
J Soler-Soler, J Sagristá-Sauleda, A Cabrera, J Sauleda-Parés, J Iglesias-Berengué,... Permanyer-Miralda and J Roca-Llop
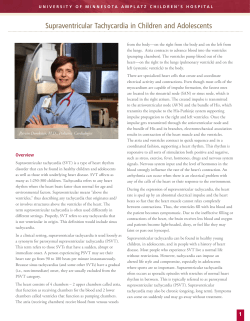
Effect of verapamil in infants with paroxysmal supraventricular tachycardia. J Soler-Soler, J Sagristá-Sauleda, A Cabrera, J Sauleda-Parés, J Iglesias-Berengué, G Permanyer-Miralda and J Roca-Llop Circulation. 1979;59:876-879 doi: 10.1161/01.CIR.59.5.876 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1979 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/59/5/876 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/ Downloaded from http://circ.ahajournals.org/ by guest on August 22, 2014 Effect of Verapamil in Infants with Paroxysmal Supraventricular Tachycardia J. SOLER-SOLER, M.D., J. SAGRISTA-SAULEDA, M.D., ALBERTO CABRERA, M.D., J. SAULEDA-PARES, M.D., J. IGLESIAS-BERENGUE, M.D., G. PERMANYER-MIRALDA, M.D., AND J. ROCA-LLOP, M.D. SUMMARY Twenty-nine consecutive spontaneous attacks of paroxysmal supraventricular tachycardia (PSVT) in 14 infants (mean age 4.4 months) were treated with verapamil. No infant had associated heart disease. Verapamil 1-2 mg i.v. was administered over 30 seconds. The dosage varied according to the weight of the infant. Within 60 seconds sinus rhythm was obtained in 28 instances (96.5%). No significant complications were observed. The high effectiveness, rapid action and lack of undesirable side effects observed in this series suggest that verapamil is the drug of choice in the treatment of PSVT in infants without underlying heart disease. VERAPAMIL is considered by many authors1-7 to be the drug of choice in the treatment of paroxysmal supraventricular tachycardia (PSVT) in adults. It has been particularly effective in reciprocating junctional tachycardias with6' 8 or without6 8 an associated extranodal pathway. The rapid action of verapamil and its quick elimination contribute to its clinical usefulness. This antiarrhythmic drug must be used with caution in patients with acute myocardial infarction,9 sick sinus syndrome'0 and obstructive bronchopulmonary disease.8' 11 Verapamil is contraindicated in patients with high-degree atrioventricular (AV) block'2 and in patients receiving A-blocking agents;4 it is probably contraindicated as well in patients with severe primary heart failure.5' 13, 14 Digitalis is considered the drug of choice in the treatment of PSVT in infants.'5 -1 However, as Lubbers et al.20 have stated, "the value of newer antiarrhythmic drugs remains to be fully evaluated" in this age group. Bein et al.22' 23 reported excellent results with verapamil in the treatment of PSVT in infants and children. The present paper reports our results with verapamil in the treatment of PSVT in infants. atrial echoes were observed after termination of tachycardia. Underlying heart disease could not be demonstrated in any infant by noninvasive methods. Only two infants had an acute intercurrent illness (pneumonia). Before the administration of verapamil, we attempted to terminate tachycardia in all cases with vagal maneuvers or with a precordial blow. Attacks had begun 15 minutes to 2 days (possibly 5 days in one case) before verapamil was administered. In 18 attacks congestive heart failure was present; in five of them it was severe (pulmonary edema and/or physical signs of shock). In two patients 0.03 mg/kg digoxin i.v. had been administered 3 hours and 5 hours previously. Another patient had received procainamide 1 hour before receiving verapamil. Verapamil was given intravenously over 30 seconds, at a dosage of 1 mg in infants weighing < 5 kg, 1.5 mg in infants weighing 5-10 kg, and 2 mg in infants weighing > 10 kg. The dosage schedule was derived from that used in adults, according to the equivalent table of Talbot et al.24 This dosage schedule was successful in our first series of treated infants.25 In one case we administered an additional 0.5 mg because the usual dose failed (1 mg in an infant weighing 4.5 kg); in another case a higher dose (2 mg in a 5.6 kg infant) was required for the same reason; and in a third infant, a dose three times greater than scheduled (4.5 mg in a 5.8 kg infant) was inadvertently administered. In all cases administration of verapamil was carried out under continuous electrocardiographic monitoring. Materials and Methods We treated 29 consecutive, spontaneous attacks of PSVT in 14 infants ages 5 days to 18 months (mean age 4.4 months) with verapamil. All attacks corresponded to supraventricular tachycardia (regular tachycardia with narrow QRS in a 12-lead ECG) of the paroxysmal type. Heart rate ranged from 214-330 beats/min. In seven infants (13 attacks) the ECG between attacks showed a Wolff-Parkinson-White syndrome, and in two other infants (three attacks) Results Stable sinus rhythm was obtained in 28 of 29 treated attacks. The only failure occurred in an infant in whom a higher-than-usual dose (2 mg in a 5.6 kg infant) did not abolish the tachycardia. This attack was terminated with a precordial blow, the same maneuver that was repeatedly ineffective before administration of verapamil. All attacks ceased immediately or within 60 seconds after administration of the drug. The heart rate usually slowed before the tachycardia stopped. In four instances there were atrial echoes or From the Servicio de Cardiologia y Hospital Infantil, Ciudad Sanitaria Seguridad Social, Paseo Valle de Hebr6n, Barcelona, and the Hospital Infantil de Cruces, Bilbao, Spain. Address for reprints: Dr. J. Soler-Soler, Departamento de Medicina, Servicio de Cardiologia, Ciudad Sanitaria de la Seguridad Social, Paseo Valle de Hebr6n, s/n, Barcelona (35), Spain. Received May 10, 1978; revision accepted December 8, 1978. Circulation 59, No. 5, 1979. 876 Downloaded from http://circ.ahajournals.org/ by guest on August 22, 2014 VERAPAMIL IN INFANTS WITH PSVT/Soler-Soler et al. 877 A.L.F. 2M 1MGR D ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ FIGURE 1. A) Control tracing of a paroxysmal supraventricular tachycardia (PSVT) in a 2-month-old infant with a heart rate oF315 beats/mmi B) PSVTstops 48 seconds after the administration of 1 mg of verapamil. Three sinus beats are followed by severe depression of sinus automaticity and atrioventricular (A V) junctional escape rhythm at a frequency of 68-75 beats/min. C) A run of sinus beats interrulpts a more rapid A V junctional escape rhythm. This tracing was obtained 13 seconds after strip B. D) Stable sinus rhythm registered 17 seconds after strip C. short, self-limited runs of paroxysmal tachycardia. We observed transient depression of sinus automaticity (fig. 1) requiring no treatment in the only infant who had received procainamide 1 hour before. When present, heart failure disappeared a few hours after termination of tachycardia. The only complication (severe hypotension with shock) was seen in the infant who inadvertently received a dose three times greater than recommended. This complication was successfully treated with isoproterenol. Discussion PSVT in infants is often a cardiac emergency. In this age group, correct diagnosis is often delayed because the initial symptoms (pallor, feeding troubles, vomiting) are vague. The degree of heart failure depends on the duration of the attack, on the heart rate and on any associated cardiac anomaly. Although prognosis is usually good,'6' 20, 25 isolated fatal cases have been reported.26'2,27 In some series 16,282 mortality iis 2-11%, and death is related to heart failure or to complications of therapy. Digitalis, considered to be the first-choice drug in the treatment of PSVT in infants,'5-21 abolishes more than 90% of attacks. Usually, sinus rhythm is obtained within 10 hours.16 This delay is distressingly long in patients who do not tolerate PSVT, which may require the administration of other antiarrhythmic drugs, with unpredictable combined effects. Verapamil involves neither blockade of the ,Badrenoreceptors of the heart nor quinidine-like activity. Vaughan Williams29 considers verapamil to be a new, fourth type of antiarrhythmic drug. Specifically, verapamil blocks the slow calcium inward channel,30 but does not significantly modify the transmembrane sodium influx through the fast inward channel.3' The sinus node and the AV node are particularly sensitive to verapamil because normal impulse formation in the sinus node and conduction in the AV node appear to be maintained by slow channel-dependent mechanisms. The effect exerted by verapamil on AV conduction may explain its effectiveness in treating tachyarrhythmias.33 3 Our results with verapamil are dramatic: Within 60 seconds sinus rhythm was obtained in 28 of 29 instances (96.5%). The only refractory attack was observed in a patient in whom verapamil had been successful in two previous episodes of tachycardia during his first admission. Interestingly, this refractory tachycardia was abolished with a precordial blow shortly after administration of verapamil. As this maneuver had been unsuccessful before verapamil we assume the the drug had some influence in the interruption of the tachycardia. Our results are similar to those reported by Bein et al.,22 who obtained sinus rhythm in all the 70 attacks of PSVT in patients aged 4 days to 14 years. Since some PSVTs are short-lived, the purist may argue that the termination of tachycardia is not always related to verapamil, but may be a spontaneous event. However, the very short interval between administration of the drug and termination of the tachycardia observed in this and other series3 5 6, 22 strongly suggests that termination of tachycardia is due to the action of verapamil. The following points should be emphasized: Quick Action of Verapamil All attacks but one ceased immediately after the administration of verapamil or within 60 seconds. We stress that after 3-5 minutes of its administration, verapamil cannot be assumed to have stopped the tachycardia.5 In case of failure of the drug, another therapeutic approach can be safely undertaken after this interval. Downloaded from http://circ.ahajournals.org/ by guest on August 22, 2014 878 CIRCULATION Stable Sinus Rhythm The arrhythmia relapsed within 24 hours after its termination in only two infants. This frequency is similar to that reported with digitalis.16 18, 20 Verapamil and Heart Failure In spite of the negative inotropic effect of verapamil,'2' 13, 35 the signs of heart failure quickly subsided after termination of tachycardia. In our series heart failure was secondary to PSVT, and no infant had underlying heart disease. In the series of Bein et al,22 two infants with severe congenital heart disease developed PSVT during heart catheterization; in both cases verapamil administration was followed by complete AV block with spontaneous return to sinus rhythm. Apitz et al.36 reported a fatal case after administration of verapamil in a 9-year-old child with primary cardiomyopathy and chronic heart failure. Singh et al.35 studied the effects of verapamil on hemodynamics in patients with heart failure and conclude that "the intrinsic negative inotropic action of verapamil is minimized by its effects on afterload so that cardiac index is not reduced by the drug in patients with cardiac disease." However, in their series no patient was in functional class IV and all had basal left ventricular end-diastolic pressure < 20 mm Hg and ejection fraction > 40%. These authors were probably aware that their patients represented a selected heart disease population because at the end of the paper, in spite of the above-mentioned conclusions, they state: "caution should nevertheless be exercised in the use of verapamil in patients with severe myocardial decompensation." All these data, along with the experimental studies of Nayler et al.,'3 the clinical observations of Witchitz et al.'4 and our own experience in the adult5 suggest that verapamil is probably contraindicated in patients with severe heart failure secondary to or coincident with severe heart disease. Absence of Complications The important bradycardia and shock observed in one case must be related to the overdose administered by mistake. The effects of a dose three times greater than standard, however, were readily controlled by administration of isoproterenol, as has been reported in VOL 59, No 5, MAY 1979 interrupted all instances of PSVT: directly in 28 cases and indirectly in one. Contrary to what has been reported in comparable series,'5 2 administration of antiarrhythmic drugs or cardioversion were not needed. It is possible to use other drugs (personal experience in adults, unpublished data) or electrical cardioversion7 shortly after administration of verapamil if this drug has been unsuccessful. Previous administration of digitalis does not contraindicate the use of verapamil, but concurrent use of A-blocking agents does.4 The high effectiveness, rapid action and lack of undesirable side effects observed in our series suggest that verapamil is the drug of choice in the treatment of PSVT in infants without underlying heart disease. References Bender F: Isoptin zur Behandlung der tachykarden Form des Vorhofflatterns. Med Klin 62: 634, 1967 2. Diewitz M, Lange BM: Zur Behandlung tachykarder Rhythmusst6rungen mit verapamil. Med Klin 64: 1699, 1969 3. Schamroth L, Krikler DM, Garrett C: Immediate effects of intravenous verapamil in cardiac arrhythmias. Br Med J 1: 660, 1972 4. Krikler DM: Verapamil in cardiology. Eur J Cardiol 2: 3, 1974 5. Soler-Soler J, Sagrista-Sauleda J: Accion del verapamil, por via endovenosa, en las taquirritmias supraventriculares. Rev Esp Cardiol 28: 237, 1975 6. Wellens HJJ, Tan SL, Bar FWH, Dilren DR, Lie KI, Dohmen HM: Effect of verapamil studied by programmed electrical stimulation of the heart in patients with paroxysmal re-entrant supraventricular tachycardia. Br Heart J 39: 1058, 1977 7. Heng MK, Singh BN, Roche AHG, Norris RM, Mercer CJ: Effects of intravenous verapamil on cardiac arrhythmias and on the electrocardiogram. Am Heart J 90: 487, 1975 8. Spurrell RAJ, Krikler DM, Sowton E: Concealed bypasses of the atrioventricular node in patients with paroxysmal supraventricular tachycardia revealed by intracardiac electrical stimulation and verapamil. Am J Cardiol 33: 590, 1974 9. Hagemeijer F: Verapamil in the management of supraventricular tachyarrhythmias occurring after a recent myocardial infarction. Circulation 57: 751, 1978 10. Husaini MH, Kvasnicka J, Ryden L, Holmberg S: Action of verapamil in sinus node, atrioventricular and intraventricular conduction. Br Heart J 35: 734, 1973 11. Donnelly GL, Scamps P: Intravenous verapamil in cardiac arrhythmias. (abstr) Aust NZ J Med 3: 63, 1973 12. Ryden L, Saetre H: The hemodynamic effect of verapamil. Eur J Clin Pharmacol 3:153, 1971 13. Nayler WG, Szeto J: Effect of verapamil on contractility, oxygen utilization, and calcium exchangeability in mammalian heart muscle. Cardiovasc Res 6: 120, 1972 14. Witchitz S, Haiat R, Tarrade T, Chiche P: Accidents cardio1. vasculaires adults.4 15. Dosage Two infants needed an additional dose (50% higher than standard) to interrupt the tachycardia. This suggests that it may be necessary to administer the higher dose in patients whose weight is on the upper limit of the range. 16. Summary The results of this study suggest that verapamil is at least as effective as digitalis is reported to be'52' in the treatment of PSVT in infants. In our series verapamil 19. 17. 18. au cours des traitements par leverapamil. A propos de 6 observations. Nouv Presse Med 4: 337, 1975 Nadas AS, Daeschner CW, Roth A, Blumenthal SL: Paroxysmal tachycardia in infants and children. Pediatrics 9: 167, 1952 Giardina ACV, Ehlers KH, Engle MA: Wolff-Parkinson-White syndrome in infants and children. A long term follow-up study. Br Heart J 34: 839, 1972 Simcha A, Bonham-Carter RE: Paroxysmal atrial tachycardia in infancy and childhood. Lancet 1: 832, 1971 Andersen ED, Jacobsen JR, Sandoe E, Videbaeck J, Wennevold A: Paroxysmal tachycardia in infancy and childhood. Acta Paediatr Scand 62: 341, 1973 Lundberg A: Paroxysmal supraventricular tachycardia in infancy. A clinical and experimental study. Acta Paediat 143 (suppl): 1, 1963 20. Lubbers WJ, Losekoot TG, Anderson RH, Wellens HJJ: Paroxysmal supraventricular tachycardia in infancy and childhood. Eur J Cardiol 2: 91, 1974 Downloaded from http://circ.ahajournals.org/ by guest on August 22, 2014 SITUS AMBIGUUS/Dickinson et al. 21. Quero M: Cardiopatias congenitas. Diagn6stico y tratamiento de urgencia. Barcelona, Editorial Cientifico Medica, 1973, pp 162, 163 22. Bein G, Wolf D: The treatment of supraventricular paroxysmal tachycardia in infants and children with verapamil. Cardiol Pneumol 9: 151, 1971 23. Bein G, Wolf D: Therapie supraventrikularer paroxysmaler Tachykardien bei Neugeborenen mit Verapamil. Padiat Prax 12: 405, 1973 24. Talbot NB, Richie RH, Crawford JD, Tagrin ES: Metabolic homeostasis - a syllabus for those concerned with the care of patients. Cambridge, Massachusetts, Harvard University Press, 1959, p i 25. Soler-Soler J, Sagrista-Sauleda J: Tratamiento de la taquicardia paroxistica auricular del lactante y del nifio: acci6n 6ptima del verapamil. Abstractos XIV Congreso Espafiol Cardiologia, edited by Cat6lica Espaniola SA, Sevilla, 1976, p 163 26. Silvermann JJ, Werner M: Fatal paroxysmal tachycardia in a newborn infant with the Wolff-Parkinson-White syndrome. J Pediatr 37: 765, 1950 27. Kimball JL, Burch G: Prognosis of the Wolff-Parkinson-White syndrome. Ann Intern Med 27: 239, 1947 28. Keith JD, Rowe RD, Vlad P: Heart disease in infancy and childhood. New York, Macmillan, 1967, p 1062 29. Vaughan Williams EM: Electrophysiologic basis for a rational 30. 31. 32. 33. 34. 35. 36. approach to anti-dysrhythmic drug therapy. Adv Drug Res 9: 69, 1974 Shigenobu K, Schneider JA, Sperelakis N: Verapamil blockade of slow Na+ and Ca+ + responses in myocardial cells. J Pharmacol Exp Ther 190: 280, 1974 Fleckenstein A: Specific inhibitors and promotors of calcium action in the excitation-contraction coupling of heart muscle and their role in prevention or production of myocardial lesions. In Calcium and the Heart, edited by Harris P, Opie L. London, Academic Press, 1971, pp 136-188 Zipes DP, Fischer JC: Effects of agents which inhibit the slow channel on sinus node automaticity and atrioventricular conduction in the dog. Circ Res 34: 184, 1974 Wit AL, Cranefield PF: Effect of verapamil on the sinoatrial and atrioventricular nodes of the rabbit and the mechanism by which it arrests reentrant atrioventricular nodal tachycardia. Circ Res 35: 413, 1974 Zipes DP, Besch HR, Watanabe AM: Role of slow current in cardiac electrophysiology. Circulation 51: 761, 1975 Singh BN, Roche AHG: Effects of intravenous verapamil on hemodynamics in patients with heart disease. Am Heart J 94: 593, 1977 Apitz J, Gaissmaier U: Zwischenfall mit todlichen Ausgang nach intravenoser Injektion von Isoptin. Med Klin 66: 751, 1971 The Cardiac Conduction System in Situs Ambiguus DAVID F. DICKINSON, M.B., M.R.C.P., D.C.H., JAMES L. WILKINSON, M.B., M.R.C.P., KENNETH R. ANDERSON, M.B., M.R.C.P., AUDREY SMITH, F.I.M.L.S., SIEN YEN Ho, M. PHIL., AND ROBERT H. ANDERSON, M.D., M.R.C. PATH. SUMMARY The cardiac specialized conduction tissue was studied by serial sectioning in 13 cases of situs ambiguus. In four cases of right isomerism, we found paired sinus nodes in relation to a crista terminalis, and in each case a sling of conduction tissue between two atrioventricular nodes was present regardless of the ventricular morphology or cardiac position. In the cases with left isomerism, the sinus node was hypoplastic and abnormally located. We saw two types of atrioventricular conduction systems. In the three cases in which the morphologically right ventricle lay to the right of the morphologically left ventricle (presumed d-loop), a single atrioventricular bundle arose from a normally located atrioventricular node. In the five cases in which the morphologically right ventricle lay to the left of the morphologically left ventricle (presumed 1-loop) and in the one case with a univentricular heart, paired atrioventricular nodes were present, linked or potentially linked by a sling of conduction tissue. visceral configuration with duplication of either left- FAILURE OF LATERALIZATION of thoracic and abdominal viscera into the pattern of either situs solitus or situs inversus results in the symmetrical or right-sided structures termed situs ambiguus.' This frequently results in major malformations in the cardiovascular system. In situs ambiguus with right isomerism, duplication of right-sided structures, such as the crista terminalis, is associated with duplication of the sinus node.2 In the left isomeric form, where the crista terminalis is absent, atrial depolarization is known to be abnormal as judged from the surface ECG.3 The sinus node has been reported to be abnormally located in two cases studied by Bharati and Lev,4 one with multiple spleens and the other with a From the Department of Child Health, University of Liverpool, and the Department of Paediatrics, Cardiothoracic Institute, Brompton Hospital, London, England. Supported by grants from the Endowment Fund, Royal Liverpool Children's Hospital, and the National Heart Research Fund. Dr. Kenneth Anderson was a New Zealand Heart Foundation Travelling Fellow; present address: Department of Pathology, University of Otago, Dunedin, New Zealand. Dr. Robert Anderson is supported by the Joseph Levy Foundation and the British Heart Foundation. Address for reprints: Dr. James L. Wilkinson, Cardiac Department, Royal Liverpool Children's Hospital, Myrtle Street, Liverpool L7 7DG, United Kingdom. Received September 22, 1978; accepted November 14, 1978. Circulation 59, No. 5, 1979. single bilobed spleen. The atrioventricular conduction system has not been studied extensively in hearts with situs ambiguus. We have previously observed5 a sling of ventricular conduction tissue connecting paired atrioventricular 879 Downloaded from http://circ.ahajournals.org/ by guest on August 22, 2014











© Copyright 2026