
Treatment for acute myelocytic leukemia with allogeneic bone marrow
From www.bloodjournal.org by guest on October 21, 2014. For personal use only.
1991 78: 838-843
Treatment for acute myelocytic leukemia with allogeneic bone marrow
transplantation following preparation with BuCy2
EA Copelan, JC Biggs, JM Thompson, P Crilley, J Szer, JP Klein, N Kapoor, BR Avalos, I
Cunningham and K Atkinson
Updated information and services can be found at:
http://www.bloodjournal.org/content/78/3/838.full.html
Articles on similar topics can be found in the following Blood collections
Information about reproducing this article in parts or in its entirety may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests
Information about ordering reprints may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#reprints
Information about subscriptions and ASH membership may be found online at:
http://www.bloodjournal.org/site/subscriptions/index.xhtml
Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American
Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036.
Copyright 2011 by The American Society of Hematology; all rights reserved.
From www.bloodjournal.org by guest on October 21, 2014. For personal use only.
Treatment for Acute Myelocytic Leukemia With Allogeneic Bone Marrow
Transplantation Following Preparation With BuCy2
By Edward A. Copelan, James C. Biggs, James M. Thompson, Pamela Crilley, Jeff Szer, John P. Klein, Neena Kapoor,
Belinda R. Avalos, Isabel Cunningham, Kerry Atkinson, Kate Downs, Glenn S. Harmon, Mary B. Daly, lsadore Brodsky,
Stephen I. Bulova, and Peter J. Tutschka
One hundred twenty-seven patients with acute myelocytic
leukemia (AML) were given busulfan 4 mg/kg on each of 4
days and cyclophosphamide 60 mg/kg on each of 2 days
(BuCy2)followed by allogeneic bone marrow transplantation
from an HLA-identical or one antigen disparate sibling. For 71
patients in first complete remission, 23 in second complete
remission or initial relapse, and 33 patients with primary
refractory disease, second or subsequent relapse, or a preceding hematologic disorder, the 3-year leukemia-free survival
(LFS) is 63.1%. 32.6%. and 24.2% respectively. The actuarial
probability of relapse for each group is 14.1%, 40.6%. and
61.0%. In multivariate analyses, relapse and decreased LFS
were associated with advanced disease phase and with
M4/M5 French-American-British classification. The LFS of
first remission patients was adversely associated with a
short time interval from diagnosis to transplantation. This
study indicates that BuCyZ is an attractive preparative regimen for marrow transplantation in patients with AML and
that prognostic factors for relapse and LFS are similar to
those described for regimens containing total body irradiation.
o 1991 by The American Society of Hematology.
A
mgkg administered over 2 days (BuCy2) might be associated with a lower incidence of lethal treatment-related
complications? We present here results for 127 individuals
with AML who underwent allogeneic marrow transplantation at five transplantation centers after BuCy2.
LLOGENEJC BONE marrow transplantation (BMT)
following high-dose chemotherapy and total-body irradiation (TBI) cures many patients with acute myelocytic
leukemia (AML). Large single and multi-institutional studies demonstrate that long-term leukemia-free survival (LFS)
is achieved in 45% to 50% of individuals under 50 years of
age when transplantation is performed in first complete
remission, and in a lower percentage of patients who have
more advanced disease.’.’ Failure of marrow transplantation to achieve long-term survival occurs due to treatmentrelated mortality or leukemic relapse.
The combination of cyclophosphamide and TBI is the
standard preparative regimen for allogeneic marrow transplantation for AML; however, alternate conditioning
schemes with less severe toxicity and/or greater antileukemic effectiveness would be desirable. Santos et a14 initially
reported that a radiation-free regimen consisting of 16
mgkg of oral busulfan (Bu) and 200 mglkg of intravenous
cyclophosphamide (Cy) (over 4 days) resulted in an extremely low relapse rate, but was associated with a high
incidence of early transplant-related mortality. A pilot
study suggested that a reduction of the Cy dose to 120
From the Departments of Internal Medicine and Statistics, The
Ohio State University, Columbus; the Department of Haematology, St
Vincent’sHospital, Sydney, Australia; the Department of Hematology1
Oncology, Wirford Hall W A F Medical Center, San Antonio, TX; the
Department of Neoplastic Diseases, Hahnemann University, Philadelphia, PA; and the Bone Marrow Transplant Unit, Alfred Hospital,
Melboume, Australia.
Submitted January 7,1991; accepted March 26, 1991.
Supported by Public Health Service Grant 2 P30 CA, 16058-16Al
awarded by the National Cancer Institute, DHHS.
Presented in part at the 19th Annual Meeting of the International
Society of Experimental Hematology, Seattle, WA,August 26-30,1990.
Address reprint requests to Edward A . Copelan, MD, The Ohio
State University Hospitals, Division of Bone Marrow Transplantation,
303 East Doan Hall, 410 W 10th Ave, Columbus, OH 43210.
The publication costs of this article were defrayed in part by page
charge payment. This article must therefore be hereby marked
“advertisement” in accordance with I8 V.S.C.section 1734 solely to
indicate this fact.
0 1991 by The American Society of Hematology.
0006-4971191l7803-0022$3.00/0
838
MATERIALS AND METHODS
Patient characteristics. The study group consisted of 127 patients with AML aged 7 to 55 (median 30) who were treated from
March 1, 1984 through June 30, 1989 at five separate centers with
allogeneic bone marrow transplantation (BMT) following preparation with Bu and Cy. Fifty-five individuals underwent transplantation at The Ohio State University Hospitals (OSU; Columbus), 23
at Wilford Hall at Lackland Air Force Base (San Antonio, TX), 22
at Hahnemann University (Philadelphia, PA), 17 at St Vincent’s
Hospital (Sydney, Australia), and 10 at the Alfred Hospital
(Melbourne, Australia). This study was designed in 1984 as a single
institution (OSU) study and was modified in 1987 to include all
institutions known to be using this preparative regimen in all
patients with AML. All patients who underwent marrow transplantation for AML using this preparative regimen at the participating
institutions are reported. Informed consent was obtained for each
patient as required by the Institutional Review Boards of the
participating centers. According to the study design, patients were
categorized into three groups. Group I consisted of 71 patients with
de novo AML in first complete remission. Group I1 included 23
patients with de novo AML who underwent BMT during first
relapse or second remission. Group I11 included 33 patients who
had never achieved complete remission, were in second or subsequent relapse, or who had a history of chemotherapy, radiation
exposure, or a myelodysplastic syndrome preceding the development of AML. French-American-British (FAB) classifications
were made by referring physicians using standard morphologic
criteria with confirmation at the transplantation center. Remission
induction and consolidation regimens varied among institutions.
Among the 71 Group I patients, 18 required more than one
induction course to achieve complete remission and 25 received
one or more courses of consolidation. The clinical characteristics of
the patients in each group are described in Table 1. Preliminary
information for 45 of these 127 patients has been p~blished.’.~
Marrow donors. All donors were siblings of recipients and gave
informed consent before marrow procurement. One hundred
twenty-four donor-recipient pairs were HLA-A, -B, and -DR
identical as determined by standard serotyping. Their cells were
mutually nonreactive in mixed lymphocyte cultures. Three pairs
were mismatched at a single HLA-A, -B, or -DR site. The
Blood, Vol78, No 3 (August l), 1991:pp 838-843
From www.bloodjournal.org by guest on October 21, 2014. For personal use only.
839
BMT FOLLOWING BuCv2
Table 1. Clinical Characteristics of 127 Patients Undergoing Marrow
TransplantationAfter BuCy2
Group 1
Group2
Group3
Total
23
33
127
Total no. of patients
71
13/10 17/16 68/59
Malesfiemales
38/33
30
35
32
Median age, years
29
(13-50) (21-55) (7-48) (7-55)
(range)
Time from diagnosis to trans8.5
6.5
6
4.5
plantation: Median, months
(range)
11-15) (4-64) (.8-30) (.8-64)
FAB class
M1
8
0
2
10
8
3
31
M2
20
5
M3
16
1
22
M4
6
18
19
43
M5
4
2
7
1
M6
3
0
3
6
M7
FAB unclassified
0
0
2
3
1
2
1
7
nucleated cell dose ranged from 0.20 to 9.5 X 10’ (median
3.7 x 10’) cellskg recipient.
Preparation for transplant. All patients at three hospitals received intrathecal methotrexate ( I 12 mg per injection) before
initiating systemic therapy. At Wilford Hall only patients whose
leukemia was categorized as FAB subclass M4 or M5 routinely
received intrathecal methotrexate. Prophylactic intrathecal therapy was not administered at the Alfred Hospital (AH).A total dose
of 16 mgkg Bu was administered orally in four divided daily doses
over 4 days. Cy 60 mgkg was administered intravenously on each of
the next 2 days. Most patients received phenytoin during the period
of Bu administration to prevent seizures.’ Marrow was infused 48
hours after the second Cy dose.
Gruft-versus-hostdiseuse (GVHD). One hundred patients (61 in
group I, 16 in group 11, 23 in group 111) at three institutions
received cyclosporine plus methylprednisolone as prophylaxis for
GVHD as previously described’ or according to a slightly modified
version. Eighteen individuals (10 in group I, 3 in group 11, 5 in
group 111) at two institutions received methotrexate and cyclosporine as described by Storb et a19 or with a reduced methotrexate
dose. Five individuals (one in group 11, four in group 111) received
methotrexate, cyclosporine, and methylprednisolone. Four patients (three in group 11, one in group 111) received either
single-agent prophylaxis or marrow depleted of T lymphocytes with
Campath I antibody. Clinical acute GVHD was graded according
to the criteria of Glucksberg et al.” Chronic GVHD was diagnosed
according to the criteria of Shulman et al.”
Statistical methods. Analysis was performed on all data collected as of October 1, 1990. The time on study was defined to be
the shortest of the times from transplantation to relapse, death, or
date of most recent follow-up. For LFS the event of interest was
death or relapse. For estimation of relapse rates those patients who
died before relapse were treated as censored, Estimates of the LFS
and relapse rates were obtained using the Kaplan-Meier estimator.”
To estimate the effects of the various potential risk factors a Cox
regression analysis” was performed. Fixed time effects used in this
multivariate analysis were sex; age ( < 3 0 or 230); acute GVHD
grade 2 2 (yes or no); treatment regimen (methotrexate + cyclosporine, yes or no; methylprednisolone cyclosporine, yes or no);
transplant hospital (four indicator variables); FAB subclass (M4 or
M5, yes or no); interval from diagnosis to transplantation; group by
clinical phase; and number of days that the patient received
intravenous (IV) antibiotics. Two time-dependent covariates were
+
used. These included an indicator for prolonged neutrophil recovery (coded as 1 if at time t the patient had a granulocyte level 2
0.5 x 109/L,and 0 otherwise) and time to platelet recovery (coded 1
if at time t the platelet count was 240 X lo9& 0 otherwise). Tests
for covariate effects were analyzed using the fitted multivariate
model using Wald statistics.
Comparisons of the incidence of acute and/or chronic GVHD
between participating hospitals, clinical stages, and prophylactic
regimens were made using Fisher’s exact test. Comparison of other
continuous variables were made using the Wilcoxon test.
RESULTS
Engraftment. Marrow engraftment occurred in 124 of
the 127 patients. Two patients who underwent marrow
transplantation for leukemia that was refractory to chemotherapy failed to engraft. Residual leukemia cells were
subsequently detected in both. One patient died 2 days
after transplantation without evidence of engraftment. The
granulocyte count decreased to below 0.5 X 109/L at a
median of 4 days (range 0 to 7 days) after transplantation
with neutropenia lasting a median of 10 days (range 4 to 23
days). The median time of recovery to granulocyte levels 2
0.5 x 109/Lfor 2 consecutive days was 14 days (range 9 to 28
days) after transplantation. Thirty-three patients (26%) did
not develop a fever or receive IV antibiotics during their
neutropenic period. The median time to reach a platelet
count 2 4 0 x 109/L for 2 consecutive days was 17 days
(range 7 to 108 days). Patients receiving methylprednisolone and cyclosporine as GVHD prophylaxis experienced
a more rapid return of the granulocytes to 20.5 x 109/L
(P = .Owl),a shorter duration of neutropenia (P = .OOOl),
and a more rapid rate of return of platelets to 2 40 x 109/L
(P = .008) than did patients receiving methotrexate and
cyclosporine. The median duration of neutropenia was 9
days (range 4 to 21 days) and 13 days (range 8 to 23 days),
respectively, in these groups. During the period of marrow
aplasia, patients received a median of 4 U of red blood cells
(RBCs) (range 0 to 21 units) and five transfusions (range 0
to 30 transfusions) of single-donor or random-donor platelets. Patients were discharged from the hospital a median of
23 days (range 16 to 79 days) after transplantation. No
significant difference in transfusion requirements or time to
discharge was detected between the groups analyzed according to GVHD prophylactic regimen.
Nonmortal transplant-related complications. Two patients, neither of whom received phenytoin prophylaxis,
developed seizures during Bu administration. Moderate
oral mucositis was common; severe mucositis requiring
preventative intubation or resulting in aspiration pneumonia did not occur. Symptomatic hemorrhagic cystitis developed in 27 patients (21%), none of whom required surgical
intervention.
G W D . The Kaplan-Meier prediction of the incidence
of grade 2 2 acute GVHD was 16.5% (95% confidence
interval [CI], 9.7% to 23.3%). The estimated incidence of
chronic GVHD at 3 years was 48.8% (95% CI, 38.4% to
59.2%). The incidence of chronic GVHD was significantly
different among the groups analyzed according to the
clinical grouping at transplantation (P = .04). Patients in
group I11 (72.6%; 95% CI, 50.6% to 94.6%) had a higher
From www.bloodjournal.org by guest on October 21, 2014. For personal use only.
COPELAN ET AL
840
actuarial incidence of chronic GVHD than did patients in
group I (42.9%; 95% CI, 30.3% to 55.5%) or group I1
(43.8%; 95% CI, 16.4% to 71.2%). The incidence of acute
GVHD was not significantly different among these groups,
nor was the incidence of acute or chronic GVHD significantly different among patients analyzed according to
GVHD prophylactic regimen (P > .2).
Mortal transplant-related complications. As shown in
Table 2 , 6 2 patients, 28 with relapsed leukemia, have died.
One patient, transplanted for AML complicating treatment
for Hodgkin’s disease, died from recurrent Hodgkm’s.
Thirty-three of the 127 patients (26%) died of treatmentrelated complications, 14 (11%) within 100 days of transplantation. Sixteen of 71 (23%) first-remission patients died of
treatment-related causes, seven (10%) within 100 days of
transplantation. Six patients (5%) died directly as a result
of extramedullary organ toxicity due to the preparative
regimen. Hepatic veno-occlusive disease (VOD) contributed to the death of 5 (4% of total group) of 18 patients in
whom it was identified. One patient developed left ventricular necrosis and died 2 days after BMT. Lethal interstitial
pneumonia (IP) developed in 10 patients (8%), eight of
whom had cytomegalovirus and two adenovirus infections.
The actuarial incidence of lethal IP was 10% (95% CI; 4%
to 16%). Acute GVHD in six patients and chronic GVHD
in seven patients were identified as important contributors
to the deaths of those individuals.
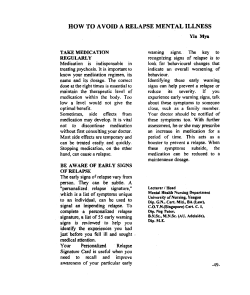
Relapse. Thirty-one patients have relapsed, all within 25
months of transplantation. Only three of these patients
survive. The estimated relapse rate for group I was 14.1%
(95% CI; 6.1% to 22.1%), for group I1 40.6% (95% CI,
13.6% to 67.6%), and for group I11 61.0% (95% CI, 41.8%
to 80.2%) (Fig 1). The most significant prognostic factors
for relapse were clinical group (P = .0001) and M4/M5
FAB classification (P = .003). Twenty-one of the 50 patients classified as FAB M4 or M5 relapsed (estimated
relapse rate 49.7%, 95% CI; 33.7% to 65.7%) compared
with 8 of 70 patients classified as FAB M1, M2, M3, M6, or
M7 (14.8%, 95% CI, 5.0% to 24.6%). The risk of relapse for
patients classified as M4 or M5 was 4.73 times that for
patients in other FAB groups.
Elevated white blood cell (WBC) count (P = .002) and
peripheral blast count (P = .005) at diagnosis were associated with relapse; however, they also were significantly
correlated with FAB subtype. The median initial WBC
count was 57 x 109/Lin 45 patients with FAB subtypes M4
or M5 and 19 x 109/L among 62 patients with other FAB
subtypes. The combination of FAB subtypes M4 and M5
correlated more closely with relapse than did WBC count
or peripheral blast count in a multivariate analysis. No
significant decrease in the risk of relapse was detected for
patients who developed acute GVHD, chronic GVHD, or
both (P > .2). Among first-remission patients the small
number of relapses did not permit reasonable analysis of
differences on the basis of FAB classification, interval from
diagnosis to transplantation, number of chemotherapy
courses required for remission induction, or administration
of consolidation therapy.
LFS. Sixty-two patients survive free of leukemia at a
median of 36 months (range 17 to 78 months) of follow-up.
The projected 3-year LFS for the entire group is 47.4%
(95% CI, 38.2% to 56.6%). Grouping based on phase of
disease was predictive of LFS (P = .007). An LFS of 63.1%
(95% CI, 51.1% to 75.1%) is estimated for the 71 patients
transplanted while in first complete remission, 32.6% (95%
CI, 12.2% to 53.0%) for 23 patients in first relapse or
second remission, and 24.2% (95% CI, 9.2% to 39.2%) for
the 33 patients with refractory/advanced disease or myelodysplastic syndromes preceding AML (Fig 2). In group 11,4
of 11 patients in second remission and 4 of 12 patients in
first relapse at the time of marrow transplantation are
leukemia-free survivors. Among patients in group 111, one
of nine with primary refractory disease and 4 of 16 who
were in second or subsequent relapse are leukemia-free
survivors. Two of four patients with secondary AML and
one of four with AML following a myelodysplastic syndrome who underwent marrow transplantation without
prior chemotherapy (four patients, two alive), while in first
complete remission (three patients, one alive) or with
refractory disease (one patient, none alive) are leukemiafree survivors.
Within group I, a short time interval between diagnosis
and transplantation predicted poor LFS (P = .04). Time
interval was not associated with M4/M5 classification.
Patients who received one or more courses of consolidation
had longer time intervals from diagnosis to transplantation
than those who did not receive consolidation (P = .01).
However, a long time interval was associated more strongly
with LFS than was the administration of consolidation
therapy (P = .1). Neither number of induction courses,
patient age, development of grade 2 I1 acute or chronic
GVHD, GVHD prophylactic regimen, prolonged neutrophil recovery, nor the hospital where transplantation was
performed were found to be statistically significant risk
factors for prediction of LFS (P > .2). FAB subclasses M4
and M5 were associated with poorer LFS (P = .07). Delayed platelet recovery after transplantation predicted for
poor LFS. (Relative risk for a patient with a platelet count
<40 x 109/Lv a patient with a count of 2 4 0 X 109/L at a
given time was 4.32 [P = .OW31 for the entire group, and
18.65 [P = .0001] for group I.)
Table 2. Causes of Death
No. of
Patients
Group I
Group II
GroupIII
Total
71
23
33
127
IP
Relapse
Infection
(bacterial
or fungal)
6 (8%)
2 (9%)
2 (6%)
l0(8%)
6 (8%)
6 (26%)
16 (48%)
28(22%)
5 (7%)
6 (26%)
5(15%)
l6(13%)
DISCUSSION
Other
5 (7%)
1 (4%)
2 (6%)
8(6%)
The present multi-institutional study permits analysis of
a large number of patients treated for AML with allogeneic
BMT after a radiation-free conditioning regimen of 16
mgkg Bu and 120 mgkg Cy. BuCy2 is sufficiently immunosuppressive to permit permanent engraftment for related
histocompatible donors. The total neutropenic period is
From www.bloodjournal.org by guest on October 21, 2014. For personal use only.
BMT FOLLOWING BuCv2
841
0.0-
+
{o..;
b
:
62 :
+
0.4-
i ;
Fig 1. Actuarial probability of relapse among patients transplanted for AML in first remission (bottom curve), second remission or first relapse (middle
curve), or with more advanced disease or history of a
preceding hematologic disorder (top curve). Tick
marks depict the duration of survival of patients who
did not relapse.
,
o.2:
‘
0
6
brief, in part due to the absence of methotrexate from the
GVHD prophylactic regimen of the majority of study
patients, and also due to the slow decrease in the neutrophil
count following this preparative regimen.14 A substantial
percentage (26%) of individuals did not develop fever
during the neutropenic period. The relatively large proportion of individuals who did not develop fever may be related
to the short duration of neutropenia. Additionally, less
severe injury to the mucosa of the gastrointestinal tract may
be caused by BuCy2 than by TBI-containing regimens.I4
These factors are likely to have contributed to the early
hospital discharge described in this study because discharge
is generally limited by cytopenias, infection, or inability to
eat adequately.
Six patients (5%), five with VOD and one with left
ventricular necrosis, died as a direct result of organ toxicity
attributable to the preparative regimen. Ten patients (8%)
died from IP. Twenty-six percent of the present study group
died of treatment-related complications, 11% within 100
$2
L6
24
30
36
42
48
54
€4
66
72
78
84
MONTH
days of transplantation. Twenty-one percent developed
symptomatic hemorrhagic cystitis. A higher frequency of
this complication after this preparative regimen than with
Cy/TBI has been previously r e p ~ r t e d .A
’ ~high incidence of
chronic GVHD occurred in this study; however, the influence of the preparative regimen is unclear. The vast
majority of patients received corticosteroids for GVHD
prophylaxis. A significantly higher rate of chronic GVHD in
patients who received prednisone for prevention of acute
GVHD was recently demonstrated by Storb et al,” who
suggested that corticosteroids might interfere with induction of tolerance after transplantation.
The association of subclasses M4 and M5 with relapse
after marrow transplantation has been reported following
preparation with CyRBI.l63”Because of the limited number
of patients, we were unable to define the factors responsible
for the poorer survival of patients who underwent transplantation at shorter intervals after diagnosis. However, as
patients survive in remission for increasing intervals follow-
”jk
0.8f
‘ti“----------
: I
P
! j
4
.
0.4-
1 ;
0.2-
Fig 2. Actuarial probability of LFS among patients
transplanted for AML in first remission (top curve),
second remission or first relapse (middle curve), or
with more advanced disease or history of a preceding
From www.bloodjournal.org by guest on October 21, 2014. For personal use only.
842
COPELAN ET AL
ing treatment, they are less likely to relapse with or without
marrow transplantation. These results emphasize the importance of time-dependent censoring of patients undergoing
marrow transplantation when comparisons with chemotherapy results are p e r f ~ r m e d . ~
Because of its limited follow-up, this investigation cannot
adequately address the important issue of late complications of transplantation. Preclinical and clinical studies
have suggested that radiation-free regimens are associated
with a lower frequency of these complications’’m; however,
this has not been adequately studied.
The development of sensitive, specific assays for Bu has
shown that patterns of absorption and elimination vary
widely between patients and are associated with the development of VOD” and perhaps other transplant-related
complication^.^^^^^ Thus, dose adjustment based on plasma
Bu levels might reduce the risk of transplant-related death.
Increased drug exposure in patients with low Bu plasma
levels might result in better antileukemic effectiveness.
Ongoing studies of dose adjustment based on Bu levels may
imprave the results of marrow transplantation using BuCy.
Other modifications of the BuCy2 preparative regimen
under investigation include the addition of etoposidex or
cytarabine%in individuals at high risk of relapse.
This report demonstrates that BuCy2 is an effective
preparative regimen for marrow transplantation in AML.
The relatively low incidence of transplant-related deaths
reported is noteworthy in view of the median age (30) of the
participants in this trial and the previously reported adverse
effect of age on transplant-related death and LFS.IJ At the
same time the relatively high proportion of group I patients
with FAB M3 morphology and the exclusion of individuals
with secondary leukemia or preceding myelodysplasia from
group I are two differences with other studies that might
contribute to the favorable results obtained.
If BuCy2 is proven to be at least as safe and effective as
Cy/TBI, the ease of administration of Bu compared with
TBI would favor its use. The present study suggests that
comparatively brief durations of neutropenia and hospitalization may be additional advantages of BuCy2. However, it
is impossible to adequately compare the results achieved in
this study group with that of the other series of patients who
have undergone transplantation for AML. Prospective
randomized studies are necessary to compare the toxicities
and effectiveness of BuCy2 to Cy/TBI. Such a study has
been initiated in AML by the European Group for Bone
Marrow Transplantation.26Future treatment strategies include the addition of other agents to BuCy in patients at
high risk for relapse and dose adjustment of Bu based on
plasma levels in individual patients. The development of
better preparative regimens is crucial to improving the
results of allogeneic marrow transplantation in AML and
other disorders.
ACKNOWLEDGMENT
We thank the nursing staffs and housestaffs of the participating
transplant centers; all referring physicians; Judy Fisher, Brenda
Berstler, and Carolee Polek for their assistance in management of
data; S.T. Wang for statistical programming; and Diana Barker and
Judy French for preparing the manuscript. Computing resources
were supplied by The Instruction and Research Computer Center
of The Ohio State University.
REFERENCES
1. Clift RA, Buckner CD, Thomas ED, Kopecky KJ, Appelbaum FR, Tallman M, Storb R, Sanders J, Sullivan K, Banaji M,
Beatty PS, Bensinger W, Cheever M, Deeg J, Doney K, Fefer A,
Greenberg P, Hansen JA, Hackman R, Hill R, Martin P, Meyers J,
McGuffin R, Neiman P, Sale G, Shulman H, Singer J, Stewart P,
Weiden P, Witherspoon R: The treatment of acute non-lymphoblastic leukemia by allogeneic marrow transplantation. Bone Marrow
Transplant 2243,1987
2. Gratwohl A, Hermans J, Barrett AF, Ernest P, Frassoni F,
Gahrton G, Granena A, Kolb HJ, Marmont A, Prentice HG, Speck
B, Vernant JP, Zwaan FJ: Allogeneic bone marrow transplantation
for leukemia in Europe (report from the working party on
leukemia, European Group for Bone Marrow Transplantation).
Lancet 1:1379,1988
3. Gale RP, Horowitz MM, Biggs JC, Herzig RH, Kersey JH,
Marmont AM, Masaoka T, Runin AA, Speck B, Weiner RS,
Zwaan FE, Borton MM: Transplant or chemotherapy in AML.
Lancet 1:1119,1989
4. Santos GW, Tutschka PJ, Brookmeyer R, Sara1 R, Beschorner WE, Bias WB, Braine HG, Burns WH, Elfenbein GJ,
Kaizer H, Mellits D, Sensenbrenner LL, Stuart RK, Yeager AM:
Marrow transplantation for acute nonlymphocytic leukemia after
treatment with busulfan and cyclophosphamide. N Engl J Med
309:1347,1983
5. Tutschka PJ, Copelan EA, Klein JP: Bone marrow transplantation for leukemia following a new busulfan and cyclophosphamide regimen. Blood 70:1382,1987
6. Crilley P, Topolsky D, Bulova S, Bigler R, Brodsky I: Bone
marrow transplantation following busulfan and cyclophosphamide
for acute myelogenous leukemia. Bone Marrow Transplant 5:187,
1990
7. Sureda A, Perez de Oteyza J, Garcia LT, Odriozola J: High
dose busulfan and seizures (letter). Ann Intern Med 111543, 1989
8. Tutschka PJ, Copelan E A Prevention of severe GVHD
employing cyclosporine in HLA-matched transplant for leukemia,
in Baum SJ, Santos GW, Takaku F, (eds): Experimental Hematology Today, 1987. New York, NY,Springer-Verlag, 1987, p 145
9. Storb R, Deeg HJ, Whitehead J, Appelbaum F, Beatty P,
Bensinger W, Buckner CD, Clift R, Doney K, Farewell V, Hansen
J, Hill R, Lum L, Martin P, McGuffin R, Sanders J, Stewart R,
Sullivan K, Witherspoon R, Yee G, Thomas ED: Methotrexate and
cyclosporine compared with cyclosporine alone for prophylaxis of
acute graft versus host disease after marrow transplantation for
leukemia. N Engl J Med 314:729,1986
10. Glucksberg H, Storb R, Fefer A, Buckner CD, Neiman PE,
Clift RA, Lerner KG, Thomas ED: Clinical manifestations of
graft-versus-host disease in human recipients of marrow from
HLA-matched sibling donors. Transplantation 18:295,1974
11. Shulman HM, Sale GE, Lerner KG, Barker EA, Weiden PL,
Sullivan K, Gallucci B, Thomas ED, Storb R: Chronic cutaneous
graft-versus-host disease in man. Am J Pathol91:570,1978
12. Kaplan EL, Meier P: Nonparametric estimation from incomplete observations. J Am Stat Assoc 53:457,1958
13. Cox DR: Regression models and life tables. J R Stat SOC(B)
34:187,1972
14. Atkinson K, Biggs J, Noble G, Ashby M, Concannon A,
From www.bloodjournal.org by guest on October 21, 2014. For personal use only.
BMT FOLLOWING BuCv2
Dodds A Preparative regimes for marrow transplantation containing busulphan are associated with haemorrhagic cystitis and
hepatic veno-occlusive disease but a short duration of leukopenia
and little oro-pharyngeal mucositis. Bone Marrow Transplant
2:285,1987
15. Storb R, Pepe M, Anasetti C, Appelbaum FR, Beatty P,
Doney K, Martin P, Stewart P, Sullivan KM, Witherspoon R,
Bensinger W, Buckner CD, Clift R, Hansen J, Longton G,
Loughran T, Petersen FB, Singer J, Sanders J, Thomas ED: What
role for prednisone in prevention of acute graft-versus-host disease
in patients undergoing marrow transplants? Blood 761037,1990
16. Zwaan FE, Hermans J, Barrett AJ, Speck B: Bone marrow
transplantation for acute nonlymphoblastic leukemia: A survey of
the European group for bone marrow transplantation. Br J
Haematol56:645,1984
17. McGlave PB, Haake RJ, Bostrom BC, Brunning R, Hurd
DD, Kim TH, Nesbit ME, Vercellotti GM, Weisdorf D, Woods
WG, Ramsay NKC, Kersey JH: Allogeneic bone marrow transplantation for acute nonlymphocytic leukemia in first remission. Blood
72:1512,1988
18. Deeg HJ, Storb R, Prentice R, Fritz TE, Weiden PL, Sale
GE, Graham TC, Thomas ED: Increased cancer risk in canine
radiation chimeras. Blood 55:233,1980
19. Urban C, SchwingshandlJ, Slavc I, GamillschegA, Hauer C,
Schmid G, Yaulfersch W, Borkenstein M Endocrine function after
bone marrow transplantation without the use of preparative total
body irradiation. Bone Marrow Transplant 3:291,1988
20. Kanfer EJ, McCarthy DM: Cytoreductive preparation for
843
bone marrow transplantation in leukemia: To irradiate or not? Br J
of Haematol71:447,1989
21. Grochow LB, Jones RJ, Brundrett RB, Braine HG, Chen
T-L, Saral R, Santos GW, Colvin OM: Pharmacokinetics of
busulfan: Correlation with veno-occlusivedisease in patients undergoing bone marrow transplantation. Cancer Chemother Pharmacol
25:55,1989
22. Wingard JR, Mellits ED, Jones RJ, Beschorner WE, Sostrin
MB, Burns WH, Santos GW, Saral R: Association of hepatic
veno-occlusive disease with interstitial pneumonitis in bone marrow transplant recipients. Bone Marrow Transplant 4:685, 1989
23. Grochow LB, Krivit W, Whitley CB, Blazar B: Busulfan
disposition in children. Blood 75:1723,1990
24. Vaughan WP,Dennison D, Klassen L, Coccia P, Strandjord
S, Armitage J: Reducing the risk of relapse after allogeneic bone
marrow transplantation (BMT) for hematologic malignancyBuCyVP. J Cell Biochem 14A289,1990 (abstr)
25. Geller RB, Larson RA, Myers S, Williams SF, Hauck U,
Daly K Phase I study of busulfan, cyclophosphamide and escalating doses of continuous infusion cytosine arabinoside (Ara-C)
followed by bone marrow transplantation. Blood 76:541a, 1990
(abstr)
26. Blaise D, Reiffers J, Guyotat D, Harousseau JL, Ifrah N,
Michallet M, Bordigoni P, Vilmer E, Attal M, Jouet A, Maraninchi
D for the GEGMO: A randomized study of Cy-TBI vs BUS-Cy +
All0 BMT for ANL in first CR. J Cell Biochem 14A282, 1990
(abstr)











© Copyright 2026