
INSIDE THIS ISSUE:
ANAESTHESIA The Newsletter of the Association of Anaesthetists of Great Britain and Ireland NEWS ISSN 0959-2962 No. 332 MARCH 2015 INSIDE THIS ISSUE: AAGBI Board/Council elections 2015 The perfect storm requires perfect standards Challenges to the wellbeing of the Irish anaesthetic trainee X-Porte – The World’s First Ultrasound Kiosk Editorial Contents 03Editorial 04 One look and the difference is clear: • Onboard Education: Watch 3D learning animations concurrently with live scans for real-time comparisons and guidance. • Fully customisable: Multi-gesture touch-screen interface. Sealed to facilitate cleaning and infection control. • Industry-leading five-year warranty. Learn more about X-Porte today by downloading our X-Porte iPad app. Or, better still, request a demonstration to experience X-Porte yourself. Email us at [email protected] www.sonosite.co.uk/products/x-porte 05 Spring is in the air and by the time this arrives on your doorstep, I expect election fever will have gripped the political classes of the UK. The NHS will no doubt be supported strongly by politicians of every hue. But those of us working at the coalface know that laudable ambitions are not always translated into better-resourced services. As Mario Cuomo put it, ‘You campaign in poetry; you govern in prose’. 05 AAGBI Board/Council elections 2015 Emma Plunkett provides an insight into her first six months on the GAT committee and our Irish trainee colleagues describe their work in addressing several concerns including wellbeing and inequalities in pay and conditions. Ireland features again in an article describing how the activity data collected for NAP5 has informed the debate about service provision, recruitment and retention. There are two very different personal perspectives from trainees. One outlines how funding from the National Institute of Academic Anaesthesia enabled him to complete his PhD on metabolic dysfunction and ischaemia following head injury. The other, describing a doctorpatient’s perspective on losing her baby, makes harrowing reading but includes some excellent points about how well patients remember details, particularly when matters have not gone well. One of the observations that has stayed with me from my certificate in education was the comment that ‘Teachers teach some of the time, learners learn all the time.’ It’s the same for us as doctors – patients notice all the time, even in our less auspicious moments. Something for the politicians to note as well perhaps! Nancy Redfern 08 The perfect storm requires perfect standards 12 A history of the Committee of Anaesthesia Trainees 15 Challenges to the wellbeing of the Irish anaesthetic trainee We too have elections for the AAGBI Council and GAT council members. If you would like to stand, or have a colleague who you think would contribute well to the work of the AAGBI, this is your chance to make a difference. I need not expand on the breadth of opportunity; education, safety, research, wellbeing, heritage, innovation and publication. The safety page, a new feature, includes two contributions from our Chair of Safety, Tom Woodcock. One describes the progress of the ‘The Small Bore Connector Clinical Advisory Group’ in encouraging standard processes for connector design, to minimise the risk of connecting the wrong tubes, and ensuring UK medical devices fit those used in other countries. The other is a more light-hearted piece about safety and the human tourniquet. The letters page this month covers anaesthetic machines suitable for resource poor environments and one admonishing those playing ‘revalidation bingo’ with the RCoA CPD codes. A bit of learning for me as a member of the education committee – point taken! FUJIFILM SonoSite, Inc. the SonoSite logo and other trademarks not owned by third parties are registered and unregistered trademarks of FUJIFILM SonoSite, Inc. in various jurisdictions. All other trademarks are the property of their respective owners. ©2014 FUJIFILM SonoSite, Inc. All rights reserved. Clinical research training fellowship in anaesthesia and intensive care medicine funded by the AAGBI 07 We invite you to stand for election to the Group of Anaesthetists in Training X-Porte delivers a type of image clarity never before seen in point-of-care ultrasound systems. X-Porte’s Extreme Definition Imaging (XDI) was specifically created to meet the challenge of unwanted phantom echoes from side-lobe beams. Using XDI proprietary beamforming technology, visual clutter is substantially reduced while significantly enhancing clarity. 04 08 19 Year 2007 21 Joining the GAT Committee: the first six months 23 Anaesthesia Digested 24 Safety Matters 26 Your Letters 12 28 Particles 16 21 Correction In the November issue of Anaesthesia News we published Anaesthetic training in underdeveloped countries: what is the role of junior trainees (pps 16–17). The authors would like to acknowledge the Tropical Health & Education Trust (THET) for managing the Zambia MMed Anaesthesia Programme, and the Department for International Development (UK Aid) for financing the programme. The Association of Anaesthetists of Great Britain and Ireland 21 Portland Place, London W1B 1PY Telephone: 020 7631 1650 Fax: 020 7631 4352 Email: [email protected] Website: www.aagbi.org Anaesthesia News Chair Editorial Board: Nancy Redfern Editors: Phil Bewley and Sarah Gibb (GAT), Nancy Redfern, Richard Griffiths, Sean Tighe, Tom Woodcock, Mike Nathanson, Rachel Collis, Upma Misra, Felicity Platt and Gerry Keenan Address for all correspondence, advertising or submissions: Email: [email protected] Website: www.aagbi.org/publications/anaesthesia-news Editorial Assistant: Rona Gloag Email: [email protected] Design: Chris Steer AAGBI Website & Publications Officer Telephone: 020 7631 8803 Email: [email protected] Printing: Portland Print Copyright 2015 The Association of Anaesthetists of Great Britain and Ireland The Association cannot be responsible for the statements or views of the contributors. No part of this newsletter may be reproduced without prior permission. Anaesthesia News March 2015 • Issue 332 Advertisements are accepted in good faith. Readers are reminded that Anaesthesia News cannot be held responsible in any way for the quality or correctness of products or services offered in advertisements. 3 Clinical research training fellowship in anaesthesia and intensive care medicine funded by the AAGBI Anaesthesia and intensive care medicine provides a valuable window into disease models for many chronic diseases such as neurodegeneration and dementias. Pathophysiological processes that evolve over a lifetime in chronic disease are contracted to a few days or weeks following an insult from a critical illness. To investigate the acute pathophysiological processes that culminate in morbidity following a head injury I decided to take a year out to undertake a clinical research fellowship with Professor David Menon in Cambridge, performing experiments and observational studies in patients with traumatic brain injury (TBI). Figure 1: 18F-FMISO and 15O triple oxygen positron emission tomography in a patient after traumatic brain injury In my fourth year as a specialist trainee (SpR 4) in anaesthesia and intensive care medicine, I took up a one-year research attachment to the University Division of Anaesthesia and Intensive Care at the University of Cambridge (funded by the East of England Deanery and awarded by open competition). I was then successful in obtaining a grant from the AAGBI, funded via the National Institute of Academic Anaesthesia, to support my fellowship for a further two years to progress towards a PhD. The £143,419 was used for my salary and to fund the volunteer studies (using magnetic resonance spectroscopy and diffusion tensor imaging) required before my patient experiments. Working with Professor David Menon and Dr Jonathan Coles, I used magnetic resonance imaging (MRI), proton spectroscopy (1HMRS) and positron emission tomography (PET) to investigate patients with acute brain injury. I learned generic skills such as interacting with clinical academics and basic scientists, collecting and interpreting data, time management, and about funding and research teams. I completed courses relevant to the conduct of my proposed research, including MR and radiation safety, image analysis, statistics, preparation of manuscripts and Good Clinical Practice in research. The fellowship funded by the National Institute of Academic Anaesthesia and the AAGBI enabled me to complete my PhD in energy failure following TBI and gave me a solid foundation from which to initiate and set up further research activity. To investigate the mechanisms responsible for neuronal loss following TBI, I used PET using various ligands (11C PIB, 15 O triple oxygen and 18F FMISO; Figure 1) to demonstrate derangements in cerebral metabolism and to elucidate long term sequelae of ischaemia and derangement in metabolism following head injury.1-5 I also published various articles pertinent to current intensive care practice. I successfully optimised 44 whole brain spectroscopy for patients after TBI at the Wolfson Brain Imaging Centre and visited collaborators at the Miller School of Medicine in Miami, Florida. I gained experience in performing and analysing imaging data (obtained from PET and MRI) to demonstrate derangements in cerebral metabolism and to investigate interventions (such as hyperoxia) to ameliorate metabolic dysfunction and ischaemia following head injury. My research has provided invaluable insights on the diffusion barrier to oxygen after TBI, and ways to overcome such tissue hypoxia. After finishing my fellowship and the remainder of my training I obtained a substantive consultant job in Birmingham. I am in the process of writing my thesis to be examined early next year. By the end of the clinical research training fellowship I acquired transferable research skills in PET, diffusion tensor imaging and spectroscopy to investigate critically ill patients for neurocognitive dysfunction and decline. Dr Tonny Veenith Consultant in Critical Care Medicine, University Hospitals Birmingham NHS Foundation Trust Honorary Clinical Research Fellow, University of Cambridge References 1. 2. 3. 4. 5. Veenith TV, Carter E, Grossac J, et al. Inter subject variability and reproducibility of diffusion tensor imaging within and between different imaging sessions. PLoS One 2013; e65941 Veenith T, Coles JP. Anaesthesia for magnetic resonance imaging and positron emission tomography. Current Opinion in Anaesthesiology 2011; 24: 451–8. Hong YT, Veenith T, Dewar D, et al. Amyloid imaging with carbon 11-labeled Pittsburgh compound B for traumatic brain injury. JAMA Neurology 2014; 71: 23–31. Veenith TV, Carter EL, Grossac J, et al. Use of diffusion tensor imaging to assess the impact of normobaric hyperoxia within at-risk pericontusional tissue after traumatic brain injury. Journal of Cerebral Blood Flow and Metabolism 2014; 34: 1622–7. Veenith TV, Mada M, Carter E, et al. Comparison of inter subject variability and reproducibility of whole brain proton spectroscopy. PLoS One 2014; e115304. Anaesthesia AnaesthesiaNews NewsMarch March2015 2015••Issue Issue332 332 AAGBI Board/Council Elections 2015 In 2015, three members of the Board and Council of the AAGBI will have completed their 4 year terms as Elected Members: Drs Nancy Redfern, Kathleen Ferguson and Tom Woodcock. Nancy will be staying on as Honorary Membership Secretary, and Kathleen will continue in her role as Honorary Treasurer. In his 4 years on Council, Tom has achieved a huge amount, not only in his role as Chair of the International Relations Committee, but also as Chair of the Safety Committee. He has lectured widely on IV fluids and organised a highly successful joint AAGBI meeting with the Physiological Society. Tom has created the National Essential Anaesthetic Drug List (NEADL) and has championed the use of the Yellow Card Scheme for reporting adverse drug reactions within the UK. He has always been a wise voice of reason on Council as well as making us laugh when no one can agree on things. Thanks go to Tom for all of the above. Grants). All of the meetings are on a Friday. Elected members should expect to be at the Association’s headquarters at 21 Portland Place, London, for at least two Fridays a month: always the first Friday and usually one other Friday. In addition, Council members will be expected to attend WSM, Annual Congress, the Linkman meeting and the GAT meeting. You may also be asked to represent the AAGBI at Core Topics/Seminars and at occasional external meetings, such as the RCoA, which may be on a different day of the week. You do not have to attend them all, but you do have to attend most of them. I would strongly advise that you talk to your Clinical Director and Medical Director before seeking nomination, to ensure that you have departmental and Trust support for this work. This year we need three new Board members who will be elected for a 4 year term. Elected Board members are automatically members of the Council. Candidates must be ordinary members of the AAGBI, in good standing, and as Board and Council members must represent and work for the whole speciality. Currently Council comprises a mixed bunch of anaesthetists with a wide range of professional interests: obstetrics, paediatrics, trauma, regional, ITU, neuro and cardiac as well as those who excel in research, or enjoy the buzz of working abroad. What unites us all is a great team spirit, work ethic, time management skills and, perhaps more importantly, an enthusiasm and a drive to make things better for anaesthetists and improve quality of care and safety for our patients. What has always struck me about the AAGBI is what a friendly and effective organisation it is. In my 6 years, I have been a Council member, Chair of Education and now Honorary Secretary. I have learnt to ride a bike, shared a room and chamois cream with various AAGBI members (all legit, Ed!), had tea at the Palace, tasted food and wine at the Savoy, seen the numbers attending our education events rise by a third, and double for our GAT meetings. I have been involved with Learn@AAGBI, seen the launch of our fabulous AAGBI Guideline and Anaesthesia apps, and been proud of the many ‘glossies’ that we have produced. I have become Twitter positive, Facebook negative, LinkedIn phobic, and the queen of acronyms! I have learnt to appreciate the details of finance spreadsheets and to recognise a set of management accounts from a mile off! None of this would possible, however, without the wonderful team of staff at 21 Portland Place. The AAGBI is more than a membership organisation for over 10,700 members. It consists of two legal entities (a limited company and a charity), employs 30 staff, with a combined turnover of over £4 million per year. Board members are automatically directors/trustees of both company and charity and so must be eligible to serve in this capacity. So, what’s the catch? Honestly, there is only one, and that is TIME! Elected members are expected to attend Board and Council meetings and will be allocated to 2-3 other committees (e.g. IRC/ Safety/Education/Anaesthesia News/Wellbeing/GAT/Research and Anaesthesia News March 2015 • Issue 332 So if you are interested in joining us….. stand for election! I would be more than happy to chat to you about life at the AAGBI. The closing date for nominations is 17:00 on Friday 10 April 2015 and the successful candidates will take up their posts from the Annual Members meeting at Annual Congress Edinburgh in September 2015. The Election will be run by Electoral Reform Services and this year the ballot will be online only. Please ensure that we hold a current email address for you so that you don’t miss out on your chance to vote. You can check and update your details by logging in to the members’ area on the website; if you’re unsure how, please contact [email protected] for assistance. The results will be announced at June’s meeting of Council, although candidates will have heard from the AAGBI President before then. I wish you luck and I look forward to see you in Edinburgh for Annual Congress! Dr Samantha Shinde Honorary Secretary 5 REGIONAL ANAESTHESIA UK EETING ANNUAL SCIENTIFIC M MANCHESTER ENEATESITHNESGIA M C I F I T N E I ATLHESBOCUNDARIES OF REGIONAL A ANNENU GING CHALL ri 15 May Thurs 14 & F MANCHESTER , UNI VERSITY OF RENOLD BUILDING Who are the Group of Anaesthetists in Training (GAT)? 2015 D R O F X O all H n w o T d r Oxfo S WORKSHOP COURSE REFRESHER PETITION POSTER COM E DINNER CONFERENC LEAVE NOW! Y D U ST R U YO K O BO 17-19 JUNE 2015 cludinglectures, nalprogrammein • Greateducatio ps ningandworksho lear ed ce bas blem pro nualDinner&Dan tsincludingtheAn including • Funsocialeven ities topportun men lop eve ald sandprizes • Profession antinterview,poster mentoring,consult ingof mwithlivestream • Parent&babyroo s conferencelecture FOR MORE DETAILS, REGISTRATION OR ABSTRACT FORM, GO TO www.ra-uk.org CALL FOR NO The Group of Anaesthetists in Training (GAT Committee) comprises elected trainees of all grades. We are a democratically elected body representing anaesthetic trainees at AAGBI committees, Royal College of Anaesthetists Trainee Committee and other national medical bodies. The GAT Committee also works on publications, seminars and the ever-popular Annual Scientific Meeting. Nominations are now invited from trainee members of the Association wishing to stand for election. In 2015 there will be at least five seats available on the committee. Those standing for election will be expected to serve a minimum term of two years and be resident in the United Kingdom or Ireland. If elected, nominees agree to fulfil the duties and responsibilities required of them. Further information and nomination forms are available from the AAGBI Secretariat on 0207 631 1650 (option 3), by emailing [email protected] or can be downloaded from the AAGBI website (www.aagbi.org/gatcommittee). All nominees should be proposed and seconded by other trainee members of the AAGBI and submitted to: GAT Committee, 21 Portland Place London W1B 1PY, by email to [email protected] or faxed to 020 7631 4352. Closing date is Friday 10 April 2015 at 17:00. ANAESTHESIA NEWS GAT COMMMINITATTIEOENS www.gatasm.org Anaesthesia News now reaches over 10,700 anaesthetists every month and is a great way of advertising your course, meeting, seminar or product. Anaesthesia News is the official magazine of the Association of Anaesthetists of Great Britain & Ireland. CALL NOW FOR A MEDIA PACK For further information on advertising Tel: 020 7631 8803 We represent trainee members of the AAGBI; currently this is over 3500 trainees and over 85% of trainee anaesthetists within Great Britain and Ireland. If you become a member of the GAT Committee you will be in a position to impact nationally on how training evolves within anaesthesia over the next decade. It is very easy to criticise, much more difficult to suggest compromise and solutions. If you think you can represent your colleagues and peers, are innovative and resourceful, and can work well within a team of enthusiastic individuals, then we want you on the GAT Committee. We invite you to stand for election to the Group of Anaesthetists in Training What do we do? What to do next? The Committee has 13 elected members, with an executive comprising the Chair, Vice Chair and Honorary Secretary. We meet three times a year at the AAGBI headquarters in London and also at the GAT Annual Scientific Meeting (ASM). In 2015, there will be at least five seats available for election to the Committee. Those standing for election will be expected to serve a minimum term of two years, up to a maximum of four years. You need to be resident in the UK or Ireland for your term of office. Most meetings will take place at the AAGBI headquarters in London and are usually on Fridays. If elected, nominees agree to fulfil the duties and responsibilities required of them. The term of office on the Committee officially commences at the GAT ASM in Manchester from 17-19 June 2015. As an elected committee member you would expect to have AAGBI commitments on approximately 10 to 12 days over the course of a year in addition to the 3-day ASM. There is also a significant amount of discussion that takes place via email. The Chair and Honorary Secretary are members of AAGBI Council and voting members of the Board; the Vice Chair is co-opted to Council. The GAT Committee members represent trainees on all AAGBI committees and working parties; they are also co-opted onto several external committees, including the Royal College of Anaesthetists Trainee Committee and the BMA Junior Doctors Committee. We provide anaesthetic trainee representation to important national initiatives such as the Shape of Training Review and the government’s review of the impact and implementation of the European Working Time Regulation. The GAT Committee has editorial control of the trainee section of the Association’s monthly newsletter Anaesthesia News, and organises seminars and the GAT ASM specifically for trainees. The GAT Committee tends to attract senior trainees. We encourage core trainees and ACCS trainees to also stand for election to ensure that all grades of anaesthesia trainees are represented. We would also like representation on the Committee from all parts of Great Britain and Ireland, so we encourage nominations from Ireland, Northern Ireland and Wales in particular, as they are currently unrepresented. The responsibility we are given is a privilege. As well as being extremely interesting, this opportunity offers great scope for the development of personal skills in management, negotiation and committee working, authorship and presentation at a national level. or email Chris Steer: [email protected] www.aagbi.org/publications Dr Les Gemmell Immediate Past Honorary Secretary Anaesthesia News March 2015 • Issue 332 Further information and nomination forms are available from the AAGBI secretariat on 020 7631 1650 (option 3), [email protected] or can be downloaded from the AAGBI website (www.aagbi.org/ gatcommittee). All nominees should be proposed and seconded by other trainee members of the AAGBI and submitted to: GAT Committee, 21 Portland Place, London, W1B 1PY; by email to [email protected] or faxed to 020 7631 4352. The closing date is Friday 10 April at 17:00. We look forward to receiving your nomination form. Sarah Gibb, Caroline Wilson & Annemarie Docherty GAT Chair, Vice Chair & Honorary Secretary 7 The perfect storm requires perfect standards The results of two of the largest audits of anaesthetic services in Ireland have recently been published.1,2 The two surveys were part of the 5th National Audit Project (NAP5) of the Association of Anaesthetists of Great Britain & Ireland (AAGBI) and the Royal College of Anaesthetists (RCoA) concerning accidental awareness during general anaesthesia. Results of the main project were released on 10 September 2014.3 The College of Anaesthetists of Ireland (CAI) collaborated closely with the AAGBI and the RCoA for NAP5. 8 The first audit,1 was conducted in the 46 acute public hospitals (Health Service Executive and Voluntary hospitals) and 20 acute independent (private) hospitals during a week in December 2013. Data on anaesthetic techniques, patients’ characteristics, staffing, admission and discharge arrangements were collected on all cases for which anaesthetic care (general, regional or local anaesthesia, and sedation or monitored anaesthesia) was provided. The second paper2 details the results of a questionnaire given to every consultant anaesthetist in each of the 46 public hospitals in Ireland. This questionnaire was designed to find out the number of cases of accidental awareness under general anaesthesia that consultants became aware of in patients under their supervision. provisioning will also allow for the development of standards for healthcare delivery where these do not already exist. This is the first ever national audit carried out relating to anaesthesia in Ireland. The anaesthetic activity survey has complimented the work carried out by the CAI on provision of anaesthesia services in Ireland that culminated in a document which was publically launched in February 2014.4 The total number of anaesthetists in the UK in 2007 was 20.7 per 100,000 population and is now nearer 21 per 100,000. In Ireland in 2012 the ratio was 18.5 per 100,000. Ireland therefore has fewer anaesthetists than the UK but, more importantly, the makeup of this workforce differs significantly between the two countries. In Ireland, consultants account for 45% of the total anaesthesia workforce, trainees 25% and non-training NCHDs 30%. In the UK, consultants make up 50% of the anaesthesia workforce, trainees 35% and career grade doctors the remaining 15%. What this means in practice is that 65% of UK anaesthetists are in permanent positions compared to just 45% in Ireland. Trainees make up the balance of the UK anaesthesia workforce and, though individual trainees are not permanent in terms of individual contracts, the overall numbers and location of their posts are relatively stable in terms of workforce provision. In Ireland, trainees make up a further 25% of the anaesthesia workforce and, similar to the UK, they are a relatively stable workforce. The provision of anaesthesia services and workforce in Ireland has evolved largely in response to local requirements rather than being centrally planned. A number of centrally commissioned reports have made recommendations about overall staffing requirements in anaesthesia and ICU, but none of these has been fully implemented. Recruiting staff in this reactive manner leads to a different type of service provision than would have occurred had a more proactive approach and global recruitment process been utilised. First, the workforce is based on locally estimated service needs which often arise in advance of the anaesthesia workforce being provided, resulting in overstretching of available resources. In addition, the type of workforce provided, in terms of grade and specialty, may differ from that which is required for the long term development of the service. Proactive provisioning of workforce should allow recruitment of staff to meet centrally defined standards and centrally planned growth of the entire health service. Proactive Anaesthesia News March 2015 • Issue 332 In January 2013, the CAI and the National Clinical Programme for Anaesthesia (NCPA) published a report on anaesthesia workforce provision in Ireland which outlined the current workforce challenges, documented the shortage of consultant anaesthetists in Ireland and the difficulties in recruiting both consultants and non-consultant hospital doctors (NCHDs).4 Jonker et al.1 provide additional complimentary information on anaesthesia services in Ireland. This paper also provides an indicator of how the current staffing levels impact on delivery of anaesthesia services in Ireland when compared with the UK. Ireland differs from the UK in having an additional 30% of the workforce that are neither permanent nor on training rotations. These doctors rotate on a six monthly or yearly basis and the impact of having to replace these anaesthesia staff is a significant burden on anaesthetic departments. Anaesthesia News March 2015 • Issue 332 In 2003 the Hanly Report5 recommended that this portion of the workforce be replaced with permanent staff, increasing consultant numbers from 8 to 11 per 100,000 population. This has not happened and consultant numbers remain at 8.2 per 100,000. Worsening socioeconomic circumstances and conditions of employment for all doctors prevalent over the last few years have resulted in major difficulties in filling non-training NCHD posts. The difference in training numbers The difference in training numbers between the UK and Ireland reflect the differences in permanent staff which trainees will be required to fill. In the UK there are 13.7 permanent staff per 100,000 population (10.8 consultants and 2.9 career grade). There are 7.4 trainees per 100,000 (2007 RCoA census6) which is just over a 2:1 ratio of permanent staff to trainees. In Ireland in contrast, there are 4.7 trainees per 100,000 population which is probably appropriate for the 8.2 per 100,000 permanent staff in Ireland. If and when we do increase the number of permanent staff in Ireland, we will need a concomitant increase in training numbers. However, the question of when to increase training numbers is problematic. In 2012 the Department of Health introduced a 30% pay cut for new consultants. This has had a devastating effect on consultant recruitment in Ireland. The UK and Ireland share the problem that we are in competition with the rest of the English speaking world as regards retention of our trainees as consultants once they finish training. Currently Ireland ranks very poorly in this competition and most of our trainees leave on completion of their training. This in itself is not new, but now they leave without intending to return in the near future. Ireland is thus facing a ’Perfect Storm‘ in terms of recruitment, we are increasingly unable to recruit non-‐training NCHDs and at the same time are losing our trainees who finish training and are therefore unable to fill consultant posts. In addition to the overall anaesthetic workforce differences between Ireland and the UK, the localised nature of consultant recruitment in Ireland results in differing staffing ratios in Irish hospitals. NAP5 9 illustrates this in terms of the workload per anaesthetic consultant. This not only differs from the UK but also differs significantly across Irish hospitals. In the UK, the NAP4 study7 indicated that consultant anaesthetists deliver, on average, approximately 360 general anaesthetics per annum and an additional 25% local/regional procedures to give a total of approximately 450 procedures per consultant anaesthetist per annum. The data produced by the Irish NAP5 study indicate that Irish consultants provide a median of 720 anaesthetic procedures per annum, 60% more than their UK counterparts. This workload is unevenly distributed across the health service. In four Irish hospitals the anaesthesia consultant workload is below the UK average and in the other 37 hospitals the workload exceeds the UK average. Ten of these hospitals are more than twice the UK average and two are more than four times the UK average. Given that, in Ireland, 55% of anaesthesia practitioners are NCHDs, Irish consultants probably supervise more NCHD staff than their UK counterparts and this may account for a fraction of the higher workload of Irish consultants. The figures from NAP5 demonstrate the proportionally higher and disproportionate workload among Irish consultant anaesthetists. A handful of departments are generously staffed while most are understaffed, some significantly so. Obstetric Anaesthetists Association, the Association of Paediatric Anaesthetists and by various reports dealing with the staffing of intensive care in Ireland. Where standards were not available, the CAI/NCPA have recommended new standards. These principally revolve around workforce provisioning and include the number of consultants per roster, a 1:1 ratio of anaesthetic consultant to surgical list and recommendations on who should provide anaesthesia independently in Ireland. It will be up to the profession, both through representative bodies such as the CAI and the AAGBI and as individual anaesthetists, to insist that the high quality of anaesthesia in Ireland is maintained by adhering to these standards. Editor for The Editorial Board of Anaesthesia is looking for a new Editor to join the current team Patient care Do the workforce challenges facing anaesthesia departments impact on patient care? The paper1 did not set out to examine this question but it does provide some indicators. The central question of the incidence of awareness is slightly less than that reported in the UK and so, in this respect, there is no impact. The timing of surgery indicates that, while there is significant out of hours activity, the majority of immediate and urgent cases are accommodated during working hours. This is welcome and indicates that the lessons of CEPOD are being implemented in Ireland. There is a proportion of elective work completed out of hours. What is not clear is what proportion of this consists of overruns of elective lists or of scheduled out of hours elective activity. The paper did report that one third of hospitals had theatre closures during the study period. The reasons for this are not clear and may have resulted from insufficient anaesthesia resources or from the reduction in hospital budgets that have arisen over the last few years, neither of which are mutually exclusive. Finally the data on the site of first pre-anaesthesia interaction between the anaesthetist and the patient is more interesting. Only 15% were seen in pre- operative assessment clinics and 37% had their first contact with the anaesthetist in theatre. It is not unreasonable to assume that the current theatre workload is impacting on anaesthetists’ ability to see patients either in the pre-operative assessment clinic or on the wards prior to surgery. The current picture of the Irish anaesthesia workforce, drawn from recent reports and NAP5, poses considerable challenges. Because of changes in contractual conditions, recruitment to both consultant and NCHD posts is becoming more difficult. Hospitals are facing the daily challenge of delivering the same services with fewer anaesthetic staff than before. Solutions to these problems are not entirely within the profession’s control but we do have an important role in safely managing the situation, both our own and, more importantly, our patients’ best interests. The proposed reconfiguration of hospitals into regional trusts should allow for rationalising of anaesthetic services, such that the number of sites requiring 24/7 services are reduced. Anaesthetists will have to be at the forefront of discussions on reorganisation to ensure it meets the needs of our profession. More importantly, however, we as a profession must insist that the anaesthesia workforce meets standards defined by, among others, the CAI, the AAGBI, the 10 The successful applicant must be able to work well in a team, be able to keep to strict deadlines, have a history of publication and be able to write coherent and elegant English. Previous editorial experience is not necessary, but experience of acting as an assessor/referee for applications submitted to peer-review journals would be an advantage. Applicants should submit a brief summary, of up to 400 words, of what they think the Journal does well and/or could improve, by email to the Editor-in-Chief at [email protected], together with a short curriculum vitae with the following headings: Editors typically work between 6 and 8 hours each week on the Journal, and must also be prepared to attend biannual Editors’ and Editorial Board meetings and contribute to the AAGBI’s Winter Scientific Meetings and Annual Congresses. As well as the opportunity to work with an excellent and cohesive editorial team, rewards include an honorarium and free registration at major AAGBI meetings. • • • • Summary of current activities & professional areas of interest Reasons for applying Previous editorial/assessor experience Recent publications Shortlisted candidates may be asked to perform a small number of typical editorial tasks as part of the selection process, and need to be available to do this during May-June 2015. There will be no interview. Please direct any queries for further information to the Editorial Office at the above email address. The closing date for applications is 30th April 2015. Dr Wouter Jonker and Dr Ellen O’ Sullivan Dr David Mannion Chair Training Committee, College of Anaesthetists of Ireland Dr Wouter Jonker National Co-ordinator National Audit Project Ireland Dr Ellen O’ Sullivan President, College of Anaesthetists of Ireland, LEAD National Audit Project Ireland References 1. 2. 3. 4. 5. 6. 7. Jonker WR, Hanumanthiah D, Ryan T, Cook TM, Pandit JJ, O’Sullivan EP. Who operates when, where and on whom? A survey of anaestheticsurgical activity in Ireland as denominator of NAP5. Anaesthesia 2014; 69: 961–8. Jonker WR, Hanumanthiah D, Cook TM, Pandit JJ, O’Sullivan EP. A national survey (NAP5-Ireland baseline) to estimate an annual incidence of accidental awareness during general anaesthesia in Ireland. Anaesthesia 2014; 69: 969–76. Fifth National Audit Project of the Royal College of Anaesthetists in collaboration with the Association of Anaesthetists of Great Britain & Ireland. NAP5: Accidental Awareness during General Anaesthesia in the United Kingdom. http://www.nationalauditprojects.org.uk/NAP5_home (accessed 19/1/2015). Providing quality, safe and comprehensive anaesthesia services in Ireland – A review of manpower challenges. http://www.hse.ie/eng/ about/Who/clinical/natclinprog/anaesthesia/Providing_Quality_Safe_ and_Comprehensive_Anaesthesia_Services_in_Ireland.pdf (accessed 19/1/2015). Report of the National Task Force on Medical Staffing. 2003. http:// www.lenus.ie/hse/bitstream/10147/46569/1/1680.pdf (accessed 19/1/2015). RCoA Census Report 2007. http://www.rcoa.ac.uk/system/files/CSQ2007Censusreport-final.pdf (accessed 19/1/2015). The 4th National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society. Major complications of airway management in the United Kingdom. Report and Findings. March 2011. http://www.rcoa.ac.uk/nap4 (accessed 19/1/2015). Anaesthesia Anaesthesia News News March March 2015 2015 •• Issue Issue 332 332 EDINBURGH SCOTLAND Poster/abstract submissions deadline 01 May 2015 SAVE THE DATE The EICC is Scotland’s greenest convention centre and the AAGBI are committed to working with them to make Annual Congress as environmentally friendly as possible. After 18 months, CAT had become well established in the College and had sufficient prominence among trainees to hold formal elections. There have been two subsequent committees since the original and each has built on the success of the former, increasing the strength of the committee and the voice of the anaesthetic trainees. The success of the Information Day has led to the development of similar meetings including a CAT Consultant Interview and CV Workshop. The committee are also involved in the College Audit Study day and are in the process of establishing a nationwide Trainee Research and Audit Network. The first audit, a snapshot of EWTR compliance among trainees, achieved over 80% response rate within two weeks. Prehospital medicine is an area of focus for the current committee. A substantial proportion of trainees are interested in this field but restricted in their activities as a result of the Medical Practitioners Act 2007. A working group has been established to review the incorporation of prehospital medicine into anaesthesia training with appropriate consultant supervision. The Committee of Anaesthesia Trainees (CAT) consists of 10 trainees of the College of Anaesthetists of Ireland (CAI) elected by their peers. The committee represents the view of CAI trainees within the College, at a national level, and ensures trainees play a part in shaping the future of anaesthesia in Ireland. CAT was established in 2011. Prior to this, trainees were represented in the College by a small group known as the ATI (Anaesthetists in Training of Ireland). Their involvement in the College fluctuated over the years and was somewhat limited. As part of the accreditation process of the CAI as a training body by the Irish Medical Council, involvement of trainees in the College was analysed. As a result, the then Chair of the Training Committee, David Mannion, formerly a GAT representative, announced that the College were interested in having a new trainee committee which would be more structured and have fuller representation within the College. Following this announcement, the former President of the ATI invited interested trainees to an open meeting in the College in December 2011. This was a time of considerable change in anaesthesia and medicine as a whole in Ireland. The introduction of the Medical Practitioners Act, institution of the new streamlined 6 year SAT (Structured Anaesthesia Training) scheme, and the economic situation all had a significant impact on the structure of training, working conditions and retention of trainees in Ireland. Recognising the chance to influence the future of their training and professional lives, a small group attended the first meeting, subsequently joined by others to form the first CAT. The first task was to establish CAT within the College and increase awareness of their existence. Trainee representatives were assigned to all the relevant committees in the College and CAT terms of reference were drawn up. Over the first 18 months, CAT initiated 12 A history of the Committee of Anaesthesia Trainees various projects of its own and contributed to College proposals to improve training and conditions throughout the country. The proposals included liaison with trainees regarding the new SAT scheme with feedback to the College, ensuring competencies could be achieved within five years and minimising the number of times a trainee would be rotated out of their base location. A Rota Maker Policy was developed and communication with trainees was improved by updating the CAT section of the CAI website and establishing a CAT email address and newsletter. CAT represented the views of anaesthesia trainees nationally through attendance at College Strategy Days and having an input into the College Manpower Planning Document. Through representation on the NCPA (National Clinical Programme for Anaesthesia), CAT also contributed to drafting of national policy proposals such as the Transport Medicine document and Pathway for the Critically Ill Obstetric Patient. By having a member on the trainee subcommittee of the Forum of Postgraduate Training Bodies, CAT was able to represent the views of anaesthesia and medical trainees in general nationwide and suspend the introduction of a junior consultant grade in Ireland. In addition, CAT established education sessions of its own. These included an Anaesthesia Information Day in 2013 for those interested in a career in anaesthesia and a trainee session at the Irish Annual Congress of Anaesthesia. Anaesthesia News March 2015 • Issue 332 Our communication tools have improved and expanded. An extended version of the newsletter, CAT News, is now circulated to both trainees and College fellows. We have a closed Facebook group with details of upcoming events, rotation swaps, special interest years and Fellowships and we hope to establish Lead Anaesthetic Trainees (LATs) in each hospital as a direct link between trainees, departments, the CAI and CAT. Through these forums and more, CAT has strengthened the voice of anaesthesia trainees in Ireland. A recent example is the debate over pay scales in Ireland, with the HSE introducing a new salary scale for run-through training schemes without prior agreement of the IMO. These changes affected only a small number of anaesthesia trainees who were unfairly disadvantaged financially. CAT raised awareness of this issue in the medical community at large via articles in the Irish Medical Times, a trainee petition and communication with the IMO who took steps rectify the issue. A major influence on CAT has been the link with GAT. One of the first undertakings of the original committee was to re-establish dormant links with GAT and to have a representative on the Irish Standing Committee. GAT and the AAGBI’s involvement with the Irish anaesthesia trainees, throughout the years, has been significant. At the AAGBI’s ASM in Dublin in 2013, Dr Nancy Redfern, Chair of the Support and Wellbeing Committee, co-chaired a trainee forum with CAT with the aim of highlighting trainees’ perspectives about anaesthesia training in Ireland. At this meeting, Dr Redfern’s approach to tackling issues caught CAT’s attention, and a sense of optimism in these times of fiscal adversity spread throughout CAT and the Irish trainee community in general. Since then, CAT has continued to engage with GAT and the AAGBI via regular GAT meetings at 21 Portland Place. Following the success of the trainee forum, it was proposed that GAT join CAT in Dublin for a joint meeting. The objective was to advance each committee’s knowledge of Irish and UK training, and to discuss and act on many pertinent issues facing both communities. The following were topics discussed and action points created: 1. Structure of Anaesthesia Training: o Multisource feedback for trainees in competencies necessary from an Irish perspective o Is combining a run-through scheme, a special interest year and EWTD feasible for Certificate of Clinical Specialist Training in Ireland? 2. Structure of the Committees o GAT represents both UK and Irish trainees. Should they have Irish representation on the committee and not just a co-opted CAT member? 3. Workforce statistics o Both groups see similar issues in consultant recruitment 4. Trainees in difficulty o Buddying and mentoring systems already established in UK seem logical to Irish trainee welfare. Appropriate training is preferable (via the AAGBI and Dr Redfern). An Irish section for trainees in difficulty will appear in the GAT Handbook 5. Communications strategies o CAT to refine social media policy document and appoint an e-communications role 6. Trainee Network Leads (TNL) o CAT are working on an accurate description of this role in Ireland, whether it will be hospital or region based, and will liaise with GAT TNL’s to disseminate information between both committees appropriately 7. Pre-hospital care (PHEC) o Irish PHEC working party may benefit from GAT representative while CAT representation on the AAGBI PHEC glossy creation was suggested Following the success of the 2014 meeting in Ireland, a joint collaboration in 2015 is already being discussed, with the GAT ASM in Manchester being suggested as the ideal setting. The combination of the two groups, as we have seen this year, is a positive step forward in helping to further develop and nurture the impact of CAT and GAT on their respective trainee populations. GAT, as the trainee committee of the AAGBI, represents trainees throughout the British Isles. In the past several Irish trainees have held position on GAT. Following the joint meeting, it has been strongly suggested that an Irish voice becomes established on GAT. This can only happen democratically during the annual GAT elections in April/ May. Therefore, CAT and the CAI will be urging Irish trainees to use their vote to establish Irish representation on GAT, something which will inevitably be hugely beneficial not only to Irish trainees and CAT, but in a sense creating a more geographically representative GAT. The Irish trainee voting voice will need to be heard, and CAT will be keeping trainees up-to-date on such developments in 2015. Aisling McMahon Vice-Chair, CAT Colm Keane CAT representative co-opted onto GAT Through some hard work behind the scenes, the joint CAT/GAT meeting took place at the 2014 Winter Anaesthesia Weekend, in conjunction with the Irish Standing Committee of the AAGBI and the CAI. The two committees collaborated on various topics, mostly suggested by CAT. A GAT and CAT member discussed each in detail, and action points were drawn up. Anaesthesia News March 2015 • Issue 332 13 Society of Anaesthetists of the South West Region ANNUAL SPRING MEETING Start your summer early with a long weekend in the West Country Thursday, 14 May and Friday, 15 May 2015 Plymouth Postgraduate Medical Centre Derriford Hospital, Plymouth Study Days for 2015 Confirmed speakers Preoperative Cardiac and Respiratory Investigations 19 May 2015 ■ Dr J-P van Besouw, President, RCoA ■ Dr Ellen O’Sullivan, President, College of Anaesthetists of Ireland ■ Professor Adrian Furnham, Professor of Psychology, UCL and Sunday Times Columnist Cardiopulmonary Exercise Testing 20 May 2015 ■ Professor Rob Sneyd, Plymouth ■ Dr Rupert Pearse, London ■ Dr David Grant, Bristol Society Dinner at Royal Marines Officer’s Mess, Stonehouse For full details and to book your place, please visit www.pre-op.org or call 020 7631 8896. Location: AAGBI, 21 Portland Place, London Anaesthesia and Perioperative Care Anaesthesia nd Perioperative Anaesthesia and Sa Petting erioperative Care Care Priority Partnership Anaesthesia and Perioperative Care Priority Setting Partnership Priority Setting P artnership Priority Setting Partnership Over 3 million patients an anaesthetic Over 3 million patients h ave an haave naesthetic every year. e very year. research ould help improve care? Over What 3 mWhat pwatients hillion ave n acare? naesthetic every eyvery ear. rillion esearch ould help improve tatients heir Over 3w m pa have their an anaesthetic year. This famous piece of Irish poetry refers to Patrick Kavanagh’s birth place in Monaghan – the title betrays his negative emotions for his home county. Upon moving to the more enlightened and cosmopolitan Dublin, he reflected on the hardships of his youth, and the lost opportunities that stunted his development. Kavanagh lived the rest of his life, and died, in Dublin. Lost the long hours of pleasure All the women that love young men. O can I still stroke the monster's back Or write with unpoisoned pen. Stony Grey Soil – Patrick Kavanagh Delegate fees for both days including dinner Consultants: £210, Doctors in Training £120 A wide array of reduced fee options depending on your choice of sessions. Approved by the RCoA for 10 CPD credits. Enquiries to: [email protected]. For full programme and booking, please see: www.saswr.org. All of our study days are at a subsidised price of £75 for members and £99 for non-members. Challenges to the wellbeing of the Irish anaesthetic trainee i nitial in s2ummer 2014 a plmost roduced lmost r1sesearch 500 research uggestions. It’s now time to choose Our Our i nitial survey siurvey n summer 014 produced 1500 raesearch uggestions. It’s nsow time to choose What would h elp improve their care? What r esearch would h elp i–mprove tto heir cware? the m ost i mportant o nes. V isit o ur p rioritisation s urvey d uring F ebruary M arch 2 015 t ell u s hat the most important ones. Visit our prioritisation survey uring Falmost ebruary March 2015 to tIt’s ell nuow s twime hat Our i nitial survey in summer 2014 pdroduced 1500 –research suggestions. to choose summer 014 roduced 1500 esearch ssurvey uggestions. It’s n–ow time to to cthoose you Our think i nitial are the survey biggest ipn riorities for f2uture esearch. the mrp ost important aolmost nes. Visit our prrioritisation during February March 2015 ell us what you think are the biggest priorities for future research. you think are the biggest spurvey riorities d for future Frebruary esearch. – March 2015 to tell us what the for most important ones. Vsisit our prioritisation uring Vote your top 10 and help hape the future of anaesthesia and perioperative care Vote f or y our t op 1 0 a nd h elp s hape t he f uture o f a naesthesia nd perioperative care care Vote ffor or fyuture our top 10 and help shape the future of aanaesthesia and perioperative you think are the biggest priorities research. Vote at: http://www.niaa.org.uk/PSPSurvey#pt Vote at: http://www.niaa.org.uk/PSPSurvey#pt Vote at: hsttp://www.niaa.org.uk/PSPSurvey#pt Vote for your top 10 and help hape the future of anaesthesia and perioperative care For more information go to our website at http://www.niaa.org.uk/PSP#pt For more information go to our website at http://www.niaa.org.uk/PSP#pt For more information to our website at http://www.niaa.org.uk/PSP#pt Vote at: gho ttp://www.niaa.org.uk/PSPSurvey#pt For more information go to our website at http://www.niaa.org.uk/PSP#pt On a daily basis, my colleagues express similar (less poetic) commentaries on the Irish health system. The long hours, poor management, reduced pay, inadequate training are blamed for a malaise amongst Irish trainees. Similar to Kavanagh, a growing number are emigrating to greener pastures, leaving their country, their family, and their friends behind for a better life. An individual’s ‘wellbeing’ was probably a foreign concept in 1940s Ireland but, in his poetry, Kavanagh routinely catalogues the neglected elements of his own wellbeing. of wellbeing. An employer will successfully retain their workforce it they value and support their employees’ wellbeing. Wellbeing is determined by your physical, social and mental state.3 It depends on six domains (Figure 1). Everybody will have slightly different requirements to satisfy their wellbeing, but most people prioritise the domains of health, and relationships and care. The other four domains vary in significance depending on the individual. Figure 1 The concept of physician wellbeing is topical in modern Irish medicine. Our health system is in a deep recruitment and retention crisis. The Medical Workforce Report 2014, shows a worrying trend with another 10% of young doctors (under 30 years old) exiting medical practice in Ireland. Today, over 30% of our doctors have qualified in a non-EU country, compared to 7.4% in 2000.1 The specialty of anaesthesia has been affected by the medical exodus. Over half of the anaesthesia training graduates in 2014 have left the country, and an unprecedented number of consultant posts lie vacant in many anaesthetic departments. In 2006, the Fottrell Report made recommendations about the number of graduates required to staff our health system and ease our reliance on non-EU doctors.2 The numbers in Irish medical schools rose from 305 in 2007 to the target of 750 in 2011. This is a substantial increase in supply and yet we’ve never been so reliant on foreign doctors to support the system. This simple supply and demand strategy failed. Medical professionals expect reasonable working conditions and a meaningful life for themselves and their families. These basic elements are encapsulated in the principle Anaesthesia News March 2015 • Issue 332 The Committee of Anaesthesia Trainees (CAT) invited anaesthetic trainees to describe the most important factors that affect their wellbeing. Common themes emerged, with excessive working hours, staff shortages, sub-standard training, unfair pay arrangements and disrupted family life having a particularly negative impact. 15 Work and participation In 2013, Irish junior doctors went on strike over excessive working hours. The majority of doctors were not compliant with European Working Time Regulations (EWTR). In response to the strike, the Health Service Executive (HSE) committed to limit shifts to less than 24 hours by the end of 2013, and to be fully compliant by 2015. This has not happened. The CAT conducted a survey of EWTR compliance amongst anaesthesia trainees in November 2014 that showed 71% of trainees continued to work over 48 hours per week, and 37% of trainees work a shift in excess of 24 hours. The silver lining of our survey was the significant efforts made by the anaesthesia departments to implement more compliant on-call rotas, with 49% of trainees on alternative rotas. The excessive hours are taking a major toll on anaesthesia trainees. Many reported exhaustion and burnout in the survey, and they lacked confidence that the EWTR would be implemented appropriately by the HSE. A smaller survey of trainees assessed occupational stress, and 58% of trainee respondents scored as ‘high risk of burnout or mental health disorder’ due to work-related stress. Fifty percent felt their hours were excessive and prevented them from performing optimally. Democracy and values Kavanagh’s poem details all the principles he believed and trusted in, and how betrayed he felt when these values were challenged. A breach of trust and a perceived lack of fairness, can seriously challenge an individual’s wellbeing. In 2012, the HSE introduced a 30% pay cut to all new-entrant hospital consultants. This was an isolated pay cut for one group of public servants, in addition to all other cost containment measures introduced over the preceding six years. This has introduced an inequality between new and existing consultant colleagues, and has had a profoundly negative impact on recruitment. In July 2014, the HSE issued a directive to all HR departments to cut the salaries of middle grade anaesthesia trainees. This breach of contract resulted in a pay reduction of €10,000 for some trainees. Following threatened strike action, the HSE have postponed the introduction of these scales, but have committed to review trainee pay in 2015. These recent events have severely damaged trainee trust in their employer. Irish trainees who emigrate are often struck by the willingness of their foreign employers to honour the terms of their contract. Such a simple principle is challenged on a daily basis in Irish HR departments. Relationships and care Along with health, this is one of the key domains of our personal wellbeing. In one of our surveys, 72% of anaesthesia trainees said their workload affected their home, family or personal life on a regular basis. Our EWTR survey had a response rate of 90%, but only 1% of respondents (two trainees) were engaged in less than full-time training. From discussions with our GAT colleagues, we realise this is significantly less than the UK. Nearly half (45%) of Irish anaesthesia trainees are female, and we need to support familyfriendly initiatives to improve retention. The HSE are planning to introduce new proposals to improve the availability of less than fulltime options, job-sharing and couple-matching. When a trainee’s wellbeing is not valued by his or her employer, their health may suffer. In our occupational stress assessment, 44% of anaesthesia trainees reported feeling ‘emotionally, mentally or physically exhausted’ on a regular basis. It is not surprising that many trainees working in such a demanding system neglect their physical health. However, with the introduction of initiatives like the ‘Bike-to-Work Scheme’, more doctors are fitting physical exercise into their busy daily lives. What can we do? The CAT is committed to working with anaesthesia trainees and the College of Anaesthetists to improve the wellbeing of trainees. Our colleagues in GAT and at the AAGBI have a wealth of experience in the area of trainee welfare, and we look forward to learning from them as we collaborate on future projects. We have conducted two large national surveys, examining EWTR compliance and recruitment in intensive care medicine. The results of these surveys will be communicated to the relevant authorities and hopefully drive changes to improve trainee wellbeing. We have been working hard to establish and develop an Irish anaesthesia community. Our private Facebook page facilitates trainee discussion. We are currently developing a ‘Lead Anaesthetic Trainee’ network, similar to GAT’s Trainee Network Leads in the UK. The importance of a strong community was highlighted in 2014 following the trainee pay-cuts. The CAT wrote a letter to our medical union (IMO) requesting intervention and over 220 trainees signed this letter. This represented a very strong response that inspired the IMO to intervene, and successfully reverse the cuts. The AAGBI would like to offer a Patient Safety Prize to showcase examples of improved safety in anaesthesia. The prize is open to members of the AAGBI. The project could involve an individual, department, medical students or allied health care professionals, provided the project lead is a member of the AAGBI. Applicants may like to consider projects based on themes identified in SALG patient safety updates. You will need to demonstrate: Clear aims and objectives An innovative idea(s) How the project was introduced and implemented How performance was measured and benchmarked How information about the project was disseminated The sustainability of the project Transferability of the project to other departments The deadline for submissions is 23:59 on Friday 01 May 2015 Amount: Up to £500 (at the discretion of the awarding Committee). There may be more than one prize. Awarded: At the AAGBI Annual Congress, Edinburgh Format of submissions: Poster presentation In addition, the shortlisted entries may be expected to: Make a brief oral presentation to the judges at Annual Congress The winner will be expected to: Make a five minute oral presentation during the prize giving at Annual Congress Please visit www.annualcongress.org/content/aagbi-patient-safety-prize for further details. If you have any queries, please contact the AAGBI Secretariat on 020 7631 1650 (option 3) or [email protected] What can our employer do? Ultimately, we depend on our government and senior managers to implement the required changes. As a trainee committee, we can simply highlight problems, but have little power to fix them. Dramatic changes are required – that is certain. The government and the HSE need to respect the wellbeing of their employees, and not use them as simple commodities. As an Irish citizen, it’s demoralising to observe this ‘brain drain’. There is a long tradition of Irish medical professionals moving abroad, but the majority harboured ambitions to return home. This is no longer the case. Similar to Kavanagh, we must ask ourselves: ‘Can I still stroke the monster's back? Can I return to work in the Irish health system? Is there any remaining trust or optimism?’ These are vital questions, because the future of safe, high quality medical practice in Ireland depends on the answer. Dr David Moore Chair, Committee of Anaesthesia Trainees (CAT) Anaesthesia SpR 4, St James’s Hospital, Dublin References 1. 2. 3. Working Group on Undergraduate Medical Education. Medical Education in Ireland: A New Direction. Report of the Working Group on Undergraduate Medical Education. Dublin: Department of Health and Children; 2006. Humphries N, Tyrrell E, McAleese S, et al. A cycle of brain gain, waste and drain - a qualitative study of non-EU migrant doctors in Ireland. Human Resources for Health 2013 11: 63. http://www.human-resources-health.com/ content/11/1/63 National Economic and Social Council. Well-being Matters: A Social Report for Ireland. Volume 1. NESC Report No. 119. Dublin: NESC; 2009. http://files.nesc.ie/nesc_reports/en/NESC_119_vol_I_2009.pdf (accessed 19/1/2015). NASGBI 50TH Anniversary Annual Scientific Meeting Manchester 7-8th May 2015 Hilton Hotel, Deansgate, M3 4LQ Dealing with chimps in the clinical environment Prof Steve Peters Consultant Psychiatrist and Chief Psychologist Sky Pro Cycling Team Inflammation and Brain Injury: Discovery and Treatment Dame Nancy Rothwell President and Vice Chancellor, University of Manchester Delayed Neurological Deficit Prof Gabriel Rinkel University of Utrecht Extensive social programme to accompany the main event. Abstract Submission now open - Deadline: 6th March 2015 £300 Members / £350 Non-members / £150 Trainees. One day rate £150 / £200 www.nasgbi.org.uk Health 16 AAGBI PATIENT SAFETY PRIZE 2015 Registration now open Anaesthesia News March 2015 • Issue 332 @NASGBI #50thASM Year 2007 BRITISH SOCIETY OF ORTHOPAEDIC ANAESTHETISTS SPRING SCIENTIFIC MEETING SAS AUDIT POSTER PRIZE 2015 Thursday 04th June 2015 Etc.venues Maple House, 150 Corporation Street, Birmingham, B4 6TB Delegate Fees: Consultant Anaesthetist: £75 (BSoA members £70) Registrars / Specialty Doctors / PA(A): £55 (BSoA members £50) (See BSOA website for membership details) www.facebook.com/pages/The-British-Society-of-Orthopaedic-Anaesthetists Twitter: Ortho Gas Person, @Bsoa_org_uk Peri-operative Medical Care Speakers include: Dr W Chimbira, Michigan, USA Dr M Swart, Consultant Anaesthetist, Devon Dr W Lester, Consultant Haematologist Dr O Bagshaw, Consultant Anaesthetist Dr S Wharton, Consultant Respiratory Physician Dr K Patel, Consultant Anaesthetist Dr H Jones, Consultant Anaesthetist Mr M Phillips, PA(A) Lead HEFT Contact and Registration Information: (Application Form available from) Joanne McCaffery BSoA Meeting Administrator Email: [email protected] Phone: 07594 878 668 Anaesthetic Department The Royal Orthopaedic Hospital Bristol Road South Birmingham B31 2AP Attracts 5 CEPD points (applied for) Many of us will remember 2007 for the uncertainty of MMC and MTAS, but for me the stress came from my personal life. After passing my Primary exam I moved region for family reasons and felt like an outsider. I was pregnant with my first child and wasn’t shortlisted for an ST3 post; all quite worrying. The AAGBI invites abstracts for the SAS Audit Poster Prize. The prize is open to all SAS grade anaesthetists. A preliminary review of the abstracts received will determine which ones are accepted for poster presentation at the Annual Congress in Edinburgh. Prizes will be awarded to authors of the best posters and the abstracts will be published in Anaesthesia in the form of a fully referenceable online supplement (NB Editor-in-Chief reserves the right to refuse publication, e.g. where there are major concerns over ethics and/or content). The deadline for submission is 23:59 on Friday 01 May 2015 and full instructions can be found on our Annual Congress microsite: www.annualcongress.org/content/oral-posterpresentations If you have any queries, please contact the AAGBI Secretariat on 020 7631 1650 (option 3) or [email protected] It began with a bit of pain in the back of my neck. At first, I thought it was just a sprain or a pregnancy-related minor ache. But it gradually got worse, and soon I had to turn my whole body to look around. Being in the first trimester, I didn’t want to take any non-steroidals or opioids, and restricted myself to paracetamol, which was not very effective. I mentioned to my GP that my left carotid artery was more obviously palpable that the right; she put it down to muscle spasm and suggested physiotherapy. Three weeks and a few agonising physiotherapy sessions later, I noticed a swelling on the left side of my neck, which appeared to be getting bigger. I was referred to ENT who ruled out a branchial cyst, performed a needle aspiration and an ultrasound guided incision and drainage. Three weeks later, we had a result. Acid fast bacilli; I had tuberculosis. An urgent MRI provided the final diagnosis – tuberculous osteomyelitis of the cervical spine, with changes from C1 to D1 vertebrae, along with a large prevertebral abscess. Having a diagnosis was an immense relief after three months of pain, nausea and appetite and weight loss. But I still shudder when I remember what the TB nurse said ‘I know two patients with this condition in the lumbar spine, and they are both paraplegic’. For me it all resolved after nine months of treatment. In spite of everything, my pregnancy seemed to be progressing well, with good fetal growth. As I got better, I looked forward to the baby. I went into spontaneous labour and all was well until I had my epidural and an ARM, after which the CTG showed fetal decelerations. Delivery was expedited with ventouse, but the baby had severe meconium aspiration and had to be intubated. After 10 hours in SCBU, support was withdrawn and she died. The night she died, as I tossed and turned in bed, I could hear babies crying in the next room and wanted to run away, to escape the cruelty of it all. The following morning, a tactless anaesthetic registrar doing his follow up ward round asked me how the labour and epidural experience was. He didn’t know I had lost my baby. To me, this seemed very insensitive. The target: The AAGBI wants to raise £96,000 which will buy 600 Lifebox Pulse Oximeters over the next 2 years - the same as the number of Team GB athletes attending the Olympic and Paralympic Games in Rio de Janeiro in 2016. During the days that followed, the pain, shock and grief were unbearable, and I was an emotional wreck. Sleep deserted me, I could barely function in the day, and I refused to talk to anyone. But life had to go on, and I needed a job. I approached my college tutor, who arranged for me to return to an SHO job for a month. During this time, I was offered a LAT post. The aim: To save thousands of lives around the world where patients are at risk of death from hypoxia. Help us to reach the target! Join the campaign and become a Lifeboxes for Rio fundraiser Bake, bike ride, run or walk – or devise your own fundraising concept. From the employer’s perspective, I was a liability. I had been off sick, on maternity leave, and was emotionally fragile. Not the ideal candidate to take on the new responsibilities of the specialist registrar role. Six years and two delightful children later, I am now a final year trainee, and to this date, I remain grateful for their trust and kindness. www.aagbi.org/lifeboxesforrio AAGBI Foundation: Registered as a charity in England & Wales no. 293575 and in Scotland no. SC040697 Lifebox: Registered as a charity in England & Wales (1143018) Rio_Poster.indd 1 19/01/2015 10:31 Anaesthesia News March 2015 • Issue 332 Returning to work was hard. Although I was relatively new to the hospital, most people knew I had been pregnant, and the inevitable question was asked, ‘How is the baby?‘ or even ‘Why have you returned so soon?’ The people in the anaesthetic department knew everything and did not ask questions. Knowledge of the tragedy seemed to make it difficult for them to greet me, and some just avoided eye contact. I would have preferred them to talk to me. To paraphrase the lines of a famous poem: What is this life, if, full of care, we have no time to talk and share! My department provided practical support, and offered to change my rotation so I didn’t have to work in the maternity unit where I lost my baby. Working in the labour ward was never the same. I now visit any mothers awaiting delivery of an intrauterine death and help in any way I can, especially with pain relief. I found that keeping busy was the best way to cope with my loss. Staying at home just made me irritable, brooding and, worse still, insomniac. Focusing on other people’s problems made mine less stressful, and made me forget, if only temporarily. Dealing with a colleague who has had bereavement can be challenging, and it is crucial to try and get it right. Here are a few suggestions: Hints and tips • • • • • • Returning to the same place of work after bereavement is hard. Don’t avoid someone who has had a tragedy. Make eye contact when you see them. Send a card or email to say you know what’s happened and offer your sympathy. If you have suffered a stillbirth or neonatal death, people will ask ‘How’s the baby’ or ‘Why are you back so soon?’ Be prepared for this; give a brief answer and explain what you would find helpful from them now. It is normal to have flashbacks, to feel irritable, and to find it hard to sleep. Keeping busy by coming to work and focusing on other people’s problems can be helpful. Being alone at home makes some people feel worse. Practical support from the department is vital, e.g. helping them get back to work even on a part-time basis, ensuring they don’t work alone in case they feel wobbly, changing someone’s rotation so they don’t have to work in the unit where the bereavement occurred. Ask what would be helpful. People need company, even if they may not feel they do at the time. If you know them, offer to meet up. Gently encourage them to talk about events. If they’ve lost a child, ask them if they have a photograph. 19 NIAA National Institute of Academic Anaesthesia Director, UK Perioperative Medicine Clinical Trials Group The National Institute of Academic Anaesthesia (NIAA) wishes to appoint a Director to lead the development of a national Clinical Trials Group (CTG) for perioperative medicine, capable of supporting world-class multi-centre trials from idea to publication and dissemination. The postholder will be expected to develop a national network of hospitals and investigators to recruit to trials and develop and implement a transparent and robust process for identifying and selecting studies to be considered by the CTG. He/she will also need to engage the appropriate stakeholders in the project and work effectively with the NIAA and its founding and funding partners and trainee research networks. The post is a three-year, fixed-term appointment, subject to annual review. Further information about the NIAA, the job description, person specification and details on how to apply is available on the NIAA, RCoA and AAGBI websites. Closing date for applications: Friday, 1 May 2015 at 12 noon Shortlisted candidates will be contacted and interviews will be held on: Tuesday, 9 June 2015 Pain Foundation LIVERPOOL COURSE ON CLINICAL MANAGEMENT OF CHRONIC PAIN : A PRACTICAL APPROACH Limited to 30 participants RCoA CPD Matrix 2E03 and 3E00 FEE £450 (Register after 2nd May 2015 £500) All delegates will receive a complimentary copy of the handbook ‘Practical Management Of Complex Cancer Pain’ Demonstration Joint Pain Clinics • Imaging for Spinal Interventions • Cancer Pain Management • CRPS Management • Neuromodulation • Pain Management Programme • Demonstration Theatres • Hands on Manakin Spinal Injection • Ultra Sound Guided Pain Interventions • Botox Injections and Capsaisin Patch Application • Physiotherapy Assessment and External Neuromodulation Contact: Mrs Brenda Hall, Pain Relief Foundation, Clinical Sciences Centre, University Hospital Aintree, Lower Lane, Liverpool L9 7AL UK. Tel +151 529 5822 [email protected] www.painrelieffoundation.org.uk Registered Charity Number: 1156227 Anaesthesia News is always looking for articles of relevance to trainees. As recently elected members to the committee we thought it might be interesting to give an account of our first few months on the committee. Perhaps naïvely, we didn't quite appreciate the breadth of trainees’ involvement in AAGBI activity and it has been a busy, but rewarding, six months so far. For most of us, our first experience of an AAGBI meeting was the Joint AAGBI Board and GAT Strategy meeting in Newcastle. We got straight into discussing the objectives for GAT during 2014/15. Even from the very beginning our opinions were sought and considered, and we were made to feel part of the team. Of course it is by design that the newly elected members join the committee at the ASM. It was useful to attend the meeting, not only because it is full of great educational content (and very good value for money!) but also because it is a great chance to get to know fellow committee members and learn about how a major medical conference is run. Relief 2ND TO 4TH JULY 2015 An advanced practical course in clinical pain medicine for Pain Professionals and Trainees aiming to further develop skills of assessing and treating complex chronic pain patients, specialists and pain specialists in training. Joining the GAT Committee: the first six months In association with The Walton Centre for Neurology & Neurosurgery NHS Foundation Trust Meetings Our first face-to-face meeting was in September 2014. GAT committee members are offered the opportunity to do an Advanced Management Module and part of each committee meeting is set aside to address some of these learning objectives. In line with this we take turns to chair our own committee meetings. This is a new skill for most of us and, as is often the case when doing something new, has been associated with varying degrees of apprehension. This has been eased with excellent chairing resources form senior council members, and plenty of support from fellow committee members! A buddy system to link each GAT committee member with an AAGBI council member has also been developed so we have someone to turn to for additional advice if necessary. We have now had several other meetings; including a joint meeting with the Trainee Committee of the College of Anaesthesia News March 2015 • Issue 332 Anaesthetists of Ireland in Dublin. Although we discuss many issues by email, we are learning fast how useful it is to have a faceto-face discussion where ideas can develop. Recurring themes at our meetings are education (in particular the GAT ASM and seminars), communication, reports from our co-opted members (the RCoA, BMA, CAI and the military) and any external meetings at which we represent GAT. We normally have at least a couple of members teleconferencing in or on Skype and we are learning to make sure we include those members as much as possible. It is often easier to discuss ideas in a less formal environment, so we make sure there is time to chat outside of the meeting itself. With so many new members in the committee this is an important part of getting to know one another, providing valuable peer-support and improving our ability to work as a team. External representation As well as our internal committee meetings, some of us represent GAT at external meetings such as the series of Shape of Training workshops that were held across the country. We are also due to represent anaesthetic trainees at a RCoA Perioperative Medicine Stakeholder event and a NIAA meeting to improve trainee access to research. Before attending meetings like these we canvas the opinions of the whole committee, helping the person attending to give a balanced view. Following any meeting we attend, we prepare a report to share with the GAT committee, often done on the train journey home! All meeting documents and reports are shared via Dropbox, which we are fast becoming experts at navigating. 21 Committee work Other opportunities Members of the GAT committee are actively involved in many AAGBI and external committees. Since joining in June we have been representing anaesthetic trainees on a number of key issues: • Commenting on the government’s response to the Review of the Impact of EWTD in the NHS (a letter was sent to the Rt Hon Jeremy Hunt) • Health Education England Workforce planning call for evidence and a survey by the European Commission on the impact of the EWTD (we contributed to the AAGBI response) • Providing trainee evidence for a response to the Doctors and Dentists Review Board on contract negotiations • The Shape of Training Review and how we should respond to and engage with the Steering Group • Improving links with medical students and trainee research networks • Provided input to the AAGBI members’ survey • Options for locations for future GAT ASMs (Manchester in 2015 and Nottingham in 2016) • Potential topics and articles for the GAT issue of Anaesthesia News, (we decided on a Wellbeing theme – look out for it in June) and a trainee session at the 2015 AAGBI Annual Congress (Edinburgh) In addition to everything we’ve mentioned so far, we have been involved in many other projects. We have contributed to the National Essential Anaesthesia Drug List and will help edit future editions of publications such as the GAT Handbook. We have also been asked to participate in working parties, to be on National Organising Committees for conferences, and to provide trainee representation on bursary and awards panels. Thankfully we have a diverse range of interests and skills between us and the work seems to be naturally shared according to these. Sometimes it has been difficult to know exactly what the right answer is and how best to comment. However, the point of being on the committee is to consider different viewpoints, and it is through discussion that we get to know each other better and find a way forward. In addition to the GAT committee emails, we also receive emails from the other committees we sit on. Some of these generate more email traffic than others and something we are all learning from being on the committee is time-management and the effective management of large volumes of emails. Impression so far So we attend meetings and send a lot of emails. What is it all for? This is probably a good moment to reflect on whether being on the GAT committee is meeting our expectations? Thinking back to our nomination statements we all identified various issues and mentioned how we wanted to make things better for our fellow anaesthetists and this is what we as a committee are trying to do. Be it via education, promoting peer-support or our more political activities, it all comes down to helping anaesthetists to do their job as well as they can. So yes, this meets our expectations. Perhaps what we didn’t realise was the extent of trainees involvement in the AAGBI. This was probably naïve as, after all, trainees make up a third of the membership. We have learnt that although the range and breadth of GAT and the AAGBI activities are wide, the overall aim is simple: to make anaesthesia as safe as possible. This needs not only safe and effective anaesthetists who are knowledgeable and adequately rested, but also safe and effective systems for them to work with. What about the amount of work involved? Having written it all down, it does seem like rather a lot. However, the work is interesting and feels worthwhile and the volume of it is made easier by us all working as a team and the support of the AAGBI staff. As already mentioned, at times it can feel daunting. At the beginning we all felt under-prepared and often like we had Imposter Syndrome, however this has lessened as we have become more involved. We have all thrown ourselves into our roles with the support of our fellow GAT committee and AAGBI council members. It is an amazing privilege to represent our colleagues and to meet like-minded colleagues who want to make a difference. We have lots to learn from each other, as well as from the inspirational leaders in our field, and it has been eye-opening to discover what goes on outside the hospital in the world of anaesthesia. We are only six months in so perhaps it is a bit early to say, but would we recommend it? Definitely. If you would like to join the GAT Committee, nominations are open and close on Friday 10 April at 17:00. Please see page 7 for more information. Although it may seem like lots of work, there is also time to talk about other events in our lives. We all recognise the importance of our lives outside of work. Many of us have young children and in the last six months there have been two additions to the families of committee members. 22 Emma Plunkett, ST6, Birmingham School of Anaesthesia Phil Bewley, ST3, Bristol School of Anaesthesia Anna Costello, ST7, Oxford School of Anaesthesia Sally El-Ghazali, ST3, Imperial School of Anaesthesia Rowena Clark, ST6, South East Scotland School of Anaesthesia Lyndsey Forbes, ST4, Tayside School of Anaesthesia Surrah Leifer, ST6, North West School of Anaesthesia Digested March 2015 Cranial nerve injuries with supraglottic airway devices: a systematic review of published case reports and series Thiruvenkatarajan V, Van Wijk RM, Rajbhoj A. Cranial nerve injuries are unusual complications of supraglottic airway use, and may well occur but go unrecognised or misdiagnosed as they are so uncommon. The authors of this review took great pains to seek out and collate case reports and case series of cranial nerve injuries associated with the use of supraglottic airway devices. They found that lingual nerve injury was the most commonly reported (22 patients) followed by recurrent laryngeal (17 patients), hypoglossal (11 patients), glossopharyngeal (three patients), inferior alveolar (two patients) and infraorbital (one patient). Although information on the mechanism of injury was not presented in many of the reports, it was often usually thought to be due to pressure neuropraxia from either the cuff or the shaft of the device. Injuries to most of the nerves are usually mild and self-limiting, but recurrent laryngeal nerve injuries could be much more serious, sometimes presenting with respiratory distress. Contributing factors to injury may include an inappropriate size or misplacement of the device and too high a pressure in the cuff of the device. The authors go on to suggest that cranial nerve injuries may not be completely preventable and should not always be assumed to represent sub-standard care. Nevertheless, it seems sensible to limit cuff pressure to a maximum of 60 cm H2O, use a gentle insertion technique and correct misplacement promptly. The impact of autonomic dysfunction on peri-operative cardiovascular complications Lankhorst S, Keet SWM, Bulte CSE, Boer C. Even for anaesthetists, to whom the autonomic nervous system is more familiar than many doctors, it is still the poorly understood relation of the somatic nervous system. This narrative review examines the possible anaesthetic implications of autonomic neuropathy. Cardiovascular autonomic neuropathy is frequently observed in patients with diabetes mellitus. As a lead-in to exploring the relationship between such neuropathy and possible complications, the authors first describe commonlyused tests of autonomic function. The most frequently used seeks abnormalities of heart rate variability measured at rest for 5 min or 24h. There are different frequency bands within heart rate variability, reflecting sympathetic and parasympathetic activity differently. The authors suggest that, depending on the type of anaesthesia, the presence of cardiovascular autonomic neuropathy in surgical patients can markedly affect perioperative haemodynamics and postoperative recovery. However, there are few data to support the use of a particular drug regimen or anaesthetic technique in this regard. Nevertheless, it may well be beneficial to use preoperative testing of the extent of autonomic dysfunction in particular patients, such as diabetics, as this would then allow more careful handling and greater cardiovascular support for patients who might be more prone to haemodynamic instability. Defining and developing expertise in tracheal intubation using a GlideScope® for anaesthetists with expertise in Macintosh direct laryngoscopy: an in-vivo longitudinal study Cortellazzi P, Caldiroli D, Byrne A, Sommariva A, Orena EF, Tramacere I. There are some existing studies that suggest that the number of attempts at videolaryngoscopy needed to achieve competence is in single figures. This paper complements such work by posing a slightly different question; how many attempts does it take to become expert? The authors observed the performance of nine trainees during 890 intubations, with an additional 72 intubations performed by expert anaesthetists used as a control group. Statistical techniques were used to search for potential predictors of successful intubation and define the number of intubations necessary for a trainee to achieve expertise. Herein lies one of the central problems of such work – defining what is meant by ‘expertise’. The authors defined this by specifying a greater than 90% probability of optimal performance. They found that it took 76 intubations to achieve this likelihood of success, but also noted the limitations of a simple measurement of success rate: ‘The suggestion is that expertise cannot be equated to a single, successful completion of a complex task, but rather that expertise is demonstrated by such outcomes as speed, accuracy, lack of excessive force, lack of complications, a subjective rating of competence and, most importantly, a high success rate over a prolonged period.’ So there’s more to it than simply ‘getting the tube through the cords’! N.B. the articles referred to can be found in either the latest issue of Anaesthesia or on Early View (ePub ahead of print) Anaesthesia News March 2015 • Issue 332 A.F. Smith Editor, Anaesthesia SAFETY MATTERS Safety point: needlestick injuries Here’s another pearl for you to reflect upon and consider how safe your own practice is. In December 2014, the AAGBI Safety Committee found itself consulting the Health and Safety (Sharp Instruments in Healthcare) Regulations 2013.1 This little bit of legislation was needed to implement aspects of the European Council’s ‘Sharps Directive’ 20102 that were not specifically addressed in existing UK law, which you can find at the Control of Substances Hazardous to Health website.3 It is only six pages and deserving of 10 minutes of your time. It reminds us that your employer has a duty of care to you and your co-workers to make your working environment as safe as is ‘reasonably practicable’ (they like that formulation). The principles to delivering that objective are sensible, and the most obvious is not to use sharps when a blunt instrument will do, for example drawing up drugs or taking blood from an arterial line port. A close second comes the advice to use ‘safer sharps’ whenever possible. I have to admit that I still prefer the traditional unsafe needle, and I am going to have to reflect carefully on that over the weekend. The Regulations say that if a suitable safer sharp is not available to reduce the risk of injury, the employer should ensure that safe procedures for working with and disposal of the sharp are in place. The specific question that the Committee was contemplating was whether a ‘human tourniquet’ to help us put up a drip in the anaesthetic room is a safe procedure. I was a little surprised to see that the Royal College of Nursing have a Tourniquet Standard,4 and that it equally recommends singleuse disposable non-latex pinching bands, or multiuse potentiallycontaminated single-handed release tourniquets. This illustrates the point that a risk-assessment precedes each venepuncture. The RCN Standard makes no mention of the human tourniquet, which is clean (gloves or decontaminated hands) and atraumatic (vulture nails aside), as well as reassuring and kind. I have reflected; I am going to change my practice to safer sharps whenever a colleague is being kind enough to squeeze the patient’s arm. How about you? Tom Woodcock Chair, Safety Committee References 1. Health and Safety (Sharp Instruments in Healthcare) Regulations 2013. www.hse.gov.uk/pubns/hsis7.htm (accessed 19/1/2015). 2. European Council Directive 2010/32/EU. http://eur-lex. europa.eu/legal-content/EN/TXT/?uri=CELEX:32010L0032 (accessed 19/1/2015). 3. Control of Substances Hazardous to Health. http://www. hse.gov.uk/coshh/ (accessed 19/1/2015). 4. Standards for infusion therapy. Royal College of Nursing, 2010. p. 22. http://www.bbraun.it/documents/RCNGuidlines-for-IV-therapy.pdf (accessed 27/1/2015). 24 Ephedrine or suxamethonium? Figure 1. Only connecting: extra vigilance is needed during a period of transition A box of ephedrine ampoules had been mistaken for suxamethonium and placed in the fridge alongside two other boxes of suxamethonium. Due to the similar packaging and the storage location, it would have been very easy to mistake the ephedrine for muscle relaxant, particularly if tired, or reaching for the drug ‘in anger’. • A 71-year old lady died of air embolism after the inflating tube of an automated blood pressure cuff was connected to her intravenous catheter • A child died of pneumonia after an enteral feeding supply was connected to her tracheostomy tube • An expectant mother died after her enteral feeding solution was given intravenously These awful events, occurring in various countries around the world, have inspired work by the International Organisation for Standardization (ISO) to develop global standards for non-Luer small-bore connectors which, hopefully, will prevent such tragedies in future. The work of the National Patient Safety Agency’s External Reference Group on Neuraxial Devices has been passed on to NHS England, who have convened the Small Bore Connector Clinical Advisory Group under the Chairmanship of Dr Paul Sharpe (Consultant Anaesthetist in Leicester). ‘Neuraxial connectors’ is now just one of several fields of practice that Dr Sharpe’s group are advising on. The list is the 80369 International Standard series to introduce new designs for small-bore connectors: • • • • • • Part 1: Is the introduction to the standards listed below Part 2: Connectors for breathing systems and driving gases; Part 3: Connectors for enteral applications; Part 4: Urinary collection Part 5: Connectors for limb cuff inflation applications; Part 6: Connectors for neuraxial applications; • Part 7: Connectors with 6% (Luer) taper for intravascular or hypodermic applications. While working a night shift in the local emergency theatre, we noticed the drug arrangement in our anaesthetic room fridge as shown in Figure 1. Paul Sharpe Chair, Small Bore Connector Clinical Advisory Group Anaesthesia News March 2015 • Issue 332 The concept of ‘involuntary automaticity’ or ‘seeing what we expect to see’ is well documented within human factor and patient safety documents, and to reduce the incidence of these actual or potential drug errors we feel we should work with the pharmaceutical companies to help us achieve this and so improve patient safety. After circulating details of this ‘near miss’ to colleagues in our department to ensure vigilance, a senior colleague shared his own image (Figure 2) of drug boxes he found placed next to each other in a theatre anaesthetic machine drawer. Tom Woodcock Chair, Safety Committee We write to you to highlight this potential for drug error and the subsequent disastrous consequences of not administering muscle relaxant in a rapid sequence induction and instead injecting a high concentration of ephedrine. It also raises again the question - should we insist on better differentiation in the packaging of agents used in clinical practice so as to ensure a reduction in human factor drug errors? NHS England and the Clinical Advisory Group support the introduction of devices with ISO design connectors, so that medical devices used in the UK are harmonised with those used in other countries, and there is a controlled connector design standard process to minimise the risk of cross connection of devices intended for different clinical applications. There is, however, a transition period when such changes occur during which we can expect difficulties to arise. Some devices, like enteral giving sets and feeding tubes, will have short transition periods. Other ‘legacy’ devices, like anaesthetic machines, will pose challenges for several years. Anaesthetists are often safety experts and champions in their Trusts and organisations, so we urge you to do your bit in rolling out the essential connector changes safely. The Small Bore Connector Clinical Advisory Group plans to publish information and updates on the NHS England website, which we encourage you to follow (http://www.england.nhs.uk/ourwork/patientsafety). We will also be pleased to receive your reports of problems that arise at your place of work. Please contact the Clinical Advisory Group by email ([email protected]). Figure 2. Dr Gemma Phillips ST4 Anaesthesia Dr Haitem Maghur Consultant Anaesthetist Dr Mike Oliver Consultant Anaesthetist University Hospital of Wales, Cardiff CA AB LL STR FO AC R TS Abstracts for presentation at Annual Congress Edinburgh 2015 You are invited to submit an abstract for oral (free paper) or poster presentation at the Annual Congress. The deadline for submission is 23:59 on Friday 01 May 2015 and full instructions can be found on our Annual Congress microsite: www.annualcongress.org/content/oral-poster-presentations After the deadline, a preliminary review of the abstracts received will determine which ones are accepted for presentation at the Annual Congress in Edinburgh. Some authors will be invited to present their work orally, under the following three categories: audits and surveys, case reports, and original research. The remaining successful authors will be invited to present a poster. All accepted abstracts will be published in Anaesthesia in the form of a fully referenceable online supplement (NB Editor-inChief reserves the right to refuse publication, e.g. where there are major concerns over ethics and/or content). Authors of the best poster(s) will be awarded ‘Editors’ Prizes’. If you have any queries, please contact the AAGBI Secretariat on 020 7631 1650 (option 3) or [email protected] Dear Editor I use the RCoA CPD matrix as supporting documentation at appraisal, and find the AAGBI listing the appropriate codes in its event material extremely useful in keeping it up to date. However, in the Harrogate Annual Congress programme I noticed the educational equivalent of salami publication is creeping in, with the use of multiple codes, some only tenuously relevant to the lecture delivered. The worst offender (you know who you are) suggested 14 codes for an hourlong lecture! When I have to decide for myself, I usually only enter each event under a single code, with a possible second. I would like to suggest that a maximum of four codes for any individual presentation will be more than sufficient – otherwise it gets extremely tedious (and increasingly meaningless) for those of us trying to keep our CPD matrix up to date. Hilary Aitken Consultant Anaesthetist, Paisley Dear Editor Having worked for a considerable time in Africa, I read Professor Fenton’s article1 with great interest and agreement. However, there was no mention of the Glostavent machine which has most of the desirable features he mentions, and has been in use in many countries for over a decade. A serious comparison of the two machines would be interesting and helpful. He also did not name Professor Mackintosh’s EMO machine, which is still in use in many African hospitals though, sadly, I understand that production has now stopped due to lack of demand. Not only is this a robust, simple and safe machine, ether, though denigrated, remains a very safe and effective anaesthetic! Tuppin Scrase Volunteer Lecturer at the School of Anaesthesia, St Mary’s Hospital, Lacor, Gulu, Uganda No conflicts of interest declared Reference 1. MINATIONS CALL FOR NOEL ECTIONS 2015 BOARD/COUNCIL Nominations are now invited from members of the Association wishing to stand for election. Further information and nomination forms are available from the AAGBI secretariat on 020 7631 1650 (option 3), [email protected] or can be downloaded from the AAGBI website www.aagbi.org/about-us/council your Letters Matrix codes Fenton PM. Designing an International Anaesthesia Machine. Anaesthesia News 2014, 325: 13–15. Dear Editor Professor Fenton raises some important issues in his article,1 but I am not convinced. We have six operating theatres and an eight bed ICU in a very remote area of northern Uganda where we are continually challenged by loss of electricity, limited funds, a large workload and few skilled staff. We have one Manley Multivent still performing after 10 years and five Diamedica Glostavents. Dr Manley’s brilliant vision and design for the Manley Multivent, a machine driven by an oxygen concentrator, lives on in the Diamedica Glostavent. The machine can be used both in the ICU and theatre. Peri-operative and postoperative ventilation is now a necessity in any of the referral hospitals even in resource limited countries.2 Its simplicity facilitates the training of non-physician anaesthetists to assist respiratory support in intensive care. It has an excellent track record and after sales service, truly remarkable for Africa. Raymond Towey Consultant Anaesthetist, Department of Anaesthesia, St Mary’s Hospital, Lacor, Gulu, Uganda No conflicts of interest declared SEND YOUR LETTERS TO: The Editor, Anaesthesia News at [email protected] Please see instructions for authors on the AAGBI website Dear Editor Dear Editor ‘Faulty, beyond economic repair, only for Africa’ I am pleased to reply to the three responses to my article from August 2014.1 I would like to add to Professor Fenton’s article.1 During my time working as a volunteer anaesthetist in East Africa, a fair proportion of general anaesthesia was provided with demand flow draw-over vapouriser apparatus. I was impressed by its reliability and simplicity; however I also came across many continuous flow, compressed gas dependent machines. With the exception of a small number of government hospitals where use of continuous flow machines was appropriate, the remainder of the healthcare system was ill-equipped for its safe use. Many such machines were donated with faults either present prior to donation or new faults that could not be rectified locally within the existing infrastructure, making them effectively unrepairable. Some continued to be used despite their faults. This donation of anaesthesia equipment is not only unsafe, it is a waste of money, environmentally unfriendly, producing an anaesthesia machine graveyard that should stop. In one major hospital in East Africa, I saw an entire corridor of disused anaesthesia machines, defunct diathermy machines and a redundant radiology C-arm. I was embarrassed to find tagged onto one such anaesthesia machine an original label from the medical engineering department of a NHS hospital which read ‘faulty, beyond economic repair, only for Africa’. Africa deserves better than second user, faulty, end of life kit that our NHS departments no longer need. One low income country procured over 100 new compressed gas dependent anaesthesia machines, effectively useless in operating theatres with neither a reliable electrical power supply nor compressed gas. It is difficult to follow the decision making process that led to this contract being placed using high level international money on which interest will be charged. Gradian Health (UAM) and Diamedica (Glostavent) should be credited for the good work they do to support the speciality of anaesthesia in the developing world. In the event of electrical power / UPS battery failure and nonavailability of compressed gas, their machines can still provide anaesthesia vapour in both spontaneous ventilation and IPPV modes with atmospheric air used as the carrier gas. A critical safety feature needed for operation in the developing world. The after sales support is of a very high standard, with both manufacturers genuinely interested in how their machines perform locally. In one instance, a fault was reported on a Friday afternoon and, after a weekend of exchanging emails, an in-country technician was dispatched on Monday morning to a rural area of the country 6 hours’ drive away. The machine was repaired that same afternoon. Contrast this with the large multinational companies who have no further involvement once the ink has dried on the cheque. Moiz K. Alibhai Locum Registrar in Anaesthesia, Royal Liverpool University Hospital No conflicts of interest declared Reference 1. Fenton PM. Designing an International Anaesthesia Machine. Anaesthesia News 2014, 325: 13–15. References 1. Fenton PM. Designing an International Anaesthesia Machine. Anaesthesia News 2014, 325: 13–15. 2. Towey RM, Anyai JB. Intensive care medicine in rural sub-Saharan Africa - who to admit? Update in Anaesthesia 2012; 28: 18–21. www.wfsahq.org/archive-update-inanaesthesia/update-in-anaesthesia/update-028/download (accessed 28/9/2014). Closing date is Friday 10 April 2015 at 17:00. Please note: Several of these letters were edited after initial submission Anaesthesia News March 2015 • Issue 332 Ray Towey, a respected colleague, writes from Lacor Hospital, Gulu, which I knew from the 1980s. Though located in a poor and remote part of Africa it was then, and remains today, a well-supported and rare centre of excellence where equipment is kept in service much longer than the African norm. His perspective on anaesthesia equipment design (which he admits is ‘for me’) is not necessarily shared by anaesthetists elsewhere in Africa, and especially not in Asia. He commends his preferred brand of machine but that choice takes no account of the ever-increasing burden of obtaining ISO and CE compliance and manufacturer’s insurance liability cover, all needed if an anaesthesia machine is to achieve my stated aim of equivalence between Europe, North America and the rest of the world. Dr Alibhai observes the uselessness of second-hand anaesthesia machine donations, and cautions against loan-funded purchase of machines which require a reliable electrical power supply and compressed gas to function. His poor opinion of placing such machines in hospitals without such resources is shared by most anaesthesia professionals. He points out the importance of a speedy repair service, using locally available technicians and spare parts and I thank him for mentioning the good service he experienced with one UAM in his care. Dr Scrase suggests that a comparison of the UAM and the Glostavent would be helpful and that we should not forget the EMO. The aim of my article was to stimulate interest in a generic demand-flow system, accredited for worldwide use, not to compare one machine with another. It was written independently, out of personal conviction and a passion for the concept which existed long before Gradian existed or any machine was made. Ether is an excellent and life saving agent. I have previously written about its virtues2 and used it continuously for over 15 years, when it was available. It is safer than more modern agents for certain situations. However, it is almost unavailable today and thus the EMO has effectively passed into the history books, except where used as a door stop. Finally, I should add that, following editing, the final printed version of my article differed somewhat from the original. Paul Fenton 1. Fenton PM. Designing an International Anaesthesia Machine. Anaesthesia News 2014, 325: 13–15. 2. Fenton P. An epitaph for di-ethyl ether (1846-2009). World Anaesthesia News 2009; 11: 3–4. http://www.aagbi.org/sites/default/ files/WA11.1july2009.pdf (accessed 19/1/2015). 27 Particles Myles PS, Leslie K, Chan MT et al. Peake SL, Delaney A, Bailey M et al. (on behalf of the ARISE Investigators) Olsen F, Kotyra M, Houltz E, Ricksten S-E The safety of addition of nitrous oxide to general anaesthesia in at-risk patients having major non-cardiac surgery (ENIGMA-II): a randomised, single-blind trial Goal-directed resuscitation for patients with early septic shock Bone cement implantation syndrome in cemented hemiarthroplasty for femoral neck fracture: incidence, risk factors, and effect on outcome The Lancet 2014; 384: 1446–54 Background Nitrous oxide is a commonly used anaesthetic agent which is known to increase risk of postoperative nausea and vomiting, although concerns relating to increased risk of postoperative cardiovascular complications remain unclear.1 The original ENIGMA study observed a non-significant increase from 0.7% to 1.3% (p = 0.26) of ischaemic cardiac complications within 30 days of surgery, with a follow up study finding a significant increase from 4.5% to 6.4% (p = 0.04) of late myocardial infarction.2,3 Despite these findings the ENIGMA study was not designed to monitor for cardiovascular complications and was therefore underpowered to draw these conclusions. This study aimed to establish whether addition of nitrous oxide to an anaesthetic gas mixture increases occurrence of death and cardiovascular complications in at-risk patients undergoing non-cardiac surgery. Methods A randomised, single-blind trial was undertaken with data collected prospectively from 45 centres across ten different countries between May 2008 and September 2013. Inclusion criteria included adults at least 45 years of age, receiving general anaesthesia for non-cardiac surgery expected to last more than two hours in duration. Participants also had to be at risk of cardiovascular complications, which included a history of coronary artery disease, heart failure, cerebrovascular disease, peripheral vascular disease or be greater than 70 years of age with other comorbidities. Any patients in whom supplemental intraoperative oxygen was expected (such as those requiring one lung ventilation), at high risk of postoperative emesis or with significantly impaired gas exchange were excluded. Patients were randomised to receive a carrier gas mixture of either 70% nitrous oxide with 30% oxygen, or 30% oxygen in air, to ensure that all participants were exposed to equal intraoperative inspired oxygen concentrations. The primary outcome measure was a composite of death and cardiovascular events (non-fatal myocardial infarction, cardiac arrest, pulmonary embolism and stroke) within the first 30 postoperative days. Results From 10,102 eligible patients, 7112 were enrolled and randomised to the study, with 3543 assigned to receive nitrous oxide and 3569 assigned to not receive nitrous oxide. Of these, 6992 patients were assessed for the primary outcome measure. The primary outcome occurred in 283 (8%) patients receiving nitrous oxide and in 296 (8%) patients not receiving nitrous oxide (relative risk 0.96, 95% CI 0.831.12; p = 0.64). A tertiary outcome measure of severe nausea and vomiting occurred in 506 (15%) patients receiving nitrous oxide and 378 (11%) patients not receiving nitrous oxide (p < 0.0001). Discussion The ENIGMA-II study demonstrates that in patients having general anaesthesia for major non-cardiac surgery, the addition of nitrous oxide to the gas mixture does not affect the risk of death and major cardiovascular complications. In findings consistent with previous studies, administration of nitrous oxide has again been shown to put patients at increased risk of severe postoperative nausea and vomiting, although results suggest reduced symptoms in those that received prophylactic antiemetics. Despite this, nitrous oxide is best avoided in those at high-risk of postoperative nausea and vomiting. New England Journal of Medicine 2014; 371: 1496–1506 Background Early-goal directed therapy (EGDT) has been promoted for severe sepsis since the publication of Emanuel Rivers’ landmark paper in 2001,1 despite subsequent controversy regarding the study’s methodology and interpretation. The ARISE (Australasian Resuscitation in Sepsis Evaluation) study is one of three large international, randomised controlled trials that aim to determine if providing EGDT reduces mortality compared to ‘usual care’ for adult patients with septic shock. Methods The study was a multicentre (51 hospitals, predominantly in Australia and New Zealand), unblinded, intention-to-treat, equally-randomised control trial. Patients presenting with septic shock (infection, two or more SIRS criteria, and refractory hypotension) were enrolled to receive either EGDT or ‘usual care’. ‘EGDT’ included insertion of arterial and central lines, ScvO2 measurement, and the use of oxygen, mechanical ventilation, vasopressors, fluids and red-cell transfusions to achieve pre-defined physiological targets. The primary outcome was all-cause mortality at 90 days; secondary outcomes included length of stay (in ED, ICU and the hospital), and the need for organ support. British Journal of Anaesthesia 2014; 113: 800–6 Background Bone cement implantation syndrome (BCIS) is a well-known and potentially fatal complication of orthopaedic surgery. It is characterised by hypoxia, hypotension, arrhythmias, pulmonary hypertension, and loss of consciousness occurring around the time of bone cementation. It is most often seen in cemented hemiarthroplasty but also occurs in total hip replacement and knee replacement surgery. The pathophysiology of BCIS is not fully understood, but it may be caused by pulmonary embolisation, complement activation, and release of histamine. These may act together to increase pulmonary vascular resistance causing ventilation/perfusion disturbances with hypoxia, right ventricular failure, and cardiogenic shock. Aims This study aimed to estimate the incidence of BCIS in cemented hemiarthroplasty for hip fractures using a severity classification recently proposed by Donaldsson and colleagues: Results 1600 patients were enrolled; 796 received EGDT and 804 received ‘usual care’. Baseline characteristics (age, APACHE II score, site of infection, initial lactate, time to first dose of antibiotics) were very similar between groups. At 90 days, there was no significant difference in mortality between the EGDT and usualcare groups (18.6% vs 18.8%, p = 0.90). Patients in the EGDT group received greater volumes of IV fluid, and more vasopressors, red-cell transfusions and dobutamine (p<0.001 for all comparisons). There were no significant differences in length of ICU or hospital stay, in-hospital mortality, or duration of organ support. Grade 0 No BCIS Grade 1 Moderate hypoxia (arterial oxygen saturation < 94%) or hypotension (decrease in systolic arterial pressure > 20%) Grade 2 Severe hypoxia (arterial oxygen saturation < 88%) or hypotension (decrease in systolic arterial pressure > 40%), or unexpected loss of consciousness Grade 3 Cardiovascular collapse requiring cardiopulmonary resuscitation. Conclusion The authors conclude that for adult patients presenting with early septic shock, EGDT does not reduce all-cause mortality at 90 days. Methods A total of 1016 consecutive patients were included. Data on non-invasive systolic blood pressure, heart rate, and arterial oxygen saturation was recorded every 5 minutes. This data was obtained from anaesthetic charts and used to calculate the BCIS score. Medical history and medications were also determined from charts. Discussion This is a large, appropriately powered and well-executed multicentre trial with a sound methodology. Data for the primary outcome was available for 99% of patients, and it specifically addressed the EGDT algorithm described by Rivers in 2001. Along with the ProCESS study2 published in May 2014, this paper adds to the growing weight of evidence against EGDT in severe sepsis. The third large multicentre randomised-control trial into EGDT (ProMISe) is expected to be published in December 2015. Dr Liam P Scott CT2b Cheltenham General Hospital References 1. Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. New England Journal of Medicine 2001; 345: 1368–7. 2. Yealy DM, Kellum JA, Huang DT, et al. A randomised trial of protocolbased care for early septic shock. New England Journal of Medicine 2014; 370: 1683–93. Results BCIS was a commonly occurring phenomenon in the group of patients studied, with an incidence between 25% and 30%. Mortality in Grade 1 BCIS was not different to Grade 0 (p < 0.15). Severe BCIS (Grades 2 or 3) occurred in 5–7% of the patients and was associated with a significant increase in mortality (p < 0.001). Men with severe BCIS had a 16-fold higher 30-day mortality than those with Grade 0 or 1. The excess mortality from BCIS was seen intra-operatively and in the immediate postoperative period: thereafter the survival curve of those experiencing BCIS was similar to those who did not. Independent predictors for development of severe BCIS were: ASA grades III–IV, pre-existing chronic obstructive pulmonary disease and medication with diuretics or warfarin. Discussion The authors concluded that BCIS is common and that severe episodes carry significant excess mortality. Efforts should be made to identify those at risk of BCIS, so as to guide intra-operative preventive measures which may decrease the risk of developing it to improve survival in these patients. Dr Chris James CT2 Severn Deanery Mark Callaghan ST5 Anaesthesia, Northern Deanery References 1. Gan TJ, Diemunsch P, Habib AS, et al. Consensus guidelines for the management of postoperative nausea and vomiting. Anesthesia & Analgesia 2014; 118: 85–113. 2. Myles P, Leslie K, Chan MT, et al. Avoidance of nitrous oxide for patients undergoing major surgery: a randomized controlled trial. Anesthesiology 2007; 107: 221–31. 3. Leslie K, Myles PS, Chan MT, et al. Nitrous oxide and long-term morbidity and mortality in the ENIGMA trial. Anesthesia & Analgesia 2011; 112: 387–93. 28 Anaesthesia News March 2015 • Issue 332 Anaesthesia News March 2015 • Issue 332 29 A AGBI TOPICS INCLUDE: Anaesthetists in training Clinical anaesthesia Clinical measurement/equipment GUIDELINES APP Contractual/job planning Elderly anaesthesia Ethics and law Haematology Human factors Independent practice rch First update in early Ma 2015: 6 new guidelines Irish anaesthetists Obstetric anaesthesia Resuscitation and trauma ntent Updates to existing co SAS anaesthesia Wellbeing FREEGBI FOR A A RS MEMBE Checklist for t anaesthetic equipmen ol Reflective learning to DOWNLOAD THE APP TODAY FOR APPLE AND ANDROID DEVICES www.aagbi.org/guidelines-app Learn@AAGBI Couldn’t attend WSM London 2015? Lecture videos now available Catch up on your CPD The template is easy to use allowing you to reflect on the conference as a whole or on individual lectures. Step-by-step guide on how to reflect using the site: Step 1. Go to www.aagbi.org/education Step 2. Click on the ‘Learn@AAGBI’ box Step 3. Log in note: you will need your AAGBI membership number and password Step 4. From the search page select your required option Step 5. From the list select the video that you wish to reflect on Step 6. After watching the whole video, open the reflective learning form and complete it Step 7. If you are happy with what you have written, click on ‘Submit form’, or if you would like to add more later on, click ‘save draft’. This will upload into the ‘My CPD Area’ as either ‘draft’ or a completed ‘Submitted Reflective Note’. Go to www.aagbi.org/education and use Learn@AAGBI for your reflections at our meetings, and for your ongoing CPD and exam preparation. New award for excellence in sustainability Developing a green anaesthesia agenda The AAGBI recognises that our actions have an impact on the environment and regards global warming and climate change as pressing issues. In 2013 the Environmental Task Group of the AAGBI was formed to develop the idea of sustainable practice and to promote greener anaesthesia. The Task Group and the Association have linked with Barema, the Association for Anaesthetic and Respiratory Device Suppliers, representing companies that manufacture or supply anaesthetic and respiratory equipment in or to the UK, to establish the Barema & AAGBI Environment Award. This will recognise excellence in sustainability within the speciality and engage with industry partners to further develop a greener anaesthesia agenda. Apply for the NEW Barema & AAGBI Environment Award! Applicants will have to demonstrate how their activity, project, campaign or other work (including original research), related to anaesthesia, intensive care or pain management, has had (and will continue to have) a measurable beneficial effect on the environment. The award will be for the single best initiative or project and will consist of £200 to the individual(s) or body(ies) concerned, in addition to a grant of £800 for support and development of the initiative or project. The deadline for applications is 30 April 2015 with the winners being announced at Annual Congress in Edinburgh in September. To find out more about the award and the application process visit www.aagbi.org/about-us/environment or email [email protected]








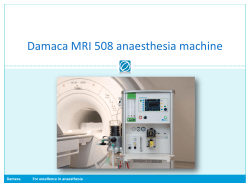

© Copyright 2026