
A Comparative Analysis of Health Markets and Private For
A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) Insert job reference Prepared for Department for International Development (DFID) December 2014 A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) Contact Information Document Information Cardno Emerging Markets (UK) Ltd Prepared for Department for International Development (DFID) Project Name Private Sector Innovation Programme for Health (PSP4H) Date 23rd December 2014 Oxford House, Oxford Road Thame Oxon UK OX9 2AH Telephone: +44 1844 216500 http://www.psp4h.com http://www.cardno.com/ Implemented by a Cardno Emerging Markets consortium: Funded by the UK Government: With partners: December 2014 Cardno ii A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) EXECUTIVE SUMMARY With development efforts in recent decades focused primarily on improving the public sector health markets, private health markets of East Africa (EA) have been relatively neglected by governments and development partners as a target of research and as a possible strategy to address health challenges confronting the region. The United Kingdom Department for International Development is supporting an action research programme in Kenya to foster better understanding on how the private for-profit health sector can benefit the working poor. The Private Sector Innovation Programme for Health (PSP4H) has commissioned this piece of research to demonstrate the value of a market systems approach in specific health markets in the region and to illustrate the steps needed to improve the functions of healthcare markets to better serve the poor. Based on PSP4H experience in the Kenyan health markets, the report then analyses health markets in the six countries (Ethiopia, Kenya, Rwanda, Somalia, Tanzania, and Uganda) in EA in terms of macroeconomics, health financing, insurance, and supply and demand for private sector healthcare services. Through this comparison, the report identified Tanzania and Uganda as similar private health sector potential with best opportunity for expanding M4P in health. The report also identified private sector, pro-poor market interventions with documentation in Kenya, Uganda, and Tanzania for comparison. The goal of this report is to share lessons learned on how to work with the private sector in health using a market based approach. The lessons are based on comparative research on PSP4H market interventions and other private sector programs in similar health markets in East Africa. Although PSP4H has only been in operation for fourteen months, emerging lessons include: M4P approach works to analyse and shape health markets but with important differences: The M4P framework is robust enough to describe and analyse what is happening in select health markets. There are, however, several key differences between the health sector and other economic sectors. Implementing M4P differs from traditional donor programming: M4P requires that donors and implementing partners play a facilitative role. By definition, facilitation of market change is a temporary role with the goal of exiting the market to foster long-term self-sustainability. There are times, however, when it is appropriate for a donor to “prime the market” through direct intervention in order to achieve critical public health objectives. It is critical when “priming the market” to have an exit strategy in place from the outset of the project. PSP4H has developed analytical approaches that can jumpstart future M4P programmes: A marketbased approach requires a full analysis of a country context focusing on understanding the health sector, the poor and the PFP in health. The report shares many suggestions, such as innovative ways to define the poor and the need to engage PFP sector early on to name a few, that can save time in applying the M4P approach in other countries. Using a portfolio approach helps minimize risk when facilitating change in health markets: PSP4H has found that the portfolio approach allows a flexible mix of interventions, entry points into different markets, and diversity in partners. As a result, the programme is less concerned with the performance of any one intervention in the portfolio than with the overall success of the portfolio. Look for opportunities in markets that meet this set of key conditions: PSP4H developed principles when exploring potential market opportunities including: i) target the “working poor”; ii) focus on geographic areas with a critical concentration of formal PFP providers; iii) stay out of donor-funded areas to avoid “over-crowded” health and geographic areas; and iv) work in underserved health areas identified by the poor and that are interest to the PFP sector, such as diagnostics, dentistry, optometry, and NCDs. Field-based learning can guide design and implementation of future market interventions: In a short timeframe, the PSP4H programme has several suggestions that may help increase the likelihood of success with market interventions: - Start with formal health providers and established institutions/networks - Introduce market interventions that are easy to adopt and do not take the PFP providers away from core, business activities December 2014 Cardno iii A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) - Plan from the start to make network management become financially sustainable - A successful business model is as important as a high-quality service - Market interventions with potential scale involving systemic changes, like private health insurance, may require a long time. Promising market interventions share several key business practices: There are lessons from outside the region that demonstrate key business practices found in successful PFP interventions targeting the poor. Indeed, many of the examples reviewed in this report share similar characteristics. They include: i) concentrating in urban locations, including as peri-urban areas and smaller towns, ii) carrying out nontraditional marketing techniques designed to reach the working poor; iii) delivering better customer service than government facilities; iv) offering flexible terms of payment in response to the working poor’s purchasing habits; v) emphasizing high volume by specializing on relatively simple, low-cost services; vi) consistently looking for ways to cut costs; and vii) keeping a narrow clinical/technical focus. PFPs serving the poor may have to partner with the government to achieve scale: Risk-sharing schemes, such as partnerships with the government or financial support from social health insurance schemes, are promising ways for governments and donors to engage the PFP to reach the poor on a larger scale in a sustainable way. Through this comparison, the report identified Tanzania and Uganda as similar private health sector potential with best opportunity for expanding M4P in health. December 2014 Cardno iv A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) ACRONYMS Acronym Full spelling ADDOs Accredited Drug Dispensing Outlets DHS Demographic Health Survey DFID Department for International Development (UK) DLDB Duka La Dawa Baridi FP Family Planning GDP Gross Domestic Product GF Global Fund to Fight AIDS, Tuberculosis, and Malaria HIV/AIDS Human Immunodeficiency Virus Infection and Acquired Immune Deficiency Syndrome HRH Human Resources for Health IFC International Finance Corporation LMIC Low- and Middle-Income Countries M4P Making Markets Work for the Poor MH Maternal Health MoH Ministry (or Ministries) of Health MSA Medical Savings Account NCD Non-Communicable Disease OECD Organization for Economic Co-operation and Development OOP Out-of-pocket PEPFAR President's Emergency Plan for AIDS Relief PFP Private For-Profit PNFP Private Not-for-profit PRINMAT Private Nurses and Midwives Association Tanzania PSP4H Private Sector Innovation Program for Health SSA Sub-Saharan Africa TB Tuberculosis THE Total Health Expenditure USAID United States Agency for International Development VfM Value for money December 2014 Cardno v A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) RECOMMENDED CITATION Private Sector Innovation Programme for Health (PSP4H), 2014. A Comparative Analysis of Health Markets and Private For Profit, Pro-Poor Interventions in East Africa. Nairobi, Kenya: PSP4H December 2014 Cardno vi A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) FOREWORD The Private Sector Innovation Programme for Health (PSP4H) began in late 2013 with the mission to explore the markets in which poor people pay for-profit providers for healthcare, a hitherto unexplored area for DFID Kenya. Informal employment makes up the lion’s share of total employment in Kenya; this group is largely uninsured, with studies showing health insurance coverage in the single digits. As such, Kenya’s mass of working poor – about half the population – have grown accustomed to paying out of pocket to the private sector for healthcare. However, because low income Kenyans do not always receive good value for the money they spend, a significant opportunity to offer a better value proposition to this vast target audience presents itself to the private sector. Successful pro-poor for-profit business models in healthcare are not yet widespread. The programme hopes to have some impact on this limitation by discovering and disseminating evidence on what does indeed work for both business and the target group. PSP4H researches existing best practice, endeavours to understand consumer health seeking and health spending behaviour through primary research, and explores ways the forprofit private sector can bring better quality of care and better access to services to low income groups through testing innovative approaches in partnership with private actors. Early lessons learnt point to more effective and sustainable programme design in the future. PSP4H commissioned this study to compare the for-profit private health markets in Kenya with those in neighbouring East African countries, with a view towards expanding – and potentially applying – lessons learnt in Kenya to the wider context. The programme trusts that this foundation of knowledge will encourage more private sector investment in pro-poor healthcare models, both in East Africa and beyond. Ron Ashkin Team Leader, The Private Sector Innovation Programme for Health (PSP4H) Nairobi, December 2014 December 2014 Cardno vii A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) PREFACE AND ACKNOWLEDGEMENTS PSP4H would like to acknowledge the work of lead writers Meghan Kumar, Barbara O’Hanlon and Salome Wawire; and the contribution of PSP4H staff Ron Ashkin, Ambrose Nyangao, Veronica Musembi, Dolapo Olusanmokun, Pamela Godia, Chris Masila, Mildred Kottonya and Patricia Guchu. We acknowledge the contributions of those interviewed for the report, particularly Edmund Rutta and Grace Njeri Gitonga, as well as assistance and recommendations from Nelson Gitonga and Catherine Goodman. December 2014 Cardno viii A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) Table of Contents EXECUTIVE SUMMARY iii ACRONYMS v RECOMMENDED CITATION vi FOREWORD vii PREFACE AND ACKNOWLEDGEMENTS viii Table of Contents ix 1 INTRODUCTION 1 2 M4P FRAMEWORK APPLIED TO HEALTH MARKETS 3 2.1 2.3 2.4 3 4 6 3 IMPLEMENTING A MARKET-BASED APPROACH IN HEALTH 3.1 3.2 3.3 3.4 3.5 3.6 4 5 What is M4P? M4P Framework to Analyse and Shape Health Markets M4P and Donor Role Portfolio Approach Pathway to Design Market Interventions Discovery Phase Identification Phase Selection Phase Implementation Phase 7 7 8 8 10 10 11 READINESS FOR M4P PROGRAMMING IN EAST AFRICA 13 4.1 4.2 4.3 4.4 4.5 4.6 4.7 13 13 13 14 14 15 16 Approach to Select Comparative Health Markets Level of Macro-Economic Development Health Financing Private Sector Contribution Health Insurance Demand for Private Health Services Ranking of EA Countries LESSONS LEARNED FROM PRIVATE SECTOR PROJECTS IN COMPARATIVE HEALTH MARKETS AND PSP4H INTERVENTIONS 17 5.1 5.2 Preliminary Findings from the Field Lessons Learned from other Regions 17 22 6 CONCLUSIONS AND RECOMMENDATIONS 24 7 References. 26 8 APPENDIX 1: KEY M4P CONCEPTS ADAPTED TO HEALTH 28 9 appendix 2: Intervention screening tool 30 10 Appendix 3. Description of PSP4H Programme 32 December 2014 Cardno ix A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) Tables Table 4-1 Table 4-2 Table 4-3 Table 4-4 Table 4-5 Table 5-1 East African Countries Economic Development Indicators (World Bank, 2014) ........................ 13 Health Finance Indicators ........................................................................................................... 14 Select Private Health Sector Indicators ...................................................................................... 14 Role of Insurance in EA Health Sectors ...................................................................................... 15 Health-Seeking Behavior in the Private For-profit Sector ........................................................... 15 Overview of Private Sector Cases in EA ..................................................................................... 17 Figures Figure 1-4 Figure 1-3 Figure 1-2 Figure 1-1 Figure 1-5 Figure 1-6 M4P Framework ............................................................................................................................ 3 Portfolio Approach ......................................................................................................................... 7 Timeframe to Achieve Market Change ......................................................................................... 8 Process to Build a Portfolio ........................................................................................................... 8 PSP4H Interventions by County.................................................................................................. 12 Ranking of Private Health Sector Development in EA ................................................................ 16 December 2014 Cardno x A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) 1 INTRODUCTION The purpose of this report is to share what PSP4H has learned about working with the private for-profit sector in different health markets. With development efforts in the last decades focused on improving the public sector health markets, private health markets of East Africa (EA) have been relatively neglected by governments and development partners as a possible strategy to address health challenges confronting the region. There is limited reliable information about the size, profitability, and dynamics of the private for-profit (PFP) healthcare market in EA, which hampers even the limited attempts to engage with it. Additionally, there is little evidence on how best to intervene in health markets and engage the PFP sector to benefit lower economic segments of the population. Initial attempts at improving this situation have been made by a number of donors (e.g. United States Agency for International Development (USAID) and International Finance Corporation (IFC), who have supported analysis of the formal for-profit sector, initiated inclusive policy dialogue between the public and private sectors, and established programs involving the private health sector. These are an important first step, but more approaches and initiatives supporting the PFP are needed to determine if this segment of service providers can deliver accessible, affordable and quality healthcare to the poor in this region. The United Kingdom Department for International Development’s (DFID) response to the situation is an action research programme in Kenya to foster better understanding on how the PFP health sector can benefit the working poor. The Private Sector Innovation Programme for Health (PSP4H) - implemented by Cardno Emerging Markets and consortium partners - utilizes a market systems approach called Making Markets Work for the Poor (M4P), originally used in the agricultural development sector. This M4P approach works to strengthen the PFP health sector’s capacity to reach the poor, then conducts research to assess if consumers get improved value for the money (VfM) they spend on health in the private sector when accessing that care through the PSP4H partner interventions. PSP4H programme objectives include: Understanding the Kenyan poor’s provider preference, health-seeking behaviour, and willingness and ability to pay. Identifying and piloting appropriate pro-poor interventions by the commercial health sector. Conducting action research to explore when and why the private health sector delivers healthcare to the poor. Providing evidence about whether the private sector can delivery affordable, quality health services that reach the poor. Sharing lessons learned from the different pro-poor health market interventions. During its first year, PSP4H has undertaken a series of research studies to help build both the Kenyan and the international community’s knowledge on market-based approaches in health. To date, PSP4H research has published the following briefs: The Kenyan Poor and Their Use of the Private Health Sector (Demand side) What Do We Know About Kenyan Private Health Sector? (Supply side) Formative Survey of the Private Health Sector in Kenya A Study on Sustainability Outcomes of Donor-Funded Healthcare Programmes Comparing Kenya’s Private Health Finance Markets with Neighbouring Markets Study of the Pharmaceutical Supply Chain in Kenya Preliminary Research Report (Year One) December 2014 Cardno 1 A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) In addition, PSP4H conducts action research on all its market interventions. To date, PSP4H is working with a portfolio of 17 Kenyan PFP health businesses in diverse areas including health finance, maternal health, supply chain, non-communicable diseases, e-health, and low-cost service delivery. The action research on each of the market interventions is designed to explore the potential for donors and developing country governments to engage and support the private health sector as a complementary strategy to current publicfocused approaches to address health priorities. As part of its focus on learning and sharing knowledge, the PSP4H commissioned this comparative analysis of the health markets and private sector programs to clarify: Market conditions motivating commercial participation in various health markets. Critical factors to engage/interest of the for-profit sector in providing services to the poor. Health areas where a market-systems based approach is most likely to succeed. Reasons for success or failure of different types of interventions in these health areas. Applicability of lessons learned under PSP4H to similar health markets in the region and perhaps beyond. Although the target audiences for this comparative analysis are donors and low- and middle-income country (LMIC) governments, the lessons learned are also relevant for implementing partners working in the international health arena. The analysis will help demonstrate the value of a market systems approach in specific health markets in the region and illustrate the steps needed to improve the functions of healthcare markets to better serve the poor. December 2014 Cardno 2 A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) 2 M4P FRAMEWORK APPLIED TO HEALTH MARKETS The Making Markets Work for the Poor framework is relevant to the health sector with some key changes in interpretation 2.1 What is M4P? M4P is an approach to analyse the participation of the poor in market systems and to offer guidance on how to “influence” markets so they benefit the poor. What distinguishes the M4P framework from others is the combination of analysis with action. M4P analyses how the poor participate in a specific market (e.g. as a consumer, producer, etc.) and then recommends how to shape and bring about change in the market system to benefit the poor based on that analysis. The M4P approach focuses on market systems and market dynamics. Market systems provide a space for consumers and suppliers to come together to carry out a transaction to purchase a good or service (core functions). As figure 1-1 illustrates, a market system is comprised of multiple actors (private sector, government agencies, representative organizations, and civil society) who carry out numerous functions (core functions in a market, formal and informal rules and supporting functions). A market system’s range of supporting functions and informal/formal rules (outer ring) shape a specific market’s performance (inner ring) by determining market players’ behavior and practices, influencing relationships between the players, providing information and knoweledge and creating incentives (SDC and DFID, 2008) Figure 1-1 M4P Framework Government Sector Representative Bodies Supporting Functions Infrastructure Coordination Informing and Communicating Informal Networks Membership Organizations Setting and Standards Regulations Standards Not-for-Profit Sector Laws Enforcing Rules Informal Rules and Norms Private Sector Source: (The Springfield Centre 2014) M4P is concerned with achieving large-scale change in markets. The type of interventions under an M4P approach go beyond engagement with individual organizations and private sector groups, involving a multiplicity of actors to achieve systemic change. However, achieving scale does not imply nationwide implementation – scale depends on the market. Sustainability in a M4P context implies: i) developing capacity in a market system and actors; ii) supporting a dynamic system to grow and evolve as the market goes to scale; and iii) the market continuing to deliver goods and service after the intervention ends. December 2014 Cardno 3 A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) In any market system, there are three main sets of functions: Core functions/market dynamics (inner ring) consists of several factors that influence the supply and demand of goods and services. The exchange between supply and demand is conventionally a transaction with money but can also occur through informal payments and/or government subsidies. Rules/market system (outer ring) sets the terms by which all the players participate in a specific market as well as shape market performance. Rules include informal rules and norms, formal regulations, guidelines and laws and practice. Rules are essentially the domain of government agencies and/or representative bodies. Their capacity to enforce the rules is as important as the rules themselves. Supporting functions/market systems (outer ring) are a range of tasks – such as coordination between the sectors, adequate infrastructure, research and development, skills and capacity and information – required to develop and grow the market. 2.2 Why M4P in Health? There are many reasons why the international health practitioners are turning their attention to the M4P approach. First, there is a growing recognition that traditional forms of donor assistance focusing exclusively on Ministries of Health (MoH) and public programs do not effectively reach the poor and, in fact, disproportionately benefit the middle- and upper-income groups (Makinen et al., 2000). Secondly, there is growing concern over sustainability of donor-initiated programs – both financially and organizationally. In the age of the President's Emergency Plan for AIDS Relief (PEPFAR) and the Global Fund (GF) to Fight AIDS, Tuberculosis (TB) and Malaria, the approach has been for donor agencies to get “the job done ourselves” by providing finance, advice, materials and labour (SDC and DFID, 2008) – which succeeds in the short run, but is not sustainable. Finally, purely analytical approaches to understanding why health systems in developing countries are underperforming are inadequate. Although policy research in OECD countries includes measurement of health markets and private sector activities, similar research in developing countries does not, perpetuating the public sector orientation that has been characteristic of donor programming in health and development to date (Introduction to Markets for Health. DFID-sponsored Workshop, Organized by the World Bank Institute, January 2013). 2.3 M4P Framework to Analyse and Shape Health Markets While there may appear to be little in common between a market for Market: A set of arrangements by food products and a market for health services, early observations which buyers and sellers are in from PSP4H show that the systems supporting these different contact to exchange goods or markets share similar characteristics. A working market – whether it services in health; the interaction of demand and supply for a health be for food production or consumption of a health service – requires service or product. an enabling environment creating incentives to participate in the market as well as multiple actors who have the capacity to play their respective roles. Upon examination, the M4P framework is robust enough to describe and analyse what is happening in select health markets. However, there are several key differences when using the M4P approach in health that should be noted and are elaborated in the following section: Market actors: The main categories of actors (e.g. government, Private for-profit: Commercial private sector, representative bodies and civil society) are similar in entities engaged in a health health to the generic M4P, though specific organizations differ. The business that provides health major differences, however, are the diversity of private sector services and/or products. organizations in healthcare in both the PFP and private not-for-profit Private not-for-profit: Faith(PNFP) sectors and the range of private health operations (e.g. based organizations, nongovernment organizations, social multiple levels of hospitals, diagnostics and laboratories, enterprises delivering health pharmaceutical production, supply and distribution, medical training, services and/or products. etc.). Another distinction is how fragmented and disorganized the private health sector is compared to other economic sectors. Examples of this fragmentation include weak representative bodies, and nascent membership organizations. These two factors make any market intervention more difficult, as actors may not be equally matched nor are they capacitated to act. Another difference is the role government plays in the health sector: MOH not only set December 2014 Cardno 4 A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) the rules (regulate) but also deliver health services. Finally, international donor agencies have become market players. Heavy reliance on donor funds and grants dampens competition and crowds out the PFP health sector in specific health markets such as human immunodeficiency virus infection and acquired immune deficiency syndrome (HIV/AIDS), family planning and maternal health (Public Service Strengthening Using Market Systems Development Strategies: M4P and Health in Kenya, Presentation delivered at 9th Annual BDS Conference, Mombasa, November 2013). Supporting functions: Developing countries’ MOH regard health as a public good and the sole domain of government. Mistrust between the public and private sectors, as well as suspicion and misunderstanding of the profit motive, still linger among policymakers and MOH officials (Hozumi, 2008). As a result, there is little to no exchange of information between the public and private actors in the health sector. Limited access to information on government health priorities, epidemiological trends and socio-economic profiles of those affected restricts the PFP and PNFP sectors’ ability to gauge market potential much less align their respective activities to help address public health goals. In addition, the MOH struggles to regulate all the actors in the health sector, including both formal and informal PFP providers. As a result, quality in the private health sector is highly variable. The lack of engagement with and regulation of these entities, particularly informal providers, can have serious consequences, placing patients’ health and lives at great risk. Governments play a critical role in ensuring access, affordability and quality of health services for all their citizenry. MOH have several policy tools and instruments at their disposal to achieve these sector goals, particularly financing. Direct free provision of health goods and services, cash grants and subsidies are all common financing tools utilized in the health sector. In recent years, international donors have promoted social health insurance and service contracts, mostly with the PNFP sector to carry out clinical (e.g. deliver specific health services or specialty care) functions and PFP to perform non-clinical (e.g. waste management, catering, security, etc) functions. Moreover, several international agencies have pumped large amounts of money and resources (including commodities, equipment and staff) into specific health sub-sectors driven by international agendas (e.g. HIV/AIDS, family planning, malaria, child health). When applied with little regard for the market dynamics, these policy interventions result in the distortion of the market and crowding out of the commercial sector. Therefore, the use – or in many cases – improper use of financing and subsidies is an important distinction when using M4P in a health system context. Very few developing countries’ MOH have the necessary systems and skills to effectively engage the PFP health sector. Most MOH do not collect data on the size and scope of private sector activities and are unaware of or do not acknowledge the private sector’s contribution in health. Moreover, MOH staff are often selected for their medical background and may lack skills or training to understand how health markets operate or how to shape them. Economic and financing skills to introduce subsidies and/or grants so as not to distort health markets (as noted above) are also limited. Rules: Another consequence of mistrust and suspicion between the public and private sectors in health is the inadequate involvement of private sector organizations, their representive bodies and membership organizations in health policy and planning (or Rules, in the M4P approach). In many cases, developing countries’ MOH implement health reforms that directly affect the private sector without understanding the policies’ potentially negative impact, nor do governments actively engage the private sector on a regular basis to implement policies and reforms, missing strategic opportunities to harness private sector resources and expertise. There is growing recognition that public-private dialogue initiatives in health to set the rules (e.g laws, policies and standards) and to implement these rules (supporting functions) is a necessary condition to overcome this deep-seated mistrust between the public and private health sectors. It is also important to note that health, when compared to other economic sectors, lags behind in putting in place market-based reforms (Price Waterhouse Cooper, 2011). Health laws and policies were written in most countries of EA after independence when the governments offered free health services, and in some cases, the private sector was actually prohibited. Half a century later, many of these countries have not updated their health policy framework to acknowledge the existence and contribution of the PFP sector with a few exceptions such as Kenya. In response, many countries have quickly established new regulations allowing for and regulating private practice but these rules are often insufficient, poorly enforced, or in conflict with other laws and policies. Another distinguishing feature of the health sector is the complexity of its rules, with life or death consequences if these are not followed or enforced effectively. These rules are set by domestic policymakers but must also December 2014 Cardno 5 A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) follow international standards. To comply with these rules requires a level of advanced training (medical/healthrelated) not required in many other economic sectors. This level of complexity sets a high barrier to entry into a health market, but many developing countries’ MOH do not have the systems and capacity to enforce these rules. As result, the PFP health sector remains mostly unregulated, allowing for the growth of a sizeable informal, illegal health sector that create strong competition with the formal private sector (PSP4H, 2014a). Moreover, poorly-enforced rules on quality disproportionately affects the private health sector as quality – aside from price – is the most important factor distinguishing them from government services in the marketplace. Any market intervention in health needs to consider impact of poor regulatory enforcement and how to address competition created by the informal sector. The M4P literature uses several terms but when applied to the health sector, these concepts can take on different meanings as described above. To assist the reader, we have developed a list of key M4P terms adapted for the health sector (see Appendix 1). Note that the M4P framework and these concepts are the basis of this paper’s analysis of markets and interventions. 2.4 M4P and Donor Role Implementing M4P differs from traditional donor programming The M4P approach suggests a role different from traditional Facilitator, noun development partners - to shape market systems and NOT Def. A facilitator is an action or agent that to participate in the market (SDC and DFID, 2008). In the is external to a market system but seeks to health arena, donors and donor-supported health programs bring about change in order to achieve a public benefit. A facilitator is a catalyst that have become actors in the health marketplace. As the stimulates the market but does not National Health Accounts data in Table 2 demonstrates, become a part of it. external funding as a proportion of total health expenditures (The Springfield Centre 2014) in East African countries ranges from over 25% in Uganda to as high as 46% and 50% in Rwanda and Ethiopia respectively. In many instances, donor-funded health programs have distorted and crowded-out the PFP sector. M4P requires that donors and implementing partners play a facilitative role. By definition, facilitation of market change is a temporary role with the goal of exiting the market to engender long-term self-sustainability. Beyond facilitation, there are times when it is appropriate for a donor to “prime the market” through direct In designing a health programme with a facilitative approach, donors need to ask: Is the program design flexible enough to allow the implementing partner latitude to adapt to market opportunities as they evolve? Does the program address the “right” problems (e.g. the root causes why markets are not serving the poor) given the country’s landscape and setting? Does the program balance the country’s health priorities and market priorities with the Agency’s priorities? Do the funder and implementing partner agree on the priority health markets and how to measure success? Is the program’s timetable long enough to allow and measure success? intervention in order to achieve critical public health objectives. If this approach is taken, it is critical to have an exit strategy in place from the outset of the project. In designing a health programme with a market priming approach, a donor needs to consider: Finite period of support: There has to be a clear end-point linked to achievable objectives. Limited in scale: There is a real danger in “flooding a market” and causing long-term distortions. Effective delivery: Carefully consider the structure of the support and the incentives it creates. Consistent policy and approaches. Co-ordination with other donor projects is critical so as not to undermine the direct market support and allow it the time and space to achieve its objectives. (The Springfield Centre, 2014) December 2014 Cardno 6 A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) 3 IMPLEMENTING A MARKET-BASED APPROACH IN HEALTH Although PSP4H has only been in operation for fourteen months as of this writing, the programme has learned many lessons in applying an M4P approach in health that can help streamline future M4P country programmes. 3.1 Portfolio Approach Using a portfolio approach helps minimize risk when facilitating change in health markets Selecting which health market to invest in can be a daunting challenge. This is particularly true when the target sector is unfamiliar to donors, in this case the PFP health sector. To minimize risk and increase the likelihood of success, it is important to support several interventions with the hope that one or two will succeed. Like a financial investor, an M4P donor spreads risk across several health markets and different market interventions, anticipating that some will fail while others will succeed. In a portfolio approach, the programme maintains a flexible mix of markets, entry points, partners and types of intervention activities. As a result, the programme is less concerned with the performance of any one intervention in the portfolio than with the overall success of the portfolio. The portfolio approach is an iterative and continuous learning process (see figure 1-2). One learns from the successes as well as failures, using the information to design, adapt, scale-up and/or shut down market interventions as the markets evolve. If there is a successful intervention, then one shares the findings with others in the same health market with the expectation that other market actors will then enter into the market and the change will go to scale. Figure 1-2 Portfolio Approach Source: Introduction to M4H. Session 11: What do we really need to know? M&E and its application to M4H, delivered by Dr. Ruth Berg, DFID-sponsored Workshop, January 2013 Key Findings of Portfolio Approach It is adaptable in programming, allowing PSP4H to shut down unsuccessful interventions or to further invest in promising ones It is flexible in budgeting, permitting PSP4H to allocate its budget according to the size and scope of each intervention and therefore manage to the bottom line of the total portfolio Fosters innovation, permitting PSP4H to take risks and experiment in new health markets with different PFP actors and new approaches while at the same time, investing in proven approaches to scale. December 2014 Cardno 7 A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) As PSP4H is learning, developing a successful market-facilitating portfolio takes time. The Project spent the first year gaining an understanding of the Kenyan health sector, its landscape the key actors, defining (or quantifying) the poor and identifying underserved health markets as possible targets for support. As figure 13 illustrates, shaping the market takes time, often more than six to 10 years. Although systemic change yields sustainable, large-scale and durable shifts in a health market, it can be difficult for funders to wait for these changes to happen. Therefore the challenge is balancing short-term impact via direct market interventions with indirect market interventions that take time but clearly produce lasting changes benefiting the poor. Figure 1-3 Timeframe to Achieve Market Change Source: Introduction to M4H. Session 11: What do we really need to know? M&E and its application to M4H, delivered by Dr. Ruth Berg, DFID-sponsored Workshop, January 2013 3.2 Pathway to Design Market Interventions PSP4H has developed analytical approaches that can streamline future M4P programmes in health PSP4H followed a systematic process shown in Figure 1-4 to identify and understand several health markets with potential to benefit poor consumers, quickly building its portfolio of 17 interventions in these markets. Through this process, PSP4H developed analytical approaches and tools as well as strategies to streamline the application of the M4P approach in health. Figure 1-4 Process to Build a Portfolio 3.3 Discovery Phase The Discovery Phase occurs at the inception of the programme. In this phase, the programme team conducts a variety of assessments and analyses to understand the enabling environment, market conditions and key actors in the health sector including PFP health providers and low-income consumers. Out of the extensive work completed by PSP4H during the Discovery Phase, the following steps were identified as essential components of future M4P programs: December 2014 Cardno 8 A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) 1. Understand the health sector: PSP4H conducted secondary research to understand the policy and regulatory environment governing health and regulating commerce. In addition, the team landscaped the key actors and the functions they play in the health sector and mapped all donor projects in health. Key Findings Data is scarce on the private health sector – gather data from a wide aray of sources (including but not limited to MOH) to develop insights into the size and scope of the private health sector. Engage the private sector early on the discovery phase to help interpret and validate the findings from the research. These contacts will also help during the Identification Phase to refer potential partner businesses. 2. Understand consumers – particularly the poor ones – of health services and products. PSP4H conducted a series of primary and secondary analyses of Demographic Health Survey and other survey data to define (in terms of size, income range, geographic location) the working poor, understand their care-seeking patterns, and identify underserved health services and products. The consumer focus groups also revealed when the poor seek care in the formal versus informal health sectors and the private sector or public, and why they prefer the private health sector. Key Findings Using traditional poverty measures is insufficient to define the segment of the poor that can be served by the private sector. PSP4H focuses on the “working poor”. The assumption that the poor can’t pay or don’t have money is wrong. The poor are paying now – but they aren’t saving and in some cases, getting poorer. The poor are active – not passive - health consumers making strategic decisions everyday about where and when to seek healthcare and how to pay for it Well-organized but informal groups may be an alternative means to reach segments of the target (e.g. poor) population (e.g. Kenya’s jua kali) 3. Understand the private for-profit health sector: Early in the programme, PSP4H established relationships and networks with the larger private health sector community (e.g. pharmaceutical companies, commodity manufacturers, laboratory and diagnostics, specialty and general hospitals in addition to service providers). Initially PSP4H carried out research directly with the private health sector. PSP4H conducted focus groups and regional stakeholder consultations with PFP healthcare providers to measure their interest in serving the poor, assess what health services and products they are currently delivering to the poor and the challenges they encounter in serving this market segment. The focus groups also explored the PFP health sector actors’ general perspective on the ease/difficulty of operating as a business and noteworthy market conditions. After the research, PSP4H met and consulted with a wide range of PFP companies and providers as individuals to further their understanding of the sector and to establish networks. Key Findings Unclear and inconsistent definition of private health sector (e.g. for-profit vs notfor-profit; social enterprise compared to for-profit) creates challenges in applying M4P. Focus on the PFP sector. To date there is little research on the PFP sector in most countries; more is known about PNFP sector because they receive considerable donor support. Private providers have strong interest in the “working poor” who have demonstrated demand for and willingingness to pay for private services and products. Private sector may be unable to reach the poor consumer, particularly those located in remote and rural areas, unless compensated. December 2014 Cardno 9 A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) The team identified a few modifications to this approach, including: > Utilize different research approaches to ensure that there is depth as well as breadth in the findings. These include brainstorming forums, qualitative methods, quantitative methods and secondary research. Each of these approaches is an important tool for gathering information. Together they create a deeper understanding of the health sector, key actors and point towards potential markets for intervention. > Involve all players (including a wide range of PFP entities delivering healthcare, manufacturing and distribution of commodities and investors in the health sector), in the research to get a broad understanding of the health markets. Private healthcare associations can quickly help identify the major PFP players and identify community groups that can organize and represent the “poor”. > Allow sufficient time to obtain research ethics approval for any research program from local Institutional Review Boards. The approval process may take more than a month even when expedited. 3.4 Identification Phase The analyses conducted in the Discovery Phase helped Health area: identify potential health areas for a greater PFP role to Def. A segment of the health system, also serve the poor. The Identification Phase drills down into known as a ‘sub-sector, e.g. family planning, these health areas, requiring additional research and malaria Health market: networking to understand: i) how each market works, ii) Def. The interaction of demand and supply for the principal market actors (formal and informal), iii) the a health service or product, e.g. Condoms, longfunctions each market actor plays, and iv) the lasting insecticide-treated bednets relationship between these actors. This diagnostic process is not a fixed sequential process using specific tools. Instead, it is a way of thinking through information needs and organizing it to inform programme strategy and market interventions (The Springfield Centre, 2014). One of the first challenges when applying M4P to the health sector is defining what is a health market. Public health practitioners might mistakenly use the terminology ‘market’ when referring to a health area – for example, malaria prevention, family planning or maternal health. However, a market is a set of arrangments in which a buyer and seller come together to exchange a health service or product. So malaria prevention, for example, is actually a series of interconnected markets in which several types of buyers and sellers exchanges goods and/or services. Key Findings Defining what is a health market is a challenge – public health practitioners confuse a market with a health area or sub-sector. Leverage networks with the private sector for referrals of potential partners. 3.5 Selection Phase While developing a more nuanced understanding of strategy health area, the PSP4H market intervention managers simultaneously engage potential private health sector companies to explore partnership opportunities. Essential components of this phase are: 1. Process to assess partners should be explicit The PSP4H team developed eleven iterations of the intervention screening tool, improving the tool with each generation of applicants (see Appendix 2). The tool covers a range of elements assessing the potential partner’s capacity to implement a proposed market intervention. The intervention manager scores each major area and sub-topic, and narrative comments are provided to justify each decision. PSP4H developed criteria by which to select which market interventions and partners to work with (see Box below). The team reviewed over one hundred proposals before deciding on the initial twelve. As the December 2014 Cardno 10 A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) programme develops, the team continues to receive and assess new partnership opportunities using the screening tool, adding new market interventions along the way. Intervention Screening Criteria: Relevance: Health sector, pro-poor, private sector, for-profit, innovative, addressing a systemic constraint? Impact: Scale, depth, feasibility, positive growth dynamic, attribution? Engagement: Mutual engagement, willing to invest, willing to share data? Do No Harm: Has the impact of the potential intervention on all stakeholders been considered so there will be no adverse unintended consequences? 2. Principles for selecting market interventions In addition to the screening criteria, the team also developed principles guiding the selection of market interventions (See below). Guiding Principles Stay out of donor-funded areas – map donor projects and avoid ‘overcrowded health and geographic areas’ when exploring potential market opportunities Jumpstart an existing business rather than initiating a new one from scratch. It saves time, creates value for money and improves portfolio performance. Start with “low hanging fruits” (in terms of ease of implementation and level of impact) to demonstrate early success and create momentum in the portfolio. Select organizations that have sound business and financial management capacity, permitting the market intervention to focus on market conditions. The most common reasons why partner proposals were not accepted included: > Partner’s business model not pro-poor; > Issues faced by partner are business-specific problems, not systemic ones; > Partner unwilling to share data publicly; > PSP4H does not give financial support. 3. Facilitative approach is new to private sectors partners The M4P approach is new to the health sector in Kenya but donor-funded programs supporting the private sector are not. Despite (or perhaps because of) this, PSP4H encountered several challenges while exploring potential partnership opportunities. Foremost among them is the lack of understanding on how a market-based approach programme will or will not support the PFP sector – particularly, that this support will not include any form of financial aid. To create a better understanding between the organization and potential partners, PSP4H developed a one-page description that the programme staff used during every contact with the private sector (see Appendix 3). Facilitative support to the PFP partners includes: market research, marketing initiatives, business/financial skills strengthening, networking existing providers and introduction of a new product into the market. 3.6 Implementation Phase 1 The PSP4H team initially selected market interventions in five sub-sectors: healthcare finance (1), maternal and child health (3), supply chain (3), non-communicable diseases (3) and E-/m-health (1). As one can 1 Implementation has been ongoing for a relatively brief period of time, with the longest-running intervention running for just about 6 months. Thus, key findings regarding implementation will be included in future program documentation when the market interventions are more mature. December 2014 Cardno 11 A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) observe, the market interventions are concentrated in population-dense areas where there is also significant private sector operations, as seen in Figure 1-5 below: Figure 1-5 PSP4H Interventions by County December 2014 Cardno 12 A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) READINESS FOR M4P PROGRAMMING IN EAST AFRICA 4 Tanzania’s and Uganda’s health sectors are the most comparable to Kenya’s 4.1 Approach to Select Comparative Health Markets The research team used a systematic approach to compare the Kenyan health sector with those of countries in the region to identify whether they represent good comparators. The team examined several factors to assess these countries in terms of the maturity of the private health sector. The following is a discussion of these factors. 4.2 Level of Macro-Economic Development First, we examined the macroeconomic development of the EA countries by examining gross domestic product (GDP), poverty profile, and urbanization rates for most recent data available (2013 except where noted parenthetically after the data point). GDP, combined with percent living in poverty, provides a general sense of a country’s overall wealth and size of the population with the ability to purchase health services in the private sector2. The data suggests that Somalia is extremely poor, with a GDP of just USD128, as might be expected given the country’s ongoing political instability. This makes it an unlikely target for successful sustained development of the private sector. Ethiopia has the next lowest GDP, though it is more than three times that of Somalia at USD498. Interestingly, low GDP does not correlate with the highest poverty gap. That suggests that the country is uniformly poor. This contrasts with Rwanda, where the GDP is USD632 but the percent living on less than $2 per day is higher, suggesting a greater income inequality than in Ethiopia. In addition, high concentration of population in urban and peri-urban settings helps private sector growth with densely population areas with many potential customers. Discounting Somalia, urbanization rates range from 15% in Uganda to 30% in Tanzania. Table 4-1 Country Ethiopia Kenya Uganda Rwanda Somalia Tanzania 4.3 East African Countries Economic Development Indicators (World Bank, 2014) GDP per capita (current USD) Poverty gap at $2 per day (PPP) % of pop in urban areas 498.1 23.6 (2011) 18.6 994.3 No data 24.8 571.7 27.4 (2009) 15.4 632.8 44.6 (2011) 26.9 128.1 No data 38.6 (est. UN data) 694.8 No data 30.2 Health Financing Beyond general macroeconomic indicators, the research team examined the size of the heath sector in EA countries. Table 4-2 shows an overview of health finance indicators.3 Although the Abuja Declaration of 2001 admonishes sub-Saharan African (SSA) countries to allocate 15% of GDP to health, one can see that Rwanda (10.7), Uganda (8.0), Kenya (4.7) and Tanzania (7.0) come closest but still fall short of the target. A low level of GDP spending in health has major consequences for the health system – aging infrastructure, out-of-date technology and staffing constraints to name a few. The very low number of hospital beds per 1,000 demonstrates the lack of public investment in the health system. More than half of all healthcare costs in SSA are currently met by out of pocket (OOP) spending (Economist Intelligence Unit, 2011), and this pattern holds true in EA as well. A significant percentage of individuals spend their healthcare dollars in the private sector (over 40% of Total Health Expenditure [THE] in three of the six countries in the region), demonstrating demand for PFP services and products. But OOP spending masks 2 3 There is no World Bank data available for Somalia, but it is placed based on UN estimate to fall below Ethiopia. Given the LMIC status of the countries of interest, it was expected that data would not be available every year and so for all data points, any data collected after 2008 (last five years) were considered. The only country with multiple missing data points was Somalia. This is due to the last 20 years of instability and current disagreement about borders and the number of governments that should be recognized. December 2014 Cardno 13 A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) inequitable access to health services, creating higher risk of impoverishment due to catastrophic health spending by individuals. And with many of the poorest unable to afford treatment, true costs are kept down artificially by people’s inability to pay (Economist Intelligence Unit, 2011). In addition, these EA countries rely on external sources to finance a significant percentage of healthcare, ranging from over a quarter (Uganda, 28.6%) to half (Ethiopia, 50.3%) of THE. The global economic crisis raises questions about the sustainability of donor funds as a major source of financing of healthcare in Africa (Economist Intelligence Unit, 2011). Table 4-2 Health Finance Indicators Country Health % Public/ Private of GDP Mix of THE Ethiopia 3.8 48.4/51.6 Kenya 4.7 38.1/61.9 Uganda 8.0 23.9/76.1 Rwanda 10.7 57.3/42.7 Somalia No data No data Tanzania 7.0 39.3/60.7 % THE that is OOP 41.2 47.6 49.3 21.1 No data 31.8 % THE from external sources 50.3 42.3 28.6 46.6 No data 37.7 Hospital beds per 1000 pop. 6.3 (2011) 1.4 (2010) 0.5 (2010) No data No data 0.7 (2010) All indicators are measured from the most recent year available as of October 2014 (2012 unless otherwise stated). Where no data are available, records were checked for a 5-year historical range, from 2009 – present. Source: (World Bank, 2014). 4.4 Private Sector Contribution There are several indicators that help measure the size and scope of the private health sector: including number and type of private health facilities levels (infrastructure), number and type of private health professionals (HRH), and total dollar amount spent in the health sector and or drugs purchased. There is limited availability of these data particularly in LMIC. Table 4-3 shows that the PFP health sector owns and operates a significant portion of the health facilities in the region, ranging from 27.4% in Tanzania to 49% in Ethiopia and Kenya of all health infrastructure. It is important to note, however, that the majority of these facilities are small- to medium-sized hospitals and solo practitioners. Also, the private health sector (PFP and PNFP combined) employs a significant number of the human resources in health (HRH), ranging from 22% of all HRH working in Tanzania to 58% in Uganda. The majority of these private HRH work in PNFP facilities. Upon further examination of the data, one observes throughout SSA/EA the majority (upwards of ¾4) of physicians – particularly specialists – and similar level of pharmacists work in the private sector at least part of the time, though some are also employed in the public sector and dual practice is common in all countries of the region. This pattern varies with nurses – in some countries such as Tanzania the majority of nurses’ work in the public sector while in Kenya, they work in the private sector. Table 4-3 Select Private Health Sector Indicators Country % PFP Sector InfrastructureA Ethiopia 49% Kenya 48% Uganda 7% Rwanda 45% Somalia No data Tanzania 27.4% % Private HRH 55% GPs (PFP only) 74% MDs (PFP only) 58% of all HRH (PFP & PNFP) No data No data No data Source: Private Sector Assessments (Barnes et al., 2010; MoH Uganda et al., 2012; White et al., 2013; Ethiopia Private Sector Assessment (Unpublished draft awaiting MoH approval); Ministry of Health [Rwanda] et al. (2003). A: Where possible, hospitals only were the facilities measured. For Rwanda, includes PFP as a % of all health facilities. For Kenya only, FBOs are included as part of PFP. These modifications are due to data availability. 4.5 Health Insurance Insurance, whether public, private or mixed, is an important driver of growth for the PFP health sector. A number of SSA countries have established or are widening eligibility for social health insurance to increase coverage of the population, including Ethiopia, Kenya and Rwanda in EA. There are currently no major 4 Estimate derived from several USAID and World Bank supported Health System Assessments (Ethiopia, Uganda, Tanzania) and Private Health Sector Assessments (Uganda, Kenya, Tanzania, Namibia, Malawi, Ghana, Nigeria). December 2014 Cardno 14 A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) initiatives in Uganda and Tanzania to expand national health insurance. At the same time, private health insurance schemes have been growing in countries with larger affluent populations and industries capable of funding large employer-based plans, such as in Kenya. However, as shown in Table 4-4, total penetration of health insurance remains low. Even in countries and communities that currently offer some form of insurance scheme, many drugs and services are still not included and must be covered by OOP spending (Economist Intelligence Unit, 2011). Furthermore, there is concern that the fragmented approach to health financing will create a two-tiered delivery system. However, this fragmented approach to financing healthcare is likely to come under scrutiny over the next 15 years as governments, multi-lateral lenders and private investors look for more sustainable ways to finance healthcare in Africa (Economic Intelligence Unit, 2011). Table 4-4 Role of Insurance in EA Health Sectors Public health insurance Availability of Public health expenditure as % of insurance THE, 2012 (%) (e.g. NHIF in Kenya) Ethiopia 48% Kenya 38% Rwanda Tanzania Uganda Somalia 57% 39% 24% N/A 4.6 Social health insurance and community based health insurance National Hospital Insurance Fund (NHIF) Community Based Health Insurance National Health Insurance Fund National Health Insurance Fund N/A Total insurance penetration (Premiums as % of GDP), 2012 0.50% 3.20% 0.90% 0.90% 0.70% N/A Demand for Private Health Services Another way to measure the contribution of the private sector in health is from the demand side. Demographic Health Surveys (DHS) provide data on consumers’ health-seeking behaviour in each EA country, with the exception of Somalia where no DHS was available. As Table 4-5 demonstrates, the public sector is the primary source of healthcare for family planning (FP) (e.g., Ethiopia, 82% public versus 14.7% PFP), maternal delivery (MH) (e.g. Rwanda, 67.9% public compared to 1.0% PFP) and malaria (e.g., Tanzania, 51% public compared to 30% private). International donors heavily subsidize these health areas. However, private health sector also contributes to these priority health services, in particularly Kenya (39.7% in FP, 10.3% in MH and 42.5% in malaria) and Uganda (45.4% in FP, 13.4% in MH and 47.3% in malaria). In contrast, Ethiopia (14.7% in FP and 1.2% MH) and Rwanda (4.2% in FP, 1.0% in MH and 15.7% in malaria) have the smallest percentage of private sector providers offering these same services. It is interesting to note that higher percentages of consumers go to the private sector when seeking care that relies on commodities (e.g. FP, malaria, childhood illnesses) when compared to clinically based services, such as MH. Table 4-5 Health-Seeking Behaviour in the Private For-profit Sector Country Public/Private Public/Private Family planning1 Maternal Delivery1 Ethiopia 82.0/14.7 (PFP only) 8.7/1.2 Kenya 57.3/39.2 (PFP only) 32.3/10.3 Uganda 46.6/45.4 44.0/13.4 (excludes FBO/NGO) Rwanda 92.0/4.2 67.9/1.0 Somalia No data No data Tanzania 65.2/26.4 (PFP only) 41.0/1.6 Public/Private MalariaA,2 68.9/46.6 (MIS) 64.8/42.5 (MIS) 36.0/47.3 (ACTw) 71.7/15.7 (MIS) No data 51.0/30.0 (PSA) All indicators are measured from the most data available as of October 2014. A: Totals may exceed 100% if patients sought treatment at multiple locations for the same illness. Source 1: Demographic Health Surveys (Kenya (2010), Uganda (2011); Rwanda (2010), Tanzania (2011); Ethiopia (2011)). Source 2: ACTwatch Group and PACE/Uganda (2013); Division of Malaria Control [Ministry of Public Health and Sanitation] et al., (2011); Ethiopia Health and Nutrition Research Institute (2012); MAL & OPD Division-RBC Rwanda and ICF International (2014); White et al., 2013. December 2014 Cardno 15 A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) 4.7 Ranking of EA Countries Figure 1-6 pulls together all the factors to rank the EA countries: countries are mapped by GDP levels, use of PFP services in three health areas and a composite of several indicators serving as proxies for the size of the private health sector. Somalia quickly dropped from the analysis due to low GDP as well as lack of data on the health sector. Ethiopia was also eliminated because of the low GDP and the small size of their private health sector. Although Rwanda shows promise – having one of the highest GDPs in the region, growing social health insurance, and important percentage of PFP health infrastructure - it still is primarily a publiclydriven health sector, as evidenced by the low demand for private sector services as shown in Figure 1-6. Based on the analysis, the research team selected Tanzania and Uganda as comparable health markets to Kenya’s and thus potential target markets for future M4P in health programming. Figure 1-6 Ranking of Private Health Sector Development in EA December 2014 Cardno 16 A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) LESSONS LEARNED FROM PRIVATE SECTOR PROJECTS IN COMPARATIVE HEALTH MARKETS AND PSP4H INTERVENTIONS 5 Field-based learning on key intervention types can guide future M4P programmes in health 5.1 Preliminary Findings from the Field Based on the regional comparison in READINESS FOR M4P PROGRAMMING IN EAST AFRICA section above, the research team reviewed documents, grey literature and spoke to contacts in Kenya and the comparison countries (Uganda and Tanzania) for non-PSP4H private sector initiatives serving the poor. Although the team uncovered many examples, very few are well-documented or mature enough to show results. As a result, the team reviewed in detail four projects similar to PSP4H market interventions (see Table 5-1). Findings that might help shape future interventions are described below, in the context of the relevant identified case. Table 5-1 Market Overview of Private Sector Cases in EA Market Intervention Drug Retail PSP4H PHARMNET Network Pooled Procurement Tunza Family Health Network Low-cost, high quality maternal service Low-cost, high quality maternal service Private Community Midwives Network Micro-insurance for health Jacaranda Health (Maternal, Newborn Other examples Tanzania - Accredited Drug Dispensing Outlets (ADDOs) Network Kenya - Kenya Association of Physician (TB) Tanzania - PRINMAT Network of Nurse Midwives (no comparator) and Child Health market research and strategic marketing planning) Jawabu Uganda - Microcare (PCMN) (Bungoma County) Key Learning: Intervene with established health providers and institutions In an effort to reach the poor, many donors consider working with informal providers as one of many strategies. For example, there has been a long history in working with traditional birth attendants to improve home delivery. But working with informal providers is fraught with challenges, as highlighted by the ADDO case. Tanzanians in rural and poor urban areas rely primarily on duka la dawa baridi (DLDB), or informal private drug shops, to get their medicines when public dispensaries and health centers have insufficient stock, are closed or are too far away to be convenient. DLDBs are licensed to sell only non-prescription medicines, but typically they provide a much broader range of products and services. Tanzania is in the process of converting all DLDBs to ADDOs, which are licensed to sell both over-the-counter and a short list of prescription drug products. Located in peri-urban and rural areas, there are currently over 2,000 ADDOs nationwide. These retail outlets offer quality medicines for illnesses commonly found in the communities they serve, open long hours (10-18 hours daily) and six days a week and are convenient for many communities. There have been several reviews of the ADDO program that have concluded that ADDOs are a frontline source of care, although the quality of care they provide can be variable (Thomson et al. 2014; Minzi and Manyilizu, 2013). In many cases, ADDOs provide an essential back-up source of drugs when medicines are not available in public dispensaries. Many of the consumers interviewed for these reviews expressed satisfaction with ADDOs, stating that ADDO staff are friendly and available (White, 2013). In Kenya, PSP4H is partnering with the Kenya Pharmaceutical Association (KPA) to network fully licensed retail pharmacies and drug shops owned or operated by pharmaceutical technologists. KPA members live and work in similar geographic areas as the ADDOs - peri-urban and rural areas. The network, PHARMNET, delivers medicines under a common brand with the promise of higher quality. PHARMNET operators also December 2014 Cardno 17 A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) undergo clinical as well as business training. Through group purchasing, PHARMNET operators will access affordably priced, quality-assured essential drugs from pre-qualified suppliers. In addition, KPA will provide supportive supervision to its network members. Both network concepts are similar in that they: i) target drugs shops and/or pharmacies located in poor communities, ii) bring them under a common name or brand, iii) work with a lower-level pharmacy health cadre, iv) provide clinical and business training, and v) offer supportive supervision and continuous professional development. There are, however, differences between the two networks that will help PHARMNET potentially become self-sufficient in a shorter timeframe. The main difference is pharmaceutical technologists are already recognized, licensed health professionals in Kenya whereas in Tanzania, the ADDOs program invested significant time to formalize the ADDO technician as a licensed health profession. Working with recognized formal providers has created savings in time and costs: > No time required to build political will, develop policies and obtain approval to create a new health cadre which takes time. > All ADDOs outlets had to undergo inspection and in many cases, upgrades, to meet facility standards, adding time and requiring resources to literally build the network. > Donors invested considerable resources in Tanzania to train and improve clinical skills compared to Kenya where the pharmaceutical technologists invested in their own education and met certain educational requirements in order to get certified by the government regulator prior to establishing a practice. A second difference is how the network is managed. PHARMNET leveraged the KPA’s existing infrastructure to create the new brand in Kenya, which will be managed under Nairobi TechPharm (NTP), an independent company owned by KPA, like a business that must be self-sustaining. In exchange for an annual membership fee, KPA offers its members a full range of services, including: i) use of unifying brand name and logo (members pay 25% for the pharmacy branding themselves); ii) standardized operating procedures, iii) quality assurance across the network; and v) pooled procurement of essential medicines from pre-qualified suppliers. In the case of ADDOs, now that donor funds have ended, the program management has been transferred to the Tanzania Federal Drug Authority, a government regulatory agency. It is unclear what will happen to the ADDOs, an ostensibly private establishment, under TFDA management (Dr. Ogillo, Association Private Health Facilities in Tanzania, interview, 2014). Key Learning: A market intervention has to be easy or else it will not be adopted Pooled procurement is considered one of many strategies to help private providers and pharmacies access affordably priced drugs and assure quality of drugs in the private sector. As observed in the ADDOS network, the cost of drugs remained a barrier to access. Although ADDOs are better stocked than the public facility, their prices are often out-of-reach for the poorest because they had to purchase their drugs in the private market. But pooled procurement, or any market intervention that makes business sense, still has to be easy for the private provider to adopt as in the case of Kenya Association for the Prevention of Tuberculosis and Lung Disease (KAPTLD) and the Tunza Family Health Network of providers. Over 15 years ago, a group of prominent Kenyan chest physicians identified a need for quality, inexpensive TB products and training on appropriate treatment regimes in the private health sector. They formed and championed KAPTLD as a mechanism to address this need among similar specialists. Over the years, with donor support, KAPTLD has worked to improve access to quality TB medicines, strengthen the quality of care of TB services and reduce the cost of TB care in the PFP sector. To access more affordably priced, quality TB drugs, KAPTLD decided not to accept free drugs donated by the Kenyan government, in part due to concerns about quality as well as the reputational implications of using local, generic products. Instead they pursued a collaboration approach combining orders for TB drugs. KAPTLD members, comprised mostly of private hospitals, successfully negotiated a reduced price on behalf of their members with an international pharmaceutical manufacturer. The agreement was a “win-win” for both KAPTLD members, saving them time and costs when ordering TB drugs, and for the manufacturer, who was looking to provide its TB drug to the Kenyan market at a reduced price as part of its social responsibility program. December 2014 Cardno 18 A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) KAPTLD was also able to leverage its established relationship with major drug wholesalers and distributors in Kenya, where in many cases, they were already supplying KAPTLD member hospitals. As a result, KAPTLD was able to outsource the distribution of the TB drugs through existing supply channels at no extra costs. Each hospital submits their order to KAPTLD, who in turn pulls the orders and ensure the TB drugs are added to the wholesaler/distributor routine deliveries to the member hospital. KAPTLD members recognized the benefits of combining orders early on. Throughout this process, KAPTLD worked closely with the public sector’s national TB program to qualify training materials and guarantee its members reported to the MOH. The members feel confident they are compliant with MOH quality standards and they can now provide long-term specialty treatment with affordable, quality products. In another example, PS-Kenya, the franchisor, offers pooled procurement through the Mission for Essential Drugs and Supplies (MEDS) as a service for the Tunza Family Health Network providers. MEDS, a faithbased organization, is one the largest wholesalers/distributors in Kenya serving not only FBOs health facilities but also private health facilities serving the poor. Tunza is composed of small private health practitioners, largely comprised of nurses and a few clinical officers, located throughout Kenya. Most of the Tunza providers are small owner-operated outlets, typically consisting of a reception, consultation room and a procedure room. Tunza clinics promise friendly, quick, affordable and high-quality family planning services by a qualified and trained provider. Community health workers, called Tunza Mobilizers, help create demand not only for family planning but also for the Tunza providers. Although many Tunza providers stated that purchasing drugs through a pooled system was a major attraction to join the network, uptake of the MEDS service has been low; currently only 22% of the 354 Tunza clinics participate in the pooled procurement. A PSP4H (PSP4H, 2014b) assessment revealed that many Tunza providers found the MEDS application and system complicated and difficult to understand. Although the providers would greatly benefit from reduced prices on quality drugs, the opportunity cost is too great. These small businesses, often owner-run with no or few employees, could not afford to take the time away from paying clients to invest in learning new systems. As a result of the study, PSP4H is working with PS-Kenya and MEDS to streamline the order forms and make the system more user-friendly and accessible. Key Learning: Plan early for network management to be financially sustainable Networking of private providers is in vogue among the global health community as a strategy to “organize” solo practitioners, improve their quality and/or independent accreditation and extend their reach among underserved population groups. The assumption is that consumers will actively seek services among branded facilities offering quality services and safe drugs, all at an affordable price. Managing provider networks, whether it is a chain of retail pharmacies or a group of private providers, is a complex task requiring a formal organizational structure. As the network examples show, their management structures vary, raising questions of long-term sustainability. The Tunza Network is a social franchise managed by PS-Kenya, a local NGO. To date, the management structure for the network is integrated into PS-Kenya’s overall portfolio of donor-funded programs with a dedicated Senior Clinical Manager for quality, two Quality Assurance Managers, and 15 Quality Assurance Officers who supervise clinics in the field. They also have a business team made up of a Senior Business Manager and two Business Officers, who assist with financing support through the PharmAccess Foundation. Beyond that, PS-Kenya staff perform many functions of a network management entity, such as branding, marketing, demand creation and clinical training, which are supported by donor funds. If Tunza Network were to become independent, PS-Kenya will need to develop a revenue-generation model and split the network management staff from those working on PS-Kenya subsidized programs. Tunza are currently discussing sustainability options, including spin-off from the NGO, but that has not yet been determined. The Private Nurses and Midwives Association Tanzania (PRINMAT) was established in 2000 as a professional association representing private sector nurses and midwives. There are 52 member owned maternity clinics that work under the PRINMAT brand and are distributed through 17 regions (with more planned for the rest of the country) to increase access to maternal, child and reproductive health services. PRINMAT offers its members several membership benefits such advocacy efforts surrounding policies and practice of nursing and midwifery, education and training workshops, supportive supervision and assistance in registering a new maternity and nursing home. They also give loans and credit to their members in order for them to upgrade their facilities and offer flexible payment terms to their clients. Some call into question if PRINMAT is really a December 2014 Cardno 19 A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) network, with the overlap between the association and network functions and the association subsidizing the network. The viability of the network remains in question until the benefits of being a network provider is more clearly defined for PRINMAT members. The management structure of PHARMNET is similar to PRINMAT’S. KPA’s secretariat overseas operations of the PHARMNET network offering strategic and regulatory support; and coordinating and mobilizing pharmacies to join the network. A few years ago, KPA had considered establishing this network but due to lack of information on how to implement the network, this initiative was delayed. The current attempt benefits from growing experience in networking private providers and the fact that the association is already established and functioning. PHARMNET is in its initial stages of network establishment (currently close to 100 branded pharmacies have completed their induction training), the association will subsidize the network management through the pro bono service of the directors until they can earn revenue from provider fees and pooled procurement. The pooled procurement is being conducted through the independent company, NTP, which is managing the network (under the aforementioned pro bono management). Once the procurement function becomes robust, a small mark-up will be added on the drugs to support 5-6 staff running the network secretariat. In the case of KAPTLD, after many years of operations, donor funds supporting the project ran out. However, KAPTLD members valued the benefits received from the program and looked for ways to keep it going. First, they defined the secretariat’s core activities and the number of staff needed to run the network. Secondly, they reduced the number of secretariat staff. Lastly, they are exploring ways to become financially selfsufficient. Just as PHARMNET envisions doing, KAPTLD added a small mark-up onto the cost of all the drugs ordered through the program, though they are still working to determine what mark-up is sufficient to cover their operational costs while at the same will not adversely impact consumer price. Key Learning: A successful business model is equally as important as a high-quality service Too many mothers in Kenya die during delivery: maternal mortality remains high at 488 deaths per 100,000 live births (KNBS and ICF Macro, 2010). In response to the maternal health crisis, Jacaranda Health opened its first maternity centre located in the outskirts of Nairobi in the year 2012. Jacaranda Health aims to build a network of private maternity clinics in resource-poor settings that combines quality and affordability. Their model focuses on a comprehensive set of maternal and newborn child services supporting non-complicated deliveries at a secondary level facility with referral of complicated pregnancies to a tertiary hospital. To date, Jacaranda Health has delivered maternal healthcare to over 4,000 women and delivered more than 250 babies at their 12-bed maternity hospital. Jacaranda relies on a number of management innovations to keep costs low and prices affordable. They include clinical task-shifting, standardization of operating procedures, and focus on cost-effectiveness. Nevertheless, the success of this business model is highly dependent on high client volumes, which the facility does not currently have. There is low uptake of its services and the facility is unable to convert its prenatal maternal health services into facility deliveries. There are several reasons why Jacaranda is underutilized: > Lack of accurate information on market size; > Limited information on community perception of services it offers; > Limited capacity to deal with complications (i.e. offer caesarean deliveries); > Inappropriate pricing for different consumer segments; > Competition (unfair) from other providers, particularly the public health facilities. Although the clinical delivery model is sound, the business model requires significant improvements. PSP4H supported a health market research to help Jacaranda Health better understand its target population (PSP4H, 2014c). Some of the findings from this market research were: > Existing clients had positive perceptions and experiences at Jacaranda Health and were satisfied with the services in terms of access to facility, cost of services and level of customer care delivered. > A high number of respondents (80.8%) had not used Jacaranda services, primarily because of low awareness (51.9%) of the facility and its services. Another important percentage (39.3%) stated quality was the reason they did not use Jacaranda Health. December 2014 Cardno 20 A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) > Although Jacaranda Health states that its target market is bottom of the pyramid, the study findings show that they actually serve a significant percentage of middle class consumers. > Clients are willing to pay for private MNH services, irrespective of the existence of subsidized or free services from public health facilities. Clients look for convenience (e.g. location, hours) and comprehensive care (e.g. one-stop shop) to save time. > Availability of emergency care is a factor in selecting which health facility to use. > Cost, although important, is not the main driver in choosing a healthcare provider for MNH. Clients will travel extra distance for a quality healthcare provider. Using the findings from the consumer research, PSP4H is supporting Jacaranda Health to develop and implement a strategic marketing plan with appropriate pricing of service bundles that will attract its originally intended market segment – low-income earning mothers and hence increase the number of facility deliveries. Key Learning: Market interventions with potential scale may require more time and several attempts Founded in 2010, Jawabu Empowerment is a for-profit commercial company with the mission of fulfilling key financial needs of Kenyans working in the informal or Jua Kali sector. The informal sector represents about 83% of the total employment in Kenya and generates 28% of GDP. Jawabu’s approach is to influence healthseeking behavior of Jua Kali Association members by encouraging savings for health. Jawabu developed Afya Poa, a micro-insurance product, that is a combination of traditional health insurance covering inpatient care and Medical Savings Accounts (MSAs) covering outpatient care. The MSA-style approach presents a departure from conventional micro-insurance schemes for health where the outpatient benefit is insured. Outpatient insurance has been cited as the biggest reason for losses and fraud in the insurance industry. One of the ways to manage this is to have the user own the money and participate fully in deciding what this money will pay for but limit the spending only to health related expenditures. Although an innovative health insurance product, Afya Poa, continues to face challenges, particularly identifying an underwriter, negotiating with Jua Kali groups and regulatory barriers. The partnership with Jawabu is one of the longest-running market interventions in the PSP4H portfolio and will still require a longer period of investment. Fortunately Jawabu has overcome one its greatest hurdles - securing an underwriter for Afya Poa. If successful, Afya Poa can potentially reach 8 million consumers through Jua Kali Associations. Microcare, which was managed by Microcare Uganda Limited, is another example of a micro-health insurance product targeting the same consumer group. Similar to Afya Poa, Microcare’s strategy was to leverage community groups and microfinance institutions (MFIs) but efforts to sell policies through MFIs proved surprisingly challenging. Although MFI clients needed an insurance product, Microcare’s sales representatives failed to develop sufficient levels of trust with them. The sales representatives underestimated the amount of time needed to convince this target group to buy health insurance and were discouraged by the small commissions that the small premiums generated. Microcare’s sales staff were provided access to the MFIs’ clients but received little support from the MFI’s field staff who were not trained to sell insurance. The poor working relationship with MFIs resulted in limited sales success (Greyling, 2013). Microcare took time and effort but ultimately failed because of solvency issues; medical insurance is a high cash turnover business that requires significant reserve cash and liquidity, particularly in the initial phases where customer premiums may not be sufficient to cover the amounts claimed. Yet lessons from Microcare’s experience can be applied to Afya Poa: > Pricing strategies need to take account of the fact that premiums are paid for a year in advance. Any variations on pricing assumptions, such as adverse selection or increased costs, will need to be carried by the insurer through the policy term. > Insurers that aim to deploy an aggressive premium growth strategy must ensure that they have the capital base to maintain solvency. Reserves usually cannot be funded from premiums because they are needed to pay on-going claims. > Careful tracking of claim patterns among individual health providers and among clients is critical and must be pro-actively managed to maintain solvency. December 2014 Cardno 21 A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) > Aligning the interests of providers, patients, and the insurer through incentives and risk-sharing (e.g. MSAs) may be a more effective way to control claim costs than elaborate external control mechanisms. Despite concerns often raised about over-valuing services and pricing out the working poor, both these cases show consumers’ willingness to pay and a potentially large market if the barriers to solvency, including obtaining a willing underwriter, are overcome. 5.2 Lessons Learned from other Regions There is growing but albeit still small literature on the PFP health providers serving the poor and the business practices that contribute to their survival and growth. Though these lessons come from outside the region, the key business practices relevant to the three identified EA health markets are: > Urban locations: The majority of PFP providers are located in urban areas with easier access to many potential customers. In a few cases, the PFP providers focused on smaller towns lacking secondary healthcare service. PFP strategy is to fill the geographic and hours available gap in service provision and reduce costs to patients associated with travel time and lost wages (Tung, 2014). Also, one avoids competition with the high-end private hospitals located in metropolitan areas. Examples include Vaatsalya, LifeSpring and CARE hospitals, all located in India. > Non-traditional marketing techniques: Community outreach, similar to the Tunza Community Mobilizers, is the main strategy to reach low-income groups given the informational and education component explaining when and why to seek healthcare. For poorer clients, personal and continued contact along with targeting specific population groups and social networks have been successful strategies to attract new and retain clients to private facilities (Tung, 2014). Aravind Eye Care and Naranyana Hrudayala Heart Hospital provide health camps to reach patients in rural areas (Bhattacharyya et al., 2010). > Customer orientation: A PFP provider must deliver better customer service than government run facilities to be competitive (Tung, 2014). Several tactics include: i) locating facilities closer to lower-income populations; ii) opening longer hours to accommodate client work schedules; iii) making appointments instead of queuing and iv) creating a culture of respect for the patient. To serve even remote areas, Aravind has set up internet kiosks in remote villages by a community member who takes pictures of the potential patient’s eye and sends the images to an Aravind physician along with medical history (Bhattacharyya et al., 2010). > Flexible terms of payment: In response to the target population’s preferences and purchasing habits, many PFP companies serving the working poor have created flexible pricing and payment terms (Bhattacharyya et al. 2010, Tung 2014). For example, private clinics and hospitals offer tiered pricing for private, semi-private and general wards. Others emphasize clear and transparent pricing and billing to help alleviate the uncertainty of paying for healthcare. Finally, several of the PFP providers offered micro-credit to finance more expensive procedures. > High volume: In order to make a profit, several of the PFP health companies emphasized volume by specializing on relatively simple, low-cost services (e.g. Narayan Hurdayalaya Heart Hospital is the larger provider of paediatric heath surgeries in the world, and Aravind, India pioneered high volume, low cost specialty services). > Low unit costs: All PFP organizations studied consistently looked for ways to cut costs including: i) avoiding costly infrastructure investments by leasing the land and/or building; ii) eliminating non-essential services (e.g. food services) and contracting out expensive services (e.g. ambulance, blood banks and diagnostics) and iv) reducing human resource costs through task shifting and creative compensations packages (Tung, 2014). > Narrow clinical/technical focus: Almost all of the large-scale PFP companies in this space concentrate on just a few medical processes (Bhattacharyya et al. 2010; Tung, 2014). This allows them to market their services on a large scale, reduce costs and streamline operations to target poor patients. The predictability of the problems and treatment strategies also allows PFP providers to task-shift to trained lower-cadre health personnel while continuing to ensure quality. December 2014 Cardno 22 A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) There are few examples of PFP companies serving the poor that have been able to achieve scale (Bhattacharyya et al. 2010; Tung, 2014). In order to be successful, PFP companies often required partnerships with the government or support from social health insurance schemes (Tung, 2014). Such risk-sharing schemes are promising ways for governments and donors to engage the PFP to reach the poor on a larger scale in a sustainable way, particularly in difficult-to-reach geographic areas or in important health areas. December 2014 Cardno 23 A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) 6 CONCLUSIONS AND RECOMMENDATIONS Key findings from analysis and implementation for future M4P programs The goal of this report is to share lessons learned on how to work with the private sector in health using a market based approach. The lessons are based on comparative research of PSP4H market interventions and other private sector programs in similar health markets in East Africa. Emerging lessons include: 1. M4P approach works to analyse and shape health markets but with important differences The M4P framework is robust enough to describe and analyse what is happening in select health markets. There are, however, several key differences between the health sector and other economic sectors. The significant differences between other sectors and health are detailed in this report; although important, these differences should not impede using M4P as an approach to understand how to engage the PFP sector in health. 2. Implementing M4P differs from traditional donor programming M4P requires that donors and implementing partners play a facilitative role. By definition, facilitation of market change is a temporary role with the goal of exiting the market to foster long-term self-sustainability. There are times, however, when it is appropriate for a donor to “prime the market” through direct intervention in order to achieve critical public health objectives. It is critical when “priming the market” to have an exit strategy in place from the outset of the project. 3. PSP4H has developed analytical approaches that can jumpstart future M4P programmes A market-based approach requires a full analysis of a country context focusing on understanding the health sector, the poor and the PFP in health. The report shares many suggestions, such as innovative ways to define the poor and the need to engage PFP sector early, only to name a few, that can save time in applying the M4P approach in other countries. 4. Using a portfolio approach helps minimize risk when facilitating change in health markets A portofolio approach offers programmes like PSP4H three essential elements: > Adaptability: allowing a programme to shut down unsuccessful interventions or to further invest in promising ones; > Flexibility: permitting a programme to allocate its budget according to the size and scope of each intervention and therefore manage to the bottom line of the total portfolio; and > Innovation: enabling a programme to take risks and experiment in new health markets, with different PFP actors and new approaches. 5. Look for opportunities in markets that meet this set of key conditions: > Target the “working poor” who have demonstrated demand for and willingingness to pay for private services and products. > Focus on geographic areas with a critical concentration of formal PFP providers with existing networks and demonstrated clientele. > Stay out of donor-funded areas to avoid “overcrowded” health and geographic areas when exploring potential market opportunities. > Explore working in stated underserved health areas (identified by the poor consumers) and that are of interest to the PFP sector, such as diagnostics, dentistry, optometry, and NCDs among others. 6. Field-based learning can guide design and implementation of market interventions In a short timeframe, the PSP4H programme has several suggestions that may help increase the likelihood of success with market interventions: > Start with formally recognized (i.e. not informal) health providers and established institutions and networks to save time and energy in trying to create them December 2014 Cardno 24 A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) > Introduce market interventions that are easy to adopt and do not take the PFP providers away from core, revenue-generating business activities > Plan early, even if initially donor-supported, for network management to be financially sustainable > A successful business model should also provide high-quality a service when targeting the poor > Market interventions with potential scale involving system changes (e.g. policy reforms, health financing, etc.) may require more time and several attempts 7. Promising market interventions share several key business practices Both the PSP4H market interventions and emerging literature demonstrate sound business practices that increase the likelihood of sustainability. They include: i) concentrating in urban locations, including as periurban areas and smaller towns, ii) carrying out non-traditional marketing techniques designed to reach the working poor; iii) delivering better customer service than public facilities; iv) offering flexible terms of payment in response to the working poor’s purchasing habits; v) emphasizing high volume by specializing on relatively simple, low-cost services; vi) consistently looking for ways to cut costs; and vii) keeping a narrow clinical/technical focus. 8. PFPs serving the poor may have to partner with the government to achieve scale Risk-sharing schemes, such as partnerships with the government or financial support from social health insurance schemes, are promising ways for governments and donors to engage the PFP to reach the poor on a larger scale in a sustainable way. 9. Consider Tanzania and Uganda as target countries for expansion of M4P in Health in the region In the region, Tanzania and Uganda have most similar health systems to Kenya’s; expanding the M4P approach in health to those countries will likely be easier than in other countries in the region. “The market is not slow when everything is ready and the price is right” -Ron Ashkin, PSP4H Kenya Team Leader December 2014 Cardno 25 A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) 7 References. ACTwatch Group & PACE/Uganda, 2013. Household Survey, Uganda, 2012 Survey Report. Washington, DC: Population Services International. Available at: www.actwatch.info. Ashkin, Ron. Public Service Strengthening Using Market Systems Development Strategies: M4P and Health in Kenya. Presentation delivered at 9th Annual BDS Conference, Mombasa 27th November 2013 Berg, Ruth (2013). What do we really need to know? M&E and its application to M4H. Presentation delivered at DFID-sponsored on Introduction to M4H, January 2013 Barnes, J., B. O'Hanlon, F. Feeley, K. McKeon, N. Gitonga and C. Decker. (2010). Private Health Sector Assessment in Kenya. Washington DC: World Bank Group. Bhattachayya, O., S. Khor, A. McGahan, D. Dunne, A. Daar, and P.A. Simon, (2010). Innovative Health Service Delivery Models in Low and Middle Income Countries – what can we learn from the private sector? Health Research Policy and Systems, 8:24. Central Statistical Agency [Ethiopia] and ICF International. 2012. Ethiopia Demographic and Health Survey 2011. Addis Ababa, Ethiopia and Calverton, Maryland, USA: Central Statistical Agency and ICF International. DFID (2013). Introduction to Markets for Health. Workshop organized by The World Bank Institute, January 2013. Division of Malaria Control [Ministry of Public Health and Sanitation], Kenya National Bureau of Statistics, and ICF Macro, (2011). 2010 Kenya Malaria Indicator Survey. Nairobi, Kenya: DOMC, KNBS and ICF Macro. Economist Intelligence Unit, (2011).The future of healthcare in Africa. London, England: The Economist Ethiopian Health and Nutrition Research Institute, (2012). Ethiopia National Malaria Indicator Survey 2011. Addis Ababa, Ethiopia: Ethiopian Health and Nutrition Research Institute Gitonga, Nelson, (2012). Ethiopia Health Systems Assessment Report. Washington D.C.: Abt Associates Greyling, L., (2013). Microcare Insurance Uganda – Case Study. Geneva: ILO Gwatkin, D., S. Rutstein, K. Johnson, A. Suliman, A. Wagstaff, and A. Amouzou, (2007). Socio-Economic Differences in Health, Nutrition and Population Within Developing Countires. Washington D.C.: The World Bank Group. Hozumi, D., L. Frost, C. Suraratdecha, B.A. Pratt, Y. Sezgin, L. Reicchenbach and M. Reich, (2008). The Role of the Private Sector in Health: A Landscape Analysis of Global Players’ Attitudes toward the Private Sector in Health Systems and Policy Levers that Influence these Attitudes. Results for Development Technical Partner Paper No 2. Washington D.C.: PATH and Harvard School of Public Health Kenya National Bureau of Statistics (KNBS) and ICF Macro. (2010). Kenya Demographic and Health Survey 2008-09. Calverton, Maryland: KNBS and ICF Macro. Makinen, M., H. Waters, M. Rauch, R. Bitran, L. Gilson, D. McIntyre, and A. L. Prieto, (2000). Inequities in Health Care Use and Expenditures: Empirical Data from Eight Developing Countires and Countries in Transition. Bullentin of the WHO. Malaria and Other Parasitic Diseases Division (MAL & OPD Division-RBC) [Rwanda] and ICF International. (2014). Rwanda Malaria Indicator Survey 2013. Rockville, Maryland, USA: MAL & OPD Division-RBC and ICF International. Ministry of Health [Rwanda], National Population Office [Rwanda], and ORC Macro, (2003). Rwanda Service Provision Assessment Survey 2001. Calverton, Maryland: Ministry of Health, National Population Office, and ORC Macro. Ministry of Health (MoH) Uganda and Makerere University School of Public Health. (2012). Uganda Health System Assessment 2011. Kampala, Uganda and Bethesda, MD: Health Systems 20/20 project, Abt Associates Inc. December 2014 Cardno 26 A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) Minzi, O.M and V.S Manyilizu. (2013). Application of Basic Pharmacology and Dispensing Practice of Antibiotics in Accredited Drug-dispensing Outlets in Tanzania. Drug, Healthcare and Patient Safety 2013:5, 5-11. National Bureau of Statistics (NBS) [Tanzania] and ICF Macro. (2011). Tanzania Demographic and Health Survey 2010. Dar es Salaam, Tanzania: NBS and ICF Macro. DHS National Institute of Statistics of Rwanda (NISR) [Rwanda], Ministry of Health (MOH) [Rwanda], and ICF International, (2012). Rwanda Demographic and Health Survey 2010. Calverton, Maryland, USA: NISR, MOH, and ICF International. Price Waterhouse Cooper (PWC), (2011). Build and Beyond: The (r)evolution of Healthcare PPPs. Delaware: Health Research Institute. Private Sector Innovation Programme for Health (PSP4H), (2014a). A Formative Survey of the Private Health Sector in Kenya in the Context of the Working Poor. Nairobi: PSP4H Private Sector Innovation Programme for Health (PSP4H), (2014b). A Feasibility Study of Pooled Procurement Models for PSKenya Tunza Providers. Nairobi: PSP4H Private Sector Innovation Programme for Health (PSP4H), (2014c) Understanding Community Perception of Maternal and Child Health Services among Low-income Populations in Nairobi, Kenya: A Case of Jacaranda Health. Nairobi, Kenya: PSP4H Tanzania Commission for AIDS (TACAIDS), Zanzibar AIDS Commission (ZAC), National Bureau of Statistics (NBS), Office of the Chief Government Statistician (OCGS), and ICF International. (2013). Tanzania HIV/AIDS and Malaria Indicator Survey 2011-12. Dar ss Salaam, Tanzania: TACAIDS, ZAC, NBS, OCGS, and ICF International. The Springfield Centre, (2014). The Operational Guide for the Making Markets Work for the Poor (M4P) Approach, 2nd edition funded by SDC & DFID: Springfield Centre Thomson, R, B. Johanes, C. Festo, A. Kalolella, M. Taylor, K. Bruxvoort, S. Tougher, Y. Ye, A. Mann, R. Ren, B. Willey, F. Arnold, K. Hanson and C. Goodman, (2014). An Assessment of the Malaria-related Knowledge and Practices of Tanzania’s Drug Retailers: Exploring the Impact of Drug Store Accreditation. Poster presentation, American Society of Tropical Medicine and Hygiene. Tung, E. and S. Bennett, (2014). Private sector, for-profit health providers in low and middle income countries: can the poor at scale? Globalization and Health: 10:52 Uganda Bureau of Statistics (UBOS) and ICF International Inc., (2012). Uganda Demographic and Health Survey 2011. Kampala, Uganda: UBOS and Calverton, Maryland: ICF International Inc. White, James, B. O’Hanlon, G. Chee, E. Malangalila, A. Kimambo, J. Coarasa, S. Callahan, I. Ron LEvey, and K. McKeon, (2013). Tanzania Private Sector Assessment. Bethesda, MD: Abt Associates Inc. World Bank. (2014). World Bank Indicators. Washington DC: World Bank. Swiss Agency for Development and Cooperation (SDC) and UK Department for International Development (DFID). (2008). A Synthesis of the Making Markets Work for the Poor (M4P) Approach. London, England: UK Department for International Development (DFID) and the Swiss Agency for Development and Cooperation. December 2014 Cardno 27 A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) 8 APPENDIX 1: KEY M4P CONCEPTS ADAPTED TO HEALTH Crowding Out: A policy or program intervention that causes existing actors in a health market to decrease an activity (e.g. investment, production, donor subsidies) or withdraw completely. Evidence of crowding out includes declining market share of some market actors or a reduction in the number of market actors. Crowding In: A policy or program intervention that causes existing market actors to: i) better perform a current and/or increase a health related activity and/or ii) motivates new players to enter a health market. Crowding in is demonstrated by shifting market shares or increasing the number of market players or increasing the level of investment current market actors are making. Demand: Demand in health is composed of two elements: 1) demand for and actual use a health service or product and 2) demand for a health service or product that would have taken place if a consumer who wanted to use the product or service had had access to it. In contrast, need is an assessment of consumers’ physical requirements to maintain some level of well-being or health. Consumers’ self-perception of their needs links closely to demand. The perception of health experts of consumers’ needs may have little or no relation to demand. Facilitation / Facilitator: Action or agent that is external to a health market system but seeks to bring about change in order to achieve a public health benefit through systemic change. Financing Functions: A range of funding activities that government and other market players perform to operation of a health market; these activities typically aim to achieve higher access, better quality, and/or lower financial risk in the provision of services and/or products than would be achieved by the “natural market.” Financing functions can be analyzed on the supply side (facilitating supplier access to credit, subsidizing supplies or supplier inputs) or the demand side (subsidizing purchases through vouchers or insurance, pooling of purchases, pooling of risk, prepayment and health savings schemes). Funder: An organization, such as a social insurer or development agency, which provides resources aiming to influence or “structure” market operations in order to increase access, strengthen quality, and/or minimize financial risk. Health System: The sum of all organizations, people and actions whose primary activity is to directly, or indirectly, promote, restore or maintain health. A health system includes both public and private institutions (see below) entities engaged in financial, policy, regulatory, research and academic, and provision of healthcare. Impact: The long-term effects on identifiable populations or groups produced by a project or programme. Impact Logic: A model showing the chain of causality through which a programme’s activities contribute to a health sector objective. Impact logics derive from the specific content of an intervention and the setting within which it will be implemented. Impact Trajectory: The impact of an intervention over time; also referred to as “impact profile”. Implementing Partner: An organization that is contracted by a Funder to implement a market development or market structuring initiative. Institutions: Social, political and economic structures and mechanisms – formal or informal – in a society or economy that shape health market players’ incentives and behaviours. Institutions establish the “rules of the game” through supporting functions and/or establishing regulations, laws and policies. Interconnected or “Linked” Markets: Markets which influence the operation of another health market – usually related “upstream” or “downstream” to the specific health market. Intervention: A defined set of temporary activities or actions seeking to effect change in a health system. Market Player: Individuals or organization active in a market system: including public, private for-profit and private not-for-profit groups. December 2014 Cardno 28 A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) Market Priming (also known as “pump-priming”): A temporary intervention to promote demand and stimulate commercial markets by demonstrating the commercial viability of the activity (e.g. demonstration effect) or by strengthening the enabling environment supporting the activity in a health market. Market: A set of arrangements by which buyers and sellers are in contact to exchange goods or services in health; the interaction of demand and supply for a health service or product. Market for the Poor (M4P): An approach that focuses on changing market systems to benefits the poor. Market Segment: A subset of consumers in a market with a common set of demographic, psychographic or biological characteristics (e.g. pregnant women living in rural areas in the lowest income quintile). Market Segmentation Strategy: A strategy that involves dividing a broad market (group of consumers) into subsets of consumers, who have common characteristics, and then designing and implementing strategies to target their needs and desires using media channels, marketing messages, and differentiated products and distribution approaches that best allow reaching them. For social products, market segmentation strategies are often deployed to target subsidies on low-income customers. Market Structure: Organizational or competitive characteristics of a market; often with reference to the number of organizations in a market that produce identical goods and services. Market structure has great influence on the behaviour of individuals firms within the market. Market System: A system comprised of multiple players (private sector, government, representative organisations, civil society, etc.) carrying out multiple functions (core, rules and supporting) through which a series of exchanges (transaction) takes place in an ongoing manner. Output: Health products and services resulting directly from project or programme activities. Adapted from A Synthesis of Making Markets Work for the Poor and World Bank DFID Training Course. December 2014 Cardno 29 A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) 9 APPENDIX 2: INTERVENTION SCREENING TOOL Intervention: Area: IM: Step Evaluation 1. Relevance Is the proposed intervention: In the health sector (preferably in a priority sub-sector)? Pro-poor? Private sector driven? For profit? Innovative? Addressing a systemic constraint? Overall Relevance 2. Impact Does the proposed intervention have: Scale (significant number of beneficiaries)? Depth (change at root cause level)? Likelihood of making a positive change (feasible business case)? Space to grow (not crowded out by subsidies and/or other donor projects)? Attribution (can change be attributed to programme assistance)? Overall Impact 3. Engagement Is there an identified private sector partner (or partners) who: Name: Has mutual objectives? Is willing to invest in the intervention? Will share data with PSP4H? Overall Engagement December 2014 Cardno 30 Comments A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) 4. Do No Harm Has the impact of the potential intervention on all stakeholders been considered so there will be no adverse unintended consequences? Overall Do No Harm Overall Evaluation December 2014 Cardno REJECT/ ACCEPT 31 A Comparative Analysis of Health Markets and Private For-Profit, Pro-Poor Interventions in East Africa Private Sector Innovation Programme for Health (PSP4H) 10 APPENDIX 3. DESCRIPTION OF PSP4H PROGRAMME For Potential Partners: Engaging with the Private Sector Innovation Programme for Health (PSP4H) The Private Sector Innovation Programme for Health (PSP4H) is a two year UK Government-funded action research project exploring a market systems approach to development entitled ‘Making Markets Work for the Poor’ (M4P). The programme fosters partnerships with for-profit private sector healthcare providers who have innovative ideas for serving the poor and wish to develop them in a sustainable manner. PSP4H encourages private sector investment to serve the poor. The target beneficiaries for partnerships are for-profit health enterprises that serve the working poor. PSP4H will facilitate new private sector approaches and invest in purely developmental activities such as market intelligence, business modeling, capacity building, introduction of innovations and risk sharing. PSP4H acts as a consulting organisation – an innovation centre for private for-profit health sector investors – but is not a market player or a financing institution. How to Work With PSP4H Following are the steps in engaging with PSP4H for potential private sector partners interested in testing propoor business models through action research – what we refer to as ‘interventions’: ENGAGEMENT • Initial stakeholder interviews and discussions with PSP4H regarding areas of opportunity • Identification of potential action research interventions that are of mutual benefit • Screening of ideas for pro-poor/M4P Relevance, Impact, Engagement, Do No Harm PLANNING • Agreement on intervention concept • Concept note development in collaboration with PSP4H (Including business case, budget) • Concept note submission and review • Concept note decision: approval/rejection IMPLEMENTATION • Feedback to partner; if approved, execute partnership agreement/MoU • Action planning and project implementation • Continuous monitoring -data gathering, analysis, operating adjustments • Documentation and dissemination of lessons learned, scale up when successful Any private sector enterprise with an innovative, sustainable, for-profit idea on how to better serve the poor by increasing access and/or improving the quality of health services/products is eligible to work with PSP4H. PSP4H and the partner organisation will enter into an agreement that specifies the mutual objectives of the partnership and the roles and responsibilities of each party, which will then fund its own activities. The partner retains control of business outcomes and can invest in scale-up. December 2014 Cardno 32
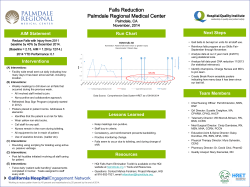




© Copyright 2026