
Document 10948
FREE NEJM E-TOC
COLLECTIONS
HOME
| SUBSCRIBE | CURRENT ISSUE | PAST ISSUES |
| Search Term
Keyw ord, citation, or autho SEARCH
Advanced Search
Free Full Text for: Colombia | Get NEJM's E-Mail Table of Contents - FREE | Sign In as an Individual
Previous
Volume 344:38-47
January 4, 2001
Number 1
Misoprostol and Pregnancy
Alisa B. Goldberg, M.D., Mara B. Greenberg, B.S.,
and Philip D. Darney, M.D.
PDF
Editorial
by Hale, R. W.
Next
Misoprostol is a prostaglandin E1 analogue that has been
approved by the Food and Drug Administration (FDA)
to be taken orally for the prevention and treatment of
Add to Personal Archive
gastric ulcers associated with the use of nonsteroidal
antiinflammatory drugs. It has also become an important
Add to Citation Manager
drug in obstetrical and gynecologic practice because of
its uterotonic and cervical-ripening actions. Misoprostol
Notify a Friend
is useful for elective medical abortion, cervical ripening
before surgical abortion, evacuation of the uterus in
E-mail When Cited
cases of embryonic or fetal death, and induction of
labor. The drug may also be used to treat and even
prevent postpartum hemorrhage. However, misoprostol
is not approved for any of these indications in the
United States. Current product labeling includes a
warning that misoprostol is contraindicated during
pregnancy because of its abortifacient properties.
However, the FDA recognizes that, in certain
PubMed Citation
circumstances, off-label uses of approved products are
appropriate, rational, and accepted medical practice.1
Prescribing a medication for an off-label indication is
common in the treatment of pregnant women and is not considered experimental if
based on sound scientific evidence.2
The purpose of this article is to review the large body of evidence supporting the use of
misoprostol in pregnancy. We review the pharmacokinetics, mechanism of action,
dosage, efficacy, and safety of misoprostol in pregnant women; we also use the scheme
of the U.S. Preventive Services Task Force to grade the strength of our
recommendations.3
Pharmacokinetics, Physiology, and Teratogenicity
Misoprostol is manufactured as an oral preparation in 100-µg unscored and 200-µg
scored tablets. After oral administration, misoprostol is rapidly absorbed and converted
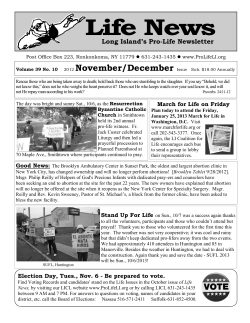
to its pharmacologically active metabolite, misoprostol acid. Plasma concentrations of
misoprostol acid peak in approximately 30 minutes and decline rapidly thereafter
(Figure 1).4 The bioavailability of misoprostol is decreased by concomitant ingestion of
food or antacids. Misoprostol is primarily metabolized in the liver, and less than 1
percent of its active metabolite is excreted in urine.5 Patients with hepatic disease should
receive a decreased dose, whereas dose adjustment is unnecessary for patients with renal
insufficiency who do not require dialysis.5 Misoprostol has no known drug interactions
and does not induce the hepatic cytochrome P-450 enzyme system.
Figure 1. Mean (±SD) Plasma Concentrations of Misoprostol Acid
after Oral or Vaginal Administration of Misoprostol in 20 Women.
View larger version
(13K):
There were 10 women (5 nonpregnant and 5 pregnant) in each
group. Reprinted from Zieman et al.4 with the permission of the
publisher.
[in this window]
[in a new window]
The most common adverse effects of misoprostol are nausea, vomiting, diarrhea,
abdominal pain, chills, shivering, and fever, all of which are dose-dependent. Although
other prostaglandins (prostaglandin E2 and prostaglandin F2 ) can cause myocardial
infarction and bronchospasm, misoprostol does not.6 Toxic doses of misoprostol have
not been determined; however, cumulative doses of up to 2200 µg administered over a
period of 12 hours have been tolerated by pregnant women, with no serious adverse
effects.7 A dose of 6000 µg of misoprostol, taken orally to induce an abortion (in
conjunction with trifluoperazine), resulted in abortion, hyperthermia, rhabdomyolysis,
hypoxemia, and a complex acid–base disorder.8
The effects of misoprostol on the reproductive tract are increased, and gastrointestinal
adverse effects are decreased, if the oral preparation of misoprostol is administered
vaginally.9,10,11 When misoprostol tablets are placed in the posterior fornix of the vagina,
plasma concentrations of misoprostol acid peak in one to two hours and then decline
slowly (Figure 1).4 Vaginal application of misoprostol results in slower increases and
lower peak plasma concentrations of misoprostol acid than does oral administration, but
overall exposure to the drug is increased (indicated by the increased area under the
curve in Figure 1).4
Among women who were 9 to 11 weeks pregnant and given misoprostol before a
surgical abortion, intrauterine pressure began to increase an average of 8 minutes after
oral administration and 21 minutes after vaginal administration and was maximal 25
minutes after oral administration and 46 minutes after vaginal administration. Uterine
contractility initially increased and then plateaued one hour after oral administration,
whereas uterine contractility increased continuously for four hours after vaginal
administration. Maximal uterine contractility was significantly higher after vaginal
administration.9
Möbius' syndrome (congenital facial paralysis) and
limb defects have occurred in the infants of women
who have taken misoprostol during the first trimester
in an unsuccessful attempt to induce abortion.12,13
Among women delivering infants with Möbius'
syndrome, the likelihood of exposure to misoprostol
in the first trimester is high, but the absolute risk of
this syndrome is probably low among all women
exposed to misoprostol in the first trimester.12 In a
recent study of 4673 malformed infants and 4980
control infants, the Latin American Collaborative
Study of Congenital Malformations noted an
increased frequency of transverse limb defects, ringshaped constrictions of the extremities,
arthrogryposis, hydrocephalus, holoprosencephaly,
and exstrophy of the bladder, but not Möbius'
syndrome, in infants exposed to misoprostol in
utero.14
Other drugs used in conjunction with misoprostol for medical abortion in the first
trimester are also teratogens. In particular, methotrexate has been associated with
craniofacial and digital anomalies.15,16 Mifepristone may also be teratogenic; however,
the risk of malformations appears to be lower with mifepristone than with methotrexate
or misoprostol.17
Misoprostol in the First Trimester of Pregnancy
Medical Abortion
For first-trimester medical abortions, misoprostol is used most extensively in
conjunction with either mifepristone or methotrexate. Both regimens are effective
(Table 1). In the initial studies of mifepristone and misoprostol for medical abortion,
both drugs were given orally. Only regimens of mifepristone in combination with oral
misoprostol have been licensed for abortion in any country. For 91 to 97 percent of
women who were no more than 49 days pregnant, 600 mg of oral mifepristone, followed
48 hours later by 400 µg of oral misoprostol, resulted in complete abortion (Table
2).18,19,20 For women who were no more than 56 days pregnant, the success rate was 83
to 95 percent.18,20,21 Lowering the dose of mifepristone to 200 mg does not reduce
efficacy.18,22 Administration of 200 mg of oral mifepristone followed by 600 µg of oral
misoprostol resulted in complete-abortion rates of 96 to 97 percent among women no
more than 49 days pregnant and 89 to 93 percent among women 50 to 63 days pregnant
(Table 2). 22,23
View this table: Table 1. Misoprostol Regimens for Pregnant Women.
[in this window]
[in a new window]
View this table: Table 2. Efficacy of Misoprostol Regimens for Medical Abortion in the First
[in this
Trimester of Pregnancy.
window]
[in a new
window]
In direct comparisons, vaginal misoprostol was more effective than oral misoprostol
when the same dose was given in combination with mifepristone.25 A single oral dose of
600 mg of mifepristone followed 48 hours later by 800 µg of vaginal misoprostol
resulted in complete abortion in 95 to 98 percent of women who were no more than 63
days pregnant.24,25 Among women with complete abortions, 93 percent had the abortion
within four hours25 and 97 percent within five days24 after taking misoprostol. In studies
of women who were no more than 56 days pregnant or no more than 63 days pregnant,
the rate of complete abortion was also high (97 or 98 percent) after the administration of
200 mg of oral mifepristone followed 48 hours later by 800 µg of vaginal misoprostol
(Table 2).26,27,28 The misoprostol dose in this regimen has been successfully
administered by women at home one to three days after they received mifepristone,27
with equal efficacy.28
A combined regimen of mifepristone and misoprostol resulted in complete abortion in
94 to 95 percent of women 9 to 13 weeks pregnant; however, the incidence of heavy
vaginal bleeding may be higher than in women with less advanced pregnancies.39,40
A single dose of intramuscular or oral methotrexate (50 mg per square meter of bodysurface area) followed five to seven days later by 800 µg of vaginal misoprostol resulted
in complete abortion in 88 to 100 percent of women (Table 2).30,31,32,33,34,41,42 With this
regimen, 53 to 60 percent of women aborted within 24 hours after one dose of
misoprostol was administered.30,31 If complete abortion did not occur within that
interval, repeating the misoprostol dose resulted in complete abortions in 19 to 32
percent of women within 24 hours after the second dose.30,31 The remaining 10 to 30
percent of women who aborted successfully had a delayed response, with the abortion
completed over an average period of 24 to 28 days (Table 2).30,31
The majority of studies of medical abortion in the first trimester with either mifepristone
or methotrexate plus misoprostol have included women who were no more than 63 days
pregnant. Usually, the rates of complete abortion among women who are no more than
49 days pregnant are higher than those among women who are 50 to 56 days pregnant,
who in turn have higher rates of complete abortion than women who are 57 to 63 days
pregnant (Table 2).20,22,23,31
Misoprostol has also been used alone for medical abortions, with variable efficacy. The
earliest studies of misoprostol-induced abortions in the first trimester reported completeabortion rates of 5 to 11 percent among women given a total dose of 400 µg of oral
misoprostol.43,44 Up to three 800-µg doses of vaginal misoprostol given every 48 hours
resulted in complete abortions in up to 96 percent of women who were no more than 63
days pregnant.38 However, in a randomized trial comparing methotrexate plus vaginal
misoprostol with vaginal misoprostol alone, only 47 percent of the women given
misoprostol alone had complete abortions, as compared with 90 percent of the women
given methotrexate plus misoprostol (P< 0.001) (Table 2).37
The variation in rates of complete abortion among women given misoprostol alone may
be due to differences in study design, since rates are often lowest in randomized trials,
or to efforts to increase vaginal absorption of misoprostol in some studies. For example,
in one study in which the success rate was high, the vagina was cleansed with either
sterile water or saline, the misoprostol tablets were moistened with two or three drops of
water or saline and then placed in the posterior fornix of the vagina, and the women
were required to remain supine for three hours after placement of the tablets.38
To determine whether moistening the misoprostol tablets increases the efficacy of the
regimen, a recent randomized study compared moistened with dry tablets of misoprostol
(800 µg) in combination with methotrexate in 240 women who were no more than 49
days pregnant.29 There was no significant difference in the rate of complete abortion (95
percent with moistened tablets and 92 percent with dry tablets, P=0.40.)29 In a
randomized study comparing moistened and dry tablets of misoprostol alone (800 µg) in
80 women who were no more than 63 days pregnant, there was also no significant
difference in the rate of complete abortion (85 percent with moistened tablets and 65
percent with dry tablets, P=0.43).35 In a study of 200 women no more than 56 days
pregnant, a dose of 800 µg of moistened vaginal misoprostol tablets alone was almost as
effective as mifepristone plus oral misoprostol (among historical controls) for inducing
complete abortions (88 percent and 94 percent, respectively; P=0.19) (Table 2).36 Given
the inconsistency of complete-abortion rates when vaginal misoprostol is used alone, as
well as the existence of safe alternative regimens, it cannot be recommended for medical
abortions in the first trimester (Table 2).
Failed Pregnancy or Fetal Death
After mifepristone or methotrexate "destabilizes" an ongoing pregnancy, misoprostol
helps expel the products of conception. In cases of anembryonic pregnancy or blighted
ovum, embryonic death, or early fetal death, the pregnancy is already destabilized, and
the physiological changes that eventually lead to spontaneous expulsion are under way
(e.g., placental degeneration and decidual sloughing). If spontaneous expulsion is
delayed, drug therapy may be indicated to evacuate the uterus, in order to avoid surgery
or a prolonged wait for expulsion.
Misoprostol is effective in evacuating the uterus in the case of an early failed pregnancy
(anembryonic pregnancy or embryonic death).45,46,47 Twenty women with early failed
pregnancies (characterized by an embryo 5 to 14 mm long with no cardiac activity or an
empty, irregular gestational sac at least 16 mm in diameter) were randomly assigned to
receive either 400 µg of oral misoprostol or 800 µg of vaginal misoprostol. If
ultrasonography performed 24 hours later revealed retained products of conception, the
dose was repeated. The rate of complete expulsion within 48 hours after the first dose of
misoprostol was 25 percent in the oral-misoprostol group and 88 percent in the vaginalmisoprostol group (P=0.01).45 There were no cases of excessive bleeding or incomplete
abortion requiring surgery. Thus, 800 µg of misoprostol given vaginally once or twice
(with the second dose given 24 hours after the first) is effective in evacuating the uterus
in the case of an early failed pregnancy or embryonic death (Table 1).
Misoprostol may also be useful for completing an inevitable or incomplete spontaneous
abortion. In the first report of the use of misoprostol for incomplete abortion, 24 women
received 400 µg of misoprostol orally, and 95 percent of them had a complete abortion
without surgical intervention.48 However, in a randomized study of 50 women with
bleeding, cramping, a dilated cervical os, and a uterine size corresponding to no more
than 14 weeks of gestation on examination, patients either were given a single dose of
400 µg of oral misoprostol or underwent immediate surgical evacuation. Surgery was
markedly more successful than misoprostol in completing the abortion within 12 hours
(97 percent vs. 13 percent, P<0.001).49 The mean hemoglobin concentration fell
significantly in women in the misoprostol group, but not in women in the surgical
group. On the basis of these findings, misoprostol is currently not recommended for the
treatment of inevitable or incomplete abortion (Table 1).
Cervical Ripening before Surgical Abortion
Cervical ripening is the softening, effacement, and gradual dilatation of the cervical os.
Before surgical abortion in the first trimester, cervical ripening reduces the incidence of
cervical lacerations and uterine perforation at the time of abortion.50,51 It can be
accomplished with hydrophilic dilators (e.g., laminaria and Hypan), which absorb water
from the cervix and slowly expand to dilate the cervical os, or biochemically with
prostaglandins (e.g., gemeprost and misoprostol). Misoprostol is less expensive than
gemeprost, is more easily stored, has fewer side effects, and is equally successful in
dilating the cervix before abortion.52 For cervical dilatation, 400 µg of vaginal
misoprostol is equivalent to one medium laminaria used for four hours preoperatively,
but laminaria placement is more painful than misoprostol placement.53 Vaginal
misoprostol causes greater dilatation than the same dose of oral misoprostol.53
In a randomized study of 120 women that compared 200 µg, 400 µg, 600 µg, and 800
µg of misoprostol given vaginally three to four hours before suction curettage, only 23
percent of women given the 200-µg dose had cervical dilatation of at least 8 mm, as
compared with 97 percent, 100 percent, and 100 percent of women given 400 µg, 600
µg, and 800 µg, respectively.54 The doses of 600 µg and 800 µg caused significantly
more adverse effects (fever, vaginal bleeding, and products of conception at the cervical
os) than the dose of 400 µg.54 Given the similar rates of cervical dilatation with 400 µg,
600 µg, and 800 µg and the higher incidence of adverse effects with 600 µg and 800 µg,
a dose of 400 µg is recommended for cervical ripening.54
Other studies have attempted to determine the ideal length of time for adequate cervical
ripening. Of 50 women given 200 µg of vaginal misoprostol six hours before suction
curettage, 74 percent had cervical dilatation of at least 8 mm.55 In a randomized trial,
women given 400 µg of misoprostol three hours before surgery had significantly greater
cervical dilatation than women given 600 µg or 800 µg two hours before surgery.56
These findings suggest that the best regimen for cervical ripening in the first trimester is
400 µg of vaginal misoprostol given three to four hours before suction curettage (Table
1).
Misoprostol in the Second Trimester of Pregnancy
Abortion
In the second trimester of pregnancy, evacuation of the uterus may be performed
because of maternal medical indications, because of severe fetal abnormalities or fetal
death, or for elective abortion. Abortions performed early in the second trimester are
usually accomplished by suction curettage, whereas procedures performed late in the
second trimester require cervical dilatation and extraction of the fetus or induction of
labor. In the second trimester, misoprostol ripens the cervix and can induce labor.
Several studies have evaluated the use of misoprostol for induction of labor in the
second trimester.57,58,59,60,61,62,63 Comparing these studies is difficult because they
included women with pregnancies of widely varying duration. Usually, the uterus
becomes more sensitive to uterotonic agents with increasing gestational age. Thus, a
dose of misoprostol given early in the second trimester may not be as effective as the
same dose given late in the second trimester. In addition, some studies have included
women carrying dead fetuses, and labor can be induced more rapidly in such women
than in those undergoing abortion for other reasons.57,58,59 It is likely that the duration of
the pregnancy after fetal death influences both the rate of successful induction of labor
and the time from induction to delivery.
Definitions of successful abortion vary. Some investigators have defined a successful
abortion as expulsion of the fetus and the intact placenta, such that curettage is not
required, whereas others have defined it as expulsion of the fetus alone. Furthermore,
these studies have involved a wide range of additional interventions. For example, in
some studies all fetuses with cardiac activity received intracardiac potassium chloride
before induction of labor.57,58,59
In the first trimester, 800 µg of vaginal misoprostol successfully induces abortion. In the
third trimester, doses in the range of 25 to 50 µg induce labor. The optimal dose of
vaginal misoprostol for induction of labor in the second trimester probably lies
somewhere between 50 and 800 µg. Within this range, higher doses may be needed to
cause abortions early in the second trimester, whereas lower doses may be sufficient
later in the second trimester.
The usual regimen for induction of labor in the second trimester is 200 µg of
misoprostol given vaginally every 12 hours. With this regimen, the rate of successful
abortion (delivery of the fetus within 48 hours) ranges from 71 percent to 100
percent.58,59,61,62,63 Increasing the frequency of misoprostol administration might be
expected to increase efficacy, but in one randomized study of 100 women, 200 µg of
misoprostol given vaginally every 6 hours was no more effective than the same dose
given every 12 hours.59
Administration of 400 µg of vaginal misoprostol every 3 hours (for a maximum of five
doses in 24 hours) resulted in complete abortion within 48 hours in 91 percent of
women undergoing induction of labor in the second trimester.60 Vaginal doses of 200
µg, 400 µg, and 600 µg given every 12 hours to women during the second trimester
resulted in abortions in 71 percent, 82 percent, and 96 percent, respectively.62 The
highest doses were associated with higher rates of adverse effects, including a
temperature above 38°C (0 percent, 2 percent, and 28 percent, respectively), nausea and
vomiting (4 percent, 12 percent, and 20 percent), and diarrhea (0 percent, 6 percent, and
22 percent).62
Uterine rupture was reported in two women undergoing abortion with the use of
misoprostol in the second trimester.64,65 One woman had undergone two cesarean
deliveries, and the other woman, who had had two prior vaginal deliveries and one
spontaneous abortion, had no history of uterine surgery or curettage.64,65 The risk of
uterine rupture associated with induction of labor with misoprostol in the second
trimester is unknown, and nearly all trials of misoprostol for induction of labor in the
second trimester have excluded women with uterine scars.
Although the optimal regimen has not been determined, it appears that 200 to 600 µg of
misoprostol given vaginally every 12 hours or 400 µg given vaginally every 3 hours
successfully induces labor in the second trimester (Table 1).
As with medical abortion in the first trimester, induction of labor in the second trimester
with misoprostol is more successful if mifepristone is given 36 to 48 hours before
misoprostol.7,66,67 The rates of successful induction of labor (delivery within 24 hours)
during the second trimester range from 90 percent among women given 200 mg of
mifepristone, followed 36 to 48 hours later by 200 µg of vaginal misoprostol given
every 3 hours,67 to 97 percent among women given the same dose of mifepristone,
followed by a loading dose of 800 µg of vaginal misoprostol and then 400 µg of oral
misoprostol every 3 hours (for a maximum of four doses).66
Misoprostol in the Third Trimester of Pregnancy
Induction of Labor with a Viable Fetus
For induction of labor at term, clinical trials have compared misoprostol with
placebo,68,69 oxytocin,70,71,72 and other prostaglandins, primarily dinoprostone
(prostaglandin E2) gel73,74,75,76,77,78,79 or the dinoprostone vaginal insert.80,81 These
studies included most indications for which labor is induced, including premature
rupture of membranes.
Misoprostol given vaginally68 or orally69 is superior to placebo for inducing cervical
ripening before induction of labor with oxytocin, and misoprostol itself is also effective
for induction of labor. In a 1997 meta-analysis of randomized, controlled trials focusing
on cervical ripening and induction of labor in a total of 488 women who received
misoprostol and 478 controls (most of whom received prostaglandin E2 gel), the time
from induction of labor to delivery was 4.6 hours shorter and the rate of cesarean
delivery was lower in the misoprostol group.82
Since this meta-analysis was performed, additional randomized, controlled trials have
been completed. The Cochrane Pregnancy and Childbirth Group reviewed 26
randomized trials comparing misoprostol with placebo, oxytocin, or prostaglandin E2 for
cervical ripening or induction of labor with a viable fetus in the third trimester.83 Some
of these trials compared oral with vaginal misoprostol, and others compared different
misoprostol regimens.83,84 The primary outcomes were the rate of vaginal delivery
within 24 hours, the incidence of uterine hyperstimulation with associated changes in
the fetal heart rate, the rate of cesarean delivery, and the incidence of serious adverse
effects in the fetus or the mother.83,84 Vaginal misoprostol (25 to 100 µg) was more
effective than oxytocin or prostaglandin E2 for inducing vaginal delivery within 24
hours. However, uterine hyperstimulation with associated changes in the fetal heart rate
was more common in women who received misoprostol than in women who received
oxytocin or prostaglandin E2.84
The frequency of meconium-stained amniotic fluid was higher in the misoprostol group
than in the prostaglandin E2 group, although it was not higher than that in the oxytocin
group.83 Whether this difference was due to increased fetal distress in the misoprostol
group or to a direct effect of misoprostol on the fetal gastrointestinal tract is unknown.
There were no differences in the rates of cesarean delivery, serious neonatal or maternal
morbidity, or neonatal or maternal mortality between women who received misoprostol
and those who received oxytocin or prostaglandin E2.83,84 However, because there were
so few serious adverse effects, the relative risk of rare adverse outcomes with the use of
misoprostol for induction of labor remains unknown.
In an effort to find an effective dose of misoprostol that does not increase the frequency
of uterine hyperstimulation, recent studies have focused on low-dose regimens of
misoprostol. In a study of 522 women given 25 µg of vaginal misoprostol every three
hours (for a maximum of eight doses) or 25 µg every six hours (for a maximum of four
doses), the regimen with the longer interval between doses resulted in a longer time to
delivery and a greater need for the additional administration of oxytocin. However, the
two regimens did not differ with respect to rates of uterine hyperstimulation with fetal
heart-rate changes, meconium passage, cesarean delivery, admission to the neonatal
intensive care unit, or Apgar scores.85 In a study of 200 women given 25 µg of vaginal
misoprostol every four hours or a dinoprostone insert, the time from induction of labor
to delivery, the rate of uterine hyperstimulation with fetal heart-rate changes, the rate of
cesarean delivery, and indexes of neonatal effects (Apgar scores, admissions to the
neonatal intensive care unit, and meconium passage) were similar in the two treatment
groups.80 The available data suggest that the best dose of misoprostol for induction of
labor is 25 µg given vaginally every four to six hours (Table 1).
Induction of Labor after Fetal Death
Misoprostol is ideally suited for induction of labor after fetal death in the third trimester
because there is no concern about the adverse effects of uterine hyperstimulation on the
fetus. A dose of 100 µg of vaginal misoprostol given every 12 hours results in success
rates that approach 100 percent.86,87 In the case of fetal death early in the third trimester,
as in the case of fetal death in the second trimester, a higher dose (200 µg of vaginal
misoprostol given every 12 hours) may be required. For fetal death at term, a dose as
low as 50 µg given every 12 hours may be adequate for induction of labor.
Induction of Labor in Women with Previous Cesarean Delivery
There have been several reports of uterine rupture associated with the administration of
misoprostol for induction of labor in women attempting vaginal delivery after cesarean
section.88,89,90 A randomized trial comparing misoprostol (25 µg given vaginally every
six hours) with oxytocin for induction of labor in women who had undergone one prior
cesarean delivery was terminated after uterine scars were disrupted in two women in the
misoprostol group.89 In a case–control study of uterine rupture in 512 women attempting
vaginal delivery after cesarean section, 5.6 percent of the women in the misoprostol
group had symptomatic uterine rupture, as compared with 0.2 percent of the women
undergoing a trial of labor without the administration of misoprostol (P<0.001).90
Notably, uterine rupture did not occur in any of the women who had undergone a prior
cesarean delivery after labor had begun spontaneously.
It remains unclear whether the use of misoprostol itself increases the frequency of
uterine rupture in women attempting vaginal delivery after cesarean section or whether
the use of any drug to induce labor in a woman with a long, firm, closed cervix
(characteristics that make it unfavorable for delivery) increases the risk of rupture. In the
case–control study described above, the women given misoprostol for induction of labor
tended to have cervixes that were unfavorable for delivery; however, an exact definition
of "unfavorable cervix" was not given.90 Until it has been proved safe, misoprostol
should not be used to induce labor in women with uterine scars (Table 1).
Misoprostol for Postpartum Hemorrhage
Because of its uterotonic effects, misoprostol has been evaluated for both the prevention
and the treatment of postpartum hemorrhage. In a prospective observational study
involving 237 women, 600 µg of misoprostol given orally just after clamping of the
umbilical cord was associated with an estimated blood loss of 500 ml or more in 6
percent of the women; none of the women had blood loss of 1000 ml or more.91
Subsequently, three randomized trials involving a total of 1115 women examined the
efficacy of misoprostol in preventing postpartum hemorrhage.92,93,94 These trials
evaluated a dose of 400 µg of misoprostol given rectally or a dose of 400 to 600 µg
given orally. The frequency of postpartum hemorrhage (blood loss, >1000 ml) was not
lower in the misoprostol group than in the control group in any of the trials; however, in
all three trials (two of which were blinded), oxytocin was given to more women in the
control groups.92,93,94 Thus, there is currently insufficient evidence to support the routine
use of misoprostol to prevent postpartum hemorrhage when oxytocin or
methylergonovine is available, but misoprostol may lower the incidence of postpartum
hemorrhage if these drugs are not readily available (Table 1).
Misoprostol has also been reported to control postpartum hemorrhage that is
unresponsive to oxytocin and methylergonovine.95 In one series of 14 women who
received 1000 µg of rectal misoprostol after the administration of oxytocin and
methylergonovine, bleeding stopped in all the women within three minutes. However,
the lack of a control group makes it impossible to know whether misoprostol was
responsible for the control of hemorrhage.
Conclusions
Misoprostol is one of the most important medications in obstetrical practice, yet its use
in pregnant women remains unapproved by the FDA. The nonexperimental, off-label
use of a drug requires sound scientific evidence. Data from clinical trials provide strong
and consistent support for the use of misoprostol as part of medical abortion regimens in
the first trimester. Used in conjunction with either mifepristone or methotrexate,
misoprostol is highly effective for medical abortion. There is also strong and consistent
evidence to support the use of misoprostol for cervical ripening before surgical abortion
in the first trimester and for induction of labor in the second and third trimesters.
Misoprostol may also prevent postpartum hemorrhage when parenteral medications are
not available. Although there are no published estimates of the extent to which
misoprostol is currently used for obstetrical or gynecologic indications, over 200 studies
involving a total of more than 16,000 women have evaluated its effectiveness in
pregnant women, and the results support its continued use.
Supported in part by a Women's Reproductive Health Research Career Development Center grant at the
National Institutes of Child Health and Human Development (to Dr. Goldberg).
Source Information
From the Department of Obstetrics, Gynecology, and Reproductive Sciences, Center for Reproductive
Health Research and Policy, San Francisco General Hospital and the University of California, San
Francisco.
Address reprint requests to Dr. Goldberg at the Department of Obstetrics, Gynecology, and Reproductive
Sciences, University of California, San Francisco, San Francisco General Hospital, 1001 Potrero Ave.
Ward 6D-11, San Francisco, CA 94110.
References
1. House Committee on Government Reform and Oversight. Off-label drug use and FDA
review of supplemental drug applications: hearing before the Subcommittee on
Human Resources and Intergovernmental Relations. 104th Congress, 2nd session,
September 12, 1996:53-94.
2. Rayburn WF. A physician's prerogative to prescribe drugs for off-label uses during
pregnancy. Obstet Gynecol 1993;81:1052-1055. [Free Full Text]
3. Scott JR, Cramer DW, Peterson HB, et al. Reading the medical literature: applying
evidence to practice. Washington, D.C.: American College of Obstetricians and
Gynecologists, 1998:1-8.
4. Zieman M, Fong SK, Benowitz NL, Banskter D, Darney PD. Absorption kinetics of
misoprostol with oral or vaginal administration. Obstet Gynecol 1997;90:8892. [Abstract]
5. Foote EF, Lee DR, Karim A, Keane WF, Halstenson CE. Disposition of misoprostol and its
active metabolite in patients with normal and impaired renal function. J Clin
Pharmacol 1995;35:384-389. [Abstract]
6. Ulmann A, Silvestre L. RU486: the French experience. Hum Reprod 1994;9:Suppl 1:126130.
7. el-Refaey H, Templeton A. Induction of abortion in the second trimester by a
combination of misoprostol and mifepristone: a randomized comparison between two
misoprostol regimens. Hum Reprod 1995;10:475-478. [Free Full Text]
8. Bond GR, Van Zee A. Overdosage of misoprostol in pregnancy. Am J Obstet Gynecol
1994;171:561-562. [Medline]
9. Danielsson KG, Marions L, Rodriguez A, Spur BW, Wong PY, Bygdeman M. Comparison
between oral and vaginal administration of misoprostol on uterine contractility. Obstet
Gynecol 1999;93:275-280. [Free Full Text]
10. Creinin MD, Darney PD. Methotrexate and misoprostol for early abortion.
Contraception 1993;48:339-48. [Erratum, Contraception 1994;49:99.]
11. Toppozada MK, Anwar MY, Hassan HA, el-Gazaerly WS. Oral or vaginal misoprostol for
induction of labor. Int J Gynaecol Obstet 1997;56:135-139. [Medline]
12. Pastuszak AL, Schüler L, Speck-Martins CE, et al. Use of misoprostol during pregnancy
and Möbius' syndrome in infants. N Engl J Med 1998;338:1881-1885. [Free Full Text]
13. Gonzalez CH, Marques-Dias MJ, Kim CA, et al. Congenital abnormalities in Brazilian
children associated with misoprostol misuse in first trimester of pregnancy. Lancet
1998;351:1624-1627. [CrossRef][ISI][Medline]
14. Orioli IM, Castilla EE. Epidemiological assessment of misoprostol teratogenicity. Br J
Obstet Gynaecol 2000;107:519-523.
15. Bawle EV, Conard JV, Weiss L. Adult and two children with fetal methotrexate
syndrome. Teratology 1998;57:51-55. [CrossRef][ISI][Medline]
16. Wiebe ER. Abortion induced with methotrexate and misoprostol: a comparison of
various protocols. Contraception 1997;55:159-163. [Medline]
17. Pons JC, Imbert MC, Elefant E, Roux C, Herschkorn P, Papiernik E. Development after
exposure to mifepristone in early pregnancy. Lancet 1991;338:763-763.
18. Comparison of two doses of mifepristone in combination with misoprostol for early
medical abortion: a randomised trial. Br J Obstet Gynaecol 2000;107:524-530.
19. Peyron R, Aubény E, Targosz V, et al. Early termination of pregnancy with mifepristone
(RU 486) and the orally active prostaglandin misoprostol. N Engl J Med 1993;328:15091513. [Free Full Text]
20. Spitz IM, Bardin CW, Benton L, Robbins A. Early pregnancy termination with
mifepristone and misoprostol in the United States. N Engl J Med 1998;338:12411247. [Free Full Text]
21. Winikoff B, Sivin I, Coyaji KJ, et al. Safety, efficacy, and acceptability of medical
abortion in China, Cuba, and India: a comparative trial of mifepristone-misoprostol
versus surgical abortion. Am J Obstet Gynecol 1997;176:431437. [CrossRef][ISI][Medline]
22. McKinley C, Thong KJ, Baird DT. The effect of dose of mifepristone and gestation on
the efficacy of medical abortion with mifepristone and misoprostol. Hum Reprod
1993;8:1502-1505. [Free Full Text]
23. Baird DT, Sukcharoen N, Thong KJ. Randomized trial of misoprostol and cervagem in
combination with a reduced dose of mifepristone for induction of abortion. Hum
Reprod 1995;10:1521-1527. [Free Full Text]
24. Schaff EA, Stadalius LS, Eisinger SH, Franks P. Vaginal misoprostol administered at
home after mifepristone (RU486) for abortion. J Fam Pract 1997;44:353360. [ISI][Medline]
25. el-Refaey H, Rajasekar D, Abdalla M, Calder L, Templeton A. Induction of abortion with
mifepristone (RU 486) and oral or vaginal misoprostol. N Engl J Med 1995;332:983987. [Free Full Text]
26. Ashok PW, Penney GC, Flett GM, Templeton A. An effective regimen for early medical
abortion: a report of 2000 consecutive cases. Hum Reprod 1998;13:29622965. [Free Full Text]
27. Schaff EA, Eisinger SH, Stadalius LS, Franks P, Gore BZ, Poppema S. Low-dose
mifepristone 200 mg and vaginal misoprostol for abortion. Contraception 1999;59:16. [CrossRef][ISI][Medline]
28. Schaff EA, Fielding SL, Westhoff C, et al. Vaginal misoprostol administered 1, 2, or 3
days after mifepristone for early medical abortion: a randomized trial. JAMA
2000;284:1948-1953. [Free Full Text]
29. Creinin MD, Carbonell JL, Schwartz JL, Varela L, Tanda R. A randomized trial of the
effect of moistening misoprostol before vaginal administration when used with
methotrexate for abortion. Contraception 1999;59:11-16. [Medline]
30. Creinin MD, Vittinghoff E, Galbraith S, Klaisle C. A randomized trial comparing
misoprostol three and seven days after methotrexate for early abortion. Am J Obstet
Gynecol 1995;173:1578-1584. [CrossRef][ISI][Medline]
31. Creinin MD, Vittinghoff E, Keder L, Darney PD, Tiller G. Methotrexate and misoprostol
for early abortion: a multicenter trial. I. Safety and efficacy. Contraception
1996;53:321-327. [CrossRef][ISI][Medline]
32. Creinin MD, Vittinghoff E, Schaff E, Klaisle C, Darney PD, Dean C. Medical abortion with
oral methotrexate and vaginal misoprostol. Obstet Gynecol 1997;90:611616. [Abstract]
33. Creinin MD. Oral methotrexate and vaginal misoprostol for early abortion.
Contraception 1996;54:15-18. [Medline]
34. Carbonell Esteve JL, Varela L, Velazco A, Tanda R, Sanchez C. 25 mg Or 50 mg of oral
methotrexate followed by vaginal misoprostol 7 days after for early abortion: a
randomized trial. Gynecol Obstet Invest 1999;47:182-187. [Medline]
35. Ngai SW, Tang OS, Chan YM, Ho PC. Vaginal misoprostol alone for medical abortion up
to 9 weeks of gestation: efficacy and acceptability. Hum Reprod 2000;15:11591162. [Free Full Text]
36. Jain JK, Meckstroth KR, Mishell DR Jr. Early pregnancy termination with intravaginally
administered sodium chloride solution-moistened misoprostol tablets: historical
comparison with mifepristone and oral misoprostol. Am J Obstet Gynecol
1999;181:1386-1391. [CrossRef][ISI][Medline]
37. Creinin MD, Vittinghoff E. Methotrexate and misoprostol vs misoprostol alone for early
abortion: a randomized controlled trial. JAMA 1994;272:1190-1195. [Abstract]
38. Carbonell JL, Varela L, Velazco A, Fernandez C. The use of misoprostol for termination
of early pregnancy. Contraception 1997;55:165-168. [CrossRef][ISI][Medline]
39. Ashok PW, Flett GM, Templeton A. Termination of pregnancy at 9-13 weeks'
amenorrhoea with mifepristone and misoprostol. Lancet 1998;352:542543. [CrossRef][ISI][Medline]
40. Gouk EV, Lincoln K, Khair A, Haslock J, Knight J, Cruickshank DJ. Medical termination of
pregnancy at 63 to 83 days gestation. Br J Obstet Gynaecol 1999;106:535539. [Medline]
41. Hausknecht RU. Methotrexate and misoprostol to terminate early pregnancy. N Engl J
Med 1995;333:537-540. [Free Full Text]
42. Carbonell JL, Varela L, Velazco A, Cabezas E, Fernandez C, Sanchez C. Oral
methotrexate and vaginal misoprostol for early abortion. Contraception 1998;57:8388. [CrossRef][ISI][Medline]
43. Lewis JH. Summary of the 29th meeting of the Gastrointestinal Drugs Advisory
Committee, Food and Drug Administration -- June 10, 1985. Am J Gastroenterol
1985;80:743-745. [Medline]
44. Norman JE, Thong KJ, Baird DT. Uterine contractility and induction of abortion in early
pregnancy by misoprostol and mifepristone. Lancet 1991;338:12331236. [CrossRef][ISI][Medline]
45. Creinin MD, Moyer R, Guido R. Misoprostol for medical evacuation of early pregnancy
failure. Obstet Gynecol 1997;89:768-772. [Abstract]
46. Zalanyi S. Vaginal misoprostol alone is effective in the treatment of missed abortion. Br
J Obstet Gynaecol 1998;105:1026-1028. [ISI][Medline]
47. Herabutya Y, O-Prasertsawat P. Misoprostol in the management of missed abortion.
Int J Gynaecol Obstet 1997;56:263-266. [CrossRef][Medline]
48. Henshaw RC, Cooper K, el-Refaey H, Smith NC, Templeton AA. Medical management of
miscarriage: non-surgical uterine evacuation of incomplete and inevitable
spontaneous abortion. BMJ 1993;306:894-5. [Erratum, BMJ 1993;306:1303.]
49. de Jonge ET, Makin JD, Manefeldt E, De Wet GH, Pattinson RC. Randomised clinical
trial of medical evacuation and surgical curettage for incomplete miscarriage. BMJ
1995;311:662-662. [Free Full Text]
50. Grimes DA, Schulz KF, Cates WJ Jr. Prevention of uterine perforation during curettage
abortion. JAMA 1984;251:2108-2111. [Abstract]
51. Schulz KF, Grimes DA, Cates W Jr. Measures to prevent cervical injury during suction
curettage abortion. Lancet 1983;1:1182-1185. [CrossRef][ISI][Medline]
52. el-Refaey H, Calder L, Wheatley DN, Templeton A. Cervical priming with prostaglandin
E1 analogues, misoprostol and gemeprost. Lancet 1994;343:1207-9. [Erratum, Lancet
1994;343:1650.]
53. MacIsaac L, Grossman D, Balistreri E, Darney P. A randomized controlled trial of
laminaria, oral misoprostol, and vaginal misoprostol before abortion. Obstet Gynecol
1999;93:766-770. [Free Full Text]
54. Singh K, Fong YF, Prasad RN, Dong F. Randomized trial to determine optimal dose of
vaginal misoprostol for preabortion cervical priming. Obstet Gynecol 1998;92:795798. [Abstract]
55. Bugalho A, Bique C, Almeida L, Bergstrom S. Application of vaginal misoprostol before
cervical dilatation to facilitate first-trimester pregnancy interruption. Obstet Gynecol
1994;83:729-731. [Medline]
56. Singh K, Fong YF, Prasad RN, Dong F. Evacuation interval after vaginal misoprostol for
preabortion cervical priming: a randomized trial. Obstet Gynecol 1999;94:431434. [Free Full Text]
57. Jain JK, Mishell DR Jr. A comparison of intravaginal misoprostol with prostaglandin E2
for termination of second-trimester abortion. N Engl J Med 1994;331:290293. [Free Full Text]
58. Jain JK, Mishell DR Jr. A comparison of misoprostol with and without laminaria tents
for induction of second-trimester abortion. Am J Obstet Gynecol 1996;175:173177. [CrossRef][ISI][Medline]
59. Jain JK, Kuo J, Mishell DR Jr. A comparison of two dosing regimens of intravaginal
misoprostol for second-trimester pregnancy termination. Obstet Gynecol 1999;93:571575. [Free Full Text]
60. Wong KS, Ngai CS, Wong AY, Tang LC, Ho PC. Vaginal misoprostol compared with
vaginal gemeprost in termination of second trimester pregnancy: a randomized trial.
Contraception 1998;58:207-210. [CrossRef][ISI][Medline]
61. Nuutila M, Toivonen J, Ylikorkala O, Halmesmaki E. A comparison between two doses
of intravaginal misoprostol and gemeprost for induction of second-trimester abortion.
Obstet Gynecol 1997;90:896-900. [Abstract]
62. Herabutya Y, O-Prasertsawat P. Second trimester abortion using intravaginal
misoprostol. Int J Gynaecol Obstet 1998;60:161-165. [Medline]
63. Bugalho A, Bique C, Almeida L, Faundes A. The effectiveness of intravaginal
misoprostol (Cytotec) in inducing abortion after eleven weeks of pregnancy. Stud Fam
Plann 1993;24:319-323. [Medline]
64. Chen M, Shih JC, Chiu WT, Hsieh FJ. Separation of cesarean scar during secondtrimester intravaginal misoprostol abortion. Obstet Gynecol 1999;94:840840. [Free Full Text]
65. Phillips K, Berry C, Mathers AM. Uterine rupture during second trimester termination
of pregnancy using mifepristone and a prostaglandin. Eur J Obstet Gynecol Reprod Biol
1996;65:175-176. [Medline]
66. Webster D, Penney GC, Templeton A. A comparison of 600 and 200 mg mifepristone
prior to second trimester abortion with the prostaglandin misoprostol. Br J Obstet
Gynaecol 1996;103:706-709. [ISI][Medline]
67. Ho PC, Chan YF, Lau W. Misoprostol is as effective as gemeprost in termination of
second trimester pregnancy when combined with mifepristone: a randomised
comparative trial. Contraception 1996;53:281-283. [ISI][Medline]
68. Fletcher HM, Mitchell S, Simeon D, Frederick J, Brown D. Intravaginal misoprostol as a
cervical ripening agent. Br J Obstet Gynaecol 1993;100:641-644. [Medline]
69. Ngai SW, To WK, Lao T, Ho PC. Cervical priming with oral misoprostol in pre-labor
rupture of membranes at term. Obstet Gynecol 1996;87:923-926. [Abstract]
70. Kramer RL, Gilson GJ, Morrison DS, Martin D, Gonzales JL, Qualls CR. A randomized
trial of misoprostol and oxytocin for induction of labor: safety and efficacy. Obstet
Gynecol 1997;89:387-391. [Abstract]
71. Sanchez-Ramos L, Chen AH, Kaunitz AM, Gaudier FL, Delke I. Labor induction with
intravaginal misoprostol in term premature rupture of membranes: a randomized
study. Obstet Gynecol 1997;89:909-912. [Abstract]
72. Wing DA, Paul RH. Induction of labor with misoprostol for premature rupture of
membranes beyond thirty-six weeks' gestation. Am J Obstet Gynecol 1998;179:9499. [Medline]
73. Varaklis K, Gumina R, Stubblefield PG. Randomized controlled trial of vaginal
misoprostol and intracervical prostaglandin E2 gel for induction of labor at term.
Obstet Gynecol 1995;86:541-544. [Abstract]
74. Wing DA, Rahall A, Jones MM, Goodwin TM, Paul RH. Misoprostol: an effective agent
for cervical ripening and labor induction. Am J Obstet Gynecol 1995;172:18111816. [Medline]
75. Wing DA, Jones MM, Rahall A, Goodwin TM, Paul RH. A comparison of misoprostol and
prostaglandin E2 gel for preinduction cervical ripening and labor induction. Am J
Obstet Gynecol 1995;172:1804-1810. [CrossRef][Medline]
76. Buser D, Mora G, Arias F. A randomized comparison between misoprostol and
dinoprostone for cervical ripening and labor induction in patients with unfavorable
cervices. Obstet Gynecol 1997;89:581-585. [Abstract]
77. Surbek DV, Boesiger H, Hoesli I, Pavic N, Holzgreve W. A double-blind comparison of
the safety and efficacy of intravaginal misoprostol and prostaglandin E2 to induce
labor. Am J Obstet Gynecol 1997;177:1018-1023. [Medline]
78. Gottschall DS, Borgida AF, Mihalek JJ, Sauer F, Rodis JF. A randomized clinical trial
comparing misoprostol with prostaglandin E2 gel for preinduction cervical ripening.
Am J Obstet Gynecol 1997;177:1067-1070. [Medline]
79. Kolderup L, McLean L, Grullon K, Safford K, Kilpatrick SJ. Misoprostol is more
efficacious for labor induction than prostaglandin E2, but is it associated with more
risk? Am J Obstet Gynecol 1999;180:1543-1550. [Medline]
80. Wing DA, Ortiz-Omphroy G, Paul RH. A comparison of intermittent vaginal
administration of misoprostol with continuous dinoprostone for cervical ripening and
labor induction. Am J Obstet Gynecol 1997;177:612-618. [CrossRef][ISI][Medline]
81. Sanchez-Ramos L, Peterson DE, Delke I, Gaudier FL, Kaunitz AM. Labor induction with
prostaglandin E1 misoprostol compared with dinoprostone vaginal insert: a
randomized trial. Obstet Gynecol 1998;91:401-405. [Abstract]
82. Sanchez-Ramos L, Kaunitz AM, Wears RL, Delke I, Gaudier FL. Misoprostol for cervical
ripening and labor induction: a meta-analysis. Obstet Gynecol 1997;89:633642. [Abstract]
83. Hofmeyr GJ, Gulmezoglu AM. Vaginal misoprostol for cervical ripening and labour
induction in late pregnancy (Cochrane review). In: Cochrane Library database, issue 3.
Oxford, England: Cochrane Update Software, 2000.
84. Hofmeyr GJ, Gulmezoglu AM, Alfirevic Z. Misoprostol for induction of labour: a
systematic review. Br J Obstet Gynaecol 1999;106:798-803. [Medline]
85. Wing DA, Paul RH. A comparison of differing dosing regimens of vaginally administered
misoprostol for preinduction cervical ripening and labor induction. Am J Obstet
Gynecol 1996;175:158-64. [Erratum, Am J Obstet Gynecol 1997;176:1423.]
86. Bugalho A, Bique C, Machungo F, Faundes A. Induction of labor with intravaginal
misoprostol in intrauterine fetal death. Am J Obstet Gynecol 1994;171:538541. [Medline]
87. Bugalho A, Bique C, Machungo F, Bergstrom S. Vaginal misoprostol as an alternative to
oxytocin for induction of labor in women with late fetal death. Acta Obstet Gynecol
Scand 1995;74:194-198. [Medline]
88. Bennett BB. Uterine rupture during induction of labor at term with intravaginal
misoprostol. Obstet Gynecol 1997;89:832-833. [Abstract]
89. Wing DA, Lovett K, Paul RH. Disruption of prior uterine incision following misoprostol
for labor induction in women with previous cesarean delivery. Obstet Gynecol
1998;91:828-830. [Abstract]
90. Plaut MM, Schwartz ML, Lubarsky SL. Uterine rupture associated with the use of
misoprostol in the gravid patient with a previous cesarean section. Am J Obstet
Gynecol 1999;180:1535-1542. [Medline]
91. el-Refaey H, O'Brien P, Morafa W, Walder J, Rodeck C. Use of oral misoprostol in the
prevention of postpartum haemorrhage. Br J Obstet Gynaecol 1997;104:336339. [ISI][Medline]
92. Bamigboye AA, Hofmeyr GJ, Merrell DA. Rectal misoprostol in the prevention of
postpartum hemorrhage: a placebo-controlled trial. Am J Obstet Gynecol
1998;179:1043-1046. [Medline]
93. Hofmeyr GJ, Nikodem VC, de Jager M, Gelbart BR. A randomised placebo controlled
trial of oral misoprostol in the third stage of labour. Br J Obstet Gynaecol
1998;105:971-975. [ISI][Medline]
94. Surbek DV, Fehr PM, Hosli I, Holzgreve W. Oral misoprostol for third stage of labor: a
randomized placebo-controlled trial. Obstet Gynecol 1999;94:255-258. [Free Full Text]
95. O'Brien P, El-Refaey H, Gordon A, Geary M, Rodeck CH. Rectally administered
misoprostol for the treatment of postpartum hemorrhage unresponsive to oxytocin
and ergometrine: a descriptive study. Obstet Gynecol 1998;92:212-214. [Abstract]
PDF
Editorial
by Hale, R. W.
Add to Personal Archive
Add to Citation Manager
Notify a Friend
This article has been cited by other
articles:
•
•
•
•
•
•
•
•
•
•
•
•
•
•
E-mail When Cited
Bos-Thompson, M.-A., Hillaire-Buys, D., Roux, C.,
Faillie, J.-L., Amram, D. (2008). Mobius Syndrome in
a Neonate After Mifepristone and Misoprostol
Elective Abortion Failure. The Annals of
Pharmacotherapy 42: 888-892 [Abstract] [Full Text]
PubMed Citation
Kapp, N., Borgatta, L., Stubblefield, P., Vragovic, O.,
Moreno, N. (2007). Mifepristone in SecondTrimester Medical Abortion: A Randomized
Controlled Trial. Obstet Gynecol 110: 1304-1310 [Abstract] [Full Text]
Aronsson, A., Fiala, C., Stephansson, O., Granath, F., Watzer, B., Schweer, H., GemzellDanielsson, K. (2007). Pharmacokinetic profiles up to 12 h after administration of
vaginal, sublingual and slow-release oral misoprostol. Hum Reprod 22: 1912-1918
[Abstract] [Full Text]
Henriques, A., Lourenco, A. V., Ribeirinho, A., Ferreira, H., Graca, L. M. (2007).
Maternal Death Related to Misoprostol Overdose. Obstet Gynecol 109: 489-490
[Abstract] [Full Text]
Creinin, M. D., Huang, X., Westhoff, C., Barnhart, K., Gilles, J. M., Zhang, J., for the
National Institute of Child Health and Hum, (2006). Factors Related to Successful
Misoprostol Treatment for Early Pregnancy Failure.. Obstet Gynecol 107: 901-907
[Abstract] [Full Text]
Lin, M. G., Nuthalapaty, F. S., Carver, A. R., Case, A. S., Ramsey, P. S. (2005).
Misoprostol for Labor Induction in Women With Term Premature Rupture of
Membranes: A Meta-Analysis. Obstet Gynecol 106: 593-601 [Abstract] [Full Text]
Winikoff, B. (2005). Pregnancy Failure and Misoprostol -- Time for a Change. NEJM
353: 834-836 [Full Text]
Goldberg, A. B., Drey, E. A., Whitaker, A. K., Kang, M.-S., Meckstroth, K. R., Darney, P.
D. (2005). Misoprostol Compared With Laminaria Before Early Second-Trimester
Surgical Abortion: A Randomized Trial. Obstet Gynecol 106: 234-241 [Abstract] [Full
Text]
Steinauer, J., Drey, E. A., Lewis, R., Landy, U., Learman, L. A. (2005). Obstetrics and
Gynecology Resident Satisfaction With an Integrated, Comprehensive Abortion
Rotation. Obstet Gynecol 105: 1335-1340 [Abstract] [Full Text]
Yedlinsky, N. T., Morgan, F. C., Whitecar, P. W. (2005). Anomalies Associated With
Failed Methotrexate and Misoprostol Termination. Obstet Gynecol 105: 1203-1205
[Abstract] [Full Text]
Graziosi, G.C.M., van der Steeg, J.W., Reuwer, P.H.W., Drogtrop, A.P., Bruinse, H.W.,
Mol, B.W.J. (2005). Economic evaluation of misoprostol in the treatment of early
pregnancy failure compared to curettage after an expectant management. Hum
Reprod 20: 1067-1071 [Abstract] [Full Text]
Ramsey, P. S., Meyer, L., Walkes, B. A., Harris, D., Ogburn, P. L. Jr, Heise, R. H., Ramin,
K. D. (2005). Cardiotocographic Abnormalities Associated With Dinoprostone and
Misoprostol Cervical Ripening. Obstet Gynecol 105: 85-90 [Abstract] [Full Text]
Bhullar, A., Carlan, S. J., Hamm, J., Lamberty, N., White, L., Richichi, K. (2004). Buccal
Misoprostol to Decrease Blood Loss After Vaginal Delivery: A Randomized Trial. Obstet
Gynecol 104: 1282-1288 [Abstract] [Full Text]
Chen, A., Yuan, W., Meirik, O., Wang, X., Wu, S.-Z., Zhou, L., Luo, L., Gao, E., Cheng, Y.
(2004). Mifepristone-induced Early Abortion and Outcome of Subsequent Wanted
Pregnancy. Am J Epidemiol 160: 110-117 [Abstract] [Full Text]
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Ramsey, P. S., Savage, K., Lincoln, T., Owen, J. (2004). Vaginal Misoprostol Versus
Concentrated Oxytocin and Vaginal PGE2 for Second-Trimester Labor Induction. Obstet
Gynecol 104: 138-145 [Abstract] [Full Text]
Stubblefield, P. G., Carr-Ellis, S., Borgatta, L. (2004). Methods for Induced Abortion.
Obstet Gynecol 104: 174-185 [Abstract] [Full Text]
El-Refaey, H., Rodeck, C. (2003). Post-partum haemorrhage: definitions, medical and
surgical management. A time for change. Br Med Bull 67: 205-217 [Abstract] [Full Text]
Verzijl, H. T.F.M., van der Zwaag, B., Cruysberg, J. R.M., Padberg, G. W. (2003). Mobius
syndrome redefined: A syndrome of rhombencephalic maldevelopment. Neurology 61:
327-333 [Abstract] [Full Text]
Lo, J. Y., Alexander, J. M., McIntire, D. D., Leveno, K. J. (2003). Ruptured Membranes at
Term: Randomized, Double-Blind Trial of Oral Misoprostol for Labor Induction. Obstet
Gynecol 101: 685-689 [Abstract] [Full Text]
Villar, J., Gulmezoglu, A. M., Hofmeyr, G. J., Forna, F. (2002). Systematic Review of
Randomized Controlled Trials of Misoprostol to Prevent Postpartum Hemorrhage.
Obstet Gynecol 100: 1301-1312 [Abstract] [Full Text]
Creinin, M. D., Harwood, B., Guido, R. S., Wagaarachchi, P., Ashok, P., Templeton, A.
(2002). Medical Management of Missed Abortion: A Randomized Clinical Trial. Obstet
Gynecol 100: 382-383 [Full Text]
Sanchez-Ramos, L., Danner, C. J., Delke, I., Kaunitz, A. M. (2002). The Effect of Tablet
Moistening on Labor Induction With Intravaginal Misoprostol: A Randomized Trial.
Obstet Gynecol 99: 1080-1084 [Abstract] [Full Text]
van der Zwaag, B, Verzijl, H T F M, Beltran-Valero de Bernabe, D, Schuster, V L, van
Bokhoven, H, Kremer, H, van Reen, M, Wichers, G H, Brunner, H G, Padberg, G W
(2002). Mutation analysis in the candidate Mobius syndrome genes PGT and GATA2 on
chromosome 3 and EGR2 on chromosome 10. J. Med. Genet. 39: e30-30 [Full Text]
Perrone, J. F., Caldito, G., Mailhes, J. B., Tucker, A. N., Ford, W. R., London, S. N. (2002).
Oral Misoprostol Before Office Endometrial Biopsy. Obstet Gynecol 99: 439-444
[Abstract] [Full Text]
Lowenstein, E., Wanzer, S. H. (2002). The U.S. Attorney General's Intrusion into
Medical Practice. NEJM 346: 447-448 [Full Text]
Blanchard, K., Clark, S., Winikoff, B., Gaines, G., Kabani, G., Shannon, C. (2002).
Misoprostol for Women's Health: A Review. Obstet Gynecol 99: 316-332 [Abstract]
[Full Text]
Sanchez-Ramos, L., Kaunitz, A. M., Delke, I. (2002). Labor Induction With 25 {micro}g
Versus 50 {micro}g Intravaginal Misoprostol: A Systematic Review. Obstet Gynecol 99:
145-151 [Abstract] [Full Text]
Berghahn, L., Christensen, D., Droste, S. (2001). Uterine Rupture During SecondTrimester Abortion Associated With Misoprostol. Obstet Gynecol 98: 976-977
[Abstract] [Full Text]
Pang, M.W., Lee, T.S., Chung, T.K.H. (2001). Incomplete miscarriage: a randomized
controlled trial comparing oral with vaginal misoprostol for medical evacuation. Hum
Reprod 16: 2283-2287 [Abstract] [Full Text]
Gebhardt, D O E (2001). Misoprostol in a topsyturvy world. J. Med. Ethics 27: 205-205
[Full Text]
(2001). Recommendations for Use of Misoprostol in Pregnant Women. JWatch
Women's Health 2001: 1-1 [Full Text]
Hale, R. W., Zinberg, S. (2001). Use of Misoprostol in Pregnancy. NEJM 344: 59-60 [Full
Text]
Friedman, M. A. (2001). Manufacturer's Warning Regarding Unapproved Uses of
Misoprostol. NEJM 344: 61-61 [Full Text]











© Copyright 2026