
Evidence for Nonclonal Hematopoietic Progenitor
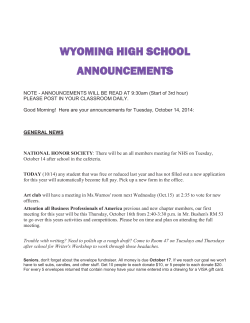
From www.bloodjournal.org by guest on December 22, 2014. For personal use only. Evidence for Nonclonal Hematopoietic Progenitor Cell Populations in Bone Marrow of Patients With Myelodysplastic Syndromes By Haruhiko Asano, Haruhiko Ohashi, Masatoshi Ichihara, Tomohiro Kinoshita, Takashi Murate, Miya Kobayashi, Hidehiko Saito. and Tomomitsu Hotta Clonality of marrow hematopoietic progenitor cells in myelodysplastic syndromes (MDSI wasanalyzed by X-chromosome inactivation pattern using polymerase chain reaction (PCR). Fivefemale patients were included in this study; two with refractory anemia (RA) and three with RA with excess blasts (RAEBI. They were heterozygous for BstXl restriction fragment length polymorphisms (RFLP)of the X-chromosome-linked phosphoglycerate kinase (PGK) gene. In each patient, erythroid and nonerythroid colonies, grown in the presence of erythropoietin and granulocyte-macrophage colony-stimulating factor (GM-CSFI, exhibited no remarkable difference in clonal constitution. Two patients showed only one methylation pattern, suggesting the monoclonal origin of hematopoietic progenitor cells.Coloniesof two other patients exhibited predominant and minor methylation patterns in PGKgene, indicating that nonclonal progenitor cells remain a minor population. The bone marrow of one patient appeared to contain a greater proportion of nonclonal progenitors. Stem cell factor (SCF), a potent colony stimulating factor, enhanced both erythroid and nonerythroid colony formation. However, it did not notably alter the clonal constitutions. We conclude that nonclonal hematopoietic progenitor cells canpersist in a substantial number of MDS patients. 0 1994 by The American Society of Hematology. T applicability forclonal studies, evenfor patients with no genetic markers. Using the method, many investigators disclosed the clonal nature of MDS,".''~?'' as well as other neoplastic Because X-inactivation the pattern is sustained in the daughter cells in a highly stable manner,'h clonal analysis of individual colonies grown in culture should show the clonality of hematopoietic progenitor cells. Inclusion of polymerase chain reaction (PCR) in the genetic analysis has made it possible to examine the clonality of a small cell population.?* In this study, we wish to clarify the clonalorigin of MDS marrowhematopoieticprogenitor cells. X-inactivation patterns of single erythroid (burst-forming units-erythroid[BFU-E]) and nonerythroid colonies wereanalyzedusing PCR. Resultssuggestthatnonclonal progenitor cells remain in a substantial number of MDS patients, which might be important implication for the therapy of MDS. HEMYELODYSPLASTICsyndromes(MDS)are a morphologically defined heterogeneous group of stem cell disorders characterized by maturational defects of marrow hematopoietic cells, resulting in peripheral blood cytopenias.'.? Clonal hematopoiesis isanothercharacteristicin MDS.' Analyses using X-linked isoenzyme system of glucose-6-phosphate dehydrogenase (G6PD) revealed the clonal origin of peripheral blood cells of MDS patients."' These studies have provided valuable information on the clonality ofhematologicdisorders because itisapplicable for the analysis of erythrocytes and platelets lacking nuclei. However, the rarity of females with heterogeneity of G6PD has limited further study. Cytogenetic analyse^"'^ and studies of nonspecific gene rnutation~,'~ further clarifyingthe clonal nature of MDS, have been powerful tools for direct demonstration of the clonal population. If the karyotypic (genetic) changes occurred after the clonal evolution, the dataof such analyses might not reflect the real clonality in the patient. For thatreason,reportsonthemosaicism of normal and abnormal karyotypes in hematopoietic progenitor cells"'.' I do not necessarily provide evidence for the presence of normal clone in MDS. In any event, investigators have targeted mainly mature peripheralblood cellsfor clonalanalysis. Adequate information on the clonality of marrow progenitor cells has not been available in MDS. Vogelstein et al" established an elegant method for clonality analysis by means of DNA polymorphisms atX-linked loci, which uses random X-chromosome inactivation in females." This strategyhas the great advantage of general From the First Department of Internal Medicine, and the Second Department of Anatomy, Nagoyu Universiv School of Medicine, Nagoya, Japan. Submitted December 2, 1993; accepted March 23, 1994. Address reprint requests to Haruhiko Asano, MD, the First Department of Internal Medicine, Nagoya University School of Medicine, 65 Tsurumai-cho, Showa-ku, Nagoyu 466, Japan. The publication costs of this article were defrayed in part by page chargepayment. This article must thereforebeherebymarked "advertisement" in accordance with 18 U.S.C. section 1734 solely to indicate this fact. 0 1994 by The American Society of Hematology. 0006-4971/94/8402-0006$3.00/0 588 MATERIALS AND METHODS Patients. Five female patients with primary MDS were included in this investigation (Table 1); two with refractory anemia (RA) and three with RA with excess blasts (RAEB) according to the FrenchAmerican-British(FAB) nomenclature.'' Theywereheterozygous for BstXI restriction fragment length polymorphisms (RFLP) of the X-chromosome gene phosphoglycerate kinase ( PG K ) and received neither chemotherapy nor bone marrow transplantation before the study. Their marrow and peripheral blood samples were obtained with informed consent. As a control, two healthy female volunteers whowereheterozygousforthe RFLP were also included in this study, after informed consent was obtained. Cell preparation. Light-density mononuclear cells (MNC) were obtained from marrow and peripheralblood samples by Ficoll-Paque (Pharmacia, Uppsala, Sweden) density gradient centrifugation. Marrow MNC were washed and resuspended in RPM1 1640 (GIBCO, GrandIsland,NY) with 20% fetal calf serum(FCS,Boehringer Mannheim, Mannheim, Germany) at I X IOh/mL and incubated for 2 hrs at 37°C in a fully humidified atmosphere of 5 % CO,, then nonadherent cells were collected. Polymorphonuclear cells (PMN) were recovered from the peripheral blood erythrocyte pellet by removal of lysed red cells after incubation in Tris.NH,CI buffer. The purity of the PMN obtained was 94.0% 2 3.5% (mean t SD) by morphologicexamination. In somepatients,Tlymphocytes were separated from peripheral blood MNC by agglutination with sheep Blood, Vol 84, NO 2 (July 15). 1994: pp 588-594 From www.bloodjournal.org by guest on December 22, 2014. For personal use only. EMATOPOIETIC NONCLONAL 589 IN MDS Table 1. Clinical and Hematologic Data of Patients at theTime of Study Peripheral Blood UPN 1 2 3 4 5 AgeISex 46/F 71F 71F 75F 68/F Diagnosis* RA RA 2.9 RAEB RAEB RAEB Time After Diagnosis (mo) 13 9 26 66 13 Bone Marrow WBC c1oSn) 2.5 3.3 Blast 1%) 0 0 2 3.8 1.1 2 0 12.7 Hb WdL) Platelets 12.1 7.1 8.7 6.6 4.7 9 6 ( 109/u 42 99 43 Blast (96) <l <l 4 8 Karyotype 46,XX 46,XX 46,XX 46,XX 46,XX Abbreviations: UPN, unique patient number; Hb, hemoglobin. * French-American-British(FAB) classification. redblood cells (Kyokuto, Tokyo, Japan). Immunohistochemical analysis showed 93.7% 2 1.5% of the cells obtained were CD2+. Hematopoietic growth factors. Recombinant human erythropoietin (EPO) and stem cell factor (SCF) were generous gifts from Kirin Brewery CO(Tokyo, Japan). They were used at a concentration of 100 ng/mL and 4 UlmL, respectively. Recombinant human granulocyte-macrophage colony-stimulating factor (GM-CSF) (100 ng/ mL) was a generous gift of Sumitomo Pharmaceutical (Hyogo, Japan). Cell culture. Cells from MDS and control marrow samples were grown at 5 x l@/mL in 1 mL of Minimum Essential Medium-a (MEM-a, GIBCO) containing 1.1% methylcellulose supplemented with 20% FCS, 1% dialyzed bovine serum albumin (BSA; Sigma m o m of 2-mercaptoethanol Chemical CO, St Louis, MO), 5 x (2-ME; Nacalai Tesque, Kyoto, Japan), EPO, and GM-CSF, either with or without SCF in a 35-mm culture dish (Nunc, Naperville, Ill) for 14 days at 37°C in a fully humidified atmosphere of 5% CO2. After 14 days of incubation, cell groups composed of more than 40 cells were scored as colonies. DNA extraction and processing. Individual red-colored (erythroid) and other (nonerythroid) colonies were randomly plucked by hand with a micropipette and immediately placed in 200 pL buffer containing 1% sodium dodecyl sulfate (SDS), 2 mmol/L EDTA, 20 pmoVL Tris (pH 7.4), and 1 mg/mL proteinase K (Boehringer Mannheim) followed by incubation for 12 hours at 37°C. Highmolecular weight DNA, extracted from each colony with phenol/ chloroform24using 44 pg of glycogen (Boehringer Mannheim) as a DNA container, was equally divided into two aliquots; one was digested by 40 U of HpaII, methylation-sensitive restriction endonuclease (all restriction enzymes except BstXI were purchased from Boehringer Mannheim) for more than 6 hours at 37T, and the other was left undigested. Similarly, high-molecular weight DNA of blood T lymphocytes or MNC and PMN was extracted and two aliquots containing about 100 ng of DNA were obtained. One was digested by HpaII in the same condition as described earlier. The DNA after HpaII-cutting was precipitated in ethanol and the pellet was then rinsed once with 70% ethanol. PCR analysis of PGK gene. Clonality analysis was conducted according to the method established by Gilliland et alZZwith some modifications. DNA from each colony and peripheral blood samples both with and without HpaII digestion were added to 50 pL of a solution (16.6 mmoVL ammonium sulfate, 67 mmol/L Tris.HC1 [pH 8.8 at25"C],6.7 mmoVL MgClZ, 10 mmoVL 2-ME, 6.7 pmoVL EDTA, 1.5 mmoVL dNTPs, and BSA at 170 pg/mL) with a set of outer primers at 1 pmoVL each and 1 U of Taq polymerase (Boehringer Mannheim). Samples were amplified for 35 cycles (1 minute, 94°C; 1 minute, 55°C; 2 minutes, 72°C). One tenth of each product was further amplified for 50 cycles in the same solution with a set of inner primers. Sequences of the two sets of primers were described elsewhere.22Following the amplification, each product was digested by 40 U of BstXI (New England Biolabs, Beverly, MA) at 55°C for more than 6 hours, then electrophoresed in 2% agarose geland stained with ethidium bromide. Determination of clonal pattern of individual colonies. The clonal origin of each colony was determined on the basis of the band pattern of amplified DNA with precutting by HpaII. To assess the band pattern, artificial cell-mixtures were prepared as follows. Blood mononuclear cells were obtained from two healthy male volunteers with informed consent; one had PGK gene lacking the BstXI site, and the other, containing the site. Cells were mixed at the ratios of 1W0, 95:5, 90:10, 85:15, 80:20, 70:30, 60:40, 50:50, 40:60, 30:70, 20:80, 15:85, 10:90, 5:95, and 0:100, respectively. DNA extracted from each cell-mixture was amplified and then electrophoresed in the same condition as described earlier (Fig 1). The band pattern of amplified DNA from each colony, with precutting by HpaII, was compared with bands in the artificial cellmixtures. Band patterns between 40:60 and 60:40 were regarded as ambiguous, and the others as having the inactivated allele without BstXI site (pattern A, dominant band at 530 bp) or withthe site (pattern B, dominant band at 433 bp). The complete digestion with HpaII and BstXl was confirmed using the male DNA containing the BstXI site. Each step of DNA digestion and the amplification was performed in the same condition as noted above. The amplification of the DNA cut with HpaII failed (not shown), indicating the complete digestion withthe enzyme. BstXI digestion of products from the DNA undigested with HpaII yielded a single 433-bp band as in the first lane from the left in Fig 1, which showed that complete digestion with BstXI was achieved. Clonal analysis of blood PMN by Southern blotting. According 20 pg DNAwas tothemethod established by Vogelstein et completely digested with BgA, BgAI, and EcoRI, then equally divided into two aliquots; one was further cleaved with HpaII, and the other was left undigested. Each aliquot of DNA was electrophoresed through 1.5% agarose gel, transferred to a nylon membrane, and hybridized with a 0.8-kbp genomic probe containing the 5' region of the PGK gene (provided by Dr J. Singer-Sam, Beckman Research Institute of the City of Hope, Duarte, CA). RESULTS Clonality of erythroid progenitors. In the presence of EPO and GM-CSF, erythroid (BFU-E) colonies were formed in all five MDS patients, as well as two control individuals (Fig 2A), and were randomly plucked. Although each colony from patients was generally small-sized, DNAwas effectively amplified by PCR (data not shown). The clonal origin could be determined even if the colony was composed of less than 100 cells. In two patients (UPN 3 and 4), all the erythroid colonies From www.bloodjournal.org by guest on December 22, 2014. For personal use only. ASANO ET AL 590 Fig 1. Band patterns of PGK gene from artificial cell-mixtures for determining the clonal origin of individual colonies. Because of the formation of heteroduplex,a the intensity of upper bands is high. - YO cells containing theBstXl site examined had the same X-inactivation pattern (Table 2). yielding a dominant band at 530 bp (pattern A) as illustrated in Fig 3A. Colonies of two other patients (UPN 1 and 2) had extremely skewed inactivation patterns; most of them exhibited pattern A, while four of 25 colonies in UPN 1 and two of 22 in UPN 2 produced a dominant band at 433 bp (pattern B). In UPN 5 , five of 18 colonies examined were pattern A and other 13, pattern B (Table 2 and Fig 3B). In control individuals (Cl and C2), the ratios of pattern A to B of the colonies were 8: 1 I and 8:21, respectively (Table 2). Representative band patterns in C2 are shown in Fig 3C. Clonality of nonerythroid progenitors. Nonerythroid colonies grown in the presence of EPO and GM-CSF (Fig 2B) were randomly plucked andtheir clonal origin was determined. In patients UPN 3 and 4, all of the nonerythroid colonies had only one inactivation pattern (Table 2 and Fig 4A). The colonies of UPN I and 2 gave three band patterns: pattern A, pattern B, and ambiguous. The ratios were skewed B A T T 1 2 3 4 UPN 5 C l C 2 1 2 3 4 5 C l C 2 UPN Fig 2. Erythroid (A) and nonerythroid(B) colony growthin each patient and normal individual. Adherent cell-depleted marrow mononuclear cells were stimulated by bothEPO and GM-CSF, and either(W) with or (0) without SCF. Data represent mean colony number grown from lo5 mononuclear cells. The error bars depict1 SD from the mean. From www.bloodjournal.org by guest on December 22, 2014. For personal use only. MATOPOIETIC NONCLONAL IN MDS 591 Table 2. X-Chromosome Inactivation Pattern of Individual Colonies Pattern of BstXl RFLP Erythroid FAB Nonerythroid SCF' A B Ambiguous A - - 7 + - 20 5 + 7 Control ( C l ) - 8 5 Control (C2) - 4 5 2 2 0 0 0 0 13 11 11 14 21 23 0 + 21 25 20 23 13 17 15 18 15 16 18 21 15 13 4 4 10 6 10 9 UPN RA l + RA 2 - + 3 RAEB 4 RAEB RAEB 5 - + + a 7 0 1 0 0 0 0 0 0 0 0 0 0 0 B Ambiguous 1 2 3 2 0 1 0 2 2 0 0 0 0 1 13 17 5 13 16 19 0 0 l 1 4 1 4 1 Clonality analysis of erythroid and nonerythroid colonies grown in the presence of both EPO and GM-CSF, and either with or without SCF. The clonal origin of each colony was determined on the basis of the ratio of amplified DNA. The ratio of between 40:60 and 60:40 in artificial cell-mixtures (Fig 1)was regarded as ambiguous, and the others as having the inactivated allele without the BstXl site (pattern A) or with the site (pattern B). The ambiguous pattern may result from contamination by cells having another clonality. The diffuse nature of the nonerythroid colonies presumably leads to the plucking of cells with a differentclonal origin. x Symbols and - represent the stimulation with and without the factor, respectively. + as 15: 1: 1 (UPN 1) and 1 5 3 2 (UPN 2) (Table 2). In UPN 5 , the ratio was also skewed as 4: 13:1 (Table 2 and Fig 49). In controls, three band patterns were observed (Table 2 and Fig 4C). The clonal constitutions of nonerythroid colonies of all patients and control individuals were similar to those of erythroid. Efects (.f SCF on progenitor cell clortaliv i n MDS. SCF was added to the culture system to investigate whether it could alter the clonal constitution of colonies in MDS. Among patients, colonies of both erythroid and nonerythroid lineages grew approximately two to six times more in the presence of SCF (Fig 2AB), which was observed also in two control individuals. The clonal origin was determined for colonies plucked randomly(Table 2). In patients and controls alike, the clonal constitutions of both erythroid and nonerythroid colonies were similar to those grown without SCF. However, one of 14 nonerythroid colonies in UPN 4 carried a different pattern of X-inactivation (Table 2). indicating the presence of nonclonal hematopoietic progenitor cells in the marrow. Clonal acquisition ann!\:ed t>v peripheral blood cells. It is necessary to know if the clonal nature of MDS marrow hematopoietic progenitor cells was theresult of acquired clonal evolution or of extreme lyonization. Clonality of peripheral blood PMN and either T lymphocytes or MNC was analyzed by means of PCR, andtheresults are shown in Table 3 and Fig S. In PMN of three patients (UPN I , 3 and 4). DNA precut with HpaII produced only an upper (530bp) band, indicating PMN were of monoclonal origin. The T-lymphocyte DNA gave rise to extremelyskewed (oligoclonal) band patterns in UPN I and 3, which were composed of dominant upper (530-bp) and minor lower (433bp) bands, suggesting that their T lymphocytes included a smallnonclonal population. Such a difference in clonality of PMN and T lymphocytes indicated that acquired clonal events were going on in their hematopoietic system. In UPN 4, the T-lymphocyte DNA also yielded only the upper band, indicating monoclonal origin. The X-inactivation pattern of PMN from UPN2 was oligoclonal, but the MNCDNA produced an unskewed polyclonal band pattern, which im- Fig 3. X-chromosome inactivation pattern of individual erythroid colonies. Representative band patterns are illustrated. All bands in H(+) lanes were derived from DNA precut with Hpall. (A) AnRAEB patient (UPN 3). DNA in H(+) lanes yielded a band at 530 bp, indicating inactivated X-chromosomes of cells in the colonies lacked BstXl site of PGK gene. (B) An RAEB patient (UPN 5).A dominant band at433 bp isobserved in each H(+) lane, indicating inactivated X-chromosomes contained the BstXlsite. (C) A normal individual (Cl). Both patterns are noticed. From www.bloodjournal.org by guest on December 22, 2014. For personal use only. ASANO ETAL 592 C B A * Fig 4. X-inactivation pattern of individual nonerythroid colonies. Representative band patterns are illustrated. All bands in H(+) lanes were derived from DNA precut with Hpall. (A) An RAEB patient (UPN 4). DNA in H(+) lanes yielded a band at 530 bp. (B) An RAEB patient (UPN 5). A dominant band at 433 bp is observed in each H(+) lane. (C) A normal individual (C21. Three band patterns are noticed. ‘Denotes ambiguous band pattern. A dominant 433-bp band in each H(+) lane is often accompanied by a faint 530-bp band, which may be explained either by the contamination of nonclonal cells or by the escape from restriction endonuclease digestion. Slight contamination of alleles containing the BsrXl site by the site-lacking alleles might yield the 530-bp band, which was strengthened by the formation of heteroduplex.= plied that acquired clonal evolution in hematopoiesis took place in the marrow. UPN 5 , who had a greater proportion of nonclonal marrow hematopoietic progenitor cells than any other patients, showed almost the same polyclonal patterns in PMN and MNC. Thus, despite the presence of nonclonal hematopoietic progenitor cells, peripheral bloodPMNofUPN 1 and 2 showed monoclonal and oligoclonal appearances, respectively. To clarify this discrepancy, we further performed clonal analysis of PMN of these patients by Southern blotting. PMN of UPN 1 appeared to be monoclonal and those of UPN 2 had an extremely skewed clonal constitution (Fig 6), which were similar to the results of PCR-based clonal analysis. DISCUSSION To know the clonal constitution of MDS marrow hematopoietic progenitor cells, we performed a PCR-based clonal analysis for colonies grown in culture. X-chromosome inactivation patterns were determined on individual erythroid and nonerythroid colonies. Nonclonal hematopoietic progenitor cells were present in four out of five patients tested. In patients UPN 3 and 4, few, if any, nonclonal progenitor cells were detected; in UPN 1 and 2, nonclonal cells formed a small progenitor cell population, while UPN 5 had more of these cells. These clonal constitutions of marrow hematopoietic progenitor cells were well reflected in the clonality of circulating PMN. PMN exhibited monoclonal or extremely skewed (oligoclonal) band patterns in UPN I , 2, 3, and 4, Table 3. Clonal Patterns of Peripheral Blood Cells Cell Population UPN FAB PMN T Cells MNC 1 RA RA RAEB RAEB RAEB M 0 - 0 - P M M P 0 M - - P 2 3 4 5 - PCR-based clonality analysis was performed on peripheral blood PMN and either T cells or MNC. Abbreviations: M, monoclonal band pattern; 0, oligoclonal band pattern; P, polyclonal band pattern; -, not available. while PMN of UPN 5 exhibited a polyclonal band pattern. Itisworth noting that, despite the presence of nonclonal marrow progenitors, PMN of UPN 1 showed a monoclonal band pattern. This apparent discrepancy could be caused by the sensitivity of our PCR-based clonal analysis or by selective release of monoclonal cells into the peripheral blood. Specifically, the amplification ofDNA from artificial cellmixtures containing 85% cells whose X-chromosomes lacked the BstXl site apparently yielded only one bandat 530 bp (Fig l).It isvery probable that if the nonclonal hematopoietic progenitor cell population is small, the circulating PMN show a monoclonalbandpattern. Our results indicated that in MDS the monoclonal appearance of PMN PCR”’,?’ by or by Southern would not necessarily represent the total marrowreplacement by clonal progenitor cells. We demonstrated that erythroid and nonerythroidprogenitors of MDS had a similar clonal constitution, which indicates that the partially committed or earlier stem cells capable of differentiating into at least both erythroid and myelomonocytic lineages were affected. In MDS, clonal involvement of erythroid cells, whose clonality was not fully studied because of the anucleated nature of erythrocytes, has beenreported to be always accompanied by myeloidcell i n ~ o l v e m e n t . ~ ~This ~ ~ “ ’was ~ ’ ’confirmed again in the present study. Many cytokines have been reported toimprove the cytopenias of MDS Whether they can bring about qualitative improvement (polyclonal hematopoiesis) in MDS is a matter of consideration. In the present study, we added SCF to our culture system and analyzed the clonal origin of resulting colonies. SCF, or designated as either mastcell growth factor (MGF) or c-kitligand (KL), acts relatively early in the scheme of normal In addition, it improves colony formation by MDS marrow cells in synergy with GM-CSF” or EPO,” although the responses vary among patients.33In the present study, SCF enhanced colony formation two to six times more in each patient as well as normal individuals, but it did notalter the clonal constitution of either erythroid or nonerythroid progenitor cells. Thus, the additional colonies stimulated by SCF were not the result of the preferential stimuli to nonclonal progenitor cells. It is difficult to expect SCF will restore normal (polyclonal) hematopoiesis in MDS patients. However, it cannot be ex- From www.bloodjournal.org by guest on December 22, 2014. For personal use only. IN MDS EMATOPOIETIC NONCLONAL PMN T cell PMN ” PMN 593 MNC ” T cell PMN MNC PMN T cell “ UPN Fig 5. Clonal patterns of peripheral blood cells. DNA from PMNand either T cell or MNC wereamplified by nested-PCR. DNA in HI+) lanes were precut with Hpall. cluded that other cytokines, or their combinations, preferentially act on residualnonclonal progenitor cells, resulting in qualitative improvement in MDS hematopoiesis. Present clonal analysis is useful in evaluating the cytokine effects in vivo as well as in vitro. Whenever X-inactivation is used in clonal analysis, extreme ly~nization’~.” should be considered. To rule out such lyonization, we analyzed clonality of either T lymphocytes or MNC from peripheral blood and compared the clonality with that of PMN. Among three patients whose PMN showed a monoclonal band pattern, two (UPN 1 and 3) had T lymphocytes of oligoclonal band patterns. MNC of one patient with oligoclonal PMN (UPN 2) yielded a polyclonal band pattern. In these three cases, acquired clonal evolution may have occurred in marrow. In UPN 4,because her T lymphocytes showed a monoclonal band pattern identical to PMN, we could not rule out completely the possibility that clonal UPN 2 UPN 1 1 I. 11.7 kb hematopoiesis resulted from extreme lyonization. However, buccal mucosa of UPN 4 were composed of polyclonal cell populations (data not shown), which might indicate pluripotent hematopoietic stem cell involvement in the patient. Circulating PMN and MNC of UPN S showed a similar polyclonal band pattern. Therefore, we could not ascertain that acquired clonal evolution had caused the skewed clonal constitution of marrow progenitor cells. As monoclonal hematopoiesis has been considered one of the characteristics in MDS, the polyclonal appearance in UPN S may seem extraordinary. However, this case may not be so exceptional because polyclonal blood-cell populations, other than lymphocytes, have been reported in some MDS patients.I4.” Here, we demonstrated that polyclonal hematopoiesis can persist in MDS marrow. In addition, the clonal composition of hematopoietic progenitor cells may be different from patient to patient. Thus, the heterogeneity of MDS might be true also in the hematopoietic progenitor cell clonality. Finally, it is of great interest whether the mosaicism of clonal andpolyclonalprogenitorcellsisstableornotwithdisease progression and whether remaining polyclonal progenitors affect the outcome with chemotherapy and cytokine stimulation. Studies in this area are in progress in our laboratory. REFERENCES 1.3kb Fig 6. Clonal analysis of PMN by Southern blotting. DNA in H[+) lanes werecut withHpall. Asingle band in H[+) lane of UPN 1 damonstrates monoclonal PMN, while the band pattern in H[+)lane of UPN 2 demonstratesthe extremely skewed clonal constitution. 1. Koeffler H P Myelodysplastic syndromes (preleukemia). Semin Hematol 23284, 1986 2. Mufti GJ, Galton DAG: Myelodysplastic syndromes: Natural history and features of prognostic importance. Clin Haematol15:953, 1986 3. Bens P Primary clonal myelodysplastic syndromes. Semin Hematol 26:2 16, l989 4. Prchal JT, ThrockmortonDW, Carroll AJ Ill, Fuson EW, Gams From www.bloodjournal.org by guest on December 22, 2014. For personal use only. 594 RA,Prchal JF: A common progenitor for human myeloid and lymphoid cells. Nature 274:590, 1978 5. Abkowitz JL, Fialkow PJ, Niebrugge DJ, Raskind WH, Adamson JW: Pancytopenia as a clonal disorder of a multipotent hematopoietic stem cell. J Clin Invest 73:258, 1984 6. Raskind WH, Tirumali N, Jacobson R, Singer J, Fialkow PJ: Evidence for a multistep pathogenesis of a myelodysplastic syndrome. Blood 63:1318, 1984 7. Mecucci C, Rege-Cambrin G, Michaux JL, Tricot G, van den Berghe H: Multiple chromosomally distinct cell populations in myelodysplastic syndromes and their possible significance in the evolution of the disease. Br J Haematol 64:699, 1986 8. Lawrence HJ, Broudy VC, Magenis RE, Olson S, Tomar D, Barton S, Fitchen JH, BagbyGC Jr: Cytogenetic evidence for involvement of B lymphocytes in acquired idiopathic sideroblastic anemias. Blood 70:1003, 1987 9. Kere J, Ruutu T, de la Chapelle A: Monosomy 7 in granulocytes and monocytes in myelodysplastic syndrome. N Engl J Med 3 l6:499, 1987 10. Amenomori T, Tomonaga M, Jinnai I, Soda H, Nonaka H, Matsuo T, Yoshida Y, Kuriyama K, Ichimaru M, Suematsu T: Cytogenetic and cytochemical studies on progenitor cells ofprimary acquired sideroblastic anemia (PASA): Involvement of multipotent stem cells in PASA clone and mosaicism with normal clone. Blood 70: 1367, 1987 1 I . Okuda T, Yokota S, Maekawa T, Sonoda Y, Taniwaki M, Misawa S, Takino T, Abe T: Cytogenetic evidence for a clonal involvement of granulocyte-macrophage and erythroid lineages in a patient with refractory anaemia. Acta Haematol 80:110, 1988 12. Kibbelaar RE, van Kamp H, Dreef El, de Groot-Swings G, Kluin-Nelemans JC, Beverstock GC, Fibbe WE, Kluin PM: Combined immunophenotyping and DNA in situ hybridization to study lineage involvement in patients with myelodysplastic syndromes. Blood 79: 1823, 1992 13. Anastasi J, Feng J, Le Beau MM, Larson RA, Rowley JD, Vardiman JW: Cytogenetic clonality in myelodysplastic syndromes studied with fluorescence in situ hybridization: Lineage, response to growth factor therapy, and clone expansion. Blood 81:1580, 1993 14. Janssen JWG, Buschle M, Layton M, Drexler HG, Lyons J, van den Berghe H, HeimpelH,Kubanek B, Kleihauer E, Mufti GJ, Bartram CR: Clonal analysis of myelodysplastic syndromes: Evidence of multipotent stem cell origin. Blood 73:248, 1989 15. Vogelstein B, Fearon ER, Hamilton SR, Preisinger AC, Willard HF, Michelson AM, Riggs AD, Orkin SH: Clonal analysis using recombinant DNA probes from the X-chromosome. Cancer Res 47:4806, 1987 16.LyonMF: X-chromosome inactivation and developmental patterns in mammals. Biol Rev 47:1, 1972 17. Tefferi A, Thibodeau SN, Solberg LA Jr: Clonal studies in the myelodysplastic syndrome using X-linked restriction fragment length polymorphisms. Blood 75: 1770, 1990 18. Abrahamson G, Boultwood J, Madden J, Kelly S, Oscier DG, Rack K, Buckle VJ, Wainscoat JS: Clonality of cell populations in refractory anaemia using combined approach of gene loss and Xlinked restriction fragment length polymorphism-methylation analyses. Br J Haematol 79:550, 1991 19. Culligan DJ, Cachia P, Whittaker J, Jacobs A,Padua RA: Clonal lymphocytes are detectable in only some cases of MDS. Br J Haematol 81 546, 1992 ASANO ET AL 20. van KampH,FibbeWE,JansenRPM,vanderKeur M, de Graaff E, Willemze R, Landegent J E Clonal involvementof granulocytes and monocytes, but not of T and B lymphocytes and natural killer cells inpatientswithmyelodysplasia:Analysis by X-linked restriction fragment length polymorphisms and polymerase chain reaction of the phosphoglycerate kinase gene. Blood 80:1774, 1992 21. Ohashi H, Ichikawa A, Takagi N, Hotta T, Naoe T, Ohno R, Saito H: Remission induction of acute promyelocytic leukemia by all-trans-retinoic acid: Molecular evidence of restoration of normal hematopoiesis after differentiation and subsequent extinction of leukemic clone. Leukemia 6:59, 1992 22. Gilliland DG, Blanchard KL, Levy J , Perrin S, Bunn HE': Clonality in myeloproliferative disorders: Analysis by means of the polymerase chain reaction. Proc Natl Acad Sci USA 88:6848, 1991 23. Bennett JM, Catovsky D, Daniel MT, Flandrin G, Galton DAG, Gralnick HR, Sultan C: Proposals for the classification of the myelodysplastic syndromes. Br J Haematol 5 1 : 189, 1982 24. Sambrook J, Fritsch EF, Maniatis T: Molecular Cloning, A Laboratory Manual (ed 2). Cold Spring Harbor, NY. Cold Spring Harbor Laboratory, 1989, p E.3 25. Vadhan-Raj S, KeatingM, LeMaistre A, Hittelman WN, McCredie K, Trujillo JM, Broxmeyer HE, Henney C, Gutterman JU: Effects of recombinant human granulocyte-macrophage colonystimulating factor in patients with myelodysplastic syndromes. N Engl J Med 317:1545, 1987 26. Bowen D, Culligan D, Jacobs A: The treatment of anaemia in the myelodysplastic syndromes with recombinant human erythropoietin. Br J Haematol 77:419, 1991 27. Nrgrin RS, Haeuber DH, Nagler A, Olds LC, Donlon T, Souza LM, Greenberg PL: Treatment of myelodysplastic syndromes with recombinant human granulocyte colony-stimulating factor. Ann Intern Med 110:976, 1989 28. Ganser A, Seipelt G, Lindemann A, Ottmann OG, Falk S, Eder M, Herrmann F, Becher R, Hoffken K, Buchner T, Klausmann M, Frisch J, Schulz G, Mertelsmann R, Hoelzer D: Effects of recombinant human interleukin-3 in patients with myelodysplastic syndromes. Blood 76:455, 1990 29. Broxmeyer HE, Cooper S, Lu L, Hangoc G, AndersonD, CosmanD,Lyman SD, Williams DE: Effect of murine mast cell growth factor (c-kit proto-oncogene ligand) on colony formation by human marrow hematopoietic progenitor cells. Blood 77:2142, 1991 30. Bernstein ID, Andrews RG, Zsebo KM: Recombinant human stem cell factor enhances the formation of colonies by CD34' and CD34'lin- cells, and the generation of colony- forming cell progeny from CD34'lin- cells cultured with interleukin-3, granulocyte colony-stimulating factor, or granulocyte-macrophage colony-stimulating factor. Blood 77:2316, 1991 3 1. Goselink HM, Williams DE, Fibbe WE, Wessels HW, Beverstock GC, Willemze R, Falkenburg JHF: Effect of mast cell growth factor (c-kit ligand) on clonogenic leukemic precursor cells. Blood 80:750, 1992 32.BackxB,BroedersL, LAwenbergB: Kit ligandimproves in vitro erythropoiesis in myelodysplastic syndrome. Blood 801213, 1992 33. AsanoH,Hotta T, Ichihara M, Murate T, Kobayashi M, Saito H: Growth analysis of marrow CD34-positive hematopoietic progenitor cells in patients with myelodysplastic syndromes. Leukemia (in press) 34. Gale RE, Wheadon H, Linch DC: X-chromosome inactivation patterns using HPRT and PGK polymorphisms in haematologically normal and post-chemotherapy females. Br J Haematol79:193, 1991 From www.bloodjournal.org by guest on December 22, 2014. For personal use only. 1994 84: 588-594 Evidence for nonclonal hematopoietic progenitor cell populations in bone marrow of patients with myelodysplastic syndromes H Asano, H Ohashi, M Ichihara, T Kinoshita, T Murate, M Kobayashi, H Saito and T Hotta Updated information and services can be found at: http://www.bloodjournal.org/content/84/2/588.full.html Articles on similar topics can be found in the following Blood collections Information about reproducing this article in parts or in its entirety may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests Information about ordering reprints may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#reprints Information about subscriptions and ASH membership may be found online at: http://www.bloodjournal.org/site/subscriptions/index.xhtml Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036. Copyright 2011 by The American Society of Hematology; all rights reserved.









© Copyright 2026