
Corrigendum 1 ~ Final ToR for CCM Endline (with
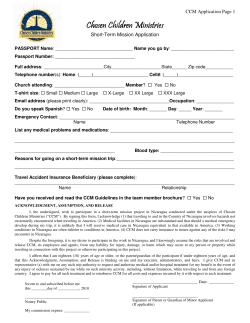
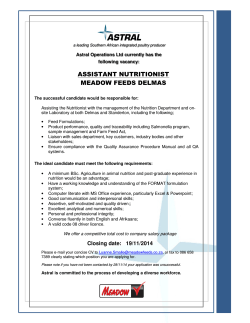
Corrigendum 1: Final ToR for CCM Endline (with sampling) SECTOR WISE APPROACH TO STRENGTHENING HEALTH (SWASTH) BIHAR TECHNICAL ASSISTANCE SUPPORT TEAM (BTAST) TERMS OF REFERENCE FOR DATA COLLECTION AGENCY FOR CONCURRENT MONITORING (ENDLINE 2015/2016) OF HEALTH, WATSAN AND NUTRITION SERVICES 1. INTRODUCTION The Government of Bihar (GoB) has launched the “Sector Wide Approach to Strengthening Health” (SWASTH) programme. DFID provides health sector budget support to the GoB channeled through the Department for Health and Family Welfare (DoHFW); Social Welfare Department (SWD); and Public Health Engineering Department (PHED). DFID support includes provision of technical assistance through the Bihar Technical Assistance Support Team (B-TAST). B-TAST is managed by a consortium of CARE (UK), IPE Global, and Options Consultancy Services, and consists of national and international consultants who provide technical and managerial support to the state government. SWASTH’s goal is “to improve the health and nutritional status of people in Bihar, particularly the poorest of the poor, and thereby accelerate the state’s progress towards the Millennium Development Goals (MDGs)”. Its purpose is “increased use of quality, essential health, nutrition, water and sanitation services especially by poorest people and excluded groups.” The SWASTH programme is implemented across all 38 districts of Bihar, and the Technical Assistance Support Team undertakes additional interventions to support SWASTH implementation in 11 priority districts (9 initially chosen and 2 added later)1 that are highly underserved (which were identified through a vulnerability composite index). A complete description of these additional programmes that are being implemented through BTAST as a part of the technical assistance to SWASTH in the 11 priority districts, is provided in Annex 1. The Department of Health and Family Welfare (DoHFW) and Social Welfare Department (SWD) through the Integrated Child Development Services (ICDS) are responsible for delivering health and nutrition services through a vast number of village-based centres (- 82,797 Anganwadi Centres (AWCs) and 9696 health sub centres). There are also a number of special outreach days and activities for immunization, vitamin A supplementation etc, and as part of the NRHM mandate, the state has recently launched Village Health, Sanitation and Nutrition Days (VHSNDs) to be conducted in each AWC once a month across the state. To complement this, Public Health Engineering Department (PHED) is implementing two national flagship programs, Total Sanitation Campaign (TSC) (with focus on Household, school and Anganwadi sanitation) and the National Rural Drinking Water Programme (NRDWP) to improve the access of sanitation and safe water to the rural community for improved health outcomes of women, children and men. Both these programs are being implemented in the entire state. Some of the interventions described above are included as part of SWASTH’s systematic and innovative approach to working with communities through its Community Based Approaches (CBA) being delivered in the priority districts. Through this approach, SWASTH aims to increase the access and use of community Health, Nutrition, and Water and Sanitation services, to improve nutrition, hygiene and health behaviours, and achieve improved health and nutrition outcomes in the state. SWASTH will build on existing social capital including: frontline workers and supervisory staff of the three Departments of Social Welfare (SWD), Health & Family Welfare (DHFW), and Public Health Engineering (PHED); community based organisations such as women’s 1 The priority districts for SWASTH are Araria, Banka, Sheohar, Madhubani, Jehanabad, Kishanganj, Purnia, Banka, Madhepura, Jamui, Supaul Page 1 of 31 Corrigendum 1: Final ToR for CCM Endline (with sampling) Self Help Groups (SHGs) through their Federations, and Civil Society Organisations (CSOs) in the State. The theory of change underpinning CBA puts women, families and communities as the drivers of improved health and nutrition, WASH outcomes (see Annex 1 for more information). CBA brings together a powerful set of demand and supply side, and community led governance interventions to empower women and communities to adopt healthier, nutrition and WASH practices and increase access to quality services. Through a synergistic package of community based interventions the theory is that demand will be created for better quality, more responsive and more accountable service delivery, and by strengthening the quality of community services, and the capacity of front line workers to deliver, services will be more effective and efficient. The CBA model recognises that in addition to community based efforts, service and systems strengthening, and policy reforms are essential for institutionalising responsive and inclusive service improvements. Hence the CBA model sits alongside systems strengthening and policy level interventions to create a positive circle of community, service, systems and policy development. The combined result of which is improved health outcomes. 2. BACKGROUND TO CONCURRENT MONITORING Accurate and reliable data about the status of various programmes that are implemented by the three GoB Departments (DoHFW, SWD and PHED) are needed, to enable evidence-based decision-making and improvements to the services being provided. Bihar is implementing some key flagship programmes across the three sectors through SWASTH. It is essential to have a monitoring system which can assess the quality and effectiveness of the programmes. Hence, BTAST in close cooperation with SWD, DoHFW and PHED has introduced concurrent monitoring for important indicators in health, nutrition and WATSAN, as an integral part of SWASTH. The concurrent monitoring system is expected to generate data to assess the status of the various programmes and to cross-check against data produced through GoB and SWASTH management information systems (MIS). Information from the CCM is expected to provide data that can help informed decision-making across the three Departments and thereby make quality improvements in their specific areas of work. The CCM data will also be used to quantitatively evaluate a package of community based approaches (CBA) being implemented in the priority districts. This TOR covers both CCM and the nested CBA evaluation. To meet these objectives an external agency with substantial expertise in data collection, analysis and management needs to be engaged. The agency must also be able to demonstrate that they have strong and transparent quality assurance mechanisms in place at each stage of the work and be willing to share raw data on request. 2.1. Objectives of Concurrent Monitoring The broad objective of CCM is to generate high quality data and reports on the status of health, nutrition and WATSAN service implementation, and the outcomes of these services. Specifically, CCM aims to: • Generate high quality, objective primary data from all block/ districts across Bihar on health nutrition and WATSAN service provision, utilisation and outcomes. • Generate data that specifically allows assessment of the effect of SWASTH related programmes being undertaken in the 11 priority districts e.g. the CBA package, role of VHSNDs, etc). Page 2 of 31 Corrigendum 1: Final ToR for CCM Endline (with sampling) 2.2. • Generate high quality data on specific behaviours at the household and village level on health, nutriton and WASH, which can help understand the uptake of SWASTH related programmes. • Generate data that enables disaggregation by social group and gender. • Generate data that allows spatial disaggregation of data on key indicators that are presented through GIS maps. • Triangulate the data generated through this process, with routine and survey data from other reliable sources to make a ‘best assessment’ of the health, nutrition and WATSAN status in Bihar. Progress to date The concurrent monitoring baseline was delivered between 2012 and 2014 in two phases (the second phase is currently underway). 3. SCOPE OF WORK This terms of reference specifically refers to the quantitative endline concurrent monitoring survey to take place in 2015. Data collection from across 38 districts of Bihar is required. A research agency with robust data collection and data management skills is required to undertake the endline quantitative survey as per this ToR. This assignment will be conducted through a contractual agreement with BTAST, and in consultation with the relevant departments of GoB. 3.1 Assignment aims a. To conduct a household survey in all blocks of Bihar to track progress on key health, nutrition, water, sanitation and hygiene indicators; the sample size per block will be larger in CBA evaluation areas for evaluation purposes. b. To administer questionnaires to other key stakeholders including Frontline Health Workers (ANMs, ASHAs, AWWs) to track changes in service supply and demand since the introduction of CP interventions. c. To conduct an observation checklist at facilities and events. 3.2 Assignment objectives a. To form an agreement with BTAST, in accordance with the quality assurance requirements set-out in this ToR, for the training of data collectors and the provision of regular updates about progress and monitoring of data collection. b. To collect high quality household level data from all blocks of Bihar on health, nutrition, water, sanitation and hygiene (HNWASH). c. To conduct anthropometric measurement of children under 5 years old in accordance with guidelines given in the United Nation’s “How to weigh and measure children” (DP/UN/INT-81-041/6E Manual). d. To collect questionnaire data from frontline workers (FLW). e. To complete the observation checklist. f. To provide accurate and timely schedules for data collection to enable third party quality assurance of fieldwork. g. To provide visual maps of basic health and health-service indicators using GIS or similar software for CCM. h. To provide BTAST with clean and clearly labelled databases for all surveys (i.e. CCM household, anthropometric measurements, FLW and observation checklist data) in a Page 3 of 31 Corrigendum 1: Final ToR for CCM Endline (with sampling) timely fashion (as per payment deliverables), preferably collected through PDAs or similar. 3.3 Tasks BTAST will be leading on the design, sampling and analysis for CCM, but will outsource other components to the research agency including data collection and management, quality assurance and graphical presentation of the data using mapping software. There will be a close working relationship between BTAST and the research agency, including facilitating third party quality assurance of fieldwork and input into staff training. BTAST will closely monitor progress and quality of work delivered. Specific responsibilities of the research agency include: a. Pre-testing and finalising the required tools in partnership with BTAST staff (BTAST will provide a final version of the questionnaires for pre-testing). NB: there will only be minor modifications to the tools used and pre-tested during the baseline survey. As a result, extensive pre-testing of tools is not anticipated. The agency will also be required to undertake any translation into local language, that may be required for the data collection tools. b. Establishing an appropriate managerial structure. c. Working with BTAST to develop plans for high quality staff training for field data collectors, supervisors and other staff. This will be done in accordance to the quality assurance clauses provided by BTAST. d. Recruit and train staff to collect the data. This must include strong quality assurance mechanisms to ensure validity of the data. e. Putting in place appropriate IT hardware and application software for data collection and management. The database designer will need to work closely with BTAST in the initial weeks of data collection to ensure appropriate coding and to rectify any issues with the database. The database used for the baseline (SPSS) will be made available to the research agency. i. This includes mapping software (such as GIS) to enable clear illustration of variations in service coverage and health indicators in districts and blocks. ii. It is also essential that agencies will have the necessary programming experience and equipment to collect data using PDAs, smart phones or similar for rapid assessment of the data. f. Abiding by a quality assurance agreement which sets-out arrangements with regard to data collection and data management data (developing and testing the data entry software, coding responses, entry and cleaning). This will inlcude providing required information on fieldwork scheduling to enable QA consultants to provide third party data verification. g. Collecting and compiling the quality data from selected areas. h. High quality data management and adherence to quality assurance mechanisms per agreed protocols, plans and schedules. i. Providing BTAST with the complete and clearly labelled CCM endline databases after completion of data cleaning. The agency must also be willing to provide BTAST and GoB staff access to the raw data on request (within 5 days). This is likely to occur several times during the course of data collection to enable BTAST to prepare Page 4 of 31 Corrigendum 1: Final ToR for CCM Endline (with sampling) periodic reports throughout the year and to assess CCM progress. It may also be necessary to liaise with BTAST and government staff if clarification about the data is required. Please note that ownership of the data rests with the Government of Bihar. 4. QUANTITATIVE METHODS, SAMPLING AND DATA COLLECTION Concurrent monitoring will be undertaken to capture learning from across various levels of SWASTH implementation, as well as from a wide sample of different stakeholders. It covers 534 administrative blocks across the 38 districts. Please note that the Integrated Child Development Services programme across the same geographical area (38 districts) is implemented through 544 project blocks (instead of the standard adminstrative structure) and the CCM methods and sampling are cognisant of this distinction to ensure that all ICDS project blocks are covered. The CCM endline will adopt an diagnostic research design to include a nested component to evaluate CBA. Emphasis will be given to measuring outcome indicators pertinent to the study through primary block-level data collection. The survey will collect data from : • Beneficiaries at the household level through a survey instrument (including a sufficient sample to enable disaggregation by exposure to different packages of CBA intervention) • Service providers and key stakeholders through a survey instrument • Observations through checklists – including observations of facilities and events • Anthropometric measurements of children less than 5 years through standard and universally accepted methods • Estimation of maternal mortality through the the sisterhood method and direct measurement for the under-5 mortality rate. Table 1 below is a summary of the different components of CCM, and lists the key respondents/ sources of information under each of these categories. TABLE 1: CCM COMPONENT SURVEYS BENEFICIARY SURVEYS Households (Heads Household) Mothers (0 - 5 yrs children) Pregnant Women Adolescent girls Men (husbands) Mothers-in-laws/senior decision-maker OBSERVATIONS OF FACILITIES, VILLAGE OUTREACH AND WATSAN SERVICES Anganwadi Centre (AWC) Auxilary Nurse Midwife (ANM) Primary Health Centre of Anganwadi Worker (AWW) Uddeepika (PHC) of Acrredited Social Health Activist Health Sub-Centre (ASHA) Village Details Panchayati Raj Insitution member Observations of events Medical Officer or Medical Officerincluding: In-Charge - Village Heath Chief District Project Officer (ICDS) Sanitation and Nirmal Bharat Abhiyan (NBA) block Nutrition Day coordinator (including Take Home Ration SERVICE PROVIDER AND STAKEHOLDER INTERVIEWS Page 5 of 31 Corrigendum 1: Final ToR for CCM Endline (with sampling) - Days) School Sanitation Bachpan Divas Others Measurement/Estimates: Anthropometric Measurement Weight Height MUAC Oedema Estimates of Maternal Mortality & U-5 Children Mortality Data collection tools that were used for the CCM baseline survey will be modified for the endline survey. The research agency will be consulted for inputs on these tools, whilst BTAST finalises them. 5. SAMPLING TECHNIQUES Considering that while SWASTH is implemented across all districts of Bihar and taking into account that CBA package is implemented, in a selected number of districts, the survey incorporates a nested evaluation component. The focus of the survey is to provide adequate and reliable information for concurrent monitoring across all districts at the district level, and for the evaluation component at the block level. The indicators that we are particularly interested in monitoring and evaluating are those which impact on the maternal mortality ratio, under-5 mortality rate, contraceptive prevalence rate, malnutrition in children under age 5 years, and anaemia amongst pregnant women in the rural Bihar. Results from the survey can be useful for management of existing programmes, deployment of resources and future planning. The findings of this survey can also identify gaps and barriers to achieving the desired outcomes. This section briefly lays out the sampling framework and sample size estimates that BTAST aims to follow. A stratified sampling approach will be employed to select respondents for the CCM across a sample of 145 blocks from the non-priority districts to provide district level results. The nested evaluation component will comparing a sample of the intervention blocks with non-intervention blocks to provide block level results. Complete details of the sampling strategy with instruction on sample selection will be shared with the data collection agency at the time of data collection. The flow chart below presents the sampling design. As laid out in the flow chart, the CCM survey component will be carried out in all the blocks. The evaluation of the CBA intervention blocks will take place by comparing intervention and non-intervention blocks, which will be matched on a set of defined criteria. The CBA intervention is currently being implemented in 79 blocks across various district. An equal number of non-intervention blocks will be selected for comparison. Page 6 of 31 Corrigendum 1: Final ToR for CCM Endline (with sampling) All 38 districts in Bihar SWASTH Concurrent Monitoring Survey 27 districts in Bihar 27% blocks in each block be surveyed across all 27 districts (145 blocks) SWASTH concurrent monitoring + CBA evaluation (nested component) 11 Priority districts Bihar 20% of the 79 intervention blocks (16 blocks) from 11 districts and 20% of matched nonintervention blocks (16 blocks) 2356 villages 1984 villages No segmentation, if HHs are <500 Segmentation done if HHs are >500 33 Households per village No segmentation, if HHs are <500 Segmentation done if HHs are >500 33 Households per village In principle, sample size calculations need to be run for almost all important outcome variables. In this particular case of complex intervention with key indicators have been selected for which sample size is calculated. The optimal sample size would is the indicator that requires the largest sample size. Based on key indicator estimates, the sample required for each block is estimated as 2046 households, in order to provide robust information on MCH, nutrition and WATSAN programs at the block level. (Note due to the small number of mortality cases, infant mortality rate estimates are considered for the district level and maternal mortality ratio at the state level). Three-stage sampling design will be adopted in selection of household. Block, village, and households will be selected at the first, second and third stage respectively as given in the flow chart. Complete details of the sampling strategy and sample size calculations will be shared with the agency at the contractual stage. TABLE 2 SAMPLE SIZES FOR CONCURRENT MONITORING AND NESTED EVALUATION A. Household B. Women C. Un-married D. District/Nesting E. Village Questionnaire Questionnaire Adolescent Male/Moth Total Blocks Questionnaire (Male) ** Girls er-in-law SWASTH Districts 77748 92520 12160 12160 2356 172624 CBA Intervention blocks (20% of 79 = 32736 38956 5120 5120 992 72684 16) CBA nonIntervention blocks 32736 38956 5120 5120 992 72684 (16) Total 143220 170432 22400 22400 4340 317991.8 ** Note: The women’s questionnaire includes sub-samples with specific questionnaires relevant for (a). currently Page 7 of 31 Corrigendum 1: Final ToR for CCM Endline (with sampling) pregnant women; (b) Women having 0-23 month children; (c) Women having children 24-59 months old; and (d) Women 15-49 per HH The distribution of this sample across the blocks for the survey and the nested component is given below: Frontline workers and officers at the different level will be interviewed as per sample size mentioned in the Table 3 through in-depth interviews. The different type of facilities/events will also be observed during this study. Further details on indicators that were used for the baseline CCM survey are given in Annex 2. And a list of tools used in the baseline CCM survey are given in Annex 3. TABLE 3: SAMPLE SIZES FOR FRONTLINE WORKERS/GOVT. OFFICIALS AND EVENTS Frontline No. of per Total No. for workers/Facilities Block State MOIC 1 177 CDPO 1 177 TSC block 1 177 coordinator ANM 5 885 AWW 10 1770 ASHA 10 1770 VHSND 8 1416 BACHPAN DIVAS 4 708 PRI members 4 708 School Sanitation 4 708 THR 6 1062 6. QUALITY ASSURANCE ARRANGEMENTS 6.1. Quality assurance procedures to be stipulated in contract with research agency The collection of high quality CCM data is of utmost importance as the data will be used to monitor health, nutrition, water, sanitation and hygiene outcomes in all blocks of Bihar. Data collection will be taking place over a wide area simultaneously, involving hundreds of data collectors. The evidence obtained from CCM will be used to guide decision-making (e.g. about resource allocation) across the state. Thus, it is necessary to systematically monitor the quality of data collection – in particular to assess whether the data collection agency are minimising sampling and non-sampling errors during the survey. Although strong quality assurance mechanisms will be put in place and agreed between BTAST and the agency to ensure the validity of the data through high quality training and data collection/management processes, previous experience and standards of best practice dictate that independent verification of data quality is also required. The QA procedures listed below will be in place for this study and the agency should ensure that its programme of work is designed to facilitate this. These procedures will be written into the contract with the research agency and penalties specified in the contract will be enforced should the agency fail to abide by these contractual clauses. Page 8 of 31 Corrigendum 1: Final ToR for CCM Endline (with sampling) The agency should also be aware that Quality Assurance (QA) Consultants will be contracted to support this study and to provide on-going independent appraisal of the quality of data collection, undertake supportive supervision of data collectors and data collection supervisors, and feedback the findings to B-TAST. Details of their specific role are provided in Annex 4. 7. TIMELINE The tentative timeline for the endline survey process is given below. Agencies will be expected to propose a realistic timeline for each survey, including time for staff recruitment and training, data management and data cleaning. This will be discussed and exact dates will be finalised through discussions between BTAST and the research agency. Open tender Inception stage discussions (finalising sampling strategy) Contract issued Inception stage (staff training, piloting tools, field work preparatio n) Data collection/ cleaning B-TAST QA reviews GIS Maps X Feb Jan Dec Nov Oct Sept 2016 Aug Jul Jun May Apr Mar Feb Jan Dec 2015 Nov Oct Sept Aug 2014 X X X X X X X X X X X X X Key Activity underway Deliverable submitted to BTAST 8. DELIVERABLES AND PAYMENT Payments will be made on the basis of agreed deliverables. Indicative deliverables are given below. The detailed payment schedule will be agreed in the final contract. Page 9 of 31 Corrigendum 1: Final ToR for CCM Endline (with sampling) S. NO. • 1a DELIVERABLE TO TRIGGER PAYMENT DATE* Submission of the inception report with full details of training plan and content, quality assurance plans, field work schedule and data management plans including data cleaning approach 6th January 2015 1b • Approval of the inception report 2a • Evidence of completion of appropriate training of all data collectors 2b 3 4 5 6 7 8 9 10 11 • All necessary equipment purchased and approved by B-TAST (including evidence of receipts) • Data collection tools piloted • Draft databases developed • Data collection tools finalized and approved • Databases finalized and approved • Data collection instruments programmed Submission of 1st 25% of data (one raw database, one cleaned database – both clearly labelled) Submission of 2nd 25% of data (one raw database, one cleaned database – both clearly labelled) Submission of preliminary GIS maps for the 50% of blocks (using indicator data provided by B-TAST) Submission of 3rd 25% of data (one raw database, one cleaned database – both clearly labelled) Submission of 4th 25% of data (one raw database, one cleaned database – both clearly labelled) Submission of final GIS maps for all 534 blocks (based on indicator data provided by B-TAST) Approved brief data collection summary report based on template to be provided by B-TAST 20th January 2015 5th February 2015 6th February 2015 15th February 2015 8th March 2015 1st May 2015 1st June 2015 1st July 2015 1st August 2015 1st October 2015 1st November 2015 1st January 2016 * tentative 9. REPORTING ARRANGEMENTS The research agency shall submit the deliverables listed above in hard copy and electronic form (as relevant) to BTAST as per the timeline, which will be finalized at the time of signing the contract. In most cases, one or two drafts of the deliverable will need to be submitted for feedback before the deliverable can be considered final and approved as fulfilling the terms of the contract. 1. The agency will report directly to the Director and the Senior M &E Expert of the Monitoring, Learning and Evaluation Team within BTAST. 2. All the necessary orders and support to collect data and other information from the Health, ICDS and PHED Projects for concurrent monitoring will be provided by the State to the respective authorities. 3. Without explicit permission to GoB and BTAST the contracted agency will not be able to use CCM data for any kind of publication or reference. Page 10 of 31 Corrigendum 1: Final ToR for CCM Endline (with sampling) 10.TERMINATION OF CONTRACT IF ANY DEFAULT BY THE SURVEY AGENCY 10.1 BTAST may notify the Survey Agency of the suspension or termination of this Contract where the services or any part of them are not provided to the satisfaction of BTAST giving the reasons for such dissatisfaction and, in the case of suspension, the action required by the Survey Agency to remedy that dissatisfaction and the time within which it must be completed. 10.2 Where this Contract is suspended under Clause 1.1 and the Survey Agency subsequently fails to remedy the dissatisfaction BTAST may terminate the Contract forthwith or make penalty of 5% out of total budget. 10.3 Payment will be done basis on the completion of work in the following ways; 20% work completion – 20% payment release and so on. Page 11 of 31 Corrigendum 1: Final ToR for CCM Endline (with sampling) ANNEX 1 – SWASTH PROGRAMMES SWASTH covers a wide range of innovative programmes to improve health, nutrition and WASH services and increase the demand for and uptake of services. While the strong focus on community based approaches recognises that most people will access services and learn health seeking behaviours in their own neighbourhood, major system level reforms are also being undertaken. Examples of system level reforms implemented ♦ Human Resource Information System at the DoH, with computerised database of all health workers for use in human resource planning ♦ Public Private Partnership Cell under the State Health Society, to promote, plan and monitor private sector involvement in services to increase service availability and quality ♦ Bihar Medical Services and Infrastructure Corporation for efficient procurement and supply of drugs and equipment to health facilities and construction of buildings ♦ Nutrition monitoring unit at the SWD to monitor services and track expenditure Examples of district and community initiatives ♦ Family Friendly Hospital Initiative: Helping hospitals improve their quality of service ♦ Nursing skill labs and virtual classrooms: Using information technology to transmit quality training to nursing schools ♦ Community based approaches: A package of health, nutrition and WASH services aimed at increasing community participation in both provision and utilisation ♦ Nodal Anganwadi Centres: Using a cluster approach to enhance quality and use of AWC services ♦ Gram Varta: Promoting health messages through women self-help groups ♦ First 1000 days: Training frontline workers to monitor babies during this critical period ♦ Community led total sanitation: Generating community motivation to stop open defecation, rather than purely focusing on toilet construction ♦ Hand pump maintenance: Training women self-help group members to maintain and repair hand pumps and thus assure local water supplies. Further details of the interventions that are specifically referred to as the ‘CBA package’, particularly for the purposes of CCM, are given below The CBA package Empowering women and mobilising communities to take control of their health and nutrition are pivotal to improving family health, nutrition, and water and sanitation behaviours, and increasing demand for services. BTAST recognises this, and is implementing a a bundle of interventions to strengthen health outcomes, through enhanced programme responsiveness, improved quality of services and greater engagement and dialogue between service users and frontline workers, in some of the districts in Bihar which include those identified as ‘vulnerable’ (9 priority districts) and two other districts (total 11 districts). As an approach, CBA involves building on existing social capital, for example community structures and platforms such as women’s Self Help Groups (SHG). It also contains complementary components focussing on service and systems strengthening initiatives in health and nutrition. Implementing partners Page 12 of 31 Corrigendum 1: Final ToR for CCM Endline (with sampling) CBA activities are undertaken in partnership with the Women’s Development Corporation (WDC), two Federations which support women’s Self Help Groups (Jeevika-BRLPS and Mahila Samakhya) in districts where they have a presence, and community-level women’s Self Help Groups (SHG). In districts where Jeevika and Mahila Samakhya are not active, CBA will be expanded through networks of NGOs, civil society and community based organisations. Integrated Child Development Services (ICDS) are partnering with B-TAST for provision of FLW training. Training has been rolled out through a cascade system following training of trainers by B-TAST. The purpose of the training is to: • Build capacities and knowledge of community led institutions and groups to adopt improved nutrition, health and water and sanitation (WATSAN) practices and increase demand for services; • Build the skills of frontline workers to provide correct and timely knowledge, information and counselling support to households; • Strengthen the performance of Village Health, Sanitation and Nutrition Days (VHSND); • Mobilise communities to address domestic violence; • Improve community level monitoring of services through capacity building of existing community based institutions, such as SHGs and Village Health Sanitation and Nutrition Committees (VHSNC). Components of CBA SWASTH’s community based methodology is based on five inter-related strategies: • Improve the knowledge and health promoting behavior of women, families, and communities, especially of the poor and vulnerable. • Mobilise women and communities to improve their health and well-being. Address the social and cultural barriers that impede women and socially excluded groups from adopting improved behaviour and accessing quality services, and create an enabling environment for communities to demand quality services. • Build the capacity of frontline workers and through SWASTH’s systems building inputs, the supervision, logistics and management systems that support their functioning. • Strengthen the management and delivery of local health, nutrition, water and sanitation services which in the case of health, are anchored to well-functioning referral mechanisms to higher order medical services. • Improve community level governance of health, nutrition, and water and sanitation services, and increase the social accountability of providers and managers. CBA comprises three key interventions as given in the table below CBA Interventions INTERVENTION ABBREVIATION GROUP Gram Varta or Gram Varta Plus Gram Varta or (including Community Led Total Communities Gram Varta + Sanitation) Community Mobilisation to VAW Communities IMPLEMENTING GROUP SHGs Federations via SHGs via Page 13 of 31 Corrigendum 1: Final ToR for CCM Endline (with sampling) INTERVENTION ABBREVIATION IMPLEMENTING GROUP Federations GROUP Address Domestic Violence Strengthening of VHSNCs and VHSND VHSND VHSNC FLWs, VHSNC Mukhya, and Supervisor, members, Nirmal Abhiyan (NBA) Coordinator (ANM, Lady B-TAST and Ward Department of Bharat Health (GoB) Block Gram Varta: Participatory Learning for Action (PLA) through SHG Platforms: The SHG movement in Bihar started in the 1980s. The potential of SHGs as local financial intermediaries to reach the poor has gained national recognition, mainly due to their community based participatory approach and sustainability. The main SHPIs within Bihar include a mix of government and non-governmental bodies which have different origins, objectives, and operational approaches, and lend themselves to different degrees to the inclusion of SWASTH’s objectives related to health, nutrition, water and sanitation and women’s empowerment. The agencies include: the Women’s Development Corporation, SGSY, Jeevika, MahilaSamakya, NABARD and PACS. The state has over 350,000 SHGs2, and has created a strong social capital which by further empowering can reap rich dividends for the state. SWASTH in its intention to build upon this platform for its community mobilisation interventions initiated the PLA work through the existing government platform, Women Development Corporation which has been the nodal department for coordination the economic and social empowerment under the Mukhya Mantri Nari Shakti Yojana and National Rural Livelihood Mission (NRLM) programmes. The aim to engage with SHGs through the PLA was to: • Empower women through group solidarity, access to finance, and improved skills. This improves women’s control over resources and decision-making, increases girl’s and women’s status and improves women’s, children’s and family health. • Inform and coach women, the primary carers in the family and community, on improved health, nutrition and water and sanitation behaviours that they can internalise and share with their families and social networks. • Inform and coach women on their entitlements and rights, to reflect on and help redefine the social norms and culture that undermine their wellbeing, and to take action against injustice. The PLA work through SHGs, coined “Gram Varta” aims to mobilise women, especially the marginalised, both SHG members and community women at large for addressing health, nutrition, water and sanitation and gender issues by using their SHG meeting forums. The underlying principle is that participatory learning and action delivered through women’s SHGs is a process through which women can learn and build confidence through shared experience to understand that their health is in their own hands, and to have the self-determination and social support to practice new behaviours. Gram Varta is a 20 meeting cycle Participatory Learning and Action concept which normally ranges between 10- 12 months. It is a continuous process of disseminating information and taking stock of ‘how that information gets translated into action’. The PLA will focus on maternal and newborn 2 APMAS 2009 Page 14 of 31 Corrigendum 1: Final ToR for CCM Endline (with sampling) health messages, and a package of what we are calling nutrition+ messages that address nutrition, child health, family planning, water and sanitation, and gender issues. The two PLA cycles will promote the priority behaviours that SWASTH has identified in its Behaviour Change Communications Approach. Gram Varta Plus (SHG PLA Gram Varta which includes CLTS) In some areas, the Community Led Total Sanitation (CLTS) approach has also been embedded in the Gram Varta cycle, thus called “Gram Varta Plus” which is able to demonstrate a paradigm shift in promoting improved sanitation practices along with health and nutrition through a communityfocused strategy. CLTS is among one of the community wide sanitation approaches tested on a large scale in different settings with impressive initial success. Evidence is emerging that CLTS can be an effective approach to improve hygiene and sanitation behaviours where large scale open defecation is in practice. In Bihar, in the recent past, CLTS has emerged as an empowering approach to seek open defection free communities improve the usage of constructed toilets and create demand for sanitation under ongoing total sanitation campaign (TSC). It is with this aim in mind that CLTS was embedded into the Gram Varta PLA cycle and called Gram Varta Plus. The “Gram Varta Plus” pilot PLA cycle has been well established in pilot areas after which the process for scale up started. Community Mobilisation to Address Domestic Violence (VAW) Bihar is one of the states in India with the highest percentage of spousal violence cases at 59%, as per the NFHS III survey. The state has initiated several women empowerment programmes and schemes towards preventing as well as responding to the issues of violence against women. In keeping with this objective, the state in the recent years has implemented an intensive year long social awareness programme under the aegis of WDC to end gender based violence alongside strict implementation of the Protection of Women from Domestic Violence Act, 2005. As part of SWASTH support to the state, SWASTH had developed an Operational Plan to address domestic violence in Bihar; this plan rests heavily not only on strengthening existing state and district based institutions for dealing and responding to VAW cases but also focuses on preventive approaches through working with communities, schools, health systems and police and judiciary in the state. SWASTH has engaged with Bihar Mahila Samakhya to pilot a community based initiative in 2 blocks each in Gaya and Jehanabad districts. The pilot has been successfully implemented with the completion of training of trainers for all cadres including folk theatre artists, core facilitators who will be conducting the debriefing sessions and the team of community volunteers who have been selected from local communities for conducting home visits and acting as referral points. After successful intervention scale up the interventions to five more districts, SWASTH priority district with technical support from Bihar Mahila Samakhya. Strengthening -VHSNCs and VHSNDs Government of Bihar, through the State Health Society, is leading on VHSND strengthening, largely through capacity building of Frontline Health Workers (ANM, AWW, ASHA) and PRI member as well as supportive supervision of front line health workers and monitoring. State Health Society is also working towards strengthening VHSNCs in the State again through capacity building of VHSNC members (ANM, AWW, ASHA, Senior mechanic from PHED, Lady Supervisor). B-TAST is actively involved in supporting GoB in strengthening VHSND and VHSNC in the State. Under NRHM, VHSNCs are mandated to prepare and implement village health plans using the allocated Rs. 10,000 per year untied fund they receive, and to support VHSNDs. In Bihar, training of VHSNCs has been generally poor, and VHSNCs have not been decentralised down to the village but remain at Gram Panchayat level. SWASTH CBA in partnership with State Health Society therefore Page 15 of 31 Corrigendum 1: Final ToR for CCM Endline (with sampling) proposed to support the strengthening of capacities of VHSNCs as a vehicle for community led change as envisaged under NRHM. Village health, sanitation and nutrition day (VHSND) is a key strategy of NRHM to improve access to primary health care and improve community participation in the programme. It has been envisaged as a convergent platform for health, nutrition and Watsan services. The last is poorly conceptualized under NRHM, and here lies an opportunity for SWASTH to develop a doable and scalable model that can be replicated. The VHSNCs are standing committees of the PRI system and have a pivotal role to play in the implementation of VHSNDs in the state. In Bihar the village level committees have not yet been formed and the Gram Panchayat level VHSNCs are responsible for the conduct and oversight of VHNDs. The state’s efforts in introducing the village health, sanitation and nutrition day strategy have also met with limited success mainly because of poor planning and weak monitoring and supervision. In other states, VHSND has emerged as a powerful platform for improving utilisation of health services and inculcating health seeking behaviours. SWASTH CBA realises the potential of both VHSNC and VHSND in collaboration with State Health Society has agreed on certain approaches to strengthen the capacities of VHSNDs The multi-dimensional, multi-partner approach to CBA adopted by SWASTH (and supported by BTAST) is ambitious but necessary to achieve the multiple objectives set by the programme (Fig. 1). CBA coverage Roll-out of CBA is a staged process, by intervention and by geographical coverage. Whilst a couple of other interventions (not included in the CBA package here in the ToR) may be piloted and developed, those which are included in the current CBA package are well-established in other settings (VHSND, Gram Varta+) and, as a result, can be rolled out more rapidly. Geographical coverage of CBA is, itself, staged: Firstly, CBA was initially implemented in four of the 11 priority districts before expanding to the remaining 7 districts. Secondly, interventions which are resource intensive, for example Gram Varta+, have been introduced in selected areas of these districts as the aim is to create local resources and capacity which will then be used to scale-up CBA to additional parts of the same district (intra-district expansion). Over time the number of districts in which CBA is active will also increase (inter-district expansion). Each year there will be an increase in both intra- and inter-district expansion. The location of the 11 SWASTH priority districts, B-TAST CBA priority districts and blocks are shown below. Page 16 of 31 Corrigendum 1: Final ToR for CCM Endline (with sampling) FIG. 2: SWASTH PRIORITY DISTRICTS Initial CBA Blocks by District: District Block Gaya Belaganj Gaya Town Imamganj Konch Mohanpur Jehanabad Ghosi Jehanabad Sadar Makhdumpur District Banka Purnia Block Bausi Katuria Amour Baisa Baisi Banmankhi Bhawanipur Dhamdaha Krityanand Nagar Rupauli It should be remembered that CBA is not being implemented in isolation from other health programmes and initiatives, some initiated by GoB, others by development partners. This has implications for M&E of CBA. Page 17 of 31 Corrigendum 1: Final ToR for CCM Endline (with sampling) ANNEX 2 - INDICATORS FOR CCM HOUSEHOLD AND FACILITY SURVEYS INDICATOR WATER & SANITATION (WATSAN) % of households access to toilet facilities % of households using toilet facilities MATCHING INDICATORS CCM CBA RESPONDENTS/DEFINITIONS Mothers/caregivers of children <5 years Flush/pour flush to piped sewer system, Flush/pour flush to septic tank, Flush/pour flush to a pit latrine, Ventilated improved pit (VIP) latrine, Pit latrine with a slab, Composting toilet % of household using cleaning agents for hand Hand washing with soap or ash after washing defecation, before eating, before feeding an infant or young child and safe disposal of child excreta % of women/caregivers of children under-five Mothers/caregivers of children <5 years hand washing with soap after defecation % of women/caregivers of children under-five Mothers/caregivers of children <5 years reporting safe disposal of child excreta (usual practices) % of households using improved drinking Piped water into dwelling/yard/plot, Public water sources tap/standpipe, Tubewell/borehole, Protected dug well, Protected spring, Rainwater, Bottled water % of household using an appropriate Appropriate water treatment methods treatment method of water prior to drinking include boiling, bleaching, straining, filtering and solar disinfecting % of children (under 5 years) who had Mothers/caregivers of children <5 years diarrhoea during last two weeks. # of dysfunctional hand pumps made Gram Pradhan/teacher functional in last three months MATERNAL & CHILD HEALTH CARE (HEALTH) ANTENATAL CARE % of women who received any antenatal Mothers of children <5 years (we could check-up (ANC) during pregnancy. consider restricting to mothers of children <1 or <2 years to minimise recall error for perinatal indicators) % of women who had antenatal check-up in As above first trimester % of women who had three or more ANC As above % of women who had at least one tetanus As above toxoid injection % of women whose Blood Pressure (BP) taken As above % of women who consumed 100 IFA Tablets As above % of women who had full antenatal check-up As above % of women who had extra diet/food during As above her pregnancy DEIVERY CARE % Institutional delivery As above % Delivery at home As above √ √ √ √ √ √ √ √ √ √ √ √ √ √ X √ √ √ √ √ √ √ √ √ √ √ √ Page 18 of 31 √ Corrigendum 1: Final ToR for CCM Endline (with sampling) INDICATOR MATCHING INDICATORS CCM CBA RESPONDENTS/DEFINITIONS % Delivery at home conducted by skilled As above health personnel % Safe Delivery As above % women who received post-natal care within As above two weeks of delivery % women who received financial assistance As above for delivery under JSY % of women who received post natal care As above within 48 hours of delivery of their last child NEWBORN CARE PRACTICES % of women practicing kangaroo care As above immediately after birth % of infants wrapped immediately after birth As above % safe cord care practices As above CHILD FEEDING PRACTICES % of infants breastfed within one hour of birth As above % of infants (age <6 months) exclusively Children <6 months; children 6-23 months breastfed % of children (6 to 23 months) given Children 6-23 months complementary feeding (breast milk + semi solids) CHILD IMMUNIZATION AND VITAMIN A SUPLIMENTATION % of Children (12-23 months) fully immunized Children 12-23 months; BCG, 3 doses each of DPT, and Polio and Measles % of Children 12-23 months who have Children 12-23 months received BCG % of Children 12-23 months who have Children 12-23 months received 3 doses of polio vaccine % of Children 12-23 months who have Children 12-23 months received 3 doses of DPT vaccine % of Children 12-23 months who have Children 12-23 months received measles vaccine % of Children age 12-35 months who received Children 12-35 months a vitamin A dose in last 6 months % of Children (9-35 months) who have Children 9-35 months received at least one dose of Vitamin A TREATMENT OF CHILDHOOD DISEASE (CHILDREN UNDER 5 YEARS BASED ON LAST SURVIVING CHILDREN) % of child morbidity in the last 14 days: fever, Children under-five cough, diarrhea % of Children with acute respiratory Children under-five infection/fever in the last two weeks who were given treatment % of children under-five with symptoms of Children under-five fever in the last two weeks who sought treatment from a health facility or formal health provider % of Children with Diarrhoea in the last two Children under-five √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ Page 19 of 31 √ Corrigendum 1: Final ToR for CCM Endline (with sampling) INDICATOR RESPONDENTS/DEFINITIONS weeks who received ORS % of Children with Diarrhoea in the last two Children under-five weeks who were given (HAF/ORS/ORT) treatment % of Children had check-up within 24 hours Children under-five after delivery (based on last live birth) FAMILY PLANNING (CURRENTLY MARRIED AGE 0-5 YEARS OF CHILDREN MOTHER) % Any Method Mothers of children <5 years % Any Modern method Mothers of children <5 years % Female Sterilization Mothers of children <5 years % Male Sterilization Mothers of children <5 years % IUD Mothers of children <5 years % Pill Mothers of children <5 years % Condom Mothers of children <5 years % Total unmet need Mothers of children <5 years % For spacing Mothers of children <5 years % For limiting Mothers of children <5 years QUALITY OF CARE % of women who visited any health facility in Mothers of children <5 years 12 months % of women who ever visited a health facility Mothers of children <5 years by main source of health care % of women by services they went for to a Mothers of children <5 years public or private clinic during 12 months Quality of clinical service: Public vs. Private Mothers of children <5 years facilities • Median waiting time • Percentage who said the staff spent enough time • Percentage who said the staff talked to them: Nicely, Somewhat nicely, Not nicely % who said the staff respected their need for Mothers of children <5 years privacy % who said the staff explained things to Mothers of children <5 years them: Clearly, Somewhat clearly, Not clearly % who said the staff were: Helpful, Somewhat Mothers of children <5 years helpful, Not helpful % who rated facility as: Very clean, Mothers of children <5 years Somewhat clean, Not clean % who paid money for: Provider fees, Mothers of children <5 years Medicine, Transport, Other % distribution of women who, based on their Mothers of children <5 years own experience or perception, compare the public and private facilities on a number of issues relating to quality of clinical services • Closer to home or work place • Availability of doctor MATCHING INDICATORS CCM CBA √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ Page 20 of 31 √ Corrigendum 1: Final ToR for CCM Endline (with sampling) INDICATOR • Short waiting time • Availability of medicine • Cleanliness of the facility • Staff's treatment of the client • Provision of privacy if needed • Affordability of services • Effectiveness of treatment % of sterilised women or their husbands who were told about other methods of contraception at the time of sterilisation % of sterilised women or their husbands who were told about side effects of sterilisation • Quality of clinical services for sterilization • Facility was clean • Had enough privacy • Provider answered the questions • Staff treated nicely • Would recommend this facility NUTRITION % of children under five weighed at the AWC in the last month % of chidren under 5 years who are underweight (weight-for-age) % of children under 5 years who are stunted (height-for-age) % of children under 5 years who are wasted (weight-for-height) % children under two with MUAC <115cm % children under two with bilateral pitting oedema % of children under 5 years who are severely malnourished (WHZ <-3SD) who are referred to a PHC/CHC % of children under 5 years who are severely malnourished (WHZ <-3SD) who are referred to a Nutritional Rehabilitation Center % of women who have consumed foods rich in bio-available iron in the last 24 hours % of adolescent girls 10-19 years old who have taken a deworming tablet in the last 6 months % of adolescent girls 10-19 years old who have taken an iron and folic acid supplement in the previous week % of children 1-5 yrs old having received deworming tablets in the previous 12 months % of children 6 months to 5 yrs old having received two doses of vitamin A in the RESPONDENTS/DEFINITIONS MATCHING INDICATORS CCM CBA Mothers of children <5 years √ Mothers of children <5 years Children under-five Children under-five Children under-five Children under-five Children under-two Children under-two √ √ √ √ √ √ √ √ √ √ Children under-five √ Children under-five √ Mothers of children <5 years Adolescent girls 10-19 years √ √ √ √ √ √ √ √ Adolescent girls 10-19 years Children one to five years Children 6 months to five years √ Page 21 of 31 Corrigendum 1: Final ToR for CCM Endline (with sampling) INDICATOR MATCHING INDICATORS CCM CBA RESPONDENTS/DEFINITIONS previous 12 months % of 3 IYCF practices in children aged 6-23 Children 6-23 months months Average No. of times Child weighed by AWW Children under-five in last 3 months ADDITIONAL INDICATORS ON WASH, WOMEN’S & CHILD HEALTH % of households using iodized salt 0-5 years of children mother; also potentially at the household level via the household head % of children under-five who slept under a Mothers of children <5 years, recall period Long Lasting Insecticidal Net (LLIN) last night 24 hours % of women who tested positive for malaria, Mothers of children <5 years and received treatment % of women who slept under a LLIN last night Mothers of children <5 years; recall period 24 hours % with regular exposure to media (TV, radio, Mothers of children <5 years or news paper at least once a week) % children aged 6-59 months receiving Children 6-59 months supplementary nutrition provision from the AWC in the last month (and for how many days in the last month) Maternal mortality ratio (MMR) and 0-5 years of children mother; also potentially pregnancy mortality ratio: using the at the household level via the household ‘sisterhood’ method (the survival of all adult head sisters) and whether women were pregnant, or within 42 days of delivery or pregnancy termination when they died (VAW) WOMEN EMPOWERMENT AND VIOLENCE AGAINST WOMEN % distribution of women age 15-49 who Mothers of children <5 years decides how men’s cash earnings will use % distribution of women & men who usually Mothers of children <5 years make decision about four kind of issues • Own health care • Major household purchases • Purchases of daily household needs • Visits to her family or relatives % of women who usually make Mothers of children <5 years specific decisions alone or jointly % of men age 15-49 who think a wife should Men married to women have an equal or greater say than her husband household interview on five specific kinds of decisions • Making major household purchases • Making purchases for daily household needs • Visits to her family or relatives • What to do with the money the wife √ √ √ √ √ √ √ √ √ √ √ √ √ eligible for √ Page 22 of 31 √ Corrigendum 1: Final ToR for CCM Endline (with sampling) INDICATOR • RESPONDENTS/DEFINITIONS MATCHING INDICATORS CCM CBA earns How many children to have % of women who will be allowed to go alone to specific places and percentage who will not allowed to go at all (alone or with someone else) to any of the specific place % of women who reported being verbally or physically abused by their family in their most recent pregnancy % of women experienced violence in 12 months preceding the survey % of women who have ever experienced any type of domestic violence % of women who have experienced physical violence in the past 12 months % of women who have ever suffered emotional, physical, or sexual violence in the family % of women who have ever sought help from any source to end the violence % of women who have reported that in past few weeks they lost/felt her mental health due to any type of domestic violence % of women who have ever experienced domestic violence by participation in decisionmaking (Own health care, Large household Purchases, Small household purchases, Visits to her family or relatives). % of women aware about Acts of violence KNOWLEDGE AND AWARENESS Women’s knowledge and awareness about: - Aware of treatment for diarrhoea - Treatment of ARI/ Pneumonia - women who are aware importance of HAF/ORS/ORT - Vitamin A doses/schedule - Hygiene practices danger signs in pregnancy - Danger signs of reproductive morbidity - RTI/STI - danger signs of New Born which required medical care - IFA tablets and syrup for pregnant women - Early initiation of breastfeeding - Importance of colostrum Mothers of children <5 years √ Mothers of children <5 years √ Mothers of children <5 years Mothers of children <5 years Mothers of children <5 years √ √ √ √ √ √ Mothers of children <5 years Mothers of children <5 years √ Mothers of children <5 years √ Mothers of children <5 years √ Mothers of children <5 years Mothers of children <5 years √ Page 23 of 31 Corrigendum 1: Final ToR for CCM Endline (with sampling) INDICATOR MATCHING INDICATORS CCM CBA RESPONDENTS/DEFINITIONS - At what age should a child be exclusively breast-fed - prevent iron deficiency among children - Timing of introduction of complementary foods % of women who think weight gain in Mothers of children <5 years (we could pregnancy should be monitored consider restricting to mothers of children <1 or <2 years) % of women reporting they ate less, the same, As above or more during their most recent pregnancy than before in different trimesters Women’s perceptions, awareness and Mothers of children under-five participation in: - AWC services/activities - ASHA services/activities - ANM services/activities - Village health sanitation and nutrition day - Referral process for malnourished children to NRC - Village health sanitation and nutrition committees - Mata Samiti - Nigrani committees Sources of data from the Health Sub centre (HSC), Anganwadi Centre (AWC), Households (HH), VHSND/VHSNC/BD/Mata Samiti apart from these we will collect the data to services provider. Data from more than one source will be used for triangulation. √ √ √ Page 24 of 31 Corrigendum 1: Final ToR for CCM Endline (with sampling) ANNEX 3 –COMPONENTS USED IN THE BASELINE CCM SURVEY The following components/tools were used as a part of the baseline CCM and will form the basis for the endline survey, but this open to additions and refinements after discussions between BTAST and the contracted agency. This list is provided here to assist the development of the initial expressions from interested agencies. A. Beneficiary interviews 1) Interview with the head of the household For each sampled household the head of the household will be interviewed using a household questionnaire to collect basic information such as age, sex, marital status, and educational status of each member in the household. In addition, the household questionnaire will collect information on sources of livelihood and ownership of assets, landholdings, type of house, media exposure, materials used for cooking, source of lighting, source of drinking water, access to toilet facilities, and types of toilets. The above information will be collected for all the households having at least one eligible respondent considered for the study. 2) Men’s questionnaire Husbands of women with a child under-five will also be interviewed. Areas of enquiry include: Information from eligible women’s husbands about age, educational status, occupation, knowledge and source of knowledge and practices of health, nutrition and watsan services, reported symptoms of RTI/STI , knowledge to violence against women and male participation. Apart from these information desires for children, reasons for not using Family Planning methods, future intention to use Family Planning methods and knowledge about no scalpel vasectomy (NSV) data will collect. 3) Interview among mothers/primary caregivers of children under 5 years As per the objective of the study the mothers of children under 5 years (or their primary caregiver if not the mother) will be interviewed using a structured questionnaire. The issues to be covered during the interviews include maternal/caregiver factors, coverage and quality of services, child factors, and other relevant indictors for estimating maternal mortality 4) Interview among pregnant women Pregnant women will be interviewed using a structured questionnaire to assess: Knowledge, awareness and practices in relation to pregnancy; Knowledge Awareness and Practice regarding nutrition needs and care of women and young children; Availability, accessibility, quality and utilization of antenatal services at AWC/VHSND; Availability, utilization and perceptions regarding SNP at the AWCs; Coverage of micro nutrients supplements including IFA; Interactions with FLWs and kind of advise received on pregnancy and delivery related and health care seeking; the regularity and content of outreach services in the village/status of (village health sanitation and nutrition committee (VHSNC). 5) Interview among adolescent girls Adolescent girls will be interviewed using a structured questionnaire. Data will be collected about: Health and hygiene (e.g. menstrual hygiene); Coverage of micro nutrients supplements including IFA; Availability, utilization and perceptions (e.g. of quality) regarding services at the AWCs Page 25 of 31 Corrigendum 1: Final ToR for CCM Endline (with sampling) 6) Interview among women who had a pregnancy outcome in the reference period This will enable measurement of stillbirths, neonatal mortality and other indicators such as the sex ratio. B. Service Provider Interviews 1) ASHA Interview Attempts will be made to assess the Knowledge Awareness and Practices of ASHA workers on health nutrition and watsan of mothers of young children, pregnant women, child feeding, immunization, ANC, PNC, etc. Apart from this AHSA worker’s role in preparing micro birth plan, motivating pregnant women for institutional deliveries will be assessed. Areas specific to training and capacity building activities will be also looked into. 2) ANM Interview Attempts will be made to assess the Knowledge Awareness and Practices (KAP) of ANMs on health nutrition and watsan of mothers of young children, pregnant women, child feeding, immunization, ANC, PNC etc. Apart from this ANM’s involvement in preparation of micro birth plan, promoting family planning and institutional deliveries will be assessed. In addition to this her monthly progress report (MPR) will be reviewed and analysed and vital statistics pertaining to her sub-centre will be gathered. Areas specific to training and capacity building activities will also be assessed. 3) MOIC / CDPO Interview MOIC and CDPOs will be interviewed in every block. Attempts will made to assess the Knowledge Awareness and Practices (KAP) on various issues relating to supply of instruments/equipment and medicines to the AWCs, Sub-center, PHC, up-gradation/construction of AWC / sub-center buildings, coverage of training programmes, MIS system, performance of AWCs in providing and implementation of nutrition other than those of ICDS and SHIFW etc and role of PRIs. 4) DSWO Interview At the district level quarterly report will share to the DSWO. One meeting will held at the district level to understand the status of the outcome indicators. Efforts will be made to understand the impediments to health nutrition and watsan village level services. C. Facility Surveys 1) AWC Observation and services In each sampled AWC the team will spend a full day and make observation on the location of the AWC, electricity, water and sanitation facilities, availability and working condition of the instruments/equipment, SNP (THR), availability and display of IEC materials, stock position of various supplies, availability of preschool kits/play materials, storage facilities, availability and maintenance of records registers and growth charts at the AWCs etc. The number and type of beneficiary’s visit the facility and method of providing services to the beneficiaries will be observed at the AWCs. An observation check list will use to record the observations at the AWCs. AWWs will also be interviewed using the same lines of enquiry as given in B1 and B2 above. 2) Observation of facilities and services in Sub Centers (SC) Page 26 of 31 Corrigendum 1: Final ToR for CCM Endline (with sampling) Sub-centres will be assessed using an observation check list covering the availability of basic medicine, IEC materials, drinking water, sanitation, instruments and equipment, adequate staff, buildings, condition of the buildings, attendance of service users etc. 3) VHSND Observation The village health sanitation and nutrition day (VHSND) is the fixed health and nutrition day observed at the AWC. An observation check list will be used to observe participation of service providers and beneficiaries, number of beneficiaries attending the AWC. The checklist will also be used to check the availability of electricity, water and sanitation facilities, availability and working condition of the instruments/equipment, SNP (THR), availability and display of IEC materials, stock position of various supplies, storage facilities, availability and maintenance of records registers and growth charts at the AWCs etc. The number and type of beneficiaries visit at facility and method of providing services to the beneficiaries will observe at the AWCs. An observation check list will be used to record the observations at the AWCs on VHSN days. 4) Bachpan Divas Observation Bachpan Divas will be observed in each Block though an observation checklist. Participation of service providers and beneficiaries, number of beneficiaries attending the Bachpan Divas and the activities undertaken will be observed. 5) Village level checklist A village check list will be used to observe availability of drinking water in the village, sanitation facilities, drainage facilities, location of the AWC and the sub-center, improved percentage of functional tube well in the village, and average number of improved water sources (quality tested) in the village. Areas of inquiries will fed back in consultation with B-TAST and NBA coordinator. 6) Assessment of Nodal Anganwadi Centres Nodal AWCs are another SWASTH programme of interest. We request that the agencies propose a nested methodology, including the sampling approach and indicators to assess the functioning of Nodal AWCs. D. Other estimates and measurements 1) Anthropometric Measurement Among Children Under 5 Years Undernutrition will be assessed as follows: - Wasting (weight-for-height Z-score <-2.00, MUAC <115 mm), - Stunting (height-for-age Z-score <-2.00) - Underweight (weight-for-age Z-score <-2.00) - Global and Severe Malnutrition (wasting + oedema) The following procedure will be followed for ascertaining the age of the child - The information on date of birth, and age of each child in completed months will be ascertained from the mother of the child using a specially designed local event calendar. A variety of probing techniques will be used to ensure maximum accuracy in recording child age. Page 27 of 31 Corrigendum 1: Final ToR for CCM Endline (with sampling) - The guidelines given in the United Nation’s “How to weigh and measure children” will be followed whilst taking anthropometric measurements of children (DP/UN/INT-81-041/6E Manual) - The weight of each child will measure by using digital weighing machines. The weight measurement will record up to 100 grams. - Children under-two years of age should have their recumbent length measured, and children two and older should have their standing height measured to the nearest mm with appropriate equipment. - MUAC should be measured with an appropriately marked tape, and measured to the nearest mm. - Assessment for the presence of bilateral pitting oedema in both feet should be made. Page 28 of 31 Corrigendum 1: Final ToR for CCM Endline (with sampling) ANNEX 4 - QUALITY ASSURANCE PROCEDURES INCLUDE: A. Selection of Interviewers & Supervisors Investigators and supervisors should be graduates having 1-2 years’ experience in health-nutrition related survey and CAPI Should be familiar with local dialect Should be able to conduct interviews in the villages with appropriate respondent Should be able to conduct in-depth interviews with Government functionaries B. Training: Interviewers & Supervisors: Trainers should be well trained on the topic/subject Need to follow training rules: No more than 30 participants in one batch of training Required training materials should be submitted to and approved by B-TAST before training begins Required training materials should be provided to each interviewer/participant during the training Training should be conducted over the duration specified by BTAST Required equipment should be available in the venue Participatory methods should be used in training instead of one-way training Mock interviews and focus group practice should be done during training Two days field practice and follow-up debriefing session should be conducted to rectify any query, confusion, problems etc. encountered by the participants 1-2 persons from B-TAST will be present in the training to provide support as well as monitor the training C. Formation of Survey Teams Team size and number of teams should be formed as per MoU A list of team members (name of interviewers and supervisor) will be provided to B-TAST before starting fieldwork Only trained interviewers will be in the team throughout the fieldwork, and no substitute will be allowed Team should contain 2-male, 2-female interviewers and 1-supervisor Incomplete teams will not start fieldwork – In such cases, BTAST representative must be informed so that appropriate action can be taken D. Survey Implementation/field Visit Plan The survey agency will submit a visit plan before starting fieldwork and BTAST should be notified of any deviation to the plan well in advance (at least 1 week) so that appropriate arrangements can be made for monitoring purpose. Visit plan should be prepared with name of interviewers and supervisors and their assigned district, block, & villages and contact details (i.e. mobile phone number) Page 29 of 31 Corrigendum 1: Final ToR for CCM Endline (with sampling) Only complete team will conduct survey – no substitute or temporary arrangements will be allowed Each interviewer must have CAPI without CAPI team will be considered incomplete All essential equipment must be taken to each site and used by the fieldwork teams e.g. correct measuring equipment BTAST will provide an initial list of selected sample sites (sampled by an independent statistician). After this, the remaining list will be provided only when BTAST is satisfied with the data quality and completion of previous work which will be measured based on the raw data provided by the survey agency after completion of each Block. If for any reason it is not possible to collect data from the specified sites (e.g. household) then an agreed plan for selection of alternatives will be followed. E. Quality Control at the Field and office Level >40% back check, cross check, and spot check should be done by the survey agency field supervisors and 10% supervision will be done by the survey agency coordinator in the field Supervisor should check data collected before leaving the village and take all reasonable efforts to ensure the data is of good quality A list should be prepared for daily monitoring checks by the supervisors B-TAST will select Quality Assurance officers for field monitoring & supportive supervision B-TAST will also conduct quality assurance checks BTAST team will visit the research agency offices to check office editing work as well as data entry and analysis F. Other Key Instructions Survey work will start in Priority Districts Survey will be started in 2 districts at a time and move forward simultaneously B-TAST will provide a list of selected villages of each block Survey will be conducted as per the final sampling strategy Raw data will be shared on weekly basis Based on data quality, approval will be given for further work Standard instruments will be used in data collection like BMI tap, digital weighing machine, height measurement instrument etc. Temporary arrangements will not be allowed or compromise with the standard G. Responsibilities of Survey Agency • Survey Agency will be required to ensure quality of data collected by adhering to the following: o The Field Survey Team should ensure complete coverage of the sample units in the block, households in sample unit and also the contents of the surveyed schedules by undertaking a thorough checking. Due care should be taken for legibility of writing, Page 30 of 31 Corrigendum 1: Final ToR for CCM Endline (with sampling) clarity of figures, correct transfer entries between schedules, etc. as per the field scrutiny guidelines, to be prepared and used by the agency and guidelines to be shared with B-TAST. o The primary responsibility of the Survey Supervisor will be to supervise the fieldwork of the survey teams allotted to him/her. He/she will carry out independent inspections in not less than 10% of the households in each of the sample units. Besides, he/she would also carry out a detailed scrutiny of all the surveyed schedules to check for inter and intra consistency of data and also to rule out any other kind of mistakes as per the scrutiny plan, to be prepared and used by the agency and scrutiny plan to be shared with B-TAST. • Survey agency will have to rectify errors generated during data entry due to various inbuilt validation checks in the data entry application. • Regular inspections by B-TAST officials will be carried out to secure the overall quality of data. The inspections may be in the form of concurrent or post-survey inspection. If any irregularities are found as a result of these inspections, the survey agency needs to rectify the same. Survey agency shall be responsible to provide requisite information and facilitate inspection by B-TAST officials. • B-TAST will deploy a third-party or independent research officers for auditing the surveyed data to ensure its quality and also to maintain the credibility during the survey. Survey agency shall be required to provide requisite information and facilitate inspection by the third party audit team or independent research officers. The findings of the third party audit team or independent research officers shall be binding on the survey agencies. The role of independent QA consultants Sampling errors will be monitored by establishing whether the agency has collected data in the specific villages that have been sampled. Non-sampling errors (e.g. whether supervisors and interviewers are adhering to agreed data collection protocols, and whether survey responses are consistent during back-checks) will be minimized through field assessments by 9 QA consultants. QA consultants will undertake frequent spot checks and back checks to ensure field data quality. They will also attend the training of data collectors to gain a deeper understanding of the expectations of the different cadres of field staff. A checklist for the QA consultants to use in the field is being developed by B-TAST. Training on how to use the tool and undertake QA activities will be provided by B-TAST. Page 31 of 31





© Copyright 2026