
2010 Drug Endangered Children Training Evaluation Report
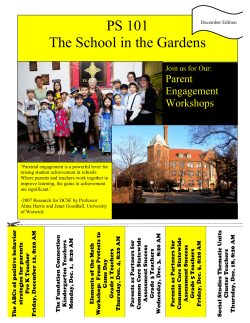
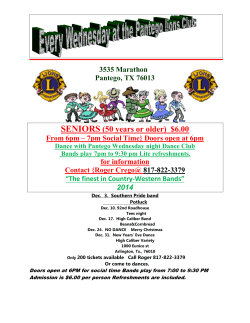
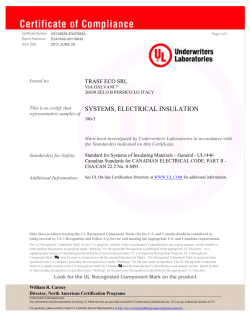
Evaluation of the Drug Endangered Children Training Project Dr. Mark Totten Totten and Associates April 6, 2011 Acknowledgements The author would like to acknowledge the following individuals for their support, guidance and critical feedback in conducting the evaluation. They include: Trudy Bangloy and Ian Sanderson, RCMP; Barbara Spencer, Zebra Child Protection Centre; Pat Toland, Noreen Majek and Cora Walkinshaw, Alberta Child and Youth Services; and Dr. Craig Bennell, Carleton University Department of Psychology. 1 1. Executive Summary Over the past two years, the Zebra Child Protection Centre has been working in partnership with Alberta Child and Youth Services and the RCMP Drugs and Organized Crime Awareness Service to oversee the development and delivery of evaluated training workshops to front line child intervention workers, police and community stakeholders. The purpose of this evaluation report is to present the findings from these training workshops. The purpose of the Canadian D.E.C. movement is to intervene on behalf of children who have been exposed to home-based drug activity in order to improve their life trajectory. A child is considered “drug endangered” if they are—or are likely to be—harmed by an adult’s drug activity. They are deemed especially endangered if they are growing up in a home where drugs are being produced or sold, whether through an indoor marijuana grow operation or a synthetic drug lab. The D.E.C. model approaches the plight of drug endangered children from four vantage points: awareness, team-building, training and advocacy. The first aim is to raise awareness about the critical effects of drug activity, specifically its impacts on children. The second aim is to describe the D.E.C. team approach to current and potential team members, which range from police officers, firefighters and medical care providers to mental health and substance abuse experts, environmental health inspectors and concerned stakeholders. The third aim is to equip D.E.C. team members with knowledge and training to ensure the health and safety of at-risk children. Last, the fourth aim is to spark public interest about D.E.C. issues in order to provide information for those involved in legislative changes that redefines drug endangered children as victims of abuse. The purpose of this project is to evaluate the Pilot Drug Endangered Children Training Curriculum. Two curricula were developed and tested during the time period of September 2010 – March 2011. A two-day Train the Trainer workshop was held in September 2010 and one-day training workshops were subsequently held up to March 25, 2011. The facilitators for the oneday workshops were selected from those interested candidates who participated in the train the trainer workshop. Two tools were developed by the Evaluator in consultation with the Advisory Committee. The data collected for this training evaluation include scores on a knowledge test that were obtained from each participant before and after they took part in training (i.e., pre-test and post-test scores), as well as several variables that describe each participant and the training that they received (length of the training session [1 day vs. 2 days], gender of the participant [male vs. female], and profession of the participant [police officer vs. child welfare worker]). As well, a satisfaction survey was completed by 134 participants. A total of 153 participants took part in the DEC training. One hundred and twenty six of these individuals (82.4%) took part in a 1-day training session, whereas the remaining 27 participants (17.6%) took part in a 2-day train the trainer session. Of the 153 participants, 104 (68%) were female and 49 (32%) were male. In terms of professions, there was a near even split amongst participants. Sixty seven of the participants (43.8%) were police officers and 86 (56.2%) were child welfare workers. One hundred and fifty two of the 153 participants completed the pre-test (there was one missing test). The mean score on this pre-test (out of 30) was 22.47 (SD = 3.06, range = 13.50 to 29). Only 149 of the 153 participants completed the post2 test (there were four missing tests). The mean score on the post-test (out of 30) was 25.61 (SD = 2.04, range = 20 to 30). The results of the mixed factorial ANOVA indicated that there was a significant main effect for the test factor when controlling for all other factors (the duration of training, the gender of participants, and the profession of participants). Specifically, scores on the pre-test (M = 22.81, SE = .39) were found to be significantly lower than scores on the post-test (M = 26.32, SE = .25), F (1,140) = 91.28, p = .00. This result indicates that the training had its desired effect of increasing knowledge of participants. The effect size associated with this test was also relatively large (η2 = .40) indicating that the training itself accounted for 40% of the variation in test scores from pre- to post-test (after controlling for all other variables in the analysis, and their interactions). The power of the test was also found to be very high (power = 1.00), suggesting that we can be confident that there is indeed a reasonably large effect of training on the knowledge test scores. There was also a significant main effect found for the duration factor when controlling for all other factors. Specifically, overall test scores (averaged across pre- and post-tests) obtained from the 1-day session (M = 23.85, SE = .22) were found to be significantly lower than the overall test scores (averaged across pre- and post-tests) obtained from the 2-day session (M = 25.28, SE = .50), F (1,140) = 6.82, p = .01. Given the increased exposure that participants would have to training in the 2-day session this result is not particularly surprising. Notwithstanding this significant result, the effect size for this comparison was relatively small (η2 = .05) indicating that only 5% of the variation in overall test scores could be accounted for by the duration of the training session (after controlling for all other variables in the analysis, and their interactions). While the power of this test was slightly below the generally accepted .80 threshold (power = .74), we can be reasonably confident in concluding that there is a small effect of training duration on overall test scores. No significant differences were found for any of the other variables that were analyzed, or their interactions. In addition, the effect sizes associated with these analyses were all very small (though the power of the tests was also very low). Again, this is all unsurprising. There is no reason why the gender of participants, or their professions, should relate to test performance. There is also no reason why any interactions between these variables (including the duration of training) should be significant. Overall, most participants were satisfied with the training. Yet, only 64% of participants gave the training an “A” grade or higher and there was a relatively high number of participants who did not complete sections of the satisfaction questionnaire. In summary, the findings from the pre/post knowledge tests strongly suggest that the training had a very positive impact on knowledge acquisition. Statistical analyses demonstrate that these beneficial outcomes were attained irrespective of gender or professional role. For a number of reasons, findings are less clear regarding participant satisfaction with the training. Recommendations include expanding the training to include firefighters, medical care providers, mental health and substance abuse experts, environmental health inspectors and other concerned stakeholders. Special focus should be directed at engaging Aboriginal partners and representatives from ethno-racial communities. 3 Table of Contents 1. Executive Summary p. 2 2. Introduction p. 5 3. Project Overview p. 7 4. Evaluation Methodology p. 8 5. Findings 5.1 Pre/Post Knowledge Test Findings 5.2 Satisfaction Survey Findings p. 9 p. 9 p. 12 6. Conclusion p. 16 7. Recommendations p. 17 8. Appendices Appendix A: Pre/Post Knowledge Test Appendix B: Satisfaction Survey Appendix C: Results from the Mixed Factorial ANOVA p. 18 p. 18 p. 35 p. 40 4 2. Introduction The Canadian Drug Endangered Children (D.E.C.) initiative is modeled on the American model, developed in response to the high number of children found in home-based methamphetamine labs. Although Canada does not face the same proliferation of home-based labs as the U.S.A., the concept of a D.E.C. initiative provides governments and communities with the opportunity to recognize and address emerging methamphetamine issues, as well as the spectrum of other drug activity to which children are exposed. In 2002, the D.E.C. initiative became a major component in the Royal Canadian Mounted Police (R.C.M.P.) Meth Prevention Strategy in Alberta. In St. Albert, AB, trained officers conducted a pilot D.E.C. project to identify ways to build collaborative D.E.C. responses in Canadian communities. The project highlighted numerous key issues, notably the need to extend the program on a national level, as a means to intervene and protect children from the immediate harm of drug activity, as well as from the long-term psychosocial impact of drug exposure. A Resource Guide (Drug Endangered Children Program: Equating Drug Activity to Child Abuse) was developed. This guide builds on the experiences of the pilot group established by the R.C.M.P.’s “K” Division and a number of Albertan stakeholder partners. It also reflects the refinements in scope and implementation necessary in the creation of an effective national initiative. This guide emphasizes two major points: first, drug activity is not victimless—it often affects the most vulnerable and innocent in society. Second, because drug activity exposes children to immediate risks and dangers as well as to lasting psychosocial harms, it is considered child abuse. Canadian police services and government agencies have vast experience with collaborative, integrated intervention efforts—a key skill set for multidisciplinary D.E.C. response teams. D.E.C. teams require these approaches to effectively break patterns of abusive child-rearing and drug-related violence. The R.C.M.P. is committed to promoting these efforts through the advancement of a national D.E.C. initiative that is relevant across communities. The purpose of the Canadian D.E.C. movement is to intervene on behalf of children who have been exposed to home-based drug activity in order to improve their life trajectory. A child is considered “drug endangered” if they are - or are likely to be - harmed by an adult’s drug activity. They are deemed especially endangered if they are growing up in a home where drugs are being produced or sold, whether through an indoor marijuana grow operation or a synthetic drug lab. The effective protection of drug endangered children increasingly demands a coordinated response from multiple stakeholder agencies. A Canadian approach enables such coordinated efforts by building strong response teams, capable of removing children from immediate danger, providing them with urgent and ongoing medical care, and facilitating positive, professional attention. By providing such rescue possibilities, D.E.C. interventions give children the opportunity to break the destructive cycle of intergenerational drug and drug-related abuse. The D.E.C. model approaches the plight of drug endangered children from four vantage points: awareness, team-building, training and advocacy. The first aim is to raise awareness about the critical effects of drug activity, specifically its impacts on children. The second aim is to describe the D.E.C. team approach to current and potential team members, which range from police officers, firefighters and medical care providers to mental health and substance abuse experts, environmental health inspectors and concerned stakeholders. The third aim is to equip D.E.C. team members with knowledge and training to ensure the health and safety of at-risk children. Last, the fourth aim is to spark public interest about D.E.C. issues in order to provide 5 information for those involved in legislative changes that redefines drug endangered children as victims of abuse. In the past, there was no established protocol for ensuring that children removed from a drug crime scene were placed in a safe, appropriate environment. Without a collaborative approach, children are left unable to protect themselves from danger. Various agencies may respond to the children’s needs based on their own protocols, but they tend to operate independently. If they do not co-ordinate their responses to address the complex requirements of D.E.C. situations, children’s needs may be overlooked or ignored, based on the assumption that another agency is looking after them. With the D.E.C. approach, drug endangered children enter an integrated system of care. The effectiveness of a D.E.C. team depends on the equal and active participation of all specialized D.E.C. team members. This collaboration ensures a mutual understanding of roles, a coordinated response and an established flow of communication. D.E.C. teams are committed to protecting children exposed to drug use and production in order to help them thrive in drug-free family environments. In response to the above, the Zebra Child Protection Centre has been working since 2010 on a joint venture with the Alberta Government, Alberta Child and Youth Services and the RCMP Drugs and Organized Crime Awareness Services to oversee the development and delivery of evaluated training workshops to front line child intervention workers, police and community stakeholders. The purpose of this report is to present the findings from these training workshops. 6 3. Project Overview Two curricula were developed and tested during the time period of September 2010 – March 2011. A two-day Train the Trainer workshop was held in September 2010 and one-day training workshops were subsequently held up to March 25, 2011. The facilitators for the one-day workshops were selected from those interested candidates who participated in the train the trainer workshop. Two-day Train-the-Trainer Session Workshop: The purpose of this workshop is to provide police, community and child intervention personnel with an understanding of the scope of drug activity that places children at risk, along with an overview of the DEC training initiative. Facilitators should be able to describe to participants the DEC team approach and provide DEC participants with the knowledge and skills necessary to confidently and capably respond as a team to drug activity cases where children and exposed. The facilitation package includes the material and tools required for a facilitator to deliver the DEC workshop. It includes: a facilitator guide that provides a facilitation plan with detailed instructions and key messages to support delivery of the workshop material to achieve the learning objectives and a reference to the corresponding PowerPoint slide and page in the participant material; the PowerPoint slides coordinated to the course material; PowerPoint games to support exercises and activities from the course material; a copy of the Drug Endangered Children: Equating Drug Activity to Child Abuse Resource Guide; a copy of the participant materials; and a copy of each of the participant handouts. The facilitator role is to share the content with participants and facilitate discussion. It involves ensuring that discussion and activities stay on track. Upon completion of the workshop, the trainers should be able to: • Facilitate a one day training program for police, community and child intervention services staff that addresses drug endangered children; • Confidently provide police, community and child intervention services personnel with an understanding of their respective roles in responding to DEC situations; • Identify and apply a child centered approach to responding to children exposed to drug use and/or manufacturing; • Outline the DEC team model for response to drug endangered children; and • Facilitate discussion of how these organization can work together to ensure the health and safety of at risk children. One-day Training Workshop: The DEC one day workshop is designed to describe the DEC Team approach to current and potential team members and to equip them with the knowledge and skills to confidently and capably respond to situations where children are exposed to drug activity. It is based upon the Drug Endangered Children Act and the Drug Endangered Children: Equating Drug Activity to Child Abuse Resource Guide. The workshop is designed for potential team members, including caseworkers, police, fire fighters, medical care providers, mental health professionals, substance abuse experts, environmental health inspectors, emergency medical technicians and Crown prosecutors. The workshop material has been designed for classroom delivery and consists of facilitator-presented information, large group discussion, small group and individual 7 activities/exercises, application exercises to promote discussion, understanding and skill building, and opportunities for question and answer. Upon completion of the workshop, participants should be able to: • Describe the relationship between drug exposure and child abuse; • Explain the effects of exposure to drug manufacturing and use on children; • Identify the signs and symptoms of drug exposure; • Apply a child-centered approach to responding to children exposed to drug use and/or manufacturing; • Outline the process for an effective DEC response; • Describe the roles of all DEC team members; • Identify the steps in setting up a DEC team; • Engage in a multidisciplinary response to situations where children are exposed to drugs; • Explain and follow the protocols of working together; • Describe the risks to first responders; and • Identify organizations, agencies and stakeholders involved in providing a comprehensive DEC response. 4. Evaluation Methodology Two tools were developed by the Evaluator in consultation with the Advisory Committee. Both tools are contained in the Appendices. The first tool is a Pre/Post Knowledge questionnaire, modified from the U.S.A. National DEC program questionnaire (see Appendix A). The second tool is a modified version of the Alberta Child and Youth Services Training Evaluation Questionnaire (See Appendix B). Participants were asked to complete the pre-test at the start of the first day and likewise to complete the post-test at the end of the last day of training. The tests were closed-book and participants were instructed to fill out the questionnaires individually (they could not consult with peers). The Satisfaction Survey was completed by participants after they completed the post-test questionnaire. In addition, the Evaluator observed the delivery of one one-day pilot session of the Drug Endangered Children Training Curriculum along with the two-day Train the Trainer session 8 5. Findings 5.1 Pre/Post Knowledge Test Findings The data collected for this training evaluation include scores on a knowledge test that were obtained from each participant before and after they took part in training (i.e., pre-test and posttest scores), as well as several variables that describe each participant and the training that they received (length of the training session [1 day vs. 2 days], gender of the participant [male vs. female], and profession of the participant [police officer vs. child welfare worker]). The knowledge test is referred to as a within-subject factor because the same measure (i.e., a score on a knowledge test) was collected multiple times from each participant. The other variables are referred to as between-subject factors because they describe differences between participants, and thus divide the overall sample into sub-groups (e.g., those participants that took part in the 1day vs. 2-day training, males vs. females, and police officers vs. child welfare workers). In cases where within- and between-subject factors are included in the same evaluation, the appropriate statistical test to use to analyze the data is a mixed factorial analysis of variance (ANOVA). This test allows one to examine potential main effects, which in the current case refer to the effects of between-subject factors and within-subject factors on the knowledge test scores (e.g., did males score higher than females on the knowledge tests?; did participants score higher on the post-test than on the pre-test?). In addition, this statistical test allows one to investigate potential interaction effects, which describe how the variables might affect one another (e.g., whether the effect of training duration on test performance [as measured by the pre- and posttests for the 1- and 2-day training sessions] varies as a function of some other variable, such as the gender or profession of participants). For each of the potential main effects and interactions, a mixed factorial ANOVA provides F statistics along with degrees of freedom and associated p-values for each test. The pvalue is used to determine if the main effects and interaction effects are statistically significant. For this set of analyses, statistical significance was determined using the conventional alpha level (p-value) of .05. In other words, an effect will be deemed significant if there is a 5% or lower probability that the effect occurred simply by chance. In addition to the above information, effect sizes will also be calculated for each of the potential effects. In contrast to measures of statistical significance, which indicate the extent to which effects can occur simply by chance, effect sizes estimate the magnitude of any effects that are found. In this way, effect sizes complement measures of statistical significance and speak more directly to the practical significance of an effect. The effect size used in this evaluation is referred to as partial eta squared (η2). This effect size relates to the proportion of variation in knowledge test scores accounted for by each of the main and interaction effects. For example, if a significant effect is found for gender (e.g., males perform significantly better than females on the tests) and this effect is associated with a η2 of .40, then gender accounts for 40% of the total variability in knowledge test scores after statistically controlling for all other variables, including their interactions. Finally, estimates of power will also be provided for each of the tests. Whereas measures of statistical significance indicate the likelihood of declaring that there is an effect when such an effect actually does not exist, power refers to the probability that the statistical test will find a statistically significant effect when such an effect actually does exist. Basically, a power analysis helps to determine the power of a particular test for detecting an effect size of a particular magnitude. For example, a comparison of participant gender might indicate that a gender difference exists with respect to test scores, but that the effect size is rather small (e.g., 0.10). If 9 power was calculated for this test and it was found to be high (e.g., .90), we could be confident in concluding, on the basis of this test, that there is indeed a small effect of gender on test scores. Although there are no hard and fast rules, .80 is usually considered to be a reasonable level of power for any given test. Descriptive Results A total of 153 participants took part in the DEC training. One hundred and twenty six of these individuals (82.4%) took part in a 1-day training session, whereas the remaining 27 participants (17.6%) took part in a 2-day train the trainer session. Of the 153 participants, 104 (68%) were female and 49 (32%) were male. In terms of professions, there was a near even split amongst participants. Sixty seven of the participants (43.8%) were police officers and 86 (56.2%) were child welfare workers. One hundred and fifty two of the 153 participants completed the pre-test (there was one missing test). The mean score on this pre-test (out of 30) was 22.47 (SD = 3.06, range = 13.50 to 29). Only 149 of the 153 participants completed the post-test (there were four missing tests). The mean score on the post-test (out of 30) was 25.61 (SD = 2.04, range = 20 to 30). Results from the Mixed Factorial ANOVA All of the results from the mixed factorial ANOVA are reported in Appendix C. Here, the focus is just on those comparisons that reached statistical significance. As illustrated in Figure 1, the results of the mixed factorial ANOVA indicated that there was a significant main effect for the test factor when controlling for all other factors (the duration of training, the gender of participants, and the profession of participants). Specifically, scores on the pre-test (M = 22.81, SE = .39) were found to be significantly lower than scores on the posttest (M = 26.32, SE = .25), F (1,140) = 91.28, p = .00. This result indicates that the training had its desired effect of increasing knowledge of DEC. The effect size associated with this test was also relatively large (η2 = .40) indicating that the training itself accounted for 40% of the variation in test scores from pre- to post-test (after controlling for all other variables in the analysis, and their interactions). The power of the test was also found to be very high (power = 1.00), suggesting that we can be confident that there is indeed a reasonably large effect of training on the knowledge test scores. 10 Figure 1. A comparison of pre- and post-test scores (controlling for all other variables). As illustrated in Figure 2, there was also a significant main effect found for the duration factor when controlling for all other factors. Specifically, overall test scores (averaged across pre- and post-tests) obtained from the 1-day session (M = 23.85, SE = .22) were found to be significantly lower than the overall test scores (averaged across pre- and post-tests) obtained from the 2-day session (M = 25.28, SE = .50), F (1,140) = 6.82, p = .01. Given the increased exposure that participants would have to training in the 2-day session this result is not particularly surprising. Notwithstanding this significant result, the effect size for this comparison was relatively small (η2 = .05) indicating that only 5% of the variation in overall test scores could be accounted for by the duration of the training session (after controlling for all other variables in the analysis, and their interactions). While the power of this test was slightly below the generally accepted .80 threshold (power = .74), we can reasonably be confident in concluding that there is a small effect of training duration on overall test scores. 11 Figure 2. A comparison of pre- and post-test scores for the 1-day and 2-day training sessions (controlling for all other variables). No significant differences were found for any of the other variables that were analyzed, or their interactions. In addition, the effect sizes associated with these analyses were all very small (though the power of the tests was also very low). Again, this is all unsurprising. There is no reason why the gender of participants, or their professions, should relate to test performance. There is also no reason why any interactions between these variables (including the duration of training) should be significant. 5.2 Satisfaction Survey Findings A total of 134 participants completed satisfaction surveys. The survey tool was a slightly modified version of the Alberta Child and Youth Services Training Evaluation Questionnaire. Presentation of findings in this report include overall rating for workshop presentation, overall rating for workshop learning, overall rating for course administration, and finally overall rating for the course. The overall ratings for workshop presentation was based on a series of statements for which participants were asked to indicate how much they agreed or disagreed (strongly disagree, mildly disagree, mildly agree, strongly agree): • • • The course learning objectives were clearly defined The course met stated learning objectives The content was relevant for my job 12 • • • • • • • • • • The instructor(s) was knowledgeable and well informed The instructor(s) listened and responded effectively to questions and concerns The instructor(s) gave examples and/or solicited them from the participants Engaged participants in active learning Used appropriate technology to support learning Written materials and handouts were useful, organized and easy to use I will be able to use the materials as a reference My skills and knowledge increased as a result of the training The course content was current The content was appropriate to my professional education, experience and/or licensure Participants were asked to use a 4-point scale to rate workshop presentation. As illustrated in Figure 3, 83% of participants scored this area as a ‘three’ or ‘four’. Three participants gave workshop presentation a ‘one’ or ‘two’. Results should be interpreted with caution as twenty participants did not answer this question. Figure 3: Overall Rating for Workshop Presentation (N=134) 50 40 % 30 20 10 0 Poor 2 3 Excellent Missing Participants were asked to use a 4-point scale to rate workshop learning. The overall rating for workshop learning was based on a series of statements for which participants were asked to indicate how much they agreed or disagreed (strongly disagree, mildly disagree, mildly agree, strongly agree) if the following aspects of the program aided learning: • Pre-reading material • Large group discussion • Small group activities • Skill practice activities 13 • • • Lectures and lecture reviews Independent activities Audio-visual materials As seen in Figure 4, 73% of participants rated workshop learning as a ‘three’ or ‘four’. Four participants rated it as a ‘one’ or ‘two’. Results should be interpreted with caution as 32 participants did not answer this question. Figure 4: Overall Rating for Workshop Learning (N=134) 40 30 % 20 10 0 Poor 2 3 Excellent Missing Participants were asked to use a 4-point scale to rate course administration. Course administration consisted of using the same ratings as above for the following areas: • Requests for accommodation and assistance for disability • Workshop facilities • Program structure • Distance education/home study As illustrated in Figure 5, 65% of participants rated this area as a ‘three’ or ‘four’. Three participants rated it as a ‘two’. Again, results should be interpreted with caution one-third of participants did not answer this question. 14 Figure 5: Overall Rating for Course Administration (N=134) 35 30 25 % 20 15 10 5 0 Poor 2 3 Excellent Missing Finally, participants were asked to use a 10-point scale to rate the course overall. As seen in Figure 6, twelve percent gave the course a failing grade (five or lower). Fifteen percent gave it a ‘B’ or ‘C’ (6-7 rating), 45% gave it an ‘A’ or ‘A+’, and 19% gave it a perfect grade. Again, results should be interpreted with caution as twenty-four participants did not answer this question. Figure 6: Overall Rating for the Course (N=134) 50 40 % 30 20 10 0 3 (Poor) 4-5 6-7 15 8-9 10 (Excellent) Missing 6. Conclusions The findings from the pre/post knowledge tests strongly suggest that the training had a very positive impact on knowledge acquisition. Statistical analyses demonstrate that these beneficial outcomes were attained irrespective of gender, professional role or location of workshop. Findings are less clear regarding participant satisfaction with the training. A relatively large number of participants did not complete certain sections of the questionnaires. This is likely due to a number of factors: some facilitators did not stress the importance of completing all of the questions in this survey, instead leaving participants with the impression that it was voluntary; formatting problems for some questions; and minor issues related to shipping of course materials (for example, some participants did not receive pre-conference readings). These issues resulted in overall ratings of satisfaction with the one-day workshop being quite low. Therefore, despite the fact that a majority of participants gave high ratings in the various areas covered by the satisfaction questionnaire, it would be inappropriate to make generalizations from these data. 16 7. Recommendations A number of recommendations are made to improve future D.E.C. training workshops. They include: a) Expand the one-day training sessions to include other relevant stakeholders outside of police and child welfare, including firefighters, medical care providers, mental health and substance abuse experts, environmental health inspectors and other concerned stakeholders. b) Expand future train the trainer workshops to include firefighters, medical care providers, mental health and substance abuse experts, environmental health inspectors and other concerned stakeholders. c) Ensure that all subsequent workshops are properly evaluated, using the two tools developed for the evaluation of the pilot workshops. In particular, facilitators should make every effort to ensure that all participants complete the questionnaires. d) Ensure that participants and facilitators reflect the diversity of their communities. For example, Aboriginal people and members of ethno-racial minority groups are important stakeholders in the D.E.C. movement. Elders, role models and leaders from these communities should be engaged. Every effort should be made to ensure that training workshops are accessible to these groups. e) Identify a key organization to take the lead in ongoing delivery of the training workshops. This will present challenges for training coordination, funding and human resources. Ultimately, this will determine the success of the D.E.C. program in stimulating community response and improved outcomes for children exposed to drug activity. 17 8. Appendices Appendix A: Pre/Post Knowledge Test CORE DRUG ENDANGERED CHILDREN TRAINING PROGRAM Zebra/ACYS/RCMP Training 2010 This booklet contains pre- and post-assessment tests for DEC training. It is based on the USA National DEC program and modified by Dr. Mark Totten, evaluator of the Zebra/RCMP DEC project. Your responses will be used to assess the effectiveness of this training program, help guide Canadian DEC project efforts, and provide information to further develop resources. Please return this book to course facilitators after completion of the course. Thank you again for your participation. 18 Participant Information Name: ___________________________________________________________________________ Title: _____________________________________________________________________________ Gender: M_____ F_____ Current Organization Name: ________________________________________________________________________ Address: ______________________________________________________________________________ Phone: ______________________________________________________________________________ E-mail:________________________________________________________________________ Years in Current Occupation: _______________________________________________________________________ Past Occupation(s) Related to Drugs or Children: ___________________________________________________________________________ ____________________________________________________________________________ 19 Pre-Course Assessment Please choose the most appropriate response according to your thoughts, opinions, and current knowledge prior to attending the Drug Endangered Children Training Program. 1. The Canadian drug endangered children movement started in: a. 1990 b. 1993 c. 2002 d. 2009 e. I don’t’ know 2. The first province to develop a formalized response to the problem of drug endangered children was: a. Alberta b. Ontario c. British Columbia d. Nova Scotia e. I don’t know 3. The Canadian model was developed in response to home-based methamphetamine labs. a. True b. False c. I don’t know 4. The DEC approach addresses the plight of drug endangered children from three vantage points: awareness, team building and advocacy. a. True b. False c. I don’t know 20 5. The child-centered response model includes: a. Rescuing children b. Defending the rights of children c. Sheltering children d. Supporting children e. All of the above 6. According to the 2004 Canadian Health Survey , about 3 million Canadians used marijuana in the past year, almost double the number in 1994. a. True b. False c. I don’t know 7. The primary concern of parents and guardians who use, traffic, or manufacture drugs is the drug they are using or producing: a. True b. False c. I don’t know 8. Complete the sentence: The Canadian Drug Endangered Children initiative considers a child to be drug endangered if she or he is: 9. A primary message in the Canadian DEC initiative is: a. Some drug endangered children are at risk b. Children + Drugs = Risk c. Drugs and related drug activity are perfectly acceptable around children d. Both a and b 21 10. The effects of prenatal drug exposure: a. Are difficult to isolate, owing to other variables such as poor prenatal care, poor nutrition, prematurity, and adverse postnatal environment b. Depend on the substance being used, the frequency of use, the duration of use and quantity c. Both a and b d. Neither a nor b 11. Postnatal risks to drug endangered children include: a. Physical, sexual, and emotional abuse b. Neglect c. Exposure to illegal drug activity d. Exposure to violence e. All of the above 12. All drug endangered children are at risk. a. True b. False 13. Illicit drug activities include: a. Possession b. Use c. Manufacture d. Cultivation e. Distribution f. All of the above 22 14. Methamphetamine is the only illegal drug manufactured in clandestine drug labs. a. True b. False c. I don’t know 15. How many categories of drugs does the Canadian DEC movement consider in its response strategies? a. Just methamphetamine and clandestine methamphetamine labs b. Three: Methamphetamine, heroin, and cocaine c. Five: Depressants, cocaine, methamphetamine, heroin, and prescription drugs d. Seven: Depressants, inhalants, PCP, cannabis, stimulants, hallucinogens, and narcotic analgesics 16. Children growing up in drug environments: a. Are denied the fundamental developmental experiences required to self-regulate, relate, communicate and think b. Experience neglect, daily chaos, a lack of safety, poor communication, violence, and disorganization c. May experience emotional, behavioral and cognitive problems d. All of the above 17. Please list two emotional problems drug endangered children may experience. a. b. 18. Please list two behavioral problems drug endangered children may experience. a. b. 23 19. Please list two cognitive problems drug endangered children may experience. a. b. 20. The earlier the intervention, the more efficient and effective the outcome. a. True b. False c. I don’t know 21. Research and clinical trends support the potential for change throughout life. a. True b. False c. I don’t know 22. Circle the correct answer: The DEC effort is about collaborative or cooperative interventions. 23. Networking, coordination, cooperation and collaboration all basically mean the same thing. a. True b. False c. I don’t know 24. Please list at least three common challenges to collaboration: a. b. c. 24 25. Major symptoms of drug endangered children include: a. Symptoms of neglect and abuse b. Symptoms of chemical exposure c. Symptoms of drug exposure d. All of the above 26. Being part of the DEC movement: a. Makes you part of the larger solution b. Connects you to other professionals working on the same challenges c. Helps you advocate more effectively on behalf of children and families d. All of the above 27. A major purpose of the Canadian DEC initiative is to redefine our understanding of child abuse: a. True b. False c. I don’t know 28. How many provincial DEC initiatives are there in Canada? a. 1 b. 2 c. 4 d. 5 25 29. Common elements for change include: a. Recognition of an unacceptable situation b. A shared vision for a desired outcome c. Strong leadership d. The guided activities of many e. Persistence f. All of the above 30. The overall goal for DEC efforts is for ______ of the children we serve to end up happy, and in safe, nurturing environments. a. 10% b. 25% c. 75% d. 100% 26 Post-Course Assessment Participant Information Name: ______________________________________________________________________________ Title: ______________________________________________________________________________ Gender: M_____ F_____ Current Organization Name: ________________________________________________________________________ Address: ______________________________________________________________________________ Phone: ______________________________________________________________________________ E-mail:________________________________________________________________________ Years in Current Occupation: _______________________________________________________________________ Past Occupation(s) Related to Drugs or Children: _______________________________________________________________________ 27 Please choose the most appropriate response according to your thoughts, opinions, and current knowledge after attending the Drug Endangered Children Training Program. 1. The Canadian drug endangered children movement started in: a. 1990 b. 1993 c. 2002 d. 2009 e. I don’t’ know 2. The first province to develop a formalized response to the problem of drug endangered children was: a. Alberta b. Ontario c. British Columbia d. Nova Scotia e. I don’t know 3. The Canadian model was developed in response to home-based methamphetamine labs. a. True b. False c. I don’t know 4. The DEC approach addresses the plight of drug endangered children from three vantage points: awareness, team building and advocacy. a. True b. False c. I don’t know 28 5. The child-centered response model includes: a. Rescuing children b. Defending the rights of children c. Sheltering children d. Supporting children e. All of the above 6. According to the 2004 Canadian Health Survey , about 3 million Canadians used marijuana in the past year, almost double the number in 1994. a. True b. False c. I don’t know 7. The primary concern of parents and guardians who use, traffic, or manufacture drugs is the drug they are using or producing: a. True b. False c. I don’t know 8. Complete the sentence: The Canadian Drug Endangered Children initiative considers a child to be drug endangered if she or he is: 9. A primary message in the Canadian DEC initiative is: a. Some drug endangered children are at risk b. Children + Drugs = Risk c. Drugs and related drug activity are perfectly acceptable around children d. Both a and b 29 10. The effects of prenatal drug exposure: a. Are difficult to isolate, owing to other variables such as poor prenatal care, poor nutrition, prematurity, and adverse postnatal environment b. Depend on the substance being used, the frequency of use, the duration of use and quantity c. Both a and b d. Neither a nor b 11. Postnatal risks to drug endangered children include: a. Physical, sexual, and emotional abuse b. Neglect c. Exposure to illegal drug activity d. Exposure to violence e. All of the above 12. All drug endangered children are at risk. a. True b. False 13. Illicit drug activities include: g. Possession h. Use i. Manufacture j. Cultivation k. Distribution l. All of the above 30 14. Methamphetamine is the only illegal drug manufactured in clandestine drug labs. a. True b. False c. I don’t know 15. How many categories of drugs does the Canadian DEC movement consider in its response strategies? a. Just methamphetamine and clandestine methamphetamine labs b. Three: Methamphetamine, heroin, and cocaine c. Five: Depressants, cocaine, methamphetamine, heroin, and prescription drugs d. Seven: Depressants, inhalants, PCP, cannabis, stimulants, hallucinogens, and narcotic analgesics 16. Children growing up in drug environments: a. Are denied the fundamental developmental experiences required to selfregulate, relate, communicate and think b. Experience neglect, daily chaos, a lack of safety, poor communication, violence, and disorganization c. May experience emotional, behavioral and cognitive problems d. All of the above 17. Please list two emotional problems drug endangered children may experience. a. b. 18. Please list two behavioral problems drug endangered children may experience. a. b. 31 19. Please list two cognitive problems drug endangered children may experience. a. b. 20. The earlier the intervention, the more efficient and effective the outcome. a. True b. False c. I don’t know 21. Research and clinical trends support the potential for change throughout life. a. True b. False c. I don’t know 22. Circle the correct answer: The DEC effort is about collaborative or cooperative interventions. 23. Networking, coordination, cooperation and collaboration all basically mean the same thing. a. True b. False c. I don’t know 24. Please list at least three common challenges to collaboration: a. b. c. 32 25. Major symptoms of drug endangered children include: a. Symptoms of neglect and abuse b. Symptoms of chemical exposure c. Symptoms of drug exposure d. All of the above 26. Being part of the DEC movement: a. Makes you part of the larger solution b. Connects you to other professionals working on the same challenges c. Helps you advocate more effectively on behalf of children and families d. All of the above 27. A major purpose of the Canadian DEC initiative is to redefine our understanding of child abuse: a. True b. False c. I don’t know 28. How many provincial DEC initiatives are there in Canada? a. 1 b. 2 c. 4 d. 5 33 29. Common elements for change include: a. Recognition of an unacceptable situation b. A shared vision for a desired outcome c. Strong leadership d. The guided activities of many e. Persistence f. All of the above 30. The overall goal for DEC efforts is for ______ of the children we serve to end up happy, and in safe, nurturing environments. a. 10% b. 25% c. 75% d. 100% 34 Appendix B: Satisfaction Survey Zebra/ACYS/RCMP Drug Endangered Children Project Training Evaluation Questionnaire Course Name: Trainer Drug Endangered Children - Pilot and Technical Train the Instructor(s) Name: Date(s): Location: Course Presentation 3. Mildly Agree Strongly Agree 2. Mildly Disagree Mildly Agree 1. Strongly Disagree Mildly Disagree 0. Not Applicable N/A (Circle one number) Strongly Disagree To what extent do you agree or disagree with each of the following statements. 0 1 2 3 4 0 1 2 3 4 Objective 2 0 1 2 3 4 Objective 3 0 1 2 3 4 Objective 4 0 1 2 3 4 Objective 5 0 1 2 3 4 0 1 2 3 4 0 1 2 3 4 0 1 2 3 4 0 1 2 3 4 0 1 2 3 4 0 1 2 3 4 0 1 2 3 4 0 1 2 3 4 0 1 2 3 4 0 1 2 3 4 1. The course learning objectives were clearly defined. 2. This course met stated learning objectives (please see attached for detailed list of learning objectives. Objective 1 4. Strongly Agree 3. The content was relevant to my job. 4. The instructor(s) was knowledgeable and well informed. 5. The instructor(s) listened and responded effectively to questions and concerns. 6. The instructor(s) gave examples and/or solicited them from the participants. 7. The instructor(s) engaged participants in active learning. 8. The instructor (s) used appropriate technology to support learning. 9. Written materials and handouts were useful, organized and easy to use. 10. I will be able to use the materials as a reference. 11. My skills and knowledge increased as a result of the training. 12. The course content was current. 35 13. The content was appropriate to my professional education, experience and/or licensure. 0 1 2 3 4 Strongly Agree Mildly Agree Mildly Disagree (please check n/a if not part of the program) Strongly Disagree The following aspects of the program aided my learning: N/A My overall rating for course presentation is: (Please circle) 1 2 3 4 (Poor) (Excellent) 1. Pre-reading materials 0 1 2 3 4 2. Large group discussion 0 1 2 3 4 3. Small group activities 0 1 2 3 4 4. Skill practice activities (role plays/role modelling) 0 1 2 3 4 5. Lectures and lecture reviews 0 1 2 3 4 6. Independent activities 0 1 2 3 4 7. Audio-visual materials (video, graphics, power-point) 0 1 2 3 4 Workshop Facilities 1 3 Strongly Agree Mildly Agree Mildly Disagree 2 4 Strongly Agree 0 Mildly Agree My request for assistance and/or accommodation for disability were addressed promptly and respectfully. N/A 1. Mildly Disagree Course Administration Strongly Disagree 4 (Excellent) Strongly Disagree 3 N/A My overall rating for learning is: (Please circle) 1 2 (Poor) 1. Location was appropriate 0 1 2 3 4 2. Registration, information, service were adequate 0 1 2 3 4 3. Training room was appropriate 0 1 2 3 4 36 3. Pace of the course should. 4. Amount of audio visual should. 5. Amount of handouts should. 6. Group Activities should. 7. Lectures should. Stay the same Decrease Increase Distance Education/ Home Study ( if applicable) Strongly Agree Course difficulty should. Mildly Agree 2. Mildly Disagree Amount of course content should Strongly Disagree 1. N/A Structure of Program (check mark column that applies) 1. This course was suitable for distance education. 0 1 2 3 4 2. I was able to easily access distance learning consultation. 0 1 2 3 4 3. I was able to transfer knowledge from the distance education program to my practice. 0 1 2 3 4 My overall rating for course administration is: (Please circle) 1 2 3 4 (Poor) (Excellent) 37 1. What was most valuable about this workshop? 2. What was least valuable about this workshop? 3. Was there anything that interfered with your learning during this workshop? 4. Additional Suggestions or Comments: Overall rating of the entire course, is: [Scale: 1 (low) - 10 (high)] The information that you provide in this form is to be used in the evaluation of the course, presenter(s)/ facilitator(s), and presentation methods. It is collected under the authority of, and in compliance with the Freedom of Information and Protection of Privacy Act, and will not be used for any other purpose. (Optional) Name: Phone Number: Learning Objectives Drug Endangered Children - Pilot Upon completion of this module, you will be able to: Learning Objective 1: Describe the relationship to drug exposure and child abuse; Learning Objective 2: Identify the signs and symptoms of drug exposure; Learning Objective 3: Apply a child-centered approach to responding to children exposed to drug use and / or manufacturing; Learning Objective 4: Describe the roles of all DEC team members; 38 Learning Objective 5: Engage in a multi-disciplinary response to situations where children are exposed to drugs. Learning Objectives Drug Endangered Children – Technical Train the Trainer Upon completion of this workshop you will be able to: Learning Objective 1: Facilitate a one day training program for police, community and child intervention services staff that addresses drug endangered children; Learning Objective 2: Confidently provide police, community and child intervention services personnel with an understanding of their respective roles in responding to drug endangered children situations; Learning Objective 3: Identify and apply a child-centered approach to responding to children exposed to drug use and/or manufacturing; Learning Objective 4: Outline the DEC team model for response to drug endangered children; Learning Objective 5: Facilitate discussion of how these organizations can work together to ensure the health and safety of at-risk children. 39 Appendix C: Results from the Mixed Factorial ANOVA Analysis of potential within-subject effects F df Sig η2 Power Test 91.28 1 .00* .40 1.00 Test*Duration 2.69 1 .10 .02 .37 Test*Gender .92 1 .34 .01 .16 Test*Profession 1.96 1 .16 .01 .29 Test*Duration*Gender 1.35 1 .25 .01 .21 Test*Duration*Profession .00 1 .97 .00 .05 Test*Gender*Profession .15 1 .70 .00 .07 Test*Duration*Gender*Profession .57 1 .45 .00 .12 Factor Error 140 *: p < .05 Analysis of potential between-subject effects F df Sig η2 Power Duration 6.82 1 .01* .05 .74 Gender .01 1 .92 .00 .05 Profession 1.02 1 .32 .01 .17 Duration*Gender .52 1 .47 .00 .11 Duration*Profession .07 1 .79 .00 .06 Gender*Profession 2.34 1 .13 .02 .33 Duration*Gender*Profession .02 1 .90 .00 .05 Factor Error 140 40







© Copyright 2026