
FOR HKMA CME MEMBER USE ONLY. DO NOT REPRODUCE OR...
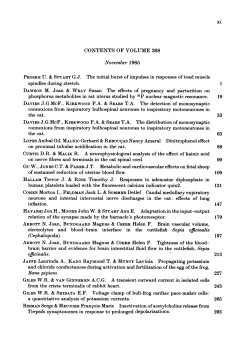
FOR HKMA CME MEMBER USE ONLY. DO NOT REPRODUCE OR DISTRIBUTE. International Journal of Pediatric Otorhinolaryngology (2005) 69, 1521—1528 www.elsevier.com/locate/ijporl Pediatric facial nerve paralysis: Patients, management and outcomes Adele Karen Evans a, Gregory Licameli a,b, Scott Brietzke c, Kenneth Whittemore d, Margaret Kenna a,b,* a Department of Otology and Laryngology, Harvard Medical School, 243 Charles Street, Boston, MA 02214, USA b Department of Otolaryngology and Communication Disorders, Children’s Hospital Boston, Fegan 9, 300 Longwood Avenue, Boston, MA 02215, USA c Walter Reed Army Medical Center, 6900 Georgia Avenue, NW, Washington, DC 20307-5001, USA d Department of Otolaryngology, University of Rochester School of Medicine, 2365 S. Clinton Street, Rochester, NY 14618, USA Received 19 January 2005; accepted 18 April 2005 KEYWORDS Facial nerve paralysis; Bell’s palsy; Otitis media; Temporal bone; Pediatric Summary Objective: To characterize the causes and treatment of facial nerve paresis (FNP) in pediatric patients. Method: Retrospective study in a tertiary care pediatric hospital. Thirty-four patients identified with partial or complete FNP evaluated between 1997 and 2003. A review of the medical records including sex, age, laterality, etiology, therapy, severity of paralysis according to House—Brackman (HB) six-point grading scale, duration, and degree of recovery. Results: Thirty-five cases of FNP. Causes of FNP were infectious (13), traumatic (7), iatrogenic (5), congenital (4), Bell’s/Idiopathic (3), relapsing (2) and neoplastic (1). Peak age distributions for both infectious and traumatic etiologies were bimodal: 1—3 and 8—12 years. Of the 13 infectious cases, 11 were associated with acute otitis media with effusion (AOME). Four (4/11) were bacterial-culture negative. Seven (7/11) were bacterialculture positive, four (4/7) of which required prolonged, broth-medium culture. Bacteria cultured predominantly included Staphylococcus non-aureus species (5/7) and Propionobacterium acnes (3/7). One (1/13) was viral culture positive (Herpes Simplex Virus). * Corresponding author. Tel.: +1 617 355 4534; fax: +1 617 730 0337. E-mail addresses: [email protected] (A.K. Evans), [email protected] (G. Licameli), [email protected] (S. Brietzke), [email protected] (K. Whittemore), [email protected] (M. Kenna). 0165-5876/$ — see front matter # 2005 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.ijporl.2005.04.025 FOR HKMA CME MEMBER USE ONLY. DO NOT REPRODUCE OR DISTRIBUTE. FOR HKMA CME MEMBER USE ONLY. DO NOT REPRODUCE OR DISTRIBUTE. 1522 A.K. Evans et al. All six patients who received intravenous steroids for OME-associated FNP received the doses within the first week of presentation and had complete recovery (HB I/VI); three of five patients who did not receive steroids had complete recovery. There were five iatrogenic cases; two (2/5) were planned surgical sacrifices and three (3/5) were complications of middle ear/mastoid surgery. Facial nerve function associated with infection returned in 0.5—2 months while, when associated with trauma, returned in 0.25—30 months. Conclusions: In infectious or traumatic FNP, children aged 1—3 and 8—12 years are the primary groups involved. In AOME FNP, culture-identified organisms may not be representative of traditional pathogens. Infectious FNP averaged 1 month for recovery while traumatic FNP averaged 9 months. Intravenous steroid therapy may improve the outcome. Recovery was complete (HB I/VI) in 8/10 infectious and 4/6 traumatic cases. # 2005 Elsevier Ireland Ltd. All rights reserved. 1. Introduction Paralysis of the seventh cranial nerve, the facial nerve, is usually immediately obvious. Whether it develops in a child or an adult, it results in weakness of the musculature of the face, impacting verbal communication, social interaction with respect to facial expression, oral competence, taste and, most importantly, protection of the cornea, ocular globe and vision. Such a paralysis can seem devastating when it occurs in a child and parents present with not unreasonable concerns for the well-being of their child. Questions arise regarding the reason that their child has been affected, the utility of treatment modalities, the anticipated outcome, and the duration of time until recovery is complete. Whereas several studies began to address these issues, the largest of these studies are now years to decades old [1—3]. With several recent patients presenting to the emergency ward at Children’s Hospital Boston, our group began to ask the following questions: Is FNP occurring more frequently? What is the distribution of patients in our population, regarding age, year of onset, and etiology of onset? What is the anticipated duration of symptoms? What have been our management techniques? What are our outcomes? 2. Methods A literature search for the years 1977 to October 2003 using the NLM PubMed using the keyword groups ‘‘facial nerve paralysis pediatrics’’ and ‘‘facial nerve paralysis otitis media’’ was performed. Pertinent articles identified were published in 2003, 2000, 1990, 1981, 1974 and 1972. The Children’s Hospital Boston Otolaryngology Foundation records were searched from 1997 to 2003 for the following diagnostic codes and their associated representative diagnoses: 767.5 (facial nerve injury with facial paralysis–—birth trauma), 951.4 (injury to facial nerve–—trauma), 998.2 (accidental iatrogenic injury), 351.0 (Bell’s Paralysis–— unilateral facial nerve paralysis due to lesion on nerve), 351.8 (other facial nerve disorders), 351.9 (other facial nerve disorder, NOS). The Children’s Hospital Boston IRB approved the retrospective chart review proposal. The electronic charts, hospital records and foundation records were then reviewed for detailed information, which included sex, age at presentation, the results of middle ear cultures, the results of temporal bone imaging studies obtained, the details of pertinent operative reports and the outcomes, including degree of and time to recovery. The House—Brackman grade scale for facial nerve paralysis recovery was used to classify the degree of paralysis at the nadir and after recovery. This information was compiled into a database using Microsoft Excel_XP#, removing all unique identifiers in compliance with HIPAA regulations. Analysis was then performed using the database, with more extensive evaluation performed for the patients whose facial nerve diagnosis was of infectious or traumatic etiology. Medical records were available with sufficient data for 34 patients. 3. Results There were 35 cases of FNP identified. There were 14 (40%) males and 21 (60%) females affected. The left facial nerve was affected in 15 (43%) cases; the right facial nerve was affected in 19 (54%) cases, and one case was not recorded (2.9%). Thirteen cases of facial nerve paralysis were of infectious etiology (37%); this was followed by traumatic (7 cases, 20%), iatrogenic (5 cases, 14%), congenital (4 cases, 11%), Bell’s/ idiopathic (3 cases, 9%), relapsing (2 cases, 6%), and neoplastic (1 case, 3%). Basic patient demographics are detailed in Table 1, and the mechanism of paralysis and the outcome is listed in Table 2. The overall average age at presentation was 7.32 years (range: 2.4 months—20 years). However for FOR HKMA CME MEMBER USE ONLY. DO NOT REPRODUCE OR DISTRIBUTE. FOR HKMA CME MEMBER USE ONLY. DO NOT REPRODUCE OR DISTRIBUTE. Pediatric facial nerve paralysis: Patients, management and outcomes 1523 Table 1 FNP patient demographics Case # Age (years) Gender Side Etiology Mechanism 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 0.7 1.1 12 1.8 12 12 10 9 3 14 2.5 2 13 10 8 2 9 10 1.75 6 5 3.8 0.5 0.2 1.6 14 15 M M F F F M F M F F M F F M F F F M F F F M M F F F M F M M F F M F M L R R L R R L R R L R R ? L L R L L L L R R R L R R R R L L L R R L>R R Infectious Infectious Infectious Infectious Infectious Infectious Infectious Infectious Infectious Infectious Infectious Infectious Infectious Trauma Trauma Trauma Trauma Trauma Trauma Trauma Neoplasm Congenital Congenital Congenital Congenital Idiopathic Idiopathic Idiopathic Iatrogenic Iatrogenic Iatrogenic Iatrogenic Iatrogenic Relapsing Relapsing AOM w/o mastoiditis AOM w/o mastoiditis AOM w/o mastoiditis AOM w/o mastoiditis AOM w/o mastoiditis AOM w/mastoiditis AOM w/o mastoiditis AOM w/o mastoiditis AOM w/o mastoiditis AMO w/mastoiditis AOM w/o mastoiditis MAI HSV Blunt trauma to cheek Blunt trauma to cheek T-bone frx (ped v MV) T-bone frx (seizure/fall) T-bone frx (sledding) bil T-bone frx (ped v MV) Snowball to cheek Embryonal rhabdomyosarcoma R cheek COM AD; ? ME mass on CT Goldenhar syndrome; small CN7 by CT CN 12 palsy CHARGE 14 19 17 1.6 20 3.5 0.75 both traumatic and infectious causes there was a bimodal distribution of ages, with average peaks at approximately 2 years (1.85—2.38 years) and 11.5 years (8.6—11.71 years) of age (see Fig. 1). 3.1. Infectious There were 13 patients diagnosed with facial nerve paralysis of infectious etiology. Of these thirteen Fig. 1 Age distribution of facial nerve palsy patients. Resxn of nasal angiofibroma w/MCF extension Transparotid Infratemporal Fossa Approach AS tympanomastoidectomy s/p cochlear implant Tympanoplasty dx hemiplegic migraine patients, one was diagnosed with disseminated Herpes simplex virus and one with Mycobacterium avium-intracellulare complex parotitis. There were 11 cases of facial nerve paralysis due to acute otitis media. Seven cases (64%) involved the right and 4 cases (36%) involved the left. Although the overall average age at presentation for the infectious group was 7.1 years, there was a clear bimodal distribution with peaks at 1.85 and 11.7 years. Two patients were clearly diagnosed with acute coalescent mastoiditis based on physical exam and CT scan findings involving the temporal bone. One patient had a strong history of chronic otitis media; one patient had a remote childhood history of Eustachian tube dysfunction. The House—Brackman (HB) grading scale was used to characterize all patients with an infectious etiology at the nadir of function [4]. The findings are detailed in Fig. 2. FOR HKMA CME MEMBER USE ONLY. DO NOT REPRODUCE OR DISTRIBUTE. FOR HKMA CME MEMBER USE ONLY. DO NOT REPRODUCE OR DISTRIBUTE. 1524 A.K. Evans et al. Table 2 FNP outcomes Case # Etiology Initial H-B grade Outcome H-B grade Duration (month) 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 Infectious Infectious Infectious Infectious Infectious Infectious Infectious Infectious Infectious Infectious Infectious Infectious Infectious Trauma Trauma Trauma Trauma Trauma Trauma Trauma Neoplasm Congenital Congenital Congenital Congenital Idiopathic Idiopathic Idiopathic Iatrogenic Iatrogenic Iatrogenic Iatrogenic Iatrogenic Relapsing Relapsing 6/6 6/6 6/6 6/6 5/6 4/6 5/6 6/6 2/6 2/6—3/6 6/6 5/6 6/6 2/6—3/6 6/6 6/6 6/6 6/6 6/6 6/6 NA NA 3/6 4/6—5/6 6/6 6/6 NA 3/6 NA NA 6/6 6/6 3/6 NA NA 1/6 1/6 1/6 1/6 1/6 NA 1/6 1/6 2/6 2/6 Deceased NA 1/6 1/6 2/6 3/6 1/6 1/6 NA 1/6 1/6 a NA NA NA 6/6 1/6 1/6 1/6 NA NA 1/6 1/6 1/6 1/6 1/6 1 1 0.5 0.75 1.25 NA 2 0.5 0.5 NA Deceased NA 0.38 <0.25 6 30 1 2 NA 2 60 NA NA NA 72 <1 8 1 NA NA 4 2.5 2 NA NA a Eye only, after free flap reconstruction with heavy scarring in the buccal and marginal branch distributions. In patients with otitis media, myringotomy and ventilation tube placement was performed in all 11 patients (100%). Mastoidectomy was performed in one patient (9.5%). Intravenous antibiotics were administered to all 11 patients (100%). Intravenous antibiotics were used while the child was an inpatient and switched to oral antibiotics for outpatient care. Topical antibiotic drops containing topical steroids, most often neomycin/polymixin B/hydrocortisone otic suspension or solution or ciprofloxacin/hydrocortisone solution, were used in all 11 patients (100%). Intravenous steroids, usually dexamethasone, were administered to five patients. In the 11 cases associated with acute otitis media with effusion, a sample of middle ear fluid was obtained and sent to the Microbiology Lab for Gram stain and culture. Data was not available for one patient. Of the seven bacterial-culture positive results, three specimens grew immediately on plates. Four specimens resulted in no growth on plates, but demonstrated growth in broth with prolonged culture. Four specimens had a final report of no growth. Viral culture was obtained for one patient, revealing Herpes Simplex Virus (HSV). Overall, culture results demonstrated Staphylococcus non-aureus species in five (5/7) cases, Pro- Fig. 2 Degree of loss of facial nerve function. FOR HKMA CME MEMBER USE ONLY. DO NOT REPRODUCE OR DISTRIBUTE. FOR HKMA CME MEMBER USE ONLY. DO NOT REPRODUCE OR DISTRIBUTE. Pediatric facial nerve paralysis: Patients, management and outcomes Fig. 3 Degree of recovery of facial nerve function. 1525 Four patients (57%) were treated with steroids. One had a nadir HB grade of VI/VI and had complete recovery. One had a nadir HB grade of VI/VI and had a near-complete recovery to HB grade II/VI. One had a nadir HB grade of III/VI and complete recovery. The degree of recovery was not available for one patient who had a nadir HB grade of VI/VI. Results of recovery are detailed in Fig. 3. The average length of duration of the paralysis for the six trauma patients with complete follow-up was 6.875 months. pionobacterium acnes in three (3/7) cases, Streptococcus viridans in two (2/7) cases, Staphylococcus aureus in one (1/7) case, and Corynebacterium afermentans in one (1/7) case. Four (4/7) cultures had polymicrobial growth. The results of recovery are detailed in Fig. 3. There were three cases without available outcome measures: one patient died of his underlying leukemia before recovery of his FNP and two patients had no documented follow-up visits. The average length of paralysis for these 10 patients until resolution was 0.875 months. 3.3. Congenital 3.2. Trauma Two (2/5) of our iatrogenic etiologies were the anticipated result of a surgical procedure performed to access the parapharyngeal space and the skull base for resection of a tumor. In these cases, the facial nerve branches were identified, labeled, transected, and then neurorrhaphy was performed for each branch. Outcome data was not available for these patients. The other three (3/5) iatrogenic cases occurred with cases of middle ear surgery, two delayed and one immediate in onset. In no case was there direct evidence of damage to the facial nerve either at the time of the original surgery or upon re-exploration. In the first case a mastoidectomy and tympanoplasty was performed for chronic otitis media with cholesteatoma in a patient with Smith-Lemli-Opitz Syndrome and pre-operative facial asymmetry. One week after surgery, she developed a facial nerve paralysis. She was not explored, but she was treated with systemic steroids. She recovered function over the course of 5 months. The second patient was a healthy teenage male who underwent an uncomplicated Type-I tympanoplasty. On post-operative day 4, he noted onset and progression over a few hours of an ipsilateral facial nerve paralysis. He was treated with steroids and antivirals, and he underwent surgical exploration with removal of middle-ear Gelfoam1 packing. He completely recovered facial nerve function within 2 months. There were seven cases of facial nerve paralysis due to traumatic injury. Two occurred in males, five occurred in females. One case involved the right side, six cases involved the left. Although the overall average age at presentation for the group was 5.8 years, there was a clear bimodal distribution with peaks at 2.38 and 8.6 years. The predominant traumatic mechanisms included blunt trauma to the cheek (n = 3) (a direct hit from a flying snowball, running into a pole while trying to look over the shoulder, and ‘‘blunt trauma to the cheek’’) and temporal bone fracture (n = 4) (sledding, fall during seizure and in two direct strikes by motor vehicles). The HB grading scale was used to characterize all seven of these patients at the nadir of function. The findings are detailed in Fig. 2. Six (6/7) of the patients underwent CTscan of the temporal bone. Of these patients, three (3/6) had significant, associated CT findings (congenital absence of the parotid gland, temporal bone fracture, skull base fracture, extraparotid facial nerve edema). The seventh patient (1/7) underwent MRI evaluation with resultant significant MRI findings. One patient (14%) underwent operative management of the injury with middle ear exploration and decompression of the facial nerve. This patient had a nadir HB grade of VI/VI and recovered to HB III/VI (normal resting tone, eye closure with effort, moderate weakness). Of our five patients with congenital facial nerve paralysis, two (2/5) had craniofacial syndromes and a third (1/5) patient had multiple cranial nerve neuropathies. One (1/5) patient had a suggestion of a middle ear mass by CT scan and underwent surgical exploration that was unrevealing of an etiology. Outcomes data were not available for this group of patients. 3.4. Iatrogenic FOR HKMA CME MEMBER USE ONLY. DO NOT REPRODUCE OR DISTRIBUTE. FOR HKMA CME MEMBER USE ONLY. DO NOT REPRODUCE OR DISTRIBUTE. 1526 A.K. Evans et al. The third patient had a history of profound sensorineural hearing loss and underwent simple mastoidectomy with facial recess approach to the round window for cochlear implantation. Complete paralysis on the operated side was noted upon awakening. She was treated with systemic steroids and explored with facial nerve decompression 48 h later. She recovered completely. 3.5. Bell’s/idiopathic Three (3/3) patients with Bell’s palsy or idiopathic facial nerve paralysis were treated with steroids, and two (2/3) were treated with antiviral agents and antibiotics. Two (2/3) of them had evidence on MRI of contrast-enhancement of a segment of the facial nerve. All three patients completely recovered nerve function. 3.6. Relapsing There were two patients with diagnoses of relapsing facial nerve paralysis. One patient presented at 3.5 years of age with bilateral involvement, the left side more frequently than the right. The paralysis consisted of 45—60 s of facial droop followed by complete resolution. The patient had no significant findings on MRI. This patient’s ultimate diagnosis was hemiplegic migraine. The second patient presented at the age of 9 months with a right-sided relapsing facial nerve paralysis that lasted anywhere from 1 week to 1 month at a time. Events were followed by complete resolution of the paralysis. There were no significant findings on CT scan of the temporal bone or on MRI. No further diagnosis was given. 3.7. Neoplastic Our single case of neoplasm-associated facial nerve paralysis was due to an embryonal cell rhabdomyosarcoma of the cheek in a 5-year-old patient. Management included resection of the lesion and reconstruction of the defect with a myoadipofascial free flap. She had excellent eye closure 5 years postoperatively, but heavy scarring in the buccal and marginal branch distributions made isolated assessment of VII function difficult. 4. Discussion In 1972, a large study of pediatric facial nerve paralysis was conducted at the Kaiser-Permanente Facial Paralysis Clinic in Oakland, California. In this study, 61 children under the age of 14 were diag- nosed with facial nerve paralysis. This study determined demographics of facial nerve paralysis in a primary care establishment whose patient population closely reflected the demographics of the entire region of Northern California. More than 50% were diagnosed with Bell’s Paralysis; other palsies were secondary to otitis media (9.8%), birth trauma (7.1%), other infections (6.5%), neoplasia (Histiocytosis-X) (3.2%), other trauma (3.2%), congenital (3.2%) and unknown (3.2%) [5]. Similarly, May et al. in Pittsburgh published a comprehensive article in 1981 reviewing 170 cases of pediatric facial nerve paralysis over 17 years and discussing differential diagnosis of pediatric facial nerve paralysis. In this study, Bell’s Paralysis represented the ultimate diagnosis in 42% of the patients. Other causes included trauma (15%), otitis media (12%), congenital (7.6%), birth trauma (5%) and neoplasia (4%) [1]. In contrast to those results are the results published by Dr. Grundfast et al. in 1990 from the Children’s National Medical Center in Washington, DC. Twenty-five patients were diagnosed with a facial nerve paralysis; 84% were due to specific etiology or were associated with a recognizable syndrome and only 16% were ultimately diagnosed as Bell’s Palsy. Specific causes were trauma (24%), otitis media (16%), other infectious agents (12%), neoplastic origin (12%), and congenital (8%). One patient (4%) presented with paralysis secondary to osteopetrosa tarda [2]. In our study, infectious causes were the most common etiologies of the facial nerve paralysis, representing 36% of the cases. This was followed by trauma (19%), iatrogenic (14%), congenital (14%), Bell’s/idiopathic (8%), relapsing (6%) and neoplastic (3%). Our data is similar to the Grundfast et al. data. Both data sets underscore the importance of searching for the specific etiology of a facial nerve paralysis (i.e., otitis media, trauma, neoplasm) in order to provide the appropriate treatment for the paralysis (i.e., antibacterials, antivirals, steroids, surgical decompression) as well as to identify any occult disorder (i.e., CNS or temporal bone neoplasm). The largest single cause of FNP in our series was acute otitis media. The age distribution was bimodal, with peaks at 1.85 and 11.7 years. In 10/11 cases, true coalescent mastoiditis was not present. The one patient who underwent mastoidectomy had an acute episode of otitis media superimposed on a chronic otitis media. In 1998, Drs. Joseph and Sperling published a small series of case reports in which adult patients with acute otitis media presented with acute facial nerve paralysis. Despite the fact that the patients were all treated for the acute otitis media with FOR HKMA CME MEMBER USE ONLY. DO NOT REPRODUCE OR DISTRIBUTE. FOR HKMA CME MEMBER USE ONLY. DO NOT REPRODUCE OR DISTRIBUTE. Pediatric facial nerve paralysis: Patients, management and outcomes antibiotics, they developed a facial nerve paralysis. Of the three patients, two patients had a dry ear on myringotomy and one patient had serous effusion [6]. All three patients recovered facial nerve function within a few weeks of myringotomy. Similarly, most of our patients had already started antibiotic therapy for otitis media prior to presentation. All patients went to the OR for myringotomy and tympanostomy tube placement. They all received intravenous antibiotics. Half of the patients received intravenous steroids. Although few ears contained frankly purulent effusions at myringotomy, effusion was present in all patients. Often, organisms were not readily isolated from the intraoperative cultures. Broth inoculation grew Staphylococcus non-aureus species (5/7), Propionobacterium acnes (4/7), Streptococcus viridans (2/7), Staphylococcus aureus (1/7) and Corynebacterium afermentans (1/7). Controversy will exist as to whether these were etiologic organisms or contaminants. Drs. Elliot, Zalzal and Gottlieb published an outcomes study in 1996 in which they reviewed the etiology, management and outcomes of 10 pediatric patients who presented with facial nerve paralysis due to otitis media. Their ultimate findings were that incomplete paralysis recovered more quickly than did complete paralysis [3]. Given the overall small population in our study and even smaller population with only partial paralysis, it is difficult to refute or support this statement with our data. 4.1. Trauma Our second greatest etiologic contribution came from trauma, representing 19% of the patient population. Interestingly, more commonly girls were affected. Again, there was a bimodal age distribution, with peaks at 2.38 and 8.6 years of age. The majority of patients had a complete paralysis (VI/ VI). This group did contain blunt facial trauma and temporal bone fractures. Our patient group did not contain any patients with birth-associated facial nerve paralysis. A 1990 study of congenital facial nerve paralysis conducted at Brigham & Women’s Hospital yielded results that may well be considered applicable to blunt facial nerve trauma. In this study, 81 acquired cases were identified in 92 documented congenital facial nerve pareses. They found the acquired pareses to be associated with forceps delivery, delivery weight of 3500 g or more and primaparity. Of those patients for whom follow-up was adequate, there was an 89% complete recov- 1527 ery rate and a mean recovery time of nearly 3 years [7]. A large French study published in 2001 compared medical and surgical management and outcomes of temporal bone fractures. They found that 98% of medically managed fractures associated with facial nerve paralysis resulted in recovery of function to normal or near-normal (House—Brackman grade I— II/VI). Surgical management identified a nerve gap in only 14% of cases. It resulted in a 94% recovery to normal or near-normal (House—Brackman grade I— III/VI) at 2 years post-operatively [8]. Half of our trauma patients underwent imaging studies of the temporal bone with identification of a lesion (i.e., congenital absence of the parotid gland, temporal bone fracture, skull base fracture, extraparotid facial nerve edema). Four of the seven of the patients were treated with steroids independent of the CT or MRI findings. Only one patient underwent surgical management. Four patients experienced complete recovery (HB grade I/VI) and one experienced near-complete recovery (HB grade II/VI) with an average duration of approximately 10 months. As a group, these good outcomes reflect the results obtained by Falco and Eriksson, and Darrouzet et al. In contrast to both studies, less than a year was adequate time for recovery of function rather than 2 years. 4.2. Iatrogenic At our hospital, a total of 919 surgeries involving the temporal bone were performed throughout the duration of this study. Of those surgeries, 467 involved myringoplasty and/or tympanotomy without mastoidectomy; 178 involved mastoidotomy or simple mastoidectomy with or without ossiculoplasty; 51 involved radical or modified radical mastoidectomy; and 223 involved middle cranial fossa approach, posterior cranial fossa approach or the implantation of cochlear devices. There were only three unanticipated iatrogenic complications that resulted in facial nerve paralysis, a rate of 0.3%. All three patients experienced complete recovery to baseline function with a mean time to recovery of 2.8 months. It would be safe to say that this complication is very rare and expected to be fully reversible if no direct damage to the facial nerve occurred intraoperatively. 5. Conclusions Facial nerve paresis or paralysis has a tremendous impact on the patient as well as the family, particularly when a pediatric patient is involved. Tod- FOR HKMA CME MEMBER USE ONLY. DO NOT REPRODUCE OR DISTRIBUTE. FOR HKMA CME MEMBER USE ONLY. DO NOT REPRODUCE OR DISTRIBUTE. 1528 A.K. Evans et al. dlers (children between ages 1 and 3 years) and preteenagers (between ages 8 and 12 years) may be at higher risk for facial nerve paralysis due to infectious and traumatic causes. These complications of infection and facial or temporal bone trauma are still rare. Other broad categories of differential diagnoses include congenital defects, neoplasms, idiopathic/Bell’s palsy, and iatrogenic injury during facial or middle ear surgery. Recovery of facial nerve paralysis usually takes 1 month or less in cases of infectious etiology but 8 months in cases of traumatic etiology. In these cases, recovery is nearly always substantial (II/VI) to complete (I/VI), except in cases of laceration and reconstruction. The date concerning infectious etiologies for facial nerve paralysis provides new information for the pediatric population and supports similar data in the adult population. This article exemplifies the need for prospective study of treatment algorithms to answer clinical questions regarding management in contrast to the available retrospective review which helps us to define the questions. References [1] M. May, T. Fria, F. Blumenthal, H. Curtin, Facial paralysis in children: differential diagnosis, Otolaryngol. Head Neck Surg. 89 (1981) 841—848. [2] K.M. Grundfast, J.L. Guarisco, J.R. Thomsen, B. Koch, Diverse etiologies of facial paralysis in children, Int. J. Pediatr. Otorhinolaryngol. 19 (1990) 223—239. [3] C.A. Elliott, G.H. Zalzal, W.R. Gottlieb, Acute otitis media and facial paralysis in children, Ann. Otol. Rhinol. Laryngol. 105 (1) (1996) 58—62. [4] I.M. Smith, J.A. Murray, R.E. Cull, J. Slattery, A comparison of facial grading systems, Clin. Otolaryngol. 17 (4) (1992) 303— 307. [5] J.J. Manning, K.K. Adour, Facial paralysis in children, Pediatrics 49 (1) (1972) 102—109. [6] E.M. Joseph, N.M. Sperling, Facial nerve paralysis in acute otitis media: cause and management revisited, Otolaryngol. Head Neck Surg. 118 (5) (1998) 694—696. [7] N.A. Falco, E. Eriksson, Facial nerve paralysis in the newborn: incidence and outcome, Plast. Reconstr. Surg. 85 (1) (1990) 1—4. [8] V. Darrouzet, J.Y. Cuclos, D. Liguoro, Y. Truilhe, C. De Bonfils, J.P. Bebear, Management of facial paralysis resulting from temporal bone fractures: our experience in 115 cases, Otolaryngol. Head Neck Surg. 125 (1) (2001) 77—84. FOR HKMA CME MEMBER USE ONLY. DO NOT REPRODUCE OR DISTRIBUTE.









© Copyright 2026