
Case Study: Delirium in an Adolescent Girl With Human Immunodeficiency Virus-
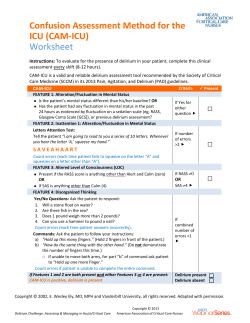
Case Study: Delirium in an Adolescent Girl With Human Immunodeficiency VirusAssociated Dementia Michelle Lisk Background Info ► Female ► 15 years old ► History of HIV infection ► From the inner city of Baltimore Problems ► HIV virus in its late stages causes development of HIV-associated dementia (HAD) ► Fevers incited bouts of delirium due to her current condition of HAD ► The top row of images are of the patient ► The bottom row of images were taken of a normal 16-yearold Damages ► Overall thinning of the corpus callosum ► Prominent ventricles and sulci ► Signal abnormalities were observed in the right caudate nucleus ► Extensive cerebral atrophy Examination 3 Years Prior ► ► ► ► Preformed in the 93rd percentile in adaptive behavior skills tests Talkative and able to carry on reciprocal conversation No reported disruptions in thinking, behavior or skills Normal motor functioning, posture and gait Current Examination (After treating the episode of delirium) ► ► ► ► Vineland Adaptive Behavior assessment showed patient to be in the first percentile for adaptive functioning Could recall names of people around her, but conversation was empty and non-reciprocal. Also exhibited speech latency when responding to a question. Easily agitated and physically aggressive Displayed resting tremors and a decline in posture and gait Discussion ► Severe cognitive decline is most likely caused by marked cerebral atrophy ► Damage to the right caudate nucleus could explain the lack of response to the attempts to restrain and calm the patient ► Lack of attention and inability to maintain productive conversation is likely due to the thinning of the corpus callosum ► Interestingly, the patient showed no deficits in IQ knowledge as compared to earlier scores suggesting her long-term memory was relatively in tact Outlook ► The acute episode of delirium was treated on site ► HAD currently has no cure ► The best treatment for HAD is highly active antiretroviral therapy to attempt to slow down the process of atrophy ► Patient has currently discontinued treatment with antiretroviral meds due to resistance ► Treatment with these types of medications is problematic due to the interactions they have with other drugs Interesting Thoughts ► Patient showed a severe decline in both memory and cognition in a matter of three years with no treatment for this continued atrophy ► While the atrophy itself may not be halted, are there any alternate treatments that would stave off the cerebral decline?










© Copyright 2026