
Rearrangement of the MLL gene confers a poor prognosis in
From www.bloodjournal.org by guest on October 15, 2014. For personal use only.
1996 87: 2870-2877
Rearrangement of the MLL gene confers a poor prognosis in
childhood acute lymphoblastic leukemia, regardless of presenting
age
FG Behm, SC Raimondi, JL Frestedt, Q Liu, WM Crist, JR Downing, GK Rivera, JH Kersey and
CH Pui
Updated information and services can be found at:
http://www.bloodjournal.org/content/87/7/2870.full.html
Articles on similar topics can be found in the following Blood collections
Information about reproducing this article in parts or in its entirety may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests
Information about ordering reprints may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#reprints
Information about subscriptions and ASH membership may be found online at:
http://www.bloodjournal.org/site/subscriptions/index.xhtml
Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American
Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036.
Copyright 2011 by The American Society of Hematology; all rights reserved.
From www.bloodjournal.org by guest on October 15, 2014. For personal use only.
Rearrangement of the MLL Gene Confers a Poor Prognosis in Childhood
Acute Lymphoblastic Leukemia, Regardless of Presenting Age
By F.G. Behm, S.C.Raimondi, J.L. Frestedt, Q. Liu, W.M. Crist, JR. Downing, G.K. Rivera, J.H. Kersey, and C.-H. Pui
MLL gene rearrangements are associated with an extremely
poor prognosis in infants with acute lymphoblastic leukemia
(ALL), but little is knownabout their clinical significance in
older children. Therefore, we studied 45 cases of childhood
ALL with abnormalities of chromosome 11q23 for rearrangement of the MLL gene t o determine if this feature confers a
uniformly poor prognosis. MLL gene rearrangements were
detected in all 18 cases with the commont(4; 11). t(9;ll) or
t(11;19) translocations, whereas only 5 of 12 patients with
either unbalanced or uncommon balanced translocations
demonstrated a rearrangement. Abnormalities of the MLL
gene were notdetected in any of the 15 caseswith a deletion
or inversion of thechromosome l l q 2 3 region. The presence
of an MLL rearrangement was significantly associated with
age less than 1 year (P< .001), leukocyte count >50 x lo9/
A
BNORMALITIES OF chromosome 1 1, band q23, are
relatively frequent in childhood acute lymphoblastic
leukemia (ALL). In an earlier study of 368 childrenwith
newly diagnosed ALL, alterations of this chromosome region, including balanced and unbalanced translocations, deletions, andduplications,werefound
in lymphoblasts of
5.7% of patients.' Although generally characterized
by hyperleukocytosis, a very young age, lack of CD10 expression,
and a poor clinical outcome, these cases appeared to constitute a heterogeneous group of B- and T-lineage leukemias
1l),
bearinga
variety of translocations,includingt(4;
t( 1 I ; 19), and others.
Of the several genes that are affected by structural abnormalities ofthe 1 lq23 region,"(' MLL (alsotermed H R X ,
ALLI, HTRX1) is the most c o m ~ n o n . The
~ ~ ~MLL
'
gene is
uniformly rearranged in cases with the t(4; 1 l)(q21;q23),'"'
but the frequency of its involvement in other translocations
affecting the 1 lq23 regions is uncertain. By contrast, most
cases of ALL with deletions or inversions of 1 lq23 do not
involve MLL." We and others haveshown a high frequency
From the Departments of Pathology and Laboratory Medicine,
Biostatistics, Tumor Cell Biology and Hematology/Oncolog.~,St
Jude Children's Reseurch Hospitai; the Departments of Patholop
and Pediutrics, Universir?,of Tennessee College of Medicine. Memphis, TN; and the Departments of Laboratory Medicine and Pathology and Pediatric Hematology/Oncology, University of Minnesota,
Minneapolis.
Submitted July 13, 1995; accepted November 7, 1995.
Supported in part by Grants No. CA 20180, CA 21765, and an
Outstanding Investigator Grant award CA 49721 (J.H.K.)from the
National Cancer Institute; Children's Cancer ResearchFund Grant
(J.L.F. und J.H.K.); and by the American Lebanese Syrian Associuted Charities (ALSAC).
Address reprint reque.st.r to F.G. Behm, MD, Department of Pathology andLaboru601yMedicine, St Jude Children's Research Hospital. 332 N Lauderdale, Memphis, TN 38105.
The publication C O S ~ S($this urticle were defrayedin part by puge
charge puyment. This article must therefore be hereby marked
"advertisement" in accordance with 18 U.S.C. section 1734 solely to
indicate this fact.
0 1996 by The American Sociel): of Hematology.
0006-4971/96/8707-0037$3.00/0
2870
L (P= .003),and theabsence of leukemic cell CD10 expression ( P < .001). In a stratified statistical analysis adjusted
for age and treatment protocol, MLL gene rearrangement
was correlated with an inferior treatment outcome ( P =
.028). The 4-year event-free survival estimate(?SE)was 10%
k 6.5% for cases with a rearranged MLL gene and 64% C
19.2% for other cases. When infants were excluded from the
analysis, MLL rearrangement was still significantly associated with a poor outcome (P= .02), and remained so with
the exclusion of t(4;llJ-positivecases (P=.05). Thus,regardless of presenting age, MLL gene rearrangement identifies
a high-risk subgroup of patients who are not likely to be
cured with conventional treatment.
0 1996 by The American Society of Hematology.
of MLL rearrangements in ALL of infants (70% to 80%) that
may account for the dismalprognosis in this subgroup.".","
More recently, we attributed the relatively favorable prognosis of ALL with deletions or inversions of the 1 lq23 region
to thelack of MLL rearrangement." Whether rearrangements
of the MLL gene has prognostic importance in children over
1 year of age or in those with
1 lq23 translocations other
than the t(4; 1 1 ) is unknown. Therefore, we studied a large
cohort of childhood ALL patients with various 1 lq23 abnormalities to address these issues.
MATERIALS AND METHODS
Putients. From September 1984 to September 1994,715 consecutive children with newly diagnosed ALL were admitted to St Jude
Children's Research Hospital and enrolled
in one ofthree successive
XI-XIII,'h.'7 at St
clinicaltrials,designatedTotalTherapystudies
Jude Children's Research Hospital. Although testing different therapeutic strategies, these protocols uniformly relied on a similar multidrug induction regimen and intensification therapy. The diagnosis
of ALL was based on morphologic criteriaof the French-AmericanBritish (FAB) Cooperative Group," and confirmed by immunologic
testing. Leukemic cells were successfully karyotyped in 669 cases,
S3 (8%) of which had abnormalities of chromosome 1 lq23. Banked
cryopreserved leukemic cellsor banked DNA was available for analysis of MLL gene rearrangements in 45 of these S3 cases. Studies
of the MLL gene of 12 cases (patients 8, 19-21, 24, 28, 30, 33, 37,
and 41-43, Table I ) have been reported previously.'3 Informed conor their guardians, and the investisent was obtained from all patients
gations were approved by the institution's Clinical Trials
Review
Committee.
Cytogeneticevaluation.
Bonemarrowsampleswere
prepared
by a direct method," with or without short-term (24-hour) culture.
A modifiedtrypsin-Wrighttechnique
was used forchromosome
banding.Chromosomeabnormalitiesweredescribedaccording
to
conventions of the International Systemfor Human Cytogenetic Nomenclature (ISCN-91)."'
Immunophenotyping studies. Surfaceantigensweredetected on
leukemic cells by standard indirect immunofluorescence assayswith
monoclonalantibodies to lymphoid-andmyeloid-associatedantigens. Blast cells were also tested for surface (slg) and cytoplasmic
(clg) immunoglobulin as previously described." Depending on reactivity patterns, cells were classified as T (CD7' plus CD2', CD3 '
or CDS'), B (slg'), pre-B (clg'). transitional pre-B (clgp'. algp'.
.
Blood, Vol 87, No 7 (April 1 ), 1996: pp 2870-2877
From www.bloodjournal.org by guest on October 15, 2014. For personal use only.
ALLPROGNOSIS IN
WITH REARRANGEMENT OF MLL
287 1
4
0
11
5
38
17
H
IF
H
R
PB
EPB
EPB
EPB
EPB
EPB
44.4
17.7
106
23.6
R
G
G
R
EPB
T
EPB
EPB
6
8
35
11
CNS
H
H
H
0.5
78.2
R
EPB
60 +
12
13
0.6
0.6
106.4
6
R
PB
PB
19
3.3+
Death
R
14
15
16
17
18
19
0.6
0.8
0.9
1.1
1.7
2
67.7
250
8.7
21.8
164
71.4
R
PB
EPB
PB
PB
PB
EPB
8
13
11+
291
42
7+
H
H, CNS
20
21
22
23
24
25
2.3
3.2
3.3
4.3
4.7
4.9
3.8
24.9
1.8
10.3
6
22.9
G
G
G
G
G
EPB
EPB
NA
EPB
PB
EPB
90+
7+
41
76+
30+
13+
26
5.0
31.7
G
EPB
13+
27
6.1
15.1
G
EPB
38+
28
6.2
43.4
G
PB
30 +
29
6.6
8.7
G
PB
33+
30
6.8
1.2
G
EPB
9+
31
7.5
3.5
G
UD
43 +
32
33
9.7
9.2
R
34
9.6
1
2
3
4
5
6
0.1
0.2
0.2
0.3
0.3
0.4
7
8
9
10
0.4
0.5
0.5
0.5
11
110
440
330
438
1,136
81
R
R
R
R
R
R
R
R
R
G
R
H
H, CNS
H
H
A ML
G
EPB
EPB
25
10+
A ML
2.4
6.9
G
EPB
44
H, CNS
581
From www.bloodjournal.org by guest on October 15, 2014. For personal use only.
BEHM ET AL
2872
Table 1 (Cont'd).
Characteristics of Patients With ALL and Chromosome l l q 2 3 Abnormalities Ordered by Age
Remisslon
Duration
MLL
Patient
13.3
Age (yr)
WBC (x109/LI
35
36
10
10
1512
18.4
37
38
39
40
11.9
12.5
13.7
76.7
383
367
7.5
41
42
43
14
14.4
14.7
18.9
52
85.7
Karyotype
Status
46,XX,t(4; 1 l)(q21;q23)
R
46,X,-Y,t(2;12)(q23;p13),der(ll)t(3;11)
lpll;q23),+mar/
47.X.-Y,+X,der(l)t(l;?)(q32;?1,
t(2;12),der(ll)t(3;11),+mar
46,XY,del(ll)(q23)*
46,XY,t(4;1l)(q21;q23),i(71(q10)
G
CD10
CD15
(mol
lrnrnunotype
EPB
PB
35+
T
46,XY,t(ll;lS)(q23;p131*
46.XY.t(9;22)(q34;qll),de11111(q23)/
G
R
R
G
EPB
PB
EPB
18+
19+
4
54 +
47,XY,de1(11)(q23),+18*
46,XY,de111l)(q23)*
46,XX,del(ll)(q23)*
45,XX,inv(5)(p13q14),del~lO)(q22~,
G
G
G
EPB
20
EPB
T
Type of
Relapse
20+
H
CNS
27 i
0
IF
del~ll)(q22-23).dic(12;17)(pll;pll)*
44
45
15.5
16.6
573
6.2
47.XY,+X.t~4;11)(q21;q23)/46,idem,-X*
48,XY,de1(4)(q21q31),deI(S)(p13),
dic(9;13)(pl2;p121,t(11;19)(q23;p13)
x2,+19,+20,-22,+marl/
48,idem,-marl,+mar2*
R
R
TPB
T
13
1
H
AML
Boldface type indicates type of chromosome 11, band q23 abnormality.
Abbreviations: R, rearranged; G, gerrnline; ND, not done; UD. undetermined; PB, pre-B ALL; EPB, early pre-B ALL; T, TALL; TPB, transitional
pre-B ALL; H, hematologic; IF, induction failure; CNS, central nervous system; AML, relapse a s acute myeloidleukemia (lineage switch of
secondary AML).
*Previously reported karyotype.
s l g C , slgx-), or early pre-B (clg-, slg", HLA-DR', CD19',
CD10').2'
Southern blot analysis. Genomic DNA was extracted from leukemic blasts obtained from patients at diagnosis. Aliquots (5 to
I O pg) of high-molecular-weight DNA were digested with BamH1,
HindIII, and Sac I restriction endonucleases, separated by electrophoresis in 0.8% agarose gels, and blotted onto nylon membranes
using a standard Southern method. All blots were hybridized with a
"P-labeled probe, termed MLL (Oncor, Gaithersburg, MD), derived
from a 0.74-kb BumHI cDNA fragment of the MLL gene." The probe
detects the common breakpoints of MLL between exons 5 through
1 I with BamHI digests, and breaks centromeric to exon 5 and telomeric to exon 11 with Hind111 and Sac I digests (Fig I). Membranes containing BamHI and Hind111 restricted DNA of cases demonstrating germline MLL bands with the cDNA MLL probe were
stripped, and then sequentially examined with MLL genomic probes
98.40, 4.2E. and PS/4.'r.22.Z3
When used in parallel studies, these
four probes detect breaks between exons 2 and I8 with DNArestricted with BamHIor Hind111 (Fig I). The 4.2E probe required
300 pg/mL total human placental DNA (Sigma Chemical CO, St
Louis, MO) in the hybridization solution to block repetitive sequences. All blots included restricted DNA from a cervical carcinoma cell line that has two normal MLL genes. All blots also included DNA from the RS4; 11 cell line that contains one normal
MLL gene and one MLL gene split by the t(4; 11) translocation."
Hybridized membranes were exposed to Kodak XAR-5 film (Eastman Kodak, Rochester, NY) at -70°C for 5 to 7 days.
Statistical analysis. Because of the limited number of patient
samples, analyses were adjusted only for age and treatment that
largely corrects for other presenting risk features. Event-free survival
curves were constructed by the Kaplan-Meier method and were compared by the stratified log-rank test. Values ( P ) of .05 or less for
survival were considered significant. Differences in the distribution
of presenting features [age, sex, race, leukocyte count, central ner-
vous system leukemia, CDIO, CD15, DNA index, mediastinal mass,
and the t(4; 1 1 ) translocation] between cases with or without MLL
rearrangements were tested by the two-sided Fisher exact test. For
comparisons of presenting features, we adjusted the target significance value (.05) to compensate for the problem of multiple signiticance testing. This was done by dividing the target value of .05 by
the number of comparisons performed (n = 10 in these analyses),
so that a P value of at least ,005 was required to declare statistical
significance.
RESULTS
Of the 45 cases studied, 30 (67%)had an 1 lq23 translocation, 13 (29%) had a del(1 l)(q23), and 2 (4%) an
inv( 1 l)(pl3q23). The modal chromosome number was 46
in all but eight cases-4 with 47 chromosomes, 2 with 45,
and 1 eachwith 48 and 55 (Table 1). The distribution of
balanced translocations favored the t(4; I l)(q21 ;q23) and the
t(l l ; 19)(q23;p13) [including a t(2; 19; 1 l)(q33;p13:q23)
variant], each present in eight cases, followed by the
t(9; ll)(p21;q23) intwo additional cases. The remaining
five cases had other llq23 translocations, including a
t(4; 1 l)(q31;q23) in an infant with pre-B leukemia (Table
1, patient 12). In addition to a del(1 l)(q23) or der(l1)
t( I l;?)(q23;?), leukemic cells of patients 29, 3 I , and 40 also
contained a t(9;22)(q34;ql l), but these children surprisingly
remain free of disease at 33+, 43+ and 54+ months, respectively.
A rearranged MLL gene was demonstrated in 21 of the
45 cases using the cDNA probe and BarnHI digests. Two
additional cases (patients 2 and 3) were detected with HindIII
and Suc I digests. To exclude possible MLL breaks in the
From www.bloodjournal.org by guest on October 15, 2014. For personal use only.
PROGNOSIS IN ALLWITHREARRANGEMENT
15+ kb
4
2873
OF MLL
L
8.5W
B H
H HH
15+ W
L
r -
b
r -
E B E BH SE
E H HHE
EEHB
EH
B H BH H
I Dl II I I I ! I I
I I I II I I I I I I I
1
4
3
2
1314 15 16
7586
Tel
I
18
19
21 20
17
11
12
98.40
PSI4 4.2E
MLL
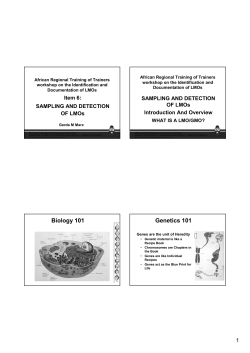
Fig 1. Schematic representationof MLL gene. Locations of exons 1through 21 are representedby black rectangles. BsmH1, Hindlll. EcoRI.
and Sac I restriction sites are denoted by B, H, E, and S,respectively. Regions of
MLL identified by 98.40, PSl4. and 4.2E probes are represented
by grey rectangles. Line enclosed by arrowheads shows portion of MLL detected by cDNA MLL probe. The 98.40 probe detects a 15+ kb
BamHl fragment (telomeric to exon 1through exon 5). The cDNA MLLand PSI4 probes recognize an
8.5 kb BamHl fragment (exons 5 through
11). The 4.2E probe recognizes 8.5 kb (exons 5 through 11) and 15+ kb (exons 11 through 18) BamHl fragments.
remaining 22 patients, membranes with their BurnHI and
Hind111 restricted DNA were stripped and reexamined with
probes 4.2E, 98.40, and PSl4. None of these studies uncovered additional cases with an MLL gene rearrangement.
The frequency of MLL rearrangement varied according to
the type of 1 Iq23 abnormality (Tables 1 and 2). Rearrangement of MLL was detected in 20 of 23 cases with a balanced
translocation, including all 18 cases with the common
t(4; I 1 ), t( 1 I ; 19) or t(9; 1 I), and 2 of 5 cases (patients 9, 12,
22,23, and 26) with other balanced 1 lq23 translocations. In
Table 2. Involvement of the M L L Gene in 45 Cases of Acute
Lymphoblastic Leukemia With Cytogenetic
Abnormalities of Chromosome llq23
Clinical Outcome
Cytogenetic Group
and MLL Status
t(4;11)(q21;q23)
MLL
3 rearranged
t(11;19)(q23;p13)'
MLL rearranged
t(9;11)(p21;q23)
MLL rearranged
t(ll;V)(q23;V)t
5 germline .
MLL
MLL rearranged 4
Deletion 1lq23
11 germline
MLL
inv(ll)(p13q23)
MLL germline 1
No. of
Patients
No. in
Remission
No. of
Relapses
addition, 3 of 7 cases with an unbalanced I lq23 translocation
involved the MLL gene (Fig 2). None of the 15 cases with
either del( I l)(q23) or inv( 1 I)(pl3q23) demonstrated an abnormal MLL gene.
The presence of an MLL rearrangement was significantly
associated with age less than 1 year ( P < .001), leukocyte
count >50 X IOy/L ( P = .003), and lack of CD10 expression
( P < .001) (Table 3). Cases with rearranged MLL also had
a higher frequency of initial CNS leukemia and CD15 expression than did other cases. When infant cases were excluded from the analysis, MLL rearrangements were correlated with lack of CD10 and aberrant CD15 expression ( P
= .005 and P = .001, respectively), and tended to have
higher leukocyte counts ( P = .03) (Table 4). With further
elimination of the t(4; 1 l)-positive cases from the group older
than I year, none of the presenting features were significantly
associated with MLL rearrangement.
The Kaplan-Meier estimate of event-free survival (+SE)
for all patients at 4 years of follow-up was 10% 5 6.5% for
patients with a rearranged MLL gene and 64% 19.2% for
those without this abnormality (Fig 3). The difference in
outcome was significant by the stratified log-rank test after
adjustment for age (< I v > 1 year) and treatment ( P = .028).
When the analysis was restricted to patients > I year of age,
MLL rearrangement still correlated with aninferior treatment
outcome ( P = .02, Fig 4). Even when only cases over 1 year
of age with no t(4; 1 1) were analyzed, MLL rearrangement
remained an adverse prognostic feature ( P = .05). Results
of this latter analysis are not likely to be confounded by
other presenting risk factors, because these factors did not
differ significantly between children greater than 1 year of
age with a rearranged MLL gene but no t(4; 1 1) and patients
greater than 1 year of age and normal MLL genes. Of the 7
patients with an 1 lq23 translocation that did not involve
MLL, only patients 9 and 34 had an adverse event; the other
+
5
8
8
2
6
2
0
2
7
5
1
13
2
2
1
Includes patient4 with a t(2;19;1l)(q33;p13;q23).
t Includes patient 12 with a t(4;11)(q31;q23) and 7 patients with
unbalanced translocations. The "V" in t(ll;V)(q23;V) indicates variable or unknown translocation partners.
From www.bloodjournal.org by guest on October 15, 2014. For personal use only.
2874
BEHM
N R S 3 4 2 9 2 5
AL
N RS23362612 7 17
6
v*.-
b . " " V . " ~
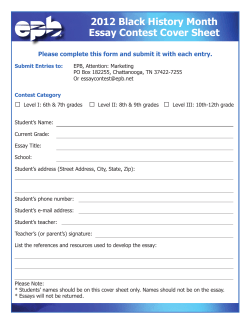
Fig 2. Southern blots of BamHI-digested DNA of leukemic marrow cells from patients with translocations of llq23. Lanes labeled " N
contain DNA from a cell linewith two normal MLL genes. Lanes labeled "RS" contain DNA from the RS4;ll cell line that contains
one normal
and one rearranged MLL gene. Other lanes are labeled with patient numbers thatcorrespond t o Table 1. Blots were hybridizedwith a cDNA
probe that recognizes sequences between exons 5 and l 1 of the MLL gene. Arrowheads identify the 8.5-kb band of germline MLL. Lanes
labeled "RS" show one germline band andt w o additional bands respresenting one normal MLL gene and one splithearranged MLL gene,
respectively. Cases 6, 12, 7, and 17 (lanes labeled accordingly) had der(ll)t(7;117)17;pl4
q23;7), t(4;11)(q3l;q231, t(9;ll)(p21;q23) and
t(ll;19)(q23;p13), respectively, and show a germline band and one or t w o additional rearranged bands. All other cases had translocationsof
1lq23 and show only germline
bands.
-
S patients (nos. 23, 25, 26, 29, and 36) remain in complete
remission for 13+ to 76+ months (median, 27+ months).
DISCUSSION
This study illustrates the heterogeneity of clinical and molecular findings among cases with structural abnormalities
involving band 23 of chromosome 1 I . MLL gene involve-
ment was found in all cases with the common t(4; 1 I ) ,
t( 1 1 ;19) or t(9; 1 l ) translocations; however, not all cases
with other 1 lq23 translocations involved this gene, especially patients over I year of age. Cases with deletions or
inversions of 1 lq23 also did not have MLL rearrangements.
It is unlikely thatrearrangements of MLL were missed in
this study, because the multiple probes used should have
detected allbreaks between exons 2 and 18. Indeed, the
reported breakpoints of MLL in acute leukemias have oc-
Table 3. Correlations of MLL Gene Rearrangements With
Presenting Features in 45 Childhood Acute Lymphoblastic
Leukemias With Abnormalities ofChromosome l l q 2 3
Table 4. Correlations of MLL Gene Rearrangements With
Presenting Features in 29 Children Over Age 1 With Acute
Lymphoblastic Leukemias With Abnormalities
of Chromosome l l q 2 3
MLL Status
Feature
Age (yr)
Sex
.25Race
Leukocyte count
(X 1 0 ~ ~ )
CNS leukemia
Present
Category
>50
S 50
Present
Absent
21
CDlO
CD15 11
Rearranged
<l
1-9
210
Male
.90
Female
20 White
Black
Absent
Present
Absent
14
4
5
14
9
18
5
16
7
7
14
<.001=
5
17
11
Germline
P
2
14
6
13
9
<.001*
MLL Status
Feature
Sex
Race
2
5
17
0
.003*
,009
Leukocyte count
(~1091~)
CNS leukemia
CDlO
18
3
2
18
CD15
.007
Values less than .005 are considered significant (see comment in
Materials and Methods for correction of significance values in multiple comparisons). Not included in the table are comparisons for the
t(4;ll) translocation, DNA index, and mediastinal mass. Ofthese three
features, only the t(4;ll) was significantly associated with MLL gene
rearrangement.
t(4;llI
Category
Rearranged
Germline
Male
Female
White
Black
>50
s50
Absent
Present
Absent
Present
Absent
Present
Absent
6
3
7
.22
2
6
3
8
3
6
6
3
12
8
19
1
4
10
20
17
2
1
18
4
5
20
0
P
1.o
.03
,005
.001*
.005
Values less than ,005 are considered significant (see comment in
Materials and Methods for correction of significance values in multiple comparisons). Not included in the table are comparisons for DNA
index and mediastinal mass. Neither of these two features was significantly associated with MLL gene rearrangement.
From www.bloodjournal.org by guest on October 15, 2014. For personal use only.
2875
PROGNOSIS IN ALL WITH REARRANGEMENT OF MLL
1
0.8
0 1
0
I
I
I
I
I
I
I
1
2
3
4
5
6
7
I
8
Yean from Dlagnosls
Number of patients ai risk a1:
Rearranged
Y Y Y Y
14
Fig 3. Kaplan-Meier estimates of event-free survival (EFS) for all
patients with (n = 23)or without (n = 2 2 ) MLL rearrangements. The
subgroup with rearrangedgenes had a significantlyworse treatment
outcome than did other patients.
The poor outcome relationship in older children was seen
even when the analysis excluded cases with the t(4; 11) translocation. Thus, the poor prognosis of older children with
ALL involving the MLL gene is further evidence of this
gene's adverse influence on clinical outcome, irrespective of
the 1lq23 chromosome partner.
The investigators of a previous study of childhood ALL
with the t(4; 11)suggest that age has a significant prognostic
impact on outcome for patients over I year of age.27.28
This
study, which did not include molecular studies for MLL gene
rearrangements, found that 3 of 8 (38%) patients with ages
from 1 to 9 years failed therapy as compared to 7 of 8 (88%)
patients 10 years of age or older. In the present study 60%
or more of patients in both age groups had a poor clinical
outcome. An explanation for the different outcome in our
patients in not readily evident, but may be due to differences
in therapy or to the small number of patients investigated.
Although unlikely, it is also possible that the translocations
in some of the patients in the t(4; l 1) study did notinvolve the
MLL gene. The t(4; 1 l)(q21;q23)is thought to be invariably
associated with rearrangement of the MLL
but a single case of t(4; I I ) without a detectable rearrangement of
MLL was described in a large molecular study of infant
ALL." These unexplained differences clearly indicate the
need for a larger, prospective cytogenetic and molecular investigation to determine the prognostic impact of MLL gene
rearrangements in patients with ALL who are 1 to 9 years
old.
The results of this investigation provide a compelling reason to test for MLL rearrangements in all newly diagnosed
cases of ALL entered onto treatment protocols. Cytogenetic
studies may fail to detect llq23 translocations, even in infants.lZ.i5.30
A substantial proportion of cases with llq23
abnormalities, especially children older than 1 year, may not
involve the MLL gene." Further, this report underscores the
increasingly important role of molecular studies in establishing prognostic categories of childhood ALL and the need to
curred exclusively between exons 4 and 15.R"0~'"i5~22~25
Several other genes, including RCK and PLZF, can also be
involved in 1 lq23 translocations in cases of myeloid leukemias and lymphomas,'-' but they were not evaluated in the
present analysis.
In contrast to other molecular studies of pediatric leukemiaswith chromosome llq23 abnormalities, 7 of our 12
patients with unbalanced or uncommon translocations of
1 lq23 had no detectable breaks of the MLL gene. In two
previous studies, all of 16 leukemia patients with translocations or aberrations of 1 lq23 other than t(4; 1 l), t(6; 1 l),
t(9; 1 l), and t( 1 l: 19), demonstrated rearrangements of
MLL.9.22However, only 2 of these 16 patients had ALL. This
suggests that in acute leukemias with chromosome 1 lq23
abnormalities, breaks in loci other than MLL may be more
common in ALL than in AML. This may be especially true
for older children with ALL, because 6 of our 7 patients
I
n
with unbalanced or uncommon translocations of l lq23 and
no rearrangement of MLL were over age 1 year.
In agreement with previous molecular s t ~ d i e s , ' ~ we
.~~.'~
show that infants with ALL and rearrangement of MLL have
an extremely poor prognosis. Furthermore, the poor outcome
in infants with MLL gene rearrangements is irrespective of
the type of cytogenetic abnormality. Of the 14 infants with
0.4
p30.02
MLL rearrangements, 4 of 5 with t(4; 11) and 7 of 9 with
other I lq23 translocations failed treatment. These findings
are in agreement with a larger molecular study of infant
M U rearranged (n = 9)
ALL," but contrasts with a smaller cytogenetic study.26In
0 ,
I
I
I
1
l
I
I
the latter study, the investigators suggested that the specific
0
1
2
3
4
5
6
7
8
t(4; 11) translocation, and not other llq23 translocations or
Y e e n from Dlagno6ls
abnormalities, was associated with the poor prognosis of
Number of patients ai risk m:
% Yywyearsm
infants. Because this latter study did not include molecular
2
1
Rearranged
8
2
studies for rearrangements of the MLL gene, it is possible
that some of the non-t(4; 11) cases did not involve the MLL
Fig 4. Kaplan-Meier estimates of event-free survival (EFS) for pagene and hence account for a better treatment outcome. More
tients older than l year, with (n = 9) or without (n = 20) MLL rearimportantly, the adverse prognostic impact of an MLL rearrangements.The subgroup with rearrangedgenes had a significantly
rangement in infant ALL appears to extend to older children.
worse prognosis than did other patients.
-l
,
I
From www.bloodjournal.org by guest on October 15, 2014. For personal use only.
2876
BEHM ET AL
devise treatments specifically directed to the molecular
events underlying leukemogenesis. This studyand others
have clearly shown that infants and older children with ALL
and a rearranged MLL gene, irrespective of cytogenetic findings, have a very poor prognosis and should be considered
for innovative therapies, including bone marrow transplant.
Additional investigations into the prognostic importance of
MLL gene rearrangements in ALL in children between I and
9 years of age are required before making more definitive
therapeutic recommendations for this patient group.
ACKNOWLEDGMENT
We thank P. Odom, M. Griffin, J. Freeman, and R.O. Moore for
technical assistance, and John Gilbert for editorial assistance.
REFERENCES
1. Raimondi SC, Peiper SC, Kitchingman GR, Behm FG, Williams DL, Hancock ML, Mirro J: Childhood acute lymphoblastic
leukemia with chromosomal breakpoints at 1 lq23. Blood 73:1627,
I989
2. Akao Y, Seto M, Yamamoto K, Iida S, Nakazawa S, Inazawa
J, Abe T, Takahashi T, Ueda R: The RCK geneassociated with
t( I I ; 14) translocation is distinct from the MLUALL-l gene with
t(4; 1 I ) translocations. Cancer Res 52:6083, 1992
3. Radice P, Tunnacliffe A: Distinct breakpoints in band l lq23
of the t(4; 1 1 ) and t( 11; 14) associated with leukocyte malignancy.
Genes Chromosom Cancer 5:50, 1992
4. Chen Z, Brand NJ, Chen A, Chen S-J, Tong J-H, Wang 2-Y,
Waxman S , Zelent A: FusionbetweenanovelKruppel-likezinc
finger gene and the retinoic acid receptor
cy locus due to a variant
t( 1 1 ; 17) translocation associated with acute promyelocytic leukaemia. EMBO J 12:1161, 1993
S. BurnettRC,EspinosaR
111, ShowsTB,EddyRL,LeBeau
MM,RowleyJD,Diaz
MO: Molecularanalysisofa
t(l1; 14)
(q23;qI 1) from a patient with null-cell acute lymphoblastic leukemia. Genes Chromosom Cancer 7:38, 1993
6. Height SE, Dainton MG, Keamey L, Swansbury GJ, Matutes
E, Dyer MJS, Treleaven JG, Powles RL, Catovsky D: Acute myelomonocyticleukemia
with t( IO; 1 l)(p13;q23):heterogeneity
of
breakpoints at 1 lq23 and association with recombinase activation.
Genes Chromosom Cancer 1 I :136, 1994
7. Zieman-vanderPoel
S, McCabe NR, GillHJ,Espinosa R,
Patel S, Harden A, Rubinelli P, Smith SD, LeBeau MM, Rowley JD,
Diaz MO: Identificationof a gene, MLL, that spans the breakpointin
I lq23 translocations associated with human leukemias. Proc Natl
Acad Sci USA 88:10735, 1991
8. Cimino G, Moir DT. Canaani 0, Williams K, Crist WM, Katzav S, Cannizzaro L, Lange B, Nowell PC, Croce CM, Canaani E:
Cloning of ALL-I, thelocusinvolved
in leukemias with the
t(4; 1 l)(q21;q23), t(9; 1 l)(p22;q23), and t(lI ; 19)(q23;p13) chromosome translocations. Cancer Res 5 1:6712, 1991
9. ThirmanMJ, Gill HJ, Burnett RC,MbangkolloD,McCabe
NR, Kobayashi H, Ziemin-van der Poel S, Kaneko Y, Morgan R,
Sandberg AA, Chaganti RSK, Larson RA, LeBeau MM, Diaz MO,
Rowley JD: Rearrangement of theMLL gene in acute lymphoblastic
and acute myeloid leukemias with 1 lq23 chromosomal translocations. N Engl J Med 329:909. 1993
IO. Gu Y, Nakamura T, Alder H, Prasad R, Canaani 0, Cimino
G, Croce CM, Canaani E: The t(4; 11) chromosome translocationof
human acute leukemias fuses the ALL-I gene, related to Drosophila
trithorax, to the AF-4 gene. Cell 71:701, 1992
1 I . Tkachuk DC, Kohler S, Cleary ML: Involvement of a homolog of Drosophila trithorax by 1 lq23 chromosomal translocationsin
acute leukemias. Cell 7 1 :691. I992
12. RubnitzJE, Link MP, Shuster JJ, Carroll AJ, Hakami N.
Frankel LS. Pullen DJ, Cleary ML: Frequency and prognostic significance of HRX rearrangements in infant acute lymphoblastic leukemia: A Pediatric Oncology Group Study. Blood 84570. 1994
13. Raimondi SC, Frestedt JL, Pui C-H, Downing JR, Head DR,
Kersey JH, Behm FG: Acute lymphoblastic leukemia with deletion
o f 1 lq23 or novel inversion ( I I)(p I3q23) lack MLL gene rearrangements and have favorable clinical features. Blood 86: 188 I 1995
14. Pui C-H,BehmFG,DowningJR,HancockML,Shuflleff
SA,RibeiroRC, Head DR,MahmoudHH,SandlundJT,
Furman
WL, Roberts WM, Crist WM. Raimondi SC: 1 lq23/MLL rearrangement confers a poor prognosis in infants with acute lymphoblahtic
leukemia. J Clin Oncol 12:909, 1994
IS. ChenC-S,SorensenPHB,DomerPH,Reaman
GH, Korsmeyer SJ, Heerema NA, Hammond GD, Kersey JH: Molecularrearrangements on chromosome l l q 2 3 predominate in infant acute
lymphoblasticleukemiaandareassociated
with specific biologic
variables and poor outcome. Blood 81:2386. 1993
16. Evans WE, Rodman J, Relling MV, Crom WR, Rivera GK,
Crist WM, Pui C-H: Individual dosages of chemotherapy as a strategy to improveresponseforacutelymphocyticleukemia.Semin
Hematol 28: I S, 199 I
17. Pui C-H, Relling MV. Behm FG, Hancock ML, Boyett JH,
Raimondi SC, Krance RA. Mahmoud H, Riberio RL. Sandlund JT,
Head DR, Evans WE, Crist WM, Rivera GK: L-asparaginase
may
potentiate the leukemogenic effect of the epipodophyllotoxins. Leukemia (in press)
18. BennettJC,Catovsky
D, DanielMT,Flandrin
G, Galton
DAG, Gralnick HR. Sultan C: The French-American-British (FAB)
Cooperative Group: The morphologic classificationof acute lymphoblastic leukemia: Concordance among observers and clinical correlations. Br J Haematol 47553, 1981
19. Williams DL, Harris A, Williams KJ, Brosius MJ, Lemonds
W: A direct bone marrow chromosome technique for acute lymphoblastic leukemia. Cancer Genet and Cytogenet 13329, 1984
20. ISCN: in Mitelman F (ed): Guidelines for Cancer Cytogenetics, Supplement to An International System for Human Cytogenetic
Nomenclature. Basel, Switzerland, Karger, I99 I , p I
2 I . Behm FG, Raimondi SC, Schell MJ, Look AT, Rivera GK,
Pui C-H: Lack of CD45 antigen
on blast cells in childhood acute
lymphoblastic leukemia is associated with chromosomal hyperdiploidy and other favorable prognostic features. Blood 79: 101 1, 1992
22. Sorensen PHB, Chen C-S, Smith FO, Arthur DC, Domer PH,
Bernstein ID, Korsmeyer SJ, Hamond GD,
Kersey JH: Molecular
rearrangements of the MLL gene are present in most cases of infant
acute myeloid leukemia and are strongly correlated with monocytic
o r myelon~onocytic phenotypes.J Clin Invest 93:429. 1994
23. Domer PH, Fakharzadeh SS, Chen C-S, Jockel J. Johansen
L, Silverman GA, Kersey JH, Korsmeyer SJ: Acute mixed-lineage
leukemia t(4; I l)(q21;q23) generates an MLL-AF4 fusion product.
Proc Natl Acad Sci USA 90:7884, 1993
24.StrongRC,KorsmeyerSJ,ParkinJL,ArthurDC,
Kersey
JH: Human acute leukemia cell line with the t(4; I I ) chromosomal
rearrangementexhibitsBlineageandmonocyticcharacteristics.
Blood 65:2 I , I985
25. Cimino G, Lo Coco F, Biondi A, Elia L, Luciano A, Croce
CM, Masera G. Mandelli F, Canaani E: ALL-l gene at chromosome
l lq23 is consistentlyaltered in acuteleukemiaofearlyinfancy.
Blood 82544, 1993
V, Feusner J.
26.HeeremaNA,ArthurDC.SatherH,Albo
LangeBJ,SteinherzPG,ZelterP,Hammond
D, ReamanGH:
of age at
Cytogeneticfeatures of infantslessthan12months
diagnosis of acute lymphoblastic leukemia: Impact of the 1 lq23
breakpoint on outcome: A report of the Childrens Cancer Group.
Blood83:2274,1994
~
From www.bloodjournal.org by guest on October 15, 2014. For personal use only.
PROGNOSIS IN ALL WITH REARRANGEMENT OF MLL
27. Pui C-H, Frankel LS, Carroll A J , Raimondi SC, Shuster JJ,
Head DR, Crist WM, Land VJ, Pullen DJ, Steuber CP, Behm FG,
Borowitz MJ: Clinical characteristics and treatment outcome of
childhood acute lymphoblastic leukemia with the t(4; 1l)(q21;q23):
A collaborative study of 40 cases. Blood 77440, 1991
28. Pui C-H, Carroll AJ, Raimondi SC, Shuster JJ, Crist WM,
Pullen DJ: Childhood acute lymphoblastic leukemia with the
t(4; 1l)(q21;q23): An update. Blood 83:2384, 1994 (letter)
29. Downing JR, HeadDR, Raimondi SC, Carroll AJ, Curio-
2877
Brint A M , Motroni TA, Hulshof MG, Pullen J, Domer PH: The
der(] ])-encoded MLWAF-4 fusion transcript is consistently detected
in t(4; 1l)(q2l;q23)-containing acute lymphoblastic leukemia. Blood
83:330, 1993
30. Griesinger F, Elfers H, Ludwig W-D, Falk M, Rieder H,
Harbott J, Lampert F, Heinze B, Hoelzer D, Thiel E, Riehm H,
Wormann B, Fonatsch C, Hiddemann W: Detection of HRX-FEL
fusion transcripts in pre-pre-B-ALL with and without cytogenetic
demonstration of t(4; 11). Leukemia 8542, 1994









© Copyright 2026