
Stents before CABG tied to higher risk for diabetic patients
VOL. 11 C OURTESY OF AATS Stents before CABG tied to higher risk for diabetic patients Human malignant mesothelioma spheroids treated with PaxeNPs demonstrated caspase-3 up-regulation from negligible within the 24 hours after Pax-Rho-eNP treatment to significantly increased at 28 and 72 hours, compared with Pax-C/E. 3-D tumor cell model validates nanotech Frontline Medical News M alignant mesothelioma poses a significant challenge for clinicians because of its ability to resist chemotherapy, but the use of three-dimensional tumor spheroid models has shown that local administration of paclitaxel in a nanoparticle platform achieved better tumor penetration than conventional paclitaxel therapy, investigators reported. The study is in the May issue of the Journal of Thoracic and Cardiovascular Surgery. Dr. Hongyi Lei of Brigham and Women’s Hospital, Boston, and his colleagues used the in vi- tro mesothelioma spheroid model because two-dimensional in vitro monolayer cell culture experiments do not replicate the superior efficacy of paclitaxel-loaded expansile nanoparticles (PaxeNPs), suggesting that PaxeNPs utilize a unique drug delivery mechanism. The study observed that spheroids treated with Pax-eNP showed increased drug penetration and a 38-fold higher intraspheroidal drug concentration at 24 hours than that of paclitaxel dissolved in Cremophor EL/ethanol ( J. Thorac. Cardiovasc. Surg. 2014 [doi:10.1016/ j.jtcvs.2015.02.020]). See Nanotech · page 15 THORACIC SURGERY NEWS 151 Fairchild Ave., Suite 2, Plainview, NY 11803-1709 BY RICHARD KIRKNER Higher 5-year death rates observed. BY RICHARD KIRKNER Frontline Medical News S ince the debut of drug-eluting stents, more high-risk patient groups, namely diabetic patients, have undergone coronary stenting as opposed to coronary artery bypass grafting (CABG) as an option to open blocked arteries. However, a review study of 7,005 CABG procedures from 1996 to 2007 at Mercy St. Vincent Medical Center in Toledo, Ohio, found that diabetic patients with triple-vessel disease and a prior percutaneous coronary intervention with stenting (PCI-S) who underwent CABG had a 39% greater risk of death within 5 years of the operation. The findings, published in the May issue of the Journal of Thoracic and Cardiovascular Surgery, are significant, according to Dr. Victor Nauffal and his colleagues at the American University of Beirut, because increasing numbers of patients with coronary stents are referred for CABG (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/ See Stents · page 8 • NO. 5 • MAY 2015 I N S I D E News Mini-Pump FDA approves mini heart pump to help maintain function and circulation during high-risk PCI. • 2 Cardiopulmonary Transplantation High/Low ECMO Use of ECMO as a bridgeto-transplant showed worse outcomes at low-volume centers. • 9 Residents’ Corner Percutaneous Predicament The skills are needed; training must move with the times, but where’s the time? • 11 News from AATS Fellowships Galore See the awardees, apply for new opportunities, and register for meetings around the world. • 12 Dr. Michael J. Davidson remembered BY MITCHEL L. ZOLER Frontline Medical News I t’s extremely unusual for a cardiologist or cardiac surgeon to die in the line of duty, but that tragedy occurred this January in Boston when the enraged son of a patient mortally shot Dr. Michael J. Davidson while he was on the job as director of endovascular cardiac surgery at Brigham and Women’s Hospital. Dr. Davidson had been an active coinvestigator in the PARTNER study since it began in 2007 to make the first direct comparison of a transcatheter aortic valve replacement (TAVR) system against aortic valve replacement with conventional heart surgery. Because of Dr. Davidson’s long and active involvement with the PARTNER trial, his colleagues decided to dedicate the study’s 5-year follow-up findings to him, making the announcement during the first public release of the 5-year results in mid-March at the annual meeting of the American College of Cardiology. “On behalf of the PARTNER team, we would like to dedicate this study – the See Davidson · page 2 CHANGE SERVICE REQUESTED Presorted Standard U.S. Postage PAID Permit No. 384 Lebanon Jct. KY NEWS 2 MAY 2 0 1 5 • THO R A C IC S UR G ERY NEW S Slain surgeon honored Davidson from page 1 5-year outcomes – to Mike Davidson,” said Dr. Michael J. Mack as he finished his podium presentation of the report. Preceding Dr. Mack’s talk, the session began with brief remarks about Dr. Davidson from Dr. Martin B. Leon, coleader of the PARTNER trial, and then the airing of a 6-minute video featuring several of Dr. Davidson’s colleagues recalling his unique career and accomplishments. Notable in their comments was the outline they provided of the unusual training and career path Dr. Davidson forged for himself, based on his remarkably prescient realization a decade or more ago that the future of cardiology and cardiac sur- gery lay in fusing the two into a hybrid discipline. Dr. Davidson’s colleagues cited the training he undertook to become both a fully qualified cardiac surgeon and a skilled interventional cardiologist, turning himself into an embodiment of the “heart team.” Several in the video called him “visionary” for recognizing this fusion as an important step toward the future of treating heart disease. The poignancy of the moment did not stop there. After the video ended and before Dr. Mack delivered the session’s first talk, ACC president Dr. Patrick T. O’Gara presented a posthumous distinguished-service award from the ACC to Dr. Davidson – with Dr. O’Gara handing the award to the fallen surgeon’s parents, including his father, Dr. Robert M. Davidson, a longtime ACC fellow and former clinical chief of cardiology at Cedars-Sinai Medical Center in Los Angeles. Following the award, Dr. Athena Poppas, chair of the meeting’s program committee and cochair for the latebreaker session on heart valve replacement, stressed that the entire session was dedicated to honor Dr. Michael J. Davidson. Perhaps most moving of all were the small white buttons that Dr. O’Gara, Dr. Davidson’s parents, and others wore on their lapels during the session, featuring a blue heart and the initials MJD. It combined for an affecting tribute to someone who had played a central role in transforming heart valve replacement and then was murdered for doing this work. [email protected] On Twitter @mitchelzoler FDA approves mini heart pump for use during high-risk PCI BY ELIZABETH MECHCATIE Frontline Medical News A miniature heart pump has been approved by the Food and Drug Administration to “help certain patients maintain stable heart function and circulation during certain highrisk percutaneous coronary intervention (HRPCI) procedures,” the agency has announced. The Impella 2.5 System, manufactured by Abiomed, is “intended for temporary use by patients with severe symptomatic CAD [coronary artery disease] and diminished (but stable) heart function who are undergoing HRPCI but are not candidates for surgical coronary bypass treatment,” according to the FDA’s statement. “Use of the Impella 2.5 System is intended to prevent episodes of unstable heart function, including unstable blood pressure and poor circulation, in patients who are at high risk for its occurrence,” Dr. William Maisel, acting director of the Office of Device Evaluation in the FDA’s Center for Devices and Radiological Health, said in the statement. Approval was based on the PROTECT II study and observational data from the USpella Registry. “The overall data provided evidence that, for patients with severe CAD and diminished heart function, the temporary circulatory support provided by the Impella 2.5 System during an HRPCI procedure may allow a longer and more thorough procedure by preventing episodes of hemodynamic instability ... due to temporary abnormalities in heart function,” the FDA statement said. In addition, “fewer later adverse events,” such as the need for repeat HRPCI procedures, “may occur in patients undergoing HRPCI with the pump compared to patients undergoing HRPCI with an intra-aortic balloon pump,” according to the FDA. The FDA statement also noted that the system can be used as an alternative to the intra-aortic balloon pump “without significantly increasing the safety risks of the HRPCI procedure.” As a postmarketing requirement, the manufacturer will conduct a single-arm study of the device in high-risk PCI patients, according to the company’s statement announcing approval. The wording of the approved indication is as follows, according to Abiomed: “The Impella 2.5 is a temporary (less than or equal to 6 hours) ventricular support device indicated for use during high-risk PCI performed in elective or urgent hemodynamically stable patients with severe coronary artery disease and depressed left ventricular ejection fraction, when a heart team, including a cardiac surgeon, has determined high-risk PCI is the appropriate therapeutic option. Use of the Impella 2.5 in these patients may prevent hemodynamic instability that may occur during planned temporary coronary occlusions and may reduce peri- and postprocedural adverse events.” [email protected] THORACIC SURGERY NEWS AMERICAN ASSOCIATION FOR THORACIC SURGERY Editor Michael J. Liptay, M.D. Associate Editor, General Thoracic Sai Yendamuri, M.D. Associate Editor, Adult Cardiac Jennifer S. Lawton, M.D. Associate Editor, Cardiopulmonary Transplant Matthias Loebe, M.D. Associate Editor, Congenital Heart Robert Jaquiss, M.D. Resident/Fellow Editors: Elliot Servais, M.D., David Shersher, M.D. Executive Director Cindy VerColen Thoracic Surgery News is the official newspaper of the American Association for Thoracic Surgery and provides the thoracic surgeon with timely and relevant news and commentary about clinical developments and about the impact of health care policy on the profession and on surgical practice. Content for Thoracic Surgery News is provided by Frontline Medical Communications Inc. company. Content for the News From the Association is provided by the American Association for Thoracic Surgery. The ideas and opinions expressed in Thoracic Surgery News do not necessarily reflect those of the Association or the Publisher. The American Association for Thoracic Surgery and Frontline Medical Communications Inc. will not assume responsibility for damages, loss, or claims of any kind arising from or related to the information contained in this publication, including any claims related to the products, drugs, or services mentioned herein. POSTMASTER: Send changes of address (with old mailing label) to THORACIC SURGERY NEWS, Subscription Service, 151 Fairchild Ave., Suite 2, Plainview, NY 11803-1709 The American Association for Thoracic Surgery headquarters is located at 900 Cummings Center, Suite 221-U, Beverly, MA 01915. THORACIC SURGERY NEWS (ISSN 1558-0156) is published monthly for the American Association for Thoracic Surgery by Frontline Medical Communications Inc., 7 Century Drive, Suite 302, Parsippany, NJ 07054-4609. Phone 973-206-3434, fax 973-206-9378. Subscription price is $154.00 per year. National Account Manager Artie Krivopal, 973-206-2326, cell 973202-5402, [email protected] Classified Senior Director of Sales Tim LePella, 484-921-5001, cell 610-506-3474, [email protected] Classified Sales Representative Linda Wilson, 973-290-8243, [email protected] Advertising Offices 7 Century Drive, Suite 302, Parsippany, NJ 07054-4609 973-206-3434, fax 973-206-9378 ©Copyright 2015, by the American Association for Thoracic Surgery Scan this QR Code to visit thoracicsurgerynews.com FRONTLINE MEDICAL COMMUNICATIONS SOCIETY PARTNERS VP/Group Publisher; Director, FMC Society Partners Mark Branca Editor in Chief Mary Jo M. Dales Executive Editors Denise Fulton, Kathy Scarbeck Managing Editor Mark S. Lesney Creative Director Louise A. Koenig Print Production Manager Rebecca Slebodnik Editorial Offices 5635 Fishers Lane, Suite 6100, Rockville, MD 20852, 240-221-2400, fax 240-221-2548 Letters to the Editor: [email protected] FRONTLINE MEDICAL COMMUNICATIONS Stephen Stoneburn, Chairman Douglas E. Grose, EVP Digital Business Development/CFO Alan J. Imhoff, President/CEO JoAnn Wahl, President, Custom Solutions, 973-206-8989 [email protected] Dennis Quirk, VP, Finance Jim Chicca, Executive Director, Operations Jim McDonough, VP, Marketing & Customer Advocacy Carol Nathan, VP, Custom Programs Lori Raskin, Corporate Director, Research & Communications Donna Sickles, VP, Audience Development Subscription Inquiry Line 1-800-480-4851 In affiliation with Global Academy for Medical Education, LLC. Sylvia H. Reitman, MBA, VP, Medical Education & Conferences David J. Small, MBA, VP, Events NEWS THOR AC ICS URGE RYNE W S. COM • M AY 2015 3 Updated IMPROVE-IT results show bigger benefits BY BRUCE JANCIN Frontline Medical News S AN DIE GO – The initial presentation of the IMPROVE-IT trial at last November’s American Heart Association Scientific Sessions told only half the story of the actual clinical impact of lipid-lowering with the combination of ezetimibe and simvastatin as opposed to simvastatin alone. That’s because the main analysis included only the first cardiovascular event patients experienced. Many participants with a nonfatal first event went on to have a second, third, or even a fourth event. And while additional events haven’t traditionally been counted in acute coronary syndrome clinical trials, they should be, Sabina A. Murphy said at the annual meeting of the American College of Cardiology. “All events, not just first events, are important to patients and clinicians. Total events have implications for patient morbidity, clinical management, need for recurrent hospitalization, and total costs,” said Ms. Murphy, head of biostatistics at the TIMI Study Group at Brigham and Women’s Hospital, Boston. Analyses that include recurrent events are common in some other medical fields, including oncology and rheumatology, she added. In last November’s initial findings from IMPROVE-IT (Improved Reduction of Outcomes: Vytorin Efficacy International Trial), the combination of 10 mg ezetimibe/40 mg simvastatin (Vytorin) daily resulted in a modest yet statistically significant 6.4% relative risk reduction in the primary composite endpoint, compared with 40 mg of simvastatin alone, reported Dr. Christopher P. Cannon, professor of medicine at Harvard Medical School, Boston. Most observers hailed this result as clinically important, since IMPROVE-IT was the first study to show that lowering cholesterol with a nonstatin reduces cardiovascular events, and it showed that the lower a patient’s LDL cholesterol, the better the outcomes: The mean LDL with combination therapy was 54 mg/dL, compared with 70 mg/dL in controls. The double-blind study included 18,144 patients randomized within 10 days of an acute coronary syndrome. The primary composite outcome comprised cardiovascular death, nonfatal MI, nonfatal stroke, rehospitalization for unstable angina, and coronary revascularization. The 6.4% relative risk reduction was based solely on first events, of which there were 5,314 during a median 6 years of follow-up. But there were also 4,231 subsequent primary endpoint events, including 2,297 second events, 972 third events, and 456 fourth ones. While 170 fewer first events occurred with combination therapy than with simvastatin alone, there were also 251 fewer additional or recurrent cardiovascular events in the ezetimibe/simvastatin group that were not incorporated in the initial analysis. Here’s the key point: While the relative risk reduction for first primary endpoint events was 6.4% with combination therapy, the risk of additional events was reduced by 12%, resulting in a more substantial 9% relative risk reduction for total events. For the prespecified secondary composite endpoint consisting of death due to coronary heart disease, nonfatal MI, or urgent coronary revascularization, the initial analysis based solely upon first events showed an 8.8% relative risk reduction with ezetimibe/simvastatin. But the fuller view includes a 21% reduction in the risk of additional events, resulting in a 15% relative risk reduction for total events during a median 6 years of follow-up. In an exploratory analysis examining the harder endpoints of cardiovascular death, nonfatal MI, or cerebrovascular accident, the relative risk reduction for total events was 12% with combination therapy. Ezetimibe/simvastatin was associated with a 13% reduction in all nonfatal MIs occurring during follow-up and a 23% reduction in nonfatal strokes, according to Ms. Murphy. Among every 1,000 IMPROVE-IT participants on ezetimibe/simvastatin rather than simvastatin alone for 1 year there were 11 fewer total primary outcome events, including 5 fewer nonfatal MIs, 2 less nonfatal strokes, and 4 fewer revascularization procedures. She reported serving as a consultant to Merck and receiving research grants from AstraZeneca, Daiichi Sanko, GlaxoSmithKline, and Merck. [email protected] CoreValve receives first TAVR valve-in-valve indication BY MITCHEL L. ZOLER Frontline Medical News T he U.S. Food and Drug Administration has expanded its approved use of the CoreValve transcatheter aortic-valve replacement (TAVR) system to include patients who already have undergone aortic valve replacement and need a second valve replacement done as a valve-in-valve placement. With this action, CoreValve became the first TAVR system to receive U.S. approval for valve-in-valve use. The CoreValve System received FDA approval for TAVR performed on native aortic valves in January 2014 in patients at “extreme risk,” and in June 2014 for those at “high risk,” for surgical aortic valve replacement. Valve-in-valve TAVR is only feasible in patients with a failing bioprosthetic aortic valve: It is not for patients with a failing mechanical aortic valve. “The CoreValve System offers a less-invasive treatment option for a significant number of patients with failed tissue aortic valves whose medical teams determine that the risks associated with repeat open-heart surgery are high or extremely high,” Dr. William H. Maisel, deputy center director for science and chief scientist in the FDA’s Center for Devices and Radiological Health, said in a written statement. The CoreValve, which is designed to sit in a supra-annular DR. MAISEL location 12 mm above the aortic valve annulus, is well suited for valve-in-valve replacement because the only portion of the CoreValve that actually fills the annular space and the ring of the existing valve is the CoreValve’s sealer. This results in a tight seal that produces less paravalvular leak than when the sealer sits in a native annulus that is often deformed with calcium, noted Dr. Michael J. Reardon, professor of cardiothoracic surgery at Methodist Hospital in Houston. Because the sealer exerts pressure on the old valve ring in the annulus instead of on myocardium, placing the Core- Valve as a valve-in-valve produces much less conduction disruption and results in fewer patients who need a pacemaker after TAVR, he said. Dr. Reardon anticipates that many U.S. patients now in their 80s with a failing bioprosthetic aortic valve will be interested in nonsurgical TAVR replacement. These patients often do not want conventional open-heart surgery, he said in an interview. The FDA reviewed clinical data collected from a U.S. clinical trial with 143 patients, an agency representative said in the statement. In the clinical trial, the estimated rate of 30-day survival without major stroke was 96%, and 89% after 6 months. According to the agency, aortic valve-in-valve use of the CoreValve System should be limited to patients who need replacement of a failed tissue aortic valve but are at extreme or high risk of death or serious complications from traditional open-heart surgery. A decision as to whether the product and procedure are appropriate for a patient “should involve careful evaluation by the patient’s heart medical team, including a cardiologist and a cardiac surgeon.” The FDA said that the CoreValve System should not be used in patients who have any infection, have a mechanical aortic heart valve, cannot tolerate anticoagulant drugs, or have sensitivity to titanium, nickel, or contrast media. Dr. Maisel had no disclosures. Dr. Reardon has served as an adviser to Medtronic, the company that markets the CoreValve. [email protected] On Twitter @mitchelzoler Note in clarification With regard to the article “Hybrid revascularization remains relatively rare” in the April issue of Thoracic Surgery News (p. 9): Dr. Vinod H. Thourani wished to clarify that, as he stated in his presentation, the current work he reported on from Emory University was performed by Dr. Michael Halkos, who is the leader of hybrid revascularization at Emory, and that Dr. Halkos was lead author and researcher in several of the other studies reported upon. 4 NEWS MAY 2 0 1 5 • THO R A C IC S UR G ERY NEW S Fast-track protocol cuts lung resection complications BY PATRICE WENDLING Frontline Medical News CHICAGO – An enhanced recovery pathway reduces short-term complications and hospital stays following cancer-related lung resection without raising readmissions or emergency visits after discharge, a study showed. “A multimodal pathway for open, elective lobectomy seems to improve efficiency and quality of care,” Dr. Amin Madani, from McGill University in Montreal, said at the annual meeting of the Central Surgical Association (CSA). Prior research suggests that an enhanced recovery pathway (ERP), also known as fast-track protocols, can improve surgical outcomes, but there is little evidence to support its use and effectiveness in lung resection. Surgeons at McGill established an integrated, multimodal approach to perioperative care of these patients after creating a written, evidence-based, step-by-step pathway. Key elements, Dr. Madani explained, are standardized preoperative patient education; removal of urine drains on postoperative day 1; removal of the last chest tube by postop (POD) day 3, if there is <300 cc of drainage in 24 hours and no air leak; ambulation goals of more than 75 m thrice-daily by POD 3; introduction of solid food on POD 1; and a target discharge of POD 4. To examine the effectiveness of the pathway, the authors retrospectively analyzed outcomes in 127 patients undergoing elective lung resection for primary or secondary lung cancer receiving traditional care and 107 patients treated after the ERP was implemented in September 2012. At baseline, the two groups were similar with respect to age, sex, body mass index (BMI), American Society of Anesthesiologists (ASA) scores, pulmonary function, and smoking history. Hospital length of stay was significantly reduced after the ERP from a median of 7 days with traditional care to 6 days (P < .01), driven largely by patients with an uncomplicated hospital course who were discharged after a median of 5 days after the pathway was implemented, according to Dr. Madani. It was not the case that patients went home too early, as readmissions (5% vs. 6%) and ED visits (3% vs. 5%) were similar between both groups, he added. After the pathway was implemented, patients had earlier Foley catheter removal (POD 2 vs. 1), IV discontinuation (POD 3 vs. 2), ambulation (POD 2 vs. 1), last chest tube removal (POD 5 vs. 4), and epidural removal (POD 5 vs. 4). The enhanced recovery pathway group had fewer overall complications than did the traditional care group (37% vs. 50%; P = .03), a threefold decrease in urinary tract infections (3% vs. 12%; P < .01), and a trend toward fewer pulmonary complications (25% vs. 31%; P = .38) and surgical site infections (1% vs. 6%; P = .07), he said. DR. MADANI Despite significantly earlier removal of chest tubes after the pathway, there was no difference in the incidence of pneumothorax or pleural effusion requiring tube re-insertion, affirming that “Chest tubes were not being removed too early, causing harm to patients,” Dr. Madani said. In multivariate regression analysis adjusted for age, sex, BMI, and ASA score, there was a significant negative association between implementation of an enhanced recovery pathway and length of stay (beta, –0.18; P < .01) and complications (odds ratio, 0.46; P < .01), but not readmissions (OR, 1.59; P = .44). Early removal of chest tubes and urinary catheter were independent predictors of decreased length of stay. Dr. L. Michael Brunt, a discussant from Washington University in St. Louis, said that the development of care pathways to enhance recovery after surgery is gaining a lot of interest in the surgical community, but he went on to ask how much it cost to implement. The overall cost of the surgeon-driven initiative, involving multiple pathways for various surgical procedures, is about $120,000 annually, or $100/ patient for the 1,200 patients undergoing surgery using an ERP program at the McGill University Health Centre each year, Dr. Madani said. This cost also includes a full-time nurse practitioner now serving as the pathway coordinator and roughly $13,000 for patient education booklets, but no additional staff. An audience member questioned whether the authors have identified factors predicting which patients would fail to meet pathway goals, observing that in the colorectal field, there are patients such as the 80-year-old, narcotic-naive woman with diabetes, who simply won’t progress. “That’s a very good point, and I agree there are some patients whom you can’t fast track,” Dr. Madani replied. “Part of the deal here is that, yes, we have this protocolized pathway; however, the surgeon still has the right to change that if they feel it is important. We didn’t look at the specifics of which patient [factors] achieved adherence, but we could at some point in the future.” CSA President and session moderator Christopher McHenry, from MetroHealth Medical Center in Cleveland, said he was impressed with the study and called the findings very believable. “I think all of these recovery pathways can be very beneficial,” Dr. McHenry said in an interview. “It helps us re-look at how we’re managing our patients and see if there are ways that we can improve on their postoperative management that may lead to earlier discharge.” The study was funded by an investigator-initiated research grant from Ethicon Canada. Dr. Madani, his coauthors, Dr. Brunt, and Dr. McHenry reported having no financial conflicts. [email protected] Digoxin linked to higher mortality in AFib patients EWPATIES BY PATRICE WENDLING Frontline Medical News SAN DIEGO – Digoxin increases the risk of death by 27% in patients with atrial fibrillation, a meta-analysis of 19 studies showed. Patients with AF and kidney failure faced a 60% to 70% increase in mortality, compared with their counterparts not taking digoxin, according to a press release on the study. A weaker association between digoxin and death was observed in AF patients who also had heart failure, a finding the authors suggest warrants further investigation. “Until further research can be done, I would suggest physicians use caution when prescribing digoxin for patients with atrial fibrillation, especially given that there are alternative drugs available that might be safer,” lead author Dr. Waqas Qureshi said in a statement. The results were released in advance of their March 15 presentation at the annual meeting of the American College of Cardiology in San Diego. About 5.6 million Americans have atrial fibrillation and roughly 1 in 5 are prescribed digoxin for heart rate control. Current guidelines recommend digoxin as first-line therapy in patients who aren’t physically active and as a second-line drug for more active patients. “Based on consistent results com- ing out of many studies, our results suggest digoxin should be downgraded from its position as a front-line agent for certain patients with atrial fibrillation,” Dr. Qureshi, a clinical and research cardiology fellow at Wake Forest School of Medicine in Winston-Salem, N.C., recommended. The authors reviewed 19 studies including five cohort and randomized controlled trials involving 501,681 patients. Of these, 458,311 patients had AF and 111,978 were prescribed digoxin. In a random effects model, digoxin was associated with an increased risk of mortality, with a pooled hazard ratio of 1.27 (95% confidence interval 1.19-1.36; P < .001). Several studies in the meta-analysis suggest that higher blood levels of digoxin increase the risk of death. The mechanism behind the increased mortality is not known, although previous studies have suggested digoxin increases the risk of thromboembolism. The meta-analysis accounted for risk factors and comorbidities reported in the various studies, but it’s possible that some confounding factors may not have been accounted for, the authors acknowledge. “The study points to the need for a well-structured, targeted trial to investigate digoxin’s safety,” Dr. Qureshi stated. [email protected] CONGENITAL HEART DISEASE THOR AC ICS URGE RYNE W S. COM • M AY 2015 5 Linking registries, databases may reduce SSIs Database (STS-CHSD). To further facilitate the flow and interpretation of data, the invesurveillance of cardiac surgical tigators used a visualization tool site infections (SSIs) improved to analyze the STS-CHSD for case significantly when ascertainment; to resolve registry and infection discrepancies among STScontrol surveillance data CHSD, infection surveilwere linked with electronic lance, and billing of SSI health records, a retrospeccases; and to assess the imtive analysis showed. pact of the hospital’s qualiOver the course of a ty improvement protocols. 47-month period starting These protocols consistin 2011, Vaidehi Nayar of ed of wound alert reports the Children’s Hospital from the EHR, bedside reDR. NAYAR of Philadelphia and her views for SSI adjudication, coinvestigators launched inpatient and outpatient a quality improvement initiative at SSI prevention bundles, prophylactic their institution that linked adminantibiotic dosing changes, removal of istrative databases with their clinical steroids from the bypass circuit, and registry, allowing caregivers to more biller education on SSIs. accurately monitor and assess SSIs Control charts in the data visuand provide more effective adjudicaalization tool allowed for statistical tion and treatments thereafter. monitoring of SSI rate changes, and The investigators chose to link SSI case discrepancies across the datheir hospital’s electronic health tabases were reviewed to ensure that record (EHR) billing information differences were the result of variaand reporting from the infection tions in SSI reporting criteria for each surveillance database for the Nationdatabase, not inaccurate surveillance al Healthcare Safety Network with population ascertainment or inaccudata from the Society of Thoracic rate SSI identification, according to Surgeons Congenital Heart Surgery Ms. Nayar and her colleagues, BY DEEPAK CHITNIS PERSPECTIVE Frontline Medical News S AATS CARDIOVASCULAR VALVE SYMPOSIUM 2015 SAVE THE DATE T his study demonstrates dramatically different surgical site infection (SSI) rates for the same patient cohort as detected by three different surveillance methods: hospital billing (derived from the electronic health records), a surgical database, and a tracking system developed by the Centers for Disease Control and Prevention. On the low end, 79 SSIs were reported by one system, 156 by another, and 433 by the third method – a more than fivefold discrepancy. The authors developed a technique to reconcile the three systems and then evaluated a variety of interventions designed to reduce the SSI rate. As a result of this initiative, the quality of event reporting was improved (with greater agreement between reporting methods) and the rate of SSIs was reduced. The implications of this report are sobering and should be of great “Workflow changes, including the wound alert report and bedside reviews, facilitated communication interest to all surgeons and hospital administrators for several reasons. First and fundamentally, the report suggests that widely used reporting systems may be inaccurate and produce conflicting results. Since the results of these reports are used to assess and modify clinical practice, this is very disturbing. Additionally, the results may be used by payers as a basis for financial reward (or penalty) and therefore must be accurate. Finally, exposure of the use of erroneous information as the source data for billing may render an institution vulnerable to civil and criminal penalties. For all of these reasons, the present report should prompt self-assessment by all institutions, if it has not already been undertaken. Dr. Robert Jaquiss is associate medical editor for congenital heart disease for Thoracic Surgery News. among providers and improved adjudication of suspected SSIs,” she said Continued on following page COURSE DIRECTORS David H. Adams Mount Sinai School of Medicine New York, New York, USA Joseph S. Coselli Baylor College of Medicine Houston, Texas, USA Walter J. Gomes Federal University of São Paulo São Paulo, Brazil Pedro J. del Nido Boston Children’s Hospital Boston, Massachusetts, USA Thoralf M. Sundt, III Massachusetts General Hospital Boston, Massachusetts, USA November 20 - 21, 2015 Renaissance Marriott São Paulo São Paulo, Brazil www.aats.org/valvebrazil 6 CONGENITAL HEART DISEASE Continued from previous page in presenting the J. Maxwell Chamberlain Memorial Paper for Congenital Heart Surgery at the annual meeting of the Society of Thoracic Surgeons in San Diego earlier this year. In total, 156 SSIs were identified via THE OFFICIAL NEWSPAPER OF THE the STS-CHSD, 79 via the infection surveillance database, and 433 via billing. There was a significant decrease in the rolling 12-month SSI rate from 2.48% (21/848 in January 2013) to 0.76% (11/1,442 in January 2014), based on the STS-CHSD data, although Ms. Nayar pointed out that MAY 2 0 1 5 • THO R A C IC S UR G ERY NEW S Accurate assessment of SSI data ‘has implications for public reporting, benchmarking, assessment of [quality improvement] impact, and possible denial of payments.’ ® Serving the cardiothoracic community since 2005 with news, features, and expert analysis from the United States and around the world. Read our Print, Interactive app and Digital Edition! this decline could not definitely be attributed to reporting improvements or to the specific quality improvement initiatives that were implemented. Ms. Nayar also explained that there was a “general improvement in reporting, as shown by the stark drop in billing” and “a general alignment of all three data sources.” “Accurate assessment of morbidity data, including [SSIs], has implications for public reporting, benchmarking, assessment of [quality improvement] impact, and possible denial of payments,” said Ms. Nayar. “In summary, we achieved our two simultaneous goals of improving SSI reporting – or decreasing the data errors – and decreasing SSI incidents by improving overall patient care.” During discussion, Ms. Nayar elaborated on the study’s generalizability and potential application to other facets of congenital heart disease treatments, saying that such application is, in fact, possible. “Yes, this is very generalizable, but one key important fact is relevant: As long as there is a source of truth for case ascertainment, this methodology can be used in several different areas,” she explained. “For example, we are currently working at our institution to integrate and link the [Pediatric Cardiac Critical Care Consortium] database to be able to better monitor any critical care–related morbidity information and ultimately use similar methodology to assess the impact of outcomes in the critical care field.” Ms. Nayar said that she did not have any relevant financial conflicts of interest to disclose. [email protected] For daily updates follow @ThoracicTweets on Follow us on Twitter (@ThoracicTweets) and like us on Facebook. www.thoracicsurgerynews.com and Thoracic Surgery News on ACQUIRED CARDIAC DISEASE THOR AC ICS URGE RYNE W S. COM • M AY 2015 7 26% 1-year death, Restrictive vs. liberal stroke rate after TAVR transfusion after surgery BY MARY ANN MOON Frontline Medical News O ne year after transcatheter aortic valve replacement in the United States, the overall mortality was 23.7%, the stroke rate was 4.1%, and the composite outcome of death and stroke was 26.0%, according to a report published in JAMA. Long-term outcomes for TAVR haven’t been well studied until now, yet the procedure is being performed with increasing frequency for aortic stenosis in patients who are too high risk to undergo conventional surgical aortic valve replacement, said Dr. David R. Holmes Jr. of the Mayo Clinic, Rochester, Minn., and his associates. They assessed 1-year outcomes by analyzing administrative data from the Centers for Medicare & Medicaid Services and clinical data from the Transcatheter Valve Therapies Registry, an initiative of the Society of Thoracic Surgeons and the American College of Cardiology. The study involved 12,182 patients who underwent TAVR at 299 medical centers across the country during a 19-month period. The patients’ median age was 84 years; 95% were white and 52% were women. The transfemoral approach was used in most patients, but alternative approaches were used in roughly 44%. As expected for an elderly, highrisk study population, baseline functional status was poor and comorbidities were common. They included reduced left ventricular ejection fraction (26% of patients), prior stroke (12%), moderate or severe lung disease (28%), renal failure (16%), peripheral vascular disease (32%), and atrial fibrillation (42%), Dr. Holmes and his associates reported (JAMA 2015 March 10 [doi:10.1001/ jama.2015.1474]). In addition to the mortality and stroke rates listed above, the 1-year rate of one rehos- pitalization was 24.4%, that of two rehospitalizations was 12.5%, and that of three or more rehospitalizations was 11.6%. The 1-year readmission rate specifically for stroke, heart failure, or repeat aortic valve intervention was 18.6%. These are important considerations for elderly, fragile patients because rehospitalizations indicate “an unacceptable quality-of-life outcome” and are very costly, the investigators noted. Several baseline charac‘It may be possible [from this data] to identify patients who may not benefit from this procedure.’ DR. HOLMES teristics, including male sex, severe chronic obstructive pulmonary disease, dialysis-dependent end-stage renal disease, older age, higher STS Predicted Risk of Operative Mortality (PROM) score, a history of atrial fibrillation/flutter, and use of an access route (other than transfemoral), were found to be independently associated with higher 1-year mortality. Thus, “It may be possible to identify patients who may not benefit from this procedure and who should be counseled accordingly.” For example, in this study there was a small (77 patients) very high-risk subset of patients – aged 85-94 years, dependent on dialysis, and having an STS PROM score greater than 15% – whose 1-year mortality was 53.5%. The STS and the ACC supported this study, and support the Transcatheter Valve Therapies Registry. Dr. Holmes reported having no relevant financial disclosures; his associates reported ties to Boston Scientific, Edwards Lifesciences, Janssen, Eli Lilly, Boehringer Ingelheim, Bayer, and AstraZeneca. BY MARY ANN MOON Frontline Medical News A fter cardiac surgery, using a restrictive transfusion threshold – forgoing transfusion until hemoglobin level drops to 7.5 g/dL – does not decrease morbidity or costs of care, compared with using a liberal transfusion threshold of 9 g/dL, according to a report published online in the New England Journal of Medicine. Several blood management guidelines and health policy statements recommend the restrictive approach in the hope that it will reduce the increasing demand on blood services and the high costs of storing, handling, and administering redcell units, and also because transfusions following cardiac surgery have been linked to infection, low cardiac output, acute kidney injury, and increased mortality. Clinicians remain uncertain about a safe threshold for transfusions in this setting, which is evidenced by the striking variation in transfusion rates among cardiac centers in the United States (8%-93%) and the United Kingdom (25%-75%), said Dr. Gavin J. Murphy of the British Heart Foundation and department of cardiovascular sciences, University of Leicester (England) and his associates. They performed the Transfusion Indication Threshold Reduction (TITRe2) study to test the hypothesis that the restrictive approach is superior to the liberal approach regarding both postoperative morbidity and health care costs. Adults undergoing nonemergency cardiac surgery at 17 specialty centers in the United Kingdom were randomly assigned to a restricted (1,000 patients) or a liberal (1,003 patients) transfusion threshold. The median patient age was 70 years, and 68% were men. Most of the procedures were CABG or valve surgeries. Contrary to expectations, the primary outcome – a composite of serious infection or an ischemic event such as stroke, MI, gut infarction, or acute kidney injury within 3 months – occurred in 35.1% of patients in the restrictive-threshold group and 33.0% in the liberal-threshold group. Secondary outcomes, including length of ICU stay and rates of clinically significant pulmonary complications, also were similar between the two study groups. Rates of other serious postoperative complications were similar, at 35.7% and 34.2%, as was general health status as assessed via the EuroQol Group 5-Dimension Self-Report Questionnaire, further contradicting the study hypothesis. Mean health care costs were similar between the two study groups: the equivalent of $17,762 with restrictive-threshhold transfusions and $18,059 with liberal-threshold transfusions, Dr. Murphy and his associates noted (N. Engl. J. Med. 2015 March 12 [doi:10.1056/NEJMoa1403612]). Unexpectedly, 3-month mortality was significantly higher with restrictive- than with liberal-threshold transfusions (4.2% vs 2.6%). This association persisted in sensitivity analyses and “is a cause for concern,” but it may be due to chance alone, the investigators added. PERSPECTIVE F indings like those of Murphy et al. provide a great opportunity for discussion and debate, which could lead to development of a consensus on the best postoperative care for these patients. Cardiac surgery departments should review the TITRe2 trial results and decide which threshold they deem to be the most appropriate for transfusion. The extreme range in hospitals’ rates of transfusion in cardiac surgery – from less than 5% to more than 90% – is extraordinary. Having clinicians actively debate the evidence presented in TITRe2, create transparent interpretations, develop protocols, and hold themselves accountable for following those protocols would represent important steps for improving patient care. John Spertus, M.D., is at the University of Missouri-Kansas City and Saint Luke’s Mid America Heart Institute, Kansas City. He reported receiving grant support from Lilly, Gilead, Amorcyte, Genentech, and Abbott Vascular; receiving personal fees from United Healthcare, Novartis, and Amgen; having an equity interest in Health Outcomes Sciences; and owning copyrights to the Seattle Angina Questionnaire, the Kansas City Cardiomyopathy Questionnaire, and the Peripheral Artery Questionnaire. Dr. Spertus made these remarks in an editorial accompanying Dr. Murphy’s report (N. Engl. J. Med. 2015 March 12 [doi: 10.1056/ NEJMe1415394]). 8 ACQUIRED CARDIAC DISEASE Mortality risk after CABG Stents from page 1 j.jtcvs.2015.01.051). This study investigated whether diabetic patients with triple-vessel disease and a stent had poorer outcomes because of endothelial dysfunction and the strain of triple-vessel disease on the heart. The final study comprised 1,583 diabetic patients with triple-vessel disease, 202 (12.8%) of whom had coronary stents. The study defined triple-vessel disease as blockages of 50% or more in all three native coronary vessels or left main artery plus right coronary artery disease. Early mortality rates – death within 30 days of the procedure – were similar between the two groups: 3.3% overall, 3% in the prior-PCI group, and 3.3% in the no-PCI group; therefore, prior PCI was not a predictor of early mortality. Five-year cumulative survival was 78.5% in the no-PCI group, compared with 74.8% in the PCI group. When adjusting for a variety of clinical variables before CABG, stenting was associated with a 39% greater mortality at 5 years. The investigators found the emergence of drug-eluting stents during the 10-year study period did not contribute significantly to outcomes. The cause of death was known for 81.7% (282 of 345) of the deaths in the overall cohort, with 5-year cardiac deaths higher in the PCI-S group: 8.4% vs. 7.5% for the no-PCI group. MAY 2 0 1 5 • THO R A C IC S UR G ERY NEW S “Notably, 100% of PCI-S cardiac mortality was categorized as coronary heart disease related compared to 89.3% (92/103) of cardiac mortality in the no-PCI group.” Dr. Nauffal and his colleagues concluded that: “An early team-based approach including a cardiologist and cardiac surgeon should be im- plemented for optimal revascularization strategy selection in diabetics with triple-vessel disease and for close medical follow-up of those higher risk CABG patients with history of intracoronary stents.” The Johns Hopkins Murex Research Award supported Dr. Nauffal. The authors had no other disclosures. PERSPECTIVE B ecause diabetes affects vascular physiology and can lead to multivessel disease, surgical revascularization vs. percutaneous coronary intervention has proved more successful in diabetic patients, Dr. Paul Kurlansky said in his invited commentary. However, “the potential impact of newer generation drug-eluting stents on improving these results remains to be seen,” he wrote ( J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/ j.jtcvs.2015.02.007). Comparing CABG and PCI in diabetic patients has been challenging for a variety of reasons, including the nuances of clinical judgment and different techniques. “It is in this gray zone of clinical ambiguity that many if not most patients actually reside,” he said, giving credit to Dr. Nauffal and his colleagues for trying to address this ambiguity. The study data, however, had many limitations, Dr. Kurlansky said. The authors could not specify indications for stent deployment, disease severity at the time of stenting and the choice of procedure among them. “An equally plausible hypothesis might therefore suggest that the appropriate need for prior stenting identified a subset of patients with more aggressive disease who therefore succumbed at an earlier age,” he said. CABG that utilizes the internal mammary artery has been linked to enhanced physiologic properties that promote vasodilatation, inhibit thrombosis and atherosclerosis, and support the health of the vascular endothelium, he noted. In the diabetic patient, these properties may enhance the ability of CABG to address not only arterial blockages, but also the underlying physiology of atherosclerosis. “With the rising tide of diabetic vasculopathy, it will become increasingly important to consider both clinical utility and underlying physiology in navigating the uncertain path to optimal patient care,” Dr. Kurlansky wrote. Dr. Kurlansky is with the department of surgery at Columbia University, New York. AMERICAN ASSOCIATION FOR THORACIC SURGERY We Model Excellence AATS FOCUS ON THORACIC SURGERY:TECHNICAL CHALLENGES AND COMPLICATIONS SAVE THE DATE October 23-24, 2015 PROGRAM DIRECTORS Seaport Hotel and World Trade Center Boston, MA, USA G. Alec Patterson David J. Sugarbaker www.aats.org THOR AC ICS URGE RYNE W S. COM • M AY 2015 CARDIOPULMONARY TRANSPLANTATION 9 Low-volume centers have poorest results with ECMO BY DEEPAK CHITNIS Frontline Medical News SAN DIEGO – Lung transplantation centers that are considered low volume tend to have lower rates of survival than do those of their medium- and high-volume counterparts when patients are bridged to transplant using extracorporeal membrane oxygenation (ECMO), according to researchers. “Increasingly, [ECMO] is used as a bridge to lung transplantation; indeed, the use of ECMO has tripled over the past 15 years and survival has increased by the same magnitude,” Dr. Jeremiah A. Hayanga said at the annual meeting of the Society of Thoracic Surgeons. “An entire body of literature has linked high-volume [centers] to improved outcomes in the context of complex surgical procedures. Lung transplantation [LTx] falls within the same domain, and has been considered subject to the same inverse volume-outcome paradigm,” said Dr. Hayanga of Michigan State University, Grand Rapids. He and his coinvestigators conducted a retrospective analysis of 16,603 LTx recipients in the International survival rates when ECMO was Registry for Heart and Lung Transused for bridging. plantation who underwent ECMO as One-year survival probability was their bridging strategy between 2005 roughly 40% in low-volume centers and 2010. and roughly 70% in high-volume Centers were stratified into catego- centers, while 5-year survival probries of low, medium, and high based ability was well under 25% for reon the volume of LTx procedures cipients from low-volume centers they performed over the study interand around 50% for those from val: Low was defined as fewhigh-volume centers (P er than 25, medium as 25-50, = .0006). No significant and high volume as more differences existed for than 50. non-ECMO patients, Overall, 85 of the 16,603 regardless of center voltransplant recipients in ume. the study population were “No differences existed bridged via ECMO: 20 in survival in medium(23.5%) of them in low-voland high-volume cenume centers, 30 (35.3%) in ters,” said Dr. Hayanga. DR. HAYANGA medium-volume centers, “Transplanting withand 35 (41.2%) in high-volout ECMO as a bridge ume centers. The researchers used showed fewer survival differences Cox proportional hazard modeling [among centers] for both 1-year to identify predictors of both 1- and and 5-year survival. However, when 5-year survival rates, which were ECMO was used as a bridge, the found to be significantly lower in low-volume center [survival rates] low-volume centers – 13.61% at 5 were dramatically lower at both 1 years post LTx. year and 5 years.” Looking at just the high-volume When Dr. Hayanga and his and low-volume centers, the recolleagues examined procedural searchers noted “significant differvolume as a continuous variable, ences” in both 1-year and 5-year however, a single inflection point was determined as the point at which survival outcomes steadily improve – 19 procedures. Centers that performed at least 19 LTx procedures between 2005 and 2010 experienced an uptick in survival rates, even though centers that saw 19-25 procedures were still considered low volume, the researchers noted. “The corresponding C-statistic, however, is just under 60%,” cautioned Dr. Hayanga. “The C-statistic is a measure of the explanatory power of a variable – in this case, [center] volume – in accounting for the variability in outcome, or survival in this case. To put that number into context, a C-statistic of 50% means ‘no explanatory power’ whatsoever.” Dr. Hayanga explained that he and his coauthors compared transplant recipient and donor characteristics using analysis of variance (ANOVA) and chi-square tests to compare variables, cumulative survival using Kaplan-Meier curves, and significance using log-rank tests. Dr. Hayanga reported no financial conflicts of interest. [email protected] GENERAL THORACIC 10 MAY 2 0 1 5 • THO R A C IC S UR G ERY NEW S Biopsy bests HRCT for lung fibrosis, has risks BY RICHARD M. KIRKNER Frontline Medical News S urgical lung biopsy performs well and is relatively safe for evaluating suspected interstitial lung diseases, but may be especially helpful in confirming the diagnosis and directing the treatment of patients with idiopathic pulmonary fibrosis with atypical signs and symptoms, researchers have found. In patients with immune disorders or severe respiratory dysfunction, or on mechanical ventilation, clinicians should weigh the diagnostic benefits of surgical lung biopsy (SLB) against its potential risks, according to a systematic review and meta-analysis of 23 studies that were published In 8 studies, biopsy influenced a change in treatment plan 42%-90% of the time. Overall, treatment plans were altered for 59.5% of patients who received a specific diagnosis and in 55.2% of those without a definitive diagnosis. between 2000 and 2014, comprising 2,148 patients. Dr. Qian Han of the Guangzhou Institute of Respiratory Disease in China led the investigative team. The findings were published in the May issue of the Journal of Thoracic and Cardiovascular Surgery. The meta-analysis focused on diagnostic yield of biopsy samples and postbiopsy mortality within 90 days of surgery ( J. Thorac. Cardiovasc. Surg. 2014 [doi:10.1016/j. jtcvs.2014.12.057). The mean age of patients across the studies ranged from 36 to 62 years. The population of the meta-analysis included 1,632 (76%) who had undergone video-assisted thoracic surgery (VATS) and 268 (12.5%) who had open-lung biopsy. Slightly more than one third (33.5%) of diagnoses involved idiopathic pulmonary fibrosis, followed by nonspecific interstitial pneumonia (12%), hypersensitivity pneumonitis (9.6%), cryptogenic organizing pneumonia (7.5%), sarcoidosis (6.8%), and connective tissue disease related to interstitial lung disease (4%). The median diagnostic yield across all studies was 95%, ranging from 42% to 100% depending on the study. One study showed a diagnostic yield below 70%. Eight studies showed that the biopsy influenced a change in the treatment plan 42%-90% of the time. In the entire meta-analysis, treatment plans were altered for 59.5% of patients who received a specific diagnosis and in 55.2% of those without a definitive diagnosis. “These results suggested that an alteration in treatment may not be directed by a definitive histological diagnosis, and nonspecific histological results could also be useful in clinical practice,” Dr. Han said. Eleven of the studies used CT guidance to obtain biopsies without a preference to lobe, but two studies predisposed to the right lobes had diagnostic yields of 84% and 94%. One study avoided the lingual or middle lobe, with a diagnostic yield of 97%, and another focused on the lingular lobe only, and demonstrated a 100% yield. Two studies showed that biopsy samples from lingual or middle lobes had the same diagnostic yield as did those from other lobes. With regard to diagnostic performance based on biopsy numbers, one PERSPECTIVE T he role of surgical biopsy in the high-risk population with interstitial lung disease is well suited for surgical review because thoracic surgeons must weigh the risks, including potential mortality, and benefits when discussing options with patients and families, Dr. Katie S. Nason noted in her invited editorial commentary. Current guidelines suggest that SLB is no longer essential for diagnosis of idiopathic pulmonary fibrosis and they now consider an HRCT scan showing unusual interstitial pneumonia (UIP) sufficient for diagnosis. “However, in the absence of diagnostic imaging criteria for UIP, specifically honeycombing, surgical lung biopsy with inter- study showed that multiple biopsies may increase the diagnostic yield. Twelve studies obtained one to three samples, and among them eight studies suggested that one sample containing both lesion and normal tissue was sufficient to represent pathological changes. One study showed that multiple biopsies may increase diagnostic yield. Of the 16 studies that provided sufficient data on mortality rates, the pooled 30- and 90-day mortality rates were 2.2% (95% CI, 1.0-4.0) and 3.4% (95% CI, 1.8-5.5), respectively. The composite postoperative mortality rate was 3.6% (95% CI, 2.1-5.5). In their discussion, Dr. Han and colleagues addressed the controversy surrounding the use of lingual vs. middle lobe biopsy by noting that high-resolution CT (HRCT) can be valuable in identifying the appropriate biopsy location. While multiple studies supported the effectiveness of only one biopsy as long as it contained both normal and abnormal tissue, the researchers pointed out that future studies evaluating biopsy samples would do well to evaluate biopsy number combined with sample size. HRCT, while highly specific, may be less sensitive than SLB in the diagnosis of idiopathic pulmonary fibrosis, they found. Two studies that the meta-analysis looked at compared the diagnostic yield between SLB and HRCT; SLB finally diagnosed idiopathic pulmonary pretation by an expert pathologist is necessary and should be performed to further define patients with possible UIP,” Dr. Nason wrote. “Comprehensive application of this approach will delineate circumstances in which a surgical biopsy will be more informative than an HRCT scan as well as when a surgical biopsy is not necessary.” She called for a multi-institutional, international registry to collect and better understand data on the diagnostic yield and mortality after SLB for interstitial lung disease. Dr. Nason is an assistant professor of cardiothoracic surgery at the University of Pittsburgh. fibrosis in 75%-91% of suspected cases and in 19%-74% of cases when HRCT did not raise suspicion of the disease. “These findings suggested that HRCT, albeit highly specific, is less sensitive in the diagnosis of IPF, therefore necessitating the utility ‘These findings suggested that HRCT, albeit highly specific, is less sensitive in the diagnosis of IPF, therefore necessitating the utility of SLB in the diagnosis of these HRCT-omitted cases.’ of SLB in the diagnosis of these HRCT-omitted cases,” they wrote. On the safety issue, while studies that excluded patients on mechanical ventilation reported lower mortality rates and two studies identified ventilator dependence as an independent risk factor for mortality, the investigators reported that the higher mortality rates were probably the result of a sicker patient population rather than the SLB procedure itself. They wrote that to “indiscreetly refuse” to perform SLB in these patients is “overcautious and inappropriate” given the benefits of SLB in validating diagnoses and influencing treatment plans. Dr. Han and his colleagues reported having no relevant disclosures. RESIDENTS CORNER THOR AC ICS URGE RYNE W S. COM • M AY 2015 11 Why cardiac surgeons must adopt the appropriate percutaneous skills to stay relevant BY RICHARD M. KIRKNER Frontline Medical News W ith the widespread adoption of transcatheter aortic valve replacement and the public’s embrace of minimally invasive procedures, cardiac surgeons must adapt quickly to stay relevant in the future, and that means acquiring skills to perform percutaneous procedures, Dr. Tom C. Nguyen and Dr. Isaac George wrote in the Young Surgeon column in the May issue of the Journal of Thoracic and Cardiovascular Surgery. Drawing upon their own year in a structural heart endovascular fellowship, Dr. Nguyen and In fact, in order to provide the best comprehensive care for patients, a collaborative heart team including cardiologists and surgeons who all are equally proficient in endovascular techniques is essential. Dr. George both called for a new approach to surgical training that encompasses percutaneous technology and procedures, “with a caveat that failure to do so will exclude surgeons from treat- ing valve disease altogether in the future” ( J. Thorac. Cardiovasc. Surg. 2015;149:675-77 [doi: 10.1016/j.jtcvs.2014.11.091]). In making their case, Dr. Nguyen and Dr. George invoked psychologist Abraham Maslow’s famous “law of the instrument,” saying: “I suppose it is tempting, if the only tool you have is a hammer, to treat everything as if it were a nail.” Dr. Nguyen is with the University of Texas and Memorial DR. NGUYEN Hermann Heart and Vascular Institute in Houston. Dr. George is with New York-Presbyterian Hospital and Columbia University in New York. Cardiac surgeons must break out of that sort of limiting mindset and learn from the evolution of vascular surgery, which was once just a domain of general surgery but then evolved into its own specialty, they said. Patients with peripheral vascular disease who were once surgical candidates instead opted for less-invasive endovascular procedures as interventional radiology techniques advanced. “This direction may have had devastating consequences for vascular surgeons if it were not PERSPECTIVE D r. Nguyen and Dr. George address an important current topic regarding the need for cardiothoracic surgeons to quickly adopt and become experts in nontraditional techniques (percutaneous, minimally invasive interventions). Alluding to the historic failure of cardiac surgeons to adopt early angiography (and subsequently lose a valuable share of the market to interventional cardiology) and citing vascular surgeons who aggressively avoided this fate (by being early adopters of endovascular techniques), the authors propose an alternate schema moving forward. As is clear, TAVR is here to stay. There is a growing emphasis on percutaneous and minimally invasive cardiac interventions that require an elaborate set of nontraditional skills (access, wires, fluoroscopy, angiography, endostenting, and percutaneous closure, to name a few) that take time and experience to develop. Programs are currently mandated by the Centers for Medicare & Medicaid Services to team a cardiologist and a cardiac surgeon for reimbursement, although this limitation may eventually be eased. When that happens, will cardiac surgeons have the market share, hospital privileges, and experience to be able to independently handle a TAVR case? If not, will the cardiac surgeon play second fiddle to an experienced interventional cardiologist as valvular disease will become increasingly better managed without a traditional sternotomy? This issue is critical to the young cardiothoracic trainee. How do “the cardiac surgeons of the past … transform into the surgeons of the future?” Dr. Nguyen and Dr. George propose a three-pronged approach: early clinical adoption (mainly by attendings, departments, and institutions); appropriate training; and innovation to move technology forward. The discussed training arm is critical and requires dedicated time. Both authors spent 1 year as advanced fellows in structural heart disease, and only after a high-volume, multidisciplinary experience did they become more facile with catheter-based techniques. I agree with the authors’ conclusion that advanced fellowship training in percutaneous and endovascular techniques (which includes intimate collaboration with cardiology) is critical. This advanced training needs to be regulated and restricted to centers of high-volume excellence, where the surgeon is capable of being the team leader, thus making it a much more robust learning experience. Dr. David D. Shersher is one of the resident medical editors for Thoracic Surgery News. for their ability and willingness to learn new skills so that they could also perform catheter-based interventions,” according to Dr. Nguyen and Dr. George. Catheter-based treatment for heart valve disease is following a similar path, but that doesn’t mean cardiac surgeons should vacate this field to cardiologists. “In fact, in order to provide the best comprehensive care for patients, a collaborative heart team including cardiologists and surgeons who all are equally proficient in endovascular techniques is essential,” they wrote. Further, if surgeons can work independently of cardiologists by learning and adopting percutaneous techniques, new technologies will be able to advance even faster. “Surgeons have an intimate knowledge of the heart that is unmatched by any specialty; translation of this knowledge into structural heart valve technology is logical and needed,” Dr. Nguyen and Dr. George said. Also, surgeons well versed in all techniques – endovascular, minimally invasive surgery, and conventional surgery – will be equipped to objectively offer the procedure that’s best suited for the patient rather than their own skill set. Acquiring the necessary percutaneous skills, however, poses a high hurdle for cardiDR. GEORGE ac surgeons. They must be able to perform the entire transapical and transaortic transcatheter aortic valve replacement (TAVR) procedure and thus seize the currently held lead for the procedure from the cardiologist, accordResidents continued on page 15 12 NEWS FROM AATS MAY 2 0 1 5 • THO R A C IC S UR G ERY NEW S F. Griffith Pearson Fellowship Awardees Named T he AATS is proud to announce the awardees of the F. Griffith Pearson Fellowship, the first “Honoring Our Mentors” Fellowship. The program acknowledges the leadership and dedication of surgeons in the field. to defray living expenses during his four to six weeks of training. DR. SANCHEZ The awardees are Pablo Sanchez and James L. Lubawski, Jr. The fellowship supports surgeons who have finished their residencies, allowing them to advance their clinical techniques at a North American institution. Each winner will receive $3,500 DR. LUBAWSKI Pablo Sanchez, MD Institution: University of Maryland Host Institution: Toronto General Hospital, Toronto Lung Transplant Program Fellowship Focus: Build Ex Vivo Perfusion skills James L. Lubawski, Jr., MD Institution: Central DuPage Hospital (Illinois) Host Institution: The University of Texas MD Anderson Cancer Center Fellowship Focus: Advanced lung cancer cases Apply Today for the Advanced Valve Disease Educational Fellowship Sponsor: Medtronic Fellowship Overview: Offers surgeons the opportunity to interactively observe valvular heart disease specialists and connect with them about treatment, technical skills and management of perioperative patients for a minimum of one month up to three months Potential Host Institutions Cleveland Clinic Johns Hopkins University Mount-Sinai Medical Center New York University University of Southern California Deadline: June 15, 2015 More information/application submission: http://aatsgrahamfoundation.org/awards_valveEDU.cgi First Edwards Lifesciences Advanced Treatments of Valve Disease Fellow Chosen V ictor Dayan has been named the first Edwards Lifesciences Advanced Treatments of Valve Disease Fellow. He will receive a $25,000 award to defray travel and living expenses for a minimum of three months training at a host institution in valve repair, transcatheter repair or replacement of valves. DR. DAYAN Victor Dayan, MD Institution: Hospital de Clinicas, Centro Cardiovascular (Montevideo, Uruguay) Host Institution: Mayo Clinic Fellowship Focus: Enhancing clinical techniques in valve disease Applications Now Open for the Advanced Endobronchial Ultrasound (EBUS) Training Fellowship Sponsor: Olympus America Fellowship Overview: Permits young North American thoracic surgeons to spend between one and six months studying clinical techniques at an EBUS-proficient institution. Host Sites Toronto General Hospital, Division of Thoracic Surgery University of Texas MD Anderson Cancer Center Deadline: June 1, 2015 More information/application submission: http://aatsgrahamfoundation. org/awards_advancedEBUS.cgi Submit Today for the James L. Cox Fellowship in Atrial Fibrillation Surgery Also Don’t Miss These Important Fellowship & Training Opportunities This Spring Sponsor: AtriCure Sentara Heart Hospital (Norfolk, VA) Swedish Medical Center (Englewood, CO) University of Pittsburgh Medical Center University of Virginia Washington University School of Medicine, Barnes Jewish Hospital (St. Louis, MO) Ethicon Fellowship for Advanced Thoracic Minimally Invasive Surgery (MIS) Sponsored by Ethicon Endo-Surgery Offers North American young CT surgeons and their surgical teams the opportunity to enhance their skills in thoracic minimally invasive surgery by spending a one- or two-day period at clinical sites. Thoracic Surgery Training Fellowship Sponsored by Ethicon China/Chinese International Medical Foundation Offers young Chinese surgeons the opportunity to spend between one month and one year obtaining advanced thoracic surgery skills at North American institutions. Deadline: May 26, 2015 More information/application submission: http://aatsgrahamfoundation.org/awards_atricure. cgi Learn more: http://aatsgrahamfoundation.org/activities.cgi Learn more about eligibility and application requirements: http://aatsgrahamfoundation.org/ activities.cgi Fellowship Overview: Gives newly graduated CT surgeons the opportunity to spend up to three months improving their atrial fibrillation techniques at a host institution. Potential Host Sites Franciscan St. Francis Hospital (Indianapolis, IN) Inova Fairfax Hospital (Fairfax, VA) Pauley Heart Center at Virginia Commonwealth University Health System Deadline: May 31, 2015 Deadline: May 31, 2015 NEWS FROM AATS THOR AC ICS URGE RYNE W S. COM • M AY 2015 13 AATS Launches Lung Cancer Screening Calculator Online T he American Association for Thoracic Surgery (AATS) has launched a Lung Cancer Screening Calculator to help individuals determine whether or not they should seek diagnostic screening. The tool is especially relevant given that the Centers for Medicare and Medicaid Services (CMS) announced on February 5, 2015 that Medicare will now cover an annual CT lung cancer screening for patients that meet certain criteria. AATS was very involved in the process of getting CMS to approve such screenings. Covered individuals must: ** Be between ages 55 and 77, who are currently smokers or quit within the last 15 years. ** Have a tobacco smoking history of at least 30 “pack years” (an average of one pack a day for 30 years). ** Receive a written order from a physician or a qualified non-physician practitioner. The AATS Writing Group for Lung Cancer Screening and Surveillance under co-chairs Drs. Francine L. Jacobson and Michael T. Jaklitsch (Brigham and Women’s Hospital) was instrumental in developing this diagnostic tool. The Group has identified other high-risk groups, including people between 54 and 77 who: ** Are lung cancer survivors. ** Have 20 “pack years” of smoking plus an additional factor that places their lung cancer risk at five percent over the next five years. Lung cancer is the third most common cancer and a leading cause of US cancer deaths. Individuals can use the calculator online at aats. org/tools/lung-cancer/ to determine whether or not they should pursue a CT screening. The page allows them to print out the results for discussion with their patients. Save the Date: Heart Valve Summit – Medical, Surgical & Interventional Decision-making October 1-3, 2015 Radisson Blu Aqua Hotel Chicago, IL than five million individuals just in this country. VHD can be congenital or acquired, and patients may or may not exhibit symptoms. Although there are national guidelines regarding management of VHD, controversies in care in the areas of advanced technology and medicine demand that collaborative methods be created for diagnosis and strategic medical, surgical and interventional management. Course Directors David H. Adams Mount Sinai Medical Center Steven F. Bolling University of Michigan Robert O. Bonow Northwestern University Howard C. Herrmann University of Pennsylvania Nurse Planner Michele Mistovich, RN, MS Northwestern Memorial Hospital Course Background Heart disease is the leading cause of death in the United States. Valvular heart disease (VHD) affects more conference will engage participants in discussions, debates and potential controversies using real-world cases. Its faculty will include renowned experts, who are on the cutting edge of clinically relevant VHD data. Course Objective The American College for Cardiology (ACC) and AATS once again will bring together cardiologists and surgeons for a case-based course addressing the rapid advances in VHD treatment. This interdisciplinary course will combine clinical decision-making with medical, surgical and interventional options for patient care, taking into account that constantly changing management tools can impact the surgical team. Breakout sessions for cardiologists, cardiac surgeons, nurses and physician assistants have been designed to help specialists manage their unique challenges from a team perspective. Focusing on interactivity and practical decision-making, this unique Target Audience The 2015 Heart Valve Summit is intended for cardiologists, interventional cardiologists, cardiothoracic surgeons, internists, nurses, physician assistants and all health care professionals involved in the evaluation, diagnosis and/or management of VHD patients. Accreditation Physicians This course has been approved for AMA PRA Category 1 Credits™. Nurses The American College of Cardiology Foundation is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation. Registration/housing information: http://www.aats.org/valve Save the Date: Focus on Thoracic Surgery – Technical Challenges and Complications Mark your calendar for the 2015 Focus on Thoracic Surgery. This year’s emphasis is on technical challenges and complications. October 23-24, 2015 Seaport Hotel & World Trade Center, Boston, MA Overview Complications remain one of the major challenges in treating patients. The 2015 Focus on Thoracic Surgery will concentrate on the intraoperative challenges and management complications facing thoracic surgeons in treating lung and esophageal cancers. This year’s course is particularly aimed at operating surgeons who are active and seek to learn innovative solutions to clinical problems during surgery. This course will display new advanced diagnosis and prompt management approaches, allowing attendees to understand and readily translate them into daily practice. The two-day conference will have a faculty of experts in the field who are leaders in the application of new technologies in surgical manage- ment. It will combine informational sessions, panel discussions and complex case presentations. Focus on Thoracic Surgery is a must for surgeons who specialize in the treatment of lung and esophageal cancers and want to enhance their skills so they can overcome challenges and complications in their surgical practices. Program Committee Members Thomas A. D’Amico Duke University Shaf Keshavjee University of Toronto James D. Luketich University of Pittsburgh Bryan F. Meyers Washington University Scott J. Swanson Brigham and Women’s Hospital Program Directors G. Alec Patterson Washington University David J. Sugarbaker Baylor College of Medicine For more information: http://aats.org/focus/ 14 NEWS FROM AATS MAY 2 0 1 5 • THO R A C IC S UR G ERY NEW S Save the Date: First AATS Aortic Symposium in Asia Don’t miss the AATS Aortic Symposium Workshop Kobe to be held the day before the Japanese Association for Thoracic Surgery Annual Meeting. October 16, 2015 Kobe Portopia Hotel, Kobe, Japan In partnership with: Japanese Association for Thoracic Surgery Japanese Society for Cardiovascular Surgery Japanese Society for Vascular Surgery This one-day symposium will include expert lec- For Central & South American Surgeons: AATS Cardiovascular Valve Symposium/Brazil November 20-21, 2015 November 20-21, 2015 Renaissance Marriott São Paolo São Paolo, Brazil This symposium is part of the Edwards Lifesciences Foundation Every Heartbeat Matters initiative aimed at impacting the global burden of heart valve disease by 2020 — reaching one million underserved people through education, screening and treatment. Course Directors David H. Adams Mount Sinai Medical Center Joseph S. Coselli Texas Heart Institute Pedro J. del Nido Children’s Hospital, Department of Cardiac Surgery Walter Jose Gomes Escola Paulista de Medicina - Federal University of São Paulo It is for physicians whose patients have limited health care, are over 60, and are vulnerable to rheumatic heart disease and/or at risk of heart valve disease today or in the future. More information: To come tures from invited faculty on the pathophysiology, diagnosis and treatment of aortic aneurysms and dissections, as well as presented abstracts. For more information: www.aats.org/KobeWorkshop Coming in 2016: The Inaugural AATS Surgical Patient Safety Course AATS announces its inaugural AATS Surgical Patient Safety Course aimed at advancing patient care -- the mission of every surgical team. June 24-25, 2016 Renaissance Boston Waterfront Hotel Boston, MA Course Objective/Content The course will promote a culture of safety and help reduce preventable harm by offering surgical team members with a multidimensional ap- proach to improved patient care. The curriculum will combine didactic and interactive presentations and focused workshops. It will provide essential knowledge, skills and attitudes about patient safety aimed at improving care now and in the future. Target Audience All members of the CT surgical team including surgeons, perfusionists, nurse practitioners, and physician assistants. For more information: www.aats.org/patientsafety. CLASSIFIEDS Also available at MedJobNetwork.com Disclaimer THORACIC SURGERY NEWS assumes the statements made in classified advertisements are accurate, but cannot investigate the statements and assumes no responsibility or liability concerning their content. The Publisher reserves the right to decline, withdraw, or edit advertisements. Every effort will be made to avoid mistakes, but responsibility cannot be accepted for clerical or printer errors. EVOLVING SCIENCE AND TECHNOLOGY THOR AC ICS URGE RYNE W S. COM • M AY 2015 3-D mesothelioma model Nanotech from page 1 The researchers said their findings showed that three-dimensional spheroid models “are valuable tools for investigating cytotoxic mechanisms and nanoparticle-tumor interactions, particularly given the costs and limitations of in vivo animal studies.” Their findings were first presented at the 94th Annual Meeting of the American Association for Thoracic Surgery last year in Toronto. Despite advances of nanoparticle-based drug delivery systems, difficulties in evaluating the effectiveness of these drugs in local chemotherapy have hindered their adoption in the clinic. Studies of the same agent utilizing in vitro vs. in vivo methods have shown con- flicting results, they noted. The observation that Pax-eNP treatment of intraperitoneal mesothelioma significantly improved survival in lab animals in vivo, compared with conventional paclitaxel, led to the use of the three-dimensional spheroid model. Dr. Lei and colleagues called this revelation “striking” because Pax-eNP exposure of the identical mesothelioma tumor cells plated as a two-dimensional monolayer in vitro demonstrated equal or worse results. PERSPECTIVE “W hile this study contributes greatly to the body of knowledge available regarding potential treatment strategies for malignant mesothelioma, one might argue that the more important impact of this paper relates to the successful implementation of an unconventional tumor model,” Dr. Mara B. Antonoff wrote in her invited commentary (J. Thorac. Cardiovasc. Surg. 2015 [doi: 10.1016/j.jtcvs.2015.02.015]. Dr. Antonoff acknowledged their quest for a solution that was more cost-effective than animal models and better approximated in vivo biological actions of the drug. However, she Residents noted the three-dimensional models “are not without limits, either.” Adoption is limited because of the time and expertise involved in spheroid formation. “Nonetheless, it is clear that such models are a huge improvement over our current in vitro models,” she wrote. Among the limits of the three-dimensional spheroid model she pointed out are that it lacks the continued from page 11 ing to Dr. Nguyen and Dr. George. “To do this, surgeons will have to change their mindset regarding their role in the procedure and be willing to learn the technology.” The minimum time commitment to learn these procedures is 6 months; for residents, a multiple cell types typical in an actual tumor and quantitative assessment of the results can be difficult. But the spheroid model does enhance the ability to screen novel drugs and drug-delivery systems. “This timely and well-constructed study provides a foundation upon which we may build our knowledge of chemotherapeutic delivery mechanisms, while setting an outstanding example, and perhaps a new standard, for in vitro methodology.” Dr. Antonoff is a clinical instructor at University of Texas M.D. Anderson Cancer Center in Houston. dedicated structural heart fellowship can take up to a year. The 20 interventional procedures that graduates are now required to perform “is not nearly enough,” they wrote. It may require significant changes to the overall training model to allow proficiency. Because percutaneous skills also apply to all future structural heart interventions, such as 15 “This suggested that eNP may be more effective at penetration and/ or persistence within multicellular tumors and led to the use of a 3-D tumor spheroid mode,” according to the researchers. “Given the high cost and limitations of in vivo animal studies, spheroid models may present a clinically relevant platform for screening novel pharmaceuticals and unique drug-delivery systems during the preclinical phase,” the researchers indicated. They also investigated spheroid cytotoxicity in a clinic-like setting following a 4-hour, high-dose (1,000 ng/mL) paclitaxel exposure via conventional and eNP vehicles. They found that Pax-eNP exposure led to greater tumor cytotoxicity at 72 hours, and that cytotoxicity continued seven days later because Pax-eNPs rapidly enter the tumor spheroid and remain intracellular, slowly releasing the drug. “The prolonged drug release mechanism that pH-triggered PaxeNP uses appears to be unique, leading to markedly higher intraspheroidal drug delivery, prolonged intratumoral drug release and superior antitumor efficacy,” the investigators concluded. The authors had no disclosures. percutaneous mitral valve repair and replacement, percutaneous tricuspid valve repair and replacement, and pulmonary valve replacement, such skills can help the cardiac surgeon get past seeing valvular heart disease as just a nail, but rather something requiring a suite of different tools to treat. The authors reported having no disclosures. PERSPECTIVE N guyen and George’s expert review, “Beyond the hammer: The future of cardiothoracic surgery” addresses a question that resonates in the mind of any CT resident completing their training – how can I best position myself today for success as a practicing cardiothoracic surgeon tomorrow? The authors astutely identify several factors that predict an increasing emphasis on percutaneous and minimally invasive techniques in the management of structural heart disease, drawing parallels between modern-day cardiac surgeons and the vascular surgeons who have successfully integrated endovascular techniques into their practice and training paradigm. I would extend this discussion to include general thoracic surgery wherein endoscopic and broncho- scopic techniques are rapidly gaining momentum in oncologic staging and the management of both benign and malignant chest diseases. The authors commend the Thoracic Surgery Residency Review Committee and American Board of Thoracic Surgery for recognizing the need for endovascular skills; however, they note that the 20 required cases is far fewer than what is needed for proficiency. Nevertheless, the article suggests pursuing additional fellowship training rather than promoting a significant change in the current cardiothoracic residency curriculum – a very important message. The authors clearly recognize that success in CT surgery requires, first and foremost, excellent surgical skills. As noted in the article, “The first step is to master traditional surgical techniques…” The ability to operate will always be what sets the surgeon apart and allows us to bring a complete “toolbox” to the bedside. So while I read this article with great interest, I remind myself to resist the temptation as a CT resident to focus too much on these endovascular and endoscopic techniques during the core training. The 2-3 year traditional residency is simply too short; emphasis must remain on fundamentals of the craft. Thereafter, as Nguyen and George suggest, young CT surgeons can pursue additional training whether in the form of advanced fellowship programs or as junior faculty. This may be an argument in favor of the I-6 pathway. Perhaps the I-6 thoracic residency provides the time frame and early integration necessary to successfully train a CT surgeon in all the aforementioned techniques. This remains to be seen. However, as the first wave of I-6 trainees begins to matriculate, we will soon have our answer. The bottom line is that advanced endoscopic and endovascular techniques will undoubtedly be necessary components in the CT surgeon’s toolbox and each CT resident should have a clear plan for how best to acquire these skills, but only after first becoming really good with that hammer.… Dr. Elliot Servais is one of our resident medical editors for Thoracic Surgery News. indd single with guides.indd 1 4/27/2015 5:18:15 PM






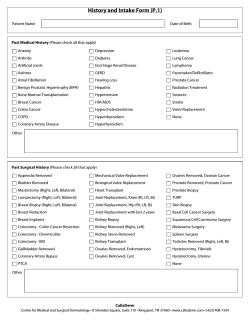



© Copyright 2026