
Market Conduct & Consumer Affairs (EX3) Subcommittee
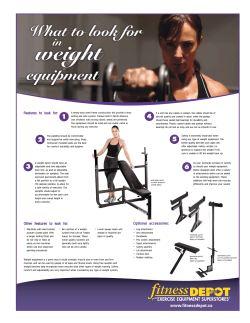
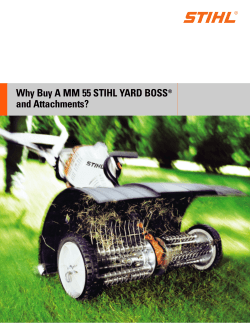
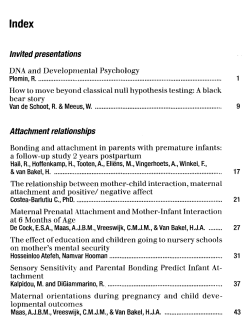
Date: 12/19/14 Conference Call MARKET REGULATION AND CONSUMER AFFAIRS (D) COMMITTEE Friday, December 19, 2014 12:00 p.m. ET ROLL CALL Stephen W. Robertson, Chair Therese M. Goldsmith, Vice Chair Jay Bradford Chester A. McPherson Sharon P. Clark Mike Rothman Bruce R. Ramge Wayne Goodwin Mark O. Rabauliman Laura N. Cali Susan L. Donegan Michael D. Riley Tom C. Hirsig Indiana Maryland Arkansas District of Columbia Kentucky Minnesota Nebraska North Carolina N. Mariana Islands Oregon Vermont West Virginia Wyoming AGENDA 1. Consider Adoption of its Nov. 18 Minutes—Commissioner Stephen W. Robertson (IN) Attachment A 2. Consider Adoption of Health Reform Data Call and Definitions —Commissioner Stephen W. Robertson (IN) Attachment B 3. Receive Update on 2014 Market Regulation Summit Action Items —Commissioner Stephen W. Robertson (IN) Attachment C © 2014 National Association of Insurance Commissioners Draft Pending Adoption Attachment A Draft: 11/26/14 Market Regulation and Consumer Affairs (D) Committee Washington, District of Columbia November 18, 2014 The Market Regulation and Consumer Affairs (D) Committee met in Washington, DC, Nov. 18, 2014. The following Committee members participated: Stephen W. Robertson, Chair (IN); Therese M. Goldsmith, Vice Chair (MD); Jay Bradford represented by Ashley Fisher (AR); Chester A. McPherson represented by Lee Backus (DC); Sharon P. Clark (KY); Mike Rothman (MN); Wayne Goodwin represented by Tracy Biehn (NC); Bruce R. Ramge (NE); Laura N. Cali (OR); Susan L. Donegan (VT); Michael D. Riley and Mark Hooker (WV); and Tom C. Hirsig (WY). Also participating were: Randy Adair (KS); and Chuck Vanasdalan (NH). 1. Adopted its Oct. 20 Minutes Commissioner Rothman made a motion, seconded by Commissioner Clark, to adopt the Committee’s Oct. 20 minutes (Attachment One). The motion was unanimously adopted. 2. Adopted ACA Market Conduct Examination Standards Director Ramge said since the Summer National Meeting, the Market Conduct Examination Standards (D) Working Group has adopted: 1) health reform-related market conduct examination standards relating to prohibition of excessive waiting periods; and 2) health reform-related market conduct examination standards relating to essential health benefits. Director Ramge said the Working Group has been working since 2012 on drafting market conduct examination standards for the immediate health reforms of the federal Affordable Care Act (ACA), as well as for the health reforms effective Jan. 1, 2014. He said that once the examination standards are adopted by the Executive (EX) Committee and Plenary, they will be included in the Market Regulation Handbook. Director Ramge said that recognizing jurisdictions have varying policy directions regarding the enforcement of the ACA, the examination standards developed by the Working Group are designed to provide uniform guidance to insurance regulators in their oversight of regulated entity activity, as appropriate for their consumers. Director Ramge made a motion, seconded by Commissioner Rothman, to adopt the examination standards related to prohibition of excessive waiting periods (Attachment Two) and essential health benefits (Attachment Three). The motion was unanimously adopted. 3. Adopted Revised Core Competencies Director Ramge said the Market Conduct Examination Standards (D) Working Group was asked by the Market Regulation and Consumer Affairs (D) Committee, on its June 23 conference call, to perform a review of the core competencies regarding state insurance department oversight of contract examiners, in response to one of the recommendations found in the December 2013 Federal Insurance Office (FIO) report. He said that at the Fall National Meeting, the Working Group adopted revisions concerning: 1) professional designations of both insurance department and contract examiner staff; 2) status reports to insurance departments from contract examiners; 3) insurance department oversight of contract examiner activity; and 4) contract examiner conduct, adherence to work plan and conflict of interest guidelines. Director Ramge made a motion, seconded by Commissioner Goldsmith, to adopt the revised core competencies (Attachment Four). The motion was unanimously adopted. 4. Adopted the Health Reform Survey Mr. Vanasdalan said the Market Analysis Procedures (D) Working Group had adopted a survey to be placed in the NAIC Market Regulation Handbook, which could be used as a template by states, either individually or collaboratively, to perform analysis or examination work. He said the survey essentially asks companies to certify if they have taken steps required to implement the ACA. Director Rothman made a motion, seconded by Commissioner Clark, to adopt the health reform survey (Attachment Five). The motion was unanimously adopted. 5. Adopted the Health Reform Data Call Mr. Vanasdalan said the Market Analysis Procedures (D) Working Group had also adopted a health reform data call, which could be placed in the Market Regulation Handbook so it can be used as a template by states to perform analysis or © 2014 National Association of Insurance Commissioners 1 Draft Pending Adoption Attachment A examination work on active carriers. He said that since he understood the ACA eliminated issues with closed blocks of business, the data call would not collect data on closed blocks of business. He said that the Working Group, when adopting the data elements for the data call, also agreed to request permission for an interim meeting to work with all interested parties to develop definitions. Director Ramge asked if a pilot program had been considered to test the data elements. Mr. Vanasdalan said the Working Group had not discussed a pilot program since he believed this data call, like the other standard data requests in the Market Regulation Handbook, is only to be used as a template by states. Mr. Vanasdalan said it might be possible to request data from a small group of carriers to identify issues with the data elements. Marty Mitchell (America’s Health Insurance Plans—AHIP) said that he supported an interim meeting or conference calls to finalize definitions and ensure that the data elements could be provided by health insurance carriers. Commissioner Robertson asked if it was acceptable to exclude closed blocks of business from the data call. Mr. Mitchell said excluding information from the data call would not be an issue. Timothy S. Jost (Virginia Organizing) said that since the ACA has been in effect for four years, and the U.S. Department of Health and Human Services (HHS) had not yet collected any data, he believed they were clearly signaling to the state regulators that HHS is deferring to state regulators for the collection of data for analysis and examinations. He said that while he understood there were a few definitional issues to be worked out, he would like to see the data call finalized as soon as possible. Commissioner Goldsmith asked Mr. Mitchell if he had concerns about the definitions or the data elements themselves. Mr., Mitchell said he was concerned with both the data definitions and the data elements. He said that since the data elements were requesting information by metal level, he was unsure if companies could provide the information as requested. Commissioner Goldsmith said she was concerned about opening up both the data elements and definitions for continued discussion. Commissioner Robertson asked Mr. Mitchell if he had discussed the issue with his member carriers and wanted to know how long it would take to do so. Mr. Mitchell said he was uncertain how long it would take. Commissioner Robertson said he was concerned that nothing would be accomplished if the group continued to wait for answers from carriers. Commissioner Rothman made a motion, seconded by Commissioner Cali, to adopt the data call framework subject to an interim meeting in mid-December to finalize the data elements and definitions, as well to discuss a potential pilot project, and then submit any changes to the Committee for adoption in December. The motion was unanimously adopted (Attachment Six). Andrea Routh (Missouri Health Advocacy Alliance) said there is a great deal of activity in the health insurance marketplace and that the data call could currently be used by any state to collect data for analysis. She thanked the Committee for trying to get the documents finalized by the end of the year. 6. Adopted Market Information Systems Data Analysis Metrics Mr. Hooker said the Market Information Systems (MIS) data analysis metrics had been developed to analyze the data currently in the NAIC’s MIS to see what was entered and what training needs to occur to ensure better data quality. For this analysis, the Market Information Systems (D) Task Force included Complaint, Exam, Market Analysis Reporting System, Market Conduct Annual Statement and Regulatory Action data. For each of these systems, the Market Information Systems (D) Task Force evaluated three aspects of data quality: completeness, timeliness and accuracy. The objective of this analysis is to identify potential data quality issues. In some areas, a direct correlation cannot be drawn between the data and the measure; therefore, the test is intended to measure reasonableness. In other areas, a threshold is recommended, again to measure reasonableness. Some outliers may be accurate and acceptable. Commissioner Riley made a motion, seconded by Commissioner Goldsmith, to adopt the MIS data analysis metrics. The motion was unanimously adopted (Attachment Seven). 7. Adopted a Compendium of Reports on the Pricing of Personal Automobile Insurance Commissioner Hirsig said the Auto Study (C/D) Study Group adopted a “Summary of Consumer Groups’ Comments related to the Availability and Affordability of Auto Insurance for Low Income Drivers.” Commissioner Hirsig said this summary will be included in the “Compendium of Reports on the Pricing of Personal Automobile Insurance.” Commissioner Hirsig © 2014 National Association of Insurance Commissioners 2 Draft Pending Adoption Attachment A made a motion, seconded by Commissioner Goldsmith, to adopt the “Summary of Consumer Groups’ Comments related to the Availability and Affordability of Auto Insurance for Low Income Drivers.” The motion was unanimously adopted [Drafting Note: joint minutes are attached to the Property and Casualty Insurance (C) Committee, Nov. 18, 2014, minutes]. 8. Adopted Task Force and Working Group Reports Mr. Adair said the Antifraud (D) Task Force adopted its Sept. 17 and Aug. 17 minutes. He said the Task Force had received a report on NAIC participation as a partner in the Healthcare Fraud Prevention Partnership and that the NAIC has remained a full partner since 2011. He said the Task Force will continue to participate and provide information to the Committee on how it can benefit from the participation. He said the Task Force also received a report on the Online Fraud Reporting System (OFRS), as well as a report on the 2014 antifraud education programs. Mr. Adair said that due to the success of the 2013 Insurance Department Investigator Safety Guideline webinar, the Task Force had discussed offering an additional webinar on Dec. 9. He said the Task Force will also be working on the creation of an industry insurance investigator safety guideline for 2015. He said the Task Force discussed the NAIC Antifraud Resources Report data updates for 2014. He said the Task Force will be opening the report to update the type of data collected. He said the Task Force will solicit comments and suggestions from its members, interested regulators and interested parties on the information published in the report. He said the Task Force received reports from Coalition Against Insurance Fraud, National Insurance Crime Bureau (NICB) and National Health Care Anti-Fraud Association (NHCAA) on matters of national interest to insurance fraud bureaus. Commissioner Riley said the Market Information Systems (D) Task Force adopted its Aug. 16 minutes and adopted the report of the Market Information Systems Research and Development (D) Working Group from its Oct. 30, Oct. 8 and Sept. 10 meetings. He said the report included direction given on several Uniform System Enhancement Request (USER) forms and a review of criteria to analyze the MIS data. He said the Task Force adopted the report of the Regulatory Information Retrieval System (D) Subgroup from its Oct. 28 meeting. He said the Task Force also adopted criteria to analyze the MIS data and directed NAIC staff to generate the associated results. Director Ramge said the Market Conduct Examination Standards (D) Working Group continues to work on ACA standards and Chapter 14 regarding sampling for market conduct examinations. He said the Working Group had also adopted revisions to core competencies related to insurance department staff professional designations and contract examiner professional designations, state insurance department oversight of contract examiners, and conflict of interest (Attachment Eight). Commissioner Hirsig said the Auto Insurance (C/D) Study Group adopted its Aug. 16 minutes and a revised version of the Compendium of Reports on the Pricing of Personal Automobile Insurance. He said the Study Group also discussed comments received on the draft data call template and a memorandum the Study Group sent to the Casualty Actuarial and Statistical (C) Task Force asking the Task Force to study the issue of price optimization. He said the Study Group: 1) heard an update from Maryland concerning a bulletin prohibiting the use of price optimization; 2) discussed the possibility of studying the issue of rating tools, such as one from TransUnion/CARFAX, that use vehicle records to rate auto insurance policies; and 3) heard an update from Oklahoma on its Temporary Motorist Liability Plan, which attempts to address the issue of uninsured motorists in Oklahoma. Commissioner Hirsig said he would like a data call template adopted by the Study Group to be discussed on an upcoming call for possible adoption [Drafting Note: joint minutes are attached to the Property and Casualty Insurance (C) Committee, Nov. 18, 2014, minutes]. Mr. Vanasdalan said the Market Analysis Procedures (D) Working Group adopted its Oct. 29, Sept. 25 and Aug. 17 minutes, and agreed to add health as the next line of business in the Market Conduct Annual Statement (MCAS) (Attachment Nine). Commissioner Goldsmith said the Market Regulation Accreditation (D) Working Group had discussed a Market Regulation Accreditation Goals, Objectives and Guiding Principles draft and the Working Group’s projected timeline (Attachment Ten). Commissioner Robertson said the Market Actions (D) Working Group met Nov. 6, Oct. 7 and Sept. 2 in regulator-toregulator session pursuant to paragraph 3 (specific companies, entities or individuals) of the NAIC Policy Statement on Open Meetings. Commissioner Rothman made a motion, seconded by Commissioner Donegan, to adopt the reports from the Committee’s task forces and working groups. The motion was unanimously adopted. © 2014 National Association of Insurance Commissioners 3 Draft Pending Adoption 9. Attachment A Heard a Presentation on Amendments to Regulation P: Annual Privacy Notice Requirements Under the Federal GrammLeach-Bliley Act Joseph Devlin (Consumer Financial Protection Bureau—CFPB) said that a new rule had been adopted regarding the nature of annual privacy notice distributions. He said under the federal Gramm-Leach-Bliley Act, financial institutions are required to provide privacy information to customers when a relationship is first established and then on an annual basis. However, he said that since studies show that consumers often do not read the annual notices, they are not receiving the information they need. He said that under certain conditions, financial institutions will now be able to post the privacy notice online and then alert concerns with a Web address on other notices provided to the consumer. Consumers must also be given a phone number for them to call if they want a hard copy of the notice. This method will not be allowed for financial institutions that distribute customer information to other parties. 10. Heard a Report on Market Conduct Activities of the IAIS Commissioner Donegan said the IAIS had developed issues papers and other documents to assist regulators worldwide in the regulation of their insurance marketplace. She said that starting in 2015, the IAIS will require the Market Conduct Working Group to interact with stakeholders: 1) when specific, technical input is required on an issue; 2) to solicit targeted feedback on an issue or proposal; 3) to receive an explanation of practices and developments within the industry or certain regions or jurisdictions; and 4) to engage with consumer groups or representatives and other stakeholders on relevant issues. She said she would recommend a brief presentation to the Committee on all international activities at the 2015 Spring National Meeting. 11. Heard a Report on Federal Activities Tony Cotto (NAIC) said Commissioner Consedine will be testifying in front of the U.S. House Financial Services Committee on international transparency issues. 12. Heard a Presentation on Weblining and Implications for Insurance Market Regulation Birny Birnbaum (Center for Economic Justice—CEJ) said big data is defined as massive databases of information of individual consumers; associated data mining and predictive analytics applied to those data; and scoring models produced from those analytics. He said that originally, advisory organizations, like the Insurance Services Office (ISO), collected data from many insurers to develop advisory loss costs. He said information was organized and gathered according to predefined characteristics and used to evaluate those predefined risk classes. He said their activities were subject to regulatory oversight. He said the use of insurance credit score was a watershed event because it was the first time a large non-insurance database was data-mined to predict outcomes for insurance companies. Mr. Birnbaum said that using a database from consumer credit information on 200 million consumers, Fair Isaac identified 500 data elements within consumer credit reports, added some individual insurance outcome information to the data and associated insurance outcomes with consumer credit information to identify 10 to 20 data elements most predictive of the insurance outcome to create “credit-based insurance scores.” He said this dramatically increased the segmentation of consumers into risk classes and led insurers to review traditional insurance classifications to develop more granularity. He said the new use of big data occurs when financial service firms, including insurers, tap into a variety of non-insurance databases to steer and segment consumers with little or no transparency or oversight. He said this occurs with the steering of consumers without the consumers’ knowledge and skirting protections form consumers required by the federal Fair Credit Reporting Act (FCRA). Commissioner Robertson said Mr. Birnbaum would have opportunities at future NAIC meetings to expand on the issue. 13. Discussed Other Matters Commissioner Robertson said he would like the minutes to reflect his appreciation for the prior contributions of Commissioner Hirsig, Ted Clark (KS), Jim Mumford (IA) and Craig Leonard (NAIC). Having no further business, the Market Regulation and Consumer Affairs (D) Committee adjourned. W:\National Meetings\2014\Fall\Cmte\D\11-Dmin.docx © 2014 National Association of Insurance Commissioners 4 Attachment B HEALTH REFORM DATA CALL DEFINITIONS Adopted by the Market Analysis Procedures (D) Working Group – December 11, 2014 © 2014 National Association of Insurance Commissioners 1 Attachment B Line # Terms and Data Elements Health Insurance Coverage Exchange (Marketplace) Definition Benefits consisting of medical care (provided directly, through insurance or reimbursement, or otherwise and including items and services paid for as medical care) under any hospital or medical service policy or certificate, hospital or medical service plan contract, or health maintenance organization contract offered by a health insurance issuer. This is not intended to include excepted benefits as defined in 42 U.S.C. § 300gg-91(c). This is also not intended to include closed blocks not subject to Medical Loss Ratio (MLR) reporting under Centers for Medicare & Medicaid Services (CMS) guidance nor is it intended to include self-funded plans. The Affordable Care Act (ACA) creates new “American Health Benefit Exchanges” in each state to assist individuals and small businesses in comparing and purchasing qualified health insurance plans. An exchange may be a governmental agency or nonprofit entity that meets the applicable standards of the ACA and makes Qualified Health Plans (QHPs) available on the marketplace to qualified individuals and/or qualified employers. Unless otherwise identified, this term includes an Exchange serving the individual market for qualified individuals and a Small Business Health Options Program (SHOP) serving the small group market for qualified employers, regardless of whether the Exchange is established and operated by a State (including a regional Exchange or subsidiary Exchange) or by Health and Human Services (HHS). The individual Exchange will determine who qualifies for subsidies and make subsidy payments to insurers on behalf of individuals receiving them. © 2014 National Association of Insurance Commissioners Reference 42 U.S.C. § 300gg91 (c) CCIIO Technical Guidance (CCIIO 2013-0001) Part 155.20-Exchange Establishment Standards and Other Related Standards under the Affordable Care Act 2 Attachment B Line # Terms and Data Elements Definition Reference In Exchange Health insurance coverage acquired through the Exchange (marketplace) as described above. Out of Exchange Health insurance coverage acquired outside the Exchange (marketplace) as described above. Bronze (Metal Level) Health insurance coverage in the bronze level shall provide a level of coverage that is designed to provide benefits that are actuarially equivalent to 60 percent of the full 42 U.S.C. § 18022 actuarial value (with allowable de minimus variations as described in 45 CFD 156.140(c)) (d)(1)(A) of the benefits provided under the plan. Silver (Metal Level) Health insurance coverage in the silver level shall provide a level of coverage that is designed to provide benefits that are actuarially equivalent to 70 percent of the full 42 U.S.C. § 18022 actuarial value (with allowable de minimus variations as described in 45 CFD 156.140(c)) (d)(1)(B) of the benefits provided under the plan. © 2014 National Association of Insurance Commissioners 3 Attachment B Line # Terms and Data Elements Definition Reference Gold (Metal Level) Health insurance coverage in the gold level shall provide a level of coverage that is designed to provide benefits that are actuarially equivalent to 80 percent of the full 42 U.S.C. § 18022 actuarial value (with allowable de minimus variations as described in 45 CFD 156.140(c)) (d)(1)(C) of the benefits provided under the plan. Platinum (Metal Level) Health insurance coverage in the platinum level shall provide a level of coverage that is designed to provide benefits that are actuarially equivalent to 90 percent of the full 42 U.S.C. § 18022 actuarial value (with allowable de minimus variations as described in 45 CFD 156.140(c)) (d)(1)(D) of the benefits provided under the plan. Catastrophic Health insurance coverage that does not provide a metal level of coverage. Catastrophic coverage plans pay less than 60% of the total average cost of care and are available only to people who are under 30 years of age before the beginning of the plan year or who have received an exemption from the requirement to maintain minimum essential coverage by reason of hardship or lack of affordability. 42 U.S.C. § 18022 (E) Individual Health Health insurance coverage offered in the individual market, but does not include shortInsurance Coverage term limited duration insurance. 42 U.S.C. § 300gg91 (b) (5) © 2014 National Association of Insurance Commissioners 4 Attachment B Line # Terms and Data Elements Definition Reference Grandfathered Health insurance coverage that an individual was enrolled in prior to March 23, 2010 either through an individual health insurance coverage or group health insurance coverage plan. Grandfathered plans are exempted from most changes required by the 29 CFR § ACA. New employees may be added to group plans that are grandfathered, and new 2590.715-1251 family members may be added to all grandfathered plans. The plan may lose grandfathered status if significant changes are made to the plan... Multi-State Health insurance coverage created by ACA operated under contract with The U.S. Office of Personnel Management (OPM) and available in multiple states. ACA 1334 Short-Term Health insurance coverage provided pursuant to a contract with an issuer that has an expiration date specified in the contract (taking into account any extensions that may be elected by the policyholder without the issuer's consent) that is less than 12 months after the original effective date of the contract. 45 CFR § 144.103 Small Group Health Health insurance coverage offered in the small group market. Insurance Coverage © 2014 National Association of Insurance Commissioners 45 CFR § 144.103 5 Attachment B Line # Terms and Data Elements Definition Reference Student Individual health insurance coverage that is provided pursuant to a written agreement between an institution of higher education and a health insurance issuer, and provided to students enrolled in that institution of higher education and their dependents, that meets the following conditions: (1) Does not make health insurance coverage available other than in connection with enrollment as a student (or as a dependent of a student) in the institution of higher education. (2) Does not condition eligibility for the health insurance coverage on any health status-related factor relating to a student (or a dependent of a student). (3) Meets any additional requirement that may be imposed under State law. 45 CFR § 147.145 Transitional Plan Plans that are issued pursuant to the policy promulgated by the Centers for Medicare & Medicaid Services (CMS) in a letter dated November 14, 2013 to the State Insurance Commissioners. If permitted by applicable State authorities, health insurance issuers may choose to continue certain coverage that would otherwise be cancelled or modified to comply with the ACA, and affected individuals and small businesses may choose to re-enroll in such coverage. CMS has further stated that, under the transitional policy, non-grandfathered health insurance coverage in the individual or small group market that is renewed for a policy year starting between January 1, 2014 and October 1, 2016 will not be considered to be out of compliance with certain market reforms if certain specific conditions are met including the approval of state authorities. © 2014 National Association of Insurance Commissioners 6 Attachment B Line # Terms and Data Elements Definition Reference Policy Administration Rescission A rescission is a cancellation or discontinuance of coverage that has retroactive effect. (Does not include cancellations for non-payment.) PA1 Earned Premium Total premium earned from all policies written by the insurer during the specified period. PA2 Number of policies issued Number of policies (contracts) for health insurance coverage issued during the specified period. © 2014 National Association of Insurance Commissioners 29 CFR § 2590.715-2712 A (2) NAIC Model Act 36 - Individual Market Health Insurance Coverage Model Act 7 Attachment B Line # Terms and Data Elements Definition PA3 Applications received by carrier that did not result in a policy Number of applications (questionnaires and forms required by the insurer to determine eligibility) which were received by the carrier during the period but which did not result in a policy being issued. PA4 Number of lives on policies issued Total number of persons covered under all the insurance contracts during the period. Reasonable approximations are allowed when exact information is not administratively available to the reporting entity. PA5 Member months for policies issued Accident & Health The sum of total number of lives insured on a pre-specified day of each month of the Policy Experience reported year. Reasonable approximations are allowed when exact information is not Exhibit of the administratively available to the reporting entity. Financial Annual Statement PA6 Number of policy terminations and cancellations initiated by the consumer Number of policies terminated at the insured's request. © 2014 National Association of Insurance Commissioners Reference 8 Attachment B Line # Terms and Data Elements PA7 Number of policy terminations and cancellations due to non-payment of premium Number of policies terminated because the insured never paid, or stopped paying, the required premium for coverage. PA8 Number of lives impacted on terminations and cancellations initiated by the consumer Total number of lives which were no longer covered as a result of policies terminated at the insured's request. Reasonable approximations are allowed when exact information is not administratively available to the reporting entity. PA9 Number of lives impacted on policies terminated and cancelled due to non-payment Total number of lives which were no longer covered as a result of policies terminated because the insured never paid, or stopped paying, the required premium for coverage. Reasonable approximations are allowed when exact information is not administratively available to the reporting entity. Definition © 2014 National Association of Insurance Commissioners Reference 9 Attachment B Line # PA10 Terms and Data Elements Number of rescissions Number of lives PA11 impacted by rescissions Definition Reference Number of policies cancelled as a result of a rescission. Total number of lives which were no longer covered as a result of rescissions. Reasonable approximations are allowed when exact information is not administratively available to the reporting entity. Claims Administration CA1 Claim For the purposes of this data call a claim means any individual line of service within a bill for services. Number of claims received Number of claims received by a carrier during the period requesting payment or reimbursement based on the terms of the insurance policy. Note: For the purposes of this data call a claim means any individual line of service. © 2014 National Association of Insurance Commissioners 42 CFR § 447.45 (b) 10 Attachment B Line # Terms and Data Elements Definition CA2 Number of claims submitted by innetwork providers Number of claims received by a carrier asking for a payment or reimbursement by or on behalf of an in-network health care provider (such as a hospital or doctor) that is contracted to be part of the network for a carrier (such as a Health Maintenance Organization (HMO) or Preferred Provider Organization (PPO)). The provider agrees to the carriers' rules and fee schedules in order to be part of the network and usually agrees not to balance bill patients for amounts beyond the agreed upon fee. Note: For the purposes of this data call a claim means any individual line of service. CA3 Number of claims submitted by outof-network Providers Number of claims received by a carrier asking for a payment or reimbursement by or on behalf of an out-of-network health care provider (such as a hospital or doctor) that is not contracted to be part of a carrier's network (such as an HMO or PPO). Note: For the purposes of this data call a claim means any individual line of service. Number of claim denials for innetwork claims Number of claims received by a carrier asking for a payment or reimbursement by or on behalf of an in-network health care provider (such as a hospital or doctor) that is contracted to be part of the network for a carrier (such as an HMO or PPO) and were subsequently denied by the carrier. Note: For the purposes of this data call a claim means any individual line of service. Do not include claims that were pended for additional information and subsequently paid. CA4 CA5 Reference Stratification of A grouping of number of days that it has taken to deny in-network claims. (0-15, 16-30, days (tied to CA4) 31 to 45, 46 to 90, 91 to 180, 181 to 360, 360+). © 2014 National Association of Insurance Commissioners 11 Attachment B Line # CA6 CA7 CA8 CA9 Terms and Data Elements Number of claims denials for out-ofnetwork claims Definition Reference Total number of claims received by a carrier asking for a payment or reimbursement by or on behalf of an out-of-network health care provider (such as a hospital or doctor) that is not contracted to be part of a carrier's network (such as an HMO or PPO) and subsequently denied by the carrier. Note: For the purposes of this data call a claim means any individual line of service. Do not include claims that were pended for additional information and subsequently paid. Stratification of A grouping of number of days that it has taken to deny out-of-network claims. (0-15, days (tied to CA6) 16-30, 31 to 45, 46 to 90, 91 to 180, 181 to 360, 360+). Number of paid claims for innetwork services Total number of claims received by a carrier asking for a payment or reimbursement by or on behalf of an in-network health care provider (such as a hospital or doctor) that is contracted to be part of the network for a carrier (such as an HMO or PPO) and were subsequently paid by the carrier. Note: For the purposes of this data call a claim means any individual line of service. Include claims that were pended for additional information and subsequently paid. Stratification of A grouping of number of days that it has taken to pay in-network claims. (0-15, 16-30, days (tied to CA8) 31 to 45, 46 to 90, 91 to 180, 181 to 360, 360+). © 2014 National Association of Insurance Commissioners 12 Attachment B Line # Terms and Data Elements Number of paid CA10 claims for out-ofnetwork services CA11 Definition Reference Total number of claims received by a carrier asking for a payment or reimbursement by or on behalf of an out-of-network health care provider (such as a hospital or doctor) that is not contracted to be part of a carrier's network (such as an HMO or PPO) and subsequently paid by the carrier. Note: For the purposes of this data call a claim means any individual line of service. Include claims that were pended for additional information and subsequently paid. Stratification of A grouping of number of days that it has taken to pay out-of-network claims. (0-15, 16days (tied to CA10) 30, 31 to 45, 46 to 90, 91 to 180, 181 to 360, 360+). CA12 Claims Paid Total dollar value of payments by the carrier for benefits reflected in claimants’ Explanations of Benefits (EOBs) for the requested period. © 2014 National Association of Insurance Commissioners 13 Attachment B Line # Terms and Data Elements Definition Reference Total dollar value of co-payments reflected in claimants' EOBs for the requested period. Insured/beneficiary A co-payment is a fixed amount (for example, $15) paid by a covered life for a covered CA13 co-payment health care service, usually paid when the service is provided. The amount can vary by responsibility the type of covered health care service. Insured CA14 coinsurance responsibility Total dollar value of co-insurance applied on benefits reflected in claimants’ EOBs for the requested period. Co-insurance is the percentage amount, if any, of a covered benefit which the insured pays as share of the payment made against a claim. Insured deductible CA15 responsibility Total dollar value of deductibles applied by the carrier for the requested period. A deductible is the amount owed for health care services the plan covers before the health insurance or plan begins to pay. © 2014 National Association of Insurance Commissioners 14 Attachment B Line # Terms and Data Elements Definition Reference A rescission, or a denial, reduction, termination of, or a failure to provide or make payment (in whole or in part) for, a benefit, including any such denial, reduction, termination, or failure to provide or make payment that is based on a determination of a member’s, or eligible dependent’s, eligibility to participate in a plan, and including a denial, reduction, termination of, or a failure to provide or make payment (in whole or in part) for, a benefit resulting from the application of any utilization review, as well as a failure to cover an item or service for which benefits are otherwise provided because it is determined to be experimental or investigational or not medically necessary or appropriate. NAIC Model Act 76 - Uniform Health Carrier External Review Model Act; NAIC Model Act 72 - Health Carrier Grievance Procedure Model Act, Section 3(A) An independent review of an adverse determination or final adverse determination. NAIC Model Act 76 - Uniform Health Carrier External Review Model Act Consumer Requested Internal Reviews (Grievances) Adverse Determination External Review © 2014 National Association of Insurance Commissioners 15 Attachment B Line # Terms and Data Elements Definition Reference External (Independent) Review Organization NAIC Model Act 76 - Uniform An entity that conducts independent external review of adverse determinations or final Health Carrier adverse determination. External Review Model Act Grievance A written complaint, or oral complaint if the complaint involves an urgent care request, submitted by or on behalf of a covered person regarding: (1) Availability, delivery or quality of health care services, including a complaint regarding an adverse determination made pursuant to utilization review; (2) Claims payment, handling or reimbursement for health care services; or (3) Matters pertaining to the contractual relationship between a covered person and a health carrier. Grievance for NonAdverse Determination A grievance arising from any issue other than an adverse determination. Internal Review A process by which the insured may have an adverse determination reviewed by the carrier with respect to a denial of an admission, availability of care, continued stay or health care services for a covered person. © 2014 National Association of Insurance Commissioners NAIC Model Act 72 - Health Carrier Grievance Procedure Model Act NAIC Model Act 72 - Health Carrier Grievance Procedure Model Act NAIC Model Act 72 - Health Carrier Grievance Procedure Model Act 16 Attachment B Line # Terms and Data Elements Overturned Decision A reversal of a denial of an adverse determination by a health carrier or its designee utilization review organization. Upheld Decision A denial of an adverse determination that has been found to be supported by a health carrier or its designee utilization review organization. Voluntary Review Level IR1 Definition A level of review beyond the normal internal appeals process. Reference NAIC Model Act 72 - Health Carrier Grievance Procedure Model Act - Section 9 Number of customer requests for internal reviews of grievances involving adverse See definition of internal review above. determinations (Do not include additional voluntary levels of reviews.) © 2014 National Association of Insurance Commissioners 17 Attachment B Line # IR2 IR3 Terms and Data Elements Definition Reference Number of adverse determinations upheld upon request for internal See definition of upheld decision above. review (Do not include additional voluntary levels of reviews.) Number of final adverse determinations overturned upon request for See definition of overturned decision above. external review (Do not include additional voluntary levels of reviews.) © 2014 National Association of Insurance Commissioners 18 Attachment B Line # IR4 IR5 ER1 Terms and Data Elements Definition Reference Does the company have an additional voluntary level of review for See definition of voluntary review level above. grievances? Y/N (Applies to all plans and all metal levels) Number of customer requests for internal reviews See definition of grievance for non-adverse determination. of grievances not involving adverse determinations Number of customer requested appeals on final adverse See definition of external review above. determinations to an external review organization © 2014 National Association of Insurance Commissioners 19 Attachment B Line # ER2 ER3 Terms and Data Elements Number of final adverse determinations upheld upon request for external review Number of final adverse determinations overturned upon request for external review Definition Reference See definition of upheld decision above. See definition of overturned decision above. © 2014 National Association of Insurance Commissioners 20 Attachment B B C 3 Policy Administration 15 1 Earned premiums for Reporting Year 2 Number of policies issued Number of Applications received by the carrier that 3 did not result in an issued policy 4 Number of lives on policies issued 5 Member months for policies issued Number of policy terminations and cancellations 6 initiated by consumer Number of policy terminations and cancellations due 7 to non-payment of premium. Number of lives impacted on terminations and 8 cancellations initiated by the consumer Number of lives impacted on policies terminated and 9 cancelled due to non-payment 10 Number of carrier initiated rescissions Number of lives impacted by carrier initiated 11 rescissions 16 17 1 Number of claims received 7 8 9 10 11 12 13 14 18 19 20 21 22 23 24 25 26 27 28 E F G For all Individual comprehensive major medical and managed care (EHB compliant) policies - other than multi-states policies Health insurance coverage other than transitional, grandfathered, multi-state, or student 2 4 5 6 D H I J K L M N O P Q R S T U V W X In Exchange (Note: there are two sections with the same questions. In Exchange would not include large group or student coverage. Out-of Exchange would not include Multi-State) 1 Claims Administration 2 Number of claims submitted by network providers Number of claims submitted for by out of network providers 4 Number of claim denials for in-network claims Stratification by number of days -- 0-15, 16-30, 31 to 5 45, 46 to 90, 91 to 180, 181 to 360, 360+ 3 6 Number of claim denials for out-of-network claims Stratification by number of days -- 0-15, 16-30, 31 to 45, 46 to 90, 91 to 180, 181 to 360, 360+ 8 Number of paid claims for in-network services Stratification by number of days -- 0-15, 16-30, 31 to 9 45, 46 to 90, 91 to 180, 181 to 360, 360+ 7 10 Number of paid claims for out-of-network services 11 Stratification by number of days -- 0-15, 16-30, 31 to 45, 46 to 90, 91 to 180, 181 to 360, 360+ 12 Number of claims delayed due to untimely issuance of policy (Perhaps as an interrog: If more than 5% of your claims are paid/denied past 90 days, please explain) (c) 2014 National Association of Insurance Commissioners Bronze Silver Gold Platinum For all Small Group Health Insurance Coveage comprehensive major medical and managed care (EHB compliant) policies - other than transitional, grandfathered,or multi-state policies Bronze Silver Gold Platinum Multi-State (Individual) Catastrophic Bronze Silver Gold Multi-State (Small Group) Platinum Bronze Silver Gold Platinum Y Z Attachment B B C 3 29 12 Claims Paid Incurred Claims 30 13 Insured/beneficiary co-payment responsibility 31 14 Insured coinsurance responsibility 32 15 Insured deductible responsibility 33 Consumer Requested Internal Reviews Number of customer requests for internal reviews of grievances involving adverse benefit determinations 1 (Do not include additional voluntary levels of 34 reviews.) 36 Number of adverse benefit determinations upheld 2 upon request for internal review (Do not include additional voluntary levels of reviews.) Number of adverse benefit determinations 3 overturned upon request for internal review (Do not include additional voluntary levels of reviews.) Does the company have an additional voluntary level of review for grievances? Y/N (Applies to all plans and all metal levels) Number of customer requests for internal reviews of 5 grievances not involving adverse benefit determinations 4 37 38 39 Consumer Requested External Reviews 40 Number of customer requested appeals on final 1 adverse benefit determinations to an external review organization 2 Number of final adverse benefit determinations upheld upon request for external review 3 Number of final adverse benefit determinations overturned upon request for external review 41 42 43 E F G For all Individual comprehensive major medical and managed care (EHB compliant) policies - other than multi-states policies Health insurance coverage other than transitional, grandfathered, multi-state, or student 2 35 D H I J K L M N O P Q R S T U V W X In Exchange (Note: there are two sections with the same questions. In Exchange would not include large group or student coverage. Out-of Exchange would not include Multi-State) 1 Total number of external reviews of final adverse 4 benefit determinations which either party appeals after the external review decision (c) 2014 National Association of Insurance Commissioners Bronze Silver Gold Platinum For all Small Group Health Insurance Coveage comprehensive major medical and managed care (EHB compliant) policies - other than transitional, grandfathered,or multi-state policies Bronze Silver Gold Platinum Multi-State (Individual) Catastrophic Bronze Silver Gold Multi-State (Small Group) Platinum Bronze Silver Gold Platinum Y Z Attachment B B C Bronze 3 10 Policy Administration 1 Earned premiums for Reporting Year 2 Number of policies issued Number of Applications received by the carrier that 3 did not result in an issued policy 4 Number of lives on policies issued 5 Member months for policies issued Number of policy terminations and cancellations 6 initiated by consumer 7 11 12 13 14 15 8 9 Number of policy terminations and cancellations due to non-payment of premium. Number of lives impacted on terminations and cancellations initiated by the consumer Number of lives impacted on policies terminated and cancelled due to non-payment 10 Number of carrier initiated rescissions 11 Number of lives impacted by carrier initiated rescissions Claims Administration 16 17 1 Number of claims received 18 2 Number of claims submitted by network providers 19 20 21 22 23 24 25 26 27 F G H For all Individual comprehensive major medical and managed care (EHB compliant) policies - other than multi-states policies Health insurance coverage other than transitional, grandfathered, multi-state, or student 2 7 8 9 E I J K L M N O P Q R S T U V W X Y Z AA AB AC AD Out of Exchange (Note: there are two sections with the same questions. In Exchange does not include large group or student coverage. Out-of Exchange does not include Multi-State) 1 4 5 6 D Number of claims submitted for by out of network providers 4 Number of claim denials for in-network claims 3 5 Stratification by number of days -- 0-15, 16-30, 31 to 45, 46 to 90, 91 to 180, 181 to 360, 360+ 6 Number of claim denials for out-of-network claims 7 Stratification by number of days -- 0-15, 16-30, 31 to 45, 46 to 90, 91 to 180, 181 to 360, 360+ 8 Number of paid claims for in-network services 9 Stratification by number of days -- 0-15, 16-30, 31 to 45, 46 to 90, 91 to 180, 181 to 360, 360+ 10 Number of paid claims for out-of-network services 11 Stratification by number of days -- 0-15, 16-30, 31 to 45, 46 to 90, 91 to 180, 181 to 360, 360+ 12 Number of claims delayed due to untimely issuance of policy (Perhaps as an interrog: If more than 5% of your claims are paid/denied past 90 days, please explain) 28 29 12 Claims Paid Incurred Claims (c) 2014 National Association of Insurance Commissioners Silver Gold Platinum For all Small Group Health Insurance Coveage comprehensive major medical and managed care (EHB compliant) policies - other than transitional, grandfathered,or multi-state policies Bronze Silver Gold Platinum Grandfathered Large Group Small Group Catastrophic Individual For all Large Group comprehensive major medical and managed care (Minimum Essential Coverage) policies For Student Coverage Transitional Plans Large Group Small Group Mini-Med Individual Large Group Small Group Short Term Individual Attachment B B C D E F G H I J K L M N O P Q R S T U V W X Y Z AA AB AC AD Out of Exchange (Note: there are two sections with the same questions. In Exchange does not include large group or student coverage. Out-of Exchange does not include Multi-State) 1 For all Individual comprehensive major medical and managed care (EHB compliant) policies - other than multi-states policies Health insurance coverage other than transitional, grandfathered, multi-state, or student 2 3 30 13 Insured/beneficiary co-payment responsibility 31 32 14 Insured coinsurance responsibility 15 Insured deductible responsibility Consumer Requested Internal Reviews (Grievances) 33 1 34 35 36 Number of customer requests for internal reviews of grievances involving adverse benefit determinations (Do not include additional voluntary levels of reviews.) Number of adverse benefit determinations upheld 2 upon request for internal review (Do not include additional voluntary levels of reviews.) Number of adverse benefit determinations 3 overturned upon request for internal review (Do not include additional voluntary levels of reviews.) 38 Does the company have an additional voluntary level of review for grievances? Y/N (Applies to all plans and all metal levels) Number of customer requests for internal reviews of 5 grievances not involving adverse benefit 39 Consumer Requested External Reviews 40 Number of customer requested appeals on final 1 adverse benefit determinations to an external review organization 4 37 2 Number of final adverse benefit determinations upheld upon request for external review 3 Number of final adverse benefit determinations overturned upon request for external review 41 42 43 Total number of external reviews of final adverse 4 benefit determinations which either party appeals after the external review decision (c) 2014 National Association of Insurance Commissioners Bronze Silver Gold Platinum For all Small Group Health Insurance Coveage comprehensive major medical and managed care (EHB compliant) policies - other than transitional, grandfathered,or multi-state policies Bronze Silver Gold Platinum Grandfathered Large Group Small Group Catastrophic Individual For all Large Group comprehensive major medical and managed care (Minimum Essential Coverage) policies For Student Coverage Mini-Med Transitional Plans Large Group Small Group Individual Large Group Small Group Short Term Individual Attachment C Market Regulation and Consumer Affairs (D) Committee Action Items of the 2014 Market Regulation Summit Progress Status – Dec. 17, 2014 Shaded Areas are Complete Market Regulation and Consumer Affairs (D) Committee 1. 2. 3. 4. 5. 6. 7. 8. Action Items and Deadlines for Completion Action Items 7-31 8-31 9-30 10-31 In response to Federal Insurance Office (FIO) recommendations, provide FIO X information regarding how states use the Handbook and how it is updated. (Addressed in draft memo to Government Relations Leadership Council) In response to FIO recommendations, provide FIO detail on how states share information with each other: NAIC X systems, NAIC bulletin boards, PICS notifications, informal conversations at meetings, review of publicly available resources, etc. (Addressed in draft memo to Government Relations Leadership Council) In response to FIO recommendations, develop specific minimum qualifications for contractors. In response to FIO recommendations, review and update core competency addressing contract examiners. In response to FIO recommendations, recognize the evolution of states’ market X conduct examiners to market conduct specialists. (Addressed in draft memo to Government Relations Leadership Council) In response to FIO recommendations, ensure contractors are required to provide status reports to state insurance regulators, and send a state employee to visit contractors on site at examination. (Addressed in draft memo to Government Relations Leadership Council) In response to FIO recommendations, develop a list of contractors for X registration at the NAIC similar to what is done for financial contract examiners. Continue the NAIC partnership with the X National Conference of Insurance Legislators (NCOIL). © 2014 National Association of Insurance Commissioners 1 11-30 12-31 2015 X X X Attachment C 9. Focus on creating a uniform process and state accountability to the process as a starting point for market regulation accreditation. 10. Obtain state statutes that reference the use of the Market Regulation Handbook. X X Market Information Systems (D) Task Force Action Items and Deadlines for Completion Action Items 7-31 8-31 9-30 10-31 11-30 1. Ensure completion of Market Information Systems (D) Task Force action plan. 2. Develop a system/database that better shares information on actions other than examinations. 3. Analyze the data currently in the NAIC Market Information Systems to see what was entered and what training needs to occur to ensure better data quality (if needed.) 4. Review the NAIC Market Information Systems and develop a way that analysis can be performed on an insurance group basis instead of limited to the individual company (CoCode) basis. 5. Find a way to allow state users of I-SITE data to query the NAIC Market Information Systems. 6. Monitor how state data entry to the NAIC Market Information Systems has changed after the action plan has been implemented. 12-31 2015 X X X X X X Market Conduct Examination Standards (D) Working Group Action Items and Deadlines for Completion Action Items 7-31 8-31 9-30 10-31 1. Review the Core Competencies to determine which competencies need to be X updated. 2. Update the core competency addressing contract examiners. Ensure contractors are required to provide status reports to state insurance regulators, and send state employees to visit contractors on site at examinations. 3. Consider revising the sampling procedures outlined in the Market Regulation Handbook to provide for greater flexibility, © 2014 National Association of Insurance Commissioners 2 11-30 X X 12-31 2015 Attachment C as appropriate. 4. Collect and then post a list of best practices for state use of the Market Regulation Handbook on MyNAIC.org. 5. Review Chapter 16 of the Market Regulation Handbook (General Examination Standards), and determine which standards would not be applicable to all exams so they can be moved to the appropriate chapters. 6. Reevaluate the use of the 10% and 7% tolerance thresholds outlined in the Market Regulation Handbook. X X X Market Analysis Procedures (D) Working Group 1. 2. 3. 4. 5. 6. 7. 8. 9. Action Items and Deadlines for Completion Action Items 7-31 8-31 9-30 10-31 Develop routine trending reports for the analysis of Market Conduct Annual Statement (MCAS) data. Develop a standard process for determining MCAS outliers at the state level. Identify ways to notify companies that they are attesting to the accuracy of MCAS data and that entering incorrect data may result in regulatory actions. This may include a review of the attestation language. X (Because many incorrect filings are related to life insurance, MAP should notify ACLI of potential regulatory actions for incorrect filings.) Explore ways to obtain more current market regulation data. Establish a process for the better coordination between states when issues are identified during the analysis of the MCAS data. Establish a process for the better coordination between states when validation issues are identified during the MCAS filing process. Review the market analysis process, and determine what analysis can be done on a more frequent basis than annually. Review analysis-related chapters of the Market Regulation Handbook on a rotating basis to ensure information is current. Investigate ways to better tie complaints to X © 2014 National Association of Insurance Commissioners 3 11-30 12-31 2015 X X X X X X X Attachment C premium amounts. (Re-assigned from the Market Information Systems (D) Task Force.) Market Actions (D) Working Group 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. Action Items and Deadlines for Completion Action Items 7-31 8-31 9-30 10-31 Distribute the Market Actions (D) Working Group policies and procedures to all X regulators who participated in the Summit, and make sure the procedures are available on MyNAIC.org. Make sure a summary of ongoing actions is available to Collaborative Action X Designees after each Working Group meeting or call. Discuss ways to make the annual National Analysis Project more of an ongoing X process. Explore ways to make the Working Group more proactive rather than reactive, such as X increasing Working Group-dedicated resources. Develop a process to fast-track referrals to the Working Group that are close to settlement. Prepare a summary report of the National Analysis Process that shows what activities occurred because of the national analysis. Explore ways to look at groups (and not just individual companies) on a national level. (Discussions Ongoing) Consider ways to increase participation of all states, such as (a) clarifying that a state’s referral to the Working Group does not commit the referring state to a role as a X lead or managing lead state and (b) combining the NAIC’s Exam Tracking Systems and Market Initiative Tracking System for enhanced collaboration through the Working Group. (Discussions Ongoing) Discuss the Working Group’s structure and membership to evaluate whether X membership on a rotational basis would be desirable. (Discussions Ongoing) Review collaborative actions-related chapters of the Market Regulation X Handbook on a rotating basis to ensure information is current. (Discussions © 2014 National Association of Insurance Commissioners 4 11-30 12-31 X X X 2015 Attachment C Ongoing) NAIC Education & Training Department Action Item and Deadline for Completion Action Item 7-31 8-31 9-30 10-31 1. Develop a training program on how to properly use the Market Regulation Handbook. 11-30 12-31 2015 X NAIC Market Regulation Department Action Items and Deadlines for Completion Action Items 7-31 8-31 9-30 10-31 1. Conduct annual webinars on Market X Regulation Handbook updates. 2. Conduct a webinar regarding Market Actions (D) Working Group policies and procedures. (On demand webinar developed/notice needs to be sent to regulators) 11-30 12-31 2015 12-31 2015 X X NAIC Information Systems Division Action Items and Deadlines for Completion Action Items 7-31 8-31 9-30 10-31 1. Train states on ways to query the data in the NAIC Market Information Systems. 2. Develop training and webinars regarding submission of data to each of the NAIC Market Information Systems. 3. Identify and maintain a list of NAIC and X state contacts responsible for data entry. W:\National Meetings\2014\Fall\Cmte\D\MR Summit Status\MR Action Items Final Status 121714.docx © 2014 National Association of Insurance Commissioners 5 11-30 X






© Copyright 2026