
Evidence of a Graft-Versus-Lymphoma Effect
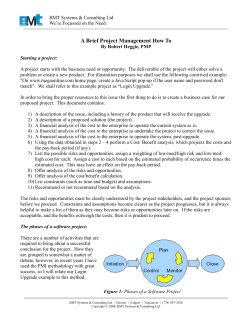
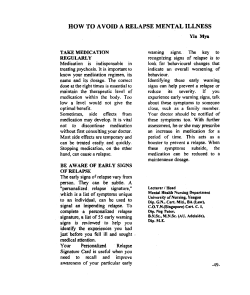
From www.bloodjournal.org by guest on December 29, 2014. For personal use only. Evidence of a Graft-Versus-Lymphoma Effect Associated With Allogeneic Bone Marrow Transplantation By Richard J. Jones, Richard F. Ambinder, Steven Piantadosi, and George W. Santos The existence of an immunologic antileukemia reaction associated with allogeneic bone marrow transplantation (BMT) is well established. However, a similar graft-versus-tumor effect against lymphomas has not been demonstrated. We analyzed the results of BMT in 118 consecutive patients with relapsed Hodgkin‘s disease or aggressive non-Hodgkin’s lymphoma. The 38 patients less than 50 years of age with HLA-matched donors had allogeneic marrow transplants, and the other 80 patients received purged autologous grafts. The median age was 26 years in both the allogeneic and the autologous graft recipients. The patient’s responset o conventional salvage therapy before transplant was the only factor that influenced the event-free survival after BMT (P < .001). Both the patient’s response t o salvage therapy before BMT (P < .001) and the type of graft (P = .02) significantly influ- enced the probability of relapse after BMT. The actuarial probability of relapse in patients who responded t o conventional salvage therapy before BMT was only 18% after allogeneic BMT compared with 46% after autologous BMT. However, the actuarial probability of event-free survival at 4 years was the same, 47% versus 41%. for patients with responsive lymphomas who received allogeneic and autologous transplants, respectively (P = .8).The beneficial antitumor effect of allogeneic BMT was offset by its higher transplant-related mortality (P = .01), largely resulting from graftversus-host disease. Allogeneic BMT appears t o induce a clinically significant graft-versus-lymphoma effect. The magnitude of this effect is similar t o that reported against leukemias. 0 1991 by The American Society of Hematology. A involvement by lymphoma at the time of BMT. All patients gave informed consent for study participation as approved by the Johns Hopkins Joint Committee on Clinical Investigation. Treatment protocol. Patients less than 50 years old with an HLA-identical (or one antigen mismatched) family member received allogeneic marrow transplants. All other patients received autologous transplants. Autologous bone marrow was obtained, treated with 4-hydroperoxycyclophosphamideor pan-T cell monoclonal antibodies (four patients), and stored before beginning the BMT preparative therapy, as previously de~cribed.’.~ Preparative therapy consisted of busulfan followed by cyclophosphamide in patients who had previously received over 3,000 cGy of radiation to either their lungs or spinal cord, or cyclophosphamide followed by total body irradiation (TBI) in the other patients, as described previously?’ In addition, 10 patients undergoing BMT while in resistant relapse (see below) after August 1986 were entered on a dose escalation study of a preparative regimen consisting of busulfan (4mg/kg/d, orally in four divided doses every 6 hours, for 4 consecutive days), etoposide (10 to 50 mgkg intravenously [IV] on the fifth day), and cyclophosphamide (60 mgkg/d IV on the sixth and seventh days). Bone marrow was infused 1 day after completing cyclophosphamide and TBI, and 2 days after completing the busulfan-containing regimens. Supportive care, including GVHD prophylaxis (with cyclosporine) and treatment, was provided as previously described.’.’” Study defmitions and statistical analysis. The patients’ disease status was classified according to their response to a median of two cycles (range, 1 to 12) of conventional salvage therapy administered before BMT.7s11-’3 The salvage therapy was administered by the referring physician and was not standardized. The salvage LLOGENEIC bone marrow transplantation (BMT) is associated with a clinically significant antitumor effect, independent from the pretransplant cytotoxic therapy, against acute leukemias and chronic myelogenous 1e~kemia.I’~ The mechanisms responsible for this graftversus-leukemia effect are not completely understood. Although graft-versus-host disease (GVHD), especially chronic GVHD, accounts for much of this graft-versus-leukemia activity,“’ allogeneic grafts appear to produce an antileukemic effect independent of clinically apparent GVHD.4*5 A similar graft-versus-tumor effect against lymphomas has not been demonstrated after allogeneic BMT.6,7The inability to establish a graft-versus-lymphoma effect may be explained by biologic differences between lymphomas and leukemias, or may be the result of the relatively small number of patients who have received allogeneic transplants for lymphomas. We examined the results of BMT in 118 consecutive patients with relapsed Hodgkin’s disease and intermediate-grade or high-grade nomHodgkin’s lymphoma, based on type of marrow graft, for evidence of a graft-versus-lymphoma effect. Patients with a histocompatible donor received allogeneic grafts, while-patients without a matched donor received autologous grafts. We also analyzed the influence of various other prognostic factors, including age, type of preparative regimen, and response to standard salvage therapy before BMT, on the outcome of BMT for lymphomas. MATERIALS AND METHODS Patients. We analyzed 118 consecutive patients with relapsed Hodgkin’s disease or diffuse intermediate-grade or high-grade non-Hodgkin’s lymphoma who underwent BMT at the Johns Hopkins Oncology Center between January 1981 and October 1988. Some of the patients have been described previ~usly.~.’ Patients were eligible for BMT if they were less than 60 years old and had progressed during or relapsed after standard chemotherapy. Patients with Hodgkin’s disease whose first relapse followed a disease-free interval of greater than 12 months after chemotherapy were not eligible until second relapse. Additional eligibilityrequirements included a Karnofsky performance status of at least 70%, no evidence of morphologic lymphoma in the bone marrow by aspirate and biopsy, and the absence of active central nervous system Blood, Vol77, No 3 (February 1). 1991: pp 649-653 From The Johns Hopkins Oncology Center, The Johns Hopkins Medical Institutions, Baltimore, MD 21205. Submitted April IS, 1990; accepted October 4,1990. Supported in part by National Institutes of Health Grants CA-15396 and CA-06973. Address reprint requests to Richard J. Jones, MD, Room 2-127, The Johns Hopkins Oncology Center, 600 N Wove St, Baltimore, MD 21205. The publication costs of this article were defrayed in part by page charge payment. This article must therefore be hereby marked “advertisement” in accordance with 18 U.S.C. section I734 solely to indicate this fact. 0 1991 by The American Society of Hematology. 0006-4971191/7703-0027$3.0010 649 From www.bloodjournal.org by guest on December 29, 2014. For personal use only. 650 JONES ET AL therapies given to the patients with Hodgkin’s disease have been described previously.’ For the patients with non-Hodgkin’s lymphoma, the salvage therapy was a standard first, second, or third generation lymphoma regimen14in 47 patients, cisplatinlcytarabinebased regimens in 8 patients, and other regimens in 8 patients. A sensitive relapse was defined as showing at least a partial response (250% decrease in tumor size by the sum of the products of the perpendicular diameters of all areas of known disease) to salvage therapy immediately before BMT. Patients were defined as being in resistant relapse if their lymphoma progressed through their initial combination chemotherapy treatment (five patients), or if their disease showed less than a partial response to salvage therapy immediately before BMT. The major statistical endpoints of this study were event-free survival and time to relapse after BMT. Event-free survival was defined as the time from the day of BMT until disease progression or death from any cause. The time to relapse was defined as the time to disease progression with deaths being censored. Because residual masses often do not represent residual lymphoma,I5-l7 patients with both complete and partial remissions after BMT were included in these analyses until disease progression. Event-time distributions were estimated using the method of Kaplan and Meier.” For categorical factors, the differences between eventtime distributions were tested using the log-rank statistic.’’ The prognostic significance of continuously distributed variables (ie, age) was assessed using the proportional hazards model’’ with hazard ratios expressed per unit change. To adjust for the effect of several prognostic factors simultaneously, the multivariate proportional hazards model was used. Hazard ratios exceeding 1.0 indicate an increased risk for death or relapse in the presence of the prognostic factor. Similarly, hazard ratios less than 1.0 indicate a lower risk of relapse or death with the prognostic factor. The following prognostic factors were analyzed for their effects on the event-time distributions: type of graft, preparative regimen, disease status at the time of BMT, number of relapses, type of lymphoma (Hodgkin’s v non-Hodgkin’s), age, and sex. For time-toevent distributions, point estimates are given 295% confidence intervals as determined from standard life table methods. The association of type of graft with patient characteristics and transplant-related mortality was tested using the Chi-square test or the Student’s t-test. All Pvalues reported are two-sided. Analyses were performed as of April 1, 1990. ; ; RESULTS The actuarial probability of event-free survival for the entire 118 patients a t 4 years after BMT was 29% (95% confidence interval, 21% t o 37%) (Fig 1). The median follow-up after BMT for the event-free survivors was 44 months with a minimum follow-up of 18 months. Multivariate analysis showed that the status of the lymphoma a t the time of BMT was the only factor that influenced the event-free survival (Table 1). Patients in sensitive relapse had a significantly improved probability of event-free survival (Fig 1, P < .001). Whether or not the patient was in a complete or partial remission before BMT was not a significant prognostic factor (hazard ratio = 0.98, P = .9). T h e overall actuarial probability of relapse after B M T was 48% (37% t o 58%). All but 3 of the 43 relapses were in areas of prior disease. Having sensitive disease a t the time of BMT also had a favorable influence on the probability of relapse (Table 1). The actuarial probability of relapse after BMT was 41% (30% t o 55%) for the patients transplanted 5 LL g : 0 00 IO 2 0 30 40 50 a 60 70 80 90 100 110 MONTHS Fig 1. Actuarial probability of event-free survival after BMT for relapsed lymphoma in the entire 118 patients (-1, in the 80 patients in sensitive relapse (- -1, and in the 38 patients in resistant relapse I...). The proportions event-free are 29% (21% t o 37%). 42% (31% t o 53%). and 0, respectively (P < .001). Each tick mark represents a patient surviving in continuous complete remission. with sensitive disease a n d 100% for the patients with resistant disease. Although the type of graft was not a significant prognostic factor for event-free survival after BMT, it was an independent significant prognostic factor for the probability of relapse after BMT in the multivariate proportional hazards model (Table 1). The median age was 26 years for Table 1. Patient Characteristics and Their Influence o n Outcome Hazard Ratios Characteristics Sex Female Male Age Type of lymphoma Hodgkin’s Non-Hodgkin’s No. of relapses 1 22 Preparative regimen Cy-TBI Bu-Cy BU-VP16-Cy Disease status at BMT Sensitive relapse Resistant relapse Type of graft Allogeneic Autologous No. of Patients Event-Free Survival Relapse 33 85 0.74 (P = 2 3 ) 0.93 (P = .82) - 1.01 (P = .14) 0.99 (P = .48) 55 63 0.92 (P = .73) 0.65 (P = .18) 61 52 0.97 (P = .89) 1.02 (P = .96) 1.3 (P = .29) 0.81 (P = .6) 1.7 (P = .14) 1.4 (P = .6) 72 36 10 < ,001) 80 38 0.24 (P 38 80 0.84 (P = .49) 0.18 (P < ,001) 0.4 (P = .02) P values are for the multivariate proportional hazards model. The reference group for each categorical variable is the first patient group listed, except for preparative regimens where the hazard ratios for Bu-Cy and Bu-VP16-Cy are versus Cy-TBI. Abbreviations: Cy-TBI, cyclophosphamide and TBI; Bu-Cy, busulfan and cyclophosphamide; Bu-VP16-Cy, busulfan, etoposide, and cyclophosphamide. From www.bloodjournal.org by guest on December 29, 2014. For personal use only. GRAFT-VERSUS-LYMPHOMA EFFECT 651 both the autologous (range 2 to 60) and the allogeneic (range 5 to 45) graft recipients. There were no significant differences between the clinical features of patients in sensitive relapse receiving either autologous or allogeneic grafts (Table 2). The actuarial event-free survival of the patients in sensitive relapse was 41% (28% to 53%) for the autologous patients and 47% (24% to 67%) for the allogeneic patients (Fig 2A, P = 3 ) . However, the actuarial probability of relapse after BMT was 46% (33% to 60%) for patients with sensitive disease receiving autologous grafts compared with only 18% (5% to 55%) for allogeneic graft recipients with sensitive disease (Fig 2B, P = .02). The difference in relapse rates between allogeneic and autologous transplants was similar for patients with Hodgkin’s disease (24% difference) and non-Hodgkin’s lymphomas (29%). Two patients relapsed after allogeneic BMT for a sensitive lymphoma; neither patient had demonstrated any evidence of acute GVHD, and one patient had developed mild chronic GVHD involving only the mouth. Acute GVHD developed in five of nine allogeneic patients in sensitive relapse who survive event-free, and chronic GVHD developed in three of these nine patients. The type of marrow graft also influenced the transplantrelated mortality. Whereas 18 of 38 patients (47%) with allogeneic grafts died of causes directly related to BMT, 17 of 80 patients (21%) with autologous grafts died of transplant-related causes (P = .007, Chi-square). We have previously shown that the status of the lymphoma at BMT also influenced the peritransplant mortality, with patients in resistant relapse having a significantly higher mortality.’ Patients in sensitive relapse also had a higher transplantrelated mortality after allogeneic BMT than following autologous BMT; the peritransplant mortality was 42% (8 of 19) in allogeneic graft recipients compared with 13% (8 Table 2. Characteristics of Patients in Sensitive Relapse by Type of Graft -I Q 2 > U A I.On 3 v) W W [L t 2 w > w LL 0 > t -I - m a m 0 [L a I .o- w cn 0.9 - a a 0.8-I W [L 0.7 - 0.6 F 0.5 - LL 0 t A m Q m 0 [L a MONTHS Fig 2. Actuarial probability of event-free survival (A) and relapse (B) in the 61 patients who underwent autologous BMT 1-( and the 19 patients who underwent allogeneic BMT (- -) for lymphomas in sensitive relapse. The proportions event-free are 41% (28% to 53%) and 47% (24% to 67%). respectively (P = .E). The probabilities of relapse are 46% (33% to 60%) and 18% (5% to 55%), respectively (P = .02). No. of Patients Characteristics Autologous Age 0-10 6 11-20 18 21-30 11 9 31-40 9 41-50 8 51-60 No. of relapses 1 43 2 14 23 4 Type of lymphoma Hodgkin’s 20 Non-Hodgkin’s 41 Preparative regimen Cy-TBI 46 Bu-Cy 15 Interval from diagnosis to BMT (mean 2 SEM) 23 2 2.1 mo *Chi-square test. tstudent’s t-test. Allogeneic PValue 1 2 10 3 3 0 .09* 10 5 4 .16* 9 10 .38* 14 5 .79* 27 2 3.2 mo .31t of 61) in autologous graft recipients (P = .01, Chi-square). Acute GVHD developed in 24 of the 38 allogeneic patients (63%), and chronic GVHD developed in 8 of 25 allogeneic patients (32%) who survived at least 100 days. The majority of deaths resulting from allogeneic BMT (11 of 18 patients overall and 5 of 8 patients in sensitive relapse) were related to GVHD. DISCUSSION Our results show that for both Hodgkin’s disease and non-Hodgkin’s lymphoma, the probability of relapse after allogeneic BMT is decreased compared with autologous BMT. All the autologous marrow grafts were morphologically free of lymphoma at the time of BMT, and were purged ex vivo in an attempt to eradicate any occult lymphoma cells that might have been present in the graft. Nevertheless, it is possible that the difference in relapse rates between autologous and allogeneic BMT was the result of infusing viable lymphoma cells with the autologous grafts. The relapse rates after autologous BMT for patients From www.bloodjournal.org by guest on December 29, 2014. For personal use only. 652 JONES ET AL with lymphomas in this report and others that use marrow purging2‘,=are similar to studies that did not use p~rging.6,’”’~ However, the pattern of relapse in all of these studies suggests that failure to eradicate lymphoma in the patient is a more important cause of disease progression than infusion of occult lymphoma cells with the autologous marrow graft, although we cannot completely discount that areas of prior disease are “permissive” sites for the growth of tumor cells infused with the autologous marrow graft. Therefore, it is very unlikely that much of the difference in relapse rates between autologous and allogeneic BMT is a consequence of reinfusingviable lymphoma cells with the autologous grafts; the decreased lymphoma recurrence after allogeneic BMT likely results largely from an immunologic graft-versus-lymphoma effect. Previous studies have failed to show a graft-versuslymphoma effect with allogeneic BMT.6,7This is probably a consequence of the limited statistical power of small sample sizes rather than the result of differences in the biology of the graft-versus-tumor effect between lymphomas and leukemias. In fact, both studies6,’ showed a trend toward a lower relapse rate after allogeneic BMT. In addition, the magnitude of the graft-versus-lymphoma effect in our patients is similar to the reported graft-versus-leukemia effect associated with allogeneic BMT.’s3.’ Allogeneic BMT was associated with a 28% lower relapse rate than autologous BMT in our patients with sensitive lymphomas, compared with 23% to 25% lower relapse rates than syngeneic or autologous BMT in patients with acute leukemias in remission.'^^ The mechanisms responsible for the graft-versus-tumor effect associated with allogeneic BMT are not completely understood. Both acute and chronic GVHD appear to generate antitumor activity.’.’ However, there also appears to be a graft-versus-tumor effect with allogeneic BMT separate from clinically apparent GVHD.4.’ There are too few relapses in our patients who received allogeneic grafts for sensitive lymphomas to evaluate the role of GVHD in the graft-versus-lymphoma effect. The tumor cell kill provided by the graft-versus-tumor effect, although qualitatively very important, is probably quantitatively rather small. Animal models suggest that a 25% to 50% improvement in relapse rate, as occurs with the graft-versus-tumor effect, probably represents no more than 1 to 2 logs of additional tumor cell kill over that provided by the preparative However, this small amount of additional tumor cell kill likely represents the most drug-resistant population of cells. As seen with acute leukemia: the improved control of lymphoma with allogeneic BMT did not lead to an improvement in event-free survival (Fig 2). The beneficial graftversus-lymphoma effect with allogeneic BMT is offset by increased peritransplant mortality, largely resulting from GVHD. Nevertheless, its superior antitumor activity makes allogeneic BMT an important approach for continued study in patients with lymphoma, especially in those patients at low risk for the complications of GVHD. REFERENCES 1. Weiden PL, Flournoy N, Thomas ED, Prentice R, Fefer A, Buckner CD, Storb R: Antileukemic effect of graft-versus-host disease in human recipients of allogeneic-marrow grafts. N Engl J Med 300:1068,1979 2. Weiden PL, Sullivan KM, Flournoy N, Storb R, Thomas ED: Antileukemic effect of chronic graft-versus-host disease. N Engl J Med 304:1529,1981 3. Kersey JH, Weisdorf D, Nesbit ME, LeBien TW,Woods WG, McGlave PB, Kim T, Vallera DA, Goldman AI, Bostrom B, Hurd D, Ramsay NKC Comparison of autologous and allogeneic bone marrow transplantation for treatment of high-risk refractory acute lymphoblastic leukemia. N Engl J Med 317:461,1987 4. Butturini A, Bortin MM, Gale RP: Graft-versus-leukemia following bone marrow transplantation. Bone Marrow Transplant 2:233,1987 5. Horowitz MM, Gale RP, Sonde1 PM, Goldman JM, Kersey J, Kolb H-J, Rimm AA, Ringden 0, Rozman C, Speck B, Truitt RL, Zwaan FE, Bortin MM: Graft-versus-leukemia reactions after bone marrow transplantation. Blood 75:555,1990 6. Appelbaum FR, Sullivan KM, Buckner CD, Clift RA, Deeg HJ, Fefer A, Hill R, Mortimer J, Neiman PE, Sanders JE, Singer J, Stewart P, Storb R, Thomas ED: Treatment of malignant lymphoma in 100 patients with chemotherapy, total body irradiation, and marrow transplantation. J Clin Oncol5:1340,1987 7. Jones RJ,Piantadosi S, Mann RB, Ambinder RF, Seifter EJ, Vriesendorp HM, Abeloff MD, Burns WH, May WS, Rowley SD, Vogelsang GB, Wagner JE, Wiley JM, Wingard JR, Yeager AM, Saral R, Santos GW: High-dose cytotoxic therapy and bone marrow transplantation for relapsed Hodgkm’s disease. J Clin Oncol8:527,1990 8. Braine HG, Santos GW, Kaizer H, Yeager AM, Mann RB, Burns WH, Civin CI, Fuller DJ, Rowley SD, Saral R, Sensenbrenner LL, Stuart RK, Wingard JR, Munoz L L Treatment of poor prognosis non-Hodgkin’s lymphoma using cyclophosphamide and total body irradiation regimens with autologous bone marrow rescue. Bone Marrow Transplant 2:7,1987 9. Yeager AM, Kaizer H, Santos GW, Saral R, Colvin OM, Stuart RK, Braine HG, Burke PJ, Ambinder RF, Burns WH, Fuller DJ, Davis JM, Karp JE, May WS, Rowley SD, Sensenbrenner LL, Vogelsang GB, Wingard J R Autologous bone marrow transplantation in patients with acute nonlymphocytic leukemia, using ex vivo marrow treatment with 4-hydroperoxycyclophosphamide. N Engl J Med 315:141,1986 10. Santos GW, Tutschka PJ, Brookmeyer R, Saral R, Beschorner WE, Bias WB, Braine HG, Burns WH, Farmer ER, Hess AD, Kaizer H, Mellits D, Sensenbrenner LL, Stuart R, Yeager AM: Cyclosporine plus methylprednisolone versus cyclophosphamide plus methylprednisolone as prophylaxis for graft-versus-host disease: A randomized double-blind study in patients undergoing allogeneic marrow transplantation. Clin Transplant 1:21,1987 11. Philip T, Armitage JO, Spitzer G, Chauvin F, Jagannath S, Cahn J-Y, Colombat P, Goldstone AH, Gorin NC, Flesh M, Laporte J-P, Maraninchi D, Pic0 J, Bosly A, Anderson C, Schots R, Biron P, Cabanillas F, Dicke K High-dose therapy and autologous bone marrow transplantation after failure of conventional chemotherapy in adults with intermediate-grade or high-grade nonHodgkin’s lymphoma. N Engl J Med 316:1493,1987 12. Carella AM, Congiu AM, Gaozza E, Mazza P, Ricci P, Visani G, Meloni G, Cimino G, Mangoni L, Coser P, Cetto GL, Cimino R, Alessandrino EP, Brusamolino E, Santini G, Tura S, Mandelli F, Rizzoli V, Bernasconi C, Marmont AM: High-dose chemotherapy with autologous bone marrow transplantation in 50 From www.bloodjournal.org by guest on December 29, 2014. For personal use only. GRAFT-VERSUS-LYMPHOMA EFFECT advanced resistant Hodgkin’s disease patients: An Italian study group report. J Clin Oncol6:1411,1988 13. Jagannath S, Armitage JO, Dicke KA, Tucker SL, Velasquez WS, Smith K, Vaughan WP, Kessinger A, Horwitz U,Hagemeister FB, McLaughlin P, Cabanillas F, Spitzer G: Prognostic factors for response and survival after high-dose cyclophosphamide, carmustine, and etoposide with autologous bone marrow transplantation for relapsed Hodgkin’s disease. J Clin Oncol7:179,1989 14. Coleman M Chemotherapy for large-cell lymphomas: Optimism and caution. Ann Intern Med 103:140,1985 15. Jochelson M, Mauch P, Balikian J, Rosenthal D, Canellos G: The significance of the residual mediastinal mass in treated Hodgkin’s disease. J Clin Oncol3:637,1985 16. Radford JA, Cowan RA, Flanagan M, Dunn G, Crowther D, Johnson RJ, Eddleston B: The significance of residual mediastinal abnormality on the chest radiograph following treatment for Hodgkin’s disease. J Clin Oncol6:940,1988 17. Surbone A, Longo DL, DeVita VT Jr, Ihde DC, Duffey PL, Jaffe ES, Solomon D, Hubbard SM, Young RC: Residual abdominal masses in aggressive nomHodgkin’s lymphoma after combination chemotherapy: Significance and management. J Clin Oncol 6:1832, 1988 18. Kaplan EL, Meier P: Nonparametric estimation from incomplete observations. J Am Stat Assoc 53:457,1958 653 19. Mantel N, Haenzel W: Statistical aspects of the analysis of data from retrospective studies of disease. J Natl Cancer Inst 22:719,1959 20. Cox DR: Regression models and life tables (with discussion). J R Stat SOC34:187,1972 21. Takvorian T, Canellos GP, Ritz J, Freedman AS, Anderson KC, Mauch P, Tarbell N, Coral F, Daley H, Yeap B, Schlossman SF, Nadler LM: Prolonged disease-free survival after autologous bone marrow transplantation in patients with non-Hodgkin’s lymphoma with a poor prognosis. N Engl J Med 316:1499,1987 22. Gulati SC, Shank B, Black P, Yopp J, Koziner B, Straus D, Filippa D, Kempin S, Castro-Malaspina H, Cunningham I, Berman E, Coleman M, Langleben A, Colvin OM, Fuks Z, O’Reilly R, Clarkson B: Autologous bone marrow transplantation for patients with poor-prognosis lymphoma. J Clin Oncol6:1303,1988 23. Skipper HE, Schabel FM Jr, Wilcox WS: Experimental evaluation of potential anticancer agents. XIII. On the criteria and kinetics associated with “curability” of experimental leukemia. Cancer Chemother Reports 351,1964 24. Hagenbeek A How to prevent a leukemia relapse after bone marrow transplantation in acute leukemia: Preclinical animal model studies. Exp Hematol16:418, 1988 (abstr) From www.bloodjournal.org by guest on December 29, 2014. For personal use only. 1991 77: 649-653 Evidence of a graft-versus-lymphoma effect associated with allogeneic bone marrow transplantation RJ Jones, RF Ambinder, S Piantadosi and GW Santos Updated information and services can be found at: http://www.bloodjournal.org/content/77/3/649.full.html Articles on similar topics can be found in the following Blood collections Information about reproducing this article in parts or in its entirety may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests Information about ordering reprints may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#reprints Information about subscriptions and ASH membership may be found online at: http://www.bloodjournal.org/site/subscriptions/index.xhtml Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036. Copyright 2011 by The American Society of Hematology; all rights reserved.








© Copyright 2026