
Medicare Advantage Provider Manual
Medicare Advantage Provider Manual Section 5: HealthSpan Integrated Care Section 5: Provider Manual HealthSpan Integrated Care Billing and Payment Medicare Advantage Provider Manual Billing and Payment Table of Contents SECTION 5: BILLING AND PAYMENT ........................................................................ 5 5.1 INTRODUCTION ....................................................................................................................................... 5 5.2 KEY CONTACTS .................................................................................................................................... 5 5.3 ELECTRONIC DATA INTERCHANGE (EDI) ..................................................................................... 6 5.3.1 Billing Guidelines for Electronic Claims .............................................................................................. 6 5.3.1.1 National Provider Identifier (NPI) ...................................................................................... 6 5.3.1.2 Federal Tax Identification Number (TIN) ..................................................................... 6 5.3.1.3 Coordination of Benefits....................................................................................................... 8 5.3.2 Electronic Data Interchange (EDI) Requirements ....................................................................... 8 BENEFITS OF EDI CLAIMS SUBMISSION ...................................................................................................... 8 HIPPA Requirements ................................................................................................................................................ 8 EDI ROLES...................................................................................................................................................................... 8 UNDERSTANDING ELECTRONIC SUBMISSION PROCESS ................................................................. 9 TO INITIATE ELECTRONIC CLAIM SUBMISSIONS ................................................................................. 10 TO INITIATE ELECTRONIC PAYMENT/ REMITTANCE ADVICE ..................................................... 10 TO INITIATE ELECTRONIC FUNDS TRANSFER ...................................................................................... 10 HEALTHSPAN REQUIREMENTS......................................................................................................................... 11 SUPPORTING DOCUMENTATION ..................................................................................................................... 11 EDI CLAIM ERRORS .................................................................................................................................................. 11 CORRECTION & RESUBMISSION FOR ACCEPTED EDI CLAIMS ..................................................... 11 5.4 PAPER CLAIMS ..................................................................................................................................... 12 5.4.1 Billing Guidelines for Paper Claims...................................................................................................... 12 5.4.1.1 National Provider Identifier (NPI)..................................................................................... 12 5.4.1.2 Paper Claims Address: .......................................................................................................... 12 5.4.1.3 Paper Claim Tips ...................................................................................................................... 12 5.4.1.4 Federal Tax Identification Number (TIN) ...................................................................14 5.4.1.5 Coordination of Benefits .....................................................................................................15 5.5 SUPPORTING DOCUMENTATION......................................................................................................15 5.5.1 Supporting Documentation Cover Sheet......................................................................................... 17 5.6 CLAIM CORRECTIONS ........................................................................................................................ 17 5.7 CLAIM SUBMISSION TIMEFRAMES .................................................................................................. 18 HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 2 5.8 CLAIM PROCESSING TIMEFRAMES ................................................................................................. 18 5.9 INCORRECT CLAIM PAYMENTS ....................................................................................................... 19 5.10 PROVIDER PAYMENT DISPUTES .................................................................................................. 20 5.11 PROVIDER APPEALS ......................................................................................................................... 20 5.12 MEMBER HOLD HARMLESS ........................................................................................................... 20 5.13 CODING AND BILLING VALIDATION .............................................................................................. 21 5.13.1 CODING RULE DESCRIPTIONS ........................................................................................................... 21 5.14 DO NOT BILL EVENTS (DNBE) ................................................................................................... 31 5.14.1 Claims Submission Related to a Do Not Bill Event ..................................................................32 5.15 ANESTHESIA ...................................................................................................................................... 33 GLOBAL ANESTHESIA PACKAGE ..................................................................................................................33 OFFICE-BASED SURGICAL PROCEDURES .............................................................................................. 34 ANESTHESIA REPORTING REQUIREMENTS & REIMBURSEMENT .............................................. 34 EXCEPTIONS TO BILLING ANESTHESIA CODES ...................................................................................35 ANESTHESIA MODIFIERS ................................................................................................................................... 36 5.16 ADDITIONAL SERVICES .................................................................................................................. 37 BEHAVIORAL HEALTH SERVICES .................................................................................................................37 DURABLE MEDICAL EQUIPMENT (DME) ...................................................................................................38 EVALUATION/ MANAGEMENT (E/M) SERVICES ..................................................................................38 EMERGENCY ROOM (ER) SERVICES........................................................................................................... 39 EMERGENCY ROOM (ER) SERVICES cont................................................................................................ 40 INJECTIONS/ IMMUNIZATIONS ...................................................................................................................... 40 NEWBORN SERVICES .......................................................................................................................................... 40 OUTPATIENT REHABILITATION ..................................................................................................................... 40 5.17 COORDINATION OF BENEFITS (COB) ........................................................................................ 41 DESCRIPTIONS OF COB PAYMENT METHODOLOGIES .....................................................................41 COB QUESTIONS ......................................................................................................................................................41 EOB or MSN STATEMENT ....................................................................................................................................41 MEMBERS ENROLLED IN TWO HEALTHSPAN PLANS ..................................................................... 42 IMPORTANT COB POINTS TO REMEMBER .............................................................................................. 42 5.17.1 COB Fields on the CMS-1500 Claim Form ................................................................................... 43 5.17.2 COB Fields on the UB-04 Claim Form .......................................................................................... 44 PRIOR PAYMENTS .................................................................................................................................................. 45 INSURED’S NAME.................................................................................................................................................... 45 5.18 EXPLANATION OF PAYMENT (EOP) FORM ............................................................................. 46 HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 3 5.18.1 Explanation of Payment (EOP) Form Field Descriptions .................................................... 46 5.18.2 Sample Explanation of Payment (EOP) Form .......................................................................... 46 5.19 INSTRUCTIONS FOR BILLING SAME/DIFFERENT DATES OF SERVICE & PLACES OF SERVICE TABLE ........................................................................................................................................... 47 HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 4 Section 5: Billing and Payment 5.1 Introduction HealthSpan has developed Section 5 of the Provider Manual for use by all Plan Practitioners/Providers and their staff to: • Educate Practitioners/Providers about HealthSpan’s Claims submission requirements. • Reduce the number of Claim rejections and/or Claim re-submissions because of initial Claim errors. • Facilitate timely payment of Claims. • Simplify and clarify increasingly complex coding/billing requirements. NOTE: HealthSpan will only pay for Covered healthcare Services when HealthSpan Referral and Authorization requirements are met. This policy includes those instances when HealthSpan is the secondary Payor for HealthSpan Medicare Advantage Members. If you have any questions relating to Claims policies and procedures, Claim status Provider Disputes or Appeals, call the HealthSpan Customer Relations Department at 800-441-9742, option 1. We encourage all Plan Practitioners/Providers and their staff to become familiar with the requirements outlined in this Section of the Provider Manual which either conform to or are permitted by applicable federal, state and local regulations. We welcome Plan Provider input as to how we can make this Section of the Manual more useful and informative. Please forward any comments/suggestions for documentation improvements to: HealthSpan Network Development and Performance Department 1001 Lakeside Avenue, Suite 1200 Cleveland, OH 44114 5.2 Key Contacts See Section Two of this HealthSpan Medicare Advantage Provider Manual for a list of Key Contacts by Department. HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 5 5.3 Electronic Data Interchange (EDI) EDI is an exchange of information in a standardized format that adheres to all Health Insurance Portability and Accountability Act (HIPAA) requirements. EDI Claims transactions replace the submission of paper Claims. The Claim Status Inquiry and Notification transactions eliminate the need to telephone HealthSpan to determine the status of an outstanding Claim. The Benefit Coverage and Eligibility Inquiry and Response eliminates the need to telephone HealthSpan to determine a Member’s Eligibility status. 5.3.1 Billing Guidelines for Electronic Claims 5.3.1.1 National Provider Identifier (NPI) National Provider Identifier (NPI): The Health Insurance Portability and Accountability Act of 1996 (HIPAA) mandates that all providers use a standard unique identifier on all standard electronic transactions. Your National Provider Identifier (NPI) must be used on all HIPAA-standard electronic transactions. Electronic Transactions: HealthSpan exchanges the following electronic transactions: Healthspan receives: • 837P - Professional Healthcare Claim • 837I - Institutional Healthcare Claim • 270 - Healthcare Eligibility, Coverage or Benefit Inquiry • 276 - Healthcare Claim Status Request HealthSpan sends: • 999 - Functional Acknowledgement • 835 - Healthcare Claim payment/remittance advice • 270 - Healthcare Eligibility, Coverage or Benefit Information • 277 - Healthcare Claims status Notification • 277U - Unsolicited Healthcare Claim Status Notification 5.3.1.2 Federal Tax Identification Number (TIN) The Federal Tax ID Number as reported on any and all Claim forms must match the information filed with the Internal Revenue Service (IRS). Failure to report the correct Federal Tax ID Number -- as filed with the IRS at the time of incorporation or start of the “business” -- could result in a 28% backup withholding tax (payable to the IRS) and/or the suspension of any and all payments made to the Practitioner/Provider by HealthSpan, until this matter is resolved. HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 6 IRS Form W-9: Request for Taxpayer Identification Number and Certification. When completing IRS Form W-9, note the following: 1) Name This should be the equivalent of your “entity name,” which you use to file your tax forms with the IRS. Sole Practitioner/Proprietor: List your name, as registered with the IRS. Group Practice/Facility: List your “group” or “facility” name, as registered with the IRS. 2) Business Name Leave this field blank, unless you have registered with the IRS as a “Doing Business As” (DBA) entity. If you are doing business under a different name, enter that name here. 3) Address/City, State, Zip Code Enter the address where HealthSpan should mail your IRS Form 1099. 4) Taxpayer Identification Number (TIN) The number reported in this field (either the social security number or the employer identification number) MUST be used on all Claims submitted to HealthSpan. • Sole Practitioner/Proprietor: Enter your taxpayer identification number, which will usually be your social security number (SSN), unless you have been assigned a unique employer identification number (because you are “doing business as” an entity under a different name). • Group Practice/Facility: Enter your taxpayer identification number, which will usually be your unique employer identification number (EIN). If you have any questions regarding the proper completion of IRS Form W-9, or the correct reporting of your Federal Taxpayer ID Number on your Claim forms, call the IRS help line in your area or refer to the following website: irs.gov/Forms-&-Pubs Completed IRS Form W-9 should be mailed to the following address: HealthSpan Network Development and Performance Department 1001 Lakeside Avenue, Suite 1200 Cleveland, OH 44101 HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 7 NOTE: If your Federal Tax ID Number should change, notify the HealthSpan Network Development and Performance Department immediately, so that appropriate corrections can be made to HealthSpan’s records. Failure to do so may delay Claim payment. 5.3.1.3 Coordination of Benefits Explanation of Benefit (EOB) or Medicare Summary Notice (MSN) Required. If HealthSpan is the secondary Payor, send the completed electronic Claim with the payment fields from the primary insurance carrier, as per the X12 requirements. For more information regarding see page 41 5.3.2 Electronic Data Interchange (EDI) Requirements TOPIC BENEFITS OF EDI CLAIMS SUBMISSION INSTRUCTIONS 1) Reduced Overhead Expenses Administrative expenses are reduced; there is no longer a need to print or mail Claims or to call HealthSpan by phone for information. 2) Improved Data Accuracy Since there is no need to re-enter data, data accuracy of Claims is improved, improving Claims payment quality and speed. Both the billing software and the EDI Clearinghouse apply validations to the data that ensure the Claims data is accurate before the Claim is processed. 3) Decreased Claim Turnaround Electronic Claims can be received more quickly than those submitted on paper. Once received, they can be loaded to the Claims processing system more quickly and accurately, enabling a faster turnaround time. HIPPA Requirements EDI ROLES Claims submitted electronically must adhere to all Health Insurance Portability and Accountability Act (HIPAA) requirements. The following websites (listed in alphabetical order) include additional information on HIPAA and electronic loops and segments. If a Practitioner/Provider does not have internet access, HIPAA Implementation Guides can be ordered by calling Washington Publishing Company (WPC) at 301-949-9740. • www.dhhs.gov • www.wedi.org • www.wpc-edi.com 1) Submitter: An EDI submitter is the party sending a transaction. For Claims submission, this is usually the Practitioner/Provider or a billing service submitting Claims on its behalf. 2) Clearinghouse: An intermediary that receives transactions from multiple submitters and sends transactions to the correct recipient. A Clearinghouse may also perform validations and edits on the transactions to ensure their compliance with HIPAA guidelines, or HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 8 TOPIC INSTRUCTIONS EDI ROLES cont. with standards unique to a specific recipient. 3) Recipient: The party receiving a transaction. For Claims submission, this is HealthSpan. UNDERSTANDING ELECTRONIC SUBMISSION PROCESS 1) Practitioners’/Providers’ EDI Responsibilities: A Practitioner/Provider sets up a contract with a Clearinghouse to submit Claims to payers. The Practitioner/Provider enters all of the required data Claims elements and sends all of this information to the contracted Clearinghouse for further data sorting and distribution. The Practitioner/Provider is responsible for ensuring that the transaction complies with the HIPAA requirements and contains all information necessary to process the Claim. 2) Clearinghouse’s EDI Responsibilities: The Clearinghouse receives information from a variety of Practitioners/Providers. The Clearinghouse batches all of the information sorts the information by payer, and then sends the information to the correct payer for processing. The Clearinghouse should ensure the transactions are in compliance with the HIPAA requirements, and may apply unique edits specified by the payer. In addition, Clearinghouses: • Often provide software enabling direct data entry in the Practitioner’s/Provider’s office. • Edit the submitted data so that it is accepted by the payer. • Transmit the data to the correct payer in a standard format NOTE: If a Clearinghouse has a contract with a Practitioner/Provider to process Claims transactions, but does not have a contract with the payer to send that payer Claims transactions, the Clearinghouse will work with other Clearinghouse’s to route the claim to the payer. Therefore, the Clearinghouse to which a Practitioner/Provider submits Claims may not be the same Clearinghouse that delivers those Claims to HealthSpan. 3) HealthSpan’s EDI Responsibilities: HealthSpan receives the EDI information from the Clearinghouse distribution, and loads it into HealthSpan Claims processing system. When Claims are received, HealthSpan prepares an electronic acknowledgement (997 transaction) which is sent to the Clearinghouse. NOTE: A Practitioner/Provider may work with their Clearinghouse to receive HealthSpan’s acknowledgement. When Claims are rejected by HealthSpan for Fatal front-end Errors, HealthSpan returns a Claims status transaction (277U) detailing why the claim was rejected. Rejected Claims may be re-submitted once they are corrected. When Claims are paid, HealthSpan will, if requested, return a payment/remittance advice (835) transaction to the Clearinghouse requested by the provider. HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 9 TOPIC TO INITIATE ELECTRONIC CLAIM SUBMISSIONS INSTRUCTIONS 1) No Registration with HealthSpan is Required for Claims Submission A Practitioner/Provider does not need to register with HealthSpan to submit Claims electronically. It is the Practitioner/Provider’s responsibility to set up a contract with a Clearinghouse to process the Claim submissions. 2) Electronic Payer ID HealthSpan is contracted exclusively with RelayHealth. Relayhealth identifies us using the electronic payor ID RH007 which needs to be populated in loop 2010BB, segment NM109 on all submitted claims. TO INITIATE ELECTRONIC PAYMENT/ REMITTANCE ADVICE 1) Registration Is Required to receive Electronic /Remittance Advice (835) A Practitioner/Provider must register with both their Clearinghouse and HealthSpan to receive a Payment/Remittance Advice (835) transaction when Claims are finalized. 2) Requesting an 835 Registration Form To register for 835, a Practitioner/Provider can: • Go to HealthSpan’s Provider website (healthspan.org/providers/north-coast) and download the registration form. • Call the Network Development Department (Option 4) and request the form. • E-mail the HealthSpan EDI Coordinator ([email protected]) to request the form. Once the form is received by HealthSpan, set-up can take up to two weeks. 3) Paper Remittance Advice Unless requested, HealthSpan will continue to send the Explanation of Payment even when the Electronic Payment/Remittance advice transaction is enabled. TO INITIATE ELECTRONIC FUNDS TRANSFER While not technically an EDI transaction, Electronic Funds Transfer (EFT) or Direct Deposit is also available from HealthSpan. An EFT transaction replaces a paper check for the payment of Claims. Requesting an EFT Authorization Agreement To request an EFT Authorization Agreement , a Practitioner/Provider can: • Go to HealthSpan’s Provider website (healthspan.org/providers/north-coast) and download the form. • Call the Network Development Department (Option 4) and request the form. • E-mail the HealthSpan EDI Coordinator ([email protected]) to request the form. Once the form is received by HealthSpan, set-up and pre-payment testing with the bank can take up to four weeks. HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 10 TOPIC INSTRUCTIONS HEALTHSPAN REQUIREMENTS Additional HealthSpan EDI data requirements are reflected within the HealthSpan EDI Companion Guide, which may be obtained by contacting the Network Development Department (Option #4). Items of note within this document include: • • Unique Provider Per Claim In cases where there are multiple providers for the same Claim, split the Claim by provider and list the individual provider only at the Claim level. HealthSpan Member Identification Number (Medical Record Number) Subscriber vs Patient: Submit Claims using only the patient's information (e.g. name, date of birth, Medical Record Number/ID). Do not use the Subscriber's information. Since each HealthSpan Member has a unique Medical Record Number/ID, they are considered their own Subscriber for electronic transmissions, i.e. patient relationship = self (18). Professional Claims: Institutional Claims: SUPPORTING DOCUMENTATION EDI CLAIM ERRORS CORRECTION & RESUBMISSION FOR ACCEPTED EDI CLAIMS Paper: blocks #1a, 2, 3, 4, 5, 6, 7 EDI: 2010BA Paper: blocks #12, 13, 14, 15, 58, 59, 60 EDI: 2010BA NOTE: Each HealthSpan Member has a unique Member identification number (Medical Record Number). Do not use a parent’s HealthSpan Medical Record Number on a Claim for a child; similarly, do not use a spouse’s Medical Record Number on a Claim for the other spouse. See page 15. All electronic Claim submissions are monitored to ensure that an acceptable percentage of Claims are error-free. HealthSpan will contact the Practitioner/Provider if a high rate of Fatal Errors are detected in their EDI Claim submissions. The error(s) will be analyzed and resolved by working with the Practitioner/Provider office or their billing service. CMS-1500 Claim Forms: (837P) HealthSpan prefers corrections to 837P Claims which were already accepted by HealthSpan to be submitted on paper Claim forms. Corrections submitted electronically may inadvertently be denied as a duplicate Claim. UB-04 Claim Forms: (837I) NOTE: 837I corrections may be submitted electronically Electronic Include the appropriate Type of Bill code when electronically submitting a corrected 837I Claim to HealthSpan for processing. rd NOTE: Claims submitted without the appropriate 3 digit (XXX) in the “Type of Bill” code will be denied. Paper Refer to page 17 for further information and instructions pertaining to paper submission of corrected Claims to HealthSpan for processing. HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 11 5.4 Paper Claims Paper Claims MUST be submitted on one of the following standard Claim forms: CMS-1500 (02/12) Required for all professional services and suppliers. Any professional services (for example, services rendered by radiologists, ER physicians, etc.) should be billed on CMS-1500 Claim forms, unless you are contracted under a GLOBAL rate, in which case “professional services” should not be billed separately. UB-04 Required for all facilities (i.e., hospitals) services. Any professional services (for example, services rendered by radiologists, ER physicians, etc.) should be billed on CMS-1500 Claim forms, unless you are contracted under a GLOBAL rate, in which case “professional services” should not be billed separately. NOTE: Use standard Claim forms formatted with RED ink to ensure maximum compatibility with HealthSpan’s optical scanning equipment. Claim forms formatted with black or blue lines will not scan as efficiently as those formatted with red. 5.4.1 Billing Guidelines for Paper Claims 5.4.1.1 National Provider Identifier (NPI) The Health Insurance Portability and Accountability Act of 1996 (HIPAA) mandates that all providers use a standard unique identifier on all standard electronic transactions. Your National Provider Identifier (NPI) must be used on all HIPAA-standard electronic transactions. 5.4.1.2 Paper Claims Address: HealthSpan P.O. Box 5316 Cleveland, OH 44101 5.4.1.3 Paper Claim Tips Avoid Highlighter Usage/ Use Blue or Black Ink • Do not use a highlighter on any Claims or any attachments to a Claim (for example, a Referral form, EOB statement, etc.). When a Claim form or a Referral form is scanned, highlighter shading turns black and blocks key data under the highlighter. HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 12 • You may use blue or black ink. Align Your Office Printer Correctly • Align your office printer with the fields on the Claim form. Letters and numbers that fall on the lines of the form will not scan clearly. • Verify that the print is clear and dark. If a printer ribbon or cartridge is light, the Claim will not scan clearly and Claims processing will be delayed. Use Paper Clips for Attachments • Do not use staples for attachments. Paper clips are acceptable. Avoid Handwritten Information • Poor, light handwriting affects scanning quality and processing accuracy. Please submit typed Claims. Do Not Use “Super Bills” or “Encounter Forms” as Claim Forms • Office “super bill” or “encounter” forms are NOT acceptable as Claim forms. These forms delay processing because important Claims information is not in the standard format. Send Originals Whenever Possible • Do not submit the second or third page of a multi-part Claim form. The print is often light, smeared, or unreadable. • Avoid the use of photocopies and fax copies as well. One Member per Claim Form/One Provider per Claim Form • Do not bill for different Members on the same Claim form. • Do not bill for different Practitioners/Providers on the same Claim form. Complete a separate Claim form for each Member and for each Practitioner/Provider. Record Each Procedure on a Separate Line • Only one procedure should be reported on a Claim line number. Do not enter two reimbursable procedures under one Claim line. Do Not Record Any “Extraneous” or “Extra” Information on Claim Forms • Do not list the narrative “descriptions” of ICD-9-CM codes, CPT codes, etc. on the CMS-1500 (HCFA-1500) Claim form. Example: 99213 – Office or Other Outpatient Visit Record only the code itself (99213) on the Claim form, without the accompanying narrative description (Office or Other Outpatient Visit). • Do not list any “explanations” or “notes” on Claim forms, unless you are specifically instructed to do so. Exceptions: • Unclassified drugs: Specify the name of the drug and the NDC#. • Durable Medical Equipment (DME) special supplies: Specify the durable medical equipment/supply used. HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 13 5.4.1.4 Federal Tax Identification Number (TIN) The Federal Tax ID Number as reported on any and all Claim forms must match the information filed with the Internal Revenue Service (IRS). Failure to report the correct Federal Tax ID Number -- as filed with the IRS at the time of incorporation or start of the “business” -- could result in a 28% backup withholding tax (payable to the IRS) and/or the suspension of any and all payments made to the Practitioner/Provider by HealthSpan, until this matter is resolved. IRS Form W-9: Request for Taxpayer Identification Number and Certification When completing IRS Form W-9, note the following: 1) Name This should be the equivalent of your “entity name,” which you use to file your tax forms with the IRS. • Sole Practitioner/Proprietor: List your name, as registered with the IRS. • Group Practice/Facility: List your “group” or “facility” name, as registered with the IRS. 2) Business Name Leave this field blank, unless you have registered with the IRS as a “Doing Business As” (DBA) entity. If you are doing business under a different name, enter that name here. 3) Address/City, State, Zip Code Enter the address where HealthSpan should mail your IRS Form 1099. 4) Taxpayer Identification Number (TIN) The number reported in this field (either the social security number or the employer identification number) MUST be used on all Claims submitted to HealthSpan. • Sole Practitioner/Proprietor: Enter your taxpayer identification number, which will usually be your social security number (SSN), unless you have been assigned a unique employer identification number (because you are “doing business as” an entity under a different name). • Group Practice/Facility: Enter your taxpayer identification number, which will usually be your unique employer identification number (EIN). HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 14 If you have any questions regarding the proper completion of IRS Form W-9, or the correct reporting of your Federal Taxpayer ID Number on your Claim forms, call the IRS help line in your area or refer to the following website: irs.gov/Forms-&-Pubs Completed IRS Form W-9 should be mailed to the following address: HealthSpan Network Development and Performance Department 1001 Lakeside Avenue, Suite 1200 Cleveland, OH 44101 NOTE: If your Federal Tax ID Number should change, notify the Healthspan Network Development and Performance Department immediately, so that appropriate corrections can be made to HealthSpan’s records. Failure to do so may delay Claim payment. 5.4.1.5 Coordination of Benefits If HealthSpan is the secondary Payor, send the completed Claim form with a copy of the corresponding Explanation of Benefit (EOB) or Medicare Summary Notice (MSN) from the primary insurance carrier attached to the paper Claim to ensure efficient processing/adjudication. HealthSpan cannot process a Claim without an EOB or MSN from the primary insurance carrier. If you are submitting a paper Claim for more than one Member on the same MSN, attach a copy of the MSN to each Claim form being submitted. CMS-1500 claim form Complete Field 29 (Amount Paid) UB-04 claim form Complete Field 54 (Prior Payments) See page 41 for additional information regarding Coordination of Benefits, and for a list of the specific COB fields which must be completed to ensure accurate COB payment determinations. NOTE: Upon a Member’s appointment check in, verify if there have been any changes to the insurance coverage. This could include more than one coverage. 5.5 Supporting Documentation To expedite Claims processing and adjudication, a Practitioner/Provider should submit supporting written documentation (for example, copies of pertinent medical records) with certain types of Claims. HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 15 Supporting Documentation Submitted WITH a Claim: When supporting documentation is submitted WITH the corresponding paper Claim form, attach/secure the documentation to the paper Claim with a paper clip (do not staple) and mail to HealthSpan’s mailing address (see page 12 in this section). Supporting Documentation Submitted SEPARATELY From a Claim: • When sending supporting documentation SEPARATELY from the Claim (for example, when sending in requested medical information for a pended Claim) 1) Complete a Supporting Documentation Cover Sheet (see sample and instructions on page 17) for each Member for whom you are submitting paper documentation. 2) Attach the cover sheet to each Member’s paper documentation with a paper clip. 3) Mail the supporting documentation as per the instructions on the form. For electronic Claim submissions, complete a Supporting Documentation Cover Sheet (see page 17 for additional information and complete instructions) to submit supporting written documentation. Exception: Coordination of Benefits. ATTACHMENT ADMITTING NOTES CONTRACTUAL REQUIREMENTS IN THE GLOBAL CONTRACT EXPLANATION OF BENEFITS/ MEDICARE SUMMARY NOTICE ITEMIZED BILL OFFICE/PHYSICIAN NOTES CIRCUMSTANCE Except in the case of Emergency Services rendered in accordance with Prudent Layperson guidelines, if the Claim is for inpatient services provided outside of the time or scope of the Authorization. Documents referenced in global contract between HealthSpan and a health care Practitioner, hospital, or person entitled to reimbursement. To determine HealthSpan liability when another health plan and/or Medicare is primary for medical coverage. Except in the case of Emergency Services rendered in accordance with Prudent Layperson guidelines, if the claim is for services rendered in a hospital and the hospital claim has no prior authorization for an admission or the admission is inconsistent with a HealthSpan concurrent review determination rendered prior to the delivery of services, regarding the medical necessity of the service. Except in the case of Emergency Services rendered in accordance with Prudent Layperson guidelines, if the claim for services provided is outside of the time or scope of the authorization, or when there is an authorization in dispute. HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 16 ATTACHMENT OFFICE VISIT NOTES/ ANESTHESIA RECORDS CIRCUMSTANCE If the claim includes modifier 21 or 22. If the claim for anesthesia services rendered includes modifier P4 or P5. OPERATIVE NOTES If the claim is for multiple surgeries, or includes modifier 22, 58, 62, 66 or 78. 5.5.1 Supporting Documentation Cover Sheet See Appendix F.13. 5.6 Claim Corrections Professional Claims: NOTE: HealthSpan prefers corrections to 837P Claims which were already accepted by HealthSpan to be submitted on paper Claim forms. Corrections submitted electronically may inadvertently be denied as a duplicate Claim. 837P Electronic Claims Ensure you include the correct Claim Frequency code is populated in Loop 2300, segment CLM05-3 to indicate the void or replacement claim. CMS-1500 Form Paper Claims When submitting a corrected CMS-1500 paper Claim to HealthSpan for processing: 1) Write “CORRECTED CLAIM” in the top (blank) portion of the standard Claim form. 2) Attach a copy of the corresponding page of HealthSpan’s Explanation of Payment (EOP) to each corrected Claim, to prevent these Claims from being rejected by HealthSpan as duplicate Claims. Attach with a paper clip. 3) Mail the corrected Claim(s) to HealthSpan using the standard Claims mailing address (see page 12 in this section). Institutional Claims: When submitting a corrected Institutional Claim to HealthSpan for processing: 387I Claims Ensure you include the appropriate Claim Frequency Code is populated in Loop 2300, segment CLM05-03 to indicate a void or replacement claim. HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 17 5.7 Claim Submission Timeframes Initial Claim Submissions: All Claims must be submitted for processing within 12 months (365 days) of the date of service. Any Claims submitted after 12 months (365 days) from the date of service must be accompanied by documentation as to why the Claims should be considered for payment. Complete a Supporting Documentation Cover Sheet (see sample and instructions on page 17) and attach the documentation with a paper clip. Claims submitted without this documentation will be denied. Payment consideration for Claims filed/appealed after filing limit: Examples of documentation deemed valid are: 1. Documented call into the HealthSpan Network Development or Customer Relations Departments: Provide the date that you contacted HealthSpan inquiring about a Claim status or payment rejection. If you followed up with an appropriate HealthSpan area, we will have documentation of that call and will be able to accept that in order to determine if the filing limit rejection will be overturned. Follow up calls in relation to a previous payment must occur within 180 days of the last processed date. This would be considered as proof of filing. 2. Fax Confirmation: Provide a copy of a fax confirmation sheet showing the fax was successful, detailing that you faxed a Claim over for processing or reconsideration. This would be considered as proof of filing. 3. HealthSpan EDI Claim Receipt Confirmation: HealthSpan assigns all Claims received a HealthSpan Claim number whether they are received via paper or electronically. Upon receipt, the claims system generates a confirmation back to the submitter with the Claim number, in a 999. This would be considered as proof of filing. 4. Copy of delivery confirmation from U.S. Postal Service or Commercial Carrier (i.e. UPS, FedEx….): If you have a delivery confirmation from a package submitted to HealthSpan as it relates to Claims involved in a timely filing dispute, we will consider that receipt as proof of filing. 5.8 Claim Processing Timeframes Clean Claims: Allow 30 days for HealthSpan to process and adjudicate your Claim(s). Claims requiring additional supporting documentation and/or Coordination of Benefits may take longer to process. HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 18 NOTE: While HealthSpan may require the submission of specific supporting documentation necessary for benefit determination (including medical and/or Coordination of Benefits information), HealthSpan may have to make a decision on the Claim before such information is received. A "complete” or “clean" Claim is defined as a Claim that has no defect or impropriety, including lack of required substantiating documentation from providers, suppliers, or Members or particular circumstances requiring special treatment that prevents timely payments from being made on the Claim. 5.9 Incorrect Claim Payments If you receive an incorrect payment (i.e., either an overpayment or an underpayment), do one of the following: Option 1: Do not cash or deposit the incorrect payment check. • Mail the incorrect payment check back to HealthSpan, along with a copy of the Explanation of Payment (EOP) and a brief note explaining the payment error to: HealthSpan Recovery Unit P.O. Box 74843 Cleveland, OH 44194-4843 NOTE: If HealthSpan’s EOP is not available, record the Member’s Medical Record Number on the payment check you are returning. • HealthSpan will re-issue and mail you a new, corrected payment check within 30 days. Option 2: Deposit the incorrect HealthSpan payment check in your account or accept the Electronic Funds Transfer (EFT). For an Underpayment Error: Call the HealthSpan Customer Relations Department at 800-441-9742, option 1, and explain the error. Upon verification of the error, appropriate corrections will be made to HealthSpan’s accounting system and the underpayment amount owed you will be added to/reflected in your next HealthSpan reimbursement check. For an Overpayment Error: You may do either one of the following: Write a refund check to HealthSpan for the excess amount paid to you by HealthSpan. Attach a copy of HealthSpan’s Explanation of Payment (EOP) to your refund check, as well as a brief note explaining the error. Attach with a paper clip. HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 19 NOTE: If HealthSpan’s EOP is not available, record the Member’s Medical Record Number on the payment check you are returning. Mail your refund check (and brief note) to: HealthSpan Recovery Unit P.O. Box 74843 Cleveland, OH 44194-4843 Appropriate corrections will be made to HealthSpan’s accounting system and the overpayment amount will be automatically deducted from your next HealthSpan reimbursement. 5.10 Provider Payment Disputes See Section 4.14 of this HealthSpan Medicare Advantage Provider Manual. 5.11 Provider Appeals See Section 4.12.4 of this HealthSpan Medicare Advantage Provider Manual. 5.12 Member Hold Harmless A Practitioner/Provider should not bill a Member for a Covered Service that is not the responsibility of the Member under the Evidence of Coverage, such as an amount denied by HealthSpan because of inaccurate coding or the Practitioner’s/Provider’s failure to obtain an Authorization. The Practitioner/Provider may bill for Copayments, Coinsurance amounts, subject to the Deductible or amounts the Member has expressly agreed to pay prior to the services being rendered. HealthSpan Payments: The payments from HealthSpan shall be limited to the amount specified in the Practitioner’s/Provider’s Agreement with HealthSpan, less any Copayments, Coinsurance, or Deductibles in accordance with the Member’s specific Evidence of Coverage. Items You May Bill For: The Practitioner/Provider may bill the Member for any applicable Copayments, Coinsurance, or Deductibles, and/or for any non-covered services as indicated on the remittance advice received from HealthSpan. HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 20 5.13 Coding and Billing Validation HealthSpan uses code editing software (CES) from third party vendors to assist in determining the appropriate processing and reimbursement of Claims. Currently, HealthSpan has selected Optum™ for CES. From time to time, HealthSpan may change this coding editor or the specific rules that it uses in analyzing Claims submissions. HealthSpan’s goal is to help ensure the accuracy of Claims payments. Optum’s CES is a code editor application designed to evaluate Claims data including procedure codes and associated modifiers. CES assists HealthSpan in identifying various categories of Claims coding and possible inconsistencies. Claims with coding errors/inconsistencies are pended to the Medical Claim Review staff for manual review. Each Claim is validated against HealthSpan’s payment criteria, and then is subsequently released for processing. This process has a goal of improving the accuracy of coding and consistency in Claims payment procedures. To help illustrate how this process works, examples have been provided. If you have questions about the application of these rules, call the HealthSpan Customer Relations Department at 800-441-9742, option 1. 5.13.1 CODING RULE DESCRIPTIONS EDIT RULE # / NAME #1 MULTIPLE PROCEDURS REDUCTION CODING RULE DESCRIPTIONS / RULE JUSTIFICATION Rule Description: Identifies procedures that require a reduction based on multiple procedure guidelines. Rule Justification: American Medical Association (AMA) guidelines establish that certain procedures require the billing of the multiple procedure modifiers. Any procedure included in Appendix D or E of the Current Procedural Terminology book are exempt and not included in this list of procedures. Rule Application: Use all procedures in the surgical section (10021 – 69990) from the Current Procedural Terminology book to determine procedure codes that will accept the multiple modifier. Any codes the AMA has designated to be “Add-On” codes or “Modifier 51 Exempt” will not be considered. • • Multiple surgeries are indicated by use of modifier 51 The primary procedure is identified by the highest total RVU as set by the Centers for Medicare & Medicaid Services (CMS). Example: Multiple surgeries are separate procedures performed by a Practitioner/Provider on the same patient at the same operative session or on the same day. HealthSpan will reimburse for multiple procedures performed during the same operative session according to the following schedule: HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 21 EDIT RULE # / NAME #1 MULTIPLE PROCEDURS REDUCTION cont. #2 OUTPATIENT CONSULTATIONS CODING RULE DESCRIPTIONS / RULE JUSTIFICATION 1st (major) procedure ………100% of allowed fee, no modifier required 2nd procedure ……………….50% of allowed fee, modifier 51 required 3rd procedure ………………..50% of allowed fee, modifier 51 required 4th procedure ………......……50% of allowed fee, modifier 51 required Each procedure after the fourth procedure will require submission of documentation and HealthSpan review, to determine an appropriate reimbursement amount. Rule Description: Identifies office or other outpatient consultations that should have been billed at the appropriate level of office visit, established patient, or subsequent hospital care. Rule Justification: According to the AMA, "A consultation is a type of service provided by a physician whose opinion or advice regarding evaluation and/or management of a specific problem is requested by another physician or other appropriate source." Furthermore, "If subsequent to the completion of the consultation, the consultant assumes responsibility for the management of a portion or all of the patient's condition[s], the follow-up consultation codes should not be used." Rule Application: • Deny the consultation with the reason code indicating the denial reason. • Match on the first three digits of an ICD9 code to determine same diagnosis. Definition: A non-initial consultation is a consultation billed with a date of service within 6 months of another consultation. #4 INITIAL INPATIENT CONSULTATIONS Example: Office or other outpatient consultation codes (99241-99245) are services provided by a Practitioner/Provider whose opinion or advice regarding evaluation and/or management of a specific problem is requested by another physician. These consultation services should be performed at the written or verbal request of another Practitioner/Provider and documented in the patient's medical record. If the consulting Practitioner/Provider assumes responsibility for the management of a portion or all of the patient's condition, the follow-up visits should be coded using the established patient office evaluation and management codes. 99241 DOS 1/5/13 Dx Code of 250.30 99241 DOS 3/1/13 Dx Code of 250.30 Service for DOS 3/1/13 will be denied. Rule Description: Identifies initial inpatient consultations that should have been billed at the appropriate level of subsequent hospital care. Rule Justification: According to the AMA, "A consultation is a type of service provided by a physician whose opinion or advice regarding evaluation and/or management of a specific problem is requested by another physician or other appropriate source." Furthermore, "If subsequent to the completion of the consultation, the consultant assumes responsibility for the management of a portion or all of the patient's condition[s], the follow-up consultation codes should not be used." Rule Application: AMA/CPT industry standard of payment is followed for HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 22 EDIT RULE # / NAME #4 CODING RULE DESCRIPTIONS / RULE JUSTIFICATION paying initial inpatient consultations, only when they are truly the initial. INITIAL INPATIENT CONSULTATIONS cont. Example: A consultation is a type of service provided by a Practitioner/Provider whose opinion or advice regarding evaluation and management of a specific problem is requested by another Practitioner/Provider. CPT states that only one initial consultation should be reported by a Consultant per admission utilizing the initial inpatient consultation codes (99251-99255). #5 Rule Description: Identifies consultation codes that are billed by the Member's Primary Care Physician (PCP). CONSULTATIONS BY PRIMARY CARE PHYSICIANS (PCP) #6 NEW PATIENT CODE FOR ESTABLISHED PATIENT Rule Justification: According to the AMA, "A consultation is a type of service provided by a physician whose opinion or advice regarding evaluation and/or management of a specific problem is requested by another physician or other appropriate source.” Rule Application: All consultations will be denied when billed by the Member’s PCP, except for Claims submitted with a pre-op diagnosis (V72.81-V72.85) when appropriate. Rule Description: Identifies new patient procedure codes that are submitted for established patients. Rule Justification: According to the AMA "A new patient is one who has not received any professional services from the physician or another physician of the same specialty who belongs to the same group practice, within the past three years." Rule Application: • Deny with a reason code indicating the denial reason when a Practitioner/Provider bills more than one new patient code for the same Member. • In addition, same group, same specialty within the 3 years will be denied. • The time period is three (3) years to determine if the visit is for a new patient. Example: Member ID 1234 DOS 1/5/14 99201 This service will be denied. Member ID 1234 DOS 12/20/12 99201 This service will be approved. #7 GLOBAL SURGICAL PACKAGE (GSP) Rule Description: Identifies Evaluation & Management (E/M) or certain supply codes billed within a procedure’s follow-up period. Rule Justification: The Centers for Medicare & Medicaid Services (CMS) guidelines have established that the concept of the Global surgical package applies to certain procedures. Additional payment should not be made for services that fall within the follow-up days. Rule Application: • Deny E/M codes and supplies billed within the Global surgical package for surgeries with Global periods of 10 or 90 days. • Use Modifiers 22, 24, 25, 27, 50,51,52,53,54,55,57,58,59,62,78,79,80,82 HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 23 EDIT RULE # / NAME #7 GLOBAL SURGICAL PACKAGE (GSP) cont. #8 SAME DAY SURGERY INCLUSIVE CODING RULE DESCRIPTIONS / RULE JUSTIFICATION and AS, if applicable. Example: A Global surgical package is an all-inclusive fee for the surgical procedure which includes the surgery and some pre-operative and postoperative care. Below outlines types of Global surgical packages and what each package includes. Major Surgery: The following services are included in the Global surgical package: • Pre-operative visit/services, in or out of the hospital, one day prior to surgery all intra-operative procedures medical/surgical services for complications which DO NOT require a return trip to the Operating Room all related post-operative care and visits, for a period of 90 days following surgery Minor Surgery: The following services are included in the Global surgical package: • The Practitioner’s/Provider’s visit/services performed on the day of surgery the procedure itself all related post-operative care and visits, for a period of ten days after surgery Endoscopic Procedures: For endoscopic procedures, the Global "package" includes: • The Practitioner’s/Provider’s visit/services on the day of the procedure, • The procedure itself, • There is NO post-operative period for endoscopic procedures performed through an existing body orifice; procedures requiring an incision for insertion of a scope (for example, a laparoscopic cholecystectomy) will be subject to either the MAJOR or MINOR surgical policy, whichever is appropriate. Rule Description: Identifies supplies that have been submitted on the same day as a surgical procedure. Rule Justification: According to the Centers for Medicare & Medicaid Services (CMS) Program Manuals - Medicare Carriers (PUB. 14), guidelines have established that additional payment should not be made for some supplies when billed on the same day as certain surgical procedures. This list includes, but is not limited to, "Items such as dressing changes; local incisional care; removal of operative pack; removal of cutaneous sutures and staples, lines, wires, tubes, drains, casts, and splints; insertion, irrigation and removal of urinary catheters, routine peripheral intravenous lines, nasogastric and rectal tubes; and changes and removal of tracheostomy tubes.” Rule Application: Deny supplies when billed on the same day as a surgery. HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 24 EDIT RULE # / NAME #9 OPTUM™ BUNDLING # 10 CMS CORRECT CODING INITIATIVE BUNDLING CODING RULE DESCRIPTIONS / RULE JUSTIFICATION Rule Description: Identifies procedures that have been unbundled according to the Optum’s CES product. Rule Justification: The Optum’s CES product has identified re-bundling coding relationships. Coding relationships are established and influenced by CPT Code definitions, CPT Instructions and Guidelines, Medicare Guidelines and Physician Specialty Organizations. Edit level justifications are available upon request. Rule Application: Use Optum edits for all Claims. Definition: Procedure unbundling occurs when two or more CPT-4 procedures are used to describe a procedure performed, when a single, more comprehensive, CPT-4 procedure code exists that accurately describes the entire procedure performed or when mutually exclusive procedures (procedures which would not be reasonably performed at the same session by the same provider on the same Member) are reported. Example: Billing the following two codes together: 58150 Total abdominal hysterectomy (corpus and cervix) with or without removal of tubes; with or without removal of ovary(s). 58240 Pelvic exenterating for gynecologic malignancy with total abdominal hysterectomy or cervicectomy with or without removal of tube(s); with or without removal of ovary(s). 58150 would be rebundled into 58240. Rule Description: Identifies procedures that have been unbundled according to the Correct Coding Initiative (CCI) of the Centers for Medicare & Medicaid Services (CMS). Rule Justification: The correct coding initiative coding policies are based on coding conventions defined in the American Medical Association's CPT manual, national and local policies and edits, coding guidelines developed by national societies, analysis of standard medical and surgical practice and review of current coding practice. Rule Application: • Use CMS CCI edits for all Claims. • Deny the code with the lowest work RVU for mutually exclusive procedures • Apply the Correct Coding Initiative modifier overrides 25, 58, 59, 78, 79, E1-E4, F1-F9, FA, LC, LD, LT, RC, RT, T1-T9, and TA if appropriate. Definition: Procedure unbundling occurs when two or more CPT-4 procedures are used to describe a procedure performed, when a single -- more comprehensive -- CPT-4 procedure code exists that accurately describes the entire procedure performed or when mutually exclusive procedures (procedures which would not be reasonably performed at the same session by the same provider on the same Member) are reported. Example: Billing the following two codes together: 58150: Total abdominal hysterectomy (corpus and cervix) with or without removal of tubes; with or without removal of ovary(s). 58240: Pelvic exenteration for gynecologic malignancy with total abdominal hysterectomy or cervicectomy with or without removal of tube(s); with or without removal of ovary(s). 58150 would be rebundled into 58240. HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 25 EDIT RULE # / NAME # 11 CMS ALWAYS BUNDLED PROCEDURES # 12 ANESTHESIA CROSSWALK # 13 HOLIDAY CODING RULE DESCRIPTIONS / RULE JUSTIFICATION Rule Description: Identifies procedures indicated by the Centers for Medicare & Medicaid Services (CMS) as always bundled when billed with any other procedure. Rule Justification: According to CMS National Physician Fee Schedule Relative Value File, this procedure has a status code indicator of "B", which is defined as: "Payment for covered services is always bundled into payment for other services not specified. There will be no RVUs or payment amount for these codes and no separate payment is made. When these services are covered, payment for them is subsumed by the payment for the services to which they are incident." Rule Application: Deny services indicated by CMS as always bundled when billed with any other procedure not indicated as always bundled. Rule Description: Identifies and crosswalks non-anesthesia services to a designated anesthesia code as appropriate based on the provider's specialty. Rule Justification: The Optum Anesthesia Crosswalk Table converts E/M, surgery, radiology, laboratory/pathology, and medicine codes to anesthesia codes as appropriate when a Claim for anesthesia services, as identified by provider type, specialty, or identification number is submitted with other than a designated anesthesia code (00100–01996). Rule Application: • Use Optum’s crosswalk list to crosswalk any non-anesthesia codes billed by an anesthesiologist to the appropriate anesthesia code and deny with anesthesia reason code. • For non-anesthesia codes that have a “one to many” crosswalk, flag the code for review and deny anesthesia with denial reason code. • For non-anesthesia codes that do not have an established crosswalk, flag the code for review and deny anesthesia with denial reason code. Example: Code 10080 would be denied because the anesthesia code of 00300 is a valid crosswalk. Rule Description: Identifies misuse of procedure codes designated for Federal holidays or Sundays. Rule Justification: According to the AMA, this procedure code has been defined as "Services requested on Sundays and holidays in addition to basic service." The date of service on this line is not a Federal holiday or a Sunday. Rule Application: Deny code 99050 when it is NOT billed on a Sunday or Federal holiday. Example: A provider billed 99050 and the date of service is not 12/31/2015 or 12/25/2015. # 14 GENDER/AGE SPECIFIC CODES Rule Description: Identifies procedures and diagnoses that are inconsistent with the Member's gender or which are inconsistent with the Member’s age. Rule Justification: The Optum CES product has identified this procedure or diagnosis as gender specific. The Optum CES product also edits the Member HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 26 EDIT RULE # / NAME # 14 GENDER/AGE SPECIFIC CODES cont. # 15 PROCEDURES NOT COVERED CODING RULE DESCRIPTIONS / RULE JUSTIFICATION age for inconsistent for stated diagnosis codes. The procedure code or diagnosis on this line is not consistent with the Member's gender or age. Rule Application: Use Optum’s list to deny any Claim lines with procedures or diagnoses that are inconsistent with the Member’s gender or age. Rule Description: Identifies procedure codes that are typically not covered by the plan. Rule Justification: The Centers for Medicare & Medicaid Services (CMS) guidelines or industry accepted standards establish that certain procedures are not covered by the plan. In regards to CMS not covered services, procedures with a Status Indicator of E, G, I, N, P, or X in the National Physician Fee Schedule Relative Value File are included in this list of procedures. Rule Application: Deny procedure codes that are not covered. Services not covered by CMS and which are covered by HealthSpan are excluded from this rule. # 16 Rule Description: Identifies procedure codes that are "unlisted." UNLISTED PROCEDURE RULE Rule Justification: The Optum CES product has identified procedure codes that contain phrases in their descriptions such as “not elsewhere specified” or “not otherwise specified”. Rule Application: Pend for review CPT codes that are unlisted procedures. # 17 DUPLICATE LINE ITEMS Definition: An unlisted procedure is a "catch all" code for a procedure that cannot be assigned a more specific procedure code. These procedures are identified in CPT-4 with the word "unlisted" in the procedure code’s description. Example: Unlisted musculoskeletal procedure, head (21499). Clinical Review staff will review all Claims with an unlisted procedure code listed on the Claim form. After a detailed review of the Claim -- and any required supporting documentation -Clinical Review staff may be able to assign a more specific CPT code to the procedure. Rule Description: Identifies line items that have been submitted on a previous Claim. Rule Justification: Duplicate claim lines match a previous Claim's Member, Practitioner/Provider, procedure code, modifier, date of service, quantity, and billed amount. Rule Application: • Deny the Claim line based on a match on Member ID, procedure code, Provider ID or vendor Federal Tax Identification Number, date of service, requested amount, quantity and modifier. • An exact match is not required on Evaluation and Management CPT Codes. HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 27 EDIT RULE # / NAME # 18 PROFESSIONAL/ TECHNICAL CODES VS. MODIFIERS CODING RULE DESCRIPTIONS / RULE JUSTIFICATION Rule Description: Identifies situations where a modifier 26, denoting professional component, should have been reported for the procedure performed at the noted place of service. Rule Justification: The Centers for Medicare & Medicaid Services (CMS) guidelines establish that certain procedures, when performed in certain settings, require the billing of the professional component modifier. Procedures with a "PCTC Ind" indicator of 1 or 6 in the National Physician Fee Schedule Relative Value File are included in this list of procedures. Rule Application: • Add the professional component (modifier 26) when an applicable procedure is performed in a facility setting by a non-hospital Provider. • Use CMS’s list of procedures that will accept technical/professional component split. # 19 INVALID ASSISTANT SURGEON Rule Description: Identifies surgical procedures billed with an assistant surgeon modifier that typically do not require an assistant surgeon. Rule Justification: The Centers for Medicare Services (CMS) guidelines establish that certain procedures do not warrant an assistant surgeon. Procedures with an "Asst. Surg" indicator of 1 or 9 in the National Physician Fee Schedule Relative Value File are included in this list of procedures. Rule Application: Use CMS’s list to identify codes that typically do not require an assistant surgeon in the procedure, but have an assistant surgeon modifier attached, and deny those procedures. Definition: An assistant at surgery is defined as an individual who assists the primary surgeon during surgery. An assistant at surgery can be another physician, a physician’s assistant (PA), or a qualified resident. Example: CMS has identified a list of procedures which require the skills of an assistant surgeon. HealthSpan reviews all "assistant surgeon" Claims to determine the appropriateness of the assistant surgeon’s services. HealthSpan uses physician consultants, as well as current, publicly available assistant surgeon guidelines (CMS). # 20 FILING DEADLINES Rule Description: Identifies Claim lines that have been submitted after the filing deadline. Rule Justification: According to the Centers for Medicare & Medicaid Services (CMS) Program Manuals - Medicare Carriers (PUB. 14), "the terms of the law require that the Claim be filed no later than the end of the calendar year following the year in which the service was furnished, except as follows: The time limit on filing Claims for service furnished in the last 3 months of a year is the same as if the services had been furnished in the subsequent year. Thus, the time limit on filing Claims for services furnished in the last 3 months of the year is December 31 of the second year following the year in which the services were rendered." HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 28 EDIT RULE # / NAME # 20 FILING DEADLINES cont. CODING RULE DESCRIPTIONS / RULE JUSTIFICATION Rule Application: • The decision is to compare the date of service to the received date to determine whether a Claim has been filed on time. Contracted Providers • Deny Claims submitted beyond the HealthSpan initial Claims submission of 12 months from date of service. Non Contracted Providers • # 21 INVALID / DELETED CODES Deny Claims submitted beyond the CMS filing deadline. Rule Description: Identifies procedures codes invalid or deleted by the AMA received after the Centers for Medicare & Medicaid Services (CMS) submission guidelines. Rule Justification: The Centers for Medicare & Medicaid Services (CMS) guidelines have established that AMA deleted CPT and HCPCS codes should not be reimbursed when they are submitted after the procedure code's deletion and beyond the permitted submission period. A valid procedure code is one that is present in the system and is effective. Rule Application: If a Claim line has a date of service in the current year, CMS permits a three-month grace period (based on the date the Claim is received). When a Claim is received beyond the grace period, deny the code. # 22 ADD-ON CODES # 23 BILATERAL Example: 33035 - Complete ventricular decortication, with cardiopulmonary bypass (Code deleted in 1990; to report, use 33031). Rule Description: Identifies an add-on code billed without the presence of a primary service/procedure. Rule Justification: According to the AMA, "add-on codes are always performed in addition to the primary service/procedure, and must never be reported as a stand-alone code." The indicated add-on procedure has been identified because this provider has not billed its related primary service/procedure for this Member on the same date of service. Rule Application: Deny add-on codes when billed without the appropriate base code. Example: 11000 (Base Code) billed with 11001 (Add-on) Rule Description: Identifies the same surgical code being billed twice without the appropriate use of modifier 50. Rule Justification: When performed bilaterally, the same surgical procedure should not be billed twice. HealthSpan’s reimbursement guidelines require the code to be billed on one line with a bilateral modifier indicated. Rule Application: • Modify lines for bilateral procedures that are submitted incorrectly. • The decision determines an incorrect submission by the presence of the same surgical code billed twice for the same date of service. HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 29 EDIT RULE # / NAME # 23 BILATERAL cont. CODING RULE DESCRIPTIONS / RULE JUSTIFICATION Definition: Bilateral procedures are surgeries performed on both sides of the body during the same operative session or on the same day. Example: If two codes are billed, and both have a -50 modifier, the Plan will pay one line with the -50 modifier accordingly, and deny one line. First (bilateral) procedure: Report the appropriate 5-digit CPT code, which describes the bilateral procedure, with a modifier -50 as required. Second (bilateral) procedure: The same 5-digit CPT code for the second procedure will be denied. # 25 BASE CODE QUANTITY Example: A bilateral mastectomy should be reported as follows: 19303 (Mastectomy, simple, complete) Add Modifier 50. Rule Description: Identifies situations where a Practitioner/Provider is billing a primary service/procedure with a quantity greater than one, rather than billing the appropriate add-on code(s). Rule Justification: When a Practitioner/Provider is billing a primary service/procedure with a quantity greater than one, those additional services beyond the primary service/procedure should be billed as add-on codes. According to the AMA, add-on procedures are to be listed in addition to the primary service/procedure. Rule Application: Deny base codes when billed with a quantity greater than one. #26 PLACE OF SERVICE NOT TYPICAL FOR PROCEDURE Rule Description: Identifies claim lines that contain a specified procedure performed in a place of service inconsistent with Centers for Medicare & Medicaid Services (CMS) guidelines. Rule Justification: According to CMS the service location and procedure code information used by physicians/practitioners/suppliers to report the name, address and Zip code of the service location where they furnished services (e.g., hospital, clinic, or office). Furthermore, the service location is used by contractors to determine the applicable “locality” and Geographic Practice Cost Index. Rule Application: If a claim contains procedures which are performed at a place of service that is inconsistent with CMS guidelines those claim lines will be denied. Example: Procedure code 99231 Subsequent hospital care is not typically performed in Place of Service 11 (Physician Office). #27 MEDICARE NONPHYSICIAN SERVICE Rule Description: This edit identifies claim lines that contain a certain place of service (hospital Inpatient, hospital Outpatient, or nursing facility residents) and a PC/TC status indicator of 5. These procedures typically are not performed by a physician. HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 30 EDIT RULE # / NAME #27 MEDICARE NONPHYSICIAN SERVICE CODING RULE DESCRIPTIONS / RULE JUSTIFICATION Rule Justification: According to Centers for Medicare & Medicaid Services (CMS), CPT or HCPCS codes with PC/TC indicators of 0, 2, 3, 4, 5, 7, 8, and 9 are not considered eligible for reimbursement when submitted with modifiers 26 and/or TC. Rule Applications: Deny procedures when performed by a physician. Example: Procedure Code 92977 does not require a physician to perform the procedure and therefore is not considered eligible for reimbursement when submitted with modifiers 26 and/or TC. 5.14 Do Not Bill Events (DNBE) HealthSpan’s DNBE policy is based on payment rules that waive fees for all or part of health care services directly related to the occurrence of certain adverse events as defined by the Centers for Medicaid and Medicare Services (CMS) National Coverage Determinations for surgical errors and the published listing of CMS Hospital Acquired Conditions, as may be amended from time to time. The DNBE policy will apply to all Claims for all Members enrolled in HealthSpan. HealthSpan expects Plan Providers to report every DNBE as set forth in Section 8.31 of this HealthSpan Medicare Advantage Provider Manual. Waive or Reimburse Fees – Plan Providers may not be compensated for Services directly related to any Do Not Bill Event (as defined below) and may be required to waive Member Cost Share associated with, and hold Members harmless from, any liability for Services directly related to DNBE. Plan Providers shall waive fees otherwise owed by Payors and Members (or reimburse such fees that may have already been paid by Payors or Members) that are directly related to the DNBE, whether the DNBE is reported by the Plan Provider or later discovered by HealthSpan. “Directly related” fees mean fees associated with the Medically Necessary health care Services required to treat the DNBE, taking into account all relevant factors. Surgical Do Not Bill Events include the following surgical errors (SEs) identified by CMS in its National Coverage Determinations (NCD) that occur in any care setting: • • • Wrong surgery or other invasive procedure performed on patient. Surgery or other invasive procedure performed on wrong patient. Surgery or other invasive procedure performed on wrong body part. HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 31 The Hospital Acquired Conditions (HAC) identified by CMS that occur in a general hospital or acute care setting are as follows: • Intravascular air embolism that occurs while being cared for in a health care facility. • Blood incompatibility (hemolytic reaction due to administration of ABO/HLA incompatible blood or blood products). • Pressure ulcer (stage three or four) acquired after admission to a health care facility • Falls and Trauma (fractures, dislocations, intracranial injuries, crushing injuries, burns, electric shock). • Catheter associated urinary tract infection. • Vascular catheter associated infection. • Manifestation of poor glycemic control (diabetic ketoacidosis, nonketotic hyperosmolar coma, hypoglycemic coma, secondary diabetes with ketoacidosis, and secondary diabetes with hypersmolarity). • Mediastinitis following coronary artery bypass graft. • Surgical site infection following orthopedic procedures (spine, neck, shoulder, elbow). • Surgical site infection following bariatric surgery for obesity (laparoscopic gastric bypass, gastroenterostomy, laparoscopic gastric restrictive surgery). • Deep vein thrombosis or pulmonary embolism following orthopedic procedures (total knee or hip replacement). • Any new HAC later added by CMS. In any care setting, the following HAC if not present on admission for inpatient services or if not present prior to provision of other Services: • Removal (if medically indicated) of foreign object retained after surgery (RFO). 5.14.1 Claims Submission Related to a Do Not Bill Event HealthSpan will follow the Centers for Medicare & Medicaid Services (CMS) billing requirements for Services directly related to a DNBE. Institutional – If you submit a UB-04 or 837I claim for inpatient facility Services to a Member wherein a HAC (including a RFO) has occurred, you must include the following information: Present on Admission (POA) indicators, applicable diagnostic (ICD) codes and all applicable standard modifiers (including CMS National Coverage HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 32 Determination (NCD) modifiers for Surgical Errors) in the manner required by CMS for Medicare fee-for-service Claims. Submit Services directly related to a DNBE as a no-pay Claim (Type of Bill 110). If there are also unrelated Services provided during the same stay as the DNBE, you must split the Claim and submit both a no-pay Claim (Type of Bill 110) setting forth all Services directly related to the DNBE including the applicable ICD codes, present on admission indicators and all standard modifiers (including CMS National Coverage Determination modifiers for Surgical Errors) in the manner required by CMS for Medicare fee-for-service Claims and a Type of Bill ‘11X’ (with the exception of 110)’ setting forth all Covered Services not directly related to the DNBE. Professional– If you submit a CMS 1500 form or 837P claim for any inpatient or outpatient professional Services provided to a Member wherein a SE or RFO has occurred, you must include the applicable ICD codes and all applicable standard modifiers (including CMS NCD HCPCS modifiers for Surgical Errors) for the associated charges on all lines related to the surgical error in the manner required by CMS for Medicare fee-for-service Claims as follows: PA: Surgery on Wrong Body Part. PB: Surgery on Wrong Patient. PC: Wrong Surgery on Patient. Additionally, any claim submission should reflect all Services provided (including those related to a DNBE) and all associated fees (including those related to the DNBE) with an adjustment in fees to reflect the waiver of fees directly related to the DNBE. 5.15 Anesthesia HealthSpan provides coverage for anesthesia services that are Medically Necessary as part of authorized medical or surgical care in accordance with the Member’s Evidence of Coverage. TOPIC EXPLANATION/INSTRUCTIONS GLOBAL ANESTHESIA PACKAGE The “Global” anesthesia package includes: • The performance of a pre-anesthetic examination and evaluation (even if the exam is done on a date different from the date of surgery). • The administration of the anesthetic. • The administration of fluids and/or blood Incidental to the HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 33 TOPIC GLOBAL ANESTHESIA PACKAGE cont. EXPLANATION/INSTRUCTIONS delivery of anesthesia (or the procedure being performed). • The usual monitoring services (ECG, blood pressure, etc.). The provision of post-operative anesthesia care (post-operative visit). OFFICE-BASED SURGICAL PROCEDURES When an office-based surgical procedure is performed, reimbursement for the procedure includes reimbursement for anesthesia services as part of the Global surgical Fee, because it is expected that appropriate anesthesia will be administered with the office-based procedure. ANESTHESIA REPORTING REQUIREMENTS & REIMBURSEMENT HealthSpan reimburses participating providers for anesthesia services based on nationally recognized criteria for reporting of anesthesia services, including: • The American Medical Association (AMA) CPT codes (00100 – 01999). • American Society of Anesthesiologists’ (ASA) Relative Value Guide (RVG). • Medicare Guidelines. BASE UNITS: Providers are NOT to indicate the ASA base unit values in the Days/Units field on the Centers for Medicare & Medicaid Services (CMS) 1500 (Field 24, Box G). Base units are determined as defined by the American Society of Anesthesiologists Relative Value Guide. The base units assigned to a procedure are intended to demonstrate the relative complexity of a specific procedure and include the value of all anesthesia services, except the value of the actual time spent administering the anesthesia. HealthSpan stores the base unit value within our Claims system and will calculate the anesthesia payment of the base units according to the information provided on the Claim. REPORTING OF ANESTHESIA TIME: Anesthesia time begins when the anesthesiologist starts to prepare the patient for the induction of anesthesia in the operating room or in an equivalent area. Anesthesia time ends when the anesthesiologist is no longer in personal attendance, which is when the patient may be safely placed under postoperative supervision. Time units are calculated by allowing 1 unit for each 15 minute interval or remaining fraction thereof. Providers are to show time as follows. Paper: Providers are to show time as total number of minutes in the Units field (Item 24, Box G). EDI: 837 Professional Claim Service Line - Unit or Basis for Measurement Loop: 2400 Segment: SV103 HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 34 TOPIC EXPLANATION/INSTRUCTIONS ANESTHESIA REPORTING REQUIREMENTS & REIMBURSEMENT cont. Description: For claims requiring minutes, such as Anesthesia claims, submit using the qualifier of "MJ" to denote minutes in loop 2400 SV103. Example: Submitted claim line with 100 minutes. SV1*HC:01967*12.25*MJ*100****1:2:3**N~ REIMBURSEMENT: Payment for most anesthesia services is based on: • The base unit value. • Plus anesthesia time units. • Multiplied by the fee schedule conversion factor, as appropriate. Other services are reimbursed based upon the CPT code. MULTIPLE SURGICAL PROCEDURES: When multiple surgical procedures are performed during a single anesthetic administration, the anesthesia code representing the most complex with the multiple procedure modifier “-51“ is reported. The time reported is the combined total of all procedures reported on the primary procedure. EXCEPTIONS TO BILLING ANESTHESIA CODES Anesthesiologists should bill using anesthesia codes only, unless one or more of the following services was performed by the anesthesiologist (in which case the appropriate “non-anesthesia” CPT code(s) may be reported and billed in accordance with Centers for Medicare & Medicaid Services (CMS) guidelines): • Evaluation and management services. • Hospital inpatient services. • Consultations. • Critical care services. • Pain management. • Nerve blocks. Destruction by neurolytic agents. • Services not included in the Global anesthesia Fee. • Other miscellaneous services. QUALIFYING CIRCUMSTANCES: CPT codes 99100, 99116, 99135 and 99140 represent various patient conditions that may impact the anesthesia service provided. Such codes may be billed in addition to the anesthesia being billed. Charges for these codes are to be shown on the same line as the CPT Qualifying Circumstances Code in Field 24, Box F on the CMS-1500. PATIENT-CONTROLLED ANALGESIA (PCA): Benefits may be available for the administration of patient-controlled analgesia (PCA) following a surgical procedure. PCA billed by a surgeon is covered as part of the Global surgical package and is not separately reimbursable. PCA reimbursements are limited to anesthesiologists only. An anesthesiologist’s services for PCA should be submitted as a single line HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 35 TOPIC EXPLANATION/INSTRUCTIONS EXCEPTIONS TO BILLING ANESTHESIA CODES cont. on the claim form as follows: • Span the dates to include the entire care for the PCA (reimbursement will be made as a Global allowance, and will include the entire course of PCA). • Any “hospital care” provided by the anesthesiologist subsequent to the initial day of PCA will be considered covered under the Global PCA Fee. • Use CPT code 01996 when billing for PCA services. CONSCIOUS SEDATION: Sedation with or without analgesia (conscious sedation), CPT codes 9914399145, are considered eligible for reimbursement when billed by an anesthesiologist, pain management or certified registered nurse anesthetist ANESTHESIA MODIFIERS Personally Performed or Medically-Directed/Supervised Anesthesia Services: Use an appropriate HCPCS anesthesia modifier to denote whether the anesthesia services were personally performed, medically directed, or medically supervised: AA - Anesthesia service performed personally by the Anesthesiologist. AD - Medical supervision by a physician of more than four concurrent procedures. G8 - Monitored anesthesia care (MAC) for deep complex complicated, or markedly invasive surgical procedures. G9 - Monitored anesthesia care for patient who has a history of severe cardio-pulmonary condition. QK - Medical direction of two, three, or four concurrent anesthesia procedures involving qualified individuals. QX - CRNA service with medical direction by a physician. QY - Medical direction of one CRNA by anesthesiologist QZ - CRNA service without medical direction by a physician. QS - Monitored anesthesia care service (can be billed by a CRNA or a physician). GC - These services have been performed by a resident under the direction of a teaching physician. Physical Status Modifiers: As indicated in the CPT book, the following Physical Status modifiers should be appended to the CPT anesthesia code to distinguish between the various levels of complexity of the anesthesia service(s) provided: P1 - A normal healthy patient. P2 - A patient with mild systemic disease. HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 36 TOPIC EXPLANATION/INSTRUCTIONS ANESTHESIA MODIFIERS cont. P3 - A patient with severe systemic disease. P4 - A patient with severe systemic disease that is a constant threat to life. P5 - A moribund patient who is not expected to survive without the operation. P6 - A declared brain-dead patient whose organs are being removed for donor purposes. DO NOT enter additional minutes for the Physical Status modifier. If eligible for reimbursement, the additional unit(s) will be calculated by our Claims system. The patient cannot be billed for Physical Status modifiers not allowed by HealthSpan. Other CPT Modifiers/Qualifying Circumstances Codes: Other modifiers and “qualifying circumstances” codes may be used as appropriate. Follow the instructions in the CPT/HCPCS books when reporting these additional modifiers and/or codes. 5.16 Additional Services TOPIC EXPLANATION/INSTRUCTIONS BEHAVIORAL HEALTH SERVICES Description: Behavioral health procedures are used to identify the psychological, behavioral, emotional, cognitive, and social factors in relation to the prevention, treatment, or management of behavioral health problems. CMS-1500 Field 24d CPT codes are required for all professional services. Record the code for the predominant service only when performing psychiatric health assessment/ intervention on the same date as psychiatric therapeutic procedures. UB-04 • Field 14 Required for all inpatient behavioral health Claims • Field 44 For outpatient services, enter the appropriate HCPCS/CPT code that corresponds to the Revenue Code in Field 42. Supporting Documentation for Behavioral Health Claims: • Unlisted Procedure Codes: Any behavioral health claims which contain any “unlisted,” “unclassified,” “unspecified” or “miscellaneous” CPT or HCPCS procedure codes. Repeated procedures performed on the SAME date of service require supporting documentation. HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 37 TOPIC EXPLANATION/INSTRUCTIONS DURABLE MEDICAL EQUIPMENT (DME) Description: Durable Medical Equipment is medically necessary equipment that is: • Appropriate for use at home. • Primarily and customarily used to service a medical purpose. • Not useful to a person in absence of an illness. • Able to withstand repeated use. CMS-1500 • Field 24d CPT codes are required for all professional services. Use HCPCS Level II codes to define DME. Use modifiers, if applicable. UB-04 EVALUATION/ MANAGEMENT (E/M) SERVICES • Field 42 Enter the appropriate revenue code. • Field 44 HCPCS/Rates required. • Field 46 Number of rental months. • Field 54 DME cost sharing amounts collected from the Member. • Field 80 For DME billing, rental rate costs and anticipated months of usage. CMS-1500 • Field 19 When “covering” for another physician, enter the name of the physician you are covering for. NOTE: If a non-participating Practitioner/Provider will be covering for you in your absence, notify that individual of this requirement. Inpatient E/M Services: If a patient is admitted for observation following the performance of a major/minor “surgical package” procedure, do not report hospital observation service codes, because all post-operative E/M services are included as part of the Global surgical package. Consultations: • HealthSpan will reimburse for initial consultations when billed with any surgical procedure done on the same day of service. • For office/outpatient: If the consultant assumes patient management responsibilities following the initial consultation, office E/M (established patient) visit codes should be used for all subsequent patient encounters, NOT office consultation codes. • For inpatient: If the consultant assumes patient management responsibilities, use subsequent hospital care codes (NOT follow-up inpatient consultation codes) to report all additional E/M encounters with the patient. Surgery and E/M Services: • Reimbursement will generally NOT be made for a pre- or postoperative E/M visit provided on the same day as major/minor surgery, or an endoscopic procedure, unless HealthSpan agrees that there was a significant, separately identifiable E/M service provided HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 38 TOPIC EVALUATION/ MANAGEMENT (E/M) SERVICES cont. EXPLANATION/INSTRUCTIONS in addition to the procedure. In these instances, the provider must bill for the E/M visit using the appropriate modifier. • If E/M services are performed during the post-operative period for a reason unrelated to the original procedure (such as for other disease or injuries), you may bill for these services using modifier 24 (Unrelated E/M service by the same physician during a postoperative period), and you must list a corresponding diagnosis code which reflects that the E/M services were for a problem other than the surgical diagnosis. Urgent or Emergency Services Provided in the Office: For urgent or Emergency Services provided in the office setting, use code Office services provided on an Emergency basis in addition to the appropriate E/M office visit code. Because CPT procedure codes series are considered to be adjunct services to the basic services provided, HealthSpan will reimburse providers for BOTH the E/M visit code and “Emergency Services” code. Non-Surgical Procedure that Include E/M Services: There are certain instances where HealthSpan will deny medical visits when billed with certain non-surgical procedures, because the codes for these procedures include admission to the hospital and/or daily visits. The nonsurgical procedures which fall into this category include: • Clinical brachytherapy. • End stage renal disease services. • Allergy immunotherapy services. Preventive Medicine Services: Preventive medicine codes -- NOT office evaluation/management codes -should be used to report the routine evaluation and management of adults and children, in the absence of patient complaints. For example, preventive medicine codes should be used for: EMERGENCY ROOM (ER) SERVICES • Well-baby checkups. • Routine pediatric visits. • Camp or school physicals. • Routine, annual gynecological exams. UB-04 • Field 15 Enter the code indicating the source of the admission or outpatient registration • Field 44 The emergency department E/M visit codes should ONLY be used if the patient is seen in the emergency department. For urgent or Emergency Services provided in the office setting, bill code 99058 (Office services provided on an emergency basis) in addition to the appropriate E/M office visit code. Emergency department E/M visit codes should be used for E/M services provided in the emergency department, even if these were “nonemergency” services. The only requirement for using “emergency department” codes is that the patient must be registered in the emergency department. Office visit E/M codes should be used if the patient is seen in HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 39 TOPIC EXPLANATION/INSTRUCTIONS EMERGENCY ROOM (ER) SERVICES cont. the ER as a convenience to the physician and/or patient, but the patient is not registered in the emergency department. NOTE: If both an “emergency department” physician and an “attending” physician are involved in admitting a patient from the ER, the ER physician should bill for his services utilizing the emergency department E/M codes, and the attending physician should bill for his services using the initial hospital visit codes. The two physicians cannot each bill for both the ER services rendered and the hospital admission. INJECTIONS/ IMMUNIZATIONS CPT codes are required for all professional services. Use HCPCS Level II codes to define Injections/ Immunizations. NOTE: If there was no identifiable E/M service rendered by the nurse or the provider, and the patient received only an injection during the encounter, it is permissible to report an injection administration code in lieu of the E/M visit code and the appropriate HCPCS code (specifying the drug administered). Unlike injections, immunization procedures include the supply of materials. Additionally, injection administration fees are not eligible for reimbursement when billed with immunization codes. NEWBORN SERVICES CMS-1500 • OUTPATIENT REHABILITATION Field 2 Enter the first and last name of the newborn. • Field 3 Enter the newborn’s date of birth. The Claim must include one of the following modifiers to distinguish the discipline of the plan of care under which the service was delivered for therapy, even if the code is not recognized by Centers for Medicare & Medicaid Services (CMS) as requiring a therapy modifier; such as 97014 or 97545: • • • GN- Services delivered under an outpatient speech-language pathology plan of care. GO- Services delivered under an outpatient occupational therapy plan of care. GP- Services delivered under an outpatient physical therapy plan of care. This is applicable to all claims from physicians, non-physician practitioners, hospitals and skilled nursing facilities. Modifiers GN, GO, and GP refer only to services provided under plans of care for physical therapy, occupational therapy and speech-language pathology services. The inclusion of these modifiers will assist HealthSpan in applying the correct benefits as part of Claims adjudication for Claims for outpatient rehabilitation services. HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 40 5.17 Coordination of Benefits (COB) Coordination of Benefits is a way of determining the order in which benefits are paid and the amounts which are payable when a claimant is covered under more than one plan. It prevents duplication of benefits when an individual is covered by multiple plans providing benefits or services for medical, dental or other care and treatment. NOTE: HealthSpan will only pay for Covered healthcare Services when HealthSpan Referral and Authorization requirements are met. This policy includes those instances when HealthSpan is the secondary Payor for HealthSpan Medicare Advantage Members. HealthSpan follows the National Association of Insurance Commissioners (NAIC) model regulations for coordinating benefits, except in those instances where the NAIC model regulations differ from Ohio state Law. Ohio state Law supersedes the NAIC model regulations. TOPIC EXPLANATION / INSTRUCTIONS DESCRIPTIONS OF COB PAYMENT METHODOLOGIES HealthSpan Coordination of Benefits allows benefits from multiple carriers to be added on top of each other so that the Member receives the full benefits from their primary carrier and the secondary carrier pays their entire benefit up to 100% of allowed charges. Benefit carve-out calculations are based on whether or not the provider accepts Medicare assignment for the provider contract corresponding to the Claim. Medicare assignment means the provider has agreed to accept the Medicare Allowed Amount as payment. COB QUESTIONS If you have any questions relating to the Coordination of Benefits, call the HealthSpan Customer Relations Department at 800-444--9742, option 1. EOB or MSN STATEMENT Whenever HealthSpan is the SECONDARY Payor, Claims can be submitted EITHER electronically or on one of the standard paper Claim forms: • Electronic Claims If HealthSpan is the secondary Payor, send the completed electronic Claim formatted per the Implementation Guide’s direction on Provider to Payer COB. • Paper Claims If HealthSpan is the secondary Payor, send the completed Claim form with a copy of the corresponding Explanation of Benefit (EOB) or Medicare Summary Notice (MSN) from the primary insurance carrier attached to the paper claim to ensure efficient claims processing/adjudication. HealthSpan will deny a Claim without an EOB or MSN from the primary insurance carrier. CMS-1500 claim form Complete Field 29 (Amount Paid). UB-04 claim form Complete Field 54 (Prior Payments). HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 41 TOPIC EXPLANATION / INSTRUCTIONS MEMBERS ENROLLED IN TWO HEALTHSPAN PLANS Some Members may be enrolled under two separate plans offered through HealthSpan (dual coverage). In these situations, standard COB rules still apply. Example: A married couple both work for a company that offers HealthSpan to its employees. Both the husband and wife enroll in HealthSpan as Subscribers and each lists the other as a dependent spouse and each lists their children as dependent children. Practitioners/Providers should submit one claim under the primary plan to HealthSpan for processing. After we pay under the primary plan, HealthSpan will then process and pay the second claim under the secondary plan. IMPORTANT COB POINTS TO REMEMBER COB ANNUAL UPDATES HealthSpan reviews and updates Coordination of Benefits information annually (by contacting Members as required), in an attempt to maintain upto-date COB records. BIRTHDAY RULE HealthSpan follows the “birthday rule”, which states that the insurance carried by the parent/Subscriber whose birthday falls earlier in the calendar year will be the primary Payor for a dependent child who is covered by two different insurances (for example, when a dependent child is covered BOTH by an insurance carried by the dependent’s mother, as well as under a different insurance carried by the dependent’s father). Example: Parent A: Date of Birth: 03/06/1948. This coverage is primary. Parent B: Date of Birth: 07/20/1948. This coverage is secondary. NOTE: In rare cases both parents may have the same birth date. In these cases the plan that has been in effect the longest is the primary carrier. DEPENDENT CHILD OF SEPARATED OR DIVORCED PARENTS • Divorce Decree/Court Order If specific terms of a court decree state that one of the parents is responsible for the healthcare expenses of a child, and the entity obligated to pay or provide benefits of the plan of that parent has actual knowledge of those terms, the benefits of that plan are determined first. The Member may be required to submit a copy of their court order or divorce decree. In the absence of a divorce decree/court order stipulating parental healthcare responsibilities for a dependent child, insurance benefits for that child are applied according to the following order: Insurance carried by the 1) Natural parent with custody pays first 2) Step-parent with custody pays next 3) Natural parent without custody pays next 4) Step-parent without custody pays last. If the parents have joint custody of the dependent child, then benefits are applied according to the birthday rule referenced above. HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 42 5.17.1 COB Fields on the CMS-1500 Claim Form The following fields should be completed on the CMS-1500 Claim form, to ensure timely and efficient Claims processing. Incomplete, missing, or erroneous COB information in these fields may cause Claims to be denied or pended and reimbursements delayed. For electronic Claim submissions, refer to a HIPAA website for additional information on electronic loops and segments (suggested websites on page 8 in this section). FIELD NUMBER 9 FIELD NAME INSTRUCTIONS/EXAMPLES OTHER INSURED’S NAME When additional insurance coverage exists (through a spouse, parent, etc.) enter the LAST NAME, FIRST NAME, and MIDDLE INITIAL of the insured. NOTE: This field must be completed when there is an entry in Field 11d (Is There Another Health Benefit Plan?). 9a OTHER INSURED’S POLICY OR GROUP NUMBER Enter the policy and/or group number of the insured individual named in Field 9. If you do not know the policy number, enter the Social Security number of the insured individual. NOTE: 1: Field 9a must be completed when there is an entry in Field 11d (Is There Another Health Benefit Plan?). 2. For each entry in this field, there must be a corresponding entry in 9d (Insurance Plan Name or Program Name). 9b OTHER INSURED’S DATE OF BIRTH/SEX Enter date of birth and sex, of the insured named in Field 9. The date of birth must include the month, day, and FOUR DIGITS for the year (MM/DD/YYYY). Example: 01/05/1971 NOTE: This field must be completed when there is an entry in Field 11d (Is There Another Health Benefit Plan?). 9c EMPLOYER’S NAME or SCHOOL NAME Enter the name of the employer or school name (if a student), of the insured named in Field 9. NOTE: This field must be completed when there is an entry in Field 11d (Is There Another Health Benefit Plan?). 9d INSURANCE PLAN NAME or PROGRAM NAME Enter the name of the insurance plan or program, of the insured individual named in Field 9. NOTE: This field must be completed when there is an entry in Field 11d (Is There Another Health Benefit Plan?). 10 IS PATIENT’S CONDITION RELATED TO: a. Employment? b. Auto Accident? Check “yes” or “no” to indicate whether employment, auto liability, or other accident involvement applies to one or more of the services described in Field 24. NOTE: If yes, there must be a corresponding entry in Field HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 43 FIELD NUMBER 10 cont. FIELD NAME c. Other Accident? PLACE (State) 11d IS THERE ANOTHER HEALTH BENEFIT PLAN? INSTRUCTIONS/EXAMPLES 14 (Date of Current Illness/ Injury) and in Field 21 (Diagnosis). PLACE (State) Enter the state the Auto Accident occurred in. Check “yes” or “no” to indicate if there is another health benefit plan. (For example, the patient may be covered under insurance held by a spouse, parent, or some other person). NOTE: If “yes,” then Field Items 9 and 9a-d must be completed. 14 21 DATE OF CURRENT • Illness (First symptom) • Injury (Accident) • Pregnancy (LMP) Enter the date of the current illness or injury. The date must include the month, day, and FOUR DIGITS for the year (MM/DD/YYYY). DIAGNOSIS OR NATURE OF ILLNESS OR INJURY Enter the diagnosis and if applicable, enter the Supplementary Classification of External Cause of Injury and Poisoning Code. Example: 01/05/2004 NOTE: This field must be completed when there is an entry in Field 10 (Is The Patient’s Condition Related To). 29 AMOUNT PAID Enter the amount paid by the primary insurance carrier in Field 29. 5.17.2 COB Fields on the UB-04 Claim Form The following fields should be completed on the UB-04 Claim form to ensure timely and efficient Claims processing. Incomplete, missing, or erroneous COB information in these fields may cause Claims to be denied or pended and reimbursements delayed. For additional information, refer to the current UB-04 National Uniform Billing Data Element Specifications Manual. For electronic Claim submissions, refer to a HIPAA website for additional information on electronic loops and segments (suggested websites on page 8 in this section). FIELD NUMBER 31-36 (UB-04) FIELD NAME INSTRUCTIONS/EXAMPLES OCCURRENCE CODE/DATE Enter the appropriate occurrence code and date defining the specific event(s) relating to the Claim billing period. NOTE: If the injuries are a result of an accident, complete Field 77 (E-Code) on the UB-04. You can include the ecode in Field 81 (Code-Code). HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 44 FIELD NUMBER 50 54 FIELD NAME INSTRUCTIONS/EXAMPLES PAYOR (Payer Identification) Enter the name and number (if known) for each Payor organization from whom the provider expects (or has received) payment towards the bill. List payers in the following order on the claim form: A = primary Payor. B = secondary Payor. C = tertiary Payor. PRIOR PAYMENTS Enter the amount(s), if any, that the provider has received toward payment of the bill PRIOR to the billing date, by the indicated payer(s). List prior payments in the following order on the Claim form: A = primary payer. B = secondary payer. C = tertiary payer. INSURED’S NAME Enter the name (Last Name, First Name) of the individual in whose name insurance is being carried. List entries in the following order on the Claim form: A = primary payer. B = secondary payer C = tertiary payer. (Payers and Patient) 58 NOTE: For each entry in Field 58 , there MUST be corresponding entries in Fields 59 through 62 and 65. 59 PATIENT’S RELATION TO INSURED Enter the code indicating the relationship of the patient to the insured individual(s) listed in Field 58 (Insured’s Name). List entries in the following order: A = primary payer. B = secondary payer. C = tertiary payer. 60 INSURED’S UNIQUE ID CERT. – SSN – HIC – ID NO. (Certificate/Social Security Number/Health Insurance Claim/Identification Number) Enter the insured person’s (listed in Field 58) unique individual Member identification number (medical/health record number), as assigned by the payer organization. List entries in the following order: A = primary payer. B = secondary payer. C = tertiary payer 61 GROUP NAME (Insured Group Name) 62 INSURANCE GROUP NO. Enter the name of the group or plan through which the insurance is being provided to the insured individual (listed in Field 58). Record entries in the following order: A = primary payer. B = secondary payer. C = tertiary payer. Enter the identification number, control number, or code assigned by the carrier or administrator to identify the GROUP under which the individual (listed in Field 58) is covered. List entries in the following order: A = primary payer. B = secondary payer. C = tertiary payer. HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 45 FIELD NUMBER 64 FIELD NAME INSTRUCTIONS/EXAMPLES ESC (Employment Status Code of the Insured) Enter the code used to define the employment status of the insured individual (listed in Field 58). Record entries in the following order: A = primary payer. B = secondary payer. C = tertiary payer. NOTE: This field has been deleted from the UB-04 65 EMPLOYER NAME (Employer Name of the Insured) Enter the name of the employer who provides health care coverage for the insured individual (listed in Field 58). Record entries in the following order: A = primary payer. B = secondary payer. C = tertiary payer. 67 A-Q (UB-04) DIAGNOSIS CODE The primary diagnosis code should be reported in Field 67. Additional diagnosis code can be entered in Field 68-76. 72 (UB04) EXTERNAL CAUSE OF INJURY CODE (E-CODE) If applicable, enter an ICD-9-CM “E-code” in this field. 5.18 Explanation of Payment (EOP) Form An EOP is a written statement to a Plan Provider showing action taken on a Claim for a Member. 5.18.1 Explanation of Payment (EOP) Form Field Descriptions Reserve for future use. 5.18.2 Sample Explanation of Payment (EOP) Form Reserved for future use. HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 46 5.19 Instructions for Billing Same/Different Dates of Service & Places of Service Table NOTE: Only one Practitioner/Provider and one Member may be listed on a claim form. If DATE(S) of SERVICE are: AND PLACE(S) of SERVICE are: AND SERVICE(S) Are: Number of Claims to SUBMIT: Explanation And Instructions Different Different Related Two Separate Claims Different Unrelated Two Separate Claims If a Practitioner/Provider renders care/treatment to a Member on DIFFERENT dates of service in DIFFERENT places of service, the Practitioner/Provider must submit a SEPARATE Claim form for each different place of service, reflecting the services/ treatment rendered in each location. If a Practitioner/Provider renders care/treatment to a Member on the SAME date in two DIFFERENT places of service, for UNRELATED diagnoses, the practitioner/ provider may submit a SEPARATE claim for each different place of service reflecting the services/ treatment rendered in each location. Same Same Different Related Two Separate Claims Example(s) If a Practitioner/Provider sees a Member on the SAME day in DIFFERENT locations for RELATED diagnoses/ services, these services should be billed on SEPARATE Claim forms. If a Practitioner/Provider sees a Member in his OFFICE on 1/2/04, and then a few days later sees the Member in the HOSPITAL on 1/5/04 – ONE claim should be submitted for the OFFICE visit, and another (separate) claim should be submitted for services rendered in the HOSPITAL. If a Practitioner/Provider sees a Member early in the day in his OFFICE for a routine physical, and then later that same day sees the Member in the HOSPITAL because the Member was stung by a bee and suffered a severe allergic reaction -- ONE claim may be submitted for the OFFICE visit and another (SEPARATE) Claim may be submitted for the unrelated services rendered in the HOSPITAL. Do NOT bill separately for E/M services (office visit, hospital observation service, nursing facility visit, etc.) provided on the SAME DATE as a hospital admission. All E/M services provided by the physician in conjunction with a Member’s admission are considered part of the initial hospital care when provided on the SAME DATE as the hospital admission. Do not bill separately for emergency department E/M codes when the Member is admitted directly from the ER. HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 47 If DATE(S) of SERVICE are: AND PLACE(S) of SERVICE are: AND SERVICE(S) Are: Different Same Related Number of Claims to SUBMIT: Explanation And Instructions One Claim If the Practitioner/Provider sees the Member on DIFFERENT dates but at the SAME place of service/location (i.e., hospital, physician’s office, etc.) – these services may be billed on ONE Claim form, with each different date of service listed as a separate line on the form, along with the corresponding diagnosis code(s), procedure code(s), and charges. Example(s) 1) If a Practitioner/Provider sees a Member in his OFFICE on 2/2/04 and then a few days later sees the Member in his OFFICE on 2/5/04 – list each date of service as a separate line on ONE Claim form, along with the diagnosis, procedure code(s), and corresponding charge relating to each date of service. 2) If a physical therapist renders services to a Member on 3/2, 3/4, and 3/6 at the same location for each date of service, list each date of service as a SEPARATE line on the Claim form, along with the corresponding service/procedure code, diagnosis, and charge relating to each date of service. Same (multiple on same day) Same Related or Unrelated One Claim If a Practitioner/Provider sees the SAME Member two or more times on the SAME day, in the SAME location (i.e., hospital, physician’s office, etc.) – these services should be billed on ONE Claim form. 1) If a Practitioner/Provider sees the Member in the HOSPITAL early in the day, and then LATER that SAME day sees the Member in the HOSPITAL again to monitor the Member’s progress/ condition-- only ONE Claim form should be submitted for both hospital visits, with all services billed at the cumulative level of intensity for both visits. 2) If the Member is seen TWICE in the OFFICE on the SAME day for UNRELATED problems/diagnoses, these services should be billed as separate lines on ONE Claim form. HealthSpan Integrated Care Medicare Advantage Provider Manual Section 5: Billing and Payment January 2015 48







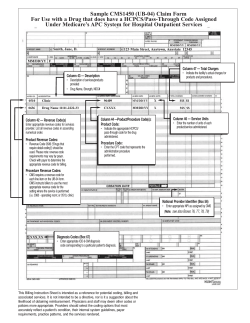


© Copyright 2026