
Document 4388
Apoptotic Retinal Cell Death Induced by Antirecoverin
Autoandbodies of Cancer-Associated Retinopathy
Grazyna Adamus* MichalMachnicki* and GailM. Seigel~\
Purpose. Recoverin has been identified as a target autoantigen for antirecoverin antibodies
found in the sera of some patients with cancer-associated retinopathy. The aim of this study
was to investigate the role of antirecoverin antibodies in cancer-associated retinopathy.
Methods. Human, rat, and rabbit antirecoverin antibodies were purified using a recoverinaffinity column. Purified biotinylated antibodies were cultured with recoverin-positive rat
retinal cells E1A.NR3. Antibody uptake by retinal cells in vitro was analyzed by immunocytochemistry. Cytotoxic effect of antibodies on retinal cells was measured by the MTT colorimetric
method. Apoptosis was shown by the ladder DNA fragmentation method and by fluorescent
dye chromatin fragmentation analysis.
Results. Antirecoverin antibodies obtained either from sera from five cancer-associated retinopathy patients or from sera of immunized animals were internalized by E1A.NR3 cells. Only
specific, antirecoverin antibodies produced destruction of the cells in a dose- and time-dependent manner. Normal immunoglobulin G did not have such effects on retinal cells. No
additional cell destruction was observed in the presence of complement as compared with
cultures incubated with antirecoverin antibodies alone. Internucleosomal DNA fragmentation
and presence of apoptotic cells was observed throughout the culture treated with recoverinspecific antibodies but not with normal antibodies. Cells not expressing recoverin (Y79, PCI 2,
and GH3) were not susceptible to cell destruction because of antirecoverin antibody action.
Conclusions. These studies showed that antibodies specific to recoverin are able to enter and
cause death of cells expressing recoverin. In humans, autoandbodies originally elicited against
recoverin expressed in tumor cells may damage retinal photoreceptors and play a role in the
pathogenesis of cancer-associated retinopathy. Results suggest that autoantibody to recoverin,
when given access to recoverin in the retina through the blood-retina barrier, could initiate
photoreceptor degeneration leading to blindness. Such mechanism may be common for other
paraneoplastic disorders or autoimmune diseases where antibodies interfere with the normal
cell physiology. Invest Ophthalmol Vis Sci. 1997;38:283-291.
V>»ancer-associated retinopathy (CAR) is a paraneoplastic blinding disease, in which retinal degeneration occurs in the presence of systemic tumor growth.1
Over the past few years, progress has been made toward understanding the involvement of the immune
response in the cause and pathogenesis of neurologic
disorders associated with systemic cancer.2 It has been
From the *R.S. Dow Neurological Sciences Institute, Legacy-Good Samaritan
Hospital and Medical Center, Portland, Oregon; and the fDepartment of
Neurobiology and Anatomy, University of Rochester School of Medicine and
Dentistry, New York.
Supported by grants N1H EY10316 (CA) and EY10676 (GMS).
Submitted for publication April 16, 1996; revised October 7, 1996; accepted October
8, 1996.
Proprietary interest category: N.
Reprint requests: Grazyna Adamus, R.S. Dow Neurological Sciences Institute, 1220
NW 20 Avenue, Portland, OR 97209.
Investigative Ophthalmology & Visual Science, February 1997, Vol. 38, No. 2
Copyright © Association for Research in Vision and Ophthalmology
proposed that expression of tumor antigens and their
release during tumor turnover and necrosis can lead
to an immunologic response that then recognizes the
same or similar antigen in the nervous system. Effects
of cancer on the visual system, often including complete loss of vision, consist of marked attenuation of
the electroretinogram, blurred vision, night blindness,
impaired color vision, central or ring scotomas, constriction of visual fields, and iritis. In most cases, small
cell carcinoma of the lung, gynecologic malignancies,
and breast carcinomas are involved in the paraneoplastic syndrome.
CAR syndrome is thought to be mediated by autoantibodies specific to retinal antigens such as recoverin, a photo receptor-specific calcium-binding pro-
283
284
Investigative Ophthalmology & Visual Science, February 1997, Vol. 38, No. 2
tein. It has been established that some patients diagnosed with CAR possess high titers of circulating
autoantibodies against recoverin.3"5 Because visual
symptoms may occur before neoplastic disease is diagnosed or before recurrence is recognized, detection
of antirecoverin autoantibodies can help to diagnose
cancer.
Considerable new information is now available
about the possible role of recoverin in the development of CAR. High antirecoverin autoantibody titers
are associated with loss of vision, and steroid treatment
temporarily can stabilize progressive loss of vision. Our
knowledge of a potential pathogenicity of recoverin
has been strengthened by the use of purified recoverin
to induce the degeneration of photoreceptors in Lewis
rats.6'7 We and others also have shown that the tumor
tissue from patients with CAR selectively expresses recoverin that reacts with patients' own autoantibodies.8'9 This raises the possibility that the expressed recoverin, if released, can trigger the autoimmune responses that lead to the degeneration of the retina.
However, there is little information for the direct role
of such antibodies in the pathogenicity of CAR. In this
study, we examined the role of antirecoverin antibodies in pathogenic processes. We studied the effect of
antibodies specific to recoverin on retinal cells in vitro.
We showed that the antirecoverin antibodies gain access to cells and subsequently cause cell death through
apoptotic mechanism.
METHODS
Antibody
Human sera containing antirecoverin autoantibodies
were obtained from five patients diagnosed with CAR
syndrome3'8 or from normal subjects without antirecoverin antibodies. The studies were performed in accordance with institution's guidelines and the Declaration of Helsinki on Biomedical Research Involving Human Subjects, and protocols were approved by the
Legacy Institutional Review Board. Animal antirecoverin antisera were produced in New Zealand White
rabbits or Lewis rats by injection of purified retinal
recoverin mixed with complete Freund's adjuvant. All
procedures adhered to the Association for Research
in Vision and Ophthalmology Resolution on Animal
Use in Research. Monoclonal antibody against arrestin
S65-38 was produced in mice immunized with purified
arrestin (Adamus and Hargrave, unpublished data,
1990).
Recoverin Purification
Recoverin was isolated from frozen retinas as described previously.6 To obtain large quantities, recoverin was purified from bacterial cells expressing recov-
erin. Cells containing vector pTrec2 were a gift from
Drs. Lubert Stryer and Sergey Zazulya. Recoverin was
expressed and purified from these cells according to
previously published culture conditions and purification methods.1011
Antibody Purification and Biotinylation
Antirecoverin antibodies were purified using a Sepharose 4B-recoverin affinity column. The affinity column
was prepared by coupling 5-mg recoverin per 1 ml
of CNBr-activated Sepharose 4B (Pharmacia Biotech,
Piscataway, NJ). A serum sample diluted two times
with phosphate-buffered saline (PBS) was loaded and
washed with 10 volumes of starting buffer. Antirecoverin antibodies were eluted with 0.1-M glycine, pH
2.5, and neutralized immediately. The purity of the
immunoglobulin fraction collected was determined by
mini sodium dodecyl sulfate-polyacrylamide gel.12
Protein content was measured by the bicinchoninic
acid method (Pierce, Rockford, IL). Activity of antibody was measured by enzyme-linked immunosorbent
assay using recoverin-coated microplates.6 For biotinylation, purified antibodies were dialyzed against 50mmol sodium carbonate, pH 8.5. For 20 mg of immunoglobulin G (IgG)/l ml, 0.4 mg/0.4 ml of sulfosuccinimidyl-6-(biotinamido) hexanoate (ImmunoPure
NHS-LC-biotin, Pierce, Rockford, IL) was used. The
mixture was incubated for 2 hours at 4°C. Unreacted
biotin was removed by centrifugation using a Cenrticon-30 (Amicon, Beverly, MA) microconcentrator. Activity of biotinylated antibody was tested by enzymelinked immunosorbent assay.
Cell Culture
Immortalized E1A.NR3 rat retinal cells13 were maintained in Dulbecco's modified Eagle's medium
(DMEM) supplemented with 10% fetal bovine serum
(FBS), IX MEM nonessential amino acids, IX MEM
vitamins, and 100 mg/ml gentamicin. Human retinoblastoma cells Y79 (American Type Culture Collection
HTB-18) and rat adrenal pheochromocytoma cells PC12 (American Type Culture Collection CRL-1721)
were maintained in RPMI-1640 medium containing
15% FBS, and rat pituitary tumor cells GH3 (American
Type Culture Collection CCL82.1) were maintained
in DMEM containing 10% FBS. All tissue culture reagents were purchased from Sigma (St. Louis, MO).
Uptake of Antibody by Immunocytochemistry
Cells were allowed to attach to an eight-chamber slide
dish (Nunc 177445) and then cultured in the presence
of human, rat, or rabbit normal or antirecoverin biotinylated antibodies (100 /zg/ml). Twenty-four hours
later, cells were washed and fixed for 10 minutes at
room temperature in 2% paraformaldehyde and permeabilized in 0.25% Triton X-100 for 5 minutes. After
285
Autoantibodies Induce Apoptotic Cell Death
a rinse in PBS, cells were incubated for 1 hour with a
horseradish peroxidase-conjugated streptavidin. The
cells were rinsed in PBS, and color reaction was developed with a diaminobenzidine kit (Pierce, Rockford,
IL). Negative control specimens consisting of cells cultured without antibodies were processed simultaneously with experimental cells.
DNA Analysis
Cells (2 X 105) were allowed to attach to TC-25 flasks.
They then were exposed to antibodies (100 //g/ml)
for 36 hours, harvested, washed, and DNA was extracted using a hypotonic lysing buffer consisting of
10-mmol Tris, 1-mmol ethylenediaminetetraacetic
acid, 0.5% Triton X-100, pH 7.5. The extract was spun
at 16,000 X g for 15 minutes and supernatant extracted with phenol-chloroform. DNA was precipitated in ice-cold 100% ethanol and then digested overnight with proteinase K followed by RNAse (DNAsefree) digestion. DNA samples were run on 1% agarose
gel in Tris-acetic acid-EDTA buffer and stained with
ethidium bromide.
Cytotoxicity Assay
The E1A.NR3 cells were allowed to attach to 96-well
flat-bottomed microtiter plates overnight at a density
of 104 cells/well in DMEM at a final volume of 200 fj\
per well. Cells were cultured in the presence of various
concentrations of antibodies, and growth of these cells
was measured using a colorimetric MTT assay. After
24 or 48 hours, 25 //I of 0.5% solution of MTT (Thiazolyl blue, Sigma) was added to each well, and the plates
were incubated for another 3 hours at 37°C. MTT
is a pale yellow substrate that produces a dark blue
formazan product when incubated with live cells. At
the end of incubation, 100 /A of cell lysing buffer
(SDS-DMF) was added to dissolve the blue crystals
of formazan. The plates were read in a BioRad (Hercules, CA) enzyme-linked immunosorbent assay
reader at 570 nm. Cytotoxicity is presented as cell
survival calculated based on the following formula:
%cell survival = [1 — (absorbance total — absorbance
sample)/absorbance total] X 100, where absorbance
total is the optical density of the cell cultured without
Ab, and absorbance sample is the optical density of
cells cultured in the presence of Ab. The optical density of blank wells was subtracted from all samples.
To study the cytotoxic effect of complement,
guinea pig complement (GIBCO BRL, Grand Island,
NY) was added to cultured cells at a final dilution
of 50X. Cells were cultured with complement alone,
complement with antibody, antibody alone, and cells
alone as a control specimen. Colorimetric MTT assay
was performed 24 and 48 hours later as described
above.
Assay for Functional Fc Receptor
(Rosette Assay)
Fresh sheep red blood cells (SRBCs) from the local
animal facility were collected to the sterile Alsever's
solution (1:1) and stored at 4°C for 0 to 3 days. For
the experiment, 1 ml of SRBC was washed three times
in PBS and a 5% suspension was prepared in PBS.
Then, cells were coated with the maximum subagglutinating concentration of a rabbit IgG against SRBCs
(Sigma) at the dilution 1:8000 or no antibodies for 2
hours at 37°C. The sensitized SRBCs were washed
three times and resuspended in DMEM containing
heat-inactivated 2% FBS. E1A.NR3 cells (105/ml) were
seeded in a 35-mm Petri dish and allowed to attach
for 2 hours. The original medium was aspirated, and
1% of antibody-coated SRBCs was added for 1-hour
incubation at 37°C. Unsensitized SRBCs were used as
negative control specimens. One hour later, when the
SRBC had formed a uniform layer, cells were washed
carefully three times in PBS and examined for rosettes
formation under light microscope.
Cell Staining for Apoptotic Morphologic
Analysis
The E1A.NR3 cells were allowed to attach to an eightchamber slide dish (Nunc 177445) for 4 hours at a
density of 5 X 104 cells/chamber in DMEM at a final
volume of 250 fi\ per well. Antibody then was added
at a final concentration of 300 /xg/ml. At different
times, the medium was discarded, and 250 fil fluorescent dye (Hoechst 33342; Sigma, St. Louis, MO)
(200X of 1 mg/ml dimethyl sulfoxide) was added and
incubated with the cells for 15 minutes. Then, 5 [A
of propidium iodide (1 mg/ml PBS) was added for
another 10 minutes. Cells were rinsed and examined
at 40X using a Zeiss fluorescent microscope and an
ultraviolet excitation filter.
RESULTS
Antibody Uptake by Retinal Cells
To evaluate pathogenic effects of antirecoverin antibody on retinal cells, we performed in vitro experiments using a recently developed immortalized rat
retinal cell culture E1A.NR3.13 This cell line contains
cells expressing antigens specific for photoreceptor,
bipolar, and ganglion cells. Recoverin, among other
proteins, is expressed by these cells as is shown by
immunocytochemistry in Figure 1A. To examine
whether antirecoverin antibodies can access the antigen inside the cells, biotinylated affinity-purified antibodies specific to recoverin obtained from five patients with CAR were tested. As control, antirecoverin
antibodies from rats or rabbits immunized with recoverin were used. All antibodies used had similar speci-
286
Investigative Ophthalmology & Visual Science, February 1997, Vol. 38, No. 2
B
\
%
D
1
t
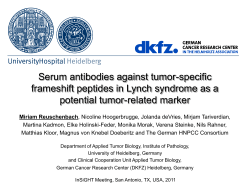
FIGURE l. Internalization of antibodies by E1A.NR3 cells. (A) lmmunoperoxidase staining
of recoverin using rabbit antirecoverin antibodies. Cells were grown in a chamber dish,
fixed with 2% paraformaldehyde, permeabilized, and then antirecoverin antibodies were
added (1:1000). (B to E) Antibody uptake. E1A.NR3 cells were allowed to attach to a dish,
and biotinylated antirecoverin or normal antibodies were added to the culture medium.
The cells were washed with phosphate-buffered saline and fixed with 2% paraformaldehyde.
Localization of antibody was shown using biotin-streptavidin-peroxidase. Cells were counterstained with methyl green. (B) Dark-stained cells indicate internalized antirecoverin antibodies (arrows). Magnification, X100. (C) Higher magnification of untreated cells. No cytoplasm immunostaining was observed; methyl green counterstained cells. (D) A representative
micrograph of immunoperoxidase cytoplasm staining in cells grown in the presence of
human antirecoverin antibodies from a patient with cancer-associated retinopathy. (E) Immunoperoxidase cytoplasm staining in cells grown in the presence of normal human immunoglobulins. Magnification, X1000 (C,D,E).
ficities; they all recognized the same major binding
site localized within residues 64 through 70, Lys-AlaTyr-Ala-Gln-His-Val.14 We cultured the E1A.NR3 cells
in the presence of affinity-purified antibodies for 24 to
72 hours. Normal IgG fractions of appropriate species
were used as negative control specimens. Using an
immunoperoxidase method, we found normal and
antirecoverin antibodies in the cytoplasm of the cells
after a 24-hour incubation with antibodies. As shown
in Figures IB, 1C, ID, and IE, both human antirecoverin and normal nonspecific antibodies can be internalized by retinal cells. The same staining pattern was
observed when antirecoverin antibodies produced in
rats or rabbits were added to the cultures.
Effects of Antibodies and Complement on Cell
Growth
In the previous experiment, we showed that both normal and specific antibodies entered retinal cells. In
the next set of experiments, we studied the effect of
antibodies on cell growth. We tested the effect of five
different antirecoverin autoantibodies from patients
with CAR, rat antirecoverin antibodies from rats widi
active experimental autoimmune uveoretinitis,6 and
rabbit antirecoverin antibodies. Our data show that all
antirecoverin antibodies tested had a similar cytotoxic
effect on E1A.NR3 cell survival. Figure 2 shows representative results obtained after incubation with human, rat, and rabbit antibodies. Cytotoxic action of
antibodies on cell growth was dependent on the
amount of antirecoverin antibodies added and on the
time of exposure. The toxic effect was more pronounced in higher antirecoverin antibody doses (Fig.
2A), and the number of surviving cells significantly
decreased after 48 hours (Fig. 2B). Normal nonspecific antibodies had no effect on cell survival at the
same doses and times.
In the next experiment, E1A.NR3 cells were
grown in the presence of antibodies and complement.
Human antirecoverin antibodies were IgGl class;
therefore, they could bind complement. When compared with cultures incubated with antirecoverin antibodies alone, no additional cell destruction was observed in the presence of complement over a period
of 48 hours (data not shown).
To determine whether the Fc receptor is expressed on the surface of E1A.NR3 cells, we performed an Fc resetting assay using IgG-coated SRBC.
The SRBCs did not form rosettes with E1A.NR3 cell
surface. To test the possibility that Fc receptor is induced by antibody, cells first were incubated for 4
hours with antibodies, and then the rosette assay was
performed. No rosette formation was observed. These
results show that E1A.NR3 cells do not express an Fc
binding activity on their surface.
Specificity of Antibody Action
To establish whether antirecoverin antibodies can influence the growth of cells that do not express recoverin, we cultured antirecoverin antibodies with three
Autoantibodies Induce Apoptotic Cell Death
DOSE
TIME
120
100 -
80 60 40 20 -
DC
HUMAN
\
0
120
100
80
60
LLJ
40
20
<
LU
100 -
O
80 -
CC
LU
CL
RAT
0
120
60 40 20 -
RABBIT
0 15 35 75 150 300
HOURS
FIGURE 2. Effect of antibodies on cell survival measured by
a colorimetric MTT assay, (left) Dose response. E1A.NR3
cells were allowed to attach to 96-well flat-bottomed microtiter plates at a density of 104 cells/well in Dulbecco's modified Eagle's medium at final volume of 200 /zl/ml. Cells
were cultured in the presence of various concentrations of
antibodies, and survival of the cells was measured after 48
hours, (right) Time course of cell death induced by 300
/ig/ml antirecoverin antibodies 0, 24, and 48 hours after
treatment with the antibody (O) antirecoverin antibodies;
(•) normal immunoglobulin G fraction.
cell lines: human retinoblastoma cell line Y79, rat adrenal pheochromocytoma cell line PCI2, and rat pituitary tumor cell line GH3. Proteins extracted from the
cells were checked for the presence of recoverin by
Western blot analysis using antirecoverin antibodies.
None of the cells expressed recoverin in our culture
conditions, although we found that retinoblastoma
Y79 expressed an mRNA for recoverin. These cells
were grown in the presence of high doses of antirecoverin antibodies (300 //g/ml) for 24 to 48 hours. Using
an immunoperoxidase method, we detected the presence of normal and antirecoverin antibodies in the
cytoplasm ofY79, PC12, and GH3 cells (Fig. 3A). However, the results from the MTT cytotoxic assay show
that antirecoverin antibodies did not influence cell
growth and survival (Fig. 3B).
In the next experiment, monoclonal antibody specific to another photoreceptor-specific protein, ar-
287
restin (S-antigen), was added to E1A.NR3 cell culture
for 48 hours. Arrestin is expressed by E1A.NR3 cells.13
Our results show that antiarrestin antibody was almost
as effective as were antirecoverin antibodies. After incubation with the highest dose of antibody, 40% of
the cells were alive as compared with the action of
normal antibodies, where 100% cells survived (Fig. 4).
Evidence for Apoptosis
Comparative analysis of E1A.NR3 cells grown in the
presence of recoverin-specific antibodies, regardless
of their origin (human, rat, or rabbit), showed morphologic changes, including shrinking of cell bodies,
blebs, retraction of processes, and detachment from
the tissue culture dish. Cells retained a normal morphology when cultured with the same amount of control antibodies (Fig. 5). Because both specific and control antibodies were internalized, this effect of antirecoverin antibody must be because of specific antibody
action. Incubation of cells in the presence of antirecoverin antibodies caused DNA fragmentation into
200-bp integers and nuclear chromatin condensation
(Figs. 5C, 5D, 5E). DNA fragmentation was observed
for all antirecoverin antibodies from patients' sera as
well as from animal's sera. Fragmentation of DNA was
not seen when cells were grown with normal antibodies. Chromatin condensation was analyzed using the
fluorescent dye Hoechst 33342 (Sigma) and propidium iodide (Figs. 5D, 5E). Treatment of cells with
antirecoverin antibodies induced apoptosis as shown
by multiple, brightly stained nuclei, most of which
were from dead cells (pink). On average, approximately 20% of cells in the culture showed fragmentation and condensed nuclei. The percentage of apoptotic cells in the cell population was underestimated
because growing the cells in the presence of antiretinal antibodies caused them to detach from the tissue
culture dish, and the lost cells were not scored. Control cultures treated with either normal antibodies or
with no antibodies had 1% to 2% of cells that were
apoptotic, presumably due to natural processes of the
cell cycle. The very low level of apoptotic cells in normal antibody experiments was not detectable by DNA
fragmentation analysis because of the lower sensitivity
of the test. Figures 5D and 5E show a typical Hoechst
(Sigma) staining of cells cultured in the presence of
human normal and antirecoverin autoantibodies.
DISCUSSION
The function of autoantibodies in the pathogenicity of
most autoimmune diseases, including paraneoplastic
syndromes, is unknown. In CAR syndrome, a high titer
of circulating antibodies is associated with retinal degeneration. Although inflammatory infiltrates are observed sporadically in diseased tissues of patients with
Investigative Ophthalmology & Visual Science, February 1997, Vol. 38, No. 2
288
Anti-recoverin Ab
NORMAL IgG
ANTI-RECOVERIN Ab
Y79
FIGURE 3. Effect of antirecoverin antibodies on Y79, PCI2, and CH3 cells. (A) Antibody
uptake. Cells were grown in the presence of biotinylated antibodies against recoverin for
48 hours. Immunoperoxidase staining was performed, {left panel) Dark-stained cells indicate
cells internalized antirecoverin antibodies, {rightpanel) No antibody was added to the culture.
Arrows point toward the cells. (B) Effect of antibodies on the cell survival by the MTT
colorimetric assay. Cells were grown with 300 /ig/ml antirecoverin and normal antibodies
for 48 hours.
CAR,3'15'16 little evidence of retinal inflammation has
been reported. In the absence of visible inflammation,
such as seen in patients with uveitis, one can assume
that retinal degeneration occurs by some noninflammatory process involving humoral immunity. This led
us to the hypothesis that apoptotic mechanisms may
be involved in the disease. There is a possibility that in
pathologic conditions, the antibodies cross the bloodretina barrier (BRB), enter photoreceptor cells, and
by, altering their function, trigger cell death. Our present studies show evidence to support the pathogenic
role
of autoantibodies in CAR. The major result is that
120
autoantibodies specific to recoverin penetrate into living cells and trigger retinal cell death, which occurs
<
through apoptotic mechanism.
C
100 The apoptotic nature of E1A.NR3 cell death is
cc
supported by two lines of experimental evidence. Inin
ternucleosomal DNA fragmentation was observed by
LL
agarose gel electrophoresis as described for apoptotic
O
cell death in other tissues.17 Apoptotic cells showing
LJJ
multiple, brightly stained condensed nuclei by fluorescent method were observed throughout the culture
incubated with recoverin-specific antibodies but in
cultures incubated with normal antibodies. This antiLJJ
O
body-mediated destruction of retinal cells was indecc
pendent of complement.
LJJ
The initial process of antibody internalization was
Q_
^ _ _ _
zu -1
——•
nonspecific
because both normal and specific IgG
75
150
300
were
taken
up
by EA1.NR3 retinal cells. It is not clear
ANTIBODY lfjLQlm\]
by what mechanism antibodies access retinal cells.
ncuRE 4. Uptake of antiarrestin antibodies by E1A.NR3
One possibility is that IgG is transported through Fc
cells. The E1A.NR3 cells were allowed to attach to 96-well
receptors expressed on the surface of cells. However,
flat-bottomed microtiter plates at a density of 104 cells/well
retinal cells grown with or without antibodies did not
in Dulbecco's modified Eagle's medium at a final volume
express an Fc binding activity on their surface. It is
of 200 //I/ml. Cells were cultured in the presence of various
possible that internalization of antibodies may occur
concentrations of monoclonal antibody S65-38 specific for
arrestin {black bars) or control immunoglobulin G {white nonspecifically by endocytosis. This suggestion is supbars), and survival of these cells was measured after 48 hours. ported by data published previously indicating that
289
Autoantibodies Induce Apoptotic Cell Death
FIGURE 5. Apoptosis of retinal cells E1A.NR3 triggered by antirecoverin antibodies. After
cells attached, antirecoverin or normal antibodies were added. (A) Photomicrograph of
E1A.NR3 cells grown without antibodies. Cells display epithelioid morphology interspersed
with process-bearing cells. (B) Photomicrograph of the cells grown in the presence of human
antirecoverin antibodies for 24 hours. Dead cells loosely attach to the tissue culture dish.
Retraction of the processes can be observed as indicated by arrows. (C) DNA ladders on
1% agarose gel electrophoresis from cells grown in the presence and in the absence of
human antirecoverin antibodies. Ethidium brornide-stained gels. Lane 1 represents DNA
markers (multiples of 123 bp). Lane 2 represents DNA isolated from cells cultured in the
presence of normal human immunoglobulin or absence of antibodies. Lane 3 represents
DNA isolated from cells exposed to human antirecoverin antibodies. (D,E) Nuclear chromatin condensation in cells grown for 24 hours with antibodies and examined with the DNA
dyes Hoechst 33342 (Sigma, St. Louis, MO) and propidium iodide. Cells grown in the
presence of normal antibodies (D) showed only rare dead cells, whereas the treatment
with antirecoverin antibodies (E) induces apoptosis as shown by multiple, brightly stained
condensed nuclei (arrow). Enumeration of apoptotic nuclei by fluorescent microscopy
showed 20% apoptotic nuclei for antibody-treated cells and 1% to 2% for normal antibody
or untreated cells. Only attached cells were counted.
the rod photoreceptors inner segment is capable of
extensive endocytotic activity to retrieve components
of interphotoreceptor matrix and that photoreceptor
and bipolar cells participate in endocytosis at the synapse.18"20
In view of the fact that normal antibodies do not
influence cell physiology and cells lacking the target
antigen are not affected by the presence of specific
antibodies, a hypothetical mechanism by which antirecoverin antibody might cause dysfunction or death of
photoreceptor cells is by blocking recoverin function.
Because the initial process of internalization seems to
be nonspecific, a possible mechanism for this action
of antirecoverin antibodies results from the calciumbinding properties of recoverin. Recoverin is a calcium-binding protein present in retinal photoreceptor cells and also found in bipolar cells.21 The calciumbound form of recoverin plays a role in regulating
rhodopsin phosphorylation.22'23 Blocking recoverin
function may cause an increase in free calcium and
lead to the activation of endonuclease, a calcium-sensitive molecule, resulting in nuclear morphologic
changes and DNA fragmentation. This would not be
observed in the case of normal antibodies that enter
the cells but do not affect cell physiology. Support for
this is provided by our recent studies that antirecoverin antibody binding was calcium dependent.1' We
showed that conformational changes induced by
bound calcium enhance the binding of antibodies to
recoverin. Furthermore, the sequence within residues
64 through 70 (Lys-Ala-Tyr-Ala-Gln-His-Val) in proximity to the calcium-binding domain EF-hand 2 was
found to be a major antigenic and pathogenic reThe central question that has always arisen in CAR
is how autoantibodies get to the target antigen in the
retina. The BRB is the most obvious separation of
circulating autoantibodies from the cells, and it is
290
Investigative Ophthalmology & Visual Science, February 1997, Vol. 38, No. 2
likely to be disrupted for dysfunction to occur; this
study does not address this question. In the pathologic
condition, increased vascular permeability often is observed, which may permit access of serum antibodies
to the retina through the BRB.24 There also are some
experimental data supporting the ability of antibody
to cross the BRB. Systemically injected anti-S antigen
antibodies into normal rats induced electroretinographic supernormality, suggesting their passage
across the BRB.25 In the paraneoplastic cerebellar degeneration model, Greenlee et al26 showed uptake of
systemically administrated IgG by cerebellar Purkinje's
cells in the setting of the BRB disruption. In addition,
the role of cellular immunity and cytokines in BRB
disturbance also cannot be excluded and should be
investigated.
In conclusion, our studies show for the first
time that antirecoverin antibodies can be cytotoxic
for retinal cells and can cause retinal cell death
through apoptotic mechanisms. This effect of specific antibodies might be more generalized in cases
of diseases where cell loss does not induce inflammatory response and apoptosis seems to be the
mechanism of cell death. We propose that in patients with CAR, autoantibodies originally are elicited against recoverin expressed in tumor cells.
When given access to recoverin through the BRB,
these antibodies could initiate photoreceptor degeneration, which could lead to visual loss and
blindness. Moreover, such mechanisms may be
common for other paraneoplastic disorders and autoimmune diseases where antibodies interfere with
normal cell physiology.27 Interference with such
apoptotic processes could be considered as a possible strategy for treatment of CAR.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
Key Words
apoptosis, autoantibody, paraneoplastic syndrome, recoverin, retina
15.
Acknowledgments
The authors thank Drs. Lubert Stryer and Sergey Zazulya
for the cells expressing recoverin.
References
16.
17.
1. Thirkill CE, FitzGerald P, Sergott RC, Roth AM, Tyler
18.
NK, Kaltner JL. Cancer-associated retinopathy (CAR
syndrome) with antibodies reacting with retinal, opticnerve, and cancer cells. NEnglJMed. 1989; 321:15891594.
19.
2. Posner JB, Furneoux HM. Paraneoplastic syndromes.
In: Waksman BH, ed. Immunologic Mechanisms in Neurologic and Psychiatric Disease. New York: Raven;
1990:187-219.
20.
3. Adamus G, Guy J, Schmied JL, Arendt A, Hargrave
PA. Role of anti-recoverin autoantibodies in cancer-
associated retinopathy. Invest Ophthalmol Vis Sci.
1993; 34:2626-2633.
Polans AS, Buczylko J, Crabb J, Palczewski K. A photoreceptor calcium binding protein is recognized by autoantibodies obtained from patients with cancer-associated retinopathy. / Cell Biol. 1991; 112:981-989.
Thirkill CE, Tait RC, Tyler NK, Roth AM, Keltner JL.
The cancer-associated retinopathy antigen is a recoverin-like protein. Invest Ophthalmol Vis Sci. 1992;
33:2768-2772.
Adamus G, Ortega H, Widcowska D, Polans A. Recoverin: a potent uveitogen for the induction of photoreceptor degeneration in Lewis rats. Exp Eye Res.
1994; 59:447-456.
Gery I, Chanaud NP III, Anglade E. Recoverin is
highly uveitogenic in Lewis rats. Invest Ophthalmol Vis
Sci. 1994; 35:3342-3345.
Polans A, Witkowska D, Haley T, Amundson D, Baizer
L, Adamus G. Recoverin, a photoreceptor-specific calcium-binding protein, is expressed by the tumor of a
patient with cancer-associated retinopathy. Proc Natl
AcadSci USA. 1995;92:9l76-9180.
Yamaji Y, Matsubara S, Yamadori I, et al. Characterization of a small-cell-lung-carcinoma line from a patient
with cancer-associated retinopathy. Inter J Cancer.
1996; 65:671-676.
Ray S, Zazula S, Niemi GA, et al. Cloning, expression,
and crystallization of recoverin, a calcium sensor in
vision. Proc Natl Acad Sci USA. 1992;89:5705-5709.
Zozulya S, Ladant D, Stryer L. Expression and characterization of calcium-myristoyl switch proteins. Methods EnzymoL 1995; 250:383-393.
Laemmli UK. Cleavage of structural proteins during
die assembly of die head of bacteriophage T4. Nature
(London). 1970; 227:680-688.
Seigel GM. Establishment of an ElA-immortalized retinal cell line. In Vitro Cell Devel Biol. 1996; 32:66-68.
Adamus G, Amundson D. Epitope recognition of recoverin in cancer associated retinopathy: Evidence for
calcium-dependent conformational epitopes. / NeurosciRes. 1996; 45:863-872.
Buchanan TAS, Gardiner TA, Archer DB. An ultrastructural study of retinal photoreceptor degeneration associated with bronchial carcinoma. Am J Ophthalmol. 1984; 97:277-287.
Sawyer RA, Selhorst JB, Zimmerman LE, Hoyt WF.
Blindness caused by photoreceptor degeneration as a
remote effect of cancer. Am J Ophthalmol. 1976;
81:606-613.
Thompson CB. Apoptosis in the pathogenesis and
treatment of disease. Science. 1995;267:1456-1462.
Evans JA, Liscum L, Hood DC, Holtzman E. Uptake
of horseradish peroxidase by presynaptic terminals of
bipolar cells and photoreceptor cells of die frog retina. /Hiostochem Cytochem. 1981;29:511-518.
Hollyfield JG, Rayborn ME. Endocytosis in the inner
segment of rod photoreceptors: analysis of Xenopus
laevis retinas using horseradish peroxidase. Exp Eye
Res. 1987; 45:703-719.
Hollyfield JG, Varner HH, Rayborn ME, Liou GI, Bridges CD. Endocytosis and degradation of interstitial
Autoantibodies Induce Apoptotic Cell Death
retinol-binding protein: differential capabilities of cell
that border the interphotoreceptor matrix. J Cell Biol.
1985; 100:1676-1681.
21. Milam AH, Dacey DM, Dizhoor AM. Recoverin imraunoreactivity in mammalian cone bipolar cells. Vis Neurosci. 1992; 10:1-12.
22. Kawamura S, CoxJA, Nef P. Inhibition of rhodopsin
phosphorylation by non-myristoylated recombinant
recoverin. Biochem Biophys Res Covvmun. 1994; 203:121127.
23. Ohguro H, Rudnicka-Nawrot M, Buczylko J, et al.
Structural and enzymatic aspects of rhodopsin phosphorylation. JBiol Chem. 1996;271:5215-5224.
291
24. Greenwood J. Mechanisms of blood-brain barrier
breakdown. Neuroradiology. 1991;33:95-100.
25. Stanford MR, Robbins J, Kasp E, Dumonde DC. Passive administration of antibody against retinal S-antigen induces ERG supernormality. Invest Ophthalmol Vis
Sci. 1992; 33:30-35.
26. Greenlee JE, Burns JB, Rose JW, Jaeckle A, Clawson
S. Uptake of systemically administrated human anticerebellar antibody rat Purkinje cells following bloodbrain barrier disruption. Ada Neuropathol. 1995;
89:341-345.
27. Alarcon-Segovia D, Ruiz-Arguelles A, Llorente L. Broken dogma: Penetration of autoantibodies into living
cells. Immunol Today. 1996; 17:163-164.











© Copyright 2026