
Correlative Morphologic and Molecular Genetic Analysis
From www.bloodjournal.org by guest on December 22, 2014. For personal use only.
Correlative Morphologic and Molecular Genetic Analysis
Demonstrates Three Distinct Categories of Posttransplantation
Lymphoproliferative Disorders
By Daniel M. Knowles, Ethel Cesarman, Amy Chadburn, Glauco Frizzera, Jonathan Chen, Eric A. Rose,
and Robert E. Michler
The posttransplantation lymphoproliferative disorders (PTLPDs) are a morphologically heterogeneous group of Epstein-Barr virus (EBVI-driven lymphoid proliferations of
varying clonal composition. Some PT-LPDs regress after a
reduction in immunosuppression, while others progress in
spite of aggressive therapy. Previously defined morphologic
categories do not correlate with clonality, and neither morphology nor clonality has reliably predicted the clinical behavior of PT-LPDs. We investigated 28 PT-LPD lesions ocalterations involving the
curring in22 patients for activating
bckl, bel-2, c-myc, and H-, K- and N-ras proto-oncogenes
and for mutations involving p53
the tumor suppressor gene.
We correlated the results of these studies
with the morphology of thelesions, their clonality based on lgheavy and light
chain gene rearrangement analysis, and the presence and
clonality of EBV infection. We found that the PT-LPDs are
divisible into three distinct categories as follows: ( 1 ) plasmacytic hyperplasia: most commonly arise in the oropharynx or lymph nodes, are nearly always polyclonal, usually
contain multiple EBV infection events or only a minor cell
population infected by a single form of EBV, and lack oncogene and tumor suppressor gene alterations; (2) polymorphic B-cell hyperplasia and polymorphic B-cell lymphoma:
may arise in lymph nodes or various extranodal sites, are
nearly always monoclonal, usually contain a single form of
EBV, and lack oncogene and tumor suppressor gene alterations; and (3) immunoblastic lymphoma or multiple myeloma: present with widelydisseminated disease, are monoclonal, contain a single form of EBV, and containalterations
of one or more oncogene or tumor suppressor genes (N-ras
gene codon 61 point mutation, p53 gene mutation, or c-myc
gene rearrangement). The PT-LPDs are divisible into three
categories exhibiting distinct morphologicand molecular
genetic characteristics. Alterations involving the N-ras and
c-myc proto-oncogenes and
the p53 tumor suppressor gene
may playan important role in the development andlor progression of the PT-LPDs.
0 7995 by The American Society of Hematology.
T
generally considered to represent a clinicallyand morphologically heterogeneous group of lymphoid proliferations and
are commonly referred to as posttransplantation lymphoproliferative disorders (PT-LPDs).”
lmmunohistochemica1 analysis for Ig light chain expressionhasshownthat
some PT-LPDs contain polyclonalB
cells, while others consist almost entirely of monoclonal B
cells.’.’’ However,Cleary et alI4.l5have demonstrated that the
majority of PT-LPDs, including those lacking Ig expression,
exhibit clonal Ig heavy and light chain gene rearrangements
and contain homogeneous episomal EBV DNA. Therefore,
many PT-LPDs appear to be
EBV-containingmonoclonal
B-cell proliferations. Separate PT-LPD lesions occurring in
the same patient, however, may be polyclonal, oligoclonal,
or monoclonal,“ and separate monoclonal lesions occurring
in the same patient frequently display different Ig
gene rearrangement patterns” and contain different clonal EBV infections,” suggestingamulticlonalprocess.
Sometimes, a
polyclonal PT-LPD may contain multiple forms of EBV.“
The results of all these studies suggestthat PT-LPDs actually
represent a spectrum of EBV-driven lymphoid proliferations
of varying clonal composition that may arise as polyclonal
expansions of EBV-infected B cells and progress to monoclonal B-cell malignant lymphomas in some individuals.
Several investigators have attempted to separate the PTLPDsinto distinctmorphologiccategories.
Frizzera” and
Frizzera et al” formulated strict morphologic criteria to distinguishbenignandmalignant
PT-LPDs, designatedpolymorphic B-cell hyperplasia
and
polymorphic B-cell
lymphoma, respectively. However, these morphologic criteria have not been adequately evaluatedas they have not been
correlated with the results of Ig gene rearrangementanalysis
and clinical outcome in a large series of PT-LPDs. Nalesnik
et al’ recognized two principal morphologically distinct categories of PT-LPDs designated polymorphic and monomor-
HE DEVELOPMENT of lymphoid neoplasms in organ
transplant
recipients
receiving
immunosuppressive
therapy has been recognized as a significant complication of
organ transplantation for 25 years.’.’ Their occurrence appears tovary according tothe organ transplanted and the type
and degreeof immunosuppressive therapy administered. The
incidence appears to be highest in heart ( I 3% to 9.8%) and
combinedheadlung (4.6% to 9.4%) transplants3-5and in
thoseindividuals who receive cyclosporine A” and monoclonal antibody OKT3.’ Lymphoid neoplasms were initially
believed to be Epstein-Barr virus (EBV)-associated malignant lymphomas because of their virtually universal
EBV
content8.’ and their frequent extranodallocation, pleomorphichistology, and associatedrapidandhighmortality.“’
However, Starzl et all’ demonstrated that they often regress
after the reduction of immunosuppressive therapy, rendering
their malignant status questionable. These lesions are now
From the Department of Pathology, The New York Hospital-Cornell Medical Center; the Department (VSurgery, Division qf Cardiothoracic Surgety, College of Physicians and Surgeons of Columbia
University; and the Department of Pathology, New York Universir).
Medical Center, New York, NY.
Submitted May 9, 1994; uccepted September
19, 1994.
Supported in part byNational Institutes of HealthGrantNo.
EY06337 (D.M.K.).
AddressreprintrequeststoDaniel
M. Knowles, MD, The New
York Hospital-Cornell Medical Center, Department
of Pathology3
525 E 68th St, New York, NY 10021.
The publication costs of this article were defrayedin part by page
chargepayment.Thisarticle
must thereforebeherebymarked
“advertisement” in accordance with 18 U.S.C. section 1734 solrly to
indicate this fact.
0 1995 by The American Socieiy of Hematology.
0006-497//95/8502-0004$3.00/0
552
Blood, Vol 85, No 2 (January 15),
1995:
pp 552-565
From www.bloodjournal.org by guest on December 22, 2014. For personal use only.
POSTTRANSPIANT LYMPHOPROLIFERATIVE DISORDERS
phic. These morphologic categories often have not been
useful in predicting the clonality of these lymphoid proliferat i o n ~ however,
,~
and neither morphology nor clonality has
proven capable of reliably predicting disease b e h a ~ i o r . ~
Locker and Nalesnik” observed, however, that those monomorphic PT-LPDs displaying a strong clonal Ig gene rearrangement band on Southern blotting and c-myc gene rearrangement exhibit disease progression. This observation
is important, as proto-oncogene and tumor suppressor gene
alterations are highly associated with the development and
progression of lymphoid malignan~y.’~
We hypothesized that
the inability of the current criteria to reliably subcategorize
PT-LPDs as benign and malignant and predict clinical behavior may be partially related to the failure to identify the
structural alterations of these genes in the PT-LPDs and to
correlate them with the morphologic features and an accurate
molecular assessment of the clonality of the PT-LPDs.
Therefore, we investigated 28 PT-LPD lesions occurring in
22 patients for activating alterations involving the bcl- 1, bcl2, c-myc,and H-, K-, and N-rus proto-oncogenes and for
mutations involving the p53 tumor suppressor gene. We correlated the results of these studies with the morphology of
the lesions, their clonality based on Ig heavy and light chain
gene rearrangement analysis, and the presence and clonality
of EBV infection. We discovered that the FT-LPDs are divisible into three categories exhibiting distinctive morphologic
and molecular genetic characteristics and identified some of
the genetic alterations that may play a role in the development andor progression of PT-LPDs.
MATERIALS AND METHODS
Patients. One lung, two kidney, and 19 heart transplant recipients who developed one or more lymphoproliferative disorders after
organ transplantation at the Columbia-Presbyterian Medical Center
(New York, NY) during the period from April 1988 to February
1993 were included in this study. Their inclusion was based on the
availability of a minimum of one fresh unfixed tissue specimen
sufficient in quantity to permit the molecular genetic and other studies described below. All relevant clinical information was collected
by reviewing the medical records of each patient. Portions of the
clinical data concerning 15 of these 22 patients have been reported
previously.2”,2’The complete clinical data of all of these patients
will be presented in detail elsewhere.
The one lung, one of the two kidneys, and all 19 cardiac transplant
recipients were maintained on an immunosuppressive regimen comprised of cyclosporine, azothioprine, and prednisone, as previously
described”; one renal transplant recipient was maintained on
cyclosporine and prednisone. In addition, 10 of the patients received
anti-CD3 Ig (Orthoclone OKT3; Ortho Pharmaceutical Corp, Raritan, NJ). The mean doses of each individual immunosuppressive
drug at the time of transplantation and at the time of PT-LPD diagnosis in this cohort of PT-LPD patients did not differ significantly
from that of the entire cardiac transplant patient population at the
Columbia-Presbyterian Medical Center during this time period.”
Rejection episodes were treated with oral steroids, intravenous steroids, OKT3, and/or antithymocyte globulin as previously described.”
Pathologic specimens. Twenty-eight PT-LPD specimens were
collected from the 22 patients during the course of clinical evaluation
using standard diagnostic procedures: nine from lymph nodes, six
from lungs. five from tonsils and/or adenoids, one from jejunum,
553
one from colon, one from liver, one from brain, one from breast,
one from skin, one from bone marrow, and one from soft tissues of
the thigh. Ofthe 28 specimens, 27 were collected under sterile
conditions, placed in tissue culture media RPM1 1640 or physiologic
saline, and immediately delivered to the Hematopathology Laboratory (Columbia-Presbyterian Medical Center). Representative portions of these 27 specimens were snap-frozen in a cryopreservative
solution (OCT compound Miles, Eckhart, IN) and stored at -70°C.
The remaining specimen, a sample of aspirated bone marrow, was
collected in a heparinized syringe. A viable mononuclear cell suspension was prepared from this sample by Ficoll-Hypaque (Pharmacia,
Piscataway, NJ) density gradient centrifugation. The cells were cryopreserved in dimethylsulfoxide and fetal calf serum in vapor-phase
liquid nitrogen at-170°C. Portions of each of the 28 specimens
were routinely fixed in formalin, B5, and/or Bouin’s and embedded
in paraffin, from which hematoxylin- and eosin-stained sections were
prepared.
DNA extraction and Southern blot hybridization analysis. Genomic DNA was extracted from cryopreserved tissue blocks and mononuclear cell suspensions using a salting-out procedure.” Aliquots (5
pg) of genomic DNA were digested with the appropriate restriction
endonucleases according to the manufacturer’s instructions (Boehringer-Mannheim, Indianapolis, IN), electrophoresed in 0.8% agarose gels, denatured with alkali, neutralized, and transferred to nitrocellulose filters according to the method of So~thern.’~
The filters
were hybridized in 50% formamide/3 X standard sodium citrate
(SSC) at 37°C to probes that had been ”P-labeled by the random
primer extension method.” The filters were washed in 0.2 X SSC/
0.5% sodium dodecyl sulfate (SDS) at 60°C for 2 hours and then
autoradiographed at -70°C for 16 to 48 hours, as previously de~cribed.’~
DNA probes. The Ig heavy chain, kappa light chain, and lambda
light chain genes were investigated by hybridization of EcoRI- and
HindIII-digested DNAs toan Ig heavy chain gene joining region
(JH) probe,26BamHI-digested DNAs to a kappa light chain joining
region (J,) probe:’ and EcoRI-digested DNAs to a lambda light
chain constant region (C,) probe?6 The T-cell receptor beta chain
(To) gene was investigated by hybridization of EcoRI- and BamHIdigested DNAs to a DNA probe that hybridizes to the constant
region of the To
The organization of the c-myc gene was
analyzed by hybridization of EcoRI- and HindIII-digested DNAs to
the human c-myc probe MC413RC. representative of the third exon
of the c-myc gene.” The presence of bcl-l gene rearrangements was
analyzed by hybridization of Bcl I-digested DNAs to a 2.3-kb Sst 1
fragment from the bcl-l IOCUS,~~
as previously de~cribed.~’
The presence of bcl-2 gene rearrangements was analyzed by hybridization
of HindIII-digested DNAs to the pFL-l probe, representing a portion
and to
of chromosome 18 at the major bcl-2 breakpoint regi~n,~’
the pFL-2 probe, representing a portion of chromosome 18 at a
minor bcl-2 breakpoint region.” The presence of EBV genome and
the clonality of EBV infection was investigated by hybridization of
BamHI-digested DNAs to a probe specific for the EBV genomic
termini (5.2-kb BamHI-EcoRI fragment isolated from the fused
BarnHI-terminal fragment NJ-het).34,35
Oligonucleotide primers. Allofthe
oligonucleotides used for
polymerase chain reaction (PCR) amplification were synthesized
by the solid-phase triester method. Pairs of primers derived from
published sequences were used to analyze the c-mycgene first exonand
first intron boundary region,36p53 gene exons 5 through 9,37.38
the H-, K-, and N-RAS gene codons 12, 13, and 61.’9
Single-strand conformation polymorphism (SSCP) analysis.
SSCP analysis was accomplished according to an adapted version”
of a previously reported method.40 Briefly, PCRs were performed
with 100 ng of genomic DNA, 10 pmol of each primer, 2.5 pmoV
From www.bloodjournal.org by guest on December 22, 2014. For personal use only.
554
KNOWLES ET AL
Fig 1. The histopathology of the PT-LPDs. (A, Bl Plasmacytic hyperplasia [original magnification (OM): x 40, x 630, respectively]. [C)
Polymorphic B-cell hyperplasia (OM: x 630). (D, E, and F) Polymorphic B-cell lymphoma (OM: x 630, x 630, x 40, respectively). (G, H)
lmmunoblastic lymphoma (OM: x 630, x 630, respectively). (1) Multiple myeloma (OM: x 630). Plasmacytic hyperplasia of a lymph node is
characterized by diffuse expansion, with sparing of the sinuses (A), by a predominant population of plasmacytoid lymphocytes associated
with plasma cells, and by sparse immunoblasts (B). Polymorphic B-cell hyperplasia is composed of a mixture of plasmacytoid lymphocytes
and abundant plasma cells and immunoblasts without cytologic atypia in which
necrosis is limitedto single cells or small foci(C). Polymorphic
B-cell lymphoma iscomposed of a mixture of lymphoidcells lacking prominentplasmacytic differentiation and displaying significant cytologic
atypia (Dl andlarge, atypical immunoblasts (El and containing large confluentareas of necrosis (F).
L dNTPs (for p53 and c-my primers) or 50 pmol/L dNTPs (for
RAS primers), I p,Ci of [&-"P]dCTP [New England Nuclear (NEN).
Boston, MA; specific activity. 3,000 Cilmmol], 10 m m o l n Tris (pH
8.8). 50 mmollL KCI, 1 mn~ol/LMgCI2 (for p53, N-RAS 12-13. NRAS 61, K-RAS12-13.and
H-RAS 12-13), or 1.5 mmol/L MgC12
(K-RAS 61 and c-mnyc). 0.01% gelatin. 0.5 U Taq polymerase. in a
final volume of 10 pL. Thirty cycles of denaturation (94°C). annealing (63°C for p53 exons 5. 6, and 9; 62°C for p53 exon 7; 58°C for
p53 exon 8: 58°C for all RAS amplifications: and 63°C for c-rnyc.),
and extension (72°C) were performed on an automaled heat-block
(DNA Thermal-Cycler; Perkin-Elmer Cetus, Norwalk, CT). The reaction mixture (2 pL) was diluted 1:25 in 0.1% SDS. 10 mmoln
From www.bloodjournal.org by guest on December 22, 2014. For personal use only.
POSTRANSPLANT LYMPHOPROLIFERATIVE DISORDERS
555
Fig 1. (Cont'd) lmmunoblastic lymphomas are composed of a monomorphic collection of cytologically malignant cells. Some may contain large, bizarre, and pleomorphic nuclei (G), while others contain
plasmacytoidnuclei (H).
Multiple myeloma is composed of
a monomorphic population of cytologically atypical plasma cells (I).
EDTA. and further mixed I :I with a sequencing stop solution (95%
formamide, 20 mmoUL EDTA. 0.058 bromophenol blue. and 0.05%
xylene cyanol). Samples were heated at 85°C for 5 minutes, chilled
on ice, and immediately loaded onto a 6% acrylamide-Tris-borate
EDTA (TBE) gel containing 10% glycerol. The gels were run ar 4
to 8 W for 14 to 16 hours at room temperature. They werethen
fixed in 10% acetic acidand air-dried, and autoradiography was
performed at -70°C with an intensifying screen for 6 to 24 hours.
Cloning und sequencing of PCR products. PCR products were
cloned in thepCR 1000 vector using theTA cloning system (Invitrogen Corp. San Diego, CA) following the manufacturer's instructions. The DNA sequencing was performed directly from a smallscale plasmidpreparation" after determining the presence of an
insert. The Sequenase version 2.0 system (US Biochemical, Cleveland. OH) was used, and a modification ofthe procedure in the
manufacturer's instructions was performed as previously described.''
RESULTS
Histopatllology. Drs Knowles. Chadbum. and Frizzera
reviewed all of the histologic sections prepared from each
specimen and classified each PT-LPD without knowledge of
the clinical characteristics of the patients or the results of any
of the additional studies performed here. Five morphologic
categories became apparent from this review: ( 1 ) plasmacytic hyperplasia, ( 2 ) polymorphic B-cell hyperplasia, (3)
polymorphic B-celllymphoma.
(4) immunoblastic lymphoma, and ( 5 ) multiple myeloma (Fig l ) . We designated
the term "plasmacytic hyperplasia" to indicate those lesions
exhibiting retention of the underlying architecture of the
lymph node or other tissue and expansion of the interfollicular area or diffuse infiltration of other tissue by a predominant
population of plasmacytoid lymphocytes, associated with
plasma cells and sparse immunoblasts. Germinal centers
were hyperplastic, involuted, or were absent in these cases.
The histopathologic criteria for inclusion into categories 2
and 3 werethosepreviously
described by Frizzera" and
Frizzera et al." Briefly. lesions producing extensive disturbance of the organ architecture and composed of a mixture
of lymphoid cells with prominent plasmacytoid differentiation and abundant immunoblasts without cytologic atypia,
in which necrosis was limited to single cells or small foci,
were classified as polymorphic B-cell hyperplasia. Lesions
composed of a mixture of lymphoid cells lacking prominent
plasmacytoid differentiation and displaying significant cytologic atypia, atypical immunoblasts, and containing large
confluent areas of coagulative necrosis wereclassified as
polymorphic B-cell lymphoma. Lesions composed of a monomorphic collection of cytologically malignant cells were
classified as immunoblastic lymphoma. Lesions composed
of a monomorphicpopulation
of cytologically atypical
plasma cells were classified as multiple myeloma.
Ten specimens collected from eight patients were classified as plasmacytic hyperplasia. These includedfive from
tonsils and/or adenoids. four from lymph nodes, and one
from lung (Table I ). Five specimens obtained from five pa-
From www.bloodjournal.org by guest on December 22, 2014. For personal use only.
KNOWLES ET AL
556
Table 1. Results of Molecular Genetic Analysis of 28 PT-LPDs Occurring in 22 Patients
Antigen Receptor Genes
Oncogenes and Tumor Suppressor Genes
Patient/
Specimen No.
Histopathology
Specimen
22
4A
8A
88
8C
18
16
1
10
11A
11B
17
2
15
21
5
6
7
12
13
20
9A
9B
3
14A
148
48
19
PH
PH
PH
PH
PH
PH
PH
PH
PH
PH
PBCH
PBCH
PBCH
PBCH
PBCH
PBCL
PBCL
PBCL
PBCL
PBCL
PBCL
PBCL
PBCL
PIB
IB-P
PIB
MM
MM
Adenoids
LN
Tonsil
Tonsil
Adenoids
LN
Lung
Adenoids
LN
LN
Colon
LN
Lung
Lung
LN
LN
Lung
Lung
Jejunum
Lung
Liver
Brain
Breast
LN
LN
Skin
Thigh
BM
JH
JH
EcoRl Hindlll
G
G
G
G
G
G
G
RI*
G
G
G
G
G
G
G
G
G
R1'
G
G
RI
R1
RI*
G
RI
R2
RI
R1
RI
R1
RI
R1*
R2
R1
R2 R1' R2
R2
R2
R2
R2
R1R1 R1
R2 R1 R2
R1t
Rlt
R1R1 R1
R1
R1
ND NDND
R2
R1
R2
R2
J,
C,
To
G
G
G
G
G
G
G
R2*
G
G
R1*
G
R1*
G
G
R1*
R2
G
G
G
G
G
G
G
G
G
G
G
G
G
R1
G
R1
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
R2
R1
Rlt
D
G
D
R1
R1
G
G
G
G
G
G
R1
ND
ND
G
G
R2
G
E BV
bcl-l
G
NEG
Smear
G
1band*
G
l band* + smear
G
1 band*
G
Smear
G
1 band*
G
G
1 band
Smear
G
G
NEG
G
1band
NEG
G
G
2 bands (1 + 1')
NEG
G
1band
G
1band
G
1band
G
1 band
G
1 band
G
1 band
G
G
3 bands (1 2*)
3 bands (2 l * )
G
G
1 bandt
G
1 band
G
1 band
ND
ND
ND
ND
1 bandt
G
1 band
G
+
+
bcl-2
c-myc
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
R
G
G
G
G
W
W
W
W
W
W
W
W
W
W
W
W
W
W
W
W
W
W
W
W
W
W
W
W
W
H-RAS
T
T
T
T
T
T
T
T
T
T
T
T
T
T
T
T
T
T
T
T
T
T
T
T
T
WT
W
T
W
T
K-RAS
W T
W T
WT
WT
N-RAS
W T
W T
WT
WT
WT WT
W T W T
WT WT
WT WT
W WT
WTW
WT WT
WT WT
WT
W T W T
WT WT
W T W T
WT WT
WT WT
WT WT
WT
WT
WT WT
WT
WT
WT WT
WT WT
WT "C61
W T W T
WT "C61
WT
"C61
P53
WT
WT
WT
WT
WT
WT
WT
WT
WT
WT
WT
WT
WT
WT
WT
WT
WT
WT
WT
WT
WT
WT
WT
M-Ex8
WT
M-Ex7
WT
WT
Abbreviations: PH, plasmacytic hyperplasia; PBCH, polymorphic B-cell hyperplasia; PBCL, polymorphic B-cell lymphoma; PIB, pleomorphic
immunoblastic lymphoma; IB-P, plasmacytoid immunoblastic lymphoma; MM, multiple myeloma; LN, lymph node; BM, bone marrow; G,
germline; R, rearrangement; ND, not done; D, deletion; NEG, negative; W, wild type; M-C, mutation, codon; M-Ex, mutation, exon.
* Faint band.
t Different pattern in same patient.
tients were classified as polymorphic B-cell hyperplasia, and
eight specimens collected from seven patients were classified
as polymorphic B-cell lymphoma. The anatomic sites involvedby these two categories of PT-LPDs were diverse
but overlapped: five from lungs, three from lymph nodes,
one from jejunum, one from colon, one from liver, one from
brain, and one from breast. Three PT-LPDs occurring in
lymph nodes and skin in two patients (cases 3 and 14) were
classified as immunoblastic lymphoma. The immunoblastic
lymphoma in patient 3 and one of the two in patient 14
were characterized as pleomorphic because of large, bizarre
nuclei. The other immunoblastic lymphoma in patient 14
had distinctly plasmacytoid features. The lesions occurring
in the soft tissues of the thigh of patient 4 and the bone
marrow of patient 19 were classified as multiple myeloma.
Patient 4 had plasmacytic hyperplasia of a lymph node 14
months before presenting with disseminated multiple myeloma. Patient 11 had plasmacytic hyperplasia of a pericolonic lymph node synchronous with polymorphic B-cell hyperplasia of the colon.
Antigen receptor gene rearrangements. Of the 10 speci-
mens classified morphologically as plasmacytic hyperplasia,
9 lacked clonal rearrangements of the Ig heavy chain and
kappa and lambda light chain genes on Southern blot hybridization (Table 1 ; Fig 2 ) . The tenth specimen (patient I , adenoids) displayed a solitary faint Ig heavy chain gene rearrangement bandand two faint kappa light chain gene
rearrangement bands, consistent with the presence of a small
clonal B-cell population. The 17 remaining specimens studied here, which included all the PT-LPDs classified as polymorphic B-cell hyperplasia, polymorphic B-cell lymphoma,
immunoblastic lymphoma, and multiple myeloma, exhibited
clonal Ig heavy chain gene rearrangements detectable as one
or two new, non-germline hybridization bands on Southern
blotting. Of these 17 PT-LPDs, 14 also displayed clonal
kappa and/or lambda light chain gene rearrangements, and
2 of these 14 PT-LPDs exhibited kappa light chain deletion
in conjunction with lambda light chain rearrangement. The
hybridization signals were clear and of variable but generally
strong intensity, indicating the presence of a significant
clonal B-cell population in each of these pathologic specimens. The one exception was specimen 17, which displayed
ERATIVE
From www.bloodjournal.org by guest on December 22, 2014. For personal use only.
POSTTRANSPLANT
DISORDERS
557
C 1 2 3 5 6 7 8 8 8 99 10 11 11121314 1516 44181719202122
A B CBAAB
A
A B
#*&******###****#*#****@*##@#*@***#
A
5
4
v
.I?,
L
B -
?
b
U
1-
-17kb
PROBE :JH
ENZYME : Eco RI
- 23kb
- 9.4kb
6
PROBE : EBV-TR
ENZYME : Barn HI
Fig 2. Southern blot hybridizationanalysis for lg heavy chain gene rearrangements (A) and for EBV termini heterogeneity (B). DNAs were
digested with EcoRl and hybridized t o an lg heavy chain joining region(JH)probe andwith 8amHl and hybridizedt o a DNA probe specific for
the fused termini of the EBV genome. Numbers 1 through 22 above each lane correspond to the case number, and the letters under these
numbers denote different specimens from the same patient. C indicates the germline or negative control (HL60 cell line). The histologic
classification of each case is indicatedabove each lane as follows: #, plasmacytic hyperplasia; *, polymorphic B-cell hyperplasia; **, polymorphic
B-cell lymphoma; &, pleomorphic immunoblastic lymphoma; and @, plasmacytoid immunoblastic lymphomaor multiple myeloma. (A) All of
the cases show the germline band 17
atkb (dash), and additional clonal rearrangement bands are marked byarrowheads. Of the 10 plasmacytic
hyperplasia W), 9 lacked clonal lg gene rearrangements, and the tenth(case 1I exhibited a solitary faintclonal lg heavy chain gene rearrangement
band. All of the polymorphicB-cell hyperplasias (*),polymorphic B-cell lymphomas (**l, immunoblastic lymphomas(&l, and multiple myelomas
(0)exhibited one or two, generally strong, lg heavy chain gene rearrangement bands, indicating the presence of a significant clonal B-cell
population in each of these specimens. (B) The location of the 23-kb and 9.4-kb size markers is shown(dashes). Of 10 plasmacytic hyperplasias
W), 8 exhibited hybridization smears andlor a solitary, usually faint, band indicative of multiple EBV infection events andlor a minor cell
population infected by asingle form of EBV. Three of five polymorphic B-cell hyperplasias I*) and all 12 polymorphic B-cell lymphomas p ) ,
immunoblastic lymphomas(&l, and multiple myelomas
(@I exhibited solitary strong
bands, sometimes accompanied by one or more additional
faint bands, indicative of clonal EBV infection, sometimes in conjunction with a second or third EBV infection event.
only a solitary faint Ig heavy chain rearrangement band in
the absence of light chain gene rearrangements. Interestingly.
two separate PT-LPDs (brain and breast) classified as polymorphic B-cell lymphoma obtained frompatient 9 only 6
days apart displayed different Ig heavy and light chain gene
rearrangement patterns, suggesting distinct clonal derivations. None of the 27 PT-LPDs studied herecontained clonal
T, gene rearrangements (data not shown). These results indicate that the large majority of plasmacytic hyperplasias are
polyclonal lymphoid proliferations or contain onlyminor
clonal B-cell populations, while all other PT-LPDs are
monoclonal B-cell proliferations.
ERV. The presence andthe clonality ofEBVinfection
was determined by analysis of the structure of thefused
termini of the EBV genome.I5-" Because EBV genomic termini contain a variable number of tandem repeated sequences. the molecular configuration ofthefusedtermini
serves as a distinct marker for eachEBVinfection event.
Multiple identical viral episomes with the same fused termini
are maintained in the progeny of the infected cell, providing
a means of analyzing clonality in the EBV-infected specimen." Differences in the configuration of EBV-fused termini
are detectable as differently sized fragments on Southern
blots. The detection of a hybridization smear, two bands. or
a single band indicates infection by multipleforms,two
distinct forms. or a single form of EBV. r e ~ p e c t i v e l y . ' ~ ~ ~ ~
Eight of IO PT-LPDs classified a s plasmacytic hyperplasia. three of five classified as polymorphic B-cell hyperplasia, and all 12 classified as polymorphic B-cell lymphoma,
immunoblastic lymphoma, andmultiplemyeloma
studied
here contained evidence ofEBV infection (Table I ; Fig
2 ) . The four EBV-negative lesions were rehybridized twice
more,butEBVwas
still not demonstrable in these cases.
The clonal patterns ofEBV infection were highly variable
among the eight EBV-containing plasmacytic hyperplasias.
The patternswere as follows: hybridization smear alone,
three: hybridization smear accompanied by a solitary faint
band, one; solitary faint band, three: and a solitary intense
band. one. The faint bands detected in the three PT-LPD
specimens obtained simultaneously from patient 8 (right tonsil, left tonsil, and adenoids) were identical, suggesting the
presence of the same single form of EBV in all three lesions.
In contrast withthe plasmacytic hyperplasias, none of the
PT-LPDs belonging to the other categories that were studied
here displayed hybridization smears. The clonal pattern of
EBV infection in these 15 PT-LPDs was as follows: solitary
intense band. 12; one faint and one intense band, one; two
faintand one intense bands, one:and one faintandtwo
From www.bloodjournal.org by guest on December 22, 2014. For personal use only.
KNOWLES ET AL
558
intense bands, one. The two PT-LPDs occurring in patient
9 that displayed different clonal Ig gene rearrangement patterns exhibited different EBV band patterns, suggesting that
these two clonally distinct PT-LPDs were infected by different formsof EBV. These results indicate that plasmacytic
the
hyperplasias, which are polyclonal, represent a spectrum of
largely EBV-containinglymphoid proliferations,ranging
from those containingmultiple distinct EBV infections to
thosecontaining only a single form of EBV. In contrast,
virtually all lesions belonging to the other PT-LPD categories, which are monoclonal B-cellproliferations, are infected
by a single form of EBV or occasionally contain evidence
of a second or third infection event.
Proto-oncogenes and tumorsuppressor genes. Allthe
PT-LPDs except one wereinvestigated for bcl-l, bcl-2, and
c-myc gene rearrangements by Southern blot hybridization.
A c-myc gene rearrangement was detected in the plasmacytoid immunoblastic lymphoma occurring patient
in
14 (specimen 14A; data not shown). All
the remaining PT-LPDs lacking c-myc gene rearrangements were analyzed by SSCP for
smalldeletions/insertions or pointmutationsintheregion
surroundingthe first exon-first intron of the c-myc gene.
In addition, all the PT-LPDs were analyzed by SSCP for
mutations occurring within codons12and
13 of the H-,
K-, and N-rus genes, codon 61 of the K- and N-rus genes,
and exons 5 through 9 of the p53 gene-the regions known
tocontainthe
majorityof the mutations involvingthese
This technique allows the detection of single base
pair mutations as the wild type and mutantradiolabeled PCR
products display different migration patterns because of the
formation of alternative secondary structures after denaturation and subsequent electrophoresisin a polyacrylamide gel
under nondenaturing conditions. This method waspreviously
shown to be highly specific and sensitive to the l % level.”
In those cases displaying an abnormal migration pattern suggesting mutations, the DNA fragmentsof altered electrophoretic mobility were reamplified in separate
a
reaction, cloned,
andsequencedto
verifythe presence of amutation and
delineate its nature. The three PT-LPDs classified as plasmacytoidimmunoblasticlymphomaor
multiple myeloma
exhibited N-rus gene mutations, and the two PT-LPDsclassified aspleomorphicimmunoblasticlymphoma
exhibited
p53 tumor suppressor gene mutations (Table 1). The plasmacytoid immunoblastic lymphoma occurring in patient 14
(specimen 14A) and the two multiple myelomas (specimens
4B and 19) contained identicalpointmutations:aC
to A
transversion in the first nucleotide of codon 61 leading to a
change in the encoded amino acid from glutamine to lysine
(Table 1, Fig 3). The pleomorphic immunoblastic lymphoma
occurring in patient 3 contained an insertion of a C nucleotide in codon 301 of p53 gene exon 8 leading to a frameshift
(data notshown). The pleomorphic immunoblasticlymphoma occurring in patient 14 (specimen 14B) contained a
missense mutation in p53 gene exon7: a C to A transversion
in the second nucleotide of codon 248 leading to a change
in the encoded amino acid from arginine to leucine (Fig 4).
The presence of different genetic lesions in the two separate
PT-LPDs occurring in patient 14 suggest that these lesions
not
are of distinct clonal derivation. However,wecould
prove this unequivocally because of insufficient DNA from
specimen 14B to perform Ig gene rearrangement
analysis.
None of the 24 PT-LPDsclassified as plasmacytic hyperplasia, polymorphic B-cell hyperplasia, or polymorphic B-cell
lymphoma contained evidenceof mutations involving the cmyc, the N-rus, or the p53 genes. None of thePT-LPDs
studied here exhibited bcl-1 or bcl-2 gene rearrangements
or H- or K-rus gene
mutations. The results of thesemolecular
genetic studies are summarized in Table 2.
DISCUSSION
The results of the studies described here confirm that the
PT-LPDs represent a heterogeneous group of EBV-driven
lymphoid proliferations of varying clonal composition. However, these results extend all prior observations by identifying some of the molecular genetic events that may play
an important role in the development and/or progression of
thePT-LPDs.Bydemonstrating
thatthePT-LPDsare
broadly divisible into three categories, each exhibiting distinctive morphologic and molecular genetic characteristics,
these findings also provide an explanation for some of the
previously reported incongruities between the morphology,
clonality, and clinical behavior of PT-LPDs.
In summary, we foundthat those PT-LPDs that we classified as plasmacytic hyperplasia most commonly arise in the
oropharynx or lymph nodes, are nearly, always polyclonal,
usually contain evidence of multiple EBV infection events
and/or only aminor cell populationinfected by a single
form of EBV, and lack oncogene and tumor suppressor gene
alterations. Those PT-LPDs that we classified as polymorphicB-cellhyperplasia
orpolymorphic B-cell lymphoma
according to earliermorphologic criteria”.13 exhibit overlapping molecular genetic characteristics that unite them into
one category. These PT-LPDs may arise in lymph nodes or
in a variety of extranodal sites, especially the lungs and the
gastrointestinal tract, are nearly always monoclonal, usually
contain evidence of infection by a single form of EBV, and
lack oncogene and tumor suppressor gene alterations. Those
PT-LPDs that we classified as immunoblastic lymphoma or
multiple myeloma usually present with widely disseminated
disease, are monoclonal, contain evidence of infection by a
single form of EBV, and contain alterations of one or more
oncogene or tumor suppressor genes.
The PT-LPDs that we designated plasmacytic hyperplasia
appear to be morphologically identical to the diffusereactive
plasma cell hyperplasia of lymph nodes described by Nalesnik et al’ in some patients who either had a concurrent or
subsequently developed a polymorphic or monomorphic PTLPD.In bothseries,theselesions
were characterized by
retention of the underlying lymph node architecture, a diffuse, benign-appearing plasmacytoid cellular infiltrateexhibiting minimal polymorphism, and an invariably polyclonal
composition, exceptin one of our cases wherea small clonal
B-cell population was identified. Nalesnik et ai3 were uncertain of the relationship between these lesions and their polymorphic and monomorphic PT-LPDs and
proposed that their
presence “should suggest the possibility of early PT-LPD
From www.bloodjournal.org by guest on December 22, 2014. For personal use only.
559
POSTTRANSPLANTLYMPHOPROLIFERATIVEDISORDERS
I
B
G A T C G A T C G A T C G A T C
I.
/:
CA
A
A
CODON
61
Gln
G
I.
NORMAL
CASE46
(")
CASE 14A
(I B-P)
CASE 19
(")
Fig 3. Analysis of N-rascodon61 mutations byPCR-SSCP (A) andsequencing (B). (A) Representative samples corresponding t o radiolabeled,
PCR-amplifiedfragments from exon
2 of the N-rasgene, after denaturation and electrophoresis on a6% acrylamide gel containing 10% glycerol,
specimens from the
are shown. Lanes 1 through 19 indicate thecase number analyzed, and theletters under these numbers denote different
same patient. ND, amplified DNA that was notdenatured before electrophoresis; -,the
same PCR reaction in the absence of DNA; C, wildtype control, for which DNA extracted from areactive lymph node was used. The histologic classification of each case is indicated above each
lane as follows: #, plasmacytic hyperplasia; *, polymorphic B-cell hyperplasia; *", polymorphic B-cell lymphoma; &, pleomorphic immunoblastic
lymphoma; @, plasmacytoid immunoblastic lymphoma
or multiple myeloma. Several identical bands were seen in allof the samples containing
the wild type sequence. Specimens 48, 14A. and 19 showed a different pattern (arrowheads). These cases were interpreted as positive for
mutations and were further studiedby generic sequence analysis (B). (B) Each mutation is matchedt o a control wild typeDNA. Arrowheads
point t o the mutated bases. The nucleotide change in cases 46, 14A, and 19 is identicaland consists of a C t o A transversion in codon 61 of
the N-rasgene leading t o an amino acid substitution from glutaminet o lysine.
or the presence of PT-LPD elsewhere and prompt a search
for EBV infection." However, we believe that these lesions
are part of the PT-LPD spectrum as they occur as clinically
detectable lymphoid proliferations posttransplantation, usually contain EBV, are associated with other morphologic
forms of PT-LPD in the same patient, and regress after a
reduction in immunosuppression. Indeed. it is highly likely
that these lesions represent the earliest recognizable
lymphoid proliferations that occur posttransplantation, as
they often appear to contain occult B-cell clones, based on
the analysis of EBV-fused termini, that are undetectable by
Ig gene rearrangement analysis. Cleary et all5 already SUEgested that analysis of the EBV-fused terminimay be a more
sensitive approach thanIg gene rearrangement analysis to
detect occult B-cell clones. The term plasmacytic hyperplasia seems appropriate for these lesions based on their benign
morphology, molecular characteristics, and clinical behavior.
Unlike Nalesnik et al,' we also recognized these lesions
From www.bloodjournal.org by guest on December 22, 2014. For personal use only.
KNOWLES ET AL
560
ND
- 1314814A 15
16 17 18 19 20 C
**ai@ * # * #@**
I
W*.
"
"
A
CODON
248
t
Leu
Fig 4. Analysis of p53 gene exon 7 mutations by PCR-SSCP (A)
and sequencing (B). (A) Representative samples corresponding t o
radiolabeled, PCR-amplified fragments fromexon 7 of the p53 gene,
after denaturation and electrophoresis on a 6% acrylamide gel containing 10Y0 glycerol, are shown. Lanes 13, 148, 14A. 15, 16, 17, 18,
19, and 20 correspond to the case number analyzed. ND, amplified
DNA that was not denatured before electrophoresis; -, the same
PCR reaction in the absence of DNA; C, positive control, harboring a
known mutation within the regiontested. The histologic classification of each case is indicated above each lane as follows: #, plasmacytic hyperplasia; *, polymorphic B-cell hyperplasia; **, polymorphic B-cell lymphoma; &, pleomorphic immunoblasticlymphoma; @,
plasmacytoid immunoblastic lymphoma or multiple myeloma. Several identical bands were seen in all of the samples in the cases
containing thewild typesequence. Case 14B showed a different pattern (arrowheads). Thus, this case was interpreted as positive for
mutations and was further studiedgeneric
by
sequence analysis (B).
(B) The mutation is matchedt o a control wild typeDNA. The arrowhead points to the mutated
base, which consists of a C t o A transversion in codon 248 of p53 gene exon 7 leading t o an amino acid substitution from argininet o leucine.
in tonsils and adenoids. In fact, in our experience, all PTLPDs occurring in the tonsils and adenoids are plasmacytic
hyperplasias. It is noteworthy in this regard that of the 10
PT-LPDs occurring in this region in the series reported by
Nalesnik et al,' all were described as polymorphic. only one
was monoclonal by virtue of a faint Ig gene rearrangement
band, and nineregressed or resolved. Therefore, some, many,
or even all of their oropharnygeal PT-LPDs may correspond
to our category of plasmacytic hyperplasia. This would explain why a large proportionof the PT-LPDs that they classified as polymorphic werepolyclonalandpartiallyexplain
why a polymorphic appearance did not correlate more consistently with monoclonality in their series, as it did in ours.
The latter discrepancy can also bepartially explained by
the factthatNalesnik et a13 concluded thatsixadditional
polymorphic PT-LPDs were polyclonal based on immunophenotypic analysis alone, which is notoriously less sensitive
than antigen receptor gene rearrangement analysis.
The results of the studies described here support the contention of Frizzera" and Frizzera et all' that the majority of
PT-LPDs possess a distinctive. albeit highly variable, polymorphic lymphoid cellular composition that distinguishes
them from thevarious forms of malignant lymphoma.including immunoblastic lymphoma, that are observed in immunocompetent hosts. However, our results do not supportthe
separation of polymorphic PT-LPDs into benign and malignant categories according to the degree of plasmacytic differentiation, the presence or absence of cytologic atypia. and
thetypeand degree of necrosis as proposed by Frizzera"
and Frizzera et al.'; Instead. our results demonstrate that
both polymorphic B-cell hyperplasias andpolymorphicBcell lymphomas are monoclonal B-cell proliferations that are
homogeneous with respect to the presence and clonality of
EBV infection and the absence of oncogene and tumor suppressor gene alterations. and thusappear to represent a single
category of PT-LPDs.
Cleary et all4 proposed that the PT-LPDs are malignant
lymphomas ab initio because of their monoclonality and, as
such, should be treated with antineoplastic therapy. Nevertheless, these monoclonal PT-LPDs often regress after a reduction in immunosuppression. Furthermore, while it is true
thatnearly all malignant lymphomas are monoclonal, the
converse, namely that all monoclonal proliferations are malignant lymphomas, maynotbe
true. For example, clonal
B-cell populations have been documented in human immunodeficiency virus (HIV)-associated hyperplastic lymphadenopathy:
systemic Castleman's disease,J4 and extranodal
pseudolymphomas,4' and clonal T-cell populations have
been documented in a variety of cutaneous lymphoproliferative disorders that may regress ~pontaneously.~~."~
Recently.
Kame1 et aI4' described EBV-associated lymphoid proliferations morphologically resembling malignant lymphomas that
arise during methotrexate therapy for rheumatoid arthritis or
dermatomyositis and apparently regress after cessation of
methotrexate. Finally, our studies demonstrate thatthe
monoclonal polymorphic PT-LPDs invariably lack structural
alterations of the proto-oncogenes andtumor suppressor
genes that are commonly associated with lymphoid malignancy. For all of these reasons, the benign or malignant
nature of the polymorphic PT-LPDs has been controversial
in the past and will probably remain so in the near future.
Therefore, we prefer tousethenoncommittaldesignation
"polymorphic" PT-LPD for this category of lymphoid proliferations until the controversy is resolved.
Nalesnik et a13 have proposed that the subset of PT-LPDs
that they term monomorphic are morphologically indistin-
From www.bloodjournal.org by guest on December 22, 2014. For personal use only.
POSTTRANSPLANT LYMPHOPROLIFERATIVE DISORDERS
56 1
Table 2. Summary of Results of Molecular Genetic Analysis of 28 PT-LPh Occurring in 22 Patients
SSCP and Sequence Analysis
Southern Blot Analysis
Histopathology
PH
No. of
Specimens
Clonal Ig Gene
Rearrangement
10
1 (faint)
PBCH
5
5
PBCL
PI6
IB-P, MM
8
2
8
l*
3
3
EBV
Negative, 2
Smear, 3
Clonal, 5
Negative, 2
Clonal, 3
Clonal, 8
Clonal, l *
Clonal, 3
c-myc Gene
Rearrangement
N-Ras
Mutation
P53
Mutation
0
0
0
0
0
0
0
0
O*
0
0
2
1
3
0
Abbreviations: PH, plasmacytic hyperplasia; PBCH, polymorphic B-cell hyperplasia; PBCL, polymorphic B-cell lymphoma; PIE, pleomorphic
immunoblastic lymphoma; IB-P, plasmacytoid immunoblastic lymphoma; MM, multiple myeloma.
* Only one of the two specimens was evaluated because of insufficient fresh tissue in one case.
guishable from small or large noncleaved cell (Burkitt’s or
centroblastic) lymphomas occumng in immunocompetent
hosts. Hanto et ala and Frizzera” have argued that PT-LPDs
exhibiting such morphology are uncommon, but that a small
number of PT-LPDs resemble immunoblastic lymphoma
morphologically. We did not identify any PT-LPDs in this
series exhibiting the morphology of small or large noncleaved cell lymphoma, but we did identify three PT-LPDs
exhibiting the morphology of immunoblastic lymphoma. We
also identified two PT-LPDs composed of a monomorphic
collection of atypical plasma cells. Further evaluation
showed that both patients had the classical clinical triad of
multiple myeloma. These five PT-LPDs were distinguished
rather easily from the polymorphic PT-LPDs by their relatively monomorphic and frankly malignant cytopathology.
Although the term monomorphic could be applied to these
five PT-LPDs, we believe that it is better to avoid ambiguous
terminology in refemng to these obvious lymphoid malignancies, and it is more precise to use the standard and accepted nomenclature used for identical lymphoid malignancies occumng in immunocompetent hosts. Therefore, we
prefer to designate them as PT-LPD, malignant lymphoma,
immunoblastic and PT-LPD, multiple myeloma, respectively.
It is now generally believed that structural alterations involving several well-described proto-oncogenes and tumor
suppressor genes play a significant role in the development
and/or progression of human lymphoid neoplasia.” We were
able to identify one or more such genetic lesions in each
of thefive PT-LPDs that we classified as immunoblastic
lymphoma or multiple myeloma, presumably confirming
their truly malignant status. In contrast, we did not identify
comparable genetic lesions in any of the other PT-LPDs
studied here, regardless of their clonal composition or the
nature of their EBV content. Thus, the presence of one or
more proto-oncogene or tumor suppressor gene alterations
was the single feature that correlated with clearly malignant
morphology in this series.
It is not entirely surprising that we detected p53 gene
mutations in the two pleomorphic immunoblastic lymphomas (specimens 3 and 14B) and N-ras gene mutations in
the two multiple myelomas (specimens 4B and 19) and in
the plasmacytoid immunoblastic lymphoma (specimen 14A)
and that these genetic lesions correlate with aggressive clinical behavior and advanced-stage disease in these patients.
We previously demonstrated that p53 gene mutations preferentially occur in certain categories of high-grade lymphoid
m a l i g n a n ~ y . ~Moreover,
~.~~.~~
Nakamura et al” recently documented p53 gene mutations in about 10% of immunoblastic
B-cell lymphomas, and Ichikawa et als2 reported that p53
gene mutations are present significantly more frequently in
B-cell lymphomas in advanced clinical stage (stage IV). The
p53 gene mutations that we identified in two PT-LPDs are
consistent with the mutational spectrum of the p53 tumor
suppressor gene among lymphoid malignancies. In fact, one
was a point mutation involving codon 248, a known mutational hot spot53that we have identified in other lymphoid
m a 1 i g n a n ~ i e . s In
. ~ ~addition,
~~~
we have previously demonstrated that the introduction of ras oncogenes into EBVimmortalized human lymphoblastoid cells results in their
malignant transformation and terminal differentiation into
clonal plasma cells.s4 Neri et a155,s6 have demonstrated that
mutations involving N-ras codons 12, 13, and 61 and Kras codon 12 occur in approximately 32%of plasma cell
leukemias and multiple myelomas. We have further shown
that multiple myelomas containing ras gene mutations are
characterized by advanced-stage disease and adverse prognostic parameters and that ras gene mutations do not occur
in monoclonal gammopathies of undetermined significance
or in solitary plasma~ytornas.~~
Taken together, these findings strongly suggest that ras gene mutations play an important role in the development and progression of multiple
myeloma. In the past, we did not identify ras gene mutations
in malignant lymph~rnas,”~~’
except for occasional AIDSassociated high-grade lyrnphoma~.~~
The presence of an Nras gene mutation in the immunoblastic lymphoma in this
series may reflect the marked plasmacytic differentiation of
this particular neoplasm; indeed, we found it difficult to
distinguish this neoplasm morphologically from the two myelomas in this series. Point mutations involving N-ras account for approximately 80% of all ras gene mutations
among cases of multiple myeloma and plasma cell leukemia,
and the majority of these involve codon 61.55-57
Moreover,
From www.bloodjournal.org by guest on December 22, 2014. For personal use only.
562
KNOWLES ET AL
several cases of multiple myeloma containing a Cto A transgene rearrangements was performed, however, an oligoclonal population of T cells was apparently identified in only
version in the first nucleotide of N-rus codon 61 resulting
one PT-LPD.7' Moreover, we did not identify clonal T;) gene
in the substitution of lysine for glutamine have been docurearrangements in any of the 28 PT-LPDs studied here.
mented in the past.'".'7 Nevertheless, it is rather astonishing
Therefore, clonal T-cell populations appear to be present in
that this specific point mutation occurred in three separate
very few lymphoid proliferations that arise posttransplantaPT-LPDs and accounted forall the rus gene mutations identitied in the PT-LPDs inthisseries. This intriguingfinding
tion. Consequently, the pathogenesis of the rare T-cell maligmay reflect thehighlyselectivenature
of thesegenetic
nanciesthat occur aftertransplantationandwhether
their
development is directly related to posttransplantation immuchanges andsuggests, among otherpossibilities, the involvenosuppression or is merely coincidental remain unclear and
ment of a particular, albeit unknown, mutagen or a selective
advantage conferred in vivo to malignant plasma cells by a
must await additional studies.
Finally, Locker and NalesnikIx previously proposed that
specific N-rus gene mutation.
Similarly,it is not toosurprisingthat
we detectedrethe results of molecular genetic analysis of PT-LPDs may
arrangementof the c-myc gene in only onePT-LPD, the
haveprognosticvalue.
They suggestedthat monomorphic
plasmacytoidimmunoblastic
lymphoma (specimen14A),
PT-LPDs containingastrong Ig gene rearrangementband
bel-l and bel-2 gene reandthatwe
did notdetect
and a c-myc gene rearrangement usually progress in spite
arrangements in any of the PT-LPDs inthisseries.Reof a reduction in immunosuppression.lx We confirmed that
arrangements of the c-myc gene occurin only a small propor- observation in this series in that all four PT-LPDs that containedgeneticalterationswereclassifiedmorphologically
tion of diffuseaggressivemalignantlymphomas
lacking
small noncleaved cell (Burkitt's andBurkitt's-like) morpholas immunoblastic lymphoma or multiple myeloma, and the
patients had advanced-stage andprogressive disease that did
ogy,5x except forthose occurring in association with AIDS'"
not regress after reduction in immunosuppression. They also
or arising in the gastrointestinal tract," and occur only very
rarelyinmultiple myeloma." This is probably the reason
suggested that those PT-LPDs possessing high clone strength
(a semiquantitative estimate of the proportion of clonal B
why c-myc gene rearrangements have been detected in only
cells in an individual PT-LPD lesion, based on the intensity
a small number of PT-LPDs in the past." Moreover, all past
of the Ig gene rearrangement hybridization signal on Southstudies of the c-mvc gene in PT-LPDs have been limited to
e m blotting)inthe absence of c - m y gene rearrangement
detection of c-myc gene rearrangements by Southern blotalso progress despite reduced immunosuppression.'X Howting. However, mutational analysis by SSCP in conjunction
ever, based on our findings, it is likely that some of Locker
with direct sequencingis necessary to detect the small mutaand Nalesnik's clinicallyprogressivemonomorphicPTtions in the region surrounding the tirst exon-first intron of
LPDs exhibiting high clone strength and lacking C-mvcgene
the c-myc gene. Our combined use of both approaches in
rearrangements contained alterations of other genes, such as
the studies described here allowed us to determine concluRus and p53, that were not investigated. Therefore, the biosively that the c-myc gene is infrequently involved in PTlogic characteristics of PT-LPDs that predict their clinical
LPDs. This is unlike lymphomagenesis associated with other
behavior are notentirely clear. We suggest
that a comprehenimmunodeficiency states, such asAIDS." The putative oncosive correlative clinical, morphologic, and molecular genetic
gene bel-l is associated with the t( 1I; 14) and occurs in only
analysis of a largecohort of PT-LPDs is necessary to identify
leukeabout 4% of malignant lymphomasandlymphoid
those factors that determine disease progression and, thus,
mias,3' most commonly in low-grade mantle-cell(centroare useful in predicting the eventualoutcome of patients who
cytic) lymphomas.6' The bel-2 oncogene is associated with
develop a PT-LPD.
the t( 14; 18) and occurs preferentially in malignant lymphoSeveralinvestigatorshavesubscribed
to thehypothesis
mas of follicular center cell derivation.62.63The PT-LPDs do
that the development of lymphoid proliferations after transnot resemble mantle-cell or follicular center-cell lymphomas
plantation is a multistep process.'7.''.'h,72.73 Immunosuppresmorphologically, and our findings suggest that the PT-LPDs
sive therapy is believed to lead to reactivation of latent EBV
are not related to mantle zone or follicular center B cells.
or primary infection by EBV, which acts as a continuously
In addition, while it is widely acknowledged that the mapresent oncogenic agent in these patients. It is theorized that
jority of PT-LPDs are B-cellproliferations,occasional
Tthelack of normal immune surveillance in thesepatients
celllymphomashave beenreported tooccur aftertranspermits the expansionof multiple EBV-infected and immorplantation
as
The relationship
between
their
develtalized B-cell clones (polyclonal). Thoseclones having a
opment and posttransplantation immunosuppression is unproliferative advantageoutgrow
and obscure the other
clear. However, human T cells may be immortalized after
clones, so that only a few (oligoclonal) or only one (monotransfection with EBV DNA:'
and several T-cell malignanclonal) EBV-infected B-cell clone eventually predominates.
cies containing clonal integration of EBV,includingone
occurring after transplantation, have been d o c ~ r n e n t e d . ' ~ . ~ ~ Such
. ~ ~ clones are believed to be susceptible to further genetic
changes, ie, structural alterations of oncogenes andor tumor
It is conceivable, therefore, that EBV may contribute to the
suppressor genes, resulting in the emergenceof a fully transpathogenesis of these posttransplantation T-cell lymphomas
formed monoclonal B-cell proliferation containing homogein a manner analogous to that of the more common B-cell
neous episomal EBV. The results of the studies described
PT-LPDs. In one of the few prior studies where Southern
here supportthishypothesis.
Our resultsstrongly suggest
blot hybridization analysis of PT-LPDs for T-cell receptor
From www.bloodjournal.org by guest on December 22, 2014. For personal use only.
POSlTRANSPLANT LYMPHOPROLIFERATIVE DISORDERS
that the PT-LPDs represent a spectrum of EBV-driven
lymphoid proliferations that parallel the stages along this
continuum from polyclonal (plasmacytic hyperplasia) to
monoclonal (polymorphic PT-LPDs) to frankly malignant
(immunoblastic lymphomdmultiple myeloma). This hypothesis also provides an explanation for the several examples
in the l i t e r a t ~ r e ~ * ~and
. ' ~in
" ~this series (patients 4, 9, 11,
and 14) of two or more morphologically and/or clonally
distinct FT-LPDs occumng in the same individual. These
separate lesions probably represent independent primary
lymphoid proliferations in some instances and the result of
clonal evolution and genetic progression of a single progenitor clone in other instances.
ACKNOWLEDGMENT
We thank Linda Addonizio, Mark Barr, David Blood, Debbie
Frye, Daphne Hsu, Frank Livelli, Melissa McGovem, and Dennis
Reison for their helpful participation in these studies. We also thank
Rina Israelian for assistance in preparing the manuscript and Alfred
Lamme for the excellent photomicrographs.
REFERENCES
1. McKhann CF: Primary malignancy in patients undergoing immunosuppression for renal transplantation. Transplantation 8:209,
1969
2. Penn I, Hammon W, Brettschneider L, Starzl TE: Malignant
lymphomas in transplantation patients. Transplant Roc 1:106, 1969
3. Nalesnik MA, Jaffe R, Starzl TE, Demetris AJ, Porter K, Burnham JA, Makowka L, Ho M, Locker J: The pathology of posttransplant lymphoproliferative disorders occurring in the setting of
cyclosporine A-prednisone immunosuppression. Am
Path01
J
133:173, 1988
4. Ferry JA, Jacobson JO, Conti D, Delmonico F, Harris NL:
Lymphoproliferative disorders and hematologic malignancies following organ transplantation. Mod Pathol 2583, 1989
5. Randhawa PS, Yousem SA, Paradis IL, Dauber JA, Griffith
BP, Locker J: The clinical spectrum, pathology and clonal analysis of
Epstein-Barr virus-associated lymphoproliferative disorder in heartlung transplant recipients. Am J Clin Pathol 92:177, 1989
6. Wilkinson AH, Smith JL, Hunsicker LG, Tobacman J, Kapelanski DP, Johnson M, Wright FH, Behrendt DM, Cony RJ: Increased frequency of posttransplant lymphomas in patients treated
with cyclosporine, azathioprine, and prednisone. Transplantation
47:293, 1989
7. Swinnen LJ, Costanzo-Nordin MR, Fisher SG, O'Sullivan ET,
Johnson MR, Heroux AL, Dizikes GJ, Pifarre R, Fisher RI: Increased
incidence of lymphoproliferative disorder after immunosuppression
with the monoclonal antibody OKT3 in cardiac transplant recipients.
N Engl J Med 323:1723, 1990
8. Hanto DW, Sakamoto K, F'urtilo DT, Simmons RI, Najarian
JS: The Epstein-Barr virus in the pathogenesis of posttransplant
lymphoproliferative disorders. Surgery 90204, 1981
9. Hanto DW, Frizzera G, Purtilo DT, Sakamoto K, Sullivan
JL, Saemundsen AK, Klein G, Simmons RL, Najarian JS: Clinical
spectrum of lymphoproliferative disorders in renal transplant recipients and evidence for the role of Epstein-Barr virus. Cancer Res
41:4253, 1981
10. Penn I: Malignant lymphomas in organ transplant recipients.
Transplant Proc 13:736, 1981
11. Starzl TE, Nalesnik MA, Porter KA, H0 M, Iwatsuki S , Griffith BP, Rosenthal JT, Hakala TR, Shaw BW Jr. Hardesty RL, Atchison RW, Jaffe R, Bahnson HT: Reversibility of lymphomas and
563
lymphoproliferative lesions developing under cyclosporin-steroid
therapy. Lancet 1583, 1984
12. Frizzera G: Atypical lymphoproliferative disorders, in
Knowles DM (ed): Neoplastic Hematopathology. Baltimore, MD,
Williams and Wilkins, 1992, p 459
13. Frizzera G, Hanto DW, Gajl-Peczalska KJ, Rosai J, McKenna
RW, Sibley RK, Holahan KP, Lindquist LL: Polymorphic diffuse
B-cell hyperplasias and lymphomas in renal transplant recipients.
Cancer Res 41:4262, 1981
14. Cleary ML, Warnke R, Sklar J: Monoclonality of lymphoproliferative lesions in cardiac-transplant recipients. N Engl J Med
310:477, 1984
15. Cleary ML, Nalesnik MA, Shearer WT, Sklar J: Clonal analysis of transplant-associated lymphoproliferations based on the structure of the genomic termini of the Epstein-Barr virus. Blood 72:349,
1988
16. Shearer WT, Ritz J, Finegold MJ, Guerra IC, Rosenblatt HM,
Lewis DE, Pollack MS, Taber LH, Sumaya CV, Grumet FC, Cleary
ML, Warnke R, Sklar J: Epstein-Barr virus-associated B-cell proliferations of diverse clonal origins after bone marrow transplantation
in a 12-year-old patient with severe combined immunodeficiency.
N Engl J Med 312:1151, 1985
17. Cleary ML, Sklar J: Lymphoproliferative disorders in cardiac
transplant recipients are multiclonal lymphomas. Lancet 2:489, 1984
18. Locker J, Nalesnik M: Molecular genetic analysis of lymphoid
tumors arising after organ transplantation. AmJ Pathol 135:977,
1989
19. Gaidano G, Dalla-Favera R: Protooncogenes and tumor suppressor genes, in Knowles DM (ed): Neoplastic Hematopathology.
Baltimore, MD, Williams and Wilkins, 1992, p 245
20.. Chen JM, Barr ML, Chadburn A, Frizzera G, Schenkel FA,
Sciacca RR, Reison DS, Addonizio LJ, Rose EA, Knowles DM,
Michler RE: Management of lymphoproliferative disorders following cardiac transplantation. Ann Thorac Surg 56:527, 1993
21. Garrett TJ, Chadburn A, Barr ML, Drusin RE, Chen JM,
Schulman LL, Smith CR. Reison DS, Rose EA, Michler RE,
Knowles DM: Post-transplantation lymphoproliferative disorders
treated with CHOP chemotherapy. Cancer 72:2782, 1993
22. Miller SA, Dykes DD, Polesky HF: A simple salting out
procedure for extracting DNA from human nucleated cells. Nucleic
Acids Res 16:1215, 1988
23. Southern EM: Detection of specific sequences among DNA
fragments separated by gel electrophoresis. J Mol Biol98503, 1975
24. Feinberg AP, Vogelstein B: A technique for radiolabelling
DNA restriction endonuclease fragments to high specific activity.
Anal Biochem 132:6, 1983
25. Pelicci PG, Knowles DM, Dalla-Favera R: Lymphoid tumors
displaying rearrangements of both immunoglobulin and Tcell receptor genes. J Exp Med 162:1015, 1985
26. Korsmeyer SJ, Hieter PA, Ravetch JV, Poplack DG, Waldmann TA, Leder P Developmental hierarchy of immunoglobulin
gene rearrangements inhuman leukemic pre-B-cells. Proc Natl
Acad Sci USA 78:7096, 1981
27. Siminovitch KA, Bakhskhi A, Goldman P, Korsmeyer SJ:
Uniform deleting element mediates the loss of kappa genes in human
B cells. Nature 316:260, 1985
28. Yanagi Y, Yoshikai Y, Legett K, Clark SP, Alexander I, Mak
TW: cDNA clone encodes a protein having extensive homology to
immunoglobulin chains. Nature 308: 145, 1984
29. Dalla-Favera R, Martinotti S, Gallo RC, Erikson J, Croce
CM: Translocation and rearrangement of the c-myc oncogene locus
in human undifferentiated B-cell lymphomas. Science 219:963, 1983
30. Tsujimoto Y, Jaffe E, Cossman J, Gorham J, Nowell PC,
Croce CM: Clustering of breakpoints on chromosome 11 in human
From www.bloodjournal.org by guest on December 22, 2014. For personal use only.
564
B-cell neoplasms with the t(ll; 14) chromosome translocation. Nature 315:340, 1985
3 I . Athan E, Foitl DR, Knowles DM: bcl-l gene rearrangement:
Frequency and clinical significance among B cell chronic lymphocytic leukemias and non-Hodgkin’s lymphomas. Am J Pathol
138591, 1991
32. Cleary ML, Sklar J: Nucleotide sequence of a t(14; 18) chromosomal breakpoint in follicular lymphoma and demonstration of a
breakpoint-cluster region near a transcriptionally active locus on
chromosome 18. Proc Natl Acad Sci USA 82:7439, 1985
33. Cleary ML, Galili N. Sklar J: Detection of a second t( 14;18)
breakpoint cluster region in humanfollicular lymphomas. J Exp Med
164:315, 1986
34. Raab-Traub N, Flynn K: The structure of the termini of the
Epstein-Barr virus as a marker of clonal cellular proliferation. Cell
47:883, 1986
35. Weiss LM, Strickler J, Warnke R, Purtilo DT, Sklar J: Epstein-Barr viral DNA in tissues of Hodgkin’s disease. Am J Pathol
129:86, 1987
36. Gazin C, Dupont de Dinechin S, Hampe A, Masson J-M,
Martin P, Stehelin D, Galibert F: Nucleotide sequence of the human
c-myc locus: Provocative open reading frame within the first exon.
EMBO J 3:383, 1984
37. Buchman VL, Chumakov PM, Ninkina NN, Samarina OP,
Georgiev GP. A variation in the structure of the protein-coding
region of the human p53 gene. Gene 70:245, 1988
38. Gaidano G, Ballerini P, Gong JZ, Inghirami G, Neri A, Newcomb EW, Magrath IT, Knowles DM, Dalla-Favera R: p53 mutations
human
in
lymphoid malignancies: Association with Burkitt
lymphoma and chronic lymphocytic leukemia. Proc Natl Acad Sci
USA 885413, 1991
39. Neri A, Knowles DM, Greco A, McCormic F, Dalla-Favera
R: Analysis of RAS oncogene mutations in human lymphoid malignancies. Proc Natl Acad Sci USA 85:9268, 1988
40. Orita M, Suzuki Y, Sekiya T, Hayashi K: Rapid and sensitive
detection of point mutations andDNA polymorphisms using the
polymerase chain reaction. Genomics 5:874, 1989
41. Maniatis T, Fritsch EF, Sambrook J: Molecular Cloning. A
Laboratory Manual. Cold Spring Harbor, NY, Cold Spring Harbor
Laboratory, 1982
42. Matsushima AY, Cesarman E, Chadburn A, Knowles DM:
Post-thymic T cell lymphomas frequently overexpress p53 protein
but infrequently exhibit p53 gene mutations. Am J Pathol 144:573,
1994
43. Pelicci PG, Knowles DM, Wieczorek R, Wormser G, Arlin
Z, Luciw P, Dina D, Basillico C, Dalla-Favera R: Multiple monoclonal B-cell expansions and c-myc gene rearrangements in AIDSrelated lymphoproliferative disorders: Implications for lymphomagenesis. J Exp Med 164:2049, 1986
44. Hanson CA, Frizzera G, Patton DF, Peterson BA, McClain
KL, Gajl-Peczalska KJ, Kersey JH: Clonal rearrangement for immunoglobulin and T-cell receptor genes in systemic Castleman’s disease: Association with Epstein-Barr virus. Am J Pathol 131:84, 1988
45. Knowles DM, Athan E, Ubriaco A, McNally L, Inghirami G ,
Wieczorek R, Finfer M, Jakobiec FA: Extranodal non-cutaneous
lymphoid hyperplasia represent a continuous spectrum of B-cell neoplasia: Demonstration by molecular genetic analysis. Blood 73: 1635,
1989
46. Weiss LM, Wood GS, Trela M, Warnke RA, Sklar J: Clonal
T-cell populations in lymphomatoid papulosis. Evidence of a lymphoproliferative origin for a clinically benign disease. N Engl J Med
315:475, 1986
47. Weiss LM, Wood GS, Ellisen LW, Reynolds TC, Sklar J:
KNOWLES ET AL
Clonal T cell populations in pityriasis lichenoides et varioliformis
acuta (Mucha-Haberman disease). Am J Path01 126:417, 1987
48. Kame1 OW, van de Rijn M, Weiss LM, Del Zoppo GJ, Hench
PK, Robbins BA, Montgomery PG, Wamke RA, Dorfman RF: Reversible lymphomas associated with Epstein-Barr virus occurring
during methotrexate therapy for rheumatoid arthritis and dermatomyositis. N Engl J Med 328:1317, 1993
49. Cesarman E, Chadburn A, Inghirami G, Gaidano G, Knowles
DM: Structural and functional analysis of oncogenes and tumor
suppressor genes in adult T-cell leukemidymphoma (ATLL) reveals
frequent p53 mutations. Blood 80:3205, 1992
SO. Ballerini P, Gaidano G, Gong JZ, Tassi V, Saglio G, Knowles
DM, Dalla-Favera R: Multiple genetic lesions in acquired immunodeficiency syndrome-related non-Hodgkin’s lymphoma. Blood
81:166, 1993
51. Nakamura H, Said JW, Miller CW, Koeffler HP: Mutations
and protein expression of p53 in acquired immunodeficiency syndrome-related lymphomas. Blood 82:920, 1993
52. Ichikawa A, Hotta T, Takagi N, Tsushita K, Kinoshita T,
Nagi H, Murakami Y, Hayashi K, Saito H: Mutations of p53 gene
and their relation to disease progression in B-cell lymphoma. Blood
79:270 I , I992
53. de Fromentel CC, Soussi T: TP53 tumor suppressor gene: A
model for investigating human mutagenesis. Genes Chrom Cancer
4.1, 1992
54. Seremetis S, Inghirami G, Ferrero D, Newcomb EW, Knowles
DM, Dotto GP, Dalla-Favera R:RAS oncogenes cause malignant
transformation and plasmacytoid differentiation of EBV-infected human B-lymphoblasts. Science 243:660, l989
SS. Neri A, Baldini L, Ferrero D, Murphy JP, Knowles DM,
Dalla-Favera R: Frequency and type of RAS oncogenes in lymphoid
malignancies, in: Molecular Diagnostics of Human Cancer. Cancer
Cells, v01 7. Cold Spring Harbor, NY, Cold Spring Harbor Laboratory Press, 1989, p 101
56. Neri A, Murphy JP, Cro L, Ferrero D, Tarella C, Baldini L,
Dalla-Favera R: Ras oncogene mutation in multiple myeloma. J Exp
Med 170:1715, 1989
57. Corradini P, Ladetto M, Voena C, Palumbo A, Inghirami G,
Knowles DM, Boccadoro M, Pileri A: Mutational activation of Nand K-ras oncogenes in plasma cell dyscrasias. Blood 81:2708, 1993
58. Dalla-Favera R: Chromosomal translocations involving the cmyc oncogene and their role in the pathogenesis of B-cell neoplasia,
in Brugge J, Curran T, Harlow E, McCormick F (eds): Origins of
Human Cancer. A Comprehensive Review. Cold Spring Harbor, NY,
Cold Spring Harbor Laboratory Press, 1991, p 543
59. Van Krieken JHJM, Raffeld M, Raghoebier S, Jaffee ES, Van
Ommen GJB, KluinPhM: Molecular genetics of gastrointestinal
non-Hodgkin’s lymphomas: Unusual prevalence and pattern of cmyc rearrangements in aggressive lymphomas. Blood 76:797, 1990
60. Subar M, Neri A, Inghirami G, Knowles DM, Dalla-Favera
R: Frequent c-myc oncogene activation and infrequent presence of
Epstein-Barr virus genome in AIDS-associated lymphoma. Blood
72:667, 1988
61. Raffeld M, Jaffe ES: bcl-l, t( I I ; 14), and mantle cell-derived
lymphomas. Blood 78:259, 1991
62. Tsujimoto Y , Cossman J, Jaffe E, Croce CM: Involvement
of the bcl-2 gene in human follicular lymphoma. Science 228: 1440,
1985
63. Weiss LM, Warnke RA,Sklar J, Cleary ML: Molecular analysis of the t(14; 18) chromosomal translocation in malignant lymphomas. N Engl J Med 317:1185, 1987
64. Lippman SM, Grogan TM, Carry P, Pgden DA, Miller TP:
Post-transplantation T cell lymphoblastic lymphoma. Am J Med
82:814, 1987
From www.bloodjournal.org by guest on December 22, 2014. For personal use only.
POSTTRANSPIANT LYMPHOPROLIFERATIVEDISORDERS
65. Garvin AJ, Self S, Sahome EA,Stuart RK, Marchalonis J J The
occurrence of a peripheral T-cell lymphoma in a chronically immunosuppressed renal transplant patient. Am J Surg path01 1264,1988
66. Kemnitz J, Cremer J, Gebel M, Uysal A, HaverichA, Georgii
A: T-cell lymphoma after heart transplantation. Am J Clin Path01
94:95, 1990
67.Kumar S, Kumar D, KingmaDW, Jaffe ES:Epstein-Barr
virus-associated T-cell lymphoma in a renal transplant patient. Am
J Surg Path01 17:1046, 1993
68. Stevenson M, Volsky B, Hedenskog M, Volsky DJ: Immortalization of human T lymphocytes after transfection
of Epstein-Barr
virus DNA. Science 233:980, 1986
69. Jones W,Shurin S, Carlos A, TubbsRR, Sciotto CG, WahlR,
Sands J, GottmanD, Katz BZ,Sklar J: T-cell lymphoma containing
Epstein-Barr viral DNA in patients with chronic Epstein-Barr virus
infections. N Engl J Med 318:733, 1988
566
70. Harabuchi Y, Yamanaka N, Kataura A, Imai S, Kinoshita
T, Mizuno F, Osato T: Epstein-Barr virus in nasal T-cell lymphomas in patients with lethal midline granuloma. Lancet 335:128,
1990
71. Osterhage D, Steele PE, Witte D, Schroeder T, Yochman L,
Swerdlow SH: T cells in posttransplant lymphoproliferative disorders: An immunophenotypic and genotypic investigation. Lab Invest
66:85A, 1992 (abstr)
72. Klein G, Purtilo D: Summary: Symposium on Epstein-Barr
virus induced lymphoproliferative diseases in immunodeficient patients. Cancer Res 41:4302, 1981
73. Hanto DW, Gajl-Peczalska KJ, Frizzera G, Arthur DC, Balfour HH Jr. McClain K, Simmons RL, Najarian JS: Epstein-Barr
virus (EBV) induced polyclonal and monoclonal B-cell lymphoproliferativediseaseoccurringafterrenaltransplantation.
Ann Surg
198:356,1983
From www.bloodjournal.org by guest on December 22, 2014. For personal use only.
1995 85: 552-565
Correlative morphologic and molecular genetic analysis
demonstrates three distinct categories of posttransplantation
lymphoproliferative disorders
DM Knowles, E Cesarman, A Chadburn, G Frizzera, J Chen, EA Rose and RE Michler
Updated information and services can be found at:
http://www.bloodjournal.org/content/85/2/552.full.html
Articles on similar topics can be found in the following Blood collections
Information about reproducing this article in parts or in its entirety may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests
Information about ordering reprints may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#reprints
Information about subscriptions and ASH membership may be found online at:
http://www.bloodjournal.org/site/subscriptions/index.xhtml
Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American
Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036.
Copyright 2011 by The American Society of Hematology; all rights reserved.

![Inter-VH-gene-family shared idiotype on acquired immunodeficiency syndrome-associated lymphomas [letter]](http://cdn1.abcdocz.com/store/data/000330859_1-00457593ce606a102a7fab7f68f3e852-250x500.png)



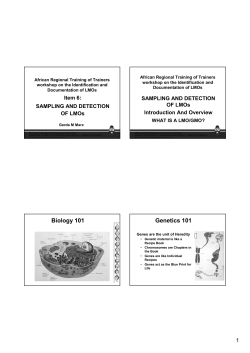




© Copyright 2026