
Document 3385
PN-ABJ- 'I51
The Health Technologies
TABLE OF CONTENTS
THE HEALTH PROBLEM:
WHY CHILDREN DIE...........................l
.......................................8
IMMUNIZATION...................................................22
NUTRITION RELATED TECHNOLOGIES .................................29
BIRTH SPACING. .................................................44
DIARRHEAL DISEASE CONTROL
HEALTHCOM i s designed t o a s s i s t developing c o u n t r i e s use
communications more e f f e c t i v e l y i n support o f n a t i o n a l c h i l d
s u r v i v a l programs.
T h i s document has been prepared f o r HEALTHCOM
p l a n n i n g and assistance teams by HEALTHCOM s t a f f and s e n i o r
consultants as a guide to each of the major child survival
technologies:
D i a r r h e a l disease c o n t r o l
Imnunization
N u t r i t i o n r e l a t e d technologies
B i r t h spacing
THE HEALTH PROBLEM:
WHY CHILDREN D I E *
*This
M.P.H.,
paper was reviewed f o r t e c h n i c a l c o n t e n t by Robert E. Black,
The John Hopkins U n i v e r s i t y School o f Hygiene and Pub1 i c H e a l t h
M.D.,
Health cpnditions vary greatly from country to country and kithin most
countries, but throughout the developing world they are substantially inferior
to those in affluent countries. It is estimated that one-tenth of the life of
the average person in a developing country is seriously disrupted by i l l
health.
The major killers of small children are gastrointestinal and
respiratory infections, measles, and malnutrition--conditions for which
inexpensive, effective prevention or treatment is technically possible.
Most countries now have publicly financed systems of health care and
programs of investment in sanitation, water supply, and health education.
Government health care facilities generally reach to the district or, in a few
countries, even to the village level. Fragmentary evidence suggests that in
total as much as six percent to ten percent of gross domestic product (GDP) is
spent by the public sector and by private individuals on health care.
Despite the large expenditures on health and the technical feasibility of
addressing many of the most common health problems, efforts to improve health
have had a modest impact on the health of the vast majority of the population
in most developing countries. Health care systems in developing countries
have often been patterned after those found in industrialized countries. As
such, they have focused on the institutional care of sick people, often in
highly sophisticated hospitals. At the same time, physicians in developing
countries have been supported by fewer auxiliary health workers--nurses,
technicians, clerks, administrators, and so forth--than is customary in
industrialized countries. Instead of a health manpower pyramid in which a few
physicians are supported by a much larger number of nurses and auxiliary
workers, most developing countries have a manpower hourglass with doctors at
the top, indigenous practitioners at the bottom, and few people in between.
Though no't present in all developing countries, the following problems
are frequently encountered:
o
o
o
o
o
o
o
o
Health facilities are geographically inaccessible.
Economic barriers exclude many people.
Curative care is emphasized over prevention.
Hospital facilities are excessive.
Education of physicians neglects common local health problems.
Health workers are not sufficiently trained, supported, or
supervised.
The availability of services is erratic.
The services provided are not perceived as being efficacious by
their intended beneficiaries.
1. Sections selectively excerpted from World Bank Health Sector Pol icy Paper, 1980.
For the developing countries as a group, life expectancy at birth is
approximately 53 years. Life expectancy at birth in Africa is now about 47
years; in S w t h Asia it is approximately 49 years; and in Latin America,
approximately 61 years. In contrast, life expectancy in the developed regions
is approximately 70 years. The low life expectancy in developing countries
can largely be attributed to very high death rates among children. In the
poorest regions of low-income countries, half of all children die during the
first year of life; in Africa as a whole, the infant mortality rate is more
than 100 deaths per thousand births compared with 15 per thousand in developed
countries.
Assessment of the health situation requires knowledge not only of death
rates and life expectancy rates for all age groups but also of the
distribution, by cause, of mortality and morbidity. Reliable information on
patterns of disease is unavailable on a countrywide basis for most nations.
Many problems arise in analyzing such data: underreporting is more common for
some diseases than for others; multiple causation leads to misreporting; and
many deaths are registered without identification of causes (in Thailand, for
example, such deaths account for 59 percent of the total reported, and in Iraq
the proportion is 44 percent). The following table from UNICEF's Assignment
Children shows the variation of primary causes of infant mortality and
possible reductions due to critical interventions.
A.
-
Causes of Mortality/Morbidity in Infants
Fecal-oral Diseases
The most widespread diseases in developing countries are those
transmitted by human feces--the intestinal parasitic and infectious diarrheal
diseases--but also poliomyelitis and typhoid fever. These diseases spread
easily in areas without community water supply systems. The category "all
forms of dysentery'' was the most frequently noted communicable disease in
~akistan.' In Egypt, Iran, and Venezuela, the monthly incidence of diarrhea
among children p f preschool age has been estimated to be between 40 percent
and 50 p e r c e n t .
Airborne Diseases
The second major group consists of airborne diseases. The group includes
tuberculosis, pneumonia, diphtheria, bronchitis, whooping cough, meningitis,
influenza, measles, smallpox, and chicken pox. These diseases are spread by
inhaling the airborne respiratory secretions of infected persons. A study of
deaths among children five years of age in selected areas of Latin America and
the Caribbean reveals that more than 70 percent of the deaths beyond the
2.
World Health Organization. The Fifth Report on the World Health Situation,
1969-1972--Part I I ; Review by Country and Territory (Geneva: WHO, 1974).
3.
Van Zijl, W.J. "Studies in Diarrheal Diseases in Seven Countries," Bulletin of the
World Health Orqanization 35 (Geneva: WHO, 1966), pp. 249-261.
3
f
B
POTENTIAL REDUCTION IN INFANT NiD CUILD DEATllS WITH P R O V W DISEASE CONTROL TECUNOLOCIES
ESTIMATED NO.
OF DIWTIIS
(in mill ions)
DISEASE
Diarrhea
Imnuniznble diseases
3.3
~neumonia/Lower respiratory
infection
Low birth weight,
malnutrition
TOTALS
INTERVENTION:;
EFFECIIVINESS
(percent )
S
ORT
50
- 75
-5
Vaccines
80
- 95
4
Penicillin
Rohde, J.E.
2.5
3
-
3.5
-
4.5
2
Maternal
supplements
Treat infections
Cont racept i011
1:
nSource:
50
P O T W TI AL
REDUCTION
(in millions)
1
Assignment Childrc.1 #61-62; 35-67, 1983 ( U N I G E P / C ~ ~ ~ V ~ )
10
perinatal period were due to fecally related diseases, airborne diseases, or
malnutrition.
-
Vectorborne Diseases
Vectorborne diseases are less widespread and figure less prominently in
mortality and morbidity statistics but are, nonetheless, significant in the
developing world. The most widespread of these diseases are malaria, trypanosomiasis (sleeping sickness), Chagas disease, schistosomiasis (bilharzia), and
onchocerciasis (river blindness).
Approximately 850 million people live in
areas where malaria continues to be transmitted despite activities to control
it. An additional 345 m'llion people reside in areas with little or no active
malaria control efforts. 1
Malnutrition
Malnutrition is also a major contributing factor in infectious disease;
it impairs normal body responses to disease and reduces acquired immunity.
The importance of malnutrition as a contributing cause of illness and death
has been widely documented. Diarrheal diseases have resulted in large numbers
of deaths among undernourished children in Guatemala. Similarly, it has been
observed that mortality due to measles was 274 times as high in Ecuador as in
the United States in 1960-61 prior to the development of immunization to the
disease.
Disease and Hygiene
The fecally related and fecally transmitted diseases found throughout the
developing world share a common origin: the contamination of food, water, or
soil with human waste. If water is unsafe for drinking or is insufficient for
personal hygiene, diarrheal disease will spread easily. Several diseases are
related to personal cleanliness rather than to fecal contamination. These
include trachoma, conjunctivitis, and other skin infections.
The link between sanitary conditions and health is illustrated by studies
that report on health improvement resulting from better water supply and
sewerage facilities.
Studies in several developing countries document a
reduction in diarrhea{ diseases brought about by better water supply and
sanitation facilities.
Not all studies, however, show that improved water supply systems and
sanitation facilities result in improvements in health. Several studies have
concluded that the source of water supply for a family matters less than :light
be expected:
"The bacteriological purity of water as measured by type, city
4.
World Health Organization.
Malaria:
Processed Report for the Special
Programme for Research and Training in Tropical Diseases (Geneva: WHO, 1976).
5.
Van Zijl, "Studies on Diarrheal Disease in Seven Countries," pp. 249-261.
-5-
or well, did not influence infection rate^."^ The answer to this paradox may
possibly be found in the cultural practices of the population studied. For
water is often stored in cooling jars that are nearly always
example, drinking
contaminated. Or families may continue to drink well or river water because
of greater convenience, better taste, social reasons, or its supposed special
qualities. Cases also can be found where latrines hap little effect on the
prevalence of disease or even had a negative effect.
Here, too, cultural
habits may offer an explanation. A poorly maintained latrine may be worse
than none at all.
The ambiguous findings do not cast doubt on the link
between sanitary conditions and disease.
Rather, they point to the
difficulties encountered in trying to change traditional patterns of behavior.
In general, improvements in water supply, sanitation, and housing can
reduce the incidence of disease and in this way affect mortality. Improved
nutrition not only reduces the incidence but also decreases the effects of
disease. Health care can do little to alter the incidence of many infectious
and parasitic diseases common in developing countries, although it can often
speed recovery.
Most importantly, a growing package of new health care
technologies offers the hope of saving millions of lives.
The 100 million children born in developing countries this year begin
facing risks the moment they are born. Because their mothers are likely to be
malnourished, they are born smaller. Infants weighing less than 2,500 grams
account for 50 to 80 percent of all neonatal deaths. One observer theorizes
that as much as 50 7ercent of perinatal mortality may be attributable to
unrecognized and inadequately managed maternal i n f e ~ t i o n . ~In countries where
prenatal care is either inadequate or nonexistent, such infection is
especially likely to be undetected.
The lack of prenatal care also increases the danger of neonatal
tetanus.
Babies born in unsanitary conditions, without the protection of
their mother's being immunized, face the risk of tetanus, which is often
fatal. Approximately one million children die from tetanus each year.
B.
The Synergy BetweenDiseaseand Nutrition
The synergy between disease and nutrition is responsible for killing
children in developing countries. The severity of infections would not be so
great if children were well nourished. The infections themselves result in
food loss, food withholding, and lack of appetite. While health interventions
may reduce morbidity and mortality from a specific cause, they may not have a
profound impact on overall morbidity and mortality. A program in Bangladesh,
6.
Stewart, William H., Leland J. McCabe, Jr., Emmarie C. Hemphill, and Thelma
DeCapito. "The Relationship of Certain Environmental Factors t o t h e Prevalence
of Shigella Infection," American Journal of Tropical Medicine and Hygiene, 4:718724, 1955.
7.
Van Zijl, "Studies on Diarrheal Disease in Seven Countries," p. 252.
8.
UNICEF, State o f t h e W o r l d l sChildren, 1985, UNICEF, New York, p. 43.
for example, reduced the diarrhea case fatality rate by fpproximately 80
percent but had a negligible impact on overall mortality.
A study of a
measles outbreak in The Gambia found that 5 percent of the children died
during the outbreak; but that 10 percent of those who survived measles were
dead as a result of other causes nine months later.
By focusing on the health technologies most likely to enable families to
break this cycle of disease and malnutrition, health care systems will have
some hope of improving chi ld survival.
Once considered isolated
interventions, immunization, ORT, infant and maternal feeding, growth
monitoring, child spacing, and now vitamin A supplementation are being
considered vital elements in a technology package.
9.
Rahaman, et al., ICDDR, B, unpublished data, 1979.
DIARRHEAL DISEASE CONTROL*
*This paper was reviewed f o r t e c h n i c a l content by Norbert Hirschhorn, M.D.,
t h e John Snow P u b l i c H e a l t h Group, Inc., Boston, MA.
-8-
DIARRHEAL DISEASE CONTROL
A.
Acute I n f a n t Diarrhea
The World Health Organization estimates t h a t t h e r e are some 500 m i l l i o n
episodes o f i n f a n t d i a r r h e a a year which r e s u l t i n t h e deaths o f about f o u r
m i l l i o n c h i l d r e n i n A f r i c a , Asia, and L a t i n America.
Studies i n Guatemala i n d i c a t e t h a t a v i l l a g e c h i l d may have as many as
i x t o t e n bouts o f d i a r r h e a a year, each l a s t i n g an average o f t h r e e days.
n a d d i t i o n t o being a pervasive k i l l e r , d i a r r h e a i s a l s o a s i g n i f i c a n t
c o n t r i b u t o r t o m a l n u t r i t i o n i n those c h i l d r e n who survive. Through increased
malabsorption, reduced food i n t a k e caused by l o s s of a p p e t i t e and food
withdrawal, and fever, c h i l d r e n are deprived of needed nourishment.
Diarrhea i s caused by b a c t e r i a l , p a r a s i t i c and v i r a l agents, b u t t h e
p r e c i s e e t i o l o g y of most s e r i o u s d i a r r h e a i n developing c o u n t r i e s i s n o t w e l l
understood.
B a c t e r i a l agents a r e t r a n s m i t t e d by unclean water, food and
hands, w h i l e v i r a l agents are borne l a r g e l y by d r o p l e t s o f mucous o r by a i r .
B a c t e r i a account f o r t h e l a r g e s t number of d i a r r h e a l episodes i n poor
c o u n t r i e s and u s u a l l y peak i n t h e summer. The general c l i n i c a l p r o f i l e f o r
both b a c t e r i a l and v i r a l i n f e c t i o n s i s s i m i l a r , although v i r a l cases tend t o
be shorter and more severe.
Unsanitary b i r t h procedures and a mother's s o i l e d hands o r breasts
represent p o t e n t i a l sources of contamination f o r t h e newborn i n f a n t .
As the
c h i l d grows and begins t o d r i n k water and e a t weaning foods t h e r i s k o f
d i a r r h e a l i n f e c t i o n increases.
A d u l t s and o l d e r c h i l d r e n can discharge
disease-causing b a c t e r i a l agents i n t h e i r feces and y e t m a n i f e s t no symptoms
o f disease.
These agents may be t r a n s m i t t e d i n a v a r i e t y of ways, i n c l u d i n g
d i r e c t c o n t a c t w i t h feces through another person's d i r t y hands, o r by a c h i l d
c r a w l i n g on t h e ground o r f l o o r o r i n d i r e c t c o n t a c t through contaminated water
which i s then t r a n s m i t t e d t o t h e c h i l d through b o t t l e d formulas o r weaning
foods prepared by those w i t h d i r t y hands.
Perhaps t h e g r e a t e s t source o f
i n f e c t i o n i s weaning foods.
I n t r o p i c a l heat, b a c t e r i a grow r a p i d l y i n these
types o f foods which r e s u l t s i n d i a r r h e a .
Because s t o o l consistency and frequency vary from one c h i l d t o another,
t h e mother i s probably t h e best judge o f what i s abnormal.
Generally, any
increase i n t h e number and l i q u i d i t y o f s t o o l s w i l l be recognized as
diarrhea. I n some cases, t h e c h i l d may recover from d i a r r h e a w i t h i n 24 hours,
b u t i t u s u a l l y l a s t s t h r e e t o f i v e days.
I n most cases, continued d i a r r h e a
w i 11 produce dehydration.
The m o t h e r ' s response t o d i a r r h e a i s cu1 t u r e
s p e c i f i c b u t g e n e r a l l y includes one o r a l l o f t h e f o l l o w i n g :
o
Withholding l i q u i d s and food i n t h e b e l i e f t h a t they caused o r
may worsen t h e d i a r r h e a and t h a t t h e c h i l d ' s system needs t o
"rest".
o
Administering a c a t h a r t i c o r l a x a t i v e t o e l i m i n a t e t h e cause of
t h e diarrhea,which may be viewed as worms, p a r a s i t e s , and so
forth.
o Administering an antidiarrhetic, which may reduce the amount of
stool but which wi 1 1 neither destroy the pathogen nor decrease
the dehydration.
If the child does not recover, prolonged or severe diarrhea will usually
lead to dehydration and electrolyte imbalance. Dehydration in infants is
particularly dangerous because the child is dependent on others to provide
fluids and is more likely than adults to become dehydrated by diarrhea. -he
physical signs of dehydration incTude the following:
o Dryness of mouth
o Loss of appetite
o Decreased skin turgor
o Sunken fontanel and eyes
o Crying without tears
o Vomiting
o General listlessness
Even without proper care at this stage, most children will recover but
some will become more dehydrated and die. Death from diarrheal dehydration
can occur within a matter of hours depending upon the type of bacterial
infection, the severity of the diarrhea, the mother's response, and the
child's prior nutritional level. Undernourished children tend to get more
severe diarrhea.
B.
WHO'S Diarrheal Disease Control Proqram
Perhaps the most comprehensive and certainly the most recognized program
for controlling infant diarrhea is the Diarrheal Disease Control Program of
the World Health Organization. This program hinges upon the discovery of a
single technology, oral rehydration therapy (ORT), to treat 85 to 95 percent
of cases of dehydration from diarrhea in all age groups. The oral rehydration
solution does not cure diarrhea but prevents the dehydration which leads to
death. ORT is used instead of intravenous therapy which requires trained
personnel, sterile fluids, and expensive equipment.
ORT is simpler to
administer and much less expensive, thereby making it .less dependent upon
highly trained health workers and fixed facilities. ORS also compensates more
quickly for nutritional loss due to diarrheal disease. Oral rehydration
solution is not the only element in the WHO program, however. WHO also
emphasizes the need for:
o Adequate feeding during and after diarrhea including breast
milk, diluted formula, and usual foods given to children;
o Withholding of antimicrobial agents, antispasmodics, and antidiarrheal drugs because they are unnecessary and may prolong the
infection and inhibit recovery;
o Support of breastfeeding for its immunological effects and
because
it reduces the risk of infection;
o Effective water and sanitation systems along with appropriate
food and personal hygiene practices;
o Health education programs which build upon traditional practices
and beliefs to promote positive changes in decision-makers,
mothers, health personnel, and community leaders;
o Epidemiological surveillance to determine the prevalence and
incidence of diarrhea among populations at high risk.
C.
Oral Rehydration Solution
While the foregoing elements play important roles in the overall WHO
program, it is oral rehydration therapy which offers the hope of saving
thousands of infants by moving effective treatment out of the clinic and into
the community. The rationale for ORT rests upon understanding how the human
digestive system operates. During diarrhea, the gut decreases its capacity to
absorb sodium.
Research on cholera patients demonstrated that sodium
absarption is restored in the presence of glucose and that the ability to
absorb bicarbonate and potassium is not lost during diarrhea. Bicarbonate is
added to the formula to correct acidosis, while potassium is used to replace
the potassium lost through increased stools and urine.
The WHO formula is consequently composed of these four ingredients per
liter of water:
o Glucose
o Sodium chloride
o Sodium bicarbonate or
Trisodium citrate dihydrate
o Potassium chloride
20.Og
3.59
2.59
2.99
1.59
At the first sign of prolonged diarrhea, the child's mother should obtain
a packet of premixed oral rehydration salts. She should add these salts to a
one-liter container of the cleanest water available, not necessarily boiled
water. She then should mix the salts until dissolved and use a spoon to
administer small amounts of the solution to her child over a 24-hour period.
As she administers the solution the child may have a bowel movement,
potentially a- sign to the mother that the solution is causing more diarrhea
which it is not. The child also may vomit if the ORS is given too quickly.
During the first 24-hour period, the mother should give the child all the
breast milk and/or plain water it will take. If the diarrhea continues after
three days, the mother should seek medical assistance. When the child's
diarrhea stops, the mother should continue to give it breast milk and solids
if the child is old enough for solids, adding high calorie foods, if possible,
for several days after the diarrhea.
Mixing
'
Overconcentration o f sodium i n i n f a n t s can cause hypernatremi'a and lead
t o shock and subsequent death. The p o t e n t i a l f o r hypernatremia appears t o be
increased i n dehydrated i n f a n t s .
Research has n o t y e t e s t a b l i s h e d t h e
p e r m i s s i b l e range of sodium v a r i a t i o n , b u t i t i s c e r t a i n t h a t m i x i n g t h e WHO
formula w i t h h a l f t h e r e q u i r e d water i s dangerous and w i t h one t h i r d i s l i f e
threatening. And o b v i o u s l y t o o d i l u t e a s o l u t i o n w i l l n o t be e f f e c t i v e .
I n a d d i t i o n t o c o r r e c t mixing,
t h e s o l u t i o n must be c o r r e c t l y
administered. T h i s i n c l u d e s g i v i n g t h e c o r r e c t amount o f t h e o r a l r e h y d r a t i o n
Some
solution.
Some mothers f e e l t h e baby w i l l n o t d r i n k so much f l u i d .
mothers w i t h h o l d water and/or b r e a s t m i l k d u r i n g therapy, thus adding t o t h e
danger of h i g h sodium concentrations. I n o t h e r instances, o t h e r substances a r e
added t o t h e mix o r i t i s b o i l e d and o v e r - d i l u t e d o r food i s w i t h h e l d i n t h e
b e l i e f t h a t t h e o r a l r e h y d r a t i o n s o l u t i o n c o n t a i n s s u f f i c i e n t n u t r i e n t s . Each
o f these c o u l d p o t e n t i a l l y reduce t h e e f f e c t i v e n e s s o f t h e therapy.
Oel i v e r y
A l i v e l y debate continues among p h y s i c i a n s and p r a c t i t i o n e r s over t h e
most- a p p r o p r i a t e d i s t r i b u t i o n , mixing, and a d m i n i s t r a t i o n o f o r a l r e h y d r a t i o n
s o l u t i o n . The range o f a l t e r n a t i v e s include:
o
Complete f o r m u l a ( a l l f o u r i n g r e d i e n t s )
prepackaged and
d i s t r i b u t e d t o h e a l t h p o s t s where i t i s mixed and administered
by a h e a l t h worker.
I n t h i s s e t t i n g , ORT i s s u p e r i o r t o
intravenous s o l u t i o n s because i t i s cheaper,
safer, and
simpler.
Because i t occurs i n a f i x e d f a c i l i t y , however, i t i s
s t i l l l i m i t e d t o t h a t small percentage o f t h e p o p u l a t i o n which
a c t u a l l y uses h e a l t h posts.
o
Complete formula, prepackaged and d i s t r i b u t e d t o v i l l a g e h e a l t h
workers who have r e c e i v e d some simple t r a i n i n g i n m i x i n g and
a d m i n i s t r a t i o n . These i n d i v i d u a l s would recognize who needs t h e
formula and how much they need and know how t o mix and
They would have a standard l i t e r
administer i t properly.
c o n t a i n e r and would understand t h e danger i n v o l v e d i n t h e
therapy.
Even though t h e t r a i n i n g f o r such an i n d i v i d u a l i s
r e l a t i v e l y simple, many argue t h a t i t i s s t i l l t o o expensive t o
t r a i n -and support such a h e a l t h worker i n every v i l l a g e .
o
Conrplete formula, prepackaged and d i s t r i b u t e d through some
c o m e r c i a 1 o r p u b l i c system d i r e c t l y t o mothers. I n t h i s model,
t h e mothers would l e a r n how t o mix and a d m i n i s t e r t h e s o l u t i o n
from w r i t t e n i n s t r u c t i o n s i n c l u d e d i n t h e package, from verbal
i n s t r u c t i o n s g i v e n a t t h e t i m e o f purchase, o r from r a d i o
broadcasts.
Although t h i s approach c o u l d ready a l a r g e number
i t r a i s e s questions about safe m i x i n g and
o f families,
administration.
.
o
A simple s a l t and sugar formula advocated by h e a l t h workers and
mass media so t h a t mothers can a c t u a l l y make and a d m i n i s t e r t h e
s o l u t i o n i n . t h e i r own home, w i t h l i t t l e o r no o u t s i d e
assistance.
The major s t r e n g t h of t h i s approach i s t h a t i t
ensures t h e widest degree of d i s t r i b u t i o n by using substances
already i n t h e home.
I t a l s o introduces t h e h i g h e s t degree o f
r i s k by i n c r e a s i n g t h e p o t e n t i a l f o r improper m i x i n g and
a d m i n i s t r a t i o n and by excluding bicarbonate and potassium which
may be c r i t i c a l t o c h i l d r e n who have been severely purged o r who
have been vomiting.
I n areas where sugar and s a l t are scarce i t
a l s o r a i s e s problems o f a v a i l a b i l i t y and cost.
The l a t t e r a l t e r n a t i v e has spawned a s e r i e s o f technologies t o h e l p
reduce t h e r i s k o f improper mixing.
These i n c l u d e a pinch and scoop
technique, promotion o f a b o t t l e cap as a measuring spoon, and a v a r i e t y o f
commercially produced double-ended spoons f o r measuring sugar and s a l t
concentrations.
Indeed, a good deal o f experimenting w i t h new ORS
technologies i s t a k i n g place.
Experiments are c o n t i n u i n g w i t h p l a s t i c
packaging r a t h e r than more c o s t l y aluminum, w i t h packages which convert i n t o
one l i t e r containers, w i t h t a b l e t s r a t h e r than powders, and w i t h measurements
by t h e g l a s s r a t h e r than by t h e l i t e r .
I n t h e p a s t few years, f u r t h e r s t u d i e s have been undertaken t o
The bicarbonate anion
i n v e s t i g a t e p o s s i b l e improvements i n the ORS formula.
i n t h e " u n i v e r s a l " formula a v i d l y absorbs water from the environment, thereby
r e s u l t i n g i n an ORS powder w i t h a reduced s h e l f l i f e ( i t cakes and d i s c o l o r s
i f stored t o o long).
C e r t a i n o t h e r anions have been i d e n t i f i e d which can
serve the same p h y s i o l o g i c a l f u n c t i o n as bicarbonate b u t w i t h o u t t h e u n d e s i r able p h y s i c a l p r o p e r t i e s .
I n p a r t i c u l a r , a formula substitut-ing sodium
c i t r a t e f o r sodium bicarbonate has proven e f f e c t i v e i n f i e l d s t u d i e s sponsored
worldwide by WHO.
The c i t r a t e i s now recommended f o r a l l packets because i t
extends s h e l f l i f e .
4.
Cereal-Based ORS
Other a l t e r n a t i v e s and supplements t o t h e simple sugar (glucose) i n t h e
formula a l s o are under i n v e s t i g a t i o n . Rice powder (ground r i c e ) , f o r example,
These starches
has been used t o r e p l a c e t h e glucose i n some ORS formulas.
come i n several forms, which a r e f a m i l i a r and r e a d i l y a v a i l a b l e i n developing
c o u n t r i e s - - f o r example, p l a i n cooked r i c e o r a powder made from g r i n d i n g
popped, unhusked r i c e ("pop r i c e " ) .
Such starches have t h e advantage o f
breaking down t o produce simple sugars, i n c l u d i n g glucose, and c e r t a i n amino
acids, such as g l y c i n e , as w e l l as d i p e p t i d e s which enhance sodium absorption
from the i n t e s t i n a l lumen.
S o l u t i o n s u s i n g rice-based starches have been
demonstrated t o be as e f f e c t i v e i n c o r r e c t i n g dehydration as those formulas
u s i n g glucose o r sucrose and more e f f e c t i v e i n decreasing t h e volume of
diarrhea.
I n a d d i t i o n , t h e c a l o r i c i n t a k e i s t w i c e as h i g h w i t h r i c e f o r t i f i e d ORS as w i t h r e g u l a r ORS.
5.
ORS Market P r e s e n t a t i o n s
More a t t r a c t i v e p r e s e n t a t i o n o f ORS through b e t t e r packaging, packet
sizes adapted t o l o c a l volume measures, ORS i n t a b l e t form, and t h e p r o v i s i o n
o f premixed s o l u t i o n s i n cheap c o n t a i n e r s such as those used commercially f o r
.
juices or soft drinks are being commercially produced in many countries. The
establishment of an ORS "line of products" ranging from homemade solutions to
expensive premixed solutions in sterile water should appeal to the full
spectrum of the buyi-ng public. This is important to ensure wide use at all
levels of society as well as the fiscal viability of ORT programs.
One delivery system promotes different treatments for different degrees
of dehydration. For example, when a mother first detects signs of diarrhea,
she is encouraged to avoid purges; to continue giving the child liquids and to
administer the simple formula home mix. If the diarrhea continues and early
signs of dehydration appear, she should use the prepackaged ORS formula
available from a store, health center, midwife, etc., and administer it as
required over a 24-hours and up to three days if necessary. During this time,
she should continue to breastfeed, give extra water, and feed the child soft
foods.
If the dehydration becomes more serious, she should seek medical
assistance. Oral therapy should be available through all community health
workers and in all health centers and hospitals in the country. Intravenous
therapy should only be used in cases of shock.
In the above system, the least dehydrated child gets the highest risk ORS
As
formula.
Most episodes probably end without further complication.
dehydration increases, safer but less available packets are used and probably
prevent most of the remaining episodes from becoming more serious. In the
re1 ati vely few cases where diarrhea and dehydration continue, either because
the previous treatment failed to work or because it was administered
improperly, the least available treatment alternative becomes necessary and
the child must be taken to the clinic. The principal difficulties with this
seemingly ideal model are that:
o The teaching burden is heavy because all regimens must be taught
to all people.
o Those most likely to need the packets and the health facilities
are those least likely to have access to them because they are
the poorest and most isolated.
6.
Comnunication Issues and ORT
From a communication viewpoint, the behavioral changes required to make
ORT effective raise critical questions which must be answered within the
context of a specific cultural group. They include:
Prevention-Re1 ated Issues
o What personal hygiene practices, for instance hand washing, will
be accepted and will help reduce contamination?
o Can acceptable breastfeeding practices be introduced which will
help reduce the risk of contamination and provide nourishment
during diarrhea?
o What practical weaning practices will reduce contamination and
provide catch-up growth after diarrhea?
The appl ication of ORT and sodium concentrations in WHO prepackaged
formu1 a
-
o Does a common standard liquid volume container exist in the
target area?
o Does the target community have the experience and ability to
follow verbal mixing instructions?
o Does sufficient experience exist with liquid remedies to make
home administration practical?
o Does the target population's attitude toward medicine suggest
that double or triple concentrations of the salts will be
common?
Excessive sodium concentration in home made simple sugar and salt
solution
o Are sugar and salt commonly available in the target area?
o What measuring instrument will be needed to ensure accurate
concentrations of salt and sugar?
o Does the population's attitude toward salt and sugar permit
these ingredients to be mixed In the appropriate manner?
Importance of Potassium
o Do members of the intended audience usually give purges as a
remedy for infant diarrhea?
o Does vomiting occur frequently as part of the diarrheal episode?
o Is there an available source of potassium in the village?
Recognition of the Problem
o What immediate outcome does the target population expect from a
remedy for diarrhea?
o Will the fact that ORT does not halt diarrhea deter the target
population from continued administration of the solution?
o Does the population prefer medicines which are foreign and
modern or those which are traditional and familiar to them?
o Do members of the intended audience accept diarrhea as a serious
problem for which they desire some help?
o Do members of the target population recognize dehydration and
can they differentiate levels of severity?
De 1 iv e r y
o
Who i s t h e most c r e d i b l e source o f
d i a r r h e a among t h e t a r g e t p o p u l a t i o n ?
information
on
infant
o
What i s t h e most e f f e c t i v e d i s t r i b u t i o n p o i n t f o r prepackaging
ORT i n a r u r a l v i l l a g e ?
ORT S t a t u s Today
Over t h e p a s t f i v e years d i a r r h e a l disease c o n t r o l programs have begun i n
52 c o u n t r i e s . With assistance from WHO and t h e Centers f o r Disease Control o f
t h e United S t a t e s P u b l i c H e a l t h Service, 677 h e a l t h system managers from 117
developing c o u n t r i e s have been t r a i n e d i n i n t e r n a t i o n a l t r a i n i n g courses i n
d i a r r h e a l disease c o n t r o l , planning, and management. Another 410 workers have
been t r a i n e d i n supervisory and f i e l d worker courses.
More than 50 m i l l i o n
packets o f ORS have been produced and d i s t r i b u t e d throughout t h e world.
UNICEF has provided 29 m i l l i o n packets, t h e U. S. Agency f o r I n t e r n a t i o n a l
Development has provided approximately n i n e m i l l i o n packets, and 38 developing
c o u n t r i e s produce t h e i r own ORS. Even if u n i f o r m l y d i s t r i b u t e d , these packets
would have t r e a t e d fewer t h a n one i n t e n cases of diarrhea, b u t combined w i t h
t h e a p p r o p r i a t e use o f homemade s o l u t i o n s , t h i s l a r g e q u a n t i t y o f ORS packets
can be expected t o have an important e f f e c t and save t e n s o r even hundreds o f
thousands o f l i v e s .
0.
D i e t a r y Management o f D i a r r h e a l Disease
..,.
The a p p r o p r i a t e emphasis on o r a l r e h y d r a t i o n s o l u t i o n t o prevent death
from acute d e h y d r a t i o n has u n f o r t u n a t e l y been associated w i t h widespread
n e g l e c t o f t h e n u t r i t i o n a l o r f e e d i n g component of ORT.
F a i l u r e t o emphasize
o f therapy can be l a r g e l y a t t r i b u t e d t o both t h e
t h e n u t r i t i o n a l aspec:.
r e l u c t a n c e by c a r e t a k e r s and h e a l t h p r o f e s s i o n a l s t o feed c h i l d r e n d u r i n g
i l l n e s s , t o t h e l i m i t e d s c i e n t i f i c knowledge r e g a r d i n g t h e a b i l i t y o f c h i l d r e n
t o consume and t o l e r a t e s p e c i f i c foods d u r i n g and a f t e r i l l n e s s , and t o t h e
almost t o t a l ignorance o f t h e c l i n i c a l and n u t r i t i o n a l e f f e c t s o f s p e c i f i c
d i e t a r y regimens.
The adverse consequences o f d i a r r h e a on n u t r i t i o n a l s t a t u s and prolonged
episodes o f i l l n e s s have been w e l l documented i n t h e l i t e r a t u r e .
The
n u t r i t i o n a l c o s t o f i n f e c t i o n i n general, and d i a r r h e a s p e c i f i c a l l y , can be
a t t r i b u t e d t o decreased d i e t a r y i n t a k e and i n t e s t i n a l malabsorption d u r i n g
diarrheal illness.
The approach t o n u t r i t i o n a l management o f d i a r r h e a l i l l n e s s by t h e h e a l t h
community has been t o reduce o r e l i m i n a t e food i n t a k e d u r i n g t h e i l l n e s s and
t o compensatory "overfeeding" d u r i n g t h e recovery period. The appropriateness
o f t h i s therapy has r e c e n t l y been questioned by h e a l t h p r o f e s s i o n a l s who
advocate continued f e e d i n g d u r i n g d i a r r h e a l i11ness. The c o r r e c t t h e r a p e u t i c
approach i s s t i l l b e i n g debated, because w e l l - c o n t r o l l e d s t u d i e s o f t h e
a l t e r n a t i v e s have been l a c k i n g .
E.
D i a r r h e a l Disease P r e v e n t i o n
As succe-ssful as ORT i s i n r e d u c i n g d i a r r h e a l m o r t a l i t y , Feachem and
others p o i n t out t h a t i t i s only a p a r t i a l solution t o t h i s serious health
problem. To b e g i n w i t h , ORT s u c c e s s f u l l y reduces m o r t a l i t y b u t has l i t t l e o r
no impact on d i a r r h e a l m o r b i d i t y r a t e s . ORT i s a c u r a t i v e measure, b u t o t h e r
i n t e r v e n t i o n s , such as improved maternal and c h i l d n u t r i t i o n o r improved water
supply and s a n i t a t i o n and improved personal and domestic hygiene are e f f e c t i v e
i n preventing diarrhea.
Back-up i n t e r v e n t i o n s a r e necessary f o r an e f f e c t i v e
d i a r r h e a l disease c o n t r o l program.
Thus f a r , s i x p o t e n t i a l a n t i d i a r r h e a l i n t e r v e n t i o n s have been reviewed by
Feachem:*
(a) measles immunization, (b) supplementary f e e d i n g programs, ( c )
low b i r t h weight, (d) b r e a s t f e e d i n g , ( e ) personal and domestic hygiene, and
( f ) chemoprophylaxis.
Measles I m n i z a t i o n
The r o l e o f measles immunization i n c o n t r o l l i n g d i a r r h e a l disease seems
s i g n i f i c a n t enough t o w a r r a n t t h e a t t e n t i o n o f n a t i o n a l program planners.
T h e o r e t i c a l c a l c u l a t i o n s e s t i m a t e a one p e r c e n t t o seven p e r c e n t i n c i d e n c e o f
measles-associated d i a r r h e a ; f i e l d s t u d i e s i n N i g e r i a and Guatemala r e p o r t a
s i x p e r c e n t m o r b i d i t y . The e s t i m a t e d percentage o f deaths caused by measlesassociated d i a r r h e a a r e t h e o r e t i c a l l y e s t i m a t e d t o be n i n e p e r c e n t t o 77
percent.
One f i e l d s t u d y i n Bangladesh suggests 37 p e r c e n t of d i a r r h e a l
deaths a r e measles associated.
The e t i o l o g y o f t h e d i a r r h e a a s s o c i a t e d w i t h measles i s unknown.
Some
evidence, however, i n d i c a t e s t h a t s h i g e l l o s i s ( b a c i l l a r y d y s e n t e r y ) and o t h e r
forms o f d y s e n t e r y may be t h e most common c u l p r i t s .
Data from f i e l d s t u d i e s and t h e o r e t i c a l c a l c u l a t i o n s i n d i c a t e t h a t
measles immunization can s u b s t a n t i a l l y reduce d i a r r h e a l m o r t a l i t y among
c h i l d r e n from b i r t h t o f i v e years.
Feachem e s t i m a t e s t h a t measles
immunization a t t h e age o f n i n e t o 11 months, w i t h a 45 percent t o 90 p e r c e n t
coverage w i l l a v e r t 44 p e r c e n t t o 64 p e r c e n t o f measles cases, 3.8 p e r c e n t t o
9.6 p e r c e n t o f d i a r r h e a a t t a c k s , and s i x p e r c e n t t o 26 p e r c e n t o f d i a r r h e a
deaths among c h i l d r e n f i v e y e a r s o l d and under.
Although s t u d i e s a r e
r e p o r t e d l y under way i n Bangladesh, t h e r e a r e no f i e l d r e p o r t s t h a t can v e r i f y
these t h e o r e t i c a l assessments.
The c o n s i d e r a b l e h y p o t h e t i c a l impact o f
measles immunization on d i a r r h e a m o r t a l it y ( s i x p e r c e n t t o 26 p e r c e n t ) should,
however, w a r r a n t f i e l d s t u d i e s t o assess t h e r o l e o f measles immunization i n
reducing d i a r r h e a l m o r t a l i t y .
Community research i s needed t o t e s t these
t h e o r e t i c a l s u p p o s i t i o n s , t o determine t h e e t i o l o g y o f measles-associated
d i a r r h e a , and t o determine t h e c o s t - e f f e c t i v e n e s s o f measles immunization as
an i n t e r v e n t i o n f o r an e f f e c t i v e n a t i o n a l d i a r r h e a l disease c o n t r o l program.
*
Feacham, R.G, R.C. Hogan, and M. H. Merson, "Diarrhoea1 Disease C o n t r o l :
Review o f P o t e n t i a l I n t e r v e n t i o n s , " WHO B u l l e t i n , 6 1 (4), 1983.
Suppl enkntary Feeding
Supplementary feeding programs for preschool children have a dubious
impact on diarrheal- morbid1 ty among this age group.
Associations have
frequently been reported between poor nutritional status and increased
diarrheal morbidity, severity and mortality.
Evidence exists that poor
nutritional status makes children susceptible to more severe diarrhea and to
higher case fatality rates and that supplementary feeding programs can reduce
diarrhea severity and mortality.
Diarrheal morbidity, however, seems
unaffected, particularly since supplementary feeding programs are ineffective
among the age group at highest risk for diarrhea, children six months to 23
months old. The nutritional status of this age group seems to be unaffected
by supplementary feeding programs probably as a result of traditional late
weaning and maternal attitudes toward feeding. Feachem suggests attention
might, therefore, be better focused on improving weaning practices and on
modifying maternal attitudes.
In addition to having a dubious impact on mortality and no impact on
morbidity, supplementary feeding programs also are expensive and require
considerable logistical and managerial talents. Consequently, a supplementary
feeding program is un1 i kely to be a cost-effective intervention for the
reduction of diarrhea morbidity. Prospective studies on the relationsh-ip of
nutrition status to the severity of diarrhea are, nevertheless, warranted.
Low Birth Weight
Low birth weight (LBW) is a major determinant of infant mortality in
developing countries. Although no satisfactory evidence has yet been gathered
to indicate that LBW causes diarrheal mortality or morbidity, Feachem
theoretically asserts that in those developing countries where diarrhea is a
major cause of infant deaths, there is likely to be a causal link between LBW
and diarrheal mortality.
An estimated 20 million LBW infants (weighing less than 2,5009 at birth)
are born each year. This constitutes 16 percent of all births around the
world. Recent reports indicate that although only six percent of the infants
born in the United States have LBW, they make up the largest proportion of
infant deaths--as much as 55 percent. Similar findings are expected in
developing countries. The prevalence of LBW seemingly can be reduced once
exacerbating factors are alleviated. These include poor maternal nutrition,
certain infections, pre-eclampsia, arduous work after mid-pregnancy, short
birth intervals, teenage pregnancy, cigarette smoking, and alcohol
consumption. Maternal food supplementation has received the most attention as
an intervention to prevent LBW. One maternal food supplementary program
sponsored by the U. S. Department of Agriculture resulted in increased weight
gain during pregnancy, increased birth weight, and a reduction in the
prevalence of LBW, from ten percent to six percent. Similar studies need to
be conducted and carefully documented in developing countries. A maternal
food supplementation program can be an expensive endeavor, however, and
further research is necessary to verify the results of programs.
If maternal nutrition, health, and lifestyles can be improved in
developing countries, it is theoretically possible that the prevalence of LBW
would fall from 30 percent to 15 percent. Infant mortality rates could be
expected to fall about 26 percent.
Feachem asserts the fall in infant
diarrhea mortality might be similar.
Prospective studies are needed to
investigate these theoretical suppositions. Research is also required to
clarify the etiology of LBW, to determine which interventions are most
effective, and to determine whether those interventions can be cost-effective
strategies for reducing infant mortality. Whatever the relationship with
diarrhea, LBW should receive greater attention in developing countries simply
because it is a major cause of infant mortality.
Breastfeeding
Little reliable data exist to support the argument that breastfeeding
reduces diarrheal mortal i ty. Nevertheless, there is significant evidence, as
Feachem stresses, to indicate that breastfeeding does decrease diarrheal
morbidity. Breastfed children may also be less likely to suffer from severe
or prolonged diarrhea.
This protection is caused not only by increased
nutritional benefits afforded by breastfeeding but also by immunological
properties found in breast milk, the presence of intestional flora exclusively
found in breastfed infants which may inhibit colonization by specific
diarrheal pathogens and the lack of food contamination often found when bottle
milk is used.
In addition, breastfeeding leads to increased intestinal
absorption.
- Theoretical calculations and a recent study in Costa Rica reveal a
dramatic impact of the promotion of breastfeeding on neonatal diarrheal
morbidity and mortality. During a four-year period (1976-1980), a hospital in
Costa Rica promoted early breastfeeding and close mother-child contact.
Neonatal diarrhea1 morbidity fell from 17.7 to 1.6 cases per 1,000 live
births; mortality fell from 3.9 to 0 deaths per 10,000 live births.
Appropriate promotional activities have proven to be particularly
effective in increasing the prevalence of breastfed infants. To promote
breastfeeding, evidence indicates that changes in hospital routines are
necessary, along with the development of information and support programs for
mothers.
The cost-effectiveness of breastfeeding promotion has not been
documented, but it is probably lower than most other antidiarrheal
interventions. On the basis of current evidence, Feachem now encourages the
promotion of breastfeeding. At the same time, however, research is needed to
determine the cost-effectiveness of breastfeeding promotion in developing
countries.
Research also is needed to clarify the levels of protection
afforded by breastfeeding against diarrheal mortality,, to determine the
effectiveness of breastfeeding promotion, and to discern the most suitable
design for a breastfeeding program.
Despite limited mortality data and the need for continued research,
evidence suggests that breastfeeding protects young infants against diarrhea
and should be implemented as an antidiarrheal intervention. Future research
will present new findings that will improve the effectiveness of a program to
promote breastfeeding.
Improved Personal and Domestic Hygiene
Improved personal and domestic hygiene interrupts the direct fecal-oral
transmission of diarrheal pathogens. Low education levels, certain religious
customs,
and s p e c i f i c behavior promote t h e t r a n s m i s s i o n o f e n t e r i c
pathogens.
Handwashing i s one s p e c i f i c behavior most studied.
Washing w i t h
soap and water can be as much as 90 percent t o 100 percent e f f e c t i v e i n
remov ing bacter ia.
Appropriate hygiene education programs can a l t e r behavior and thereby
decrease t h e transmission of d i a r r h e a l pathogens.
The r e s u l t s o f t h r e e
s t u d i e s i n Bangladesh, t h e United States, and Guatemala document t h e impact o f
hygiene education on d i a r r h e a l m o r b i d i t y .
I n Bangladesh, t h e use o f soap and
water r e s u l t e d i n a 35 percent r e d u c t i o n i n t h e incidence o f s h i g e l l o s i s among
A 37 percent r e d u c t i o n i n a
a l l ages i n t h e urban f a m i l i e s studied.
n o n s h i g e l l a d i a r r h e a was observed.
The U.S. study a l s o promoted handwashing
i n day care c e n t e r s among attendants and c h i l d r e n aged s i x t o 29 months. The
r e s u l t s were a 48 percent r e d u c t i o n i n t h e i n c i d e n c e r a t e of a l l d i a r r h e a
among t h e c h i l d r e n .
I n t h e Guatemala v i l l a g e study, t h e promotion of h e a l t h
awareness and h y g i e n i c behavior r e s u l t e d i n a 14 p e r c e n t r e d u c t i o n i n r a t e s o f
d i a r r h e a throughout t h e year among c h i l d r e n aged 0 t o 71 months and a 32 t o 36
percent r e d u c t i o n d u r i n g t h e peak d i a r r h e a seasons.
These s t u d i e s suggest
hygiene education ( p r i m a r i l y t h e promotion of handwashing) has a marked impact
on d i a r r h e a m o r b i d i t y .
Feachem .emphasizes t h r e e general p o i n t s . General education and diseases p e c i f i c education can o f f e r increased p r o t e c t i o n a g a i n s t d i a r r h e a .
Hygiene
education can s u c c e s s f u l l y increase hygiene and decrease d i a r r h e a m o r b i d i t y
r a t e s by 14 t o 48 percent.
And f i n a l l y , hygiene education seems p a r t i c u l a r l y a t t r a c t i v e i n terms o f
c o s t e f f e c t i v e n e s s i n comparison t o water supply and s a n i t a t i o n p r o j e c t s .
Hygiene education programs a r e cheaper and have a l a s t i n g , s u b s t a n t i a l impact.
I n conclusion, 'eachem encourages research t o determine t h e c o s t e f f e c t i v e n e s s o f hygiene education.
More i n f o r m a t i o n i s needed on t h e
a s s o c i a t i o n between s p e c i f i c behaviors and r i s k s of d i a r r h e a l m o r b i d i t y and
mortality.
Operational research i s needed t o c l a r i f y t h e most e f f e c t i v e and
f e a s i b l e types o f hygiene education.
F i n a l l y , i t i s important t o c l a r i f y t h e
impact on d i a r r h e a o f c a r e f u l l y designed hygiene education programs. Hygiene
education programs a r e an e f f e c t i v e a n t i d i a r r h e a i n t e r v e n t i o n and should be
launched i n a l l c o u n t r i e s t h a t want a successful n a t i o n a l d i a r r h e a l disease
c o n t r o l program.
Chemoprophylaxis
L i t t l e evidence e x i s t s t o i n d i c a t e t h a t chemoprophylaxis i s e f f e c t i v e i n
reducing d i a r r h e a l m o r b i d i t y and m o r t a l i t y , except perhaps i n t r a v e l e r s .
The
main use of drugs i n t h e c o n t r o l o f d i a r r h e a l disease i n developing c o u n t r i e s
i s t o prevent c h o l e r a o r s h i g e l l o s i s i n households o f known cases.
'Theoretical c a l c u l a t i o n s suggest t h a t chemoprophylaxis o f households w i t h
known c h o l e r a cases i n Bangladesh might reduce t h e d i a r r h e a i n c i d e n c e i n
c h i l d r e n under f i v e years o f age by 0.02 t o 0.06 percent and d i a r r h e a
m o r t a l i t y r a t e s by 0.4 t o 1.2 percent.
For s h i g e l l o s i s , d i a r r h e a i n c i d e n c e
might be reduced by 0.15 t o 0.35 percent and m o r t a l i t y by 0.3 t o 0.7
percent.
The success o f chemoprophylaxis, however, depends on s k i l l s and
resources t h a t a r e scarce i n developing c o u n t r i e s f o r b o t h t h e c o r r e c t
i d e n t i f i c a t i o n o f c h o l e r a and s h i g e l l o s i s and t h e r a p i d a d m i n i s t r a t i o n o f
drugs to all households with either disease. In addition, chemoprophylaxis
causes side-effects and can contribute to the widespread emergence and
dissemination of antimicrobial resistance. All of the available evidence thus
suggests that chemoprophylaxis is not feasible in many settings, and, even if
adequately implemented, it is not a cost-effective intervention for national
diarrheal disease control programs.
IMMUNIZATION*
*
This paper was reviewed for technical context by Stanley Foster, M.D.,
Centers for Disease Control, U S P k A t l a n t a , GA
-22-
IMUNIZATION
I t i s estimated t h a t , i n t h e developing world, s i x i n f e c t i o u s diseases
k i 11 some f i v e m i 1l - i o n c h i l d r e n annual l y .
These diseases are preventable
through immunization, which i s a much more e f f i c i e n t use o f scarce medical
re'sources than attempting t o t r e a t these diseases a f t e r they occur.
The
e s s e n t i a l components o f an immunization program i n c l u d e t h e a v a i l a b i l i t y of
safe, e f f e c t i v e vaccines, t h e maintenance of t h e potency o f t h e vaccines from
t h e p o i n t o f manufacture through d i s t r i b u t i o n throughout t h e country u n t i l
t h e i r a p p l i c a t i o n , t h e i r c o r r e c t a d m i n i s t r a t i o n , and t h e e f f i c i e n t management
o f program resources t o achieve maximum immunization coverage. Great advances
have been made i n t h i s century i n developing and i r ~ p r o v i r l g vaccines a g a i n s t
t h e major i n f e c t i o u s diseases.
As developing c o u n t r i e s strengthen t h e i r
h e a l t h care systems and extend immunization s e r v i c e s t o a l a r g e r p r o p o r t i o n of
t h e i r populations, they encounter problems d i f f e r e n t from those experienced by
t h e i n d u s t r i a l i z e d nations--problems such as t r o p i c a l temperatures, lack o f
e l e c t r i c i t y , inadequate t r a n s p o r t a t i o n , shortages o f t r a i n e d - p e r s o n n e l and
equipment, and low l e v e l s o f l i t e r a c y among t h e i r populations.
I n r e c o g n i t i o n o f t h e seriousness o f t h e problem o f i n f e c t i o u s childhood
diseases and t h e g r e a t b e n e f i t s o f immunization, t h e World Health O r g a n i z a t i o n
i n s t i t u t e d t h e Expanded Programme on Immunization (EPI) i n 1974. E P I ' s goal
i s t o make b a s i c immunizations a v a i l a b l e t o a l l t h e c h i l d r e n o f t h e world by
1990, w i t h s p e c i a l p r i o r i t y g i v e n t o those i n developing c o u n t r i e s .
The E P I covers s i x major k i l l e r s o f c h i l d r e n i n t h e developing world:
d i p h t h e r i a , whooping cough ( o r p e r t u s s i s ) , tetanus, measles, p o l i o , and
tuberculosis.
Because many cases o f these diseases, and o f t e n t h e most
serious complications, occur i n t h e f i r s t year o f l i f e , E P I has focused i t s
e f f o r t s on reaching i n f a n t s under one year o f age and pregnant women ( t h e
l a t t e r f o r immunizing t h e mothers and thus t h e i r newborn babies a g a i n s t
tetanus).
Measles i s a p a r t i c u l a r l y important k i l l e r o f small c h i l d r e n .
A
case f a t a l i t y r a t e o f 20 percent i n A f r i c a n h o s p i t a l s suggests t h e magnitude
o f the problem.
I n developed countries, t h e case f a t a l i t y r a t e i s l e s s t h a n
one p e r c e n t .
A.
Vaccines
An understanding o f how t h e immuni z a t i o n process works can p r o v i d e
i n s i g h t i n t o many o f t h e t e c h n i c a l problems o f d e l i v e r i n g e f f e c t i v e
immunization services.
Immunity can be o f two b a s i c types, a c t i v e and
passive. I n a c t i v e immunity, t h e body develops i t s own a n t i b o d i e s i n response
t o t h e presence o f a f o r e i g n antigen. Passive immunity r e s u l t s when a person
r e c e i v e s a n t i b o d i e s developed i n another host.
Vaccines are prepared from
m o d i f i e d antigens t h a t are r e l a t i v e l y safe y e t cause t h e body t o produce
a n t i b o d i e s against t h e disease thereby causing antigens.
These m o d i f i e d
antigens must remain unchanged t o guarantee s t i m u l a t i o n o f antibody p r o d u c t i o n
(vaccine potency).
Some vaccines are s e n s i t i v e t o heat and if exposed t o
higher temperatures w i l l change and no longer s t i m u l a t e antibody p r o d u c t i o n
( a r e u n s t a b l e o r heat l a b i l e ) .
Each vaccine has i t s own c h a r a c t e r i s t i c s
regarding safety, e f f e c t i v e n e s s , and s t a b i l i t y .
These are determined i n p a r t
by the n a t u r e o f t h e disease organism i t s e l f , i n p a r t by t h e type o f vaccine
( l i v e , k i l l e d , o r t o x o i d ) and i n p a r t by t h e manufacturing p r a c t i c e used.
D i p h t h e r i a Toxoid
Serious disease caused by t h e C d i p h t h e r i a bacterium i s due t o t o x i n s
result
i n neurologic
and c a r d i a c
produced b y t h e - organism t h a t
abnormalities. D i p h t h e r i a t o x o i d i s u s u a l l y g i v e n i n combination w i t h t e t a n u s
t o x o i d (DT) o r i n a t r i p l e a n t i g e n vaccine (DPT) w i t h p e r t u s s i s and tetanus.
D i p h t h e r i a t o x o i d i s a safe and r e l a t i v e l y s t a b l e vaccine. Few r e a c t i o n s t o
t h e vaccine occur among i n f a n t s and young c h i l d r e n .
To avoid r e a c t i o n s i n
c h i l d r e n s i x years and o l d e r and f o r a d u l t s , a lower dose i s recommended ( l e s s
The
t h a n 2 L f u n i t s r a t h e r than t h e 10 L f u n i t s o r more g i v e n t o i n f a n t s ) .
t o x o i d can be s t o r e d s a f e l y f o r several years a t 4" t o 8"C, b u t i t must n o t be
allowed t o freeze.
Measles
Measles i s a h i g h l y contagious disease and can spread r a p i d l y through
crowded populations.
It can be associated w i t h s e r i o u s c o m p l i c a t i o n s such as
pneumonia and e n c e p h a l i t i s .
L i v e attenuated measles v i r u s vaccine i s a safe,
h i g h l y e f f e c t i v e vaccine, b u t i t r e q u i r e s c a r e f u l h a n d l i n g and storage t o
prevent damage due t o excessive heat o r 1i g h t exposure. Since 1967, when t h e
l i v e vaccine replaced a much l e s s e f f e c t i v e , k i l l e d vaccine i n t h e U.S.A., t h e
deaths and d i s a b i l i t y associated w i t h measles have been g r e a t l y reduced. One
dose r e s u l t s i n t h e development o f a n t i b o d i e s i n 95 percent o f those
vaccinated and i s known t o p r o t e c t a g a i n s t measles f o r a t l e a s t 15 years,
perhaps even f o r l i f e . I t i s recommended t h a t i n f a n t s i n developing c o u n t r i e s
be vaccinated a t younger ages--as soon a f t e r n i n e months as p o s s i b l e - - t o
provide e a r l i e r protection.
Fear t h a t measles vaccine may n o t be e f f e c t i v e
f o r malnourished c h i l d r e n has n o t been supported i n f i e l d s t u d i e s , s i n c e these
c h i l d r e n a l s o develop immunity a f t e r vaccination.
N i n e t y - f i v e percent o f
unvaccinated c h i l d r e n i n developing c o u n t r i e s have had t h e disease by age
f o u r . Both measles and p e r t u s s i s c o n t r i b u t e t o t h e m a l n u t r i t i o n c y c l e and 30
percent o f measles episodes are associated w i t h d i a r r h e a l episodes.
Pertussis
P e r t u s s i s (whooping cough) i s a h i g h l y contagious r e s p i r a t o r y disease.
It has been estimated t h a t , i n an unvaccinated population, a t l e a s t 80 percent
I n developing c o u n t r i e s , one t o t h r e e
o f c h i l d r e n w i l l g e t t h e disease.
percent o f these c h i l d r e n w i l l d i e from p e r t u s s i s , even i f t h e y r e c e i v e
medical care, and many more w i l l s u f f e r s e r i o u s i l l n e s s o r permanent
disability.
The vaccine used f o r p e r t u s s i s i s a s a l i n e suspension
B o r d e t e l l a p e r t u s s i s b a c t e r i a . The vaccine i s u s u a l l y administered
t h e t r i p l e DPT vaccine.
The vaccine i s 80 percent e f f e c t i v e i n
m o r b i d i t y due t o p e r t u s s i s b u t i s c l o s e t o 100 percent e f f e c t i v e i n
m o r t a l i t y due t o p e r t u s s i s .
of killed
as p a r t o f
preventing
preventing
I n o r d e r t o understand t h e i s s u e o f s a f e t y r e g a r d i n g p e r t u s s i s vaccine,
one must compare t h e s i z e and n a t u r e o f t h e r i s k s o f vaccine r e a c t i o n s t o t h e
r i s k s o f c o n t r a c t i n g whooping cough and i t s complications.
R e l a t i v e l y mild,
temporary r e a c t i o n s r e p o r t e d i n c l u d e l o c a l p a i n and s w e l l i n g a t t h e i n j e c t i o n
s i t e , f e v e r , i r r i t a b i l i t y , vomiting, and l o s s o f a p p e t i t e .
Prolonged,
uncontrollable crying,
excessive sleepiness,
and,
even more r a r e l y ,
convulsions~ shock1 i ke state, and encephal i tis are among the more serious
conditions reported in association with pertussis vaccination. Convulsions,
the most frequent immunological reaction following DPT injection, occurred 100
to 3,000 times mdre often during whooping cough than following DPT
immunization. It appears, then, that the risks of the illness far outweigh
the risks of vaccine complications. In the DPT form, pertussis vaccine is
convenient and stable as long as it is refrigerated at 4" to 8°C (it must not
be frozen); it has the additional advantage of acting as an adjuvant for diptheria and tetanus toxoids.
Pol i o
Polio is an acute viral disease that results in permanent paralysis in
approximately one percent of the children infected; ten percent of these
result in death.
In developing countries, paralysis due to polio has been
observed in four out of 1,000 children between the ages of five and nine
years. The paralysis is permanent and quite disabling, often resulting in a
loss of productivity.
Two types of polio vaccine are available: a live,
attenuated vaccine given orally (Sabin) and a ki 1 led inactivated vaccine
injected intramuscularly (Salk).
Both types of vaccine are quite safe. As with any live vaccine, oral
polio is sensitive to excessive heat and light. It should be stored frozen at
minus 20°C or kept refrigerated at 4" to 8°C. The killed vaccine is more
stable and needs only careful refrigeration at plus 4" to 8°C. Because of the
high cost of killed polio vaccine WHO/EPI currently recommends oral polio
vaccine for routine use in developing countries.
Tetanus
Tetanus toxoid is safe and relatively stable. The few side effects
reported are usually due to impurities or allergy and can be avoided by using
highly purified toxoid and not giving boosters too frequently. The three
doses of DPT given to infants provide long-lasting protection against
tetanus.
The two doses o f t e t a n u s t o x o i d g i v e n t o p r e g n a n t women d u r i n g t h e
second half of pregnancy protect both the mother during childbirth and the
baby, because the mother's antibodies pass through the placenta. During the
first month of life, neonatal tetanus has a fatality rate of 85 percent and is
common in many developing countries; thus, the health benefits to be gained
from widespread tetanus immunization of pregnant women are significant.
Neonatal tetanus results from nonhygienic treatment of the umbilical cord
during delivery and the first week of life.
BCG
The bacillus of Calmette and Guerin (known as BCG) was derived from bacteria (Mycobacteria bovis) which are closely related to the bacteria
(M.tuberculosis) that cause tuberculosis (TB). There have been two important
recent developments related to BCG: the availability of a freeze-dried form
and the publication of data from India raising serious questions about the
value of BCG in protecting against tuberculosis. Data suggest that BCG may
protect infants against the more serious life-threatening and meningeal forms
of disease.
As with other live vaccines, BCG is sensitive to sunlight and warm
temperatures. The new freeze-dried vaccine represents a great improvement
over the old liquid form because it is more heat stable. The old form,
however, is sti 1 1 being produced by some companies, but is generally not
recommended for use. When kept at 4°C to 8"C, freeze-dried BCG can be stored
safely for one to two years. BCG also can be kept frozen. If it is not kept
refrigerated, it will gradually lose its potency. The higher the temperature,
the more rapidly potency decreases. The reconstituted vaccine is unstable
and, therefore, must be used within eight hours of reconstitution.
Overall, BCG is considered a safe vaccine. Mild ulcers are occasionally
reported at the site of the intradermal injection. More rarely, inflamed
lymph glands are observed, particularly among infants.
Serious local
reactions can occur when administered subcutaneously and, therefore, the
technique of administration is an important factor in its safety.
B.
Imnrnization Schedules
Immunization schedules are deterrnined by considering the health needs of
the population, the requirements and costs of the particular vaccines chosen,
the resources available, and the way in which services are structured. It i s
seldom possible to achieve the ideal schedule because of conflicting needs;
therefore, many compromises are necessary. The immunological requirements of
the ~accinesmust also be taken into account. Because maternal antibodies can
pass through the placenta and the breast milk, they may interfere with an
infant's ability to respond to a vaccine and to produce his or her own antibodies. The OPT vaccine, for example, should not be given before the age of
six weeks and measles not until nine months of age. A delicate balance is
involved, because the goal of completing the series of doses in time to
protect the child at high risk may conflict with the goal of delaying
vaccination until maternal antibodies subside so the vaccine will "take"
well. Much controversy has arisen regarding the best age at which to give
measles vaccine. In developed countries, where measles usually occurs after
18 months of age, the vaccination is given around age 15 months. In many
developing countries, though, where the incidence of and mortality from
measles are high in the first year of life, the age for immunization
recommended by the EPI is as soon as possible after nine months of age.
Programs that have tried vaccinating for measles at six months have found that
a reinforcing dose after the age of one year is often needed to obtain
long-lasting immunity.
The EPI recommendation is based on a balance of
factors such as maternal antibodies, the pattern of weaning, the rates of
measles occurrence, and the effectiveness of the vaccine at different ages.
For multiple-dose vaccines, the interval between doses presents a similar
dilemma. The longer the interval, the better the "take," but completion of
the schedule is delayed. For OPT, oral polio, and tetanus toxoid, the minimum
interval between sequential doses is one month.
The resources available (including the existing health care system)
determine the type of schedule that is workable. Because each visit is costly
in terms of personnel and transport, the goal is to limit the number of times
a child must return for immunizations. Several types of vaccinations can be
given at the same time, but the minimum interval between doses must still be
observed.
When services are organized around mobile teams or special campaigns,
six-month intervals are the longest that can be used without leaving too many
infants unprotected during the first year of life. Many programs have
developed immunization cards which are retained by the parents (often in a
plastic envelope) and contain a record of the child's vaccinations and the
date of needed return visits.
C.
Vaccination Equipment
For injectable vaccines, supplies of needles and syringes and a method of
sterilizing them are needed. Although disposable, presterilized needles and
syringes seem convenient, they often pose considerable storage and
distribution problems. Reusable glass or nylon syringes work well, and with
correct sterilization techniques are quite safe.
Alternative means of administering vaccines, other than standard needles
and syringes, have also been investigated.
For example, a bifurcated
(two-lined) needle, originally developed for use in smallpox vaccination
campaigns, has been used to administer BCG. It is simpler to use than a
standard intradermal needle and syringe, but it seems to produce less
effective immunity than intradermal injections and requires a more
concentrated and costly form of BCG. Jet injectors which force vaccines
through the skin in a pressurized spray without the use of a needle have been
tried with BCG, DPT, and measles with varying degrees of success. Concerns
about their ability to deliver uniform doses have led to recommendations
against their use, especially with BCG vaccine.
D.
Cold Chain Equipment
The cold chain refers to the maintenance of temperature requirements
during distribution of heat-sensitive vaccines from the manufacturer to the
national vaccine store and eventually to the health workers who give the
vaccinations.
Numerous challenges exist in maintaining an effective cold
chain under the special circumstances often found in developing countries:
the lack of reliable electrical power, high temperatures, the variety of
transport used to carry vaccines and the time needed to reach remote areas,
the shortage of trained equipment maintenance personnel, the difficulties of
communication and transportation when repairs or spare parts are needed, and
the limited funds available. In recent years, WHO/EPI has played a major role
in aiding the development, adaptation, and field testing of equipment to meet
these conditions and in disseminating practical information about the results
of these activities.
The principal elements in the cold chain include:
o Cold rooms for bulk storage of vaccine,
o Vehicles and systems for refrigerated bulk transport of vaccine,
o Refrigerators and freezers for the storage of vaccines,
o Cold boxes, carriers, and vaccine packaging,
o Ice packs and cold packs for cooling insulated containers,
o Thermometers and thermorecorders for monitoring vaccine storage,
o Accessories,
including alarm systems.
E.
Increasing Imnunization Coverage
Several factors are important in improving coverage.
Whenever and
wherever infants and pregnant women come in contact with the health system,
they should be immunized. Attendance at health facilities in most developing
countries tends to occur only at times of illness. Therefore, the World
Health Organization recommends immunization of sick children as well as health
children, except for those critically i l l and requiring hospitalization. From
the standpoint of measles epidemiology, measles immunization during the first
contact at, or after, nine months of age is especially important.
Most immunizations in the developing world are administered by nurses or
paramedical personnel.
The interest, however, that the supervisor
(physician/nurse) takes in what is done, how it is done, and who is doing it
determines in part its success. Where supervisors themselves are involved in
immunization, programs usually succeed. When trying to improve coverage,
reorienting supervisors' attitudes is important.
In the 1970s, logistic problems of vaccine supply and cold chain
maintenance were frequently cited as constraints on immunization. As few as
17 out of every 100 measles injections were, in fact, protective. Although
there are still areas where there is neither fuel for transportation of
vaccine nor kerosene to refrigerate it, immunization is feasible today in most
areas of the developing world. Vaccine costs to fully immunize a child are
approximately US $1.00.
In addition, UNICEF frequently assists in the
procurement of appropriate cold chain equipment and immunization supplies.
Recognizing that most of the obstacles to successful immunization
programs are managerial rather than technical, EPI trains senior and mid-level
staff in planning, logistics (including cold chain management), supervision,
and evaluation. Additional constraints to coverage include a low demand for
these services and superstitions that vaccines are harmful to well children.
Parents do not understand the concept of prevention. Further, when a reaction
occurs after the first dose of OPT, parents refuse to return for more doses
since it made the child i l l , even if the illness was a mild fever. This child
will not complete the OPT series or the ClPV and measles series.
A mutual understanding of goals among managers, health workers, and
communities is essental to success in immunization. When the importance of
measles immunization for all infants nine to eleven months of age is
recognized and such children are monitored, the probability of success is
increased.
Communication with and understanding by the public are
important.
When success is achieved, it needs to be documented and
recognized. When quantitative goals are not reached, problems need to be
identified and solved.
NUTRITION-RELATED TECHNOLOGIES*
*
This paper was reviewed f o r technical content by A l f r e d Sommer, M.D.,
I n t e r n a t i o n a l Center f o r Epidemologic and Preventive Ophthalmology, Wilmer
I n s t i t u t e , Johns Hopkins U n i v e r s i t y , and Kenneth Brown, M.D., School o f
Hygiene and Public Health, Johns Hopkins U n i v e r s i t y , Baltimore, MD.
NUTRITION-RELATED TECHNOLOGIES
The synergy between i n f e c t i o n and m a l n u t r i t i o n i s now w e l l accepted.
There are a s e r i e s of n u t r i t ion-re1 ated technologies and approaches which seem
promi sing f o r reducing the consequences of t h i s i n t e r a c t ion. They are d i v i d e d
i n t o the f o l l o w i n g areas:
A.
1.
Growth Monitoring and E a r l y Childhood N u t r i t i o n
2.
Breastfeeding and Appropriate Weaning
3.
Vitamin A Therapy
4.
Food Supplementation and Weaning Foods
5.
P o s i t i v e Deviance Studies.
Growth Monitorinq and E a r l y Childhood N u t r i t i o n 1
The growth c h a r t i s l i k e an a s t r o l o g e r ' s p r e d i c t i o n f o r
your c h i l d ; buy one f o r him.
Quoted from an I n d i a n mother
The growth c h a r t i s a t o o l f o r both preventive and c u r a t i v e care.
In
developing countries, the c h i l d i s subjected t o m u l t i p l e i n f e c t i o n s s t a r t i n g
a t the age o f s i x months and continuing throughout a l l t h e pre-school years,
although they are g r e a t e r i n under threes.
These i n f e c t i o n s o f t e n impair
growth because they may reduce a p p e t i t e o r i n t e r f e r e w i t h food absorption.
Growth can be monitored w i t h a growth c h a r t and t h e information can be used t o
improve t h e c h i l d ' s n u t r i t i o n a l status.
The major r o l e o f a growth c h a r t i s
t o focus the a t t e n t i o n o f h e a l t h workers on promotion o f adequate growth and
t o teach mothers.
The growth c h a r t i s p a r t i c u l a r l y u s e f u l i n promotion o f
adequate growth, but i t i s a l s o u s e f u l f o r i d e n t i f y i n g and managing many
childhood diseases.
Adequate growth can be achieved o n l y i f the c h i l d i s adequately
nourished.
I t i s o f t e n assumed i n a r u r a l s o c i e t y t h a t breastfeeding alone
w i l l ensure adequate growth up t o the f o u r t h o r even s i x t h month o f l i f e .
Research, however, suggests t h a t many c h i l d r e n might be growing inadequately
by the t h i r d month.
Although c o n t r o v e r s i a l , some studies have shown t h a t
c h i l d r e n under s i x months o l d recovering from m a l n u t r i t i o ' n f a i l e d t o catch up
i n t h e i r mental development.
Measurement o f h e i g h t alone i s o f l i t t l e use i n making day-to-day
decisions regarding c h i l d care.
Because i t i s d i f f i c u l t t o measure height
accurately, t h i s measurement i s n o t s e n s i t i v e t o small changes which might be
c r i t i c a l i n diagnosing inadequate growth.
Even when a c h i l d i s acutely ill,
he does not l o s e h e i g h t i n t h e way he loses weight.
Weight changes can be
1.
S e l e c t i v e l y excerpted from See How They Grow, Morley & Woodland, 1983.
- 30-
easily identified.
Weight i s a much more
n u t r i t i o n a l complications o f i n f e c t i o n .
sensitive
indicator o f
the
-
Stages of Growth
U n t i 1 r e c e n t l y , t h e r e has been i n s u f f i c i e n t research avai l a b l e f o r
designing n u t r i t i o n education programs.
Recent s t u d i e s on stages o f growth
have r e s u l t e d i n important suggestions f o r n u t r i t i o n education.
B i r t h t o Three Months:
The f i r s t t h r e e months o f l i f e are t h e most
important f o r breastfeeding which, however, should r e a l l y continue f o r a t
l e a s t two years. The l i f e of t h e c h i l d i n u n d e r p r i v i l e g e d communities depends
almost e n t i r e l y on q u i c k l y e s t a b l i s h i n g breastfeeding.
The normal c h i l d
should g a i n more than 0.5 kg per month d u r i n g t h e f i r s t t h r e e months o f l i f e .
I n many communities, a c h i l d begins t o r e c e i v e o t h e r
Months 4 t o 6:
foods a t about t h i s age although t h i s v a r i e s widely across c u l t u r e s . Weight
m o n i t o r i n g i s p a r t i c u l a r l y useful between t h e months t h r e e and s i x t o i d e n t i f y
t h e a p p r o p r i a t e time t o supplement breast m i l k . Mothers need t o be encouraged
t o g i v e a wide v a r i e t y o f foods.
Advice i s needed on h i g h energy foods and
t h e i r preparation.
Months 7 t o 12: A t t h i s age, t h e signs o f poor growth o f t e n become more
obvious.
Breast m i l k by i t s e l f i s no longer an adequate source o f energy.
The c h i l d no longer has t h e p r o t e c t i o n g i v e n by a n t i b o d i e s t r a n s f e r r e d b e f o r e
b i r t h , and r a t e s o f i n f e c t i o n increase.
Up t o t h e end o f t h e f i r s t year, b r e a s t m i l k normally contr-ibutes 75
percent o f a c h i l d ' s c a l o r i e s .
Mothers must be c o n t i n u a l l y advised t o
m a i n t a i n f r e q u e n t breastfeeding.
During months seven t o twelve, however, t h e
c h i l d should be o f f e r e d d i f f e r e n t foods.
Months 13 t o 18:
During t h e second year o f 1i f e , t h e l e v e l o f energy
I f a c h i l d eats o n l y one l a r g e meal per
i n t a k e i s p a r t i c u l a r l y important.
Even t h r e e l a r g e meals per day may
day, he w i l l be d e f i c i e n t i n c a l o r i e s .
be i n s u f f i c i e n t .
Research has demonstrated t h a t a c h i l d t y p i c a l l y reduces h i s c a l o r i c
i n t a k e by 25 percent when breastfeeding stops. A c h i l d needs a t l e a s t t h r e e
l a r g e meals a day as w e l l as snacks. F i n a l l y , the c h i l d should be g i v e n foods
t h a t have a h i g h c o n c e n t r a t i o n o f c a l o r i e s t o overcome t h e b u l k problem and
balanced n u t r i e n t s .
I n t h e second year o f l i f e , t h e c h i l d i n a developiug country i s l i k e l y
t o have a t l e a s t two bouts o f s i g n i f i c a n t d i a r r h e a and between f i v e t o t e n
times as many i n f e c t i o n s as a c h i l d i n an i n d u s t r i a l s o c i e t y . Many o f these
episodes a l s o are l i k e l y t o be more severe and prolonged.
Months 19 t o 24: During t h i s period, s p e c i a l a t t e n t i o n must be p a i d t o
breastfeeding. Many advantages are t o be r e a l i z e d i f b r e a s t f e e d i n g continues
and few, i f any, disadvantages.
Unfortunately, many h e a l t h workers s t i l l
advise mothers t o stop breastfeeding a f t e r 18 months. Emphasis must continue
t o be placed on high-energy foods, especial l y i f t h e mother discontinues
breastfeeding.
b n t h s ' 2 5 t o 36: During t h e t h i r d year of l i f e , i n f e c t i o n s become l e s s
frequent.
An East A f r i c a n study showed, however, t h a t energy i n t a k e as a
p r o p o r t i o n of needs was lower d u r i n g t h i s p e r i o d than a t any o t h e r p e r i o d
d u r i n g chilhood.
The c h i l d should have t h r e e n u t r i t i o u s meals a day as w e l l
as snacks.
Weighing C h i l d r e n
Weighing must occur a t an e a r l y stage o f development.
It i s t h e h e a l t h
w o r k e r ' s f i r s t s u b s t a n t i a l c o n t a c t w i t h t h e mother. As such, t h e a t t i t u d e s o f
t h e weigher are important and t h e weigher must speak w i t h t h e mother i n a
r e a s s u r i n g manner.
L i t t l e thought has been g i v e n t o how a mother views
weighing and c h a r t i n g .
Many mothers do n o t understand t h a t t h e weight and
r a t e of growth o f t h e i r c h i l d r e n are r e l a t e d t o t h e i n t a k e o f b r e a s t m i l k and
o t h e r foods.
I n some c u l t u r e s , t h e r e may even be a resentment a g a i n s t
weighing c h i l d r e n , as t h e mothers may associate weighing w i t h s e l l i n g . Hence,
e x p l a n a t i o n should be f u r n i s h e d r e g a r d i n g t h i s important i n t e r v e n t i o n .
While t h e weighing i s t a k i n g place, t h e weigher should take t h e
o p p o r t u n i t y t o f i n d o u t about t h e c h i l d ' s d i e t , t o discuss what foods are
a v a i l a b l e , and t o educate t h e mother concerning t h e c h i l d ' s d i e t i n t h e
future.
I n instances where weight i s inadequate,
i n f o r m a t i o n should be
f u r n i s h e d on t h e importance o f adequate food i n t a k e .
The w e i g h e r ' s a t t i t u d e
must be pleasant and encouraging. An e f f o r t should be made t o ensure t h a t
a1 1 c l i n i c workers demonstrate t h a t t h e y are pleased t o see t h e mothers and
children.
I n a d d i t i o n , t h e a b i l i t i e s and shortcomings o f mothers must be
accepted and understood.
Because t h e need i s f o r one s c a l e f o r approximately 2,000 people, scales
c l e a r l y r e p r e s e n t a major i t e m o f h e a l t h s e r v i c e s expenditure. As such, g r e a t
care i s needed i n s e l e c t i n g which t y p e t o use. Several major types o f scales
a r e a v a i l a b l e b u t hanging scales and beam balances are t h e o n l y ones s u i t a b l e
f o r f i e l d use.
Hanging Scales.
This type o f scale consists o f a spring t h a t stretches
when weight i s hung on it. The e x t e n s i o n o f t h e s p r i n g moves a needle along
t h e weight scale.
I n t h e past, i t was l i k e l y t o become inaccurate, because
t h e s p r i n g ' s c h a r a c t e r i s t i c s change w i t h use.
Recent advances i n t h e
technology o f s t e e l springs, however, have r e s u l t e d i n improved accuracy and
reliability.
Modern hanging scales a r e i d e a l f o r weighing l a r g e numbers o f
children.
Many types o f hanging scales a r e a v a i l a b l e .
New d i g i t a l , s e l f z e r o i n g scales o f f e r g r e a t use, r e l i a b i l i t y , and c o s t advantages. The hanging
s c a l e can be hung from a r a f t e r , a hook i n t h e doorway, t h e c e i l i n g , o r a
t r e e . It should be hung so t h a t t h e d i a l i s on t h e same l e v e l as t h e w o r k e r ' s
eyes.
Whatever methods o f suspension and m a t e r i a l s f o r h o l d i n g t h e baby, i t
i s important t h a t t h e y be based on l o c a l technology and p r a c t i c e .
Beam Balance Scales. The major drawback o f t h e beam balance s c a l e i s i t s
h i g h purchase price--between US$lOO and $150.
Other m i nor disadvantages
i n c l u d e t h e d i f f i c u l t y o f weighing o l d e r c h i l d r e n and t h e problem o f h o l d i n g
c h i l d r e n s t i l l and p r e v e n t i n g them from t r y i n g t o g e t o f f t h e s c a l e w h i l e t h e
weights a r e balanced.
Using Growth Charts
The growth c h a r t i s d i f f i c u l t t o use c o r r e c t l y .
One must ensure t h a t
r e l e v a n t i n f o r m a t i o n i s being c o l l e c t e d , t h a t the i n f o r m a t i o n i s entered
co,rrectly, and t h a t the h e a l t h worker does n o t f a i l t o e n t e r any o f t h e
information.
Problems a l s o e x i s t regarding t h e use of i n f o r m a t i o n entered on
t h e weight c h a r t .
Experience has shown t h a t the concepts necessary f o r
understanding and making the appropriate decisions are the most d i f f i c u l t t o
teach.
Therefore, i t i s necessary t o t r a i n h e a l t h workers thoroughly and
carefully.
Recording I n f o r m a t i o n
The most important i n f o r m a t i o n i s t h e d i r e c t i o n of t h e c h i l d ' s growth
curve. The f o l l o w i n g i n s t r u c t i o n s are the b a s i s f o r teaching.
F i r s t Weighing
o
F i n d o u t t h e month and year o f b i r t h o f t h e c h i l d .
o
W r i t e t h e month and year o f b i r t h on t h e weight c h a r t .
o
A f t e r w r i t i n g t h e b i r t h month i n t h i s f i r s t box, w r i t e t h e same
month i n t h e boxes w i t h a heavier o u t l i n e .
o
Record t h e months i n between.
o
Weigh t h e c h i l d .
o
Place a l a r g e dot on t h e graph on t h e same l e v e l as the weight:
on t h e same h o r i z o n t a l l i n e d i r e c t l y above the month and on the
same v e r t i c a l l i n e as t h e date o f weighing.
L a t e r Weighings
o
Weigh the c h i l d .
o
Find t o d a y ' s date along t h e bottom o f t h e graph.
o
Put another d o t on t h e graph,
today, and above t o d a y ' s date.
o
J o i n t o g e t h e r t h e dots f o r t h e two weighings.
opposite the c h i l d ' s weight
Interpretation
o
Look a t t h e Growth Line.
o
If t h e
Note t h e change i n weight between t h e two weighings.
weight has increased, t h i s i s good.
I f t h e weight has stayed
t h e same o r gone down, t h i s i s n o t good.
o
e.
B.
If'the child's weight, as marked by the dot, is below the lower
line, encourage the mother to increase his food intake and
bring him next month.
Constraints
o
For growth monitoring to be effective, children have to be
weighed frequently. This requires the use of a scale which is
not always culturally acceptable. It also requires that the
child be brought to the scale, a journey that may be costly
both in terms of money and time.
o
Growth monitoring has no immediate benefit and is not limited
to sick children. It may be inconvenient or even difficult for
families to bring a healthy child to the weighing center.
o
Growth monitoring does not contribute to the profile of a
country's health care system and so may not be attractive to
political decision-makers.
o
Unlike ORT and immunization, it is not considered part of the
world of "medicine" and, therefore, is frequently neither
supported nor understood by medical professionals.
o
Growth monitoring requires that mothers do something that is
frequently costly in terms of either time or resources and has
no quick, tangible satisfaction or reinforcement.
o
Growth monitoring asks mothers to invest considerable time in a
well child.
o
The growth monitoring "product" (the growth chart) is now
geared toward health workers more than mothers and is generally
not useful or even understandable to most users.
o
Growth monitoring is a relatively expensive intervention which
appears to have few immediate health status benefits.
o
The actual weighing frequently goes against cultural taboos or
restrictions. For example, in Bangladesh, some fathers do not
permit their children to be weighed because they believe the
fright the child feels hanging in the weighing bag causes
i 1 lness.
Breastfeeding and Appropriate Weaning
Up until approximately 100 years ago, infants worldwide were totally
dependent on breast milk for their survival. The introduction of refined
milk-based products has presented an alternative to breast milk. Human milk
is ideally suited to the needs of the human infant. It provides all of the
nutrients an infant needs during its first few months. The colostrum, which
is produced in the first week after birth, contains more protein, sodium,
zinc, immunoglobulin A, lactoferrin, Vitamin A, and white blood cells and less
fat and lactose than mature milk.
Breast milk also protects the infants
against certain bacteria and viruses.
The proport ion of women choosing to breastfeed their infants has been
declining in some developing countries.
This may in part be because of
increasing female employment and lack of provision for feeding during the
day. Breast milk substitutes provide adequate and safe nutrition for infants
if they are given in sufficient quantities, mixed in the correct proportions
with clean water using sterile equipment, and kept cool and free of contamination until used. However, these conditions are extremely difficult to meet
in most developing countries. Breast milk substitutes also are expensive. A
recent study shows that formula to feed a two-month-old infant costs 40
percent of the salary of a ministry clerk in Burma, 51 percent in Indonesia,
Families substituting formula for breast milk are
and 13 percent in yemen.'
significantly reducing the amount of money available for other essentials.
Mothers choosing to breastfeed need family and community support. Their
nutritional requirements increase, they need to be with the infant often
during the day and night, and they may need to reduce their stress and
workload.
Most of all, however, they need positive reinforcement and
encouragement at the time of birth and throughout lactation. Breastfeeding
and appropriate weaning have been demonstrated to have a dramatic impact on
infant and child health.
The list of benefits is long and well known to
public health specialists.
Benefits
Protection Against Disease:
It has long been recognized that the
breastfed infant is better protected against infections, especially diarrheal
diseases, and has a better chance of survival than a bottle-fed baby. Only
recently have the reasons for this difference been established. Studies of
breast milk and its affect on the intestine have demonstrated that properties
such as lactoferrin, immunoglobulins, lysozyme, white blood cells, and other
factors discourage the growth of harmful bacteria, certain viruses, and some
parasites.
Studies in Brazil, the Philippines, Egypt, and Honduras have
demonstrated that breastfed children have lower diarrhea morbidity and lower
mortality than their bottle-fed counterparts. Even in the developed world,
studies have demonstrated that breastfed babies are healthier. In Britain, o f
the 609 infants treated for gastroenteritis at the Queen Elizabeth Hospital in
London, only two were breastfed.
The link between bottle-feeding and
malnutrition also has been demonstrated.
For example, in Brazil, among a
sample of urban poor school-age children 32 percent of the children who were
bottle-fed were malnourished, while only nine percent of the children who had
been breastfed for more than six months were malnourished.
Lowered Fertility:
Breastfeeding, particularly without supplements,
tends to increase the period of infertility after delivery.
In fact,
breastfeeding has a greater impact on birth spacing in developing countries
than many family planning programs.
Lactating women generally resume
menstruation several months later than nonbreastfeeding mothers although there
are wide variations.
2.
M. Cameron and Y. Hofvander, Manual on Feeding Infants and Young
Children, Oxford Medical Publications, Delhi & Nairobi, 1983, p. 87.
Protection from Allergies:
Breast milk a1 so offers protection from
a1 lergic diseases such as infanti le eczemas.
Conversely, some a1 lergic
diseases and s o m e cases of colic may be provoked by an early introduction of
cow's milk.
Breastfeeding and Cancer:
In developing countries, where the
breastfeeding period is usually longer, the rate of breast cancer is
considerably lower. Preliminary studies indicate that prolonged and repeated
lactation may diminish the risk of breast cancer.
Breastfeeding and Mother-Child Bonding: Breastfeeding immediately after
birth has been demonstrated to strengthen mother-child bonding in both
developing and developed countries.
Despite the proven benefits, the reality is that breastfeeding is
declining throughout the Third World. Some of the most startling figures come
from Chile where 25 years ago 95 percent of the mothers breastfed their
children for one year. Now only 20 percent of the women are breastfeeding.
The reasons for this decline reflect the realities of the 20th century. Women
are increasingly part of the labor force and must work part or full time out
of the home.
Most of these work situations are not conducive to
breastfeeding--working hours are rigid and long and there are usually no
nurseries at the workplace. Family structures are changing and the support
traditionally provided by grandmothers and older women in extended families
does not exist in the urban, semiurban, migrant, or single-parent home. This
has resulted in women having less support for breastfeeding. Finally, women's
decisions regarding breastfeeding are greatly influenced by attitudes and
images.
The public health community is well aware of the success of the
infant formula companies marketing bottle-feeding as more modern, statusgiving, and "sexy" than breastfeeding.
Public health communications incorporating marketing techniques which
have been used so effectively to "sell" bottle-feeding has been applied to
changing and supporting correct breastfeeding and weaning behaviors. Most
breastfeeding campaigns, however, have been used to simply promote the concept
that "breast is best," without considering some of the socioeconomic and
cultural constraints that motivate mothers to bottle-feed.
In addition,
although many physicians agree that "breast is bestn they recommend practices
that interfere with breastfeeding, i.e., timed feedings and early supplements.
Potential Audiences
Decision-makers: Public health communications should be used to educate
and motivate decision-makers to support mothers of infants through codes and
regulations. Ideally, provisions for maternity leave, flexible working hours,
part-time work options, breastfeeding breaks, nurseries in the work place and
day care facilities for older children are potential objectives for public
health communications programs. Public health communications can also assist
women to know their rights in countries where legislation already exists.
(Unfortunately in some places the results of such laws have been to reduce
work opportunities for women.)
Medical Professionals:
The infant formula companies have done an
excellent job of marketing their products both to and through medical
professionals. Complimentary milk samples in hospitals, gifts, free trips,
and additional training for medical professionals have all been used to
involve these important opinion leaders in promoting bottle-feeding. Even in
those countries where these practices have been regulated and changed due to
the International Marketing Code, Western-trained professionals use drugs to
relieve pain or induce labor, which can interfere with the baby's sucking and
make the start of breastfeeding difficult. In most hospitals, babies are
still separated from their mothers for at least 24 hours so that "the mother
can rest."
Recent work in hospitals in Indonesia and Honduras have
demonstrated a dramatic increase in breastfeeding where public health communications are linked with changes in hospital practices.
Families:
Breastfeeding is not carried out in a vacuum, but rather
within the complex socioeconomic context of modern life.
One study in
Honduras demonstrated that urban mothers began bottle-feeding, not because
they felt that it was healthier for their child, but because the supply of
powdered milk was a way that migrant fathers demonstrated they cared about
their wives and children. Fathers and children must be educated and motivated
to provide a "community of support" to replace that which was traditionally
provided by the extended family or the tribe. The MMHP Project in Honduras,
for example, targeted fathers for specific behavior to support mothers while
they were breastfeeding.
Primary health care workers, clinic staff, and
upbeat spots taught fathers that the "breastfeeding mother is special and
needs special care--additional food, liquids, and tenderness while she is
breastfeeding."
Mothers Due in part to the marketing success of the infant formula,
breastfeeding is suffering from an image problem. Social marketing has been
effectively used in several countries to begin to change the image of bottlefeeding as modern.
Extensive work in social marketing of breastfeeding
demonstrates, however, that even many mothers who believe that "breast is
best" do not have either the knowledge or the skills to breastfeed
effectively. In Honduras for example, the MMHP project found that virtually
no mothers understood the relationship between suckling and milk production
and so would bottle-feed if they felt their child was still hungry. They were
also breastfeeding incorrectly--usually for just a few moments whenever the
child cried.
The resulting strategy focused on teaching mothers the
relationship between suckling and milk production and specific skills such as
emptying the breast at each feeding and feeding from both breasts to increase
milk production.
Constraints
o
Promotion of breastfeeding requires counteracting the promotion
of breast milk substitutes. The International Code establishes
principles agreed to by most governments, but health care
providers, pol it ical 1 eaders, and local shopkeepers may not be
aware of the dangers of the incorrect use of substitutes and
the advantages of breastfeeding.
o
Mothers may choose not to breastfeed or stop breastfeeding too
soon because of their income-generating responsibilities.
Employers, other members of cooperative organizations, and
other income earners in the family need to be flexible about
t h e demands they place on breastfeeding mothers although t h i s
may be d i f f i c u l t t o implement.
o
~ e c h n i ~ uon
e how t o breastfeed, qua1 i t y o f breastfeeding, how
much i s given, where o t h e r foods are introduced, and t h e use o f
colostrum are c r i t i c a l .
It i s n o t enough t o promote general
messages such as " b r e a s t i s best."
Careful analysis o f
b r e a s t f e e d i n g p r a c t i c e s must lead t o more s p e c i f i c messages
aimed a t p a r t i c u l a r problems.
V i t a m i n A Therapy
It i s estimated t h a t 500,000 c h i l d r e n i n developing c o u n t r i e s a r e b l i n d e d
S i g n i f i c a n t l y higher i n f a n t
each year because o f Vitamin A d e f i c i e n c e s .
m o r t a l i t y r a t e s among c h i l d r e n one t o f i v e years o l d w i t h m i l d V i t a m i n A
d e f i c i e n c i e s , o r xerophthalmia (on average f o u r time? h i g h e r t h a n m o r t a l it y
r a t e s o f normal c h i l d r e n ) , have a l s o been observed.
D r . Sommer estimates
t h a t as much as 20 t o 30 percent o f i n f a n t deaths i n developing c o u n t r i e s may
be associated w i t h m i l d xerophthalmia.
I n s u f f i c i e n t Vitamin A r e s u l t s i n t h e k e r a t i n i z a t i o n (abnormal
maturation) o f n o t o n l y t h e cornea, t h u s causing blindness, b u t a l s o o f
important mucous membranes found i n t h e surface 1 i n i ngs o f r e s p i r a t o r y ,
u r i n a r y , and i n t e s t i n a l t r a c t s .
This insufficiency impairs the surface
l i n i n g ' s a b i l i t y t o keep o u t b a c t e r i a and e v e n t u a l l y p r o v i d e s an e x c e l l e n t
breeding ground f o r b a c t e r i a .
Consequently, m i l d xerophthalmia predisposes
c h i l d r e n t o two t o t h r e e times more a t t a c k s of d i a r r h e a and r e s p i r a t o r y
diseases.
Indeed, r e s u l t s from a f i e l d t r i a l conducted by D r . Sommer i n
Indonesia demonstrate t h a t V i t a m i n A d e f i c i e n c y i s more i m p o r t a n t t o t h e
development o f d i a r r h e a and r e s p i r a t o r y diseases t h a n i s t h e o v e r a l l
n u t r i t i o n a l status.
Benefits
Xerophthalmia i s e f f e c t i v e l y t r e a t e d and prevented by V i t a m i n A, which
can be administered i n a v a r i e t y o f ways.
V i t a m i n A i s present i n n a t u r a l
foods, such as dark green, l e a f y vegetables, y e l l o w f r u i t s and a l s o can be
prepared i n capsule form o r added t o common foods (such as sugar, wheat f l o u r ,
maize meal, m i l k powder, f a t s
o i l s and weaning foods and seasonings
(monosodium glutamate and s a l t )
I n Indonesia, D r . S o m e r administered two
Vitamin A capsules (each capsule c o s t s between two t o f o u r c e n t s ) s i x months
a p a r t and observed a r e d u c t i o n i n m o r t a l i t y among t h e c h i l d r e n who r e c e i v e d
S t u d i e s i n Guatemala and Costa
t h e Vitamin A o f approximately 30 percent.
Rica demonstrate t h e e f f e c t i v e n e s s o f sugar f o r t i f i e d w i t h V i t a m i n A.
Prior
.'
3.
Somer, A., Tarwotjo, I.,Hussaini, G., Susanto, D., "Increased M o r t a l i t y
i n M i l d Vitamin A Deficiency," Lancet, 2, 1983, pp. 585-588.
4.
Bauernfeind, J.C.,
The Safe Use o f V i t a m i n A - A Report
I n t e r n a t i o n a l Vitamin A C o n s u l t a t i v e Group (IVACG), 1980, p. 10.
of
the
to fortification, 18.2 percent of Guatemala's preschool children had low
Vitamin A levels; after two years of fortification, this figure dropped to 0.3
percent. Costa Rica,had a 32.5 percent incidence of Vitamin A deficiency in
1966 which dr pped to 2.3 percent in 1978 after three years of Vitamin A
fortification.!
As indicated earlier, Vitamin A will not only treat xerophthalmia and
prevent blindness, but it may alsa reduce susceptibility to other major causes
of childhood mortality--notably diarrhea and respiratory diseases. If this is
true in countries other than Indonesia, then it will be evident that Vitamin A
can become yet another powerful and complementary tool in reducing infant
mortality throughout the world.
Constraints
0.
o
Large doses of Vitamin A are toxic if given too frequently.
Unless a child shows signs of xerophthalmia, capsules should
not be given more than once every two or three months, though
once every four to six months will prevent most blindness and
deaths.
This schedule may be difficult to maintain where
health care iystem coverage is meager.
o
In many societies, the early signs of xerophthalmia are not
recognized as abnormal. Children with mild xerophthalmia who
do not receive Vitamin A will move fairly rapidly into a stage
where the disease cannot be cured and partial or complete
blindness will follow.
Food Supplementation and Weaning Foods
Malnutrition in early childhood, primarily due to deficiences of protein
and calories, is considered by many experts to be the world's number one
public health problem.
In addition to protein-calorie malnutrition (PCM),
other forms of severe malnutrition are widespread among children in some
developing countries, notably iron-deficiency anemia and Vitamin A deficiency,
which is the most common cause of blindness in severely affected areas (see
above).
Up to two-thirds of the 400 million children in the world below the age
of five suffer from malnutrition, which is not dramatically apparent, but
which markedly diminishes their ability to withstand infections and hinders
their normal growth and development.
A major proportion of weaning
malnutrition is caused by lack of education, incorrect food and health
beliefs, and poor feeding and health practices. For example, in Burma a
review of several surveys indicates that Burmese women, particularly in rural
areas, withhold primary protein sources from children being weaned, believing
the foods will cause allergies, and purges also are used because of cultural
beliefs.
-
5.
Caplan, E.,
"Vitamin A Decreases Death Rate", Frontlines, March 1985.
- 39-
Poor communities exist in many LDC's where nutrition education cannot be
effective without simultaneous increases in real income. Nutrition education
teaches better use of resources already available to the family. If these
resources do not exist, redistribution efforts will not help. Zeitlin (1978)
has calculated that if the family cannot afford the three to five percent of
total family caloric intake required by the youngest child, nutrition
education probably will have little effect. Improved food availability by
gardening or other agricultural activities is obviously a necessary component
of improved child nutrition.
The challenge of food supplementation for young children is to determine
the best mix of methods to improve weaning food behavior and practices, given
the diversity of causes of infant and early childhood malnutrition and
death. The introduction of other foods (together with breast milk) which are
the most appropriate for the particular culture is the primary goal. This
will require scientific research on the quality and availablility of such
foods and on methods of preparing them and must consider local circumstances,
culturally acceptable and available foods, available cooking facilities, and
current weaning food beliefs and practices, to name just a few. In addition,
where there is a cash economy, particularly in urban areas, it will be
important to advise mothers about the most nutritious and least expensive
weaning foods.,
- Ideally, a child should be gradually weaned to well-cooked nutritious
mashed and/or chopped foods. During this period, the infant will adjust to
the mechanics of chewing, to new tastes and textures, and to the nonsterile
nature of the new foods. In some parts of the world, however, breastfeeding
can be stopped abruptly or prolonged for up two years by those who do not
realize the connection between such practices and infant and child
malnutrition. In other parts of the world, certain nutritious and available
products are not fed to children because of traditional be1 iefs and taboos.
In addition, many traditional societies reserve the most nutritious foods for
the adult males within the family or distribute the food in a hierarchical
order that leaves women and young children ti 1 1 the end. Finally, food bulk
may limit the amount of food a child's stomach can comfortably hold. Because
cereals absorb two to three times their volume of water when cooked, young
children on cereal-grain diets are unable to eat enough to support growth.
The problem of bulkiness can be solved either by providing smaller, more
frequent feedings or by increasing the density of nutrients in the food.
Usually, weaning foods are not offered to the child frequently enough. Field
workers in India have been successful in educating mothers to feed the child
its total daily ration in smaller, more frequent meals.
As a result,
preschoolers have been able to eat sufficient calories and protein to support
growth.
The general characteristics of good weaning food or diet include high
energy and protein content, good supplementary micro-nutrients, acceptability
to parents and infant, locally produced with local ingredients, available in
dry form which is easily stored in tropical environments and which can be
easily prepared by boiling or by the addition of freshly boiled water, and
minimum bulk and maximum availability of nutrients. Methods of weaning food
production general ly may be characterized as conimercial , v i 1 1 age (or
community), and home. Each of these approaches is discussed briefly below.
-.,
~omnercial Production:
Commercially processed foods involve more
sophisticated and costly technology than is used in home or village production
and allows production on a large scale. In addition, vitamin and mineral
mixes may be added to the these foods more easily than is to foods prepared at
home.
Village Production:
Village production of food is similar to home
production, with the exception that the local miller prepares the
ingredients.
The actual weaning food continues to be prepared at home.
Village-level blends cost significantly more than an equivalent quantity of
staples, even per unit of protein. The cost differential represents the price
of the improved quality (usable protein and nutrient density) achieved through
the application of food technology. A combination of industrially processed
ingredients distributed in bulk to villages for mixing also deserves
consideration.
Home Production: From a technological point of view, home production is
the simplest method of developing a weaning food; home production relies on
ordinary techniques of food preparation and thus can be easily implemented.
This approach decreases costs to the needy population and increases community
participation. Locally available foods, such as cereals and legumes may be
combined with a dark green leafy vegetable to provide a nutrient-dense diet
for the child. A number of countries have developed recipes for multimix
dishes that make use of nutritionally adequate foods that are available
local ly.
Recipes for weaning foods stress the use of low-cost, locally available
foods. A recipe that is practical in one season, however, may not be in
another season because the basic ingredients are unavailable.
If
interventions are to be successful, a series of weaning recipes may need to be
developed to reflect seasonal variations in the availability of certain
foods. In addition, .hygiene will remain an important, unresolved problem
unless carefu1,attention is given to proper instruction.
In addition to the problem of malnourished infants, food supplementation
strategies can and must address the problem of maternal undernourishment and
low birth weight (LBW) infants. As noted previously, an estimated 20 million
LBW infants--90 percent of them in developing countries--are born each year
and are more than three times as likely to die in infancy than bpbies of
normal weight. The most important factor in LBW is the mother's own level of
nutrition; quite simply, if the mother does not have enough to eat--roughly
2,500 calories a day--then the growing fetus will not receive the nourishment
it needs.
Preventing LBW by supplementing the diet of at-risk pregnant mothers
promises to be one of the most effecti've ways of breaking into the infectionmalnutrition cycle. A total supplement of 10,000 calories for a severely
malnourished pregnant woman during the last trimester can increase her baby's
birth weight by 50 grams. An average of 600 calories per day for those three
months could lead to an increase of approximately 300 grams.
To date, however, maternal food supplementation programs have not been
particularly successful. Many tend to be expensive, logistically complicated,
and limited in effectivs coverage. Alternative delivery approaches using
community d i s t r i b u t i o n mechanisms and l o c a l p r o d u c t i o n as much as p o s s i b l e
must be developed and tested.
p o s i t i v e Deviance Studies
Mechanisms which enable some households i n impoverished environments t o
b r i n g up h e a l t h y w e l l nourished c h i l d r e n have been r e f e r r e d t o under t h e name
" p o s i t i v e deviance."
The p o s i t i v e d e v i a n t i s t h e young c h i l d who d e v i a t e s
f a v o r a b l y from expected norms of poor growth and ill health.
Most previous
n u t r i t i o n research i n developing c o u n t r i e s has focused on t h e problems o f
m a l n u t r i t i o n from a c u r a t i v e p e r s p e c t i v e and has n o t s t u d i e d t h e w e l l
nourished.
The few s t u d i e s comparing w e l l nourished and malnourished c h i l d r e n p o i n t
t o t h r e e types o f v a r i a b l e s associated w i t h good growth under c o n d i t i o n s o f
socioeconomic underdevelopment and poverty:
o
Psycho-social and behavioral
interaction, t h e i r individual
network s u p p o r t i n g t h e dyad;
aspects o f t h e mother-child
temperaments, and t h e s o c i a l
o
Known sociodemographic c o r r e l a t e s o f m a l n u t r i t i o n , such as
mother's education, f a m i l y s i z e and b i r t h spacing, u t i l i z a t i o n
o f modern h e a l t h services, and o t h e r f a c t o r s associated w i t h
growth s t a t u s i n low income environments;
o
P h y s i o l o g i c a l determinants o f growth, i n c l u d i n g maternal h e i g h t
and weight, m o r b i d i t y , d i e t a r y i n t a k e of n u t r i e n t s , and so
forth.
The main purpose o f s t u d y i n g p o s i t i v e deviance i s t o l e a r n from adaptive
c h i l d c a r e and f e e d i n g behaviors and t h e s o c i a l networks t h a t support them and
t o develop programs t h a t t r a n s f e r these adaptive mechanisms a t low c o s t t o t h e
f a m i l i e s o f t h e malnourished.
F i n d i n g s Already Appl i c a b l e t o Program Design:
o
C h i l d b i r t h r o u t i n e s t h a t p e r m i t a neonatal "bonding" experience
i n which t h e i n f a n t i s p u t d i r e c t l y t o t h e mother's b r e a s t may
reduce t h e r i s k o f l a t e r n e g l e c t f u l o r harmful c h i l d c a r e
p r a c t i c e s f o r h i g h r i s k mothers whose b o r d e r l i n e p s y c h o l o g i c a l
readiness f o r motherhood predisposes them t o such harmful
behav- io r .
o
P r a c t i c e s o f a b r u p t l y sending o l d e r i n f a n t s and newly weaned
t o d d l e r s away from home t o lrive w i t h "grannies" o r i n o t h e r
f o s t e r i n g arrangements should be discouraged.
o
E a r l y childhood i n t e r v e n t i o n s t h a t teach mothers t o s t i m u l a t e
t h e i r i n f a n t ' s p s y c h o l o g i c a l development should a l s o have a
A nutrition/health
b e n e f i c i a l e f f e c t on growth s t a t u s .
component i n these programs should enhance t h i s e f f e c t .
.
o
Prenatal n u t r i t i o n programs t h a t increase b i r t h weight and
reduce p r e m a t u r i t y are favorable t o an i n f a n t ' s behavioral
competence .and increase i t s abi 1 i t y t o o b t a i n food and
psychological s t i m u l a t i o n from the mother.
o
Postnatal n u t r i t i o n programs a l s o enhance t h e i n f a n t ' s
behavioral c o n t r i b u t i o n t o a p o s i t i v e outcome by i n c r e a s i n g i t s
energy l e v e l and t h e s t r e n g t h of i t s food e l i c i t i n g behaviors.
o
E x i s t i n g program types, such as primary h e a l t h care, growth
m o n i t o r i n g , f a m i l y planning, female education, women's income
generating a c t i v i t i e s , and so f o r t h , support the psychosocial
c h a r a c t e r i s t i c s t h a t c h a r a c t e r i z e t h e mothers o f p o s i t i v e
deviant children.
o
N u t r i t i o n programs r e l y i n g on v o l u n t a r y v i l l a g e workers may be
most successful i f they e n l i s t p o s i t i v e d e v i a n t mothers t o
organize mothers' c l u b s and t o p r o v i d e outreach t o the e n t i r e
community, w i t h a focus on reaching t h e most e l u s i v e and
secluded.
o
Social l e g i s l a t i o n t h a t obligates fathers t o f i n a n c i a l l y
support t h e i r c h i l d r e n i s badly needed i n r a p i d l y modernizing
areas where customary l e g a l and moral o b l i g a t i o n s have broken
down.
o
Where churches, o t h e r r e l i g i o u s groups, o r o t h e r e x i s t i n g
community
organizations
are
strong
and a l t r u i s t i c
in
o r i e n t a t i o n , they should be encouraged t o reach o u t t o
u n e n r o l l e d community members.
BIRTH SPACING I N
DEVELOP1 NG COUNTRI E S
Prepared by
Margot L. Zimnennan
Danusia Szumowski
PIACT/PATH
Washington, D.C.
S t u d i e s i n I n d i a , T u r k e y , t h e P h i l i p p i n e s , and Lebanon have shown t h a t
i n f a n t m o r t a l i t y . r a t e s f o r b a b i e s b o r n w i t h i n one y e a r o f a s i b l i n g ' s
b i r t h a r e between two and f o u r t i m e s h i g h e r t h a n f o r b a b i e s b o r n a f t e r
A s i m i l a r s u r v e y o f 6,000 women i n
an i n t e r v a l o f t w o y e a r s o r more.
I n d i a has shown i n f a n t m o r t a l i t y r a t e s o f a p p r o x i m a t e l y 8 0 p e r 1,000
when t h e i n t e r v a l between b i r t h s was t h r e e t o f o u r y e a r s , b u t 200 p e r
1,000 when t h e i n t e r v a l between b i r t h s was l e s s t h a n one y e a r .
In
f a c t , f i n d i n g s from 4 1 d e v e l o p i n g c o u n t r i e s i n c l u d e d i n t h e W o r l d
F e r t i l i t y Survey program i n d i c a t e t h a t c h i l d r e n b o r n l e s s t h a n t w o
y e a r s a p a r t a r e much more l i k e l y t o d i e i n i n f a n c y o r e a r l y c h i l d h o o d
t h a n t h o s e whose b i r t h s a r e spaced t w o y e a r s o r more a p a r t . C u r r e n t l y ,
some t e n m i l l i o n i n f a n t s d i e each y e a r i n t h e T h i r d World.
It i s
e s t i m a t e d t h a t a major expansion o f f a m i l y p l a n n i n g s e r v i c e s l e a d i n g t o
l e n g t h e n i n g t h e b i r t h i n t e r v a l c o u l d c u t t h e s e d e a t h s by h a l f o r more.1
S t u d i e s i n b o t h i n d u s t r i a l i z e d and devel o p i n g c o u n t r i e s , however, h a v e
a l s o shown t h a t " t o o many" c a n be a l m o s t as dangerous as " t o o c l o s e . "
Research i n China, E l Sal vador, C h i l e , a n d G r e a t B r i t a i n , f o r example,
has shown t h a t t h e chances o f s u r v i v a l f o r t h e f i r s t and second c h i l d
a r e s l i g h t l y h i g h e r t h a n f o r t h e t h i r d c h i l d and very s i g n i f i c a n t l y
h i g h e r t h a n f o r t h e f o u r t h and f i f t h c h i l d i n a f a m i l y . I n f a n t m o r t a l i t y
- r a t e s i n E l S a l v a d o r a r e a p p r o x i m a t e l y 6 0 p e r 1,000 f o r f i r s t - b o r n
c h i 1 dren, and r i s e t o 160 p e r 1,000 among f i f t h and subsequent c h i l d r e n . 2
F i n a l l y , b i r t h s t o women who a r e y o u n g e r t h a n 20 o r o l d e r t h a n 35 a r e
a l s o known t o i n c r e a s e t h e r i s k s t o b o t h m o t h e r and c h i l d .
Studies i n
A l g e r i a , Mexico, and t h e U n i t e d S t a t e s have a l l c o n c l u d e d t h a t a c h i l d
b o r n t o a woman under t h e age o f 20 i s a p p r o x i m a t e l y t w i c e a s l i k e l y t o
d i e i n i n f a n c y as a c h i l d b o r n t o a woman i n h e r mid-20s.
After the
age o f 30, t h e l e v e l o f r i s k a g a i n begins t o r i s e .
These r i s k s t o l i f e and h e a l t h , summarized by " t o o c l o s e , t o o many, t o o
01 d, o r t o o young,"
hold t r u e f o r a l l
income groups,
thou$
i n each
c a s e t h e i n c r e a s e i n r i s k i s e x a c e r b a t e d by p o v e r t y .
Worldwide, a t
l e a s t h a l f of t h e women who a r e now a t r i s k o f a n unwanted pregnancy
a r e n o t u s i n g any e f f e c t i v e method o f f a m i l y p l a n n i n g .
Increasing
women's c o n t r o l o v e r t h e i r own f e r t i l i t y , t h e r e f o r e , c o u l d c l e a r l y h a v e
a r e v o l u t i o n a r y i m p a c t on t h e h e a l t h o f m o t h e r s as we1 1 as t h e g r o w t h
and s u r v i v a l o f t h e i r c h i l d r e n .
I n p r a c t i c e , however, many women h a v e
n e i t h e r t h e means n o r t h e freedom t o e x e r c i s e t h a t p r e f e r e n c e .
B.
METHODS
Recent c o n t r a c e p t i v e prevalence surveys i n a v a r i e t y o f c o u n t r i e s
d e m o n s t r a t e a heavy r e l i a n c e by most o f t h e w o r l d ' s p o p u l a t i o n on a
v e r y s m a l l number o f c o n t r a c e p t i v e methods.
Worldwide o u t o f n e a r l y
8 0 0 m i l l i o n m a r r i e d c o u p l e s o f r e p r o d u c t i v e age a b o u t 325 m i l l i o n , o r
o n l y 4 1 p e r c e n t , a r e t h o u g h t t o u s e an e f f e c t i v e , modern f o r m o f c o n t r a c e p t i o n . Of t h e s e , a b o u t 136 m i l l i o n r e l y on v o l u n t a r y male o r f e m a l e
s t e r i l i z a t i o n ; 70 m i l l i o n u s e t h e IUD ( 5 1 m i l l i o n i n C h i n a a l o n e ) ; 55
m i l l i o n u s e o r a l c o n t r a c e p t i v e s ; and 37 m i l l i o n u s e condoms.
Use o f
a l l o t h e r e f f e c t i v e modern methods ( s u c h as i n j e c t a b l e s and o t h e r
b a r r i e r - m e t h o d s ) may t o t a l a n o t h e r 30 m i l l i o n . An a d d i t i o n a l 20 t o 40
m i l l i o n c o u p l e s may u s e methods such as p e r i o d i c abstinence, w i t h d r a w a l ,
o r o t h e r t r a d i t i o n a l forms of b i r t h c o n t r o l . The l i m i t e d d a t a a v a i l a b l e
suggest t h a t each y e a r somewhere between 40 and 45 m i l l i o n womn undergo
i n d u c e d a b o r t i o n s , about h a l f of them i l l e g a l procedures. One e s t i m a t e
i s t h a t 20 m i 1 l i o n of t h e s e procedures f o l 1 ow c o n t r a c e p t i v e f a i l u r e - - a
s t r o n g i n d i c a t i o n of t h e inadequacies of b o t h c u r r e n t c o n t r a c e p t i v e
choices and c o u p l e s ' knowledge of h w t o p r o p e r l y use whatever method
t h e y s e l e c t .3
The e f f e c t i v e n e s s of c o n t r a c e p t i v e methods can be viewed i n two ways:
(1) t h e o r e t i c a l effectiveness,
which d e s c r i b e s t h e 1 o w s t observed
pregnancy ( o r f a i l u r e ) r a t e i n 100 users who s t a r t o u t t h e y e a r u s i n g a
g i v e n method and who use i t c o r r e c t l y and c o n s i s t e n t l y under o p t i m a l
c o n d i t i o n s ; and ( 2 ) t h e u s e - e f f e c t i v e n e s s r a t e , which d e s c r i b e s t h e
f a i l u r e r a t e i n 100 " t y p i c a l " o r a c t u a l u s e r s who s t a r t out t h e y e a r
u s i n g a g i v e n method.
The a c t u a l r a t e s gauge e f f e c t i v e n e s s f o r a
" t y p i c a l " group o f u s e r s , some a f whom may n o t be u s i n g t h e m t h o d c o r r Botn t y p e s o f pregnancy r a t e s a r e usual l y
e c t l y o r consistently.
r e p o r t e d f o r t h e f i r s t y e a r o f use. Longer-term u s e r s experience 1 ower
pregnancy r a t e s , p a r t l y because they have found an e f f e c t i v e method
t h a t is convenient f o r thern.4
- A1 1 o f t h e m a j o r c o n t r a c e p t i v e methods can be q u i t e e f f e c t i v e when used
p r o p e r l y , as judged by t h e l o w e s t observed pregnancy r a t e s r e p o r t e d i n
m a j o r s t u d i e s . A c t u a l o r " t y p i c a l " pregnancy r a t e s a r e low f o r volunt a r y s t e r i l i z a t i o n , o r a l c o n t r a c e p t i v e s , and IUDs. A c t u a l pregnancy
r a t e s a r e somewhat h i g h e r f o r condoms, diaphragms, spermi cides, and
p e r i o d i c abstinence.
The d i f f e r e n c e s between t h e 1 owest observed
pregnancy r a t e s and t h e a c t u a l pregnancy r a t e s f o r t h e s e methods i n d i c a t e t h a t t h e r e i s some d i f f i c u l t y i n u s i n g t h e method o r t h a t t h e
method i s i n a p p r o p r i a t e f o r c e r t a i n people.
I t i s p r e c i s e l y f o r t h e s e reasons t h a t t h e r o l e o f h e a l t h e d u c a t i o n and
Speci f i c a l l y , approe f f e c t i v e communication cannot be overestimated.
p r i a t e and e f f e c t i v e e d u c a t i o n a l s t r a t e g i e s and c o u n s e l i ng can he1 p
b r i d g e t h e gap between t h e l o w e s t observed pregnancy r a t e s and a c t u a l
r a t e s f o r any g i v e n p o p u l a t i o n .
For example, t h e p i 1 1 has t o be t a k e n
Likewise, i t i s
each d a y - - t h u s a new b e h a v i o r has t o be learned.
i m p o r t a n t t o t e a c h u s e r s t h a t condoms, diaphragms, and s p e r m i c i d e s r m s t
be used d u r i n g each a c t o f sexual i n t e r c o u r s e . Methods which r e q u i r e
p e r i o d i c a b s t i n e n c e need p a r t i c u l a r l y e f f e c t i v e c o u n s e l i n g and e d u c a t i o n
programs t o h e l p c o u p l e s i d e n t i f y when o v u l a t i o n has t a k e n p l a c e and t o
a v o i d i n t e r c o u r s e d u r i n g f e r t i l e days.
The e f f e c t i v e n e s s o f a c o n t r a c e p t i v e method a l s o depends on why i t i s
used. W i t h most methods, c o u p l e s who have a l l t h e c h i l d r e n t h e y want
and so i n t e n d t o p r e v e n t f u r t h e r b i r t h s e x p e r i e n c e f e w e r unplanned
pregnancies t h a n couples who want more c h i 1 d r e n eventual l y but i n t e n d
t o delay b i r t h s .
The d i f f e r e n c e p r o b a b l y occurs because couples who
want n o more c h i l d r e n a r e more m o t i v a t e d t o u s e c o n t r a c e p t i v e s c o r r e c t l y
and c o n s i s t e n t l y .
Lack o f ' p e r s o n a l m o t i v a t i o n i s n o t always t h e cause o f 1ow c o n t r a c e p t i v e
p r e v a l e n c e . Many o f t h e n o n u s e r s of c o n t r a c e p t i o n l i v e i n T h i r d W o r l d
c o u n t r i e s where c o n t r a c e p t i v e u s e r a t e s a r e u s u a l l y u n d e r 1 0 p e r c e n t o f
t h e r e p r o d u c t i v e - a g e p o p u l a t i o n (compared t o 65-75 p e r c e n t i n Western
c o u n t r i e s ) .5 A c c o r d i ng t o l o n g i t u d i rial s t u d i e s , a s i g n i f i c a n t p r o p o r t i o n
o f t h e s e c o u p l e s a r e h a v i n g more c h i l d r e n t h a n t h e y want.
Most f i n d
t h e i d e a o f p l a n n i n g d e s i r a b l e i n p r i n c i p l e.
U n f o r t u n a t e l y , many
e i t h e r l a c k r e a d y a c c e s s t o a f f o r d a b l e farni l y p l a n n i n g s e r v i c e s o r f a i l
t o f i n d a n a c c e p t a b l e method -among t h e c h o i c e s a v a i l a b l e . F o r example,
i n 29 low-income c o u n t r i e s i n A s i a and L a t i n America, h a l f o f t h e women
i n t e r v i e w e d f o r t h e W o r l d F e r t i l i t y Survey s a i d t h e y wanted no more
c h i l d r e n , b u t o n l y a b o u t a q u a r t e r o f them were u s i n g an e f f e c t i v e
c o n t r a c e p t ive method.
U n f o r t u n a t e l y , many c o n t r a c e p t i v e u s e r s i n t h e T h i r d W o r l d d i s c o n t i n u e
use r a t h e r q u i c k l y . Much o f t h i s d i s c o n t i n u a t i o n c o u l d be p r e v e n t e d by
s e n s i t i v e p r o v i s i o n o f fami l y p l a n n i n g s e r v i ces, a p p r o p r i a t e e d u c a t i o n a l
m a t e r i a l s , p r o p e r c o u n s e l i n g as t o t h e s u i t a b i l i t y o f v a r i ous methods,
and good g e n e r a l h e a l t h s e r v i c e s and f o l low-up.
W o r l d F e r t i l i t y S u r v e y d a t a show t h a t fami l y p l a n n i n g methods can b e
e f f e c t i v e l y used t o a v o i d pregnancy, and t h a t c o n t r a c e p t i v e u s e r s have
l o n g e r b i r t h i n t e r v a l s t h a n nonusers.
The d i f f e r e n c e s v a r y , dependi n g
- o n t h e l e n g t h o f b r e a s t f e e d i ng and o t h e r f a c t o r s , f r o m l e s s t h a n one
month i n Bangladesh a n d Turkey t o more t h a n t e n months i n Paraguay a n d
S y r i a . S i m i l a r l y , t h e Danfa Comprehensive R u r a l H e a l t h and F a m i l y
P l a n n i n g P r o j e c t i n Ghana f o u n d t h a t t h e mean b i r t h i n t e r v a l of c o n t r a c e p t i v e u s e r s was f i v e t o s i x months l o n g e r t h a n t h a t of nonusers.
W h i l e t h e p e r f e c t method of c o n t r a c e p t i o n has n o t y e t been d i s c o v e r e d ,
c o u p l e s t o d a y who w a n t t o space t h e i r c h i 1 d r e n can choose among numerous
r e v e r s i b l e methods.
Each has c e r t a i n a d v a n t a g e s and d i s a d v a n t a g e s ,
w h i c h must be c a r e f u l l y weighed based on i n f o r m a t i o n p r o v i d e d t o t h e new
o r p o t e n t i a l a c c e p t o r . I t s h o u l d be remembered t h a t w h i l e most methods
o f c o n t r a c e p t i o n have c e r t a i n r i s k s , m u l t i p l e c l o s e l y spaced b i r t h s
pose much g r e a t e r r i s k s t o t h e h e a l t h and l i f e o f t h e mother and h e r
c h i 1 dren.
1
.
O r a l Cont r a c e p t ives
M o r e t h a n 55 m i l l i o n women a r o u n d t h e w o r l d a r e u s i n g o r a l c o n t r a Their popularity i s r e l a t e d t o t h e i r high l e v e l s
c e p t i v e s (OCs).
o f e f f e c t i v e n e s s , o v e r a l l s a f e t y , and a c c e s s i b i l i t y t h r o u g h comnerc i a 1 and p u b l i c l y s u b s i d i z e d c h a n n e l s as w e l l as t h r o u * p r i v a t e
p h y s i c i a n s . Even i n c o u n t r i e s where laws o r i n a d e q u a t e p u b l i c
h e a l t h s e r v i c e s 1 i m i t c o n t r a c e p t i v e a v a i l a b i lit y , OCs a r e u s u a l l y
a v a i l a b l e i n pharmacies and o t h e r c o m n e r c i a l o u t l e t s t o women who
can a f f o r d them.
I n d e v e l o p e d c o u n t r i e s , where almost a1 1 u s e r s
buy t h e i r OCs, s a l e s dropped d u r i n g t h e m i d t o l a t e 1970s, b u t r o s e
a g a i n i n t h e 1980s. I n t h e T h i r d World, p u b l i c and p r i v a t e f a m i l y
p l a n n i n g programs s u p p l y a1 1 b u t a m a 1 1 p e r c e n t a g e o f u s e r s .
In
d e v e l o p i n g c o u n t r i e s , t h e U.S. Agency f o r I n t e r n a t i o n a l Devel opment
O t h e r donors
p r o v i d e s a p p r o x i m a t e l y 100 m i 1 l i o n c y c l e s annual l y .
and in t e r n a t i o n a l a g e n c i e s p r o v i d e a p p r o x i m a t e l y 20 m i l l i o n a d d i
t i o n a l c y c l e s each y e a r .
-
K n w l e d g e o f t h e b e n e f i t s o f p i 1 1 u s e has grown c o n s i d e r a b l y i n
r e c e n t years among t h o s e i n t h e medical community who a r e a b l e t o
keep a b r e a s t o f c u r r e n t research. ( B u t t h e s e h e a l t h b e n e f i t s s t i l l
need-to be w i d e l y communicated t o a1 1 l e v e l s o f t h e p o p u l a t i o n . )
I m p o r t a n t h e a l t h b e n e f i t s o f o r a l c o n t r a c e p t i v e s have been i d e n t i f i e d i n a d d i t i o n t o t h e p r e v e n t i o n of c l o s e l y spaced pregnancies.
A t t h e same time, i t has become c l e a r t h a t t h e r i s k s a s s o c i a t e d w i t h
o r a l c o n t r a c e p t i v e s a r e l a r g e l y c o n f i n e d t o women over age 35 and
e s p e c i a l l y t o women over. 35 who smoke. The r i s k f o r younger women
i s s l i g h t . Although more research i n t o t h e p o s s i b l e h e a l t h r i s k s
o f c o n t r a c e p t i v e s t e r o i d use s p e c i f i c t o women i n developing count r i e s would be valuable, research so f a r i n d i c a t e s t h a t t h e i r
o v e r a l l impact i s b e n e f i c i a l t o h e a l t h .
For example, t h e p i l l
causes decreased menstrual flow, a b e n e f i t t o women w i t h i r o n d e f i c i e n c y anemi a, a c o n d i t i o n p r e v a l e n t i n p o o r l y n o u r i s h e d popul at i o n s w i t h i n t e r n a l p a r a s i t e s , and m a l a r i a , as w e l l as among women
who have borne many c h i 1 dren.
W h i l e OCs a r e e x t e n s i v e l y used i n t h e 'Third World, c o n t i n u a t i o n and
There a r e numerous v a r i a b l e s t h a t
acceptance r a t e s va ry w i d e l y .
can adversely a f f e c t successful OC use, such as t h e l o g i s t i c s o f
r e s u p p l y and t h e l i k e l i h o o d t h a t p r o p e r p i l l use w i l l n o t be exp l a i n e d t o t h e user. Also, myths can p l a y a c e n t r a l r o l e i n d e t e r m i n i ng c o n t r a c e p t i v e e f f e c t i v e n e s s .
For example, some common m i sconceptions a r e t h a t p i 1 1s should o n l y be t a k e n i f sexual i n t e r c o u r s e i s expected o r t h a t i t does n o t m a t t e r i f p i l l s a r e t a k e n i n
t h e p r o p e r sequence.
I n a 28-day packet, where seven p i l l s a r e
Comnunications
placebos, i t can o b v i o u s l y make a b i g d i f f e r e n c e .
strategies t h a t provide c u l t u r a l l y appropriate information f o r
f ami l y p l a n n i ng acceptors, emphas i z i ng p r o p e r use and addressi ng
t h e f e a r s o f t h e c l i e n t , can g r e a t l y i n c r e a s e t h e c o n t i n u a t i o n
r a t e s and a c t u a l e f f e c t i v e n e s s o f a1 1 f a m i l y p l a n n i n g methods.
2.
IUDs
I n t r a u t e r i n e devices a r e used by an e s t i m a t e d 70 m i l l i o n women
worldwide. F o r t h e many women who can use them w i t h o u t d i f f i c u l t y ,
t h e y r e p r e s e n t a v e r y e f f e c t i v e , 1o n g - a c t i n g method of c o n t r a c e p t i o n
which r e q u i r e s l i t t l e a t t e n t i o n on t h e p a r t o f t h e user. Although
t h e l o w e s t observed pregnancy r a t e of most ILlDs i s n o t as g r e a t as
t h a t o f combined o r a l c o n t r a c e p t i v e s , s t u d i e s conducted i n c o u n t r i e s
w i t h low l e v e l s o f e d u c a t i o n general l y f i n d t h a t t h e u s e - e f f e c t i v e ness of t h e IUD i s much s u p e r i o r t o t h a t o f t h e p i 1 1. The usee f f e c t i v e n e s s o f t h e IUD can be g r e a t e r i n such circumstances
because t h e r e a r e fewer v a r i a b l e s a s s o c i a t e d w i t h successful use.
However, an e s t i m a t e d 10 t o 15 p e r c e n t o f IUD users d i s c o n t i n u e use
because of p a i n and i r r e g u l a r o r heavy b l e e d i n g .
Innovations i n
IUDs have sought t o improve c o n t r a c e p t i v e e f f e c t i v e n e s s as we1 1 as
c o n t r o l s i d e e f f e c t s such as these.
Copper-beari ng and p r o g e s t e r o n e - r e l e a s i ng IUDs have been among t h e s e i n n o v a t i o n s . However,
p r o p e r c o u n s e l i n g and c a r e f u l p a t i e n t s e l e c t i o n may a l s o have a b i g
impact on o v e r a l l u s e r acceptabi 1it y and c o n t i n u a t i o n rates. Studi e s have shown t h a t i f a woman has been c a r e f u l l y i n s t r u c t e d i n
what t o expect a f t e r t h e i n s e r t i o n , she i s l i k e l y t o be l e s s f r i g h t ened o r concerned s h o u l d any minor s i d e e f f e c t s occur and more
l i k e l y t o manage t h e s e complaints h e r s e l f .
I n a d d i t i o n , many of
t h e problems- a s s o c i a t e d w i t h c u r r e n t l y a v a i l a b l e IUDs can be e l i m i nated by s k i 1 l f u l i n s e r t i o n techniques and f o l l o w - u p by w e l l - t r a i n e d
health practitioners.
I n j e c t a b l es and Imp1 a n t s
An e s t i m a t e d two m i 1 l i o n women use t h e i n j e c t a b l e c o n t r a c e p t i v e
Depo-Provera (depot-medroxyprogesterone a c e t a t e , o r DMPA) whi ch i s
now approved f o r c o n t r a c e p t i v e use i n o v e r 80 c o u n t r i e s , and 200,000
u s e N o r i s t e r a t " ( n o r e t h i s t e r o n e enanthat e, o r NET-EN).
B o t h Mexico
and China manufacture t h e i r own i n j e c t a b l e s , and about 900,000
women use i n j e c t a b l e s i n those c o u n t r i e s .
In j e c t ables have a number o f i m p o r t a n t advantages o v e r o t h e r c o n t r a c e p t i v e s . They c o n t a i n p r o g e s t i n o n l y ( i n i t s e l f an advantage f o r
some groups of women, as many o f t h e s e r i o u s s i d e e f f e c t s a s s o c i a t e d
w i t h s t e r o i d a l c o n t r a c e p t ives a r e li nked t o e s t r o g e n ) . I n j e c t a b l e s
have a h i g h e r u s e - e f f e c t i v e n e s s t h a n OCs, which have t o be t a k e n
every day. Furthermore, f o r women 1 i v i ng a t a d i s t a n c e from c o n t r a c e p t i v e o u t l e t s o r f o r women i n overcrowded l i v i n g q u a r t e r s who
wish t o m a i n t a i n p r i v a c y r e g a r d i n g t h e i r c o n t r a c e p t i v e use, i n j e c t ables a r e t h e method o f choice, s i n c e they o f f e r l o n g - a c t i n g p r o t e c t i o n ( t y p i c a l l y , two t o t h r e e months) and r e q u i r e no a c t i o n on t h e
p a r t o f t h e user.
A new c o n t r a c e p t i v e method, NORPLANTQ i m p l a n t s , c o n s i s t s o f small
hormone-releasi ng capsules wh- :h,
when in s e r t e d under t h e s k i n,
p r e v e n t pregnancy f o r up t o i i v e years.
Unlike the injectable,
t h i s method i s r e v e r s i b l e a t any t i m e and i s one o f t h e most e f f e c t i v e methods a v a i l a b l e today.
The NORPLANT@ system i s c u r r e n t l y
b e i n g i n t r o d u c e d i n s e v e r a l devel oping c o u n t r i e s : Chi1 e, Dominican
R e p u b l i c , Ecuador, Egypt, Indonesia, Kenya, S r i Lanka, P h i l i p p i n e s ,
and Thailand, and i t i s expected t h a t t h e worldwide demand f o r
NORPLANT@ i m p l a n t s w i l l be s t r o n g . The method w i 11 be e s p e c i a l l y
v a l u a b l e i n devel oping c o u n t r i e s where use o f a l o n g - t e n c o n t r a c e p t i v e can overcome many o f t h e l o g i s t i c a l o b s t a c l e s t o t h e d e l i v Current i n t r o d u c t i o n s t r a t e g i e s
e r y o f fami l y p l a n n i ng s e r v i c e s .
f o r NORPLANT@ i m p l a n t s a r e emphasizing i n f o r m a t i o n a l and i n s t r u c t i o n a l m a t e r i a l s f o r p o t e n t i a l acceptors a s w e l l as f o r c l i n i c i a n s ,
f i e l d w o r k e r s , counselors, and d e c i s i o n makers.
4.
Vaginal C o n t r a c e p t i o n
New a t t e n t i o n i s a l s o f o c u s i n g on some o f t h e o l d e s t and more
t r a d i t i o n a l forms o f c o n t r a c e p t i o n - - f e m a l e vagi n a l methods such as
spenni cides, sponges, diaphragms, and c e r v i c a l caps.
Spenni cides,
e s p e c i a l l y foaming t a b l e t s , a r e i n c r e a s i n g l y a v a i l a b l e t h r o u g h o u t
t h e w o r l d and r e q u i r e no p r e s c r i p t i o n . A new c o n t r a c e p t i v e sponge,
Today@, approved by t h e U.S. Food and Drug A d m i n i s t r a t i o n i n 1983,
i s a l s o s o l d w i t h o u t a p r e s c r i p t i o n and has a t t r a c t e d widespread
a t t e n t i o n and in t e r e s t i n t h e U.S.
The manufacturer began m a r k e t i n g
i n t h e U.K. i n 1985. Mowever, t h e sponge i s r e l a t i v e l y e x p e n s i v e
and cannot be reused; hence i t w i 11 p r o b a b l y never become v e r y
p o p u l a r i n devel opi ng c o u n t r i e s ' n a t i o n a l fami l y p l a n n i n g programs.
There i s a g r e a t need t o educate people about t h e e f f e c t i v e n e s s o f
t h e two methods.
When used p r o p e r l y , a female b a r r i e r method
coupled w i t h a condom i s as e f f e c t i v e as t h e p i l l o r IUD i n p r e v e n t i n g an unwanted pregnancy, but a l l b a r r i e r methods c o n t i n u e t o have
some m a j o r disadvantages..
A c t u a l f a i l u r e r a t e s of between 10 and
20 p e r c e n t p e r y e a r a r e much h i g h e r t h a n t h o s e f o r s t e r o i d a l methods
o r IllDs, i n p a r t due t o t h e absence of good communication programs
t h a t emphasize t h e importance of c o r r e c t use.
A l t h o u g h b a r r i e r methods a r e g e n e r a l l y f r e e of m a j o r s i d e e f f e c t s ,
t h e i n c r e a s e d r i s k of pregnancy necessari l y a f f e c t s t h e r i s k - b e n e f i t
c a l c u l a t i o n s f o r women who must d e f i n i t e l y a v o i d pregnancy.
Moreo v e r , most b a r r i e r methods r e q u i r e t h e u s e r t o t a k e a c o n s c i o u s
a c t i o n t o a v o i d pregnancy b e f o r e each sexual a c t . F o r many coup1 es,
t h a t requirement i s e s t h e t i c a l ly unappeali ng o r d i f f i c u l t , e i t h e r
p h y s i c a l l y o r p s y c h o l o g i c a l l y , t o f o l low c o n s i s t e n t l y . 7
5.
Condoms
Condoms a r e a safe, e f f e c t i v e , r e v e r s i b l e method o f c h i l d spacing.
I n a d d i t i o n t o p r e v e n t i ng pregnancy, condoms p r o t e c t b o t h men and
women from sexual ly t r a n s m i t t e d d i seases.
They have no s i d e e f f e c t s , r e q u i r e no medical s u p e r v i s i o n and minimal i n t e r a c t i o n , and
can be purchased w i t h o u t a p r e s c r i p t i o n .
Yet condoms a r e underu t i 1 i z e d , b o t h i n d e v e l o p i n g c o u n t r i e s where f e r t i l i t y i s h i g h and
in developed c o u n t r i e s , especi a1 l y among younger couples a t g r e a t e s t
r i s k of sexual ly t r a n s m i t t e d disease.
Also, condom a r e l e s s
e f f e c t i v e i n many LDCs because men have n o t been i n s t r u c t e d i n
p r o p e r use. Condom a r e o f t e n n o t p r o v i d e d w i t h a p p r o p r i a t e packa g i ng , e x p l a i n i n g u s e and/or a package i n s e r t . I n c o r r e c t use g r e a t l y
i n c r e a s e s t h e r i s k of t e a r i n g . Another problem i s t h a t o f t e n condoms a r e reused f o r economic reasons and t h i s t o o i n c r e a s e s t h e
r i s k of t e a r i n g .
I n a d d i t i o n , improper o r l e n g t h y s t o r a g e of
condoms i n hot, humid c l i m a t e s can cause t h e r u b b e r t o d e t e r i o r a t e .
An e s t i m a t e d 37 m i l l i o n couples t h r o u g h o u t t h e w o r l d r e l y on condoms. Use i s h e a v i l y c o n c e n t r a t e d i n a few areas, however. Twot h i r d s of condom u s e r s a r e i n developed c o u n t r i e s .
Japan a l o n e
accounts f o r a p p r o x i m a t e l y 25 p e r c e n t o f t h e condom u s e r s i n t h e
world. China accounts f o r a n o t h e r 20 p e r c e n t .
Compared w i t h u s e
o f o t h e r methods, condom use i s low i n L a t i n America, t h e Caribbean,
A f r i c a , t h e M i d d l e East, and most o f Asia.
I n t h e p a s t , condoms
were o f t e n i g n o r e d by t h e medical c m u n i t y and frowned on by
s o c i e t y because t h e y were l i n k e d i n p e o p l e ' s minds w i t h p r o s t i t u t i o n
and venereal disease.
Today, perhaps due t o t h e i n c r e a s e i n sexu a l l y t r a n s m i t t e d d i s e a s e and t o t h e g r o w i n g AIDS scare, condoms
a r e r e c e i v i ng new a t t e n t i o n f r a n h e a l t h personnel and n a t i o n a l
f a m i l y p l a n n i n g programs.
Proper e d u c a t i o n and c o u n s e l i n g a r e
p l a y i n g a c e n t r a l r o l e i n changing p e o p l e ' s p e r c e p t i o n s of t h e
condom and t e a c h i n g them how t o use i t c o r r e c t l y .
Research in
A f r i c a n c o u n t r i e s i n c l u d i n g Botswana showed t h a t men wanted t o know
mor'e about condom use, as w e l l as s u i t a b l e c o n t r a c e p t i v e methods
f o r t h e i r spouses. The n a t i o n a l f a m i l y p l a n n i n g program i n B o t s w a n a
has r e c e n t l y prepared a t t r a c t i v e p i c t o r i a1 m a t e r i a l t o k e t t h e
need.
6.
N a t u r a l F a m i l y P l a n n i n g Methods
Two t o f o u r p e r c e n t of m a r r i e d couples w o r l d w i d e a r e e s t i m a t e d t o
Abstinence f r o m
be u s i n g some form of n a t u r a l f a m i l y p l a n n i n g .
sexual i n t e r c o u r s e d u r i n g t h e woman's f e r t i l e p e r i o d t o a v o i d
pregnancy, o f t e n r e f e r r e d t o as n a t u r a l f a m i l y p l a n n i n g (NFP) o r
p e r i o d i c abstinence, r e l i e s on such t e c h n i q u e s as: ( 1 ) t h e c a l e n d a r
( o r rhythm) method which u t i l i z e s a h i s t o r y o f t h e woman's m e n s t r u a l
c y c l e s t o c a l c u l a t e t h e f e r t i l e time; ( 2 ) t h e basal body t e m p e r a t u r e
(BBT) method which i s based on d e t e c t i n g a c y c l i c a l r i s e i n d a i l y
BBT t o i n d i c a t e t h e p r o b a b l e end of t h e f e r t i l e p e r i o d ; ( 3 ) t h e
c e r v i c a l mucus method (CMM o r B i l l i n g s method) which i n v o l ves d a i l y
o b s e r v a t i o n o f t h e amount and c o n s i s t e n c y o f a woman's c e r v i c a l
mucus t o i d e n t i f y t h e o n s e t o f t h e f e r t i l e t i m e ; and ( 4 ) t h e symptot h e n n a l method which i s a c o m b i n a t i o n of t h e CMM and BBT.
A v a i l a b l e e s t i m a t e s o f NFP prevalence r a t e s a r e very l w f o r L a t i n
America and Asia, and t h e r e a r e almost no p r e v a l e n c e d a t a f o r
Africa.
Some o f t h e h i g h e s t prevalence r a t e s a r e t h o u @ t t o be i n
t h e P h i l i p p i n e s , Sri Lanka, Peru, and M a u r i t i u s . However, s i g n i f i c a n t numbers o f women worldwide a r e u n a b l e t o use any of t h e c u r r e n t l y a v a i l a b l e t e c h n i q u e s r e l i a b l y because they have i r r e g u l a r
m e n s t r u a l c y c l e s o r no c l e a r l y d e t e c t a b l e p a t t e r n of change i n body
temperature, c e r v i c a l mucus, o r o t h e r i n d i c a t o r s . Although among
small groups o f d e d i c a t e d , e x p e r i e n c e d u s e r s , p e r i o d i c a b s t i n e n c e
has proved s u c c e s s f u l , i n widespread general u s e t h e methods show
f a i l u r e r a t e s o f 10 t o 30 p e r c e n t p e r y e a r .
The i m p o r t a n c e o f e f f e c t i v e c o u n s e l i ng and e d u c a t i o n f o r
i s e v i d e n t . T r a i n i n g a c o u p l e i n t h e u s e o f NFP should
i n c l u d e how t o d e t e c t t h e f e r t i l e days, b u t a l s o how t o
a b s t i n e n c e . With p r o p e r t r a i n i n g , t h e NFP methods can be
t o couples who cannot, o r w i l l n o t ( p e r h a p s f o r r e l i g i o u s
use o t h e r methods o f c h i l d spacing.
NFP u s e r s
not only
cope w i t h
important
reasons),
Breastfeeding
B i r t h i n t e r v a l s a r e l o n g e r , and f e r t i l i t y reduced, i n many populat i ons where women p r a c t i c e intens ive and l e n g t h y b r e a s t f e e d i ng.
I t i s p a r t l y f o r t h i s reason t h a t r e c e n t d e c l i n e s i n b r e a s t f e e d i ng
i n c i t i e s and some r u r a l areas o f many l e s s developed c o u n t r i e s
have caused concern among p o p u l a t i o n e x p e r t s .
Unless compensatory
i n c r e a s e s i n t h e use o f modern c o n t r a c e p t i v e s occur, women who
breastfeed f o r s h o r t e r periods w i l l experience s h o r t e r b i r t h i n t e r v a l s and h i g h e r f e r t i l i t y , w i t h p o t e n t i a l l y adverse consequences
f o r t h e i r own h e a l t h and t h a t o f t h e i r c h i l d r e n . 8
C.
FEWER DEATHS/FEWER BIRTHS
I t would seem p a r a d o x i c a l t h a t t h e r a t e of p o p u l a t i o n g r w t A h should
fa1 1 when t h e r a t e of c h i l d s u r v i v a l c o n t i nues t o improve d r a m t i c a l l y .
'The e x p l a n a t i o n of t h a t paradox, however, s h o u l d a l l a y t h e fears o f those
who b e l i e v e t h a t a c h i l d h e a l t h r e v o l u t i o n w i l l l e a d t o another populat i o n explosion. For, i n p r a c t i c e , r e d u c i n g t h e r a t e s o f i n f a n t m o r t a l i t y i s l i k e l y t o h e l p s t a b i l i z e w o r l d p o p u l a t i o n growth a t a l o w e r
l e v e l and a t an e a r l i e r time,
I n t h e case o f young T h i r d World women, t h e death o f a c h i l d d u r i n g t h e
f i r s t month of l i f e reduces t h e average i n t e r v a l between b i r t h s f r o m
A c h i l d d y i n g even i n t h e second
t h r e e y e a r s t o l e s s t h a n two years.
y e a r of l i f e reduces t h e average b i r t h i n t e r v a l by almost s i x months.
S i m i l a r l y , s t u d i e s i n t h e Gambia have s h w n t h a t i f a baby d i e s i n t h e
f i r s t month o f l i f e , t h e n t h e average t i m e b e f o r e t h e next b i r t h i s
o n l y 16 months; if a Gambian c h i l d s ~ ~ r v i v ef os r t h e f i r s t two years, on
t h e o t h e r hand, then t h e average gap between one b i r t h and t h e n e x t
i n c r e a s e s t o approximately t h r e e years.
I n Bangladesh, t h e average
i n t e r v a l between one b i r t h and t h e next i s a l s o increased by more t h a n
a y e a r i f t h e f i r s t c h i l d survives i t s infancy.
C h i l d s u r v i v a l tends t o reduce b i r t h r a t e s i n t h r e e separate ways.
- F i r s t , c h i l d s u r v i v a l usual l y means t h a t t h e mother c o n t i n u e s b r e a s t feedi ng. As discussed, prolonged and unsuppl emented b r e a s t f e e d i ng i s a
n a t u r a l c o n t r a c e p t i v e , which d e l a y s t h e r e t u r n o f o v u l a t i o n .
Second,
improved c h i l d s u r v i v a l means t h a t parents can more c o n f i d e n t l y g i v e
b i rt h t o o n l y t h e number o f c h i l d r e n they a c t u a l l y w a n t - r a t h e r t h a n
h a v i n g a d d i t i o n a l c h i l d r e n t o compensate f o r t h e f a c t t h a t one o r more o f
t h e i r c h i l d r e n m i g h t die.
Thus a decrease i n deaths would l i k e l y
i n c r e a s e t h e use o f e f f e c t i v e methods o f f ami l y p l a n n i ng--even among
couples w i t h t h e same number o f s u r v i v i ng c h i 1dren.
A t h i r d mechanism by which an i n c r e a s e i n s u r v i v a l may l e a d t o a decrease
i n b i r t h s i s b o t h more profound and perhaps more powerful.
Whether o r
n o t a husband and w i f e w i l l decide t o p l a n t h e number and spacing o f
t h e i r c h i l d r e n i s c l o s e l y r e l a t e d t o t h e i r personal sense o f c o n t r o l
over t h e i r own 1 i v e s and circumstances.
Ma1 n u t r i t i o n , il l i t e r a c y , ill
h e a l t h , and oppression can leave people w i t h so l i t t l e sense o f c o n t r o l
over t h e i r own l i v e s and circumstances t h a t t h e y a r e a l i e n a t e d from t h e
I f p r o g r e s s i n h e a l t h and education, i n
very i d e a o f "planning."
p o l i t i c a l p a r t i c i p a t i o n , and economic a c t i v i t y has helped t o c r e a t e a
g r e a t e r sense o f mastery o v e r one's own d e s t i n y - t h e n t h e i d e a o f f a m i l y
s p a c i n g is l i k e l y t o be welcomed as another o p p o r t u n i t y t o t a k e more
c o n t r o l o v e r one's m n l i f e , t h e r e b y b e i n g a b l e t o a f f e c t and improve
o n e ' s own and one's c h i l d r e n ' s l i v e s .
Programs t o encourage b i r t h spaci ng can work t o g e t h e r w i t h o t h e r c h i l d
s u r v i v a l a c t i v i t i e s , such as p r o g r a m o f immunization o r of o r a l r e h y d r a t i o n f o r d i a r r h e a l diseases.
When h e a l t h workers a r e t a l k i n g t o
m t h e r s about t h e b e n e f i t s o f immunization, o r a l r e h y d r a t i on, and
b r e a s t f e e d i ng, t h e y can e a s i l y d i s c u s s t h e b e n e f i t s o f good b i r t h
spaci ng. 8
D.
CONSTRAI NTS TO CHILD SPACI NG
O
"
O
C o u p k s cannot u s e r e l i a b l e methods of c o n t r a c e p t i o n u n l e s s t h e y
have access t o in f o r m a t i on and c o n t r a c e p t i v e s u p p l ies.
I n some s o c i e t i e s , c o u p l e s may choose n o t t o space b i r t h s f o r v a r i ous reasons, such as f e a r t h a t t h e i r e x i s t i n g c h i l d r e n w i l l d i e ,
r e 1 ig i ous be1 iefs, f e a r o f s i d e - e f f e c t s , and s t a t u s a s s o c i a t e d w i t h
large families.
Lack o f encouragement by program p l a n n e r s , d e c i s i o n makers,
medical c o m u n i t y .
and t h e
O
Low p r i o r i t y w i t h i n e x i s t i n g MCH programs i n many h e a l t h m i n i s t r i e s .
O
F a i l u r e t o reach men w i t h a c c u r a t e i n f o r m a t i o n on f a m i l y p l a n n i n g /
c h i 1 d s g a c i ng.
"
Myths t h a t becane p e o p l e ' s " r e a l i t y . "
"
Noncompliance and misuse o f t h e v a r i a r s methods o f f a m i l y p l a n n i n g .
D i s c o n t i n u a t i o n : I n some d e v e l o p i q g c o u n t r i e s , f o r e v e r y 100 women
who b e g i n u s i ng t h e p i 1 1 , 70-80 d i scont i nue b e f o r e t h e end of one
year.
I n each o f t h e above c o n s t r a i n t s , t h e key t o overcoming i t i s communic a t i o n o f one s o r t o r a n o t h e r and t h u s a n o t h e r f a c t o r i n c h i 1 d s u r v i v a l
becomes one o f d e v e l o p i n g a n a p p r o p r i a t e communication s t r a t e g y .
REFERENCES
. 7,
No. 9, September 1985, P. 3 .
1.
pop1 i n e , Vol
2.
S t a t e o f t h e w o r l d ' s C h i l d r e n , 1984, and P o p u l a t i o n R e p o r t s , No. 6,
1 / 2 7 , H/6, H/7, A/6, D/4.
3.
" I s s u e s i n C o n t r a c e p t i v e Development," P o p u l a t i o n , P o p u l a t i o n C r i s i s
Committee, May 1985, p. 2,
4.
S t a t e of t h e W o r l d ' s C h i l d r e n , 1984, P o p u l a t i o n Re o r t s , No. 6,
1/27, H/6, ,H/7, A/6, D/4, and H a t c h e r , R-racepti
ve
Techno1 ogy 1984-1985, Ir v i n g t o n P u b l i s h e r s , Inc., 5 5 1 F i f t h Avenue,
New York, NY, 1 0 0 1 i .
5.
World Development R e p o r t 1984,
P r e s s , New York, NY, p. 196.
6.
" I s s u e s i n C o n t r a c e p t i v e Development,"
p. 2.
7.
" I s s u e s i n C o n t r a c e p t i v e Development,"
pp. 8-10.
8.
Habicht, J.P.
-
ing."
.
The W o r l d Bank,
Oxford U n i v e r s i t y
e t a1 , "The C o n t r a c e p t i v e R o l e o f B r e a s t f e e d -
P o p u l a t i o n S t u d i e s , 39 (1985), pp. 213-232.

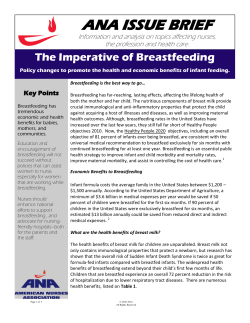








© Copyright 2026