
Evaluation of non–lead-based protective radiological material in spinal surgery MD ,
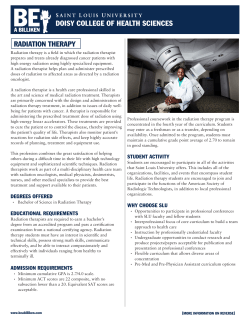
The Spine Journal 6 (2006) 577–582 Technical Review Evaluation of non–lead-based protective radiological material in spinal surgery Gaetano J. Scuderi, MDa, Georgiy V. Brusovanik, MDb,*, David R. Campbell, MDc, Robert P. Henry, MDd, Brain Kwone, Alexander R. Vaccaro, MDf a Private Practice, 2055 Military Trail #204, Jupiter FL 33458, USA Jupiter, FL, USA Orthopaedic Surgery Resident, Department of Orthopedic Surgery, University of Hawaii, 1356 Lusitana Street, 6th Floor, Honolulu, HI 96813, USA University of Hawaii, Honolulu, HI, USA c Private Practice, 2055 Military Trail #204, Jupiter FL 33458, USA, Jupiter, FL, USA d Department of Radiology, Jackson Memorial Hospital, 1611 NW 12th Ave, Miami, FL 33136, USA e Department of Orthopaedic University of British Columbia, D6 Heather Pavilion, Vancouver General Hospital, Vancouver BC, V5Z 3J5, Canada, British Columbia, Canada f Department of Orthopaedic Surgery, Thomas Jefferson University and the Rothman Institute, 925 Chestnut Street, 5th Floor, Philadelphia, PA 19107, USA Received 6 June 2005; accepted 11 September 2005 b Abstract BACKGROUND CONTEXT: Traditionally, lead-based garments are the standard method of intraoperative radiation protection during fluoroscopy. Unfortunately, the lead used is heavy, lacks durability, is difficult to launder, and its disposal is associated with environmental hazards. PURPOSE: An evaluation of the protective radiation efficiency of three commercially available radiation protective garments compared with a standardized lead protective shield. STUDY DESIGN/SETTING: Measured radiation transmission through lead and three commercially available lightweight radiological protective garments (Xenolite, EarthSafe, and Demron) was performed using a standard, calibrated dosimeter. METHODS: Radiation transmission, attenuation, lead equivalencies as well as garment weight comparisons were measured. The tests were repeated through a range of voltage and tube current settings that are common to clinical radiological applications (60–120 keV). RESULTS: All materials tested demonstrated effectiveness at common clinically relevant energy exposures (100 keV). EarthSafe and Xenolite demonstrated 0.5 mm lead equivalency protection at 80 and 100 keV X-ray energies but not at higher energy levels (O100 keV), which is where most radiological procedures are performed utilizing more advanced technological imaging equipment. Demron was best able to effectively shield ionizing radiation at higher energy levels (O100 keV). The lightweight nature of these lead-free materials may result in less fatigue and musculoskeletal complaints by the wearer. CONCLUSIONS: Of the tested lead-free garments, Demron appears to offer equivalent levels of protection to standard lead-based shields within traditional energy zones but with less weight than standard lead-based shields. Ó 2006 Elsevier Inc. All rights reserved. Keywords: Protective radiation garments; Lead; Radiation transmission; Lead equivalencies; Lead-free garments; Ionizing radiation shield Introduction FDA device/drug status: not applicable. Nothing of value received from a commercial entity related to this manuscript. * Corresponding author. Department of Orthopedic Surgery, University of Hawaii, 1356 Lusitana Street, 6th Floor, Honolulu, HI 96813. Tel.: (808) 586-2920; fax: (808) 956-9481. 1529-9430/06/$ – see front matter Ó 2006 Elsevier Inc. All rights reserved. doi:10.1016/j.spinee.2005.09.010 As more spinal pathology is being treated with minimally invasive procedures, the spinal surgeon must rely on other means of identifying surgical anatomy besides direct visualization. The most common method today for indirect visualization of the spinal elements is via bi-planar 578 G.J. Scuderi et al. / The Spine Journal 6 (2006) 577–582 fluoroscopy. Technological advances have allowed better indirect visualization of spinal anatomy and have enabled the spinal surgeon to accomplish complicated spinal procedures minimizing the magnitude of tissue trauma [1]. This has not come without increased risk. Radiation exposure can be up to 10 times higher in spinal surgery compared with other procedures [2]. The use of fluoroscopy is also vital in other areas of medicine including pain management, interventional cardiology, urology, general orthopedics, and of course radiology. Despite this, little attention by surgical clinicians has been paid to the potential seriousness and means of protecting operating personnel from the harmful ionizing radiation that occurs intraoperatively. Traditionally, clinicians have relied on cumbersome protective lead-reinforced garments despite numerous issues surrounding their use [5]. These lead-based garments serve as the standard radiation attenuating shields for operating personnel. Unfortunately, lead has difficulties associated with its use. A lead apron is relatively heavy and is frequently associated with musculoskeletal complaints with extended use. Additionally, there are environmental issues with its disposal secondary to its known toxicity. Lead within protective aprons may exude into soil and permeate water supplies. In this study, we evaluated three commercially available non–lead-based radiological protective garments purported to be similar in function to standard lead aprons in attenuating radiation. These garments are 30–40% lighter than lead and therefore may be helpful in terms of compliance and in minimizing musculoskeletal complaints associated with extended apron use. Material and methods All testing was performed at Massachusetts General Hospital, Boston, Massachusetts. A polycarbonate test stand (Radcal Corporation, Monrovia, CA; Part. No. 10T5) was placed beneath an X-ray tube and aligned such that the X-rays emitted from the tube were centered (a laser is used as a guide) on sample material/filters placed on top of a stand. The stand was secured to the X-ray table. An ionization chamber (Model No. 10X5-60; Radcal Corporation) was also set up on an adjustable metal stand so that it was centered beneath the sample material/filters. The ionization chamber was then connected to a Dosimeter (Model No. 9010; Radcal Corporation) by a cable with a converter (Model No. 9060; Radcal Corporation). The Dosimeter, which displays the Exposure in milliRoentgens (mR or millirem), was calibrated to read 0.00 mR. The X-ray machine was then set to the desired voltage (kVp) and tube current (mAs). The protocol called for the following voltages and currents: (1) 60 kVp and 10.0 mAs; (2) 80 kVp and 8.0 mAs; (3) 100 kVp and 6.4 mAs; (4) 120 kVp and 5.0 mAs; (5) 130 kVp and 3.2 mAs. The procedure for testing each of the samples was as follows: A dosimeter reading for 0 mm or air was initially recorded (in this experiment, for example @60 kVp and 10 mAs, the dosimeter read 34.24 mR). Testing was then performed to calculate the aluminum (Al) half value layer. An aluminum filter (0.51 mm) was placed on top of the BRH test stand and aligned properly so that the majority of the incident X-rays hit the center of the plate. The X-ray machine was switched on, and the dosimeter reading was taken. The Al thickness was increased gradually by adding more filters. The filters were added one by one until the radiation was halved (until the reading on the dosimeter showed approximately half the initial value of 34.24 mR). The reading in mR for the corresponding Al thickness was recorded. The dosimeter was zeroed each time an extra Al plate was added. Four Al plates were required to cut the radiation by half. The aluminum plates were removed and the dosimeter zeroed. The sample to be tested was then placed on the BRH test stand and the dosimeter was zeroed again. The X-ray machine was switched on, and the dosimeter reading was noted. The sample was removed, and a similar procedure was followed for other samples. Standard lead was then tested after the designated numbers of samples were tested. A lead foil of 1 mil (1 mil51/ 1,000th inch) thickness was placed on the stand, and the X-ray machine was switched on. The dosimeter reading was noted. The thickness of lead foils was increased until the final dosimeter reading was the same as that of the sample. If many layers of the same sample were used, the dosimeter reading of all the combined layers was taken. Results Table 1 lists and compares the transmission, attenuation, and lead equivalencies of all material tested. The results for lead, summarized in Table 1, were obtained experimentally by testing lead foils; transmission data were collected for 19.68 mil (0.5 mm) thick lead foils. As one may glean from the table, % attenuation diminishes with higher energy (keV). At lower energies, attenuation approaches 100%. At 60 keV, attenuation for all materials is O99%. The discrepancy in radiation attenuation is magnified at higher energies (Fig. 1). The three non–lead-based radioactive shields tested included EarthSafe, Xenolite, and Demron. EarthSafe was noted to have over 0.5 mm lead equivalency protection at 80 and 100 keV X-ray energies but not at energies at the higher end of the spectrum (O100 keV), which is where most radiological procedures are performed. Xenolite followed similar trends as EarthSafe and did not have the required 0.5 mm lead equivalency protection at the energy extremes. Demron was effective both in the lower energy range (below 100 keV) as well as the higher energy range (100, 120, and 130 keV). It should be noted from Figure 1A and 1B that although Demron did not give 0.5 mm lead equivalency protection at energies lower than 100 keV, the difference in the transmission percentages G.J. Scuderi et al. / The Spine Journal 6 (2006) 577–582 Table 1 Comparison of transmission, attenuation, and lead equivalencies Energy (KeV) Demron 60 80 100 120 130 EarthSafe 60 80 100 120 130 Xenolite 60 80 100 120 130 Lead 60 80 100 120 130 Transmission (%) Attenuation (%) Lead equivalency (mm) 0.55 2.21 3.14 4.00 4.50 99.45 97.79 96.86 96.00 95.50 0.39 0.44 0.54 0.55 0.54 0.46 1.47 3.67 6.78 8.43 99.54 98.53 96.33 93.22 91.57 0.42 0.53 0.51 0.42 0.39 0.4 1.75 3.46 5.89 7.18 99.6 98.25 96.54 94.11 92.82 0.44 0.5 0.52 0.45 0.44 0.23 1.80 3.50 4.80 5.20 99.77 98.2 96.5 95.2 94.8 0.5 0.5 0.5 0.5 0.5 between lead and Demron was negligible at lower energies. The differences in percent transmission between Demron, Xenolite, and EarthSafe became significant at higher energies. Lead equivalencies and transmission percentages of lead at 100, 120, and 130 keV X-ray energies are summarized in Table 2. The number of layers required to achieve 0.5 mm lead equivalency above 100 keV, and their weights for each product are tabulated in Table 3. A sample piece of 10.2 cm2 area was taken from each of the garments and weighed separately using a digital balance. Although a single layer of EarthSafe or Xenolite weighs less than a single layer of Demron, the number of layers required to achieve 0.5 mm lead equivalency above 100 keV is more than that of Demron. It took approximately four layers of Demron to achieve the required 0.5 mm lead equivalency above 100 keV; whereas five layers were needed for EarthSafe and Xenolite to achieve the same. To offer the same attenuation protection, Demron is approximately 15.8% lighter than EarthSafe and approximately 3.5% lighter than Xenolite. Discussion Exposure to ionizing radiation (alpha, beta, X-rays and gamma rays) is clearly dangerous to humans. Skin lesions are a known consequence of high-level exposure, and numerous malignancies have been associated with chronic low-level exposure [12]. We are becoming increasingly 579 aware of the risks of occupational exposure in the medical arena. A study by Wall constructed radiation risk projection models for computer tomography examinations and found that a lifetime risk of fatal cancer can reach 1 in 1,000 for children, depending on the frequency of examinations [3]. Although not well studied, it is felt that the health effects of radiation exposure are linear with no threshold [9]. With the widespread use of computer tomography, plain roentgenography, and the increasing use of ionizing radiological equipment by nonmedical personnel, the potential problems of radiation exposure may be more widespread than reported [4]. To accomplish enhanced visualization, the newer generation fluoroscopes produce higher amounts of energy. X-ray energy is measured in kVp. A typical chest X-ray utilizes an average energy of 80 kVp for a period of 0.1 second. Fluoroscopes, on the other hand, emit energies up to 130 kVp, and because they are continuous, emit for substantially longer periods of time [10]. The physician must take appropriate measures to reduce the risk of radiation exposure to the patient, the operating staff, and himself. Concepts such as time, distance, and shielding are the most common ways of reducing radiation exposure. By reducing the time of exposure, maximizing the distance from the anode, and utilizing shielding apparatus, medical personnel may limit the amount of radiation exposure to a minimum [11,12]. Exposure rates to the patient of 1,200 to 4,000 mrem/min have been recorded [6]. The close proximity of operating room personnel to fluoroscopy equipment may result in higher dosages of backscatter, a concept that has received little attention in the past [7]. Exposure rates from scatter at 2 feet from the anode have been recorded at approximately 5 mrem/min. A heightened risk of radiation exposure to the assistant surgeon has been demonstrated [8]. Health-care workers may lower radiation exposure in a limited number of ways. Decreasing the exposure time clearly reduces the dose received from the radiation source. However, this is not always practical, especially in long fluoroscopic procedures common in orthopedics and cardiovascular surgery. Increasing the distance from the source, another well-known factor in limiting radiation exposure, similarly may not be practical for the surgeon and assistants as surgical technique may require proximity. The simplest way to minimize exposure is via shielding, which creates a barrier between the source and the individual. Traditionally this has resulted in the cumbersome donning of heavy and awkward undergarments that include lead. Although they provide good attenuation to radiation exposure, they are heavy, uncomfortable, and often crack, leaving the wearer unknowingly exposed. Lead-based polymer composites are made by incorporating lead or other heavy metal compounds into a resin or polymer matrix. Attempts have been made to obtain similar protection with composite materials that reduce weight. These materials have had variable results in laboratory testing, are more 580 G.J. Scuderi et al. / The Spine Journal 6 (2006) 577–582 A B 9.00 8.00 Transmission (%) 7.00 6.00 5.00 4.00 3.00 2.00 1.00 0.00 50 60 70 80 90 100 110 120 130 140 X-Ray Energy (kVP) Fig. 1. Comparison of percent transmission of X-rays. expensive, and have been associated in some cases with an unpleasant odor. Additionally, because they contain lead, they cannot be laundered, and are prone to cracking, which renders the garment unusable. An additional problem for the health-care facility is the problem of apron disposal. Lead is considered to be the gold standard in X-ray protection. The American Society for Testing Materials (ASTM) guidelines have recommended 0.5-mm lead equivalent garments for standard protection. However, the ASTM has not devised a standard protocol for testing radiological equipment in the health-care field. Traditionally, private companies have tested their product in a single radiological dose (usually 100 kVp), or at the specific dose that the lightest material composite can achieve 0.5 mm of lead equivalency. We chose to evaluate five different levels of kVp (60–130). This is the field where approximately 99% of radiologic energy is utilized in the medical environment. Data from studied manufacturers are published only at 100 kVp. These data correlated with the findings of our study at 100 kVp. However, by evaluating other levels of radiation exposure we were able to elucidate a trend for different composites at both lower and higher energies. At various levels of energy (or keV), lead has been shown to predictably reduce X-ray transmission as a function of thickness. For example, a 0.25-mm lead foil has known values of X-ray transmission reduction at various levels of energy. When an attenuating material reduces a certain G.J. Scuderi et al. / The Spine Journal 6 (2006) 577–582 Table 2 Lead equivalencies and % transmission of lead at 100, 120, and 130 keV X-ray energies 100 kVp Lead equivalency (mm) 0.25 Apron 0.35 Apron 0.50 Apron Transmission (%) 0.25 Apron 0.35 Apron 0.50 Apron 120 kVp 130 kVp 0.24 0.39 0.54 0.25 0.39 0.55 0.25 0.39 0.54 11.50 5.73 3.14 13.69 7.22 4.00 14.85 8.01 4.50 keV by the same percentage as a 0.25-mm piece of lead foil, that material is described as having a lead equivalence of 0.25 mm of lead at that keV. Low-lead or lead-free composites will market their product’s attenuation ability at either a percent reduction in transmission or as a function of lead equivalence. These values are usually referenced at a certain energy level or kVp. The usual kVp quoted is 80 or 100 kVp. In order to communicate the effectiveness of X-ray attenuation, various terms such as lead equivalency and percent transmission are often used. The percent transmission refers to the amount or percent of radiation transmission that is allowed to pass through a material at a certain amount of energy or keV. With all attenuators, the higher the keV, the more difficult it is to attenuate, and hence the higher the transmission. We focused on a range of energy levels currently encountered in the performance of minimally invasive spinal procedures. In the United States, most state regulations require that the X-ray aprons have a lead equivalence of 0.5 mm of lead. As such, the wearer could predict his or her level of protection at various levels of energy or keV. The difficulty arises with the introduction of lead substitutes. Convention has dictated that companies advertise their lead substitute products at 0.5 mm of lead equivalency at 100 keV. When a manufacturer claims that their reduced or lead-free apron has a lead equivalence of 0.5 mm at 80 kVp, the wearer should not assume that the apron will perform similar to the same thickness of lead at other kVp values because it is not lead. This is especially pertinent for medical personnel who are exposed to higher X-ray energies during lengthy or complicated fluoroscopic procedures. The clinician/purchaser of radiological protective gear needs to be aware of this fact in order to properly evaluate the efficiency of differing materials used for lead substitution. Table 3 Comparison of weights Product name No. of layers (area of 1 layer 5 4 in2) Weight (g) Demron EarthSafe Xenolite 4 5 5 16.4 19.5 17 581 In this study, we compared three popular reduced lead or lead-free composites with lead and their ability to attenuate X-ray radiation at various energies. The most common lead substitutes for medical radiation exposure protection are EarthSafe, Xenolite, and Demron. The manufacturers of each product claim that their composite material possesses similar attenuation coefficients as traditional lead-based garments. Although the exact composition of these materials is proprietary and is protected by patents, both EarthSafe and Xenolite are composed of varying amounts of tin, antimony, arsenic, and cadmium in addition to other unknown materials. The manufacturer of Demron discloses the presence of bismuth, barium, tungsten, iodine, as well as proprietary nanocomposites which contribute to its structure and ability to attenuate radiation. In summary, all materials tested in this study demonstrated effectiveness in radiation attenuation at 100 keV. This level of protection may not be relevant in today’s newer fluoroscopic procedures, which use radiation sources of higher energy for longer periods of time. It appears from this study that Demron is best able to shield ionizing radiation of higher energy. Demron was the only material to maintain very low percent transmission over 120 and 130 keV, and was the only composite that provided satisfactory protection at energies superseding 100 keV. In fact, the composite material in Demron attenuated ionizing radiation better than lead at higher energies. Additionally, Demron’s physical characteristics as a flexible fabric may enable the life of the material to be significantly prolonged. Both EarthSafe and Xenolite contain tin, which may hinder flexibility. Because it is lead-free, Demron is nontoxic, washable, and easily disposable without environmental concerns. The reduced weight of Demron compared with lead may reduce the incidence of musculoskeletal complaints for medical personnel involved in lengthy fluoroscopic procedures. References [1] Kruger R, Faciszewski T. Radiation dose reduction to medical staff during vertebroplasty: a review of techniques and methods to mitigate occupational dose. Spine 2003;28:1608–13. [2] Rampersaud YR, Foley KT, Shen AC, Williams S, Solomito M. Radiation exposure to the spine surgeon during fluoroscopically assisted pedicle screw instrumentation. Spine 2000;25:2637–45. [3] Wall BF. Radiation protection dosimetry for diagnostic radiology patients. Radiat Prot Dosimetry 2004;109:409–19. [4] Mettler FA Jr. Medical perspective on ways to improve radiation protection standards. Health Phys 2004;87:289–92. [5] Yaffe MJ, Mawdsley GE, Lilley M, Servant R, Reh G. Composite materials for x-ray protection. Health Phys 1991;60:661–4. [6] Norris TG. Radiation safety in fluoroscopy. Radiol Techniques 2002;73:511–33. [7] Brateman L. Radiation safety considerations for diagnostic radiology personnel. Radiographics 1999;19:1037–55. [8] Tasbas BA, Yagmurlu MF, Bayrakci K, Ucaner A, Heybeli M. Which one is at risk in intraoperative fluoroscopy? Assistant surgeon or orthopaedic surgeon? Arch Orthop Trauma Surg 2003;123:242–4. Epub 2003 May 10. [9] Birch R, Marshall M, Ardran GM. Catalogue of spectral data for diagnostic X-rays. London: Hospital Physicists’ Association, 1979. 582 G.J. Scuderi / The Spine Journal 6 (2006) 577–582 [10] Johlin FC, Pelsang RE, Greenleaf M. Phantom study to determine radiation exposure to medical personnel involved in ERCP fluoroscopy and its reduction through equipment and behavior modifications. Am J Gastroenterol 2002;97:893–7. [11] Kuon E, Schmitt M, Dahm JB. Significant reduction of radiation exposure to operator and staff during cardiac interventions by analysis 125 Years Ago in Spine of radiation leakage and improved lead shielding. Am J Cardiol 2002;89:44–9. [12] Simons GR, Orrison WW Jr. Use of a sterile, disposable, radiationabsorbing shield reduces occupational exposure to scatter radiation during pectoral device implantation. Pacing Clin Electrophysiol 2004;27(6 Pt 1):726–9. stretch test was Forst’s doctoral thesis [1]. That Laza K. Lazarevic had published the same observation the year before in the Serbian literature [2] did not keep the sign from being named for Laséque. References J.J. Forst, a pupil of E.C. Laséque, first reported the sign of nerve root irritation that had been observed by his mentor. The description of the sciatic [1] Forst JJ. Contribution à l’étude clinique de la sciatique. Paris, Thèse No. 33, 1881. [2] Lazarevic LK. Srpski Arh. 7:23. Cited in: Rang M. Anthology of orthopaedics 1966. Edinburgh: Churchill Livingstone, 1966:150.











© Copyright 2026