
Prescribing Points
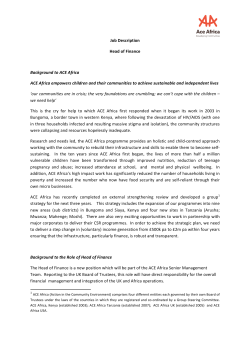
October 2001 Volume 10.4 Prescribing Points A NEWSLETTER FOR GENERAL PRACTITIONERS AND PHARMACISTS IN OXFORDSHIRE PRODUCED BY THE PRESCRIBING TEAM, DIRECTORATE OF PUBLIC HEALTH & HEALTH POLICY, OXFORDSHIRE HEALTH AUTHORITY, OLD ROAD HEADINGTON, OXFORD OX3 7LG This article was initially prepared for prescribers in the Oxford Radcliffe Hospital NHS Trust. However as many points are pertinent to prescribing in primary care we though it would be of value to publish it here. Angiotensin Converting Enzyme (ACE) Inhibitors A ngiotensin converting enzyme inhibitors block the conversion of angiotensin I to its acute metabolite angiotensin II. EDITORIAL BOARD Editor Julie Dandridge Editorial Board Tom Jones Ian G. Simpson Louise Cotton Unless stated otherwise, the views expressed in this publication are those of the authors, and do not necessarily represent the policy of Oxfordshire Health Authority. Desk Top Publishing Louise Carlisle The renin-angiotensin system is central to the pathophysiology of hypertension and heart failure. Although ACE inhibitors are effective antihypertensive drugs, their benefits go beyond simple blood pressure reduction or vasodilatation and include vascular and cardiac remodelling. There are now eleven ACE inhibitors licensed in the UK, of which four are in the Oxford Radcliffe formulary (captopril, enalapril, lisinopril, and ramipril). The choice has been based on historical precedent, cost, and data from published studies. While there are important pharmacological differences between ACE inhibitors, it is not clearly established whether these result in significant differences in the clinical benefits produced. The purpose of this article is to provide clinicians with a summary of the trial / evidence relating to the agents in the ORH formulary, with guidance on doses and frequency of administration. Pharmacological Differences Pharmacodynamics It is not known whether full 24-hour ACE inhibition is required for the beneficial effects of ACE inhibitors in hypertension or heart disease. It is essential to optimise treatment in terms of target doses and dosing frequency (see Table 1). For patient convenience, and hence compliance, captopril is not suitable for long-term treatment. Elimination All ACE inhibitors are renally excreted but lisinopril and ramipril have significant faecal excretion (via the bile). Renal toxicity is well described; all patients should have their renal function checked before starting/ or changing the dose of ACE inhibitor, and during treatment. Licensed Indications Table 1 summarises the licensed indications and dosages for the ACE inhibitors in the ORH formulary. Captopril with its short half-life, is useful for initiation in unstable patients, but is not ideal for longer-term use. Lisinopril is the only ACE inhibitor recommended for once-daily dosing for all its indications. 1. Heart Failure The use of ACE inhibitors in patients with heart failure characterised by left ventricular systolic dysfunction is supported by good clinical evidence. [1, 2] Table 2 summarises the results of the major clinical studies of ACE inhibitors in heart failure. Table 1 – Licensed indications for ACE inhibitors with costs per 28 days in community Indication Dosage Cost/28days a Hypertension Indication Dosage Cost/28days a Diabetic Nephropathy Captoprilb 12.5 - 50mg twice daily £2.21 - £3.75 Captoprilb 75mg - 100mg daily, in 2 to 3 divided doses £3.75 - £4.42 Lisinopril 2.5 - 40mg once daily £6.26 - £21.94 Lisinopril 2.5 - 20mg once daily £6.26 - £10.97 Enalapril 10 - 20mg twice daily £10.46 - £12.64 Ramipril 1.25 - 10mg once daily £5.30 - £13.00 Heart Failure Captoprilb 50mg three times daily Lisinopril 30 - 35mg once daily £20.67 - £28.53 £5.62 Enalapril 10 - 20mg twice daily £10.46 - £12.64 Ramipril 5mg twice daily £19.10 Acute MI Captoprilb 50mg three time daily £5.62 Lisinopril 10mg once daily £9.70 Enalapril 10 - 20mg twice daily £10.46 - £12.64 Ramipril 1.25mg - 5mg twice daily £10.30 - £19.10 HOPE studyc Ramiprild 10mg once daily £13.00 3 a. b. c. d. Prescribing Points Based on Drug Tariff March 2001 For patient convenience and compliance, captopril is not suitable for longterm treatment Reducing the risk of myocardial infarction, stroke or cardiovascular death and/or the need for revascularisation procedures It is not known whether this benefit is a class effect. It is however not necessary to switch if a patient is already on an ACE inhibitor. Table 2 - Studies of ACE inhibitors in Heart Failure (includes only ACE inhibitors on ORH formulary) Drug Trial Captopril Enalapril Enalapril Average daily dose ξ Patient Selection Follow up period SAVE[1] LVEF <40% 42 months 150mg 24 SOLVD[2] SOLVD[2] LVEF<35% Symptomatic LVEF <35% (Asymptomatic) 41 months 37 months 11.2 mg 16.7 mg 22 105 NNT Table 3 - Studies of ACE inhibitors Post MI (includes only ACE inhibitors on ORH formulary) Drug Trial Patient Selection Captopril Captopril Enalapril Lisinopril Ramipril SAVE[1] ISIS-4[3] CONSENSUS-II[4] GISSI 3[5] AIRE[6] LVEF<40% (Asymptomatic) All patients All patients All patients Heart failure (clinical evidence) Days drug started 3-16 days (Average 11dy) <24hrs <24hrs <24hrs 3-10 days Average daily dose NNT 90% on 150mg 18.4mg 8.8mg 8.2 mg ξ 24 200 125 17 ξ NNT = Number needed to treat to prevent one death. The NNT is greatly affected by the event rate. Thus the NNT is much more favourable in trials where overall mortality was higher i.e. in those with clinically apparent heart failure. 2. Acute Myocardial Infarction ACE inhibitors significantly reduce mortality following acute myocardial infarction.[1, 3-6] The size of the benefit appears greater in patients with left ventricular impairment or clinical evidence of heart failure (Table 3). 3. Hypertension All ACE inhibitors are effective antihypertensives, but the effect of a single dose of enalapril is less marked in the second 12 hours of the day. Twice- daily dosing is recommended for enalapril. 4. Diabetic Nephropathy The ACE inhibitors slow the progression of diabetic nephropathy. The mechanism appears to involve not only blood pressure. 5. HOPE Study HOPE was a 5-year study of 9000 patients with vascular disease or diabetes plus one other cardiovascular risk factor, i.e. they were at high risk of cardiovascular events but were not known to have left ventricular impairment.[7] Outcome was a composite of myocardial infarction, stroke, and cardiovascular death. The absolute risk reduction for this outcome was 3.7% (NNT= 27). The dose used was 10mg of ramipril once a day. Whilst it is likely that this benefit is a class effect, at present ramipril is the only ACE inhibitor licensed in this group of patients. Adverse Drug Reactions • ACE inhibitors cause first-dose hypotension, especially in patients taking diuretics, on a lowsodium diet, on dialysis, dehydrated, or with heart failure. • Cough is the most troublesome common adverse effect. Reporting of this in trials is very variable, and there are no sound systematic data on the relative incidences for the different agents. ACE may cause angioedema (onset may be delayed), and should be used with care (or avoided • 4 • Prescribing Points ACE inhibitors should be avoided in patients who are volume depleted. This is a particular problem in patients with decompensated liver cirrhosis. Contraindications/Cautions • • • • • ACE inhibitors are contraindicated in patients with severe bilateral renal artery stenosis. ACE inhibitors are best avoided in patients with known or suspected renovascular disease. Use of prodrugs such as enalapril and ramipril, requires close monitoring in patients with impaired liver function. Renal function and electrolytes (particularly potassium) should be checked before starting ACE inhibitors and monitored during treatment. Concomitant treatment with NSAIDs increases the risk of renal damage, and potassiumsparing diuretics (or potassium-containing salt substitutes) increase the risk of hyperkalaemia References 1. 2. 3. 4. 5. 6. 7. Pfeffer, M.A., et al., Effect of captopril on mortality and morbidity in patients with left ventricular dysfunction after myocardial infarction. Results of the survival and ventricular enlargement trial. The SAVE Investigators. N Engl J Med, 1992. 327(10): p. 669-77. Effect of enalapril on survival in patients with reduced left ventricular ejection fractions and congestive heart failure. The SOLVD Investigators. N Engl J Med, 1991. 325(5): p. 293-302. ISIS-4: a randomised factorial trial assessing early oral captopril, oral mononitrate, and intravenous magnesium sulphate in 58,050 patients with suspected acute myocardial infarction. ISIS4 (Fourth International Study of Infarct Survival) Collaborative Group. Lancet, 1995. 345(8951): p. 669-85. Edner, M., et al., Effect of enalapril initiated early after acute myocardial infarction on heart failure parameters, with reference to clinical class and echocardiographic determinants. CONSENSUS II Multi-Echo Study Group. Clin Cardiol, 1996. 19(7): p. 543-8. GISSI-3: effects of lisinopril and transdermal glyceryl trinitrate singly and together on 6-week mortality and ventricular function after acute myocardial infarction. Gruppo Italiano per lo Studio della Sopravvivenza nell'infarto Miocardico. Lancet, 1994. 343(8906): p. 1115-22. Effect of ramipril on mortality and morbidity of survivors of acute myocardial infarction with clinical evidence of heart failure. The Acute Infarction Ramipril Efficacy (AIRE) Study Investigators. Lancet, 1993. 342(8875): p. 821-8. Effects of ramipril on cardiovascular and microvascular outcomes in people with diabetes mellitus: results of the HOPE study and MICRO-HOPE substudy. Heart Outcomes Prevention Evaluation Study Investigators. Lancet, 2000. 355(9200): p. 253-9. Contributors: Dr Duncan Richards (Clinical Pharmacology, RI); Dr DJ Reynolds (Consultant Physician, JR) 'Bunmi Fajemisin (Clinical Effectiveness Pharmacist) With advice from: Dr. K Channon (Honorary Consultant Cardiologist, JR) The follow ing gra ph give s de ta ils of pre scribing costs in Ox fordshire 10000 9000 8000 7000 5000 4000 3000 2000 1000 captopril lis inopril ram ipril Apr-01 Mar-01 Feb-01 Jan-01 Dec-00 Oct-00 Nov-00 Sep-00 Aug-00 Jul-00 Jun-00 Apr-00 May-00 Mar-00 Jan-00 Feb-00 Dec-99 Oct-99 Nov-99 Sep-99 Jul-99 Aug-99 Jun-99 0 May-99 total items 6000 enalapril perindopril











© Copyright 2026