
Blood Culture and Bacteremia Predictors in Infants Less Than
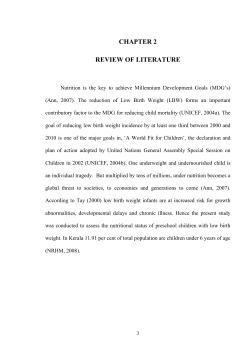
ORIGINAL STUDIES Blood Culture and Bacteremia Predictors in Infants Less Than Three Months of Age With Fever Without Source Borja Gómez, MD, Santiago Mintegi, MD, Javier Benito, MD, Andere Egireun, MD, Diego Garcia, MD, and Eider Astobiza, MD Objectives: (1) To assess the rate of bacteremia in febrile infants less than 3 months of age admitted to a pediatric emergency department at a tertiary hospital; (2) to describe the bacteria isolated; and (3) to analyze factors related to increased probability of having a positive blood culture. Methods: A retrospective, cross-sectional, 5-year descriptive study that includes all infants less than 3 months of age who presented with fever without source (FWS) and had a blood culture performed. Results: A blood culture was performed in 1018 (91.5%) of 1125 infants admitted, and a bacterial pathogen was grown in 23 (2.2%) of these; 8 were associated with a positive urine culture. The most frequently isolated pathogen was Escherichia coli (9), followed by Streptococcus pneumoniae (4). The risk factors detected by multivariate analysis were: (a) being classified as “not well-appearing” (12.5% vs. 1.8%; odds ratio: 8.37) and (b) leukocyturia and/or nitrituria in a urine dipstick test (5.6% vs. 1.6%; odds ratio: 3.73). C-reactive protein value was higher than white blood cell count and absolute neutrophil count in detecting bacteremia; a 70 g/L cut-off had a specificity of 93.8%, but sensitivity of only 69.6%. Conclusions: A positive blood culture rate of 2.2% was found in infants less than 3 months of age with FWS. C-reactive protein, white blood cell count, and absolute neutrophil count were not good bacteremia predictors. We recommend obtaining a blood culture in infants less than 3 months of age with FWS, particularly those patients considered “not well-appearing” and those with leukocyturia and/or nitrituria. Key Words: fever, young infant, blood culture, diagnostic tests, bacteremia (Pediatr Infect Dis J 2010;29: 000 – 000) F ever is the most common reason for healthy young children to be brought to a pediatric emergency department.1,2 Most of these infants have fever without source (FWS). Despite the fact that most cases of FWS are caused by viral infections, for which no treatment is required, they can also be caused by a severe underlying bacterial infection, mainly in young infants.3 Serious bacterial infection (SBI) is found in 10% to 15% of febrile infants younger than 3 months.4 – 6 Infants eventually diagnosed with SBI can appear well and have nonspecific signs. Several management protocols have been designed to evaluate these children to identify those at high risk of developing SBI. The traditional approach to febrile young infants involves performing a white blood cell count (WBC) and blood and urine cultures, administering antibiotics, and Accepted for publication October 20, 2009. From the Paediatric Emergency Department, Cruces Hospital, Barakaldo, Spain. Address for correspondence: Borja Gómez, MD, Paediatric Emergency Department, Cruces Hospital, Plaza de Cruces s/n, Barakaldo, Spain. E-mail: [email protected]. Supplemental digital content is available for this article. Direct URL citations appear in the printed text and are provided in the HTML and PDF versions of this article on the journal’s Web site (www.pidj.com). Copyright © 2009 by Lippincott Williams & Wilkins ISSN: 0891-3668/10/2901-0001 DOI: 10.1097/INF.0b013e3181c6dd14 admitting them to hospital. Recent articles analyzing the usefulness of classic indices such as WBC, absolute neutrophil count (ANC), and C-reactive protein (CRP) for predicting the risk of an SBI at this age have had conflicting results.7–9 Infants have commonly been split into following 3 different age groups: neonates (0 –28 days old), young infants (1–3 months old), and older infants (3–36 months old).10,11 Some authors have recently suggested reducing the cut-off age in febrile young infants to include only children between 1 and 2 months old as young infants.12 In addition, a less aggressive management has been suggested in recently published guidelines for well-appearing infants more than 28 days old.3,13,14 The rate of SBI in young infants has apparently changed in recent years, as have the pathogens producing them. Group B Streptococcus, for example, a classic bacterial pathogen in these children, has been associated with high rates of meningitis (39%), nonmeningeal infection foci (10%), and sepsis (7%).15 The use of intrapartum antibiotic prophylaxis has reduced the incidence of early-onset infections caused by group B Streptococcus, but a parallel reduction in the incidence of late-onset diseases has not been reported.16 –18 The early detection of urinary malformations using prenatal ultrasound19,20 and the introduction of the heptavalent pneumococcal conjugate vaccine21 have also decreased SBI rates in these patients. The objectives of our study were as follows: (1) to assess the rate of bacteremia in febrile infants less than 3 months of age admitted to the Pediatric Emergency Department of a tertiary hospital; (2) to describe the bacteria isolated in these children; and (3) to analyze any factors related to a higher probability of having a positive blood culture. MATERIALS AND METHODS Setting and Participants We conducted a retrospective, cross-sectional, descriptive study that included all infants younger than 90 days of age with FWS admitted to our Pediatric Emergency Department during 5 consecutive years (September 2003 through August 2008). Our tertiary teaching hospital has a Pediatric Emergency Department that provides care for approximately 63,000 children less than 14 years of age every year. Design Data were extracted from our registry of infants with FWS younger than 3 months old. Infants younger than 90 days with a measured temperature ⱖ38.0°C at home or on arrival in the Pediatric Emergency Department are eligible for inclusion in the registry. All subjects received clinical care as determined by the emergency physician. Our Pediatric Emergency Department algorithm for the management of infants less than 3 months of age with FWS recommends urine dipstick testing, CBC, CRP, blood culture, and urine culture for all children. Gram stain of urine is not routinely performed. We consider performing a lumbar puncture, including Gram stain, bacterial culture, viral culture, and enterovirus polymerase chain reaction, on an individual basis. If an infant is well-appearing, over 15 days old, and all ancillary tests appear The Pediatric Infectious Disease Journal • Volume 29, Number 1, January 2010 www.pidj.com | 1 Gómez et al The Pediatric Infectious Disease Journal • Volume 29, Number 1, January 2010 to be normal, we recommend that the patient be discharged without antibiotic treatment after several hours of observation in the Pediatric Emergency Department, generally up to 24 hours after fever developed (this means that if an infant is brought to the Pediatric Emergency Department 6 hours after fever was first registered, this infant remains in our Observation Unit for about 18 hours for clinical evaluation). We recommend hospital admission for infants less than 15 days of age, those with abnormal laboratory tests and when the clinical situation worsens during the patient’s stay in the Observation Unit. Although most guidelines recommend that all febrile infants under 28 to 30 days of age be hospitalized, 16- to 30-day-old infants at our Pediatric Emergency Department are observed in the Observation Unit, as explained above, and then either hospitalized or discharged depending on their clinical evolution. An electronic log of Pediatric Emergency Department visits was reviewed monthly by a pediatric emergency physician to ensure proper identification of all potentially eligible febrile infants and to assess the capture rate for the study. Data Collection Electronic Pediatric Emergency Department medical records were reviewed, and the following data recorded for each patient: demographics (age, gender, month when care was provided), medical history, time elapsed between moment when fever was first detected and when the infant was brought to the hospital, temperature registered at home and at the Pediatric Emergency Department, whether the child appeared ill upon arrival or not, symptoms and findings on physical examination, results of any tests performed, treatment received, diagnosis, site of care, and evolution. Final discharge patient charts were reviewed if the infants were admitted. If infants were not admitted to hospital, a follow-up phone call was made by resident doctors, after training, to assess their evolution. The hospital database was checked to determine whether there had been any new, unscheduled emergency visits after the initial discharge. Definitions • FWS: axillary or rectal temperature at home, or rectal temperature in the Pediatric Emergency Department, of ⱖ38°C, without catarrhal or respiratory symptoms/signs (such as tachypnea) or a diarrheal process, in patients with normal physical examination, according to the diagnostic codes issued by the Spanish Society of Pediatric Emergencies (SEUP).22 Infants were included even if fever was assessed by parents at home without using a thermometer. The degree of sensitivity in terms of subjective fever assessments carried out by parents ranges between 74% and 84%, with a specificity of 76% to 96%.23,24 • Well-appearing: defined by a normal pediatric assessment after being evaluated by a pediatric emergency physician during the first hour after attending the Pediatric Emergency Department. Appearance, respiratory and circulatory items had to be classified as normal for infants to be classified as well-appearing, and data had to be reflected on the patient’s charts. • Positive blood culture: blood culture from which a true bacterial pathogen was grown (Streptococcus pneumoniae, Neisseria meningitidis, Enterococcus, Escherichia coli, Klebsiella pneumoniae, Staphylococcus aureus, group A and B Streptococcus, Listeria monocytogenes, or Salmonella species). Staphylococcus epidermidis, Propionibacterium acnes, and diphtheroids grown from previously healthy immunocompetent infants (with no history of heart disease, ventriculoperitoneal shunt, indwelling catheter, or other prosthetic devices) were categorized as contaminants. • SBI: isolation of a bacterial pathogen from the cerebrospinal fluid (CSF), blood, or urine. 2 | www.pidj.com • Occult bacteremia: positive blood culture in a well-appearing infant diagnosed with FWS. • Bacterial meningitis: (a) positive CSF culture or CSF gram, (b) positive blood culture with pleocytosis. • Urinary tract infection (UTI): growth of more than 50,000 colony forming units/mm3 of a unique bacterial pathogen in a urine sample collected by bladder catheterization. Growth of 10,000 to 50,000 colony forming units/mm3 was also considered an UTI when associated with leukocyturia and or nitrituria. • Previously healthy infant. To be classified as previously healthy, the patient must meet all the following criteria: born at term (after ⱖ37 weeks’ gestation), not treated for unexplained hyperbilirubinemia, not hospitalized longer than the mother, not receiving current or prior antimicrobial therapy, no previous hospitalization, and no chronic or underlying illness. • Low-risk SBI patient. To be classified as a low-risk SBI patient, the infant must meet all the following criteria: previously healthy infant, well-appearing, urine dipstick testing without leukocyturia or nitrituria, WBC between 5000 and 15,000/mm3, ANC ⬍10,000/mm3, no pleocytosis if lumbar puncture was performed, and staying several hours in the Observation Unit with normal clinical evaluations. Exclusion Criteria Patients in whom the history and/or the physical examination performed upon arrival in the Pediatric Emergency Department allowed the origin of the fever to be identified. Patients with fever referred to us by parents reporting a mild nasal congestion were included in the study. Patients with a diarrheal process or certain respiratory symptoms/signs (such as tachypnea, breathing difficulties, wheezing, grunting, nasal flaring, retractions, rhonchi, rales, focal areas of decreased breath sounds) were not included. Risk Factors We analyzed blood culture-positive rates in relation to factors that can easily be assessed before performing a blood culture: general appearance, medical history, gender, sex, highest temperature detected, and urine dipstick result. Statistical Analyses Statistical analyses were conducted using the Statistical Program for the Social Sciences version 15 (SPSS 15, Chicago, IL). Data are expressed as the mean and standard deviation for quantitative variables or numbers and percentages for categorical variables. Continuous data were compared using the Student t test. Categorical data were examined using the 2 test or the Fisher exact test probability test. Statistical significance was defined as P ⬍ 0.05. Prevalence rates were expressed as a percentage with their respective confidence intervals (CI). The performance levels of WBC, ANC, and CRP for identifying bacteremia were assessed by receiver operating characteristics (ROC) curves analysis. ROC curves were constructed by comparing patients with positive and negative blood culture. This study was approved by the Research Committee of the Pediatric Emergency Department. Since the data were extracted from a registry, the information contained in it is anonymous, and that no intervention was performed on patients, informed consent was not requested. RESULTS During the study period, 1125 infants younger than 3 months with FWS were admitted. Blood culture was performed in 1018 cases (91.5%). General information concerning the global sample is provided in Table, Supplemental Digital Content 1, http://links.lww.com/INF/A324. The final diagnoses for all pa© 2009 Lippincott Williams & Wilkins The Pediatric Infectious Disease Journal • Volume 29, Number 1, January 2010 TABLE 1. Final Diagnoses for the 1018 Patients Included in This Study No SBI SBI UTI Occult bacteremia UTI and bacteremia Bacterial meningitis Sepsis Cellulitis Acute otitis media 820 (80.6%) 198 (19.4%) 172 9 8 4 2 2 1 Results are expressed as number (%). tients are listed in Table 1. A true bacterial pathogen grew in 23 (2.2%; CI: 1.3%–3.1%) of the 1018 blood culture cases (Table, Supplemental Digital Content 2, http://links.lww.com/INF/A325). Of them, 8 were associated with a positive urine culture. The most common final diagnoses for these 23 infants with a positive blood culture were occult bacteremia in 9 cases (39.1%, 0.88% of the global sample) and UTI in 8 (34.7%). Blood culture- and occult bacteremia-positive rates by age group are listed in Table 2. Infants in whom blood culture was not performed were older than the study performed (80.4% of patients were older than 2 months vs. 35.2% of those with blood culture; P ⬍ 0.0001); 5 were diagnosed with a UTI and 24 with influenza (positive rapid influenza test). None of them was diagnosed with bacteremia in a posterior unscheduled visit and all of them recovered well. The most frequently isolated bacterial pathogen was Escherichia coli (9 infants, 8 of whom had positive urine cultures) (Table 3). Only 2 samples were positive for Group B Streptococcus (both in infants more than 28 days old who were not wellappearing upon arrival at the Pediatric Emergency Department). Univariate analysis of the risk factors studied is shown in Table 4. All showed an increase in the rate of positive blood culture, although statistical significance could only be shown for general appearance, highest temperature detected, and urine dipstick outcome. The results of a multivariate analysis by polychotomous logistic regression (Table, Supplemental Digital Content 3, http://links.lww.com/INF/A326) showed that only the combination of general appearance (odds ratio: 8.37, CI: 2.84 –21.97, for those who were not well appearing) and urine dipstick outcome (odds ratio: 3.73, CI: 1.54 – 8.80, for those with leukocyturia and/or TABLE 2. Positive Blood Cultures and Occult Bacteremia Cases by Age Age Positive Blood Culture Occult Bacteremia ⱕ1 mo 1–2 mo 2–3 mo 8/243; 3.29% (1.04%–5.53%) 9/417; 2.15% (0.76%–3.55%) 6/358; 1.67% (0.34%–3.00%) 2/243; 0.82% (0%–1.95%) 3/417; 0.71% (0%–1.53%) 4/358; 1.11% (0.02%–2.20%) TABLE 3. Bacteria Isolated From Blood Cultures Bacterium No. Cases Escherichia coli Streptococcus pneumoniae Group B Neisseria meningitidis Enterococcus faecalis Streptococcus agalactiae Klebsiella pneumoniae Staphylococcus aureus 9 4 3 3 2 1 1 © 2009 Lippincott Williams & Wilkins Bacteremia in Infants TABLE 4. Risk of Bacteremia Related to Factors That Can be Assessed Before Performing a Blood Culture (Unadjusted) Risk Factor Positive Blood Culture Medical history Not previously healthy vs 5/119 (4.2%) Previously healthy 18/899 (2.0%) General appearance Not well-appearing vs 6/48 (12.5%) Well-appearing 17/970 (1.8%) Age ⱕ30 d vs 8/243 (3.3%) ⬎30 d 15/775 (1.9%) Gender Male vs 17/585 (2.9%) Female 6/433 (1.4%) Highest temperature detected 38°C–39.5°C vs 17/895 (1.9%) ⱖ39.5°C 6/98 (6.1%) Urine dipstick* Leukocyturia and/or nitrituria vs 10/178 (5.6%) Normal 13/822 (1.6%) OR (95% CI) 2.15 (0.68 – 6.29) 8.01 (2.76 –23.05) 1.72 (0.66 – 4.39) 2.13 (0.78 – 6.09) 3.37 (1.16 –9.36) 3.70 (1.48 –9.19) Results are expressed as number (%). *This information was not recorded for 9 patients. nitrituria) was predictive for a positive blood culture. We therefore designed a flow-chart based on these results to determine the yield of blood culture according to these 2 characteristics (Fig. 1). Exclusion of these factors results in a decrease in the blood culture-positive rate, which means that the rate in well-appearing infants with normal urine dipsticks is 1%. Among the 1018 infants, 217 (21.3%) had a rectal temperature lower than 38°C on arrival in the Pediatric Emergency Department (22 lower than 37°C). In all cases, the parents had recorded a temperature greater than 38°C at home, although in most cases, it is not known whether this temperature was measured rectally or axillary. There were 2 blood culture-positive cases in infants who were afebrile upon arrival in the Pediatric Emergency Department (cases 11 and 15 in Table, Supplemental Digital Content 2, http://links.lww.com/INF/A325) but whose parents had noted fever at home (38.3°C and 40°C, respectively). We also analyzed the value of WBC, ANC, and CRP for predicting bacteremia. The ROC curves for this analysis are shown in Figure, Supplemental Digital Content 5, http://links.lww.com/INF/A328. CRP, at 0.847 (0.754 – 0.940), had the largest area, but the difference between this area and those for ANC and WBC was not statistically significant. A CRP value of 70 g/L had a 93.8% specificity (CI: 92.1%–95.1%) for the detection of positive blood culture and a 99.3% (CI: 98.5%–99.6%) negative predictive value (NPV) in our population, but a sensitivity of only 69.6% (CI: 49.1%– 89.4%). Selecting lower cut-offs does not improve these results: decreasing this cut-off to 20 g/L increased the sensitivity to only 73.9% (CI: 53.5%– 87.5%), and the specificity was reduced to 74.8% (CI: 72.0%–77.5%). The common cut-off points for ANC (ⱖ10,000/mm3) and WBC (ⱖ15,000/mm3) present lower degrees of sensitivity and NPV in our population (data not shown). The selection of well-appearing infants with normal urine dipstick results brought the areas under the ROC curves for CRP, WBC, and ANC closer as the sensitivity and NPV decrease for CRP and increase for WBC and ANC (data not shown). Three infants with a positive blood culture were classified as low-risk SBI patients. As shown in the flow chart, the blood culture-positive rate in low-risk SBI patients was 0.6% (3/480). The use of our low-risk SBI criteria gave a sensitivity of 87% www.pidj.com | 3 The Pediatric Infectious Disease Journal • Volume 29, Number 1, January 2010 Gómez et al FIGURE 1. Flow chart. (67.9%–95.5%) for detecting bacteremia, with a 99.4% NPV (98.2%–99.8%). The mean length of stay of the 464 low-risk SBI infants older than 15 days in the Observation Unit was 11.1 hours. All of the 23 children recovered well, although HIV infection was eventually diagnosed in 1 patient. DISCUSSION Our data (a 2.2% blood culture-positive rate in the global sample; 1% in well-appearing and previously healthy infants with a normal urine dipstick) suggest that a blood culture should be performed in all infants less than 3 months of age with FWS and it is essential in infants with a suspected UTI (leukocyturia and/or nitrituria in the dipstick), in whom the blood culture-positive rate is 4.4%. Some authors have recommended this approach only for infants under 2 months of age.7,8 We found a higher prevalence of positive blood culture among febrile infants younger than 1 month, although the difference was not statistically significant. It may be unnecessary to obtain a blood culture systematically in all febrile infants between 1 and 3 months of age, but a larger sample from a multicenter study is required to negate these recommendations. We are currently considering reducing the cut-off from 3 to 2 months of age and to manage these infants in a similar way to those older than 3 months. The former infants who were previously healthy and well-appearing, with low fever (⬍39.5°C) and with a normal urine dipstick result, would be managed as outpatients without performing CBC, CRP, and blood culture. In our series, 1 infant who met all these requirements had a positive blood culture (E. faecalis; blood culture-positive rate in this group: 0.5%). The most frequently isolated bacterium was E. coli, followed by S. pneumoniae and Group B N. meningitidis. Only 2 cases of S. agalactiae were reported. The systematic screening of women in their third term of pregnancy (rectal and vaginal culture in weeks 35–37) for this bacterium, and the use of intrapartum 4 | www.pidj.com antibiotic prophylaxis, have reduced the incidence of infected newborns.13,14 We use a risk-based approach at our hospital to identify candidates suitable for intrapartum prophylaxis—the pregnant women who receive intrapartum antibiotic prophylaxis (intravenous penicillin) include those with the risk factors listed in Table, Supplemental Digital Content 4, http://links.lww.com/INF/A327. According to our results, the blood culture-positive rate is related to following 2 factors that can be easily evaluated when evaluating a febrile infant: general appearance and urine dipstick result. These factors can help identify infants at increased risk of having bacteremia. UTI, with a prevalence of about 7.5%,25,26 is the most commonly found SBI in young infants. The blood culture-positive rate in patients younger than 3 months with a positive urine culture in our sample was 4.4%, thus highlighting the importance of obtaining a blood culture in young febrile infants with a suspected UTI. The bacteremia rate detected in young infants with a UTI in previous studies was even higher; Bachur and Caputo27 reported an incidence of 21% for infants less than 1 month, 13% for infants 1 to 2 months, and 4% for infants 2 to 3 months. In our study, CRP, WBC, and ANC were not good predictors of bacteremia in young febrile infants as test sensitivity in terms of positive blood culture was quite low and even the use of our low-risk SBI criteria gave a sensitivity of only 87%. Consequently, we do not systematically admit low-risk infants, although we recommend they be monitored in the Observation Unit of our Pediatric Emergency Department for up to 24 hours to detect a possible worsening of their condition irrespective of their CBC, WBC, and ANC values. Hsiao and Baker28 reviewed some of the recent literature on these classic markers. In their 2005 manuscript, they concluded that WBC was neither sensitive nor specific as an indicator of bacteremia and other SBI in infants and that although CRP seems to be a reliable indicator of bacterial infection in children, no study have targeted young infants. © 2009 Lippincott Williams & Wilkins The Pediatric Infectious Disease Journal • Volume 29, Number 1, January 2010 In November 2007, we included the procalcitonin (PCT) in the evaluation of the infant less than 3 months of age with FWS. We have not analyzed the value of this new marker for the detection of bacteremia in this group of infants because, since its introduction, we still have few patients in whom PCT was performed. According to previous studies, PCT offers higher specificity than CRP for differentiating between the viral and bacterial etiology of the fever.29,30 However, to the best of our knowledge, the use of PCT to detect occult bacteremia in young infants has not been studied and most children with SBI included in previous studies evaluating the value of PCT for the detection of SBI were not well-appearing,31,32 which means that its practical utility is not fully established. Maniaci et al33 reported recently that PCT has favorable test characteristics for detecting SBIs in young febrile infants. The figure given for the prevalence of positive blood culture (2.5%) is similar to that in our study. However, only 6 infants with bacteremia were included in this study and, as stated by the authors, 2 of the 6 bacteremia cases were caused by E. coli and their relatively low PCT values should be noted. This study had several limitations. A prospective study would have allowed for better patient follow-up than the retrospective study performed, although the telephone follow-up carried out by a properly trained pediatric resident may serve to minimize this limitation. Second, it was not a multicenter study, so the results might not apply to other populations. Third, the availability of a larger sample would have allowed us to analyze test performance levels in different age groups. The fact that all infants enrolled in this study were evaluated by an experienced pediatric emergency physician in the first hour after arriving in the emergency department can be considered a constraint as regards making these outcomes more widespread. We conclude that the blood culture-positive rate in young febrile infants admitted to a pediatric emergency department is approximately 2% and that higher rates can be related to the infants’ appearance and their dipstick results. Blood culture is important for infants upon admission to the emergency department, although larger samples are required to establish whether a blood culture should or should not be recommended in the case of selected infants over 1 month old. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. REFERENCES 1. Nelson DS, Walsh K, Fleisher GR. Spectrum and frequency of pediatric illness presenting to a general community hospital emergency department. Pediatrics. 1992;90(1 pt 1):5–10. 2. Massin MM, Montesanti J, Gerard P, et al. Spectrum and frequency of illness presenting to a pediatric emergency department. Acta Clin Belg. 2006;61:161–165. 3. Ishimine P. Fever without source in children 0 to 36 months of age. Pediatr Clin North Am. 2006;53:167–194. 4. Baskin MN. The prevalence of serious bacterial infections by age in febrile infants during the first 3 months of life. Pediatr Ann. 1993;22:462– 466. 5. Slater M, Krug SE. Evaluation of the infant with fever without source: an evidence based approach. Emerg Med Clin North Am. 1999;17:97–126. 6. Harper MB. Update on the management of the febrile infant. Clin Pediatr Emerg Med. 2004;5:5–12. 7. Baker MD, Bell LM. Unpredictability of serious bacterial illness in febrile infants from birth to 1 month of age. Arch Pediatr Adolesc Med. 1999;153: 508 –511. 8. Bachur RG, Harper MB. Predictive model for serious bacterial infections among infants younger than 3 months of age. Pediatrics. 2001;108:311–316. 9. Bema K, ChB M, Harper MB. Identifying febrile young infants with bacteremia: is the peripheral white blood cell count an accurate screen? Ann Emerg Med. 2003;42:216 –225. 10. American College of Emergency Physicians Clinical Committee; American College of Emergency Physicians Clinical Policies Subcommittee on Pediatric © 2009 Lippincott Williams & Wilkins 26. 27. 28. 29. 30. 31. 32. 33. Bacteremia in Infants Fever. Clinical policy for children younger than three years presenting to the emergency department with fever. Ann Emerg Med. 2003;42:530–545. Baraff LJ. Editorial: clinical policy for children younger than three years presenting to the emergency department with fever. Ann Emerg Med. 2003;42:546 –549. Cincinnati Children’s Hospital medical Center. Fever of uncertain source in infants 60 days of age or less. Available at: http://www.cincinnatichildrens.org/ svc/alpha/h/health-policy/ev-based/fever-0–60-days.htm. Accessed June 2003. Baker MD, Bell LM, Avner JR. The efficacy of routine outpatient management without antibiotics of fever in selected infants. Pediatrics. 1999; 103:627– 631. Kourtis AP, Sullivan DT, Sathian U. Practice guidelines for the management of febrile infants less than 90 days of age at the ambulatory network of a large pediatric health care system in the United States: summary of new evidence. Clin Pediatr. 2004;43:11–16. Pena BM, Harper MB, Fleischer GR. Occult bacteremia with group B streptococci in an outpatient setting. Pediatrics. 1998;102(1 pt 1):67–72. Schrag SJ, Zywicki S, Farley MM, et al. Group B streptococcal disease in the era of intrapartum antibiotic prophylaxis. N Engl J Med. 2000;342:15–20. Centers for Disease Control and Prevention (CDC). Early-onset and lateonset neonatal group B streptococcal disease–United States, 1996 –2004. Morb Mortal Wkly Rep. 2005;54:1205–1208. Phares CR, Lynfield R, Farley MM. Epidemiology of invasive group B streptococcal disease in the United States, 1999 –2005. JAMA. 2008;299: 2055–2065. Raynor BD. Routine ultrasound in pregnancy. Clin Obstet Gynecol. 2003; 46:882– 889. Sairam S, Al-Habib A, Sasson S, et al. Natural history of fetal hydronephrosis diagnosed on mid-trimester ultrasound. Ultrasound Obstet Gynecol. 2001;17:191–196. Poehling KM, Talbot TR, Griffin MR, et al. Invasive pneumococcal disease among infants before and after introduction of pneumococcal conjugate vaccine. JAMA. 2006;295:1668 –1674. Grupo de trabajo de codificación diagnóstica de la Sociedad de Urgencias de Pediatría de la AEP. Codificación diagnóstica en Urgencias de Pediatría. Available at: http://www.seup.org/seup/html/gtrabajo/cod_diagnostica.htm. Accessed December 8, 2002. Hooker EA, Smith SW, Miles T, et al. Subjective assessment of fever by parents: comparison with measurement by noncontact tympanic thermometer and calibrated rectal glass mercury thermometer. Ann Emerg Med. 1996;28:313–317. Graneto JW, Soglin DF. Maternal screening of childhood fever by palpation. Pediatr Emerg Care. 1996;12:183–184. Shaikh N, Morone NE, Boost JE, et al. Prevalence of urinary tract infection in childhood: a meta-analysis. Pediatr Infect Dies J. 2008;27:302–308. Bonacorsi S, Houdouin V, Mariani-Kurkdjian P, et al. Comparative prevalence of virulence factors in Escherichia coli causing urinary tract infection in male infants with and without bacteremia. J Clin Microbiol. 2006;44:1156 –1158. Bachur RG, Caputo GL. Bacteremia and meningitis among infants with urinary tract infections. Pediatr Emerg Care. 1995;11:280 –284. Hsiao AL, Baker MD. Fever in the new millennium: a review of recent studies of markers of serious bacterial infection in febrile children. Curr Opin Pediatr. 2005;17:56 – 61. Lacour AG, Gervaix A, Zamora SA, et al. Procalcitonin, IL-6, IL-8, IL-1 receptor antagonist and C-reactive protein as identifiers of serious bacterial infections in children with fever without localising signs. Eur J Pediatr. 2001;160:95–100. Fernández A, Luaces C, García JJ, et al. Procalcitonin in pediatric emergency departments for the early diagnosis of invasive bacterial infections in febrile infants: results of a multicenter study and utility of a rapid qualitative test for this marker. Pediatr Infect Dis J. 2003;22:895–903. Andreola B, Bressan S, Callegaro S, et al. Procalcitonin and C-reactive protein as diagnostic markers of severe bacterial infections in febrile infants and children in the emergency department. Pediatr Infect Dis J. 2007;26:672–677. Arkader R, Troster EJ, Lopes MR, et al. Procalcitonin does discriminate between sepsis and systemic inflammatory response syndrome. Arch Dis Child. 2006;91:117–120. Maniaci V, Dauber A, Weiss S, et al. Procalcitonin in young febrile infants for the detection of serious bacterial infections. Pediatrics. 2008;122:701–710. www.pidj.com | 5











© Copyright 2026