
full text
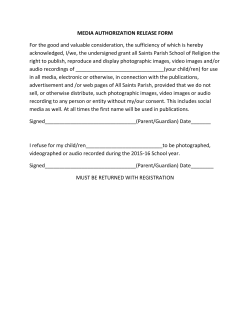
Journal of Audiovisual Media in Medicine, Vol. 27, No. 3, pp. 115–119 An intranet-based clinical imaging service TREVOR HILL, SCOTT REYNOLDS AND TED BALK This paper explains how the Photographic Department at The Queen Victoria Hospital, East Grinstead, has transformed its clinical photography service through the use of digital technology. The Department now plays a more proactive role in patient care, and its intranet-based digital imaging system has been recognized as an area of best practice by The Department of Health Information Policy Unit and by the Medicines and Healthcare Products Regulatory Agency. and illustration services, and the department is always busy with a case mix of emergency, urgent and elective surgery (Figure 2). Approximately 40,000 clinical images were produced in 2003. The Department also offers a wide range of digital video services, including a modern editing suite, the usual graphic services, and the provision of a teleconferencing service, which is used as part of the Kent & Medway Cancer Network, and as a ‘cross site’ teaching facility. Introduction The ‘digital revolution’ has rapidly transformed the photographic industry, both technically and culturally, to a level where it is now as much about visual communication as about image-based recordings for reference purposes (Figure 1). Digital technology has allowed clinical photographers to raise the profile of their profession by integrating their departments into the clinical service delivery system, offering a service in which the finished product is essentially a tool for the advancement of health and surgical science, education, medicolegal solutions, and, of course, patient care. This paper explains how the Photographic Department at The Queen Victoria Hospital (QVH), East Grinstead, has transformed its core business, i.e., clinical photography, and how the department now plays a more proactive role, which has led to an improvement in patient care. The Queen Victoria Hospital was established as a reconstructive centre during the Second World War, when Sir William Kelsey-Fry and Sir Archibald McIndoe set up their respective maxillofacial and plastic surgery units on the site of the present cottage hospital to treat injuries sustained by servicemen.1 This regional specialty unit now serves a population of over four million in the south-east of England. Its specialties include burns, severe trauma (often involving replantation), reconstructive plastic surgery, maxillofacial surgery, oculoplastic and corneo-plastic surgery, and orthodontics. The hospital is also a centre for cleft-lip and palate repair, and craniofacial anomalies, and has four consultants dedicated to hand surgery. There are a number of smaller clinical areas requiring photography Corresponding author: Trevor Hill, Manager, Medical Illustration Services, Queen Victoria Hospital, Holtye Road, East Grinstead, West Sussex RH19 3RL, UK. E-mail: [email protected] Scott Reynolds, Managing Director ‘GCP Software Systems Ltd’ (GCP). Ted Balk, Head of Information Management and Technology, Queen Victoria Hospital. Figure 1. Digital technology has raised the profile of the clinical photography profession. Figure 2. Breakdown of the use of clinical photography services according to speciality at QVH. ISSN 0140-511X printed/ISSN 1465-3494 online/04/030115-05 # 2004 Institute of Medical Illustrators DOI: 10.1080/01405110400010092 116 T. Hill et al. Rationale for digital For more than thirty years the department has supplied clinical images in the form of colour transparencies, either directly filed in patients’ case notes or cross-referenced into a teaching slide library. With the advent of digital imaging, its potential in health-care was immediately obvious. Digital technology would also provide an opportunity to address a number of outstanding issues: for example, over several years patient numbers, and hence workload, had steadily increased by approximately 8% per year, but with the planned appointment of four additional consultants there would be a sharper rise. Implemented correctly, digital technology could provide a means of: (a) making more efficient use of staff time, (b) controlling escalating material costs, and (c) improving the speed of service. To achieve these goals it was imperative that the change to digital be complete; there would be no printed (hard) copies because all images would be viewed electronically (soft copies). It seemed pointless to originate electronically, only to print and then laboriously file hard copies. Also, there would have been considerable costs with the production of large numbers of prints, which would have compromised the improvement in financial efficiency. In essence, the specification for the digital system was: that it would manage and document images from the cameras prior to uploading to a central server; that the images would be immediately available for viewing at appropriate locations across the site on terminals linked to the hospital intranet; and that the images would be easy to retrieve by staff with access privileges, fully documented, and securely stored, whilst satisfying all requirements of patient confidentiality. Finance and Support QVH is fortunate to have an enthusiastic Information Technology (IT) Department, which was keen to run such a system over the network. The Photographic Department is managed within the Surgical Care Directorate and represented at many forums, so it maintains a high profile, and there is positive awareness within the hospital of its work. Following a presentation to the Clinical Information Advisory Group, and subsequently to the Trust Board, the proposal was given unanimous approval. The IT implications were considered, along with the initial setup costs; the presentation also indicated a conservative, but immediate, saving of £13,000 per year on material costs. It was also argued that non-implementation of the proposal would require an increase in staffing in the Department to accommodate the extra work following the new consultant appointments. With the support of the Trust Board a request for £25,000 was made to the QVH League of Friends, in order to purchase four complete Nikon D1x systems, each comprising a camera body, 105-, 60- and 35-mm lenses, two 64-MB Compact Flash cards, an SB-29 flash unit, and a carry-bag. Some computer hardware and software was also purchased, including slide and flatbed scanners, and card readers. The League had been looking for involvement in an active project and the digital programme was considered ideal. It was agreed the money should be ring-fenced, and could be spent over a five-year period. Software selection Included in the initial set-up package was an off-the-shelf image management software program, which, at the time, was considered to be a suitable platform for the database. However, subsequently there were problems linking this software to the Patient Administration System (PAS), and operating it through Internet Explorer for use over the hospital intranet, so eventually it was abandoned. At this time there was considerable interest at QVH for telemedicine.2 The Plastic Surgery Department alone receives approximately twenty acute referrals each day, so consequently trauma services are under great pressure, and a method of improving efficiency was sought. Telemedicine seemed to be an ideal medium, whereby emailed images from referral hospitals would help towards better wound assessment, which, in turn, would lead to a more appropriate transfer of patients. Therefore, Godalming Computer Product Software Systems Ltd. (GCP) designed and built a system to transmit images securely via normal e-mail or NHS-Net, such that, when received at the hospital, they become available for immediate review using an ordinary web browser. This has meant that consultants can give an instant opinion, even when in theatre. Having successfully designed the database and web interface for the telemedicine project, GCP was approached to see if it could assist the Photographic Department with the digital project. During the development of the management software, known as DISTAR (Digital Image Storage And Retrieval), GCP also incorporated automatic patient data transfer via a direct link to the PAS. As DISTAR evolved it was brought gradually on line, whilst patients were photographed both on slide film and digitally. However, many consultants were immediately content to receive images over the hospital intranet and instructed the department not to bother with slides; the department was shooting 90% of its work digitally within six months, and 100% within a year. Operation of the system Following a photography session, the CompactFlash cards are removed from the cameras and entered into a card reader linked to one of four PCs loaded with DISTAR. Accompanying the CompactFlash cards are the hospital’s pink photographic request forms, which hold the relevant patient details. From a desktop icon, the first screen to appear gives the operator a choice of actions from the digital image database: for uploading images ADD NEW PINK SLIPS is selected (Figure 3). This displays a screen, which is basically a copy of the pink request form (Figure 4a). By clicking on GET NEW the operator is An intranet-based clinical imaging service 117 Figure 3. The first screen to appear when using the DISTAR system. Figure 5. The images are viewed as thumbnails, then selected and uploaded to the hospital database. asked for the patient’s HOSPITAL REGISTRATION NUMBER; entering the number provides all the patient’s details, which are automatically drawn from the PAS and entered into the relevant boxes (Figure 4b). The operator then tabs down and enters the relevant exposure details for that particular patient, such as VIEWS, CLINICAL CONDITION, LOCATION, PHOTOGRAPHER, and LEVEL OF PATIENT CONSENT. A click on LOAD IMAGE TRANSFER PROGRAMME lists the various patients’ entries. Once the files have been selected, the images on the CompactFlash card are displayed as thumbnails. If necessary, images are rotated for correct viewing, or flipped in the case of dental mirror views. They are then highlighted for selection, and uploaded to the hospital database (Figure 5). At this stage the originals are stored on the Hospital’s file-server, but simultaneously copies are made which have a ‘text’ copyright message applied; these are the images used for general viewing over the intranet. As soon as the images are transferred to the server they are available for viewing from the internal telemedicine website. The clinician who requested the photography can view the images elsewhere, and the case can then be discussed with the patient or other clinicians. It should be noted that any alteration of the original image is prohibited: the images can be enlarged, rotated and panned, and aspects such as brightness, contrast and sharpness can also be adjusted (Figure 6); but any changes do not affect the original images, which remain untouched and available for retrieval by the Department in the event that they are required for high-quality reproduction purposes. Technical information The file-server is installed with Windows NT4 operating software and is a stand-alone unit with IIS4 (Internet Information Service), which is used for publishing web Figure 4. (a) The operator is prompted for the patient’s hospital number; (b) the patient’s details are automatically entered from the PAS. Figure 6. Viewers can manipulate the image to improve appearance without altering the original files. 118 T. Hill et al. content. The system initially used a Pentium 4 rack-mount server with 256 MB of RAM and dual (RAID-1) 14-GB disks, but it has since had a second pair of RAID-1 disks added for growth. The system will shortly be upgraded to a Windows 2000 SQL server for exponential growth. Original images are uploaded and stored on mirrored hard-drives at the standard 8:1 JPEG compression produced by the Nikon D1x cameras. During the uploading process they are copyright branded, and resized as smaller separate thumbnail JPEG files (to fit a 2006200 pixel square) before being stored on the server. The use of pre-generated thumbnail files affords quick loading from the server (and therefore less bandwidth use) when they are required for viewing simultaneously on a web page. Each evening the images are backed up on a secondary server at a separate location on-site, and this is repeated monthly as part of the normal IT Department backup protocol. Hence the original images are effectively stored four times. During the development of the system, considerable thought was given to the original file format before adopting the D1x JPEG 8:1 medium setting, which gives an approximate file size of 640 KB. This was chosen because the image quality is more than fit for its intended purpose, and larger file sizes were impractical because approximately 40,000 pictures need to be stored each year. Additionally, as the system is operated over the Trust intranet, the JPEG file format is inherently supported by the web browsers. Digital management In order to maintain strict management control, images can only be uploaded to the database using the software on PCs in the Photographic Department. Other functions of this software include the ability to amend incorrect details, transfer images, extract images, delete entries, and add images to an existing session. This is ideal during long reconstructive operations when surgical teams sometimes like to view the earlier stages. In their administrative role the IT staff also have full access to the system so that software maintenance and system updates are straightforward. Viewing page Images from the Photographic Department and the telemedicine service are stored on the same file server and accessed via a common home page. Only authorized staff with access privileges can access images, and PCs for viewing are limited to ‘view only’; although, as noted above, they are able to adjust, temporarily, the brightness and contrast of the image, and to zoom into selected areas. This function is particularly useful when viewing telemedicine referral images as the quality of pictures varies considerably. Access privileges to enter the DISTAR system are authorized on an individual basis by the Human Resources Department, and issued by the IT Department in its administration role. Figure 7. A summary of the QVH Photographic and Video Recording Policy. The Burns Unit has particularly welcomed the digital service, and a photographer attends all admissions and dressing changes at key stages of treatment. It is not always possible for some clinical members to be present at these times, but they are able to see pictures at any viewing terminal before the wound is dressed, and so make informed decisions which improve clinical efficiency and patient care. In such cases the wound need not be disturbed for a second examination, correspondingly reducing distress, pain and risk of infection. Morning ward reports are also more meaningful when the notes regarding a patient who has been admitted during the night has pictures readily available for viewing (N.B. the Photographic Department operates a 24-hour on-call service). Photographic and video recording policy With images being uploaded from the telemedicine service and the Photographic Department, it was clear that the publication of a Trust Photographic and Video Recording Policy was vital. In addition, many clinicians were using their own digital cameras on site for personal reasons, so the Trust has addressed these issues with a Policy Statement (Figure 7). The DISTAR software has had to satisfy all aspects of this policy and of issues detailed in the Data Protection Act, such as the safe-keeping of information and the potential problems of image alteration. A comprehensive policy should help to control the problems associated with clinicians undertaking their own photography for personal use. An intranet-based clinical imaging service 119 Future developments Figure 8. Trevor Hill demonstrates the DISTAR system to the Princess Royal. There are increasing demands from consultants to view images at home; this facilitates out-of-hours assessments by on-call consultants at a junior doctor’s request. DISTAR can send encrypted data over the internet to a home e-mail address, where it is downloaded by a separate DISTAR program, which decrypts and unpacks the images and any accompanying demographic data. The management aspect of the software will soon have designated sections to accommodate images from the Corneo-plastic Unit and the Clinical Research Department, which have both discovered problems associated with localized image management and storage. QVH is scheduled to install a PACS DICOM digital radiography system that will be networked to peripheral hospitals via the QVH ‘hub-and-spoke’ scheme and the Kent & Medway Cancer Network. It is planned to incorporate all forms of clinical images within this system, where they can be accessed via a common platform: not only will communication between specialists at disparate locations be greatly improved, but also all clinical images of patients will be readily available to health-care professionals at any networked site. This will be a natural step toward achieving the aims of the National Programme for Information Technology, whereby each patient will have an electronic record. Conclusion Operational costs The Department is now in its fourth year of digital operation. Although it was clear that a substantial saving on material costs would be achieved, 20% of the initial cost per year was estimated to cover maintenance of the equipment. So far, however, photographic equipment repairs have cost £50, and additional software modifications, specifically requested by the hospital, and maintenance charges have cost approximately £2,000. An estimated £45,000 has been saved on material costs over the same period. In its four years, the intranet-based digital imaging system has proven to be reliable and entirely successful for both operators and users. In the Commission for Health Improvement Report it is highlighted as an area of improved patient care within the Hospital. The whole concept has been recognized as an area of best practice by the Department of Health Information Policy Unit and by the Medicines and Healthcare Products Regulatory Agency (Figure 8). Given the importance placed on the photographic service at QVH, where it is an integral part of the clinical support network, it is now difficult to imagine how the department would have survived had digital technology not been implemented. Support and Maintenance Acknowledgements First-level support for the system is provided by the IT Department, including an element of out-of-hours cover. Further support is provided by GCP under an ongoing maintenance agreement with the Trust, with particular regard to software support. Where appropriate, rapid intervention to resolve any problem, including the installation of software upgrades or hotfixes, is carried out by GCP via a secure remote access connection. The maintenance agreement incorporates the ongoing provision of updated versions of the software in respect of both host software, based at the Trust, and client software, based at remote A&E departments and minor injuries units. Dr Nicolas Bowley, Consultant Radiologist, Queen Victoria Hospital; Mr Derek Pocock, Chairman, League of Friends, Queen Victoria Hospital; Mr Ian Chell, Senior Medical Device Specialist, Medicines and Healthcare Products Regulatory Agency. References 1. Dennison EJ. A cottage hospital grown up. East Grinstead, 1963. 2. Jones SM, Balk EJ, Hill TJ, Reynolds S. Setting up a storeand-forward telemedicine service for acute trauma in a hospital trust. J Audiovis Media Med 2004; 27(3): 107–14.









© Copyright 2026