
Rate Response (RR)
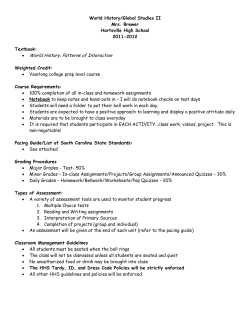
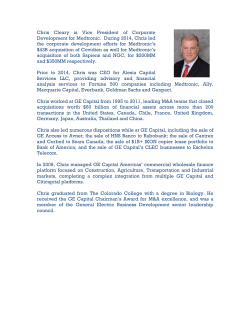
Rate Response (RR) Overview Rate-responsive pacing adapts the pacing rate to changes in patients’ physical activity. An activity sensor is used to measure the patients’ movement and to determine the appropriate pacing rate. Programming Programming parameters include: Rate Profile Optimization* Automatically adjusts the rate response slope as a patient’s conditions change. Changes are based on comparing the pacemaker’s historical sensor-indicated rate profiles against a clinician prescribed target rate profile of the patient. Nominally On. Lower Rate The programmed rate at which a pacemaker will pace the heart in the absence of intrinsic cardiac activity. Nominally 60 bpm. ADL (Activities of Daily Living) Rate* The average target rate that the patient achieves for moderate activities. Nominally 95 bpm. ADL Response* Determines the incremental increase or decrease in the sensor-driven rate for a given level of activity in the ADL rate range. o The nominal setting for the ADL Response parameter is 3. o Programming a higher number increases the sensor indicated pacing rate for a given amount of activity, increasing rate responsiveness in the ADL rate range. o Programming a lower number decreases the sensor indicated pacing rate for a given amount of activity, thereby decreasing rate responsiveness. Upper Sensor Rate The fastest rate at which the heart will be paced in response to signals from the rate-response sensor. Nominally 130 bpm. Exertion Response* Determines the incremental increase or decrease in the sensor-driven rate for a given level of activity in the exertion rate range. o The nominal setting for the Exertion Response parameter is 3. o Programming a higher number increases the sensor indicated pacing rate for a given amount of activity, increasing rate responsiveness in the exertion rate range. o Programming a lower number decreases the sensor indicated pacing rate for a given amount of activity, thereby decreasing rate responsiveness. Activity Threshold The activity sensor converts detected motion into electrical signals and is used in computing the sensor-indicated rate. o Programmable settings: Low Responds to most body activity, including minimal exertion. Medium/Low Limited response to minimal exertion, responds to moderate/greater exertion. Medium/High Limited response to moderate body movements and exertion. High Responds to only vigorous body movements and exertion. © 2013 Medtronic, Inc. www.medtronicfeatures.com Page 1 of 6 Activity Acceleration Determines how quickly the pacing rate increases to the target sensor rate when the patient exercises. Activity Deceleration Determines how quickly the pacing rate declines to the target sensor rate when the patient’s activity stops. Rate Response Determines the level of rate response for devices with single zone rate response programming options. Higher numbers indicate a more aggressive increase in rate for a given level of sensed physical activity. * These programming options are only available in devices that have dual zone rate response. To program this feature in pacemakers, go to Params -> Rate Response. To program this feature in ICDs, go to Params -> Pacing -> Rate Response. Programming for devices with dual zone rate response © 2013 Medtronic, Inc. www.medtronicfeatures.com Page 2 of 6 Programming for devices with single zone rate response Feature Operation Rate responsive (also called rate modulated) devices provide patients with the ability to vary heart rate (between the programmed lower and upper sensor rate) when the sinus node cannot provide the appropriate rate. Operation of Rate Response in devices with dual zone Rate Response The device may provide appropriate rate response for patients who require cardiac pacing support at both submaximal and maximal rates. Submaximal rates are moderate pacing rates near the Activities of Daily Living Rate (ADL Rate) obtained during typical daily activities, such as walking or daily chores. Maximal rates are rates (at or near the Upper Sensor Rate) obtained during vigorous activities. To achieve appropriate rate response, the pacemaker provides activity sensor-driven pacing with rate response control in both the ADL rate range and the exertion rate range. The device provides appropriate rate response by employing the following operations: Three programmable rates control the submaximal and maximal rate ranges: Lower Rate, ADL Rate (Activities of Daily Living Rate), and Upper Sensor Rate. The ADL Rate is equivalent to the average target rate that the patient achieves for moderate activities. Independent control of rate response is provided in the Activity Threshold setting and the ADL/Exertion rate ranges. o Activity Threshold is used in computing the sensor-indicated rate. The activity sensor converts detected motion into electrical signals. o Programmable settings: Low Responds to most body activity, including minimal exertion. Medium/Low Limited response to minimal exertion, responds to moderate/greater exertion. Medium/High Limited response to moderate body movements and exertion. High Responds to only vigorous body movements and exertion. For models in a rate responsive mode, the device automatically enables rate response after implant and automatically adjusts rate response using Rate Profile Optimization, if necessary, once each day. © 2013 Medtronic, Inc. www.medtronicfeatures.com Page 3 of 6 For pacemakers during the first 30 minutes after implant, pacing occurs at the implanted mode but without rate response. 30 minutes after implant, rate response operation is enabled. For ICDs Rate Response and Rate Profile Optimization begin operating after implant, when VF Detection is programmed to On. Once each day, rate response is assessed and adjusted, if necessary, in the ADL and exertion rate ranges. The assessment is based on comparing the pacemaker’s historical sensor-indicated rate profiles against a clinician prescribed target rate profile of the patient. If the rate profiles differ, rate response is adjusted slightly in the appropriate rate range, and the assessment is repeated again the next day. As the ADL Response and Exertion Response parameter settings are changed, the device will make it easier or harder to achieve these rate regions. Increasing the ADL or Exertion response settings results in the device defining a new Target Profile, or ideal rate distribution. This may eventually cause the device to automatically adjust the corresponding setpoints for the ADL Rate and USR to a different value. For example, as the setpoint value decreases, the slope is made more aggressive, thus the patient is able to achieve higher rates with less effort, and ultimately, spend a larger percentage of time in that particular rate range. If Rate Profile Optimization is set to Off, the setpoints will not change and a new Target Profile will not be created. Operation of Rate Response in devices with single zone Rate Response The sensor-indicated rate is determined by the sensed activity and the Rate Response parameter setting, and it can range between the programmed Lower Rate and the Upper Sensor Rate. The sensed activity is measured using the activity threshold that operates as described in the dual zone operation description above. The Rate Response parameter is set to a number between 1and 10 (see Figure below). If this parameter is set to a larger number, the indicated pacing rate is higher for a specified level of detected activity. If the sensor-indicated rate is greater than the current pacing rate, the pacing rate accelerates toward the sensor-indicated rate. The speed of this increase is determined by the Activity Acceleration parameter setting. If the sensor-indicated rate decreases, the pacing rate decelerates to the sensor-indicated rate. The rate of deceleration is determined by the programmed Activity Deceleration setting. © 2013 Medtronic, Inc. www.medtronicfeatures.com Page 4 of 6 Devices Pacemakers/CRT-P With dual zone Rate Response Advisa MRITM SureScan® Pacing System, Adapta® SR, Adapta DR, Versa® DR, Sensia® SR, Sensia DR, Consulta® CRT-P, Syncra® CRT-P With single zone Rate Response Revo MRI® SureScan® Pacing System, EnRhythm® DR ICDs/CRT-D With dual zone Rate Response EveraTM XT VR, Evera XT DR, Evera S VR, Evera S DR, Protecta® XT VR, Protecta XT DR, Protecta VR, Protecta DR, Secura® VR, Secura DR, Virtuoso® II VR, Virtuoso II DR, Maximo® II VR, Maximo II DR, VivaTM XT CRT-D, Viva S CRT-D, Protecta XT CRT-D, Protecta CRT-D, Consulta CRT-D, Concerto® II CRT-D, Maximo II CRT-D With single zone Rate Response Virtuoso DR, Virtuoso VR, Concerto CRT-D ® ® ® ® Sources: Medtronic Adapta /Versa /Sensia Reference Guide; Medtronic Consulta CRT-P Clinician Manual; Medtronic ® ® Protecta XT DR Clinician Manual; Medtronic Protecta XT CRT-D Clinician Manual. This document is provided for general educational purposes only and should not be considered the exclusive source for this type of information. At all times, it is the professional responsibility of the practitioner to exercise independent clinical judgment in a particular situation. Changes in a patient’s disease and/or medications may alter the efficacy of a device’s programmed parameters or related features and results may vary. The device functionality and programming described in this document are based on Medtronic products and can be referenced in the published device manuals. © 2013 Medtronic, Inc. www.medtronicfeatures.com Page 5 of 6 Indications, Safety, and Warnings Brief Statement: IPGs, ICDs, CRT ICDs and CRT IPGs Indications Implantable pulse generators (IPGs) are indicated for rate adaptive pacing in patients who may benefit from increased pacing rates concurrent with increases in activity and increases in activity and/or minute ventilation. Pacemakers are also indicated for dual chamber and atrial tracking modes in patients who may benefit from maintenance of AV synchrony. Dual chamber modes are specifically indicated for treatment of conduction disorders that require restoration of both rate and AV synchrony, which include various degrees of AV block to maintain the atrial contribution to cardiac output and VVI intolerance (e.g. pacemaker syndrome) in the presence of persistent sinus rhythm. For the MR conditional IPGs, a complete pacing system consisting of a Revo MRI or Advisa MRI IPG and 2 SureScan leads is required for use in the MR environment. Implantable cardioverter defibrillators (ICDs) are indicated for ventricular antitachycardia pacing and ventricular defibrillation for automated treatment of life-threatening ventricular arrhythmias. Cardiac resynchronization therapy (CRT) ICDs are indicated for ventricular antitachycardia pacing and ventricular defibrillation for automated treatment of life-threatening ventricular arrhythmias and for providing cardiac resynchronization therapy in heart failure patients who remain symptomatic despite optimal medical therapy, and meet any of the following classifications: New York Heart Association (NYHA) Functional Class III or IV and who have a left ventricular ejection fraction ≤ 35% and a prolonged QRS duration. Left bundle branch block (LBBB) with a QRS duration ≥ 130 ms, left ventricular ejection fraction ≤ 30%, and NYHA Functional Class II. CRT IPGs are indicated for the reduction of the symptoms of moderate to severe heart failure (NYHA Functional Class III or IV) in those patients who remain symptomatic despite stable, optimal medical therapy, and have a left ventricular ejection fraction less than or equal to 35% and a prolonged QRS duration. Contraindications IPGs and CRT IPGs are contraindicated for dual chamber atrial pacing in patients with chronic refractory atrial tachyarrhythmias; asynchronous pacing in the presence (or likelihood) of competitive paced and intrinsic rhythms; unipolar pacing for patients with an implanted cardioverter defibrillator because it may cause unwanted delivery or inhibition of ICD therapy; and certain IPGs are contraindicated for use with epicardial leads and with abdominal implantation. ICDs and CRT ICDs are contraindicated in patients whose ventricular tachyarrhythmias may have transient or reversible causes, patients with incessant VT or VF, and for patients who have a unipolar pacemaker. In CRT ICD systems, the leads are contraindicated for patients with coronary venous vasculature that is inadequate for lead placement, as indicated by venogram. The lead is also contraindicated in patients for whom a single dose of 1.0 mg of dexamethasone acetate and/or dexamethasone sodium phosphate may be contraindicated. Warnings/Precautions Changes in a patient’s disease and/or medications may alter the efficacy of the device’s programmed parameters. Patients should avoid sources of magnetic and electromagnetic radiation to avoid possible underdetection, inappropriate sensing and/or therapy delivery, tissue damage, induction of an arrhythmia, device electrical reset or device damage. Do not place transthoracic defibrillation paddles directly over the device. Additionally, for CRT ICDs, certain programming and device operations may not provide cardiac resynchronization. Potential Complications Potential complications include, but are not limited to, rejection phenomena, erosion through the skin, muscle or nerve stimulation, oversensing, failure to detect and/or terminate arrhythmia episodes, and surgical complications such as hematoma, infection, inflammation, and thrombosis. An additional complication for ICDs and CRT ICDs is the acceleration of ventricular tachycardia. See the device manual for detailed information regarding the implant procedure, indications, contraindications, warnings, precautions, and potential complications/adverse events. For further information, please call Medtronic at 1-800-328-2518 and/or consult Medtronic’s website at www.medtronic.com. Caution: Federal law (USA) restricts these devices to sale by or on the order of a physician. World Headquarters Medtronic, Inc. 710 Medtronic Parkway Minneapolis, MN 55432-5604 USA © 2013 Medtronic, Inc. Tel: (763) 514-4000 Fax: (763) 514-4879 Toll-free: 1 (800) 328-2518 (24-hour technical support for physicians and medical professionals) www.medtronicfeatures.com Page 6 of 6










© Copyright 2026