
Cardiac
Cardiac • 12-Lead ECG acquisition • Cardiac monitoring • Coronary artery reperfusion • Synchronised cardioversion • Transcutaneous cardiac pacing • Valsalva manoeuvre Clinical Practice Procedures – Cardiac Clinical practice procedures 12-Lead ECG acquisition Version 1.0 – September 2011 Authorisation to practice 12-Lead ECG acquistion The 12-lead electrocardiogram (ECG) is used to detect many conditions affecting the heart, underlying myocardial ischaemia, dysrrhythmias, drug toxicity and electrolyte imbalances. Use in the pre-hospital setting is paramount to the diagnosis and treatment of STEMI, (via the QAS cardiac reperfusion strategy). Additional information • The 12-Lead ECG should be acquired as part of an early secondary assessment of the patient, especially in the setting of suspected cardiac ischaemia or infarct. • Electrodes should remain in their original placement throughout management to facilitate the comparison of serial 12-Lead ECGs. Note: Similar complications as with cardiac monitoring, also ensuring that: • ECG frequency is set at 0.05 – 40 Hz, and • paper speed is set at 25 mm/sec These factors ensure the 12-Lead ECG printout is of diagnostic quality.[1] Page 1 of 2 Indications • To aid in the identification of: -- myocardial ischaemia or infarct -- rhythm and conduction disturbance -- electrolyte imbalance -- hypertrophy of the heart -- drug toxicity Contraindications • Nil in this setting Precautions • Nil in this setting Procedure • Explain to the patient what is required, ensure privacy and obtain consent to place electrodes. • Position the patient preferably supine or semi-recumbent, (without arms or legs crossed). • Attach electrodes to the snap connectors on each wire, ensuring electrodes are in date and gel is still moist. • Accurately position the electrodes on the patient: [2] -- Limb electrodes -- Limb leads can be placed on the distal location of the inner wrists and the medial aspect of the ankles. -- If required, electrodes may be placed more proximally along the limbs to reduce electrical and mechanic artefact. -- Chest electrodes -- Refer to table opposite. Procedure (continued) PLACEMENT OF ECG CHEST ELECTRODES Placement order Chest lead 1st V1 Anatomical position 4th Intercostal space, right of the sternum 2nd V2 4th Intercostal space, left of the sternum 3rd V4 5th Intercostal space, on left midclavicular line 4th V6 On the left mid-axillary line, level with V5 5th V3 Midway between V3 and V4 6th V5 Midway between V4 and V6 Optional * V4R 5th Intercostal space, on the right midclavicular line * For evaluation of right ventricular involvement with inferior STEMI, consider acquiring a 12-Lead ECG with V4 repositioned to V4R.[3] If V4R is acquired, the 12-Lead ECG must be annotated to indicate that V4 is now representing V4R. • Ask the patient to breathe normally and to remain still, without talking. • Commence 12-Lead ECG acquisition as per specific manufacturer’s instructions.[1] Angle of Louis 1 2 3 4 5 6 12-Lead electrode placement 12-Lead ECG acquisition – Page 2 of 2 Clinical practice procedures Cardiac monitoring Version 1.0 – September 2011 Authorisation to practice Cardiac monitoring Continuous cardiac monitoring records the electrical activity of the heart as an electrocardiogram (ECG) either on the cardiac monitor screen or via a paper print out. Page 1 of 2 Contraindications • Nil in this setting Precautions Be aware of potential artefacts in the ECG from: [1] Cardiac monitoring is indicated for identification of potentially lethal dysrrhythmias. • Detached electrodes due to diaphoresis, oily skin, or chest hair ST segment analysis via the monitor screen is non-diagnostic. • Patient movement, breathing, muscle tremor or lead movement Note: The VF/VT alarm should always be turned on. Indications Cardiac monitoring is essential in the following patients’ groups, though not limited to: • All unconscious patients or collapse patients (or those who have recently been unconscious) • Patients complaining of chest pain or dyspnoea • Poisoned patients • Patients who are poorly perfused/shocked or hypoxic, or with abnormal vital signs • When a medical officer requests the patient to be monitored • Patients in cardiac arrest are also to bemonitored but this is done through the defibrillation pads in anticipation of a shockable rhythm. • AC electricity/50 hertz interference • Broken cable tip, wire or machine malfunction • Dry electrode conductive gel Note: If the patient goes into cardiac arrest, any electrodes impeding the proper application of the defibrillator pads must be removed. Procedure • Explain procedure to patient and ensure privacy where possible. • Clean the surface of the skin to ensure monitoring electrodes will adhere. • It may also be necessary to: -- Shave chest hair if necessary. -- Inspect the monitoring electrode pad to ensure that the surface is going to adhere and the gel in the centre of the pad is moist. RA/R LA/L • Attach the leads to the monitoring electrode pads. • Smooth electrode pads on from one edge. The leads primarily used in continuous cardiac monitoring are those referred to as ‘limb leads’, identified as follows: [2] • • • • RA = right arm LA = left arm RL = right leg LL = left leg RL/N LL/F The monitoring electrodes for these leads are generally placed distally on the limbs, but to limit motion artefact they can be applied as follows: [2] • RA & LA placed proximally on arms, but not on torso. Placement of limb lead monitoring electrodes • RL & LL placed proximally, but not higher than iliac crests. Cardiac monitoring – Page 2 of 2 Clinical practice procedures Coronary artery reperfusion Version 1.2 – June 2012 Authorisation to practice Coronary artery reperfusion Reperfusion therapy consists of fibrinolysis ( pre-hospital or hospital based ) or primary percutaneous coronary intervention (pPCI). This CPP outlines the following: • Requirements for triaging patients with acute ST elevation myocardial infarction (STEMI) for either pre-hospital or hospital fibrinolysis or pPCI • Assessment of patients meeting pre-hospital fibrinolysis and anticoagulation triage criteria • Administration of pre-hospital fibrinolysis and anticoagulation therapy • Documentation for reporting patients with STEMI • Audit and quality assurance requirements for patients with STEMI The choice of reperfusion therapy will depend on a number of factors, including: • Time from the onset of symptoms • Time of assessment and STEMI diagnosis by QAS paramedics • Availability of pPCI and time to balloon inflation • Time to hospital fibrinolysis • Contraindications to pPCI or fibrinolytic therapy • Consent to pre-hospital fibrinolysis and anticoagulation The purpose of reperfusion is to restore blood flow through a partially or fully obstructed coronary artery as early as possible in an attempt to minimise the extent and duration of myocardial ischaemia. Page 1 of 12 Indications Reperfusion is to be considered for all patients with classic ongoing ischaemic chest pain (atypical ischaemic chest pain is excluded) and ECG criteria indicating STEMI, as demonstrated on a 12-Lead ECG. ECG criteria are: • Persistent ST-segment elevation of ≥ 1 mm in two contiguous limb leads AND/OR ST-segment elevation of ≥ 2 mm in two contiguous chest leads (V1 – V6 ). • Normal QRS width (< 0.12 seconds) OR right bundle branch block (RBBB) identified on the 12-Lead ECG. Increased scrutiny and threshold must be applied to patients < 35 years due to the higher likelihood of STEMI mimics in this age group such as pericarditis. Paramedics should exercise extreme caution and demonstrate a low threshold for waiting to gain a second opinion at the receiving emergency department. If doubt exists regarding the diagnosis of STEMI, the QAS paramedic is not to administer reperfusion therapy. Contraindications Pre-hospital fibrinolysis is contraindicated in the following situations: • Ongoing ischaemic chest pain ≥ 6 hours duration • Patient is ≥ 75 years • Systolic BP ≥ 180 mmHg (at any stage during current acute episode. • Diastolic BP ≥ 110 mmHg (at any stage during current acute episode) • GCS < 15 • Known allergy to tenecteplase, enoxaparin/heparin and/or clopidogrel (as appropriate) • Left BBB identified on 12-Lead ECG • Current or history of thrombocytopenia • Active tuberculosis • Known structural nervous system disease, in particular a malignant intracranial neoplasm (primary or metastatic) • Known structural cerebral vascular lesion (e.g. arteriovenous malformation) • Prior intracranial haemorrhage • Ischaemic stroke or TIA within last three months • Acute myocardial infarction in the setting of acute trauma • History of significant closed head or facial trauma within last three months • Suspected aortic dissection (including new neurological symptoms) • History of major trauma or surgery (including laser eye surgery) within last six weeks • Internal bleeding (e.g. gastrointestinal (GI) or urinary tract bleed) within last four weeks Contraindications (continued) • Active bleeding or bleeding disorder e.g. haemophilia (excluding menses) • Current use of anticoagulants (e.g. warfarin or dabigatran (Pradaxa® ) – excludes antiplatelet medications e.g. aspirin AND/OR clopidogrel) • Non-compressible vascular punctures • Active peptic ulcers, as evidenced by recent malaena within last six weeks, or active ongoing symptoms prior to current cardiac event • Prolonged (> 10 minutes) CPR. • Known pregnancy or delivered within the last two weeks • History of serious systemic disease (advanced/ terminal cancer, severe liver or kidney disease) • Resident of an aged care facility requiring significant assistance with activities of daily living and/or GCS < 15 Special notes: • All STEMI patients who are contraindicated for QAS pre-hospital fibrinolysis and who are located within a primary pPCI catchment area are to be referred for pPCI in accordance with the appropriate local work instruction (LWI), except residents of an aged care facility requiring significant assistance with activities of daily living and/or GCS < 15. • In patients with cardiogenic shock associated with STEMI, there is a clear mortality benefit for pPCI over fibrinolysis.[1] These patients should be discussed with the receiving hospital in accordance with the LWI. Complications • Haemorrhage Coronary artery reperfusion – Page 2 of 12 Clinical practice procedures Coronary artery reperfusion Version 1.2 – June 2012 Procedure Advice • All patients who are candidates for both pre-hospital fibrinolysis or pPCI must be provided with advice regarding the possible side effects and risks associated with enoxaparin/heparin, tenecteplase and clopidogrel (as appropriate) administration. Consent Clinicians are to: • Read the consent section of the ‘Reperfusion checklist’ to the patient. • If the patient consents to enoxaparin/heparin, tenecteplase and clopidogrel (as appropriate) administration, ensure the patient signs the consent section of the ‘QAS Reperfusion checklist’. Recording advice, consent and contraindications Clinicians MUST record the following information on the eARF: • The advice that was provided to the patient. • Any known contraindication to enoxaparin/heparin, tenecteplase and clopidogrel (as appropriate). • That there were no contraindications present when enoxaparin/heparin, tenecteplase and clopidogrel (as appropriate) were adminisered. • If the patient has consented, or refused enoxaparin/ heparin, tenecteplase and clopidogrel (as appropriate) administration. Page 3 of 12 Procedure (continued) Drug therapy • Whenever possible, the ACF should be avoided when gaining IV access as this may be inaccessible during angiography. • If a patient is to be transported directly to a pPCI centre then administer the following medications after aspirin and other standard cares: -- heparin in accordance with the QAS DTP and -- clopidogrel in accordance with the QAS DTP • If the patient meets the criteria for pre-hospital fibrinolysis then administer the following medications after aspirin and standard cares: -- enoxaparin in accordance with the QAS DTP; and -- tenecteplase in accordance with the QAS DTP; and -- clopidogrel in accordance with the QAS DTP. Transport • Patients must be regularly reassessed and transported to the bedside with continuous comprehensive monitoring. All ongoing treatment must be in accordance with the appropriate CPG. • Where possible all thrombolysed patients should be transported to the closest PCI capable facility, not a Regional Hospital – as the ability to have a rescue PCI or timely adjuvant PCI < 24 hours is required to optimise patient outcomes. Treatment of dysrrhythmias post fibrinolysis • It is not uncommon to have dysrrhythmias post-fibrinolysis.[2] Dysrrhythmias should be managed according to their relevant CPGs. Procedure (continued) pPCI • LWIs in areas with rapid access to pPCI will direct patients to this mode of therapy in the first instance. • This assumes rapid notification and balloon opening time of less than 90 minutes from activation of the process. This recognises that pPCI is of benefit if performed within 60 minutes of potential fibrinolysis (assuming maximum of 30 minutes to diagnose and treat from first patient contact).[3] Procedure (continued) -- Complete the ‘STEMI reperfusion capture form’ and attach a copy of the 12-Lead ECG, ‘Reperfusion checklist’ and if appropriate, the Death & Cardiac Arrest Report Form (DCARF). -- Forward the documentation package directly to the Australian Centre for Pre-hospital Research. Note: All cases are to be reviewed by the Medical Director. Local work instruction • LWIs have been developed outlining the local practices for providing early reperfusion, including, but not limited to: -- Contraindications, accessing and availability of pPCI -- The system for pre-alerting medical facilities Audit • All STEMIs are to be reported to the QAS on-call medical officer (24/7). Cases after 12 midnight can be telephones through the next morning if there were no complications. • All cases of suspected Acute Myocardial Infartion attended by the ICP where a 12-Lead ECG is acquired (whether treated with fibrinolysis/referred for pPCI or not) are subject to clinical review through the following process: -- Select final assessment as ‘Acute Myocardial Infarction’ and complete the eARF in accordance with current standards. Coronary artery reperfusion – Page 4 of 12 Clinical practice procedures Coronary artery reperfusion Version 1.2 – June 2012 Page 5 of 12 Additional information Fibrinolysis Patient meets fibrinolysis criteria pPCI Patient meets PCI criteria according to Local Work Instruction Notify hospital of potential pPCI candidate Consent given for enoxaparin and tenecleplase and consent form signed by patient Consent given for heparin and clopidogrel and consent form signed by patient Assuming standard cares given Assuming standard cares given Enoxaparin 30 mg IV Tenecteplase Clopidogrel 300mg Heparin 5000 units IV Clopidogrel 600 mg Enoxaparin 1 mg/kg (up to max 100 mg) subcut at 15 min post initial dose Pre-notify as appropriate Code 2 transport unless altered vital signs Code 1 transport to hospital QAS Coronary Artery Reperfusion Check List QAS Coronary Artery Reperfusion Check List (back of form) PATIENT DETAILS Patient Surname Age CONSENT Given Name Date All patients eligible for reperfusion MUST read the following and, if consent is given, the patient must sign the bottom section of this form. Incident Number INDICATIONS – if the answer is NO or UNSURE to ANY of the following, do NOT administer any reperfusion drugs Yes No Unsure Ongoing ischaemic chest pain < 6 hours duration? 12-Lead ECG with persistent ST- elevation ≥ 1mm in at least two contiguous limb leads AND/OR ≥ 2mm in two contiguous chest leads V1 – V6? Normal QRS width (< 0.12 seconds) OR right bundle branch block? Patient is < 75 years of age? Systolic BP < 180 (at all times during current acute episode)? Diastolic BP < 110 (at all times during current acute episode)? GCS = 15? CONTRA-INDICATIONS – if the answer is YES or UNSURE to ANY of the following questions, do NOT administer any reperfusion drugs Known allergy to Tenecteplase, Enoxaparin / Heparin or Clopidogrel (as appropriate)? Left BBB identified on 12-Lead ECG? Current or history of thrombocytopenia? Active tuberculosis? Known structural nervous system disease, in particular a malignant intracranial neoplasm (primary or metastatic)? Known structural cerebral vascular lesion (e.g. arteriovenous malformation)? Prior intracranial haemorrhage? Ischaemic stroke of TIA within last 3 months? History of significant closed head / facial trauma within last 3 months? Suspected aortic dissection (including new neurological symptoms)? History of major trauma or surgery (including laser eye surgery) within last 6 weeks? Internal bleeding (e.g. GI / urinary tract bleed) within last 4 weeks? Active bleeding or clotting problem (haemophilia etc), excluding menses? Current use of anticoagulants (e.g. warfarin or dabigatran (Pradaxa® ) – excludes antiplatelet medications e.g. aspirin AND/OR clopidogrel)? Non-compressible vascular punctures? Active peptic ulcer, as evidenced by recent melaena within last 6 weeks, or active ongoing symptoms prior to this cardic event? Prolonged (>10 minutes) CPR? Known to be pregnant or delivered within last 2 weeks? It is likely that you are suffering a heart attack, and your treatment options include: (choose one of the following as appropriate) • a drug which reduces new clot formation called ENOXAPARIN; and a clot dissolving drug called TENECTEPLASE; and a drug call CLOPIDOGREL which will assist in preventing further clot formation. (cross out if not applicable) OR • a drug which reduces new clot formation called HEPARIN; and a drug called CLOPIDORGEL which will assist in keeping a stent open should a cardiologist perform this procedure at hospital. (cross out if not applicable) Yes No Unsure The sooner you receive these drugs, the lower the risk from the heart attack – which is why it is recommended that the treatment is started as soon as possible. These drugs can cause serious side affects in a small number of patients but the risks attached to this treatment are much less then the likely benefit. I will now give you more details. (choose the appropriate paragraph) Enoxaparin/Tenecteplase/Clopidogrel therapy: Treatment at this stage improved the chances or survival by 20 – 25% but it can sometimes cause serious bleeding. The biggest risk is potentially life-threatening stroke which affects about 1 patient in every 100. Other significant bleeding which is not normally life-threatening can occur in about 4 in 100 patients. Some patients also have allergic reactions and other side effects that do not usually cause any major problem. Heparin/Clopidogrel therapy: Heparin and Clopidogrel can cause life threatening bleeding, albeit the risk is very small. The administration of these drugs in this setting has been recommended by national and international cardiology bodies. Medical Records: I give permission for the QAS to access my hospital record for information relating to this procedure. Patient signature X ....................................................................................................... PARAMEDIC DETAILS I certified that I have completed and read the QAS Coronary Artery Reperfusion Check List and the patient has given / has not given consent for the administration of the approved drugs. (circle appropriate response) Number Signature History of serious systemic disease (e.g. advanced / terminal cancer, severe liver or kidney disease)? Resident of an aged care facility requiring significant assistance with activities of daily living and/or GCS < 15? Acute myocardial infarction in the setting of acute trauma? Coronary artery reperfusion – Page 6 of 12 Clinical practice procedures Coronary artery reperfusion Version 1.2 – June 2012 Page 7 of 12 -Local Work Instruction – Far Northern Region Introduction This LWI sets out the procedure for triaging patients with acute ST elevation myocardial infarction (STEMI) for Far Northern QAS region. All public patients with acute STEMIs are to be transported to the closest appropriate public hospital. Private patients with acute STEMI are to be treated in accordance with this LWI, however may be considered for referral to Cairns Private Hospital (Monday to Friday 0800 – 1600 hrs) following pre-hospital fibrinolysis. Procedure ALL ACUTE STEMIs (cont.) AFTER HOURS AND WEEKENDS Patient contraindicated for pre-hospital fibrinolysis OUT OF HOSPITAL CARDIAC ARREST WITH ROSC ALL ACUTE STEMIs MONDAY – FRIDAY 0800 – 1600 hrs Patient indicated for pre-hospital fibrinolysis AFTER HOURS AND WEEKENDS Patient indicated for pre-hospital fibrinolysis MONDAY – FRIDAY 0800 – 1600 hrs Patient contraindicated for pre-hospital fibrinolysis Public & Private patient Withhold fibrinolysis and transport Code 1 to the closest appropriate public emergency department. Public & Private patient GCS 15 Administer pre-hospital fibrinolysis and transport to the closest appropriate public emergency department. GCS < 15 Transport Code 1 to the closest appropriate public emergency department. Public patient Administer pre-hospital fibrinolysis and transport to the closest appropriate public emergency department. Private patient Administer pre-hospital fibrinolysis and consider referral to the Cairns Private Hospital Rapid Cardiac Assessment Centre 1300 264 462. • Minimise on-scene delays. • Treat patient in accordance with appropriate CPG. Public & Private patient Administer pre-hospital fibrinolysis and transport to the closest appropriate public emergency department. • The ICP is to make all notifications. At Cairns Private Hospital notification is to be with the Cardiologist (who is then responsible for all subsequent notifications). At all other hospitals the ICP will notify the Emergency Department. Public patient Private patient Withhold fibrinolysis and transport Code 1 to the closest appropriate public emergency department. Withhold fibrinolysis and consider referral to the Cairns Private Hospital Rapid Cardiac Assessment Centre 1300 264 462. All other cases Transport to closest appropriate emergency department. • For patients accepted for admission at Cairns Private Hospital, the crew are to take the patient direct to the Coronary Care Unit. Forall other hospitals the patient will be received into the Emergency Department. • The receiving hospital should be notified of all relevant clinical information as per normal communication procedures. Local Work Instruction – Northern, Central & South Western Regions Introduction This LWI sets out the procedure for triaging patients with acute ST elevation myocardial infarction (STEMI) in the Northern, Central & South Western regions. Currently primary percutaneous coronary intervention (pPCI) for acute STEMIs is not available outside of the Brisbane and South Eastern QAS regions. The QAS continues to negotiate with major public hospitals and private institutions regarding the availability of pPCI in the future. Local work instructions will be released when these services become available. Procedure ALL ACUTE STEMIs THAT MEET QAS REPERFUSION CRITERIA MONDAY – SUNDAY 24 hrs Administer pre-hospital fibrinolysis and transport to the closest appropriate emergency department. OUT OF HOSPITAL CARDIAC ARREST WITH ROSC GCS 15 Follow criteria above. GCS < 15 Transport to the closest appropriate emergency department. All other cases Transport to the closest appropriate emergency department. • Minimise delays on-scene. • Treat patient in accordance with appropriate CPG. • The receiving hospital should be notified of all relevant clinical information as per normal communication procedures. Coronary artery reperfusion – Page 8 of 12 Clinical practice procedures Coronary artery reperfusion Version 1.2 – June 2012 Page 9 of 12 Local Work Instruction – North Coast Region Procedure – Sunshine Coast Area Introduction ALL ACUTE STEMIs This LWI sets out the procedure for triaging patients with acute ST elevation myocardial infarction (STEMI) in the North Coast region. Patients indicated for QAS pre-hospital fibrinolysis Administer pre-hospital fibrinolysis and transport to the closest appropriate emergency department. Ensure notification of the Clinical Deployment Supervisor (CDS) OR Communication Centre Supervisor (CCS) who will notify the Queensland Coordination Centre (QCC) to initiate emergent transfer to a Brisbane PCI centre. Patients contraindicated for QAS pre-hospital fibrinolysis and not a resident of a care facility (ie. requiring assistance with activities of daily cares) Transport to the closest appropriate emergency department. Ensure notification of the Clinical Deployment Supervisor (CDS) OR Communication Centre Supervisor (CCS) who will notify the Queensland Coordination Centre (QCC) to initiate emergent transfer to a Brisbane PCI centre. OUT OF HOSPITAL CARDIAC ARREST WITH ROSC GCS 15 Follow criteria above. GCS < 15 Transport to the closest appropriate emergency department. Ensure notification of the Clinical Deployment Supervisor (CDS) OR Communication Centre Supervisor (CCS) who will notify the Queensland Coordination Centre (QCC) to initiate emergent transfer to a Brisbane PCI centre. All other cases Transport to the closest appropriate emergency department. Currently primary percutaneous coronary intervention (pPCI) for acute STEMIs is not available outside of the Brisbane and South Eastern QAS region. The potential for direct transfer to private hospitals either post fibrinolysis or for pPCI is currently being negotiated. Until a finalised work instruction, paramedic should take all patients with an acute STEMI to the closest public hospital following the listed procedure. Procedure – Wide Bay and Cooloola Burnett Areas ALL ACUTE STEMIs THAT MEET QAS REPERFUSION CRITERIA Patient indicated for QAS pre-hospital fibrinolysis Administer pre-hospital fibrinolysis and transport to the closest appropriate emergency department. OUT OF HOSPITAL CARDIAC ARREST WITH ROSC GCS 15 Follow criteria above. GCS < 15 Transport to closest appropriate emergency department. All other cases Transport to the closest appropriate emergency department. • Minimise delays on-scene. • Treat patient in accordance with appropriate CPG. • The receiving hospital should be notified of all relevant clinical information as per normal communication procedures. • Minimise delays on-scene. • Treat patient in accordance with appropriate CPG. • The receiving hospital should be notified of all relevant clinical information as per normal communication procedures. Local Work Instruction Brisbane & South Eastern Regions This LWI sets out the procedure for triaging patients with acute ST elevation myocardial infarction (STEMI) to primary Percutaneous Coronary Intervention (pPCI) for the Brisbane & South Eastern QAS regions. All public patients with STEMI that meet the QAS reperfusion criteria are now to be transported to the closest appropriate public hospital pPCI facility. Private patients with acute STEMIs are to be transported in accordance with the LWI, but every attempt should be made to refer the patient to the private hospital of their choice that has 24/7 pPCI capability. These include: • St Andrew’s Hospital (Brisbane); • Wesley Hospital; • Mater Private Hospital; • Greenslopes Private Hospital; • Holy Spirit Northside Hospital; • Allamanda Private Hospital; • Pindara Private Hospital; or • John Flynn Private Hospital. The private hospitals have no fixed geographical boundaries, but time to reperfusion must be a priority. Therefore, the closest private pPCI capable facility should be chosen where possible. Furthermore, private patients should be transported to the hospital of their treating cardiologist where possible. Procedure ALL ACUTE STEMIs MONDAY – SUNDAY 24 hrs Patient indicated for pre-hospital fibrinolysis/ pPCI referal MONDAY – SUNDAY 24 hrs Patient contraindicated for QAS pre-hospital fibrinolysis/pPCI referral however NOT a resident of an aged care facility requiring significant assistance with daily living and/or GCS < 15 OUT OF HOSPITAL CARDIAC ARREST WITH ROSC Call appropriate interventional cardiologist OR hospital emergency department specialist (dependant on receiving hospital preference) to determine reperfusion therapy of choice. Call appropriate interventional cardiologist OR hospital emergency department specialist (dependant on receiving hospital preference) to determine if patient is suitable for reperfusion therapy. GCS 15 Follow criteria above. GCS < 15 Call hospital agreed contact to activate PCI lab and transport Code 1 to pPCI centre. Coronary artery reperfusion – Page 10 of 12 Clinical practice procedures Version 1.2 – June 2012 ALL ACUTE STEMIs (cont.) • Minimise delays on-scene. • Treat patient in accordance with appropriate CPG. • The ICP is to make all notifications via the appropriate phone number (see next page). At the Princess Alexandra Hospital (PAH) and The Prince Charles Hospital (TPCH) notification is to be with the interventional cardiologist (who is then responsible for the subsequent notifications to the emergency department). At all other hospitals the ICP will make notification to the emergency department. • When calling, the following narrative should be used: “I am an Intensive Care Paramedic with the QAS. We have a STEMI at [suburb], the estimated transport time to your hospital is [minutes], is the cath lab available for emergency Primary PCI?” • The doctor will advise whether the patient should be transported immediately for pPCI. • For patients triaged to pPCI at RBWH, PAH, TPCH & GCH, the crew will be met at the emergency department and directed to the catheter laboratory. For all other hospitals the patient will be received into the emergency department until the catheter laboratory is available. Coronary artery reperfusion Page 11 of 12 EMERGENCY CONTACT NUMBERS (not to be disclosed to patients/public) PUBLIC HOSPITALS NOTIFICATION PREFERENCES PHONE NUMBERS Princess Alexandra Interventional Cardiologist 1800 450 468 Royal Brisbane & Women’s Interventional Cardiologist 3646 3434 The Prince Charles Interventional Cardiologist 3139 4004 Gold Coast Interventional Cardiologist 0478 324 861 PRIVATE HOSPITALS NOTIFICATION PREFERENCE PHONE NUMBERS Allamanda ED Senior Medical Officer 5591 9488 (reperfusion cases only) Greenslopes ED Senior Medical Officer 3397 8617 Holy Spirit Northside ED Senior Medical Officer 3326 3303 John Flynn ED Senior Medical Officer 5598 9005 Mater Adults ED Senior Medical Officer 3163 1030 Pindara ED Senior Medical Officer 5588 9000 St Andrew’s ED Senior Medical Officer 3832 7344 Wesley ED Senior Medical Officer 3232 7961 Additional information • If there is a clinical concern regarding the mangement advice given by the cardiology service, please call the QAS on-call medical officer immediately to clarify the issue. Coronary artery reperfusion – Page 12 of 12 Clinical practice procedures Synchronised cardioversion Version 1.0 – September 2011 Authorisation to practice Synchronised cardioversion Synchronised cardioversion is a method of restoring the normal rhythm of the heart in patients presenting with a rapid ventricular rate associated with severely compromised cardiac output (i.e. GCS is < 15, SBP < 90 mmHg, chest pain, heart failure). This is achieved using a purpose modified defibrillator capable of delivering a controlled direct current shock, synchronised with the R-wave of the ECG. [1] Synchronised DC shock * Up to three attempts Page 1 of 2 Indications Rapid ventricular rate with severely compromised cardiac output, in the following cardiac rhythms: [2] • Pulsatile ventricular tachycardia • Supra-ventricular tachycardia • Atrial fibrillation • Atrial flutter CAUTION: Cardioversion of SVT including Atrial Fibrillation and Atrial Flutter is rarely required in the pre-hospital seting. Contraindications • VF/pulseless VT • Dysrrhythmias where the patient is adequately perfused Complications • Pain and discomfort • Paradoxical asystole or VF Procedure • Explain the procedure to the patient. • Establish IV access with a sodium chloride 0.9% running line. • Ensure resuscitative drugs are available. • Prepare airway, suction and ventilation equipment. • Consider sedation as per Sedation CPG. • Position electrodes and pads as appropriate. • Ensure that the synchroniser is on. • Confirm synchronisation is occurring on the R wave. Change the ECG amplitude on the monitor if necessary. • Ensure the patient is well oxygenated/ventilated prior to and after sedation and cardioversion. • Perform a maximum of three attempted synchronised cardioversions in accordance with the following joule sequence: 100 : 150 : 200 joules • Press and hold the shock button until the synchronised shock is delivered. • Assess the patient following each cardioversion attempt. • Ensure the synchroniser button is pressed again before each shock is delivered. Additional information • If synchronised cardioversion produces VF/Asystole then immediately treat as per guidelines. • Always consider other possible causes of the tachyarrhythmia such as hypovolaemia. • Should synchronised cardioversion be unsuccessful, confirm monitoring electrodes and pads are appropriately placed, ensure the synchroniser is on and the R wave is being sensed, and consider alternative pad placement. Note: The requirement for pre-hospital synchronised cardioversion in the paediatric patient is extremely rare. Should it be deemed as necessary, consultation with the on-call QAS Medical Officer is required in all circumstances with a recommended sequence at 0.5 – 1 joule/kg increasing to 2 joules/kg if required. Synchronised cardioversion – Page 2 of 2 Clinical practice procedures Transcutaneous cardiac pacing Version 1.0 – September 2011 Authorisation to practice Transcutaneous cardiac pacing Transcutaneous cardiac pacing (TCP) works as an artificial pacemaker, delivering repetitive electrical currents when the natural pacemaker has become blocked or dysfunctional. TCP is often beneficial for patients with haemodynamically unstable bradycardia, especially if the patient is unresponsive to Atropine. [1] To have effect, the myocardium must be capable of generating cardiac output with the muscular contractions. There are two modes of TCP: [2] • demand pacing and • non-demand/asynchronous pacing Demand pacing is designed to sense the inherent QRS complex, delivering electrical stimuli only when needed. Note: Non-demand/asynchronous pacing is not indicated within QAS. Page 1 of 2 Indications Poor perfusion resulting from significant: • bradycardia • heart block Contraindications TCP is contraindicated within the QAS for: • asystole/PEA • overdrive pacing of a ventricular dysrrhythmia. Complications • Pain • Discomfort • Anxiety Procedure • Explain the procedure to the patient (cutaneous nerve stimulation and/or skeletal muscle contraction). • Establish IV access with a sodium chloride 0.9% running line. • Ensure adequate oxygenation and ventilation and basic cares are completed. • Consider sedation and/or analgesia as per the Sedation and procedural sedation and Pain management CPG. • Position electrodes and pads as appropriate. • Turn pacer on and select appropriate rate (60 – 80 in adults: rates > 90 may be associated with worsening myocardial perfusion). Additional information Patients in cardiac arrest do not respond to pacing because the heart is metabolically compromised from inadequate perfusion and is therefore incapable of effective contractions. There is no evidence to support routine pacing in cardiac arrest as there is no improved return of spontaneous circulation or survival.[1] Capture is defined as depolarisation of the heart by an artificial electrical stimulus: • Electrical capture is evidenced by a wide QRS complex followed by a tall, broad T wave. • Mechanical capture is myocardial contraction and is evidenced by a pulse and signs of improved cardiac output. The most common reason for failing to achieve capture is insufficient current.[2] Additional reasons to consider are; • Increase current incrementally, while observing the patient and assessing for electrical and mechanical capture; this may change over time. • The cause of the natural pacemaker failure and whether the myocardium is capable of contractions (e.g. Hypoxia and acidosis impairs cardiac contractility). • The minimum current effective to obtain reliable mechanical capture should be used to minimise heart damage and patient discomfort. • Adequate sensing of demand pacemaker by ensuring ECG trace is properly sized • If the patient becomes intolerant of the procedure, consider further analgesia/sedation. • Alternative pad placement (anterior/posterior), pad adherence and machine and lead check Transcutaneous cardiac pacing – Page 2 of 2 Clinical practice procedures Valsalva manoeuvre Version 1.0 – September 2011 Authorisation to practice Valsalva manoeuvre The Valsalva manoeuvre is a first line treatment for the management of haemodynamically stable, narrow complex SVT. The Valsalva manoeuvre has four phases: [1] Phase one: onset of strain brings about an increase in intrathoracic pressure. This has a compressive effect on the aorta, resulting in a transient increase in aortic pressure. Phase two: the end of this transient period, which results in decreasing aortic pressure and increasing heart rate Phase three: release of the strain leading to sudden pressure drop within the aorta with a resultant compensatory increase in heart rate Phase four: increased venous return, preload and therefore cardiac output results in an increased aortic pressure with compensatory ‘overshoot’ of blood pressure, leading to a reflex bradycardia This reflex bradycardia is induced in an effort to break the pattern of a re-entrant circuit causing the SVT. A maximum of three attempts at the Valsalva manoeuvre is recommended. Page 1 of 2 Indications • Haemodynamically stable SVT Contraindications • Haemodynamic compromise Complications • Syncope • Prolonged hypotensive state Procedure • Ensure all standard cares have been performed. • Explain the procedure to the patient. • Obtain IV access with a one litre bag of sodium chloride 0.9% attached. Additional information • Evidence suggests the following ‘gold standard’ criteria for the Valsalva manoeuvre technique: [2] -- minimum pressure of 40 mmHg -- optimal duration of 15 seconds -- supine position as an ideal posture • Position the patient supine. • Instruct the patient to blow into a sterile 10 mL syringe for 15 seconds, aiming to move the plunger up the barrel of the syringe. • Print the ECG, indicating the start of the maneouvre. • After 15 seconds, stop the procedure and retrieve the syringe from the patient. • Indicate the end of the manoeuvre on the ECG print out and continue the print out until the ECG has stabilised. • Ensure the patient has returned to a haemodynamically stable SVT presentation prior to repeating the procedure. Valsalva manoeuvre – Page 2 of 2







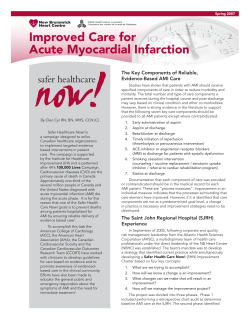




© Copyright 2026