
Document 357231
European Heart Journal (1997) 18 {Supplement E), E14-E18
From kinetics to dynamics: are there differences
between ACE inhibitors?
J. L. Reid
Gardiner Institute, Department of Medicine and Therapeutics, University of Glasgow, Glasgow, Scotland
Angiotensin converting enzyme inhibitors are established
treatment for hypertension and heart failure. There are
well documented differences between ACE inhibitors
both in physicochemical properties and pharmacokinetics.
Pharmacodynamic actions are similar for most members
of the ACE inhibitor class but there are compounds with
additional effects which may reflect protease inhibition or
non-enzyme-directed pharmacological properties.
Clinically relevant differences are few and far between,
particularly in the treatment of hypertension when the
optimal dose and dose intervals are used. In heart failure
Angiotensin converting enzyme (ACE) inhibitors are
now established as effective anti-hypertensive drugs''1.
They also prolong life and delay progression of cardiac
failure'21. In treatment of hypertension for over 16 years
and heart failure for over 10 years, information has
accumulated not only on ACE inhibitors as a therapeutic class but also on a number of individual drugs.
Many more have been studied in pre-clinical and early
clinical research (up to 70 compounds) in addition to the
ten agents currently licensed for therapeutic use in the
U.K. and Europe'31. It is pertinent to ask whether there
are any differences between ACE inhibitors? In particular, differences which cannot be attributed to the underlying 'class' effect of inhibition on kininase II or the
angiotensin converting enzyme? As will be discussed
later, anti-hypertensive efficacy appears to be a 'class'
effect associated with ACE inhibition and accompanied
by characteristic endocrine changes. Experience of benefits on survival and progression of heart failure have
now been reported from several trials with several
agents'21. Can the effects of ACE inhibitors in heart
failure also be considered a 'class' effect? This review
addresses these issues by considering what pharmacokinetic or pharmacodynamic differences can be identified
Key Words: ACE inhibitors, pharmacokinetics, pharmacodynamics, hypertension, heart failure, hypotension.
between ACE inhibitors and explores whether any of
these differences might be clinically relevant to the
treatment of hypertension or heart failure.
Pharmacokinetic differences
Examination of differences between drugs of a class can
conveniently be divided between those differences
dependent on the pharmacokinetic properties (physicochemical characteristics, absorption, disposition, metabolism or elimination) and the pharmacodynamic
properties (Table 1). It is self-evident that different drug
molecules by definition will have different physicochemical properties which, in turn, will affect drug disposition.
Could any such differences be clinically relevant?
Amongst the well-characterized kinetic differences
between ACE inhibitors, several have been proposed to
be of potential or real clinical relevance.
The presence of a sulphydryl (SH group) in the
molecule differs between ACE inhibitors (Table 2).
Captopril and zofenopril possess this group. Others do
not. The SH group which has antioxidant or free radical
scavenging potential has been claimed to be potentially
beneficial in ischaemic states, atherosclerosis and other
circumstances where free radicals may accumulate'41.
However, there have been alternative claims that the SH
group may confer a specific profile of toxicity including
Correspondence: Dr J. L. Reid, Department of Medicine and taste51disturbance and, possibly, skin rash and proteinuria' . This is supported by the reported differences,
Therapeutics, Western Infirmary, Glasgow Gil 6NT, Scotland.
0195-668X/97/000014+05 S18.00/0
c. 1997 The European Society of Cardiology
Downloaded from by guest on October 21, 2014
Introduction
there may be a role for drugs with additional properties
such as neutral endopeptidase inhibition. In addition, ACE
inhibitors differ in the profile of blood pressure changes
after thefirstdose. Early haemodynamic changes with a fall
in blood pressure in heart failure patients may be disadvantageous in terms of subsequent outcome. Thus the haemodynamic effects of the first dose may be relevant to the
choice of ACE inhibitors in heart failure.
(Eur Heart J 1997; 18 (Suppl E): E14-E18)
Differences between ACE inhibitors
Table 1 Differences between A CE inhibitors
Pharmacokinetics
Chemical — SH group
Prodrug ester
Route of metabolism/elimination
Oral and tissue absorption and
penetration
Pharmacodynamics
Potency
Binding to ACE
Tissue accumulation
Other peptidase activity
Non-enzymatic actions
Table 2 Differences between A CE inhibitors
Drug
SH group
Prodrug ester
Captopril
Enalapril
Lisinopril
Perindopril
Quinapril
Cilazapnl
Ramipril
Benazapril
Zofenopril
Prodrug activation may be expected to be
impaired in patients with hepatic impairment. In practice, the kinetics of perindopril were not significantly
changed in patients with liver disease'10'. Even amongst
the prodrug ACE inhibitors there are differences in that
some prodrugs are weakly active and some not active at
all. The distribution and tissue penetration of prodrug
and active diacid will vary and there is evidence of
interactions between prodrug and diacid at the level of
ACE enzyme inhibitors. Prodrugs in some cases
appear to inhibit the effects of the active diacid'1''. Such
interactions could be important determinants of the
responses to ACE inhibitors, especially at early times
after the first dose when prodrug concentration may be
particularly high compared with the active metabolite.
Such drug specific interactions could contribute to the
profile of response to the first dose of ACE inhibitors'"'
(Fig. 1).
Other kinetic differences which are well characterized are the profile of drug elimination and whether
this is predominantly by renal excretion or after hepatic
metabolism and inactive metabolites'12'. ACE inhibitors
show a range of routes of elimination from those which
are largely dependent on renal excretion (captopril,
enalapril, perindopril) to those with a greater or lesser
hepatic component and include examples when both
pathways participate (Table 3). These differences may be
important considerations in choosing an individual drug
for an individual patient or group of patients. For
example, in treating patients with severe renal failure the
clinician can thus choose between using a drug not
eliminated by the kidney, where dose adjustment may
not be necessary, or a drug which depends on renal
excretion, where the dose may need to be reduced
depending on the degree of renal failure.
The pharmacokinetic properties of ACE inhibitors will determine plasma concentration profile which
in turn determines the duration of effect. The duration
of effect is of practical clinical importance as it will
influence the choice of optimal dose and dose frequency.
Pharmacokinetics of ACE inhibitors are unusual in that
the disposition cannot adequately be described by simple
one- or two-compartment kinetic models. It appears that
slow, tight binding to sites, including plasma and tissue
ACE contributes to the late elimination phase' 1314 '. The
consequence is that the duration of effect of some ACE
inhibitors is longer than would be anticipated from more
superficial kinetic overview. Another relevant feature of
most ACE inhibitors is the nature of the relationship
between plasma concentration and effect in the therapeutic dose range. Unlike most calcium antagonists and
a-blockers the relationship is not linear but of a nonlinear saturable E max nature'15'. For most ACE inhibitors the doses used in clinical practice are on the upper
linear plateau of the concentration effect curve. As
a consequence it is possible to prolong the apparent
drug effect by further increasing the dose. Whilst most
ACE inhibitors may be given once-daily (if the dose is
sufficiently high), the optimal regimen for some ACE
inhibitors may be twice-daily at a greatly reduced daily
dose"6'.
Pharmacodynamic differences
Competitive inhibition of angiotensin-converting enzyme
is the common pharmacological property of all ACE
inhibitors and results in a reduction or absence of
formation of angiotensin II. As ACE and kininase II,
which breaks down bradykinin, are identical, all ACE
inhibitors will potentiate kinin actions. In addition,
several other peptide hormones or modulators may be
Eur Heart J, Vol. 18, Suppl E 1997
Downloaded from by guest on October 21, 2014
particularly in taste disturbance, between captopril and
non-SH drugs and by the recognized side effect profile of
pencillamine, another SH-containing drug.
Another difference between ACE inhibitors is
whether this drug is active in its own right or requires
biotransformation (Table 2). Captopril16' and lisinopril'71, for example, are the active moieties while enalapril181 and perindopril'9' are examples of drugs given as
inactive (or relatively inactive) esters which depend on in
vivo metabolism by diesterification to generate the active
diacid. There are advantages on occasion in giving
prodrugs to improve absorption and bioavailability and
to provide an in vivo depot to prolong drug action.
However, prodrugs may result in a delay in onset of
action and may result in inter-individual differences
resulting from genetic polymorphism of drugmetabolizing enzymes and drug interactions. In the case
of ACE inhibitors, prodrugs may show a somewhat
(4-6 h) delayed peak effect on ACE inhibition and blood
pressure fall after oral dosing18'91 although this is unlikely
to be of clinical significance. The esterases affecting activations are ubiquitous and appear promiscuous with
regard to substrate so that problems of delayed, limited
or absent de-esterification have not been reported'8'.
El 5
E16
J. L. Reid
100
1000
Enalaprilat concentration (ng ml
Downloaded from by guest on October 21, 2014
0.01
1000
Perindoprilat concentration (ng ml
Figure 1 Effect of ester prodrug on in vitro inhibition of ACE activity.
(a) Enalapril effect on inhibition by enalaprilat:
, enalapril alone;
, with addition of 200 ng . ml ~' enalapril;
, with addition
of 500 ng . ml ~' enalapril;
, with addition of 2000 ng . ml ~'
enalapril. (b) Perindopril effect on inhibition by perindoprilat:
,
perindoprilat alone;
, with addition of 5 ng. ml ' perindopril;
, with addition of 10ng.ml~' perindopril;
, with
addition of 50 ng . ml" ' perindopril. (Reproduced with permission1"1.)
influenced if their formation or degradation involves a
neutral carboxypeptide. Such peptides include substance
P, enkephalins and luteinizing hormone releasing hormone. Individual ACE inhibitor molecules can have
additional properties which could be of therapeutic
relevance. Such properties may include non-enzymeinhibiting properties such as free radical scavenging
potential as discussed above for SH-containing
compounds'4'.
Other molecules have been identified and are in
clinical development which possess not only ACE inhibiting properties but also neutral endopeptidase inhibition'171. This latter effect will impair the breakdown of
natriuretic peptides and potentiate the vasodilating and
Eur Heart J, Vol. 18, Suppl E 1997
Table 3 Differences in metabolism and elimination of
ACE inhibitors
Drug
Liver
Captopril
Enalapril
Lisinopril
Perindopril
Benazapril
Cilazapril
Quinapril
Ramipril
Spirapril
Minor
Minor
-
Minor
+
-
Minor
+
+
Kidney
Differences between ACE inhibitors
0 1
-4 -
1
to
B
S
El 7
-8 -
1
)
1
ISs: y ) ^
p
»•
-16 -
1
0)
1
t,
a
-20 a
a
-24 -
1
a
O
1
© —28
be
C
•>
)—<i
c
r
L
I
4
6
10
24
Time (h)
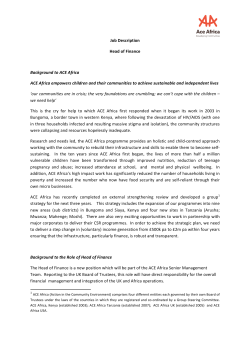
Figure 2 Change in mean arterial pressure in groups of patients with mild to moderate
heart failure after administration of placebo, captopril, enalapril or perindopril in a
double-blind design. D denotes placebo (n=12); O denotes enalapril 2-5 mg (n = 12);
• denotes captopril 6-25 mg (n=12); • denotes perindopril 2 mg (n = 12). (Reproduced
with permission1 '.)
Clinical relevant differences in
hypertension
As far as anti-hypertensive efficacy is concerned it
appears that all clinically available ACE inhibitors lower
blood pressure if given in an appropriate dose to
patients with essential hypertension1'1. There are well
recognized differences between the time course of onset
of maximum effect, offset and duration of action. Thus
the optimal dose and dose frequency/dose interval
may vary from three times daily to once-daily[l21. At
present there is no convincing data comparing ACE
inhibitors suggesting clinically relevant differences in
anti-hypertensive efficacy. Similarly, although there is
evidence that ACE inhibitors will reverse left ventricular
hypertrophy and reduce proteinuria, there is no compelling evidence of difference between drugs if an appropriate regimen is employed. As far as 'hard' end-points of
morbidity and mortality are concerned, there are not
only no comparative data, but at present there is no
prospective clinical trial evidence at all with respect to
this class of drugs.
Side effects may reveal more consistent and
potentially relevant differences. Early reports of taste
disturbance (dysgeusia) suggested this was more common with captopril and has been attributed to the
presence of an SH group'5'. Cough as a side effect
appears to be related to bradykinin or other nonangiotensin mechanism as cough is not a feature of
angiotensin II receptor antagonists1'81. Although cough
has been reported with all ACE inhibitors marketed to
date in Europe1'91, there have been claims in clinical
trials that an ACE inhibitor being developed in Japan
does not cause cough'201. More extensive clinical experience and patient exposure is required before such a claim
can be accepted.
Clinically relevant differences in heart
failure
The objectives of treatment of heart failure with ACE
inhibitors differ from those in hypertension. In the latter
group blood pressure presents a readily measurable
marker of drug effect to which a quantitative 'target' can
be applied. Blood pressure as an intermediate phenotype
for cardiovascular outcome can be used to monitor
response to treatment and adherence to an optimal
regimen.
In contrast, in heart failure there is no such
simple quantitative index and there remain doubts and
difficulty about determining the optimal dose and dose
frequency. The therapeutic objective of ACE inhibition
in heart failure is to prevent progression of left ventricular dysfunction and ultimately to delay or arrest progression of heart failure and death'2'. Several ACE inhibitors
with differing kinetic profiles have been confirmed to
achieve these objectives'2'. This increasingly suggests
that the improvement in outcome in heart failure is a
class effect of ACE inhibitors. There is no information
on comparative studies of the effects of different ACE
inhibitors on outcome. However, subgroup analysis
of some of the large trials suggest that early haemodynamic changes, particularly early hypotension in the
Eur Heart J, Vol. 18, Suppl E 1997
Downloaded from by guest on October 21, 2014
natriuretic effects of endogenous ANP and BNP. The
latter compounds are a good example of ACE inhibitors
with distinct and different pharmacodynamic profiles
which could be of potential clinical relevance.
E18 J. L. Reid
CONSENSUS II Study may be associated with a less
good outcome than patients without hypotension'2''.
This could be of clinical importance to the choice of
ACE inhibitor in heart failure as the best documented
differences between ACE inhibitors are in the time
course and intensity of the early blood pressure changes
after the first dose[22).
In three placebo-controlled parallel group
studies of blood pressure changes after initiation of
anti-hypertensive treatment we have observed characteristic and consistent patterns of blood pressure fall'23"251.
Captopril caused an early short-lived fall, enalapril led
to a delayed but long-lasting fall, while perindopril in
two studies did not alter blood pressure differently to
placebo over the first 24 h (Fig. 2). These findings
have been subsequently confirmed in a similar study in
another centre1261.
There could be advantages in initiating treatment with the ACE inhibitor least likely to cause early
hypotension.
References
Eur Heart J. Vol. 18, Supp! E 1997
Downloaded from by guest on October 21, 2014
[1] Brunner HR, Waebber B, Nussberger J. Angiotensin converting enzyme inhibitors. In: Messerli F, ed. Cardiovascular
Drug Therapy, 2nd edn. Philadelphia: W.B. Saunders, 1996:
670-700.
[2] Consensus Trial Study Group. Effects of enalapril on mortality in severe congestive heart failure. N Engl J Med 1987;
316: 1429-35.
[3] British National Formulary. Cardiovascular system — drugs
affecting the renin angiotensin system, No. 32, 1996; 80-90.
[4] McMurray J, Chopra M. Influence of ACE inhibitors on free
radical and reperfusion injury. Br J Clin Pharmacol 1991; 31:
373-9.
[5] Cooper WD, Sheldon D, Brown D, Kimber GR. Postmarketing surveillance of enalapril: experience in 11710
patients in general practice. J Royal Coll Gen Pract 1987; 37:
346-9.
[6] Migdalof BH, Antonaccio MJ, McKinstry D el al. Captopril:
pharmacology, metabolism and disposition. Drug Metab Rev
1984; 15: 841-69.
[7] Gomez HJ, Sromorsky J, Knstianson K. Lisinopril dose
response in mild to moderate hypertension. Clin Pharmacol
Ther 1985; 37: 198.
[8] Ulm EH, Hichens M, Gomez HJ. Enalapril maleate and a
lysine analogue: disposition in man. Br J Clin Pharmacol
1982; 14: 357-62.
[9] MacFadyen RJ, Lees KR, Reid JL. Perindopril: a review of its
pharmacokinetics and clinical pharmacology. Drugs 1990; 39:
49-63.
[10] Tsai HH, Lees KR, Howden CW, Reid JL. The pharmacokinetics and pharmacodynamics of perindopril in patients
with hepatic cirrhosis. Br J Clin Pharmacol 1989; 28: 53-9.
[11] Harrigan JR, Hughes DM, Meredith PA, Reid JL. Characterization of the effects of prodrug concentration on the in
vivo potency of the metabolites of five ACE inhibitors. Eur J
Clin Pharmacol 1989; 36 (Suppl): A186.
[12] Johnston CI. Angiotensin converting enzyme inhibitors. In:
Doyle AE, eds. Clinical Pharmacology of Antihypertensive
Drugs. Handbook of Hypertension, Vol II. Amsterdam:
Elsevier Science Publishers, 1988; 301-26.
[13] Ryan JW, Chung A, Berryer P, Murray MA, Ryan JPA. Slow
tight binding inhibitors of angiotensin converting enzyme.
Adv Exp Med Biol 1986; 198: 419-25.
[14] Lees KR, Kelman AW, Reid JL, Whiting B. Pharmacokinetic
of an ACE inhibitor S9780 in man: Evidence of tissue binding.
J Pharmacokinet Biopharm 1989; 17: 529-50.
[15] Donnelly R, Meredith PA, Elliott HL, Reid JL. Kinetic
dynamic relations and individual responses to enalapril.
Hypertension 1990; 15: 301-9.
[16] Meredith PA, Elliott HL, Donnelly R, Reid JL. Dose response
clarification in early drug development. J Hypertens 1991; 9
(Suppl 6): 356-7.
[17] Seymour AA, Assad MM, Abboa-Offei B, Smith PL, Rogers
WL, Dorso CR. Determinants of in vivo activity of neutral
endopeptidase and angiotensin converting enzyme inhibitors.
J Pharmacol Exp Ther 1996; 276: 708-13.
[18] Lacourciere Y, Brunner HR, Irwin R, Karlberg BE, Ramsay
LE. Effects of modulators of the renin-angiotensin aldosterone system on cough. J Hypertension 1994; 12: 1387-93.
[19] Israili ZH, Hall WD. Cough and angioneurotic edema associated with ACE inhibitor therapy — a review of the literature
and pathophysiology. Ann Intern Med 1992; 117: 234-42.
[20] Saruta T, Omae T, Kuramuchi M, Iimura O. Imidapril
hydrochloride in essential hypertension: a double blind comparative study using enalapril maleate as a control. J Hypertens 1995; 13 (Suppl 3): 23-30.
[21] Swedberg K, Held P, Kjekshus J, Rasmussen P, Ryden L,
Weach H. Effects of early administration of enalapril in
patients with acute myocardial infarction' Results of the
Cooperative New Scandinavian Enalapril Survival Study II. N
Engl J Med 1992; 327: 678-84.
[22] Reid J, Lees ICR, Squire I. First dose hypotension and ACE
inhibitors in heart failure. Chester, England: ADIS International, 1995; 1-23.
[23] MacFadyen RJ, Lees KR, Reid JL. Differences in first dose
response to ACE inhibition in congestive cardiac failure: a
placebo controlled study. Br Heart J 1991; 66: 206-11.
[24] Squire IB, MacFadyen RJ, Lees KR, Meredith PA, Hilhs WS,
Reid JL. Haemodynamic response and pharmacokinetics after
the first dose of quinapnl in patients with congestive heart
failure. Br J Clin Pharmacol 1994; 38: 117-23.
[25] Squire IB, MacFadyen RJ, Lees KR, Reid JL. Differing BP
and renin angiotensin system responses to ACE inhibition in
heart failure (Abstr). Am Congr Cardiol Atlanta, 1994.
[26] MacFadyen RJ, Barr CS, Sturrock NDC, Fenwick M,
Struthers AD. Further evidence that chronic perindopril
treatment maintains neurohumoral suppression but does not
lower blood pressure in chronic cardiac failure. Br J Clin
Pharmacol 1997 (in press).









© Copyright 2026