
2015 Drug Formulary - HealthPlus of Michigan
2015 Drug Formulary For Commercial, Medicaid, Point-of-Service, PPO, Signature PPO Closed Formulary, TPA, MIChild and Medicare (non-Part D) Effective 1/1/2015 The Drug Formulary for Commercial, Medicaid, Point-of-Service, PPO, Signature PPO Closed Formulary, TPA, MIChild and Medicare (non-Part D) 2015 DRUG FORMULARY TABLE OF CONTENTS PREFACE TO THE NINETEENTH EDITION ............................................................................................ ii TABLE OF FORMULARY SECTIONS ..................................................................................................... iii HOW TO USE THIS FORMULARY........................................................................................................ viii DEFINITIONS ...........................................................................................................................................x MEMBER PRESCRIPTION BENEFIT ...................................................................................................... xi GENERIC SUBSTITUTION GUIDELINES ............................................................................................... xi PREFERRED MEDICATION PROGRAM ............................................................................................... xii PRIOR AUTHORIZATION PROGRAM ................................................................................................... xii PHARMACY AUDIT PROGRAM............................................................................................................ xiii DRUG RECALL SURVEILLANCE PROGRAM ...................................................................................... xiii DOSE OPTIMIZATION PROGRAM ....................................................................................................... xiv DRUG UTILIZATION REVIEW (DUR) .................................................................................................... xiv CONTROLLED SUBSTANCES PHARMACY PROGRAM (CSPP) ........................................................ xiv ASK FOR 90 RX PROGRAM ................................................................................................................. xiv SPECIALTY PHARMACY PROGRAM .................................................................................................... xv HEALTHPLUS DENTAL FORMULARY .................................................................................................. xv PHARMACY & THERAPEUTICS COMMITTEE ................................................................................... xviii FORMULARY UPDATES AND REVISIONS ........................................................................................ xviii SMOKING CESSATION PHARMACOTHERAPY .................................................................................. xix FORMULARY KEY ................................................................................................................................. xx FORMULARY DRUG PRODUCT .......................................................................................................... 21 HEALTHPLUS REQUEST FOR ADDITION TO THE FORMULARY .................................................... 114 HEALTHPLUS PARTNERS (MEDICAID) OVER-THE-COUNTER (OTC) MEDICATIONS .................. 115 PHARMACY PRIOR AUTHORIZATION FORM ................................................................................... 116 MEDICAID PRIOR AUTHORIZATION CRITERIA ................................................................................ 145 SPECIALTY/INJECTABLE PRIOR AUTHORIZATION CRITERIA ....................................................... 170 A RESOURCE FOR PROMOTING QUALITY IN HEALTHCARE Visit the HealthPlus website at www.healthplus.org PREFACE TO THE NINETEENTH EDITION Since the publication of the 2014 edition of the HealthPlus Drug Formulary, many new drugs and treatment options have become available. Every section of the Formulary has been reviewed and updated. Recommendations in the Formulary are intended to promote the most cost-effective therapy while maintaining a high quality drug benefit. The Drug Formulary is not meant to take the place of the product package insert, and users are encouraged to refer to the full prescribing information provided with the product. Input and suggestions for inclusion in the 2016 edition are encouraged. Please direct your comments and suggestions to: HealthPlus of Michigan Pharmacy Department 2050 S Linden Road P.O. Box 1700 Flint, MI 48501-1700 Or e-mail: [email protected] Formulary information is also available at www.healthplus.org. Formulary information may also be available through various e-prescribing applications (along with eligibility verification and prescription history). ii TABLE OF FORMULARY SECTIONS GASTROINTESTINAL DRUGS ..................................................................................................... 21 ANTI-ULCER AGENTS .............................................................................................................. 21 INFLAMMATORY BOWEL DISEASE ......................................................................................... 22 DIGESTIVE ENZYMES .............................................................................................................. 22 HEMORRHOIDS AND OTHER GASTROINTESTINALS ............................................................ 23 ANTIEMETICS ........................................................................................................................... 23 PROMOTILITY AGENTS ........................................................................................................... 24 ANTIDIARRHEALS .................................................................................................................... 24 ANTISPASMODICS ................................................................................................................... 24 LAXATIVES/CATHARTICS ........................................................................................................... 25 CARDIOVASCULAR AGENTS ..................................................................................................... 26 NITRATES ................................................................................................................................. 26 ANTIARRHYTHMICS ................................................................................................................. 26 CARDIAC GLYCOSIDES ........................................................................................................... 27 DIURETICS ................................................................................................................................ 27 ANGIOTENSIN CONVERTING ENZYME INHIBITORS (ACEIs) ................................................ 27 ANGIOTENSIN II RECEPTOR ANTAGONISTS (ARBs) ............................................................ 28 VASODILATORS ....................................................................................................................... 29 CALCIUM CHANNEL BLOCKERS ............................................................................................. 29 BETA-BLOCKERS ..................................................................................................................... 30 ALPHA BLOCKERS ................................................................................................................... 31 PULMONARY ANTIHYPERTENSIVES ...................................................................................... 31 MISCELLANEOUS ANTIHYPERTENSIVES .............................................................................. 31 ANTIHYPERLIPIDEMICS .............................................................................................................. 32 ANTIMICROBIALS AND INFECTIOUS DISEASE ........................................................................ 33 PENICILLINS ............................................................................................................................. 33 CEPHALOSPORINS .................................................................................................................. 33 TETRACYCLINES ...................................................................................................................... 34 MACROLIDES............................................................................................................................ 34 SULFONAMIDES ....................................................................................................................... 35 QUINOLONES ........................................................................................................................... 35 MISCELLANEOUS ANTIBIOTICS .............................................................................................. 35 URINARY ANTI-INFECTIVES (UTI) ........................................................................................... 36 ORAL ANTIFUNGALS................................................................................................................ 36 ANTITUBERCULOSIS AGENTS ................................................................................................ 37 iii ANTIVIRALS .............................................................................................................................. 37 ANTIMALARIALS/ANTIPROTOZOALS ...................................................................................... 38 ANTIHELMINTICS ..................................................................................................................... 38 AMEBICIDES ............................................................................................................................. 38 ANALGESICS ............................................................................................................................... 38 NONSTEROIDAL ANTI-INFLAMMATORY DRUGS (NSAIDS) ................................................... 39 NARCOTIC ANALGESICS ......................................................................................................... 40 RESPIRATORY DRUGS ............................................................................................................... 42 ALLERGIES ............................................................................................................................... 42 NASAL SPRAYS ........................................................................................................................ 43 ANTIHISTAMINE/ANTITUSSIVES ............................................................................................. 43 DECONGESTANT/ANTIHISTAMINES ....................................................................................... 43 DECONGESTANT/ANTITUSSIVE OR EXPECTORANT ............................................................ 44 DECONGESTANT/ANTIHISTAMINE AND ANTITUSSIVES ...................................................... 44 ORALLY INHALED DRUGS ....................................................................................................... 44 OTHER BRONCHODILATORS, ORAL ...................................................................................... 46 THEOPHYLLINES...................................................................................................................... 46 LEUKOTRIENE RECEPTOR ANTAGONISTS ........................................................................... 46 MUCOLYTICS ............................................................................................................................ 47 DERMATOLOGICS ....................................................................................................................... 47 TOPICAL STEROIDS ................................................................................................................. 47 TOPICAL SULFONAMIDES ....................................................................................................... 49 TOPICAL EMOLLIENTS ............................................................................................................ 49 TOPICAL IMMUNOMODULATORS ........................................................................................... 50 PSORIASIS ................................................................................................................................ 50 ANTI-INFECTIVES (TOPICAL) .................................................................................................. 51 BURN PREPARATIONS ............................................................................................................ 51 ANTIFUNGALS (TOPICAL) ........................................................................................................ 51 ACNE ......................................................................................................................................... 53 VAGINAL ANTIBIOTIC/ANTIFUNGAL PRODUCTS ................................................................... 54 SCABICIDES & PEDICULOCIDES ............................................................................................ 55 TOPICAL ENZYMES .................................................................................................................. 55 OTHER AGENTS ....................................................................................................................... 55 BLOOD MODIFIERS ..................................................................................................................... 55 ANTICOAGULANTS................................................................................................................... 55 ANTI-PLATELET DRUGS .......................................................................................................... 56 iv HEMORRHEOLOGIC AGENTS ................................................................................................. 56 COLONY STIMULATING FACTORS ......................................................................................... 56 ERYTHROCYTE STIMULATORS .............................................................................................. 56 HEMOSTATICS ......................................................................................................................... 56 EENT DRUGS ............................................................................................................................... 57 GLAUCOMA AGENTS ............................................................................................................... 57 TOPICAL OPHTHALMIC STEROIDS......................................................................................... 58 TOPICAL OPHTHALMIC ANTIBIOTICS..................................................................................... 59 TOPICAL OPHTHALMIC ANTI-INFECTIVE/ANTI-INFLAMMATORY ......................................... 60 TOPICAL OPHTHALMIC VASOCONSTRICTORS/ANTIHISTAMINES ...................................... 60 TOPICAL OPHTHALMIC NSAIDS.............................................................................................. 61 OTIC AGENTS ........................................................................................................................... 61 BEHAVIORAL HEALTH ................................................................................................................ 62 DEPRESSION ............................................................................................................................ 62 ANXIETY .................................................................................................................................... 63 INSOMNIA ................................................................................................................................. 63 PSYCHOSIS/MANIC DEPRESSIVES ........................................................................................ 64 ATTENTION DEFICIT DISORDER/NARCOLEPSY ................................................................... 65 ANTICONVULSANTS ................................................................................................................... 66 MIGRAINE MEDICATIONS ........................................................................................................... 67 SKELETAL MUSCLE RELAXANTS ............................................................................................. 68 MISCELLANEOUS AUTONOMIC AGENTS ................................................................................. 69 PARKINSON'S DISEASE (PD) ..................................................................................................... 69 ALZHEIMER'S DISEASE .............................................................................................................. 70 HORMONES.................................................................................................................................. 70 ORAL ADRENAL CORTICOSTEROIDS .................................................................................... 70 ORAL CONTRACEPTIVES, GF ................................................................................................. 70 NON-ORAL CONTRACEPTIVES, GF ........................................................................................ 76 ESTROGENS, GF ...................................................................................................................... 76 PROGESTINS ............................................................................................................................ 77 COMBINATION ESTROGEN/ANDROGEN ................................................................................ 77 COMBINATION ESTROGEN/PROGESTINS ............................................................................. 77 DDAVP-DESMOPRESSIN ACETATE ........................................................................................ 78 ANDROGENS, GM .................................................................................................................... 78 INFERTILITY .............................................................................................................................. 78 ENDOMETRIOSIS ......................................................................................................................... 79 v OSTEOPOROSIS .......................................................................................................................... 79 SELECTIVE ESTROGEN RECEPTOR MODULATOR............................................................... 79 BISPHOSPHONATES ................................................................................................................ 79 THYROID DISORDERS................................................................................................................. 80 DIABETES..................................................................................................................................... 80 INSULINS................................................................................................................................... 80 NEEDLES/SYRINGES ............................................................................................................... 81 SULFONYLUREAS .................................................................................................................... 81 ORAL ANTIHYPERGLYCEMICS ............................................................................................... 81 DPP-4 INHIBITORS ................................................................................................................... 82 THIAZOLIDINEDIONES ............................................................................................................. 82 MISCELLANEOUS ..................................................................................................................... 83 GLUCAGON............................................................................................................................... 83 ANTI-GOUT DRUGS ..................................................................................................................... 83 SUPPLEMENTS ............................................................................................................................ 84 ANTI-ANEMIA DRUGS .............................................................................................................. 84 PRENATAL VITAMINS............................................................................................................... 84 POTASSIUM .............................................................................................................................. 85 VITAMIN D ................................................................................................................................. 86 VITAMINS WITH FLUORIDE ..................................................................................................... 86 TOPICAL FLUORIDE ................................................................................................................. 86 VITAMIN K ................................................................................................................................. 86 MISCELLANEOUS AGENTS ........................................................................................................ 86 ALLERGENIC EXTRACTS ......................................................................................................... 86 ANAPHYLAXIS .......................................................................................................................... 87 HEAVY METAL ANTAGONISTS ................................................................................................ 87 QUININE SULFATE ................................................................................................................... 87 ALKALINIZING AGENTS ........................................................................................................... 87 AMINO ACID DERIVATIVES...................................................................................................... 87 GALLSTONE SOLUBILIZERS ................................................................................................... 87 SUBSTANCE ABUSE DETERRENTS ....................................................................................... 87 ERECTILE DYSFUNCTION (ED) ............................................................................................... 88 IMMUNE SUPPRESSANTS ....................................................................................................... 88 RHEUMATOLOGIC MEDCATIONS ........................................................................................... 89 LOCAL ANESTHETICS.............................................................................................................. 89 POTASSIUM REMOVING RESINS ............................................................................................ 90 vi UROLOGY ................................................................................................................................. 90 WOMEN’S HEALTH ................................................................................................................... 91 OXYTOCICS .............................................................................................................................. 91 HEPATITIS C PRODUCTS ........................................................................................................ 91 IRRITABLE BOWEL SYNDROME/CHRONIC CONSTIPATION ................................................. 91 FIBROMYALGIA ........................................................................................................................ 92 CYSTIC FIBROSIS .................................................................................................................... 92 MULTIPLE SCLEROSIS ............................................................................................................ 92 NEUROLOGICAL MISCELLANEOUS ........................................................................................ 92 ELECTROLYTES & MISCELLANEOUS NUTRIENTS................................................................ 92 ONCOLOGY-ONCOLOGY DRUGS ARE ON FORMULARY UNLESS LISTED OTHERWISE ... 93 GROWTH HORMONES ............................................................................................................. 93 HIV – ALL HIV SELF-ADMINISTERED DRUGS ARE ON FORMULARY ................................... 93 MEDICAL PRIOR AUTHORIZATION DRUGS WITH A MEDICAL BENEFIT COPAY ................ 94 PREVENTATIVE MEDICATION FOR HEALTH CARE REFORM COVERED AT A ZERO COPAY WITH PRESCRIPTION .......................................................................................................................... 95 vii HOW TO USE THIS FORMULARY ORGANIZATION The HealthPlus Drug Formulary contains information about medication coverage, generic and preferred brand prescriptions, and information about HealthPlus Pharmacy policies and procedures that reflect best practices in the pharmacy industry and current treatment standards. The Formulary is organized into SECTIONS according to classes of drugs and/or disease state. When searching for a particular drug, you may use the Find or Search function if you are viewing the PDF document electronically. If you are viewing a paper copy, it is best to refer to the index (see last section) under the brand or generic name. Similarly, when looking for the drugs used to treat a particular disease state, you may use the Find or Search function or refer to the TABLE OF FORMULARY SECTIONS starting on page iii. CONTENT Formulary recommendations are developed through the Pharmacy & Therapeutics Committee and are based on a review of current drug information and medical literature. HealthPlus recognizes that it is the sole responsibility of the physician to determine the best course of care for a particular patient. The HealthPlus Drug Formulary is VOLUNTARY or OPEN, with some restrictions for drugs included in special programs such as the Prior Authorization program (including Step Therapy). Procedures for requesting consideration of non-Formulary drugs for addition to the Formulary are discussed under the heading “Formulary Revisions” on page xviii. This document also includes copay tier and status of drugs for a closed formulary (currently administered only for historical Signature PPO products). DRUG LISTING For each Formulary Section, there is an alphabetic listing of medications that includes both the commonly used brand name and the generic name. The list includes products that are Formulary and Non-Formulary. There is also a column that indicates generic availability (Y=yes, a generic is available). The copay level/tier is included for each medication, along with any type of restrictions such as prior authorization, quantity limits, etc. For Commercial/Medicaid/POS/TPA/ Medicare (non-Part D) products, the following copay tiers apply: Generic Drugs=Tier 1, lowest copay Formulary/Preferred Brand Drugs=Tier 2, medium copay Non-Formulary/Non-Preferred Brand Drugs=Tier 3, highest copay NOTE: For members with a two tier copay (generic/brand), the standard brand copay applies for all drugs in copay tiers 2 and 3. For some benefits, a fourth tier copay may apply for specific medications or for specialty medications. In some cases, an employer group(s) may choose to place specific drugs in a different copay tier from the standard formulary. Members have access to up-to-date information about prescription drugs, the formulary and information specific to their benefit at the website at www.healthplus.org. Formulary updates are routinely posted at the website to keep members and providers informed about general changes. viii HealthPlus encourages the consideration of OTC products. In general, OTC products are not covered for the Commercial/PPO/ Medicare (non-Part D) lines of business, with the exception of insulin, insulin syringes, AEROCHAMBER, and sterile saline for nebulization. There are some additional exceptions, including generic Claritin and Claritin-D OTC products, Zaditor OTC and generic Nicotine Patches. These products are a covered benefit, with a written prescription, unless specifically excluded from the member’s benefit. If an OTC product is a covered product, it will be included in the category/drug listing. Specifically for the HealthPlus Partners program, a small list of OTC products is included for coverage as mandated by the State of Michigan. Please refer to the HealthPlus Partners (Medicaid) OTC summary list (Appendix B) on page 115. There are also a number of preventative OTC products covered for members based on health care reform regulations. Please see page 95. ix DEFINITIONS 1. FORMULARY: A list of medications and medical devices recommended for use under the HealthPlus prescription drug benefit. 2. OPEN FORMULARY: A Drug Formulary that is voluntary. The HealthPlus Drug Formulary is currently an “open” or “voluntary” Formulary, with some restrictions for drugs included in special programs, such as the Prior Authorization program. Prescriptions for drugs not listed in the HealthPlus Drug Formulary are still a covered benefit to the patient as stipulated in the individual group subscriber contract, with exceptions as noted. 3. CLOSED FORMULARY: A Drug Formulary that is mandatory. In a “mandatory” Formulary, prescriptions for products not listed in the Formulary are not a covered benefit for the patient. Patients are still at liberty to use out-of-pocket expenses for nonformulary drug products. 4. PHARMACY & THERAPEUTICS COMMITTEE: An interdisciplinary committee comprised of HealthPlus staff and community physicians and pharmacists who are primarily responsible for the maintenance of the HealthPlus Drug Formulary, including the evaluation and selection of drug products. The Pharmacy & Therapeutics Committee meets at least five times annually. 5. FORMULARY (Preferred) DRUGS: Drugs that are recommended for use. These are usually included in copay tier 1 or 2 in the HealthPlus Drug Formulary or updates to the Formulary. For benefits with a 4-tier copay, the 4th tier may contain formulary and nonformulary drugs. 6. NON-FORMULARY (Non-Preferred) DRUGS: Drug products not recommended by the Pharmacy & Therapeutics Committee, usually included in copay tier 3. Non-formulary drugs are still a covered benefit in an Open Formulary, with the exception of specific limitations. See Prescription Benefit Limitations (Appendix E, page 217). For benefits with a 4-tier copay, the 4th tier may contain formulary and non-formulary drugs. 7. MAXIMUM ALLOWABLE COST (MAC): The maximum allowable cost that HealthPlus reimburses to a pharmacy for generic medications. 8. EXCLUDED DRUGS: Drugs that are excluded from the drug benefit based on the subscriber certificate or regulatory requirements. Excluded drugs that are not reimbursable to the pharmacy include (but are not limited to): products for cosmetic use, experimental drugs and medical foods. Also, prescriptions written by a dentist that are not included on the DENTAL FORMULARY (see page xv) are excluded. Exclusions may also vary depending on the member’s benefit. See Prescription Benefit Limitations (Appendix E, page 217) for specific limitations. 9. PRIOR AUTHORIZATION DRUGS: Drugs for which specific established criteria must be met for coverage. Criteria is usually based on appropriate selection of recommended first-line alternatives prior to selection of the prior authorization drug. A sample prior authorization request form is included as Appendix C, page 116. 10. STEP THERAPY: Drugs for which a “first step” medication is required before coverage of the second step drug. Step therapy is a process that may be used for administering established Prior Authorization criteria. 11. COPAYMENT: A fee charged to the member for each prescription filled. Copayments vary depending on the member’s benefit level. x MEMBER PRESCRIPTION BENEFIT For HMO Commercial/Medicaid/ Medicare (non-Part D), prescriptions must be written by a participating physician, or a non-participating physician with the required referral (this does not apply to PPO members). If the medication is a covered benefit, members may fill their prescription at a participating HealthPlus pharmacy by presenting their identification card. A list of participating pharmacies may be found in the Provider Directory, on-line at www.healthplus.org or by contacting the Customer Service Department. Based on the member’s benefit level, a copayment may be required. Copayments vary. If you or the member has questions about copayments or deductibles (if applicable), please contact the HealthPlus Customer Service Department at 1-800-332-9161. For specific information about PPO members, please contact HealthPlus PPO Customer Service at 1-888-212-1512. GENERIC SUBSTITUTION GUIDELINES Specified drugs which have generic equivalents MUST BE DISPENSED GENERICALLY. These drugs are identified by a “Y” for YES in the GEQ column in the Formulary. Maximum Allowable Cost (MAC) limits have been established for the majority of these agents. Drug products considered to be generically and therapeutically equivalent are pharmaceutical equivalents that can be expected to have the same therapeutic effects when administered to patients under the conditions specified in the labeling. The FDA assigns a rating for all generic products. Products with a rating that begins with an “A” are considered equivalent to the brand name product. Some products approved before 1962 do not have a designated rating. Therefore, even though generic equivalents are available, no “A” rating has been assigned. These products will be reviewed on a case-by-case basis for addition to the MAC list. Brand drugs with a generic equivalent are non-formulary and are covered in the non-formulary copay tier. In cases of medical necessity, generic substitution may be overridden by the use of the “Dispense as Written” notation, with Prior Authorization required in these instances (please refer to Appendix D, page 117, Prior Authorization Criteria). For Commercial/PPO/Medicare (non-Part D) and RDS lines of business, if DAW is not medically necessary on a generically available brand name prescription or the member chooses the brand product in the absence of a DAW, he or she may do so by paying the difference in cost and/or any applicable copayment. For HealthPlus Partners, if the member requests the brand name drug he or she may be responsible for the entire cost of the prescription. xi Generic substitution is not required for some products that may have an “A” rating, due to a narrow therapeutic index. These include: Coumadin® Depakene® Depakote® Dilantin® Lanoxin® Premarin® Synthroid® Tegretol® Theo-Dur® Narrow therapeutic index drugs are reviewed on a case by case basis for addition to the MAC list. If a HealthPlus pharmacy submits the claim for the brand name drug, the brand name drug is covered, and reimbursement is based on the price of the brand name drug and applicable discounts. If a HealthPlus pharmacy submits the claim for a generic product, and the drug is included on the MAC list, reimbursement is based on the MAC price. PREFERRED MEDICATION PROGRAM HealthPlus administers a Preferred Medication Program to promote the use of specific cobranded products or specific multi-source brand products. HealthPlus uses system messaging in the pharmacy claims system to provide information to the dispensing pharmacist. PRIOR AUTHORIZATION PROGRAM HealthPlus requires prior authorization for selected drug products based on clinical, safety, or cost reasons. A copy of the Pharmacy Prior Authorization Form and the Prior Authorization Criteria for medications that require prior authorization at the time of publication are included as Appendix C and D (pages 116 and 117). Please note that the criteria documents include criteria for Commercial/PPO/Medicare (non-Part D) lines of business, MIChild, HealthPlus Partners (Medicaid) criteria, and criteria for specialty/injectable medications. For PPO, requirements for Prior Authorization may or may not apply based on the benefit purchased by the employer. HealthPlus may use Step Therapy for some medications that require Prior Authorization. This means that there are established “first step” drugs that must be used before the “second step” drug is covered. If the member has tried and failed therapy with the first step drug, the second step drug will be approved for that member. For the Signature PPO Closed Formulary, an Exceptions Process is available for review of medical necessity for coverage of non-formulary medications.The Exceptions Process also applies to drugs that are excluded as specified by the employer. To prescribe a medication that requires prior authorization or to submit a request for the Exceptions Process: The physician or office staff may complete the Pharmacy Prior Authorization form. xii Fax the form to the HealthPlus Pharmacy Department: FAX (810) 720-2757 (FLINT) If the patient presents a prescription to the pharmacy and prior authorization or an exception has not been obtained, the pharmacy should contact the prescribing physician and suggest preferred alternatives or instruct the physician to complete the Pharmacy Prior Authorization Form. For medications included in the specialty/injectable program, the physician may initiate the request for medication through the specialty vendor. The specialty vendor will then contact HealthPlus. 7-Day Starter Dose: To ensure that members are never in a situation where they are unable to obtain their medication, a 7-day starter dose may be dispensed by the pharmacy when an on-line edit is received for a medication or quantity that requires prior authorization. This override is a onetime override and is subject to audit. If the prescribing physician is unavailable for consult, the pharmacy may dispense up to a 7-day starter dose to initiate care for the member. Place a “06” in the denial clarification field (field 420) and enter up to a “7” for the days supply. Emergency Override: Pharmacies may also override non-participating physician edits that may apply when a prescription is written for an emergency situation. Entering “03” in the level of service field (field 418) will allow an override for emergency prescriptions only. This override is intended to be a one-time override and is subject to audit. If you would like an updated list of medications that require prior authorization, or if you have questions about this program, please call the Prior Authorization line at: Flint local phone (810) 720-2758 Toll-free phone (877) 710-0993 Note: These overrides do not apply to the Signature PPO Closed Formulary Benefit. PHARMACY AUDIT PROGRAM HealthPlus (or its designee) performs pharmacy audits to help ensure consistent and accurate electronic submission of prescription claims by the pharmacy network. Prescription claim audit activities may include a review of utilization by pharmacies, physicians, and members. The pharmacy audit program includes desk (paper) audits, on-site audits, and an appeals process. DRUG RECALL SURVEILLANCE PROGRAM When a particular drug product is recalled or withdrawn from the market due to safety reasons, HealthPlus reviews prescription utilization to identify members receiving that drug. HealthPlus notifies members and physicians affected by the recall, as appropriate. xiii DOSE OPTIMIZATION PROGRAM HealthPlus administers a Dose Optimization Program to target medications that are recommended for once daily dosing and/or support maximum dose recommendations through quantity limits. By optimizing the dose and decreasing the frequency, patient compliance increases and prescription costs decrease. System edits apply for the targeted medications when prescribed more often than once daily or above the quantity limits. Physicians may submit the standard HealthPlus Pharmacy Prior Authorization form, with information that includes a current diagnosis and medical necessity for the dosage regimen. Some of the categories included in the Dose Optimization Program are: proton pump inhibitors, HMG CoA reductase inhibitors, COX-II inhibitors, angiotensin II receptor antagonists, selected narcotic analgesics, selected antipsychotics, selected urinary incontinence drugs and selected sleeping medications. For more information regarding the Dose Optimization Program, please contact the HealthPlus Pharmacy Department at 1-810-720-2758 or toll-free at 1-877-710-0993. DRUG UTILIZATION REVIEW (DUR) HealthPlus administers a comprehensive DUR program to help ensure the quality and safety of prescribing and dispensing medications to members. The program includes point-of-service quality and safety edits to the pharmacist when a prescription is being filled, and retrospective analysis of claims data (with integration of medical and pharmacy data) to identify opportunities for educational intervention and improve quality and outcomes. For more information regarding the DUR program, please contact the HealthPlus Pharmacy Department at 1-810-720-2758 or toll-free at 1-877-710-0993. CONTROLLED SUBSTANCES PHARMACY PROGRAM (CSPP) HealthPlus offers services through a Controlled Substances Pharmacy Program to support the appropriate management of pain, ensure patient safety of narcotic use, and monitor for and prevent potential fraud and abuse of narcotics. For more information about the CSPP program, please contact the HealthPlus Pharmacy Department at 1-810-720-2758 or toll-free at 1-877710-0993. ASK FOR 90 RX PROGRAM Based on their benefit, the member may be eligible for the HealthPlus Ask for 90 Rx medication program for an extended supply of medication. With the Ask for 90 Rx program, there are two options for obtaining a 90-day supply of medications: 1. LOCAL PHARMACIES-Members may receive up to a 90-day supply of medication from participating local retail pharmacies.Copay savings may apply. For more information, go to www.healthplus.org for a list of retail pharmacies that participate in the Ask for 90 Rx program and an Ask for 90 Rx Patient Brochure. Or, you may contact the HealthPlus Customer Service Department. 2. MAIL SERVICE PROGRAM-Members may receive up to a 90-day of medication by mail order through Express Scripts and have prescriptions delivered to their home with no xiv shipping costs.Copay savings may apply. For more information about mail service, go to www.healthplus.org, or contact the HealthPlus Customer Service Department. For most benefits, copay savings from both of these programs are the same. Based on their benefit, the member pays the same copay for a 90-day supply at an Ask for 90 Rx retail pharmacy as they do at mail order. Most chronic medications are covered through the 90-day programs. Compounded medications and specialty/injectable medications, with the exception of injectable diabetes medications, glucagon, EpiPen and Imitrex, are NOT covered through the 90-day programs. To receive a 90-day supply in the Ask for 90 Rx Program, HealthPlus requires that the member has already received a 30-day supply of the same drug and same strength within the last year (to help assure the member is stabilized on the drug and dose before receiving a 90-day supply). The prescription claims processing system looks for previous pharmacy claims billed to HealthPlus for the member. NOTE: Based on their benefit, the member may be enrolled in the Mandatory 90-Day Medication Program. For most chronic medications, members are required to receive a 90-day supply each time they fill their prescription at a participating local retail pharmacy or through mail order with Express Scripts. SPECIALTY PHARMACY PROGRAM HealthPlus administers a specialty pharmacy program for injectable and oral specialty medications; including medications administered in the physician’s office and self-administered medications. For more information about the specialty pharmacy program, please contact the HealthPlus Customer Service Department at 1-800-332-9161. For PPO, please contact HealthPlus PPO Customer Service at 1-888-212-1512. NOTE: Based on their benefit, the member may be enrolled in the Mandatory Specialty Program. For specific self-injected or oral specialty medications, the member is required to receive the medication from a HealthPlus-contracted specialty pharmacy (the specialty pharmacy will mail the medication to the physician’s office or the member’s home). This program applies to self-injected medications for Rheumatoid Arthritis, Hepatitis C, Multiple Sclerosis, Infertility, Endometriosis (for HealthPlus Partners), and specialty medications from other targeted categories. HEALTHPLUS DENTAL FORMULARY The HealthPlus Dental Formulary is a restricted list of pharmaceutical agents covered when prescribed by dentists. This list was established by the Medical Affairs Committee and Board of Directors with recommendations by the Pharmacy & Therapeutics Committee. In the opinion of the Medical Affairs Committee, these medications are of established value in the treatment or prophylaxis of dental conditions, and present a broad range of choices to meet the usual clinical problems. These products are covered when written by a dental provider treating a patient with a HealthPlus drug benefit. Products that are not listed on the Dental Formulary are not a covered benefit when prescribed by a dentist. Medications listed in the Dental Formulary are available as either oral solids or oral liquids, whichever fits the clinical situation as determined by the prescriber. Products listed with “Y” for YES in the GEQ column in the Formulary, must be filled with a generic equivalent; for these generic medications, a tier 1 copay applies. In cases xv of medical necessity, generic substitution may be overridden by the use of the “Dispense as Written” (DAW) notation, with prior authorization required for these instances. A copy of the HEALTHPLUS DENTAL FORMULARY is printed on the next page. xvi HEALTHPLUS DENTAL FORMULARY Antifungals nystatin MYCOSTATIN* Antivirals acyclovir valacyclovir ZOVIRAX* VALTREX* Antibiotics Cephalosporins cephalexin HCL cefadroxil cefuroxime KEFLEX* (NOT 750MG) DURICEF* CEFTIN* Erythromycins erythromycin ERYTHROMYCIN* Penicillins amoxicillin amoxicillin-clavulanate potassium penicillin V potassium AMOXIL* AUGMENTIN* PENVEEK* Tetracyclines doxycycline hyclate tetracycline HCL VIBRAMYCIN*, VIBRATABS* (NOT DORYX, ORACEA) Miscellaneous Antibiotics clindamycin HCL CLEOCIN 150mg* Miscellaneous Anti-Infectives metronidazole FLAGYL* Skeletal Muscle Relaxants diazepam ibuprofen indomethacin naproxen VALIUM* Nonsteroidal Anti-Inflammatory Agents RX MOTRIN* INDOCIN CAPSULES* NAPROSYN* Narcotic Analgesics acetaminophen/codeine acetaminophen 325/oxycodone 5 aspirin/caffeine/dihydrocodeine aspirin/codeine aspirin 325/oxycodone 5 butalbital/aspirin/caffeine/codeine acetaminophen 325/hydrocodone 10 acetaminophen 325/hydrocodone 7.5 acetaminophen 325/hydrocodone 5 ibuprofen 200/hydrocodone 7.5 TYLENOL W/CODEINE* PERCOCET* SYNALGOS-DC* EMPIRIN W/CODEINE* PERCODAN* FIORINAL W/CODEINE* NORCO* NORCO* NORCO* VICOPROFEN* Systemic Corticosteroids methylprednisolone MEDROL DOSE PAK* Miscellaneous Rinses chlorhexidine gluconate PERIDEX* Miscellaneous lidocaine viscous solution/ointment LIDOCAINE* NOTE: Behavioral health medications (ex. diazepam) are carved out for HealthPlus Partners Medicaid. *generic available xvii PHARMACY & THERAPEUTICS COMMITTEE The Pharmacy & Therapeutics Committee is an interdisciplinary body made up of practicing physicians and pharmacists from the community, in addition to staff. The committee may invite persons within or outside the organization who can contribute specialized or unique knowledge, skills, and judgments. The function of the committee is to serve in an evaluative, educational, and advisory capacity to the physician providers in all matters pertaining to drug use. The committee also provides strategic guidance for pharmacy programs. The committee is involved in the development and updating of pharmaceutical management procedures. In addition, the committee meets at least five times annually to evaluate drugs for inclusion in the formulary. The recommendations of the Pharmacy & Therapeutics Committee are communicated to the Medical Affairs Committee and finally sent to the Board of Directors for approval. FORMULARY UPDATES AND REVISIONS The Formulary is revised regularly through recommendations from the Pharmacy & Therapeutics Committee. HealthPlus reviews medications and medication categories on an ongoing basis to help ensure that the Drug Formulary provides an ample, up-to-date selection of quality, cost-effective medication choices. The Formulary is revised and republished annually with notification to providers, with periodic updates on the website at www.healthplus.org; providers and members may also receive a printed copy of the formulary upon request. HealthPlus routinely provides updated information to physicians, pharmacies and members with updates at the website, articles in the newsletters, etc. The Formulary is also available for providers through various e-prescribing software applications available to physicians. Specifically for negative changes to the formulary (addition of prior authorization requirements, step therapy, or a change in status from formulary to non-formulary when a generic equivalent is not available), HealthPlus notifies affected members and their prescribers of the change. Members may also obtain up-to-date formulary and cost information specific to their benefit and copays at www.healthplus.org. For more information, please contact the HealthPlus Pharmacy Department at 1-810-230-2118. Physician requests for additions to the Formulary must be made on a Request for Addition to the Formulary form, which includes the reason for the request and any clinical data supporting that request. Please refer to APPENDIX A (page 114) for a copy of the HEALTHPLUS REQUEST FOR ADDITION TO THE FORMULARY form. Member requests for additions to the formulary are forwarded to the Pharmacy Department for appropriate review and consideration. xviii SMOKING CESSATION PHARMACOTHERAPY For all HealthPlus members all OTC and prescription nicotine agents are covered to promote smoking cessation: patch, inhaler, nasal spray, gum or lozenges. In addition, the following nonnicotine prescription medications are covered: Chantix and Zyban (bupropion). These products are covered with no copay and prior authorization is not required. Duration limits may apply for specific products. xix FORMULARY KEY Abbreviation AG DL DME DO GEQ GF GM HMO M M-NC MAND 90 MAND SPEC MDCH NA NC NF-NC NF-PA PA PARTNERS POS PPO QL SP SPEC TPA Description Age Restriction Duration Limit Available through Durable Medical Equipment benefit only, with a copay as applicable. Dose Optimization Generically Available Female Gender Restriction Male Gender Restriction Health Maintenance Organization Medical injectable or infused drugs (not self-administered) Medical benefit only, not processed by Pharmacy Mandatory 90-Day Program (specific medications must be filled in a 90-day supply) Mandatory Specialty Drug Program (specific medications must be obtained through a contracted specialty pharmacy) Michigan Department of Community Health (carve-out for specific medications) Not Applicable Not Covered, Excluded Non-Formulary, Not Covered (for Signature PPO Closed formulary) Non-Formulary, Prior Authorization Required (for Signature PPO Closed formulary) Prior Authorization and/or Step Therapy Required HealthPlus Partners Medicaid Point of Service Plan Preferred Provider Organization Quantity Limit Specialty Pharmacy Product with Limited Distribution (through a specific specialty pharmacy) Specialty Drugs, self-injected or self-administered Third Party Administrator xx FORMULARY DRUG PRODUCT NOTES BRAND NAME ACIPHEX ACIPHEX SPRINKLE AXID CARAFATE CARAFATE SUSP CYTOTEC DEXILANT ESOMEPRAZOLE STRONTIUM HMO POS TPA M-SUPP RDS PARTNERS MICHILD PPO MEDICAID GASTROINTESTINAL DRUGS ANTI-ULCER AGENTS GEQ GENERIC NAME TIER Y RABEPRAZOLE 1 RABEPRAZOLE NIZATIDINE SUCRALFATE SUCRALFATE MISOPROSTOL DEXLANSOPRAZOLE 3 1 1 2 1 3 PA, DO PA, DO PA, DO PA, DO PA, DO PA, DO NF-NC 1 1 2 1 NF-NC ESOMEPRAZOLE STRONTIUM 3 PA, DO PA, DO PA, DO NF-NC LANSOPRAZOLE 3 PA, DO PA, DO PA, DO NF-NC OMEPRAZOLE ESOMEPRAZOLE OMEPRAZOLECLARITHROMYCINAMOXICILLIN FAMOTIDINE 3 3 PA, DO PA, DO PA, DO PA, DO PA, DO PA, DO NF-NC NF-NC 3 3 NF-NC NF-NC 1 NF-NC Y Y Y Y FIRSTLANSOPRAZOLE FIRSTOMEPRAZOLE NEXIUM Y FAMOTIDINE 1 PREVACID Y LANSOPRAZOLE 1 PREVACID SOLUTAB PRILOSEC 20MG PRILOSEC 40MG LANSOPRAZOLE OMEPRAZOLE OMEPRAZOLE 3 1 1 PA, DO Y Y 3 1 3 1 PA, DO PA, DO PA, DO Y Y Y OMEPRAZOLE MAGNESIUM PANTOPRAZOLE PANTOPRAZOLE CIMETIDINE PA, DO PA, DO PA, DO th th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS MAND 90 MAND SPEC PARTNERS MAND SPEC NF-NC OMECLAMOX-PAK PEPCID RPD PEPCID TABS, SUSP PRILOSEC DR SUSP PROTONIX TABS PROTONIX PAK TAGAMET SIGNATURE PPO CLOSED FORMULARY PA, DO PA, DO NF-NC 1 NF-NC NF-NC NF-NC NF-NC 1 21 FORMULARY DRUG PRODUCT NOTES BRAND NAME ZANTAC ZANTAC EFFERDOSE ZEGERID 40MG CAPS GEQ Y Y ZEGERID SUSP APRISO ASACOL ASACOL HD AZULFIDINE, ENTAB CANASA COLAZAL Y Y CORTIFOAM DELZICOL DIPENTUM ENTOCORT EC GIAZO LIALDA PENTASA ROWASA ENEMA SF ROWASA ENEMA *UCERIS CREON th Y Y GENERIC NAME TIER HMO POS TPA M-SUPP RDS MICHILD PPO PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY RANITIDINE 1 1 RANITIDINE 3 NF-NC OMEPRAZOLE/SODIUM BICARBONATE 1 NF-NC OMEPRAZOLE/SODIUM BICARBONATE 3 MESALAMINE MESALAMINE MESALAMINE 2 2 2 SULFASALAZINE MESALAMINE 1 2 BALSALAZIDE DISODIUM 1 1 HYDROCORTISONE ACETATE 3 NF-NC MESALAMINE OLSALAZINE BUDESONIDE BALSALAZIDE DISODIUM MESALAMINE MESALAMINE MESALAMINE 2 3 1 MESALAMINE BUDESONIDE 2 3 AMYLASE/ LIPASE/ PROTEASE 2 3 3 2 1 th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS PA, DO PA, DO PA, DO INFLAMMATORY BOWEL DISEASE DO DO 1 2 DO PA PA PA 2 NF-NC 1 PA PA PA PA PA PA NF-NC NF-NC 2 1 PA PA DIGESTIVE ENZYMES PA PARTNERS MAND SPEC NF-NC 2 2 2 DO MAND 90 MAND SPEC Y Y Y Y Y Y Y 2 NF-NC 2 Y 22 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ GENERIC NAME VIOKASE ZENPEP AMYLASE/ LIPASE/ PROTEASE PANCREAZE PERTZYE ULTRASE ULTRASE MT ULTRESA AMITIZA ANUSOL HC FULYZAQ GASTROCROM *LOTRONEX PROCTOFOAM Y Y Y PROCTOFOAM HC SIGNATURE PPO CLOSED FORMULARY MAND 90 3 NF-NC Y 3 NF-NC Y 3 NF-NC Y 3 NF-NC Y 3 NF-NC Y 3 NF-NC Y 3 HEMORRHOIDS AND OTHER GASTROINTESTINALS NF-NC Y TIER AMYLASE/ LIPASE/ PROTEASE AMYLASE/ LIPASE/ PROTEASE AMYLASE/ LIPASE/ PROTEASE AMYLASE/ LIPASE/ PROTEASE AMYLASE/ LIPASE/ PROTEASE AMYLASE/ LIPASE/ PROTEASE LUBIPROSTONE HYDROCORTISONE SUPP CROFELEMER CROMOLYN SODIUM ALOSETRON PRAMOXINE HYDROCORTISONE/ PRAMOXINE HMO POS TPA M-SUPP RDS MICHILD PPO PARTNERS MEDICAID PA 2 1 3 1 2 1 MAND SPEC PARTNERS MAND SPEC 2 1 NF-NC 1 NF-NC 1 2 2 ANTIEMETICS ANTIVERT 12.5, 25MG ANTIVERT 50MG Y 1 2 *ANZEMET MECLIZINE MECLIZINE DOLASETRON MESYLATE COMPAZINE SYRUP PROCHLORPERAZINE 2 2 PROCHLORPERAZINE 1 1 COMPAZINE TABS, SUPP th Y 3 th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 1 2 PA NF-NC 23 FORMULARY DRUG PRODUCT NOTES BRAND NAME DICLEGIS EMEND PHENERGAN SANCUSO TIGAN TRANSDERMSCOP ZOFRAN, ODT GEQ Y Y Y ZUPLENZ REGLAN Y GENERIC NAME DOXYLAMINE/ PYRIDOXINE APREPITANT PROMETHAZINE GRANISETRON TRIMETHOBENZAMIDE TIER 3 3 1 3 1 SCOPOLAMINE ONDANSETRON ONDANSETRON 2 1 3 METOCLOPRAMIDE 1 HMO POS TPA M-SUPP RDS MICHILD PPO PARTNERS MEDICAID PA, DO PA, DO PA, DO AG AG AG AG AG AG NF-NC NF-NC 1 AG NF-NC 1 AG PA 2 1 NF-NC PA PA PROMOTILITY AGENTS SIGNATURE PPO CLOSED FORMULARY MAND 90 MAND SPEC PARTNERS MAND SPEC 1 ANTIDIARRHEALS IMODIUM LOMOTIL MOTOFEN Y LOPERAMIDE 1 1 Y DIPHENOXYLATE/ ATROPINE DIFENOXIN/ ATROPINE 1 3 1 NF-NC ANTISPASMODICS ANASPAZ BENTYL Y Y HYOSCYAMINE DICYCLOMINE 1 1 CANTIL CYSTOSPAZ M MEPENZOLATE BROMIDE HYOSCYAMINE 3 3 DONNATAL TAB, ELIXIR BELLADONNA ALKALOIDS/ PHENOBARBITAL 3 NF-NC DONNATAL ER GLYCATE LEVSIN BELLADONNA ALKALOIDS/ PHENOBARBITAL GLYCOPYRROLATE HYOSCYAMINE 3 3 1 NF-NC NF-NC th Y th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 1 1 PA NF-NC NF-NC 1 24 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ GENERIC NAME TIER HMO POS TPA M-SUPP RDS MICHILD PPO PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY LIBRAX NULEV Y Y CLIDINIUM BROMIDE/ CHLORDIAZEPOXIDE HYOSCYAMINE 1 1 1 1 PAMINE Y METHSCOPOLAMINE BROMIDE 1 1 PAMINE FORTE Y METHSCOPOLAMINE BROMIDE 1 1 METHSCOPOLAMINE COMBO 3 NF-NC PROPANTHELINE HYOSCYAMINE 2 1 2 1 HYOSCYAMINE 3 PAMINE FQ PRO-BANTHINE 7.5MG SYMAX FASTABS Y SYMAX DUOTAB MAND 90 MAND SPEC PARTNERS MAND SPEC NF-NC LAXATIVES/CATHARTICS COLYTE Y PEG3350/NA SULF/BICARB/CL/KCL 1 1 GOLYTELY #LACTULOSE SOLN Y PEG3350/NA SULF/BICARB/CL/KCL 1 1 Y LACTULOSE 1 1 MOVIPREP PEG3350/SOD SUL/NACL/ASB/CL/KCL 3 PA NF-NC OSMOPREP NAPHOS MBMH/NAPHOS, DI-BA 3 PA NF-NC PREPOPIK NA PICOSUL/MAG-OX/ CITRIC ACID 3 NF-NC SUCLEAR PEG3350/NA SULF/ BICARB/KCL 3 NF-NC SUPREP SODIUM /POTASSIUM/MAG SULFATES 3 NF-NC th th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 25 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ HMO POS TPA M-SUPP RDS PARTNERS MICHILD PPO MEDICAID CARDIOVASCULAR AGENTS SIGNATURE PPO CLOSED FORMULARY MAND 90 3 NF-NC Y 2 2 Y ISOSORBIDE MONONITRATE 1 1 Y ISOSORBIDE DINITRATE NITROGLYCERIN 3 2 NF-NC 2 Y Y 1 1 Y 2 Y GENERIC NAME TIER MAND SPEC PARTNERS MAND SPEC NITRATES ISOSORBIDE DINITRATE/ HYDRALAZINE ISOSORBIDE DINITRATE BIDIL DILATRATE-SR IMDUR ISORDIL NITRO-BID OINT NITRO-DUR PATCHES 0.1, 0.2, 0.4, 0.6MG/HR NITRO-DUR PATCHES 0.3, 0.8MG/HR NITROLINGUAL SPRAY NITROSTAT PAPAVERINE Y Y NITROGLYCERIN TRANSDERMAL NITROGLYCERIN TRANSDERMAL Y Y RECTIV OINT PA 2 NITROGLYCERIN 1 1 Y NITROGLYCERIN SUBLINGUAL PAPAVERINE 3 1 NF-NC 1 Y Y NITROGLYCERIN 3 NF-NC Y 1 1 1 1 1 1 1 1 Y Y Y Y 2 1 2 1 Y 3 NF-NC Y ANTIARRHYTHMICS BETAPACE, AF CALAN CORDARONE LANOXIN Y Y Y Y MULTAQ NORPACE Y NORPACE CR th SOTALOL VERAPAMIL AMIODARONE DIGOXIN DRONEDARONE HYDROCHLORIDE DISOPYRAMIDE DISOPYRAMIDE th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 26 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ GENERIC NAME TIER PACERONE PRONESTYL RANEXA RYTHMOL, SR SECTRAL TAMBOCOR TIKOSYN Y AMIODARONE PROCAINAMIDE RANOLAZINE PROPAFENONE ACEBUTOLOL FLECAINIDE DOFETILIDE 1 3 2 1 1 1 3 Y Y Y HMO POS TPA M-SUPP RDS MICHILD PPO PARTNERS MEDICAID PA SIGNATURE PPO CLOSED FORMULARY 1 NF-NC 2 1 1 1 NF-NC MAND 90 Y MAND SPEC PARTNERS MAND SPEC Y Y Y CARDIAC GLYCOSIDES LANOXIN Y DIGOXIN 1 1 Y 1 Y DIURETICS ALDACTAZIDE 25/25 ALDACTAZIDE 50/50 ALDACTONE CHLORTHALIDONE DEMADEX DYAZIDE DYRENIUM INSPRA LASIX LOZOL MAXZIDE ZAROXOLYN ACCUPRIL ACCURETIC ACEON ALTACE CAPOTEN EPANED SOLUTION th Y Y Y Y Y SPIRONOLACTONE/ HCTZ SPIRONOLACTONE/ HCTZ SPIRONOLACTONE CHLORTHALIDONE TORSEMIDE TRIAMTERENE/ HCTZ TRIAMTERENE EPLERENONE FUROSEMIDE INDAPAMIDE TRIAMTERENE/ HCTZ METOLAZONE Y Y Y Y Y QUINAPRIL QUINAPRIL/ HCTZ PERINDOPRIL RAMIPRIL CAPTOPRIL Y Y Y Y Y 1 NF-NC 3 1 1 1 1 1 1 1 1 NF-NC 3 1 1 1 1 1 1 1 1 1 1 ANGIOTENSIN CONVERTING ENZYME INHIBITORS (ACEIs) ENALAPRIL th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS Y Y Y Y Y Y Y Y Y Y Y 1 1 1 1 1 1 1 1 1 1 Y Y Y Y Y 3 NF-NC Y 27 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ LOTENSIN LOTENSIN HCT Y Y LOTREL MAVIK MONOPRIL MONOPRIL HCT PRINIVIL PRINZIDE Y Y Y Y Y Y TARKA UNIRETIC UNIVASC VASERETIC VASOTEC ZESTORETIC ZESTRIL GENERIC NAME TIER HMO POS TPA M-SUPP RDS MICHILD PPO PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY 1 1 1 1 MAND 90 Y Y 1 1 1 1 1 1 1 1 1 1 1 1 Y Y Y Y Y Y Y Y Y Y Y BENAZEPRIL BENAZEPRIL/ HCTZ AMLODIPINE/ BENAZEPRIL TRANDOLAPRIL FOSINOPRIL FOSINOPRIL/ HCTZ LISINOPRIL LISINOPRIL/ HCTZ TRANDOLAPRIL/ VERAPAMIL MOEXIPRIL/ HCTZ MOEXIPRIL ENALAPRIL/ HCTZ ENALAPRIL LISINOPRIL/ HCTZ 2 1 1 1 1 1 2 1 1 1 1 1 Y Y Y Y Y Y Y LISINOPRIL 1 1 Y Y Y Y Y 2 1 1 DO 1 Y Y Y Y Y Y NF-NC Y MAND SPEC PARTNERS MAND SPEC ANGIOTENSIN II RECEPTOR ANTAGONISTS (ARBs) ATACAND ATACAND HCT AVALIDE AVAPRO AZOR BENICAR BENICAR HCT COZAAR DIOVAN DIOVAN HCT EDARBI th Y Y Y Y Y Y Y CANDESARTAN CANDESARTAN IRBESARTAN/ HCTZ IRBESARTAN AMLODIPINE/ OLMESARTAN OLMESARTAN OLMESARTAN/ HCTZ LOSARTAN VALSARTAN VALSARTAN/ HCTZ AZILSARTAN MEDOXOMIL th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 1 1 1 1 2 2 2 1 1 1 3 DO DO DO DO DO DO 1 DO 1 1 1 DO DO DO DO 2 2 DO DO DO DO PA, DO PA, DO PA, DO 28 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ Y GENERIC NAME AZILSARTAN MEDOXOMIL/ CHLORTHALIDONE AMLODIPINE/ VALSARTAN Y Y Y Y AMLODIPINE/ VALSARTAN/HCTZ LOSARTAN/ HCTZ TELMISARTAN TELMISARTAN/ HCTZ EPROSARTAN EDARBYCLOR EXFORGE EXFORGE HCT HYZAAR MICARDIS MICARDIS HCT TEVETEN TEVETEN HCT TRIBENZOR TWYNSTA Y VALTURNA EPROSARTAN/ HCTZ OLMESARTAN MED/ AMLODIPINE/HCTZ TELMISARTAN/ AMLODIPINE ALISKIREN/ VALSARTAN TIER HMO POS TPA M-SUPP RDS MICHILD 3 PA, DO PPO PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY MAND 90 PA, DO PA, DO NF-NC Y 1 1 Y 2 1 1 1 1 DO DO DO DO DO DO 2 1 1 DO 1 1 DO Y Y Y Y Y 3 PA PA PA NF-NC Y 2 2 Y 1 1 Y 2 Y 1 Y 2 MAND SPEC PARTNERS MAND SPEC VASODILATORS APRESOLINE Y HYDRALAZINE 1 CALCIUM CHANNEL BLOCKERS ADALAT CC AMTURNIDE CALAN, SR CARDENE CARDENE SR CARDIZEM CARDIZEM CD 120, 180, 240, 300, 360 CARDIZEM LA 120MG CARDIZEM LA 180, 240, 300, 360 420MG th Y 1 1 Y 2 1 1 3 1 2 1 1 NF-NC Y NIFEDIPINE ALISKIREN/ AMLODIPINE/HCTZ VERAPAMIL NICARDIPINE NICARDIPINE DILTIAZEM 1 Y Y Y Y Y Y DILTIAZEM 1 1 Y NF-NC Y 1 Y Y Y DILTIAZEM Y 3 DILTIAZEM 1 th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS PA PA 29 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ CARTIA XT COVERA HS DILACOR XR DYNACIRC CR ISOPTIN SR Y LOTREL NIMOTOP NORVASC PROCARDIA, XL SULAR 8.5, 17, 25.5, 34 Y Y Y Y TEKAMLO VERELAN, PM Y Y Y Y GENERIC NAME TIER HMO POS TPA M-SUPP RDS MICHILD PPO PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY 1 3 1 3 1 1 1 1 1 1 1 1 1 Y NISOLDIPINE ALISKIREN/ AMLODIPINE VERAPAMIL 1 1 Y 2 1 2 1 Y Y TIMOLOL NEBIVOLOL CARVEDILOL CARVEDILOL NADOLOL NADOLOL/ BENDROFLUMETHIAZIDE METOPROLOL/HCTZ PROPRANOLOL BETAXOLOL PENBUTOLOL METOPROLOL METOPROLOL/ HCTZ LABETALOL ACEBUTOLOL 1 2 1 3 1 1 2 DO 1 NF-NC 1 Y Y Y Y Y 1 NF-NC Y Y Y Y Y Y Y Y Y PA PA PA 1 NF-NC 1 NF-NC 1 MAND 90 Y Y Y Y Y DILTIAZEM VERAPAMIL DILTIAZEM ISRADIPINE VERAPAMIL AMLODIPINE/ BENAZEPRIL NIMODIPINE AMLODIPINE NIFEDIPINE MAND SPEC PARTNERS MAND SPEC Y BETA-BLOCKERS BLOCADREN BYSTOLIC COREG COREG CR CORGARD Y CORZIDE DUTOPROL INDERAL LA KERLONE LEVATOL LOPRESSOR LOPRESSOR HCT NORMODYNE SECTRAL Y th Y Y Y Y Y Y Y Y th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 1 3 1 1 3 1 1 1 1 DO DO DO PA PA PA PA 1 1 NF-NC 1 1 1 1 30 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ TENORETIC TENORMIN Y Y TOPROL XL TRANDATE ZEBETA ZIAC Y Y Y Y GENERIC NAME SIGNATURE PPO CLOSED FORMULARY MAND 90 1 1 1 1 Y Y 1 1 1 1 1 1 1 1 Y Y Y Y 1 NF-NC 1 Y Y Y 2 1 Y TIER ATENOLOL/ CHLORTHALIDONE ATENOLOL METOPROLOL SUCCINATE LABETALOL BISOPROLOL BISOPROLOL/ HCTZ HMO POS TPA M-SUPP RDS MICHILD PPO PARTNERS MEDICAID MAND SPEC PARTNERS MAND SPEC NF-NC Y Y ALPHA BLOCKERS CARDURA CARDURA XL FLOMAX JALYN MINIPRESS Y Y DOXAZOSIN DOXAZOSIN TAMSULOSIN 1 3 1 Y DUTASTERIDE/ TAMSULOSIN PRAZOSIN 2 1 PA PA PULMONARY ANTIHYPERTENSIVES PA PA PA *ADCIRCA TADALAFIL 3 *ADEMPAS RIOCIGUAT 3 NF-NC Y Y *OPSUMIT MACITENTAN 3 NF-NC Y Y TREPROSTINIL SILDENAFIL CITRATE BOSENTAN TREPROSTINIL/NEBULIZER KIT 3 1 2 NF-NC 1 PA 4 SP Y Y Y Y METHYLDOPA METHYLDOPA METHYLDOPA/ HCTZ CLONIDINE PHENOXYBENZAMINE EPLERENONE 1 2 3 1 3 1 *ORENITRAM ER *REVATIO *TRACLEER Y *TYVASO ALDOMET ALDOMET 125 ALDORIL-D CATAPRES, TTS DIBENZYLINE INSPRA th Y Y Y th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 3 PA SP PA SP PA SP SP SP SP MISCELLANEOUS ANTIHYPERTENSIVES NF-NC 1 2 NF-NC Y Y 1 NF-NC Y 1 Y 31 FORMULARY DRUG PRODUCT NOTES BRAND NAME NEXICLON XR TEKTURNA TEKTURNA HCT TENEX GEQ Y VALTURNA GENERIC NAME TIER CLONIDINE ALISKIREN ALISKIREN/ HCTZ GUANFACINE ALISKIREN/ VALSARTAN HMO POS TPA M-SUPP RDS MICHILD PPO PARTNERS MEDICAID 3 2 2 1 2 SIGNATURE PPO CLOSED FORMULARY NF-NC 2 2 1 MAND 90 MAND SPEC PARTNERS MAND SPEC Y Y Y Y Y Y Y 2 Y NF-NC NF-NC NF-NC Y Y Y Y ANTIHYPERLIPIDEMICS ADVICOR ALTOPREV ANTARA 30, 90 ANTARA 43, 130 CADUET COLESTID COLESTID 7.5 CRESTOR FENOGLIDE FIBRICOR Y Y Y Y *JUXTAPID *KYNAMRO LESCOL LESCOL XL LIPITOR LIPOFEN Y Y LIPTRUZET LIVALO LOFIBRA LOPID Y Y LOVAZA Y th NIACIN/LOVASTATIN LOVASTATIN FENOFIBRATE FENOFIBRATE AMLODIPINE/ ATORVASTATIN COLESTIPOL COLESTIPOL ROSUVASTATIN FENOFIBRATE FENOFIBRIC ACID LOMITAPIDE MESYLATE MIPOMERSEN FLUVASTATIN FLUVASTATIN ATORVASTATIN FENOFIBRATE EZETIMIBE/ ATORVASTATIN PITAVASTATIN CALCIUM FENOFIBRATE GEMFIBROZIL OMEGA-3-ACID ETHYL ESTERS th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 3 3 3 1 PA, DO PA, DO PA 1 1 3 2 3 1 DO PA, DO PA, DO PA PA, DO PA, DO PA 1 DO DO 1 DO 1 NF-NC 2 PA, DO NF-NC 1 Y Y Y Y Y Y PA, DO PA PA, DO PA PA, DO PA 3 PA, SP PA, SP PA, SP NF-NC 3 1 3 1 3 PA, SP DO PA, DO DO PA PA, SP DO PA, DO DO PA PA, SP DO PA, DO DO PA NF-NC 1 NF-NC 1 DO NF-NC Y Y Y Y 2 DO DO DO 2 DO Y 3 1 1 PA, DO PA, DO PA, DO NF-NC 1 1 Y Y Y 1 PA PA PA 1 PA Y 32 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ MEVACOR NIASPAN PRAVACHOL Y Y Y PREVALITE Y QUESTRAN BULK SIMCOR TRICOR TRIGLIDE Y TRILIPIX TIER PPO DO PARTNERS MEDICAID DO DO DO DO LOVASTATIN NIACIN PRAVASTATIN CHOLESTYRAMINE/ ASPARTAME CHOLESTYRAMINE POWDER NIACIN/ SIMVASTATIN FENOFIBRATE FENOFIBRATE 1 1 1 Y FENOFIBRIC ACID 1 3 PA PA 2 2 2 1 DO DO Y ICOSAPENT ETHYL EZETIMIBE/ SIMVASTATIN COLESEVELAM EZETIMIBE SIMVASTATIN Y VASCEPA VYTORIN WELCHOL ZETIA ZOCOR GENERIC NAME HMO POS TPA M-SUPP RDS MICHILD DO 1 1 2 1 3 DO DO DO PA PA PA PA DO PA PA PA PA DO DO DO ANTIMICROBIALS AND INFECTIOUS DISEASE SIGNATURE PPO CLOSED FORMULARY 1 DO 1 1 DO MAND 90 Y Y Y 1 Y 1 2 DO 1 NF-NC Y Y Y Y 1 Y NF-NC Y 2 DO 2 2 PA 1 DO Y Y Y Y MAND SPEC PARTNERS MAND SPEC PENICILLINS AMOXIL AUGMENTIN CHEW TABS, 125-31.25 SUSP Y AUGMENTIN XR AUGMENTIN, ES, 250-62.5 SUSP MOXATAG 775 MG ER Y Y Y AMOXICILLIN AMOXICILLIN/ CLAVULANATE AMOXICILLIN/ CLAVULANATE AMOXICILLIN/ CLAVULANATE AMOXICILLIN TRIHYDRATE 1 1 3 NF-NC 1 1 1 1 1 1 CEPHALOSPORINS CECLOR CEDAX CEFTIN TABS th Y Y CEFACLOR CEFTIBUTEN CEFUROXIME 1 3 1 th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 1 NF-NC 1 33 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ KEFLEX SPECTRACEF SUPRAX Y Y GENERIC NAME TIER HMO POS TPA M-SUPP RDS MICHILD PPO PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY CEPHALEXIN CEFDITOREN CEFIXIME 1 1 3 DOXYCYCLINE DOXYCYCLINE DOXYCYCLINE/SALICY/ OCT/ZINC OX 3 1 NF-NC 3 NF-NC Y Y Y DOXYCYCLINE DOXYCYCLINE DOXYCYCLINE MINOCYCLINE MINOCYCLINE KIT DOXYCYCLINE DOXYCYCLINE DOXYCYCLINE 1 1 3 1 3 1 1 1 1 1 NF-NC 1 NF-NC 1 1 PA 1 Y Y Y Y MINOCYCLINE TETRACYCLINE TETRACYCLINE DOXYCYCLINE DOXYCYCLINE 3 1 1 1 1 DOXYCYCLINE 3 MAND 90 MAND SPEC PARTNERS MAND SPEC 1 1 NF-NC TETRACYCLINES *ACTICLATE *ADOXA, PAK , 150 Y AVIDOXY DK DORYX 100MG DORYX 150MG *DORYX 200MG MINOCIN MINOCIN PAC *MONODOX ORACEA PERIOSTAT *SOLODYN 55,65, 80, 105, 115 SUMYCIN SUSP TETRACYCLINE VIBRAMYCIN VIBRAMYCIN SUSP VIBRAMYCIN SYRUP Y Y Y 1 PA PA PA PA PA PA PA PA NF-NC 1 1 1 1 NF-NC MACROLIDES BIAXIN, XL Y CLARITHROMYCIN 1 3 Y FIDAXOMICIN ERYTHROMYCIN ETHYLSUCCINATE DIFICID E.E.S. E.E.S. GRANULES E-MYCIN th ERYTHROMYCIN ETHYLSUCCINATE ERYTHROMYCIN BASE th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 1 PA PA PA NF-NC 1 1 3 3 NF-NC NF-NC 34 FORMULARY DRUG PRODUCT NOTES BRAND NAME ERYPED CHEW TABS ERY-TAB ERYTHROCIN KETEK PCE ZITHROMAX GEQ Y Y Y ZMAX GENERIC NAME ERYTHROMYCIN ETHYLSUCCINATE ERYTHROMYCIN BASE ERYTHROMYCIN STEARATE TELITHROMYCIN ERYTHROMYCIN BASE AZITHROMYCIN AZITHROMYCIN TIER HMO POS TPA M-SUPP RDS MICHILD PPO PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY 1 2 1 2 1 3 3 1 1 NF-NC NF-NC MAND 90 MAND SPEC PARTNERS MAND SPEC 1 NF-NC 3 SULFONAMIDES BACTRIM DS, SEPTRA DS Y BACTRIM, SEPTRA Y SULFAMETHOXAZOLE/ TRIMETHOPRIM DS SULFAMETHOXAZOLE/ TRIMETHOPRIM 1 1 1 1 QUINOLONES AVELOX CIPRO Y Y MOXIFLOXACIN CIPROFLOXACIN 1 1 1 1 CIPRO SUSP Y CIPROFLOXACIN GEMIFLOXACIN MESYLATE LEVOFLOXACIN NORFLOXACIN CIPROFLOXACIN 1 1 FACTIVE LEVAQUIN NOROXIN PROQUIN XR Y 3 1 3 2 PA PA PA NF-NC 1 NF-NC NF-NC MISCELLANEOUS ANTIBIOTICS CLEOCIN 75, 150, 300MG FLAGYL FLAGYL ER FUROXONE HIPREX MACROBID th Y Y Y Y CLINDAMYCIN METRONIDAZOLE METRONIDAZOLE FURAZOLIDONE METHENAMINE NITROFURANTOIN th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 1 1 3 3 1 1 PA AG AG AG 1 1 NF-NC NF-NC 1 1 AG 35 FORMULARY DRUG PRODUCT NOTES BRAND NAME MACRODANTIN 25MG MACRODANTIN 50, 100MG MONUROL VANCOCIN XIFAXAN *ZYVOX GEQ Y Y TIER HMO POS TPA M-SUPP RDS MICHILD NITROFURANTOIN 2 NITROFURANTOIN FOSFOMYCIN TROMETHAMINE VANCOMYCIN, ORAL RIFAXIMIN LINEZOLID 1 GENERIC NAME PPO PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY AG AG AG 2 AG AG AG AG 1 AG MAND 90 MAND SPEC PARTNERS MAND SPEC NF-NC 1 NF-NC 3 1 3 2 2 URINARY ANTI-INFECTIVES (UTI) BACTRIM DS, SEPTRA DS Y SULFAMETHOXAZOLE/ TRIMETHOPRIM DS 1 1 BACTRIM, SEPTRA CIPRO Y Y SULFAMETHOXAZOLE/ TRIMETHOPRIM CIPROFLOXACIN 1 1 1 1 CIPRO SUSP MACROBID Y Y CIPROFLOXACIN NITROFURANTOIN 1 1 AG AG AG 1 1 AG NITROFURANTOIN 2 AG AG AG 2 AG 1 1 AG AG AG 1 AG URELLE NITROFURANTOIN TRIMETHOPRIM METHENAMINE/METH BLUE/SALICYLATE UTA VIBRAMYCIN MACRODANTIN 25MG MACRODANTIN 50, 100MG TRIMETHOPRIM Y Y 1 2 2 Y METHENAMINE/METH BLUE/SALICYLATE/NA PHOS/HYOSCY 1 1 Y DOXYCYCLINE 1 1 ORAL ANTIFUNGALS ANCOBON DIFLUCAN FULVICIN U/F th Y Y FLUCYTOSINE FLUCONAZOLE GRISEOFULVIN, ULTRAMICROSIZE th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 1 1 1 1 2 2 36 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ GRIFULVIN-V Y GRIS-PEG LAMISIL MYCELEX TROCHES *NOXAFIL ONMEL ORAVIG SPORANOX CAPS SPORANOX SOLN VFEND TABS Y Y INH MYAMBUTOL MYCOBUTIN PRIFTIN PYRAZINAMIDE RIFADIN Y Y Y Y Y Y GENERIC NAME TIER HMO POS TPA M-SUPP RDS MICHILD PPO PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY GRISEOFULVIN GRISEOFULVIN, ULTRAMICROSIZE TERBINAFINE CLOTRIMAZOLE TROCHES POSACONAZOLE ITRACONAZOLE MICONAZOLE ITRACONAZOLE ITRACONAZOLE VORICONAZOLE 1 1 1 1 1 1 1 3 3 3 1 3 1 1 NF-NC NF-NC NF-NC 1 NF-NC 1 ISONIAZID ETHAMBUTOL RIFABUTIN RIFAPENTINE PYRAZINAMIDE RIFAMPIN 1 1 1 3 1 1 1 1 1 NF-NC 1 1 RIFAMPIN/ ISONIAZID RIFAMPIN/ INH/ PYRAZINAMIDE 3 NF-NC 3 NF-NC CYCLOSERINE BEDAQUILINE FUMARATE ETHIONAMIDE 1 1 3 3 NF-NC NF-NC AMANTADINE FAMCICLOVIR RIMANTADINE ZANAMIVIR 1 1 1 2 MAND 90 MAND SPEC PARTNERS MAND SPEC Y Y ANTITUBERCULOSIS AGENTS Y Y RIFAMATE RIFATER SEROMYCIN PULVULES Y *SIRTURO TRECATOR ANTIVIRALS AMANTADINE FAMVIR FLUMADINE TABS RELENZA th Y Y Y th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 1 1 1 2 37 FORMULARY DRUG PRODUCT NOTES BRAND NAME TAMIFLU VALTREX ZOVIRAX CREAM ZOVIRAX OINT GEQ Y Y GENERIC NAME TIER OSELTAMIVIR VALACYCLOVIR ACYCLOVIR ACYCLOVIR 2 1 2 1 HMO POS TPA M-SUPP RDS MICHILD PPO PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY MAND 90 MAND SPEC PARTNERS MAND SPEC 2 1 2 1 ANTIMALARIALS/ANTIPROTOZOALS ARALEN Y CHLOROQUINE Y Y ARTEMETHER/ LUMEFANTRINE PYRIMETHAMINE ATOVAQUONE/ PROGUANIL ATOVAQUONE COARTEM DARAPRIM MALARONE *MEPRON 1 1 3 2 NF-NC 1 1 1 1 2 NEBUPENT PENTAMIDINE ISETHIONATE 3 NF-NC PLAQUENIL PRIMAQUINE TINDAMAX HYDROXYCHOLOROQUINE PRIMAQUINE TINIDAZOLE 1 2 1 1 2 1 Y Y ANTIHELMINTICS ALBENZA ALINIA BILTRICIDE STROMECTOL ALBENDAZOLE NITAZOXANIDE PRAZIQUANTEL IVERMECTIN NF-NC NF-NC 2 NF-NC 3 3 2 3 AMEBICIDES ARALEN ERY-TAB FLAGYL FLAGYL ER YODOXIN Y Y Y DOLOBID Y CHLOROQUINE ERYTHROMYCIN BASE METRONIDAZOLE METRONIDAZOLE IODOQUINOL 1 1 1 3 3 DIFLUNISAL 1 PA 1 1 1 NF-NC NF-NC ANALGESICS th th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 1 38 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ ANAPROX, DS ANSAID Y Y ARTHROTEC CATAFLAM CELEBREX CLINORIL DAYPRO Y Y *DUEXIS FELDENE FLECTOR INDOCIN SUSP INDOMETHACIN MOBIC MOTRIN NAPRELAN CR NAPROSYN PONSTEL RELAFEN TORADOL Y Y Y Y Y Y Y Y Y Y HMO POS TPA SIGNATURE M-SUPP RDS PARTNERS PPO CLOSED TIER MICHILD PPO MEDICAID FORMULARY NONSTEROIDAL ANTI-INFLAMMATORY DRUGS (NSAIDS) GENERIC NAME NAPROXEN SODIUM FLURBIPROFEN DICLOFENAC/ MISOPROSTOL DICLOFENAC CELECOXIB SULINDAC OXAPROZIN IBUPROFEN/ FAMOTIDINE PIROXICAM DICLOFENAC EPOLAMINE INDOMETHACIN INDOMETHACIN MELOXICAM IBUPROFEN NAPROXEN SODIUM NAPROXEN MEFENAMIC ACID NABUMETONE KETOROLAC ZIPSOR ESOMEPRAZOLE/ NAPROXEN DICLOFENAC DICLOFENAC, EXTENDED RELEASE DICLOFENAC POTASSIUM ZORVOLEX DICLOFENAC *VIMOVO VOLTAREN GEL VOLTAREN XR th Y th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 1 1 1 1 2 1 1 MAND 90 MAND SPEC PARTNERS MAND SPEC 1 1 PA PA PA NF-NC 1 2 DO 1 1 DO DO PA, DO 3 1 PA PA PA NF-NC 1 3 3 1 1 1 3 1 1 1 1 PA AG AG DO PA AG AG DO PA AG AG DO PA PA PA AG AG AG NF-NC NF-NC 1 AG 1 DO 1 NF-NC 1 1 1 1 AG 3 3 PA PA PA PA PA NF-NC NF-NC 1 1 3 PA PA PA NF-NC 3 PA PA PA NF-NC 39 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ 3 1 PA, QL PA, QL PA, QL PA, QL PA, QL PA, QL NF-NC 1 PA, QL MORPHINE SULFATE BUTALBITAL/ ACETAMINOPHEN BUPRENORPHINE PATCH CODEINE TRAMADOL MEPERIDINE HYDROMORPHONE HYDROMORPHONE METHADONE 1 PA, QL PA, QL PA, QL 1 PA, QL 3 PA PA PA NF-NC 3 2 3 1 1 1 1 PA, QL PA, QL PA, QL NF-NC QL QL QL 2 NF-NC 1 1 3 QL PA, QL PA, QL Y FENTANYL HYDROMORPHONE FENTANYL CITRATE BUTALBITAL/ ACETAMINOPHEN/ CAFFEINE BUTALBITAL/ ACETAMINOPHEN/ CAFFEINE BUTALBITAL/ ASPIRIN/ CAFFEINE/ CODEINE HYDROCODONE/ IBUUPROFEN Y MORPHINE SULFATE 1 QL QL QL 1 QL MORPHINE SULFATE 3 QL QL QL NF-NC MORPHINE SULFATE 3 QL QL QL NF-NC Y AVINZA Y BUPAP FIORICET 50-32540 FIORICET 50-30040 FIORINAL W/CODEINE #3 IBUDONE KADIAN 10. 20, 30, 50, 60, 80, 100MG KADIAN 40, 70, 200MG *KADIAN 130, 150MG th TIER SIGNATURE PPO CLOSED FORMULARY FENTANYL SL FENTANYL CITRATE ABSTRAL ACTIQ BUTRANS CODEINE CONZIP DEMEROL DILAUDID DILAUDID 5 LIQUID DOLOPHINE DURAGESIC PATCH EXALGO FENTORA GENERIC NAME HMO POS TPA M-SUPP RDS PARTNERS MICHILD PPO MEDICAID NARCOTIC ANALGESICS Y Y Y Y Y Y Y Y Y th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS MAND 90 MAND SPEC PARTNERS MAND SPEC 1 1 1 1 QL PA, QL PA, QL PA, QL PA, QL PA, QL 1 QL NF-NC NF-NC 1 1 1 1 1 1 1 1 40 FORMULARY DRUG PRODUCT NOTES TIER HMO POS TPA M-SUPP RDS MICHILD FENTANYL ACETAMINOPHEN/ HYDROCODONE METHADONE 3 1 1 Y MORPHINE MORPHINE SULFATE TAPENTADOL HYDROCHLORIDE TAPENTADOL HYDROCHLORIDE OXYMORPHONE OXYMORPHONE OXYCODONE/ IBUPROFEN Y PERCOCET PERCODAN Y Y REPREXAIN PHRENILIN/ PHRENILIN FORTE Y PPO PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY PA, QL PA, QL PA, QL NF-NC QL QL QL 1 QL 1 1 1 QL QL QL 1 1 QL 3 QL QL QL NF-NC 3 3 1 QL QL QL QL QL QL NF-NC NF-NC 1 QL 1 QL QL QL 1 QL OXYMORPHONE 1 PA, QL PA, QL PA, QL 1 PA, QL OXYMORPHONE OXYCODONE ACETAMINOPHEN/ OXYCODONE ASPIRIN/ OXYCODONE IBUPROFEN/ HYDROCODONE BUTALBITAL/ ACETAMINOPHEN 3 2 PA, QL QL PA, QL QL PA, QL PA, QL NF-NC NF-NC 1 1 QL QL QL 1 QL 1 3 PA TRAMADOL 3 PA TRAMADOL ER 1 QL STADOL NS BUTORPHANOL 1 *SUBSYS FENTANYL SL SPRAY 3 BRAND NAME GEQ LAZANDA LORCET, PLUS METHADONE MORPHINE TABLETS MS CONTIN Y Y Y Y NUCYNTA NUCYNTA ER NUMORPHAN OPANA OXYCODONE/ IBUPROFEN OXYMORPHONE ER (NON-CRUSH RESISTANT) OPANA ER (CRUSH RESISTANT) OXYCONTIN Y RYBIX ODT RYZOLT th Y GENERIC NAME th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 1 MAND 90 MAND SPEC PARTNERS MAND SPEC 1 PA PA NF-NC PA NF-NC QL QL 1 QL QL QL QL 1 QL PA, QL PA, QL PA, QL NF-NC 41 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ TYLENOL W/CODEINE Y TYLOX Y ULTRACET ULTRAM Y Y ULTRAM ER Y VICODIN 5/300 VICODIN ES 7.5/300 Y VICODIN HP 10/300 Y VICOPROFEN Y Y XARTEMIS XR XODOL Y ZOHYDRO ER GENERIC NAME ACETAMINOPHEN/ CODEINE ACETAMINOPHEN/ OXYCODONE TRAMADOL/ ACETAMINOPHEN TRAMADOL TRAMADOL SUST. RELEASE ACETAMINOPHEN/ HYDROCODONE ACETAMINOPHEN/ HYDROCODONE ACETAMINOPHEN/ HYDROCODONE IBUPROFEN/ HYDROCODONE ACETAMINOPHEN/ OXYCODONE HYDROCODONE BIT/ ACETAMINOPHEN HYDROCODONE TIER HMO POS TPA M-SUPP RDS MICHILD 1 PPO PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY QL QL QL 1 QL 1 QL QL QL 1 QL 1 1 QL QL QL 1 QL 1 PARTNERS MAND SPEC 1 1 1 PA, QL PA, QL PA, QL 1 PA, QL 1 PA, QL PA, QL PA, QL 1 PA, QL 1 PA, QL PA, QL PA, QL 1 PA, QL 1 1 3 PA, QL PA, QL PA, QL NF-NC 1 QL QL QL 1 QL PA, QL NF-NC 3 MAND 90 MAND SPEC PA, QL PA, QL RESPIRATORY DRUGS ALLERGIES ACCOLATE ALAVERT OTC ALLEGRA OTC BENADRYL CLARINEX TABS/REDITABS CLARITIN OTC PHENERGAN SINGULAIR th Y Y Y Y ZAFIRLUKAST LORATADINE FEXOFENADINE DIPHENHYDRAMINE 1 1 1 1 Y Y Y Y DESLORATIDINE LORATADINE PROMETHAZINE MONTELUKAST 1 1 1 1 th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS NC 1 NC NC NC Y 1 DO DO DO AG AG AG NC NC 1 AG 1 Y 42 FORMULARY DRUG PRODUCT NOTES HMO POS TPA M-SUPP RDS MICHILD PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY BRAND NAME GEQ GENERIC NAME TIER TAVIST XYZAL TABS ZYRTEC OTC Y Y Y CLEMASTINE LEVOCETIRIZINE CETIRIZINE 1 1 1 ASTELIN ASTEPRO ATROVENT NASAL SPRAY Y 1 2 1 2 1 1 QNASL RHINOCORT AQUA AZELASTINE AZELASTINE IPRATROPIUM BROMIDE BECLOMETHASONE, AQUEOUS AZELASTINE/ FLUTICASONE FLUTICASONE TRIAMCINOLONE, AQUEOUS MOMETASONE CICLESONIDE OLOPATADINE BECLOMETHASONE DIPROPIONATE BUDESONIDE VERAMYST ZETONNA Y BECONASE AQ DYMISTA FLONASE NASACORT AQ NASONEX OMNARIS PATANASE TUSSIONEX PENNKINETIC Y Y Y VITUZ ALLEGRA-D 12 HOUR OTC th Y NC PPO NC NASAL SPRAYS PA PA PA NF-NC 3 1 PA PA PA NF-NC 1 PA PA PA PA PA PA 3 1 PA PA PA NF-NC NF-NC FLUTICASONE FUROATE 3 PA PA PA NF-NC CICLESONIDE 3 PA PA PA ANTIHISTAMINE/ANTITUSSIVES NF-NC 1 NC NF-NC 3 PA PA NC DECONGESTANT/ANTIHISTAMINES NF-NC HYDROCODONE/ CHLORPHEN POLIS HYDROCODONE/ CHLORPHENIRAMINE FEXOFENADINE/ PSEUDOEPHEDRINE th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 1 NC NC PARTNERS MAND SPEC 1 1 NC 3 1 3 3 3 MAND 90 MAND SPEC 1 NF-NC NF-NC NF-NC NC 43 FORMULARY DRUG PRODUCT NOTES BRAND NAME ALLEGRA-D 24 HOUR OTC GEQ Y GENERIC NAME FEXOFENADINE/ PSEUDOEPHEDRINE PSEUDOEPHEDRINE/ DESLORATADINE LORATIDINE/ PSEUDOEPHEDRINE PHENYLEPHRINE/ CHLORPHENIRAMINE Y PSEUDOEPHEDRINE/ CHLORPHENIRAMINE Y CLARINEX-D CLARITIN-D OTC DECONAMINE SYRUP DECONAMINE TABS Y TIER HMO POS TPA M-SUPP RDS MICHILD PPO 1 NC NC 3 PA PA PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY PA NC NC 1 1 NC 1 1 NC 1 SEMPREX-D ENTEX LA GUAIFENESIN/ PHENYLEPHRINE 3 NC NF-NC ENTEX LQ GUAIFENESIN/ PHENYLEPHRINE 3 NC NF-NC ZOTEX GP GUAIFENESIN/ PHENYLEPHRINE 3 NC NF-NC BROMFED-DM TESSALON PERLES NC 3 DECONGESTANT/ANTITUSSIVE OR EXPECTORANT Y GUAIFENESIN/ PHENYLEPHRINE Y BROMPHENIRAMINE/ PSEUDOEPHEDRINE/ DEXTROMETHORPHAN 1 Y BENZONATATE 1 PARTNERS MAND SPEC NC PSEUDOEPHEDRINE/ ACRIVAS ZOTEX MAND 90 MAND SPEC NC 1 DECONGESTANT/ANTIHISTAMINE AND ANTITUSSIVES NC NF-NC 1 1 1 ORALLY INHALED DRUGS ACCUNEB ADVAIR AEROSPAN th Y ALBUTEROL SULFATE FLUTICASONE/ SALMETEROL FLUNISOLIDE th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 1 1 2 3 2 NF-NC 44 FORMULARY DRUG PRODUCT NOTES BRAND NAME ALVESCO GEQ ANORO ELLIPTA ARCAPTA ASMANEX ATROVENT HFA BREO ELLIPTA BROVANA COMBIVENT COMBIVENT RESPIMAT CROMOLYN SOLN Y DULERA DUONEB FLOVENT HFA FORADIL ISOETHARINE MAXAIR PROAIR HFA PROVENTIL HFA PULMICORT 0.25MG/2ML AND 0.5MG/2ML RESPULE th Y Y Y GENERIC NAME CICLESONIDE UMECLIDINIUM/ VILANTEROL TIER 3 HMO POS TPA M-SUPP RDS MICHILD PPO PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY NF-NC 3 NF-NC INDACATEROL MOMETASONE FUROATE IPRATROPIUM BROMIDE FLUTICASONE/ VILANTEROL ARFORMOTEROL ALBUTEROL/ IPRATROPIUM ALBUTEROL/ IPRATROPIUM 2 2 2 2 2 2 2 2 2 2 2 2 CROMOLYN SODIUM MOMETASONE/ FORMOTEROL HFA IPRATROPIUM/ ALBUTEROL SULFATE FLUTICASONE 1 1 2 2 1 2 1 2 FORMOTEROL FUMARATE ISOETHARINE PIRBUTEROL ALBUTEROL ALBUTEROL 2 1 3 3 3 2 1 NF-NC NF-NC NF-NC BUDESONIDE 1 2 th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS QL PA PA QL PA PA QL PA PA MAND 90 MAND SPEC PARTNERS MAND SPEC 2 QL 1 45 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ PULMICORT 1MG/2ML RESPULE AND FLEXHALER *PULMOZYME QVAR SEREVENT DISKUS SPIRIVA SYMBICORT TUDORZA PRESSAIR VENTOLIN HFA XOPENEX HFA XOPENEX NEB SOLN Y GENERIC NAME TIER HMO POS TPA M-SUPP RDS MICHILD PPO PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY BUDESONIDE DORNASE ALFA BECLOMETHASONE DIPROPIONATE 2 2 2 2 2 2 SALMETEROL TIOTROPIUM BROMIDE BUDESONIDE/ FORMOTEROL 2 2 2 2 2 2 ACLIDINIUM BROMIDE ALBUTEROL LEVALBUTEROL 2 2 3 2 2 NF-NC LEVALBUTEROL 1 PA PA PA MAND 90 MAND SPEC PARTNERS MAND SPEC 1 OTHER BRONCHODILATORS, ORAL DALIRESP METAPROTERENOL SYRUP VENTOLIN VOSPIRE ER Y Y Y ROFLUMILAST 2 2 METAPROTERENOL, 10MG/5ML ALBUTEROL ALBUTEROL 1 1 1 1 1 1 THEOPHYLLINES AMINOPHYLLINE ELIXOPHYLLIN ELIXIR THEO-24 SR THEOPHYLLINE Y AMINOPHYLLINE 1 1 Y Y THEOPHYLLINE THEOPHYLLINE THEOPHYLLINE 2 2 1 2 2 1 Y Y Y 1 Y LEUKOTRIENE RECEPTOR ANTAGONISTS ACCOLATE th Y ZAFIRLUKAST 1 th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 46 FORMULARY DRUG PRODUCT NOTES BRAND NAME SINGULAIR ZYFLO, CR GEQ GENERIC NAME TIER Y MONTELUKAST ZILEUTON 1 3 DORNASE ALFA 2 PULMOZYME HMO POS TPA M-SUPP RDS MICHILD PA PPO PA MUCOLYTICS PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY PA 1 NF-NC MAND 90 Y MAND SPEC PARTNERS MAND SPEC 2 DERMATOLOGICS TOPICAL STEROIDS ACLOVATE Y APEXICON OINT Y APEXICON E Y CLOBEX SPRAY CLODERM CORDRAN 4MCG/SQ CM TAPE CORDRAN, SP Y CORMAX Y CUTIVATE CUTIVATE 0.05% LOTION DERMA-SMOOTHEFS 0.01% OIL DESONATE GEL DESOWEN Y ALCLOMETASONE DIFLORASONE DIACETATE DIFLORASONE DIACETATE CLOBETASOL PROPIONATE CLOCORTOLONE PIVALATE 1 1 1 1 1 1 2 3 PA PA PA 2 NF-NC 1 PA PA PA 1 PA DIPROSONE Y FLURANDRENOLIDE FLURANDRENOLIDE CLOBETASOL PROPRIONATE FLUTICASONE PROPIONATE FLUTICASONE PROPIONATE FLUOCINOLONE ACETONIDE DESONIDE DESONIDE DESONIDE/EMOLLIENT COMBO BETAMETHASONE DIPROPIONATE ELOCON Y MOMETASONE FUROATE Y Y Y DESOWEN COMBO th th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 3 PA PA PA 1 NF-NC 1 1 1 1 1 1 3 1 PA 3 PA PA PA 1 NF-NC 1 PA PA NF-NC 1 1 1 1 47 FORMULARY DRUG PRODUCT NOTES BRAND NAME HALOG KENALOG GEQ GENERIC NAME TIER Y HALCINONIDE TRIAMCINOLONE 2 1 KENALOG AEROSOL SPRAY LOCOID, CREAM, OINT, SOL. Y LOCOID LOTION LUXIQ Y MOMEXIN NUCORT OLUX OLUX-E Y Y PANDEL PEDIADERM HC 2% KIT PEDIADERM TA SYNALAR KIT TEMOVATE/ TEMOVATE E TOPICORT BRAND ONLY PRODUCTS TOPICORT GENERIC PRODUCTS U-CORT 1%-10% CREAM th Y Y Y TRIAMCINOLONE ACETONIDE HYDROCORTISONE BUTYRATE 0.1% HYDROCORTISONE BUTYRATE/ EMOLL BETAMETHASONE MOMETASONE FUROATE/AMMONIUM LAC HYDROCORTISONE/ ALOE VERA CLOBETASOL PROPIONATE CLOBETASOL EMOLL HYDROCORTISONE PROBUTATE HYDROCORTISONE/ EMOLLIENT TRIAMCINOLONE/ EMOLLIENT FLUOCINOLONE SOLN/ CLEANSER CLOBETASOL PROPIONATE 3 HMO POS TPA M-SUPP RDS MICHILD PPO PARTNERS MEDICAID PA PA PA NF-NC PA PA PA NF-NC 1 PA NF-NC 3 NF-NC 1 1 1 1 PA PA 3 PA NF-NC PA NF-NC 3 PA PA PA NF-NC 3 PA PA PA NF-NC 1 PA PA PA 1 PA DESOXIMETASONE 3 PA PA PA NF-NC DESOXIMETASONE HYDROCORTISONE/ UREA 1 1 1 1 th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS PARTNERS MAND SPEC 1 3 3 MAND 90 MAND SPEC 2 1 1 3 1 SIGNATURE PPO CLOSED FORMULARY 48 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ ULTRAVATE PAC GENERIC NAME HALOBETASOL PROP/ AMMONIUM LAC VANOXIDE-HC 0.5%-5% LOTION HYDROCORTISONE/ BENZOYL PEROXIDE VANOS VERDESO Y WESTCORT Y FLUOCINONIDE DESONIDE HYDROCORTISONE VALERATE TIER HMO POS TPA M-SUPP RDS MICHILD 3 PPO PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY PA PA PA NF-NC 3 PA PA PA NF-NC 1 3 PA PA PA 1 NF-NC 1 MAND 90 MAND SPEC PARTNERS MAND SPEC 1 TOPICAL SULFONAMIDES SULFACETAMIDE/SULF UR AVAR SULFACETAMIDE/SULF UR SULFACETAMIDE/SULF UR AVAR-E AVAR LS PLEXION 9.8-4.8% CRM, LIQ, LOT, PADS ROSANIL SULFACETAMIDE/SULF UR SULFACETAMIDE/SULF UR SUMADAN SULFACETAMIDE/SULF UR AMLACTIN 12% Y ATOPICLAIR CARMOL EPICERAM GORDONS UREA HYDRO 35, 40 HYLATOPIC HYLATOPIC PLUS KERAFOAM Y Y th Y AMMONIUM LACTATE DL-E AC/ GRAPE/ HYALURONIC ACID UREA EMOLLIENT COMBO UREA UREA EMOLLIENT COMBO EMOLLIENT COMBO UREA th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 3 PA PA PA NF-NC 3 PA PA PA NF-NC 3 PA PA PA NF-NC 3 PA PA PA NF-NC 3 PA PA PA NF-NC 3 PA PA TOPICAL EMOLLIENTS PA NF-NC 1 1 1 1 3 3 1 3 3 3 1 1 NF-NC NF-NC 1 NF-NC NF-NC NF-NC PA PA PA PA PA 49 FORMULARY DRUG PRODUCT NOTES BRAND NAME KERALAC CREAM 47% GEQ GENERIC NAME TIER UREA 3 HMO POS TPA M-SUPP RDS MICHILD PPO PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY PA NF-NC KERALAC Y UREA 1 1 KEROL AD Y UREA/LACTIC AC/ZN UNDECYLENATE 1 1 KEROL 50% SUSPENSION Y UREA/ LACTIC ACID/ SALICYL ACID 1 1 AMMONIUM LACTATE EMOLLIENT COMBO 1 3 PA 1 NF-NC PROMISEB EMOLLIENT COMBO 3 PA NF-NC PROMISEB COMPLETE EMOLLIENT COMBO 3 PA NF-NC TROPAZONE EMOLLIENT COMBO 3 PA NF-NC Y UREA 1 UREA UREA UREA 3 1 1 PA Y Y NF-NC 1 1 UREA UREA UREA UREA EMOLLIENT COMBO 3 1 3 1 1 PA NF-NC PA 1 NF-NC PIMECROLIMUS 2 LAC-HYDRIN NEOSALUS UMECTA SUSPENSION UMECTA EMULSION URAMAXIN URAMAXIN GT URAMAXIN GT KIT UREA UTOPIC X-VIATE ZENIEVA Y Y Y Y MAND 90 MAND SPEC PARTNERS MAND SPEC 1 1 1 TOPICAL IMMUNOMODULATORS ELIDEL PA 2 PSORIASIS ANTHRALIN CALCIPOTRIENE Y Y ANTHRALIN CALCIPOTRIENE 1 1 QL QL QL 1 1 QL DOVONEX CRM Y CALCIPOTRIENE 1 QL QL QL 1 QL th th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 50 FORMULARY DRUG PRODUCT NOTES BRAND NAME HMO POS TPA M-SUPP RDS MICHILD QL PARTNERS MEDICAID QL SIGNATURE PPO CLOSED FORMULARY 1 QL MAND 90 Y GEQ GENERIC NAME TIER DOVONEX SOLN Y CALCIPOTRIENE 1 FABIOR FOAM METHOTREXATE *SORIATANE Y TAZAROTENE METHOTREXATE TABS ACITRETIN 3 1 3 NF-NC 1 NF-NC 3 1 3 3 NF-NC 1 QL NF-NC NF-NC TACLONEX SCALP SUSP TACLONEX OINT TAZORAC ZITHRANOL BETAMET DIPROP/ CALCIPOTRIENE Y TAZAROTENE ANTHRALIN SHAMPOO QL PPO QL QL QL MAND SPEC PARTNERS MAND SPEC ANTI-INFECTIVES (TOPICAL) ALTABAX BACTROBAN OINT BACTROBAN CRM BACTROBAN NASAL OINT CORTISPORIN GARAMYCIN SULFAMYLON Y RETAPAMULIN MUPIROCIN 3 1 Y MUPIROCIN 1 MUPIROCIN HYDROCORTISONE/ NEOMYCIN/POLYMYXIN/ BACITRACIN GENTAMICIN MAFENIDE ACETATE 2 Y PA PA PA NF-NC 1 1 PA, QL PA, QL PA, QL 2 1 3 2 PA, QL 2 1 NF-NC BURN PREPARATIONS SILVADENE Y SILVER SULFADIAZINE 1 1 ANTIFUNGALS (TOPICAL) CNL 8 NAIL KIT CICLOPIROX OLAMINE CREAM/ CLEANSER CICLOPIROX SOLN 8%/ LACQUER REMOVAL PADS ECOZA ECONAZOLE NITRATE 3 PA PA PA NF-NC ERTACZO SERTACONAZOLE NITRATE 3 PA PA PA NF-NC CICLODAN KIT th th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 3 PA PA PA NF-NC 3 PA PA PA NF-NC 51 FORMULARY DRUG PRODUCT NOTES BRAND NAME EXELDERM EXTINA JUBLIA SOLUTION KERYDIN KETODAN KIT LAMISIL SOLN LOPROX LOTRIMIN GEQ Y Y Y LOTRISONE LUZU MENTAX METROGEL 0.75% METROGEL 1% Y MYCOSTATIN NAFTIN Y NIZORAL Y Y Y GENERIC NAME SULCONAZOLE NITRATE KETOCONAZOLE EFINACONAZOLE TAVABOROLE KETOCONAZOLE FOAM/ CLEANSER TERBINAFINE CICLOPIROX OLAMINE CLOTRIMAZOLE 1% CLOTRIMAZOLE/ BETAMETHASONE LULICONAZOLE BUTENAFINE METRONIDAZOLE METRONIDAZOLE HMO POS TPA M-SUPP RDS MICHILD PPO PARTNERS MEDICAID 3 1 3 3 PA PA PA PA PA PA PA PA PA NF-NC 1 NF-NC NF-NC 3 3 1 1 PA PA PA PA PA PA NF-NC NF-NC TIER 1 3 3 1 1 SIGNATURE PPO CLOSED FORMULARY PA PA PA PA PA PA 1 NF-NC NF-NC 1 1 1 3 KETOCONAZOLE 1 OXICONAZOLE NITRATE 3 PA PA PA NF-NC NYSTATIN/EMOLLIENT 3 PA PA PA NF-NC 1 NC ROSADAN KIT CICLOPIROX METRONIDAZOLE/ CLEANSER 3 NF-NC TERBINEX TERBINAFINE/ HYDROXYCHITOSAN PEDIADERM AF PENLAC Y PA PA PA 1 NF-NC 1 3 PA PA PA NC 3 PA PA PA NF-NC VUSION SELENIUM SULFIDE MICONAZOLE NITRATE/ZINC OXIDE 3 PA PA PA NF-NC XOLEGEL/ COREPAK KETOCONAZOLE 3 PA PA PA NF-NC TERSI th th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS PARTNERS MAND SPEC 1 1 NYSTATIN NAFTIFINE OXISTAT MAND 90 MAND SPEC 52 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ *ABSORICA ACANYA ACZONE 5% GEL ATRALIN AZELEX BENZACLIN 1%-5% GEL Y BENZAMYCIN GEL Y BENZAMYCINPAK BENZEFOAM ULTRA BENZIQ WASH BREVOXYL CLEOCIN-T CLINDACIN PAC CLINDAGEL DESQUAM X DIFFERIN 0.1% CREAM, GEL DIFFERIN 0.1% LOTION DIFFERIN 0.3% GEL DUAC EPIDUO FINACEA th GENERIC NAME TIER HMO POS TPA M-SUPP RDS MICHILD PPO ACNE PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY 3 3 PA PA PA NF-NC DAPSONE TRETINOIN AZELAIC ACID CLINDAMYCIN/ BENZOYL PEROXIDE ERYTHROMYCIN/ BENZOYL PEROXIDE 3 3 3 PA PA, AG PA PA, AG PA PA, AG NF-NC NF-NC NF-NC 1 1 1 1 3 Y BENZOYL PEROXIDE 1 1 Y Y Y Y BENZOYL PEROXIDE BENZOYL PEROXIDE CLINDAMYCIN CLINDAMYCIN CLINDAMYCIN BENZOYL PEROXIDE 1 1 1 3 3 1 1 1 1 NF-NC NF-NC 1 Y ADAPALENE 1 ADAPALENE 3 ADAPALENE CLINDAMYCIN PHOSPHATE-BENZOYL PEROXIDE ADAPALENE/BENZOYL PEROXIDE AZELAIC ACID 1 1 1 1 Y th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 3 3 PARTNERS MAND SPEC NF-NC ISOTRETINOIN CLINDAMYCIN/ BENZOYL PEROXIDE ERYTHROMYCIN BASE/ BENZOYL PEROXIDE Y MAND 90 MAND SPEC PA PA PA PA PA PA PA PA PA NF-NC 1 PA PA PA PA PA PA NF-NC NF-NC NF-NC 53 FORMULARY DRUG PRODUCT NOTES BRAND NAME NUOX GEL PACNEX PACNEX MX RETIN A RETIN A MICRO 0.1%, 0.04% RETIN A MICRO 0.8% RIAX TRETIN X TRIAZ CLEANER/PADS/ FOAMING CLOTHS GEQ Y Y Y Y Y PA PPO SIGNATURE PPO CLOSED FORMULARY PA PA NF-NC 3 1 1 1 AG AG AG 1 1 1 AG 1 AG AG AG 1 AG 3 3 3 PA, AG PA, AG PA, AG PA, AG PA, AG PA, AG NF-NC NF-NC NF-NC 1 SULFANILAMIDE 2 2 Y CLINDAMYCIN 1 1 Y Y CLINDAMYCIN FLUCONAZOLE METRONIDAZOLE METRONIDAZOLE 3 1 1 3 NF-NC 1 1 NF-NC Y Y METRONIDAZOLE NYSTATIN 1 1 1 1 Y NYSTATIN 1 1 VELTIN ZACARE KIT ZIANA th TIER PARTNERS MEDICAID BENZOYL PEROXIDE BENZOYL PEROXIDE/ HC/SKIN CLNSR NO. 14 CLINDAMYCIN/ TRETINOIN BENZOYL PEROXIDE/ HYALURONT CLINDAMYCIN/ TRETINOIN VANOXIDE HC AVC CREAM CLEOCIN VAGINAL CREAM CLEOCIN VAGINAL OVULE DIFLUCAN FLAGYL FLAGYL ER METROGELVAGINAL 0.75% MYCOSTATIN NYSTATIN VAGINAL TABS GENERIC NAME BENZOYL PEROXIDE/ SULFUR BENZOYL PEROXIDE BENZOYL PEROXIDE TRETINOIN TRETINOIN MICROSPHERES TRETINOIN MICROSPHERES BENZOYL PEROXIDE TRETINOIN HMO POS TPA M-SUPP RDS MICHILD th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS PARTNERS MAND SPEC 1 3 PA PA PA NF-NC 3 PA, AG PA, AG PA, AG NF-NC 3 PA PA PA NF-NC 3 MAND 90 MAND SPEC PA, AG PA, AG PA, AG VAGINAL ANTIBIOTIC/ANTIFUNGAL PRODUCTS PA NF-NC 54 FORMULARY DRUG PRODUCT NOTES BRAND NAME TERAZOL GEQ GENERIC NAME TIER Y TERCONAZOLE 1 HMO POS TPA M-SUPP RDS MICHILD PPO PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY MAND 90 MAND SPEC PARTNERS MAND SPEC 1 SCABICIDES & PEDICULOCIDES EURAX OVIDE SKLICE ULESFIA Y CROTAMITON MALATHION IVERMECTIN BENZYL ALCOHOL NF-NC 1 NF-NC NF-NC 3 1 3 3 TOPICAL ENZYMES GRANULEX Y OPTASE TRYPSIN/ BALSAM PERU/ CASTOR OIL TRYPSIN/ BALSAM PERU/ CASTOR OIL 1 1 2 2 OTHER AGENTS ALDARA *CARAC CONDYLOX GEL CONDYLOX SOLUTION MIRVASO PANRETIN *PICATO PROTOPIC SOLARAZE TARGRETIN VECTICAL Y Y IMIQUIMOD FLUOROURACIL PODOFILOX 1 1 3 1 1 NF-NC Y PODOFILOX BRIMONIDINE ALITRETINOIN 1 3 2 1 NF-NC 2 INGENOL MEBUTATE TACROLIMUS DICLOFENAC SODIUM BEXAROTENE CALCITRIOL 3 1 1 2 3 SINECATECHINS IMIQUIMOD 3 3 Y *VEREGEN *ZYCLARA PA PA PA PA PA PA QL QL QL NF-NC 1 PA 1PA 2 NF-NC PA NF-NC NF-NC PA PA BLOOD MODIFIERS ANTICOAGULANTS BRILINTA COUMADIN ELIQUIS th Y TICAGRELOR WARFARIN APIXABAN 3 1 3 th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS DO DO DO DO DO DO NF-NC 1 NF-NC 55 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ GENERIC NAME TIER PRADAXA XARELTO 10mg DALTEPARIN SODIUM,PORCINE ENOXAPARIN DABIGATRAN ETEXILATE MESYLATE RIVAROXABAN XARELTO 15mg XARELTO 20mg RIVAROXABAN RIVAROXABAN *FRAGMIN LOVENOX AGGRENOX AGRYLIN EFFIENT PERSANTINE PLAVIX PLETAL Y Y Y Y Y PPO PARTNERS MEDICAID 2 2 DO QL DO QL DO DO ANTI-PLATELET DRUGS DO QL 2 DO 2 QL DO 2 2 DO NF-NC 3 1 2 1 1 1 SIGNATURE PPO CLOSED FORMULARY MAND 90 MAND SPEC PARTNERS MAND SPEC Y Y Y Y NF-NC 1 3 1 2 2 ASPIRIN/ DIPYRIDAMOLE ANEGRELIDE PRASUGREL HYDROCHLORIDE DIPYRIDAMOLE CLOPIDOGREL CILOSTAZOLE HMO POS TPA M-SUPP RDS MICHILD 1 DO AG DO AG DO AG 2 DO 1 AG Y Y 1 1 Y Y Y 1 Y HEMORRHEOLOGIC AGENTS TRENTAL Y PENTOXIFYLLINE 1 COLONY STIMULATING FACTORS LEUKINE 250MCG/ML *LEUKINE 500MCG/ML *NEUPOGEN SARGRAMOSTIM 2 4 SPEC SARGRAMOSTIM FILGRASTIM 2 2 4 SPEC 4 SPEC ERYTHROCYTE STIMULATORS ARANESP EPOGEN PROCRIT #AMICAR #AMICAR 1,000MG th Y DARBEPOETIN ALFA IN POLYSORBATE EPOETIN ALFA EPOETIN ALFA 3 2 2 AMINOCAPROIC ACID 1 1 AMINOCAPROIC ACID 3 NF-NC th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS PA PA PA PA PA PA HEMOSTATICS PA PA PA NF-NC 4 SPEC PA 4 SPEC PA 56 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ GENERIC NAME TIER HMO POS TPA M-SUPP RDS MICHILD PPO EENT DRUGS SIGNATURE PPO CLOSED FORMULARY MAND 90 1 Y PA NF-NC Y PA 1 2 1 NF-NC Y Y Y Y Y Y PARTNERS MEDICAID MAND SPEC PARTNERS MAND SPEC GLAUCOMA AGENTS ALPHAGAN P 0.15% ALPHAGAN P 0.1% ATROPINE AZOPT BETAGAN BETIMOL BETOPIC 0.5% BETOPTIC S COSOPT Y Y Y Y ISOPTO CARBACHOL1%, 2%, 4% th 3 1 2 1 3 PA PA 1 3 1 NF-NC 1 3 NF-NC Y Y Y CYCLOPENTOLATE CYCLOPENTOLATE ACETAZOLAMIDE APRACLONIDINE APRACLONIDINE 2 1 1 1 3 2 1 1 1 NF-NC Y Y Y CARBACHOL 1 1 Y CARBACHOL 3 NF-NC Y HOMATROPINE 1 1 HOMATROPINE TIMOLOL BIMATOPROST BIMATOPROST 3 3 2 3 NF-NC NF-NC 2 PA NF-NC Y ISOPTO CARBACHOL 8% ISOPTO HOMATROPINE 5% ISOPTO HOMATROPINE 2% ISTALOL LUMIGAN 0.01% LUMIGAN 0.03% 1 BETAXOLOL BETAXOLOL TIMOLOL/ DORZOLAM DORZOLAMIDE/TIMOL OL COSOPT PF CYCLOGYL 0.5%, CYCLOGYL 1%, 2% DIAMOXSEQUELS IOPIDINE 0.5% IOPIDINE 1% BRIMONIDINE TARTRATE BRIMONIDINE TARTRATE ATROPINE SULFATE BRINZOLAMIDE LEVOBUNOLOL TIMOLOL Y th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS PA PA PA PA PA PA PA PA PA Y Y 57 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ METIPRANOLOL MYDRIACYL NEPTAZANE Y Y Y PHOSPHOLINE IODIDE SOLN PILOCAR PILOPINE HS PROPINE Y TRAVATAN Z TRUSOPT XALATAN ZIOPTAN th PPO SIGNATURE PPO CLOSED FORMULARY MAND 90 Y 1 1 1 1 1 1 ECHOTHIOPHATE PILOCARPINE PILOCARPINE DIPIVEFRIN 2 1 2 3 2 1 2 NF-NC Y Y Y BRINZOLAMIDE/ BIMONIDINE TARTRATE 3 NF-NC Y Y TIMOLOL 1 1 Y Y TIMOLOL TIMOLOL 2 1 2 1 Y TRAVOPROST DORZOLAMIDE LATANOPROST TAFLUPROST 3 1 1 3 NF-NC 1 1 NF-NC Y Y Y Y Y Y ALREX DECADRON FLAREX FML FML FORTE FML S.O.P. LOTEMAX MAXIDEX PRED FORTE TIER PARTNERS MEDICAID METIPRANOLOL TROPICAMIDE METHAZOLAMIDE SIMBRINZA TIMOPTIC TIMOPTIC OCUDOSE TIMOPTIC XE GENERIC NAME HMO POS TPA M-SUPP RDS MICHILD Y LOTEPREDNOL ETABONATE DEXAMETHASONE FLUOROMETHOLONE FLUOROMETHOLONE FLUOROMETHOLONE FLUOROMETHOLONE LOTEPREDNOL ETABONATE DEXAMETHASONE PREDNISOLONE th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS PA PA PA PA, DO PA, DO PA, DO TOPICAL OPHTHALMIC STEROIDS PARTNERS MAND SPEC NF-NC NF-NC NF-NC NF-NC NF-NC 3 3 3 3 3 2 3 2 1 MAND SPEC 2 PA NF-NC 2 1 58 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ HMO POS TPA M-SUPP RDS MICHILD PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY GENERIC NAME TIER PRED MILD VEXOL PREDNISOLONE RIMEXOLONE 2 3 ALODOX AZASITE DOXYCYCLINE/ EYELID CLNS NO.2&3 AZITHROMYCIN 3 3 NF-NC NF-NC BESIVANCE BESIFLOXACIN HYDROCHLORIDE 3 NF-NC SULFACETAMIDE SODIUM CIPROFLOXACIN CIPROFLOXACIN ERYTHROMYCIN GENTAMICIN ERYTHROMYCIN LEVOFLOXACIN NATAMYCIN 1 3 1 1 1 1 3 3 1 NF-NC 1 1 1 1 1 1 1 1 2 1 2 1 1 1 2 1 2 1 3 NF-NC PPO MAND 90 MAND SPEC PARTNERS MAND SPEC 2 NF-NC TOPICAL OPHTHALMIC ANTIBIOTICS BLEPH-10 CILOXAN GEL CILOXAN SOLN ERYTHROMYCIN GARAMYCIN ILOTYCIN IQUIX NATACYN Y Y Y Y Y NEOSPORIN OCUFLOX Y Y POLYSPORIN Y POLYTRIM QUIXIN TOBREX OINT TOBREX SOLN VIGAMOX VIROPTIC Y Y ZYLET th Y Y POLYMYXIN/ BACITRACIN/ NEOMYCIN OFLOXACIN POLYMYXIN/ BACITRACIN POLYMYXIN/ TRIMETHOPRIM LEVOFLOXACIN TOBRAMYCIN TOBRAMYCIN MOXIFLOXACIN TRIFLURIDINE TOBRAMYCIN/ LOTEPRED ETAB th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 1 1 1 1 NF-NC NF-NC 59 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ BLEPHAMIDE BLEPHAMIDE S.O.P. CORTISPORIN Y HMO POS TPA SIGNATURE M-SUPP RDS PARTNERS PPO CLOSED TIER MICHILD PPO MEDICAID FORMULARY TOPICAL OPHTHALMIC ANTI-INFECTIVE/ANTI-INFLAMMATORY GENERIC NAME SULFACETAMIDE/ PREDNISOLONE SULFACETAMIDE/ PREDNISOLONE HYDROCORTISONE/ NEOMYCIN/ POLYMYXIN/ BACITRACIN TOBRADEX OINT DEXAMETHASONE/ NEOMYCIN/ POLYMYXIN CYCLOSPORINE DEXAMETHASONE/ TOBRAMYCIN DEXAMETHASONE/ TOBRAMYCIN TOBRADEX ST TOBRAMYCIN/ DEXAMETHASONE MAXITROL RESTASIS Y TOBRADEX SUSP Y ALOCRIL BEPREVE ELESTAT EMADINE LASTACAFT OPTIVAR PATADAY PATANOL ZADITOR OTC th Y Y Y 2 2 1 1 QL QL PA, QL PARTNERS MAND SPEC 1 2 QL 1 1 2 2 NF-NC 3 TOPICAL OPHTHALMIC VASOCONSTRICTORS/ANTIHISTAMINES BEPOTASTINE BESILATE EPINASTINE EMEDASTINE DIFUMARATE ALCAFTADINE AZELASTINE OLOPATADINE OLOPATADINE KETOTIFEN th 2 1 2 NEDOCROMIL SODIUM LODOXAMIDE TROMETHAMINE ALOMIDE 2 MAND 90 MAND SPEC *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 3 PA PA PA NC 3 PA PA PA NC 3 1 PA PA PA NC 1 3 3 1 3 2 1 PA PA PA PA PA PA PA PA PA PA PA PA NC NC NC NC NC 1 60 FORMULARY DRUG PRODUCT NOTES BRAND NAME ACULAR, LS ACUVAIL BROMDAY ILEVRO NEVANAC PROLENSA GEQ Y Y GENERIC NAME TIER KETOROLAC TROMETHAMINE KETOROLAC TROMETHAMINE BROMFENAC SODIUM NEPAFENAC NEPAFENAC BROMFENAC SODIUM HMO POS TPA M-SUPP RDS PARTNERS MICHILD PPO MEDICAID TOPICAL OPHTHALMIC NSAIDS 1 SIGNATURE PPO CLOSED FORMULARY MAND 90 MAND SPEC PARTNERS MAND SPEC 1 PA 3 1 3 2 3 PA PA PA NF-NC 1 NF-NC 2 NF-NC OTIC AGENTS BENZOCAINEANTIPYRINE AURALGAN CETRAXAL Y CIPRO HC CIPRODEX COLY-MYCIN S CORTISPORIN Y CORTISPORIN-TC DOMEBORO Y TREAGAN OTIC Y TRIOXIN VOSOL Y Y VOSOL HC Y th CIPROFLOXACIN CIPROFLOXACIN HCL/ HC CIPROFLOXACIN/ DEXAMETH NEOMY SULF/ COLIST SUL/ HC/ THONZ HYDROCORTISONE/ NEOMYCIN/ POLYMYXIN NEOMY SULF/ COLIST SUL/ HC/ THONZ ACETIC ACID ANTIPYRINEBENZOCAINEPOLYCOSANOL CHLOROXYLENOL/ BENZOC/HYDROCORT ACETIC ACID ACETIC ACID/ HYDROCORTISONE th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 3 NF-NC 1 1 3 PA 2 2 2 PA 1 3 1 NF-NC 2 1 PA NF-NC 1 1 1 1 1 1 1 1 1 61 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ GENERIC NAME TIER HMO POS TPA M-SUPP RDS PARTNERS MICHILD PPO MEDICAID BEHAVIORAL HEALTH SIGNATURE PPO CLOSED FORMULARY MAND 90 MAND SPEC PARTNERS MAND SPEC DEPRESSION AMITRIPTYLINE ANAFRANIL APLENZIN BRINTELLIX CELEXA CYMBALTA EFFEXOR XR EMSAM PATCH Y Y Y Y Y FETZIMA FORFIVO XL LEXAPRO Y LUVOX CR NARDIL NORPRAMIN Y Y Y OLEPTRO ER PAMELOR PARNATE PAXIL, CR PEXEVA PRISTIQ PROZAC PROZAC WEEKLY REMERON SARAFEM DOXEPIN th Y Y Y Y Y Y Y AMITRIPTYLINE CLOMIPRAMINE BUPROPION VORTIOXETINE CITALOPRAM DULOXETINE VENLAFAXINE SELEGILINE 1 1 3 3 1 1 1 3 LEVOMILNACIPRAN 3 BUPROPION ESCITALOPRAM FLUVOXAMINE MALEATE PHENELZINE DESIPRAMINE TRAZODONE HYDROCHLORIDE EXTENDED RELEASE NORTRIPTYLINE TRANYLCYPROMINE PAROXETINE PAROXETINE 3 1 DESVENLAFAXINE SUCCINATE FLUOXETINE FLUOXETINE MIRTAZAPINE FLUOXETINE DOXEPIN th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS AG AG PA PA PA PA DO DO DO 1 1 1 PA, DO PA, DO 3 1 1 1 3 PA 2 1 1 1 3 1 PA, DO DO DO PA PA PA MDCH MDCH MDCH MDCH MDCH MDCH MDCH MDCH 1 NF-NC NF-NC 1 1 1 NF-NC MDCH NF-NC MDCH MDCH NF-NC 1 DO MDCH MDCH MDCH NF-NC MDCH MDCH MDCH MDCH MDCH NF-NC 1 1 1 NF-NC MDCH MDCH MDCH MDCH MDCH MDCH 2 DO 1 AG 1 1 1 1 1 NF-NC 1 62 FORMULARY DRUG PRODUCT NOTES BRAND NAME SURMONTIL TOFRANIL, PM VIIBRYD VIVACTIL WELLBUTRIN, SR WELLBUTRIN XL ZOLOFT GEQ Y Y Y Y Y GENERIC NAME TIER TRIMIPRAMINE MALEATE IMIPRAMINE PAMOATE VILAZODONE PROTRIPTYLINE BUPROPION BUPROPION SERTRALINE 3 1 3 1 1 1 1 HMO POS TPA M-SUPP RDS MICHILD PPO AG PA, DO AG PA, DO DO DO PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY MDCH MDCH MDCH MDCH MDCH MDCH MDCH NF-NC 1 AG NF-NC 1 1 1 DO MDCH MDCH MDCH MDCH MDCH MDCH MDCH 1 1 1 1 NF-NC 1 1 AG 1 AG MDCH 1 MDCH 1 MAND 90 MAND SPEC PARTNERS MAND SPEC 1 ANXIETY ATIVAN BUSPAR MILTOWN NIRAVAM SILENOR TRANXENE T VALIUM Y Y Y Y VISTARIL 1 1 1 1 3 1 1 Y LORAZEPAM BUSPIRONE MEPROBAMATE ALPRAZOLAM DOXEPIN CLORAZEPATE DIAZEPAM HYDROXYZINE PAMOATE XANAX Y ALPRAZOLAM 1 XANAX XR Y ALPRAZOLAM 1 Y Y 1 PA, DO PA, DO AG AG INSOMNIA Y Y Y ZOLPIDEM LORAZEPAM DIPHENHYDRAMINE 1 1 1 DO DO MDCH MDCH 1 DO 1 1 EDLUAR HETLIOZ INTERMEZZO LUNESTA 3 3 3 1 PA, DO PA, DO PA, DO DO PA, DO DO MDCH MDCH MDCH Y ZOLPIDEM TARTRATE TASIMELTEON ZOLPIDEM SL ESZOPICLONE MDCH NF-NC NF-NC NF-NC 1 DO RESTORIL Y TEMAZEPAM 1 DO MDCH 1 RAMELTEON 3 PA, DO MDCH NF-NC AMBIEN, CR ATIVAN BENADRYL ROZEREM th th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS PA, DO 63 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ GENERIC NAME TIER HMO POS TPA M-SUPP RDS MICHILD PPO PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY 1 SOMNOTE Y CHLORAL HYDRATE 1 MDCH SONATA ZOLPIMIST Y ZALEPLON ZOLPIDEM TARTRATE 1 3 MDCH DO MDCH PA, DO PA, DO PSYCHOSIS/MANIC DEPRESSIVES 1 NF-NC ARIPIPRAZOLE LOXAPINE CLOZAPINE CLOZAPINE 2 3 1 1 MDCH MDCH MDCH MDCH 2 NF-NC 1 1 LITHIUM ILOPERIDONE CLOZAPINE 1 3 2 MDCH MDCH MDCH 1 NF-NC ZIPRASIDONE MESYLATE HALOPERIDOL PALIPERIDONE 1 1 2 MDCH MDCH MDCH 1 1 2 LURASIDONE LITHIUM 3 1 MDCH MDCH NF-NC 1 ABILIFY ADASUVE CLOZAPINE CLOZARIL Y Y ESKALITH, CR FANAPT FAZACLO Y GEODON HALDOL INVEGA Y Y LATUDA LITHOBID Y DO PA PA Y LOXAPINE MOLINDONE 1 3 MDCH MDCH 1 NF-NC NAVANE NAVANE 20 ORAP Y THIOTHIXENE THIOTHIXENE PIMOZIDE 1 2 2 MDCH MDCH MDCH 1 2 2 RISPERDAL Y RISPERIDONE 1 MDCH 1 RISPERDAL CONSTA RISPERIDONE MICROSPHERES M MDCH M SAPHRIS ASENAPINE 2 MDCH 2 1 MDCH 1 2 MDCH 2 SEROQUEL SEROQUEL XR th Y QUETIAPINE FUMARATE QUETIAPINE FUMARATE th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS SP PARTNERS MAND SPEC 2 LOXITANE MOBAN SP MAND 90 MAND SPEC 64 FORMULARY DRUG PRODUCT NOTES BRAND NAME PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY 1 MDCH 1 MDCH NF-NC SYMBYAX GENERIC NAME OLANZAPINE/ FLUOXETINE VERSACLOZ CLOZAPINE 3 OLANZAPINE 1 ZYPREXA, ZYDIS GEQ Y ADDERALL Y ADDERALL XR Y AMPHETAMINE/ DEXTROAMPHETAMINE XR Y CONCERTA Y DAYTRANA DESOXYN Y TIER AMPHETAMINE/ DEXTROAMPHETAMINE AMPHETAMINE/ DEXTROAMPHETAMINE XR AMPHETAMINE/ DEXTROAMPHETAMINE XR METHYLPHENIDATE, SUST. RELEASE METHYLPHENIDATE PATCH METHAMPHETAMINE DEXMETHYLPHENIDATE DEXMETHYLPHENIDATE DEXMETHYLPHENIDATE GUANFACINE HMO POS TPA M-SUPP RDS MICHILD PPO MDCH DO ATTENTION DEFICIT DISORDER/NARCOLEPSY MDCH 1 1 MDCH 1 MDCH NC MDCH 1 MDCH MDCH NF-NC 1 MDCH 1 1 MDCH 1 NF-NC NF-NC NC NC 1 3 1 PA PA 1 FOCALIN FOCALIN XR 15, 30, 40mg FOCALIN XR 5, 10, 20, 25, 35mg INTUNIV Y KAPVAY METADATE CD Y Y CLONIDINE METHYLPHENIDATE 1 1 MDCH MDCH MDCH MDCH METADATE ER METHYLIN CHEW TAB METHYLIN SOLN 5MG/5ML NUVIGIL Y METHYLPHENIDATE 1 MDCH 1 METHYLPHENIDATE 3 MDCH NF-NC METHYLPHENIDATE ARMODAFINIL 1 2 MDCH MDCH 1 2 PA, DO th Y Y th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 3 3 PA PA, DO PA, DO PA PA, DO PA, DO PARTNERS MAND SPEC 1 1 NC MAND 90 MAND SPEC 1 1 65 FORMULARY DRUG PRODUCT NOTES BRAND NAME PROVIGIL GEQ Y GENERIC NAME TIER 1 VYVANSE MODAFINIL METHYLPHENIDATE ORAL SUSP METHYLPHENIDATE METHYLPHENIDATE METHYLPHENIDATE ATOMOXETINE LISDEXAMFETAMINE DIMESYLATE *XYREM ZENZEDI 2.5, 7.5, 15, 20, 30MG SODIUM OXYBATE DEXTROAMPHETAMINE QUILLIVANT XR RITALIN RITALIN LA RITALIN SR STRATTERA Y Y Y HMO POS TPA M-SUPP RDS MICHILD PPO PARTNERS MEDICAID MDCH SIGNATURE PPO CLOSED FORMULARY PA, DO 1 1 1 2 PA, DO PA PA MDCH NF-NC PA, DO PA, DO MDCH NF-NC MDCH NF-NC PA, DO 3 3 PA 3 PARTNERS MAND SPEC 1 MDCH MDCH MDCH MDCH MDCH PA 3 1 1 1 2 MAND 90 MAND SPEC NF-NC Y ANTICONVULSANTS APTIOM 200MG *APTIOM 400, 600, 800MG BANZEL CARBATROL CELONTIN DEPAKENE DEPAKOTE DIASTAT DIASTAT ACUDIAL DILANTIN 100MG CAPS DILANTIN 30 KEPSEAL DILANTIN 50 INFATAB FANATREX FELBATOL FYCOMPA GABITRIL th Y Y Y Y Y ESLICARBAZEPINE 3 PA PA MDCH NF-NC ESLICARBAZEPINE RUFINAMIDE CARBAMAZEPINE METHSUXIMIDE VALPROIC ACID DIVALPROEX SODIUM DIAZEPAM DIAZEPAM 3 2 1 2 1 1 1 3 PA PA MDCH MDCH MDCH MDCH MDCH MDCH MDCH MDCH NF-NC 2 1 2 1 1 1 NF-NC PHENYTOIN 1 MDCH 1 MDCH NF-NC MDCH MDCH MDCH MDCH MDCH 1 2 1 NF-NC 1 3 PHENYTOIN Y Y Y PHENYTOIN GABAPENTIN FELBAMATE PERAMPANEL TIAGABINE 1 2 1 3 1 th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 66 FORMULARY DRUG PRODUCT NOTES HMO POS TPA M-SUPP RDS MICHILD SIGNATURE PPO CLOSED FORMULARY GEQ GENERIC NAME TIER Y Y Y TIAGABINE LEVETIRACETAM LEVETIRACETAM CLONAZEPAM 2 1 1 1 PARTNERS MEDICAID MDCH MDCH MDCH MDCH Y LAMOTRIGINE 1 MDCH 1 LAMICTAL/XR LAMICTAL ODT LAMICTAL/XR STARTER KIT LYRICA MYSOLINE NEURONTIN ONFI TABLETS ONFI SUSPENSION OXTELLAR XR PEGANONE PHENOBARBITAL POTIGA QUDEXY XR SABRIL TEGRETOL, XR TEGRETOL XR 100MG TOPAMAX TRILEPTAL TROKENDI XR VIMPAT ZARONTIN ZONEGRAN Y LAMOTRIGINE LAMOTRIGINE 1 2 MDCH MDCH 1 2 LAMOTRIGINE PREGABALIN PRIMIDONE GABAPENTIN CLOBAZAM CLOBAZAM OXCARBAZEPINE ETHOTOIN PHENOBARBITAL EZOGABINE TOPIRAMATE ER VIGABATRIN CARBAMAZEPINE 2 2 1 1 2 3 3 2 1 3 1 2 1 MDCH MDCH MDCH MDCH MDCH MDCH MDCH MDCH MDCH MDCH MDCH MDCH MDCH 2 2 1 1 2 NF-NC NF-NC Y Y CARBAMAZEPINE TOPIRAMATE OXCARBAZEPINE TOPIRAMATE LACOSAMIDE ETHOSUXIMIDE ZONISAMIDE 2 1 1 3 2 1 1 MDCH MDCH MDCH MDCH MDCH MDCH MDCH 2 1 1 NF-NC 2 1 1 AMERGE Y NARATRIPTAN 1 QL 1 QL BRAND NAME GABITRIL12,16MG KEPPRA KEPPRA XR KLONOPIN LAMICTAL 5, 25MG DISPER TABLET Y Y Y Y Y Y Y PPO QL MAND 90 MAND SPEC PARTNERS MAND SPEC 2 1 1 1 2 1 NF-NC 1 2 1 MIGRAINE MEDICATIONS th th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS QL QL 67 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ AXERT CAMBIA Y FROVA IMITREX INJECTION Y IMITREX SPRAY IMITREX TABLET PROPRANOLOL INDERAL LA Y Y Y Y MAXALT, MLT Y ERGOTAMINE/ CAFFEINE DICLOFENAC POTASSIUM BUTALBITAL/ ASA/ CAFFEINE PA, QL PA, QL NF-NC PA PA PA NF-NC 1 PA, QL NF-NC 1 QL QL QL 1 QL 1 1 1 1 QL QL QL QL QL QL 1QL 1 QL 1 1 1 QL QL QL 1 QL 3 PA, QL PA, QL PA, QL NF-NC 1 PA, QL PA, QL PA, QL 1 3 1 Y CYCLOBENZAPRINE BACLOFEN th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 1 2 QL QL PA, QL 1 2 QL 3 PA, QL PA, QL PA, QL NF-NC 3 PA, QL PA, QL PA, QL NF-NC 3 1 MAND 90 MAND SPEC PARTNERS MAND SPEC 1 PA, QL *AMRIX BACLOFEN th PA, QL PA, QL Y Y 3 SIGNATURE PPO CLOSED FORMULARY NF-NC 3 TREXIMET ZOMIG NASAL SPRAY ZOMIG, ZMT PRODRIN RELPAX *SUMAVEL DOSEPRO Y 3 PPO PA, QL PARTNERS MEDICAID PA, QL FROVATRIPTAN SUMATRIPTAN INJECTION SUMATRIPTAN NASAL SPRAY SUMATRIPTAN TABLET PROPRANOLOL PROPRANOLOL SR RIZATRIPTAN ERGOTAMINE TARTRATE/CAFFEINE DIHYDROERGOTAMINE ACETAMINOPHENISOMETHEPTENECAFFEINE ELETRIPTAN SUMATRIPTAN INJECTION SUMATRIPTAN/ NAPROXEN ZOLMITRIPTAN NASAL SPRAY ZOLMITRIPTAN MIGERGOT MIGRANAL NASAL SPRAY 3 TIER ALMOTRIPTAN CAFERGOT FIORINAL GENERIC NAME HMO POS TPA M-SUPP RDS MICHILD PA, QL QL QL QL QL QL QL SKELETAL MUSCLE RELAXANTS PA, AG AG PA, AG NF-NC 1 QL NF-NC 1 68 FORMULARY DRUG PRODUCT NOTES BRAND NAME COMFORT PACTIZANIDINE DANTRIUM FLEXERIL FEXMID LORZONE NORFLEX PARAFON FORTE DSC ROBAXIN SKELAXIN SOMA 250 SOMA 350 ZANAFLEX GEQ GENERIC NAME TIER Y TIZANIDINE COMBO DANTROLENE CYCLOBENZAPRINE CYCLOBENZAPRINE CHLORZOXAZONE ORPHENADRINE 3 1 1 1 3 1 Y Y Y Y Y CHLORZOXAZONE METHOCARBAMOL METAXALONE CARISOPRODOL CARISOPRODOL 1 1 1 1 1 Y TIZANIDINE 1 Y Y Y HMO POS TPA M-SUPP RDS MICHILD PPO PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY AG AG AG AG AG AG AG AG AG NF-NC 1 1 AG 1 NF-NC 1 AG AG AG AG AG AG AG AG AG AG AG AG AG AG NC NC 1 AG 1 AG 1 AG NF-NC NF-NC MAND 90 MAND SPEC PARTNERS MAND SPEC 1 MISCELLANEOUS AUTONOMIC AGENTS MESTINON MESTINON 180 Y PYRIDOSTIGMINE PYRIDOSTIGMINE 1 3 1 NF-NC PARKINSON'S DISEASE (PD) *APOKYN AZILECT COGENTIN COMTAN LODOSYN MIRAPEX MIRAPEX ER NEUPRO Y Y Y Y PARCOPA PARLODEL REQUIP Y Y Y th APOMORPHINE RASAGILINE BENZTROPINE ENTACAPONE CARBIDOPA PRAMIPEXOLE PRAMIPEXOLE DI-HCL ROTIGOTINE 3 2 1 1 1 1 3 3 CARBIDOPA/ LEVODOPA BROMOCRIPTINE ROPINIROLE 1 1 1 th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS PA PA PA MDCH NF-NC 2 1 1 1 1 NF-NC NF-NC Y 1 1 1 69 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ REQUIP XL Y SINEMET, CR Y STALEVO *TASMAR ZELAPAR GENERIC NAME TIER ROPINIROLE LEVODAPA/ CARBIDOPA CARBIDOPA/ LEVODOPA/ ENTACAPONE TOLCAPONE SELEGILINE HMO POS TPA M-SUPP RDS MICHILD PPO PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY MAND 90 1 1 1 1 Y 2 3 3 2 NF-NC NF-NC Y MAND SPEC PARTNERS MAND SPEC ALZHEIMER'S DISEASE ARICEPT EXELON CAPSULES EXELON SOLN AND PATCH NAMENDA NAMENDA XR RAZADYNE ER Y DONEPEZIL 1 1 Y RIVASTIGMINE 1 1 Y RIVASTIGMINE MEMANTINE MEMANTINE GALANTAMINE 2 2 3 1 2 2 NF-NC 1 HORMONES ORAL ADRENAL CORTICOSTEROIDS ARISTOCORT CELESTONE CORTEF TABS CORTISONE MEDROL, DOSEPAK PEDIAPRED LIQUID PREDNISOLONE Y Y TRIAMCINOLONE BETAMETHASONE HYDROCORTISONE CORTISONE ACETATE 2 2 1 1 2 2 1 1 Y METHYLPREDNISOLONE 1 1 Y Y PREDNISOLONE PREDNISOLONE 1 1 1 1 Y ETHINYL ESTRADIOL 30MCG DESOGESTREL 0.15MG ORAL CONTRACEPTIVES, GF APRI th th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 1 1 Y 70 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ ARANELLE Y AVIANE Y BEYAZ CAMILA Y CRYSELLE Y DESOGEN Y ENPRESSE Y ERRIN Y ESTROSTEP FE Y FEMCON FE Y GENERESS FE GENERIC NAME ETHINYL ESTRADIOL NORETHINDRONE ETHINYL ESTRADIOL 20MCG LEVONORGESTREL 0.1MG DROSPIR/ETH ESTRA/LEVOMEF OL CA NORETHINDRONE 0.35MG ETHINYL ESTRADIOL 30MCG NORGESTREL 0.3MG ETHINYL ESTRADIOL 30MCG DESOGESTREL 0.15MG ETHINYL ESTRADIOL LEVONORGESTREL NORETHINDRONE 0.35MG NORETH A-ET ESTRA/FE FUMARATE NORETH-ETHINYL ESTRADIOL/IRON NORETH-ETHINYL ESTRADIOL/IRON JOLIVETTE Y KARIVA Y NORETHINDRONE 0.35MG ETHINYL ESTRADIOL DESOGESTREL Y ETHINYL ESTRADION 20MCG LEVONORGESTREL 0.1MG LESSINA th th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS HMO POS TPA M-SUPP RDS MICHILD SIGNATURE PPO CLOSED FORMULARY MAND 90 1 1 Y 1 1 Y NF-PA Y 1 1 Y 1 1 Y 1 1 Y 1 1 Y 1 1 Y 1 1 Y 1 1 Y NF-PA Y 1 1 Y 1 1 Y 1 1 Y TIER 3 3 PA PA PPO PA PA PARTNERS MEDICAID PA PA MAND SPEC PARTNERS MAND SPEC 71 FORMULARY DRUG PRODUCT NOTES BRAND NAME LEVORA LO/OVRAL LOESTRIN FE 1/20 LOESTRIN 21 1.5/30 LOESTRIN 21 1/20 GEQ TIER PPO PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY MAND 90 Y ETHINYL ESTRADIOL 30MCG LEVONORGESTREL 0.15MG 1 1 Y Y ETHINYL ESTRADIOL 30MCG NORGESTREL 0.3MG 1 1 Y Y ETHINYL ESTRADIOL 20MCG NORETHINDRONE 1MG 1 1 Y Y ETHINYL ESTRADIOL 30MCG NORETHINDRONE 1.5MG 1 1 Y 1 1 Y Y LOESTRIN 24 FE LO MINASTRIN FE LOSEASONIQUE Y LOW-OGESTREL Y LYBREL Y MICROGESTIN FE 1.5/30 Y th GENERIC NAME HMO POS TPA M-SUPP RDS MICHILD ETHINYL ESTRADIOL 20MCG NORETHINDRONE 1MG ETHINYL ESTRADIOL 20MCG NORETHINDRONE 1MG ETHINYL ESTRADIOL 10MCG NORETHINDRONE 1MG L-NORGEST-ETH ESTR/ETHIN ESTRA ETHINYL ESTRADIOL 30MCG NORGESTREL 0.3MG ETHINYL ESTRADIOL LEVONORGESTREL ETHINYL ESTRADIOL 30MCG NORETHINDRONE 1.5MG th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 3 PA PA PA NF-PA Y 3 PA PA PA NF-PA Y 1 1 Y 1 1 Y 1 1 Y 1 1 Y MAND SPEC PARTNERS MAND SPEC 72 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ HMO POS TPA M-SUPP RDS MICHILD SIGNATURE PPO CLOSED FORMULARY MAND 90 1 1 Y 1 1 Y 1 1 Y 1 1 Y NF-PA Y NATAZIA GENERIC NAME ETHINYL ESTRADIOL 20MCG/ FE/ NORETHINDRONE 1MG ETHINYL ESTRADIOL DESOGESTREL ETHINYL ESTRADIOL 35MG NORETHINDRONE 0.5MG ETHINYL ESTRADIOL 30MCG NORGESTIMATE 0.25MG ESTRADIOL VALERATE/DIENOGEST NECON 0.5/35 Y ETHINYL ESTRADIOL 35MG NORETHINDRONE 0.5MG 1 1 Y NECON 1/35 Y ETHINYL ESTRADIOL 35MG NORETHINDRONE 1MG 1 1 Y NECON 1/50 Y 1 1 Y NECON 10/11 Y 1 1 Y 1 1 Y 1 1 Y 1 1 Y MICROGESTIN FE 1/20 Y MIRCETTE Y MODICON Y MONONESSA Y NECON 7/7/7 Y NORA-BE Y NORDETTE Y th MESTRANOL 50MCG NORETHINDRONE 1MG ETHINYL ESTRADIOL NORETHINDRONE ETHINYL ESTRADIOL NORETHINDRONE NORETHINDRONE 0.35MG ETHINYL ESTRADIOL 30MCG LEVONORGESTREL 0.15MG th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS TIER PARTNERS MEDICAID 3 PA PPO PA PA MAND SPEC PARTNERS MAND SPEC 73 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ NORINYL 1/35 Y GENERIC NAME ETHINYL ESTRADIOL 35MG NORETHINDRONE 1MG Y MESTRANOL 50MCG NORETHINDRONE 1MG ETHINYL ESTRADIOL 35MG NORETHINDRONE 0.5MG NORTREL 1/35 Y ETHINYL ESTRADIOL 35MG NORETHINDRONE 1MG NORTREL 7/7/7 Y OGESTREL Y NORINYL 1+50 NORTREL 0.5/35 ORTHO MICRONOR ORTHO TRICYCLEN ORTHO TRICYCLEN LO ORTHO-CYCLEN ORTHO-NOVUM 1/35 ORTHO-NOVUM 1/50 ORTHO-NOVUM 7/7/7 th ETHINYL ESTRADIOL NORETHINDRONE ETHINYL ESTRADIOL 50MCG NORGESTREL 0.5MG Y NORETHINDRONE 0.35MG ETHINYL ESTRADIOL NORGESTIMATE ETHINYL ESTRADIOL NORGESTIMATE ETHINYL ESTRADIOL 30MCG NORGESTIMATE 0.25MG Y ETHINYL ESTRADIOL 35MG NORETHINDRONE 1MG Y Y Y Y MESTRANOL 50MCG NORETHINDRONE 1MG ETHINYL ESTRADIOL NORETHINDRONE th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS HMO POS TPA M-SUPP RDS MICHILD SIGNATURE PPO CLOSED FORMULARY MAND 90 1 Y NF-PA Y 1 1 Y 1 1 Y 1 1 Y 1 1 Y 1 1 Y 1 1 Y NF-PA Y 1 1 Y 1 1 Y 1 1 Y 1 1 Y TIER PPO PARTNERS MEDICAID 1 3 3 PA PA PA PA PA PA MAND SPEC PARTNERS MAND SPEC 74 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ ORTHO-CEPT Y OVCON 35 Y OVCON 50 PORTIA Y SAFYRAL SEASONALE Y SEASONIQUE Y SPRINTEC Y TRINESSA Y TRI-NORINYL Y TRI-SPRINTEC Y TRIVORA Y YASMIN Y th GENERIC NAME ETHINYL ESTRADIOL 30MCG DESOGESTREL 0.15MG ETHINYL ESTRADIOL 35MCG NORETHINDRONE 0.4MG ETHINYL ESTRADIOL 50MCG NORETHINDRONE 1MG ETHINYL ESTRADIOL 30MCG LEVONORGESTREL 0.15MG DROSPIR/ETHESTRA/L EVOMEFOL CA ETHINYL ESTRADIOL 30MCG LEVONORGESTREL 0.15MG L-NORGEST-ETH ESTR/ETHIN ESTRA ETHINYL ESTRADIOL 30MCG NORGESTIMATE 0.25MG ETHINYL ESTRADIOL NORGESTIMATE ETHINYL ESTRADIOL NORETHINDRONE ETHINYL ESTRADIOL NORGESTIMATE ETHINYL ESTRADIOL LEVONORGESTREL ETHINYL ESTRADIOL 30MCG DROSPIRENONE 3MG th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS HMO POS TPA M-SUPP RDS MICHILD SIGNATURE PPO CLOSED FORMULARY MAND 90 1 1 Y 1 1 Y NF-PA Y 1 Y NF-PA Y 1 1 Y 1 1 Y 1 1 Y 1 1 Y 1 1 Y 1 1 Y 1 1 Y 1 1 Y TIER 3 PA PPO PA PARTNERS MEDICAID PA 1 3 PA PA PA MAND SPEC PARTNERS MAND SPEC 75 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ YAZ Y ZOVIA 1/35 Y ZOVIA 1/50 Y GENERIC NAME ETHINYL ESTRADIOL 20MCG DROSPIRENONE 3MG ETHINYL ESTRADIOL 35MG ETHYNODIOL DIACETATE 1MG ETHINYL ESTRADIOL 50MCG ETHYNODIOL DIACETATE 1MG Y ETONOGESTREL ETHINYL ESTRADIOL ETHINYL ESTRADIOL NORELGESTROMIN Y ESTRADIOL, TRANSDERMAL CONJUGATED ESTROGENS ESTRADIOL, TRANSDERMAL HMO POS TPA M-SUPP RDS MICHILD SIGNATURE PPO CLOSED FORMULARY MAND 90 1 1 Y 1 1 Y 1 1 Y TIER PPO PARTNERS MEDICAID MAND SPEC PARTNERS MAND SPEC NON-ORAL CONTRACEPTIVES, GF NUVARING ORTHO EVRA PATCH ALORA CENESTIN CLIMARA DIVIGEL ENJUVIA ESTRACE TABS ESTRACE VAGINAL CREAM ESTRASORB ESTRING ESTROGEL GEL FEMRING MENEST Y OGEN Y th 3 PA 1 PA 2 AG 3 1 PA PA NF-PA PA 1 PA AG AG 2AG Y AG AG PA, AG NF-NC Y AG AG AG 1 AG Y PA ESTROGENS, GF NF-NC ESTRADIOL CONJUGATED ESTROGENS 3 3 AG AG PA, AG NF-NC Y ESTRADIOL 1 AG AG AG 1 AG Y ESTRADIOL ESTRADIOL ESTRADIOL ESTRADIOL ESTRADIOL ESTROGENS 2 3 3 3 3 3 AG AG AG 2 NF-NC NF-NC NF-NC NF-NC NF-NC 1 AG AG AG 1 AG ESTROPIPATE th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS Y Y Y Y Y 76 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ PREMARIN ORAL PREMARIN VAG CREAM VAGIFEM VIVELLE-DOT GENERIC NAME CONJUGATED ESTROGENS CONJUGATED ESTROGENS ESTRADIOL ESTRADIOL, TRANSDERMAL TIER HMO POS TPA M-SUPP RDS MICHILD 2 AG PPO PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY MAND 90 AG PA, AG 2 AG Y 2 NF-NC Y Y 2 AG Y 1 1 Y Y 1 Y 1AG Y 1 AG Y 3 NF-NC Y 3 NF-NC Y 2 AG Y 1 1 Y 3 NF-NC Y 2 3 2 AYGESTIN PROMETRIUM Y Y NORETHINDRONE ACETATE PROGESTERONE 1 1 PROVERA Y MEDROXYPROGESTERONE/ MPA 1 AG AG PROGESTINS AG MAND SPEC PARTNERS MAND SPEC COMBINATION ESTROGEN/ANDROGEN ESTRATEST ACTIVELLA Y ESTERIFIED ESTROGENS/ METHYLTESTOSTERO NE 1 Y ESTRADIOL/ NORETHINDRONE ACETATE 1 ANGELIQ CLIMARA PRO COMBIPATCH FEMHRT 1MG5MCG FEMHRT 0.5MG2.5MCG th Y ESTRADIOL/ DROSPIRENONE ESTRADIOL/ LEVONORGESTREL ESTRADIOL/ NORETHINDRONE ACETATE ETHINYL ESTRADIOL/ NORETHINDRONE ACETATE ETHINYL ESTRADIOL/ NORETHINDRONE ACETATE th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 2 AG AG AG COMBINATION ESTROGEN/PROGESTINS AG AG AG AG AG AG 77 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ PREFEST PREMPHASE PREMPRO DDAVP NASAL SPRAY DDAVP RHINAL TUBE Y Y GENERIC NAME ESTRADIOL/ NORGESTIMATE CONJUGATED ESTROGEN/ MPA CONJUGATED ESTROGEN/ MPA TIER HMO POS TPA M-SUPP RDS MICHILD SIGNATURE PPO CLOSED FORMULARY MAND 90 NF-NC Y PA, AG 2 Y AG AG PA, AG DDAVP-DESMOPRESSIN ACETATE 2 Y PPO PARTNERS MEDICAID 3 2 2 DESMOPRESSIN ACETATE DESMOPRESSIN ACETATE AG AG 1 MAND SPEC PARTNERS MAND SPEC 1 1 1 ANDROGENS, GM ANDRODERM PA PA NF-NC Y 2 2 Y 2 2 Y NF-NC Y 1 Y PA NF-NC 1 Y Y PA NF-NC Y 1 Y PA NF-NC Y 3 *ANDROID TESTOSTERONE TESTOSTERONE, TRANSDERMAL METHYLTESTOSTERONE AXIRON TESTOSTERONE 3 TESTOSTERONE METHYLTESTOSTERONE OXANDROLONE 1 3 1 PA PA TESTOSTERONE 3 PA PA 1 *TESTRED TESTOSTERONE METHYLTESTOSTERONE *BRAVELLE ANDROGEL FORTESTA Y METHITEST OXANDRIN Y STRIANT TESTIM *CETROTIDE *CLOMID th Y Y PA PA PA 3 PA UROFOLLITROPIN (FSH) 3 PA PA NC NC Y CETRORELIX ACETATE CLOMIPHENE 3 1 PA PA PA PA NC NC NC NC Y Y th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS PA INFERTILITY PA 78 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ *FOLLISTIM AQ *GONAL-F *LUPRON DEPOT 3.75 KIT GENERIC NAME FOLLITROPIN BETA,RECOMB FOLLITROPIN ALPHA,RECOMB LEUPROLIDE ACETATE GONADOTROPIN, CHORIONIC,HUMAN HCG ALPHA,RECOMBINANT GONADOTROPIN, CHORIONIC,HUMAN MENOTROPINS *NOVAREL *OVIDREL *PREGNYL *REPRONEX *LUPANETA PACK *LUPRON DEPOT 3.75 KIT SYNAREL NASAL SPRAY TIER HMO POS TPA M-SUPP RDS MICHILD 3 PPO PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY PA PA NC NC Y 3 PA PA NC NC Y 3 PA PA NC NC Y 3 PA PA NC NC Y 3 PA PA NC NC Y 3 3 PA PA NC NC NC NC Y Y LEUPROLIDE/ NORETHINDRONE 3 LEUPROLIDE ACETATE 3 NAFARELIN ACETATE 3 PA PA ENDOMETRIOSIS MAND 90 MAND SPEC PARTNERS MAND SPEC NF-NC PA 4 SPEC Y NF-NC OSTEOPOROSIS SELECTIVE ESTROGEN RECEPTOR MODULATOR DUAVEE EVISTA Y CONJUGATED ESTROGENSBAZEDOXIFENE RALOXIFENE 3 1 PA NF-NC 1 Y PA 1 Y NF-NC NF-NC 1 1 NF-NC NF-NC Y Y Y Y BISPHOSPHONATES ACTONEL ATELVIA BINOSTO BONIVA DIDRONEL *FORTEO FORTICAL th Y Y Y RISEDRONATE RISEDRONATE SODIUM ALENDRONATE IBANDRONATE ETIDRONATE TERIPARATIDE CALCITONIN 1 3 3 1 1 3 3 th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS PA Y Y Y 79 FORMULARY DRUG PRODUCT NOTES BRAND NAME HMO POS TPA M-SUPP RDS MICHILD PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY GEQ GENERIC NAME TIER FOSAMAX Y 1 1 MAND 90 Y FOSAMAX PLUS D MIACALCIN NASAL Y ALENDRONATE ALENDRONATE/ VITAMIN D3 CALCITONIN 3 1 NF-NC 1 Y Y 1 AG Y 1 1 Y 1 1 Y 1 1 1 1 Y Y 1 1 Y 1 1 2 1 1 2 Y Y Y PPO MAND SPEC PARTNERS MAND SPEC THYROID DISORDERS THYROID, DESSICATED LIOTHYRONINE SODIUM ARMOUR THYROID Y CYTOMEL Y LEVOTHROID Y LEVOXYL METHIMAZOLE PROPYLTHIOURACIL Y Y LEVOTHYROXINE SODIUM LEVOTHYROXINE SODIUM METHIMAZOLE Y PROPYLTHIOURACIL SYNTHROID TAPAZOLE THYROLAR TIROSINT ZEMPLAR Y Y Y 1 LEVOTHYROXINE SODIUM METHIMAZOLE LIOTRIX LEVOTHYROXINE SODIUM PARICALCITOL AG AG AG PA NF-NC 3 1 1 DIABETES INSULINS APIDRA APIDRA SOLOSTAR HUMALOG HUMALOG MIX HUMULIN INSULINS LANTUS th INSULIN GLULISINE 3 PA PA PA NF-NC INSULIN GLULISINE INSULIN LISPRO INSULIN 3 2 2 PA PA PA NF-NC 2 2 Y INSULIN INSULIN GLARGINE 2 2 2 2 Y Y th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 80 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ LANTUS SOLOSTAR LEVEMIR LEVEMIR FLEXPEN LEVEMIR FLEXTOUCH NOVOLIN INSULINS NOVOLOG INSULINS NOVOLOG MIX INSULIN SYRINGES Y GENERIC NAME TIER HMO POS TPA M-SUPP RDS MICHILD PPO PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY MAND 90 INSULIN GLARGINE INSULIN DETEMIR INSULIN DETEMIR 2 2 2 2 2 2 Y Y Y INSULIN DETEMIR 2 2 Y INSULIN 3 PA PA NF-NC Y INSULIN ASPART INSULIN 3 3 PA PA PA PA NEEDLES/SYRINGES PA PA NF-NC NF-NC Y SYRINGES 1 1 Y 1 1 AG 1 Y Y Y 1 AG 1 AG Y Y 1 AG Y NF-NC 1 1 Y Y PA MAND SPEC PARTNERS MAND SPEC Y Y SULFONYLUREAS AMARYL DIABETA GLUCOTROL, XL GLYNASE PRESTAB MICRONASE Y Y Y GLIMEPIRIDE GLYBURIDE GLIPIZIDE 1 1 1 Y Y GLYBURIDE GLYBURIDE 1 1 DIABINESE Y CHLORPROPAMIDE 1 FARXIGA FORTAMET GLUCOPHAGE, XR GLUCOVANCE GLUMETZA INVOKANA Y Y Y AG AG AG AG AG AG AG AG ORAL ANTIHYPERGLYCEMICS AG AG AG DAPAGLIFLOZIN METFORMIN METFORMIN 3 1 1 GLYBURIDE/ METFORMIN METFORMIN 1 3 AG PA AG AG PA 1 AG NF-NC 2 DO DO DO 2 DO INVOKAMET CANAGLIFLOZIN CANAGLIFLOZIN/ METFORMIN *KORLYM MIFEPRISTONE th AG th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 2 2 3 NF-NC Y 81 FORMULARY DRUG PRODUCT NOTES BRAND NAME PRANDIMET PRANDIN STARLIX GEQ Y Y GENERIC NAME TIER REPAGLINIDE/ METFORMIN REPAGLINIDE NATEGLINIDE HMO POS TPA M-SUPP RDS MICHILD PPO PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY NF-NC 3 1 1 MAND 90 1 1 Y Y Y MAND SPEC PARTNERS MAND SPEC DPP-4 INHIBITORS SITAGLIPTIN / METFORMIN JANUMET, XR JANUVIA JENTADUETO 3 PA PA PA NF-NC Y SITAGLIPTIN LINAGLIPTIN/ METFORMIN ALOGLIPTIN/ METFORMIN SAXAGLIPTIN/ METFORMIN ALOGLIPTIN/ BENZOATE 3 PA, DO PA, DO PA, DO NF-NC Y 2 Y SAXAGLIPTIN ALOGLIPTIN/ PIOGLITAZONE LINAGLIPTIN 2 3 PA PA PA NF-NC Y 3 PA PA PA NF-NC Y 3 PA, DO PA, DO PA, DO NF-NC Y 3 PA, DO PA, DO PA, DO NF-NC Y PA DO NF-NC 2 DO Y Y 1 1 Y 3 NF-NC Y 1 1 Y 3 NF-NC Y AVANDARYL PIOGLITAZONE ROSIGLITAZONE/ METFORMIN ROSIGLITAZONE/ GLIMEPIRIDE 3 NF-NC Y AVANDIA ROSIGLITAZONE 3 NF-NC Y PIOGLITAZONE/ GLIMEPIRIDE 1 1 Y KAZANO KOMBIGLYZE XR NESINA ONGLYZA OSENI TRADJENTA ACTOPLUS MET ACTOPLUS MET XR Y ACTOS Y AVANDAMET DUETACT th Y 3 2 PIOGLITAZONE/ METFORMIN PIOGLITAZONE/ METFORMIN th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS PA PA DO DO THIAZOLIDINEDIONES 82 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ GENERIC NAME TIER HMO POS TPA M-SUPP RDS MICHILD PPO MISCELLANEOUS PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY MAND 90 BYDUREON EXENATIDE EXT. REL. 2 2 BYDUREON PEN EXENATIDE EXT. REL. 2 2 BYETTA FREESTYLE LITE/INSULINX, PRECISION XTRA GLUCOSE TEST STRIPS (no copay at a pharmacy) ALL OTHER TEST STRIPS (covered at DME only with a copay as applicable) GLYSET LANCETS PRECOSE EXENATIDE 2 2 TEST STRIPS 0 DO DO DO 0 DO Y TEST STRIPS MIGLITOL LANCETS ACARBOSE DME NF-NC NF-NC NF-NC 3 2 1 NF-NC NF-NC 2 1 Y Y Y 2 2 2 3 2 2 NF-NC 2 Y SYMLINPEN TANZEUM VICTOZA PRAMLINTIDE ACETATE PRAMLINTIDE ACETATE ALBIGLUTIDE LIRAGLUTIDE GLUCAGON GLUCAGON SYMLIN MAND SPEC PARTNERS MAND SPEC GLUCAGON 2 2 ANTI-GOUT DRUGS COLCRYS INDOCIN SUSP INDOMETHACIN PROBENECID ULORIC ZYLOPRIM th Y Y Y COLCHICINE 0.6MG INDOMETHACIN INDOMETHACIN PROBENECID FEBUXOSTAT ALLOPURINOL th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 2 3 1 1 2 1 AG AG AG AG AG AG DO, PA DO, PA DO, PA 2 2 AG 1 AG 1 NF-NC 1 Y Y 83 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ GENERIC NAME TIER HMO POS TPA M-SUPP RDS MICHILD PPO SUPPLEMENTS PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY MAND 90 MAND SPEC PARTNERS MAND SPEC ANTI-ANEMIA DRUGS FOLIC ACID Y FOLIC ACID 1 1 PRENATAL VITAMINS ATABEX EC BAL-CARE DHA ESSENTIAL VITAMINS, PRENATAL 3 PA NF-NC VITAMINS, PRENATAL 3 PA NF-NC B-NEXA CITRANATAL ASSURE CITRANATAL BCALM CITRANATAL HARMONY COMPLETE-RF PRENATAL VITAMINS, PRENATAL 3 PA NF-NC VITAMINS, PRENATAL 3 PA NF-NC VITAMINS, PRENATAL 3 PA NF-NC VITMAINS, PRENATAL 3 PA NF-NC VITAMINS, PRENATAL 3 PA NF-NC CONCEPT OB, DHA DUET DHA BALANCED VITAMINS, PRENATAL 3 PA NF-NC VITAMINS, PRENATAL 3 PA NF-NC GESTICARE DHA HEMENATAL OB MIS + DHA HEMOCYTE-F TABLET NATALVIT NATELLE ONE NESTABS NESTABS DHA NEXA SELECT OB COMPLETE, PREMIER, ONE, 400, DHA VITAMINS, PRENATAL 3 PA NF-NC VITAMINS, PRENATAL VITAMINS, PRENATAL PREP VITAMINS, PRENATAL VITAMINS, PRENATAL VITAMINS, PRENATAL VITAMINS, PRENATAL VITAMINS, PRENATAL 3 PA NF-NC 1 3 3 3 3 3 PA PA PA PA PA 1 NF-NC NF-NC NF-NC NF-NC NF-NC VITAMINS, PRENATAL 3 PA NF-NC th Y th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 84 FORMULARY DRUG PRODUCT NOTES BRAND NAME OBSTETRIX EC PREFERA OB PREFERA-OB ONE PREFERA-OB PLUS DHA GEQ Y GENERIC NAME TIER HMO POS TPA M-SUPP RDS MICHILD PPO PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY VITAMINS, PRENATAL VITAMINS, PRENATAL VITAMINS, PRENATAL 1 3 3 PA PA 1 NF-NC NF-NC VITAMINS, PRENATAL 3 PA NF-NC VITAMINS, PRENATAL 3 PA NF-NC VITAMINS, PRENATAL 3 PA NF-NC VITAMINS, PRENATAL 1 PRENATE ELITE, DHA, ESSENTIAL VITAMINS, PRENATAL 3 PA NF-NC PRENATE MINI VITAMINS, PRENATAL 3 PA NF-NC PRENEXA VITAMINS, PRENATAL 3 PA NF-NC PREQUE 10 SELECT-OB VITAMINS, PRENATAL VITAMINS, PRENATAL 3 3 PA PA NF-NC NF-NC SELECT-OB + DHA VITAMINS, PRENATAL 3 PA NF-NC PRENATA PRENATAL COMPLETE PRENATAL PLUS VITAFOL-OB Y Y VITAMINS, PRENATAL 1 VITAMINS, PRENATAL 3 PA NF-NC VITAFOL-PLUS VITAMINS, PRENATAL 3 PA NF-NC VITAMED MD ONE RX/QUATREFOLIC VITAMINS, PRENATAL 3 PA NF-NC VITAMINS, PRENATAL 3 PA NF-NC VITAMINS, PRENATAL 3 PA NF-NC VITAMINS, PRENATAL 3 PA NF-NC VIVA CT PRENATAL PARTNERS MAND SPEC 1 VITAFOL-ONE VITAMED MD PLUS VITAMED MD REDICHEW RX/QUATREFOLIC MAND 90 MAND SPEC 1 POTASSIUM KLOR-CON th Y POTASSIUM CHLORIDE th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 1 1 Y 85 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ K-PHOS ORIGINAL MICRO-K Y SSKI SOLUTION GENERIC NAME TIER HMO POS TPA M-SUPP RDS MICHILD PPO PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY POTASSIUM PHOSPHATE 2 2 POTASSIUM CHLORIDE 1 1 POTASSIUM IODIDE 2 MAND 90 MAND SPEC PARTNERS MAND SPEC Y 2 VITAMIN B CYANOCOBALAMIN/ME COBALAMIN NEURIN-SL 2 2 VITAMIN D ROCALTROL Y CALCITRIOL 1 1 VITAMINS WITH FLUORIDE FLUORABON DROPS SODIUM FLUORIDE 3 3 TOPICAL FLUORIDE PREVIDENT 5000 BOOSTER GEL PREVIDENT 5000 PLUS CREAM PREVIDENT DENTAL RINSE PREVIDENT GEL PREVIDENT 5000 SENSITIVE 1.1%5% Y SODIUM FLUORIDE 1 1 Y SODIUM FLUORIDE 1 1 Y Y SODIUM FLUORIDE SODIUM FLUORIDE 1 1 1 1 Y SODIUM FLUORIDE 1 1 VITAMIN K MEPHYTON PHYTONADIONE 2 2 MISCELLANEOUS AGENTS ALLERGENIC EXTRACTS GRASTEK ORALAIR th TIMOTHY GRASS POLLEN ALLERGEN EXTRACT MIXED POLLENS ALLERGEN EXTRACT th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 3 PA, QL PA, QL PA, QL NF-NC 3 PA, QL PA, QL PA, QL NF-NC 86 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ TIER HMO POS TPA M-SUPP RDS MICHILD 3 PA, QL PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY PA, QL NF-NC RAGWITEK GENERIC NAME SHORT RAGWEED POLLEN ALLERGEN EXTRACT AUVI-Q EPIPEN EPINEPHRINE EPINEPHRINE 3 2 CUPRIMINE PENICILLAMINE DEFEROXAMINE MESYLATE 3 NF-NC 1 1 DEFERASIROX 2 PPO PA, QL ANAPHYLAXIS MAND 90 MAND SPEC PARTNERS MAND SPEC Y Y NF-NC 2 HEAVY METAL ANTAGONISTS DESFERAL Y *EXJADE 2 Y QUININE SULFATE QUININE SULFATE Y QUININE SULFATE 1 1 ALKALINIZING AGENTS UROCIT-K 5, 10MEQ Y UROCIT-K 15MEQ POTASSIUM CITRATE 1 1 POTASSIUM CITRATE 3 NF-NC AMINO ACID DERIVATIVES #CARNITOR Y LEVOCARNITINE 1 1 GALLSTONE SOLUBILIZERS ACTIGALL Y URSODIOL 1 1 SUBSTANCE ABUSE DETERRENTS ANTABUSE Y BUNAVAIL DISULFIRAM BUPRENORPHINE/ NALOXONE 1 2 METHADONE Y METHADONE 1 REVIA Y NALTREXONE 1 Y BUPRENORPHINE/ NALOXONE BUPRENORPHINE/ NALOXONE SUBOXONE SUBOXONE SL th th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS QL QL MDCH 1 MDCH 2 QL 1 MDCH 1 2 QL QL MDCH 2 QL 1 QL QL MDCH 1 QL 87 FORMULARY DRUG PRODUCT NOTES TIER HMO POS TPA M-SUPP RDS MICHILD 1 QL ZUBSOLV BUPRENORPHINE BUPRENORPHINE/ NALOXONE CAVERJECT ALPROSTADIL 3 CIALIS 10, 20mg TADALAFIL 2 CIALIS 2.5, 5MG TADALAFIL 2 EDEX ALPROSTADIL 3 LEVITRA VARDENAFIL 3 MUSE ALPROSTADIL 3 STAXYN VARDENAFIL 3 STENDRA AVANAFIL 3 VIAGRA SILDENAFIL 2 AZASAN AZATHIOPRINE 2 2 Y BRAND NAME SUBUTEX GEQ Y GENERIC NAME 3 PPO PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY QL MDCH 1 QL QL QL MDCH ERECTILE DYSFUNCTION (ED) AG, GM, PA, AG, GM, PA, QL QL NC AG, GM, PA, AG, GM, PA, QL QL NC PA, QL PA, QL AG, GM, PA, AG, GM, PA, QL QL AG, GM, PA, AG, GM, PA, QL QL AG, GM, PA, AG, GM, PA, QL QL AG, GM, PA, AG, GM, PA, QL QL AG, GM, PA, AG, GM, PA, QL QL AG, GM, PA, AG, GM, PA, QL QL IMMUNE SUPPRESSANTS MAND 90 NC NC NC NC NC NC NC NC NC NC NC NC NC NC NC NC Y MYCOPHENOLATE MOFETIL 1 1 Y GENGRAF IMURAN Y Y CYCLOSPORINE AZATHIOPRINE 1 1 1 1 Y Y th th PARTNERS MAND SPEC NF-NC CELLCEPT *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS MAND SPEC 88 FORMULARY DRUG PRODUCT NOTES BRAND NAME GEQ GENERIC NAME TIER HMO POS TPA M-SUPP RDS MICHILD PPO PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY MYFORTIC Y MYCOPHENOLATE 1 1 MAND 90 Y NEORAL *PROGRAF *RAPAMUNE SANDIMMUNE Y Y Y Y CYCLOSPORINE TACROLIMUS SIROLIMUS CYCLOSPORINE 1 1 1 1 1 1 1 1 Y Y Y Y ZORTRESS 0.25MG EVEROLIMUS 2 2 Y *ZORTRESS 0.5, 0.75MG EVEROLIMUS 2 2 Y MAND SPEC PARTNERS MAND SPEC Y Y Y Y RHEUMATOLOGIC MEDCATIONS *ACTEMRA SQ PA PA PA NF-NC TOCILIZUMAB 3 LEFLUNOMIDE 1 *CIMZIA CERTOLIZUMAB PEGOL 3 PA PA PA NF-NC Y Y *ENBREL *HUMIRA ETANERCEPT ADALIMUMAB 2 2 PA PA PA PA PA PA 4 SPEC PA 4 SPEC PA Y Y Y Y *#KINERET *ORENCIA SQ ANAKINRA ABATACEPT 3 3 PA PA PA PA PA PA NF-NC NF-NC Y Y Y Y *OTEZLA RAYOS APREMILAST PREDNISONE 3 3 PA PA PA PA PA PA NF-NC NF-NC Y Y RIDAURA *SIMPONI AURANOFIN GOLIMUMAB 2 3 PA PA PA 2 NF-NC Y Y NF-NC Y Y ARAVA Y *XELJANZ 1 SPEC, SPEC, PA PA SPEC, PA LOCAL ANESTHETICS TOFACITINIB 3 LIDOCAINE 1 1 LIDORX GEL LIDOCAINE 3 NF-NC PLIAGLIS LIDOCAINE/ TETRACAINE 3 NF-NC LIDODERM 5% PATCH th Y th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 89 FORMULARY DRUG PRODUCT NOTES BRAND NAME KAYEXALATE GEQ GENERIC NAME TIER Y SODIUM POLYSTYRENE SULFONATE 1 HMO POS TPA M-SUPP RDS PARTNERS MICHILD PPO MEDICAID POTASSIUM REMOVING RESINS SIGNATURE PPO CLOSED FORMULARY MAND 90 MAND SPEC PARTNERS MAND SPEC 1 UROLOGY AVODART CARDURA CARDURA XL Y DETROL Y DETROL LA DITROPAN XL Y Y DUTASTERIDE DOXAZOSIN DOXAZOSIN 2 1 3 PA JALYN TOLTERODINE TARTRATE TOLTERODINE TARTRATE OXYBUTYNIN PENTOSAN POLYSULFATE SOLIFENACIN SUCCINATE TAMSULOSIN OXYBUTYNIN CHLORIDE DUTASTERIDE/ TAMSULOSIN MYRBETRIQ OXYTROL PATCH PROSCAR PYRIDIUM RAPAFLO SANCTURA SANCTURA XR 3 3 1 1 3 1 1 PA, DO Y Y MIRABEGRON OXYBUTYNIN FINASTERIDE PHENAZOPYRIDINE SILODOSIN TROSPIUM CHLORIDE TROSPIUM CHLORIDE 2 1 DO Y FESOTERODINE FUMARATE BETHANECHOL ELMIRON ENABLEX FLOMAX Y GELNIQUE TOVIAZ URECHOLINE th Y Y PA 1 1 1 DO DO DO DO DO DO 2 3 1 DO DO 1 Y 1DO 1 DO Y Y DO NF-NC 1 PA NF-NC 2 th Y 2 3 *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 2 1 NF-NC Y Y 2 PA, DO PA,DO PA PA PA DO PA DO NF-NC NF-NC 1 1 NF-NC Y Y Y 1 1 Y Y Y 2 DO Y 1 90 FORMULARY DRUG PRODUCT NOTES BRAND NAME HMO POS TPA M-SUPP RDS MICHILD GEQ GENERIC NAME TIER Y 1 VESICARE ALFUZOSIN DARIFENACIN HYDROBROMIDE 2 DO BRISDELLE PAROXETINE 3 PA OSPHENA OSPEMIFENE 3 UROXATRAL PPO SIGNATURE PPO CLOSED FORMULARY MAND 90 1 Y DO 2 DO Y MDCH NF-NC PARTNERS MEDICAID DO WOMEN’S HEALTH PA MAND SPEC PARTNERS MAND SPEC 1 Y Y NF-NC OXYTOCICS METHERGINE Y METHYLERGONOVINE 1 1 HEPATITIS C PRODUCTS *COPEGUS Y RIBAVIRIN 1 *HARVONI LEDIPASVIR/SOFOSBU VIR 3 PA, QL, DO PA, QL. DO NC 4 SPEC PA, QL, DO Y Y *PEGASYS, PROCLICK PEGINTERFERON ALFA-2A 2 PA PA PA 4 SPEC PA Y Y *OLYSIO SIMEPREVIR PEGINTERFERON ALFA-2B 3 PA, QL PA, QL PA, QL NF-NC Y Y 3 PA PA PA NF-NC Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y *PEG-INTRON REBETOL ORAL SOLUTION *REBETOL *RIBAPAK RIBASPHERE *RIBATAB *SOVALDI *VICTRELIS VIRAZOLE Y Y Y Y NF-NC 3 1 1 PA PA PA 1 PA 1 1 1 PA PA PA 1 PA 1 PA, QL PA, QL NC 4 SPEC PA, QL 2 PA, QL PA, QL PA, QL 4 SPEC PA, QL 2 NF-NC 3 IRRITABLE BOWEL SYNDROME/CHRONIC CONSTIPATION RIBAVIRIN RIBAVIRIN RIBAVIRIN RIBAVIRIN RIBAVIRIN SOFOSBUVIR BOCEPREVIR RIBAVIRIN AMITIZA LUBIPROSTONE 2 LINZESS LOTRONEX LINACLOTIDE ALOSETRON 3 2 th th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS PA 2 NF-NC NF-NC 91 FORMULARY DRUG PRODUCT NOTES BRAND NAME CYMBALTA LYRICA SAVELLA GEQ Y GENERIC NAME TIER HMO POS TPA M-SUPP RDS MICHILD PPO FIBROMYALGIA PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY MAND SPEC PARTNERS MAND SPEC MDCH MDCH PA 1 2 NF-NC MDCH NF-NC NF-NC Y Y Y Y PA PA NF-NC 1 PA Y Y Y Y Y Y Y Y MAND 90 DULOXETINE PREGABALIN MILNACIPRAN 1 2 3 BETHKIS *#KALYDECO TOBRAMYCIN IVACAFTOR 3 3 *TOBI PODHALER *TOBI SOLUTION TOBRAMYCIN TOBRAMYCIN 3 1 *AMPYRA *AUBAGIO *AVONEX *BETASERON DALFAMPRIDINE TERIFLUNOMIDE INTERFERON BETA-1A INTERFERON BETA-1B 3 3 2 3 PA, SP PA PA PA PA, SP PA PA PA PA, SP PA PA PA NF-NC NF-NC 4 SPEC PA NF-NC Y Y Y Y *COPAXONE GLATIRAMER ACETATE 2 PA PA PA 4 SPEC PA Y Y *EXTAVIA INTERFERON BETA-1B 3 PA PA PA NF-NC Y Y *GILENYA 3 PA, DO PA, DO PA, DO NF-NC Y Y 3 PA PA PA NF-NC *REBIF *TECFIDERA FINGOLIMOD PEGINTERFERON BETA-1A INTERFERON BETA1A/ALBUMIN DIMETHYL FUMERATE Y Y Y Y GRALISE GABAPENTIN 3 PA PA PA NF-NC HORIZANT GABAPENTIN ENACARBIL 3 PA, DO PA, DO PA, DO NF-NC NUEDEXTA *XENAZINE DEXTROMETHORPHAN/QUINIDINE TETRABENAZINE 3 3 Y Y *FOSRENOL LANTHANUM CARBONATE 2 *PLEGRIDY th Y th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 2 3 QL PA PA CYSTIC FIBROSIS PA PA PA PA PA PA MULTIPLE SCLEROSIS PA PA PA PA PA PA NEUROLOGICAL MISCELLANEOUS PA PA PA PA PA PA ELECTROLYTES & MISCELLANEOUS NUTRIENTS 4 SPEC PA NF-NC NF-NC NF-NC 2 92 FORMULARY DRUG PRODUCT NOTES BRAND NAME PHOSLO *RENAGEL GEQ Y GENERIC NAME TIER HMO POS TPA M-SUPP RDS MICHILD PPO PARTNERS MEDICAID SIGNATURE PPO CLOSED FORMULARY MAND SPEC PARTNERS MAND SPEC Y Y 2 2 Y Y Y Y Y Y Y Y 2 Y Y Y Y Y Y Y Y Y Y Y Y Y Y CALCIUM ACETATE SEVELAMER 1 2 1 2 RENVELA SEVELAMER CARBONATE 2 2 *SAMSCA TOLVAPTAN 3 *SENSIPAR CINACALCET 3 *VELPHORO *#COMETRIQ DROXIA *#ICLUSIG *JAKAFI *#XALKORI *XTANDI *#ZELBORAF PA, QL PA, QL PA, QL NF-NC NF-NC SUCROFERRIC NF-NC OXYHYDROXIDE 3 ONCOLOGY-ONCOLOGY DRUGS ARE ON FORMULARY UNLESS LISTED OTHERWISE CABOZANTINIB 2 2 HYDROXYUREA 2 2 PONATINIB 2 2 PA PA PA NF-NC RUXOLITINIB 3 CRIZOTINIB ENZALUTAMIDE 2 2 VEMURAFENIB 2 MAND 90 GROWTH HORMONES PA PA PA NF-NC 3 PA PA PA NF-NC 3 PA PA PA NF-NC 3 PA PA PA 4 SPEC PA 2 PA PA PA NF-NC 3 PA PA PA NF-NC 3 HIV – ALL HIV SELF-ADMINISTERED DRUGS ARE ON FORMULARY *EGRIFTA *GENOTROPIN *HUMATROPE *NORDITROPIN *NUTROPIN *OMNITROPE SOMATROPIN SOMATROPIN SOMATROPIN SOMATROPIN SOMATROPIN SOMATROPIN *APTIVUS TIPRANAVIR 2 PA PA MDCH 2 PA *COMPLERA EMTRICITABINE/RILPIV IRINE/TENOFOVIR 2 PA PA MDCH 2 PA 2 PA PA MDCH 2 PA 2 PA PA MDCH 2 PA *EDURANT *EPZICOM th RILPIVIRINE ABACAVIR SULFATE/LAMIVUDINE th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 93 FORMULARY DRUG PRODUCT NOTES *#FUZEON ENFUVIRTIDE 2 HMO POS TPA M-SUPP RDS MICHILD PA INVIRASE 200MG SAQUINAVIR 2 PA PA MDCH 2 PA *INVIRASE 500MG SAQUINAVIR 2 PA PA MDCH 2 PA *PREZISTA *SELZENTRY DARUNAVIR MARAVIROC ABACAVIR DOLUTEGRAVIR/ LAMIVUDI ABACAVIR SULFATE/LAMIVUDINE/ ZIDOVUDINE 2 2 PA PA PA PA MDCH MDCH 2 PA 2 PA 2 PA PA MDCH 2 PA 1 PA PA MDCH 2 PA 2 DO DO MDCH 2 DO BRAND NAME GEQ *TRIUMEQ *TRIZIVIR Y TIER EMTRICITABINE/TENOF OVIR DISOPROXIL FUMARATE #TRUVADA *ZIAGEN GENERIC NAME Y ABACAVIR PPO PA PARTNERS MEDICAID PA SIGNATURE PPO CLOSED FORMULARY 2 PA TOCILIZUMAB M PA PA PA M-NC PA BOTOX, DYSPORT, XEOMIN BOTULISM TOXIN TYPE A M PA PA PA M-NC PA ENTYVIO IMMUNE GLOBULIN VEDOLIZUMAB M PA PA PA M-NC PA IVIG M PA PA PA M-NC PA ORENCIA IV ABATACEPT M PA PA PA M-NC PA REMICADE RITUXAN INFLIXIMAB RITUXIMAB M M PA PA PA PA PA PA M-NC PA M-NC PA SYNAGIS PALIVIZUMAB TESTOSTERONE PELLET NATALIZUMAB M PA PA PA M-NC PA M M PA PA PA PA PA PA M-NC PA M-NC PA th PARTNERS MAND SPEC PA PA MDCH 2 PA 1 MEDICAL PRIOR AUTHORIZATION DRUGS WITH A MEDICAL BENEFIT COPAY ACTEMRA IV TESTOPEL TYSABRI MAND 90 MAND SPEC th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS 94 FORMULARY DRUG PRODUCT NOTES BRAND NAME HMO POS TPA SIGNATURE M-SUPP RDS PARTNERS PPO CLOSED GEQ GENERIC NAME TIER MICHILD PPO MEDICAID FORMULARY MAND 90 PREVENTATIVE MEDICATION FOR HEALTH CARE REFORM COVERED AT A ZERO COPAY WITH PRESCRIPTION ARIMIDEX Y ANASTROZOLE 0 NA AROMASIN Y EXEMESTANTE 0 NA VARENICLINE TARTRATE 0 CHANTIX DRISDOL CAPSULE (AGES 66 AND OLDER) Y ERGOCALCIFEROL (VITAMIN D2) 0 NA EVISTA Y RALOXIFENE 0 PA TOREMIFENE 0 NA FARESTON FEMARA Y LETROZOLE 0 NA FOLIC ACID (FEMALE ONLY) Y FOLIC ACID 0 NA IRON SUPPLEMENTS (AGES 6 MONTHS TO 1 YEAR) Y IRON SUPPLEMENTS 0 NA NICOTROL INHALER NICOTINE INHALER 0 NICOTROL NS NICOTINE NASAL SPRAY 0 FLUORIDE 0 ORAL FLUORIDE (AGES 6 MONTHS TO 6 YEARS) th Y th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS MAND SPEC PARTNERS MAND SPEC NA 95 FORMULARY DRUG PRODUCT NOTES TIER PARTNERS MEDICAID BRAND NAME GEQ OTC ASPIRIN (AGES 45-79 YEARS) Y ASPIRIN 0 OTC NICORETTE GUM Y NICOTINE POLACRILEX 0 OTC NICOTINE LOZENGE Y NICOTINE POLACRILEX 0 NICOTINE PATCHES Y NICOTINE PATCH OTC 0 TAMOXIFEN 0 NA NA SOLTAMOX GENERIC NAME HMO POS TPA M-SUPP RDS MICHILD TAMOXIFEN Y TAMOXIFEN 0 ZYBAN Y BUPROPION 0 th th *A 4 tier copay applies for plans that have a 4 tier. #This drug is carved out to MDCH for MIChild CSHCS PPO SIGNATURE PPO CLOSED FORMULARY MAND 90 MAND SPEC PARTNERS MAND SPEC NA 96 PHARMACOLOGIC STEP PROTOCOL FOR TYPE 2 DIABETES MELLITUS Initial Therapy Metformin (Titrate dose to improve tolerability and reduce diarrhea) Consider insulin if: † CI to Metformin Elevated SCr (1.5 < SCrmen) (1.4 < SCrwomen) Insulin therapy: Start basal insulin to consistently reach fasting blood glucose <180, then start post-prandial insulin. †Sulfonylureas are an oral alternative for patients CI to metformin. A1c not at goal (7% or 8%) Add Insulin If A1c is: 4 >7.5% and goal is 7% OR >8.5% and goal is 8% OR Target A1c is < 8% for patients meeting any of the criteria below: - Age over 65 - CABG or CHF Ischemic Vascular Disease - CKD or ESRD Percutaneous Coronary Intervention Thoracic Aortic Aneurysm -Blindness or amputation Oral alternatives to sulfonylurea for patients with hypoglycemia risk or weight gain concern - Thiazolidinedione (Actos, Actoplus MET, Duetact) - DPP-4 inhibitor (Tradjenta, Jentadueto) Addition of Oral Agent Diabetes Standards of Care for All Patients Action A1c A1c not at goal, and patient tolerating current therapy Addition of Third Agent ** (Not cost effective) 3 Post-prandial blood glucose Eye exam Frequency Every 3-months (6-month if A1c at goal) Every office visit: Request home readings Every office visit: Request home readings Every year No retinopathy Foot exam Every year No neuropathy Urine albumin and SCr Every year No nephropathy Adherence counseling Every office visit No intolerance to current therapy Fasting blood glucose Intensify Insulin Therapy If A1c is: 4 >7.5% and goal is 7% OR >8.5% and goal is 8% Goal < 7 or 8% 70-130 < 180 Hypoglycemia management (Specifically for elderly patients currently on insulin or a sulfonylurea) Hypoglycemia defined as blood glucose < 70, can occur at higher levels for patients with chronic elevated blood glucose. For new patients, patient education should include identification of hypoglycemia (dizziness, jitteriness, fast heart-beat, sweating, and hunger), and management. Patients can manage hypoglycemia by taking glucose tablets or using glucagon. FORMULARY ANTIDIABETIC AGENTS Sulfonylureas Biguanides Insulin Amaryl* (glimepiride) Diabinese* (chlorpropamide) Glucotrol*/Glucotrol XL* (glipizide) Glynase* (glyburide) Micronase* (glyburide) Glucophage* (metformin) Glucophage XR*, Fortamet* (metformin ER) Humulin or Humalog (Regular) Humalog (lispro) Lantus (insulin glargine) Levemir (insulin detemir) Alpha-Glucosidase Inhibitors Tradjenta (linagliptin) Misc Precose* (acarbose) Combination Products GLP-1 Receptor Agonists Actoplus MET* (pioglitazone/metformin) Duetact* (pioglitazone/glimepiride) Glucovance* (glyburide/metformin) Jentadueto (linagliptin/metformin) Symlin (pramlintide) Starlix* (nateglinide) Prandin* (repaglinide) Byetta (exenatide) Bydureon (exenatide once-weekly) Victoza (liraglutide) Thiazolidinediones Actos* (pioglitazone) DPP 4 inhibitors *available in generic References: 1. 2. 3. 4. Swinnen SG, Hoekstra JB, Devries JH. Insulin therapy for type 2 diabetes. Diabetes Care. 2009;32 Suppl 2:S253-9. American Diabetes Association. Standards of medical care in diabetes. Diabetes Care, January 2014. vol. 37, Supplement 1. Levin PA, Wei W, Zhou S, Xie L, Baser O. Outcomes and treatment patterns of adding a third agent to 2 OADs in patients with type 2 diabetes. J Manag Care Pharm. 2014;20(5):501-12. National Institute for Health and Care Excellence (NICE), Diabetes, last updated June 2014, accessed July 2014 Revised date: 7/2014 97 HYPERTENSION STEP PROTOCOL PHARMACOLOGIC THERAPY Adults ≥18 y with hypertension LIFESTYLE MODIFICATIONS Set BP goals and initiate medication INITIAL DRUG CHOICES General Population (no diabetes or CKD) Diabetes or CKD present All Ages Diabetes No CKD Age ≥ 60 y Age <60 y BP Goal <150/90 mmHg BP Goal <140/90 mmHg Non-Black Thiazide, ACE, ARB or CCB, alone or in combo All Ages CKD Diabetes/No Diabetes BP Goal <140/90 mmHg Black Thiazide or CCB alone, or in combo BP Goal <140/90 mmHg All Races ACE or ARB alone, or in combo with another drug class BLOOD PRESSURE NOT AT GOAL (After 1 month of treatment) Optimize dosages or add additional drugs until goal blood pressure is achieved. Consider consultation with hypertension specialist. Diuretics Chlorthalidone* Demadex* Dyazide* Inspra* Lasix* Lozol* Maxzide* Zaroxolyn* Miscellaneous agents Aldomet* Catapres* Tenex Tekturna Beta-Blockers Bystolic Coreg* Corgard* Inderal LA* Kerlone* Lopressor* Normodyne* Sectral* Tenormin* Toprol XL* Trandate* Zebeta* Formulary Agents ACE-I CCBs Accupril* Adalat CC* Altace* CalanSR* Capoten* Cardene* Lotensin* Cardiazem* Mavik* Cardiazem CD/LA* Prinivil* Cartia XT* Univasc* Dilacor XR* Vasotec* Isoptin SR* Zestril* Nimotop* Norvasc* ARBs Procardia XL* Atacand* Sular* Atacand HCT* Verelan* Avapro* Benicar (HCT) Cozaar* Diovan* Micardis* Teveten* Combos Accuretic* Azor Avalide* Benicar HCT Diovan HCT* Exforge* Hyzaar* Lotrel* Lopressor HCT* Micardis HCT* Monopril HCT Prinzide* Tenoretic* Tribenzor Twynsta* Uniretic* Valturna Vaseretic* Zestoretic* Ziac* * Generic available References:James PA, Oparil S, Carter BL, et al. 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report From the Panel Members Appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014 Feb 5;311(5):507-20. Available at: http://jama.jamanetwork.com/article.aspx?articleid=1791497 Accessed July 18, 2014. Review Date: 7/2014 98 Pharmacologic Step Protocol for Heart Failure (HF) Pharmacologic Therapy Based on symptoms or ACC/AHA and NYHA classification Stage A At high risk for HF but without structural heart disease or symptoms of HF Patients with: - Hypertension - Atherosclerotic disease - Diabetes mellitus - Obesity - Metabolic syndrome - Family history of cardiomyopathy - Exposure of cardiotoxins Class I Stage B ∞ Structural heart disease but without signs or symptoms of HF Patients with: - Previous MI - LV remodeling including LVH and low ejection fraction - Asymptomatic valvular disease Patients with: - Known structural heart disease - Shortness of breath, fatigue, and reduced exercise tolerance Class IV Stage D Refractory HF requiring specialized interventions Patients who have marked symptoms at rest despite maximal medical therapy Goals - All goals under Stages A and B - Dietary salt restriction Goals All goals under Stage A Goals - Control hypertension - Encourage smoking cessation - Control lipid disorders - Encourage regular exercise - Discourage alcohol, illicit drugs - Control metabolic syndrome - Control blood sugar - Treat thyroid disorders Class II & III Stage C Structural heart disease with prior or current symptoms of HF Drugs - ACEI or ARB^ - Beta-Blockers Devices in Selected Patients - Implantable Defibrillators Drugs - ACEI or ARB^ Drugs - Diuretics for fluid retention - Use ACEI or ARB^ - Use Beta-Blockers Drugs in select patients - Aldosterone antagonist - ARB - Digitalis # - Hydralazine/Nitrates Devices in Selected Patients -Biventricular Pacing -Implantable Defibrillators Goals Appropriate measures under Stages A, B, and C Options - End-of-life care options/hospice - Extraordinary measures * Heart transplant * Chronic inotropes * Permanent mechanical support * Experimental surgery or drugs ∞ Patients at stage B or higher whose condition is worsening should be referred to a specialist ^Consider an Angiotensin II Receptor Blocker (e.g., Benicar, Cozaar*, Diovan*) for patients who are contraindicated or intolerant to an ACE Inhibitor. * Generic available # Digoxin has a narrow therapeutic range and the toxicity is affected by individual hydration/electrolytes status. Frequent renal function and digoxin monitoring is highly recommended. The use of digoxin at a 0.25 mg dose or higher should be avoided in the elderly and in patients with renal insufficiency. FORMULARY AGENTS Cardiovascular Medications Indicated for Treatment of Various Stages of HF ACE Inhibitors Stage B Stage C Capoten* (captopril) Post MI HF Vasotec* (enalapril) Asymptomatic LVSD HF Monopril* (fosinopril) HF Zestril* (lisinopril) Post MI HF Accupril* (quinapril) HF Altace* (ramipril) Post MI Post MI Mavik* (trandolapril) Post MI Post MI ARBs Cozaar* (losartan potassium) Benicar (olmesartan) Diovan* (valsartan) Post MI Post MI, HF Avapro* (irbesartan) Beta Blockers with mortality benefit Coreg* (carvedilol) Toprol XL* (metoprolol) Zebeta* (bisoprolol) Aldosterone Antagonists for HF Aldactone* (spironolactone) Inspra* (eplerenone) Common Diuretics for HF Lasix* (furosemide) Bumex* (bumatanide) Zaroxolyn* (metolazone) Microzide* (hydrochlorothiazide) Aldactone* (spironolactone) References: 2009 Focused Update American College of Cardiology/American Heart Association Guideline Update for the Diagnosis and Management of Chronic Heart Failure in Adults. Circulation 2009;119;1977-2016. Review Date: 7/2014 99 PHARMACOLOGIC STEP PROTOCOL FOR MIGRAINE Make or confirm migraine diagnosis (Consider co-morbid conditions and treat, e.g., HTN) Key migraine signs/symptoms: Symptoms not usually associated with migraine: Chronic, episodic headache Duration of 4 to 72 hours Pulsatile/throbbing pain Unilateral or bilateral location Aggravated by light and/or sound Nausea and/or vomiting Onset age 12-44 years First headache >50 years Abnormal headache pattern “Worst ever” experience Abrupt onset Pain progressively worsens over time Abnormal medical evaluation Abnormal neurological exam Assess frequency, severity, and disability Assess management needs and set individual goals; define action plan Self-care techniques (Non-pharmacologic management) Initiate pharmacologic management for abortive treatment based on STEP CARE for 4 MIDAS Questionnaire grade I (score 0-5) NSAIDs (First Line): (e.g., ibuprofen, naproxen, ketorolac, diclofenac) Simple Analgesics: (e.g., aspirin, Excedrin) Initiate pharmacologic management for abortive treatment based on STRATIFIED CARE for MIDAS 4 Questionnaire grades II-IV (score 6-21+) Mild Intensity, Low Disability (MIDAS Scale Grade II) NSAIDs (First Line): (e.g., ibuprofen, naproxen, ketorolac, diclofenac) Simple Analgesics: (e.g., aspirin, Excedrin,) No relief 2 hours later 2 Anti-migraine (triptan therapy) Stronger analgesics may be used if antimigraine therapy is contraindicated 1 Moderate to Severe Intensity/Disability (MIDAS Scale Grade III & IV) or Non-Responsive to NSAIDs Anti-migraine (triptan) 2 therapy Stronger analgesics may be used if anti-migraine therapy is contraindicated Considerations: I. Ergotamine products may be used in patients that respond poorly to NSAIDs and triptans (note: CYP3A4 inhibitor interaction possible). II. Avoid the long-term prescribing of opiates and barbiturates. 3 Initiate pharmacologic management for prophylactic treatment (low dose, titrate slow) Beta-Blocker (e.g., propranolol 40-240 mg/day or Timolol 5-30 mg/day) Calcium Channel Blocker (e.g., verapamil 120 mg/day) - modest effect Antidepressant (e.g., TCA, amitriptyline 10-150 mg/day, Doxepin 25-100mg QHS and Nortriptyline 10-150mg QHS) Anti-epileptic agent (Depakote 500-1250 mg/day or Depacon 500-1250 mg/day, Gabapentin 900-2400mg/day [titrate from 300mg], Topamax 50-200mg/day [titrate slowly from 15-25mg]) Principles of Treatment 1. Self-care techniques include avoidance of any aggravating factors associated with migraine (e.g., stress, environmental, dietary). 2. HealthPlus formulary anti-migraine agents include: Amerge, Imitrex, and Relpax. Quantities greater than 9 tablets of anti-migraine agents per month require prior authorization. Non-formulary triptans (Axert, Frova, , Zomig/ZMT, Treximet) require Prior Authorization. 3. Prophylactic treatment is used to reduce the frequency and severity of attacks. Consider using prophylactic treatment when patient has two or more severe migraines per month with the attacks producing disability for three or more days per month, use of abortive medication more than twice a week, failure of or contraindication to acute treatments, or presence of uncommon migraine conditions (eg. Prolonged aura, migrainous infarction, hemiplegic migraine). 4. The MIDAS Questionnaire assesses the impact a patient’s migraine has on their work and social life to aid in their treatment plan. It is available at: http://www.achenet.org/tools/migraine/index.asp References: AAFP/ACP-ASIM release guidelines on the management and prevention of migraines. Am Fam Physician, Mar 2003 Stratified Care vs. Step Care Strategies for Migraine, JAMA Nov 2000 Saper JR, Magee KR. Freedom From Headaches. First Fireside Edition. New York: Simon & Schuster, Inc; 1981 Comparison of Available Triptans, Pharmaceutical Letter/Prescriber’s Letter, 2009; 25(5); 250509 Diagnosis and Treatment of Headache. Institute for Clinical System Improvement. January 2011. NOTE: Behavioral health medications are carved out to the State for HealthPlus Partners Medicaid and to CMH for MIChild. Reviewed: 7/2014 100 HYPERLIPIDEMIA PHARMACOLOGIC TREATMENT RECOMMENDATIONS ASCVD Statin Benefit Groups Individuals over 21 years with Clinical Atherosclerotic Cardiovascular Disease (ASCVD) † Individuals with primary elevations of LDL ≥190 mg/dl Individuals 40-75 years of age with diabetes with LDL 70-189 mg/dl and without ASCVD Individuals without clinical ASCVD or diabetes who are 40 to 75 years of age with LDL 70-189 mg/dl o With 10-year ASCVD risk ≥7.5% o With 10-year ASCVD risk < 7.5% † ASCVD includes coronary heart disease (CHD), stroke and peripheral arterial disease If not receiving cholesterol lowering therapy, re-calculate estimated 10-y ASCVD risk every 4-6 y if age 40-75 without clinical ASCVD or diabetes with LDL 70-189 mg/dL. Age ≤75 High Intensity Statin Adults >21 Population not covered in guideline NYHA II-IV Heart Failure patients Maintenance hemodialysis Individuals under 40 years of age, without ASCVD and with low 10year ASCVD risk HIV, rheumatoid conditions, inflammatory disease or solid organ transplant Clinical ASCVD Age >75 OR not eligible for high intensity statin Moderate-intensity statin Yes High Intensity Statin Moderate Intensity Statin Only use non-statin if a statin is not tolerated 10-y ASCVD risk 5-7.5% and age 40-75 Statin intolerance? Yes High Intensity Statin if ASCVD risk ≥ 7.5% No 10-y ASCVD risk ≥7.5% and age 40-75 Reinforce adherence Follow-up 3-12 mo No Yes Estimate 10-y ASCVD Risk Combination of statin with nonstatin agents has not shown greater ASCVD risk reduction than statin alone, and thus generally not recommended. Anticipated therapeutic response? - 50% > LDL reduction in high intensity statin - 30-50% LDL reduction in moderate intensity statin Yes No Diabetes Age 40-75 Assess medication and lifestyle adherence Yes No LDL-C ≥ 190 mg/dL Initial considerations prior to statin initiation: -Fasting lipid panel -Creatinine kinase & ALT -Secondary causes of hyperlipidemia No Management of statin intolerance If therapeutic response is still suboptimal: Yes Moderate-to-High Intensity Statin Increase statin intensity OR Consider addition of non-statin drug Follow-up in 4-12 weeks Yes Moderate Intensity Statin High Intensity Statin Therapy Daily dose lowers LDL-C on average by approximately >50% Atorvastatin (40†)-80 mg* Rosuvastatin 20 (40) mg Moderate Intensity Statin Therapy Low Intensity Statin Therapy Daily dose lowers LDL-C on average by Daily dose lowers LDL-C on average by approximately 30% to <50% approximately <30% Atorvastatin 10 (20) mg* Simvastatin 10 mg * Rosuvastatin (5) 10 mg Pravastatin 10-20 mg* Simvastatin 20-40 mg‡* Fluvastatin 20-40 mg* Pravastatin 40 (80) mg* Fluvastatin 40 mg BID* *Generic available, †Evidence for Atorvastatin 80 mg is stronger than 40 mg, ‡Simvastatin 80 mg is not recommended Online ASCVD risk calculator and full guideline: http://my.americanheart.org/professional/StatementsGuidelines/Prevention-Guidelines_UCM_457698_SubHomePage.jsp Reference Stone NJ, Robinson J, Lichtenstein AH, et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013 Revised date 7/2014 101 CHRONIC PAIN MANAGEMENT PHARMACOLOGIC THERAPY INITIAL ASSESSMENT OF PAIN 1) 2) 3) 4) 5) 6) 7) 8) 9) Determine causes of pain: (Malignant vs. Non-malignant) Differentiate type of pain: Structural (MRI) vs. Functional (EMG) Screen for alcohol use (AUDIT tool). Screen for depression (PHQ-2, PHQ-9). Screen for addiction/abuse risk (DAST, DIRE) Urine Drug Screen and blood work (e.g., CBC, ESR, LFT, BUN/SCr) Evaluate history of pain and results of previous treatments. Evaluate fatigue for malignant pain. Evaluate the effect of co-existing illness related to pain. Psycho-social evaluations (e.g., impact of life, family or work, potential addiction) If decision is made to start chronic opioid therapy (for pain greater than 3 months duration), a written contractual agreement between patient and physician is recommended. FIRST STEP: NON-OPIOIDS: 1) NSAIDs 2) Acetaminophen 3) Tramadol + ADJUNCTS^ Note: NSAIDs may cause GI bleeding/pain/ulcer Tramadol may be preferred for neurological pain SECOND STEP: THIRD STEP: OPIOIDS: 1) Codeine with acetaminophen/aspirin OPIOIDS: 1) Long-acting opioids (e.g., Morphine SR, Kadian, fentanyl, extended release oxycodone, methadone) 2) Hydrocodone or oxycodone with acetaminophen/aspirin 2) Short-acting opioids for breakthrough pain (as needed) + NON-OPIOIDS + NON-OPIOIDS + ADJUNCTS + ADJUNCTS^ Note: Potential risk for acetaminophen toxicity or opioid addiction Short-acting opioids require frequent dosing Note: There are no dosage limits for opioids and opioids should be titrated to response Adjuncts should be utilized to minimize opioid dosage increases Monitor potential addiction ^ADJUNCTS (see Table 7): 1) Consider diet, exercise (especially for weight bearing joints), heat/cold applications, smoking cessation or physical therapy if needed. 2) Antidepressants (i.e., SNRI) or anticonvulsants (i.e., Neurontin, Lyrica) may be helpful for neurological type of pain. 3) Short-term muscle relaxants may be used for spasm-related pain; long-term use for pain management is NOT recommended. A written contractual agreement may include the following discussion: Goals of therapy (pain relief, physical improvement or social functioning) The requirement for a single provider or treatment team A prohibition on use of alcohol, other sedating or illegal medications without discussing with providers (e.g., urine drug screening and alcohol testing) The limitation on dose, quantities or refills of prescribed medications (e.g., pill counts, no early refills). Against changing dosage or quantities without permission Prohibition of selling, sharing, lending or giving prescribed medications to others Agree to keep medication safe and secure and understand the potential side effects and dependence The option of sharing information with family members and other providers if necessary Compliance with all components of overall treatment plan and need for periodic reevaluation Consequences of non-adherence Reference: 1. Assessment and Management of Chronic Pain. Institute for Clinical Systems Improvement. November 2011 2. Opioid Treatment Guidelines. The Journal of Pain. Vol 10, No 2. February 2009 3. WHO Pain Relief Ladder Revised date: 7/2014 102 TABLE 1. Comparison of Non-opioid Analgesics Chemical Class Drug Name HalfLife (hr) 2-4h Recommended Starting Dose Aspirin Diflunisal (Dolobid) Choline magnesium trisalicylate (Trilisate) Ibuprofen (Motrin, Advil) Naproxen (Naprosyn) Naproxen sodium (Anaprox) Oxaprozin (Daypro) Ketoprofen (Orudis) Flurbiprofen (Ansaid) Indomethacin (Indocin) Diclofenac (Voltaren) Etodolac (Lodine) Ketorolac (Toradol) 3-12h 8-12h 650mg q4-6h 500mg q12h 4000mg 1500mg Consider a maximum of 2-3 gm/day for chronic use to avoid the risk of liver toxicity. Lack of anti-inflammatory effects Risk of GI bleed Less GI toxicity than aspirin 8-12h 1000mg q12h 4000mg Less GI toxicity than aspirin 3-4h 400mg q6-8h 3200mg 13h 250mg q12h 1000mg 275mg q12h 1100mg 4250h 2-3h 1200mg q24h 1800mg 200mg q6h ER-Extended Release IR-Immediate Release 5-6h 50mg q8-12h 200mg ER 300mg IR 300mg 4-5h 25mg q8-12h 200mg High risk of GI toxicity. CNS side effects. Avoid in elderly. 2h 25mg q6-8h 200mg 7h 200mg q6-8h 1200mg Less risk of GI toxicity 4-7h 10mg q6h 40mg Sulindac (Clinoril) 14h 150mg q12h 400mg High risk of GI toxicity. FDA recommends not to exceed 5 days therapy Possibly less renal toxicity than other NSAIDs. Metabolized via liver. Good choice for patients also on beta-blocker. Piroxicam (Feldene) Meloxicam (Mobic) Nabumetone (Relafen) Meclofenamate (Meclomen) Celecoxib (Celebrex) 45h 20mg q24h 20mg 20h 7.5mg q24h 15mg 2035h 2-4h 1000mg q24h 2000mg 50mg q4-6h 400mg 9-10h 200mg q24h 400mg Acetaminophen Salicylates Propionic Acid Acetic Acid Oxicams Naphthylalkanone Fenamate Cox-2 Inhibitors 325-650mg q46h Maximum Recommended Dose (mg/day) 4000mg 3,4 Note: Less risk of GI toxicity (lowdose). No more effective than other NSAIDs. Prior Authorization required. Acetaminophen is considered as a first-line for treating osteoarthritis pain in elderly. The initial dose should be reduced to 30-50% of recommended starting dose in elderly or patients with renal dysfunction. All nonsteroidal anti-inflammatory drugs (NSAIDs) including Cox-2 inhibitors include a boxed warning of increased risk of cardiovascular events and serious, potential life-threatening gastrointestinal bleeding associated with their use. When switching to different NSAIDs due to efficacy or side effects, consider selecting one from different chemical class. Consider PPI (i.e., generic Prilosec RX 20mg) for patients with risk of GI bleed requiring long-term NSAID therapy. 103 TABLE 2. Comparison of Oral Opioid Analgesics3,4,5,6,7 Plasma Oral Equianalgesic Half-Life (hr) Dose (mg) Short-Acting Opioids (For breakthrough pain) Codeine 200mg 3h (alone or in combination with APAP or ASA) Usual Starting Dose Usual Dosing Frequency (hr) Notes 30mg 4 – 6h Fentanyl (Actiq) Oral lozenge Hydrocodone 200mcg Limited dosing due to potential acetaminophen toxicity with which it is often combined. (see Table 6) Not recommended for long-term use. Analgesia does not increase with doses >200 mg (ceiling dose). Must be metabolized to active metabolite (morphine). Little-no response may be present in poor metabolizers of 2D6 Difficult to predict the daily maintenance dose. Handle and dispose of in a manner that is child-safe. Opioid Agonist NA (see Table 3) 30mg 2 – 4h 5 – 10mg 15 minutes and may repeat 4 – 6h 8mg 2 – 3h 2mg 4 – 6h 300mg 3 – 4h 50mg 3 – 4h Poor oral absorption, short half-life, longlasting active neurotoxic metabolite NOT recommended for chronic pain. Active metabolite. May accumulate in patients with renal impairment. Active metabolite, oxymorphone. Efficacy decreased in patients taking CYP 2D6 inhibitors.* Slower initiation and titration improves tolerability. Efficacy decreased in patients taking CYP 2D6 inhibitors.* Risk of seizure may be increased in patients taking SSRI, MAO, TCA. (alone or in combination with APAP or ASA) Hydromorphone (Dilaudid) Meperidine (12 –16h normeperidine) Morphine 30mg 2 – 3.5h 10 – 30mg 4h Oxycodone (alone or in combination with APAP or ASA) Tramadol (Ultram) 20mg 2 – 3h 5mg 6h 150mg 6 – 7h 50mg 4-6h 25mcg patch = 45-134mg/24h PO morphine 4mg acute 1mg chronic 20mg acute 3mg chronic 17h 25 mcg 72h Consider in patients who cannot tolerate oral long-acting morphine or methadone. 12 – 16h 2mg 6 – 8h 15 – 30h 2.5mg 6 – 8h Morphine Oramorph SR MS Contin Kadian 30mg 2 – 3.5h 15 – 30mg Oxycodone (Oxycontin) 20mg 2 – 3h 10mg 12h (Oramorph) (MS Contin) 24h (Kadian) 12h Risk of accumulation. Requires careful titration. Risk of accumulation. Requires careful titration. Good choice for opioid rotation. QTc interval prolongation, hypotension & cardiac dysrhythmias can occur. Recommend consult with pain specialist for prescribing. Baseline ECG prior to initiation of methadone, repeated after 30 days and then annually. GOLD standard therapy Due to prolonged absorption of the drug, the dosage should not be adjusted more frequently than every 48 hours. Adjust dosage in renal impairment. Consider in patients who cannot tolerate oral long-acting morphine or methadone. Conversion to the active metabolite, oxymorphone. Efficacy decreased in patients taking CYP 2D6 inhibitors.* Long-Acting Opioids Fentanyl (Duragesic) topical patch Levorphanol Methadone * Examples of CYP 2D6 inhibitors: SSRIs, ketoconazole, cimetidine, amiodarone, Haldol, Benadryl. 104 Starting dose should be determined at 50%-75% of calculated dose from equianalgesic conversion. If pain is constant or recurring, consider dosing around-the-clock. Most patients with malignant pain require fixed-schedule dosing to manage the constant pain and prevent the pain from worsening. Determine the total 24-hour dose of the current opioid. Using the estimated equianalgesic dose, calculate the equivalent dose of the new opioid. The starting conversion dose of the new opioid should be 50%75% of the equianalgesic dose to prevent overshooting the analgesic needs. As needed breakthrough or rescue doses (non-opioid medications analgesics or short-acting opioids) are helpful in titration to the optimal dose. When using short-acting for breakthrough, give opioid doses equivalent to approximately 10% of the daily opioid dose as needed. While treating breakthrough pain with short-acting opioids, consider using the same ingredient as the longacting opioid. Then, the total daily dose of the short-acting opioids can be calculated into the appropriate dose for the long-acting opioids. Dose adjustment may need to be considered in elderly or patients with renal or liver impairment. There is no maximum dose for most opioids. Titrate the current therapy to patients’ response or tolerance before switching to a different agent. The accurate assessment of opiate allergy is necessary to distinguish a true allergy from a side effect. These opioids are NOT recommended for chronic pain: Meperidine (Demerol, poor oral absorption, short half-life, and neurotoxic metabolite), opioid agonist/antagonist (pentazocine, nalbuphine). Management of Side Effects of Opioids: 4 - Nausea/ vomiting: Reglan 10 mg q6-8h or Compazine 10 mg q6-8h or Phenergan 25 mg q8h - Constipation: Diet and/or Colace 200 mg BID or Senokot 2 tablets BID (may increase to 4 tablets BID) or Dulcolax suppositories, 1 prn daily - Pruritis: hydroxyzine 25 - 100 mg q6-8h - Anxiety: hydroxyzine 25 - 100 mg q6-8h or Phenergan 25 –50 mg q8h - Sedation, CNS side effects: Prevention and recognition of the risks (e.g., elderly, post-surgery, impaired renal function, combination with other sedatives) - Opiate overdose (i.e., respiratory depression): Reverse opioids with naloxone 0.4-2 mg SC/IV/IM q2-3 minutes; if no response after 10 minutes, diagnosis should be questioned. A sudden stop or reduction in a dose of opioid after prolonged use may result in withdrawal symptoms (e.g., sweating, restlessness, anxiety, stomach or leg cramps, unable to sleep, increased heart rate or blood pressure, hot or cold flashes). Death may occur. Without treatment, most symptoms may disappear in 5 to 14 days; some symptoms (e.g., insomnia, irritability, and muscle aches) may last 2 to 6 months. After 72 hours of withdrawal, it is unlikely that withdrawal symptoms will worsen. 105 TABLE 3. Quick Conversion Table 6,8 Fentanyl Transdermal Dosing Conversion Convert FROM oral Morphine TO Fentanyl Transdermal Patch Oral Daily Fentanyl Morphine (mg/d) (mcg/h) Q 72 hr 45 – 134 25 135 – 224 50 225 – 314 75 315 – 404 100 405 – 494 125 495 – 584 150 TABLE 4. Suggested Maximum Daily Opioid Doses for Primary Care Clinicians Opioid Morphine Methadone Oxycodone Fentanyl (transdermal) Oxymorphone 13 Dose 200 mg/day 40 mg/day 120 mg/day 100mcg/hour 30mg/day *Higher doses require close, careful documentation and may prompt consultation with a pain specialist. TABLE 5. Equianalgesic Dosing of Opioids for Pain Management Refer to Table 6 for detailed doses of hydrocodone or oxycodone in acetaminophen containing products Hydrocodone Total daily dose 30 mg 90 mg 120 mg Hydrocodone Products Example Vicodin 5/300 6 tabs / day Endocet 10/325 6 tabs / day Norco 10/325 12 tabs / day Oxycodone Total daily dose Morphine Equivalent dose per DAY 20 mg 30 mg 60 mg 90 mg 80 mg 120 mg 106 TABLE 6. Dosing Guideline for Acetaminophen Containing Analgesics Brand Name Acetaminophen (Tylenol) mg/tab Other Ingredient(s) Max QTY/day (Based on safety Max QTY/day recommendation of 4gm/day with (3gm/day with short-term use: 1-3 mo) long-term use) 12 9 Anexsia 325 mg hydrocodone 5 mg Anexsia 325 mg hydrocodone 7.5 mg 12 9 Endocet 5-325 325 mg oxycodone 5 mg 12 9 Endocet 10-325 325 mg oxycodone 10 mg 12 9 Endocet 7.5-325 325 mg oxycodone 7.5 mg 12 9 Fioricet w/ codeine 325 mg 12 9 Norco 325 mg butalbital/caffeine/ codeine 30 mg hydrocodone 5 mg 12 9 Norco 325mg hydrocodone 7.5 mg 12 9 Norco 325 mg hydrocodone 10 mg 12 9 Percocet 325 mg oxycodone 5 or 10mg 12 9 Percocet 2.5-325 325 mg oxycodone 2.5 mg 12 9 Roxicet 325 mg oxycodone 5 mg 12 9 Tylenol #2 300 mg codeine 15 mg 13 10 Tylenol #3 300 mg codeine 30 mg 13 10 Tylenol #4 300 mg codeine 60 mg 13 10 Ultracet 325 mg tramadol 37.5 mg VIcodin 300 mg hydrocodone 5 mg 12 *8 9 *8 Vicodin ES 300 mg hydrocodone 7.5 mg *6 *6 Vicodin HP 300 mg hydrocodone 10 mg *6 *6 Xartemis XR 325 mg oxycodone 7.5mg 12 9 *This quantity is based on manufacturer daily dosing recommendations. 107 TABLE 7. Example of Adjuvant Analgesics 7 Class Antidepressants Drug Amitriptyline(Elavil) Doxepin (Sinequan) Imipramine (Tofranil) Venlafaxine (Effexor XR) Duloxetine (Cymbalta) Initial Dose 10 – 25 mg PO qHS 25 mg PO qHS 50 – 75 mg PO qHS 37.5 – 150 mg PO QD 60 mg QD Anticonvulsants Carbamazepine (Tegretol) Gabapentin (Neurontin) Clonazepam (Klonopin) Pregabalin (Lyrica) Lorazepam (Ativan) 100 mg PO BID – TID Dexamethasone Baclofen Methylphenidate (Ritalin) 4 mg PO TID-QID 5 mg PO TID 5 mg PO QAM Pamidronate (Aredia) 60-90 mg IV infusion monthly Others 100 mg PO TID 0.25 mg PO BID 75 mg BID 1 mg PO BID Note Useful for neuropathic pain, or pain complicated by depression or insomnia. SSRI or SNRI may also be helpful. Black Box Warning: SNRIs increase suicidal behavior in young adults Monitor serum level, liver function, CBC for Tegretol. Comprehensive (including est. GFR) for all. Anxiety. Increased sedation. Potential addiction. Advanced, malignant pain. Lacerating neuropathic pain. Reserve use, opioid-induced daily sedation in intolerant pt. Malignant, bone pain Long-term use of opioids in patients with chronic, non-malignant pain is controversial. Patients treated for prolonged periods with opiate drugs for non-malignant pain fail to demonstrate the need for escalating doses in order to achieve pain relief. Therefore, monitoring for dependence or addiction is important. 2,3 Behaviors that Require Attention: Requesting specific drugs Requesting appointment(s) at the end of day Aggressive complaining about needing more of the drug Obtaining similar drugs from different prescribers Missing appointment(s) or not following other components of the treatment plan (e.g., physical therapy or exercise) Resistance to a change in therapy (expression of anxiety) Increasing dosage or using the drug to treat another symptom without consulting physicians on more than one occasion 2,3 Predictors of Opioid Misuse: History of illegal behavior (e.g., selling, forgery, or stealing) Dangerous behavior (e.g., motor vehicle accidents, alcohol intoxication, or aggressive/threatening/violent behaviors) Obtaining opioids from multiple prescribers (including emergency room) or filling prescriptions at different pharmacy locations Multiple episodes of prescription “loss” Concurrent abuse of alcohol or illegal drugs Unexpected results from urine drug screen Evidence of sudden deterioration in the ability to function at work or socially, which appears to be related to drug use Repeated requests for dose increases, early refills, or resistance to change in therapy You may obtain a complete list of controlled substances filled for a patient in Michigan by requesting a Patient Controlled Substance Prescription report from the Michigan Automated Prescription System (MAPS). (Request Form for MAPS report is attached). Information is available at http://www.michigan.gov/mdch/0,1607,7-132-27417_27648---,00.html If opioid misuse or dependence is identified and the patient no longer needs opioids, treatment options include: 9 clonidine, naltrexone, methadone, or buprenorphine/naloxone (Suboxone). (Table 8) 108 Table 8. Example of Detoxification Schedule for Opioid Dependency: 10 Buprenorphine/Naloxone (Suboxone) dose (mg), sublingual tablet Day Number 10-day schedule 7-day schedule 3-day schedule 1 8 8 4+8 (stat and 24h) 2 6 6 8 (48h) 3 4 4 8 (72h) 4 4 4 5 4 2 6 2 2 7 2 0 8 2 9 2 10 0 *Doses may be adjusted to titrate off opioid in longer period of time. To locate the physician(s) authorized to prescribe buprenorphine, go to http://buprenorphine.samhsa.gov/bwns_locator/index.html *Sublingual tablets available as tablets; sublingual film available as brand only 109 Table 9. Pharmaceutical Interventions for Neuropathic Pain13 Drug Formulary Status Dosage Side effects, Contraindications & Comments ANTICONVULSANTS Gabapentin* (Neurontin®) Formulary 100 to 300 mg at bedtime; increase by 100-300 mg every 3 days up to 1,800 to 3,600 mg per day taken in divided doses three times daily. Higher doses might be used. Initial drug of choice. Side effects: drowsiness, dizziness, fatigue, nausea, sedation, edema, weight gain. No significant drug-drug interactions. Reduce dose/increase interval in renal failure (give 10x 1 creatinine clearance per day). Pregabalin* (Lyrica®) Formulary 50 mg – 75 mg twice daily-three times daily to start. Up to 200 mg three times daily. Lamotrigine (Lamictal®) Formulary 25 mg per day; increase by 25 mg-50 mg every 1-2 weeks up to 400 mg per day. Oxcarbazepine (Trileptal®) Formulary Start 150 mg - 300 mg twice daily. Increase by 600 mg per day each week to max 1200 mg twice daily. Initial drug of choice. Side effects: drowsiness, dizziness, fatigue, nausea, sedation, edema, weight gain. No drug-drug interactions. Reduce dose/increase interval in renal failure (give 5x creatinine clearance per 1 day). Schedule V medication. Side effects: Stevens-Johnson syndrome, rare lifethreatening rash unlikely with gradual dose titration. Dizziness, drowsiness, headache, nausea, 1 blurred/double vision. Initial drug of choice for trigeminal neuralgia. Similar adverse effects to carbamazepine but less likely. Fewer 1 drug-drug interactions. Carbamazepine* (Tegretol®) Formulary 200 mg-400 mg twice daily. Increase to max 600 mg twice daily. Topiramate (Topamax®) Formulary 25 mg twice daily to start; increase by 25-50 mg per week up to 200-400 mg per day. Duloxetine * (Cymbalta®) Formulary Initial drug of choice. Side effects: nausea, dry mouth, 2 constipation, dizziness, insomnia. Venlafaxine (Effexor®) Formulary 20 to 60 mg per day taken once or twice daily in divided doses (for depression); 60 mg twice daily for fibromyalgia. 37.5 mg per day; increase by 37.5 mg per week up to 300 mg per day. Formulary 10 to 25 mg at bedtime; increase by 10 to 25 mg per week up to 75 to 100 mg at bedtime or a therapeutic drug level. Initial drug of choice. Tertiary amines have greater anticholinergic side effects and may cause arrhythmia, orthostatic hypotension; therefore, these agents should 2 not be used in elderly patients. Formulary 25 mg in the morning or at bedtime; increase by 25 mg per week up to 100 mg per day or a therapeutic drug level. Secondary amines have fewer anticholinergic side effects, but should still be used cautiously in elderly 2 patients. Formulary Up to 3 patches to intact skin 12 hrs per day (12 hrs on/12 hrs off) Indicated for postherpetic neuralgia. Commonly used for other neuropathic conditions. May be used daily or as needed. Over-theCounter 0.025% or 0.075% apply to intact skin 3-4 times per day Burning irritation of skin, eyes, airway. Requires regular application for four to six weeks to achieve effect; then maintenance. Initial drug of choice for trigeminal neuralgia. Watch for hyponatremia, leucopenia, allergic rash (StevensJohnson syndrome). Other side effects: dizziness, drowsiness, blurred/double vision, ataxia. Not favored for other neuropathic pain. Available in extended 1,3 release. Most evidence is for migraine prevention, other neuropathic pains may respond. Side effects: drowsiness, abnormal thinking, weight loss, urinary tract 1 stones, increased intraocular pressure. ANTIDEPRESSANTS (SNRIs) Tricyclics** Amitriptyline (Elavil®), Imipramine (Tofranil®) Desipramine (Norpramin®) Nortriptyline (Pamelor®) TOPICAL MEDICATIONS Lidocaine 5% Patch* (Lidoderm®) Capsaicin (Capzasin-HP®, Capzasin-P®, DiabetAid Pain and Tingling Relief, Salonpas®Hot, Zostrix®) Side effects: headache, nausea, sweating, sedation, hypertension, seizures. Serotonergic properties in dosages below 150 mg per day; mixed serotonergic and noradrenergic properties in dosages above 150 mg per 2 day. Available in extended-release formulation. 110 Drug Formulary Status AS-NEEDED MEDS Tramadol (Ultram®); (Ultram ER®) Formulary Ultracet®) Formulary Oxycodone • w/ Acetaminophen (Endocet®) •w/Ibuprofen (Combunox®) •with Aspirin (Percodan®) Formulary Dosage Side effects, Contraindications, and Comments 50-100 mg 4 times daily as needed. Max 400 mg per day Side effects: abdominal discomfort, dizziness, constipation, seizures. May interact with other serotonergic drugs to cause serotonin syndrome. Abuse potential despite unscheduled status 5 mg-10 mg (oxycodone) every 4 hours as needed. Maximum daily doses: - Acetaminophen & Aspirin 4000mg - Ibuprofen 3200mg Schedule II medication. Side effects: constipation, drowsiness, confusion, nausea, itching, dependence, abstinence syndrome upon abrupt withdrawal at doses > 20 mg per day. *Approved by the U.S. Food and Drug Administration for treatment of neuropathic pain **Not recommended in patients > 65 years of age 1 FDA alert: Increased risk of suicidal behavior or ideation. 2 Black box warning: Increased suicidal behavior in young adults 3 Two black box warnings on carbamazepine: • Aplastic anemia and agranulocytosis have been reported in association with the use of carbamazepine. • The genetic testing is recommended prior to initiation of therapy in most patients of Asian ancestry for the presence of the HLA-B*1502 allele genetic marker to decrease the risk of developing Stevens-Johnson syndrome (SJS) and/or toxic epidermal necrolysis (TEN). Drugs labeled initial drug of choice based on a combination of evidence for efficacy from randomized controlled trials and safety profile. It does not imply superiority. References: 1. World Health Organization. Cancer Pain Relief 1996 2. http://www.oqp.med.va.gov/cpg/cpg.htm 3. http://www.guideline.gov/summary/summary.aspx?doc_id=4218&nbr=3226&string=opioid+and+%22pain+management%22 4. http://cancertrials.nci.nih.gov/cancertopics/pdq/supportivecare/pain/HealthProfessional/page3/print 5. Pain Relief Connection Vol 1 #6, June 18, 2002. “Pain Topics” and Pain Relief Connections are services of MGH Cares About Pain Relief http://www.massgeneral.org/painrelief/mghpain_equichart.htm http://www.guideline.gov/summary/summary.aspx?doc_id=3365&nbr=2591&string=opioid+and+%22pain+management%22 http://www.vapbm.org/archive/methadonedosing.pdf#search='methadone%20dose%20conversion NEJM. 2002 Sept. (347): 817-823 Drug and Alcohol Dependence 2003 (70): S59-77 http://www.rsdfoundation.org/en/en_opoid_treatment_protocol.html Refer to HealthPlus Clinical Practice Guideline for additional information on diagnosis and management of acute low back pain, substance abuse disorders, major depression, smoking cessation and pharmacologic step protocol for migraine treatment. 13. Assessment and Management of Chronic Pain. 5th Ed. Institute for Clinical Systems Improvement. pp. 106-107. November 2011 6. 7. 8. 9. 10. 11. 12. 111 TABLE 10. Narcotic Prescribing Assessment Tools ►click on the tool name to access the form Evaluation Type Tool Name ►Chronic Pain Evaluation Description A sample pain evaluation form for chart documentation. (HealthPlus Sample) ►PDI ►Wong-Baker Faces Helpful for assessing persons with moderate to severe dementia who have lost much of their ability to use language to describe pain. ►DAST-10 Drug Abuse Screening Test A yes/no self-report for identifying patients with existing drug abuse or addiction problems. ►DIRE Diagnosis, Intractability, Risk, Efficacy This is a clinician-rated, 7-item scale to screen for the appropriateness of long-term opioid therapy in patients with chronic noncancer pain, taking into account the likelihood of drug abuse, misuse, addiction, or drug diversion. Pain Assessment ►SISAP ►5-Point ►AUDIT Alcohol Use The Pain Disability Index Measures the impact that pain has on the ability of a person to participate in essential life activities. This can be used to evaluate patients initially, to monitor them over time, and to judge the effectiveness of interventions. Screening Instrument for Substance Abuse Potential Five questions to address concerns about alcohol, marijuana, and cigarette use in order to stratify patients with chronic non-cancer pain according to potential risks of developing problematic behaviors during opioid therapy. Prescription Opiate Abuse Checklist A brief checklist is based on DSM-III-R parameters to gauge a patient’s level of adherence to a current opioid analgesia regimen. Alcohol Use Disorders Identification Test The AUDIT questionnaire was developed by the World Health Organization (WHO) as a simple method of screening for excessive drinking as the cause of the presenting illness. ►CAGE A 4-question self-test to help patients become aware of alcohol abuse. This test specifically focuses on alcohol use, and not on the use of other drugs. ►TWEAK Test An alcohol screening tool to be used for pregnant women 112 ►PHQ-2 Depression Screening ►PHQ-9 Patient Health Questionnaire This 2-question tool is used as the initial screening test for major depressive episode. Patient Health Questionnaire A nine item depression scale for assisting in diagnosing depression as well as selecting and monitoring treatment. ►MDQ Mood Disorder Questionnaire This tool assists in the accurate diagnosis of bipolar disorder. ►Zung Zung Self-Rating Depression Scale A short self-administered survey to quantify the depressed status of a patient. 113 APPENDIX A HEALTHPLUS REQUEST FOR ADDITION TO THE FORMULARY Completed forms will be reviewed by the Pharmacy & Therapeutics Committee. The need for the drug, alternative therapy available, efficacy, safety and cost-effectiveness will be considered. It is essential that this form be completed for proper evaluation. 1. Generic Names: ___________________________________________________________ 2. Brand Name & Manufacturer: _________________________________________________ 3. Dosage Form(s) & Strength(s): ________________________________________________ 4. Specific pharmacologic action and indications for use: _________________________________________________________________________ _________________________________________________________________________ 5. Comparable drugs currently on the Formulary: ____________________________________ _________________________________________________________________________ 6. If the requested drug is used, which of the drugs above may be deleted from the Formulary? _________________________________________________________________________ 7. List the therapeutic advantages of the requested drugs over those already listed on the Formulary. Supply references to support these advantages: _________________________________________________________________________ _________________________________________________________________________ 8. Estimate the anticipated cost impact if the requested drug is added to the Formulary: _________________________________________________________________________ ________________________________ DATE ___________________________________ PRINT NAME _________________________________________________________________________ SIGNATURE Send to: HealthPlus ATTN: Pharmacy Department 2050 S Linden Road; PO Box 1700 Flint, MI 48501-1700 FAX: 810-720-2757 E-MAIL: [email protected] 114 APPENDIX B HEALTHPLUS PARTNERS (MEDICAID) OVER-THE-COUNTER (OTC) MEDICATIONS Michigan Medicaid regulations include a requirement for coverage of selected over-the-counter (OTC) medications as part of the prescription benefit. OTC products covered by Michigan Medicaid are covered for members in the HealthPlus Partners program only, with a written prescription. If the OTC product is available as a generic, the generic product is covered. A summary list (alphabetic by brand name) of covered OTC products is included below: Allegra (fexofenadine) Allegra-D (fexofenadine/pseudoephedrine) Artificial Tears solution Aspirin tablets (regular, buffered and enteric-coated), suppositories Bacitracin ointment Benadryl (diphenhydramine) capsules, elixir Calcium carbonate tablets, suspension Chlor-Trimeton (chlorpheniramine) tablets, syrup Claritin (loratadine) tablets, reditabs, syrup Claritin-D (loratadine/pseudoephedrine) Colace (docusate sodium) capsules, liquid Condoms, latex Dulcolax (bisacodyl) tablets, suppositories Ferrous gluconate Ferrous sulfate tablets, solution Gyne-Lotrimin (vaginal cream, suppositories) Hydrocortisone cream, ointment Imodium caplet Imodium AD (loperamide) liquid Maalox (aluminum/magnesium hydrox) suspension Metamucil (psyllium) powder Monistat-7 (miconazole) vaginal cream, suppositories Motrin (ibuprofen) tablets, suspension, chewables Neosporin (bacitracin/neomycin/polymixin) ointment Nicotine patch, inhaler, nasal spray, gum/lozenges Nix (permethrin cream rinse) Pepto-Bismol caplet, chewable, suspension Peri-Colace (docusate sodium w/ casanthranol) capsules Prevacid 24 Hour (lansoprazole) capsules Tavist (clemastine) tablets, syrup Tylenol (acetaminophen) tablets, drops, elixir, suppositories Zaditor (ketotifen) Zyrtec (cetirizine) tablets, chewable, liquid gels, solution Note: This is a summary list and does not include all covered OTC products. 115 STATUS APPENDIX C PHARMACY PRIOR AUTHORIZATION FORM Forward form to the HealthPlus Pharmacy Department via facsimile: Flint facsimile: 810-720-2757 For questions or to request via telephone: Flint local phone: 810-720-2758 Toll free phone: 877-710-0993 FOR A TIMELY RESPONSE, PLEASE PROVIDE COMPLETE INFORMATION. HealthPlus ID#: Date of Birth: Patient Name: Height: This is a request for (check one): Weight: DAW MedicarePlus Advantage Part D: Signature PPO Closed Formulary: BMI: Medication Requiring P/A Exception Request P/A for Dosage Regimen Medically Urgent Exception Request Prescribed Drug and Dosing Regimen: Reason for Use (Diagnosis): Previous Medications: Please attach pertinent laboratory test(s) or procedure(s): (if applicable) Reason why an alternative drug (or dosing regimen) cannot be used: DEA#: Office Phone: (_____) Pharmacy Name (optional): HealthPlus Provider ID#: Office Facsimile: (_____) Pharmacy Phone: Infusions/Injections (if applicable) Place of Infusion/injection: ________________________ Provider ID: ____________________________________ Lab Results (if applicable) CrCL: _________________ TG: ____________________ I represent to the best of my knowledge and belief that the information provided is true, complete, and fully disclosed. A person may be committing insurance fraud if false or deceptive information with the intent to defraud is provided. Physician’s Name (please print) ____________________ Physician’s Signature Office Contact Person: Request Date: For HealthPlus Use Only LOB: L E N Non-Urgent Request: Urgent Request: CPhT Review Time RPh Review Time Med Dir Review Time Comments: Approved Partial Approval Denied Approved by: Reason for Denial: Effective Date: Faxed to Indigent Program: If you would like to discuss this case with a physician reviewer, please call 800 332-9161. **THIS DOCUMENT MAY BE PHOTOCOPIED, or you may request additional copies by calling the HealthPlus Pharmacy Department at the telephone number(s) listed above. Rev August 2014 116 HEALTHPLUS COMMERCIAL/MEDICARE (NON-PART D)/PPO/TPA/MICHILD DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D DRUG/CATEGORY ADD Medications Vyvanse® (lisdexamfetamine dimesylate) Strattera® (atomoxetine) QTY LIMIT CRITERIA 1. The patient must have a chart documented trial or Rx claims for generic Adderall or Adderall XR in the past 120 days. 10mg, 18mg, 25mg, and 40mg: Limited to a qty of 60 units per month 60mg, 80mg and 100mg: Limited to a qty of 30 units per month 1. The patient must have a documented diagnosis of AttentionDeficit/Hyperactivity Disorder (ADHD); AND 2. The patient must have documented failure based on chart documentation or prescription claims with a generic methylphenidate (i.e., Ritalin, Concerta) AND generic Adderall; OR 3. The patient must have a documented history or risk of substance abuse; OR 4. The patient must have a documented diagnosis of anxiety or tics. Focalin XR® (dexmethylphenidate) 1. The patient must have chart documented trial or Rx claims for a generic methylphenidate in the past 120 days. Daytrana® (methylphenidate patch) Quillivant XR® (methylphenidate suspension) 1. The patient is at least six years of age and has a documented diagnosis of ADD/ADHD; AND 2. The patient must have a chart documented trial or Rx claims for a generic methylphenidate in the past 120 days; OR Intuniv® (guanfacine) Limited to a qty of 30 units per month Allergy Medications Clarinex® (desloratadine) Limited to a qty of 30 units per month Clarinex-D® (desloratadine/pseudoephedrine) For Daytrana only: If the patient has a chart documented inability to swallow, a trial of oral methylphenidate is not required. 1. The patient must have a documented diagnosis of AttentionDeficit/Hyperactivity Disorder (ADHD); AND 2. The patient must have documented failure based on chart documentation or prescription claims with a generic methylphenidate (i.e., Ritalin, Concerta) AND generic Adderall; OR 3. The patient must have a documented history or risk of substance abuse; OR 4. The patient must have a documented diagnosis of anxiety or tics. 1. The patient must have documented failure or Rx claims for generic OTC Claritin D or OTC generic Claritin in combination with OTC generic pseudoephedrine in the past year. NOTE: For Clarinex-D, prior authorization is only required for patients over 12 years of age. Generic Claritin and Claritin-D OTC products are covered with a prescription; OTC pseudoephedrine is not a covered benefit. 117 These criteria apply to all HealthPlus Commercial HMO lines of business except as noted, and may also apply to PPO benefits. HEALTHPLUS COMMERCIAL/MEDICARE (NON-PART D)/PPO/TPA/MICHILD DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D DRUG/CATEGORY Allergy Medications, continued All Brand Nasal Steroids Beconase AQ® (beclomethasone dipropionate) Nasonex® (mometasone furoate) Omnaris® (ciclesonide) Qnasl® (beclomethasone dipropionate) Veramyst® (fluticasone furoate) Zetonna® (ciclesonide) All Brand Nasal Steroids, Combination Products Dymista® (azelastine/fluticasone propionate) Analgesics On Formulary with PA: Actiq® (fentanyl citrate oral transmucosal) Non-Formulary with PA: Abstral® (fentanyl sl) Fentora® (fentanyl citrate buccal tablet) Lazanda® (fentanyl nasal spray) Subsys® (fentanyl sublingual spray) QTY LIMIT CRITERIA 1. The patient must have documented failure or Rx claims for two generic nasal steroids (i.e., Flonase, flunisolide, Nasacort AQ, Rhinocort Aqua) in the past year. 1. The patient must have documented failure or Rx claims for a generic nasal steroid (i.e., Flonase, flunisolide, Nasacort AQ) in the past year. Abstral, Fentora, Subsys qty-4 units/day Actiq qty4 units/ day 1. The patient has a documented current diagnosis of cancer. 2. The patient is already receiving and is tolerant to opioid therapy for underlying persistent cancer pain. NOTE: System will automatically approve if written by an oncologist (or if there are prescription claims for chemotherapyrelated medications) and the patient is receiving opioid pain medications. Abstral, Lazanda and Subsys– New Starts Only Lazanda qty-1 bottle (5ml)/day MS Contin® (morphine ext. release) QUANTITY LIMITS ONLY NOTE: Limited to 3 units per day Nucynta® (tapentadol) QUANTITY LIMITS ONLY NOTE: Limited to 6 units per day Nucynta ER® (tapentadol) QUANTITY LIMITS ONLY NOTE: Limited to 2 units per day QUANTITY LIMITS ONLY NOTE: Limited to 8 units per day Opana® (oxymorphone) Opana ER (Crush Resistant)® (oxymorphone) Oxymorphone ER (Non-Crush Resistant) (oxymorphone) Oxycodone/Ibuprofen Stadol NS® (butorphanol) Ultracet® (tramadol/acetaminophen) Ultram® (tramadol) Qty is limited to 3 units per day 1. The patient has a documented current diagnosis of active cancer. NOTE: System will automatically approve if written by an oncologist or if there are previous claims for chemotherapyrelated medications. QUANTITY LIMITS ONLY NOTE: Limited to 28 units per 30 days QUANTITY LIMITS ONLY NOTE: Limited to 2 bottles (5ml) per 30 days QUANTITY LIMITS ONLY NOTE: Limited to 8 units per day 118 These criteria apply to all HealthPlus Commercial HMO lines of business except as noted, and may also apply to PPO benefits. HEALTHPLUS COMMERCIAL/MEDICARE (NON-PART D)/PPO/TPA/MICHILD DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D DRUG/CATEGORY QTY LIMIT Analgesics, continued Ultram ER® (tramadol) Butrans® (buprenorphine patch) CRITERIA QUANTITY LIMITS ONLY NOTE: Limited to 1 unit per day Qty is limited to 4 units per 28 days For indications other than cancer: 1. The patient must have documented failure or prescription claims for at least two formulary alternatives within the last 3 months (including generic MS Contin and short-acting narcotic analgesic) OR 2. Based on chart documentation, all formulary alternatives are inappropriate. NOTE: System will automatically approve if written by an oncologist or if there are prescription claims for chemotherapyrelated medications. New Starts Only Conzip® (tramadol) QUANTITY LIMITS ONLY NOTE: Limited to 1 unit per day Kadian® (morphine ext. release) QUANTITY LIMITS ONLY NOTE: Limited to 2 units per day Avinza® (morphine sulfate, sustained release) Qty is limited to 30 units per 30 days Rybix ODT® (tramadol) 1. The patient has a documented current diagnosis of active cancer. 2. System will automatically approve if written by an oncologist or if there are previous claims for chemotherapy-related medications. 1. The patient must have documented failure or Rx claims with generic Ultram in the past 60 days, or 2. The patient must have documented inability to swallow or absorb oral medications. Ryzolt® (tramadol) QUANTITY LIMITS ONLY NOTE: Limited to 1 unit per day All acetaminophen-containing narcotic analgesics DOSE OPTIMIZATION ONLY NOTE: System edits apply for prescription claims with a monthly quantity that exceeds the MAX recommended dose of 4gm/day of acetaminophen. Physician must submit signed request stating he/she is allowing the patient to exceed the MAX recommended dose of acetaminophen. Duragesic Patches® (fentanyl) QUANTITY LIMITS ONLY NOTE: Limited to 15 units per 30 days Oxycontin® (oxycodone) QUANTITY LIMITS ONLY NOTE: Limited to 3 units per day Exalgo® (extended release hydromorphone) 8mg, 12mg, 16mg-qty limited to 1 unit per day Requires prior authorization for indications other than cancer. System will automatically approve if written by an oncologist or if there are previous claims for chemotherapy-related medications. 1. The patient must have documented failure or Rx claims with generic Dilaudid (hydromorphone) and generic Duragesic (fentanyl). 32mg-qty limited to 2 units per day 119 These criteria apply to all HealthPlus Commercial HMO lines of business except as noted, and may also apply to PPO benefits. HEALTHPLUS COMMERCIAL/MEDICARE (NON-PART D)/PPO/TPA/MICHILD DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D DRUG/CATEGORY Analgesics, continued Vicodin 5/300® (hydrocodone/acetaminophen) Vicodin ES 7.5/300® (hydrocodone/acetaminophen) Vicodin HP 10/300® (hydrocodone/acetaminophen) Xartemis XR® (oxycodone/APAP CR) QTY LIMIT Vicodin 5/300 limit 8 tabs/day VIcodin ES 7.5/300 & Vicodin HP 10/300 limit 6 tabs/day 120 tablets per 30 days All Brand Combination Butalbital/Acetaminophen Products Bupap® (butalbital/acetaminophen) Phrenilin/Phrenilin Forte® (butalbital/acetaminophen) All Single Ingredient Hydrocodone Products Zohydro ER® (hydrocodone) Androgens All Non-Formulary Testosterone Products Androderm® (testosterone patch) Axiron® (testosterone solution) Striant® (testosterone buccal) CRITERIA 1. Physician must provide chart documentation that shows that a product with 325mg acetaminophen (i.e. generic Norco) is contraindicated in this patient but that a product with 300mg acetaminophen is not contraindicated Note: Acetaminophen is not recommended for patients with liver disease. 1. Patient must have documented failure or Rx claims for both generic Percocet and generic MS Contin in the past 6 months; AND 2. The prescriber must submit a current MAPS report (or similar report) which shows no sign of substance abuse or multiple prescribers of narcotics in the past 6 months; AND 3. The authorization will be approved for 6 months. Renewals require submission of an updated MAPS report confirming no evidence of substance abuse. 1. The patient must have chart documented failure or prescription claims for an oral generic butalbital/acetaminophen product in the past 6 months. Zohydro ER Qty is limited to 2 units per day 1. The patient must have documented failure or Rx claims for both generic MS Contin and generic Duragesic patches in the past 6 months; AND 2. The prescriber must submit a current MAPS report (or similar report) which shows no sign of substance abuse or multiple prescribers of narcotics in the past 6 months; AND 3. The authorization will be approved for 6 months. Renewals require submission of an updated MAPS report confirming no evidence of substance abuse. 1. The patient is male, ≥ 18 years old, and has a documented diagnosis of hypogonadism; AND 2. The patient has a morning (before 11AM) serum total testosterone concentration of less than 300 ng/dL documented on 2 separate occasions in the past year; AND 3. The patient must have documented failure or Rx claims with a preferred formulary testosterone replacement product (i.e., testosterone cypionate/enanthate, AndroGel). 120 These criteria apply to all HealthPlus Commercial HMO lines of business except as noted, and may also apply to PPO benefits. HEALTHPLUS COMMERCIAL/MEDICARE (NON-PART D)/PPO/TPA/MICHILD DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D DRUG/CATEGORY QTY LIMIT Androgens, continued Non-Formulary Oral Methyltestosterone and Fluoxymesterone Products Methitest® (methyltestosterone) Testred® (methyltestosterone) All Non-Formulary Angiotensin II Receptor Blockers Teveten HCT® (eprosartan mesylate) Edarbi® (azilsartan medoxomil) Edarbyclor® (azilsartan medoxomil/chlorthalidone) Antibiotics Oracea® (doxycycline monohydrate) Dificid® (fidaxomicin) All Brand Minocycline Products Minocin PAC® (minocycline kit) Solodyn® (minocycline ER) CRITERIA 1. The patient is male and has a documented diagnosis of hypogonadism; AND 2. The patient has a morning (before 11AM) serum total testosterone concentration of less than 300 ng/dL documented on 2 separate occasions in the past year; AND 3. The patient must have documented failure or Rx claims with a preferred formulary testosterone replacement product (i.e., testosterone cypionate/enanthate, AndroGel, Android); OR 1. The patient has a documented diagnosis of delayed puberty; AND 2. The patient must have documented failure or RX claims with testosterone cypionate/enanthate or Android; OR 1. The patient is female and has a documented diagnosis of breast cancer. All ARBs except Cozaar (not combos) are limited to a qty of 30 units per month Qty is limited to 30 units per 30 days 1. The patient must have documented failure or Rx claims for all formulary ARBs or ARB combination products (i.e., Benicar/HCT, or Diovan/HCT). NOTE: If patient is a first time ARB user, patient should have documented failure or Rx claims for at least one generically available ACE inhibitor previous to ARB therapy. 1. The patient must have documented failure or Rx claim(s) for at least one formulary ARB or ARB combination product (i.e., generic Cozaar/Hyzaar, Benicar/HCT or Diovan/HCT). 1. The patient must have documented failure or Rx claim for generic Vibramycin. 1. Patient has documented diagnosis of C. difficile associated diarrhea, AND 2. Patient has tried and failed an adequate trial of vancomycin, OR 3. Patient has a contraindication or intolerance to vancomycin, OR 4. Patient has been recently discharged from a hospital or a medical facility and has had documented treatment with Dificid or vancomycin. New Starts Only 1. The patient must have documented failure or Rx claims for a generic topical acne product AND minocycline in the past 60 days. 121 These criteria apply to all HealthPlus Commercial HMO lines of business except as noted, and may also apply to PPO benefits. HEALTHPLUS COMMERCIAL/MEDICARE (NON-PART D)/PPO/TPA/MICHILD DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D DRUG/CATEGORY QTY LIMIT Antibiotics, continued Factive® (gemifloxacin mesylate) Tobi Solution/Podhaler Anticoagulants Brilinta® (ticagrelor) Effient® (prasugrel hydrochloride) Eliquis® (apixaban) Pradaxa® (dabigatran) Xarelto® 10 mg (rivaroxaban) Xarelto® 20mg (rivaroxaban) Qty is limited to 60 units per 30 days Qty is limited to 30 units per 30 days Qty is limited to 60 units per 30 days Qty is limited to 60 units per 30 days Qty for 10mg is limited to 35 units Qty is limited to 30 units per 30 days Anticonvulsants Aptiom® (eslicarbazepine) Antidepressants Luvox CR® (fluvoxamine ext. release) Pexeva® (paroxetine mesylate) Viibryd® (vilazodone) CRITERIA 1. The patient must have documented failure or Rx claim for a formulary fluoroquinolone (e.g., generic Cipro, Levaquin or Avelox) in the past 60 days. NOTE: Individual requests are reviewed to include consideration of the diagnosis, culture and sensitivity, and other documentation. 1. The patient must have a diagnosis of Cystic Fibrosis; AND 2. The drug is given for 28 days followed by 28 days off, in repeat cycles. DOSE OPTIMIZATION ONLY NOTE: System edits apply for prescription claims submitted for more than twice daily dosing. DOSE OPTIMIZATION ONLY NOTE: System edits apply for prescription claims submitted for more than once daily dosing DOSE OPTIMIZATION ONLY NOTE: System edits apply for prescription claims submitted for more than twice daily dosing. DOSE OPTIMIZATION ONLY NOTE: System edits apply for prescription claims submitted for more than twice daily dosing. DOSE OPTIMIZATION ONLY NOTE: System edits apply for prescription claims submitted for more than once daily dosing. 1. The patient must be 18 years of age or older; AND 2. Patient has a documented diagnosis of partial-onset seizures; AND 3. The patient must have documented insufficient response, intolerable side effects, or Rx claims for at least 2 generic anti-epileptic drugs (i.e., lamotrigine, topiramate, oxcarbazepine, carbamazepine, levetiracetam, divalproex, gabapentin, zonisamide). Limited to a qty of 30 units per month 1. The patient must have documented failure with dose titration and Rx claims for at least two generic SSRI medications (i.e., Prozac, Celexa, Paxil and Zoloft). 122 These criteria apply to all HealthPlus Commercial HMO lines of business except as noted, and may also apply to PPO benefits. HEALTHPLUS COMMERCIAL/MEDICARE (NON-PART D)/PPO/TPA/MICHILD DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D DRUG/CATEGORY QTY LIMIT CRITERIA Antidepressants, continued Brintellix® (vortioxetine) 1. The patient must have documented failure with dose titration and Rx claims for at least 3 generic antidepressant medications (i.e., Prozac, Paxil, Effexor, Wellbutrin). New Starts Only Prozac Weekly® (fluoxetine) 1. The patient has a diagnosis of depression, AND 2. The patient has been treated with fluoxetine 20mg daily for at least 13 weeks, based on Rx claims, and has responded to treatment with symptom control. 1. The patient must have documented failure or Rx claim for generic Prozac. On Formulary with PA: Sarafem® (fluoxetine) Effexor XR® (venlafaxine, ext. release) Lexapro® (escitalopram oxalate) Pristiq® (desvenlafaxine succinate) Oleptro ER® (trazodone hydrochloride extended release) Limited to a qty of 30 units per month DOSE OPTIMIZATION ONLY NOTE: System edits apply for prescription claims submitted for more than once daily dosing. 1. The patient must have documented failure or Rx claims with generic Desyrel (trazodone). Aplenzin® (bupropion hbr) 1. The patient must have documented failure or prescription claims at an equivalent dosage of bupropion HCl extendedrelease (24hr) in the past year. Wellbutrin XL® (bupropion, ext. release) DOSE OPTIMIZATION ONLY 1. For Wellbutrin XL 150mg tablets are limited to Once Daily 2. Dosing. Wellbutrin XL 300mg requires the physician to prescribe a 300mg tablet (not 2 of the 150mg tablets) once daily to optimize the dose. 3. Dosages greater than 450mg per day will require the physician to submit medical necessity for that dosing regimen. Antiemetic Diclegis® (doxylamine/pyridoxine) Qty is limited to 120 units per 30 days Zuplenz® (ondansetron) Antipsychotics, Atypical Latuda® (lurasidone) Abilify® (aripiprazole) Zyprexa/Zydis® (olanzapine) Limited to a qty of 30 units per month 1. The patient must have a documented diagnosis of pregnancy; AND 2. The patient must have a chart documented trial and failure or Rx claims for generic Zofran; AND 3. The patient must have a chart documented trial and failure of the individual agents (doxylamine and pyridoxine) in combination. New Starts Only 1. The patient must try and fail an adequate course of therapy with generic Zofran ODT. 1. The patient must have documented failure or prescription claims for at least two formulary atypical antipsychotic alternatives (e.g., geq Risperdal, geq Clozaril, geq Geodon or geq Seroquel). OR 2. The patient must have documented failure or prescription claims for at least 1 formulary atypical antipsychotic and 1 formulary mood stabilizer (e.g., lithium, divalproex sodium, valproate) if prescribed for Bipolar Depression DOSE OPTIMIZATION ONLY NOTE: System edits apply for prescription claims submitted for more than once daily dosing. 123 These criteria apply to all HealthPlus Commercial HMO lines of business except as noted, and may also apply to PPO benefits. HEALTHPLUS COMMERCIAL/MEDICARE (NON-PART D)/PPO/TPA/MICHILD DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D DRUG/CATEGORY Asthma/COPD Combivent Respimat® (albuterol/ ipratropium) Proventil HFA® (albuterol) ProAir HFA® (albuterol) QTY LIMIT Limited to 6 doses per day Xopenex/HFA® (levalbuterol) Zyflo/CR® (zileuton) Beta Blockers Bystolic® (nebivolol) Limited to a qty of 30 units per month Coreg CR® (carvedilol phosphate controlled release) Cardizem LA® (diltiazem, long-acting) Non-Formulary with PA: Advicor® (lovastatin/niacin) Altoprev® (lovastatinSR) Lescol XL® (fluvastatin) Livalo® (pitavastatin calcium) Liptruzet® (ezetimibe/atorvastatin) All Brand Omega-3 Fatty Acid Products Lovaza® (omega-3-acid ethyl esters) Vascepa® (icosapent ethyl) DOSE OPTIMIZATION ONLY NOTE: System edits apply for prescription claims submitted for more than 6 doses a day. 1. Patient has a documented contraindication to the preferred formulary albuterol inhaler (i.e. Ventolin HFA) 1. The patient must have documented intolerant side effects to albuterol (e.g., palpitations, tremors and tachycardia). 1. The patient must have a diagnosis of asthma; AND 2. The patient must be 12 years of age or older; AND 3. The patient must have chart documented failure or prescription claims for generic Singulair or Accolate. DOSE OPTIMIZATION ONLY NOTE: System edits apply for prescription claims submitted for more than once daily dosing. 1. The patient must have documented failure on immediate release carvedilol of equivalent dose and attempted at least one dose increase (6.25mg/day IR = 10mg/day ER when converting). 1. The patient must have documented failure on immediate release isradipine of equivalent dose and attempted at least one dose increase AND 2. The patient must have documented failure/contraindication to three generically available dihydropyridine CCB agents (e.g., nisoldipine, nifedipine, amlodipine, nicardipine, felodipine) in the past year. Calcium Channel Blockers Dynacirc CR® (isradipine controlled release) Cholesterol Medications On Formulary with PA: Crestor® (rosuvastatin) CRITERIA 1. The patient must have documented failure or Rx claims for at least two generically available formulary alternatives (e.g., Cardizem CD, Cardizem SR and Dilacor XR). All HMGs are limited to a qty of 30 units per month 1. The patient must have documented failure or Rx claim(s) for generic Zocor, OR 2. The patient is currently receiving a medication that potentiates simvastatin levels (i.e., itraconazole, ketoconazole, HIV protease inhibitors, erythromycin, gemfibrozil, cyclosporine, amiodarone, verapamil, diltiazem, amlodipine, ranolazine). Limited to a qty of 30 units per month 1. DOSE OPTIMIZATION ONLY NOTE: System edits apply for prescription claims submitted for more than once daily dosing. 1. The patient's triglyceride (TG) levels are >500mg/dL (with chart documentation provided) OR 2. The patient must have documented failure or Rx claims in the past six months for at least two or more lipid-lowering agents, with at least one being a generic product (e.g., statins, fenofibrate, nicotinic acid). 124 These criteria apply to all HealthPlus Commercial HMO lines of business except as noted, and may also apply to PPO benefits. HEALTHPLUS COMMERCIAL/MEDICARE (NON-PART D)/PPO/TPA/MICHILD DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D DRUG/CATEGORY QTY LIMIT Cholesterol Medications, continued Antara® (fenofibrate, micronized) Fenoglide® (fenofibrate) Lipofen® (fenofibrate) Triglide® (fenofibrate) On Formulary with PA: Zetia® (ezetimibe) 1. The patient must have documented failure or Rx claim for a formulary fenofibrate (i.e., generic Lofibra) in the past year with at least one documented dosage increase. AUTHORIZATION IS ONLY REQUIRED FOR THE FOLLOWING: 1. If the patient has not had an Rx claim for an HMG statin medication in the previous year. Criteria for authorization for monotherapy include a documented contraindication for both hydrophilic (Pravachol, Lescol) and lipophilic (Zocor, Lipitor) statins, elevated liver enzymes, etc. 2. A dose >10mg per day requires documentation to support safety and efficacy. 1. The patient must have a documented trial or Rx claims for at least two generically available oral contraceptives in the past year before any brand product will be covered. Contraceptives All Brand Contraceptives Beyaz® LoEstrin 24 Fe 1/20® Natazia® Ovcon-50® Safyral® NuvaRing® Ortho Evra® Ortho Tri-Cyclen Lo® Cough and Cold Vituz® NOTE: Injectable generic Depo-Provera is an alternative if compliance is a potential issue. 1. The patient must have documented failure or Rx claims for 2 generically available cough suppressants in the past month. Dermatologicals Altabax® (retapamulin) Bactroban Nasal Ointment® (mupirocin) Clobetasol Propionate Cream and Ointment -generics Cormax® (clobetasol propionate) Temovate® (clobetasol propionate) Temovate E® (clobetasol propionate) Vusion® (miconazole nitrate/zinc oxide) CRITERIA 1. The patient must have a documented treatment failure with generic Bactroban ointment for each instance of impetigo AND 2. A diagnosis of impetigo. 10 grams (10, 1gm) tubes per month 1. The patient must have a chart documented nasal colonization with methicillin-resistant S. aureus (MRSA); AND 2. The patient must have Rx claims for generic mupirocin ointment in the past 7 days. Criteria for more than 10 grams per month 1. The patient must have chart documented nasal recolonization of MRSA. 1. The patient must have documented failure or Rx claims for generic Diprolene/AF (augmented betamethasone) or generic Ultravate (halobetsol) cream or ointment in the past 60 days. 1. The patient must be an infant greater than 4 weeks old with a diagnosis of candidal diaper dermatitis or candidal infection. 125 These criteria apply to all HealthPlus Commercial HMO lines of business except as noted, and may also apply to PPO benefits. HEALTHPLUS COMMERCIAL/MEDICARE (NON-PART D)/PPO/TPA/MICHILD DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D DRUG/CATEGORY Dermatologicals, continued Zyclara® (imiquimod) All Branded Topical Antifungal Agents Ciclodan Kit® (ciclopirox olamine cream/cleanser) CNL Nail Kit® (ciclopirox/lacquer removal pads) Dermasorb AF Kit® (clioquinol-hc /emollient) Ecoza® (econazole nitrate) Ertaczo® (sertaconazole nitrate) Exelderm® (sulconazole nitrate) Jublia® (efinaconazole) Kerydin® (tavaborole) Ketodan Kit® (ketoconazole foam/cleanser) Lamisil Soln® (terbinafine soln) Mentax® (butenafine) Naftin® (naftifine) Oxistat® (oxiconazole nitrate) Pediaderm AF® (nystatin/emollient) Terbinex® (terbinafine/hydroxychitosan) Tersi® (selenium sulfide) Xolegel/Corepak ® (ketoconazole) Luzu® (luliconazole) QTY LIMIT CRITERIA 1. The patient must have a diagnosis of actinic keratosis and documented treatment failure or Rx claims for geq Aldara; OR 2. The patient must have a diagnosis of condyloma acuminate and documented treatment failure or Rx claims for geq Condylox or geq Aldara. New Starts Only 1. The patient must have documented failure and Rx claims for four generic antifungals (e.g., Loprox, Nizoral, Spectazole and Grifulvin V). 1. The patient must have documented failure or Rx claims for at least 2 generic antifungal products (i.e., clotrimazole, miconazole, tolnaftate, terbinafine). All Branded Topical Clindamycin Products Clindagel 1% Gel® (clindamycin) 1. Patient must have documented failure or Rx claim(s) for topical generic clindamycin product in the past 90 days (e.g., GEQ Cleocin T). All Brand Benzoyl Peroxide Combination Products Acanya 1.2%-2.5%® (clindamycin/benzoyl peroxide) Benzamycin Pak 3%-5% Gel® (erythromycin base/benzoyl peroxide) 1. Patient must have documented failure or Rx claim(s) for a generic combination product in the past 90 days (i.e., GEQ Benzaclin, GEQ Benzamycin. 126 These criteria apply to all HealthPlus Commercial HMO lines of business except as noted, and may also apply to PPO benefits. HEALTHPLUS COMMERCIAL/MEDICARE (NON-PART D)/PPO/TPA/MICHILD DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D DRUG/CATEGORY QTY LIMIT CRITERIA Dermatologicals, continued All Brand Topical Adapalene and Dapsone Products Aczone 5% Gel® (dapsone) Differin 0.1% Lotion® (adapalene) Epiduo 0.1%-2.5% Gel® (adapalene/benzoyl peroxide) 1. The patient must have documented failure or Rx claim(s) for a generic tretinoin (e.g., Avita, Retin-A) AND a generic adapalene (e.g., Differin gel) All Tretinoin Products Age Restriction: Patients > 25 years of age must have a documented diagnosis of acne. All Brand Tretinoin Products Atralin® (tretinoin) Retin A Micro 0.8%® (tretinoin) Tretin-X® (tretinoin) Veltin® (tretinoin/clindamycin) Ziana® (tretinoin/clindamycin) 1. The patient must have documented failure or Rx claim for a generic tretinoin product (e.g., Retin-A, Avita) in the past 90 days. All Brand Topical Steroids Clobex Spray® (clobetasol propionate) Synalar TS® (fluocinolone/cleanser) Ultravate PAC Kit® (halobetasol propionate/ammonium lactate) NOTE: Age restriction for all topical tretinoin products for age > 25 based on a diagnosis of acne. 1. The patient must have documented failure or Rx claim with a generic topical steroid in the same potency class (e.g., Ultravate, Diprolene) in the past 60 days. Kenalog Aerosol Spray® (triamcinolone acetonide) Pandel Cream® (hydrocortisone probutate) Pediaderm TA® (triamcinolone) Topicort Spray® (desoximetasone) Cordran Lotion® (flurandrenolide) Cordran SP Cream® (flurandrenolide) Locoid Lotion ® (hydrocortisone butyrate) 1. The patient must have documented failure or Rx claim with a generic topical steroid in the same potency class (e.g., Elocon, Westcort and Synalar) in the past 60 days. Desonate Gel® (desonide) Desowen Combo® (desonide/emollient) Pediaderm HC® (hydrocortisone) Vanoxide-HC Lotion® (hydrocortisone/benzoyl peroxide) Verdeso Foam® (desonide) 1. The patient must have documented failure or Rx claim with a generic topical steroid in the same potency class (e.g., Aclovate, Desowen and Synalar) in the past 60 days. Protopic® (tacrolimus) 1. The patient must have documented failure or Rx claims with at least two generically available topical steroids AND pimecrolimus in the past 180 days. Solaraze® (diclofenac 3% gel)including generics 1. The patient must have a chart documented diagnosis of actinic keratosis. 1. The patient must have documented failure or Rx claim with a generic topical steroid in the same potency class (e.g., BetaVal Cr, Cutivate Cr, Dermatop Cr) in the past 60 days. 127 These criteria apply to all HealthPlus Commercial HMO lines of business except as noted, and may also apply to PPO benefits. HEALTHPLUS COMMERCIAL/MEDICARE (NON-PART D)/PPO/TPA/MICHILD DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D DRUG/CATEGORY Dermatologicals, continued Dovonex® (calcipotriene) Taclonex® (betamethasone/calcipotriene) Vectical® (calcitriol) QTY LIMIT Safety limited to a qty of < 100g per 7 days Safety limited to a qty of < 200g per 7 days All Branded Topical Sulfonamide and Sulfonamide/Sulfur Products Avar® (sulfacetamide sodium/sulfur) Avar-E® (sulfacetamide sodium/sulfur) Avar LS® (sulfacetamide sodium/sulfur) Plexion® (sulfacetamide sodium/sulfur) Rosanil® (sulfacetamide sodium/sulfur) Sumadan® (sulfacetamide sodium/sulfur) Diabetes Glumetza® (metformin) Janumet, XR® (sitagliptin/metformin) Kazano® (alogliptin/metformin) Kombiglyze XR® (saxagliptin/metformin) Oseni® (alogliptin/pioglitazone) Januvia® (sitagliptin) Nesina® (alogliptin benzoate) Onglyza® (saxagliptin) Tradjenta® (linagliptin) Invokana® (canagliflozin) Apidra® Novolin® Insulins (insulin) Novolog® Insulins (insulin aspart) Novolog Mix® (insulin) CRITERIA QUANTITY LIMITS ONLY QUANTITY LIMITS ONLY 1. The patient must have documented failure and Rx claims for at least 2 generic sulfonamide/sulfur products in the past year. 1. The patient must have documented failure or Rx claims in the past year for generic Glucophage AND generic Glucophage XR. 1. The patient must have documented failure or Rx claims with a preferred formulary DPP-4 inhibitor (i.e. Tradjenta, Jentadueto). Limited to a qty of 30 units per month Limited to a qty of 30 units per month 1. The patient must have documented failure or Rx claims with a preferred formulary DPP-4 inhibitor (i.e. Tradjenta, Jentadueto). DOSE OPTIMIZATION ONLY NOTE: System edits apply for prescription claims submitted for more than once daily dosing. 1. Patient has a documented contraindication to a comparable preferred formulary insulin (i.e. Humulin and Humalog products), 128 These criteria apply to all HealthPlus Commercial HMO lines of business except as noted, and may also apply to PPO benefits. HEALTHPLUS COMMERCIAL/MEDICARE (NON-PART D)/PPO/TPA/MICHILD DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D DRUG/CATEGORY Diabetes, continued Glucose Test Strips Freestyle Lite® Freestyle Insulinx® Precision Xtra® Erectile Dysfunction ALL Oral Formulary: Cialis 10, 20MG® (tadalafil) Viagra® (sildenafil) QTY LIMIT Limited qty of 150 units per 30 days or 450 units per 90 days CRITERIA DOSE OPTIMIZATION ONLY All ED meds are limited to a qty of 6 units per month PRIOR AUTHORIZATION IS ONLY REQUIRED IN THE FOLLOWING INSTANCES: 1. If the patient <35, the patient must have a documented diagnosis of ED OR a history of ED with contributing OR concomitant disease state. 2. If the patient has a history of nitrate use, and the physician is prescribing Cialis, Levitra, or Viagra: Criteria: a. The physician must submit a written request stating that the patient is no longer using nitrates. **Request must be on physician letterhead with physician's signature** ALL Oral Non-Formulary with PA: Levitra® (vardenafil) Staxyn® (vardenafil) Stendra® (avanafil) ED meds are covered for males only. Limit 6 units per 30 days (for all ED drugs combined). All ED meds are limited to a qty of 6 units per month Genitourinary Medications Detrol LA® (tolterodine, long-acting) Ditropan XL® (oxybutynin, sust. release) Enablex® (solifenacin) Toviaz® (fesoterodine) Vesicare® (darifenacin hydrobromide) Limited to a qty of 30 units per month 1. The patient must have documented failure or Rx claims for both sildenafil (Viagra) AND tadalafil (Cialis) in the past 180 days. 2. If the patient <35, the patient must have a documented diagnosis of ED OR a history of ED with contributing OR concomitant disease state. The prescription must be written by a PCP or in plan urologist (this does not apply to PPO members). 3. Prior Authorization is also required if patient has a history of nitrate use. DOSE OPTIMIZATION ONLY NOTE: System edits apply for prescription claims submitted for more than once daily dosing. ALL Non-Oral Non-Formulary: Caverject®, Edex®, Muse® (alprostadil) ED meds are covered when written by PCP or in-plan urologist. Males Only. Limit 6 units per 30 days (for all ED drugs combined). 129 These criteria apply to all HealthPlus Commercial HMO lines of business except as noted, and may also apply to PPO benefits. HEALTHPLUS COMMERCIAL/MEDICARE (NON-PART D)/PPO/TPA/MICHILD DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D DRUG/CATEGORY Genitourinary Medications, continued Cialis 2.5, 5MG® (tadalafil) Myrbetriq® (mirabegron) QTY LIMIT Limited to 30 tablets per month for indication of BPH **No addl qty of drugs for ED approved when receiving Cialis daily for BPH Limited to a qty of 30 units per month CRITERIA 1. The patient must have a chart documented diagnosis of benign prostatic hyperplasia (BPH); AND 2. The patient must have documented failure or contraindication to at least one formulary alternative from either of the following classes of medication: a. Alpha-1 Adrenergic Blockers (i.e., alfuzosin, doxazosin, tamsulosin, or terazosin) b. 5-Alpha Reductase Inhibitors (i.e., finasteride or Avodart); AND 3. If the patient has a history of nitrate use a. The physician must submit a written request on physician letterhead stating that the patient is no longer using nitrates; AND b. The physician must hand-sign the request. 1. Patient must have chart documented treatment failure or intolerance to at least 2 generic formulary alternatives for overactive bladder (i.e., oxybutynin, tolterodine, trospium chloride). Rapaflo® (silodosin) 1. The patient must have documented failure based on chart documentation or Rx claims for a generically available alpha1blocker indicated for BPH (i.e., generic Cardura, Hytrin or Flomax). HIV Medications All Products Containing Abacavir Epzicom® (abacavir sulfate/lamivudine) Triumeq® (abacavir/ dolutegravir/lamivudi) Trizivir® (abacavir sulfate/ lamivudine/zidovudine) Ziagen® (abacavir) All Products Containing Rilpivirine Complera® (emtricitabine/rilpivirine/ tenofovir) Edurant® (rilpivirine) 1. The patient has been screened for the HLA-B*5701 allele with a negative test result. New Starts Only 1. The patient has a HIV-1 RNA level less than or equal to 100,000 copies/mL; AND 2. The patient has a confirmed CD4+ count greater than or equal to 200 cells/mm3. Note: Duration of prior authorization approval is limited to 12 months New Starts Only 130 These criteria apply to all HealthPlus Commercial HMO lines of business except as noted, and may also apply to PPO benefits. HEALTHPLUS COMMERCIAL/MEDICARE (NON-PART D)/PPO/TPA/MICHILD DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D DRUG/CATEGORY QTY LIMIT HIV Medications, continued Protease Inhibitors darunavir® (Prezista) saquinavir® (Invirase) tipranavir® (Aptivus) CRITERIA 1. Patient is concomitantly receiving the boosting agent ritonavir (Norvir tablets or capsules), AND 2. Pharmacy submits the claims for the boosting agent and the protease inhibitor on the same day according to the required protocol. New Starts Only Note: 1. A pharmacy must first submit, and receive, an adjudicated claim for the boosting agent ritonavir (Norvir Tablets or Capsules). 2. Once the ritonavir claim is accepted, the pharmacy may then submit a claim for the prescribed protease inhibitor. 3. Claims must be submitted on the same day. If Norvir is reversed, accompanying PI must also be reversed. If submitted out of order, the pharmacy will receive a message stating “Norvir boosting required for his agent. Please submit ritonavir (Norvir) prior to adjudicating the primary protease inhibitor”. Selzentry® (maraviroc) 1. The patient has had a coreceptor tropism assay confirming the presence of only CCR5 tropic HIV-1 virus. New Starts Only Truvada® (emtricitabine/tenofovir disoproxil fumarate) Limited to a qty of 30 units per month DOSE OPTIMIZATION ONLY NOTE: System edits apply for prescription claims submitted for more than once daily dosing Infertility All medications for infertility (subject to the member’s benefit). Confirmation of Coverage: 1. The patient’s benefit includes coverage for infertility, AND 2. There is an appropriate referral, if applicable, AND 3. The service/procedure is a covered benefit. All Human Chorionic Gonadotropin Products Novarel® (chorionic gonadotropin) Ovidrel® (choriogonadotropin alfa) Pregnyl® (chorionic gonadotropin) 1. Patient must have documentation of an FDA-approved indication (i.e., prepubertal cryptorchidism, hypogonadotropic hypogonadism, or anovulation in females with infertility). Note: All Human Chorionic Gonadotropin products are included in the Mandatory Specialty Program. 131 These criteria apply to all HealthPlus Commercial HMO lines of business except as noted, and may also apply to PPO benefits. HEALTHPLUS COMMERCIAL/MEDICARE (NON-PART D)/PPO/TPA/MICHILD DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D DRUG/CATEGORY Migraine Medications Axert® (almotriptan) Frova® (frovatriptan) Treximet® (sumatriptan/naproxen) QTY LIMIT All triptans combined are limited to a qty of 9 tablets per month Cambia® (diclofenac potassium) Imitrex Injection® (sumatriptan injection) Sumavel® (sumatriptan injection) Imitrex Nasal Spray® (sumatriptan) Zomig Nasal Spray® (zolmitriptan) CRITERIA 1. The patient must have documented failure or Rx claims for all formulary alternatives (i.e., Relpax, and generic Amerge, Imitrex, Maxalt and Zomig), or formulary alternatives must be inappropriate with chart documentation provided. NOTE: Formulary triptans are limited to nine tablets (cumulative with all oral products) CRITERIA FOR MORE THAN NINE TABLETS PER MONTH 1. Patient is currently receiving medication therapy for the prophylaxis of migraines based on Rx claims in the past 120 days and still requires more than nine tablets per month, OR 2. Patient has had documented failure of all options for migraine prophylaxis and still requires more than nine tablets per month. 1. The patient must have a diagnosis of migraine headaches; AND 2. The patient must have documented failure or Rx claims for generic diclofenac; AND 3. The patient must have documented failure or Rx claims for at least one additional non-steroidal anti-inflammatory drug (i.e., ibuprofen, naproxen sodium). All injectable sumatript an products limited to 6 injections for 30 days All injectable sumatript an products limited to 6 injections for 30 days Criteria for more than 6 injections per month 1. Patient is currently receiving medication therapy for the prophylaxis of migraines based on Rx claims in the past 120 days and still requires more than 6 injections per month, OR 2. Patient has had documented failure or contraindication to all options for migraine prophylaxis and requires more than 6 injections per month. All nasal triptan products are limited to a quantity of 6 per month Criteria for more than 6 units per month 1. Patient is currently receiving medication therapy for the prophylaxis of migraines based on Rx claims in the past 120 days and still requires more than 6 units per month, OR 2. Patient has had documented failure or contraindication to all options for migraine prophylaxis and requires more than 6 units per month. 1. The patient must have documented failure or prescription claims for generic Imitrex injection. Criteria for more than 6 injections per month 1. Patient is currently receiving medication therapy for the prophylaxis of migraines based on Rx claims in the past 120 days and still requires more than 6 injections per month, OR 2. Patient has had documented failure or contraindication to all options for migraine prophylaxis and requires more than 6 injections per month. 132 These criteria apply to all HealthPlus Commercial HMO lines of business except as noted, and may also apply to PPO benefits. HEALTHPLUS COMMERCIAL/MEDICARE (NON-PART D)/PPO/TPA/MICHILD DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D DRUG/CATEGORY All Non-Injectable Dihydroergotamine Products Migranal® (dihydroergotamine) – including generics All Brand Ergotamine Products Cafergot® (ergotamine/caffeine tablets) Migergot® (ergotamine/caffeine rectal suppositories) QTY LIMIT 8 units (ml) per month 40 tabs per 30 days OR 20 supps per 30 days CRITERIA 1. The patient must have a diagnosis of migraine headaches; AND 2. The patient must have chart documented failure or prescription claims for an oral generic triptan medication (i.e. generic Imitrex, Maxalt, Zomig, Amerge); AND 3. The patient must have chart documented failure or prescription claims for generic Imitrex nasal spray or injection; OR 4. The patient has a chart documented contraindication or intolerance to triptan medications. Criteria for more than 8 units per month 1. Patient is currently receiving medication therapy for the prophylaxis of migraines based on Rx claims in the past 120 days and still requires more 8 units per month. 2. Patient has had documented failure of all options for migraine prophylaxis and still requires more than 8 units per month. 1. The patient must have a diagnosis of migraine headaches; AND 2. The patient must have chart documented failure or prescription claims for an oral generic triptan medication (i.e. generic Imitrex, generic Amerge); AND 3. The patient has a chart documented contraindication or intolerance to triptan medications. Muscle Relaxants Amrix® (cyclobenzaprine ext release) 1. The patient must try and fail an adequate course of therapy with at least two generic prescription muscle relaxants (i.e., Flexeril, Norflex, Robaxin, Skelaxin). Miscellaneous Brisdelle® (paroxetine) 1. The patient must have documented failure and Rx claims for generic paroxetine; AND 2. The patient is not currently taking any other serotonin modulating antidepressant (i.e., SSRIs or SNRIs) Cardura XL® (doxazosin mesylate ext. release) 1. The patient must have documented failure or Rx claim in the past year for a generically available alpha 1-adrenergic antagonist (i.e., Cardura, Flomax or Hytrin). 133 These criteria apply to all HealthPlus Commercial HMO lines of business except as noted, and may also apply to PPO benefits. HEALTHPLUS COMMERCIAL/MEDICARE (NON-PART D)/PPO/TPA/MICHILD DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D DRUG/CATEGORY Miscellaneous, continued Grastek® (timothy grass pollen allergen extract) Oralair® (mixed pollens allergen extract) Ragwitek® (short ragweed pollen allergen extract) QTY LIMIT Limited to a qty of 30 units per month Lyrica® (pregabalin) Nuvigil® (armodafinil) Xyrem® (sodium oxybate) Qty is limited to 30 units per 30 days Quantity limit of 540mls every 30 days CRITERIA 1. The prescriber must be an allergist and administer the first dose under supervision; AND 2. The patient must have chart documentation of a positive skin test or in-vitro testing for pollen-specific IgE antibodies for the allergens containedin the product; AND 3. Patient must have a chart documented trial of at least one nasal steroid (i.e., Flonase, flunisolide, Nasacort AQ ) and one non-sedating antihistamine (i.e., Claritin, Zyrtec, Allegra); AND 4. There are claims for an epinephrine auto-injector within the past 6 months; AND 5. For Ragwitek and Grastek, treatment will be initiated 12 weeks prior to the expected onset of the allergen season and continued throughout the season; OR 6. For Oralair, treatment will be initiated 16 weeks prior to the expected onset of the allergen season and continued throughout the season. Ragwitek and Grastek: authorization will approved for 24 weeks per calendar year. Oralair: authorization will be approved for 28 weeks per calendar year. Note: The authorization approvals are based on a 12 week allergy season. DOSE OPTIMIZATION ONLY Quantity limits/dose optimization: 1. The 25, 50, 75, 100, 150 and 200mg capsules are limited to a quantity of 90 per month. 2. The 225 and 300mg capsules are limited to a quantity of 60 per month. 1. The patient has a documented diagnosis of narcolepsy, or excessive daytime sleepiness associated with obstructive sleep apnea/hypopnea syndrome (OSAHS) or shift work sleep disorder (SWSD). 1. The patient is 16 years of age or older AND 2. The patient has documented sleep study results resulting in a diagnosis of narcolepsy and has one of the following: a. Episodes of cataplexy demonstrated by chart documentation, OR b. Excessive daytime sleepiness with symptoms that limit the ability to perform normal daily activities demonstrated by chart documentation and: i. Provigil or Nuvigil therapy has been ineffective or contraindicated AND ii. Methylphenidate, amphetamine salts, or dextroamphetamine therapy has been ineffective or contraindicated AND 3. The patient is not being treated with a sedative hypnotic agent AND 4. The patient does not have a succinic semialdehyde dehydrogenase deficiency AND 5. The patient does not have a history of substance abuse. 134 These criteria apply to all HealthPlus Commercial HMO lines of business except as noted, and may also apply to PPO benefits. HEALTHPLUS COMMERCIAL/MEDICARE (NON-PART D)/PPO/TPA/MICHILD DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D DRUG/CATEGORY QTY LIMIT Miscellaneous, continued Rayos® (prednisone delayed release tablets) On Formulary with PA: Revatio® (sildenafil) Non-Formulary with PA: Adcirca® (tadalafil) On Formulary with PA: Savella® (milnacipran) Uloric® (febuxostat) Neurological Miscellaneous Horizant® (gabapentin enacarbil) Limited to a qty of 30 units per month Limited to a qty of 30 units per 30 days. Gralise® (gabapentin) Nuedexta® (dextromethorphan/quinidine) Limited to a qty of 60 units per 30 days. CRITERIA 1. The patient must have a documented diagnosis of rheumatoid arthritis; AND 2. The patient must have documented failure and Rx claims for 2 generically available oral corticosteroids (i.e., prednisone, methylprednisolone). 1. The patient must have a documented diagnosis of pulmonary arterial hypertension. 2. If the patient has a history of nitrate use, the physician must submit a written request on his/her letterhead stating that the patient is no longer using nitrates. 1. The patient must have a documented diagnosis of fibromyalgia, OR 2. Documentation of all of the following: a. Widespread pain for at least 3 months, AND b. Pain on both sides of the body, above and below the waist, AND c. Abnormal tenderness in at least 11 of the 18 anatomicallydefined body sites. 1. Patient must have documented failure or prescription claims with allopurinol, OR 2. The patient cannot tolerate therapeutic doses or is not an appropriate candidate for allopurinol based on documentation provided. 1. The patient must have a diagnosis of restless legs syndrome, AND 2. The patient must have documented failure and Rx claims with generic Neurontin, AND 3. The patient must have documented failure or Rx claims with generic Requip or generic Mirapex. 1. The patient must have a documented diagnosis of postherpetic neuralgia, AND 2. The patient must have documented failure and Rx claims with generic Neurontin, AND 3. The patient must have documented failure or Rx claims with a generic tricyclic antidepressant. 1. The patient must have a documented diagnosis of pseudobulbar affect; AND 2. The patient must be 18 years or older; AND 3. Patient is not currently receiving quinidine, quinine, mefloquine, an MAOI, or any drug that prolongs QT interval and is metabolized by CYP2D6 (e.g., thioridazine or pimozide); AND 4. Patient must have recent (within the past three months) platelet count, liver function panel, and ECG if patient has left ventricular dysfunction/hypertrophy. Prior authorizarion requests are approved for a 6 month duration. 135 These criteria apply to all HealthPlus Commercial HMO lines of business except as noted, and may also apply to PPO benefits. HEALTHPLUS COMMERCIAL/MEDICARE (NON-PART D)/PPO/TPA/MICHILD DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D DRUG/CATEGORY NSAIDs Arthrotec® (diclofenac/misoprostol) Naprelan CR® (naproxen sodium) QTY LIMIT All Cox-2 drugs and Mobic are limited to a qty of 30 units per month CRITERIA 1. Documented indication for acute or chronic treatment of the signs and symptoms of osteoarthritis or rheumatoid arthritis, AND 2. The patient must have documented failure or Rx claims for an adequate course of therapy with at least two generic prescription NSAID agents (e.g., ibuprofen, naproxen, piroxicam, ketoprofen, diclofenac, etc.). Adequate course of therapy is defined as a full therapeutic dose on a scheduled basis for at least 1-2 weeks; OR 3. The patient is identified as "high risk" for developing GI complications: a. Age over 60 years old AND any one of the following risks: b. Requiring prolonged use of max dose of traditional NSAIDS OR c. Concomitant use of steroids OR d. Documented history of ulcer/bleed/perforation, OR 4. Active ulcer or recent documented history of ulcer (within months) on history of GI bleed/perforation. Duexis® (ibuprofen/famotidine) 1. The patient must have a documented diagnosis of arthritis; AND 2. The patient must be high risk for developing GI complications: a. Documentation or Rx claims for concomitant use of steroids, DMARDs, or anticoagulants b. Documentation of active or previous ulcer/bleed/perforation c. Documentation of platelet dysfunction or coagulopathy; AND 3. The patient must have chart documented failure or Rx claims for both ibuprofen 800 mg and famotidine 20 mg in the past month. Vimovo® (esomeprazole/naproxen) 1. The patient must have a documented diagnosis of arthritis, AND 2. The patient must be high risk for developing GI complications: a. Documentation or Rx claims for concomitant use of steroids, DMARDs, or anticoagulants b. Documentation of active or previous ulcer/bleed/perforation c. Documentation of platelet dysfunction or coagulopathy 3. The patient must fail all formulary proton pump inhibitor alternatives (i.e., Omeprazole, generic Aciphex, generic Prevacid, generic Protonix) in combination with generic naproxen. 136 These criteria apply to all HealthPlus Commercial HMO lines of business except as noted, and may also apply to PPO benefits. HEALTHPLUS COMMERCIAL/MEDICARE (NON-PART D)/PPO/TPA/MICHILD DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D DRUG/CATEGORY QTY LIMIT CRITERIA NSAIDs, continued Flector® (diclofenac epolamine transdermal patch) 1. The patient must have documented failure or Rx claims for an adequate course of therapy with at least two generic prescription NSAID agents (e.g., ibuprofen, naproxen, piroxicam, ketoprofen, diclofenac, etc.). Adequate course of therapy is defined as a full therapeutic dose on a scheduled basis for at least 1-2 weeks; OR 2. The patient is identified as "high risk" for developing GI complications: a. Age over 60 years old AND any one of the following risks: b. Requiring prolonged use of max dose of traditional NSAIDS OR c. Concomitant use of steroids OR d. Documented history of ulcer/bleed/perforation, OR 3. Active ulcer or recent documented history of ulcer (within 6 months) or history of GI bleed/perforation. Voltaren Gel® (diclofenac sodium) 1. The patient must have documented failure or Rx claims for an adequate course of therapy with at least two generic prescription NSAID agents (e.g., ibuprofen, naproxen, piroxicam, ketoprofen, diclofenac, etc.). All Oral Brand Diclofenac Products Zipsor® (diclofenac potassium) Zorvolex® (diclofenac) 1. The patient must have documented failure or Rx claims for an adequate course of therapy with at least two generic prescription NSAID agents (e.g., ibuprofen, naproxen, piroxicam, ketoprofen, diclofenac, etc.), and one must be generic Voltaren. Adequate course of therapy is defined as a full therapeutic dose on a scheduled basis for at least 1-2 weeks. Ophthalmic Products All Brand Topical Ophthalmic Antihistamines On Formulary with PA: Patanol® (olopatadine) 1. The patient must have documented failure or Rx claim for generic OTC Zaditor in the past 90 days (covered with written prescription). 2. If the patient fails treatment with generic OTC Zaditor, then Patanol is the second-line formulary alternative with prior authorization required. 3. The patient must have documented failure or Rx claims for the formulary alternatives (OTC Zaditor and Patanol) before a nonformulary drug will be approved. Non-Formulary with PA: Alocril® (nedocromil sodium) Alomide® (lodoxamide tromethamide) Bepreve® (bepotastine besilate) Emadine® (emedastine difumarate) Lastacaft® (alcaftadine) Pataday® (olopatadine) Restasis® (cyclosporine) Betimol® (timolol) Istalol® (timolol maleate) Qty is limited to 2 units per day QUANTITY LIMITS ONLY 1. The patient must have documented failure or Rx claim for generic Timolol (i.e., Timoptic). 137 These criteria apply to all HealthPlus Commercial HMO lines of business except as noted, and may also apply to PPO benefits. HEALTHPLUS COMMERCIAL/MEDICARE (NON-PART D)/PPO/TPA/MICHILD DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D DRUG/CATEGORY Ophthalmic Products, continued All Brand Topical Ophthalmic Prostaglandin Analogs On Formulary with PA: Lumigan 0.01%® (bimatoprost) Non-Formulary with PA: Lumigan 0.03%® (bimatoprost) Travatan Z® (travoprost) Zioptan® (tafluprost) Proton Pump Inhibitors On Formulary with PA: Esomeprazole Strontium® (esomeprazole strontium) Non-Formulary with PA: Aciphex Sprinkle® (rabeprazole) Dexilant® (dexlansoprazole) First-Lansoprazole® (lansoprazole) First-Omeprazole® (omeprazole) Nexium® (esomeprazole) Prevacid Solutab® (lansoprazole) Prilosec DR Susp® (omeprazole magnesium) Protonix Pak® (pantoprazole) Zegerid Susp® (omeprazole/sodium bicarbonate) Sleeping Aids Edluar SL® (zolpidem) Intermezzo® (zolpidem) Rozerem® (ramelteon) Silenor® (doxepin) Zolpimist® (zolpidem) Ambien/CR® (zolpidem) Restoril® (temazepam) Sonata® (zaleplon) Substance Abuse Bunavail® (buprenorphine/ naloxone) Suboxone® 12-3mg, 4-1mg (buprenorphine/naloxone) QTY LIMIT Zioptan is limited to a qty of 1 unit per day CRITERIA 1. The patient must have documented failure or prescription claims for a generic prostaglandin analog (i.e., generic Xalatan). 2. If the patient fails treatment with all generic prostaglandin analogs, then Lumigan 0.01% is the second-line formulary alternative with prior authorization required. 3. The patient must have documented failure or prescription claims for all formulary alternatives (generic Xalatan AND branded Lumigan 0.01%) before a non-formulary brand drug will be approved. Brand PPIs are limited to a qty of 30 tabs/caps per month 1. The patient must have documented failure or Rx claims for 4 generic proton pump inhibitors (PPI) before a non-formulary PPI will be approved, AND 2. Specifically for Nexium and esomeprazole strontium, the patient must have a current documented diagnosis of Barrett's Esophagus, Zollinger-Ellison or Erosive Esophagitis. Approved automatically for children under 2 years of age. 3. Specifically for Dexilant, the patient must have a current documented diagnosis of Erosive Esophagitis; OR if the patient is currently taking clopidogrel, they must have documented failure or Rx claims for both pantoprazole and lansoprazole. Specifically for liquid or soluble preparations: 1. The patient must have a documented inability to swallow a solid dosage form. Quantity is limited to 30 per month 1. If there is no contraindication present, the patient must have documented failure or Rx claim(s) for three generically available sleeping agents (e.g., Ambien, Desyrel, Halcion, Prosom, Restoril or Sonata). 2. If a contraindication to benzodiazepines is present, the patient must try and fail an adequate course of therapy with generic Ambien AND Sonata. NOTE: Limited to1 unit per day. Prior Authorization for more than 1 unit per day is based on a specific review of medical necessity. QUANTITY LIMITS ONLY NOTE: Limited to 1 unit per day. Prior Authorization is only required for quantities that exceed the limit, and is based on a specific review of medical necessity. QUANTITY LIMITS ONLY NOTE: Limited to 2 units per day 138 These criteria apply to all HealthPlus Commercial HMO lines of business except as noted, and may also apply to PPO benefits. HEALTHPLUS COMMERCIAL/MEDICARE (NON-PART D)/PPO/TPA/MICHILD DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D DRUG/CATEGORY QTY LIMIT CRITERIA Substance Abuse, continued Suboxone® 2-0.5mg, 8-2mg (buprenorphine/naloxone) Subutex® (buprenorphine) Zubsolv® (buprenorphine/ naloxone) QUANTITY LIMITS ONLY NOTE: Limited to 3 units per day Inflammatory Bowel Disease All Branded Non-Formulary Oral Agents Dipentum® (olsalazine sodium) Giazo® (balsalazide) Lialda® (mesalamine) Uceris® (budesonide) 1. The patient must have documented failure or Rx claims for at least two formulary agents (e.g., generic Azulfidine, Colazal, or Asacol) in the past year. Canasa® (mesalamine) New Starts Only Limited to a qty of 30 units per month DOSE OPTIMIZATION ONLY NOTE: System edits apply for prescription claims submitted for more than once daily dosing. 139 These criteria apply to all HealthPlus Commercial HMO lines of business except as noted, and may also apply to PPO benefits. HEALTHPLUS COMMERCIAL/MEDICARE (NON-PART D)/PPO/TPA/MICHILD DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D DRUG/CATEGORY Weight Management All medications for the treatment of obesity Examples: Adipex® (phentermine) Belviq® (lorcaserin) Bontril 105mg® (phendimetrazine tartrate) Bontril PDM 35mg® (phendimetrazine tartrate) Diethylpropion® (diethylpropion) Qsymia® (phentermine/ topiramate) Suprenza® (phentermine) Xenical® (orlistat) QTY LIMIT CRITERIA 1. The patient is an adult ≥ 18 years of age; AND 2 2. The patient has a body mass index (BMI) of >30kg/m , OR 2 3. The patient has a body mass index (BMI) of >27kg/m with any of the following co-morbidities: -established coronary heart disease -atherosclerotic disease -type 2 diabetes -sleep apnea, OR 2 4. The patient has a body mass index (BMI) of >27kg/m , A. With at least three of the following risk factors: -hypertension -high LDL cholesterol -low HDL cholesterol -impaired fasting glucose -smoking -family history of early cardiovascular disease -age >45 years for men or age >55 years for women, AND B. The patient has undergone evaluation to rule out other treatable causes of obesity, not presence of malabsorption syndrome, thyroid conditions, cholestasis, pregnancy, and/or lactation, AND C. There has been a previous weight loss attempt for at least 6-12 months within one (1) year through a physician-supervised diet and exercise program consisting of low calorie diet, AND D. The patient has a strong desire, willingness and cognitive ability to make changes in diet and activity level, AND E. The medication is part of a continued treatment plan, which includes a calorie and fat reduced diet and a regular exercise program. AND 5. If the medication is a brand name product, the patient must have tried a generically available product (i.e. phentermine, diethylpropion) in the past year. If the preceding criteria are met, the request for a weight loss medication will be approved for 1 year (365 days) of total coverage. 140 These criteria apply to all HealthPlus Commercial HMO lines of business except as noted, and may also apply to PPO benefits. HEALTHPLUS COMMERCIAL/MEDICARE (NON-PART D)/PPO/TPA/MICHILD DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D DRUG/CATEGORY Non-Sterile Compounded Prescriptions Non-Formulary with PA QTY LIMIT CRITERIA 1. The compounded product contains at least one FDA-approved prescription ingredient; AND 2. Each prescription drug or active ingredient in the compounded product is approved by the Food & Drug Administration (FDA) for medical use in the United States; AND 3. The active prescription medication component(s) are in therapeutic amounts; AND 4. The compounded product is not a copy of any commercially available FDA-approved drug product; AND 5. The use for which the compounded product is being prescribed is supported by FDA approval of the active ingredient(s), or is supported by two or more articles from peer reviewed journals demonstrating the safety and efficacy of the prescribed therapy for that diagnosis and method or route of delivery; AND 6. If any prescription ingredient in the compounded product is included in the HealthPlus Prior Authorization program, the patient must meet the criteria designated for that prescription ingredient. Based on limitations or exclusions in the subscriber certificate, coverage will NOT be provided for compounds under the following circumstances: 1. Any compound that does not contain a FDA-approved prescription ingredient otherwise covered by the plan; OR 2. Any compound that contains a non-FDA approved or nonHealthPlus covered prescription ingredient. 3. Compounded formulations that contain any bulk powders that are not FDA approved or HealthPlus approved; OR 4. Compounded formulations that are being used for cosmetic purposes; OR 5. Compounded formulations that are using prescription ingredients for non-FDA approved indications or purposes that are not supported by peer-reviewed literature; OR 6. Compounded formulations that may be considered investigational or experimental; OR 7. Compounded formulations that use drugs withdrawn or removed from the market for safety reasons; OR 8. Prescription ingredient(s) compounded for the purpose of convenience only. a. Exceptions include: i. Compounded medications for those patients that cannot swallow or have trouble swallowing and require administration with an oral liquid, or administration by topical, rectal or other appropriate non-oral routes; ii. Compounded medications for those patients who have sensitivity to dyes, preservatives, or fillers in commercial products and require allergy-free medications as documented in the medical record; iii. Compounded medications for children who require prescription medications for which there are no liquid formulations available. 141 These criteria apply to all HealthPlus Commercial HMO lines of business except as noted, and may also apply to PPO benefits. HEALTHPLUS COMMERCIAL/MEDICARE (NON-PART D)/PPO/TPA/MICHILD DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D DRUG/CATEGORY QTY LIMIT Dispense as Written DAW Specific request for a brand name product when a generic is available CRITERIA 1. The benefit covers generic products when a generically equivalent product is available. 2. In general, prior authorization is required for all brand name drugs (when the drug is available and covered as a generic medication). The physician may submit a prior authorization request form for the brand name drug (when a generic equivalent is available), but this must be substantiated by medical necessity. If medical necessity is based on a trial and failure of the generic medication, a prescription claim for the generic drug must be present or chart notes documenting the failure must be provided. 3. If a physician submits a prior authorization request form for coverage of a brand name drug (when a generic equivalent is available), the request is reviewed through the same process as all other drugs that require prior authorization. 4. The member may still choose to receive a brand product without medical necessity, but would be responsible for additional costs based on their benefit (i.e., the difference in cost between the brand and generic product plus their usual copayment; or, a higher copayment). 1. The physician must provide documentation of the clinical rationale for requesting a dosage, quantity, or duration of medication greater than the criteria specified in the formulary. 2. If the dosage exceeds the manufacturer product labeling/prescribing information, the physician must submit documentation of two articles from peer reviewed journals demonstrating the safety and efficacy of the prescribed therapy. Quantity Limit QL Specific request for a dose, quantity or duration that exceeds the established limits Medical Exception Requests Signature PPO Closed Formulary/or Specific Excluded Non-Formulary Drugs DRUG/CATEGORY Exceptions Criteria (for all non-formulary drugs in a closed formulary) QTY LIMIT CRITERIA 1. Based on specific documented patient circumstances, each/all of the formulary drugs/alternatives are not appropriate because: a. Medication(s) are contraindicated or unsafe, or b. Patient is intolerant or allergic, or c. Patient had an inadequate or inappropriate response; AND 2. Chart documentation to support this medical necessity has been provided; AND 3. The requested drug and dosage is FDA-approved for the patient’s diagnosis; AND 4. If established (commercial) HealthPlus prior authorization criteria exists, the prior authorization criteria will also apply. 142 These criteria apply to all HealthPlus Commercial HMO lines of business except as noted, and may also apply to PPO benefits. HEALTHPLUS COMMERCIAL/MEDICARE (NON-PART D)/PPO/TPA/MICHILD DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D HEALTHPLUS OF MICHIGAN High Risk Medications in the Elderly (≥66 years old) HealthPlus Commercial/Medicare (non-Part D)/PPO/TPA Based on the availability of safer alternatives, the following medications have been added to the Prior Authorization Program for members 66 years of age and older for HealthPlus Commercial/Medicare (non-Part D) and PPO with the following criteria: 1) The recommended alternative treatment(s) are not appropriate, are contraindicated or are unsafe for the patient based on specific documented patient circumstances, OR 2) The patient has a documented trial and failure (or prescription claims) for the recommended alternative treatment(s). Name Concern Estrogens – all oral and topical patches only (Premarin, estradiol, Estratest, Vivelle-Dot, etc.) Promethazine (Phenergan) – including all combinations Promethazine w/ Codeine Evidence of breast/Endometrial cancer; No cardio or cognitive protection in older women Nitrofurantoin (Macrodantin) Nephrotoxicity Thyroid USP (Armour Thyroid, Desiccated) Glyburide (Micronase) Cardiac adverse effects Anticholinergic effects (i.e., urinary retention, confusion, sedation) Alternative Treatment Hot flashes: non-pharmacological therapy, Zoloft, Paxil, Effexor 2 Bone density: Calcium with vitamin D , Fosamax, 1 1 Boniva , Evista 1,2 2 Antihistamine: Claritin , Zytrec 1 Antiemetic: Antivert, Zofran Cough: Dextromethorphan Depends on site of infection, culture, and sensitivity. 1 Bactrim, Vibramycin, Azithromycin, Fluoroquinolone Levothyroxine (LT4): Synthroid, Levoxyl Associated with an increased risk of hypoglycemia compared to other agents Diabetes: Glucotrol, Amaryl, Metaglip Hydroxyzine (Vistaril, Atarax) Anticholinergic effects, urinary retention, confusion, sedation Antihistamine: Claritin , Zyrtec Carisoprodol (Soma) Anticholinergic effects, sedation, cognitive impairment, weakness, urinary retention Physiotherapy: correct seating & footwear Spasticity: Baclofen, Zanaflex. Treat underlying problems Glyburide-Metformin (Glucovance) Chlorpropamide (Diabinese) Cyclobenzaprine (Flexeril) 2 2 Orphenadrine (Norflex) Chlorzoxazone (Parafon Forte) Methocarbamol (Robaxin) Skelaxin (Metaxalone) 143 These criteria apply to all HealthPlus Commercial HMO lines of business except as noted, and may also apply to PPO benefits. HEALTHPLUS COMMERCIAL/MEDICARE (NON-PART D)/PPO/TPA/MICHILD DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D Name Amitriptyline (Elavil) Concern Alternative Treatment Highly anticholinergic, sedating, and causes orthostatic hypotension Depression: Zoloft, Paxil, Effexor Trimethobenzamide (Tigan) Extrapyramidal side effects, poor efficacy Nausea: Zofran, Compazine, or Reglan Ketorolac (Toradol) GI bleeding Pain: Tylenol , Motrin , Norco Orthostatic hypotension, poor efficacy For secondary prevention of non-cardioembolic stroke or TIA: Plavix, Aggrenox, Aspirin Imipramine (Tofranil) 2 2 Indomethacin Dipyridamole (Persantine) 1 2 Drug may require prior authorization or may have limited coverage depending on member’s benefit plan Available OTC 144 These criteria apply to all HealthPlus Commercial HMO lines of business except as noted, and may also apply to PPO benefits. HEALTHPLUS PARTNERS (MEDICAID) DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D MEDICAID PRIOR AUTHORIZATION CRITERIA CATEGORY/DRUG QTY LIMIT CRITERIA Acne Clindagel® (clindamycin phosphate) All Brand Topical Adapalene and Dapsone Products Aczone 5% Gel® (dapsone) Differin 0.1% Lotion® (adapalene) Epiduo 0.1%-2.5% Gel® (adapalene/benzoyl peroxide) 1. The patient must have documented failure or Rx claim for topical generic clindamycin (e.g., Cleocin T) in the past 90 days. 1. The patient must have documented failure or Rx claim(s) for a generic tretinoin (e.g., Avita, Retin-A) AND a generic adapalene (e.g., Differin gel) All Branded Benzoyl Peroxide Combination Products Acanya 1.2%-2.5% (clindamycin/benzoyl peroxide) Benzamycin Pak 3%-5% Gel® (erythromycin base/benzoyl peroxide) 1. Patient must have documented failure or Rx claim(s) for a generic combination product in the past 90 days (i.e., GEQ Benzaclin, GEQ Benzamycin). All Tretinoin Products Age Restriction: Patients > 25 years of age must have a documented diagnosis of acne. All Brand Tretinoin Products Atralin® (tretinoin) Retin A Micro 0.8%® (tretinoin) Tretin-X® (tretinoin) Veltin® (tretinoin/clindamycin) Ziana® (tretinoin/clindamycin) Allergy Medications Clarinex® (desloratadine) 1. The patient must have documented failure or Rx claim for a generic tretinoin product (e.g., Retin-A, Avita) in the past 90 days. NOTE: Age restriction for all topical tretinoin products for age > 25 based on a diagnosis of acne. Clarinex-D® (desloratadine/pseudoephedrine) Limited to a qty of 30 units per month for 1. The patient must have documented failure or Rx claims for generic OTC Claritin D OR OTC generic Claritin in combination with OTC generic pseudoephedrine (all are covered with written prescription) in the past year. If the patient fails treatment with a generic OTC Claritin combination, then generic OTC Allegra in combination with pseudoephedrine is the second line alternative. NOTE: Prior authorization is only required for patients over 12 years of age. 145 HEALTHPLUS PARTNERS (MEDICAID) DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D CATEGORY/DRUG Allergy Medications, continued All Brand Nasal Steroids Beconase AQ® (beclomethasone dipropionate) Nasonex® (mometasone furoate) Omnaris® (ciclesonide) Qnasl® (beclomethasone dipropionate) Veramyst® (fluticasone furoate) Zetonna® (ciclesonide) All Brand Nasal Steroids, Combination Products Dymista® (azelastine/fluticasone propionate) Analgesics On Formulary with PA: Actiq® (fentanyl citrate oral transmucosal) Non-Formulary with PA: Abstral® (fentanyl sl) Fentora® (fentanyl citrate buccal tablet) Lazanda® (fentanyl nasal spray) Subsys ® (fentanyl sublingual spray) QTY LIMIT CRITERIA 1. The patient must have documented failure or Rx claims for two generic nasal steroids (i.e., Flonase, flunisolide, Nasacort AQ, Rhinocort Aqua) in the past year. 1. The patient must have documented failure or Rx claims for a generic nasal steroid (i.e., Flonase, flunisolide, Nasacort AQ) in the past year. Abstral, Fentora, Subsys qty-4 units/day 1. The patient has a documented current diagnosis of cancer. 2. The patient is already receiving and is tolerant to opioid therapy for underlying persistent cancer pain. Actiq qty- 4 units/ day NOTE: System will automatically approve if written by an oncologist (or if there are prescription claims for chemotherapy-related medications) and the patient is receiving opioid pain medications. Lazanda qty1 bottle (5ml)/day Abstral, Lazanda and Subsys– New Starts Only DOSE OPTIMIZATION ONLY NOTE: System edits apply for prescription claims with a monthly quantity that exceeds the MAX recommended dose of 4gm/day of acetaminophen. Physician must submit signed request stating that he/she is allowing the patient to exceed the MAX recommended dose of acetaminophen. All acetaminophen-containing narcotic analgesics Duragesic Patches® (fentanyl) Qty limit of 15 patches per 30 days OxyContin® (oxycodone) Qty is limited to 3 units per day NOTE: System will automatically approve if written by an oncologist or if there are prescription claims for chemotherapy-related medications. For indications other than cancer: 1. The patient must have documented failure or prescription claims for at least two formulary alternatives (including generic MS Contin, and short-acting narcotic analgesic) OR 2. Based on chart documentation, all formulary alternatives are inappropriate. 1. The patient must have a current documented diagnosis of active cancer. NOTE: System will automatically approve if written by an oncologist (or if there are prescription claims for chemotherapy-related medications) and the patient is receiving opioid pain medications. 146 HEALTHPLUS PARTNERS (MEDICAID) DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D CATEGORY/DRUG Analgesics, continued Avinza® (morphine sulfate) QTY LIMIT Qty is limited to 30 units per 30 days CRITERIA 1. The patient must have a current documented diagnosis of active cancer. NOTE: System will automatically approve if written by an oncologist or if there are previous claims for chemotherapyrelated medications. Oxycodone/Ibuprofen QUANTITY LIMITS ONLY NOTE: Limited to 28 units per 30 days Stadol NS® (butorphanol) QUANTITY LIMITS ONLY NOTE: Limited to 2 bottles (5ml) per 30 days Ultracet® (tramadol/acetaminophen) Ultram® (tramadol) Ultram ER® (tramadol) QUANTITY LIMITS ONLY NOTE: Limited to 8 units per day Butrans® (buprenorphine patch) QUANTITY LIMITS ONLY NOTE: Limited to 1 unit per day Qty is limited to 4 units per 28 days For indications other than cancer: 1. The patient must have documented failure or prescription claims for at least two formulary alternatives (including generic MS Contin and short-acting narcotic analgesic) within the last 3 months OR 2. Based on chart documentation, all formulary alternatives are inappropriate. NOTE: System will automatically approve if written by an oncologist or if there are prescription claims for chemotherapyrelated medications. New Starts Only Conzip® (tramadol) QUANTITY LIMITS ONLY NOTE: Limited to 1 unit per day Kadian® (morphine ext. release) QUANTITY LIMITS ONLY NOTE: Limited to 2 units per day MS Contin® (morphine ext. release) QUANTITY LIMITS ONLY NOTE: Limited to 3 units per day Nucynta® (tapentadol) QUANTITY LIMITS ONLY NOTE: Limited to 6 units per day Nucynta ER® (tapentadol) QUANTITY LIMITS ONLY NOTE: Limited to 2 units per day Opana® (oxymorphone) QUANTITY LIMITS ONLY NOTE: Limited to 8 units per day Opana ER (Crush Resistant)® (oxymorphone) Oxymorphone ER (Non-Crush Resistant) (oxymorphone) Rybix ODT® (tramadol) Qty is limited to 3 units per day 1. The patient must have a current documented diagnosis of active cancer. System will automatically approve if written by an oncologist or if there are previous claims for chemotherapy-related medications. NOTE: Prior authorization applies to new start patients only. 1. The patient must have documented failure or Rx claims with generic Ultram in the past 60 days, OR 2. The patient must have documented inability to swallow or absorb oral medications. 147 HEALTHPLUS PARTNERS (MEDICAID) DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D CATEGORY/DRUG QTY LIMIT Analgesics, continued Ryzolt® (tramadol) Exalgo® (extended release hydromorphone) Vicodin 5/300® (hydrocodone/acetaminophen) Vicodin ES 7.5/300® (hydrocodone/acetaminophen) Vicodin HP 10/300® (hydrocodone/acetaminophen) Xartemis XR® (oxycodone/APAP CR) QUANTITY LIMITS ONLY NOTE: Limited to 1 unit per day 8mg, 12mg, 16mg-qty limited to 1 unit per day 32mg-qty limited to 2 units per day Vicodin 5/300 limit 8 tabs/day VIcodin ES 7.5/300 & Vicodin HP 10/300 limit 6 tabs/day 120 tablets per 30 days All Brand Combination Butalbital/Acetaminophen Products Bupap® (butalbital/acetaminophen) Phrenilin/Phrenilin Forte® (butalbital/acetaminophen) All Single Ingredient Hydrocodone Products Zohydro ER® (hydrocodone) CRITERIA Requires prior authorization for indications other than cancer. System will automatically approve if written by an oncologist or if there are previous claims for chemotherapy-related medications. 1. The patient must have documented failure or Rx claims with generic Dilaudid (hydromorphone) and generic Duragesic (fentanyl). 1. Physician must provide chart documentation that shows that a product with 325mg acetaminophen (i.e. generic Norco) is contraindicated in this patient but that a product with 300mg acetaminophen is not contraindicated Note: Acetaminophen is not recommended for patients with liver disease. 1. Patient must have documented failure or Rx claims for both generic Percocet and generic MS Contin in the past 6 months; AND 2. The prescriber must submit a current MAPS report (or similar report) which shows no sign of substance abuse or multiple prescribers of narcotics in the past 6 months; AND 3. The authorization will be approved for 6 months. Renewals require submission of an updated MAPS report confirming no evidence of substance abuse. 1. The patient must have chart documented failure or prescription claims for an oral generic butalbital/acetaminophen product in the past 6 months. Zohydro ER Qty is limited to 2 units per day 1. The patient must have documented failure or Rx claims for both generic MS Contin and generic Duragesic patches in the past 6 months; AND 2. The prescriber must submit a current MAPS report (or similar report) which shows no sign of substance abuse or multiple prescribers of narcotics in the past 6 months; AND 3. The authorization will be approved for 6 months. Renewals require submission of an updated MAPS report confirming no evidence of substance abuse. 148 HEALTHPLUS PARTNERS (MEDICAID) DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D CATEGORY/DRUG QTY LIMIT Androgens All Non-Formulary Testosterone Products Androderm® (testorterone patch) Axiron® (testosterone solution) Striant® (testosterone buccal) Non-Formulary Oral Methyltestosterone and Fluoxymesterone Products Methitest® (methyltestosterone) Testred® (methyltestosterone) All Non-Formulary Angiotensin II Receptor Blockers Teveten HCT® (eprosartan mesylate) Edarbi® (azilsartan medoxomil) Edarbyclor® (azilsartan medoxomil/chlorthalidone) Antibiotics Oracea® (doxycycline monohydrate) All ARBs except Cozaar (not combos) are limited to a qty of 30 units per month Qty is limited to 30 units per 30 days CRITERIA 1. The patient is male, ≥ 18 years old, and has a documented diagnosis of hypogonadism; AND 2. The patient has a morning (before 11AM) serum total testosterone concentration of less than 300 ng/dL documented on 2 separate occasions in the past year; AND 3. The patient must have documented failure or Rx claims with a preferred formulary testosterone replacement product (i.e., testosterone cypionate/enanthate, AndroGel). 1. The patient is male and has a documented diagnosis of hypogonadism; AND 2. The patient has a morning (before 11AM) serum total testosterone concentration of less than 300 ng/dL documented on 2 separate occasions in the past year; AND 3. The patient must have documented failure or Rx claims with a preferred formulary testosterone replacement product (i.e., testosterone cypionate/enanthate, AndroGel, Android); OR 1. The patient has a documented diagnosis of delayed puberty; AND 2. The patient must have documented failure or RX claims with testosterone cypionate/enanthate or Android; OR 1. The patient is female and has a documented diagnosis of breast cancer 1. The patient must have documented failure or Rx claims for all formulary ARBs or ARB combination products (i.e., Benicar/HCT, or Diovan/HCT). NOTE: If patient is a first time ARB user, patient should have documented failure or Rx claims for at least one generically available ACE inhibitor previous to ARB therapy. 1. The patient must have documented failure or Rx claim(s) for at least one formulary ARB or ARB combination product (i.e., generic Cozaar/Hyzaar, Benicar/HCT or Diovan/HCT). 1. The patient must have documented failure or Rx claim for generic Vibramycin. 149 HEALTHPLUS PARTNERS (MEDICAID) DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D CATEGORY/DRUG QTY LIMIT Antibiotics, continued Dificid® (fidaxomicin) CRITERIA 1. Patient has documented diagnosis of C. difficile associated diarrhea, AND 2. Patient has tried and failed an adequate trial of vancomycin, OR 3. Patient has a contraindication or intolerance to vancomycin, OR 4. Patient has been recently discharged from a hospital or a medical facility and has had documented treatment with Dificid or vancomycin. New Starts Only 1. The patient must have documented failure or Rx claims for a generic topical acne product AND minocycline in the past 60 days. All Brand Minocycline Products Minocin PAC® (minocycline kit) Solodyn® (minocycline ER) Factive® (gemifloxacin) 1. The patient must have documented failure or Rx claim for a generic quinolone (i.e.; ciprofloxacin, levofloxacin) in the past 60 days before any other brand quinolone will be covered. NOTE: Individual requests are reviewed to include consideration of the diagnosis, culture and sensitivity, and other documentation. Flagyl ER® (metronidazole) 1. The patient must have documented failure or Rx claim for generic metronidazole. Tobi Solution/Podhaler 1. The patient must have a diagnosis of Cystic Fibrosis; AND 2. The drug is given for 28 days followed by 28 days off, in repeat cycles. DOSE OPTIMIZATION ONLY NOTE: System edits apply for prescription claims submitted for more than twice daily dosing. Anticoagulants Brilinta® (ticagrelor) Effient® (prasugrel hydrochloride) Eliquis® (apixaban) Pradaxa® (dabigatran) Xarelto10mg ® (rivaroxaban) Qty is limited to 60 units per 30 days Qty is limited to 30 units per 30 days Qty is limited to 60 units per 30 days Qty is limited to 60 units per 30 days DOSE OPTIMIZATION ONLY NOTE: System edits apply for prescription claims submitted for more than once daily dosing DOSE OPTIMIZATION ONLY NOTE: System edits apply for prescription claims submitted for more than twice daily dosing. DOSE OPTIMIZATION ONLY NOTE: System edits apply for prescription claims submitted for more than twice daily dosing. Qty for 10mg is limited to 35 units 150 HEALTHPLUS PARTNERS (MEDICAID) DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D CATEGORY/DRUG Anticoagulants, continued Xarelto® 20mg (rivaroxaban) QTY LIMIT Qty is limited to 30 units per 30 days Antiemetic Anzemet® (dolasetron mesylate) Diclegis® (doxylamine/pyridoxine) DOSE OPTIMIZATION ONLY NOTE: System edits apply for prescription claims submitted for more than once daily dosing. Requires prior authorization for indications other than cancer. If the patient has cancer (and related medication), the system will allow the claim to pay at a limited quantity. Qty is limited to 120 units per 30 days Zuplenz® (ondansetron) Asthma/COPD Combivent Respimat® (albuterol/ ipratropium) Proventil HFA® (albuterol) ProAir HFA® (albuterol) CRITERIA Limited to 6 doses per day 1. The patient must try and fail an adequate course of therapy with two generically available products (e.g., Reglan, Tigan or Compazine). 1. The patient must have a documented diagnosis of pregnancy; AND 2. The patient must have a chart documented trial and failure or Rx claims for generic Zofran; AND 3. The patient must have a chart documented trial and failure of the individual agents (doxylamine and pyridoxine) in combination. New Starts Only 1. The patient must try and fail an adequate course of therapy with generic Zofran ODT. DOSE OPTIMIZATION ONLY NOTE: System edits apply for prescription claims submitted for more than 6 doses a day. 1. Patient has a documented contraindication to the preferred formulary albuterol inhaler (i.e. Ventolin HFA) Xopenex/HFA® (levalbuterol) 1. The patient must have documented intolerant side effects to albuterol (e.g., palpitations, tremors and tachycardia). Zyflo/CR® (zileuton) 1. The patient must have a diagnosis of asthma; AND 2. The patient must be 12 years of age or older; AND 3. The patient must have chart documented failure or prescription claims for generic Singulair or Accolate. 1. The patient must have documented failure or Rx claims with at least three generically available beta blockers (e.g., Inderal, Tenormin, Lopressor, Corgard). Beta Blockers Levatol® (penbutolol) Coreg CR® (carvedilol phosphate controlled release) Bystolic® (nebivolol) Limited to a qty of 30 units per month Limited to a qty of 30 units per month 1. The patient must have documented failure on immediate release carvedilol of equivalent dose and attempted at least one dose increase (6.25/day IR = 10mg/day ER when converting). DOSE OPTIMIZATION ONLY NOTE: System edits apply for prescription claims submitted for more than once daily dosing. 151 HEALTHPLUS PARTNERS (MEDICAID) DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D CATEGORY/DRUG QTY LIMIT CRITERIA Calcium Channel Blockers Dynacirc CR® (isradipine controlled release) 1. The patient must have documented failure on immediate release isradipine of equivalent dose and attempted at least one dose increase AND 2. The patient must have documented failure/contraindication to three generically available dihydropyridine CCB agents (e.g., nisoldipine, nifedipine, amlodipine, nicardipine, felodipine) in the past year. Cardizem LA® (diltiazem, long-acting) 1. The patient must have documented failure or Rx claims for at least two generically available formulary alternatives (e.g., Cardizem CD, Cardizem SR, Dilacor XR). Cholesterol Medications On Formulary with PA: Crestor® (rosuvastatin) Non-Formulary with PA: Advicor® (lovastatin/niacin) Altoprev® (lovastatin SR) Lescol XL® (fluvastatin) Livalo® (pitavastatin calcium) Liptruzet® (ezetimibe/atorvastatin) All HMGs are limited to a qty of 30 units per month 1. The patient must have documented failure or Rx claim(s) for generic Zocor, OR 2. The patient is currently receiving a medication that potentiates simvastatin levels (i.e., itraconazole, ketoconazole, HIV protease inhibitors, erythromycin, gemfibrozil, cyclosporine, amiodarone, verapamil, diltiazem, amlodipine, ranolazine). Limited to a qty of 30 units per month DOSE OPTIMIZATION ONLY NOTE: System edits apply for prescription claims submitted for more than once daily dosing. Welchol® (colesevelam) 1. The patient must have a diagnosis of diabetes and documented failure or Rx claim(s) for Metformin OR 2. The patient must have documented failure of both generic Questran AND generic Colestid. All Brand Omega-3 Fatty Acid Products Lovaza® (omega-3-acid ethyl esters) Vascepa® (icosapent ethyl) 1. The patient's triglyceride (TG) levels are >500mg/dL (with chart documentation provided) OR 2. The patient must have documented failure or Rx claims in the past six months for at least two or more lipid-lowering agents, with at least one being a generic product (i.e., statins, fenofibrate, nicotinic acid). Antara® (fenofibrate, micronized) Fenoglide® (fenofibrate) Lipofen® (fenofibrate) Triglide® (fenofibrate) On Formulary: Zetia® (ezetimibe) 1. The patient must have documented failure or Rx claim for a formulary fenofibrate (i.e., generic Lofibra) in the past year with at least one documented dosage increase. AUTHORIZATION IS ONLY REQUIRED FOR THE FOLLOWING: 1. If the patient has not had an Rx claim for an HMG statin medication in the previous year. Criteria for authorization for monotherapy include a documented contraindication for both hydrophilic (Pravachol, Lescol) and lipophilic (Zocor, Lipitor) statins, elevated liver enzymes, etc. 2. A dose >10mg per day requires documentation to support safety and efficacy. 152 HEALTHPLUS PARTNERS (MEDICAID) DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D CATEGORY/DRUG QTY LIMIT Contraceptives All Brand Oral Contraceptives Beyaz® LoEstrin 24 Fe 1/20® Natazia® NuvaRing® Ortho Evra® Ortho Tri-Cyclen Lo® Ovcon-50® Safyral® Dermatologicals On Formulary with PA: Elidel® (pimecrolimus) 1.The patient must have a documented trial or Rx claims for at least two generically available oral contraceptives in the past year before any brand product will be covered. 1. The patient must have documented failure or Rx claims for at least two generically available steroid creams in the past 6 months OR 2. Be under the treatment of a dermatologist. 1. The patient must have documented failure or Rx claims for generic Diprolene/AF (augmented betamethasone) or generic Ultravate (halobetsol) cream or ointment in the past 60 days. Clobetasol Propionate Cream and Ointment -generics Cormax® (clobetasol propionate) Temovate® (clobetasol propionate) Temovate E® (clobetasol propionate) Protopic® (tacrolimus) Solaraze® (diclofenac 3% gel)including generics Dovonex® (calcipotriene) Taclonex® (betamethasone/calcipotriene) Vectical® (calcitriol) Zyclara® (imiquimod) CRITERIA Safety limited to a qty of < 100g per 7 days Safety limited to a qty of < 200g per 7 days 1. The patient must have documented failure or Rx claims with at least two generically available topical steroids AND pimecrolimus in the past 180 days. 1. The patient must have a chart documented diagnosis of actinic keratosis. QUANTITY LIMITS ONLY QUANTITY LIMITS ONLY 1. The patient must have a diagnosis of actinic keratosis and documented treatment failure or Rx claims for geq Aldara; OR 2. The patient must have a diagnosis of condyloma acuminate and documented treatment failure or Rx claims for geq Condylox or geq Aldara. New Starts Only 153 HEALTHPLUS PARTNERS (MEDICAID) DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D CATEGORY/DRUG QTY LIMIT Dermatologicals, continued All Branded Topical Antifungal Agents Ciclodan Kit® (ciclopirox olamine cream/cleanser) CNL Nail Kit® (ciclopirox/lacquer removal pads) Dermasorb AF Kit® (clioquinolhc /emollient) Ertaczo® (sertaconazole nitrate) Exelderm® (sulconazole nitrate) Jublia® (efinaconazole) Kerydin® (tavaborole) Ketodan Kit® (ketoconazole foam/cleanser)Lamisil Soln® (terbinafine soln) Mentax® (butenafine) Naftin® (naftifine) Oxistat® (oxiconazole nitrate) Pediaderm AF® (nystatin/emollient) Terbinex® (terbinafine/hydroxychitosan) Tersi® (selenium sulfide) Xolegel/Corepak ® (ketoconazole) Luzu® (luliconazole) 1. The patient must have documented failure and Rx claims for four generic antifungals (e.g., Loprox, Nizoral, Spectazole and Grifulvin V). 1. The patient must have documented failure or Rx claims for at least 2 generic antifungal products (i.e., clotrimazole, miconazole, tolnaftate, terbinafine). 1. The patient must be greater than 4 weeks old with a diagnosis of candidal diaper dermatitis or candidal infection. Vusion® (miconazole nitrate/zinc oxide) Dermatologicals, continued Altabax® (retapamulin) Bactroban Nasal Ointment® (mupirocin) All Brand Topical Steroids Clobex Spray® (clobetasol propionate) Synalar TS® (fluocinolone/cleanser) Ultravate PAC Kit® (halobetasol propionate/ammonium lactate) CRITERIA 10 grams (10, 1gm) tubes per month 1. The patient must have a documented treatment failure with generic Bactroban ointment for each instance of impetigo AND 2. A diagnosis of impetigo. 1. The patient must have a chart documented nasal colonization with methicillin-resistant S. aureus (MRSA); AND 2. The patient must have Rx claims for generic mupirocin ointment in the past 7 days. Criteria for more than 10 grams per month 1. The patient must have chart documented nasal recolonization of MRSA. 1. The patient must have documented failure or Rx claim with a generic topical steroid in the same potency class (e.g., Ultravate, Diprolene) in the past 60 days. 154 HEALTHPLUS PARTNERS (MEDICAID) DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D CATEGORY/DRUG QTY LIMIT CRITERIA Dermatologicals, continued All Brand Topical Steroids Kenalog Aerosol Spray® (triamcinolone acetonide) Pandel® (hydrocortisone probutate) Pediaderm TA® (triamcinolone) Topicort Spray® (desoximetasone) Cordran Lotion® (flurandrenolide) Cordran SP Cream® (flurandrenolide) Locoid Lotion ® (hydrocortisone butyrate) Momexin® (mometasone furoat/ammonium lac) 1. The patient must have documented failure or Rx claim with a generic topical steroid in the same potency class (e.g., Elocon, Westcort and Synalar) in the past 60 days. Desonate Gel® (desonide) Desowen Combo® (desonide/emollient) Pediaderm HC® (hydrocortisone) Vanoxide-HC Lotion® (hydrocortisone/benzoyl peroxide) Verdeso Foam® (desonide) 1. The patient must have documented failure or Rx claim with a generic topical steroid in the same potency class (e.g., Aclovate, Desowen and Synalar) in the past 60 days. All Brand Topical Emollients Dermasorb XM Kit (urea) Epiceram® (emollient combo) Gordons Urea® (urea) Hylatopic® (emollient combo) Kerafoam® (urea) Keralac Cream 47%® (urea) Neosalus® (emollient combo) Promiseb® (emollient combo) Promiseb Complete® (emollient combo) Umecta® (urea) Umecta PD® (urea) Uramaxin GT Kit® (urea/emollient) Utopic® (urea) 1. The patient must have documented failure or Rx claim for a generic topical emollient (e.g., Carmol, Lac-Hydrin, Mectalyte and Vanamide) in the past 60 days. 1. The patient must have documented failure or Rx claim with a generic topical steroid in the same potency class (e.g., Beta-Val Cr, Cutivate Cr, Dermatop Cr) in the past 60 days. 155 HEALTHPLUS PARTNERS (MEDICAID) DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D CATEGORY/DRUG QTY LIMIT Dermatologicals, continued All Branded Topical Sulfonamide and Sulfonamide/Sulfur Products Avar® (sulfacetamide sodium/sulfur) Avar-E® (sulfacetamide sodium/sulfur) Avar LS® (sulfacetamide sodium/sulfur) Plexion® (sulfacetamide sodium/sulfur) Rosanil® (sulfacetamide sodium/sulfur) Sumadan® (sulfacetamide sodium/sulfur) Diabetes Glumetza® (metformin) Janumet, XR® (sitagliptin/metformin) Kazano® (alogliptin/metformin) Kombiglyze XR® (saxagliptin/metformin) Oseni® (alogliptin/pioglitazone) Januvia® (sitagliptin) Nesina® (alogliptin benzoate) Onglyza® (saxagliptin) Tradjenta® (linagliptin) Invokana® (canagliflozin) Apidra® (insulin glulisine) Novolin® Insulins (insulin) Novolog® Insulins (insulin aspart) Novolog Mix® (insulin) Glucose Test Strips Freestyle Lite® Freestyle Insulinx® Precision Xtra® Endometriosis Lupron Depot 3.75 Kit® (leuprolide acetate) CRITERIA 1. The patient must have documented failure and Rx claims for at least 2 generic sulfonamide/sulfur products in the past year. 1. The patient must have documented failure or Rx claims in the past year for generic Glucophage and generic Glucophage XR. 1. The patient must have documented failure or Rx claims with a preferred formulary DPP-4 inhibitor (i.e. Tradjenta, Jentadueto). Limited to a qty of 30 units per month Limited to a qty of 30 units per month 1. The patient must have documented failure or Rx claims with a preferred formulary DPP-4 inhibitor (i.e. Tradjenta, Jentadueto). DOSE OPTIMIZATION ONLY NOTE: System edits apply for prescription claims submitted for more than once daily dosing. 1. Patient has a documented contraindication to a comparable preferred formulary insulin (i.e. Humulin and Humalog products), Limited qty of 150 units per 30 days or 450 units per 90 days DOSE OPTIMIZATION ONLY 1. Confirmation of diagnosis. NOTE: Not covered for infertility (infertility services are excluded). 156 HEALTHPLUS PARTNERS (MEDICAID) DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D CATEGORY/DRUG QTY LIMIT Hormone Replacement Cenestin® (estrogens, conj synthetic) Premarin® (conjugated estrogens) Premphase® (conj estrogens/medroxypro) Prempro® (conj estrogens/medroxypro) Enjuvia® (conjugated estrogen, synthetic) Migraine Medications Formulary with PA: Relpax® (eletriptan) Non-Formulary with PA: Axert® (almotriptan) Frova® (frovatriptan) Treximet® (sumatriptan/naproxen) 1. The patient must have documented failure or Rx claims for both generically available estrogen products (i.e., Estrace, Ogen). Qty for all triptans combined are limited to 9 tablets per month 1. The patient must have documented treatment failure with generic Estrace, Ogen and Premarin (which requires Prior Authorization). For Relpax: 1. The patient must have documented failure or Rx claims for all generic triptans (i.e., Amerge, Imitrex, Maxalt, Zomig); OR 2. Generic alternatives must be inappropriate with chart documentation provided. For Non-Formulary Products: 1. The patient must have documented failure or Rx claims for all formulary alternatives (i.e., Amerge, Imitrex, Maxalt, Relpax and Zomig); OR 2. Formulary alternatives must be inappropriate with chart documentation provided. Cambia® (diclofenac potassium) Imitrex Injection® (sumatriptan injection) CRITERIA All injectable sumatriptan products limited to 6 injections for 30 days CRITERIA FOR MORE THAN NINE TABLETS PER MONTH 1. Patient is currently receiving medication therapy for the prophylaxis of migraines based on Rx claims in the past 120 days and still requires more than nine tablets per month, OR 2. Patient has had documented failure of all options for migraine prophylaxis and still requires more than nine tablets per month. 1. The patient must have a diagnosis of migraine headaches; AND 2. The patient must have documented failure or Rx claims for generic diclofenac; AND 3. The patient must have documented failure or Rx claims for at least one additional non-steroidal anti-inflammatory drug (i.e., ibuprofen, naproxen sodium). Criteria for more than 6 injections per month 1. Patient is currently receiving medication therapy for the prophylaxis of migraines based on Rx claims in the past 120 days and still requires more than 6 injections per month, OR 2. Patient has had documented failure or contraindication to all options for migraine prophylaxis and requires more than 6 injections per month 157 HEALTHPLUS PARTNERS (MEDICAID) DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D CATEGORY/DRUG Migraine Medications, continued Sumavel® (sumatriptan injection) QTY LIMIT CRITERIA All 1. The patient must have documented failure or prescription injectable claims for generic Imitrex injection. sumatriptan products Criteria for more than 6 injections per month limited to 6 1. Patient is currently receiving medication therapy for the injections prophylaxis of migraines based on Rx claims in the past 120 for 30 days Imitrex Nasal Spray® (sumatriptan) Zomig Nasal Spray® (zolmitriptan) All nasal triptan products are limited to a quantity of 6 per month All Non-Injectable Dihydroergotamine Products Migranal® (dihydroergotamine) – including generics 8 units (ml) per month days and still requires more than 6 injections per month, OR 2. Patient has had documented failure or contraindication to all options for migraine prophylaxis and requires more than 6 injections per month Criteria for more than 6 units per month 1. Patient is currently receiving medication therapy for the prophylaxis of migraines based on Rx claims in the past 120 days and still requires more than 6 units per month, OR 2. Patient has had documented failure or contraindication to all options for migraine prophylaxis and requires more than 6 units per month 1. The patient must have a diagnosis of migraine headaches; AND 2. The patient must have chart documented failure or prescription claims for an oral generic triptan medication (i.e. generic Imitrex, Maxalt, Zomig, Amerge); AND 3. The patient must have chart documented failure or prescription claims for generic Imitrex nasal spray or injection; OR 4. The patient has a chart documented contraindication or intolerance to triptan medications. Criteria for more than 8 units per month 1. Patient is currently receiving medication therapy for the prophylaxis of migraines based on Rx claims in the past 120 days and still requires more 8 units per month. 2. Patient has had documented failure of all options for migraine prophylaxis and still requires more than 8 units per month. All Brand Ergotamine Products Cafergot® (ergotamine/caffeine tablets) Migergot® (ergotamine/caffeine rectal suppositories) 40 tabs per 30 days OR 20 supps per 30 days Muscle Relaxants Amrix® (cyclobenzaprine ext release) 1. The patient must have a diagnosis of migraine headaches; AND 2. The patient must have chart documented failure or prescription claims for an oral generic triptan medication (i.e. generic Imitrex, generic Amerge); AND 3. The patient has a chart documented contraindication or intolerance to triptan medications. 1. The patient must try and fail an adequate course of therapy with at least two generic prescription muscle relaxants (i.e., Flexeril, Norflex, Robaxin, Skelaxin). 158 HEALTHPLUS PARTNERS (MEDICAID) DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D CATEGORY/DRUG QTY LIMIT CRITERIA Miscellaneous Cantil® (mepenzolate bromide) 1. The patient must have documented failure or Rx claims for at least three generically available antispasmotics (i.e., Bentyl, Levsinex, Librax) in the past year. Cardura XL® (doxazosin mesylate ext. release) 1. The patient must have documented failure or Rx claim for a generically available alpha-1 adrenergic antagonist (e.g., Cardura, Flomax or Hytrin) in the past year. Grastek® (timothy grass pollen allergen extract) Oralair® (mixed pollens allergen extract) Ragwitek® (short ragweed pollen allergen extract) Ranexa® (ranolazine) Nitroglycerin Patches Rayos® (prednisone delayed release tablets) On Formulary with PA: Revatio® (sildenafil) Non-Formulary with PA: Adcirca® (tadalafil) Limited to a qty of 30 units per month 1. The prescriber must be an allergist and administer the first dose under supervision; AND 2. The patient must have chart documentation of a positive skin test or in-vitro testing for pollen-specific IgE antibodies for the allergens containedin the product; AND 3. Patient must have a chart documented trial of at least one nasal steroid (i.e., Flonase, flunisolide, Nasacort AQ ) and one non-sedating antihistamine (i.e., Claritin, Zyrtec, Allegra); AND 4. There are claims for an epinephrine auto-injector within the past 6 months; AND 5. For Ragwitek and Grastek, treatment will be initiated 12 weeks prior to the expected onset of the allergen season and continued throughout the season; OR 6. For Oralair, treatment will be initiated 16 weeks prior to the expected onset of the allergen season and continued throughout the season. Ragwitek and Grastek: authorization will approved for 24 weeks per calendar year. Oralair: authorization will be approved for 28 weeks per calendar year. Note: The authorization approvals are based on a 12 week allergy season. 1. The patient must have a documented diagnosis of chronic angina; in addition, there must be a pharmacy claim for amlodipine or beta-blocker or non-acute nitrates. 1. The patient must have documented failure or Rx claim for generic oral nitroglycerin in the past 90 days. 1. The patient must have a documented diagnosis of rheumatoid arthritis; AND 2. The patient must have documented failure and Rx claims for 2 generically available oral corticosteroids (i.e., prednisone, methylprednisolone). 1. The patient must have a documented diagnosis of pulmonary arterial hypertension. 2. If the patient has a history of nitrate use, the physician must submit a written request on his/her letterhead stating that the patient is no longer using nitrates. 159 HEALTHPLUS PARTNERS (MEDICAID) DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D CATEGORY/DRUG QTY LIMIT Miscellaneous, continued On Formulary with PA: Savella® (milnacipran) Thyrolar® (liotrix) Amitiza® (lubiprostone) Moviprep® (peg 3350/ sod sul/nacl/asb/c/kcl) Osmoprep® (naphos mb0mh/naphos, di-ba) Uloric® (febuxostat) Limited to a qty of 30 units per month Neurological Miscellaneous Gralise® (gabapentin) Horizant® (gabapentin enacarbil) Limited to a qty of 30 units per 30 days. Nuedexta® (dextromethorphan/quinidine) Limited to a qty of 60 units per 30 days. CRITERIA 1. The patient must have a documented diagnosis of fibromyalgia, OR 2. Documentation of all of the following: a. Widespread pain for at least 3 months, AND b. Pain on both sides of the body, above and below the waist, AND c. Abnormal tenderness in at least 11 of the 18 anatomicallydefined body sites. 1. The patient must have documented failure or Rx claims for at least two generically available thyroid preparations in the past year. 1. The patient must have documented treatment failure with at least 2 generic/OTC cathartics (e.g., bisacodyl, docusate sodium, lactulose, mineral oil, etc) OR 2. A documented D(x) of constipation predominant IBS. 1. The patient must have documented contraindication or treatment failure or Rx claims with two generic polyethylene glycol electrolyte powders (e.g., Colyte, Golytely, Nulytely and Trilyte). 1. Patient must have documented failure or prescription claims with allopurinol, OR 2. The patient cannot tolerate therapeutic doses or is not an appropriate candidate for allopurinol based on documentation provided. 1. The patient must have a documented diagnosis of postherpetic neuralgia, AND 2. The patient must have documented failure and Rx claims with generic Neurontin, AND 3. The patient must have documented failure or Rx claims with a generic tricyclic antidepressant. 1. The patient must have a diagnosis of restless legs syndrome, AND 2. The patient must have documented failure and Rx claims with generic Neurontin, AND 3. The patient must have documented failure or Rx claims with generic Requip or generic Mirapex. 1. The patient must have a documented diagnosis of pseudobulbar affect; AND 2. The patient must be 18 years or older; AND 3. Patient is not currently receiving quinidine, quinine, mefloquine, an MAOI, or any drug that prolongs QT interval and is metabolized by CYP2D6 (e.g., thioridazine or pimozide); AND 4. Patient must have recent (within the past three months) platelet count, liver function panel, and ECG if patient has left ventricular dysfunction/hypertrophy. Prior authorizarion requests are approved for a 6 month duration. 160 HEALTHPLUS PARTNERS (MEDICAID) DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D CATEGORY/DRUG NSAIDs On Formulary with PA: Celebrex® (celecoxib) Non-Formulary with PA: Arthrotec® (diclofenac/misoprostol) Naprelan CR® (naproxen sodium) QTY LIMIT Cox-2 drugs and Mobic are limited to a qty of 30 units per month CRITERIA 1. Documented indication for acute or chronic treatment of the signs and symptoms of osteoarthritis or rheumatoid arthritis, AND 2. The patient must have documented failure or Rx claims for an adequate course of therapy with at least two generic prescription NSAID agents (e.g., ibuprofen, naproxen, piroxicam, ketoprofen, diclofenac, etc.). Adequate course of therapy is defined as a full therapeutic dose on a scheduled basis for at least 1-2 weeks; OR 3. The patient is identified as "high risk" for developing GI complications: a. Age over 60 years old AND any one of the following risks: b. Requiring prolonged use of max dose of traditional NSAIDS OR c. Concomitant use of steroids OR d. Documented history of ulcer/bleed/perforation, OR 4. Active ulcer or recent documented history of ulcer (within 6 months) or history of GI bleed/perforation. Duexis® (ibuprofen/famotidine) 1. The patient must have a documented diagnosis of arthritis; AND 2. The patient must be high risk for developing GI complications: a. Documentation or Rx claims for concomitant use of steroids, DMARDs, or anticoagulants b. Documentation of active or previous ulcer/bleed/perforation c. Documentation of platelet dysfunction or coagulopathy; AND 3. The patient must have chart documented failure or Rx claims for both ibuprofen 800 mg and famotidine 20 mg in the past month. Flector® (diclofenac epolamine transdermal patch) 1. The patient must have documented failure or Rx claims for an adequate course of therapy with at least two generic prescription NSAID agents (e.g., ibuprofen, naproxen, piroxicam, ketoprofen, diclofenac, etc.). Adequate course of therapy is defined as a full therapeutic dose on a scheduled basis for at least 1-2 weeks; OR 2. The patient is identified as "high risk" for developing GI complications: a. Age over 60 years old AND any one of the following risks: b. Requiring prolonged use of max dose of traditional NSAIDS OR c. Concomitant use of steroids OR d. Documented history of ulcer/bleed/perforation, OR 3. Active ulcer or recent documented history of ulcer (within 6 months) on history of GI bleed/perforation. 161 HEALTHPLUS PARTNERS (MEDICAID) DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D CATEGORY/DRUG QTY LIMIT CRITERIA NSAIDs, continued Vimovo® (esomeprazole/naproxen) 1. The patient must have a documented diagnosis of arthritis, AND 2. The patient must be high risk for developing GI complications: a. Documentation or Rx claims for concomitant use of steroids, DMARDs, or anticoagulants b. Documentation of active or previous ulcer/bleed/perforation c. Documentation of platelet dysfunction or coagulopathy 3. The patient must fail all formulary proton pump inhibitor alternatives (i.e., Omeprazole, generic Aciphex, generic Prevacid, generic Protonix) in combination with generic naproxen. Voltaren Gel® (diclofenac sodium) 1. The patient must have documented failure or Rx claims for an adequate course of therapy with at least two generic prescription NSAID agents (e.g., ibuprofen, naproxen, piroxicam, ketoprofen, diclofenac, etc.). All Oral Brand Diclofenac Products Zipsor® (diclofenac potassium) Zorvolex® (diclofenac) 1. The patient must have documented failure or Rx claims for an adequate course of therapy with at least two generic prescription NSAID agents (e.g., ibuprofen, naproxen, piroxicam, ketoprofen, diclofenac, etc.), and one must be generic Voltaren. Adequate course of therapy is defined as a full therapeutic dose on a scheduled basis for at least 1-2 weeks. 1. The patient must have documented failure or Rx claim for generic OTC Zaditor in the past 90 days (covered with written prescription). 2. If the patient fails treatment with generic OTC Zaditor, then Patanol is the second-line formulary alternative with prior authorization required. 3. The patient must have documented failure or Rx claims for the formulary alternatives (OTC Zaditor and Patanol) before a nonformulary drug will be approved. Ophthalmics All Brand Topical Ophthalmic Antihistamines On Formulary with PA: Patanol® (olopatadine) Non-Formulary with PA: Alocril® (nedocromil sodium) Alomide® (lodoxamide tromethamide) Bepreve® (bepotastine besilate) Emadine® (emedastine difumarate) Lastacaft® (alcaftadine) Pataday® (olopatadine) Restasis® (cyclosporine) Alphagan P 0.1%® (brimonidine tartrate) Qty is limited to 2 units per day 1. The patient must have a documented diagnosis of keratoconjunctivitis sicca. 1. The patient must have documented contraindication or documented treatment failure with the use of generic brimonidine ophth. 162 HEALTHPLUS PARTNERS (MEDICAID) DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D CATEGORY/DRUG QTY LIMIT CRITERIA Ophthalmics, continued Lotemax® (loteprednol etabonate) 1. The patient must have documented failure or Rx claim for at least one generic formulary topical ophthalmic steroid (e.g., Pred Forte, Inflamase Forte, FML suspension). Betimol® (timolol) Istalol® (timolol maleate) 1. The patient must have documented failure or Rx claim for at least one generic Timolol (e.g., Timoptic) ophthalmic product. All Brand Topical Ophthalmic NSAIDs Acuvail® (ketorolac tromethamine) Ilevro® (nepafenac) Nevanac® (nepafenac) Prolensa® (bromfenac sodium) All Brand Topical Ophthalmic Prostaglandin Analogs On Formulary with PA: Lumigan 0.01%® (bimatoprost) 1. The patient must have documented failure or Rx claims for at least two formulary topical ophthalmic NSAIDs (e.g., generic Voltaren, generic Ocufen, Acular, Acular LS, Bromday) before any other topical ophthalmic NSAIDs will be covered. Non-Formulary with PA: Lumigan 0.03% ® (bimatoprost) Travatan Z® (travoprost) Zioptan® (tafluprost) Osteoporosis Actonel® (risedronate sodium) Evista® (raloxifene) Zioptan is limited to a qty of 1 unit per day 1. The patient must have documented failure or prescription claims for a generic prostaglandin analog (i.e., generic Xalatan). 2. If the patient fails treatment with all generic prostaglandin analogs, then Lumigan 0.01% is the second-line formulary alternative with prior authorization required. 3. The patient must have documented failure or prescription claims for all formulary alternatives (generic Xalatan AND branded Lumigan 0.01%) before a non-formulary brand drug will be approved. 1. The patient must have documented failure or Rx claim for generic Fosamax in the past year. NOTE: Exceptions will be made for patients in active treatment for cancer. Applies to new start patients only. Forteo® (teriparatide) 1. The patient must have a documented diagnosis of osteoporosis (active or prevention). NOTE: Applies to new start patients only. Otic Products Cipro HC® (ciprofloxacin) Coly-mycin S® (colistin/ hc ace/ neo sulfate/thonzonium bromide) Cortisporin-TC® (colistin/hc ace/neo sulfate/thonzonium bromide) 1. The patient must have documented failure or Rx claims for at least two generically available products in the past 90 days before any brand otic product will be covered. 163 HEALTHPLUS PARTNERS (MEDICAID) DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D CATEGORY/DRUG Proton Pump Inhibitors On Formulary with PA: Esomeprazole Strontium® (esomeprazole strontium) Non-Formulary with PA: Aciphex Sprinkle® (rabeprazole) Dexilant® (dexlansoprazole) First-Lansoprazole® (lansoprazole) First-Omeprazole® (omeprazole) Nexium® (esomeprazole) Prevacid Solutab® (lansoprazole) Prilosec DR Susp® (omeprazole magnesium) Protonix Pak® (pantoprazole) Zegerid Susp® (omeprazole /sodium bicarbonate) Inflammatory Bowel Disease All Branded Non-Formulary Oral Agents Dipentum® (olsalazine sodium) Giazo® (balsalazide) Lialda® (mesalamine) Uceris® (budesonide) Canasa® (mesalamine) Urology Gelnique® (oxybutynin chloride) Oxytrol Patch® (oxybutynin) Myrbetriq® (mirabegron) QTY LIMIT Brand PPIs are limited to a qty of 30 tabs/caps per month 1. The patient must have documented failure or Rx claims for 4 generic proton pump inhibitors (PPI) before a non-formulary PPI will be approved, AND 2. Specifically for Nexium and esomeprazole strontium, the patient must have a current documented diagnosis of Barrett's Esophagus, Zollinger-Ellison or Erosive Esophagitis. Approved automatically for children under 2 years of age. 3. Specifically for Dexilant, the patient must have a current documented diagnosis of Erosive Esophagitis; OR if the patient is currently taking clopidogrel, they must have documented failure or Rx claims for both pantoprazole and lansoprazole. Specifically for liquid or soluble preparations: 1. The patient must have a documented inability to swallow a solid dosage form. 1. The patient must have documented failure or Rx claims for at least two formulary agents (e.g., generic Azulfidine, Colazal, or Asacol) in the past year. Limited to a qty of 30 units per month DOSE OPTIMIZATION ONLY NOTE: System edits apply for prescription claims submitted for more than once daily dosing. 1. The patient must have documented failure or Rx claim for generic Ditropan tablets in the past year. Limited to a qty of 30 units per month Rapaflo® (silodosin) Detrol LA® (tolterodine, long-acting) Ditropan XL® (oxybutynin, sust. release)Enablex® (solifenacin) Toviaz® (fesoterodine) Vesicare® (darifenacin hydrobromide) CRITERIA Limited to a qty of 30 units per month 1. Patient must have chart documented treatment failure or intolerance to at least 2 generic formulary alternatives for overactive bladder (i.e., oxybutynin, tolterodine, trospium chloride). 1. The patient must have documented failure based on chart documentation or Rx claims for a generically available alpha1blocker indicated for BPH (i.e., generic Cardura, Hytrin or Flomax). DOSE OPTIMIZATION ONLY NOTE: System edits apply for prescription claims submitted for more than once daily dosing. 164 HEALTHPLUS PARTNERS (MEDICAID) DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D CATEGORY/DRUG Vitamins All Brand Prenatal Vitamins Atabex DHA® Bal-Care DHA Essential Citranatal Assure® Citranatal Harmony® Duet DHA Balanced® Gesticare DHA® Natalvit® Natelle One® OB Complete® Obtrex® Obstetrix DHA® Prenata® Prenate Elite, DHA, Essential® Preque 10® Vitafol-One® QTY LIMIT CRITERIA 1. The patient must have documented failure or Rx claim for at least one generic prenatal vitamin in the past 90 days. 165 HEALTHPLUS PARTNERS (MEDICAID) DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D CATEGORY/DRUG Weight Management All medications for the treatment of obesity Examples: Adipex® (phentermine) Belviq® (lorcaserin) Bontril 105mg® (phendimetrazine tartrate) Bontril PDM 35mg® (phendimetrazine tartrate) Diethylpropion® (diethylpropion) Qsymia® (phentermine/ topiramate) Suprenza® (phentermine) Xenical® (orlistat) QTY LIMIT CRITERIA 1. The patient is an adult ≥ 18 years of age; AND 2 2. The patient has a body mass index (BMI) of >30kg/m , OR 2 3. The patient has a body mass index (BMI) of >27kg/m with any of the following co-morbidities: -established coronary heart disease -atherosclerotic disease -type 2 diabetes -sleep apnea, OR 2 4. The patient has a body mass index (BMI) of >27kg/m , A. With at least three of the following risk factors: -hypertension -high LDL cholesterol -low HDL cholesterol -impaired fasting glucose -smoking -family history of early cardiovascular disease -age >45 years for men or age >55 years for women, AND B. The patient has undergone evaluation to rule out other treatable causes of obesity, not presence of malabsorption syndrome, thyroid conditions, cholestasis, pregnancy, and/or lactation, AND C. There has been a previous weight loss attempt for at least 6-12 months within one (1) year through a physician supervised diet and exercise program consisting of low calorie diet, AND D. The patient has a strong desire, willingness and cognitive ability to make changes in diet and activity level, AND E. The medication is part of a continued treatment plan, which includes a calorie and fat reduced diet, and a regular exercise program. AND 5. If the medication is a brand name product, the patient must have tried a generically available product (i.e. phentermine, diethylpropion) in the past year. If the preceding criteria are met, the request for a weight loss medication will be approved for 1 year (365 days) of total coverage. 166 HEALTHPLUS PARTNERS (MEDICAID) DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D CATEGORY/DRUG Non-Sterile Compounded Prescriptions Non-Formulary with PA QTY LIMIT CRITERIA 1. The compounded product contains at least one FDA-approved prescription ingredient; AND 2. Each prescription drug or active ingredient in the compounded product is approved by the Food & Drug Administration (FDA) for medical use in the United States; AND 3. The active prescription medication component(s) are in therapeutic amounts; AND 4. The compounded product is not a copy of any commercially available FDA-approved drug product; AND 5. The use for which the compounded product is being prescribed is supported by FDA approval of the active ingredient(s), or is supported by two or more articles from peer reviewed journals demonstrating the safety and efficacy of the prescribed therapy for that diagnosis and method or route of delivery; AND 6. If any prescription ingredient in the compounded product is included in the HealthPlus Prior Authorization program, the patient must meet the criteria designated for that prescription ingredient. Based on limitations or exclusions in the subscriber certificate, coverage will NOT be provided for compounds under the following circumstances: 1. Any compound that does not contain a FDA-approved prescription ingredient otherwise covered by the plan; OR 2. Any compound that contains a non-FDA approved or nonHealthPlus covered prescription ingredient. 3. Compounded formulations that contain any bulk powders that are not FDA approved or HealthPlus approved; OR 4. Compounded formulations that are being used for cosmetic purposes; OR 5. Compounded formulations that are using prescription ingredients for non-FDA approved indications or purposes that are not supported by peer-reviewed literature; OR 6. Compounded formulations that may be considered investigational or experimental; OR 7. Compounded formulations that use drugs withdrawn or removed from the market for safety reasons; OR 8. Prescription ingredient(s) compounded for the purpose of convenience only. a. Exceptions include: i. Compounded medications for those patients that cannot swallow or have trouble swallowing and require administration with an oral liquid, or administration by topical, rectal or other appropriate non-oral routes; ii. Compounded medications for those patients who have sensitivity to dyes, preservatives, or fillers in commercial products and require allergy-free medications as documented in the medical record; iii. Compounded medications for children who require prescription medications for which there are no liquid formulations available. 167 HEALTHPLUS PARTNERS (MEDICAID) DRUG FORMULARY PRIOR AUTHORIZATION CRITERIA AND DOSE OPTIMIZATION APPENDIX D CATEGORY/DRUG QTY LIMIT CRITERIA Dispense as Written DAW Specific request for a brand name product when a generic is available 1. The benefit covers generic/specific OTC products when a generically equivalent product is available. 2. In general, prior authorization is required for all brand name drugs (when the drug is available and covered as a generic medication). The physician may submit a prior authorization request form for the brand name drug (when a generic equivalent is available), but this must be substantiated by medical necessity. If medical necessity is based on a trial and failure of the generic medication, a prescription claim for the generic drug must be present or chart notes documenting the failure must be provided. 3. If a physician submits a prior authorization request form for coverage of a brand name drug (when a generic equivalent is available), the request is reviewed through the same process as all other drugs that require prior authorization. 4. The member may still choose to receive a brand product without medical necessity, but would be responsible for the entire cost of the prescription. Quantity Limit QL Specific request for a dose, quantity or duration that exceeds the established limits 1. The physician must provide documentation of the clinical rationale for requesting a dosage, quantity, or duration of medication greater than the criteria specified in the formulary. 2. If the dosage exceeds the manufacturer product labeling/prescribing information, the physician must submit documentation of two articles from peer reviewed journals demonstrating the safety and efficacy of the prescribed therapy. Medical Exception Requests Specific Excluded Non-Formulary Drugs DRUG/CATEGORY Exceptions Criteria (for all non-formulary drugs in a closed formulary) QTY LIMIT CRITERIA 1. Based on specific documented patient circumstances, each/all of the formulary drugs/alternatives are not appropriate because: a. Medication(s) are contraindicated or unsafe, or b. Patient is intolerant or allergic, or c. Patient had an inadequate or inappropriate response; AND 2. Chart documentation to support this medical necessity has been provided; AND 3. The requested drug and dosage is FDA-approved for the patient’s diagnosis; AND 4. If established (commercial) HealthPlus prior authorization criteria exists, the prior authorization criteria will also apply. 168 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D HEALTHPLUS PARTNERS High Risk Medications in the Elderly (≥66 years old) Based on the availability of safer alternatives, the following medications have been added to the Prior Authorization Program for members 66 years of age and older for HealthPlus Partners (Medicaid) with the following criteria: 1) The recommended alternative treatment(s) are not appropriate, are contraindicated or are unsafe for the patient based on specific documented patient circumstances, OR 2) The patient has a documented trial and failure (or prescription claims) for the recommended alternative treatment(s). Name Concern Alternative Treatment Estrogens – all oral and topical patches only (Premarin, estradiol, Estratest, Vivelle-Dot, etc.) Promethazine (Phenergan) Evidence of breast/Endometrial cancer; No cardio or cognitive protection in older women Nitrofurantoin (Macrodantin) Nephrotoxicity Thyroid USP (Armour Thyroid, Desiccated) Cardiac adverse effects Glyburide (Micronase) Glyburide-Metformin (Glucovance) Chlorpropamide (Diabinese) Hydroxyzine (Vistaril, Atarax) Cyclobenzaprine (Flexeril) Orphenadrine (Norflex) Chlorzoxazone (Parafon Forte) Methocarbamol (Robaxin) Skelaxin (Metaxalone) Trimethobenzamide (Tigan) Ketorolac (Toradol) Indomethacin Dipyridamole (Persantine) Associated with an increased risk of hypoglycemia compared to other agents Diabetes: Glucotrol, Amaryl, Metaglip Anticholinergic effects, urinary retention, confusion, sedation Anticholinergic effects, sedation, cognitive impairment, weakness, urinary retention Antihistamine: Claritin , Zyrtec Physiotherapy: correct seating & footwear Spasticity: Baclofen, Zanaflex. Treat underlying problems Extrapyramidal side effects, poor efficacy GI bleeding Nausea: Zofran, Compazine, or Reglan 2 2 Pain: Tylenol , Motrin , Norco Orthostatic hypotension, poor efficacy For secondary prevention of non-cardioembolic stroke or TIA: Plavix, Aggrenox, Aspirin 1 Anticholinergic effects (i.e., urinary retention, confusion, sedation) Hot flashes: non-pharmacological therapy, Zoloft, Paxil, Effexor 2 Bone density: Calcium with vitamin D , Fosamax, 1 Boniva, Evista 1,2 2 Antihistamine: Claritin , Zyrtec 1 Antiemetic: Antivert, Zofran Cough: Dextromethorphan Depends on site of infection, culture, and sensitivity. 1 Bactrim, Vibramycin, Azithromycin, Fluoroquinolone Levothyroxine (LT4): Synthroid, Levoxyl 2 2 Drug may require prior authorization or may have limited coverage depending on member’s benefit plan, 2 Available OTC 169 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D SPECIALTY/INJECTABLE PRIOR AUTHORIZATION CRITERIA Brand (generic) Name Androgens Testopel® (testosterone implant pellets) Criteria 1. The patient is male, ≥ 18 years old, and has a documented diagnosis of hypogonadism; AND 2. The patient has a morning (before 11AM) serum total testosterone concentration of less than 300 ng/dL documented on 2 separate occasions in the past year; AND 3. The patient has a morning free serum testosterone level less than the lower limit of the lab reference range of normal based on age; AND 4. The patient must have documented failure or Rx claims with testosterone cypionate or enanthate for a minimum of 2 months; OR 1. The patient has a documented diagnosis of delayed puberty; AND 2. The patient must have documented failure or Rx claims with testosterone cypionate or enanthate. Duration of Approval Notes 170 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Antihyperlipidemics Juxtapid® (lomitapide mesylate) Criteria 1. The patient must be over 18 years old; AND 2. The patient must have a previous Rx claim for a HMG-CoA reductase inhibitor (i.e. statin); AND 3. The patient must have clinical and/or laboratory determined presence of homozygous familial hypercholesterolemia. Acceptable documentation includes*: a. Chart documentation confirming the presence of xanthomas before the age of 10, an untreated LDL of >500mg/dL, a treated LDL of ≥300mg/dL, or a treated non-HDL ≥330mg/dL; OR b. Genetic testing showing 2 mutated alleles at the LDL-Receptor, ApoB, PCSK9, or ARH adaptor protein gene locus; AND 4. If the patient is female and of childbearing potential, a negative pregnancy test must be completed just prior to initiating therapy; AND 5. The patient must have ALT, AST, alkaline phosphate, total bilirubin, INR, and SCr testing obtained just prior to initiating therapy; AND 6. The results from liver function tests must be normal (no clinically significant or unexplainable abnormalities); AND 7. The dose must be appropriate based on manufacturer recommendations. Duration of Approval Approval of prior authorization requests is limited to 12 months. Notes Recent lab results (within 3 months) are required for each renewal. 171 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Antihyperlipidemics, continued Kynamro® (mipomersen) 1. 2. 3. 4. 5. 6. Criteria The patient must be over 18 years old; AND The patient must have a previous Rx claim for a HMG-CoA reductase inhibitor (i.e. statin); AND The patient must have clinical and/or laboratory determined presence of homozygous familial hypercholesterolemia. Acceptable documentation includes*: a. Chart documentation confirming the presence of xanthomas before the age of 10, an untreated LDL of >500mg/dL, a treated LDL of ≥300mg/dL, or a treated non-HDL ≥330mg/dL; OR b. Genetic testing showing 2 mutated alleles LDL-Receptor, ApoB, PCSK9, or ARH adaptor protein gene locus; AND The patient must have ALT, AST, alkaline phosphate, total bilirubin, INR, and SCr testing obtained just prior to initiating therapy; AND The results from liver function tests must be normal (no clinically significant or unexplainable abnormalities); AND The dose must be appropriate based on manufacture recommendations Duration of Approval Approval of prior authorization requests is limited to 12 months. Notes Recent lab values (within 3 months) are required for each renewal. Discontinuation of treatment should be considered if patient does not have a sufficient response to warrant the potential risk of liver toxicity after 6 months. 172 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Antineoplastic Jakafi® (ruxolitinib) Criteria 1. Patient must have a diagnosis of myelofibrosis with a risk category of intermediate (2 prognostic factors) or high (3 or more prognostic factors) based on the International Working Group Consensus Criteria (IWG). Prognostic factors include: a. Age >65 years old 9 b. WBC > 25 X 10 /L c. Hgb < 10g/dl d. Peripheral blasts 1% or higher e. Constitutional symptoms (e.g., fatigue, weakness, shortness of breath, weight loss, night sweats, or bone pain), AND 2. Prescription must be prescribed by an Oncologist or Hematologist, AND 3. Patient must have documented palpable splenomegaly ≥ 5cm below costal margin, AND 4. Patient must have a recent (with in the last month) creatinine clearance >15 ml/min, AND 5. Patient must have a recent (with in the last 9 month) CBC with platelet count >50 X 10 /L. 6. Duration of approval is for 12 months. 7. For purposes of re-authorization, there is documentation supporting reduction of spleen size or symptom improvement. New Starts Only Duration of Approval Notes System edits apply for prescription claims submitted for more than twice daily dosing. ® Jakafi is considered a specialty drug and will be included in the Mandatory Specialty Program. 173 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Antivirals Fuzeon® (enfuvirtide) Criteria 1. For new starts, patient must have a diagnosis of HIV-1; AND 2. Fuzeon must be used in combination with other anti-retroviral agents; AND 3. Patient must be anti-retroviral treatmentexperienced; AND 4. Evidence of HIV-1 replication despite ongoing anti-retroviral therapy; AND 5. Patient or caregiver is able to demonstrate appropriate techniques for administration of Fuzeon. Duration of Approval Long-term Notes 174 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Antivirals, continued All Primary Oral Hepatitis C Treatments Harvoni® (ledipasvir/sofosbuvir) Olysio® (simeprevir) Sovaldi® (sofosbuvir) Victrelis® (boceprevir) Criteria 1. Therapy is prescribed by a hepatologist, gastroenterologist, or infectious disease specialist; AND 2. Patient must have compensated liver disease (CPT A {CPT score <6}; not CPT B or C); AND 3. Patient has advanced fibrosis as documented by a. Liver biopsy-proven fibrosis staging score of F3 or F4 on the IASL, Batts-Ludwig, or Metavir fibrosis staging scales; OR b. Liver biopsy fibrosis staging score greater than or equal to F4 on the Ishak fibrosis staging scale; OR c. If documentation contraindicating a liver biopsy is provided, medical imaging-proven fibrosis staging score of F3 or F4 on IASL, Batt-Ludwig, or Metavir scales or greater than or equal to F4 on Ishak scale; AND 4. Patient has abstained from the use of unauthorized or illicit drugs and alcohol for a minimum of 3 months immediately prior to therapy as evidenced by a MAPS report and blood serum testing (results must be submitted with request and include COC, THC, OPI, AMP, BZO, BAR, BUP, MDMA, MTD, OXY); AND 5. Patient has not initiated treatment to facilitate cessation of drug and/or alcohol abuse in the last 6 months; AND 6. If patient has a history of substance abuse, patient must be enrolled in HealthPlus case Management for the duration of treatment as deemed appropriate by HealthPlus case Management; AND 7. Patient must not have received a liver transplant; AND 2 8. Patient has eGFR >30ml/min/1.73m ; AND 9. Patient does not have significant or unstable heart disease (indicated by NYHA Functional Class III-IV or Objective Assessment Class C-D); AND 10. A quantitative HCV-RNA test must be drawn at week 4 to evaluate patient response, adherence to therapy, and/or treatment futility if applicable; AND 11. Authorization of primary oral Hepatitis C agents is limited to one treatment course per lifetime; 12. Patient must sign an acknowledgment of criteria prior to initiation of therapy; AND drug specific criteria are met. Duration of Approval Notes All Hepatitis C treatments (primary/adjunctive/oral/injectable) are included in the mandatory specialty program. Prescriptions are limited to 14 day supplies to monitor adherence to therapy. 175 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Antivirals All Primary Oral Hepatitis C Treatments, continued Harvoni® (ledipasvir/sofosbuvir) Olysio® (simeprevir) Sovaldi® (sofosbuvir) Victrelis® (boceprevir) Criteria Harvoni: 1. Patient is ≥18 yo and must have a documented diagnosis of Hepatitis C genotype 1; AND 2. Patient’s current medications have been reviewed for potential interactions. Patient is not taking any medication that significantly interacts with Harvoni. 2 a. Patient is not receiving antacids, H -receptor antagonists, or proton pump inhibitors, St. John’s wort, or any other any medications that would reduce the concentration of ledipasvir or sofosbuvir; AND b. Patient is not taking digoxin, rosuvastatin, or any other drug which could result in increased levels of these drugs in the presence of Harvoni; AND 3. Patient is not nursing or pregnant; AND 4. Baseline HCV-RNA level is submitted; AND 5. Patient has met all class criteria for oral hepatitis C therapy agents. Duration of Approval Duration of approval is dependent on treatment experience, presence of cirrhosis and viral load prior to therapy initiation. Treatment-naïve patients without cirrhosis who have pre-treatment HCV RNA less than 6 million IU/mL: 8 weeks Treatment-naïve with or without cirrhosis: 12 weeks Treatmentexperienced without cirrhosis: 12 weeks Treatmentexperienced with cirrhosis: 24 weeks Notes Viral loads (HCV-RNA test) should be drawn at 4 weeks to monitor patient response and adherence to therapy. Quantity is limited to 14 tablets per 14 days. 176 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Antivirals All Primary Oral Hepatitis C Treatments, continued Harvoni® (ledipasvir/sofosbuvir) Olysio® (simeprevir) Sovaldi® (sofosbuvir) Victrelis® (boceprevir) Criteria Olysio: 13. Patient must have a documented diagnosis of Hepatitis C genotype 1 without an NS3 Q80K polymorphism; AND 14. Patient has concurrent therapy with both ribavirin and pegylated interferon; AND 15. Patient has not received HCV treatment with a protease inhibitor in the past; AND 16. Patient does not have an allergy to sulfonamides; AND 17. Patient’s current medications have been reviewed for potential interactions. Patient is not receiving any medications that are not recommended for use with Olysio (simeprevir); AND 18. Viral loads (HCV-RNA test) must be drawn at 4 weeks after starting therapy. Treatment is considered futile and prior authorization will be rescinded if HCV-RNA level is >25 IU/mL after 4 weeks. Duration of Approval Notes Olysio: Initial duration of approval is for 6 weeks. Authorization is renewed for an additional 6 weeks provided HCV-RNA levels at week 4 are not indicative of treatment futility Sovaldi: 13. Patient must have a documented diagnosis of Hepatitis C genotype 1, 2, 3, or 4; AND 14. Patient’s current medications have been reviewed for potential interactions. Patient is not receiving any medications that are not recommended for use with Sovaldi (sofosbuvir); AND 15. Has concurrent therapy with both ribavirin and pegylated interferon if genotype 1 or genotype 4 for 12 weeks; OR 16. Has concurrent therapy with ribavirin if genotype 2 for 12 weeks; OR 17. Has concurrent therapy with ribavirin if genotype 3 for 24 weeks; OR 18. Has concurrent therapy with ribavirin for 24 weeks if genotype 1 and the patient is ineligible to receive an interferon-based regimen; AND 19. Authorization can be extended for up to 48 weeks or until the time of liver transplantation, whichever comes first, to prevent post-transplant HCV reinfection in patients with hepatocellular carcinoma. 177 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Antivirals All Primary Oral Hepatitis C Treatments, continued Harvoni® (ledipasvir/sofosbuvir) Olysio® (simeprevir) Sovaldi® (sofosbuvir) Victrelis® (boceprevir) Criteria Duration of Approval Notes Victrelis: 13. Patient must have a documented diagnosis of Hepatitis C (HCV) genotype 1, AND 14. Patient has concurrent therapy with both ribavirin and pegylated interferon, AND 15. Patient has not received HCV treatment with a protease inhibitor in the past, AND 16. Viral loads (HCV-RNA test) must be drawn at 8, 12, and 24, weeks after starting therapy. Treatment is considered futile and prior authorization will be rescinded if HCVRNA level is ≥1000 IU/ml at week 8, ≥100 IU/ml at week 12, or detectable at week 24; AND 17. Initial duration of approval is for 10 weeks; AND 18. Authorization is renewed for an additional 4 weeks provided HCV-RNA levels at week 8 are not indicative of treatment futility; AND 19. Authorization is renewed for an additional 12 weeks if HCV-RNA levels at week 12 are not indicative of treatment futility; AND 20. Authorization can be approved for up to a total of 48 weeks, in accordance with prescribing guidelines, if HCVRNA is undetectable at week 24. 178 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Antivirals, continued Intron A® (interferon alpha-2b) Criteria 1. For diagnosis of hairy cell leukemia, malignant melanoma, follicular lymphoma, AIDS related Kaposi's Sarcoma and CML, patients must be >18 years of age; OR 2. For the diagnosis of condylomata acuminata, documented failure of, or intolerance to, traditional treatment modalities (e.g., podofilox, imiquimod, acid-therapy, or surgical options); OR 3. For the diagnosis of chronic hepatitis B, patients must have documented liver disease and hepatitis B viral replication; OR 4. For the diagnosis of chronic hepatitis C, allow 6month initial authorization and 6-month renewal permitted if the patient has Genotype 1 HCV; or has initial viral load >2 million copies/mL. Duration of Approval Approvals for diagnosis of condylomata acuminata should be approved for 4 months. Notes Approvals for all other diagnoses should be approved for 6 months. 179 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Antivirals, continued On Formulary with PA: Pegasys, Proclick® (pegylated interferon alfa-2a) Non-Formulary with PA: Peg-Intron® (pegylated interferon alfa-2b) RibaPak® (ribavirin) RibaTab® (ribavirin) Criteria 1. Patient has diagnosis of Hepatitis B or C, AND 2. Peg-Intron requires prior authorization for documented failure of or intolerance to Pegasys, AND 3. Approval is for 48 weeks provided that HCV-RNA levels are not indicative of treatment futility. Viral loads (HCV RNA test) must be drawn to evaluate treatment futility. a. For pegylated interferon in combination with ribavirin, prior authorization will be rescinded if HCV-RNA is detectable after 24 weeks. b. For combination therapy involving a protease inhibitor, patient must meet criteria associated with the protease inhibitor. Prior authorization will be rescinded if: 1. HCV-RNA level is >100 IU/ml after 12 or 24 weeks of combination therapy with Victrelis New Starts Only 1. Patient must have a chart documented trial or Rx claims for generic ribavirin 200 mg tablets or capsules. Duration of Approval Initial authorization approved for 6 months. Notes Renewal approved for 6 months. -renewal permitted if the patient has Genotype 1 HCV; or has initial viral load >2 million copies/mL. 180 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Antivirals, continued Synagis® (palivizumab) 1. 2. 3. 4. 5. 6. Criteria Infants and children younger than 2 years of age with documented chronic lung disease (CLD), born less than 32 weeks gestation, who have required medical therapy (e.g., supplemental oxygen, bronchodilator, diuretics, or corticosteroid therapy) for their CLD within 6 months before the anticipated RSV season may receive a maximum of 5 monthly doses; OR Infants born at 28 weeks gestation (up to and including 28 weeks, 6 days) or earlier without CLD and who are 12 months of age or younger may receive a maximum of 5 monthly doses; OR Infants and children who are 12 months or younger with hemodynamically significant cyanotic or acyanotic congenital heart disease (CHD) or severe immunodeficiencies may receive a maximum of 5 doses. Infants and children who have either congenital abnormalities of the airway or a neuromuscular condition that compromises handling of respiratory secretions may receive a maximum of 5 doses during the first year of life. Infants and children less than 24 months of age who undergo cardiac transplantation during the RSV season. Infants and children less than 24 months of age who are profoundly immunocompromised (e.g., solid organ or hematopoietic stem cell transplantation or receiving chemotherapy) during the RSV season. Duration of Approval Approved for 5 months interval, during the region's RSV season, beginning as soon as October and ending as late as April. Notes Monthly prophylaxis should be discontinued for any child who is hospitalized for RSV. 181 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Bisphosphonates Reclast® (zoledronic acid) Criteria 1. Creatinine clearance is > 35 ml/min; AND 2. Documented failure of, or intolerance to, an oral bisphosphonate agent; AND 3. Patient has a diagnosis of osteoporosis or is postmenopausal with osteopenia as indicated by a t-score <-1; OR 4. Diagnosis of Paget’s disease; OR 5. Patient is considered high-risk (e.g., recent lowtrauma hip fracture) and Reclast® is indicated for secondary fracture prophylaxis. Duration of Approval Approved for 1 year Dose optimization not to exceed 5mg once a year (with the exception of Paget’s disease) Notes Retreatment may be necessary for patients with Paget’s disease who have relapsed, so there is no defined dosing frequency. When treating Paget’s disease, patients should receive 1500 mg elemental calcium daily in divided doses (750 mg two times a day, or 500 mg three times a day) and 800 IU vitamin D daily, particularly in the 2 weeks following administration to prevent hypocalcemia. For osteoporosis treatment (postmenopausal, in men, and glucocorticoid induced), concomitant treatment with an average of at least 1200 mg calcium and 800-1000 IU vitamin D daily is recommended (dietary + supplemental). Cystic Fibrosis Treatments Kalydeco® (ivacaftor) 1. Patient has a diagnosis of cystic fibrosis with documentation of a G551D, G1244E, G1349D, G551S, S1251N, S549N, or S549R mutation in the CFTR gene; AND 2. Patient must be 6 years of age or older; AND 3. Patient must have a recent (within the Last 3 months) liver function panel. Note: Kalydeco is carved out to MDCH for HealthPlus Partners Medicaid members. Approved for 1 year Quantity is limited to 60 units per 30 days. 182 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Enzymes Ceredase® (alglucerase) Cerezyme® (imiglucerase) VPRIV™ (velaglucerase alfa) Criteria 1. The patient must have a diagnosis of Type 1 (nonneuronopathic or adult) Gaucher's disease with evidence of at least 1 of the following: - Moderate to severe anemia OR - Thrombocytopenia OR - Bone disease OR - Hepatomegaly OR - Splenomegaly Duration of Approval Long-term Evaluate initially at 3 month intervals for maintenance dose reductions/ development of sensitivity Fabrazyme® (agalsidase) 1. The patient must have diagnosis of Fabry disease Evaluate in 3 months for response/development of sensitivity Myozyme® (alglucosidase alfa) 1. The patient must have diagnosis of Pompe disease (GAA deficiency) Evaluate in 3 months for response/development of sensitivity Notes Recommended dose: Ceredase and Cerezyme Initial dosage may begin at 2.5 units/kg of body weight infused 3 times a week up to as much as 60 units/kg administered as frequently as once a week or as infrequently as every 4 weeks. Precaution: Patients may develop antibodies to Ceredase VPRIV Dose 60units/kg IVPB every other week. Recommended dose: 1mg/kg infused once every 2 weeks Pt should receive antipyretics prior to infusion Precaution: Most patients will develop IgG antibodies to Fabrazyme; physicians should periodically monitor IgE levels/Fabrazyme sensitivity Recommended dose: 20 mg/kg body weight infused every 2 weeks Precaution: Risk of hypersensitivity and sudden cardiac death 183 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Erythrocyte Stimulating Agents Aranesp® (darbepoetin alfa) Epogen® (epoetin alfa) Procrit® (epoetin alfa) 1. 2. 1. Growth Factor, Recombinant Insulin-like Increlex® (mecasermin [rDNA origin] injection) 1. 2. 3. 4. 5. Criteria The patient must have a diagnosis of anemia associated with a. chronic renal failure, OR b. cancer treated with chemotherapy, OR c. zidovudine-treated HIV infection, OR d. hepatitis C, OR e. chronic disease, OR f. prematurity, OR g. myelodysplastic syndrome, OR h. rheumatoid arthritis, AND Hgb level is < 11g/dL or < 10g/dL if on cancer chemotherapy; OR Treatment is needed to reduce the need for allogenic blood transfusion prior to surgery for anemic patients (Hgb >10 to < 13g/dL) who are at high risk for perioperative blood loss from elective, non-cardiac, non-vascular surgery. Patient has a diagnosis of primary IGF-1 deficiency or GH gene deletion, AND Increlex is prescribed by or after consultation with a pediatric endocrinologist, AND Patient is 2 years to 18 years of age, AND Epiphyses are open, AND Patient’s bone age is < 16 years for males or < 14 years for females Duration of Approval Notes For each of the conditions listed (except for allogenic blood transfusion), therapy is to be discontinued when Hgb level > 11g/dL OR after 8 weeks of therapy if there has been no response as measured by hemoglobin levels. 1 year Starting dose: 0.04 to 0.08 mg/kg (40 to 80 mcg/kg) subcutaneously twice daily. If well-tolerated for at least one week, the dose may be increased by 0.04 mg/kg per dose, to the maximum dose of 0.12 mg/kg given twice daily. Funduscopic exam is recommended at the initiation Limitations of use: Increlex® is not a substitute to GH for approved GH indications. 184 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Growth Hormones On Formulary with PA: Norditropin® Products (somatropin) Non-Formulary with PA: All other somatropin products Egrifta® Genotropin® Humatrope® Omnitrope® Nutropin® Nutropin AQ® Nutropin AQ NuSpin® Saizen® Serostim® Tev-Tropin™ Zorbtive® Criteria Pediatric patients: 1. Diagnosis of chronic renal failure and growth retardation; OR 2. Diagnosis of hypothalamic-pituitary lesions or panhypopituitarism; OR 3. Diagnosis of growth hormone (GH) deficiency; AND Patient must meet 3 of the 4 following criteria for documentation of growth failure: a. Height is >2 standard deviations below the mean for th age and sex (less than 5 percentile for age); AND b. Growth velocity is subnormal (age specific growth th rate at less than the 25 percentile); AND c. Bone age is delayed; AND d. Documented failure of at least one GH stimulation tests (defined as a peak growth hormone level of less than 10mcg/L after GH stimulation by insulin, arginine, clonidine, glucagon, or levodopa). GH stimulation tests not required with diagnosis of Turner Syndrome, Noonan Syndrome, or PraderWilli Syndrome; OR 4. Diagnosis of Idiopathic Short Stature (ISS); AND a. Height is >2 standard deviations below the mean for th age and sex (less than 5 percentile for age); AND b. Documentation that epiphyses are not closed. Adult patients: 1. Diagnosis of HIV and an unintentional weight loss of 10% over 12 months, 7.5% over 6 months or a BMI <20mg/kg; OR 2. Diagnosis of hypothalamic-pituitary lesions or panhypopituitarism; OR 3. Documented GH deficiency; OR 4. Diagnosis of Short Bowel Syndrome; AND 5. Patient is currently receiving specialized nutrition support directed by a healthcare professional (Total Parenteral Nutrition (TPN), Peripheral Parenteral Nutrition (PPN), or high-complex carbohydrate, low-fat diet) Both Pediatric and Adult patients: 1. Patient must have documented failure of, or intolerance ® to Norditropin before a non-preferred recombinant human growth hormone product will be approved. Duration of Approval Approved for 1 year Documentation required for pediatric renewal: 1. Growth rate has exceeded 2.5cm/year 2. Epiphyses remain open Notes Contraindicated for: -Diabetic retinopathy -Epiphyseal closure -Respiratory insufficiency -Sleep Apnea -Product specific hypersensitivities (Cresol, Benzyl Alcohol,Glycerin) -Active neoplastic disease -Intracranial hypertension -Acute critical illness -Prader-Willi Syndrome in Children 185 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Hormones Lupron Depot® (leuprolide) Criteria 1. The patient must have a diagnosis of uterine fibroid tumors, endometriosis, ovarian cancer or prostate cancer; AND 2. The patient must be 18 years of age or older. Lupron Depot-Ped® (leuprolide) 1. The patient has Central Precocious Puberty (CPP) and displays onset of secondary sexual characteristics earlier than age 8 for girls and 9 for boys; AND 2. The patient is less than 13 years old; AND 3. Diagnosis is confirmed by a pubertal gonadal sex steroid level or a pubertal LH response to stimulation by native GnRH; AND 4. Tumor has been ruled out by lab tests, CT, MRI or ultrasound. Duration of Approval Notes 186 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Immunomodulators Actemra® (tocilizumab) Criteria 1. A negative TB test before initiating therapy; OR 2. Treatment for latent TB infections must be initiated before treatment with Actemra; AND 3. Patient has no active infection (including bacterial sepsis, tuberculosis, invasive fungal and other opportunistic infections; AND 3 4. Patient has ANC >2000/mm AND Platelets 3 >100,000/mm AND ALT or AST <1.5x upper limits of normal; AND 5. Patient is not also receiving TNF antagonists, or other biologics (Enbrel, Humira, Remicade, Simponi, Cimzia, Kineret, Rituxan, Orencia), or live vaccines and diagnostic specific criteria are met. Duration of Approval Notes The dose of Actemra is 4mg/kg IV every 4 weeks; may increase to 8 mg/kg IV based on clinical response (Max: 800mg per infusion). Infuse over 60 minutes with infusion set. Rheumatoid Arthritis: 6. Diagnosis of moderate to severe rheumatoid arthritis; AND 7. Patient has documented failure of, or intolerance to, both formulary subcutaneous biologic agents (e.g., Humira and Enbrel); OR 8. The patient is not physically able to administer or is not an appropriate candidate for a subcutaneously administered biologic agent (e.g., Humira, Enbrel); AND 9. Documented failure of, intolerance or contraindication to, two other disease modifying antirheumatic drugs (DMARDS) (e.g., methotrexate, sulfasalazine, azathioprine, or hydroxychloroquine). Juvenile Idiopathic Arthritis (JIA)/Juvenile Rheumatoid Arthritis (JRA) / polyarticular juvenile idiopathic arthritis (PJIA): 6. Patient is > 2 years old; AND 7. Patient has a diagnosis of active systemic JIA/JRA/PJIA. AND 8. Patient has documented failure of, or intolerance to, both formulary subcutaneous biologic agents (e.g., Humira and Enbrel). 187 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Immunomodulators, continued Berinert® (C1 esterase inhibitor) Cinryze® (C1 esterase inhibitor) Firazyr® (icatibant) Criteria 1. The patient must have a diagnosis of hereditary angiodema or C1 inhibitor deficiency 2. The prescription must be written by an allergist, immunologist, or hematologist 3. For Firazyr, the patient must be 18 years of age or older. Duration of Approval Cimzia® (certolizumab pegol) 1. A negative TB test before initiating therapy; OR 2. Treatment for latent TB infections must be initiated before treatment with Cimzia; AND 3. Patient has no active infection (including influenza, systemic fungal or bacterial infections, or acute hepatitis B or C viral infections); AND 4. Patient is not also receiving Orencia, Kineret, Enbrel, Remicade or other anti-TNF therapy; AND diagnosis specific criteria are met. Approved for 1 year Notes . Crohn’s Disease: 5. Diagnosis of moderate to severe active Crohn’s disease with documented failure of, intolerance or contraindication to, conventional therapy (azathioprine, mesalamine, mercaptopurine, sulfasalazine, methotrexate, corticosteroids); AND 6. Patient has documented failure of, or intolerance to, Humira; AND 7. Dose is 400 mg at week 0, 2, and 4 weeks. If response, dose is 400 mg every 4 weeks. Rheumatoid Arthritis: 5. Diagnosis of moderately to severely active rheumatoid arthritis. AND 6. Patient has documented failure of, or intolerance to Humira and Enbrel; AND 7. Dose is 400 mg at week 0, 2, and 4, followed by 200 mg every other week. May consider 400 mg every 4 weeks for maintenance. 188 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Immunomodulators, continued Cimzia® (certolizumab pegol), continued Criteria Duration of Approval Notes Psoriatic Arthritis: 5. Diagnosis of active psoriatic arthritis; AND 6. Patient has documented failure of, or intolerance to Humira and Enbrel; AND 7. Dose is 400 mg at week 0, 2, and 4, followed by 200 mg every other week. May consider 400 mg every 4 weeks for maintenance. Ankylosing Spondylitis: 5. Diagnosis of active ankylosing spondylitis; AND 6. Patient has documented failure of, or intolerance to Humira and Enbrel; AND 7. Dose is 400 mg at week 0, 2, and 4, followed by 200 mg every other week or 400 mg every 4 weeks. 189 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Immunomodulators , continued Enbrel® (etanercept) 1. 2. 3. 4. Criteria A negative TB test before initiating therapy; OR Treatment for latent TB infections must be initiated before treatment with Enbrel; AND Patient has no active infection (including influenza, systemic fungal or bacterial infections, or acute hepatitis B or C viral infections); AND Patient is not also receiving Orencia, Kineret, Humira, Remicade or other anti-TNF therapy; AND diagnosis specific criteria are met. Duration of Approval Approved for 1 year Dose Optimization not to exceed 50mg twice a week Notes Patients with a latex allergy or sensitivity should not handle the prefilled syringe or autoinjector syringe since the needle cap(s) contain latex. Arthritis: 5. Diagnosis of rheumatoid arthritis (RA), juvenile RA (JRA), juvenile idiopathic arthritis (JIA), or psoriatic arthritis (JRA/JIA approved for ages 2-17). Psoriasis: 5. Diagnosis of plaque psoriasis; AND 6. Prescription is written by a dermatologist; AND 7. Documented failure of, intolerance or contraindication to, at least 2 traditional therapies (e.g., PUVA, UVB, methotrexate, or cyclosporine). Spondylitis: 5. Diagnosis of ankylosing spondylitis or juvenile spondyloarthropathy. 190 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Immunomodulators , continued Entyvio® (vedolizumab) Criteria 1. Diagnosis of moderately to severely active ulcerative colitis or Crohn’s disease; AND 2. Documented failure of, intolerance or contraindication to conventional therapy (azathioprine, mesalamine, mercaptopurine, sulfasalazine, methotrexate, corticosteroids); AND 3. Patient has documented failure of, or intolerance to Humira; OR 4. The patient is not physically able to administer or is not an appropriate candidate for a subcutaneously administered biologic agent (e.g., Humira) New Starts Only Duration of Approval Initial duration of approval is for 4 months. Authorization will be renewed with documentation of therapy response. Notes Patients not responding by week 14 are unlikely to respond and therapy should be discontinued. 191 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Immunomodulators, continued Humira® (adalimumab) Criteria 1. A negative TB test before initiating therapy; OR 2. Treatment for latent TB infections must be initiated before treatment with Humira; AND 3. Patient has no active infection (including influenza, systemic fungal or bacterial infections, or acute hepatitis B or C viral infections); AND 4. Patient is not also receiving Orencia, Kineret, Enbrel, Remicade or other anti-TNF therapy; AND diagnosis specific criteria are met. Duration of Approval Approved for 1 year Notes Patients with a latex allergy or sensitivity should not handle the needle cover of the syringe as it contains latex. Ankylosing Spondylitis OR Psoriatic Arthritis: 5. Diagnosis of ankylosing spondylitis or psoriatic arthritis. 6. The dose of Humira is 40mg administered subcutaneously every other week. Crohn’s Disease: 5. Diagnosis of moderate to severe Crohn’s disease; AND 6. Documented failure of, intolerance or contraindication to, conventional therapy (azathioprine, mesalamine, mercaptopurine, sulfasalazine, methotrexate, corticosteroids); AND 7. The dose of Humira is 160mg on day 1, 80mg on day 15 and then 40mg every other week starting on day 28. Juvenile Idiopathic Arthritis (JIA)/Juvenile Rheumatoid Arthritis (JRA): 5. Patient is 4 years of age and older; AND 6. Patient has moderately to severely active polyarticular JIA/JRA. 7. The dose of Humira for patients: - 15 kg (33 lbs) to <30 kg (66 lbs) is 20 mg administered subcutaneously every other week. - ≥30 kg (66 lbs) is 40 mg administered subcutaneously every other week. 192 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Immunomodulators, continued Humira® (adalimumab), continued Criteria Duration of Approval Notes Psoriasis: 5. Diagnosis of chronic moderate to severe plaque psoriasis; AND 6. Documented failure of, intolerance or contraindication to, at least 2 traditional therapies (e.g. PUVA, UVB, methotrexate, or cyclosporine); AND 7. Prescription is written by a dermatologist. 8. The dose of Humira is 80 mg subcutaneously followed by 40 mg every other week starting 1 week after the initial dose. Rheumatoid Arthritis: 5. Diagnosis of rheumatoid arthritis; AND 6. The dose of Humira is 40mg every other week. Ulcerative Colitis: 5. Diagnosis of moderate-to-severe ulcerative colitis; AND 6. Documented failure of, intolerance or contraindication to, conventional therapy (azathioprine, mesalamine, mercaptopurine, sulfasalazine, methotrexate, corticosteroids); AND 7. The dose of Humira is 160mg on day 1, 80mg on day 15 and then 40mg every other week thereafter. Documentation of clinical remission must be submitted to continue therapy beyond 12 weeks. 193 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Immunomodulators, continued (FDA approved indications vary by product) Immune Globulin (IM) GamaSTAN™ Immune Globulin (IV) Carimune NF® Flebogamma® Gammagard® Gammagard S/D® Gammaked® Gammaplex® Gamunex® Privigen® Immune Globulin (SQ) Gamunex-C® Hizentra® Criteria Primary Immunodeficiencies [X-linked (congenital) agamma-globulinemia, X-linked (congenital) immunodeficiency with hyper-IgM, Hypogammaglobulinemia, Common variable immunodeficiency, and Combined immunodeficiency syndromes including: Wiskott-aldrich syndrome; severe combined immunodeficiency syndrome (SCIDs)] Duration of Approval 1 year Notes 1. A serum trough IgG of ≤400 mg/dl. (In rare circumstances where serum trough level is recommended >600 mg/dl, documentation should support rationale) Selective IgG subclass deficiencies with severe infection including Specific Antibody Deficiency (SAD) 1 year 1. Documentation of IgG subclass deficiency (Appendix 1), -or2. Documentation of severe polysaccharide nonresponsiveness (inability to make IgG antibody against diphtheria and tetanus toxoids, pneumococcal polysaccharide vaccine, or both), or3. Documentation of antigen testing with less than 4 fold increase in specific antibody titer and lack of protective antibody titer (specific IgG antibody titer <1.3 mcg/ml), -and4. Documented trial and failure of an antibiotic within the last year (for initial authorization only). 194 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Immunomodulators, continued (FDA approved indications vary by product) Immune Globulin (IM) GamaSTAN™ Immune Globulin (IV), continued Carimune NF ® Flebogamma® Gammagard® Gammagard S/D® Gammaked® Gammaplex® Gamunex® Privigen® Immune Globulin (SQ) Gamunex-C® Hizentra® Criteria Idiopathic Thrombocytopenia Purpura (ITP) Acute ITP 1. Platelet count <50,000/ul and rapid rise in platelet count is necessary prior to surgery, or to avoid/defer splenectomy, or patient is at risk for acute bleeding. Chronic ITP 1. Platelet count is low < 30,000/ul, -and2. Age ≥10 years of age, -and3. Duration of illness > 6 months, -and4. Documented failure of, intolerance, or contraindication to at least 3 of the following: corticosteroids, rituximab, danazol, colchicine, dapsone, cyclophosphamide, azathioprine, mycophenolate, cyclosporine, chemotherapy -or5. Splenectomy ITP in pregnancy rd 1. Platelets <30,000/ul in 3 trimester, -or2. Previously delivered infants with autoimmune thrombocytopenia and platelet counts <75,000/ul during current pregnancy, -and3. Documented failure of, intolerance, or contraindication to corticosteroids, -or4. Splenectomy Kawasaki syndrome/Mucocutaneous Lymph Node Syndrome (MCLS) 1. Therapy is started within 10 days of fever, -and2. Concurrent aspirin administration. Duration of Approval Acute ITP 1 week Notes Chronic ITP 1 year ITP in pregnancy 1year 1 week 195 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Immunomodulators, continued (FDA approved indications vary by product) Immune Globulin (IM) GamaSTAN™ Immune Globulin (IV), continued Carimune NF ® Flebogamma® Gammagard® Gammagard S/D® Gammaked® Gammaplex® Gamunex® Privigen® Immune Globulin (SQ) Gamunex-C® Hizentra® Criteria Allogeneic (genetically similar donor) bone marrow transplant 1. Therapy is started within the first 100 days post transplant, -or2. Patient is 100 days post transplant, -and3. IgG levels < 400 mg/dl (exception made for patients who underwent transplantation for multiple myeloma or malignant macroglobulinemia because total IgG concentration is affected by their underlying paraproteinemia, -or4. Patient has history of CMV or RSV. Duration of Approval 4 months Chronic Lymphocytic Leukemia (CLL) 1. Immunoglobulin (IgG) level of < 600 mg/dl, -and2. Documented trial and failure of an antibiotic within the last year (for initial authorization only) 1 year Pediatric HIV infection 1. Documentation of ≥2 bacterial infections in a 1 year period, -or2. Patient has HIV-associated thrombocytopenia, or3. Patient has bronchiectasis, -or3 4. Documentation of T4 cell count ≥200 /mm 1 year Notes 196 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Immunomodulators, continued (FDA approved indications vary by product) Immune Globulin (IM) GamaSTAN™ Immune Globulin (IV), continued Criteria Acute and Chronic Inflammatory Demyelinating Polyneuropathy (CIDP)/Guillian-Barre Syndrome (GBS) For Chronic CIDP: 1. Documented failure of, intolerance, or contraindication to prednisone or azathioprine, or2. Documented plasma exchange. Duration of Approval Not limited For GBS 1. Patient must initiate within first four weeks of illness. Carimune NF ® Flebogamma® Gammagard® Gammagard S/D® Gammaked® Gammaplex® Gamunex® Privigen® Post transfusion purpura 1. Platelet count less than 10,000/ul, -and2. Infusion must be within 14 days of bleeding post transfusion, -and3. Documented failure of, intolerance, or contraindication to corticosteroids, -or4. Documented plasma exchange. 1 month (to account for relapse) Immune Globulin (SQ) Multiple Sclerosis (MS) 1. Patient must have relapse-remitting MS only (not primary or secondary progressive MS), -and2. Documented treatment with, intolerance, or contraindication to any interferon therapy (Betaseron, Avonex, or Rebif). 1 year Gamunex-C® Hizentra® Notes 197 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Immunomodulators, continued (FDA approved indications vary by product) Immune Globulin (IM) GamaSTAN™ Immune Globulin (IV), continued Carimune NF ® Flebogamma® Gammagard® Gammagard S/D® Gammaked® Gammaplex® Gamunex® Privigen® Criteria Myasthenia Gravis (MG) and Lambert-Eaton (LE) Myasthenia MG: 1. Documented failure of, intolerance, or contraindication to at least 2 of the following: anticholinesterases (eg., Mestinon, Prostigmin), corticosteroids, cyclosporine, cyclophosphamide, or azathioprine. LE : 1. Documented failure of, intolerance, or contraindication to anticholinesterases (eg. Mestinon,Prostigmin), -or2. Documented plasma exchange. Duration of Approval 1 week Dermatomyositis and Polymyositis 1. Documented failure of, intolerance, or contraindication to at least 2 of the following: corticosteroids, methotrexate, azathioprine, cyclophosphamide, or cyclosporine. 6 months Systemic Lupus Erythematosus (SLE) 1. Documentation of severe (solid organ involvement), active SLE, -and2. Documented failure of, intolerance, or contraindication to at least 2 of the following: corticosteroids. methotrexate, azathioprine, or cyclophosphamide Not limited Notes Immune Globulin (SQ) Gamunex-C® Hizentra® 198 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Immunomodulators, continued (FDA approved indications vary by product) Immune Globulin (IM) GamaSTAN™ Immune Globulin (IV), continued Carimune NF ® Flebogamma® Gammagard® Gammagard S/D® Gammaked® Gammaplex® Gamunex® Privigen® Immune Globulin (SQ) Gamunex-C® Hizentra® Criteria Autoimmune mucocutaneous blistering diseases, including Pemphigus vulgaris, Pemphigus foliaceus, Bullous pemphigoid, Mucous membrane pemphigoid, Epidermyolysis bullosa 1. Documented failure of, intolerance, or contraindication to atleast 2 of the following: corticosteroids. methotrexate, azathioprine, or cyclophosphamide, -or2. Documentation of rapidly progressive disease in which a clinical response could not be affected quickly enough using prerequisite therapies. Duration of Approval 6 months Multifocal Motor Neuropathy 1. Diagnosis is required Not limited Stiff Person Syndrome 1. Diagnosis is required Not limited Fetal/neonatal alloimmune thrombocytopenia (FAIT/NAIT) 1. Diagnosis is required Not limited Hemolytic disease of the newborn 1. Diagnosis is required Not limited Hemolytic Uremic Syndrome 1. Diagnosis is required Not limited Complications of transplanted organs (including solid organ and bone marrow) 1. Diagnosis is required Not limited Notes 199 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Immunomodulators, continued Kineret® (anakinra) 1. 2. 3. 4. Criteria A negative TB test before initiating therapy; OR Treatment for latent TB infections must be initiated before treatment with Kineret; AND Patient has no active infection (including influenza, systemic fungal or bacterial infections, or acute hepatitis B or C viral infections); AND Patient is not also receiving Orencia, Enbrel, Remicade or other anti-TNF therapy; AND diagnosis specific criteria are met. Duration of Approval Approved for 1 year Notes Patients with a latex allergy or sensitivity should not handle the Kineret needle cover as it contains latex. Kineret should not be given by intravenous administration or intramuscular administration. Rheumatoid Arthritis: 5. The patient must be >18 years of age; AND 6. Diagnosis of rheumatoid arthritis; AND 7. Documented failure of, or intolerance to, methotrexate; AND 8. Documented failure of, or intolerance to, another disease modifying antirheumatic drug (DMARD) (e.g., azathioprine, leflunomide, cyclosporine, penicillamine, sulfasalazine); AND 9. Patient has documented failure of, or intolerance to Humira and Enbrel; AND 10. The dose of Kineret is 100mg administered subcutaneously once daily. Cryopyrin-Associated Periodic Syndromes 5. The patient must be diagnosed with NeonatalOnset Multisystem Inflammatory Disease (NOMID); AND 6. The max dose is 8mg/kg per day 200 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Immunomodulators, continued Orencia® (abatacept) Criteria 1. A negative TB test before initiating therapy; OR 2. Treatment for latent TB infections must be initiated before treatment with Orencia; AND 3. Patient has no active infection (including influenza, systemic fungal or bacterial infections, or acute hepatitis B or C viral infections); AND 4. Patient is not also receiving Cimzia, Kineret, Enbrel, or Remicade or other anti-TNF therapy; AND 5. For infused Orencia, the patient has documented failure of, intolerance to, or is not physically able to administer the subcutaneous formulation of Orencia; AND diagnosis specific criteria are met. Duration of Approval Approved for 1 year Notes Arthritis: 6. Diagnosis of moderate to severe rheumatoid arthritis; OR 7. Diagnosis of moderate to severe polyarticular juvenile rheumatoid arthritis (JRA)/juvenile idiopathic arthritis (JIA); (JRA/JIA approved for > 6 years of age). 8. Patient has documented failure of, intolerance or contraindication to, two other disease modifying antirheumatic drugs (DMARDS) (e.g., methotrexate, sulfasalazine, azathioprine, or hydroxychloroquine); AND 9. Patient has documented failure of, or intolerance to both formulary subcutaneous biologic agents (e.g., Humira and Enbrel). 201 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Immunomodulators, continued Otezla® (apremilast) Criteria Duration of Approval Notes Psoriatic Arthritis: 1. Diagnosis of active psoriatic arthritis; AND 2. Documented failure of, intolerance or contraindication to, NSAID therapy; AND 3. Documented failure of, or intolerance to, one other disease modifying antirheumatic drug (DMARDS) (e.g., methotrexate, sulfasalazine, leflunomide); AND 4. Patient has documented failure of, or intolerance to both formulary subcutaneous biologic agents (e.g., Humira and Enbrel); OR 5. The patient is not physically able to administer or is not an appropriate candidate for a subcutaneously administered biologic agent (e.g., Humira, Enbrel) Psoriasis: 1. Diagnosis of chronic moderate to severe plaque psoriasis; AND 2. Documented failure of, intolerance or contraindication to, at least 2 traditional therapies (e.g. PUVA, UVB, methotrexate, or cyclosporine); AND 3. Prescription is written by a dermatologist; AND 4. Patient has documented failure of, or intolerance to both formulary subcutaneous biologic agents (e.g., Humira and Enbrel); OR 5. The patient is not physically able to administer or is not an appropriate candidate for a subcutaneously administered biologic agent (e.g., Humira, Enbrel) 202 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Immunomodulators, continued Remicade® (infliximab) Criteria 1. A negative TB test before initiating therapy; OR 2. Treatment for latent TB infections must be initiated before treatment with Remicade; AND 3. Patient has no active infection (including influenza, systemic fungal or bacterial infections, or acute hepatitis B or C viral infections); AND 4. Patient is not also receiving Orencia, Kineret, Enbrel, or Humira or other anti-TNF therapy; AND 5. Diagnosis specific criteria are met. Duration of Approval Approved for 1 year Notes Ankylosing Spondylitis OR Psoriatic Arthritis: 6. Diagnosis of ankylosing spondylitis or psoriatic arthritis; AND 7. Patient has documented failure of, or intolerance to both formulary subcutaneous biologic agents (e.g., Humira and Enbrel); OR 8. Patient has documented failure of, or intolerance to, or inability to inject a formulary subcutaneously administered anti-TNF agent (e.g., Humira, Enbrel); AND 9. The maintenance dose is a maximum of 5 mg/kg every 6 weeks (Ankylosing Spondylitis) or every 8 weeks (Psoriatic Arthritis). Crohn’s Disease: 6. Patient is > 6 years old; AND 7. Patient has a diagnosis of moderate to severe Crohn’s disease; OR 8. Diagnosis of Crohn’s disease with draining enterocutaneous fistulae; AND 9. Documented failure of, or intolerance to, mesalamine and corticosteroids and 6-mercaptopurine or azathioprine; AND 10. Patient has documented failure of, or intolerance to, or inability to inject a formulary subcutaneously administered anti-TNF agent (e.g., Humira); AND 11. The maintenance dose is a maximum of 10mg/kg every 8 weeks. 203 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Immunomodulators, continued Remicade® (infliximab) continued Criteria Duration of Approval Notes Psoriasis: 6. Prescription is written by a dermatologist; AND 7. Patient has diagnosis of chronic, severe (i.e., extensive and/or disabling) plaque psoriasis; AND 8. Documented failure of, or intolerance to, at least 2 traditional therapies (e.g., PUVA, UVB, methotrexate, or cyclosporine); AND 9. Patient has documented failure of, or intolerance to both formulary subcutaneous biologic agents (e.g., Humira and Enbrel); OR 10. The patient is not physically able to administer or is not an appropriate candidate for a formulary subcutaneously administered biologic agent (e.g., Humira, Enbrel); AND 11. The maintenance dose is a maximum of 5 mg/kg every 8 weeks. Rheumatoid Arthritis: 6. Diagnosis of rheumatoid arthritis; AND 7. Patient has documented failure of, or intolerance to, two other disease modifying antirheumatic drugs(DMARDS) (e.g., methotrexate, sulfasalazine, azathioprine, or hydroxychloroquine); AND 8. Patient has documented failure of, or intolerance to both formulary subcutaneous biologic agents (e.g., Humira and Enbrel); OR 9. The patient is not physically able to administer or is not an appropriate candidate for a formulary subcutaneously administered biologic agent (e.g., Humira, Enbrel); AND 10. The maintenance dose is a maximum of 10mg/kg every 4 weeks. 204 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Immunomodulators, continued Remicade® (infliximab), continued Criteria Duration of Approval Notes Ulcerative Colitis: 6. Patient has moderately to severely active ulcerative colitis and required high dose systemic corticosteroid use; OR 7. Patient has documented inadequate response to conventional therapy (e.g., mesalamine (5-ASA), azathioprine, mercaptopurine); AND 8. Patient has documented failure of, or intolerance to formulary subcutaneous biologic agents (e.g., Humira); OR 9. The patient is not physically able to administer or is not an appropriate candidate for a formulary subcutaneously administered biologic agent (e.g., Humira); AND 10. The maintenance dose is a maximum of 5 mg/kg every 8 weeks. Uveitis: 6. Diagnosis of Uveitis Associated with Behcet’s Syndrome; AND 7. The maintenance dose is a maximum of 5 mg/kg every 8 weeks. 205 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Immunomodulators, continued Rituxan® (rituximab) Criteria 1. Prescription is written by an oncologist or hematologist; OR 2. The patient has a diagnosis of moderate to severe rheumatoid arthritis; AND 3. Patient has no active infection (including influenza, systemic fungal or bacterial infections, or acute hepatitis B or C viral infections); AND 4. Patient is not also receiving Cimzia, Kineret, Enbrel, or Remicade or other anti-TNF therapy; AND 5. Patient has documented failure of, or intolerance to both formulary subcutaneous biologic agents (e.g., Humira and Enbrel); OR 6. The patient is not physically able to administer or is not an appropriate candidate for a formulary subcutaneous biologic agent (e.g., Humira, Enbrel); AND 7. Documented failure of, or intolerance to, two other disease modifying antirheumatic drugs (DMARDS) (e.g., methotrexate, sulfasalazine, azathioprine, or hydroxychloroquine). Duration of Approval For a diagnosis of RA: Since safety and efficacy of retreatment have not been established in controlled trials and a limited number of patients have received two to five courses (two infusions per course) of treatment in an uncontrolled setting, the duration of approval for RA should be limited to 5 courses (3 months) with re-evaluation based on individual response. Notes The dose for use in RA is 2 x 1000mg IV infusions separated by 2 weeks. Glucocorticoids, administered as methylprednisolone 100mg IV or its equivalent, given 30 minutes prior to each infusion, are recommended to reduce the incidence and severity of infusion reactions. 206 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Immunomodulators, continued Simponi® (golimumab) Criteria 1. A negative TB test before initiating therapy; OR 2. Treatment for latent TB infections must be initiated before treatment with Simponi; AND 3. Patient has no active infection (including influenza, systemic fungal or bacterial infections, or acute hepatitis B or C viral infections); AND 4. Patient is not also receiving Orencia, Kineret, Enbrel, Remicade or other anti-TNF therapy; AND diagnosis specific criteria are met. Duration of Approval Approved for 1 year Notes Patients with a latex allergy or sensitivity should not handle the prefilled syringe or autoinjector syringe since the needle cover contains latex. Ankylosing Spondylitis OR Psoriatic Arthritis: 5. Diagnosis of ankylosing spondylitis or psoriatic arthritis; AND 6. Patient has documented failure of, or intolerance to Humira and Enbrel; AND 7. The dose of Simponi is 50mg administered subcutaneously once a month. Rheumatoid Arthritis: 5. Diagnosis of moderately to severely active rheumatoid arthritis; AND 6. Patient is receiving methotrexate concomitantly; AND 7. Patient has documented failure of, or intolerance to Humira and Enbrel; AND 8. The dose of Simponi is 50mg administered subcutaneously once a month. Ulcerative Colitis: 5. Diagnosis of moderate to severe active ulcerative colitis disease with documented failure of, intolerance or contraindication to, conventional therapy (azathioprine, mesalamine, mercaptopurine, sulfasalazine, methotrexate, corticosteroids). 6. Patient has documented failure of, or intolerance to, Humira. 7. The dose of Simponi is 200 mg administered subcutaneously, followed by 100 mg at week 2, and then 100 mg every 4 weeks, thereafter. 207 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Immunomodulators, continued Stelara® (ustekinumab) Criteria 1. A negative TB test before initiating therapy; OR 2. Treatment for latent TB infections must be initiated before treatment with Stelara; AND 3. Patient has no active infection (including bacterial, fungal or viral); AND diagnostic specific criteria are met Duration of Approval Notes Psoriasis: 4. Diagnosis of moderate to severe plaque psoriasis; AND 5. Prescription is written by a dermatologist; AND 6. Documented failure of, intolerance or contraindication to, at least two traditional therapies (e.g., PUVA, UVB, methotrexate, or cyclosporine); AND 7. Patient has documented failure of, or intolerance to Humira and Enbrel; AND 8. The dose is 45 mg (≤100 kg) or 90 mg (>100 kg) at weeks 0 and 4, followed by 45 mg (≤100 kg) or 90 mg (>100 kg) every 12 weeks. Psoriatic arthritis: 4. Diagnosis of active psoriatic arthritis; AND 5. Patient has documented failure of, or intolerance to Humira and Enbrel; AND 6. The dose is 45 mg at weeks 0 and 4, followed by 45 mg every 12 weeks; OR 7. With co-existent moderate to severe plaque psoriasis weighing >100 kg, the dose is 90 mg at week 0 and 4, followed by 90 mg every 12 weeks. 208 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Immunomodulators, continued Tysabri® (natalizumab) Criteria Duration of Approval Notes For patients with Multiple Sclerosis 1. Patient must have a diagnosis of a relapsing form of multiple sclerosis; AND 2. Patient has had treatment failure, contraindication, or intolerance to Copaxone (glatiramer acetate); AND 3. Patient is intolerant to both Avonex (interferon beta 1a) and Rebif (interferon beta 1a) (i.e. severe or intolerable injection site reactions or side effects); OR 4. Patient has had treatment failure, contraindication, or allergy to interferon therapy; AND 5. Patient must not be currently on combination therapy with Avonex, Rebif, Betaseron, Extavia, Copaxone, or Gilyena; AND 6. Patient must not be on concurrent immunosuppressive therapy; AND 7. Documentation of an MRI scan must be obtained for each patient with MS to help differentiate potential, future symptoms from progressive multifocal leukoencephalopathy (PML). For patients with Crohn’s Disease 1. Patient must have a diagnosis of moderate to severe of Crohn’s disease; AND 2. Patient must have had documented failure of, intolerance or contraindication to, conventional Crohn’s disease therapy (i.e. azathioprine, mesalamine, mercaptopurine, sulfasalazine, methotrexate, corticosteroids); AND 3. Patient must have had documented failure of, intolerance or contraindication to a, TNF-α inhibitor (i.e. Humira, Cimzia, Remicade); AND 4. Patient must not be currently on combination therapy with immunosuppressants or TNF-α inhibitors. New Starts Only 209 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Immunomodulators Xgeva™ (denosumab) Criteria 1. Patient has a diagnosis of bone metastases secondary to solid tumor; OR 2. The patient has a diagnosis of giant cell tumor of bone that is unresectable or where surgical resection is likely to result in severe morbidity. Duration of Approval 1 year Notes Dose: 120 mg every 4 weeks subcutaneously. For giant cell tumor, additional 120 mg doses are given on day 8 and 15 of the first month of therapy. Administer calcium and Vit D PRN to treat or prevent hypocalcemia Not indicated in patients with multiple myeloma. Immunomodulators, continued Cryopyrin-Associated Periodic Syndromes Arcalyst® (rilonacept) 1. Diagnosis of Cryopyrin-Associated Periodic Syndromes (CAPS), including Familial Cold Autoinflammatory Syndrome (FCAS) and MuckleWells Syndrome (MWS) in adults and children 12 years and older. Evaluate in 3 months for to determine patient response Recommended dose: Adults 18 yrs or older: Loading dose: 320mg Sub Q Maintenance dose:160mg SubQ once weekly Pediatric patients 12 to 17 yrs old: Loading dose:4.4mg/kg(to max of 320mg) SQ Maintenance dose: 2.2mg/kg SubQ once weekly *Dose should not be given more than once per week Precautions: Arcalyst should not be administered if patient has active or chronic infection. Patient should receive all recommended vaccinations prior to receiving Arcalyst. 210 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX D Brand (generic) Name Cryopyrin-Associated Periodic Syndromes Ilaris® (canakinumab) Criteria 1. Patient has no active or chronic infection (including influenza, systemic fungal or bacterial infections, or acute hepatitis B or C viral infections); AND 2. Diagnosis specific criteria are met Duration of Approval Long Term Notes Recommended dose: Adults, Adolescents, and Children >= 4 years of age and > 40kg: 150mg SC every 8 weeks. Adults, Adolescents, and Children >=4 years of age and 15-40kg: 2mg/kg SC every 8 weeks. Response is inadequate in children in this weight range, may consider dose increase to 3mg/kg SC every 8 weeks. Cryopyrin-Associated Periodic Syndromes (CAPS), including Familial Cold Autoinflammatory Syndrome (FCAS) and MuckleWells Syndrome (MWS) 3. Patient is > 4 years old; AND 4. Patient has a diagnosis of CAPS, FCAS, or MWS. Juvenile Idiopathic Arthritis (JIA)/Juvenile Rheumatoid Arthritis (JRA)/ polyarticular juvenile idiopathic arthritis (PJIA): 3. Patient is > 2 years old; AND 4. Patient has a diagnosis of active systemic JIA/JRA. AND 5. Patient has documented failure of, or intolerance to, both formulary subcutaneous biologic agents (e.g., Humira and Enbrel). Miscellaneous Samsca® (tolvaptan) 1. The patient must have clinically significant and euvolemic hyponatremia (serum sodium <125 mEq/L or less marked hyponatremia that is symptomatic and has resisted correction with fluid restriction); AND 2. Therapy will be initiated in an inpatient setting; AND 3. Maximum length of therapy is 30 days to minimize the risk of liver injury. Duration of approval is 30 days Quantity Limit: 15 mg (30 units per 30 days) 30 mg (60 units per 30 days) 211 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX 1 Brand (generic) Name Multiple Sclerosis, Adjunctive Agents Non-Formulary Ampyra® (dalfampridine) All Multiple Sclerosis, Disease-Modifying Agents On Formulary with PA Avonex®, Rebif® (interferon beta 1a) Copaxone® (glatiramer acetate) All Multiple Sclerosis, Disease-Modifying Agents Non-Formulary with PA Aubagio® (teriflunomide) Betaseron® (interferon beta 1b) Extavia® (interferon beta 1b) Plegridy® (peginterferon beta 1a) Tecfidera® (dimethyl fumerate) Criteria 1. The patient must have a diagnosis of Multiple Sclerosis; AND 2. The patient is ambulatory; AND 3. The patient has no history of a seizure disorder; AND 4. The patient must have a CrCl>50mL/min; AND 5. The patient must be receiving concurrent therapy with a disease modifying agent (i.e., Avonex, Betaseron, Copaxone); AND 6. The prescription is written by a neurologist; AND 7. For renewal, the patient has a documented 20% or greater improvement from baseline in a timed 25 foot walk. 1. Patient has a diagnosis of multiple sclerosis; OR 2. Patient has had signs and symptoms of Clinically Isolated Syndrome (CIS) suggestive of MS Duration of Approval 6 months Notes Quantity is limited to 60 units per 30 days. Long-term 1. Patient has a diagnosis of multiple sclerosis; OR 2. Patient has had signs and symptoms of Clinically Isolated Syndrome (CIS) suggestive of MS; AND 3. Patient has had treatment failure, contraindication, or intolerance to Copaxone (glatiramer acetate); AND 4. Patient is intolerant to both Avonex (interferon beta 1a) and Rebif (interferon beta 1a) (i.e. severe or intolerable injection site reactions or side effects); OR 5. Patient has had treatment failure, contraindication, or allergy to interferon therapy. 212 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX 1 Brand (generic) Name All Multiple Sclerosis, Disease-Modifying Agents Non-Formulary with PA, continued Gilenya® (fingolimod) 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. Criteria The patient must have documented diagnosis of a relapsing form of multiple sclerosis; There is documentation of the following within the last 6 months: a. CBC, Liver Function Tests, and b. Ophthalmologic Evaluation; and Physician must submit documentation that the first dose is administered in a setting with resources to appropriately manage symptomatic bradycardia. Setting allows for hourly patient monitoring of pulse and blood pressure for 6 hours for signs and symptoms of bradycardia, including an electrocardiogram prior to dosing, and at the end of the observation period. Patient has not had a recent (within the last six months) occurrence of MI, unstable angina, stroke, TIA, decompensated HF requiring hospitalization, or Class II/IV HF. Patient does not have a history or presence of Mobitz Type II 2nd degree or 3rd degree AV block or sick sinus syndrome, unless patient has a pacemaker. Patient has a QTc interval >/500ms. Patient is not receiving treatment with a Class 1a or Class III antiarrhythmic drug. Patients receiving concurrent therapy with drugs that slow heart rate (e.g., beta blockers, heart-rate lowering calcium channel blockers such as diltiazem or verapamil, or digoxin) must receive overnight continuous ECG monitoring with administration of first dose. Patient has had treatment failure, contraindication, or intolerance to Copaxone (glatiramer acetate); AND Patient is intolerant to both Avonex (interferon beta 1a) and Rebif (interferon beta 1a) (i.e. severe or intolerable injection site reactions or side effects); OR Patient has had treatment failure, contraindication, or allergy to interferon therapy. Duration of Approval Notes Quantity is limited to 30 units per month. Patient should not receive Gilenya concomitantly with another immunomodulator therapy for multiple sclerosis (e.g. Avonex, Rebif, Betaseron, Extavia, Copaxone, or Tysabri). 213 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX 1 Brand (generic) Name Neurological Xenazine® (tetrabenazine) Neuromuscular Blocking Agent Botox® Dysport® Xeomin® (botulism toxin type A) Parkinson’s Apokyn® (apomorphine) Pulmonary Cayston® (aztreonam for inhalation) Criteria 1. The patient must have a diagnosis of chorea associated with Huntington’s disease; AND 2. The patient must have documented failure of, intolerance to, or contraindication to at least two of the following: amantadine, an antipsychotic (fluphenazine, haloperidol, risperidone, ziprasidone, quetiapine or olanzapine), riluzole, or a benzodiazepine, AND 3. Prescription must be prescribed by a neurologist, AND 4. For doses greater than 50 mg/day, CYP2D6 genotyping is required. Duration of Approval 3 months 1. Patient must have a documented diagnosis of cervical dystonia. Approved 3 months 1. Diagnosis of Parkinson's Disease in advanced stages; AND 2. Documented two hours or more of "off" episodes ("end-of-dose wearing off" and unpredictable "on/off" episodes) despite aggressive oral therapy. 1. Patient must have pseudomonas aeruginosa in the lungs, AND 2. Patient must have cystic fibrosis, AND 3. Prescription must be written by a pulmonologist, or infectious disease specialist, AND 4. Patient must be 7 years of age or older, AND 5. FEV1 must be >25% or <75%. Long-term Notes Patients who do not express CYP2D6 (i.e., poor metabolizers of CYP2D6) require a daily dose of 37.5—50 mg, in 3 divided doses. Patients who do express CYP2D6 (i.e., intermediate or extensive metabolizers of CYP2D6) require a daily dose of at least 50 mg100mg in 3 divided doses. 214 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX 1 Brand (generic) Name Pulmonary, continued Xolair® (omalizumab) Criteria 1. Patient is over 12 years of age; AND 2. Diagnosis specific criteria are met. Moderate to severe allergic asthma: 3. Patient has a positive skin test or in vitro reactivity to a perennial aeroallergen; AND 4. Failure of, or intolerance to, maximum dose of oral inhaled steroids (medication compliance should be taken into consideration); AND/OR 5. Patient required long-term (>3months) oral steroids previously and had at least 1 ED or hospital admission during the last 6 months; AND 6. Maximum dose is 750 mg every 4 weeks. Rheumatoid Arthritis Misc. Xeljanz® (tofacitinib) Duration of Approval Approved 3 months to determine patient response. Notes The warnings for Xolair include malignancy and anaphylaxis. Renewals may be authorized long-term. Chronic idiopathic urticarial: 3. Patient has chart documented failure or contraindication to H1 antihistamines; AND 4. Maximum dose is 300 mg every 4 weeks. 1. Diagnosis of moderate to severe rheumatoid arthritis; AND 2. A negative TB test before initiating therapy; OR 3. Treatment for latent TB infections must be initiated before treatment with Xeljanz; AND 4. Patient has no active infection (including bacterial sepsis, tuberculosis, invasive fungal and other opportunistic infections); AND 5. Patient has a lymphocyte count >500 cells/mm3, ANC > 1000 cells/mm3, and hemoglobin level >9g/dL; AND 6. Patient is not also receiving TNF antagonists, or other biologics (e.g. Enbrel, Humira, Remicade, Simponi, Cimzia, Kineret, Rituxan, Orencia); AND 7. Patient has documented failure of, intolerance or contraindication to, two other disease- modifying antirheumatic drugs (DMARDS) (e.g., methotrexate, sulfasalazine, azathioprine, or hydroxychloroquine); AND 8. Patient has documented failure of, or intolerance to, both formulary subcutaneous biologic agents (e.g., Humira and Enbrel); OR 9. The patient is not physically able to administer or is not an appropriate candidate for a subcutaneously administered biologic agent (e.g., Humira, Enbrel). 215 HEALTHPLUS PRIOR AUTHORIZATION CRITERIA FOR SPECIALTY/INJECTABLE DRUGS APPENDIX 1 Appendix 1 (for Immune Globulin criteria): Normal Immunoglobulin Levels (mg/dl) Normal IgG Subclass Levels (mg/dl) AGE IgA IgG IgM AGE IgG1 IgG2 IgG3 IgG4 1 - 2 mo 1 - 53 251 - 906 20 - 87 cord 435 - 1084 143 - 453 27 - 146 1 - 47 2 - 3 mo 3 - 47 206 - 601 17 - 105 0 - 3 mo 218 - 496 40 - 167 4 - 23 1 - 33 3 - 4 mo 4 - 73 176 - 581 24 - 101 3 - 6 mo 143 - 394 23 - 147 4 - 100 1 - 14 4 - 5 mo 8 - 84 172 - 814 33 - 108 6 - 9 mo 190 - 388 37 - 60 12 - 62 1-1 5 - 6 mo 8 - 68 215 - 704 35 - 102 9 mo - 3 yr 286 - 680 30 - 327 13 - 82 1 - 65 6 - 8 mo 11 - 90 217 - 904 34 - 125 3 - 5 yr 381 - 884 70 - 443 17 - 90 1 - 116 8 mo – 1 yr 16 - 84 294 - 1069 41 - 149 5 - 7 yr 292 - 816 83 - 513 8 - 111 1 - 121 1 - 2 yr 14 - 106 345 - 1213 43 - 173 7 - 9 yr 442 - 802 113 - 480 15 - 133 1 - 84 2 - 3 yr 14 - 123 424 - 1051 48 - 168 9 - 11 yr 456 - 938 163 - 513 26 - 113 1 - 121 3 - 4 yr 22 - 159 441 - 1135 47 - 200 11 - 13 yr 456 - 952 147 - 493 12 - 179 1 - 168 4 - 6 yr 25 - 154 463 - 1236 43 - 196 13 - 15 yr 347 - 993 140 - 440 23 - 117 1 - 183 6 - 9 yr 33 - 202 633 - 1280 48 - 207 15 yr & up 422 - 1292 117 - 747 41 - 129 1 - 291 9 - 11 yr 45 - 236 608 - 1572 52 - 242 11 yr & up 70 - 312 639 - 1349 56 - 352 216 PRESCRIPTION BENEFIT LIMITATIONS APPENDIX E GENERAL LIMITATIONS (All Lines of Business) Michigan State Law Limitations: Schedule II prescriptions are not refillable, and must be filled within 90 days of the date prescription is actually written. Schedule III, IV, & V prescriptions are only refillable for 6 months from the date of the original prescription (if refills are indicated by the prescriber). Non-Scheduled prescriptions are refillable for 1 year from the date the prescription was actually written (if refills are indicated by the prescriber). HealthPlus Contractual Exclusions: Medications used for cosmetic purposes are not covered. Medications used in conjunction with the in-vitro fertilization procedure are not covered. Non-prescription drugs, dietary supplements and medical foods are not a covered benefit, with the exception of OTC medications specifically added to coverage by HealthPlus or medications required for coverage by health care reform. HealthPlus Administrative Limitations: Prescription drugs are limited to the reasonable cost of generically-available products, unless no generically-equivalent product exists or a member-specific review for medical necessity determines the need for the brand name medication. Prescription drugs are limited to FDA-approved indications when reviewed, unless a member-specific review for medical necessity determines the need for a particular medication for an off-label use. Prescriptions written by a Dentist are limited to those medications on the HealthPlus Dental Formulary. Prescriptions for testosterone products are limited to male members only, unless a member-specific review for a female member determines medical necessity or if the medication is being used for an FDA-approved indication. Prescriptions for products that contain estrogen are limited to female members only. Prior Authorization based on specific criteria is required for medications included in the Pharmacy Prior Authorization Program including the Dose Optimization Program. Coverage for medications included in the Dose Optimization Program is limited to once daily dosing, or maximum dose recommendations with quantity limits, unless a member specific review determines medical necessity for the specified dosing regimen. Coverage for specific migraine medications is limited to 9 tablets per month, unless a member specific review determines that the member is also currently taking medication for the prophylaxis of migraine and still requires more than 9 tablets per month. Prescription medications for weight loss require Prior Authorization, initiated through the Pharmacy Department. Prescriptions for compounded medications require Prior Authorization based on established criteria for safety and appropriateness. There is no coverage for replacement of lost, stolen or destroyed medication. Coverage for prescription drugs for primary oral drug therapy for Hepatitis C shall be subject to quantity limits and other restrictions that may include step therapy, prior authorization or duration limits. Authorization of primary oral Hepatitis C agents is limited to one treatment course per lifetime. There shall be no coverage for replacement of lost, stolen or destroyed medication. Coverage for prescription drugs with potential for abuse and/or dependency shall be subject to quantity limits and other restrictions that may include step therapy, prior authorization or duration limits. Prescription drugs with potential for abuse and/or dependency shall be limited to established quantities approved by HealthPlus Pharmacy and Therapeutics Committee and only for FDA approved indications. There shall be no coverage for replacement of lost, stolen or destroyed medication. 217 PRESCRIPTION BENEFIT LIMITATIONS APPENDIX E LIMITATIONS BY LINE OF BUSINESS HealthPlus of Michigan (Commercial, PPO, Medicare (non-Part D) Limitations: Prescription drugs for the treatment of impotency are covered for male members only and are limited to a quantity of 6 units/tablets total (for all ED products combined) every 30 days. These drugs are limited to males 35 years of age and older. If a member-specific review for a male member under 35 years of age meets medical necessity criteria, the Primary Care Physician or participating treating urologist may obtain prior authorization from HealthPlus for coverage of the product. (The same limitations for quantity apply.) For PPO members, any physician may prescribe ED medications. Selected antipsychotic medications are limited to maximum daily dosage recommendations from the manufacturer. Selected sleeping medications are limited to a quantity of 30 in 30 days. Covered medications are limited to a 30-day supply (for some benefits up to a 34-day supply) at participating “30-day supply” retail pharmacies and specialty pharmacies, and up to a 90-day supply through participating HealthPlus Ask for 90 Rx retail pharmacies and the designated mail service provider. Refills may be obtained when 80% of the day supply received has passed. Specifically for the Ask for 90 Rx programs (mail service and retail pharmacies), injectable medications are not covered with the exception of injectable diabetes medications, Epipen, glucagon, and Imitrex. Specialty medications are limited to a 30-day supply. Specifically for HealthPlus MIChild/MIChild CSHCS, covered medications are limited to a 34-day supply at participating “30-day supply” retail pharmacies, and up to a 102 day supply through participating HealthPlus Ask for 90 Rx retail pharmacies and the designated mail service provider. To receive a 3-month supply, HealthPlus requires that the member has already received a 30-day supply of the same drug and strength within the last year. HealthPlus Partners (Medicaid) State Limitations and Exclusions: Coverage is limited to the generic product when a generic product is available. Combination cough and cold products are not a covered benefit. Certain Over-the-Counter (OTC) products (as mandated by the State) are covered when written as a prescription and dispensed by the pharmacy, with coverage limited to the generic product when the product is generically available. Condoms (latex only) are a covered benefit, limited to members 10 years of age or older, and limited to a maximum of 12 condoms per prescription and 36 condoms per month. Prescription medications for weight loss require Prior Authorization, initiated through the Pharmacy Department All FDA-approved smoking cessation products (prescription and OTC) are covered. Medications used to treat infertility are not a covered benefit. Medications for erectile dysfunction are not a covered benefit. Behavioral health medications, HIV medications and specific medications in other categories are carved out to MDCH. Administrative Limitations: Covered medications are limited to a 31-day supply at participating retail pharmacies. Refills may be obtained when 85% of the day supply received has passed. There are no copays associated with covered medications. 218 PRESCRIPTION BENEFIT LIMITATIONS APPENDIX E LIMITATIONS BY LINE OF BUSINESS HealthPlus Signature PPO Limitations: Prescription drug coverage is limited to those products that are listed on the PPO Closed Formulary. Exclusions: Prescription drugs when there is a non-prescription drug available in the drug category. Non-sedating antihistamines (NSAs) and NSA antihistamine decongestants Ophthalmic antihistamines Erectile dysfunction medications Weight loss medications Drugs for the treatment of infertility. 219 A ABACAVIR ...................................................................................94 ABACAVIR SULFATE/LAMIVUDINE ..............................................93 ABACAVIR SULFATE/LAMIVUDINE/ZIDOVUDINE .......................94 ABATACEPT........................................................................... 89, 94 ABILIFY........................................................................................64 ABSTRAL .....................................................................................40 ACANYA ......................................................................................53 ACARBOSE ..................................................................................83 ACCOLATE............................................................................. 42, 46 ACCUNEB ....................................................................................44 ACCUPRIL....................................................................................27 ACCURETIC .................................................................................27 ACEBUTOLOL ........................................................................ 27, 30 ACEON ........................................................................................27 ACETAMINOPHEN/ CODEINE .....................................................42 ACETAMINOPHEN/ HYDROCODONE .................................... 41, 42 ACETAMINOPHEN/ OXYCODONE ......................................... 41, 42 ACETAMINOPHEN-ISOMETHEPTENE-CAFFEINE .........................68 ACETAZOLAMIDE ........................................................................57 ACETIC ACID ...............................................................................61 ACETIC ACID/ HYDROCORTISONE ...............................................61 ACETONIDE .................................................................................48 ACIPHEX......................................................................................21 ACITRETIN...................................................................................51 ACLIDINIUM BROMIDE ...............................................................46 ACLOVATE ..................................................................................47 ACTEMRA ...................................................................................94 ACTEMRA SQ ..............................................................................89 ACTIGALL ....................................................................................87 ACTIQ .........................................................................................40 ACTIVELLA 1.0-0.5 ......................................................................77 ACTONEL ....................................................................................79 ACTOPLUS MET ..........................................................................82 ACTOPLUS MET XR .....................................................................82 ACTOS .........................................................................................82 ACULAR LS ..................................................................................61 ACUVAIL .....................................................................................61 ACYCLOVIR .................................................................................38 ACZONE 5% GEL .........................................................................53 ADALAT CC .................................................................................29 ADALIMUMAB ............................................................................89 ADAPALENE ................................................................................53 ADAPALENE/BENZOYL PEROXIDE ...............................................53 ADASUVE ....................................................................................64 ADCIRCA .....................................................................................31 ADDERALL...................................................................................65 ADDERALL XR..............................................................................65 ADEMPAS ...................................................................................31 ADOXA, PAK................................................................................34 ADVAIR .......................................................................................44 ADVICOR.....................................................................................32 AEROSPAN ..................................................................................44 AGGRENOX .................................................................................56 AGRYLIN .....................................................................................56 ALAVERT OTC .............................................................................42 ALBENDAZOLE ............................................................................38 ALBENZA .....................................................................................38 ALBIGLUTIDE ..............................................................................83 ALBUTEROL........................................................................... 45, 46 ALBUTEROL SULFATE ..................................................................44 ALBUTEROL/ IPRATROPIUM .......................................................45 ALCAFTADINE .............................................................................60 ALCLOMETASONE .......................................................................47 ALDACTAZIDE 25/25 ...................................................................27 ALDACTAZIDE 50/50 ...................................................................27 ALDACTONE ................................................................................27 ALDARA ......................................................................................55 ALDOMET ...................................................................................31 ALDOMET 125 ............................................................................31 ALDORIL-D ..................................................................................31 ALENDRONATE ..................................................................... 79, 80 ALENDRONATE/ VITAMIN D3 .....................................................80 ALFUZOSIN .................................................................................91 ALINIA .........................................................................................38 ALISKIREN ...................................................................................32 ALISKIREN/ ..................................................................... 29, 30, 32 ALISKIREN/ HCTZ ........................................................................32 ALITRETINOIN .............................................................................55 ALL OTHER TEST STRIPS (covered at DME only with a copay as applicable) .............................................................................83 ALLEGRA OTC .............................................................................42 ALLEGRA-D .................................................................................44 ALLEGRA-D 12 HOUR ..................................................................43 ALLOPURINOL .............................................................................83 ALMOTRIPTAN............................................................................68 ALOCRIL ......................................................................................60 ALODOX ......................................................................................59 ALOGLIPTIN/ BENZOATE.............................................................82 ALOGLIPTIN/ METFORMIN .........................................................82 ALOGLIPTIN/ PIOGLITAZONE ......................................................82 ALOMIDE ....................................................................................60 ALORA ........................................................................................76 ALOSETRON .......................................................................... 23, 91 ALPHAGAN P ..............................................................................57 ALPRAZOLAM .............................................................................63 ALPROSTADIL..............................................................................88 ALREX .........................................................................................58 ALTABAX .....................................................................................51 ALTACE CAPS ..............................................................................27 ALTOPREV...................................................................................32 ALVESCO .....................................................................................45 AMANTADINE .............................................................................37 AMARYL ......................................................................................81 AMBIEN ......................................................................................63 AMERGE .....................................................................................67 AMICAR ......................................................................................56 AMICAR 1,000MG ......................................................................56 AMINOCAPROIC ACID .................................................................56 AMINOPHYLLINE ........................................................................46 AMIODARONE ...................................................................... 26, 27 AMITIZA ................................................................................ 23, 91 AMITRIPTYLINE ...........................................................................62 AMLACTIN 12%...........................................................................49 AMLODIPINE...............................................................................30 220 AMLODIPINE/ .............................................................................29 AMLODIPINE/ ATORVASTATIN ...................................................32 AMLODIPINE/ BENAZEPRIL ................................................... 28, 30 AMLODIPINE/ OLMESARTAN......................................................28 AMLODIPINE/ VALSARTAN .........................................................29 AMMONIUM LACTATE ......................................................... 49, 50 AMOXICILLIN ..............................................................................33 AMOXICILLIN TRIHYDRATE .........................................................33 AMOXICILLIN/ CLAVULANATE ....................................................33 AMOXIL ......................................................................................33 AMPHETAMINE/ DEXTROAMPHETAMINE ..................................65 AMPHETAMINE/ DEXTROAMPHET-AMINE XR ...........................65 AMPYRA .....................................................................................92 AMRIX.........................................................................................68 AMTURNIDE ...............................................................................29 AMYLASE/ LIPASE/ PROTEASE .............................................. 22, 23 ANAFRANIL .................................................................................62 ANAKINRA ..................................................................................89 ANAPROX, DS .............................................................................39 ANASPAZ ....................................................................................24 ANASTROZOLE ............................................................................95 ANCOBON...................................................................................36 ANDRODERM..............................................................................78 ANDROGEL .................................................................................78 ANDROID ....................................................................................78 ANEGRELIDE ...............................................................................56 ANGELIQ .....................................................................................77 ANORO ELLIPTA ..........................................................................45 ANSAID .......................................................................................39 ANTABUSE ..................................................................................87 ANTARA ......................................................................................32 ANTHRALIN.................................................................................50 ANTHRALIN SHAMPOO ..............................................................51 ANTIPYRINE-BENZOCAINE-POLYCOSANOL .................................61 ANTIVERT 12.5, 25MG ................................................................23 ANTIVERT 50MG.........................................................................23 ANUSOL HC.................................................................................23 ANZEMET....................................................................................23 APEXICON ...................................................................................47 APEXICON OINT ..........................................................................47 APIDRA .......................................................................................80 APIDRA SOLOSTAR .....................................................................80 APIXABAN ...................................................................................55 APLENZIN....................................................................................62 APOKYN ......................................................................................69 APOMORPHINE ..........................................................................69 APRACLONIDINE .........................................................................57 APREMILAST ...............................................................................89 APREPITANT ...............................................................................24 APRESOLINE ...............................................................................29 APRI ............................................................................................70 APRISO........................................................................................22 APTIOM 200MG .........................................................................66 APTIOM 400, 600, 800MG..........................................................66 APTIVUS......................................................................................93 ARALEN.......................................................................................38 ARANELLE ...................................................................................71 ARANESP ....................................................................................56 ARAVA ........................................................................................89 ARCAPTA ....................................................................................45 ARFORMOTEROL ........................................................................45 ARICEPT ......................................................................................70 ARIMIDEX ...................................................................................95 ARIPIPRAZOLE ............................................................................64 ARISTOCORT ...............................................................................70 ARMODAFINIL ............................................................................65 ARMOUR THYROID .....................................................................80 AROMASIN .................................................................................95 ARTEMETHER/ ............................................................................38 ARTHROTEC ................................................................................39 ASACOL .......................................................................................22 ASACOL HD .................................................................................22 ASENAPINE .................................................................................64 ASMANEX ...................................................................................45 ASPIRIN/ DIPYRIDAMOLE ...........................................................56 ASPIRIN/ OXYCODONE ...............................................................41 ASTELIN ......................................................................................43 ASTEPRO .....................................................................................43 ATABEX .......................................................................................84 ATACAND....................................................................................28 ATACAND HCT ............................................................................28 ATELVIA ......................................................................................79 ATENOLOL ..................................................................................31 ATENOLOL/ CHLORTHALIDONE ..................................................31 ATIVAN .......................................................................................63 ATOMOXETINE ...........................................................................66 ATOPICLAIR ................................................................................49 ATORVASTATIN ..........................................................................32 ATOVAQUONE ............................................................................38 ATOVAQUONE/ PROGUANIL ......................................................38 ATRALIN......................................................................................53 ATROPINE ...................................................................................57 ATROPINE SULFATE ....................................................................57 ATROVENT HFA ..........................................................................45 ATROVENT NASAL SPRAY ...........................................................43 AUBAGIO ....................................................................................92 AUGMENTIN CHEW TABS, 125-31.25 SUSP ................................33 AUGMENTIN XR ..........................................................................33 AUGMENTIN, ES .........................................................................33 AURALGAN .................................................................................61 AURANOFIN ................................................................................89 AUVI-Q........................................................................................87 AVALIDE......................................................................................28 AVANAFIL ...................................................................................88 AVANDAMET ..............................................................................82 AVANDARYL ................................................................................82 AVANDIA ....................................................................................82 AVAPRO ......................................................................................28 AVAR ..........................................................................................49 AVAR LS ......................................................................................49 AVAR-E .......................................................................................49 AVC CREAM ................................................................................54 AVELOX.......................................................................................35 AVIANE .......................................................................................71 AVIDOXY DK................................................................................34 AVINZA .......................................................................................40 AVODART....................................................................................90 AVONEX ......................................................................................92 AXERT .........................................................................................68 AXID ............................................................................................21 AXIRON .......................................................................................78 AYGESTIN....................................................................................77 221 AZASAN ......................................................................................88 AZASITE ......................................................................................59 AZATHIOPRINE ...........................................................................88 AZELAIC ACID ..............................................................................53 AZELASTINE .......................................................................... 43, 60 AZELASTINE/ ...............................................................................43 AZELEX ........................................................................................53 AZILECT .......................................................................................69 AZILSARTAN MEDOXOMIL ..........................................................28 AZILSARTAN MEDOXOMIL/ ........................................................29 AZITHROMYCIN .................................................................... 35, 59 AZOPT .........................................................................................57 AZOR...........................................................................................28 AZULFIDINE, ENTAB ....................................................................22 B BACLOFEN ..................................................................................68 BACTRIM DS, SEPTRA DS ...................................................... 35, 36 BACTRIM, SEPTRA ................................................................ 35, 36 BACTROBAN ...............................................................................51 BACTROBAN NASAL OINT ...........................................................51 BAL-CARE DHA ESSENTIAL ..........................................................84 BALSALAZIDE DISODIUM ............................................................22 BANZEL .......................................................................................66 BECLOMETHASONE DIPROPIONATE ..................................... 43, 46 BECLOMETHASONE, AQUEOUS ..................................................43 BECONASE AQ ............................................................................43 BEDAQUILINE FUMARATE ..........................................................37 BELLADONNA ALKALOIDS/ PHENOBARBITAL .............................24 BENADRYL ............................................................................ 42, 63 BENAZEPRIL ................................................................................28 BENAZEPRIL/ HCTZ .....................................................................28 BENICAR .....................................................................................28 BENICAR HCT ..............................................................................28 BENTYL .......................................................................................24 BENZACLIN 1%-5% Gel (pump) ...................................................53 BENZAMYCIN GEL .......................................................................53 BENZAMYCINPAK .......................................................................53 BENZEFOAM ...............................................................................53 BENZIQ WASH ............................................................................53 BENZOCAINE-ANTIPYRINE ..........................................................61 BENZONATATE ...........................................................................44 BENZOYL PEROXIDE .............................................................. 53, 54 BENZOYL PEROXIDE/ HC/SKIN CLNSR NO. 14 .............................54 BENZOYL PEROXIDE/ HYALURONT .............................................54 BENZOYL PEROXIDE/ SULFUR .....................................................53 BENZTROPINE .............................................................................69 BENZYL ALCOHOL .......................................................................55 BEPOTASTINE BESILATE ..............................................................60 BEPREVE .....................................................................................60 BESIFLOXACIN HYDROCHLORIDE ................................................59 BESIVANCE .................................................................................59 BETAGAN ....................................................................................57 BETAMET DIPROP/ .....................................................................51 BETAMETHASONE ................................................................ 48, 70 BETAMETHASONE DIPROPIONATE .............................................47 BETAPACE, AF .............................................................................26 BETASERON ................................................................................92 BETAXOLOL........................................................................... 30, 57 BETHANECHOL ...........................................................................90 BETHKIS ......................................................................................92 BETIMOL .....................................................................................57 BETOPIC 0.5% .............................................................................57 BETOPTIC S .................................................................................57 BEXAROTENE ..............................................................................55 BEYAZ .........................................................................................71 BIAXIN, XL ...................................................................................34 BIDIL ...........................................................................................26 BILTRICIDE ..................................................................................38 BIMATOPROST............................................................................57 BINOSTO .....................................................................................79 BISOPROLOL ...............................................................................31 BISOPROLOL/ HCTZ ....................................................................31 BLEPH-10 ....................................................................................59 BLEPHAMIDE ..............................................................................60 BLEPHAMIDE S.O.P. ....................................................................60 BLOCADREN................................................................................30 B-NEXA .......................................................................................84 BOCEPREVIR ...............................................................................91 BONIVA.......................................................................................79 BOSENTAN..................................................................................31 BOTOX, DYSPORT, XEOMIN ........................................................94 BOTULISM TOXIN TYPE A ...........................................................94 BRAVELLE ...................................................................................78 BREO ELLIPTA .............................................................................45 BREVOXYL ...................................................................................53 BRILINTA .....................................................................................55 BRIMONIDINE .............................................................................55 BRIMONIDINE TARTRATE ...........................................................57 BRINTELLIX .................................................................................62 BRINZOLAMIDE ..........................................................................57 BRINZOLAMIDE/ BIMONIDINE TARTRATE ..................................58 BRISDELLE ...................................................................................91 BROMDAY...................................................................................61 BROMFED-DM ............................................................................44 BROMFENAC SODIUM ................................................................61 BROMOCRIPTINE ........................................................................69 BROMPHENIRAMINE/ PSEUDOEPHEDRINE/ DEXTROMETHORPHAN .........................................................44 BROVANA ...................................................................................45 BUDESONIDE ............................................................ 22, 43, 45, 46 BUDESONIDE/ FORMOTEROL .....................................................46 BUNAVAIL ...................................................................................87 BUPAP ........................................................................................40 BUPRENORPHINE .......................................................................88 BUPRENORPHINE PATCH............................................................40 BUPRENORPHINE/ NALOXONE ............................................. 87, 88 BUPROPION .................................................................... 62, 63, 96 BUSPAR ......................................................................................63 BUSPIRONE .................................................................................63 BUTALBITAL/ ACETAMINOPHEN .......................................... 40, 41 BUTALBITAL/ ACETAMINOPHEN/ CAFFEINE ...............................40 BUTALBITAL/ ASA/ CAFFEINE .....................................................68 BUTALBITAL/ ASPIRIN/ CAFFEINE/ CODEINE ..............................40 BUTENAFINE ...............................................................................52 BUTORPHANOL ..........................................................................41 BUTRANS ....................................................................................40 BYDUREON .................................................................................83 BYETTA .......................................................................................83 BYSTOLIC ....................................................................................30 222 C CABOZANTINIB ...........................................................................93 CADUET ......................................................................................32 CAFERGOT ..................................................................................68 CALAN.........................................................................................26 CALAN SR ....................................................................................29 CALCIPOTRIENE .................................................................... 50, 51 CALCITONIN.......................................................................... 79, 80 CALCITRIOL ........................................................................... 55, 86 CALCIUM ACETATE .....................................................................93 CAMBIA ......................................................................................68 CAMILA .......................................................................................71 CANAGLIFLOZIN..........................................................................81 CANASA ......................................................................................22 CANDESARTAN ...........................................................................28 CANTIL ........................................................................................24 CAPOTEN ....................................................................................27 CAPTOPRIL..................................................................................27 CARAFATE ...................................................................................21 CARAFATE SUSP..........................................................................21 CARBACHOL................................................................................57 CARBAMAZEPINE.................................................................. 66, 67 CARBATROL ................................................................................66 CARBIDOPA ................................................................................69 CARBIDOPA/ LEVODOPA ............................................................69 CARBIDOPA/ LEVODOPA/ ENTACAPONE....................................70 CARDENE ....................................................................................29 CARDENE SR ...............................................................................29 CARDIZEM ..................................................................................29 CARDIZEM CD 120, 180, 240, 300 ..............................................29 CARDIZEM LA .............................................................................29 CARDURA ............................................................................. 31, 90 CARDURA XL ......................................................................... 31, 90 CARISOPRODOL ..........................................................................69 CARMOL .....................................................................................49 CARNITOR ...................................................................................87 CARTIA XT ...................................................................................30 CARVEDILOL ...............................................................................30 CATAFLAM ..................................................................................39 CATAPRES-TTS ............................................................................31 CAVERJECT..................................................................................88 CECLOR .......................................................................................33 CEDAX .........................................................................................33 CEFACLOR ...................................................................................33 CEFDITOREN ...............................................................................34 CEFIXIME ....................................................................................34 CEFTIBUTEN................................................................................33 CEFTIN ........................................................................................33 CEFUROXIME ..............................................................................33 CELEBREX....................................................................................39 CELECOXIB ..................................................................................39 CELESTONE .................................................................................70 CELEXA .......................................................................................62 CELLCEPT ....................................................................................88 CELONTIN ...................................................................................66 CENESTIN....................................................................................76 CEPHALEXIN ...............................................................................34 CERTOLIZUMAB PEGOL ..............................................................89 CETIRIZINE ..................................................................................43 CETRAXAL ...................................................................................61 CETRORELIX ACETATE .................................................................78 CETROTIDE .................................................................................78 CHANTIX .....................................................................................95 CHLORAL HYDRATE.....................................................................64 CHLOROQUINE ...........................................................................38 CHLOROXYLENOL/ ......................................................................61 CHLORPROPAMIDE.....................................................................81 CHLORTHALIDONE......................................................................27 CHLORZOXAZONE .......................................................................69 CHOLESTYRAMINE POWDER ......................................................33 CHOLESTYRAMINE/ ....................................................................33 CIALIS..........................................................................................88 CIALIS 2.5, 5MG ..........................................................................88 CICLESONIDE ........................................................................ 43, 45 CICLODAN KIT .............................................................................51 CICLOPIROX ................................................................................52 CICLOPIROX OLAMINE ................................................................52 CICLOPIROX OLAMINE CREAM/ CLEANSER ................................51 CICLOPIROX SOLN 8%/ LACQUER REMOVAL PADS.....................51 CILOSTAZOLE ..............................................................................56 CILOXAN GEL ..............................................................................59 CILOXAN SOLN............................................................................59 CIMETIDINE ................................................................................21 CIMZIA ........................................................................................89 CIPRO.................................................................................... 35, 36 CIPRO HC ....................................................................................61 CIPRO SUSP .......................................................................... 35, 36 CIPRODEX ...................................................................................61 CIPROFLOXACIN ....................................................... 35, 36, 59, 61 CIPROFLOXACIN HCL/ HC ...........................................................61 CIPROFLOXACIN/ DEXAMETH .....................................................61 CITALPRAM.................................................................................62 CITRACAL PRENATAL + DHA .......................................................84 CITRANATAL B-CALM..................................................................84 CITRANATAL HARMONY .............................................................84 CLARINEX TABS ...........................................................................42 CLARINEX-D ................................................................................44 CLARITHROMYCIN ......................................................................34 CLARITIN OTC .............................................................................42 CLARITIN-D OTC..........................................................................44 CLEMASTINE ...............................................................................43 CLEOCIN 150, 300MG .................................................................35 CLEOCIN VAGINAL CREAM .........................................................54 CLEOCIN VAGINAL OVULE ..........................................................54 CLEOCIN-T ..................................................................................53 CLIDINIUM BROMIDE/ CHLORDIAZEPOXIDE ..............................25 CLIMARA.....................................................................................76 CLIMARA PRO .............................................................................77 CLINDACIN PAC ..........................................................................53 CLINDAGEL .................................................................................53 CLINDAMYCIN ................................................................ 35, 53, 54 CLINDAMYCIN PHOSPHATE-BENZOYL PEROXIDE .......................53 CLINDAMYCIN/ ..................................................................... 53, 54 CLINDAMYCIN/BENZOYL PEROXIDE ...........................................53 CLINORIL .....................................................................................39 CLOBAZAM .................................................................................67 CLOBETASOL EMOLL...................................................................48 CLOBETASOL PROPIONATE ................................................... 47, 48 CLOBETASOL PROPRIONATE.......................................................47 CLOBEX .......................................................................................47 CLOCORTOLONE PIVALATE .........................................................47 223 CLODERM ...................................................................................47 CLOMID ......................................................................................78 CLOMIPHENE ..............................................................................78 CLOMIPRAMINE .........................................................................62 CLONAZEPAM .............................................................................67 CLONIDINE...................................................................... 31, 32, 65 CLOPIDOGREL .............................................................................56 CLORAZEPATE .............................................................................63 CLOTRIMAZOLE 1%.....................................................................52 CLOTRIMAZOLE TROCHES ..........................................................37 CLOTRIMAZOLE/ BETAMETHASONE ...........................................52 CLOZAPINE ........................................................................... 64, 65 CLOZARIL ....................................................................................64 CNL 8 NAIL KIT ............................................................................51 COARTEM ...................................................................................38 CODEINE .....................................................................................40 COGENTIN ..................................................................................69 COLAZAL .....................................................................................22 COLCHICINE 0.6MG ....................................................................83 COLCRYS .....................................................................................83 COLESEVELAM ............................................................................33 COLESTID ....................................................................................32 COLESTID 7.5 ..............................................................................32 COLESTIPOL ................................................................................32 COLY-MYCIN S ............................................................................61 COLYTE .......................................................................................25 COMBIPATCH .............................................................................77 COMBIVENT................................................................................45 COMBIVENT RESPIMAT ..............................................................45 COMETRIQ..................................................................................93 COMFORT PAC-TIZANIDINE ........................................................69 COMPAZINE SYRUP ....................................................................23 COMPAZINE TABS , SUPP ...........................................................23 COMPLERA .................................................................................93 COMPLETE-RF PRENATAL ...........................................................84 COMTAN.....................................................................................69 CONCEPT OB, DHA .....................................................................84 CONCERTA ..................................................................................65 CONDYLOX GEL...........................................................................55 CONDYLOX SOLUTION ................................................................55 CONJUGATED ESTROGEN/ MPA .................................................78 CONJUGATED ESTROGENS ................................................... 76, 77 CONJUGATED ESTROGENS- BAZEDOXIFENE...............................79 CONZIP .......................................................................................40 COPAXONE .................................................................................92 COPEGUS ....................................................................................91 CORDARONE...............................................................................26 CORDRAN 4MCG/SQ CM TAPE ...................................................47 CORDRAN, SP .............................................................................47 COREG ........................................................................................30 COREG CR ...................................................................................30 CORGARD ...................................................................................30 CORMAX .....................................................................................47 CORTEF TABS ..............................................................................70 CORTIFOAM................................................................................22 CORTISONE .................................................................................70 CORTISONE ACETATE .................................................................70 CORTISPORIN ................................................................. 51, 60, 61 CORTISPORIN-TC ........................................................................61 CORZIDE .....................................................................................30 COSOPT ......................................................................................57 COSOPT PF..................................................................................57 COUMADIN.................................................................................55 COVERA HS .................................................................................30 COZAAR ......................................................................................28 CREON ........................................................................................22 CRESTOR .....................................................................................32 CROFELEMER ..............................................................................23 CROMOLYN SODIUM ............................................................ 23, 45 CROMOLYN SOLN .......................................................................45 CROTAMITON .............................................................................55 CRYSELLE ....................................................................................71 CUPRIMINE .................................................................................87 CUTIVATE ...................................................................................47 CUTIVATE 0.05% LOTION............................................................47 CYANOCOBALAMIN/MECOBALAMIN .........................................86 CYCLOBENZAPRINE............................................................... 68, 69 CYCLOGYL 0.5%, .........................................................................57 CYCLOGYL 1% .............................................................................57 CYCLOPENTOLATE ......................................................................57 CYCLOSERINE ..............................................................................37 CYCLOSPORINE ............................................................... 60, 88, 89 CYMBALTA ............................................................................ 62, 92 CYSTOSPAZ, M ............................................................................24 CYTOMEL ....................................................................................80 CYTOTEC .....................................................................................21 D DABIGATRAN ETEXILATE MESYLATE ...........................................56 DALFAMPRIDINE ........................................................................92 DALIRESP ....................................................................................46 DALTEPARIN SODIUM,PORCINE .................................................55 DANTRIUM .................................................................................69 DANTROLENE .............................................................................69 DAPAGLIFLOZIN ..........................................................................81 DAPSONE ....................................................................................53 DARAPRIM ..................................................................................38 DARBEPOETIN ALFA IN POLYSORBATE .......................................56 DARIFENACIN HYDROBROMIDE .................................................91 DARUNAVIR ................................................................................94 DAYPRO ......................................................................................39 DAYTRANA..................................................................................65 DDAVP NASAL SPRAY .................................................................78 DDAVP RHINAL TUBE..................................................................78 DECADRON .................................................................................58 DECONAMINE SYRUP .................................................................44 DECONAMINE TABS ....................................................................44 DEFERASIROX .............................................................................87 DEFEROXAMINE MESYLATE ........................................................87 DELZICOL ....................................................................................22 DEMADEX ...................................................................................27 DEMEROL ...................................................................................40 DEPAKENE ..................................................................................66 DEPAKOTE ..................................................................................66 DERMA-SMOOTHE-FS 0.01% OIL................................................47 DESFERAL ...................................................................................87 DESIPRAMINE .............................................................................62 DESLORATIDINE ..........................................................................42 DESMOPRESSIN ACETATE ...........................................................78 DESOGEN ....................................................................................71 DESONATE GEL ...........................................................................47 224 DESONIDE ............................................................................. 47, 49 DESONIDE/EMOLLIENT COMBO .................................................47 DESOWEN...................................................................................47 DESOWEN COMBO .....................................................................47 DESOXIMETASONE .....................................................................48 DESOXYN ....................................................................................65 DESQUAM X ...............................................................................53 DESVENLAFAXINE SUCCINATE ....................................................62 DETROL .......................................................................................90 DETROL LA ..................................................................................90 DEXAMETHASONE ......................................................................58 DEXAMETHASONE/ NEOMYCIN/ POLYMYXIN ............................60 DEXAMETHASONE/ TOBRAMYCIN .............................................60 DEXILANT....................................................................................21 DEXLANSOPRAZOLE....................................................................21 DEXMETHYLPHENIDATE .............................................................65 DEXMETHYLPHENI-DATE ............................................................65 DEXTROAMPHET-AMINE ............................................................66 DIABETA .....................................................................................81 DIABINESE ..................................................................................81 DIAMOX SEQUELS ......................................................................57 DIASTAT ......................................................................................66 DIAZEPAM ............................................................................ 63, 66 DIBENZYLINE ..............................................................................31 DICLEGIS .....................................................................................24 DICLOFENAC ...............................................................................39 DICLOFENAC EPOLAMINE ...........................................................39 DICLOFENAC POTASSIUM ...........................................................68 DICLOFENAC SODIUM ................................................................55 DICLOFENAC, EXTENDED RELEASE .............................................39 DICLOFENAC/ MISOPROSTOL .....................................................39 DICLOFENAX POTASSIUM ...........................................................39 DICYCLOMINE .............................................................................24 DIDRONEL ...................................................................................79 DIFENOXIN/ ATROPINE...............................................................24 DIFFERIN 0.1% CREAM, GEL .......................................................53 DIFFERIN 0.1% LOTION ...............................................................53 DIFFERIN 0.3% GEL .....................................................................53 DIFICID ........................................................................................34 DIFLORASONE DIACETATE ..........................................................47 DIFLUCAN ............................................................................. 36, 54 DIFLUNISAL .................................................................................38 DIGOXIN ............................................................................... 26, 27 DIHYDROERGOTAMINE ..............................................................68 DILACOR XR ................................................................................30 DILANTIN 100MG CAPS ..............................................................66 DILANTIN 30 KEPSEAL.................................................................66 DILANTIN 50 INFATAB ................................................................66 DILATRATE-SR.............................................................................26 DILAUDID ....................................................................................40 DILAUDID 5 LIQUID.....................................................................40 DILTIAZEM ............................................................................ 29, 30 DIMETHYL FUMERATE ................................................................92 DIOVAN ......................................................................................28 DIOVAN HCT ...............................................................................28 DIPENTUM..................................................................................22 DIPHENHYDRAMINE ............................................................. 42, 63 DIPHENOXYLATE/ ATROPINE ......................................................24 DIPIVEFRIN .................................................................................58 DIPROSONE ................................................................................47 DIPYRIDAMOLE...........................................................................56 DISOPYRAMIDE ..........................................................................26 DISULFIRAM ...............................................................................87 DITROPAN XL ..............................................................................90 DIVALPROEX SODIUM ................................................................66 DIVIGEL .......................................................................................76 DL-E AC/ GRAPE/ HYALURONIC ACID .........................................49 DOCYCYCLINE .............................................................................34 DOFETILIDE .................................................................................27 DOLASETRON MESYLATE ............................................................23 DOLOBID.....................................................................................38 DOLOPHINE ................................................................................40 DOMEBORO................................................................................61 DONEPEZIL .................................................................................70 DONNATAL .................................................................................24 DONNATAL ER ............................................................................24 DORNASE ALFA ..................................................................... 46, 47 DORYX ........................................................................................34 DORYX 200MG............................................................................34 DORZOLAMIDE ...........................................................................58 DORZOLAMIDE/TIMOLOL ...........................................................57 DOVONEX CRM ..........................................................................50 DOVONEX SOLN .........................................................................51 DOXAZOSIN .......................................................................... 31, 90 DOXEPIN ............................................................................... 62, 63 DOXYCYCLINE ....................................................................... 34, 36 DOXYCYCLINE/ EYELID CLNS NO.2&3 .........................................59 DOXYCYCLINE/SALICY/OCT/ZINC OX ..........................................34 DOXYLAMINE/ PYRIDOXINE........................................................24 DRISDOL CAPSULE ......................................................................95 DRONEDARONE HYDROCHLORIDE .............................................26 DROSPIR/ETH ESTRA/LEVOMEF OL CA .......................................71 DROSPIR/ETHESTRA/LEVOMEFOL CA .........................................75 DROXIA .......................................................................................93 DUAC ..........................................................................................53 DUAVEE ......................................................................................79 DUET DHA BALANCED ................................................................84 DUETACT ....................................................................................82 DUEXIS ........................................................................................39 DULERA ......................................................................................45 DULOXETINE ......................................................................... 62, 92 DUONEB .....................................................................................45 DURAGESIC PATCH .....................................................................40 DUTASTERIDE .............................................................................90 DUTASTERIDE/...................................................................... 31, 90 DUTOPROL .................................................................................30 DYAZIDE......................................................................................27 DYMISTA .....................................................................................43 DYNACIRC CR ..............................................................................30 DYRENIUM..................................................................................27 E E.E.S. ...........................................................................................34 E.E.S. GRANULES ........................................................................34 ECHOTHIOPHATE ........................................................................58 ECONAZOLE NITRATE .................................................................51 ECOZA.........................................................................................51 EDARBI .......................................................................................28 EDARBYCLOR ..............................................................................29 EDEX ...........................................................................................88 EDLUAR ......................................................................................63 225 EDURANT ....................................................................................93 EFFEXOR XR ................................................................................62 EFFIENT ......................................................................................56 EFINACONAZOLE ........................................................................52 EGRIFTA ......................................................................................93 ELESTAT ......................................................................................60 ELETRIPTAN ................................................................................68 ELIDEL .........................................................................................50 ELIQUIS .......................................................................................55 ELIXOPHYLLIN ELIXIR ..................................................................46 ELMIRON ....................................................................................90 ELOCON ......................................................................................47 EMADINE ....................................................................................60 EMEDASTINE DIFUMARATE ........................................................60 EMEND .......................................................................................24 EMOLLIENT COMBO ............................................................. 49, 50 EMSAM PATCH ...........................................................................62 EMTRICITABINE/RILPIVIRINE/TENOFOVIR..................................93 EMTRICITABINE/TENOFOVIR DISOPROXIL FUMARATE ..............94 E-MYCIN .....................................................................................34 ENABLEX .....................................................................................90 ENALAPRIL ............................................................................ 27, 28 ENALAPRIL/ HCTZ .......................................................................28 ENBREL .......................................................................................89 ENFUVIRTIDE ..............................................................................94 ENJUVIA......................................................................................76 ENOXAPARIN ..............................................................................55 ENPRESSE ...................................................................................71 ENTACAPONE .............................................................................69 ENTEX ER ....................................................................................44 ENTEX LIQUID .............................................................................44 ENTOCORT EC .............................................................................22 ENTYVIO .....................................................................................94 ENZALUTAMIDE ..........................................................................93 EPANED SOLUTION.....................................................................27 EPICERAM...................................................................................49 EPIDUO .......................................................................................53 EPINASTINE ................................................................................60 EPINEPHRINE ..............................................................................87 EPIPEN ........................................................................................87 EPLERENONE ........................................................................ 27, 31 EPOETIN ALFA.............................................................................56 EPOGEN ......................................................................................56 EPROSARTAN ..............................................................................29 EPROSARTAN/ HCTZ ...................................................................29 EPZICOM.....................................................................................93 ERGOCALCIFEROL .......................................................................95 ERGOTAMINE TARTRATE/CAFFEINE ...........................................68 ERGOTAMINE/ CAFFEINE ...........................................................68 ERRIN..........................................................................................71 ERTACZO.....................................................................................51 ERYPRED .....................................................................................35 ERY-TAB ................................................................................ 35, 38 ERYTHROCIN ...............................................................................35 ERYTHROMYCIN .........................................................................59 ERYTHROMYCIN BASE .................................................... 34, 35, 38 ERYTHROMYCIN BASE/ BENZOYL PEROXIDE ..............................53 ERYTHROMYCIN ETHYLSUCCINATE ...................................... 34, 35 ERYTHROMYCIN STEARATE ........................................................35 ERYTHROMYCIN/ BENZOYL PEROXIDE .......................................53 ESCITALOPRAM ..........................................................................62 ESKALITH, CR ..............................................................................64 ESLICARBAZEPINE .......................................................................66 ESOMEPRAZOLE .........................................................................21 ESOMEPRAZOLE STRONTIUM ....................................................21 ESOMEPRAZOLE/ ........................................................................39 ESTRACE .....................................................................................76 ESTRACE VAGINAL CREAM .........................................................76 ESTRADIOL............................................................................ 76, 77 ESTRADIOL VALERATE/DIENOGEST ............................................73 ESTRADIOL, TRANSDERMAL ................................................. 76, 77 ESTRADIOL/ DROSPIRENONE .....................................................77 ESTRADIOL/ LEVONORGESTREL..................................................77 ESTRADIOL/ NORETHINDRONE ACETATE ...................................77 ESTRADIOL/ NORGESTIMATE .....................................................78 ESTRASORB.................................................................................76 ESTRATEST ..................................................................................77 ESTRING......................................................................................76 ESTROGEL GEL ............................................................................76 ESTROGENS ................................................................................76 ESTROPIPATE ..............................................................................76 ESTROSTEP FE .............................................................................71 ESZOPICLONE .............................................................................63 ETANERCEPT ...............................................................................89 ETHAMBUTOL.............................................................................37 ETHINYL ESTRADIOL ..................................... 71, 72, 73, 74, 75, 76 ETHINYL ESTRADIOL 20MCG .......................................... 71, 72, 76 ETHINYL ESTRADIOL 20MCG/ FE/ ...............................................73 ETHINYL ESTRADIOL 30MCG ........................ 70, 71, 72, 73, 74, 75 ETHINYL ESTRADIOL 35MCG ......................................................75 ETHINYL ESTRADIOL 35MG............................................. 73, 74, 76 ETHINYL ESTRADIOL 50MCG .......................................... 74, 75, 76 ETHINYL ESTRADIOL/ NORETHINDRONE ACETATE .....................77 ETHINYL ESTRADION 20MCG......................................................71 ETHIONAMIDE ............................................................................37 ETHOSUXIMIDE ..........................................................................67 ETHOTOIN ..................................................................................67 ETIDRONATE ...............................................................................79 ETONOGESTREL ..........................................................................76 EURAX ........................................................................................55 EVEROLIMUS ..............................................................................89 EVISTA .................................................................................. 79, 95 EXALGO ......................................................................................40 EXELDERM ..................................................................................52 EXELON .......................................................................................70 EXELON SOLN AND PATCH .........................................................70 EXEMESTANTE ............................................................................95 EXENATIDE .................................................................................83 EXENATIDE EXTENDED RELEASE .................................................83 EXFORGE ....................................................................................29 EXFORGE HCT .............................................................................29 EXJADE........................................................................................87 EXTAVIA ......................................................................................92 EXTINA ........................................................................................52 EZETIMIBE ..................................................................................33 EZETIMIBE/ ATORVASTATIN .......................................................32 EZETIMIBE/ SIMVASTATIN ..........................................................33 EZOGABINE .................................................................................67 F FABIOR FOAM ............................................................................51 226 FACTIVE ......................................................................................35 FAMCICLOVIR .............................................................................37 FAMOTIDINE...............................................................................21 FAMVIR.......................................................................................37 FANAPT.......................................................................................64 FANATREX ..................................................................................66 FARESTON ..................................................................................95 FARXIGA .....................................................................................81 FAZACLO .....................................................................................64 FEBUXOSTAT ..............................................................................83 FELBAMATE ................................................................................66 FELBATOL ...................................................................................66 FELDENE .....................................................................................39 FEMARA......................................................................................95 FEMCON FE ................................................................................71 FEMHRT ......................................................................................77 FEMHRT 0.5MG-2.5MCG ............................................................77 FEMRING ....................................................................................76 FENOFIBRATE ....................................................................... 32, 33 FENOFIBRIC ACID .................................................................. 32, 33 FENOGLIDE .................................................................................32 FENTANYL ............................................................................. 40, 41 FENTANYL CITRATE.....................................................................40 FENTANYL SL ..............................................................................40 FENTANYL SL SPRAY ...................................................................41 FENTORA ....................................................................................40 FESOTERODINE FUMARATE........................................................90 FETZIMA .....................................................................................62 FEXMID .......................................................................................69 FEXOFENADINE...........................................................................42 FEXOFENADINE/ .........................................................................43 FEXOFENADINE/ PSEUDOEPHEDRINE ........................................44 FIBRICOR ....................................................................................32 FIDAXOMICIN .............................................................................34 FILGRASTIM ................................................................................56 FINACEA .....................................................................................53 FINASTERIDE...............................................................................90 FINGOLIMOD ..............................................................................92 FIORICET .....................................................................................40 FIORICET 50-300-40....................................................................40 FIORINAL ....................................................................................68 FIORINAL W/CODEINE #3 ...........................................................40 FIRST-LANSOPRAZOLE ................................................................21 FIRST-OMEPRAZOLE ...................................................................21 FLAGYL............................................................................ 35, 38, 54 FLAGYL ER....................................................................... 35, 38, 54 FLAREX........................................................................................58 FLECAINIDE .................................................................................27 FLECTOR .....................................................................................39 FLEXERIL .....................................................................................69 FLOMAX ................................................................................ 31, 90 FLONASE .....................................................................................43 FLOVENT HFA .............................................................................45 FLUCONAZOLE ...................................................................... 36, 54 FLUCYTOSINE..............................................................................36 FLUMADINE TABS .......................................................................37 FLUNISOLIDE ..............................................................................44 FLUOCINOLONE ACETONIDE ......................................................47 FLUOCINOLONE SOLN/ CLEANSER .............................................48 FLUOCINONIDE ...........................................................................49 FLUORABON DROPS ...................................................................86 FLUOROMETHOLONE .................................................................58 FLUOXETINE ...............................................................................62 FLURANDRENOLIDE ....................................................................47 FLURBIPROFEN ...........................................................................39 FLUTICASONE ....................................................................... 43, 45 FLUTICASONE FUROATE .............................................................43 FLUTICASONE PROPIONATE .......................................................47 FLUTICASONE/ SALMETEROL .....................................................44 FLUTICASONE/ VILANTEROL .......................................................45 FLUVASTATIN .............................................................................32 FLUVOXAMINE MALEATE ...........................................................62 FML.............................................................................................58 FML FORTE .................................................................................58 FML S.O.P. ..................................................................................58 FOCALIN .....................................................................................65 FOCALIN XR ................................................................................65 FOLIC ACID............................................................................ 84, 95 FOLLISTIM AQ .............................................................................79 FOLLITROPIN ALPHA,RECOMB ...................................................79 FOLLITROPIN BETA,RECOMB ......................................................79 FORADIL .....................................................................................45 FORFIVO XL.................................................................................62 FORMOTEROL FUMARATE .........................................................45 FORTAMET .................................................................................81 FORTEO ......................................................................................79 FORTESTA ...................................................................................78 FORTICAL ....................................................................................79 FOSAMAX ...................................................................................80 FOSAMAX PLUS D .......................................................................80 FOSFOMYCIN TROMETHAMINE .................................................36 FOSINOPRIL ................................................................................28 FOSINOPRIL/ HCTZ .....................................................................28 FOSRENOL ..................................................................................92 FRAGMIN ....................................................................................55 FROVA ........................................................................................68 FROVATRIPTAN ..........................................................................68 FULVICIN U/F ..............................................................................36 FULYZAQ .....................................................................................23 FURAZOLIDONE ..........................................................................35 FUROSEMIDE ..............................................................................27 FUROXONE .................................................................................35 FUZEON ......................................................................................94 FYCOMPA ...................................................................................66 G GABAPENTIN .................................................................. 66, 67, 92 GABAPENTIN ENACARBIL ...........................................................92 GABITRIL .....................................................................................66 GABITRIL12,16MG ......................................................................67 GALANTAMINE ...........................................................................70 GARAMYCIN ......................................................................... 51, 59 GASTROCROM ............................................................................23 GELNIQUE ...................................................................................90 GEMFIBROZIL .............................................................................32 GEMIFLOXACIN MESYLATE .........................................................35 GENERESS FE ..............................................................................71 GENGRAF ....................................................................................88 GENOTROPIN..............................................................................93 GENTAMICIN ........................................................................ 51, 59 GEODON .....................................................................................64 227 GESTICARE, DHA .........................................................................84 GIAZO .........................................................................................22 GILENYA......................................................................................92 GLATIRAMER ACETATE ...............................................................92 GLIMEPIRIDE ..............................................................................81 GLIPIZIDE ....................................................................................81 GLUCAGON .................................................................................83 GLUCOPHAGE XR ........................................................................81 GLUCOSE TEST STRIPS ................................................................83 GLUCOTROL XL ...........................................................................81 GLUCOVANCE .............................................................................81 GLUMETZA .................................................................................81 GLYBURIDE .................................................................................81 GLYBURIDE/ METFORMIN ..........................................................81 GLYCATE .....................................................................................24 GLYCOPYRROLATE ......................................................................24 GLYNASE PRESTAB......................................................................81 GLYSET ........................................................................................83 GOLIMUMAB ..............................................................................89 GOLYTELY ...................................................................................25 GONADOTROPIN, CHORIONIC,HUMAN......................................79 GONAL-F .....................................................................................79 GORDO-UREA .............................................................................49 GRALISE ......................................................................................92 GRANISETRON ............................................................................24 GRANULEX ..................................................................................55 GRASTEK .....................................................................................86 GRIFULVIN-V...............................................................................37 GRISEOFULVIN............................................................................37 GRISEOFULVIN, ULTRAMICROSIZE ....................................... 36, 37 GRIS-PEG ....................................................................................37 GUAIFENESIN/ PHENYLEPHRINE.................................................44 GUANFACINE ........................................................................ 32, 65 H HALCINONIDE .............................................................................48 HALDOL ......................................................................................64 HALOBETASOL PROP/ AMMONIUM LAC ....................................49 HALOG ........................................................................................48 HALOPERIDOL.............................................................................64 HARVONI ....................................................................................91 HCG ALPHA,RECOMBINANT .......................................................79 HEMENATAL OB MIS + DHA .......................................................84 HEMOCYTE-F TABLET .................................................................84 HETLIOZ ......................................................................................63 HIPREX ........................................................................................35 HOMATROPINE ..........................................................................57 HORIZANT...................................................................................92 HUMALOG ..................................................................................80 HUMALOG MIX ...........................................................................80 HUMATROPE ..............................................................................93 HUMIRA......................................................................................89 HUMULIN INSULINS....................................................................80 HYDRALAZINE .............................................................................29 HYDRO 40 ...................................................................................49 HYDROCODONE..........................................................................42 HYDROCODONE BIT/ ACETAMINOPHEN ....................................42 HYDROCODONE/ CHLORPHEN POLIS .........................................43 HYDROCODONE/ CHLORPHENIRAMINE .....................................43 HYDROCODONE/ IBUUPROFEN ..................................................40 HYDROCORTISONE .....................................................................70 HYDROCORTISONE ACETATE ......................................................22 HYDROCORTISONE BUTYRATE 0.1% ...........................................48 HYDROCORTISONE BUTYRATE/ EMOLL ......................................48 HYDROCORTISONE PROBUTATE .................................................48 HYDROCORTISONE SUPP ............................................................23 HYDROCORTISONE VALERATE ....................................................49 HYDROCORTISONE/ EMOLLIENT ................................................48 HYDROCORTISONE/ NEOMYCIN/ POLYMYXIN ...........................61 HYDROCORTISONE/ NEOMYCIN/ POLYMYXIN/ BACITRACIN .....60 HYDROCORTISONE/ NEOMYCIN/POLYMYXIN/ BACITRACIN ......51 HYDROCORTISONE/ PRAMOXINE ...............................................23 HYDROCORTISONE/ALOE VERA ..................................................48 HYDROCORTISONE/BENZOYL PEROXIDE ....................................49 HYDROCORTISONE/UREA ...........................................................48 HYDROMORPHONE ....................................................................40 HYDROXYCHOLORO- ..................................................................38 HYDROXYUREA ...........................................................................93 HYDROXYZINE PAMOATE ...........................................................63 HYLATOPIC .................................................................................49 HYLATOPIC PLUS ........................................................................49 HYOSCYAMINE ..................................................................... 24, 25 HYZAAR ......................................................................................29 I IBANDRONATE............................................................................79 IBUDONE 10/200 ........................................................................40 IBUPROFEN.................................................................................39 IBUPROFEN/ FAMOTIDINE .........................................................39 IBUPROFEN/ HYDROCODONE .............................................. 41, 42 ICOSAPENT ETHYL ......................................................................33 ILEVRO ........................................................................................61 ILOPERIDONE..............................................................................64 ILOTYCIN.....................................................................................59 IMDUR ........................................................................................26 IMIPRAMINE PAMOATE .............................................................63 IMIQUIMOD ...............................................................................55 IMITREX KIT ................................................................................68 IMITREX SPRAY ...........................................................................68 IMITREX TABLET .........................................................................68 IMMUNE GLOBULIN ...................................................................94 IMODIUM ...................................................................................24 IMURAN......................................................................................88 INDACATEROL.............................................................................45 INDAPAMIDE ..............................................................................27 INDERAL .....................................................................................68 INDERAL LA.................................................................................68 INDERAL, LA................................................................................30 INDOCIN .....................................................................................39 INDOCIN SUSP ............................................................................83 INDOMETHACIN ........................................................... 39, 83, See INFLIXIMAB.................................................................................94 INH .............................................................................................37 INSPRA.................................................................................. 27, 31 INSULIN ................................................................................ 80, 81 INSULIN ASPART .........................................................................81 INSULIN DETEMIR .......................................................................81 INSULIN DETIMIR ........................................................................81 INSULIN GLARGINE ............................................................... 80, 81 INSULIN GLULISINE .....................................................................80 228 INSULIN LISPRO ..........................................................................80 INSULIN SYRINGES ......................................................................81 INTERFERON BETA-1A ................................................................92 INTERFERON BETA-1A/ALBUMIN ...............................................92 INTERFERON BETA-1B ................................................................92 INTERMEZZO ..............................................................................63 INTUNIV ......................................................................................65 INVEGA .......................................................................................64 INVIRASE 200MG ........................................................................94 INVIRASE 500MG ........................................................................94 INVOKANA ..................................................................................81 IODOQUINOL ..............................................................................38 IOPIDINE .....................................................................................57 IPRATROPIUM BROMIDE ...................................................... 43, 45 IPRATROPIUM/ ALBUTEROL SULFATE ........................................45 IQUIX ..........................................................................................59 IRBESARTAN ...............................................................................28 IRBESARTAN/ HCTZ ....................................................................28 IRON SUPPLEMENTS...................................................................95 ISOETHARINE ..............................................................................45 ISONIAZID ...................................................................................37 ISOPTIN ......................................................................................30 ISOPTO CARBACHOL ...................................................................57 ISOPTO CARBACHOL1%, 2%, 4%.................................................57 ISOPTO HOMATROPINE..............................................................57 ISORDIL 5, 10 ..............................................................................26 ISOSORBIDE DINITRATE ..............................................................26 ISOSORBIDE DINITRATE/ HYDRALAZINE .....................................26 ISOSORBIDE MONONITRATE ......................................................26 ISRADIPINE .................................................................................30 ISTALOL ......................................................................................57 ITRACONAZOLE ..........................................................................37 IVERMECTIN ......................................................................... 38, 55 IVIG .............................................................................................94 J JAKAFI .........................................................................................93 JALYN .................................................................................... 31, 90 JANUMET....................................................................................82 JANUVIA .....................................................................................82 JENTADUETO ..............................................................................82 JOLIVETTE ...................................................................................71 JUBLIA SOLUTION .......................................................................52 JUXTAPID ....................................................................................32 K KADIAN .......................................................................................40 KADIAN 10, 40, 70, 130, 150, 200MG .........................................40 KADIAN 130, 150MG ..................................................................40 KAPVAY.......................................................................................65 KARIVA .......................................................................................71 KAYEXALATE ...............................................................................90 KAZANO ......................................................................................82 KEFLEX ........................................................................................34 KENALOG ....................................................................................48 KENALOGAEROSOL SPRAY ..........................................................48 KEPPRA .......................................................................................67 KEPPRA XR ..................................................................................67 KERAFOAM .................................................................................49 KERALAC .....................................................................................50 KERLONE.....................................................................................30 KEROL 50% SUSPENSION ............................................................50 KEROL AD ...................................................................................50 KERYDIN .....................................................................................52 KETEK..........................................................................................35 KETOCONAZOLE .........................................................................52 KETOCONAZOLE FOAM/ CLEANSER ...........................................52 KETODAN KIT ..............................................................................52 KETOROLAC ................................................................................39 KETOROLAC TROMETHAMINE ....................................................61 KETOTIFEN ..................................................................................60 KINERET ......................................................................................89 KLONOPIN ..................................................................................67 KLOR-CON ..................................................................................85 KOMBIGLYZE XR .........................................................................82 KORLYM ......................................................................................81 K-PHOS ORIGINAL.......................................................................86 KYNAMRO ..................................................................................32 L LABETALOL ........................................................................... 30, 31 LAC-HYDRIN................................................................................50 LACOSAMIDE ..............................................................................67 LACTULOSE .................................................................................25 LACTULOSE SOLN .......................................................................25 LAMICTAL 5, 25MG DISPER TABLET............................................67 LAMICTAL ODT ...........................................................................67 LAMICTAL XR, STARTER KIT ........................................................67 LAMICTAL/XR .............................................................................67 LAMISIL .......................................................................................37 LAMISIL SOLN .............................................................................52 LAMOTRIGINE ............................................................................67 LANCETS .....................................................................................83 LANOXIN 125MCG ................................................................ 26, 27 LANSOPRAZOLE ..........................................................................21 LANTHANUM CARBONATE .........................................................92 LANTUS .......................................................................................80 LANTUS SOLOSTAR .....................................................................81 LASIX ...........................................................................................27 LASTACAFT .................................................................................60 LATANOPROST............................................................................58 LATUDA ......................................................................................64 LAZANDA ....................................................................................41 LEDIPASVIR/SOFOSBUVIR...........................................................91 LEFLUNOMIDE ............................................................................89 LESCOL........................................................................................32 LESCOL, XL ..................................................................................32 LESSINA ......................................................................................71 LETROZOLE .................................................................................95 LEUKINE ......................................................................................56 LEUPROLIDE ACETATE ................................................................79 LEVALBUTEROL ...........................................................................46 LEVAQUIN...................................................................................35 LEVATOL .....................................................................................30 LEVEMIR .....................................................................................81 LEVEMIR FLEXPEN ......................................................................81 LEVETIRACETAM .........................................................................67 LEVITRA ......................................................................................88 LEVOBUNOLOL ...........................................................................57 229 LEVOCARNITINE..........................................................................87 LEVOCETIRIZINE..........................................................................43 LEVODAPA/ CARBIDOPA ............................................................70 LEVOFLOXACIN ..................................................................... 35, 59 LEVOMILNACIPRAN ....................................................................62 LEVORA.......................................................................................72 LEVOTHROID ..............................................................................80 LEVOTHYROXINE SODIUM ..........................................................80 LEVOXYL .....................................................................................80 LEVSIN ........................................................................................24 LEXAPRO .....................................................................................62 LIALDA ........................................................................................22 LIBRAX ........................................................................................25 LIDOCAINE ..................................................................................89 LIDOCAINE/ TETRACAINE ...........................................................89 LIDODERM 5% PATCH ................................................................89 LIDORX GEL.................................................................................89 LINACLOTIDE ..............................................................................91 LINAGLIPTIN ...............................................................................82 LINAGLIPTIN/ ..............................................................................82 LINEZOLID ...................................................................................36 LINZESS .......................................................................................91 LIOTHYRONINE SODIUM ............................................................80 LIOTRIX .......................................................................................80 LIPITOR .......................................................................................32 LIPOFEN ......................................................................................32 LIPTRUZET ..................................................................................32 LIRAGLUTIDE ..............................................................................83 LISDEXAMFETAMINE DIMESYLATE .............................................66 LISINOPRIL ..................................................................................28 LISINOPRIL/ HCTZ .......................................................................28 LITHIUM .....................................................................................64 LITHOBID ....................................................................................64 LIVALO ........................................................................................32 L-NORGEST-ETH ESTR/ETHIN ESTRA..................................... 72, 75 LO MINASTRIN FE .......................................................................72 LO/OVRAL ...................................................................................72 LOCOID .......................................................................................48 LOCOID LOTN, LIPOCREAM ........................................................48 LODOSYN ....................................................................................69 LODOXAMIDE TROMETHAMINE .................................................60 LOESTRIN 21 1.5/30 ...................................................................72 LOESTRIN 21 1/20 ......................................................................72 LOESTRIN 24 FE ..........................................................................72 LOESTRIN FE 1/20 .......................................................................72 LOFIBRA ......................................................................................32 LOMITAPIDE MESYLATE .............................................................32 LOMOTIL.....................................................................................24 LOPERAMIDE ..............................................................................24 LOPID ..........................................................................................32 LOPRESSOR .................................................................................30 LOPRESSOR HCT .........................................................................30 LOPROX ......................................................................................52 LORATADINE...............................................................................42 LORATIDINE/ PSEUDOEPHEDRINE ..............................................44 LORAZEPAM ...............................................................................63 LORCET, PLUS .............................................................................41 LORZONE ....................................................................................69 LOSARTAN ..................................................................................28 LOSARTAN/ HCTZ .......................................................................29 LOSEASONIQUE ..........................................................................72 LOTEMAX....................................................................................58 LOTENSIN ...................................................................................28 LOTENSIN HCT ............................................................................28 LOTEPREDNOL ETABONATE .......................................................58 LOTEPREDNOLETABONATE ........................................................58 LOTREL 2.5-10, 5-10, 5-20, 10-20 ......................................... 28, 30 LOTRIMIN ...................................................................................52 LOTRISONE .................................................................................52 LOTRONEX ............................................................................ 23, 91 LOVASTATIN ......................................................................... 32, 33 LOVAZA ......................................................................................32 LOVENOX ....................................................................................55 LOW-OGESTREL ..........................................................................72 LOXAPINE ...................................................................................64 LOXITANE ...................................................................................64 LOZOL .........................................................................................27 LUBIPROSTONE .................................................................... 23, 91 LULICONAZOLE ...........................................................................52 LUMIGAN....................................................................................57 LUNESTA .....................................................................................63 LUPRON DEPOT 3.75 KIT ............................................................79 LURASIDONE ..............................................................................64 LUVOX CR ...................................................................................62 LUXIQ..........................................................................................48 LUZU ...........................................................................................52 LYBREL ........................................................................................72 LYRICA .................................................................................. 67, 92 M MACITENTAN..............................................................................31 MACROBID ........................................................................... 35, 36 MACRODANTIN 25MG ...............................................................36 MACRODANTIN 50, 100MG........................................................36 MAFENIDE ACETATE ...................................................................51 MALARONE.................................................................................38 MALATHION ...............................................................................55 MARAVIROC ...............................................................................94 MAVIK ........................................................................................28 MAXAIR ......................................................................................45 MAXALT, MLT .............................................................................68 MAXIDEX ....................................................................................58 MAXITROL ..................................................................................60 MAXZIDE.....................................................................................27 MECLIZINE ..................................................................................23 MEDROL .....................................................................................70 MEDROXY-PROGESTERONE/ MPA..............................................77 MEFENAMIC ACID ......................................................................39 MELOXICAM ...............................................................................39 MEMANTINE...............................................................................70 MENEST ......................................................................................76 MENOTROPINS ...........................................................................79 MENTAX .....................................................................................52 MEPENZOLATE BROMIDE ...........................................................24 MEPERIDINE ...............................................................................40 MEPHYTON.................................................................................86 MEPROBAMATE .........................................................................63 MEPRON .....................................................................................38 MESALAMINE .............................................................................22 MESTINON ..................................................................................69 MESTINON 180 ...........................................................................69 230 MESTRANOL 50MCG ............................................................ 73, 74 METADATE CD ............................................................................65 METADATE ER ............................................................................65 METAPROTERENOL SYRUP .........................................................46 METAPROTERENOL, 10MG/5ML ................................................46 METAXALONE .............................................................................69 METFORMIN ...............................................................................81 METHADONE .................................................................. 40, 41, 87 METHAMPHETAMINE.................................................................65 METHAZOLAMIDE ......................................................................58 METHENAMINE ..........................................................................35 METHENAMINE/METH BLUE/SALICYLATE ..................................36 METHENAMINE/METH BLUE/SALICYLATE/NA PHOS/HYOSCY ...36 METHERGINE ..............................................................................91 METHIMAZOLE ...........................................................................80 METHITEST .................................................................................78 METHOCARBAMOL.....................................................................69 METHOTREXATE .........................................................................51 METHOTREXATE TABS ................................................................51 METHSCOPOLAMINE BROMIDE .................................................25 METHSCOPOLAMINE COMBO ....................................................25 METHSUXIMIDE..........................................................................66 METHYLDOPA .............................................................................31 METHYLDOPA/ HCTZ ..................................................................31 METHYLERGONOVINE ................................................................91 METHYLIN CHEW TAB ................................................................65 METHYLIN SOLN 5MG/5ML ........................................................65 METHYLPHENIDATE.............................................................. 65, 66 METHYLPHENIDATE ORAL SUSP .................................................66 METHYLPHENIDATE PATCH ........................................................65 METHYLPHENIDATE, SUST. RELEASE ..........................................65 METHYLPREDNISOLONE .............................................................70 METHYLTESTOSTERONE .............................................................78 METIPRANOLOL..........................................................................58 METOCLOPRAMIDE ....................................................................24 METOLAZONE .............................................................................27 METOPROLOL .............................................................................30 METOPROLOL SUCCINATE ..........................................................31 METOPROLOL/ HCTZ ..................................................................30 METOPROLOL/HCTZ ...................................................................30 METROGEL 0.75%.......................................................................52 METROGEL-VAGINAL ............................................................ 52, 54 METRONIDAZOLE ..................................................... 35, 38, 52, 54 METRONIDAZOLE/ CLEANSER ....................................................52 MEVACOR ...................................................................................33 MIACALCIN NASAL ......................................................................80 MICARDIS ...................................................................................29 MICARDIS HCT ............................................................................29 MICONAZOLE .............................................................................37 MICONAZOLE NITRATE/ZINC OXIDE ...........................................52 MICROGESTIN FE 1.5/30 ............................................................72 MICROGESTIN FE 1/20 ...............................................................73 MICRO-K 10MEQ ........................................................................86 MICRONASE ................................................................................81 MIFEPRISTONE ...........................................................................81 MIGERGOT .................................................................................68 MIGLITOL ....................................................................................83 MIGRANAL NASAL SPRAY ...........................................................68 MILNACIPRAN ............................................................................92 MILTOWN ...................................................................................63 MINICYCLINE KIT ........................................................................34 MINIPRESS ..................................................................................31 MINOCIN ....................................................................................34 MINOCIN PAC .............................................................................34 MINOCYCLINE.............................................................................34 MIPOMERSEN.............................................................................32 MIRABEGRON .............................................................................90 MIRAPEX.....................................................................................69 MIRAPEX ER................................................................................69 MIRCETTE ...................................................................................73 MIRTAZAPINE .............................................................................62 MIRVASO ....................................................................................55 MISOPROSTOL ............................................................................21 MIXED POLLENS ALLERGEN EXTRACT .........................................86 MOBAN ......................................................................................64 MOBIC ........................................................................................39 MODAFINIL .................................................................................66 MODICON ...................................................................................73 MOEXIPRIL..................................................................................28 MOEXIPRIL/ HCTZ .......................................................................28 MOLINDONE ...............................................................................64 MOMETASONE ...........................................................................43 MOMETASONE FUROATE ..................................................... 45, 47 MOMETASONE FUROATE/AMMONIUM LAC .............................48 MOMETASONE/ .........................................................................45 MOMEXIN...................................................................................48 MONODOX .................................................................................34 MONONESSA ..............................................................................73 MONOPRIL .................................................................................28 MONOPRIL HCT ..........................................................................28 MONTELUKAST ..................................................................... 42, 47 MONUROL ..................................................................................36 MORPHINE .................................................................................41 MORPHINE SULFATE ............................................................ 40, 41 MORPHINE TABLETS ...................................................................41 MOTOFEN...................................................................................24 MOTRIN ......................................................................................39 MOVIPREP ..................................................................................25 MOXATAG 775 MG ER ................................................................33 MOXIFLOXACIN .................................................................... 35, 59 MS CONTIN.................................................................................41 MULTAQ .....................................................................................26 MUPIROCIN 2% ..........................................................................51 MUPIROCIN 2% CRM ..................................................................51 MUPIROCIN 2% OINT .................................................................51 MUSE ..........................................................................................88 MYAMBUTOL..............................................................................37 MYCELEX TROCHES.....................................................................37 MYCOBUTIN ...............................................................................37 MYCOPHENOLATE ......................................................................89 MYCOPHENOLATE MOFETIL .......................................................88 MYCOSTATIN ........................................................................ 52, 54 MYDRIACYL.................................................................................58 MYFORTIC...................................................................................89 MYRBETRIQ ................................................................................90 MYSOLINE...................................................................................67 N NA PICOSUL/MAG-OX/ CITRIC ACID ...........................................25 NABUMETONE............................................................................39 NADOLOL....................................................................................30 231 NADOLOL/ BENDROFLUMETHIAZIDE .........................................30 NAFARELIN ACETATE ..................................................................79 NAFTIFINE...................................................................................52 NAFTIN .......................................................................................52 NALTREXONE ..............................................................................87 NAMENDA ..................................................................................70 NAMENDA XR ............................................................................70 NAPHOS MB-MH/NAPHOS, DI-BA ..............................................25 NAPRELAN CR DOSEPAK .............................................................39 NAPROSYN..................................................................................39 NAPROXEN .................................................................................39 NAPROXEN SODIUM...................................................................39 NARATRIPTAN ............................................................................67 NARDIL .......................................................................................62 NASACORT AQ ............................................................................43 NASONEX ....................................................................................43 NATACYN ....................................................................................59 NATALIZUMAB............................................................................94 NATALVIT....................................................................................84 NATAMYCIN ...............................................................................59 NATAZIA .....................................................................................73 NATEGLINIDE ..............................................................................82 NATELLE ONE..............................................................................84 NAVANE ......................................................................................64 NAVANE 20 .................................................................................64 NEBIVOLOL .................................................................................30 NEBUPENT ..................................................................................38 NECON 0.5/35 ............................................................................73 NECON 1/35 ...............................................................................73 NECON 1/50 ...............................................................................73 NECON 10/11 .............................................................................73 NECON 7/7/7 ..............................................................................73 NEDOCROMIL SODIUM ..............................................................60 NEOMY SULF/ COLIST SUL/ HC/ THONZ .....................................61 NEORAL ......................................................................................89 NEOSALUS ..................................................................................50 NEOSPORIN ................................................................................59 NEPAFENAC ................................................................................61 NEPTAZANE ................................................................................58 NESINA .......................................................................................82 NESTABS .....................................................................................84 NESTABS DHA .............................................................................84 NEUPOGEN .................................................................................56 NEUPRO......................................................................................69 NEURIN-SL ..................................................................................86 NEURONTIN................................................................................67 NEVANAC ...................................................................................61 NEXA SELECT ..............................................................................84 NEXICLON XR ..............................................................................32 NEXIUM ......................................................................................21 NIACIN ........................................................................................33 NIACIN/ SIMVASTATIN ...............................................................33 NIACIN/LOVASTATIN ..................................................................32 NIASPAN .....................................................................................33 NICARDIPINE ..............................................................................29 NICOTINE INHALER .....................................................................95 NICOTINE NASAL SPRAY .............................................................95 NICOTINE POLACRILEX ...............................................................96 NICOTROL INHALER ....................................................................95 NICOTROL NS..............................................................................95 NIDOLDIPINE ..............................................................................30 NIFEDIPINE ........................................................................... 29, 30 NIMODIPINE ...............................................................................30 NIMOTOP ...................................................................................30 NIRAVAM....................................................................................63 NITAZOXANIDE ...........................................................................38 NITRO-BID OINT .........................................................................26 NITRO-DUR PATCHES 0.1, 0.2, 0.4, 0.6MG/HR ...........................26 NITRO-DUR PATCHES 0.3, 0.8MG/HR .........................................26 NITROFURANTOIN ................................................................ 35, 36 NITROGLYCERIN .........................................................................26 NITROGLYCERIN SUBLINGUAL ....................................................26 NITROGLYCERIN TRANSDERMAL ................................................26 NITROLINGUAL SPRAY ................................................................26 NITROSTAT .................................................................................26 NIZATIDINE .................................................................................21 NIZORAL .....................................................................................52 NORA-BE.....................................................................................73 NORDETTE ..................................................................................73 NORDITROPIN ............................................................................93 NORETH A-ET ESTRA/FE FUMARATE ..........................................71 NORETH-ETHINYL ESTRADIOL/IRON ...........................................71 NORETHINDRONE 0.35MG ............................................. 71, 73, 74 NORETHINDRONE ACETATE .......................................................77 NORFLEX .....................................................................................69 NORFLOXACIN ............................................................................35 NORINYL 1/35.............................................................................74 NORINYL 1+50 ............................................................................74 NORMODYNE .............................................................................30 NOROXIN ....................................................................................35 NORPACE ....................................................................................26 NORPACE CR 100MG ..................................................................26 NORPRAMIN ...............................................................................62 NORTREL 0.5/35 .........................................................................74 NORTREL 1/35 ............................................................................74 NORTREL 7/7/7...........................................................................74 NORTRIPTYLINE ..........................................................................62 NORVASC ....................................................................................30 NOVAREL ....................................................................................79 NOVOLIN INSULINS ....................................................................81 NOVOLOG INSULINS ...................................................................81 NOVOLOG MIX ...........................................................................81 NOXAFIL .....................................................................................37 NUCORT......................................................................................48 NUCYNTA....................................................................................41 NUCYNTA ER...............................................................................41 NULEV.........................................................................................25 NUMORPHAN .............................................................................41 NUOX GEL ...................................................................................53 NUTROPIN ..................................................................................93 NUVARING ..................................................................................76 NUVIGIL ......................................................................................65 NYSTATIN ............................................................................. 52, 54 NYSTATIN VAGINAL TABS ...........................................................54 NYSTATIN/EMOLLIENT ...............................................................52 O OB COMPLETE, PREMIER, ONE, 400, DHA ..................................84 OBSTETRIX EC .............................................................................85 OCUFLOX ....................................................................................59 OFLOXACIN .................................................................................59 232 OGEN ..........................................................................................76 OGESTREL ...................................................................................74 OLANZAPINE ...............................................................................65 OLANZAPINE/ FLUOXETINE ........................................................65 OLEPTRO ER................................................................................62 OLMESARTAN .............................................................................28 OLMESARTAN MED/ AMLODIPINE/HCTZ ...................................29 OLMESARTAN/ HCTZ ..................................................................28 OLOPATADINE ...................................................................... 43, 60 OLSALAZINE ................................................................................22 OLUX...........................................................................................48 OLUX-E .......................................................................................48 OLYSIO ........................................................................................91 OMECLAMOX-PAK ......................................................................21 OMEGA-3-ACID ETHYL ESTERS ...................................................32 OMEPRAZOLE ....................................................................... 21, 22 OMEPRAZOLE MAGNESIUM .......................................................21 OMEPRAZOLE-CLARITHROMYCIN- AMOXICILLIN .......................21 OMNARIS ....................................................................................43 OMNITROPE ...............................................................................93 ONDANSETRON ..........................................................................24 ONFI ...........................................................................................67 ONFI SUSPENSION ......................................................................67 ONGLYZA ....................................................................................82 ONMEL .......................................................................................37 OPANA ........................................................................................41 OPANA, ER ..................................................................................41 OPSUMIT ....................................................................................31 OPTASE .......................................................................................55 OPTIVAR .....................................................................................60 ORACEA ......................................................................................34 ORAL FLUORIDE ..........................................................................95 ORALAIR .....................................................................................86 ORAP ..........................................................................................64 ORAVIG.......................................................................................37 ORENCIA SQ...............................................................................89 ORENCIA IV .................................................................................94 ORPHENADRINE .........................................................................69 ORTHO EVRA PATCH ..................................................................76 ORTHO MICRONOR ....................................................................74 ORTHO TRI-CYCLEN ....................................................................74 ORTHO TRI-CYCLEN LO ...............................................................74 ORTHO-CEPT ..............................................................................75 ORTHO-CYCLEN ..........................................................................74 ORTHO-NOVUM 1/35 .................................................................74 ORTHO-NOVUM 1/50 .................................................................74 ORTHO-NOVUM 7/7/7 ...............................................................74 OSELTAMIVIR .............................................................................38 OSENI..........................................................................................82 OSMOPREP .................................................................................25 OSPEMIFENE ..............................................................................91 OSPHENA ....................................................................................91 OTC ASPIRIN ...............................................................................96 OTC NICORETTE GUM ................................................................96 OTC NICOTINE LOZENGE ............................................................96 OTC NICOTINE PATCHES .............................................................96 OTEZLA .......................................................................................89 OVCON 35 ..................................................................................75 OVCON 50 ..................................................................................75 OVIDE .........................................................................................55 OVIDREL .....................................................................................79 OXANDRIN ..................................................................................78 OXANDROLONE ..........................................................................78 OXAPROZIN ................................................................................39 OXCARBAZEPINE.........................................................................67 OXICONAZOLE NITRATE..............................................................52 OXISTAT ......................................................................................52 OXTELLAR XR ..............................................................................67 OXYBUTYNIN ..............................................................................90 OXYBUTYNIN CHLORIDE .............................................................90 OXYCODONE...............................................................................41 OXYCODONE/ IBUPROFEN .........................................................41 OXYCONTIN ................................................................................41 OXYMORPHONE .........................................................................41 OXYMORPHONE ER (NON-CRUSH RESISTANT) ...........................41 OXYTROL PATCH .........................................................................90 P PACERONE ..................................................................................27 PACNEX ......................................................................................54 PACNEX MX ................................................................................54 PALIPERIDONE ............................................................................64 PALIVIZUMAB .............................................................................94 PAMELOR ...................................................................................62 PAMINE ......................................................................................25 PAMINE FORTE ...........................................................................25 PAMINE FQ .................................................................................25 PANCREAZE ................................................................................23 PANDEL.......................................................................................48 PANRETIN ...................................................................................55 PANTOPRAZOLE .........................................................................21 PAPAVERINE ...............................................................................26 PARAFON FORTE DSC .................................................................69 PARCOPA ....................................................................................69 PARICALCITOL.............................................................................80 PARLODEL ...................................................................................69 PARNATE ....................................................................................62 PAROXETINE ......................................................................... 62, 91 PATADAY ....................................................................................60 PATANASE ..................................................................................43 PATANOL ....................................................................................60 PAXIL, CR ....................................................................................62 PCE .............................................................................................35 PEDIADERM AF ...........................................................................52 PEDIADERM HC 2% KIT ...............................................................48 PEDIADERM TA ...........................................................................48 PEDIAPRED LIQUID .....................................................................70 PEG3350/NA SULF/ BICARB/KCL ................................................25 PEG3350/NA SULF/BICARB/CL/KCL ............................................25 PEG3350/SOD SUL/NACL/ASB/CL/KCL .......................................25 PEGANONE .................................................................................67 PEGASYS .....................................................................................91 PEGINTERFERON ALFA-2A ..........................................................91 PEGINTERFERON ALFA-2B ..........................................................91 PEG-INTRON ...............................................................................91 PENBUTOLOL ..............................................................................30 PENICILLAMINE ..........................................................................87 PENLAC .......................................................................................52 PENTAMIDINE ISETHIONATE ......................................................38 PENTASA.....................................................................................22 PENTOSAN POLYSULFATE ...........................................................90 233 PENTOXIFYLLINE .........................................................................56 PEPCID RPD ................................................................................21 PEPCID TABS ...............................................................................21 PERAMPANEL .............................................................................66 PERCOCET...................................................................................41 PERCODAN .................................................................................41 PERINDOPRIL ..............................................................................27 PERIOSTAT ..................................................................................34 PERSANTINE ...............................................................................56 PERTZYE ......................................................................................23 PEXEVA .......................................................................................62 PHENAZOPYRIDINE .....................................................................90 PHENELZINE................................................................................62 PHENERGAN ......................................................................... 24, 42 PHENOBARBITAL ........................................................................67 PHENOXYBENZAMINE ................................................................31 PHENYLEPHRINE/ CHLORPHENIRAMINE ....................................44 PHENYTOIN ................................................................................66 PHOSLO ......................................................................................93 PHOSPHOLINE IODIDE SOLN ......................................................58 PHRENILIN/ PHRENILIN FORTE ...................................................41 PHYTONADIONE .........................................................................86 PILOCAR......................................................................................58 PILOCARPINE ..............................................................................58 PILOPINE HS ...............................................................................58 PIMECROLIMUS ..........................................................................50 PIMOZIDE ...................................................................................64 PIOGLITAZONE ...........................................................................82 PIOGLITAZONE/ ..........................................................................82 PIOGLITAZONE/ GLIMEPIRIDE ....................................................82 PIOGLITAZONE/ METFORMIN ....................................................82 PIRBUTEROL ...............................................................................45 PIROXICAM .................................................................................39 PITAVASTATIN CALCIUM ............................................................32 PLAQUENIL .................................................................................38 PLAVIX ........................................................................................56 PLETAL ........................................................................................56 PLEXION 9.8-4.8% CRM, LIQ, LOT, PADS ....................................49 PLIAGLIS .....................................................................................89 PODOFILOX.................................................................................55 POLYMYXIN/ BACITRACIN ..........................................................59 POLYMYXIN/ BACITRACIN/ NEOMYCIN ......................................59 POLYMYXIN/ TRIMETHOPRIM ....................................................59 POLYSPORIN ...............................................................................59 POLYTRIM ...................................................................................59 PONSTEL .....................................................................................39 PORTIA .......................................................................................75 POSACONAZOLE .........................................................................37 POTASSIUM CHLORIDE ......................................................... 85, 86 POTASSIUM CITRATE ..................................................................87 POTASSIUM IODIDE ....................................................................86 POTASSIUM PHOSPHATE............................................................86 POTIGA .......................................................................................67 PRADAXA ....................................................................................56 PRAMIPEXOLE ............................................................................69 PRAMIPEXOLE DI-HCL.................................................................69 PRAMLINTIDE ACETATE ..............................................................83 PRAMOXINE ...............................................................................23 PRANDIMET ................................................................................82 PRANDIN ....................................................................................82 PRASUGREL HYDROCHLORIDE....................................................56 PRAVACHOL................................................................................33 PRAVASTATIN .............................................................................33 PRAZIQUANTEL...........................................................................38 PRAZOSIN ...................................................................................31 PRECOSE .....................................................................................83 PRED FORTE................................................................................58 PRED MILD..................................................................................59 PREDNISOLONE .............................................................. 58, 59, 70 PREDNISONE ..............................................................................89 PREFERA-OB ONE .......................................................................85 PREFERA-OB PLUS DHA ..............................................................85 PREFEST ......................................................................................78 PREFFERA OB ..............................................................................85 PREGABALIN ......................................................................... 67, 92 PREGNYL .....................................................................................79 PREMARIN ORAL ........................................................................77 PREMARIN VAG CREAM .............................................................77 PREMPHASE ...............................................................................78 PREMPRO ...................................................................................78 PRENATA ....................................................................................85 PRENATAL COMPLETE ................................................................85 PRENATAL PLUS..........................................................................85 PRENATE ELITE ...........................................................................85 PRENATE MINI ............................................................................85 PRENEXA.....................................................................................85 PREPOPIK....................................................................................25 PREQUE 10 .................................................................................85 PREVACID ...................................................................................21 PREVACID SOLUTAB ...................................................................21 PREVALITE ..................................................................................33 PREVENTATIVE MEDICATION FOR HEALTH CARE REFORM COVERED AT A ZERO COPAY WITH PRESCRIPTION ...............95 PREVIDENT 5000 BOOSTER GEL .................................................86 PREVIDENT 5000 PLUS CREAM ...................................................86 PREVIDENT 5000 SENSITIVE 1.1%-5%.........................................86 PREVIDENT DENTAL RINSE .........................................................86 PREVIDENT GEL ..........................................................................86 PREZISTA ....................................................................................94 PRIFTIN .......................................................................................37 PRILOSEC ....................................................................................21 PRILOSEC 40MG .........................................................................21 PRILOSEC DR SUSP......................................................................21 PRIMAQUINE ..............................................................................38 PRIMIDONE ................................................................................67 PRINIVIL ......................................................................................28 PRINZIDE ....................................................................................28 PRISTIQ .......................................................................................62 PROAIR HFA ................................................................................45 PRO-BANTHINE 7.5MG ...............................................................25 PROBENECID...............................................................................83 PROCAINAMIDE ..........................................................................27 PROCARDIA, XL ...........................................................................30 PROCHLORPERAZINE ..................................................................23 PROCRIT .....................................................................................56 PROCTOFOAM ............................................................................23 PROCTOFOAM HC ......................................................................23 PRODRIN.....................................................................................68 PROGESTERONE .........................................................................77 PROGRAF ....................................................................................89 PROLENSA ..................................................................................61 PROMETHAZINE ................................................................... 24, 42 234 PROMETRIUM ............................................................................77 PROMISEB ..................................................................................50 PROMISEB COMPLETE ................................................................50 PRONESTYL 375, 500 ..................................................................27 PROPAFENONE ...........................................................................27 PROPANTHELINE ........................................................................25 PROPINE .....................................................................................58 PROPRANOLOL ..................................................................... 30, 68 PROPRANOLOL SR ......................................................................68 PROPYLTHIOURACIL ...................................................................80 PROQUIN XR ...............................................................................35 PROSCAR ....................................................................................90 PROTONIX ..................................................................................21 PROTONIX PAK ...........................................................................21 PROTOPIC ...................................................................................55 PROTRIPTYLINE...........................................................................63 PROVENTIL HFA ..........................................................................45 PROVERA ....................................................................................77 PROVIGIL ....................................................................................66 PROZAC ......................................................................................62 PROZAC WEEKLY ........................................................................62 PSEUDOEPHEDRINE/ ACRIVAS ...................................................44 PSEUDOEPHEDRINE/ CHLORPHENIRAMINE ...............................44 PSEUDOEPHEDRINE/ DESLORATADINE ......................................44 PULMICORT ................................................................................45 PULMICORT 0.25MG/2ML AND 0.5MG/2ML RESPULE ..............45 PULMICORT 1MG/2ML RESPULE, FLEXHALER AND TURBUHALER ..............................................................................................46 PULMOZYME ........................................................................ 46, 47 PYRAZINAMIDE ...........................................................................37 PYRIDIUM ...................................................................................90 PYRIDOSTIGMINE .......................................................................69 PYRIMETHAMINE........................................................................38 Q QNASL ........................................................................................43 QUDEXY XR .................................................................................67 QUESTRAN BULK ........................................................................33 QUETIAPINE FUMARATE ............................................................64 QUILLIVANT XR ...........................................................................66 QUINAPRIL..................................................................................27 QUINAPRIL/ HCTZ .......................................................................27 QUININE SULFATE ......................................................................87 QUIXIN ........................................................................................59 QVAR ..........................................................................................46 R RABEPRAZOLE ............................................................................21 RAGWITEK ..................................................................................87 RALOXIFENE ......................................................................... 79, 95 RAMELTEON ...............................................................................63 RAMIPRIL ....................................................................................27 RANEXA ......................................................................................27 RANITIDINE .................................................................................22 RANOLAZINE...............................................................................27 RAPAFLO.....................................................................................90 RAPAMUNE ................................................................................89 RASAGILINE ................................................................................69 RAYOS.........................................................................................89 RAZADYNE ..................................................................................70 REBETOL .....................................................................................91 REBETOL ORAL SOLUTION ..........................................................91 REBIF ..........................................................................................92 RECTIV OINT ...............................................................................26 REGLAN ......................................................................................24 RELAFEN .....................................................................................39 RELENZA .....................................................................................37 RELPAX .......................................................................................68 REMERON ...................................................................................62 REMICADE ..................................................................................94 RENAGEL ....................................................................................93 RENVELA .....................................................................................93 REPAGLINIDE ..............................................................................82 REPAGLINIDE/METFORMIN ........................................................82 REPREXAIN .................................................................................41 REPRONEX ..................................................................................79 REQUIP .......................................................................................69 REQUIP XL...................................................................................70 RESTASIS .....................................................................................60 RESTORIL ....................................................................................63 RETAPAMULIN ............................................................................51 RETIN A .......................................................................................54 RETIN A MICRO...........................................................................54 RETIN A MICRO 0.1% ................................................................ See REVATIO .....................................................................................31 REVIA ..........................................................................................87 RHINOCORT AQUA .....................................................................43 RIAX ............................................................................................54 RIBAPAK .....................................................................................91 RIBASPHERE................................................................................91 RIBATAB .....................................................................................91 RIBAVIRIN ...................................................................................91 RIDAURA.....................................................................................89 RIFABUTIN ..................................................................................37 RIFADIN ......................................................................................37 RIFAMATE ...................................................................................37 RIFAMPIN ...................................................................................37 RIFAMPIN/ INH/ PYRAZINAMIDE ................................................37 RIFAMPIN/ ISONIAZID ................................................................37 RIFAPENTINE ..............................................................................37 RIFATER ......................................................................................37 RIFAXIMIN ..................................................................................36 RILPIVIRINE .................................................................................93 RIMANTADINE ............................................................................37 RIMEXOLONE..............................................................................59 RIOCIGUAT .................................................................................31 RISEDRONATE .............................................................................79 RISEDRONATE SODIUM ..............................................................79 RISPERDAL ..................................................................................64 RISPERDAL CONSTA ....................................................................64 RISPERIDONE ..............................................................................64 RISPERIDONE MICROSPHERES....................................................64 RITALIN .......................................................................................66 RITALIN LA ..................................................................................66 RITALIN SR ..................................................................................66 RITUXAN .....................................................................................94 RITUXIMAB .................................................................................94 RIVAROXABAN ............................................................................56 RIVASTIGMINE ............................................................................70 RIZATRIPTAN ..............................................................................68 235 ROBAXIN.....................................................................................69 ROCALTROL ................................................................................86 ROFLUMILAST.............................................................................46 ROPINIROLE .......................................................................... 69, 70 ROSADAN KIT .............................................................................52 ROSANIL .....................................................................................49 ROSIGLITAZONE..........................................................................82 ROSIGLITAZONE/ GLIMEPIRIDE ..................................................82 ROSIGLITAZONE/ METFORMIN ..................................................82 ROSUVASTATIN ..........................................................................32 ROTIGOTINE ...............................................................................69 ROWASA ENEMA ........................................................................22 ROZEREM ...................................................................................63 RUFINAMIDE ..............................................................................66 RUXOLITINIB ...............................................................................93 RYBIX ODT ..................................................................................41 RYTHMOL SR ..............................................................................27 RYZOLT .......................................................................................41 S SABRIL ........................................................................................67 SAFYRAL .....................................................................................75 SALMETEROL ..............................................................................46 SAMSCA ......................................................................................93 SANCTURA ..................................................................................90 SANCTURA, XR ............................................................................90 SANCUSO ....................................................................................24 SANDIMMUNE ............................................................................89 SAPHRIS ......................................................................................64 SAQUINAVIR ...............................................................................94 SARAFEM ....................................................................................62 SARGRAMOSTIM ........................................................................56 SAVELLA......................................................................................92 SAXAGLIPTIN HYDROCHLORIDE..................................................82 SAXAGLIPTIN/ .............................................................................82 SCOPOLAMINE ...........................................................................24 SEASONALE.................................................................................75 SEASONIQUE ..............................................................................75 SECTRAL................................................................................ 27, 30 SELECT-OB ..................................................................................85 SELECT-OB + DHA .......................................................................85 SELEGILINE ........................................................................... 62, 70 SELENIUM SULFIDE.....................................................................52 SELZENTRY ..................................................................................94 SEMPREX-D.................................................................................44 SEREVENT DISKUS ......................................................................46 SEROMYCIN PULVULES ...............................................................37 SEROQUEL ..................................................................................64 SEROQUEL, XR ............................................................................64 SERTACONAZOLE NITRATE .........................................................51 SERTRALINE ................................................................................63 SEVELAMER ................................................................................93 SEVELAMER CARBONATE ...........................................................93 SF ROWASA ENEMA ...................................................................22 SHORT RAGWEED POLLEN ALLERGEN EXTRACT .........................87 SILDENAFIL .................................................................................88 SILDENAFIL CITRATE ...................................................................31 SILENOR ......................................................................................63 SILODOSIN ..................................................................................90 SILVADENE..................................................................................51 SILVER SULFADIAZINE .................................................................51 SIMBRINZA .................................................................................58 SIMCOR ......................................................................................33 SIMEPREVIR ................................................................................91 SIMPONI .....................................................................................89 SIMVASTATIN .............................................................................33 SINEMET, CR ...............................................................................70 SINGULAIR ............................................................................ 42, 47 SIROLIMUS .................................................................................89 SIRTURO .....................................................................................37 SITAGLIPTIN PHOS/ METFORMIN ...............................................82 SITAGLIPTIN PHOSPHATE ...........................................................82 SKELAXIN ....................................................................................69 SKLICE .........................................................................................55 SODIUM /POTASSIUM/MAG SULFATES .....................................25 SODIUM FLUORIDE .....................................................................86 SODIUM OXYBATE ......................................................................66 SODIUM POLYSTYRENE SULFONATE ..........................................90 SOFOSBUVIR ...............................................................................91 SOLARAZE ...................................................................................55 SOLIFENACIN SUCCINATE ...........................................................90 SOLODYN ....................................................................................34 SOLTAMOX .................................................................................96 SOMA .........................................................................................69 SOMATROPIN .............................................................................93 SOMNOTE...................................................................................64 SONATA ......................................................................................64 SORIATANE .................................................................................51 SOTALOL .....................................................................................26 SOVALDI .....................................................................................91 SPECTRACEF ...............................................................................34 SPIRIVA .......................................................................................46 SPIRONOLACTONE......................................................................27 SPIRONOLACTONE/ HCTZ ...........................................................27 SPORANOX CAPS ........................................................................37 SPORANOX SOLN ........................................................................37 SPRINTEC ....................................................................................75 SSKI SOLUTION ...........................................................................86 STADOL NS .................................................................................41 STALEVO .....................................................................................70 STARLIX.......................................................................................82 STAXYN .......................................................................................88 STRATTERA .................................................................................66 STRIANT ......................................................................................78 STRIPS .........................................................................................83 STROMECTOL .............................................................................38 SUBOXONE .................................................................................87 SUBSYS .......................................................................................41 SUBUTEX ....................................................................................88 SUCLEAR .....................................................................................25 SUCRALFATE ...............................................................................21 SUCROFERRIC OXYHYDROXIDE...................................................93 SULAR 20, 30, 10 ........................................................................30 SULCONAZOLE NITRATE .............................................................52 SULFACETAMIDE SODIUM ..........................................................59 SULFACETAMIDE/ PREDNISOLONE .............................................60 SULFACETAMIDE/SULFUR ..........................................................49 SULFAMETHOXAZOLE/ TRIMETHOPRIM .............................. 35, 36 SULFAMETHOXAZOLE/ TRIMETHOPRIM DS ......................... 35, 36 SULFAMYLON .............................................................................51 SULFANILAMIDE .........................................................................54 236 SULFASALAZINE ..........................................................................22 SULINDAC ...................................................................................39 SUMADAN ..................................................................................49 SUMATRIPTAN INJECTION ..........................................................68 SUMATRIPTAN NASAL SPRAY .....................................................68 SUMATRIPTAN TABLET ...............................................................68 SUMATRIPTAN/ NAPROXEN .......................................................68 SUMAVEL DOSEPRO ...................................................................68 SUMYCIN ....................................................................................34 SUPRAX.......................................................................................34 SUPREP .......................................................................................25 SURMONTIL ................................................................................63 SYMAX DUOTAB .........................................................................25 SYMAX, DUOTAB ........................................................................25 SYMBICORT ................................................................................46 SYMBYAX ....................................................................................65 SYMLIN .......................................................................................83 SYMLINPEN.................................................................................83 SYNAGIS......................................................................................94 SYNALAR TS ................................................................................48 SYNAREL NASAL SPRAY...............................................................79 SYNTHROID.................................................................................80 SYRINGES ....................................................................................81 T TACLONEX OINT .........................................................................51 TACLONEX SCALP SUSP ..............................................................51 TACROLIMUS ........................................................................ 55, 89 TADALAFIL ............................................................................ 31, 88 TAFLUPROST ...............................................................................58 TAGAMET ...................................................................................21 TAMBOCOR ................................................................................27 TAMIFLU .....................................................................................38 TAMOXIFEN ................................................................................96 TAMSULOSIN ........................................................................ 31, 90 TANZEUM ...................................................................................83 TAPAZOLE ...................................................................................80 TAPENTADOL HYDROCHLORIDE .................................................41 TARGRETIN .................................................................................55 TARKA .........................................................................................28 TASIMELTEON ............................................................................63 TASMAR ......................................................................................70 TAVABOROLE..............................................................................52 TAVIST ........................................................................................43 TAZAROTENE ..............................................................................51 TAZORAC ....................................................................................51 TECFIDERA ..................................................................................92 TEGRETOL XR ..............................................................................67 TEGRETOL XR 100MG .................................................................67 TEKAMLO....................................................................................30 TEKTURNA ..................................................................................32 TEKTURNA HCT ...........................................................................32 TELITHROMYCIN .........................................................................35 TELMISARTAN.............................................................................29 TELMISARTAN/ ...........................................................................29 TELMISARTAN/ HCTZ ..................................................................29 TEMAZEPAM ..............................................................................63 TEMOVATE .................................................................................48 TENEX .........................................................................................32 TENORETIC .................................................................................31 TENORMIN .................................................................................31 TERAZOL .....................................................................................55 TERBINAFINE ........................................................................ 37, 52 TERBINAFINE/ .............................................................................52 TERBINEX ....................................................................................52 TERCONAZOLE ............................................................................55 TERIFLUNOMIDE.........................................................................92 TERIPARATIDE ............................................................................79 TERSI...........................................................................................52 TESSALON PERLES ......................................................................44 TEST STRIPS ................................................................................83 TESTIM .......................................................................................78 TESTOPEL....................................................................................94 TESTOSTERONE ..........................................................................78 TESTOSTERONE PELLET ..............................................................94 TESTOSTERONE, TRANSDERMAL ................................................78 TESTRED .....................................................................................78 TETRACYCLINE ............................................................................34 TEVETEN .....................................................................................29 TEVETEN HCT..............................................................................29 THEO-24 SR ................................................................................46 THEOPHYLLINE ...........................................................................46 THIOTHIXENE..............................................................................64 THYROID, DESSICATED ...............................................................80 THYROLAR ..................................................................................80 TIAGABINE ............................................................................ 66, 67 TICAGRELOR ...............................................................................55 TIGAN .........................................................................................24 TIKOSYN......................................................................................27 TIMOLOL......................................................................... 30, 57, 58 TIMOLOL/ DORZOLAM ...............................................................57 TIMOPTIC ...................................................................................58 TIMOPTIC OCUDOSE...................................................................58 TIMOPTIC XE...............................................................................58 TIMOTHY GRASS POLLEN ALLERGEN EXTRACT ...........................86 TINDAMAX..................................................................................38 TINIDAZOLE ................................................................................38 TIOTROPIUM BROMIDE ..............................................................46 TIPRANAVIR ................................................................................93 TIROSINT ....................................................................................80 TIZANIDINE .................................................................................69 TIZANIDINE COMBO ...................................................................69 TOBI INHALATION /PODHALER...................................................92 TOBRADEX ..................................................................................60 TOBRADEX OINT .........................................................................60 TOBRADEX ST .............................................................................60 TOBRAMYCIN ....................................................................... 59, 92 TOBRAMYCIN/ ............................................................................60 TOBRAMYCIN/LOTEPRED ETAB ..................................................59 TOBREX OINT..............................................................................59 TOBREX SOLN .............................................................................59 TOCILIZUMAB ....................................................................... 89, 94 TOFACITINIB ...............................................................................89 TOFRANIL PM .............................................................................63 TOLCAPONE ................................................................................70 TOLTERODINE TARTRATE ...........................................................90 TOLVAPTAN ................................................................................93 TOPAMAX ...................................................................................67 TOPICORT ...................................................................................48 TOPICORT GENERIC PRODUCTS..................................................48 TOPIRAMATE ..............................................................................67 237 TOPROL XL ..................................................................................31 TORADOL ....................................................................................39 TOREMIFENE ..............................................................................95 TORSEMIDE ................................................................................27 TOVIAZ........................................................................................90 TRACLEER ...................................................................................31 TRADJENTA .................................................................................82 TRAMADOL ..................................................................... 40, 41, 42 TRAMADOL ER ............................................................................41 TRAMADOL SUST. RELEASE ........................................................42 TRAMADOL/ ACETAMINOPHEN .................................................42 TRANDATE ..................................................................................31 TRANDOLAPRIL ...........................................................................28 TRANDOLAPRIL/ VERAPAMIL .....................................................28 TRANSDERM-SCOP .....................................................................24 TRANXENE T ...............................................................................63 TRANYLCYPROMINE ...................................................................62 TRAVATAN Z ...............................................................................58 TRAVOPROST ..............................................................................58 TRAZODONE HYDROCHLORIDE EXTENDED RELEASE ..................62 TREAGAN OTIC ...........................................................................61 TRECATOR ..................................................................................37 TRENTAL .....................................................................................56 TREPROSTINIL/NEBULIZER KIT....................................................31 TRETIN X .....................................................................................54 TRETINOIN ............................................................................ 53, 54 TRETINOIN MICROSPHERES........................................................54 TREXIMET ...................................................................................68 TRIAMCINOLONE .................................................................. 48, 70 TRIAMCINOLONE, AQUEOUS .....................................................43 TRIAMCINOLONE/ ......................................................................48 TRIAMTERENE ............................................................................27 TRIAMTERENE/ HCTZ..................................................................27 TRIAZ CLEANER/PADS.................................................................54 TRIBENZOR .................................................................................29 TRICOR .......................................................................................33 TRIFLURIDINE .............................................................................59 TRIGLIDE .....................................................................................33 TRILEPTAL ...................................................................................67 TRILIPIX.......................................................................................33 TRIMETHOBENZAMIDE...............................................................24 TRIMETHOPRIM..........................................................................36 TRIMIPRAMINE MALEATE ..........................................................63 TRINESSA ....................................................................................75 TRI-NORINYL ...............................................................................75 TRIOXIN ......................................................................................61 TRI-SPRINTEC..............................................................................75 TRIVORA .....................................................................................75 TRIZIVIR ......................................................................................94 TROKENDI XR ..............................................................................67 TROPAZONE ...............................................................................50 TROPICAMIDE.............................................................................58 TROSPIUM CHLORIDE .................................................................90 TRUSOPT ....................................................................................58 TRUVADA....................................................................................94 TRYPSIN/ BALSAM PERU/ CASTOR OIL .......................................55 TUDORZA PRESSAIR....................................................................46 TUSSIONEX PENNKINETIC ...........................................................43 TWYNSTA ...................................................................................29 TYLENOL W/CODEINE .................................................................42 TYLOX .........................................................................................42 TYSABRI ......................................................................................94 TYVASO.......................................................................................31 U UCERIS ........................................................................................22 U-CORT 1%-10% CREAM ............................................................48 ULESFIA ......................................................................................55 ULORIC .......................................................................................83 ULTRACET ...................................................................................42 ULTRAM......................................................................................42 ULTRAM ER.................................................................................42 ULTRASE .....................................................................................23 ULTRASE MT 12, 18 ....................................................................23 ULTRAVATE PAC .........................................................................49 ULTRESA .....................................................................................23 UMECLIDINIUM/ VILANTEROL....................................................45 UMECTA .....................................................................................50 UMECTA EMULSION ...................................................................50 UNIRETIC ....................................................................................28 UNIVASC .....................................................................................28 URAMAXIN .................................................................................50 URAMAXIN GT ............................................................................50 URAMAXIN GT KIT ......................................................................50 UREA..................................................................................... 49, 50 UREA/ LACTIC ACID/ SALICYL ACID .............................................50 UREA/LACTIC AC/ZN UNDECYLENATE ........................................50 URECHOLINE...............................................................................90 URELLE........................................................................................36 UROCIT-K ....................................................................................87 UROCIT-K 15MEQ .......................................................................87 UROFOLLITROPIN (FSH) ..............................................................78 UROXATRAL ................................................................................91 URSODIOL...................................................................................87 UTA .............................................................................................36 UTOPIC .......................................................................................50 V VAGIFEM ....................................................................................77 VALACYCLOVIR ...........................................................................38 VALIUM ......................................................................................63 VALPROIC ACID ...........................................................................66 VALSARTAN ................................................................................28 VALSARTAN/ HCTZ .....................................................................28 VALTREX .....................................................................................38 VALTURNA ............................................................................ 29, 32 VANCOCIN ..................................................................................36 VANCOMYCIN, ORAL ..................................................................36 VANOS ........................................................................................49 VANOXIDE HC .............................................................................54 VANOXIDE-HC 0.5%-5% LOTION.................................................49 VARDENAFIL ...............................................................................88 VARENICLINE TARTRATE.............................................................95 VASCEPA .....................................................................................33 VASERETIC ..................................................................................28 VASOTEC.....................................................................................28 VECTICAL ....................................................................................55 VEDOLIZUMAB ...........................................................................94 VELPHORO ..................................................................................93 VELTIN ........................................................................................54 238 VENLAFAXINE .............................................................................62 VENTOLIN ...................................................................................46 VENTOLIN HFA............................................................................46 VERAMYST ..................................................................................43 VERAPAMIL .................................................................... 26, 29, 30 VERDESO ....................................................................................49 VERELAN .....................................................................................30 VERSACLOZ .................................................................................65 VESICARE ....................................................................................91 VEXOL .........................................................................................59 VFEND ........................................................................................37 VIAGRA .......................................................................................88 VIBRAMYCIN......................................................................... 34, 36 VIBRAMYCIN SUSP......................................................................34 VIBRAMYCIN SYRUP ...................................................................34 VICODIN 10/300 .........................................................................42 VICODIN 5/300 ...........................................................................42 VICODIN 7.5/300 ........................................................................42 VICOPROFEN ..............................................................................42 VICTOZA .....................................................................................83 VICTRELIS....................................................................................91 VIGABATRIN ...............................................................................67 VIGAMOX ...................................................................................59 VIIBRYD.......................................................................................63 VILAZODONE ..............................................................................63 VIMOVO .....................................................................................39 VIMPAT.......................................................................................67 VIOKASE 8...................................................................................23 VIRAZOLE ....................................................................................91 VIROPTIC ....................................................................................59 VISTARIL .....................................................................................63 VITAFOL-OB ................................................................................85 VITAFOL-ONE..............................................................................85 VITAFOL-PLUS.............................................................................85 VITAMED MD ONE RX/QUATREFOLIC ........................................85 VITAMED MD PLUS.....................................................................85 VITAMED MD REDICHEW RX/QUATREFOLIC ..............................85 VITAMINS, PRENATAL........................................................... 84, 85 VITAMINS, PRENATAL PREP........................................................84 VITMAINS, PRENATAL.................................................................84 VITUZ ..........................................................................................43 VIVA CT PRENATAL .....................................................................85 VIVACTIL .....................................................................................63 VIVELLE-DOT...............................................................................77 VOLTAREN GEL ...........................................................................39 VOLTAREN XR .............................................................................39 VORICONAZOLE ..........................................................................37 VORTIOXETINE............................................................................62 VOSOL ........................................................................................61 VOSOL HC ...................................................................................61 VOSPIRE ER .................................................................................46 VUSION .......................................................................................52 VYTORIN .....................................................................................33 VYVANSE ....................................................................................66 W WARFARIN ..................................................................................55 WELCHOL ...................................................................................33 WELLBUTRIN ..............................................................................63 WELLBUTRIN XL ..........................................................................63 WESTCORT .................................................................................49 X XALATAN ....................................................................................58 XANAX ........................................................................................63 XANAX XR ...................................................................................63 XARELTO 10mg ...........................................................................56 XARELTO 15mg , 20mg ...............................................................56 XARTEMIS XR ..............................................................................42 XELJANZ ......................................................................................89 XIFAXAN .....................................................................................36 XODOL ........................................................................................42 XOLEGEL .....................................................................................52 XOPENEX NEB SOLN ...................................................................46 XOPENEX, HFA ............................................................................46 XTANDI .......................................................................................93 X-VIATE .......................................................................................50 XYREM ........................................................................................66 XYZAL ..........................................................................................43 Y YASMIN ......................................................................................75 YAZ .............................................................................................76 YODOXIN ....................................................................................38 Z ZACARE KIT .................................................................................54 ZADITOR OTC..............................................................................60 ZAFIRLUKAST ........................................................................ 42, 46 ZALEPLON ...................................................................................64 ZANAFLEX TABLETS ....................................................................69 ZANAMIVIR .................................................................................37 ZANTAC ......................................................................................22 ZANTAC EFFERDOSE ...................................................................22 ZARONTIN...................................................................................67 ZAROXOLYN ................................................................................27 ZEBETA .......................................................................................31 ZEGERID ......................................................................................22 ZEGERID SUSP.............................................................................22 ZELAPAR .....................................................................................70 ZEMPLAR ....................................................................................80 ZENIEVA......................................................................................50 ZENPEP .......................................................................................23 ZENZEDI 2.5, 7.5MG ...................................................................66 ZESTORETIC ................................................................................28 ZESTRIL .......................................................................................28 ZETIA ..........................................................................................33 ZETONNA ....................................................................................43 ZIAC ............................................................................................31 ZIAGEN .......................................................................................94 ZIANA .........................................................................................54 ZILEUTON ...................................................................................47 ZIOPTAN .....................................................................................58 ZIPRASIDONE MESYLATE ............................................................64 ZIPSOR ........................................................................................39 ZITHRANOL .................................................................................51 ZITHROMAX ................................................................................35 ZMAX ..........................................................................................35 239 ZOCOR ........................................................................................33 ZOFRAN ODT ..............................................................................24 ZOHYDRO ER ..............................................................................42 ZOLMITRIPTAN ...........................................................................68 ZOLMITRIPTAN NASAL SPRAY ....................................................68 ZOLOFT .......................................................................................63 ZOLPIDEM...................................................................................63 ZOLPIDEM SL ..............................................................................63 ZOLPIDEM TARTRATE ........................................................... 63, 64 ZOLPIMIST ..................................................................................64 ZOMIG NASAL SPRAY..................................................................68 ZOMIG, ZMT ...............................................................................68 ZONEGRAN .................................................................................67 ZONISAMIDE ...............................................................................67 ZORTRESS 0.25MG .....................................................................89 ZORTRESS 0.5, 0.75MG...............................................................89 ZORVOLEX ..................................................................................39 ZOTEX .........................................................................................44 ZOTEX GP....................................................................................44 ZOVIA 1/35 .................................................................................76 ZOVIA 1/50 .................................................................................76 ZOVIRAX .....................................................................................38 ZOVIRAX CREAM.........................................................................38 ZUBSOLV.....................................................................................88 ZUPLENZ .....................................................................................24 ZYBAN .........................................................................................96 ZYCLARA .....................................................................................55 ZYFLO, CR ...................................................................................47 ZYLET ..........................................................................................59 ZYLOPRIM ...................................................................................83 ZYPREXA ZYDIS ...........................................................................65 ZYRTEC OTC ................................................................................43 ZYVOX .........................................................................................36 240








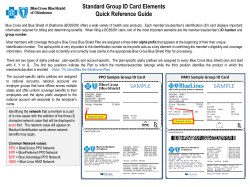

© Copyright 2026