
Contribution of bradykinin to the cardioprotective effects of ACE inhibitors Introduction
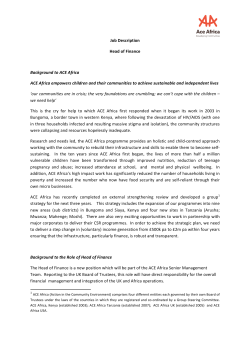
European Heart Journal Supplements (2003) 5 (Supplement A), A37–A41 Contribution of bradykinin to the cardioprotective effects of ACE inhibitors L. Murphey1, D. Vaughan2 and N. Brown1 1Division of Clinical Pharmacology, 2Division of Cardiovascular Medicine, Departments of Medicine and Pharmacology, Vanderbilt University School of Medicine, Nashville, Tennessee, USA and 2Veterans Affairs Medical Center, Nashville, Tennessee, USA Bradykinin, through its B2 receptor, stimulates endothelial release of a number of vasodilators, such as nitric oxide, prostacyclin, and endothelium-derived hyperpolarizing factor (EDHF). Angiotensin-converting enzyme (ACE) inhibitors enhance the effects of local bradykinin by decreasing its degradation and by increasing B2 receptor sensitivity. Clinical and experimental studies demonstrate that blockade of the B2 receptor attenuates the antihypertensive, antihypertrophic, and antiatherosclerotic effects of ACE inhibitors. Thus, the evidence strongly supports a role for bradykinin in mediating the cardiovascular benefits of ACE inhibitors. (Eur Heart J Supplements 2003; 5 (Suppl A): A37–A41) © 2003 The European Society of Cardiology Introduction to release bradykinin, which acts in a paracrine manner via bradykinin B2 receptors. Tissue kallikrein, a distinct enzyme activated by different mechanisms, releases lysl-bradykinin (kallidin), which also acts through the B2 receptor. Bradykinin exerts a number of vascular effects (Fig. 2). By stimulating synthesis and release of nitric oxide (NO), prostacyclin, and endothelium-derived hyperpolarizing factor (EDHF), bradykinin causes vasodilation and also inhibits platelet adhesion and smooth muscle cell proliferation[6]. Bradykinin is also one of the most potent stimuli for endothelial release of tissue plasminogen activator (tPA) in vivo[7]. Overview of the RAS and KKS The major components and actions of the RAS and the KKS are illustrated in Fig. 1. Both the RAS and KKS have been localised to the vasculature[4,5], where the effects of bradykinin oppose many of the actions of angiotensin II (Ang II). Bradykinin: Key component of the KKS The KKS is activated on the surface of endothelial cells[5]. Plasma kallikrein cleaves high-molecular-weight kininogen, Correspondence: Laine J. Murphey, MD, PhD, 556A Robinson Research Building, Vanderbilt University Medical Center, Nashville, TN 37232-6602 USA 1520-765X/03/0A0037 + 05 $35.00/0 Ang II: Key component of the RAS ACE, a bivalent dipeptidyl carboxyl metallopeptidase, is present in endothelial, epithelial or neuroepithelial cells as a membrane-bound form, and as a soluble form in the brain, blood and numerous body fluids[8]. ACE converts angiotensin I (Ang I) to Ang II, the principal effector molecule of the RAS. Four receptor subtypes have been identified for Ang II[9]: the AT1 receptor mediates vasoconstriction, vascular smooth muscle cell proliferation, and production of superoxide ions; the AT2 receptor, which is normally expressed at very low levels in adults, may be upregulated during AT1 receptor blockade and counteracts many AT1-mediated effects (see below)[10,11]; the role of the AT3 receptor is not known at present; and AT4 influences local blood flow[12] and stimulates synthesis of plasminogen activator inhibitor 1 (PAI-1), the major physiological inhibitor of fibrinolysis, in endothelial cells[13]. © 2003 The European Society of Cardiology Downloaded from by guest on November 10, 2014 Over 30 years ago, Ferreira et al.[1] isolated a bradykininpotentiating peptide from the venom of a Central American viper. Shortly thereafter, Ondetti et al.[2] reported the isolation of an angiotensin-converting enzyme (ACE) inhibitor from the venom of the same snake. Erdös subsequently demonstrated that ACE and kininase II, which degrades bradykinin to inactive metabolites, are the same enzyme[3], thus linking the renin-angiotensin system (RAS) and the kallikrein-kinin system (KKS). Key Words: ACE inhibitors, ramipril, bradykinin, endothelial dysfunction, kallikrein-kinin system, renin-angiotensin system A38 L. Murphey et al. + Figure 1 Components and major actions of the RAS and KKS. RAS / KKS linkages Bradykinin and antihypertensive effects of ACE inhibitors The availability of a specific bradykinin B2 receptor antagonist, icatibant acetate (HOE 140), has allowed investigators to determine the contribution of bradykinin to the effects of ACE inhibitors in vivo. Bradykinin receptor blockade attenuates the hypotensive response to ACE inhibition in rats and dogs[23–25]. In humans, ACE inhibition enhances[26] whereas B2 receptor blockade decreases[7,27] the vasodilator effects of exogenous bradykinin. Studies using icatibant further indicate that endogenous bradykinin contributes to the acute hemodynamic effects of ACE inhibitors in humans. For example, bradykinin receptor blockade decreases the potentiation of endotheliummediated, flow-dependent vasodilation by ACE inhibition in Eur Heart J Supplements, Vol. 5 (Suppl A) January 2003 Figure 2 Vascular effects of bradykinin. Bradykinin interacts with B2 receptors to stimulate production of NO, PGI 2 and EDHF, which diffuse from the endothelium to vascular smooth muscle cells. Through differing mechanisms these mediators produce vascular smooth cell relaxation. Antagonists and inhibitors are indicated with boxes. BK=bradykinin; EDHF=endothelium-derived hyperpolarizing factor; L-NMMA=L-NG-monomethyl-L-arginine; NO=nitric oxide; PGI2=prostacyclin; PLA2=phospholipase A2; PLC=phospholipase C. (Adapted from Vanhoutte[49]). healthy individuals[28]. Similarly, co-administration of icatibant attenuates the acute hypotensive effects of oral captopril in both normotensive and hypertensive subjects[29]. Bradykinin and antihypertrophic effects of ACE inhibitors ACE inhibitors decrease cardiac hypertrophy in patients with hypertension[30]. Bradykinin receptor antagonism decreases the antihypertrophic effect of ACE inhibitors in hypertensive animals[23]. Conversely, genetic B2 receptor deficiency is associated with the development of cardiac hypertrophy[31]. In vitro, bradykinin prevents Ang IIinduced hypertrophy of cultured cardiomyocytes by releasing nitric oxide (NO) from endothelial cells, thereby increasing cardiomyocyte guanosine 3′5′-cyclic monophosphate (cGMP)[32]. Bradykinin and anti-ischemic and antiatherosclerotic effects of ACE inhibitors ACE inhibitors reduce the risk of myocardial infarction in patients with decreased left ventricular function[33,34], as Downloaded from by guest on November 10, 2014 The RAS and KKS are linked at a number of levels. ACE not only converts Ang I to Ang II but also bradykinin to inactive metabolites[14]; hence, ACE inhibitors increase circulating concentrations of bradykinin[15]. Recent evidence suggests that ACE inhibitors also potentiate the effects of bradykinin via direct effects at the bradykinin B2 receptor[16,17]. For example, Benzing et al.[18] demonstrated that ramiprilat, a tissue-specific ACE inhibitor, inhibited the desensitization of the B2 receptor via sequestration within caveolae, lipid-rich pockets on the surface of endothelial cells. Similarly, Marcic et al. demonstrated that ACE inhibitors enhance the effect of bradykinin at its B2 receptor by inducing ‘crosstalk’ between ACE and the receptor[19]. In vitro and animal studies suggest that the AT2 receptor provides an additional connection between the RAS and the KKS. During AT1 receptor blockade, unopposed activation of the AT2 receptor leads to increased bradykinin, NO and cyclic (c)GMP[11,20]. Although acute AT1 receptor blockade does not potentiate the effects of exogenous bradykinin[21], these data potentially implicate endogenous bradykinin in the beneficial effects of chronic AT1 receptor blockade[22]. Likely mechanism of ramipril in coronary heart disease well as in patients with normal left ventricular function who are at risk for coronary artery disease[35]. Again, studies in animals using icatibant implicate bradykinin in the mechanism of the anti-ischemic effects of ACE inhibitors. Thus ACE inhibition decreases infarct size following coronary artery occlusion in dogs or rabbits and this effect is abolished by either bradykinin receptor antagonism[36,37] or nitric oxide synthase inhibition with NG-L-nitro-arginine methyl ester (L-NAME)[38]. Kallikrein A39 Angiotensinogen Kininogen Renin Ang I Bradykinin ACE Ang II Inactive peptides tPA PAI-1 Ang IV ALDO Bradykinin, ACE inhibition, and fibrinolytic balance Figure 3 Relationship between the renin-angiotensin, kallikrein-kinin, and fibrinolytic systems. Angiotensin-converting enzyme (ACE) can shift the fibrinolytic balance in favor of PAI-1 by increasing the formation of angiotensin II (Ang II) and the catabolism of bradykinin. Ang I=angiotensin I; Ang IV=angiotensin IV; PAI-1=plasminogen activator inhibitor-1; tPA=tissue-type plasminogen activator. (Adapted from Brown and Vaughan[39].) hypertensive subjects, and patients post-MI. For example, in the Healing and Early Afterload Reduction Therapy (HEART) study[45], ACE inhibition decreased PAI-1 antigen and activity in patients with acute anterior MI. Plasma tPA levels were similar in both the ramipril and control groups. The effect of ACE inhibition on PAI-1 antigen following thrombolysis for acute MI has also been described[46]. ACE inhibition was associated with a diminished rise in PAI-1 antigen following thrombolysis and an increased rate of patency of the infarct-related artery. The observation that chronic ACE inhibition but not AT1 receptor antagonism decreases circulating PAI-1 antigen concentrations[47] raises the possibility that bradykinin not only stimulates tPA release, but also contributes to the regulation of PAI-1. Because NO suppresses PAI-1 expression after stimulation by Ang II in aortic smooth muscle cells[48], it may be hypothesized that bradykinin could moderate PAI-1 expression by releasing NO. Further studies are needed to determine whether bradykinin opposes the effects of Ang II on PAI-1 expression. Conclusion Bradykinin favorably alters fibrinolytic balance and promotes release of vasoactive compounds that improve endothelial function. ACE inhibitors potentiate bradykinin by blocking (1) ACE-mediated breakdown of bradykinin, and (2) B2 receptor desensitization. A substantial body of evidence points to increased local bradykinin action as an important contributing mechanism in the reduction of cardiovascular events[35]. Eur Heart J Supplements, Vol. 5 (Suppl A) January 2003 Downloaded from by guest on November 10, 2014 One mechanism through which bradykinin may contribute to the anti-ischemic effects of ACE inhibitors involves the fibrinolytic system. The endogenous fibrinolytic system serves as one of the major defense mechanisms against intravascular thrombosis. Fibrinolytic activity is regulated by the balance between tPA and PAI-1 (Fig. 3)[39,40]. Bradykinin stimulates endothelial release of tPA,[8,42] whereas Ang II increases PAI-1 expression[13]. Brown et al.[7] have studied the mechanism of bradykinin-induced tPA release from the human vasculature. They demonstrated that bradykinin stimulates vascular tPA release in a dose-dependent manner, that this effect is independent of changes in flow, and that, like vasodilation, this effect is mediated through the bradykinin B2 receptor. However, following receptor activation, bradykinin appears to cause vasodilation and stimulate tPA release through distinct mechanisms. Thus, while administration of the nitric oxide synthase (NOS) inhibitor L-NG-monomethyl-L-arginine (L-NMMA) attenuates the forearm vasodilator response to bradykinin, indicating that NO contributes to bradykinin-induced vasodilation, L-NMMA alone or in combination with the cyclooxygenase inhibitor indomethacin did not affect the tPA response to bradykinin, suggesting that tPA release is mediated through a NOS- and cyclooxygenase-independent pathway. ACE inhibitors improve endothelial function as measured by the vasodilator response to endothelium-dependent agonists[42]. ACE inhibition, but not AT1 receptor blockade, potentiates the effect of exogenous bradykinin on tPA release in the peripheral[41] and coronary vasculature[43]. A recent study using icatibant indicates that ACE inhibition increases constitutive vascular tPA release in subjects at risk for coronary artery disease through effects on endogenous bradykinin[44]. The findings that bradykinin induces tPA expression and release while Ang II stimulates PAI-1 expression suggest that ACE inhibitors reduce risk of MI, in part, through effects on fibrinolytic balance. Indeed, activation of the renin-angiotensin-aldosterone system by salt depletion or diuretic use increases plasma PAI-1 concentrations, while ACE inhibition significantly decreases plasma PAI-1 without consistently decreasing tPA concentrations[40]. Hence, ACE inhibitors improve the molar ratio of PAI-1 to tPA. These effects have been observed in young normotensive subjects, healthy postmenopausal women, A40 L. Murphey et al. References Eur Heart J Supplements, Vol. 5 (Suppl A) January 2003 Downloaded from by guest on November 10, 2014 [1] Ferreira SH, Bartelt DC, Greene LJ. Isolation of bradykininpotentiating peptides from Bothrops jararaca venom. Biochemistry 1970; 9: 2583–93. [2] Ondetti MA, Williams NJ, Sabo EF, Pluscec J, Weaver ER, Kocy O. Angiotensin-converting enzyme inhibitors from the venom of Bothrops jararaca. Isolation, elucidation of structure, and synthesis. Biochemistry 1971; 10: 4033–9. [3] Erdös E.G. The angiotensin I converting enzyme. Fed Proc 1977; 36: 1760–5. [4] Dzau VJ Re R. Tissue angiotensin system in cardiovascular medicine - A paradigm shift. Circulation 1994; 89: 493–8. [5] Røjkjær R Schmaier AH. Activation of the plasma kallikrein/kinin system on endothelial cells. Proc Assoc Am Physicians 1999; 111: 220–7. [6] Linz W, Wohlfart P, Schölkens BA, Malinski T, Wiemer G. Interactions among ACE, kinins and NO. Cardiovasc Res 1999; 43: 549–61. [7] Brown NJ, Gainer JV, Murphey LJ, Vaughan DE. Bradykinin stimulates tissue plasminogen activator release from human forearm vasculature through B2 receptor-dependent, NO synthase-independent, and cyclooxygenase-independent pathway. Circulation 2000; 102: 2190–6. [8] Skidgel RA, Erdös EG. Biochemistry of angiotensin I-converting enzyme. In: Robertson JIS, Nicholls MG, eds. The ReninAngiotensin System. New York: Raven Press, Ltd.: 1993: 10.1–10.10. [9] Timmermans PB, Wong PC, Chiu AT et al. Angiotensin II receptors and angiotensin II receptor antagonists. Pharmacol Rev 1993; 45: 205–51. [10] Berry C, Touyz R, Dominiczak AF, Webb RC, Johns DG. Angiotensin receptors: signaling, vascular pathophysiology, and interactions with ceramide. Am J Physiol Heart Circ Physiol 2001; 281: H2337–H2365. [11] Gohlke P, Pees C, Unger T. AT2 receptor stimulation increases aortic cyclic GMP in SHRSP by a kinin-dependent mechanism. Hypertension 1998; 31: 349–55. [12] Kramar EA, Harding JW, Wright JW. Angiotensin II- and IVinduced changes in cerebral blood flow; Roles of AT1, AT2, and AT4 receptor subtypes. Regul Peptides 1997; 68: 131–8. [13] Kerins DM, Hao Q, Vaughan DE. Angiotensin induction of PAI-1 expression in endothelial cells is mediated by the hexapeptide angiotensin IV. J Clin Invest 1995; 96: 2515–20. [14] Murphey LJ, Hachey DL, Oates JA, Morrow JD, Brown NJ. Metabolism of bradykinin in vivo in humans: Identification of BK1-5 as a stable plasma peptide metabolite. J Pharmacol Exp Ther 2000; 294: 263–9. [15] Pellacani A, Brunner HR, Nussberger J. Plasma kinins increase after angiotensin-converting enzyme inhibition in human subjects. Clin Sci 1994; 87: 567–74. [16] Hecker M, Porsti I, Bara AT, Busse R. Potentiation by ACE inhibitors of the dilator response to bradykinin in the coronary microcirculation: interaction at the receptor level. Br J Pharmacol 1994; 111: 238–44. [17] Hecker M, Blaukat A, Bara AT, Müller-Esterl W, Busse R. ACE inhibitor potentiation of bradykinin-induced venoconstriction. Br J Pharmacol 1997; 121: 1475–81. [18] Benzing T, Fleming I, Blaukat A, Müller-Esterl W, Busse R. Angiotensin-converting enzyme inhibitor ramiprilat interferes with the sequestration of the B2 kinin receptor within the plasma membrane of native endothelial cells. Circulation 1999; 99: 2034–40. [19] Marcic B, Deddish PA, Jackman HL, Erdös EG. Enhancement of bradykinin and resensitization of its B2 receptor. Hypertension 1999; 33: 835–43. [20] Carey RM, Wang ZQ, Siragy HM. Role of the angiotensin type 2 receptor in the regulation of blood pressure and renal function. Hypertension 2000; 35: 155–63. [21] Cockcroft JR, Sciberras DG, Goldberg MR, Ritter JM. Comparison of angiotensin-converting enzyme inhibition with angiotensin II receptor antagonism in the human forearm. J Cardiovasc Pharmacol 1993; 22: 579–784. [22] Hornig B, Landmesser U, Kohler C et al. Comparative effect of ace inhibition and angiotensin II type 1 receptor antagonism on bioavailability of nitric oxide in patients with coronary artery disease: role of superoxide dismutase. Circulation 2001; 103: 799–805. [23] Linz W Schölkens BA. A specific B2-bradykinin receptor antagonist HOE 140 abolishes the antihypertrophic effect of ramipril. Br J Pharmacol 1992; 105: 771–2. [24] Bouaziz H, Joulin Y, Safar M, Benetos A. Effects of bradykinin B2 receptor antagonism on the hypotensive effects of ACE inhibition. Br J Pharmacol 1994; 113: 717–22. [25] Barbe F, Su JB, Guyene TT, Crozatier B, Menard J, Hittinger L. Bradykinin pathway is involved in acute hemodynamic effects of enalaprilat in dogs with heart failure. Am J Physiol 1996; 270: H1985–H1992. [26] Brown NJ, Ryder D, Gainer JV, Morrow JD, Nadeau J. Differential effects of angiotensin converting enzyme inhibitors on the vasodepressor and prostacyclin responses to bradykinin. J Pharmacol Exp Ther 1996; 279: 703–12. [27] Cockcroft JR, Chowrienczyk PJ, Brett SE, Bender N, Ritter JM. Inhibition of bradykinin-induced vasodilation in human forearm vasculature by icatibant, a potent B2-receptor antagonist. Br J Clin Pharmacol 1994; 38: 317–21. [28] Hornig B, Kohler C, Drexler H. Role of bradykinin in mediating vascular effects of angiotensin-converting enzyme inhibitors in humans. Circulation 1997; 95: 1115–8. [29] Gainer JV, Morrow JD, Loveland A, King DJ, Brown NJ. Effect of bradykinin-receptor blockade on the response to angiotensinconverting-enzyme inhibitor in normotensive and hypertensive subjects. N Engl J Med 1998; 339: 1285–92. [30] Dahlof B, Herlitz H, Aurell M, Hansson L. Reversal of cardiovascular structural changes when treating essential hypertension. The importance of the renin-angiotensin-aldosterone system. Am J Hypertens 1992; 5: 900–11. [31] Emanueli C, Maestri R, Corradi D et al. Dilated and failing cardiomyopathy in bradykinin B2 receptor knockout mice. Circulation 1999; 100: 2359–65. [32] Rosenkranz AC, Hood SG, Woods RL, Dusting GJ, Ritchie RH. Acute antihypertrophic actions of bradykinin in the rat heart: Importance of cyclic GMP. Hypertension 2002; 40: 498–503. [33] Pfeffer MA, Braunwald EA, Moye LA et al. Effect of captopril on mortality and morbidity in patients with left ventricular dysfunction after myocardial infarction. N Engl J Med 1992; 327: 669–77. [34] Effect of enalapril on survival in patients with reduced left ventricular ejection fractions and congestive heart failure. The SOLVD Investigators. N Engl J Med 1991; 325: 293–302. [35] The Heart Outcomes Prevention Evaluation Study Investigators. Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. N Engl J Med 2000; 342: 145–53. [36] Martorana PA, Kettenbach B, Breipohl G, Linz W, Schölkens BA. Reduction of infarct size by local angiotensin-converting enzyme inhibition is abolished by a bradykinin antagonist. Eur J Pharmacol 1990; 182: 395–6. [37] Hartman JC, Wall TM, Hullinger TG, Shebuski RJ. Reduction of myocardial infarct size in rabbits by ramiprilat: reversal by the bradykinin antagonist HOE 140. J Cardiovasc Pharmacol 1993; 21: 996–1003. [38] Hoshida S, Yamashita N, Kawahara K, Kuzuya T, Hori M. Amelioration by quinapril of myocardial infarction induced by coronary occlusion/reperfusion in a rabbit model of atherosclerosis: Possible mechanisms. Circulation 1999; 99: 434–40. [39] Vaughan DE. Angiotensin, fibrinolysis, and vascular homeostasis. Am J Cardiol 2001; 87: 18–24. [40] Brown NJ, Vaughan DE. Prothrombotic effects of angiotensin. Adv Intern Med 2000; 45: 419–29. [41] Labinjoh C, Newby DE, Pellegrini MP, Johnston NR, Boon NA, Webb DJ. Potentiation of bradykinin-induced tissue plasminogen activator release by angiotensin-converting enzyme inhibition. J Am Coll Cardiol 2001; 38: 1402–8. [42] Mancini GB, Henry GC, Macaya C et al. Angiotensin-converting enzyme inhibition with quinapril improves endothelial vasomotor Likely mechanism of ramipril in coronary heart disease dysfunction in patients with coronary artery disease. The TREND (Trial on Reversing Endothelial Dysfunction ) Study. Circulation 1996; 94: 258–65. [43] Minai K, Matsumoto T, Horie H et al. Bradykinin stimulates the release of tissue plasminogen activator in human coronary circulation: effects of angiotensin-converting enzyme inhibitors. J Am Coll Cardiol 2001; 37: 1565–70. [44] Pretorius M, Rosenbaum DA, Vaughan DE, Brown NJ. ACE inhibition increases human vascular tPA release through endogenous bradykinin. Circulation 2002; In Press [45] Vaughan DE, Rouleau J-L, Ridker PM et al. Effects of ramipril on plasma fibrinolytic balance in patients with acute anterior myocardial infarction. Circulation 1997; 96: 442–7. A41 [46] Wagner A, Herkner H, Schreiber W et al. Ramipril prior to thrombolysis attenuates the early increase of PAI-1 in patients with acute myocardial infarction. Thromb Haemost 2002; 88: 180–5. [47] Brown NJ, Agirbasli MA, Vaughan DE. Comparative effect of angiotensin-converting enzyme inhibition and angiotensin II type 1 receptor antagonism on plasma fibrinolytic balance in humans. Hypertension 1999; 34: 285–90. [48] Bouchie JL, Hansen H, Feener EP. Natriuretic factors and nitric oxide suppress plasminogen activator inhibitor-1 expression in vascular smooth muscle cells. Role of cGMP in the regulation of the plasminogen system. Arterioscler Thromb Vasc Biol 1998; 18: 1771–9. [49] Vanhoutte PM. Vascular biology. Old-timer makes a comeback. Nature 1998; 396: 213–6. Downloaded from by guest on November 10, 2014 Eur Heart J Supplements, Vol. 5 (Suppl A) January 2003









© Copyright 2026