
The Childhood Brain Tumor Foundation
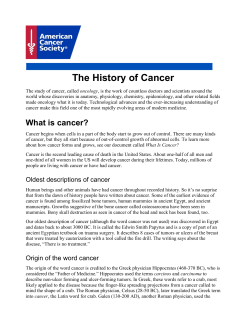
The Childhood Brain Tumor Foundation Fall –Winter 2005 20312 Watkins Meadow Drive, Germantown, MD 20876 877-217-4166 301-515-2900 CBTF is a nonprofit 501(c)(3) allvolunteer organization, founded in 1994. Board Members: Jeanne Young, President Gilbert Smith, Esq., Vice President Michelle O’Brien, Secretary James Young, Treasurer Directors: Carol Cornman Michael Greenspun Danielle Kerkovich, Ph.D. Stephen Schoenfeld, CPA Claire Wynn Senior Medical/Scientific Advisor: Roger J. Packer, M.D., pediatric neurologist, Children’s National Medical Center, Washington, D.C. Medical/Scientific Advisors: Susan Blaney, M.D., pediatric oncologist, Texas Children’s Cancer Center, Houston, TX Francisco Bracho, M.D., pediatric oncologist, Georgetown University Medical Center, Washington, D.C. Derek Bruce, M.D., pediatric neurosurgeon, Children’s National Medical Center, Washington, D.C. Peter Burger, M.D., neuro-pathologist, Johns Hopkins Medical Center, Baltimore, MD Mel’s Message of Hope By Mel Degiorgis from Billingham, England In autumn of 2004, my second to the last year of school, I had been sleeping a lot and had been getting painful headaches that had been getting worse for two years. It got so bad, my concentration was going and I was often sent home from school in excruciating pain. My colour vision was slowly going and my optician found that I had pale optic discs so I wanted to see a specialist. I was told by a neurologist on three different occasions that I was just a child complaining of headaches, and sent home on anti-depressants. My mam insisted on a brain scan and the neurologist reluctantly agreed to order one. The doctor called to say there was an abnormality on the scan and that we needed to pack a bag and go to the hospital the next morning. They admitted me to a ward and ordered more tests, including a more detailed scan to see exactly what the problem was. The neurologist came back the next day and told me and my mam that I had a brain tumour. I was devastated! This is something everyone worries about but never actually thinks it’s going to happen to them. When my dad walked into the room and we told him, he sat on the bed next to me and cried while rocking me back and forth. I Neurotransmitter Communicating our message. Http://www.childhoodbraintumor.org Surgery and Radiation Therapy for Craniopharyngioma Ori Shokek, M.D. Moody D. Wharam, Jr., M.D., F.A.C.R. Craniopharyngioma is a brain tumor that occurs in children. It is seen in the suprasellar region of the brain, a centrally located area adjacent to of critical structures including the nerves that conduct visual signal from the eyes to the brain, the ventricular system which governs the flow and pressure of the fluid that surrounds the brain, and the pituitary gland and hypothalamus which produce important regulatory hormones. Because the tumor does not invade and destroy the normal tissues that surround it, and as it does not spread distantly away from its local origin, it is said to be a benign tumor. However, as it grows, the tumor can damage those critical structures that surround it, resulting in disturbance of their normal function. Such disturbance, commonly in vision, brain pressure, and hormone production, is typically what first brings the patient to medical attention. Kenneth Cohen, M.D., pediatric oncologist, Johns Hopkins Medical Center, Baltimore, MD Marianna Horn, M.D., pediatric oncologist, Fairfax Hospital, Fairfax, VA Tobey MacDonald, M.D., pediatric oncologist, Children’s National Medical Center, Washington, D.C. Eva Perdahl-Wallace, M.D., Ph.D., pediatric oncologist, Fairfax Hospital, Fairfax, VA Katherine Warren, M.D., pediatric oncologist, Bethesda, MD Scientific Advisor: Gil Smith, Ph.D., Bethesda, MD Legal Advisor: Frederick Rickles, Esq., NY Community Representatives: Mary T Callahan, TX Carol Parham, CT Doug & Lydia DeFeis, FL Linda Quackenbush, UT Kyle Killeen, NJ Andrew Schoenfeld, CA Peggy Killeen, NJ Nancy Ward, IL Kate Lund, MA Susan Young, MD Pat Macy, NY Beth Zermani, MA Barbara Norris, MA Richard & Dorothy Suberg, TX (continued on page 4) Issue 27 • • • • • • Surgery and Radiation Therapy for Craniopharyngioma by Dr. Shokek and Wharum; Mel’s Message of Hope...page 1 Putt~Putt for Peds, Grant Fundings...page 3 CBTF Fund-raising 5K. page 6 Can I Take My Panda Daddy?; Hopes of Life.. .page 7 Remembrances page 8 Donor information….page 9 Figure 1: A 5 year old boy presented with tiredness, impaired vision, and difficulty with being awakened. His coronal (or frontal) view MRI scan shows a large central, multicystic lesion which is bright with contrast-enhancement. The adjacent ventricles are enlarged. Tissue removed at surgery revealed craniopharyngioma. This child's tumor is larger than the typical lesion. (continued on page 2) Page 2 The Childhood Brain Tumor Foundation Surgery and Radiation Therapy for Craniopharyngioma (continued from page 1) Figure 2: The axial view of the same lesion emphasizes its central location and multicystic nature. Craniopharyngioma is curable in the majority of patients. Treatment for this tumor most often involves surgery and radiation therapy. Although complete surgical resection can be sufficient for cure, the tumor is often simply sticky, and there can be significant difficulty in removing it from the critical structures to which it may adhere. The attempt at complete surgical resection may result in damage to those same critical structures. The same neurologic disturbances that can be caused by the tumor itself can also result from such surgery, and they can be life-long. In addition, MRI or CT scans performed after an attempt at a complete resection sometimes reveal residual tumor. Therefore, an established treatment approach in many medical centers in the United States involves a partial resection of the tumor (often termed ‘decompressive surgery’) followed by radiation therapy. As far as cure, results with partial resection and radiation therapy are often as good as complete surgical resection. Radiation therapy has side effects. There can be hormonal disturbances, although those caused by radiation therapy are typically easier to manage. Visual deficits are uncommon. Additional side effects exist but depend on the particular patient, on his or her age, and on the extent and size of the tumor. It is important for patients and families to be familiar with the types of treatment their physicians might recommend. Most people have a basic understanding of what surgery is, but not everyone is familiar with radiation therapy. Radiation therapy typically uses X-rays, similar to those used by a CT scan. ‘External beam’ radiation therapy is the most common way treatment is given. Here, radiation is directed toward the patient from an external machine, usually a ‘linear accelerator’. Multiple beams are used, all individually shaped and all converging upon the tumor, such that the tumor receives the sum of their individual doses of radiation; the surrounding brain structures receive only the contribution of each individual beam. Treatment is typically given in daily sessions over a course of approximately six weeks, with a small fraction of the total dose delivered on any given day. Larger doses of radiation given over a shorter time course have the potential to cause greater side effects. However, certain small craniopharyngiomas are amenable to even one single large dose of radiation, if sparing of surrounding critical structures is possible. For such selected tumors, the ‘Gamma Knife’ is a highly specialized external beam machine which is quite effective. X-rays are not the only type of radiation used in the treatment of craniopharyngioma. Protons are another type and have the advantage that their dose can be directed to a particular depth as it is aimed at the tumor. Lastly, some craniopharyngiomas which have fluid filled cysts are amenable to ‘brachytherapy’. This is a way of delivering radiation to the tumor by inserting a needle into it and injecting a radioactive liquid that emits radiation. As brachytherapy allows radiation to be delivered from the inside of the tumor, it has the advantage that only negligible doses of radiation reach adjacent normal brain structures. In summary, craniopharyngioma is a benign tumor seen in children. Its cure rate is high, and treatment is individualized and commonly includes surgery and radiation therapy. Potential side effects are carefully considered when choosing the treatment approach. Physicians at medical centers dedicated to the management of childhood brain tumors are able to offer the appropriate level of expertise and can optimally tailor treatment to the individual patient. Ori Shokek, M.D. is a fourth year resident and Chief Resident in Radiation Oncology; Moody D. Wharam, M.D., F.A.C.R. is Professor of Radiation Oncology. Both are in the Department of Radiation Oncology and Molecular Radiation Sciences, the Johns Hopkins University School of Medicine, Baltimore, Maryland. Page 3 The Childhood Brain Tumor Foundation Putt~Putt for Peds, Miniature Golf Fun while fund-raising On Saturday, October 1, 2005, the Childhood Brain Tumor Foundation launched a Our first miniature golfers ready to go! brand new fund-raising event, Putt~Putt for Peds, consisting of a round of miniature golf. The event was held at the South Germantown Recreational Park in Boyds, Maryland and was organized by CBTF Board Member, Michael Greenspun, with help from several Board Members. It was an absolutely beautiful day and the event involved action packed fun from start to finish. We were joined by countless families and supporters. The festivities included musical entertainment provided by DJs Tom O’Brien and Geoff Sockol from Electric Entertainment; balloon animals and general silliness with Daisy the Clown; angel cookies by Terry Rowe from Aunt B’s Angel Cookies; excellent food; and of course, championship miniature golf. All of the golfers are now semi-pros and had a fabulous time. Thank you to all of the supporters, volunteers, and Board Members who helped make the day a smashing success. Michael Greenspun with volunteers CBTF’s 2005 Grant Funding "Determination of TP73 Expression and Function in Medulloblastoma" Dr. John Kim, Baylor College of Medicine Personal statement (excerpt) DJ, Tom O’Brien with sons Pediatrics became the focus of my clinical interests because of its intrinsic orientation toward developmental issues. I have since had the great fortune of serving children and their families who have charged me with my life¹s work. No group of patients and families appeared to need productive translational research more desperately than those suffering from brain tumors. Therefore, during my postdoctoral research, I sought to apply emerging concepts and advances in genomics and developmental neurobiology to address problems in pediatric neurooncology. Specific areas of concentration have been (1) the application of molecular and cellular biological techniques to cell culture systems (including primary human brain tumors), (2) the development and use of complementary mouse models, and (3) the integration of clinical data as essential guidance for my translational research. My research program applies wide range of emergent and established methodologies to identify molecules of clinical significance and their cellular mechanisms in medulloblastoma. The overall challenge is to develop biologically based approaches to exploit the endogenous vulnerability of medulloblastoma to committing apoptosis that would carry the promise of more effective and less toxic therapies. (continued on page 5) Page 4 Message of Hope (continued from page 1) was shocked and asked to see my scan -- the tumour was huge! It grew along both sides of my optic nerves and expanded into the pituitary gland (controlling hormones) and hypothalamus (controlling many functions and needs). The doctor said that I probably had this tumour since birth and was lucky that I hadn’t lost some or all of my vision. This optic nerve glioma, also known as juvenile pilocytic astrocytoma, was in me all this time and nobody knew. Even worse, I had been checked for all those problems in the past and nobody paid attention. So there I stayed for the next night until the neurologist said we needed to go to Newcastle to a lovely doctor who would do some more tests the next afternoon. In the children’s ward an MRI and x-ray were done and the doctor said a biopsy would be needed to verify the tumour type. On the morning of 14 November I was taken to operating theatre. I asked for gas as I had a terrible fear of needles. I was out after two breaths. When I awoke a few hours later I felt like I had been shot and was screaming and crying from all the pain behind my eyes. My mam was holding my hand and trying to calm me down. I was finally given a dose of morphine that would have knocked out a fully grown man! I spent the next two days recovering on the ward, sleeping most of the time. I even needed my stomach pressed in whilst propped up to use the bedpan -- it was weird, feeling so weak! I came round okay and was able to go home. A few days later we saw the tumour doctor in clinic and he told us that I had a low grade optic glioma, a slow growing tumour that grows along the nerves behind the eyes. My mam was relieved because she thought it was not cancer but the doctor told us it was. My mam and I started to cry as the doctor continued to say it was far too risky to operate on my tumour, and that after consulting with colleagues, she would let us know the best way to proceed. We returned to clinic a few days later and were told that radiotherapy was my best option. I started on December 29, 2004 and every day for six weeks I traveled to Newcastle for treatment. In the second week I started feeling sickly and losing my hair. Luckily I had thick hair so the Mohican style flops covered the bald spots rather nicely. It was a relief when the treatment was over but then I went back for check-ups and started on medicines for nausea, headaches and drowsiness. My appointments got fewer, around once every two weeks, and I was still not back in school so I went to a retreat set up by a charity in the Hexam countryside for week long breaks as I recovered. Everything was going great until my left leg became swollen in January. I was diagnosed with plantar fasciitis (damaged nerves in the arch of the foot and ankle.) Apparently there was no treatment for it, and I was told there could be extreme pain for six months whilst it healed. I went The Childhood Brain Tumor Foundation home, unable to walk. After a week, while staying at my friend’s house, I woke up to my leg and ankle more swollen and darker in colour. My mam took me back to the hospital and saw a different doctor who admitted me and ordered blood tests. He diagnosed me with deep vein thrombosis, which can be caused by surgery or cancer. A scan showed that mine had spread from my calf to my stomach. I was taken to the ward and fainted on the bed after I went to the toilet. My arteries were tested for blood samples and I was put on a heart monitor and oxygen mask and moved to a cardiac ward. A couple days later I was almost off the oxygen and feeling better. After breakfast I went for a walk to the toilet and collapsed again. A nurse laid me flat then I blacked out. When I came to, I was surrounded by nurses and doctors and tried to speak, but couldn’t. I saw big black shadows and a white light and I couldn’t move or breathe. Turns out my blood clot went to my lungs and caused me to faint, then on March 10 a massive clot broke off and got lodged in my heart. I was clinically dead for one hour and 40 minutes, while doctors and nurses continually checked for pulse and gave me CPR. My liver and kidney were failing and there was fear of brain damage and my chances were one in 200 that I would fully come back. Eventually I was stable enough to move to intensive care where they gave me clotbursting injection into my chest. Six days later I was out of intensive care and in a renal unit where I had three sessions of dialysis and a whole ten litres of fluid was removed from me! I then spent the next three weeks in the teenage cancer clinic. It was brilliant news that all of my vital organs were mended. I went home in a wheelchair four weeks after being admitted, two stone lighter and 100% detoxed (ha ha)! I am now walking, learning how to remember again, my clot has disappeared, and most importantly, my tumour is shrinking. I have raised 8000 pounds for charities and the hospital that looked after me. I am back to my normal self, except that I am stronger (and my mam doesn’t mind my stubbornness -- ha ha). My memory is still bad and there is no telling how bad my eyes will get but I continue to think positively. Just before I had “come back to life,” all of my relatives either saw me or heard from me and were strangely comforted by these unexplained visions -- I feel very lucky and privileged by this whole experience. I just want you readers to know that when something just doesn’t feel right you need to persist until you get the proper diagnosis and you can still kick ass even when you are at your lowest ebb -- just believe in yourself! Thanks to all the doctors that save lives everyday and my family for being such angels during a traumatic time. I would love to hear from people who have been through a similar experience -- all my love, Mel Degiorgis. Mel is 16-years-old and lives in Billingham, England Page 5 The Childhood Brain Tumor Foundation 2005 Grant Funding (continued from page 3) Second Year Funding Dr John Kim Bayjor College of Medicine Texas Children’s Cancer Center Anna M. Krichevsky Brigham and Women's Hospital Harvard Medical School "Determination of TP73 Expression and Function in Medulloblastoma" Medulloblastoma (MB) is the most common malignant brain tumor of childhood. Unfortunately, combined therapy with surgery, radiation and chemotherapy fails to cure many children. Survivors are often left with significant long-term complications of their treatments. Developing more effective and less toxic treatment requires a better understanding of MB growth. MB appears to arise in developing brain cells. The TP73 (p73) gene regulates normal brain development. TP73 can be found in two opposing forms: in the brain and in MB: TAp73, which limits cell growth, and Np73, which promotes growth. The overall effect of TP73 reflects the balance of its mutually opposing forms. We propose that Np73 promotes MB growth by antagonizing TAp73. The overall goal is to determine the activity of TAp73 and Np73 in human MB cells and in mouse MB. Our proposed studies will determine how TP73 forms modulate growth of MB and its response to radiation and chemotherapy; ultimately paving the way for clinical studies of TP73 as a therapeutic target. “MicroTargeting in Medulloblastoma” MicroRNAs (miRNAs) are a recently discovered class of tiny non-coding regulatory RNA molecules. By regulating expression of protein-coding genes, microRNAs play critical roles in development, growth, cell proliferation, and lineage determination. At least several hundred unique microRNAs are expressed in humans and these microRNAs are estimated to affect the expression of more than 30% of human proteins. By screening about 200 microRNAs expressed in human brain, we have recently identified several of those whose expression is elevated in high-grade brain tumors. During the last year, we have developed technologies to suppress these microRNAs in cultured glioblastoma and medulloblastoma cells. Knockdown of one of these microRNAs, miR-21, in glioblastoma cells triggered activation of caspases (enzymes mediating cell death) and therefore led to increased cell death. Our data suggest that miRNAs may represent a novel class of therapeutic targets for the treatment of malignant brain tumors. Dr. Jeremy Rich The Brain Tumor Center at Duke “Targeting DNA Damage Checkpoint Signaling in Pediatric Glioma Radioresistance” Childhood malignant gliomas represent one of the deadliest forms of cancer, despite treatment with maximal therapy. Surgical resection and radiation therapy have formed the basis of standard therapy for malignant glioma treatment with some benefit of chemotherapy. Despite the benefits of radiotherapy and chemotherapy for glioma patients, tumor recurrence remains the rule with these recurrent tumors demonstrating nearly universal resistance to all therapies. As both radiotherapy and chemotherapy kill cancers through similar mechanisms, it is expected that tumors may have resistance mechanisms that provide broad resistance to these agents. To date, resistance mechanisms that may be blocked to augment tumor sensitivity in clinical trials remain elusive. Chemosensitization and radiosensitization may eventually prove to be a valuable therapeutic strategy in the treatment of childhood gliomas, but the mechanisms underlying the glioma therapeutic resistance remain poorly defined. One mechanism that may be involved involves the initial cellular response to the DNA damage caused by radiation, called the DNA damage checkpoint. This checkpoint helps the cell to decide whether the cell will stop growing and repair the damage or commit suicide. We have found that inhibitors of this checkpoint can reverse the resistance of pediatric gliomas to radiation therapy. Using these treatments, we may be able to better treat children with brain tumors. Dr. Hui-Kuo Shu, Emory University School of Medicine “Characterizing resistance to small molecule inhibitors of EGFR in Malignant Gliomas” Malignant gliomas are aggressive brain tumors in children that have an extremely poor outcome. Epidermal growth factor receptor (EGFR) is thought to be important in the pathogenesis of these tumors and likely represents a good therapeutic target, especially since inhibitors of this receptor are now available for clinical use. However, my lab has previously shown that EGFR signaling within malignant glioma cell lines are not efficiently inhibited by these new drugs. One goal of our study is to elucidate the underlying molecular mechanism for this resistant response in malignant glioma. Interestingly, we also found that in some of our cell lines, EGFR signaling was not just resistant to these EGFR inhibitors but that low levels of these drugs actually enhanced cellular proliferation. This is particularly concerning for a drug that will be used clinically because of the suggestion that subtherapeutic drug levels may actually promote tumor growth in certain instances. Therefore, we are also interested in determining the cause for this growth enhancing response and why it is seen in some but not all glioma cell lines. By defining the underlying mechanisms for these problematic responses, we hope to find new ways to improve the efficacy of these EGFR inhibitors. Page 6 The Childhood Brain Tumor Foundation Rain or Shine, 2005 Stride for Life, 5K Walk/Run and Kid’s Run Award winning group enjoying the day! Lucas in the lead, running to the finish-line. Asynith Palmer accepts her first place award. Ignoring the remnants of Hurricane Katrina and Rita, a group of more than 50 runners, some walkers and the children for the Kid’s Run braved the elements to compete in the CBTF’s 1st Annual Stride for Life 5k Cross Country Run. Despite soggy conditions, which made the course even more difficult, everyone finished and had a good time along the way! Congratulations to Gary Maisus for taking first in the Overall Male Category and Ashley Young for placing 1st in the Overall Female Category. For full race results, please see http://users.aol.com/artiming/ A special thanks to our volunteers, Jen Smith, Yvonne Soghomonian, and Neil Conley and the many committee members and friends for helping on race day. Also, much appreciation to Ashley Young who acquired some great sponsors and Susan and Owen Lyon who secured our bagel donation. Our sponsors included: Deer Park Water, BagelTowne, Whole Foods, Advertising Novelty Company, Shoppers, Potomac River Running, Amazing Race Timing, Enten & Associates, and the Tshirt Broker. Thank you to the many participants who raised additional funds through sponsorships and our Spirit Participants. We can’t wait until next year’s event and hopefully better weather. The cross country course is beautiful. Happy winners share their awards with each other. Gib Smith, event CoChair with Kid’s Run winners, an enthusiastic bunch. Happy Birthday Hersha Merrbach Lois Parham Bridget Wood Jim Young Faill In Honor of Katrina Brown Justin Martin Kate Shipman Camden Wiseman Page 7 The Childhood Brain Tumor Foundation Book Corner This story is written in diary format, chronicling the journey of the Crooks family through young Sean’s battle with his brain tumor. This very touching story is deeply honest, about the physical and emotional journey that Sean endured. At age four, Sean, a vibrant young child, living in the Woolgoolga, Australia, was diagnosed with a pontine glioma. Within a short period of time after the onset of symptoms, Sean was soon diagnosed and air ambulanced to the Children’s Hospital at Westmead in Sydney for an extended course of palliative radiotherapy. Greg Crooks, Sean’s father, kept a journal throughout the experience and chose to share the memoir about Sean and his family with others, hoping that others who suffer loss will know that they are not alone. Throughout the book Greg describes everything through a father’s eyes--one who is also knowledgeable about medicine because he is a nurse. Can I take My Panda Daddy? is the only pediatric brain tumor memoir available in Australia. The book is available through Boolarong Press and can be ordered online at www.boolarongpress.com.au. “Can I Take My Panda Daddy? is a powerful journey into the heart of a family tragedy. Told through a father’s eyes, it is the story of bravery, grief and the indomitable strength of the human spirit.” ~ Michael Robotham, author of ‘The Suspect’ and ‘Lost’ The Childhood Brain Tumor Foundation will share a story that was recently written by Greg in our next newsletter edition. About the author, Greg Crooks: Greg and his family live in Woolgoolga, a small town on the mid-north coast of NSW. He trained as a registered nurse in 1980 and works as a medical/palliative nurse at Grafton Base Hospital. He loves being with his family, surfing, reading, writing, listening to music and gardening. His wife Jane is a primary school teacher. They share a daughter, Sophie. This family hopes that those who read, Can I Take My Panda Daddy? or the article in our next newsletter will understand the many obstacles these courageous children face and the journeys a family may share. Hopes of Life for Gianna Masson Proudly submitted by Keely Harris, Markee’s mother My daughter, Markee Harris, wanted to raise funds for her friend Gianna Masson, a teenager with a beautiful contagious smile, who was diagnosed with brain stem cancer in the fall of 2004. Gianna’s prognosis was bleak due to the lack of treatment options for her cancer. Markee wanted to do something to help Gianna and show support for her friend. Markee decided to have a large sweet sixteen party in her backyard and requested that, in lieu of gifts, friends and family would donate for her wish, “Hopes of Life for Gianna Masson.” Markee and her mother, Keely Harris, worked diligently together making special invitations to send to Gianna, friends, and family. The week the invitations were to be sent, Gianna unfortunately died from complications of a minor surgery which was performed on her in hopes of making Gianna more comfortable from swelling that was increasing in her brain. As a memorial donation, in Gianna’s name, to help other children have long and healthy lives, Markee decided to go ahead with her planned birthday party, but the goal now was to raise funds for pediatric brain tumor research. Gianna would have liked that! Markee took time to search the Internet for organizations that support research for children with brain tumors and chose the Foundation. Over one hundred children came to Markee’s party and everyone felt great to know that $3,060 was raised because of the party and were being donated to The Childhood Brain Tumor Foundation and Children’s Hospital of North Shore, two great causes, in memory of Gianna. Markee and her friends are extremely happy that some good can come from a tragedy, yet at the same time they will miss their dear friend. Gianna Masson will always be remembered. (1991~2005) Page 8 The Childhood Brain Tumor Foundation Remembrances John Boyles Jeff Brown Kelley Bula Barbara W. Byrum Charles Byrum Ryan Caspar Laira Caverly Josetta Chiang Shirley Coleman Geoffrey Cornman Web Daniels Tommy Donzelli, Jr. Shawn Edwards Clay Eich Barbara Waxman Fiduccia Daniel Fiduccia Margo Flamini Doyle Garrett Frank Giacin Ian Hahn Dennis Hanlon William Hanlon Katie Harris Salmaan Hava David Hayes Jonathan Hicks Erica Holm Tara Houston Joyce Hutton William Irvin, Senior Kristi Johnson David Keith Amy Kruppenbacher Rebecca Lilly Lauren Lockard Margie Kane Emily Mau Willard Maddox Gianna Mason Araminta Mustafa Bernard Miller Hannah Miller Al Nirenberg George Nuzzo Audrey Petersen Eric Richardson Jay Rowley Nicole Ringes Andrew Rypien Amy Schiller Joseph P. Sanford Lynda Santelli Luke Shahateet Steven Sliwerski Brennen Smith Lisa Soghomonian Teresa Stargel Jaime Vanderheyden Swetha Vasudevan Matthew Wierzbicki Ian Hammond Williams Ben Zell David Zucker Mary Waugh Josie Wynn Thank you Web Daniels. Web was a long time supporter of CBTF. We will always remember him! 1921~2005 Thank you for your support! The Childhood Brain Tumor Foundation, Inc. Donation form or to be added to our mailing list. Enclosed is my contribution of $: _________________________ In Memory of: ________________________________________ In Honor of: _________________________________________ On the occasion of: ____________________________________ General donation: ______________________________________ Please send remembrance card to: Name: ______________________________________________ Address: ____________________________________________ City/State/Zip: _______________________________________ Optional Phone: ______________________________________ Please make checks payable to: The Childhood Brain Tumor Foundation 20312 Watkins Meadow Drive Germantown, Maryland 20876 telephone: 301- 515-2900 toll free: 877-217-4166 Charge my: ____MasterCard _____Visa Card#________________________________ exp._____/_____ Note: minimum charge donation is $20 Name: _____________________________________________ Address: ___________________________________________ City/State/Zip: ______________________________________ Optional Phone: _____________________________________ Optional E-Mail: _____________________________________ Donations also accepted through our secure Give Button. American Express is only accepted via our Give Button on our Web site: www.childhoodbraintumor.org Your donation is tax-deductible. Page 9 The Childhood Brain Tumor Foundation Our mission is to support and fund basic science or clinical research for childhood brain tumors. We are dedicated to heightening public awareness of this devastating disease and improving the quality of life for those that it affects by funding vital research. CBTF has a website! visit us at: If you would like to receive our newsletter publications or other information, please notify us with your contact information. Office of Liaison Activities Presents: “Understanding NCI: Toll Free Teleconference Series” A downloadable flyer is available on the NCI Web site: http://la.cancer.gov/teleconference.html http://www.childhoodbraintumor.org Thanks to Tim Ratliff, Web master. WORKPLACE GIVING The Childhood Brain Tumor Foundation appreciates the continued support shown everyday by our contributors. Together, we will make a difference. Thank you to those who choose us as their charity! CBTF is in the: cfc/cca #2742 • • • Combined Federal Campaign; Children’s Charities of America (National); and United Way Gift Matching Opportunities Many companies offer a matching gifts program to support charitable organizations. Your human resources department can tell you if such a program exists in your organization. Generally, they have a form that would be sent to the Childhood Brain Tumor Foundation reporting a contribution, stating they will match the contribution. We return the form to the employer with the proper acknowledgment and information required. CBTF accepts donations via stock securities through Bank of America Investment Services, Inc. Contact our Broker, Steven P. Burroughs at 301-493-2893 or toll free at 800-638-6507. Thank you to all who have donated through stock securities. Editor: Jeanne Young Contributing Editors: Colleen Snyder and Liz Irvin Contributing Writers: Mel Degiorgis, Michael Greenspun, Keely Harris, Dr. Moody Wharum, Dr, Kim, Dr. Krichevsky, Dr. Rich, Dr. Shu, and Gib Smith, Esq. Photo contributions: Michelle O’Brien, Jen Smith, Jeanne Young and Dr. Moody Wharum Thank you to our bulk mail team. Thank you so much to the Rocking Moon Foundation for donating printing costs for this years newsletters, brochures, and our book of compiled articles and stories. The Rocking Moon Foundation also covers the mailing costs for the newsletter. Campaign donations can be made for the United Way through the “donor option” or “donor choice.” Please check with your employer in reference to United Way campaigns. We thank our military for their support and kindness toward children with brain tumors. Vehicle Donation Program CBTF now accepts vehicle donations. Donate online or call 866332-1778 and designate the Childhood Brain Tumor Foundation as your charity of choice. QUICK FACTS FOR DONATING You are eligible for an itemized TAX DEDUCTION. The service is totally free and includes convenient pick-up of your car, truck, or RV anywhere in the U.S. Find out details by checking the Foundation Web site; Http://www.childhoodbraintumor.org A big thank you to those who have donated cars!! Bequests, Planned Giving and Trusts Through a trust, bequest, or planned giving you can contribute to furthering the future research and programs of the Childhood Brain Tumor Foundation. By including the Childhood Brain Tumor Foundation in your estate planning you can minimize your taxes.











© Copyright 2026