
- Journal of Pain, The
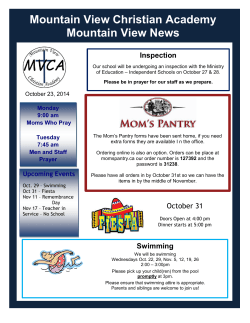
The Journal of Pain, Vol 8, No 12 (December), 2007: pp 989-997 Available online at www.sciencedirect.com Extended Swimming Exercise Reduces Inflammatory and Peripheral Neuropathic Pain in Rodents Karen E. Kuphal,*,† Eugene E. Fibuch,‡ and Bradley K. Taylor†,§ *Department of Physical Therapy and Rehabilitation Science, Kansas University Medical Center, Kansas City, Kansas. † Division of Pharmacology, School of Pharmacy, University of Missouri-Kansas City, Kansas City, Kansas. ‡ Department of Anesthesiology, School of Medicine, St. Luke’s Hospital, University of Missouri-Kansas City, Kansas City, Kansas. § Department of Pharmacology, School of Medicine, Tulane University, New Orleans, Louisiana. Abstract: Physical exercise is often recommended to patients who have chronic pain. However, only a small number of studies report exercise-induced analgesia in the setting of inflammatory pain, and even fewer relate long-term exercise to reductions in neuropathic pain. To address these questions, we evaluated the effect of extended swimming exercise in animal models of inflammatory (intraplantar injection of dilute formalin) and neuropathic (partial peripheral nerve injury) pain. We found that 9 days of swimming exercise in 37°C water for 90 min/d decreased licking and flinching responses to formalin, as compared with nonexercised control animals. In addition, 18 to 25 days of swimming decreased nerve injury–induced cold allodynia and thermal hyperalgesia in rats, and 7 days of swimming decreased nerve injury–induced thermal hyperalgesia in mice. Our data indicate that swimming exercise reduces behavioral hypersensitivity in formalin- and nerve injury–induced animal models of persistent pain. Perspective: Surprisingly, few animal studies have investigated the effects of extended exercise on chronic pain. Our results support the use of exercise as a nonpharmacological approach for the management of peripheral neuropathic pain. © 2007 by the American Pain Society Key words: Formalin, allodynia, hyperalgesia, rat, mouse. N ociception provides an early warning system that serves to minimize tissue damage in the face of potential bodily harm. The resulting acute or transient pain elicits a coordinated escape response from the threatening stimulus.50 Chronic pain, on the other hand, serves no useful purpose and instead reduces the patient’s ability to work, walk, or sleep56 and is associated with many deleterious physiological effects. Although an arsenal of analgesic drugs is readily available for the treatment of acute pain, these drugs do not provide sufficient efficacy for chronic pain in the absence of serious side effects. Numerous studies indicate that exercise decreases signs of acute pain in nonpathological conditions.22,27,30,36 HowReceived December 7, 2006; Revised August 6, 2007; Accepted August 12, 2007. Supported by NIH grant NS45954 to B.K.T. and St. Luke’s Foundation funds to E.E.F. Address reprint requests to Dr. Bradley K. Taylor, Department Pharmacology, SL83, Tulane University Health Sciences Center, New Orleans, LA 70112. E-mail: [email protected] 1526-5900/$32.00 © 2007 by the American Pain Society doi:10.1016/j.jpain.2007.08.001 ever, as reviewed by Koltyn,30 most animal studies linking exercise and pain evaluated the immediate effects of short-term exercise on transient nociceptive pain. The exceptions, using models of more persistent inflammatory pain, have yielded mixed results. Whereas Carmody and Cooper5 found that one 3-minute session of swimming in 20°C water reduced formalin-induced nociception in the mouse, Quintero et al39 found that 3 swimming sessions in warmer 24 to 26°C water increased formalin-induced nociception. The frequency and duration of swimming in these studies do not, however, reflect human exercise regimens, eg, that involve exercise training. To test the hypothesis that exercise training regimens would reduce behavioral signs of inflammatory pain, rats swam for 7 days for up to 90 min/d and were then evaluated for behavioral signs of pain in the formalin model of ongoing inflammatory nociception.13 The distinction of the effects of exercise on acute versus chronic pain is quite important, as the mechanisms underlying their control are vastly different.50 Despite this, far fewer studies have investigated the effects of exercise (particularly long-term, extended periods of exercise) on chronic pain, and the results of these studies 989 990 Extended Swimming Exercise Reduces Inflammatory and Peripheral Neuropathic Pain are mixed. Although some clinical studies suggest that exercise reduces chronic pain syndromes such as fibromyalgia, chronic low back pain, osteoporosis pain, myofascial pain, cancer treatment–related pain, and neck pain,6,14,17,20,31,33,40 others report that exercise increases the pain associated with fibromyalgia55 and chronic fatigue syndrome.57 Thus, further studies are needed to justify the widely prescribed recommendation of physical exercise (particularly long-term, extended periods of exercise) in patients who have chronic pain syndromes such as fibromyalgia, chronic low back pain, myofascial pain, and neuropathic pain.32,53,59 Specifically, there are no studies that have evaluated the effects of extended exercise in patients with a clear diagnosis of peripheral neuropathic pain. To address this gap, and to gain insight into the potential benefits of extended exercise, we evaluated the effects of repeated swimming exercise in the partial sciatic nerve injury model of peripheral neuropathic pain.43 Materials and Methods Animals Forty-four male Sprague-Dawley rats (weight range, 250 –300 g) and 33 male CD1 mice (weight range, 30 –35 g) were purchased from Charles River Laboratories (Boston, MA). For all experiments, animals were exposed to a 12-hour light/dark cycle and were given food and water ad libitum. Animals were transported daily to our laboratory for acclimation to the exercise and testing environment. All Animal Use protocols were approved by the Institutional Animal Care and Use Committee (IACUC) of University of Missouri-Kansas City (UMKC). Swimming Exercise Protocols Rodents were individually placed in 17-inch-long ⫻ 10inch-wide ⫻ 17-inch-high plastic containers filled with approximately 15 inches of water maintained at 37°C. A drop of soap was added to reduce surface tension; this reduced the frequency of “floating” behavior. In the rare instance of such behavior, animals were mildly stimulated to swim by nudging the nape with a pen. This ensured a full session of exercise conditioning. After each exercise session, animals were gently dried with a cloth towel. Control (nonexercised) rats and mice were allowed to swim for just 30 seconds each day and were then gently dried. Rat Studies We developed a swimming exercise training protocol in rats, as illustrated in Table 1. Our preliminary studies revealed that initial exercise sessions led to rapid fatigue, in agreement with previous studies showing that laboratory rats can continuously swim in warm water for approximately 60 minutes or less.10 Therefore, to produce an exercise training effect, we began with short 10minute bouts of exercise interspersed with several rest periods. Over the course of 7 days, the number of rest periods gradually decreased to 0, and the duration of Table 1. Graded Exercise Protocols DAY(S) EXERCISE DURATION (MIN) REST DURATION (MIN) SESSIONS* TOTAL EXERCISE DURATION (MIN) 1 2 3 4 5 6 7-9† 10-39‡§ 10 15 30 45 60, 30 75, 15 90 90 15 15 15 15 15 15 0 0 9 6 3 2 2 2 1 1 90 90 90 90 90 90 90 90 *Equivalent to the number of sessions performed (exercise plus rest component). †Formalin experiment animals swam for 9 days only; behavioral assessment was performed on day 10. ‡Hot plate experiment animals swam for a total 25 days; behavioral assessment was performed on day 14 (before nerve injury) and at 11 days after nerve injury only. §Nerve injury animals swam for total 39 days; partial sciatic nerve ligation (PSNL) surgery was performed on day 14, and behavioral assessments were performed at baseline (day 14 [before PSNL surgery]), on day 21 (7 days after injury), day 25 (11 days after injury), day 32 (18 days after injury), and 39 (25 days after injury). each swimming session was increased to 90 minutes. For the formalin studies of Fig 1, rats were randomly assigned to a control (n ⫽ 8) or treatment group involving 9 days of swimming (n ⫽ 8), followed 1 day later with formalin testing. For the partial sciatic nerve ligation (PSNL) studies (Fig 2), rats were randomly assigned to a control or exercise group. Rats in the exercise group swam up to 90 min/d for 13 days (Table 1). On day 14, which we term “baseline,” we evaluated behavioral signs of reflex responses to cold or heat stimuli (see “Cold Allodynia” and “Heat Hyperalgesia,” below). Immediately afterward, PSNL surgery was performed. Every day thereafter, the treatment group swam 90 min/d. Cold allodynia and heat hyperalgesia testing was repeated on day 21 (7 days after PSNL), day 25, day 32, and day 39. For the hotplate studies of Fig 3, rats were tested on day 25 (11 days after PSNL). Mouse Studies For the PSNL studies (Fig 4), 20 mice were randomized into a control (n ⫽ 10) or an exercise (n ⫽ 10) group. Mice in the exercise group swam 30 minutes per day for 5 days. On day 6, mice were tested for behavioral responses to heat and then underwent PSNL surgery. Every day thereafter for 6 days, the treatment group swam 30 minutes. The next day (7 days after PSNL), thermal hyperalgesia was assessed. For the control studies (Fig 5), 13 mice were randomized into groups that either underwent brief handling but did not swim (control; n ⫽ 4), swam once for 30 minutes in 37° water (n ⫽ 5), or swam once for 30 minutes in 20° water (n ⫽ 4). Latency to paw withdrawal from radiant heat was assessed before and 18 hours after treatment. ORIGINAL REPORT/Kuphal et al 991 Days 18 and 32 represent 2½ and 4½ weeks after injury. The latter is essentially identical to a key study in the literature by Hutchinson et al,24 who evaluated behavior 31 days after spinal cord injury. Each exercise training session was conducted in the afternoon. Behavioral testing sessions occurred in the morning, thus providing an 18-hour rest period. This time interval minimized the potentially confounding factor of stress-induced antinociception (SIA), which occurs on the order of minutes, not hours.42 Formalin Test Rats were placed in plexiglas containers (15 inches cubed) in a small, quiet room. After 1 hour of habituation, a syringe and 30 gauge needle were used to inject fresh formalin (5% of 37% formaldehyde diluted in saline; 50 L) into the plantar subcutaneous space at the center of the tori of the right hind paw. As previously described,46,48 the number of flinches and time spent licking the injected paw during the second, third, fourth, and fifth minutes after injection were evaluated during phase 1 (time points 1–5). After phase 1, flinches and time spent licking were counted in 2-minute intervals. With this method, behavior in 2 animals was simultaneously recorded by one observer for 70 minutes after the formalin injection. Cold Allodynia Figure 1. Exercise reduces persistent pain in the formalin test. Compared with the formalin-treated group that did not exercise (control), the formalin-treated group that did exercise (exercise) exhibited significantly less licking (A) and flinching behavior (B). Error bars ⫽ SEM. 夝P ⬍ .05 exercise vs control on the ipsilateral side, post hoc Bonferroni subsequent to repeatedmeasures ANOVA. Nerve Injury Surgery Rats and mice were anesthetized with a combination of ketamine (64 mg·kg⫺1, i.p.; Fort Dodge Laboratories, Fort Dodge, IA) and xylazine (5.3 mg·kg⫺1; i.p.) for PSNL. As previously described,43 an incision was made at the skin overlying the lateral femur, exposing the sciatic nerve. The nerve was dissected from surrounding connective tissue near the trocanter, just distal to the branching point of the posterior biceps semitendinosus nerve. A tight ligature was tied around one-third to onehalf the diameter of the nerve with 8-0 (rat) or 9-0 (mouse) silk suture. After ligation, the muscle was loosely sutured in layers with absorbable 4-0 and the skin was closed with 3-0 suture. Sham surgery was produced by skin incision and exposure of the sciatic distal trifurcation without ligation. After surgery, animals were housed individually to prevent damage to the sutures from cagemates. Behavioral Testing We chose to evaluate behavior at the following time points after nerve injury: 1, 1½, 2½, 3½, and 4½ weeks. Rats were acclimated for 1 hour within an inverted plexiglas box on top of an elevated one-quarter inch stainless steel mesh floor. Using a syringe connected to PE-90 tubing, flared at the tip to a diameter of 3.5 mm, a drop of acetone was applied to the plantar surface of the paw. Surface tension maintained the volume of the drop to 10 to 12 L. The length of time the animal lifted or shook its paw was recorded. The duration of paw withdrawal was recorded up to 30 seconds and 3 observations, with an interstimulus interval of 10 minutes, were averaged for subsequent analyses. Thermal Hyperalgesia (Radiant Heat) Rats or mice were acclimated for 2 hours within inverted transparent enclosures, 1 day before testing. These cages rested on a thermal paw stimulator system,11 modified from the original design.19 This device consisted of a glass surface maintained at a constant temperature of 25.0oC; underneath the glass lies a radiant heat source. An attached, angled mirror facilitated visualization of the footpad and positioning of the radiant heat. On the day of testing, animals were acclimated for an additional hour on the glass floor. Next, the radiant light was activated and paw withdrawal latency (PWL) was obtained from each hind paw (with a minimum of 2 minutes between each test). Voltage intensity was adjusted such that (pre-injury) baseline latency was 12.5 ⫾ 0.5 seconds. The first 3 measurements were discarded (they tend to be unusually high and variable), and the 5 subsequent measurements were averaged for subsequent analysis and presentation. If the animal did not 992 Extended Swimming Exercise Reduces Inflammatory and Peripheral Neuropathic Pain Figure 2. Exercise reduces nerve injury-induced cold allodynia and thermal hyperalgesia in rats. Exercise reduced cold allodynia (A and B) and heat hyperalgesia (C and D) in animals with partial sciatic nerve ligation (PSNL). Line graphs in A and C illustrate time course data. Histograms in B and D summarize data averaged across days 7 to 25 at either the ipsilateral or contralateral sides. There were no significant differences at the contralateral paw. Data are presented as mean ⫾ SEM. 夝P ⬍ .05, repeated-measures ANOVA followed by post hoc Bonferroni. n ⫽ 6 to 8. respond within 20 seconds, the heat was discontinued to prevent damage to the paw. imum of 10 minutes between each, was averaged for subsequent analysis. Thermal Hyperalgesia (Hot Plate) Data Analysis Rats were gently placed on a 52°C hot plate (Columbus Instruments, Columbus, OH). Rats were removed when they either licked the hind paw of the injured side, jumped, or a 20-sec cutoff had been reached. Latency was recorded and the average of 3 sessions, with a min- Differences between means were analyzed by 2-way repeated-measures ANOVA. Exercise treatment was the between-subjects factor and time was the repeated measure. For the formalin studies, all data were analyzed with a global ANOVA. Next, the data were binned into phase I (time points 1–5) and phase II (time points 20 Figure 3. Exercise reduces nerve injury–induced thermal hyper- Figure 4. Exercise decreases nerve injury-induced thermal hyperalgesia in mice. Latency to heat was assessed both before (Pre) and 1 week after (Post) partial sciatic nerve ligation. Neither PSNL nor exercise altered latency at the contralateral paw. Data are presented as mean ⫾ SEM. n ⫽ 10. algesia in the hotplate test. Partial sciatic nerve ligation (PSNL) reduced paw withdrawal latency to heat in control rats but not in exercised rats. Data are presented as mean ⫾ SEM. 夝P ⬍ .05 vs PSNL-exercise group. n ⫽ 7 to 9. ORIGINAL REPORT/Kuphal et al 993 To confirm exercise-induced reversal of heat hyperalgesia, we used the hotplate test as a second measure of thermal latency in sham and nerve-injured rats. Fig 3 illustrates that in control (no swim) rats, nerve injury decreased hotplate latency from 13.7 ⫾ 1.1 to 11.0 ⫾ 1.1 seconds. This heat hypersensitivity was not observed in the exercise group (control-PSNL vs exercise-PSNL: 11.0 ⫾ 1.1 vs 13.6 ⫾ 0.9 seconds, P ⫽ .049). Nerve Injury Studies in the Mouse Figure 5. Swimming in 37° water does not increase paw withdrawal latency (PWL) in uninjured mice. PWL was assessed both before and 18 hours after swimming in warm water (37°) or after a brief dip in water (controls). Data are presented as mean ⫾ SEM. n ⫽ 4 to 5. through 60) and then further analyzed by ANOVA. If significant (P ⬍ .05), the analyses were followed by post hoc t tests with Bonferroni correction to evaluate group differences at specific time points. Data are presented as mean ⫾ SEM. Results Inflammatory Pain To test the hypothesis that extended exercise reduces acute inflammatory pain, we evaluated formalininduced behavioral responses after 90 minutes ⫻ 9 days of swimming. As illustrated in Fig 1, the control group displayed the expected biphasic formalin response profile: An early phase 1 of flinching and licking responses during the first 5 minutes after formalin injection, followed by a quiescent interphase, and then a later phase 2 response during time points 20 to 60. Exercise did not change licking (F1,68 ⫽ 0.7) or flinching (F1,68 ⫽ 1.0) behavior during phase 1. We did find during phase 2, compared with control, that exercise decreased the magnitude of both licking (15.9 ⫾ 1.4 vs 8.4 ⫾ 1.7, F1,153 ⫽ 33, P ⬍ .0001) and flinching (8.9 ⫾ 1.7 vs 5.4 ⫾ 0.7, F1,153 ⫽ 23, P ⬍ .0001). Nerve Injury Studies in the Rat To test the hypothesis that extended exercise reduces peripheral neuropathic pain, we evaluated the effect of swimming on paw withdrawal responses to cold and hot stimuli after PSNL. As illustrated in Fig 2, A and B, PSNL increased cold responses at the ipsilateral hind paw. This resolved more quickly in the exercise group from days 10 to 25 (F1,35 ⫽ 6.5, P ⫽ .015), and post hoc analysis revealed significant differences between control and exercise groups on day 18 and day 25 after nerve injury (P ⬍ .05). As illustrated in Fig 2, C and D, PSNL reduced thermal latency at the ipsilateral paw. This sign of heat hyperalgesia was reduced in the exercise group from days 7 to 25 (F1,47 ⫽ 6.8, P ⫽ .012). Exercise had no effect on the contralateral paw. To extend our findings in the rat to a second species, we evaluated the effects of swimming exercise on injuryinduced thermal hyperalgesia in mice. Fig 4 illustrates that exercise decreased hyperalgesia at the ipsilateral side (F1,36 ⫽ 23, P ⬍ .0001), without altering heat latency at the contralateral side (P ⬎ .05). On the ipsilateral side, the decrease in PWL in the exercise group was significantly less than the control group (8.5 ⫾ 0.8 vs 10.4 ⫾ 0.6, P ⫽ .044). Control Studies in the Absence of Injury Our swimming protocol is forced and therefore inherently stressful. Because a single stress event can alter nociceptive thresholds,51 we next asked whether one bout of swimming alters heat withdrawal latency in the absence of injury. As illustrated in Fig 5, we evaluated latency both before and 18 hours after swimming in warm water (37°). Swimming did not change thermal PWL, arguing against an effect of swimming or swim stress on nociceptive thresholds. Discussion Our studies are the first to report the effects of longterm exercise in the formalin model of ongoing inflammatory pain13 and the partial sciatic nerve injury model of peripheral neuropathic pain.43 We found that longterm swimming exercise decreased formalin-induced and nerve injury–induced behavioral signs of persistent pain. Our data support the hypothesis that long-term exercise reduces acute and chronic pain. Exercise Reduces Inflammatory Pain Carmody and Cooper5 suggested that short-term cold swim exercise reduces formalin-induced nociception in the mouse. We extend these findings to more clinically relevant swim times (9 consecutive days of 90 min/d swimming), to warm water swim protocols that avoid SIA,51 and to a second species, the rat. On the other hand, our results contrast with Quintero et al,39 who reported three, 10- to 20-minute, forced swim sessions in cool (24 to 26°) water increased formalin nociception, particularly during the interphase. They termed this stress-induced hyperalgesia, or SIH. At least 3 differences in protocol can explain such opposite results. First, the intensity of SIH may inversely correlate with water temperature. Thus, swimming in cooler water may facilitate SIH, whereas swimming in warmer water facilitates exercise-induced antinociception. Second, the mechanisms underlying SIH may develop during the first 20 minutes 994 Extended Swimming Exercise Reduces Inflammatory and Peripheral Neuropathic Pain might subside during our 90-minute swimming protocol. Third, the severe stress during our initial swim sessions might induce SIH; we speculate that these would dissipate as the animal habituates. Indeed, we observed a dramatic decline in feces in the water over the first few swim sessions. The intraplantar injection of dilute formalin directly stimulates nociceptors, resulting in a barrage of primary afferent fiber activity that lasts about 5 minutes (phase 1). Our results indicate that exercise does not reduce this. Instead, exercise reduced phase 2. Overwhelming evidence with peripherally acting local anesthetics, neonatal capsaicin treatment, and isolated peripheral nerve recordings demonstrate that ongoing C-fiber activity, rather than central sensitization, predominantly drives nociceptive responses during phase 2 in the formalin test.34,37,38,47-49 This ongoing activity is probably driven by multiple factors, including (1) direct stimulation of peripheral afferent terminals by formalin; and (2) formalin-evoked neurogenic and non-neurogenic release of inflammatory mediators and other chemicals that produce peripheral sensitization. We do not believe that exercise reduced the former factor, because exercise did not reduce phase 1. Instead, we favor the hypothesis that long-term exercise prevents peripheral sensitization in the setting of acute inflammatory pain. Exercise Reduces Neuropathic Pain Our studies are among the first to demonstrate that extended exercise reduces behavioral signs of peripheral neuropathic pain. We found that 18 to 25 days of swimming after PSNL decreased nerve injury–induced cold allodynia and thermal hyperalgesia in rats, and 7 days of swimming decreased nerve injury–induced thermal hyperalgesia in mice. In contrast to the prophylactic effect of exercise on formalin-induced nociception, 7 days of exercise before PNSL did not prevent the development of neuropathic pain. One possibility is that SIH operates during the earlier time points, as Quintero et al39 found that 3 days of swimming in cool water decreased paw withdrawal latency to heat. Alternatively, exercise may recruit inhibitory mechanism involved in the maintenance, but not the induction, of neuropathic pain. We can only speculate that this mechanism involves the rostral ventral medulla (RVM). For example, Porreca et al found that microinjection of lidocaine into the RVM blocked the maintenance but not the induction of neuropathic pain.3,54 Whether the RVM serves as a target for the anti-allodynic actions of exercise remains an interesting question. We conclude that exercise recruits different mechanisms to inhibit acute inflammatory vs neuropathic pain. Certain features of our experimental design and results are quite similar to those of Hutchinson et al,24 who reported that both treadmill running and swimming exercise reduced mechanical allodynia in a model of central neuropathic pain involving spinal cord injury (SCI). For example, the exercise parameters (20 minutes per day, 5 days per week for 7 weeks) were quite similar to our study. Also, the time from initiation of exercise to the appearance of reduced allodynia was 31 to 32 days in both studies. They reported that swim training reduced allodynia 5 to 6 weeks after injury; this anti-allodynic effect was over by 7 weeks. We also observed a transient effect on our measure of heat hypersensitivity; we found that exercise reduced hyperalgesia until at least 18 days after PSNL, and this effect was over by 25 days. It is important to note that unlike Hutchinson et al, our study did not evaluate mechanical allodynia. Because mechanical allodynia and hyperalgesia are significant clinical problems in chronic pain patients,58 further studies are needed. Mechanisms of Exercise-Induced Analgesia Bement and Sluka2 recently reported that low-intensity treadmill exercise (treadmill speed ⫽ 3.05 m/min for 30 min/d) for 5 consecutive days reduced the chronic bilateral mechanical hyperalgesia in a rat model of noninflammatory chronic muscle pain involving 2 injections of acid (pH ⫽ 4.0) into the gastrocnemius muscle. Treadmill exercise-induced reductions in mechanical hyperalgesia were reversed by systemic administration of the opioid receptor antagonist naloxone. These results suggest that endogenous opioids mediate, in part, an inverse relationship between exercise and chronic muscle pain. Indeed, as reviewed by Koltyn et al,30 exercised-induced increases in circulating levels of endogenous opioids may feedback/inhibit acute pain at peripheral, spinal, or supraspinal sites.5,7,8,12,26,45,52 Further studies are needed to determine whether a similar relationship holds true between exercise and chronic neuropathic pain. Swimming (particularly in cold water) produces the well-known phenomenon of SIA, which is mediated by both opioid and nonopioid mechanisms,51 the latter of which include corticosteroid or endocannabinoid mediators.23 It is unlikely, however, that such stress-induced mechanisms operate in our experimental model, because we observed long-lasting reduction of inflammatory and neuropathic pain (eg, after 18 hours of rest, after exercise). Any more subtle effect, not detectable in our model, would have likely habituated across the repeated swimming sessions. We conclude that long-term exercise rather than SIA reduces the development of a neuropathic pain state in rodents. Exercise Does Not Produce Extended Antinociception in a Model of Transient Pain At the uninjured, contralateral paw, we found that exercise changed neither PWL to radiant heat or to the hotplate when measured 18 hours after the final exercise session. These results suggest that swimming exercise does not produce extended changes in acute nociception. Although Tierney et al52 reported that swimming produced antinociception in the tail-flick test in mice ORIGINAL REPORT/Kuphal et al 45 and Shyu et al reported that 4 weeks of wheelrunning produced antinociception evidenced by increased squeak thresholds (from controlled electrical stimuli of varying intensity) in rats, both studies measured nociception soon after exercise (12 and 60 minutes, respectively), and in the latter study nociception steadily returned to baseline. In agreement with our results, numerous studies in healthy humans demonstrate that exercise produces short-lasting analgesic effects. For example, activities such as running,21,25,41 cycling,28 stair-stepping,18 resistance training,29 and mixed resistance training and aerobic exercise1 increased pain threshold or reduced sensitivity to a variety of noxious stimuli, including cold25 and pressure.1,18,21,28,29 Our results emphasize that the effects of exercise on acute nociception are likely to be short-lasting, with nociception returning to baseline within 18 hr of rest. Clinical Implications Aquatic exercise is commonly prescribed to patients who must avoid weight-bearing activities such as walking or running. This includes patients with complex regional pain syndrome (CRPS), who often experience hypersensitivity of the feet. Our studies provide important initial results with a rodent swimming exercise paradigm. We must keep in mind, however, that swimming exercise in rodents is forced, whereas aquatic exercise in humans is voluntary. Further studies incorporating voluntary exercise paradigms (eg, voluntary wheel-running), will be useful in translating rodent data to therapies for chronic pain patients. References 1. Bartholomew JB, Lewis BP, Linder DE, Cook DB: Post-exercise analgesia: replication and extension. J Sports Sci 14: 329-334, 1996 2. Bement MK, Sluka KA: Low-intensity exercise reverses chronic muscle pain in the rat in a naloxone-dependent manner. Arch Phys Med Rehabil 86:1736-1740, 2005 3. Burgess SE, Gardell LR, Ossipov MH, Malan TP Jr, Vanderah TW, Lai J, Porreca F: Time-dependent descending facilitation from the rostral ventromedial medulla maintains, but does not initiate, neuropathic pain. J Neurosci 22:51295136, 2002 995 Our results support the idea that long-term exercise, in addition to its well-known benefits to general health,9 can be an effective strategy for the management of clinical inflammatory or neuropathic pain.15,35 A limited number of clinical studies indicate that moderate exercise decreases pain ratings in humans with established musculoskeletal disease14 or fibromyalgia.16,17,32,33 Exercise also enhances outcome in chronic pain patients with lower back pain,22,35,53 osteoporosis,31 and other chronic pain conditions that may have a neuropathic component.9,15 Still, several factors should be considered when prescribing exercise for chronic pain patients. First, Butler et al4 reported that swimming exercise exacerbated hyperalgesia in rats during the early stages of arthritis. This raises the important point that exercise therapy perhaps should be reserved for patients with established chronic pain, after acute inflammation has stabilized.44 Second, strenuous exercise can increase experimentally induced pain in individuals with fibromyalgia,55 demonstrating the importance of intensity as it relates to exercise prescription. Future animal and human studies are clearly warranted to determine the biological mechanisms that integrate exercise and pain, and future clinical studies are needed to determine the importance of timing and intensity of exercise in terms of injury onset and therapeutic effectiveness for chronic pain. Acknowledgments We thank Melissa Mena Vu, MD, for her assistance with the rat nerve injury studies. 7. Cooper K, Carmody J: The characteristics of the opioidrelated analgesia induced by the stress of swimming in the mouse. Neurosci Lett 31:165-170, 1982 8. D’Anci KE, Gerstein AV, Kanarek RB: Long-term voluntary access to running wheels decreases kappa-opioid antinociception. Pharmacol Biochem Behav 66:343-346, 2000 9. Davis VP, Fillingim RB, Doleys DM, Davis MP: Assessment of aerobic power in chronic pain patients before and after a multi-disciplinary treatment program. Arch Phys Med Rehabil 73:726-729, 1992 10. Dawson CA, Horvath SM: Swimming in small laboratory animals. Med Sci Sports 2:51-78, 1970 4. Butler SH, Godefroy F, Besson JM, Weil-Fugazza J: Increase in “pain sensitivity” induced by exercise applied during the onset of arthritis in a model of monoarthritis in the rat. Int J Tissue React 13:299-303, 1991 11. Dirig DM, Salami A, Rathbun ML, Ozaki GT, Yaksh TL: Characterization of variables defining hindpaw withdrawal latency evoked by radiant thermal stimuli. J Neurosci Methods 76:183-191, 1997 5. Carmody J, Cooper K: Swim stress reduces chronic pain in mice through an opioid mechanism. Neurosci Lett 74:358363, 1987 12. Droste C, Greenlee MW, Schreck M, Roskamm H: Experimental pain thresholds and plasma beta-endorphin levels during exercise. Med Sci Sports Exerc 23:334-342, 1991 6. Chatzitheodorou D, Kabitsis C, Malliou P, Mougios V: A pilot study of the effects of high-intensity aerobic exercise versus passive interventions on pain, disability, psychological strain, and serum cortisol concentrations in people with chronic low back pain. Phys Ther 87:304-312, 2007 13. Dubuisson D, Dennis SG: The formalin test: a quantitative study of the analgesic effects of morphine, meperidine, and brain stem stimulation in rats and cats. Pain 4:161-174, 1977 996 Extended Swimming Exercise Reduces Inflammatory and Peripheral Neuropathic Pain 14. Ferrell BA, Josephson KR, Pollan AM, Loy S, Ferrell BR: A randomized trial of walking versus physical methods for chronic pain management. Aging (Milano) 9:99-105, 1997 32. Mannerkorpi K, Ahlmen M, Ekdahl C: Six- and 24-month follow-up of pool exercise therapy and education for patients with fibromyalgia. Scand J Rheumatol 31:306-310, 2002 15. Fordyce W, McMahon R, Rainwater G, Jackins S, Questad K, Murphy T, De Lateur B: Pain complaint– exercise performance relationship in chronic pain. Pain 10:311-321, 1981 33. McCain GA, Bell DA, Mai FM, Halliday PD: A controlled study of the effects of a supervised cardiovascular fitness training program on the manifestations of primary fibromyalgia. Arthritis Rheum 31:1135-1141, 1988 16. Gowans SE, deHueck A: Effectiveness of exercise in management of fibromyalgia. Curr Opin Rheumatol 16:138-142, 2004 17. Gowans SE, Dehueck A, Voss S, Silaj A, Abbey SE: Sixmonth and one-year followup of 23 weeks of aerobic exercise for individuals with fibromyalgia. Arthritis Rheum 51: 890-898, 2004 18. Gurevich M, Kohn PM, Davis C: Exercise-induced analgesia and the role of reactivity in pain sensitivity. J Sports Sci 12:549-559, 1994 19. Hargreaves K, Dubner R, Brown F, Flores C, Joris J: A new and sensitive method for measuring thermal nociception in cutaneous hyperalgesia. Pain 32:77-88, 1988 20. Hayden JA, van Tulder MW, Malmivaara AV, Koes BW: Meta-analysis: Exercise therapy for nonspecific low back pain. Ann Intern Med 142:765-775, 2005 21. Hoffman MD, Shepanski MA, Ruble SB, Valic Z, Buckwalter JB, Clifford PS: Intensity and duration threshold for aerobic exercise-induced analgesia to pressure pain. Arch Phys Med Rehabil 85:1183-1187, 2004 22. Hoffman MD, Shepanski MA, Mackenzie SP, Clifford PS: Experimentally induced pain perception is acutely reduced by aerobic exercise in people with chronic low back pain. J Rehabil Res Dev 42:183-190, 2005 23. Hohmann AG, Suplita RL, Bolton NM, Neely MH, Fegley D, Mangieri R, Krey JF, Walker JM, Holmes PV, Crystal JD, Duranti A, Tontini A, Mor M, Tarzia G, Piomelli D: An endocannabinoid mechanism for stress-induced analgesia. Nature 435:1108-1112, 2005 24. Hutchinson KJ, Gomez-Pinilla F, Crowe MJ, Ying Z, Basso DM: Three exercise paradigms differentially improve sensory recovery after spinal cord contusion in rats. Brain 127: 1403-1414, 2004 25. Janal MN, Glusman M, Kuhl JP, Clark WC: Are runners stoical? An examination of pain sensitivity in habitual runners and normally active controls. Pain 58:109-116, 1994 26. Kanarek RB, Gerstein AV, Wildman RP, Mathes WF, D’Anci KE: Chronic running-wheel activity decreases sensitivity to morphine-induced analgesia in male and female rats. Pharmacol Biochem Behav 61:19-27, 1998 34. McCall WD, Tanner KD, Levine JD: Formalin induces biphasic activity in C-fibers in the rat. Neurosci Lett 208:45-48, 1996 35. Nielens H, Plaghki L: Perception of pain and exertion during exercise on a cycle ergometer in chronic pain patients. Clin J Pain 10:204-209, 1994 36. O’Connor PJ, Cook DB: Exercise and pain: The neurobiology, measurement, and laboratory study of pain in relation to exercise in humans. Exerc Sport Sci Rev 27:119-166, 1999 37. Peterson MA, Basbaum AI, Abbadie C, Rohde DS, McKay WR, Taylor BK: The differential contribution of capsaicinsensitive afferents to behavioral and cardiovascular measures of brief and persistent nociception and to Fos expression in the formalin test. Brain Res 755:9-16, 1997 38. Puig S, Rivot JP, Besson JM: Effect of subcutaneous administration of the chemical algogen formalin, on 5-HT metabolism in the nucleus raphe magnus and the medullary dorsal horn: A voltametric study in freely moving rats. Brain Res 590:250-254, 1992 39. Quintero L, Moreno M, Avila C, Arcaya J, Maixner W, Suarez-Roca H: Long-lasting delayed hyperalgesia after subchronic swim stress. Pharmacol Biochem Behav 67:449-458, 2000 40. Robb KA, Williams JE, Duvivier V, Newham DJ: A pain management program for chronic cancer-treatment-related pain: A preliminary study. J Pain 7:82-90, 2006 41. Ruble SB, Hoffman MD, Shepanski MA, Valic Z, Buckwalter JB, Clifford PS: Thermal pain perception after aerobic exercise. Arch Phys Med Rehabil 86:1019-1023, 2005 42. Schwarz L, Kindermann W: Changes in beta-endorphin levels in response to aerobic and anaerobic exercise. Sports Med 13:25-36, 1992 43. Seltzer Z, Dubner R, Shir Y: A novel behavioral model of neuropathic pain disorders produced in rats by partial sciatic nerve injury. Pain 43:205-218, 1990 44. Semble EL, Loeser RF, Wise CM: Therapeutic exercise for rheumatoid arthritis and osteoarthritis. Semin Arthritis Rheum 20:32-40, 1990 27. Kemppainen P, Hamalainen O, Kononen M: Different effects of physical exercise on cold pain sensitivity in fighter pilots with and without the history of acute in-flight neck pain attacks. Med Sci Sports Exerc 30:577-582, 1998 45. Shyu BC, Andersson SA, Thoren P: Endorphin mediated increase in pain threshold induced by long-lasting exercise in rats. Life Sci 30:833-840, 1982 28. Koltyn KF, Garvin AW, Gardiner RL, Nelson TF: Perception of pain following aerobic exercise. Med Sci Sports Exerc 28:1418-1421, 1996 46. Taylor BK, Peterson MA, Basbaum AI: Exaggerated cardiovascular and behavioral nociceptive responses to subcutaneous formalin in the spontaneously hypertensive rat. Neurosci Lett 201:9-12, 1995 29. Koltyn KF, Arbogast RW: Perception of pain after resistance exercise. Br J Sports Med 32:20-24, 1998 30. Koltyn KF: Analgesia following exercise: A review. Sports Med 29:85-98, 2000 47. Taylor BK, Peterson MA, Basbaum AI: Persistent cardiovascular and behavioral nociceptive responses to subcutaneous formalin require peripheral nerve input. J Neurosci 15: 7575-7584, 1995 31. Malmros B, Mortensen L, Jensen MB, Charles P: Positive effects of physiotherapy on chronic pain and performance in osteoporosis. Osteoporos Int 8:215-221, 1998 48. Taylor BK, Peterson MA, Basbaum AI: Early nociceptive events influence the temporal profile, but not the magnitude, of the tonic response to subcutaneous formalin: Ef- ORIGINAL REPORT/Kuphal et al fects with remifentanil. J Pharmacol Exp Ther 280:876-883, 1997 49. Taylor BK, Basbaum AI: Early antinociception delays edema but does not reduce the magnitude of persistent pain in the formalin test. J Pain 1:218-228, 2000 50. Taylor BK: Pathophysiologic mechanisms of neuropathic pain. Curr Pain Headache Rep 5:151-161, 2001 51. Terman GW, Morgan MJ, Liebeskind JC: Opioid and non-opioid stress analgesia from cold water swim: Importance of stress severity. Brain Res 372:167-171, 1986 52. Tierney G, Carmody J, Jamieson D: Stress analgesia: the opioid analgesia of long swims suppresses the non-opioid analgesia induced by short swims in mice. Pain 46:89-95, 1991 53. van Tulder MW, Koes BW, Bouter LM: Conservative treatment of acute and chronic nonspecific low back pain: A systematic review of randomized controlled trials of the most common interventions. Spine 22:2128-2156, 1997 997 54. Vera-Portocarrero LP, Zhang ET, Ossipov MH, Xie JY, King T, Lai J, Porreca F: Descending facilitation from the rostral ventromedial medulla maintains nerve injuryinduced central sensitization. Neuroscience 140:1311-1320, 2006 55. Vierck CJ Jr, Staud R, Price DD, Cannon RL, Mauderli AP, Martin AD: The effect of maximal exercise on temporal summation of second pain (windup) in patients with fibromyalgia syndrome. J Pain 2:334-344, 2001 56. Wall PD, Melzack R, eds: Textbook of Pain. New York, NY, Churchill Livingstone, 1999 57. Whiteside A, Hansen S, Chaudhuri A: Exercise lowers pain threshold in chronic fatigue syndrome. Pain 109:497499, 2004 58. Woolf CJ, Mannion RJ: Neuropathic pain: aetiology, symptoms, mechanisms, and management. Lancet 353:19591964, 1999 59. Wright A, Sluka KA: Nonpharmacological treatments for musculoskeletal pain. Clin J Pain 17:33-46, 2001









© Copyright 2026