
Clinical picture Wall-eyed bilateral inter nuclear ophthalmoplegia with vertical gaze palsy
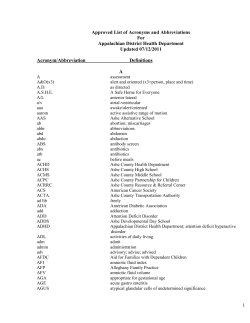
Q J Med 2014; 107:165 doi:10.1093/qjmed/hct021 Advance Access Publication 25 January 2013 Clinical picture Wall-eyed bilateral inter nuclear ophthalmoplegia with vertical gaze palsy bilateral exotropia on primary gaze, bilateral inter nuclear ophthalmoplegia (INO) and impaired convergence. It may also be associated with vertical gaze palsy, up-beat nystagmus and skew deviation. Common etiology includes inflammatory, toxic, infectious, degenerative, traumatic, postsurgical, demyelinating and neoplastic conditions, but midbrain infarction is the most common reported etiology.1 While the pathophysiology of the WEBINO syndrome remains controversial, the clinical constellation of Endings are thought to be due to bilateral medial longitudinal fasciculus (MLF) damage producing bilateral INO, likely in conjunction with abnormalities of the medial rectus sub nuclei (MRSN) of the ventral oculomotor nuclear complex culminating in bilateral exotropia and signifying bilateral convergence failure.2 As MRSN neurons are scattered within the MLF at the level of the pontomesencephalic junction, a lesion at this level could affect both structures, resulting in the WEBINO syndrome.1,2 Variable degree of vertical gaze abnormalities in WEBINO is explained by the frequent concomitant involvement of rostral interstitial nucleus of MLF or the interstitial nucleus of Cajal in the midbrain-thalamic region.2 Photographs and text from: S. Chakravarthi, P. Kesav and D. Khurana, Department of Neurology, Post Graduate Institute of Medical Education and Research, Chandigarh, India. email: [email protected] Figure 1. (a) Clinical photograph showing (in a clockwise pattern) impaired adduction of left eye with restricted abduction of right eye on attempted right horizontal gaze, impaired adduction of right eye with restricted abduction of left eye on attempted left horizontal gaze. Both upward and downward gaze paresis is evident on attempted vertical gaze as is bilateral exotropia. (b) Cranial MRI showing acute infarct in midline mesencephalic tegmentum with hyperintensity on diffusion weighted sequence and hypointensity on apparent diffusion coefficient sequence. Conflict of interest: None declared. References 1. Chen CM, Lin SH. Wall-eyed bilateral internuclear ophthalmoplegia from lesions at different levels in the brainstem. J Neuroophthalmol 2007; 27:9–15. 2. Beh SC, Frohman EM. WEBINO and the return of the King’s speech. J Neurol Sci 2012; 315:153–55. ! The Author 2013. Published by Oxford University Press on behalf of the Association of Physicians. All rights reserved. For Permissions, please email: [email protected] Downloaded from by guest on November 18, 2014 A 64-year-old woman, diabetic and hypertensive, presented with sudden onset painless diplopia and alteration of consciousness. She was drowsy with neurological examination revealing exotropia of both eyes in primary position with bilateral internuclear ophthalmoplegia on attempted horizontal gaze (Figure 1a). Pupils were normal bilaterally. Convergence, vertical saccades, pursuits and vestibular ocular reFexes were impaired. Cranial magnetic resonance imaging (MRI) showed an acute infarct in the midline of mesencephalic tegmentum involving the bilateral medial longitudinal fasciculus (Figure 1b). Wall-eyed bilateral inter nuclear ophthalmoplegia (WEBINO) is a rare disorder characterized by











© Copyright 2026