
Forest plots-trying to see the wood and the trees-BMJ
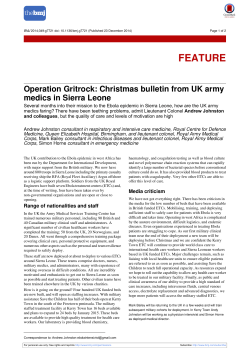
Downloaded from bmj.com on 24 September 2007 Forest plots: trying to see the wood and the trees Steff Lewis and Mike Clarke BMJ 2001;322;1479-1480 doi:10.1136/bmj.322.7300.1479 Updated information and services can be found at: http://bmj.com/cgi/content/full/322/7300/1479 These include: References This article cites 6 articles, 1 of which can be accessed free at: http://bmj.com/cgi/content/full/322/7300/1479#BIBL 12 online articles that cite this article can be accessed at: http://bmj.com/cgi/content/full/322/7300/1479#otherarticles Rapid responses 7 rapid responses have been posted to this article, which you can access for free at: http://bmj.com/cgi/content/full/322/7300/1479#responses You can respond to this article at: http://bmj.com/cgi/eletter-submit/322/7300/1479 Email alerting service Topic collections Receive free email alerts when new articles cite this article - sign up in the box at the top left of the article Articles on similar topics can be found in the following collections Systematic reviews (incl meta-analyses): descriptions (135 articles) Other Statistics and Research Methods: descriptions (600 articles) Notes To order reprints follow the "Request Permissions" link in the navigation box To subscribe to BMJ go to: http://resources.bmj.com/bmj/subscribers Downloaded from bmj.com on 24 September 2007 Education and debate Forest plots: trying to see the wood and the trees Steff Lewis, Mike Clarke Few systematic reviews containing meta-analyses are complete without a forest plot. But what are forest plots, and where did they come from? Summary points Forest plots show the information from the individual studies that went into the meta-analysis at a glance What is a forest plot? In a typical forest plot, the results of component studies are shown as squares centred on the point estimate of the result of each study. A horizontal line runs through the square to show its confidence interval— usually, but not always, a 95% confidence interval. The overall estimate from the meta-analysis and its confidence interval are put at the bottom, represented as a diamond. The centre of the diamond represents the pooled point estimate, and its horizontal tips represent the confidence interval. Significance is achieved at the set level if the diamond is clear of the line of no effect. The plot allows readers to see the information from the individual studies that went into the meta-analysis at a glance. It provides a simple visual representation of the amount of variation between the results of the studies, as well as an estimate of the overall result of all the studies together. Forest plots increasingly feature in medical journals, and the growth of the Cochrane Collaboration has seen the publication of thousands in recent years.1 They show the amount of variation between the studies and an estimate of the overall result Forest plots, in various forms, have been published for about 20 years During this time, they have been improved, but it is still not easy to draw them in most standard computer packages Neurosciences Trials Unit, Department of Clinical Neurosciences, University of Edinburgh, Western General Hospital, Edinburgh EH4 2XU Steff Lewis medical statistician UK Cochrane Centre, NHS Research and Development Programme, Oxford OX2 7LG Mike Clarke associate director (research) Correspondence to: S Lewis [email protected] nication). He based the idea on modified box plots.4 Ideas such as radial plots were also proposed.5 6 The first meta-analyses to include squares of different sizes to show the positions of the point estimates were probably those produced by the Clinical Trial Service Unit in Oxford in the 1998 overview of the prevention of vascular disease by antiplatelet therapy.7 The area of each square was proportional to the weight that the individual study contributed to the metaanalysis. BMJ 2001;322:1479–80 History The origin of forest plots goes back at least to the 1970s. Freiman et al displayed the results of several studies with horizontal lines showing the confidence interval for each study and a mark to show the point estimate. This study was not a meta-analysis, and the results of the individual studies were therefore not combined into an overall result.2 In 1982, Lewis and Ellis produced a similar plot but this time for a meta-analysis, and they put the overall effect on the bottom of the plot (fig 1 ).3 However, smaller studies, with less precise estimates of effect, had larger confidence intervals and, perversely, were the most noticeable on the plots. Means of focusing attention on the larger, more precise, studies were sought. Replacement of the mark with a square whose size was proportional to the precision of the estimate may have been first suggested by Stephen Evans at a Royal Statistical Society medical section meeting at the London School of Hygiene and Tropical Medicine in 1983 (S Evans, personal commuBMJ VOLUME 322 16 JUNE 2001 bmj.com Oxprenolol Propranolol Propranolol Propranolol Atenolol Narrow confidence limits Alprenolol Propranolol Propranolol Practolol Oxprenolol Practolol Propranolol Propranolol Timolol Metoprolol Alprenolol All β blockers -300 -250 -200 -150 -100 Increase in mortality on treatment -50 Wilcox Norris Multicentre Baber Wilcox Andersen Balcon Wilcox Barber CPRG Multicentre Barber BHAT Multicentre Hjalmarson Wilhelmsson Pooled 0 50 100% Reduction in mortality on treatment Fig 1 First use of forest plot for meta-analysis of effect of â blockers on mortality3 (reproduced with permission from Physicians World/Thomson Healthcare, Secaucus, NJ) 1479 Education and debate No (%) of deaths Study ß blocker Downloaded from bmj.com on 24 September 2007 ß blocker deaths Logrank Variance observed of observed Control – expected – expected patients Wilcox (oxprenolol) 14/157 (8.9) 10/158 (8.9) 2.0 5.6 Norris (propranolol) 21/226 (9.3) 24/228 (9.3) -1.4 10.2 Multicentre (propranolol) 15/100 (15.0) 12/95 (12.6) 1.2 5.8 Baber (propranolol) 28/355 (7.9) 27/365 (7.4) 0.9 12.7 Andersen (alprenolol) 61/238 (25.6) 64/242 (26.4) -1.0 23.2 Balcon (propranolol) 14/56 (25.0) 15/58 (25.9) -0.2 5.5 Barber (practolol) 47/221 (21.3) 53/228 (23.2) -2.2 19.5 Wilcox (propranolol) 36/259 (13.9) 19/129 (14.7) -0.7 10.5 CPRG (oxprenolol) 9/177 (5.1) 5/136 (3.6) 1.1 3.3 102/1533 (6.7) 127/1520 (8.4) -13.0 53.0 Barber (propranolol) 10/52 (19.2) 12/47 (25.5) -1.6 4.3 BHAT (propranolol) 138/1916 (7.2) 188/1921 (9.8) -24.8 74.6 Multicentre (timolol) 98/945 (10.4) 152/939 (16.2) -27.4 54.2 Hjalmarson (metoprolol) 40/698 (5.7) 62/697 (8.9) -11.0 23.7 Wilhelmsson (alprenolol) 7/114 (6.1) 14/116 (12.1) -3.4 4.8 Total* 640/7047 (9.1) 784/6879 (11.4) -81.6 Multicentre (practolol) Ratio of crude death rates (99% CI) ß blocker: control and they came from specially produced computer programs. Even now, most standard statistical packages cannot easily produce such a plot. Why a forest plot? The plot was not called a “forest plot” in print for some time, and the origins of this title are obscured by history and myth. At the September 1990 meeting of the breast cancer overview, Richard Peto jokingly mentioned that the plot was named after the breast cancer researcher Pat Forrest, and, at times, the name has been spelt “forrest plot.” However, the phrase actually originates from the idea that the typical plot appears as a forest of lines. A contender for the first use of the name “forest plot” in print is a review of nursing interventions for pain that was published in 1996.9 An abstract at the Cochrane colloquium later that year also used this name.10 We would welcome suggestions of precedents to these uses or any other versions of this brief history of the plot. We thank Jon Godwin for preparing figure 2. Funding: None. Competing interests: None declared. Cochrane Collaboration. Cochrane Library. Issue 1. Oxford: Update Software, 2001. Freiman JA, Chalmers TC, Smith H, Kuebler RR. The importance of beta, the type II error and sample size in the design and interpretation of the randomized control trial: survey of 71 “negative trials”. N Engl J Med 1978;299:690-4. 3 Lewis JA, Ellis SH. A statistical appraisal of post-infarction beta-blocker trials. Prim Cardiol 1982;suppl 1:31-7. 4 McGill R, Tukey JW, Larsen WA. Variations of box plots. Am Stat 1978;32:12-6. 5 DeMets DL. Methods for combining randomized clinical trials: strengths and weaknesses. Stat Med 1987;6:341-50. 6 Galbraith RL. A note on graphical presentation of estimated odds ratios from several clinical trials. Stat Med 1988;7:889-94. 7 Antiplatelet Trialists’ Collaboration. Secondary prevention of vascular disease by prolonged antiplatelet treatment. BMJ 1988;296:320-31. 8 Yusuf S, Peto R, Lewis J, Collins R, Sleight P. Beta blockade during and after myocardial infarction: an overview of the randomized trials. Prog Cardiovasc Dis 1985;275:335-71. 9 Sindhu F. Are non-pharmacological nursing interventions for the management of pain effective? A meta-analysis. J Adv Nurs 1996;24:1152-9. 10 Bijnens L, Collette L, Ivanov A, Hoctin Boes G, Sylvester R. Optimal graphical display of the results of meta-analyses of individual patient data. In: Proceedings of the 4th Cochrane colloquium, Adelaide, Australia, 1996. Oxford: Cochrane Collaboration, 1996. 1 2 310.7 0 Reduction 23.1% (SE5.0) P<0.0001 Heterogeneity between 15 trials: χ2 = 13.9; df = 14; P > 0.1 0.5 1.0 1.5 2.0 ß blocker better ß blocker worse Treatment effect P < 0.0001 * 95% confidence interval as shown for the odds ratio Fig 2 Updated version of Lewis and Ellis’s original plot (fig 1 ) showing effect of â blockers on mortality We have updated the original Lewis and Ellis plot3 to show how it might look in the modern style (fig 2 ). We obtained data for most of the component studies from a subsequent paper.8 In the 1980s, no standard computer packages could easily produce these plots, (Accepted 20 February 2001) A memorable patient A chandelier and a vat of custard It was a busy Friday night in casualty. We were one senior house officer down and there had been a major accident on a nearby main road. All of us had been looking after seriously injured patients for the preceding couple of hours—not all of them had survived, and emotions were running high. During that time, the backlog of minor injuries had built up to a six hour wait, and tempers were fraying in the waiting room. The nurses were fielding angry patients, often with trivial injuries, and were desperate for one of us to come and help. I returned to the minor side to start clearing the backlog as soon as possible. I was in a superefficient and slightly short-tempered mood—didn’t they realise that we had to deal with far more important things than cut fingers or drunks? I picked the next card out of the box and went to the cubicle. With barely a glance at the patient I said brusquely, “Well, what’s the matter then?” A middle aged man looked back at me and said, in a nonchalant tone, “I was preparing for my usual Friday night sexual activity when the chandelier broke, and I fell into the vat of custard.” 1480 It took a second or two for me to realise what he’d said. I looked up at him in disbelief. “Really?” I asked. “No,” he said, “but I’ve been sitting in the waiting room for two hours trying to pluck up the courage to say that.” As a grin broke over my face, I asked what had really happened, and he told me what he had done. As I treated him, I relaxed and chatted to him as a real person, not a patient. I spent the rest of the shift smiling. It inspired me to think that someone faced with a long wait had thought up something like that, and kept it in his mind, without getting annoyed or impatient. He changed my perspective, brightened up my evening, and reminded me of the fact that people, not patients, were in the waiting room. I have long since forgotten his name, but I still think about him when I’m having a bad day. Katherine Whybrew GP registrar, 19 Beaumont Street Surgery, Oxford BMJ VOLUME 322 16 JUNE 2001 bmj.com










© Copyright 2026