § Assist and support the doctor in clinical treatment of patients. § Call patient if late for appointment. § Help fill schedule. § All office personnel are required to assist with the general cleaning of the office, hallways and bathroom to keep a clean and orderly appearance Additional or different duties may be assigned from time to time ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! Position Title: Office Coordinator Employee Status: Exempt Reports To: The Office Coordinator works under the employer's direct supervision and is to report on progress, act as liaison with staff, and counsel with the employer on problem situations before taking action in other than routine matters. Dr. Mark Alexandrunas and Karl Alexandrunas Job Summary: The Office Coordinator, more than any individual, works closely with the doctor and staff to assure that all the business aspects of the practice are functioning in an orderly and proficient manner. The administrator communicates the practice philosophy through systems, problem solving and communication. This individual strives to bring out the best in the entire staff, for the benefit of our patients. As the doctor's righthand person, you make known the doctor's philosophy to dentistry in everything you do from scheduling systems, financial arrangements, and staff concerns. You are, essentially, accountable for everything, so your role is complex. You are the main conduit of information between doctor and staff. A large part of the practice's success will hinge on your efforts, and reflect on you. Coordinate, integrate and represent all facets of patient services. Meet and greet patients and make them feel welcomed and relaxed. Answer the telephone, schedule appointments, communicate with patients regarding financial and scheduling options, maintain patient records and coordinate patient flow. Manage and control the daily, weekly, and monthly schedule in order to meet the practice production and collection goals. Compile data and operate office equipment to maintain business records and reports. Helps make quality dentistry financially available to patients. Communicates with patients regarding their treatment plan, helps find the best way to finance the recommended treatment and makes appropriate financial arrangements with patients. Works with patients to resolve account problems. Assists patients in determining insurance eligibility and counsels patients regarding insurance. Communicates with insurance companies regarding claims. Qualifications: To perform this job successfully, the individual must be able to perform each essential duty satisfactorily. The requirements listed below are representative of the knowledge, skill, and/or ability required. Education / Experience: Two-year college or technical school; or six months to one year related experience and/or training; or equivalent combination of education and experience. This position requires years of experience in the dental profession or handling insurance benefits. Skills: Is proficient in working with the office equipment and computer software used by the practice. Knowledge: Can competently perform the job responsibilities required by this position. Knows how to administer CPR and first aid. Competencies: § Is emotionally and mentally mature, able to engender trust, and always ready to listen § Is able to “get along” with fellow staff members. Treats all with respect and courtesy § Can work well in teams of co-workers § Can accept constructive criticism § Is skilled in using computer software § Is proficient in using conflict resolution and problem-solving techniques in managing interpersonal conflict, patient complaints, and other discord § Has a desire and ability to work well with the public § Is organized, motivated, committed and self-directed § Has a positive attitude about the practice, the services and the products sold § Ability to communicate effectively - expresses thoughts and ideas competently § Has outstanding verbal skills that reflects well on the practice § Increases knowledge and skills through self-study and by attending courses and seminars § Able to understand concepts regarding duties and responsibilities § Has dependable job attendance and can be relied on to follow through with assigned tasks § Is discrete in handling confidential management and employer-employee relation’s matters Physical Requirements: If employee is required to “fill-in” for any of the clinical positions from time-to-time, the general physical requirements of those positions will apply. Requirements such as: doing detailed work, using arms, hands, and fingers to handle and feel object worked with. The employee intermittently is required to sit, stand, walk, stoop, bend or reach throughout the day. Good eyehand coordination and manual dexterity is needed. Specific vision abilities include close vision, color vision, peripheral vision, depth perception, and ability to adjust focus. While performing the duties of this job, the employee may be regularly required to sit for long periods. The employee must occasionally lift and/or move up to 10 pounds. Must be physically able to administer CPR. In a small practice with only a few staff members, the employee may occasionally have to physically assist drowsy patients after anesthesia and move light equipment up to 25 pounds. (When required by the Americans with Disabilities Act, reasonable accommodations may be made to enable individuals with disabilities to perform the essential functions). Work Environment: The work environment characteristics described here are representative of those the employee may encounter while performing the essential functions of the job. The employee is occasionally exposed to toxic or caustic chemicals and risk of radiation. The noise level is usually moderate. Since everyone within the practice works on a time schedule governed by patient’s appointments, the work and general environment can become somewhat hectic at times. Therefore, it is essential that the employee is able to, both physically and emotionally, effectively handle the anxieties associated with the job. Authority: The Manager/Administrator carries out supervisory responsibilities in accordance with the established policies and applicable laws. Responsibilities include interviewing, hiring, and training employees; planning, assigning, and directing work; staff performance evaluations; assigning work schedules; rewarding and disciplining employees; addressing complaints and resolving problems. Must have the employer’s permission before any employee is terminated. Essential Duties and Responsibilities: § Keep the doctor and the hygienist productively busy throughout the day § Pull and file patient records for each day’s schedule § Schedule all appointments and detail procedure and time needed § Stabilize production by booking by the ideal day concept § Maximize time efficiency in scheduling by utilizing procedure codes for doctor time, assistant time, anesthesia, etc. § Check that lab cases have been received the day before treatment § Greet patients by name and update addresses, telephone numbers and insurance information as appropriate § Alert appropriate staff of patient arrivals § Monitor the schedule throughout the day to insure that all runs smoothly § Adjust the schedule as necessary § Make sure that there are open times in the day to provide flexibility or time for emergencies § Reschedule the late patient and any no-shows that occur during the day § Check accounts balances of patients coming in and prepares to discuss any monies due § Adhere to all safety and health regulations § At the morning huddle, cover: a. Production results from yesterday; what went wrong, what went right b. Evaluate yesterday’s patient flow c. Status of Rocks for the next 5 days d. Status of today’s production goals e. Identify open time in schedule § Organize the next day’s charts; include a copy of the schedule and place in designated spot for the clinical staff to review § Determine the status of the next continuing care visit for each hygiene patient seen during the day to insure no one is missed § Keep staff and doctor informed of next available opening; time allotted for emergency patients, possible noshows § Call any patient that is 5 minutes late to determine their status and inform the clinical staff § Register new patients and provide necessary forms (welcome letter, patient information, and office policy) § Keep patients informed of expected waiting time if the doctor is behind schedule Areas of Responsibility: A. Staff Management: Consistently and fairly administers all personnel policies as outlined in the Staff Policy Manual and the Doctor’s Personnel Administration Manual. Insures proper staffing and the consistently competent job performance of each staff member. Establishes and maintains personnel files. Other areas of responsibility include: § Assisting with hiring § Assisting with training § Assisting employer with carrying out policies § Assist with Staff meetings B. Patient Management: Insure that patients are appropriately seen and treated in a professional, timely, and competent manner. Areas of responsibility include: § Patient Contact § Appointments § Patient Finances: Prepare a financial action plan by reviewing the patents for the next day and determining their financial needs and status; Research insurance benefits and prepare estimates on treatment diagnosed prior to discussing financial arrangements; If the patient is returning for a consultation, provide this information to the doctor two days in advance of the appointment; Determine patient’s insurance carrier and patient’s share of cost; Make financial arrangements on all patients according to our financial policy; Document the payment option selected by the patient; Financial arrangements must be made after the exam and consultation and prior to treatment; Obtain a signed financial agreement if you decide to offer financing to the patient; Specify number of payments and due dates. Monitor payments; Record (in red) all financial verbal discussions with patient in the chart and enter this information in the computer; Prepare and deliver a daily financial statement to the employer; Present the treatment plan, using models, diagrams and provide related literature; Prepare a treatment-planning schedule, book the first appointment and arrange for subsequent hygiene appointments; Be prepared to quantify referral sources, dollars diagnosed; dollars accepted; percent accepted; dollars completed; percentage completed; actual production compared to monthly goals § Recall Patients: Check chart for any incomplete treatment two days prior to recall; Verify chart has complete insurance information; Go over treatment to date with the patient and assess attitude toward any incomplete treatment. Update health history; Estimate costs of today's treatment; Make yourself available to recalculate financial arrangements as needed; Contact patients when preauthorization is received and proceed with scheduling § Records § Billing § Insurance: Gather information concerning the insurance plans that you deal with on an ongoing basis; Insurance booklet provided by the patient; Payment information obtained on the EOB’s; Document basic insurance information on the patient’s chart for quick reference; Determine insurance eligibility, limitations and payment estimate necessary to facilitate financial arrangements; Educate the patient to their responsibility regarding insurance, the true meaning of UCR and a basic understanding of insurance terminology; Process claims daily and mail or submit electronically within 24 hours; Research eligibility on all new patients prior to their appointment; Monitor turn around time on all claims for payment and predetermination. Follow up if the claim is outstanding at the end of the 4th week. Call or utilize the tracking form; Determine the need and send x-rays, charting, narratives and documentation with the claim when applicable; Process and mail predetermination. Contact the patient to make financial arrangements and schedule treatment; Call or correspond with insurance companies to resolve delays in payment, requests for additional information or to discuss treatment that has been denied coverage; Handle all inquiries concerning insurance on a daily basis § Payment Arrangements § Delinquent Accounts § Collections: Identify patients in the daily schedule who are a financial concern and set time to conference with them; Evaluate each situation to determine if this discussion should take place prior to or at the time of the appointment; Record (in red) all financial verbal discussions with patient in the chart and enter this information in the computer; Control and/or reduce the accounts receivable by setting up a daily monitoring system in the tickler file; Call patients who have not kept their agreement within a 5-day grace period; Prepare and send statements monthly on a regular billing cycle; Follow up missed payments with tickler system; Keep employer apprised of problems; Mail patients' statements on regular billing cycle; Make collection calls; Get firm commitment, amount to pay, and date to pay from patient; Handle all correspondence regarding collections; Send accounts to collection when necessary; Represent employer in Small Claims Court; Note payment problems on patient chart; Follow through with correspondence regarding collection when unable to contact patient on the telephone; Prepare and send uncollected accounts to collections or small claims court and follow through as needed (get employers approval); Monitor patients turned over to collection agency C. Office Procedures: § Determine insurance eligibility, limitations and payment estimate necessary to facilitate financial arrangements § Educate the patient to their responsibility regarding insurance, the true meaning of UCR and a basic understanding of insurance terminology § Process claims daily and mail or submit electronically within 24 hours § Research eligibility on all new patients prior to their appointment § Monitor turn around time on all claims for payment and predetermination. Follow up if the claim is outstanding at the end of the 4th week. Call or utilize the tracking form § Determine the need and send x-rays, charting, narratives and documentation with the claim when applicable § Process and mail predetermination. Contact the patient to make financial arrangements and schedule treatment § Call or correspond with insurance companies to resolve delays in payment, requests for additional information or to discuss treatment that has been denied coverage § Handle all inquiries concerning insurance on a daily basis § Modifying and updating systems and procedures to insure optimum service to patients, the practice and employees § Computes, types, and mails monthly statements to patients § Completes records to or through trial balance § Organize patient refund checks payment with bookeeper § Prepare ledger cards on route slips for the day's posting § Input daily production and collection figures on computer § Post and balance charges and payments daily § Keep daily record of production and collections § Close out day; begin next day's sheet § Match bank deposit slip to daily income § Write deposit slip and deposit receipts daily § Is discrete in handling confidential management and employer-employee relation’s matters § Communicate with Julie Alexandrunas via [email protected] re: ordering office supplies D. Production/Promotion: Meet with the employer to discuss, evaluate and plan for the financial welfare of the practice. Stay attuned and updated so that the practice goals can be successfully accomplished. Areas of responsibility include: § Marketing § Internal § External E. Property / Facility Maintenance: Assure that the practice property is looking clean, professional and well kept, from general maintenance to the sterilization of instruments. Make sure that all clinical and office equipment is kept in proper working order. Oversee condition of real property and arrange for landscaping/ gardening or other services as required. Additional or different duties may be assigned from time to time. § Follow up missed payments with tickler system § Keep employer apprised of problems § Mail patients' statements on regular billing cycle § Make collection calls § Get firm commitment, amount to pay, and date to pay from patient § Handle all correspondence regarding collections § Send accounts to collection when necessary § Represent employer in Small Claims Court § Note payment problems on patient chart § Follow through with correspondence regarding collection when unable to contact patient on the telephone § Prepare and send uncollected accounts to collections or small claims court and follow through as needed (get employers approval) § Monitor patients turned over to collection agency Paperwork/Recording: § Place all non-scheduled, diagnosed treatments in the tickler file for timely follow up § Mail the welcome package to all new patients entering the practice and requesting an examination § Organize and maintain all file systems § Keep the New Patient Flow Sheet current § Record broken appointments and last minute cancellations in patient chart § Keep all former patients' records up to date § Place the doctor's call list (names, home phones, and treatment for day's patients) on the doctor's desk before leaving § Prepare welcome letters, thank you letters and other correspondence for doctor's signature § Maintain Stats and Quotas as directed by the Office Manager ! Appearance Of The Work Area: § The reception area lends a strong first impression. Keep it looking comfortable, neat and cheerful § All office personnel are required to assist with the general cleaning of the office, hallways and bathroom to keep a clean and orderly appearance ! Additional or different duties may be assigned from time to time ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! Position Title: Appointment Coordinator ! Employee Status: Non-Exempt ! Reports To: (name of Manager/Supervisor) Karl Alexandrunas ! Job Summary: Coordinate, integrate and represent all facets of patient services. Meet and greet patients and make them feel welcomed and relaxed. Answer the telephone, schedule appointments, communicate with patients regarding financial and scheduling options, maintain patient records and coordinate patient flow. Manage and control the daily, weekly, and monthly schedule in order to meet the practice production and collection goals. Compile data and operate office equipment to maintain business records and reports. ! Qualifications: To perform this job successfully, an individual must be able to perform each essential duty satisfactorily. The requirements listed below are representative of the knowledge, skill, and/or ability required. ! Education and Experience: High school diploma or equivalent. This position requires profession. years of experience in the dental ! Skills: Is proficient in working with the office equipment and computer software used by the practice. ! Knowledge: Can competently perform the job responsibilities required by this position. Knows how to administer CPR and first aid. Keeps informed and updated on OSHA regulations. ! Oral surgery practice: Knows CDC guidelines. ! Physical Requirements: The physical demands described here are representative of those that must be met by an employee to successfully perform the essential functions of this job. ! While performing the duties of this job, the employee is required to do detailed work, using arms, hands, and fingers to manipulate the required office equipment. The employee intermittently is required to sit, stand, walk, stoop, bend and reach throughout the day. Good eye-hand coordination and manual dexterity is needed. Specific vision abilities include close vision, color vision, peripheral vision, depth perception, and ability to adjust focus. Must be physically able to administer CPR. ! In a small practice with only a few staff members, the employee may occasionally have to physically assist drowsy patients after anesthesia and move light equipment up to 25 pounds. (When required by the Americans with Disabilities Act, reasonable accommodations may be made to enable individuals with disabilities to perform the essential functions). ! Work Environment: The work environment characteristics described here are representative of those an employee encounters while performing the essential functions of this job. ! While performing the duties of this job, the employee is occasionally exposed to toxic or caustic chemicals and risk of radiation. The noise level is usually moderate. Since everyone within the practice works on a time schedule governed by patient’s appointments, the work and general environment can become somewhat hectic at times. Therefore, it is essential that the employee is able to, both physically and emotionally, effectively handle the normal anxieties associated with the job. ! Competencies: Is able to “get along” well with fellow employees. Can work well in teams of co-workers. Can accept constructive criticism. Has a desire and ability to work well with the public. Is organized, motivated, committed and self-directed. Has a positive attitude about the practice, the services provided and the products sold. Ability to communicate - expresses thoughts and ideas competently. Increases knowledge and skills through self-study and by attending courses and seminars. Able to quickly grasp relevant concepts regarding duties and responsibilities. Has dependable job attendance and can be relied on to follow through with assigned tasks. ! Authority: Record treatment information in the patient's chart. Enter type of treatment planned for next appointment and the amount of chair time, doctor time and assistant time needed. Dismiss patients. ! Essential Duties And Responsibilities: Keep the doctor and the hygienist productively busy throughout the day Pull and file patient records for each day’s schedule Schedule all appointments and detail procedure and time needed Stabilize production by booking by the ideal day concept Maximize time efficiency in scheduling by utilizing procedure codes for doctor time, assistant time, anesthesia, etc. Check that lab cases have been received the day before treatment Greet patients by name and update addresses, telephone numbers and insurance information as appropriate Alert appropriate staff of patient arrivals Monitor the schedule throughout the day to insure that all runs smoothly Adjust the schedule as necessary Make sure that there are open times in the day to provide flexibility or time for emergencies Reschedule the late patient and any no-shows that occur during the day Check accounts balances of patients coming in and prepares to discuss any monies due Adhere to all safety and health regulations At the morning huddle, cover: Production results from yesterday; what went wrong, what went right Evaluate yesterday’s patient flow Status of Rocks for the next 5 days Status of today’s production goals Identify open time in schedule Organize the next day’s charts; include a copy of the schedule and place in designated spot for the clinical staff to review Determine the status of the next continuing care visit for each hygiene patient seen during the day to insure no one is missed Keep staff and doctor informed of next available opening; time allotted for emergency patients, possible noshows Call any patient that is 5 minutes late to determine their status and inform the clinical staff Register new patients and provide necessary forms (welcome letter, patient information, and office policy) Keep patients informed of expected waiting time if the doctor is behind schedule ! Paperwork/Recording: Place all non-scheduled, diagnosed treatments in the tickler file for timely follow up Mail the welcome package to all new patients entering the practice and requesting an examination Organize and maintain all file systems Keep the New Patient Flow Sheet current Record broken appointments and lastminute cancellations in patient chart Keep all former patients' records up to date Place the doctor's call list (names, home phones, and treatment for day's patients) on the doctor's desk before leaving Prepare welcome letters, thank you letters and other correspondence for doctor's signature Maintain Stats and Quotas as directed ! Appearance Of The Work Area: The reception area lends a strong first impression. Keep it looking comfortable, neat and cheerful ! Additional or different duties may be assigned from time to time !! ! ! ! ! ! ! ! POSITION TITLE: Director of Public Relations ! EMPLOYEE STATUS: Exempt ! Reports To: Karl Alexandrunas, Office Manager and Julie Alexandrunas, Marketing Director ! JOB SUMMARY: Peform and direct Public Relations events in the community. ! QUALIFICATION REQUIREMENTS: Degree in Public Relations from an accredited university and experience. Ability to self-start and motivate, keep logs of budget, expenses. Make contacts, cold call, ability to work with little supervision, ability to accept constructive criticism and to work well in teams of co-workers. Know how to use a computer, basic digital camera and other types of office equipment. ! PERFORMANCE STANDARDS: Describe the physical demands, the type and amount of work to be performed. For example, typing at least 4 hours a day; requires frequent lifting of 60 lb. or more; must see an average of 8 patients a day. List any unusual demands. ! ! JOB FUNCTIONS AND DUTIES: Essesntial Duties: Attending all meetings with the BIA, Chamber of Commerce Acting as a liason with the Chamber of commerce and other groups in the community and GCDE Attending the Farmer’s Markets during the applicable months fore advertising or interviewing applicant for that position? ! Non-Essential: He or she will be required to follow any other instructions and to perform any other duties that may be requested from time-to-time. ! AUTHORITY: Can spend up to $250/month for promotion and events without prior approval. All expenses must have a receipt for tax purposes. ! Paperwork/Recording: Keep budget and expense reports with applicable receipts up to date. Turn in report monthly. Must request approval if over $250 budget by filling out a PO request form. Every Tuesday submit a report to Marketing Director and CC O/M on events over the weekend, including promotional ‘blubs’ about the event, who was there and the feedback received from contacts made during the event. Include pictures in this email. Also include events upcoming for the next few weeks, plan for the next week and any new or changes to the upcoming events schedule. ! Maintain Quotas: Example: Maintain agreed upon work hours. Contact O/M immediately for any changes to said hours. ! Appearance Of The Work Area: Keep it looking comfortable, neat and cheerful and organized. ! ADDITIONAL INFORMATION: Required to work within the community and provide own transportation to events during and after work hours. !

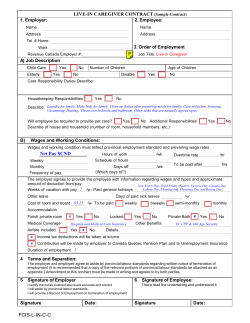




© Copyright 2026