
Document 8838
54
Sustainable Health Care for Canada
with no reduction in health outcomes.Since the developmentof this scenario,Ontario
releaseda report relating to these reductions. See Appendix 5-3 for
some implications of further decreases.
To estimate net savings to the system,one would have to account for any
relatedcostsandresourceusein the homecare sectorthat result from a reduction
in lengths of stay of acute-careinpatients. However, given the magnitude of
the gross savings and the cost differential betweenan acute-carebed-dayand
home care visits, the net savings would be significant. (See Chapter 6 in our
researchreport Cost-Effectivenessof CanadianHealth Care for more detail on
gross-to-netratios and marginal returns.) In order to refine this scenario,the
overall reduction in lengths of stay should be replaced by a targeted approach
focusing on specific activities/morbidities in the model,asdirected by empirical
evidence. The next scenario addressesthese issues.
Scenario 2: Substitute continuing care for
acute inpatient care (Chart 5-2)
This scenariotargets Major Clinical Category (MCC) 23 (other reasonsfor
hospitalization). Since a numberof case mix groupings (CMG) are aggregated
into this MCC, we had to identify a percentageof the cases within selected
CMGs that would be best suited to be de-institutionalized and shifted to
community care or homecare.The affectedCMGs relateto rehabilitation,aftercare following surgery/treatment,and other specified after-care. Cases in
~:>!glns tu~!l~du! ~A!l:>~I~ :>!J!:>~dss! puo:>~s ~Qt p~ (U°!l~~A
~t~l) StU~Wt~~J:}
U!~:Jl~:>JO ~:>U~P!:>U!~Qt U! U°!l~~A S! tS1Y ~q.L .SI~t!dsoq ~JP.:>-~m:>~
U! SgU!A~S10J
S~~JP.OMt UO S~!I~l o~u~:>s S!q.L .p~l~n~ ~JP.~:>!t:>~ld I~:>!P~W 10 tU~wt~~J:}JO
sw~n~d
~l~qM SUO!t~m!S U! tS~pOW ~lOW q:>nw ~JP.SUO!t:>np~l tSO:>~q.L
(e-s; J./eLl.?)AJa6Jns lua!ledu! JOj Aep-awes alnl!lsqns (q
:uO!le!JeA aleJ a:Jnpatj (e :e O!Jeua:JS
.tso:) Ietot ~q'! Ot UO!teI~l U! IIews ~Je stunowe
JeIIoP ~qt tnq '~gJeI ~Je~Je:)~woq pue ~Je:)At!UnWWO:)U! S~Se~l:)U!~getu~:)l~d
~q.L "l-~ llRq;) U! UMOqSS! S~!log~te:) tSO:)SnOpeAUOt:)edw! ~q.L 'SA'lV() U!
~gueq:) ou U! p~nnS~l AIJe!tU~SS~
UO!tn:t!tsqnsS!q.L.gu!pu~ds qne~q tU~WW~AOg
OpetuO U! ~Se~l:)~ptu~:)l~d 8'0 e S! q:)!qM 'UO!II!W 0171$Jo 1~p1O~qt U! ~l~M
sgU!AeSt~u ~q.L 'peoI~se:) p~se~l:)U! ~q'! Ot ~SUOdS~l
U! s~:)!Al~S~Je:)-gu!nu!tuo:)
Jo uo!suedx~ ~q'! punJ °t p~p~~u seM UO!II!W 9'~£$ AI~teW!X01dde 'tunowe
S!q'!JO '(p~Al~suo:) sAep-p~q 000'~'l£) sgU!AeSIet!dsoq U! UO!II!W9L 1$ l~AO U!
p~nns~l s~se:) ~s~qt 10J ~Je:)Iet!dsoq ~m:)e 10J ~Je:)gu!nu!tuo:) gU!tn:t!tsqns
.~9 Jo "g11 "V
J"pUn "J"M :}U":)J"d 8~ 'p"1m!1sqns S"S11:)[11101"V JO
o.<"Ie:)fl!UOnm!1SU! Jo S["A"[ sno!J1!A s"pn[:)u! q:)!qM '"Ie:) A1!unwmo:) pU11"Ie:)
"woq) "m:) gU!nUnUO:) Jo S["A"[ sno!J1!A 01U! S[111!dsoq"Ie:) "1n:)11WOJJ P"AOW
"J"M S"S11:)"s"q1 Jo Z19' LZ '°!J1!u,,:)S S!V uI 0.<
dnoJg "g111S"P[0 "V U! P"U!11g S11M
A'lVt) J"d UO![[]lli OOZ$ 1sowfI! '"[dUJ11x,, JoJ) w"q1 01 P"10A"P s":)JnOS"J ApSO:)
A["A!111["J "V U"A!g ("S11:)J"d sA 'lVt)) 1nd1no MO[ ,(J"A 11"A11qA[[11J"U"g £'l JJW
~~
l{.JlJo.lddy
ap!M -walS,{S
y -II
l.llJd
56
Sustainable Health Care for Canada
procedures where the venue for the surgery is deemed substitutable (for
example, substitute day surgery for inpatient surgery).
A 1990 report to the federal-provincial Conference of Deputy Ministers of
Health6 analyzes 13 of the most common surgical procedures. The results
demonstrate "the minimal impact of reducing the surgical rates in communities
with exceptionally high rates." In a follow-up to this study, the Hospital Medical
Records Institute (HMRI) was commissioned by the federal-provincial Advisory Committee on Institutional and Medical Services to examine geographic
variation in hospital use.7 In addition to the 13 procedures referred to above,
this report included many other surgical and medical interventions, as well as
rates of same-day surgery for specific procedures. Guided by the information
contained in both these reports, the first part of this scenario identifies six
morbidities (activities) in the RAF and reduces the procedure rates by one
standard deviation below the mean calculated in the HMRI report. The following
morbidities/procedures were targeted: cholecystectomy, lens procedures, tonsillectomy/adenoidectomy,
acute myocardial infarction,
transurethral
prostatectomy, and subtotal mastectomy.
The second area within this scenario identifies low-severity cases within
inpatient surgical CMGs and shifts them to same-day surgery. This substitution
is based on the findings of Jacobs et al.8 who report that "on average, direct
inpatient costs ($841 per case) exceeded outpatient costs ($204 per case) by
$637."
The combined effect of reducing rate variation and substituting same-day
surgery for inpatient surgery resulted in approximately $75 million in savings
(a 0.5 percent decrease in Ontario government health expenditures) and a
negligible 0.09 percent drop in QAL Ys.
Overall, the modest change in costs corroborates the findings of the studies
used to guide the development of this scenario. This does not diminish the
importance of further examining the complex issues surrounding rate variation
or the need to transfer more inpatient surgical cases to same-day surgery. There
are many other reasons for continuing to study these areas,especially to improve
the quality of care.9
The value added by this project is not in the evaluation of rate variation and
day surgery, but rather in using such evidence as exists in those areas and tying
in other resources that would be affected. The result here is an increase in home
care costs as a result of substituting day-surgery for inpatient surgery. In
Chart 5-3, it is important to understand that the increase in day-surgery home
care is based only on that portion of home care that relates to the small number
of morbidities examined for substitution, not on all home care for day-surgery
S{aAa{aA!J a~ SSOJ:>U
puaJds sasu:>{u~!dsoqWJa~-guoI.u! uo!~:>npaJ~ua:>JadOZupasodw!
~SJ!JaM °!JUua:>sS!q~a~u{n:>{u:>
o~ 'a:>uaJaJaJ
JO~u!od u su S!q~q~!A\
"UO!T1!q 1;'1$ ;}A~S pu~ S;}!1!I!:>~J;}m:> WJ;}:J-guoI U!
sA~P-:Ju;}!:J~dUO!T1!W 11;;}AJ;}Suo:>PlnoA\ 'OA\:JI;}A;}I moll J(~q pu~ ;}UO I;}A;}I moll
J(~q ':JU;}:>l;}d1;°17O:J8°9 moll
UO!:J~Z!J1!UO!:Jm!:JSU!
JO ;}:J~l ;}q:J gU!:>np;}l s:Js;}ggns
;}q 'AT1~UO!:J~N,,"(:JU;}:>l;}dI;£)Z P~ Ou;}:>l;}d 1;1) 1 SI;}A;}'l U!;}l1! (H:Jd) S;}woq
;}l~:> I~UOSl;}d s,~qo:J!U~W U! s:JU;}P!S;}lAJl;}PI;} T1~Jo J(~q-;}UO AI;}:J~W!XOldd~"
:J~q:J S;}:Jou jj;}WOH
";}l1!:> ;}woq
0:J s!s~qdw;}
;}q:} :JJ!qs P~
AJl;}PI;} ;}q:J Jo
1:IO!:J~Z!I~UO!:Jm!1sU!
;}:>np;}l :J~q:JP;}SOdOld U;};}q ;}A~q s°!l1!U;}:>s Jo l;}qwnu
V
ol"AIJapla aq1
,gU!SnoqaJBN!., )0 a:>!1:>BJdsnoIIB:> aq1 a1Bfi1awad II!N!. aN!. 'aA!1!q!qoJd
aq AIUO 10U II!N!. S1S0:>aq1 'N!.OU op aN!. a1BJ aq1 1B SUO!1fi1!1SU!U!
aldoad PIO 1nd 01 anU!1uo:> aN!.)! """ a)!I)O A1!IBnb aq1 a:>UBqua 011nq
'S1S0:>a:>npaJ 01 AIUO 10U 'alq!ssod
SB gUOI SB JO) SUO!1fi1!1SU!)0 1no
AIJapla aq1 daa:Jf 01 sa:>!AJas A1!Unwwo:»0
1uawdolaAap aq1 U! aq01
spaau AlqB!Uapun sa:>JnosaJ aJB:>q1IBaq)0 uop:>aJwaJ aq1 U! 1sruq1 aq.L
(p-g IJel./.?)
UO/lez//eUO/lnl/lsu/-ap pue UO/lnl/lsqns AI///:Je;J :p o/Jeua:JS
StSO;)It/tOt a~
L~
If.Jvo.lddy
'la~lP.I saw!t OIlaAo
'StSO;) WatSAS {mOt 'laAaMoq 'alP.
S! q;)!qM 'alP.;) awoq It/tOt ssaI q;)nw 'sast/;)
iJP!M -lUiJlS'<S Y -//l.lVJ
58 SustainableHealth Care for Canada
of care. This essentiallyremoved23,000casesand almostthree million hospital
bed-days.Second,we movedthesecasesto residentialcareinstitutions and then
transferred almost 35,000 (20 percent) of the lowest level cases(levels I and
2) out of these institutions into community care. QAL Y s were essentially
unaffected.
The result was a reduction in hospitalbed-daysof 5.9 percentand residential
care bed-daysof 17percent.The only increase(9.2 percent)was in community
care costs.The net savingsare estimatedto be $326 million, which represents
a 2-percentdecreasein Ontario governmenthealthexpenditures.This confirms
Home's conclusion12that de-institutionalizing the elderly will produce more
modestsavings than reconfiguring acute-carehospital services for the rest of
the population.
Summary
of the Scenarios
The table below summarizesthe four scenarios.Together, they represent
approximately$1.5 billion in savingsor 9 percentof Ontario governmenthealth
expenditures. Health outcomes (QAL Ys) were essentially unaffected. The
scenariostestedheredemonstratethat thereis significant scopefor costsavings,
and they do not by any means exhaust all the possibilitie;s.
"lOJ:Jas S!lJJU! Melp OJ lJ:J!lJM uodn a:Jua!ladxa J:Jal!p am!I S! alalJJ 'ale:J lJJlealJ
U! AJ!Ieal e awo:Jaq AnUa:Jal AIUO aAelJ ~U!Z!SUMOP pue UO!J:Jnpal JSO:Ja:JU!S
.sa:>!AlaS alU:> q,(Uaq JO AlaA!(ap aq, aln8guo:>al
0'
S}l°JJa S'! U! Sa!8a,Ul'S aalq, asaq, ,dopu 0' paau AUW Wa'SAS alU:> q,(Uaq aq.L
'A8a,Ul'S auo A(UO pasn ,uq, asoq, uuq, A'!IUnb 8u!u!u,U!UW puu 'SO:>8U!llOl'UO:>JO
saA!,:>afqo l!aq,
8U!Aa!q:>U U! aA!,:>aJJa alOW alaM aalq, I\U paU!qwo:> ,uq,
SUO!,UZ!UU810,uq, punoJ £IAPfiJS 'Ua:>al V '(r;-r; 'lUq:)
Sa!8a,Ul'S aP!M-Wa,SAS
pUU 'u8!sap )(lOM 'uO!J:>npal a:>lOJ'llOM -Sa!8a,Ul'S
8U!Z!SUMOP 'aA!Snl:>xa
AI\UfiJnW 'OU pUU ',UalaJJ!p aalq, s,sa88ns a:>ua!ladxa l!aq.L .8U!Z!SUMOP q,!M
pa,U!:>OSSUS'SO:>UOmSUU1' aq, JO AUUWpalln:>U! 10,:>aS a,UA!ld aq, 's086 I aq,
,noq8nolq.L .s(u,!dsoq uaAa puu spaq (u,!dsoq 8u!SOI:> Jo ,:>udw! aq, ,uasaldal
-salfiJ!puadxa
IU,!du:> Mau puu ~S8U!qS!UlnJ puu ,uawd!nba 's8u!PI!nq Jo
8u!sods!p
~SJJOAUIIO/PUUslaJsuul, a:>lnosal uuwnq -S'So:> asaq, 'sasu:> ,SOW ul
.sa8uuq:> IUlfiJ:>nl's q:>ns q,!M pa,u!:>ossu s'So:> UO!,!SUU1'aq, 10J ,uno:>:>u 'OU P!P
Aaq.L .s,ua!,ud 10J s8u!"as alU:> a,u!ldolddu alOW puu ,so:> laMol O'U! s(u,!dsoq
wall alU:> 8U!llaJsUU1' JO S8U!AUS,au aq, palap!SUO:> SO!lUua:>s InOJ asaq.L
s~so:> Uo!~!sueJ.L
'v66~ hJenJq8~ 'epeue:) 4~le8H ,,'epeue:) u! S8Jn~!pU8dX3 4~le8H ~o s8~ew!~s3 hJeu
!W!18Jd" U! p8IJOd8J (O66~) S8Jn~!pU8dX3 4~le8H ~U8WUJ8"O~ O!Je~UO UO!II!q L~$ UO p8Sea .
Log
00'0
Ov~
g'O
00'0
SL
S'O
60'0-
OOG
O~'O-
9G£
uo!~eZ!leUO!Jn~!~su!-ep
pue uo!~n~!~sqns A~!I!:>e::l
AJ86Jns
JOI Aep 8WeS
pue
Ju8!Jedu!
8JnJ!Jsqns
UO!Je!JeA 8JeJ 8:>np81:j
8Je:> 8ln:>e
JO!
8Je:> 6u!nU!luo:> 81m!lsqns
%OG I.q I.els
Jo 416uel pUB %OG
I.q speq ale:> eln:>e e:>npel::l
(~ue~Jed)
SAlVO
.seJnJipuedxe
U! e6UB4:)
4llEe4 :J!lqnd
u! eBUE4~
066~ 'O!JeluQ
t7-~ so!Jeue:>s
6~
If:JDO.lddV
Jo 1.Jewwns
iJPlM -WiJ1S.{S V -[[1.1DcI
v96
60 SustainableHealth Care for Canada
There does not appear to be a blueprint on how to downsize or close a hospital.
Each institution is faced with a unique set of challenges and constraints to which
it has to respond. For instance, the closure of the Shaughnessy Hospital in
Vancouver was announced in February 1993 and the target date to finish moving
the patients was September 1993. This short transition time minimized the
disruption to staff and physicians.
In such closures, it is important to establish a schedule, publicize it well, and
then stick to it. Delays can be very expensive. For example, the closure of the
Darenth Park Hospital in the United Kingdom fell behind schedule, causing
the hospital to stay open four and a half months beyond the scheduled closingdate.
As a result, the transition costs were greater than anticipated.14
In closing a hospital, there can be a net benefit to demolishing, selling,
converting to other uses, or renting the building and/or the land. There are
several possible approaches. For example, the 1993 preliminary report of the
McGill Academic Health Sciences Centre (AHSC) proposed that the Royal
Victoria Hospital be converted for university functions, while two other
hospitals -the Montreal Children's and Montreal Chest hospitals -be sold.
The estimated combined value of these two facilities is about $32 million.ls
The estimated $1 billion capital cost to create the McGill AHSC has not been
factored into these figures.
The Essex County Model on the Total System Reconfiguration (1994)16
provides another example of a downsizing strategy. The plans encompass
development in all sectors -from community-based services to long-term care
.paz!w!u!W
aq UU:JSJSO:JaqJ 'laAaMoq 'paJuawa\dw!
puu pauuu\d
h\aA!J:JaJJ3 .ssa\u!ud gU!Z!SUMOP pUU UO!Jurng!jUO:Jal a}{UWOJhUM ou S! alaqj,
.gU!lfi1:JnlJsal U! AeId OJ aIol lofew
e aAeq AlleaI:J
q:J!qM 'SUO!Un Alle!:Jadsa pUR 'SUO!Jfi1!JSU!I1!UO!J1!:Jnpa
'Sa!:Juage JUaWUlaAog
)0 JuawaAIOAU! aqJ S! S!qJ )0 )led l1!lgaJU! UY .UO!J!SUelJ aqJ U! d!qslauMo
awos waqJ aA!g OJssa:Jold gu!}(ew-Uo!s!:Jap
aqJU! saaAOIdwaaAIoAuI.
~;}gueq:>leJntln:> pue leJnt:>nJJsWJ;}J
-guol e JO JJed Jnq ;}gueq:> OJ;}suods;}J;}W!J-;}UOe JOUS! J! JeqJ;}Z!ugo:>;}~ .
~saWO:)1noq1I8aq jO
A1!I8nb aq1 U! ssoI U! 1(nsaJ 10Usaop UO!18Jn3'!jUo:)aJJO 3'U!Z!SUA\OP18q1aJnsu3 .
~IUt!dsoq
10 plUM
AUU
'SU!SOI:>alOJaq a\quI!UAU alU sa:>!AJaSaA!tRUlatIR pUR At!Unwwo:> tuqt amsu3
.
~SJJOAlI[
A[JSO;)P!OAlI 01 wa1sAs alll;) q1[lIaq aq1 U!q1!M sa;)lnOSal ulIwnq Ao[dapa~ .
:altl SaUD1UtlJlOdw! awos q:>!qN\ Jo 'SlOJ:>tlJ TtllaAaS
uo spuadap gU!Z!SUMOPJo ssa:>:>nsaq.L .ATaA!J:>aJJapagtlutlw aq aloJalaqJ Jsnw
AaqJ ~aTqtlP!OAtlUnPUtI JutI:>!J!ug,s altl UO!Jtllng!Juo:>al altl:> qJltlaq JO SJSO:>
aq.L
6r,,'lOJ:Jas
pastlq-AJ!UnWWo:J aqJ U! Sa:J!AlaS u~wnq pa:Ju~qua pU~ MaU Anq OJ" S8U!A~S
l~J!dsoq aJtI!paww! WOlJ UO!II!W ZZ$ aqJJo AJ!lOf~w.aqJ asn OJsasodold AJUnO:)
xass3 'aldw~xa lad 'sJSO:JUO!J!SU~lJ q:Jns az!w!u!W OJ spunj 8u!J~:J01I~al al~
SUO!JtlZ!U~8l0 'loJ:Jas al~:J qJltlaq aqJ ul 8!'saaAOldwa jJo-P!~1 OOO'Ot JS!SS~OJ
UO!II!W 006$ ap!s~ Jas swaJsAS I!~~ N:) pu~ 'sqof OO~'V awos W!lJ OJ UO!II!W
OO~$ ap!s~ Jas OlpAH O!l~JUO 'a:Ju~Jsu! lad ,a8pnq Al~ssa:Jau aqJ ap!s~ Jas
AIJ!:J!ldxa OJS! SJSO:J
UO!J!SU~lJu~wnq aqJ a8t1u~w OJA8aJ~lJs aqJ Jo Jl~d Aa)( V
u"pauaqJgualJS
alaM SlOA!AlnS aqJ gUOWR a\RlOW aqJ
pUR alflJ\n:J aJRlOdlO:J S,\RJ!dsoq aqJ 'SJSO:J
jJOAR\\R!JUaJod U! SlR\IOP)O SUO!II!W
gU!ARS OJ UO!J!PPR UJ "sqof MaU PO!} saaAoIdwa pa:JR\ds!p DOZ'I SJ! dIaq OJ
AgaJRlJS R padO\aAap J! 'I66[ }O laWWnS aqJ U! pasoI:J -SIRJ!dsoq Juau!wold
,Sa!J!J U!M.L aqJ }O aDO -alJuaJ
IR:J!paw !RU!S Junow-uRJ!IodolJaw
aqJ
uaqM 'aIdwRxa lOd "pa:JRIds!p ale OqM saaAoldwa lO} pal!nbal ale SWRlgOld
a:JuRJS!SStIla,\lOM pUR 'SWtllgOld gU!U!RlJ 'sagR,\:JRd a:JURlaAas 'SWtllgOld
Juaw';):JtlIdJno SRq:Jns Sa!gaJRlJS "SJSO:J
a:Jlnosal uRwnq ale SJSO:JUO!Jtllng!}UO:Jal
JUtI:J!}!ug!S JSOWaqJ 'aA!SuaJU! lnoqR\ A\qg!q S! waJSASalR:J qJIRaLl aLlJ a:JU!S
.S~:J!AJ~Sp~tUU!P100:J 'At!IUnb q8!q 8u!doI~A~P Aq~l~qt 'S~:J!AJ~SJO UO!tUtU~W8U1J
pUU UO!tu:J!Idnp ~tUU!W!I~ U~A~ 10 ~:Jnp~l °t SUM Iu08 ~q.L .~lU:J ~tn:Ju °t
19
1f:J/Jo.lddyaplAt-Uta1sICs
y -[[1.l/JJ
62 SustainableHealth Care for Canada
Conclusion
Canadians expect and deserve the highest standards of professionalism in
the management and operation of their health care system. By the same token,
the health care industry itself deserves the best possible management tools to
manage its resources effectively.
In this chapter we have described one such tool -the Resource Allocation
Framework -and used it to examine a number of different scenarios aimed
at optimizing outcomes or minimizing costs. For the most part, the details of
the scenarios came from existing health care research. In many respects the
results of our simulations confirmed quantitatively the findings of other studies.
In another respect, however, it went beyond the existing research in that it
combined an outcome measure with resource allocation, albeit in an exploratoryway.
Williams2o notes that "although in the concept of the quality-adjusted lifeyear we have such an outcome measure in principle, no-one would pretend that
we have yet moved beyond the pioneering stage in the practical implementation
of that concept." The Resource Allocation Framework is indeed exploratory,
but it is a significant attempt to practically implement a decision-support tool
based on this concept. It is not the last word on resource allocation, but most
certainly represents a major step forward in advancing it, not only as a decisionsupport tool, but also as a style of thinking. If the development and implementation of the RAF is indeed viewed as a pioneering project and embraced by
the research and policy communities, then there is important work ahead to
improve upon this initial work in order to bring it into the mainstream of health
research and policy.
One very promising area of future work is incorporating into the RAF the
Health Utilities Index (HUI) developed by Torrance et al. to replace the Oregon
approach to outcome measurement.21This would also present the opportunity
to strengthen outcome measures for ambulatory activities such as out-of-hospital
drugs and out-of-hospital physicians' services.
We end this chapter with a comment on ethics and resource allocation.
Resource allocation is fraught with ethical difficulties that the RAF certainly
cannot resolve. However, the RAF does make explicit many of the allocation
decisions that are currently hidden from public view. As well, employing it tends
to draw out many ethical issues that have never been meaningfully addressed.
In this sense there seems to be cautious consensus among ethicists that tools
such as the RAF have a role to play in providing a framework for organizing
information explicitly to make it useful for decision makers. However, using
it rigidly is dangerous, and it cannot be overemphasized that the RAF is not
intended to replace decision making but rather to augment it. Notwithstanding
the need to somehow account for ethical considerations within this quantitative
62 SustainableHealth Care for Canada
Conclusion
Canadians expect and deserve the highest standards of professionalism in
the management and operation of their health care system. By the same token,
the health care industry itself deserves the best possible management tools to
manage its resources effectively.
In this chapter we have described one such tool -the Resource Allocation
Framework -and used it to examine a number of different scenarios aimed
at optimizing outcomes or minimizing costs. For the most part, the details of
the scenarios came from existing health care research. In many respects the
results of our simulations confirmed quantitatively the findings of other studies.
In another respect, however, it went beyond the existing research in that it
combined an outcome measure with resource allocation, albeit in an exploratoryway.
Williams2o notes that "although in the concept of the quality-adjusted lifeyear we have such an outcome measure in principle, no-one would pretend that
we have yet moved beyond the pioneering stage in the practical implementation
of that concept." The Resource Allocation Framework is indeed exploratory,
but it is a significant attempt to practically implement a decision-support tool
based on this concept. It is not the last word on resource allocation, but most
certainly represents a major step forward in advancing it, not only as a decisionsupport tool, but also as a style of thinking. If the development and implementation of the RAF is indeed viewed as a pioneering project and embraced by
the research and policy communities, then there is important work ahead to
improve upon this initial work in order to bring it into the mainstream of health
research and policy.
One very promising area of future work is incorporating into the RAF the
Health Utilities Index (HUI) developed by Torrance et al. to replace the Oregon
approach to outcome measurement.21This would also present the opportunity
to strengthen outcome measures for ambulatory activities such as out-of-hospital
drugs and out-of-hospital physicians' services.
We end this chapter with a comment on ethics and resource allocation.
Resource allocation is fraught with ethical difficulties that the RAF certainly
cannot resolve. However, the RAF does make explicit many of the allocation
decisions that are currently hidden from public view. As well, employing it tends
to draw out many ethical issues that have never been meaningfully addressed.
In this sense there seems to be cautious consensus among ethicists that tools
such as the RAF have a role to play in providing a framework for organizing
information explicitly to make it useful for decision makers. However, using
it rigidly is dangerous, and it cannot be overemphasized that the RAF is not
intended to replace decision making but rather to augment it. Notwithstanding
the need to somehow account for ethical considerations within this quantitative
U!t!Jl~;) U! S~It!W~J put! S~It!W ~U!U!qWO;) Aq P~A~!q;)t! St!N\UO!SS~ldWO;)l~qJmJ
~WOS .OlL p~l~qwnu S~!J!A!J;)t! (t!JOJ ~qJ '(S;)!lJ~JSqO ~1t!W ,.~.~) S~St!;) OU
qJ!N\ S()!lO~~Jt!;) ~soqJ ~U!Jt!U!W!(~ Aq pUt! 'SdnOl~ x~s/~~t! PI qJ!N\ UO!Jt!U!qWO;)
uJ .I~A()I ;);)W ~qJ OJ P~Jt!~~l~~t! ~1~N\ l~PU!t!W~l ~qJ put! I~A~I OW;) ~qJ Jt!
l~poW ~qJ U! P~!J!Ju~P! ~1~N\JS~l~JU! ;)!J!;)~ds Jo S~!J!P!qlOW ~l~qN\ 'P~!J!Ju~P!
~1~N\ (S~!lO~~Jt!;) AJ!P!qlOW) S~!J!A!J;)t! L9 'It!JOJ uJ .(;);)W) AIO~~Jt!;) 1t!;)!U!I;)
loft!w put! (OW;)
~U!dnOl~ X!W ~st!;) Aq sPt!°I~st!;) ~U!Z!lO~~Jt!;) Jo JS!SUO;)
S~!J!A!J;)t! '~St!;) S!qJ uJ .s~ss~;)old uo!J;)npold Ju~s~ld~l SiJ!J!It!I.10 Jo J()S V
"s~uauodwo:> aA!~e~!~uenb aaJq~ seq lapow d'l e 'Alle:>!~S!Ja~:>eJeqJ
"aSUaSUOWWO:>JO ~saJaq~pue~s Jsnw suO!Jnlos lie 'JaAaA\oq 'S!SAleUe leu!J aqJ ul
"UO!J.fiIOSleW!Jdo aqJ JOJ~ndJno JO SWJaJU! panleA aq ue:> q:>!qA\JO lie 'sa:>JnOsaJ
JO SUO!Jeu!qwo:> leJaAaS gu!sn saA!JeUJaJle snOJawnu guowe apew aq OJ
sa:>!oq:> Auew ale aJaqJ uaqA\ Juap!Aa ~sow S! JaA\od S~I "pasn AlJadoJd uaqA\ lOOt
I nJJaA\od e S! gu!wweJgoJd Jeau!{ Aq uo!Jez!w!JdO "sJndJno OJsJndu! gU!JelaJ
Aq ssa:>oJd uo!J:>npoJd aqJ saq!J:>sap d'l 'S!SAleUe uo!J:>unJ uo!J:>npoJd a)j!'l
"s~u!eJ~suo;) a:>JnosaJJO ~ase UaA!g sa:>JnosaJJO uo!Je:>°lle leW!~do aqJ aU!WJaJap
o~ anb!uq:>aJ le:>!JewaqJew aqJ se (d'l) gu!wweJgoJd
JeaU!1 sAo{dwa dV}I
aq.L
a~ONle:>!U4:>a.l-uoN
"
(:I"~) }tJOMaWeJ:IUO!~e:>OII"a:>JnOSa~a4.l
~-9 xIPuadd'o'
.ptJaqtJ
SJtJaAaqJ U! u8!sap WaJSASjO SWJOj aA!J:>ajja-Jso:> JSOWaqJ PU!j OJ sa:>u!AoJd
dlaq
Plno:> )(JOMaWtJJj padO[aAap-A[lnj
aJOW tJ JtJqJ JtJal:> S! J! 'AIItJU!d
"lOJ p;}Juno:):)e ;}q Jsnw SJSO:)
UO!J!SUe1J'I\;}M SY "AJ!I\!J!SU;}SqJ!M p;}lpueq ;}q sJU;}W;}:)elds!p ;};}AOldW;} pue
'p;}punJ A11;}d01d pue ;}:)eld U! ;}q S;}:)!!\.l;}S;}Jm!Jsqns JeqJ JueJlodw! S! J. ";}l;}q
P;}JU;}S;}ld A:)U;}!:)!JJ;} 1;}Je;}18 OJ SUe;}W ;}qJ ;}8emo:)u;} pue Jloddns OJ A1eSS;}:);}U
;}le S;}I\!JU;}:)U! pue 'UO!Jeln8;}1 '101JUO:) lU;}WU01!I\U;} Jq8!1 ;}qJ Aq p;}Jloddns
pue p;}uueld ;}q OJ ;}I\eq s;}8ueq:) q:)ns 'l;}I\;}MOH "SJU;}W;}8Uelle ApSO:) SS;}I OJU!
pue sleJ!dsoq W01J AeMe s!seqdw;} ;}qJ Jo ;}WOS JJ!qs OJ SJloJJ;} ,SJU;}WU1;}1\08
le!:)U!I\Old J10ddns ;}lOJ;}l;}qJ A;}q.L "S;}Wo:)Jno qJle;}q U! ;}U!I:);}P e 8U!)[S!1 JnoqJ!M
s8u!l\es JSO:)10J ;}do:)s ;}lqe1;}p!SUO:) S! ;}l;}qJ JeqJ ;}Je1JSUOW;}P
SO!leU;}:)S;}q.L
zz('O;) A ;);)S s;)nss!
tJ 10d)
(tJ:J!q};) ;)q} jO uo!}!sodx;)
'SUO!S!:J;)P UO!}tJ:JO(ltJ ;):JlnOS;)l jO s;):Ju;)nb;)suo:J
"(tJ!l;)tJ,,
£9
utJ Sl;)~tJW UO!S!:J;)P plOjjtJ
If:JlJo.lddy
II!N\ dV'M
;)};)(dwo:J
putJ S}:J;)jj;) ;)q} jO N\;)!A
P;)}U;)!lO-Ol:JtJW
;)q} '}U;)WU01!AU;)
iJP!M-WiJ1S,(S Y -[[I.1lJJ
64 SustainableHealth Care for Canada
morbidities, and then expanding again by adding continuing care. Activities
link resource use to outcomes and are the accounting unit in the RAF. An
activity thus consumes resources and produces outcomes.
Resource restrictions or a set of constraints must be quantified, since a LP
problem does not exist unless resources are limited. The data required for
setting up these constraints is the existing relationship between CMGs/MCCs
and resource use. A number of national, provincial, and regional databases
were used to estimate costs and resources for each activity/morbidity in the
model.
Of key importance is the identification of a quantifiable economic objective.
This is known as the "objective function"; that is, what we are trying to
maximize. In terms of the RAF, QAL Ys will enter the objective function
and the LP algorithm will identify among a great number of alternatives the
minimum-cost or maximum-output combinations that optimize the use of
health care resources.
Finally, it is important to note that the RAF can also be used effectively withoutits
linear programming algorithm. Therefore, in its non-optimizing mode, theRAF
provides a consistent and comprehensive accounting structure for exam-ining
resource allocation scenarios that do not require this technique (e.g., cost
minimization where output is deemed to remain unchanged).
Appendix 5-2
How the Outcomes
Data Were Derived
Our use of the Oregon outcomes data was restricted to a few elements, including
the probabilities and symptoms resulting from the treatment or non-treatment
of morbidities provided by panels of physicians. We did not use other, more
controversial, elements of the experiment, such as the prioritization. We tested
the sensitivity of the outcome measures using different scales and discount rates
in calculating quality adjusted life-years (QAL Y) gained by treatment. The rank
ordering of QAL Y measures proved to be quite insensitive to the particular
quality index being used and also to the discount rate. We recalculated the
Oregon QAL Y s for different age groups and aggregated them to the level of
morbidities in the analytical framework, using distributions derived from
Canadian hospital data.l
We calculated the QALYs used for the non-hospital sector differently. For
drugs and physician services, we assigned QAL Ys on a QAL Y-per-dollar basis
;)JR=>
\RJ!dsoq AU;)P OJ;)lqRuosR;)Jun ;)q PlnoM J! ';)=>U;)P!A;)q=>nsJnoqJ!M. 'O!JRU;)=>Ss,qJ
JO uo,JRJu;)W;)\dW! ;)qJ JJoddns OJ ;)"U;)P!A;) \R=>!U!I=>-OJ:>!W
;)lqRuOSR;)J
ou S! ;)J;)qJ 'J;)A;)MOH ";)lq!SR;)J W;);)S ARw suo'J:>np;)J ;)S;)qJ Al;)A!J!nJUI
"Ju:):Jl:)d r UtJl(JSS:)I Jo sA'lVO U! uo!J:Jnp:)l Js:)pow Al:)A tJ
PUtJgu!pu:)ds l(JltJ:)q JU:)WU1:)AOgO!ltJJUO U! uo!J:Jnp:)l Ju:):Jl:)d-Z tJ sJu:)s:)ld:)l
q:J!qA\ '(lOJ:J:)S :)ltJ:J gu!nu!Juo:J :)l(J OJ S:):JlnOS:)l Jo gU!JJ!qs :)qJ l:)P!SUO:J OJ
:)AtJq PlnOA\ SgU!AtJSJ:)u) SgU!AtJSssolg U! UO!II!W O££$ :)Z!ltJ:)l PlnoA\ suo!J:Jnp:)l
:)s:)l(J 'IItJl:)AO ":)JtJ!ldolddtJ :)q AtJW :)ltJ:J wl:)J-guol Jo W10J :)wos OJ gU!JJ!qs
SdtJql:)d 'AtJJSJo Sl(Jgu:)1:)gtJl:)AtJqg!l( Aq P:)Z!l:)J:JtJltJq:J:)ltJ s:)stJ:J:)s:)qJJo IItJ :):JU!S
":)ltJ:J Jo SW10J l:)l(JO OJ P:)JJ!qs :)q OJ :)AtJq PlnOA\ dnolg :)gtJ S!qJ guowtJ s:)stJ:JtJ!uown:)ud
OOS-'v putJ s:)stJ:J :)~OlJS 000'9 JtJl(J utJ:)w PlnoA\ 'AtJJSJo l(Jgu:)1 U!
Ju:):Jl:)d S-putJ sp:)q ItJJ!dsoq U! Ju:):Jl:)d or Jo uo!J:Jnp:)l ItJUO!J!PptJ:)A!JtJAl:)suo:J
tJ u:)A3 "l:)Plo putJ :)gtJ Jo SltJ:)A S-L AI1:)PI:) :)qt uo J:JtJdw! PlnoA\ suo!J:Jnp:)l
l:)qJlnJ AUtJ'v qgnoll(J r SO!ltJU:):JSU! P:)Z!ltJ:)l sJJ!qs :)l(J PUOA:)q':)JtJ1Jsnll! 01,
.puaqu laq.lnJ UaAa"Sl',})[lUW" aq. 8U!AOWJO a8ualluq:>
aq. s.u',}sald oslu .nq 'padol',}Aap ',}M O!lUU',}:>S
S!q. JO A.!I!qU!A ',}q. SWl!JUO:>
AIUO .OU S!q.L 1".009'9 Ala.uW!XOlddu lO .ua:>lad OZ laAO Aq pau!I:>',}pasn
U! spaq ale:> a.n:>uJO laqwnu aq. pUB...SAUP ~.9 O. SAUPZ"8 wall .ua:>l',}dOZ
Aq paU!I:>apsuq AU.SJO q.8ual a8ulaAu '06-6861 a:>u!s" .uq. sa.ou ~odal aq.L
.uasald aq. o. 0661 wall A.!I!qUI!UAUu.up U! du8 aq. passalppu .uq. pasualal
SUM.lodal .uawulaA08 IU!:>U!AOldO!lU.UQ uu 'O!lUua:>sS!q. 8u!dolaAap a:>u!s
"BtS JO 4t6ual
pUB spa8 IBt!dSOH °t SUO!t:>npa~ Ja4tJn~
£-9 xIPuadd"
"asuq alu:J-Jo-IaAal u OJasuq AJ!P!qlOWu wall alnsuaw awo:JJno
A {vO aqJ paJlaAUO:JaM 'IUJ,dsoq u, SAUJS
wlaJ-guol sapnl:Ju! q:J!qM 'asuquJuP
alU:J gu!nu,Juo:J u,qwnl°:J qS'J'lg aqJ gU!SO "SAUJS
aJn:Jusu AUMawus aqJ u,
SA{vO aqJ paJuln:Jlu:Jpuu SAUJS
1UJ,dsoqwlaJ-guol aqJ pap°:J-AJ,p,qlow aM
"UJUpAJ!P!qlOWIUJ!dsoq aqJ wall alU:Jgu!nu!Juo:J lOJ sA{vO paA!lap aM
" A{a/\!1:>aJJa
pasn
aq ue:> dVlI
Alsno!/\qo
aq1 Jo s}Jed
'ale salnseaw
UMOp){ealq
';)woq)
asaq1 alOJaq
asaq.L "aseqe1ep
a8e ue JO s!seq 'aq1 uo s8mp
8mp
paU!Jal
aq 1SnW pUR apm:>
ueMaq:>1e){Ses
01 sA 'VO
pau8!sse
l'aq10 10 1U;)!1ed1nO ;)laM A;)q1 1;)q1;)qM 01 8U!plo:>:>e
01 sA ,vO
S"9
p;)u8!sse
l{:Jvo.lddV
;)1\\ 'se;)le
ap!M -UlaIS.{S
V -II
aq1 wall
;)1\\ ilaq10
Ala/\
pa/\!lap
';):>!JJo
sa:>!/\l;)S ,sue!:>!sAqd
OM1 'as;)q1 U! S;)!1!/\!1:>e le1!dsoq-u!
wall
pa/\!lap
I.lVJ
They
.There
The
66 SustainableHealth Care for Canada
to the older elderly for such problems as stroke and pneumonia. Further research
is required to examine the feasibility of reducing the lengths of stay for these
activities, which may even include considering strategies for preventing some
of these admissions and others focused on ensuring adequate resourcing of
community-based care delivery.
6
Do We Need a New Regulatory
Framework?
One of the principal ways in which Canadians can influence the cost of health
care is through the rules and regulations that govern the way it is financed and
delivered. This chapter describes the regulatory framework in Canada, sets out
alternative regulatory systems, and then briefly assesses recent reforms in
Canada and Europe.
All the provincial
health care systems have the same basic regulatory
framework, which is characterizedby the following features:
.They are financed primarily publicly. The provincial governments function
as single payers and the federal government provides financial support;
are financed largely through a progressive income tax system, though
some provinces use or have used other mechanisms such as health care
premiums and payroll and sales taxes;
It is a mixed private/public system, with governments typically accounting
for about three-quarters of total health care expenditures;
is a high degree of choice for consumers and autonomy for health care
providers;
The delivery of health care services is primarily private, consisting mostly
of non-profit hospitals (governed by independent boards) and self-employed
fee-for-service physicians;
only health care services for which the federal government is directly
responsible are those for groups under its jurisdiction (i.e., native Canadians
on reserves, the military, the Royal Canadian Mounted Police, and inmates
of federal penal institutions);
.Most
health care professionals working outside hospitals are self-employed
and are supported by varying degrees of public money;
.saJuJS paJ!uo aqJ puu 'WOP~U!)l paJ!UO aqJ 'UapaMS 'spuupaqJaN aqJ su q:>ns
sa!JJuno:> 0;)30
awos U! paJuawa(dw! ~u!aq aJU puu 'SJ!Ids Jap!AoJd-Jasuq:>Jnd
puu
'sJa)JJuw (uuJaJu! 'uo!J!J~dwo:>
p~~uuuw
su SWS!uuq:>~w q:>ns ~pnI:>u!
~s~q.L .S)JJOM~WUJjAJoJuIn~~J ~A!JUUJ~J(U
jO sJ!Jaw ~qJJap!suo:> OJJuuJJodw! S! J!
'SUO!ss~:>~JJua:>aJAq paJuqJa:>ux~ uaaq suq puu sJU~WUJ~AO~lIu OJuowwo:> S!
q:>!qM 'S!S!J:> IU!:>uUU!jawosu~pJnq ~qJ UaA!O 'MoIs S! UO!J!SUUJJ
aqJ 'UO!JoWOJd
qJIu~q puu 'uo!JuaA~Jd asuas!p 'aJu:> pasuq-AJ!Unwwo:> pJUMOJ puu JU~WJU~JJ
puu SUO!Jm!JSU! WOJj AUMU sn:>oj aqJ ~AOW OJ AJ!SS~:>~uaqJ uo sJU~WUJ~AO~
IU!:>U!AOJd puu IuJap~j ~qJ ~uowu
SQ;)!AlQS
'PQ1nSU!-QP
PlnoM
QqJ JuqJ Qn'glU
AI\U;)!PQW
.A1USSQ;)QU
'gU!Qq
~lU
UQQq 1QqJ!Q
-0;)
'PQ;)np01tU!
pUU AU!Jnl;)S
PQPUUdXQ
SQ;)!AlQS
QAUq
1QPUn
'SQ;)!AlQS
snsuasuo:> ~q OJ sJuaddu aJaqJ aI!qM
JOU Q1U AQqJ
QWOS
JO 1Qqwnu
SQ;)!AlQS
'Q'gU1QAO;)
QSnU;)Qq
;)!Iqnd
'gU!St?Q1;)U!
PQ1nSU!-QP
Jo
Ut? pUU
A1USSQ;)QU-AI\t?;)!PQW-UOU
UQQq QAUq SWU1'g01d
'gU!SUQ1;)U!
q;)!qM
MQU 1QMQd
QWO;) St?q 'PQU!JQP
("A1t?SSQ;)QU
'Sl;)guuUW (OWH)
'SO861
Jno
'gU!QqQ1U
UQ){uJ "Q'!
'PQ;)np01JU!
10J
10PQSUQ1;)U!
SJUQWAt?d
QtUI QqJ Q;)U!S I01JUO;)
1QAQU St?M pUU AISnOnU!JuO;)
AIIU;)!PQW"
"Q"!)
PQ1nSU!
JO QdO;)S Qq.L
UO!JUZ!UUglO ;):)UUU;)JU!UWqJIU;)H Aq lOSl;)lnSU!
;)JUA!ld Aq palOJ!UOW AIJ:)!lJS ale SUU!:)!SAqd 'saJuJS paJ!uo
;)qJ U!
U;)A3 'S;)!lJuno:) l;)qJO Jsow U! asoqJ op uuqJ SUO!S!:);)PIU:)!U!I:) pUR ;)U!:)!P;)W JO
a:)!J:)uld ;)qJ laAO ;):)uanuu! ;)lOW as!:)l;)Xa upuuuJ U! SUU!:)!sAqd 'laA;)h\oH
.S;):)u!AOld JSOW U! UO!Jusu;)dwo:) ,SUU!:)!sAqd UO SIOlJUO:) IU!:)uUU!J h\OU
;)lU al;)q.L 'SIUJ!dsoq OJSUO!SS!WPUpUR SJS!IU!:);)dsOJSIUll;)J;)llOJ alq!suods;)l
AI!lUW!ld
;)lU Aaq.L 'slad;);))[;)Jug su J:)U Sl;)UO!J!J:)Uld AI!wuJ pUR IUl;)Uao
~3'U!:>UUU!JJUaWUlaAO3' OJ UO!J!PPUU! 3'U!punJ
JO Sa:>lnOSlaqJO 'sasu:> AUUW U! 'pUU Sa!lJS!U!W Aq IUAolddu lO!ld sal!nballaJJU.{
aqJ ~3'u!puads IUJ!du:> puu 3'u!Julado Jo Uo!Juludas aqJ S! 3'u!Ja3'pnq
IUJ!dsoq JO al"JuaJ JuuJlodw! uv °S~!J!A!J:>U
3'U!S!Ul-pUnJ '~Idwuxa lOJ 'q3'nolqJ
'AJ!UnWWo:> ~qJ AI!luw!ld S! SIUJ!dsoq lOJ 3'u!punJ Jo ~:>lnos laqJo ~q.L °qJluaqJo
S~!lJS!U!W IU!:>U!Aold Aq sJa3'pnq IuqoI3' q3'nolqJ p~punJ ~lU SIUJ!dsOH
~SUUIdpapunJ-AI:>!Iqnd l!aqJ U! s;}:>!Alas asaqJ Jo
awos apnI:>u! S;}:>U!AOld AUUW'U;}lPI!q:> puu A\lapIa ;}qJ su q:>ns'sdnolg IU!:>ads
lod .sasaqJsold pUU 'S;}SSU\g;}A;}'Sa:>!Al;}S \uJuap 'sgrup UO!Jd!l:>sald IUJ!dsoq
-Jo-Jno ;}lU sa:>!Al;}s pa:>ueU!J-AI;}JuA!ld q:>ns Jo S;}IdwUX3 .gU!:>UUU!J:>!Iqnd
Aq palaAO:> "Sa:>!AlaS AlUSSa:>;}UA\IU:>!P;}W" Jo ;}gUUl aqJ ap!sJno lIuJ JuqJ
sJ:>npold pUUSa:>!AlaS;}rn:> qJIU;}q OJP;}J:>!lJsalS! ;}rn:>qJ\uaqJo gu!punJ aJUA!ld
~a:>U!AOld OJ a:>U!AOld
moll Sa!leA 8u!JsaJ 10J a8elaAo:> :>!Iqnd JO aa18ap aq.L .paUMOAlaJeA!ld
AIU!em ale 'sleJ!dsoq U! asoqJ 10J Jda:>xa 'Sa!loJeloqel 8u!JsaJ le:>!paw
L9
If:JlJo.lddV
i1P!M -Wi11S'<S V -II
l.llJcI
68 SustainableHealth Care for Canada
Other
Regulatory
Frameworks
Internationally there are a number of models for regulating health care
systems. They contain incentives and rules that guide decisions made by the
individuals and organizations within health care systems. Work done for this
project by Contandriopoulos et al. shows that health care systems are built
around three poles: the State, health care professionals, and health care users.
Three pure regulatory models coincide with these poles: technocratic regulation
(command and control by the State), self-regulation by professionals, and
laissez-faire or market-based regulation based on competition (Figure 6-1).
Since no health care system is governed exclusively by anyone of them, and
no country, not even the United States, has an exclusively laissez-faire model,
four other blends of regulatory approaches are possible: public competition,
mixed markets, regulation by management incentives, and regulation by
professional incentives.1
The latter two place great emphasis on incentives. In view of physicians'
significant role in health care, the professional incentives approach assumes that
it is possible to establish standards for medical practice, that doctors respond
to financial or organizational incentives, and that the use of incentives by health
Figure 6-1
Health Care System Modes of Regulation
I Professionals
I
SOURCE Andre-Pierre Corrtandriopoulos et aI (1993), "Regulatory Mechanisms in the Health Care Systems of Canada and
Other Industrialized Countries Description and Assessment," Queen's-Univers~ of Ottawa Economic Projects,
Working Paper No 93-01, Univers~ of Ottawa, Ottawa
tnoqR SUO!Sn(:Juo:J tURJjodUJ!
:(apoUJ
sta'llRUJ
aUJos SMR1p URUJt(RS 't10da1
.S;}:J!A1;)S ;}It!:J l{JIU;}lf )0 AJ!IUnb
U AUld Jsnw
:J!lqnd
;}l{J ;}lnSU;}
pauuR(d
OHM
l!;)l{J
;}l!U)-Z;}SS!UI
)0 A:JU;}!:J!));}
10 paX!UJ
J;}'llUW-P;}X!W
aqt
puu
;}l{J OJ uulfJ :J!JU1:JOUl{:J:lJ;}l{J OJl;}sol:J S!
;)l{J l{J!M p;}!dn:J:JO;)ld
U su [pUU] UO!IUln~;}l
S:J!WOUO:J;} ;}lfJ S;}:JUld"
tua:JaJ R uI
OJ 1;}P10 U! ;}101 A10JUln~;}1
SIUUO!SS;»)Old ;}lU:J lfJIU;}l{ 'SI;}POW uo!J!J;}dwo:J
;}l{J lfJoq ul .l{:Ju01ddu
I;}POW S!l{.L ~".JndJno
10) ;)A!J:JUjJJU S! J! 'JlnS;)l
;}:J!A1;}S )0
'.IU
SW;}JSAS l{JIU;}l{
l{JIU;)l{ )0 ;)10:J ;}l{J JU UO!J:Jnp01d
J;} SOlnodo!lpUUJUO:)
AUS l{:Ju01ddu
S!l{.L 'UO!~;}llO
J:J!lJS!P ;}l{J )0 SJU;}P!S:l1 ;}l{J )0 S:J!JS!1;)J:JU1Ul{:JpUU l;}qwnu
;}l{J JO
S!Suq ;)l{J uo P;}l{S!lqUJS;} sJ;}~pnq Iuqol~ l;}JS!U!WPU Ol{M 'Sl;}~UUUW IUUO!~;}l 10
J:J!lJS!P Aq p;}JUnIUA;} S;):J!ld uo P;}Suq S! UO!J!J;}dwo:)
Sl;}P!A01d
;}lU:J l{JIU;}lf :J!lqnd
rue
;}JUA!ld
:J!lqnd
puu
.S;}:J!A1;)S 1;}))0
U l{:Jns
;}JUA!ld S;}AIOAU! puu ;}P!S Alddns
;)l{J U! UO!J!J;}dwo:J
OJ 1;}P10 U!
W01) Sl;}PU;}J s'l:l;}S P;}:JUUU!) AI:J!lqnd
S! Jul{J W;}JSAS ;}lU:J l{JlU;}l{ U U;)l{M sdOI;)A;)P J;}'llUW
U! Sl;):Jnp01d
laJl.lVW-paX!w
'l{:Ju01ddu
.W;}JSAS ;}WUS ;}l{J
;}l{J uo Sln:J:JO [apaw
UO!J!J;}dwo:J
:J!lqnd
;}l{J ;}'l!IUn
"uo!Jdwnssu ;)lquUO!Js;)nb u S! q;)!qM 'S;);)!oq;)
;)A!J;);)JJ;) pUU JU;)!;)!JJ;) ;)'lUW OJ P;);)U !.;)qJ UO!JUWJOJU!;)qJ IIU OJ SSa;);)UaAuq
SJ;)WnSUO;)JuqJ sawnssu t! 'JaqtJnd "sJassu J!;)qJ Jo Juawa~uuuw puu asn aqJ U!
!.J!I!q!X;)IJ Jo ;);)Jl1';>P
q~!q u SUO!J"t!JSU!~U!AU;)I 'paZ!IUJtUa;)ap S! SJSO;);)JU;)qJIU;)q
JaAO 10JJUO;)JuqJ s;>wnssu JI t".ta'lJuw ;)!Iqnd !.IIU!Juassa U1!Jo aJuqs Ja~Jul1!
JoJ ;)J;)dwo;) OJ SJap!AoJd a;)!AJaS ;)!Iqnd S;);)JOJ" "Iu Ja sOlnodo!JpuutUoJ !.us
'Iapow S!q.L "aJU;) qJluaq aA!;););)J II!M !.aqJ aJaqM UU!J"t!JSU! aqJ t;);)laS sJua!tud
'stua!tud t;)UJtJU °t !.J!I!q1! J!aqt uo !.111!qol~ pa;)uuuy aJ1!SUO!t"t!JSU! aJU;) qtluaq
puu 'wats!.s XUt aqt q~noJqt S! wats!.s u q;)ns U! ~U!pUnd 'a;)!oq;) puu a;)uaJaJaJd
Jawnsuo;) Ot asuods;)J U! SSaUaA!J;)aJJ;)pUU !.;)Ua!;)!JJ;) 8u!suaJ;)u! uo S! s!suqdwa
aqt 'q;)1!oJddu UO!I!ladUJo:J :J!/qnd aqt ul 'SJn;);)o !.IIU"t;)U uo!J!Jadwo;) aqJ
aJaqM °t S;)JclaJ slapow "uo!t!tadwo;)"
OMJ aqJ U;);)Mtaq a;)U;)JaJJ!p ;)!Suq aq.L
'Sl;}~UUUW
;}lU;) lfJIU;}lJ Jo
S;)!J!;);}ds
~UOlJS UO S;}!I;}l
Ot" P;}lJS!lqEtS;}
;}lJJ Jo
If;)UOlddu
t;}W ;}lU S;}A!t;);}fqo
pUU Sl;}P!AOld
;}~P;}IMOU'l
;}lU;) lJJIU;}lJ ~UOWU uo!J;)npold
JO I;}A;}I lJ~!lJ U pUU uo!J!J;}dwo;)
S!lJ.L t,,'sUO!JUZ!UU~lO
tulJt ~U!lnSU;}
S! SaA!tU;};)U!
ale;)
lO SIUnp!A!pU!
~U!PlUM;}l
Aq
;}1!lJM Sl;}~UUUW ~UOWU UO!tUAOUU! ;}~UlnO;)U;}
pUU salnJ
JO W;}tSAS AlOtUln~;}l
lJtlU;}lJ JO StS;}l;}JU!
Sl;}~UUUW JO ;}IOl ;}lJtS;}SS;}ltS
;}lJJ ~U!;)UUluq
'laAaMOlJ
V
.U;}WUl;}AO~
U! (StUl;)nU;}lnq
Allunsn)
'I;}POW sa(\!Jua:JU! JuaU/a8tJutJU/
;}lJ.L
z,,'[ S;}!JIe!;);}ds]
S;}!J!A!t;)e
SnO!leA
3'UOWe J! 3'U!tu;)°IIe
-U;}dWO;) JJUJS Ie;)!p;}W
pUR [StU;}W;lOt;}S
10J p~)j1eW1U;} Junowe
tuqJ SQ1nSe;}W"
;};}J P;}tU!tO3';}U]
;})jUW
SlOJ;)°P
If:Jvo.lddy
UO!tUS
Ile1;}AO uu 3'U!)jeJ 10J ;}IQ!SUodS;}l
UO!S!;);}P U! UO!teZ!Ie1JU;};)QP JO ;};}l3';}P ;}lqe1QP!SUO;) e 10J sMoIle
'3'U!)jew
S! ;}A!3' 'IU t;} SOInodo!lpUUtU°:J
S!q.L 'SlOt;)OP hq QPUW SUO!S!;)QP ;};)U;ln\JU!
69
II!M
QIdWUX;}
;}UO
I;}POW
tU;}WU1QAO3' pUR Sl~3'UUeW ;}lU;)
iJP!/rI.-UliJls.{S Y -//I.1Vc/
."Neither
70 SustainableHealth Care for Canada
command and control planning nor pure neoclassical markets seem
to be capable of achieving the broad mix of objectives of modern health
systems";
."There
is no necessary connection between introducing competitive mechanisms and markets on the one hand, and private ownership on the other";
"Fragmentation of health care financing among multiple, independentservices,
is not necessary to achieve macro or micro organizational efficiency."6
Both Saltman
and Contandriopoulos
characteristics
of successful control
centralized health care system.
The Significance
et al. insist that one of the primary
of health care expenditures
of Central
is a fiscally
Control
Contandriopoulos et al. analyzed the influence of institutional differences
on costs and outcomes. They examined patterns and characteristics of regulation
in 22 OECD countries and then assessedtheir impact on health care expenditures
and overall system performance. Perhaps not surprisingly, the United States
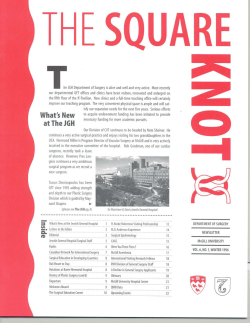
has the worst cost control performance and Denmark has the best (Chart 6-1)}
Health care outcomes as measured by life expectancy and infant mortality
vary among OECD countries, but the variation is small in the case of the former,
and somewhat larger in the case of the latter (Chart 6-2). In contrast, the wide
variations in total health care expenditures (see Chart 2-3) and cost-control
performance suggest that health care outcomes are not especially sensitive to
such variations. The fact that different countries achieve good health outcomes
with wide variation in total health care expenditures points to the possibility
of containing expenditures without damaging outcomes.
In assessing the factors that account for the high level of success enjoyedby
some countries in controlling health care expenditures, Contandriopoulos
et al. found that:
centralized
uncentralized
.the
health care systems are better able to control expenditures
fewer the sources of funding,
the greater the ability
a greater share of private sector financing
expenditures;
than
ones;
to control
costs;
is associated with less control over
6".aJOtlpuadxa q1JUaq Jo 1°j:Juo:) JoJ uol1lPuo:) ,\.ressa:)au
U sl 'UOflUXU1 IUJauag Jo 100 pa:)uuuy Swa1SAS :)llqod ul puooJ puPi aq'J Jo
'gUI:)UUUY a:)JOOS-alguIs 1Uq'JPIuS uaaq suq 11 'SJapIAoJd 01 S1UaWAUdJaq'Jo pUU
s1agpoq Jo gul11as aq1 uo A:)IIOd [IUJ1ua:)] luuofluU pau[lWa1ap U sl ,\.ressa:)au
oslV .1u~I:)YJoS 10U are Aaq'J 10q 'gulpuads JO IOJ1UO:)paUIU1sos JOJ SUOfllpuo:)
,\.ressa:)au aq AUW spoq1aw Jaq10 pUU s1agpoq JUqOlg" 1Uq'JpaAJasqo SUM 11
'ApUU1Jodw! AIJUOhH 8".wa1sAs aq'JJO A11:)udu:)aq'Juo puu sJaPIAoJd 01 s1uawAud
uo SIOJ1uo:) JUJ1ua:) 1:)aJIP gu!sodWI Aq 'slq'J JO a:)uasqu aq'J ul 'JO sJaAud A:)JUd
-PJlq'J aq'JJo puuq aq'Jguluaq'Jguaj:Js Aq" AIQIUW paAalq:)u SUMsaJOtIPuadxa are:)
q11uaq JO 1°j:Juo:) 1Uq'JpaAJasqo (wopgU!)l pa1luo aq'J pUU u!UdS 'spuupaq'JaN
aq'J 'pUUlaJI 'AuUWJao 'a:)uUJd 'wolglag JO slsAJUuU S,1SJOHuI) O;)HO aq'Jpuu
a:)upa1uI JapIAoJd-JapuoJ aq'J UO aJOtUJa111aq'JJO slsaq'JUAs slq ul U){JapZUd
.J;}~~;}J8 S! s;}Jn~!p
-u;}dx;} ;}JP.;)q:}I~;}q IOJ1UO;)o~ A~!I!q~ ;}q~ '~!l;}~!l;) P;}u!UJJ;}~;}p;}Jduuq:} J;}q~~J
S~SO;)fI!;)!l°~S!q 8u!sn 8u!~;}8pnq I~qoI8 uo P;}S~q S! 8u!punj I~~!dsoq ;}J;}qM .
p~
~daD ';}q'!Jo ,;}Jeqs S,lO'!;)';}S';}Je;) q1JU';}q';}q1S! se 'l';}MO{ ,;}Ie S';}lO"!!pu';}dx';}';}Je;)
q1{e';}q {e,!o,! 'uo!'!esu';}dwo;)
10 SW91SAS 9JB:)
pUB BpBUB:)
O!WOUOO3 BMBUQ
'SI:J9[OJd
da~
,sue!;)!s,(qd l';}AO {OI!UO;) 1';}'!e';}13S! ,;}1';}q1';}l';}qM .
10 .\JISJ91\IUn-S,U99no
4IIB9H
uo p&SBq 9JB SUOII:>9!OJd
BMBIIO
..IU9WSS9SS\I
941 UI SWSIUB4:>9~
9J""
~0IBln69~"
411B94 UO S9JnlIPUadX9
'BMBUQ 10 .\JISJ9,!Un
'~O-~60N
JadBd 6UI'lJOM
pUB UOlldlJOSea :S9!'IUnO:)
peZIIB!'ISnpUI
J941O
'(~66~)
Blld""
"lB 19 SOlnodOlJpuBjuo:)
Jad IBnlOB pUB pel:>9!OJd
OJ9Z IB 19S 'XepUI
9 dnoJ~
g dnoJ~
"dnoJ~
~ dnoJE)
c: dnoJ~
9JJ9Id-9iPU\I
U99Mjeq
.""nos
90U9J9111P 94.L
UB9W 941 WOJI UOIIB!,B"
~
~
~ dnoJ~
S086 ~ e41 U! e:>uewJoJjed 10JIUO~ISO~ Jo s5u!)jue~ leUO!leuJelul
~-9lJe4~
IL
l{:JtJo.lddy
;JPIM-W;JIS,(S
y -II
t.ltJJ
72
SustainableHealth Care for Canada
B. Infant Mortality
Rate, Selected
OECD Countries,
1970 and 1990
Live bir1hs
i
~
'"
-,
SouRCE: DECD (1993), DECO Health Systems, Facts and Trends
f
0
z
~i~
~
.,
"
~
aAeq sJUaWUJaAog 'ApUa:>aJ PUg sOL6 [ aqJ JoJ Jda:>xa 'a:>ueJnsu! qJ,eaq :>!,qnd
Jo AJOJS!q aqJ JO JSOWJOJ asne:>aq S! J! ApJed .pJeMJoFqg!eJJs Jou S! uo!Jsanb
S!qJ OJ JaMSUe aq.L lSaJfiJ!puadxa ale:> qJ,eaq aJegaJgge gU!!IOJJUO:>JO pJo:>aJ
JSJOMpuo:>as aqJ aAeq J! saop 'uaqJ 'AqM 'saJfiJ!puadxa ale:> qJ,eaq JO ,OJJUO:>
leJJua:>JO sJuawala ,eJuawepunJ aqJ u!eJuo:> swaJsAs ale:> qJ,eaq s,epeueJ JI
gu!pu;}ds
1t!!Jut!Jsqns
';}It!;)
;}It!;) ljJIt!;}lj
jO
ljJIt!;}lj
UU!PUUt!:)
£I,,"gu!punj
;)!Iqnd P;}Z!It!lJU;};) Aq P;}Jl;}X;}
l;}AO 10lJUO;) ;}lj1 AOlJS;}P PlnOM S1u;}!Jt!d OJ S;}glt!lj;) l;}Sn
WlOj ;}lj1 U! lO ;};)ut!lnSU!
jO gU!pUnj
;}Jt!A!ld
jO UO!Jt!Z!It!lJU;};);}Q"
;}lj1 U! 10lJUO;) IUlJU;};)
U;})jU;}M
pt!;}ldS;}P!M
'u)jl;}pzt!d
AUW S!lj~
jO
WlOj ;}lj1 U! l;}ljJ!;}
OJ gU!PlO;);)¥
"( ;}lU;) lj1lU;}lj
"SW;}JSAS
gU!;)UUU!j
OJ
P;}JUI;}l Jt!ljJ AllUln;)!Jlud)
gU!)juw-UO!S!;);}P
gU!Z!IUlJU;};);}P pUR S;};)!Al;}S IU;)!P;}W
gU!lnSU!-;}p
PlUMOJ PU;}lJ t! ';}ldWUX;} lOj 'S! ;}l;}lj~ "IOl~UO;) IUlJU;};) moll gU!JU;}lJ;}l
;}lU S;};)U!AOld
;}ljJ Jt!ljJ sug!S ;}lU ;}l;}lj1
;}lU SIOlJUO;)
Iuqolg
;}1!ljM
'sJs;}ggns
;}qJ U! 1U;}WU!UJuO;)-JsO;) ;};)lOjU!;}l
;}AUlj SJU;}WUl;}AOg
IU!;)U!AOld
'J;)Uj uI "JU;}!;)!jjns
QJ30
JOU ;}lU A;}qJ 'Alt!SS;};);}U
;}q1 su '1n8
pUt! ljS!lqt!JS;}
(AIJU;};);}l
OJ l;}MOd
pUR sOL61
"W;}JSAS ;}lU;) qJIU;}q
Auosdouow
l!;}qJ p;}sn
;}ljJ U!) ;}W!J OJ ;}W!J wold
.S, UPUUUJ ;})j!1 SW;}JSAS l;}AUd ;}lgU!S JO S;}gUJUUApU JUU;)!J!ug!S ;}l/J JO ;}UO S! S!l/.L
Z\"SJJUdl;}JUnO;) UU;)!l;}WY
~S;}mp~;)old
;)!JsougU!P
l!;}l/J UUl/J P;}Z!I!Jn AI;}A!SU;}JU! ;}lOW ;}lU A;}l/J 'JlnS;}l U SU
pUB IU;)!gms
X;}(dWO;) U! ;}Z!IU!;);}dS UPUUUJ U! SUU!;)!SAl/d
l;}M~J 'AIJUI!W!S .S;}JUJS P;}J!Ufl ;}l/J U! UUl/J UPUUUJ U! ;}W!J ;}IP! SS;}Il/J!M ;}Jul;}dO
Sl;}UUU;)S 1;:) 10 gU!gUW!
;};)UUUOS;}l ;)!J;}uguw
SU l/;)nS Ju;}wd!nb;}
l/;);}J-l/g!l/
';}ldWUX;}
lad
.S;}!goIOUl{;);}J
AJIU!;);}ds ;}l{J 'Ju;}wd!nb;}
,,'UO!JU;)°IIU
gU!;)np;}l
JSO;) l/g!l/
M;}U Jo UO!J!s!nb;)u
pun 'SlOJ;)°P
JO X!W
pUB S;}!J!I!;)UJ U! JU;}WJS;}AU! IUJ!du;) l;}AO S{OlJUO;) 'S! JUl/J
;};)mOS;}l wu;}lJsdn"
Jo SUU;}W JuuJlodw!
S! SW;}JSAS ;}It!;) l/JIU;}l/ P;};)UUU!J AIIUIJU;};) U! SJSO;)
uu Jul/J SACS °l/M
'u)jl;}PZUd
Aq P;}Wl!JUO;) S! S!l/.L
11,,'swa1SAS q11uaq IUUO!1UU U! SJ01:JU) 1U;)WU!U1UO:J-1S0:J Aa)(
S! JaMod 8u!suq:JJnd
Auosdouow
S!q.L 'sa:J!AJaS IU1!dsoq )0 AJaA!lap
aq1 )0 auo"
puu
UO!1uz!uu8JO
aq1 JaAO IOJ1UO:J )0 (uap 1uaJ8 u as!:JJaxa
swa1sAs JaAud-a(8u!s
a8uuRw
puu
aq1 'RPUUU:) U! 'paapuI
AlaA!1:Ja))a
(U1!dsoq
'saJn}!puadxa
°11UUM s1UaWUJaA08)!
JO) SUO!1U:J0((U JO s1a8pnq
Aq paZ!Ja1:JUJuq:J
'swa1sAs
01 sa:Ju!AoJd
MO((U
aJu:J q1(uaq a1u8aJ88u
IR!1Uassa S! 'saJn}!puadxa
luqo(8
aJu:J q1lU;)q papun)
pUR 8u!:Juuu!)
A(:J!(qnd
UU!:J!sAqd
a:JJnOS-aI8u!s
U! (OJ1uo:J (UJ1ua:)
OI".SW;}tSAS ;}teA!Jd rue ;)!Iqnd JO ;}In}X!W e te 3'U!'}JOOI
;}Je SW;}tSAS ;}Je;) qtle;}q 3'U!tS!X;} 3'U!AJ!POW JoJ slesodoJd [;};)U;}q pue] I;}A;}I
lenp!A!pu! ;}qt te SW;}lqoJd ;}Aeq tnq a/vSa.l:JSv alf/ U! S/so:>/O.l/uo:> 0/ a/qv a.lolU
a.lv slUa/siCs :>!/qnd" 'pueq J;}qtO ;}qt uQ .I;}A;}I OJ;)ew ;}qt te StSO;)3'U!IIOJtUO;) U!
Atln:>!JJ!p te;}J3' ;}Aeq A;}qt 'J;}p!AOJd ;}Je;) qtle;}q rue tu;}!ted ;}qt Jo /at1a/ O.l:>!1U
alf/ /V S/so:> /°.1/110:>0/ sat1!/ua:>lI! SIIO.l/S at1vlf slUa/s.{"sa:>uv.lnSU! If//valf pasvq
-a/vt1!.ld ;}1!qN\'pueq ;}UO ;}qt uo 'teqt punoJ ;}Aeq SJ;}q;)Je;}S;}JJ;}qJo 'SJe;}A OZ tsed
;}qt J;}AO 's;}tetS P;}t!Uf1 ;}qJ rue 'WOP3'U!)f P;}J!uf1 ;}qt 'epeueJ 3'u!JedwoJ
£L
If:>vOJddy ;JP?M-W;JJs.{S y -II
!JvJ
74 Sustainable lfealth Care for Canada
not used their power as single payers to control total health care expenditures.
It may also be traced to the divergence between the Hall projections and the
actual number of physicians (see Chapter 2). Perhaps incentives that do not
promote the efficient and effective use of health care resources are part of theproblem.
Still another contributory factor may be the nature of the existing
regulatory model, which relies heavily on professional incentives.
The countries that are most successful at controlling health care expenditures
(Denmark, Ireland, Sweden) make use of market mechanisms tempered by
technocratic management techniques (the mixed market/public competition
models; see Chart 6-1). Countries that use professional or management incentive
models as the dominant regulatory approach (Canada, the Netherlands, Germany, Australia, New Zealand, Finland, and Norway) do not achieve as effective
control over health care expenditures. In view of the limited knowledge of how
health care spending affects outcomes, the allocation of health care resources
is more effective if done through political or technocratic mechanisms than
through professional incentives. The U.S. health care system is closer to the
laissez-faire model, is very fragmented, and its total expenditures are much more
difficult to control.14
Pazderka points out that health care systems driven by professional values
emphasize state-of-the-art clinical interventions and specialization, rather than
primary care and prevention. This may lead to unnecessary surgery, excessive
prescribing of drugs, an excess supply of some types of medical specialties,
and a lack of primary care. He also argues that fee-for-service reimbursement
acts as a barrier to the substitution of cost-effective health professionals. There
is no financial incentive for physicians to use health care providers such as
midwives and nurse practitioners. Thus opportunities for labour substitution
efficiencies cannot be realized in the existing regulatory framework. Indeed,
there are many regulations that prevent more cost-effective substitutes -for
example, professional governance, bans on professional advertising, laws
against substitutes, not insuring substitutes for coverage of their services, and
impeding the establishment of alternative forms of health care delivery.15
Possible
Alternatives
for Canada?
Until recently, changes to the regulatory framework in Canada have not been
seriously considered. Is it possible to modify the present regulatory framework
or to adapt others that might control costs, achieve greater efficiency, and
allocate resources equitably? Maintaining global control of expenditure on
hospitals and physicians' expenditures requires blunt instruments, which, over
time, become difficult to justify politically. Incentives that are conducive to
realizing these efficiencies have to be built into the framework. At the same
suo!Jsanb OJ aJejaJ s)jS!J JaqJO o(uo!Jeu!wop leUO!SsaJoJd SnSJaA uo!Jed!:>!JJed
Aej pue jOJJUO:>leJJua:> panU!Juo:> SnSJaA JuawJ;)Modwa je:>oj) spJeoq U!qJ!M
SJ:>!!JUO:>pue ~(;)A!J:>!JJsaJOOJJO peOJq aq AeW q:>!qM) gu!uuejd U! sJ:>!!Juo:>
~(aJJua:>aqJ WOJJ paljoJJuo:> AjaSOOj OOJJO Anqg!J OOJgU!aq UaaMJaq) sJagpnq
JaAO SJ:>!!JUO:>~Sa!poq je:>Oj pue sJUaWUJaAog je!:>u!AoJd aqJ UaaMJaq jOJJUO:>
JO ueds aqJ U! 'sdnoJg JsaJaJu! UaaMJaq '(Sleog je!:>ueU!J rue le:>!J!lod uaaMJaq)
JaMod U! sJ:>!!Juo:>ale S)jS!JJofew aqJ 'JaAaMoq 'su!eg je!JuaJod asaqJ Jsu!egy
":)Jt!;) l/t!t!:)l/ :)p!stno st!:)Jt! U:)A:) JO l/t!t!:)l/ :)A!tU:)A:)Jd
°t St:)'3pnq !t!qO!'3 WOJ} spun}
J:)}SUt!Jt °t :)do;)s :)JOW (;) put! 's:)!;)U:)!;)!}}:)
!t!!J:)'3t!Ut!W P:);)Ut!l/U:) put! UO!tu;)![dnp :);)!AJ:)s U! UO!t;)np:)J °t :)np SS:)U:)A!t;):)}}:)
-tSO;) (q 'UO!tt!J:)doo;) !t!JOt;);)SJ:)tU! put! S:);)!AJ:)S }O UO!tt!J'3:)tU! P:)St!:)J;)U!(t!
WOJ} MOll °t P:)A:)![:)q :)Jt! UO!tt!Z!!t!JtU:);):)p WOJ} SU!t!g A;)U;)!;)!}}:) :)l/.L
"S:);)lnOS:)l JO UO!Jt!;)O\\t! :)lfJ U! AJ!nb:) :)lOW put! ~SJOJt!lJS!U!Wpt!
put! 'Splt!Oq 'sut!!;)!J!\od \t!;)0\ Jo Jlt!d :)lfJ uo SS:)U:)A!suods:)ll:)Jt!:)l'g ~W:)JSAS:)qJ
'gU!'gt!Ut!W U! ;)!Iqnd At!\ :)qJ Aq UO!JUd!;)!Jlt!d :)lOW WOlJ MOU OJP:)A:)!I:)q :)It! SU!u'g'gu!uuu\d
:)q.t "A;)U:)!;)!JJ:)lOJ :)do;)s l:)JU:)l'g 'PUO;):)s put! '( sp:):)u \t!;)°I OJ:);)Ut!A:)\:)l
'":)"U 'gu!uuu\d l:)JJ:)q 'JSl!J ':)pnI;)U! UO!JUZ!\UlJU:);):)PJo S:)'gt!JUt!Apt!U!t!W :)q.t
.UO!1t!Z!Jt!A!ld UaAa
put! 'UO!JnIOAap 'UO!Jt!galap 'UO!1t!11Ua:>Uo:>ap
011aja1 Ut!:>1! ~SgU!q11t!laAaS ut!aw
Ut!:> UO!Jt!Z!It!lJUa:>ap Jt!q1 J:>t!j aqJ Aq xaldwo:> a10W apt!w s! anSS! aq.L .gU!'lt!W
UO!S!:>apa1t!:>q11t!aq aZ!It!11Ua:>apOJSAt!M pt!q put! poog Alqt!q01d a1t! a1aqJ 'Sp10M
1aq10 uI 91".sUO!SSaj01d 1t!:>!paW aq110j al01 pa1ap!SUO:>a1t! put! 'sawo:>Jno qJIt!aq
10j A1!I!qt!Juno:>:>t! MaU t! 'A1!I!q!suodsa1 Jo UO!1t!Z!It!lJUa:>ap" 10j sang1t! (OHM)
UO!1t!Z!Ut!glO q11t!aH PI10M aq.L .0:)30
aq1 U! pall01JuO:> AllnjSsa:>:>ns a1t!
samJ!puadxa a1t!:> q11t!aq IIt!laAo a1aqM swaJsAs a1t!:> qJIt!aq jO S:>!1S!la1:>t!1t!q:>
A1t!W!ld aq1 jO aDO S! UO!Jt!Z!It!11ua:> 1t!qJ sJsaggns q:>1t!asa1 It!UO!1t!U1aJU!
'aw!J awt!s aq1 JV .a:>U!A01d q:>t!a U! Al1ua1ajj!p 'paqs!lqt!1sa put! 'padOlaAap
'paA!a:>uo:> gu!aq S! 1! 'laAaMOH .JuawaA01dw! Ut! aq At!W -UO!1t!:>°IIt! a:>mosa11aAO
A1!10q1nt! paZ!It!11ua:>ap qJ!M 101JUO:>1t!:>S!jUMop-d0110 'UO!1t!Z!It!11ua:>apsa:>U!A01d It!laAas Aq padolaAap gu!aq S! 1t!qJ wa1sAs aq1 01 UO!Jt!:>y!POWaq.L
onb smUJS :)qJ uo JU:)W:)AOldw!
's:)!lJUno:>
.:)Jq!ssod :)q pJnoqs
l:)qJO uuqJ [OlJUO:> Jso:> :)A!J:>:)JJ:) SS:)[
:)AUq S[:)pOW S:)A!JU:):>U!-JUUO!SS:)JOld lO JU:)W:)'3uuuw
:)qJ l:)qJ!:)
JuqJ pUU 'J:)pOW S:)A!JU:):>U!-JuUO!SS:)JOld u U!qJ!M A[!lUW!ld
JuqJ u:)A!D
.S[:)pow
:)qJ wall
Ju :)q Jouuu:> w'3!pUlUd
lU:)[:> S! JI .sw'3!pUlUd
AlOJU[n'3:)l
qJ!M S:)!lJUnO:>
UO!J:>unJ AjJU:)lln:>
(lOlJUO:> :>!JUl:>OUq:>:)J) JOlJUO:>-puu-puuwwo:>
-z:)SS!U[ :)qJ jO :)W:)lJX:) l:)qJ!:)
:)M
JuJoJ lO :)l!Uj
M:)U AUU JuqJ lUJ os :):>U:)P!A:)
M:)U :)loJdx:)
OJ :)W!J S! J! SdUql:)d
.WQ~SAS ~U!~S!XQ Qq~ JO SUO!s!AOJd A~!nbQ Qq~ JO
S~:>QdSBJQABd-QI~U!S
SL
pUB IOJ~UO;) IBqOI~
l{:Joo.lddy i1P!M -Wi1Js'<S y -II
Qq~ Q;)!J!J;)BS O~ QlqBJ!SQP ~OU S! ~! 'QW!~
J.l°J
76 SustainableHealth Carejor Canada
of boundaries -Are geographic boundaries defined, and if so, how? What is
the optimal size of a region? Can qualified health care planners and managers
be attracted to work in locations other than the major centres? Finally, if each
new regional board requires an administrative and planning infrastructure to
support its work, the costs could actually increase, at least in the short run.17
Another approach that may increase efficiency while maintaining the basic
principles of the present regulatory framework is the mixed-market model. This
approach, which is used in Germany, the Netherlands, and the United Kingdom,
has the following features:
Services in kind are provided to eligible consumers;
There are public third-party insurers (governments);
is through general taxation;
There are direct fee-for-service or capitation payments by public insurers
to independent providers (via contracts);
choice of health care providers on the part of consumers is preserved;
efficiency continues to be the responsibility of government; and
Micro-economic efficiency can be realized through "a combination of
consumer-led competition over quality, and the development of suitable
incentives and regulations in the contracts between the insurers and the
providers."18
The OECD (Hurst) analysis of the different regulatory approaches states that
"only the contract [mixed market] model is suited both to the pursuit of macroeconomic efficiency and to the pursuit of micro-economic efficiency. In
addition, the [mixed market] contract model seems better suited to selfregulation and appropriate provider autonomy than either of the other two
models [public reimbursement and public integrated models]."19 While these
features may help to explain the convergence on this model among the seven
OECD countries that Hurst analyzed, Pazderka points out some emerging
difficulties with the mixed-market approach.
In his review of Hurst's study, Pazderka notes additional features of the
mixed-market model that may be significant for Canada: the methods of
reimbursement that can be used and the importance of the central control
function for government (as third-party insurer). According to Pazderka, there
are three principle ways of reimbursing providers:
Financing
Free
Macro-economic
;)nleA ';):JuewJoJJ;)d}o ;)8p;)IMOU'l ;)qt Jo ;)sn s,J;),(ed ;)qt uo spu;)d;)p A;)UOW JO}
;)nIeA 8u!tt;)D 'SJ;)p!AOJd ;)qt uo Je;)q °t s8u!Jq (;)teA!Jd JO :J!lqnd) J;),(ed ,(tJed
-pJ!qt ;)qt ;)Jnss;)Jd teqM S! tU;)W;)I;) tuetJodw! tSOW;)q.L 'SJ;)p!AOJd ;)qt tUOJ}UO:J°t
II!M le:J!t!IOd ;)qt rue uo!tewJo}u!
;)qt qtoq ;)p!AOJd °t 't;)'lJew ;)qt Jo ;)P!S J;)Anq
;)qt u;)qt8u;)Jts °t MOq" }O ;)8u;)lIeq:J ;)qt S! q:J!qM 't!lds J;)p!AoJd-J;)seq:JJnd ;)qt
JO} suose;)J tue:J!J!u8!s tSOW ;)qt }O ;)UO stq8!lq8!q osle ;)H 'SJ;)p!AOJd ;)teA!Jd
rue :J!Iqnd 8u!t;)dwO:J ,(q S;):J!AJ;)Slet!dsoq }O UO!s!AOJd ;)qt rue 'S;):J!AJ;)S ;)qt
8U!P!AOJd JO} ,(t!l!q!suods;)J ;)qt WOJJ ;)Je:J qtle;)q 8u!seq:JJnd JoJ ,(t!l!q!suods;)J
}O uo!teJed;)s ;)qt S! t;)'lJew P;)X!W ;)qt }O ;):Jue:J!J!u8!s ;)qt teqt sts;)88ns
e'lJ;)pzed 'sw8!peJed ,(JOteln8;)J U! 8u!JJn:J:J0 s;)8uuq:J ;)qt Jo M;)!A;)J S!q ul
zz,,'sdnOl~
asaqJJO Jleqaq uo ,slaAnq, aA!J:)ese J:)e OJpue uo!Jelndod aqJ ~uowe SdnOl~
paau JUalaJJ!p10JsJa~pnq~u!seq:)lnd qs!lqeJsa OJsa!poq ~u!punJ AJled-pl!qJ aqJ
10J alqel!Sap aq osle AeWJI '(AJ!leJIOW10) AJ!P!qlOWaA!Jl1lalpue aln}:)nlJS a~11
se q:)ns SlOJ:)eJ10J paJq~!aM 'Sa!poq ~U!punJ aqJ Aq paAlaS aq OJUOnelndod
aqJ uo pasuq aq Plnoqs sJa~png ,[ Sl!:)uno:) qJleaq J:)!lJS!P'spleoq leUO!~al]
Sa!poq ~U!punJ AJled-pl!qJ paZ!lelJUa:)ap OJ sJa~pnq aJe~al~~e paJelal-~S!l"
aJe:)°lle OJspunJ ale:) qJleaq laAO 101JUO:)
le!:)U!AOldlelJua:) aAeq OJAlessa:)au
aq osle plnOM J! 'waJSAS ue!peue;) aqJ U! pau!eJu!I1Waq OJ S! AJ!nba JI
yz,,"(WOP'3U!)J
p;}J!Un
;}l(J pUU AUUWJ;}D U! SIt1J!dsol() SJ:>t1JJUO:>P;}Jt1I;}J-;}WnIOA
put!
PUt1 sJ;}'3pnq lt1qol'3"
,(AU~WJ;}D U! SU~!;)!SAqd) ;};)!AJ;}S-JOj-;};}j pU~ sJ;}~pnq I~qoIg"
~,,(WOP~U!)f paJ!Un aLlJ PUE
spuEIJaliJaN aLlJ'puElaJI u, sJaUo,J,J:>EJdIEJaUa~) uo,J'Jadwo:> PUEUO!JEJ,dE:>"
aJt! 'At!A!t:JnpoJd
JOj SpJt!MaJ qJ!M sdt!:J aJ"t!puadxa
:a(dwt!xa JOj'a(q!ssod
(t!qO(~ au!qwo:J
q:J!qM 'SJap!AoJd aJt!:J qJ(t!aq °t JuawAt!d jO SWJOj pax!W Jt!l(J saJou JaqJJnj aH
WOJJ J:)JJns OJ SPU:)J «:)pOW
oz f.:>U:)!:>!JJ:)U! :>!WOUO:>:)OJ:>!W
UO!JeJ~:)JU! :>![qnd) pJ!qJ :)qJ pue
'Ju:)wu!eJuo:> JSO:>OJJ[:)sJ! pu:)[ f.[!pe:)J JOU s:)op poqJ:)W (Ju:)w:)sJnq
-W!:)J) JSJ!J :)qJ :):>U!S 'poqJ:)w (J:>eJJuo:» pUO:>:)S:)qJ uo :):>U:)~J:)AUO:>
:)WOS [SeM :)J:)qJ JeqJ p:)JOU J:)qJJnJ SeM JI] """ s:)!Je[es pue sJ:)~pnq
[eqo[~ Jo WJoJ :)qJ U! 'w:)Jsf.s p:)JeJ~:)Ju! f.([e:>!JJ:)A e U! SJ:)p!AOJd
JO Ju:)wf.ed J:>:)J!P 'pJ!l!j. "uo!JeJ!de:> JO :):>!AJ:)s JoJ :):)J JO UJJoJ :)l!J
U! 'SJ:)p!AOJd (Ju;)pu:)d:)pu! f.[[ensn) Jo Ju:)wf.ed J:>:)J!PJoJ ~U!P!AOJd
J:>eJJuo:> e 'pUO:>:)S "(SJ:)P!AOJd pue sJ:)Jnsu! ;)l!J U:):)MJ:)q J:>eJJuo:>
OU) sJu:)!Jed Jo Ju:)w:)sJnqw!:)J f.q SJ:)p!AOJdJo Ju:)wf.ed J:>:)J!PU!'JSJ!d
LL
'/:JDO.lddy JP!M -WJ1S,{S Y -I/l.lDJ
78 SustainableHealth Care for Canada
Key Aspects
of the
Mixed-Market
Model
In his comparative
study of health care reform in seven OECD countries, Hurst
observes that the following key aspects of the partly self-regulating, public contract
model have already been tested in one or more of the countries:
."Universal
public cover with supplementary voluntary insurance (Belgium,
France, United Kingdom)";
."Government
control of total public health expenditure
United Kingdom)";
."A
(Germany,
Netherlands,
central fund for allocating risk-related
budgets to decentralized,
monopsony,
third-party funding bodies (Belgium, United Kingdom)";
."Decentralized
(United
funding
bodies to establish
budgets for different
public,
need groups
Kingdom)";
"Separation between decentralized 'buyers' and providers (Germany)";
"Consumer-led competition between public and private providers (France)";
."Globally-budgeted
contracts between 'buyers'
money to follow the patient (Germany)";
"A high level of self-regulation
by third parties
and providers
and providers
which
allow
(Germany)."23
In all of these countries,
the public sector is being revitalized through the
development of internal markets where competition is encouraged between public
and private providers, on the one hand, or between public and private insurers,
on the other.
of services, and effectiveness of providers."24 This separation seems to make
possible a "better expression of consumer and taxpayer preferences, setting
standards, measurement of performance, and making choices."25
Where the regional purchasing authorities have a choice among competing
hospitals, their preference would probably be those organizations that can
provide high quality, efficient, and cost-effective services. Such competition
also offers incentives for hospitals to link resources to health outcomes.
Still, as is the case with the decentralization initiatives underway in Canada,
Pazderka feels that it is "too early to assesswhether the reform [in the United
Kingdom] successfully combined the advantages of the national health service
model (control on overall spending and social equity) with the advantages of
a market model (responsiveness to consumer demands)."26 Early judgements
on the success of the reforms are mixed. For instance, Pazderka notes that, with
the exception of large districts with large movements of patients across regional
J! 'UI!:> pUI! 'S;)U![ [l!nSU;)Suo:> ~UO[I! ;)'\[0'\;)
01 A:>![Od 1!Wl;)d [[!1\\
S;)JnSI!;)W [[I!UOmSUI!J1] ;)S;)lj1 JO UO!1I!n[I!'\;) pUI! UO!11!1U;)W;)[dW! ;)IU
:SAt/S OHM
uo!J!sodwo:>
:>qJ U! s:>8ut/q:> :>Jt/J!I!:>t/J OJ p:>l!nb:>l
put/ O:>lOJ moqt/1
loft/w
'OSIV
:>q PinoN. SW:>JSAS UO!Jt/WIOJU!
:>qJ SV .SlOJ:>:>S Al:>A!I:>P Jo
oq PInoN. SJu:>wJsnfpt/ :>WO:>U!
.s:>wo:>Jno qJIt/:>q OJ s:>:>mOS:>l ){U!I O} Alt/SS:>:>:>U
l:>JJ:>q put/ 'S:>!J!loqJnt/
:>Jt/:>°llt/ OJ p:>p:>:>u :>q PInoN. SWS!ut/q:>:>w
:>q OJ :>At/q PInoN.
AIOJUln8:>1
N.:>U ':>Idwt/x:>
UO!J!SUt/1J :>qJ '){10N.:>Wt/1J
8u!Js!x:>
It/Uo!8:>1 OJ spunJ
It/qOl8
1011 .P:>UUt/ld AllnJ:>lt/:>
:>qJ AJ!POW 10 I:>POW
N.:>u t/ Jdopt/ OJ :>p!:>:>p SJUOWU1:>AO8 1t/!:>U!AOld pUt/ It/l:>P:>J :>qJ JI
sz"SwaJSAS alt/;) l{JTt/al{ a;)rnos-a['Bu!s'parnsu!
A[:>







© Copyright 2026