
Document 138495
REVIEW
CONSERVATIVE
TREATMENT
ARTICLE
FOR
IDIOPATHIC
SCOLIOSIS
R. A. DICKSON
Because
idiopathic
gress
during
subdivided
thus
infantile,
ognised
scoliosis
commences
juvenile
(Goldstein
year-old
baby
unquestionably
and
and
with
has
a 60
infantile
adolescent,
idiopathic
many
that juvenile-onset
134 patients
with
tentatively
classified
think
these
worth
(James
1954).
(Mehta
infancy
idiopathic
scoliosis,
untreated
and
and
early
common
for
will
be discussed
IDIOPATHIC
is the
of
course,
disability,
aim;
of surgical
scoliosis
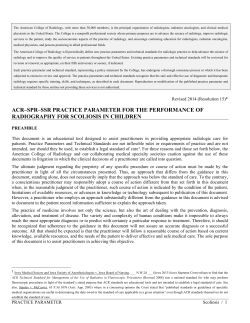
The
I 76
1
Fig.
2
idiopathic
scoliosis-a
very serious
condition
producing
compromise
and horrendous
deformity.
Figure
1Figure
2-Close-up
in the forward-bending
position.
SCOLIOSIS
strategy
this
is the
for
treating
upon
the size of
progression.
If the
then preservation
place
of conserva-
management.
needs
treatment
then
keep it
In order
at all,
to
the
of leaving
it untreated
must be known.
It
known
that scoliosis
can cause
significant
with
economic
implications
(Dahlberg
and
R. A. Dickson,
MA,
ChM.
FRCS,
Professor
and
Head
of
Department
ofOrthopaedic
and Traumatic
Surgery,
The University
Leeds
St Jarness
University
Hospital,
Leeds
LS9 7TF,
England.
(
1985 British
Editorial
Society
of Bone and Joint
Surgery
030l-620X
Fig.
Early-onset
cardiopulmonary
Erect.
first.
If the deformity
is unacceptable,
be to make
it acceptable
and
so;
this is the aim
decide
if idiopathic
is,
and he did not
infantile
group
as the strategy
for treatvery considerably
between
Treatment
for the more
late-onset
case
is more
therefore
treatment.
tive management.
the objective
must
consequences
adolescent-onset
certainly
started
there
is no clear
early-onset
and late1950; Figs
I to 4). The
and the consequences
of
idiopathic
scoliosis
depends
principally
the deformity
and its potential
for
deformity
is acceptable
at presentation,
of acceptability
child;
is an
Such cases may well be a hangover
from
1977). There
is much
merit
therefore
in
and
need
one-
thoracic
curve
classification
as ofjuvenile
onset
separating
from
the
LATE-ONSET
The
rec-
a
idiopathic
scoliosis
exists.
Of
thoracic
scoliosis,
only I 6 were
scoliosis,
as well
its efficacy,
differ
late-onset
types.
and
more
benign
“standard”
pro-
are
While
difficult
the older
the
girl with a 90 curve
considering
only
two categories,
onset
(Ponseti
and
Friedman
prevalence
rate, natural
history
ment
types
1973).
she
does
not
have
scoliosis,
as the deformity
earlier.
Furthermore,
years
may
it has been
(James
1954);
adolescent
Waugh
becomes
progressively
more
and although
a 12-year-old
evidence
James’
and
the period
of spinal
growth,
according
to when
it begins
85/2013
S2.00
the
of
Fig.
3
Fig.
Late-onset
idiopathic
Figure
3-Erect.
Figure
THE
scoliosis-a
4-Close-up
JOURNAL
4
problem
of
deformity
in the forward-bending
OF BONE
AND
JOINT
only.
position.
SURGERY
CONSERVATIVE
Nachemson
1977),
plications
can
(Nachemson
and Ponseti
cases;
and
thoracic
and
be
that
(Davies
deformity
Nachemson’s
only.
differently
from
The
original
by the age
parenchyma
there
are
this
subject
surgeon.
52 late-onset
study
of
their
organic
deformity,
deformity
the
psychological
1968; Bengtsson
obvious
selected
idiopathic
patients
counterparts
more
than
of
As there
treatment
groups
has never been a controlled
trial
its efficacy
can only be deter-
it against
of the
sources
the
little
we know
late-onset
curve.
of information.
of children
who
of the
There
are
Early
studies
presented
to
two
of
scoliosis
programmes
which
(Brooks
et al. 1975;
et al.
non-structural
have included
a longitudinal
survey
Rogala,
Drummond
and Gurr
1978;
1980;
Dickson
1983).
are
excluded,
curves
When
children
with
10%
show
only
evidence
of progression,
whereas
twice as many
improve
and more
than
two-thirds
remain
static.
The greatest
progression
potential
is associated
with the young
girl
who has a right
thoracic
curve,
but she represents
less
than one in a thousand
of those screened.
The difference
between
the data
from
these
two
sources,
although
difficult
to interpret
(Leaver,
Alvik
and Warren
1982),
a change
to a more
benign
natural
history,
and
this is supported
by the observation
that where
a lot of
screening
has been performed
the need for both conservative
and operative
management
has been
much
less
suggests
(Lonstein
el a!.
1982).
Conservative
then be set against
this background.
methods
need
to be discussed:
electrospinal
Brace
While
various
67-B.
No.
2. MARCH
1985
contraptions
used
since
for conservative
brace
(Blount
for
the
the
time
of
treatment
and Schmidt
technology
1980).
for
Although
the
the conservative
scoliosis,
1972;
Moe
that
the
distraction
Galante
between
the head and the
1969; Galante
et al. 1970)
action
dentition
refers
Alexander
or-
1974);
placed
al. 1976).
a clear
purpose
studies
exerting
effects
on
A change
on
reduction
problems
and
led to three-point
emphasis
ci
Riolo
priof
pelvis (Schultz
and
and
this modeof
by the harmful
(Alexander
1966).
and
approach
(Andriacchi
Without
this
brace
was not
management
to the throat
mould
type ofbrace
led to a great
in the distraction
force with no obvious
dental
biomechanical
to
it was soon
used for that
1973).
Early
mechanical
brace
might
function
by
was
corroborated
thereby
produced
a change
fixation
the
in
with
localiser
understanding
of
pad
the
three-
dimensional
nature
of the deformity
it would
be tempting to think
that the brace
might
work
in the manner
described,
but this is not so. The primary
deformity
of
idiopathic
scoliosis
is a lordosis
at the curve
apex
1882;
Somerville
1983, 1984) and
which
produces
ideal ofconservative
1952;
Roaf
it is rotation
the secondary
treatment
1966;
Dickson
al.
ci
of this lordosis
to the side
scoliotic
deformity.
An
would
then be to recreate
the normal
spinal
shape
in the sagittal
plane;
this,
however,
would
imply
flexion,
which
enhances
rotation
and
produces
an increase
in the secondary
scoliotic
deformity.
In contradistinction,
the opposite
deformity,
the kyphosis
of Scheuermann’s
disease,
is ideally
suited
to conservative
management,
because
the deformity
is
rotationally
stable
and braces
which
cause
spinal
extension
produce
a true
physiological
correction
of the
deformity
(Bradford
ci al. 1974).
The brace
is capable,
however,
effect
of
producing
in idiopathic
obliteration
a
small
scoliosis.
of the
lumbar
temporary
Blount
stressed
lordosis
in the
corrective
the need
brace
for
(Blount
and
Moe
1973)
and
this produces
thoracic
extension
above.
There
is now more room
for the thoracic
lordosis
to be accommodated
with a derotation
effect,
but at the
possible
expense
of increasing
the primary
lordosis
(Winter,
Lovell
and Moe
1975; Figs 5 and 6). The other
important
effect of the brace
pelvis
in the erect
position
harmful
effect of flexion.
With this mode
of action
that the optimal
measures
exactly
result
the
is to splint
the spine
which
thus
prevents
it
is not
of brace wearing
same at the end
surprising
to the
the
to find
is when the curve
of treatment
as it
did at the beginning
(Keiser
and
Shuffiebarger
1976;
Edmondson
and Morris
1977; Mellencamp,
Blount
and
Anderson
1977; Tolo and Gillespie
1978: Blount
1981).
These
stimulation.
treatment.
scoliotic
spine
have
been
Hippocrates.
real enthusiasm
started
with the Milwaukee
VoL.
treatment
should
Three
conservative
bracing,
casting
and
Newer
(cervical-thoracic-lumbar-sacral
idiopathic
(Blount
suggested
particular
the
1958).
(Nash
intended
as
clinics
suggested
a considerable
progression
potential
if
the onset
was
under
10 years
of age or before
the
menarche
(Risser
and
Ferguson
1936;
Ponseti
and
Friedman
1950; James
1954; Heine
and
Reher
1975).
More
recent
data
come
from
those
school
screening
Dickson
Blount
as a CTLSO
(Northway,
social
and
Lundgren
opinion
on
that
1957;
thosis)
manly
177
SCOLIOSIS
brace
in
no
1968).
With
regard
that the bigger
the
greater
the
likelihood
of
implications
(Nilsonne
and
ci’ al.
1974).
The patient’s
matters
cases
fared
IDIOPATHIC
(Adams
history
different
quite
130
organic
scoliosis,
even
if
Israel
and
Hall
and
Leatherman
is a problem
of
straight-backed
by evaluating
natural
mortality
of seven
or eight
is developing
no
health
(Nachemson
it is of course
true
clearly
Natural
history.
of conservative
mined
com-
and
consequences
of late-onset
idiopathic
the deformity
exceeds
100
(Kostuik,
1973;
Ponder
ci
al. 1975;
Dickson
1976).
Late-onset
idiopathic
scoliosis
regards
to the
FOR
1968; Nilsonne
and Lundgren
1968; Collis
1969).
But this applies
only to early-onset
then
only
to severe
ones,
for example,
a
and Reid 1971).
contradistinction
In
cardiopulmonary
of morbidity
curve
of over 60
when
the pulmonary
years.
the
a source
TREATMENT
progressed
treatment,
attenuated,
deformities
studies
also
suggest
that
beyond
30
before
the less satisfactorily
as gravity
and the
more
successfully
the
more
the
curve
has
the commencement
of
can curve progression
be
rigidity
of the secondary
defeat
the intentions
of
178
R.
A.
DICKSON
Milwaukee
Stanish
brace
1977;
(Park
Winter
a!.
ci
and
Watts,
1977;
Carlson
1977);
Hall
this
flexion
of these low curves
can be prevented
underarm
brace,
TLSO
(thoracic-lumbar-sacral
sis).
But
the other
mode
of action,
and
is because
even
by an
ortho-
obliteration
of the
lumbar
lordosis,
is more
obvious
and produces
a bigger
temporary
corrective
effect.
There
are no controlled
trials with an underarm
brace and the follow-up
is much
Fig.
shorter
than with a Milwaukee
efficacy
also
is questionable,
lighter
weight
and smaller
size
able to the patient.
5
Another
problem
growth.
The
when
growth
Fig.
6
The effect of obliteration
of the lumbar
lordosis.
Figure
5-A
thoracic
deformity
associated
with
a lumbar
lordosis
viewed
from
above.
Figure
6-The
same
deformity
viewed
from
above
with
the lumbar
lordosis
obliterated.
Marked
derotation
has occurred.
treatment.
The
best
results
of brace
therefore
achieved
with
smaller
curves;
history,
however,
demonstrates
that very
progressed
if left untreated.
treatment
are
their
natural
few would
have
and Copel
I 95 1 ; Inkster
Larsen
and Nordentoft
Recent
studies
when
and
Ponseti
that
the
performed.
on idiopathic
programme
of
spinal
Although
exercises
curves
(Stone
is prescribed
for
out of the
programme
brace
lest the
should
not,
flexion
are
not
usually
have no corrective
effect
ci a!. 1979),
an exercise
the one hour
a day spent
spine become
unduly
stiff; this
however,
include
flexion
exer-
will undo what the brace has been trying
to
for the previous
23 hours.
Set against
the background
of natural
history
there
is no evidence
that Milwaukee
brace treatment
alters
the
course
of the scoliosis.
This is a very serious
matter,
as
cises
as these
achieve
countless
treatment
brace
numbers
for no
on
diluted
or no
girls
of children
detectable
with
progressive
may
benefit.
have endured
If the effect
thoracic
curves
by the inclusion
ofcurves
at other
sites
progression
potential,
then
the lumbar
obliterating
ought
to
Cognisant
and
flexion-preventing
prevent
of this
progression
problem
effect
the
(Dickson
British
Association
and the British
Scoliosis
right to stress
the need for carefully
Society
controlled
of
brace
of the
was
not
with little
lordosisthe
brace
a!. 1984).
Orthopaedic
ci
(1983)
studies
idiopathic
scoliosis,
preferably
throughout
life.
It recently
became
apparent
that low thoracic
lumbar
curves
did not require
the full superstructure
are
of
and
of a
the
duration
of
spinal
the intra-uterine
phase
is during
the adolescent
further
10 years
until the vertebral
epiphyses
are fused
and that the vertebral
apophyses
have nothing
whatever
to do with spinal
growth
nor does their fusion
indicate
cessation
ofgrowth
(Bick,
Copel
and Spector
1950; Bick
etal
cycles
concerns
only
period
after
velocity
increases
growth
spurt,
which
is maximal
at about
the age of 12
years
in girls and
14 in boys
(Scammon
1927).
While
idiopathic
curves
are particularly
liable
to deteriorate
during
this phase,
general
skeletal
maturity
is reached
two
years
later (Tanner
1962). The conventional
time when
the patient
is weaned
from the brace
has been when
the
iliac crest and vertebral
ring apophyses
fuse (Risser
and
Ferguson
1936;
James
1954;
Risser
1964).
It is well
known,
however,
that
spinal
growth
continues
for a
The brace is supposed
to be worn for 23 hours
out of
24, although
it would
appear
to be unnecessary
at night
repeated
brace;
consequently
their
though
of course
their
make
them
more
accept-
of idiopathic
maturity
majority
do,
in fact.
ofcases
curves
and
While
of
not
general
1983;
studies
on
it ought
I 962;
1982).
skel-
progression
Bjerkreim
these
pregnancy
factor,
beyond
demonstrate
(Hassan
1983).
effect
responsible
I 95 1 ; Calvo
1957; Tupman
1962; Bernick
and Caillet
Weinstein
have
ligaments
in the
suggested
might
to be forgotten
be
a
that,
in
young
women,
the spine
is still growing.
Even
if there
was evidence
that
the brace
did prevent
progression,
treatment
would
need to be continued
for much
longer
than the patient
would
tolerate.
Cast
management.
The
pioneers
of
the
treatment
of
obtained
correction
by using
plaster
casts
(Risser
ci al. 1953;
Risser
1955) and it was remarkable
to
what
good
use they put them (Moe
and Valuska
1966).
With the advent
of the Milwaukee
brace,
enthusiasm
for
scoliosis
plaster
in the
many
not
parts
lose
conservative
of the
their
developed
the
as an alternative
faith
EDF
treatment
world.
French
in
plaster
rapidly
surgeons,
waned
in
however,
did
and
have
techniques
(elongation-derotation-flexion)
to brace
treatment
(Cotrel
and
cast
Morel
1964).
The function
of this cast is precisely
that
brace,
with
obliteration
of the lumbar
lordosis
elimination
of spinal
flexion
as the two priorities.
cast is worn
for three
or four months
until its wear
of the
and
Each
or the
patient’s
patients
growth
indicates
that a new one is required.
The
cannot
bathe,
but it is extraordinary
how easy it
is to change
the inner
vest and the underwear
while the
THE
JOURNAL
OF
BONE
AND
JOINT
SURGERY
CONSERVATIVE
is in place.
cast
the concave
anteriorly;
pressure
Furthermore,
the
cast
TREATMENT
has
a window
side posteriorly
and one on the
these facilitate
derotation
exercises
pads
or balloons
to be inserted
rotational
treatment
prominences.
is to finish
Since
up with
the object
the least
FOR
on
convex
side
and allow
over
the
of conservative
deformed
torso,
well to compare
their
end-results
although,
as with the majority
of
questions,
the
answer
has
never
been
by a controlled
study.
Between
casts
a proof non-skeletal
traction
and exercises
is carried
interesting
out (Cotrel
and D’Amore
1968).
This
however,
in terms
of curve
correction
Nordwell
1977; Dickson
and Leatherman
traction
of
its
kind
ofany
provides
any magnitude,
natural
range
Glasgow
of
no real
is of no
(Nachemson
1978).
benefit,
and
Indeed,
correction
of curves
only
moving
each
flexibility
(Edgar,
curve
through
Chapman
and
Recently,
has
1982).
Electrospinal
directed
scoliosis
stimulation.
been
of the
muscula-
attention
towards
obtaining
temporary
correction
by electrical
stimulation
of the spinal
1980).
179
SCOLIOSIS
Here
progression
potential
It was first thought
that
into two types-progressive
upon
the size of the
(RVAD;
“bracers”
would
do
with French
“casters”
elucidated
gramme
IDIOPATHIC
however,
progressive,
RVAD
and
three
static and
ofless
and
1972).
Mehta
confidently
diagnoses
excess
of 20 or one
angle
The
is
picture
then
reduces
small
curves
(Mehta
a definite
progression
The
serious
most
hypotonic,
has been
(Mehta
so
clear,
an
in magnitude
resolving
curve,
an RVAD
in
is increasing
does not necess-
a progressive
curve.
Other
Thoracic
and
thoracolumbar
initial
difference
not
are
now
recognised(Mehta
1977). While
which
the
that
be divided
resolving-depending
arily imply
important.
1980) tend to resolve,
relevant.
could
rib-vertebra
types
resolving
20
than
is particularly
the condition
1977;
while
Thompson
double
potential
factors
and
structural
progression
have
a!.
ci
appears
Bentley
curves
(Ceballos
low birth weight
baby
referred
to as “malignant”
also are
curves
and
1980).
to occur
in the
in whom
the condition
idiopathic
scoliosis
1977).
A very
interesting
trend
has
emerged
over
last
the
35
ture on the convexity
of the curve (Bobechko
1974). Like
the development
oforthotic
and cast treatment,
electrical
stimulation
focuses
on the secondary
coronal-plane
years.
Early
reports
indicated
a great
preponderance
of
the progressive
type
of curve
(James
195 1 ; Scott
and
Morgan
1955; James ci a!. 1959), but this situation
then
changed
dramatically
and the last 20 years
has seen a
deformity
marked
range
of
stemmed
and only
elasticity.
from
moves
the
Furthermore,
the belief
basis
to the
substantiated
deformity,
(Dickson
The
that
fact
bends
to
mild
been
demonstrated
(Bobechko,
Herbert
enjoys,
follows
1 983).
primary
tive
trical
to be
curvatures
in
then
resumes
the
in curve
magnitude
muscle
1979);
surface
to
with
the
deformity,
kyphotic
stimulation
permanent
can,
like
erect
has
stimulation
this demon-
the
uniplanar
however,
brace
(Axelgaard,
correction
and
elec-
or cast,
give
Brown
and
1982).
Natural
history.
IDIOPATHIC
This
fascinating
Holland
(Harrenstein
birth to three years
commonly
than
frequently
Roberts
girls
condition,
1929),
of age.
and
SCOLIOSIS
Wynne-Davies
No.
2. MARCH
1975;
1985
first reported
tends to affect children
Boys are affected
more
thoracic
curves
convex
to the left (James
1951;
and
Pilcher
1959;
Lloyd-Roberts
67-B,
incidence
declined
Thompson
are
more
James,
and
LloydPilcher
and
Bentley
of the
(Lloyd-Roberts
and Bentley
proportions
with
and Pilcher
1980; Ceballos
of these
infantile
and the condition
90%
1965;
ci
a!.
or more
Mau
1968;
1980). The
curves
also
has
is now rare; whether
rapidly
or not
this decline
is due to prone
lying
in the cot is unclear
(McMaster
1983). These
changes
in the natural
history
of early-onset
progressive
idiopathic
scoliosis
are very
welcome,
as these are the curves
associated
with serious
cardiopulmonary
develop
horrifying
Conservative
curves
were
disease
at an
deformities.
early
age,
and
they
also
treatment.
When
malignant
progressive
more
common,
treatment
presented
great
problems.
Progression
potential
was far too great
to be
attenuated
by a Milwaukee
brace (James
ci a!. 1959),
but
posterior
fusion
was withheld
for as long as possible
in
order
to avoid
increasing
the primary
lordosis;
meanwhile the deformity
progressed
inexorably
in the brace.
By
the time posterior
fusion
was performed,
the deformity
was often
too far advanced
for treatment;
moreover,
there is no clear evidence
that fusion
reduced
the rate of
subsequent
McMaster
Unlike
EARLY-ONSET
VOL.
and
treatment;
stable
Swank
1965:
coronal-plane
during
convex
and Friedman
conservative
rotationally
from
from
a neuromuscular
is unlikely
reversal
resolving
Thompson
the innate
flexibility
that the mild idiopathic
curve
but there is no evidence
that any real correction
electrospinal
stimulation
(Axelgaard
and Brown
Again
it is the rotationally
unstable
nature
of the
lordotic
deformity
which
militates
against
effec-
strates
rise
was
its natural
stimulation
by stimulating
muscles
on one
Monticelli
ci a!. 1975; Bobechko,
1976) is not surprising.
This
is
when
someone
with a straight
one side
improvement
Some
position.
there
a belief
which
ci a!. 1984).
animals
can be produced
side (Olsen
ci a!. 1975;
Herbert
and Friedman
precisely
what
happens
spine
that
spine
within
electrical
progression
and Macnicol
late-onset
(Letts
1979).
deformities
and
there
Bobechko
is some
1974;
evidence
that early-onset
idiopathic
scoliosis
can be treated
conservatively.
Mehta,
who has contributed
much
to our
knowledge
of infantile
idiopathic
scoliosis,
recognised
early
the bad prognosis
associated
with the hypotonic
infant,
and the moment
she saw such a child she applied
an elongation-rotation-flexion
(EDF)
cast (Mehta
and
Morel
1979).
Surprisingly.
the occasional
case that had
all the ingredients
for rapid
progression
appeared
to
become
static,
or even to resolve,
and the RVAD
became
180
R.
smaller
or did
not
increase.
This
perhaps
A.
DICKSON
Browne
demonstrates
of obliteration
of the lumbar
lordosis
and the
of flexion
in these very supple
spines;
but the
cast must
also have allowed
the thoracic
spine to become
naturally
kyphotic
in those
that subsequently
resolved.
There
are, clearly,
two important
aspects
of the conservative
prevention
management
and casting.
to whether
the deformity
(Browne
1936)
prone
lying
must
be
infant
does
an
delay
is due
upon,
particularly
1983).
idiopathic
serial
(Mehta
For
all
should
the
that
Collis
Cotrel
of
without
and treatment
oflateral
London:
J & A Churchill
Alexander
RG. The effects
on tooth
position
growth
during
treatment
of scoliosis
Ani J Orthod 1966:52:
161-89.
RA.
Dickson
RA, Lawton
Dickson
vertical
brace.
Axelgaard
surface
electrical
idiopathic
surface
scoliosis.
stimulation
Spine
S.
human
Bick
Caillet
R.
vertebrae.
EM,
Copel
Swank
Orthop
SM.
Kyphosis
Trans
1982:6:1.
EM,
Vertebral
end-plate
Spine
1982;7(2):97-102.
JW.
Contribution
to
1951 :33-A:783-7.
Bick
Copel
The
treatment
WP.
1958:19:
WP.
Blount
for the
1983;8(3):
WP.
scoliosis.
Blount
WP,
Wilkins,
Blount
human
E.
Surg
[Am]
In: Zorab
PA, ed.
scoliosis:
causation.
1968:37-43.
dans
Ia correction
spinal
KD.
Joint
Surg
des
cohort
alveoli
Dis
J 1983:286:615-8.
asymmetry.
Spinal
[Am]
J Bone
deformity
l976:58-A:729.
traction,
a pilot
trial.
scoliosis:
clinical
P, Sharp
A-M,
study
clinical
of
Harker
and
Child
The pathogenesis
IA, et a!. Combined
the
essential
lesion
[Br] 1983:65-B:368.
KD. Cotrel
idiopathic
controlled
RA, Stamper
of
Arch
Archer
Leatherman
J Bone
Br Med
IA, Butt WP.
Biplanar
JO,
JW,
Use
of
Edgar MA, Chapman
by electrical
adolescent
64-B:
530-5.
of female
of
Joint
of
Surg
median
and
idiopathic
in adults:
changing
exercises,
casting
in the
study
and
prospective
Aeta
Orthop
Scand
P. School
course.
Br
screening
for
J 1980:281:
Med
with
aging
of
the
Galante
of the
J Bone
human
Joint
Spector
growth
of
osteogeny.
J Bone
to human
and
the
Milwaukee
brace.
Bull
Joint
brace.
Orthop
Clin
North
WP,
The
virtue
of early
treatment
Joint Surg [Am] 198 I:63-A:335-6.
Moe
JH.
1973.
Schmidt
The
AC.
J Bom’
Milwaukee
The
Joint
Surg
brace.
of
Harrenstein
Dis
Milwaukee
brace
[Am] I957;39-A:693.
ischen
87-96.
idiopathic
Orthopaedic
screening
for
HL,
Azen
prospective
1975 :57-A
in the
SP,
Gerberg
E, Brooks
study.
treatment
Society.
of
Bone
James
James
I. Progression
Reher
Acta
H.
Die
bis
Skoliose
JIP,
RP,
Keiser
Surg
Kostuik
Brash
JC,
London:
ed.
GC,
Shufflebarger
HL.
evaluation
19-24.
of
structural
Pilcher
MF.
The
Milwaukee
completed
brace
cases.
surgery
J Bone
and operative
at onset.
J Bone
Infantile
1959:41-B:719-35.
JP, Israel J, Hall JE. Scoliosis
idiopath1975:113:
scoliosis.
diagnosis
the age
[Br]
123
conser-
Cunningham’s
text-hook
of
Oxford
University
Press.
the prognosis.
patterns
and
Surg
after
unbehandelten
7 Orthop
patterns
in idiopathic
[Br] 1951 :33-B:399-406.
Joint
Behandlung.
structural
in idiopathic
Cliii
Orthop
in adults.
Clin
Orthop
1973 :93: 225-34.
Larsen
a
[Am]
In:
edn.
J Bone
scoliosis:
1976:118:
School
L. Scoliosis:
Joint
Progredienz
der
Wachstumsabschluss.
Lloyd-Roberts
scoliosis.
of scoliosis.
in idiopathic
scoliosis
Scand
1983:54:88-90.
Orthop
JIP. Idiopathic
scoliosis:
indications
related
to curve
Joint Surg [Br] 1954:36-B:36-49.
James
acting
in the
for idiopathic
1-40.
JIP. Two curve
EH, Nordentoft
Orthop
R, Chan
J
1929:52:
treatment.
Joint Surg
Association
and the British
Scoliosis
scoliosis.
Brit Med J 1983:287:963-4.
epidemiological
:968-72.
Chir
RG. Osteology.
anatomy,
9th
195 1: 105-331.
&
Moe
JH, Montalvo
FJ, Winter RB. Scheuermann’s
and roundback
deformity:
results
of Milwaukee
brace
J Bone Joint Surg [Am] l974;56-A:740-58.
Bradford
DS,
kyphosis
treatment.
RJ.
Orthop
J,
Heine
Ray RD. Forces
undergoing
treatment
[Am] l970:52-A:498-506.
brace
Ort hop
1973:93:
1, Bjerkreim
Hassan
Am.
Williams
correction
in
[Br]
1982:
Surg
RL,
on patients
Joint
Surg
Inkster
Baltimore:
Pre-operative
Bone
Joint
TR. Classification
and terminology
10-22.
Die Skoliose
bei S#{228}uglingen und ihre
Orthop
vative
Milwaukee
J
LA, Waugh
Cliii
the human
Joint
Surg
Hosp
MMS.
scoliosis.
A, DeWald
brace
J Bone
scoliosis.
z
the
Editorial.
J Bone
J, Schultz
Milwaukee
vertebra.
Surg
[Am]
S. Longitudinal
RH, Glasgow
idiopathic
Edmondson
AS,
Morris
JT. Follow-up
study
of Milwaukee
treatment
in patients
with
idiopathic
scoliosis.
Clin
1977:126:58-61.
scoliosis
Bobechko
WP. Scoliosis
spinal
pacemakers.
J Bone Joint
Surg
[Am]
l974;56-A:442.
Bobechko
WP, Herbert M, Friedman
H. Electro-spinal
instrumentation. J Bone Joint
Surg [Am] 1976:58-A:
156.
Bobechko
WP, Herbert M, Friedman HG. Electrospinal
instrumentation
for
scoliosis:
current
status.
Orthop
Cli,i
North
Am
1979: 1O(4):927-41.
Brooks
Joint
on growth
ventricle.
community.
Archer
RA. Leatherman
Goldstein
Scoliosis
152-65.
scoliosis.
British
in the
JO,
Lawton
scoliosis:
l972;3:3-16.
Blount
de I’E.D.F
1964:50:59-75.
plane
asymmetry:
J Bone Joint
Surg
treatment
of
randomized
1978 :49:46-8.
A. A psychological
changes
ring
apophysis
osteogeny.
II.
vertebra:
a contribution
[Am] 1950;32-A:803-l4.
Blount
J Bone
265-7.
J, Brown
JC,
stimulation.
Bengtsson
G, Fillstr#{246}mK, Jansson
B, Nachemson
and psychiatric
investigation
of the adjustment
patients.
Acta Psrchiatr
Scand
l974;5O:50-9.
Bernick
RA,
Dickson
RA,
concepts.
Dickson
JC. Lateral
progressive
Orthop
Scoliosis
coronal
scoliosis.
Axelgaard
of
Chir
Dickson
Dickson
J, Brown
G. La technique
Ret’
C, Reid L. Effect
of scoliosis
pulmonary
arteries
and
on
right
1971 :46:623-32.
Andriacchl
TP, Schultz AB, Belytschko
TB, DeWald RL. Milwaukee
brace
correction
of idiopathic
scoliosis:
a biomechanical
analysis
and a retrospective
study.
J Bone Joint
Surg
[Am]
1976:58-A:
806-IS.
treatment
242-60.
spine
F, Fernandez-Paredes
scoliosis.
traction
in scoliosis.
second
svniposium
on
London:
E & S Livingstone.
idiopathic
scoliosis.
[Br] 1984:66-B:8-l5.
and other
& Sons,
and maxillofacial
with the Milwaukee
Castillo
a
and
Y, Morel
Davies
on the pathology
of the spine.
of curvature
M,
idiopathic
M. Spinal
of
scolioses.
R Soc
Dahlberg
L, Nachemson
AL. The economic
aspects
of scoliosis
treatment.
In: Zorab
PA, ed. Scoliosis:
proceedings
ofafif)h
symposium
held at the Cardiothoracic
Institute,
Brompton
Hospital.
London,
on
2/ct,
22nd
September.
1976.
London:
Academic
Press,
1977:73-101.
does
1977).
W. Lectures
forms
1882.
Cotrel
Proc
IV. Long-term
follow-up
of patients
with idiopathic
treated
surgically.
J Bone
Joint
Surg
[Am]
1969:
D’Amore
‘,
Proceedings
Edinburgh
REFERENCES
Adams
DK, Ponseti
origin.
growth
of the female
adolescent
Clin Orthop
1957:10:40-7.
Ferrer-Torrelles
scoliosis
not
51-A:425-45.
it
hallmarks
be applied
T,
of mechanical
on the
to scoliosis.
its relation
Prognosis
in infantile
1980:62-A:
863-75.
hypotonic
case
IJ. Observations
Ceballos
1968),
effect;
the
rare
with
casts
inhibitory
for
the
curve
EDF
an
deformities
1409-31.
I936:29:
and
moulding
in the cot (Mau
to have
Calvo
case,
namely,
continues
as
to intra-uterine
appear
insisted
progression,
the early-onset
Although
debate
or to positioning
(McMaster
develop
of
D. Congenital
Med
the effect
prevention
Leaver
Sca,icl
EL. Growth
I 962:32:210-7.
JM, Alvik A, Warren
ofthe
epiphyses
MD. Prescriptive
idiopathic
scoliosis:
1982:11(2): 101-11.
a review
THE
JOURNAL
of
the
and
screening
evidence.
OF BONE
AND
vertebra.
mt
Acta
for adolescent
J Epidemiol
JOINT
SURGERY
CONSERVATIVE
RM,
Letts
Bobechko
children:
1974:101:
WP.
effects
136-45.
Fusion
prognosis
on
of
the
and
TREATMENT
scoliotic
growth.
Structural
idiopathic
history
of I 00 patients.
McMaster
idiopathic
scoliosis:
l983:65-B:6I2-7.
can
MF. The
of progressive
[Br] l979:6I-B:36-42.
McMaster
tile
Mau
Infantile
Surg [Br]
MJ, Macnicol
idiopathic
scoliosis.
H. Does
infantile
[Br] l968:50-B:88I.
Mehta
MH.
J Bone
scoliosis
Voluntary
Surg [Am]
it be
prevented?
J
DD, Blount WP, Anderson
scoliosis:
treatment?
J Bone
JH, Valuska
J. Evaluation
Monticelli
Nachemson
Acta
by
Clin
Orthop
infan-
[Am]
A. A long
Ort/zop
Seand
Nachemson
A, Nordwell
tion for correction
1977:59-A:
504-8.
GA,
Rosen
of non-treated
Park J, Houtkin
for
Ponder
scoliosis.
CR,
5, Grossman
scoliosis
Dickson
JH,
VOL.
67-B.
No.
2. MARCH
use
a preliminary
PR,
and fusion
Joint Surg [Am]
1985
Joint
Joint
Surg
of
12:
[A;z]
1964:
prognosis.
Joint
Surg
J Bone
Cotrel
Joint
Surg
trac[Ani]
J Bone
Joint
of muscle
report.
Erwin
AB,
Schultz
WD.
Results
of scoliosis.
DS,
Galante
correction
namometers.
Scott
of
Lect
J Bone
Joint
Somerville
JO.
EW.
natural
J Bone
Rotational
curve. J Bone
history
[Br]
growth.
Am
J P/us
forces
exerted
three-component
and
1966:
prognosis
in
the
dy-
of infantile
[Br] l955:37-B:400-13.
Joint Surg
lordosis:
Joint Surg
of
using
Surg
of body
131-42.
incidence
and natural
J Bone Joint
Surg
of human
Measurement
scoliosis
1969:9:419-24.
TH. The
scoliosis.
study.
study
types
1953;10:
Course
Gurr J. Scoliosis:
idiopathic
Exp Mccli
JC, Morgan
idiopathic
the
development
of
the
single
[Br] 1952:34-B:42l-7.
B, Beekman
C, Hall V, Guess
V, Brooks
HL. The effect
of an
exercise
program
on change
in curve
in adolescents
with minimal
idiopathic
scoliosis:
a preliminary
study.
P/irs
Ther
1979:59:
759-63.
JM.
Grout/i
at adolescence
%tith a general
consideration
of the
of hereditary
and environmental
factors
upon growth
and
maturation
Irons
birth
to nuaturitr.
2nd edn.
Oxford:
Blackwell
Scientific
Publications.
1962.
Thompson
Bone
SK,
Joint
and
60-B:
Watts
Bentley
G. Prognosis
Surg [Br] 1980:62-B:
R. The
results
18 1-8.
GS.
of
A study
HG,
to
Hall
Weinstein
of
J
Stanish
RB,
Orthop
particularly
1975:57-B:
in
J
and
Moe JH. Excessive
function
in patients
with
[Am]
I 975 :57-A : 972-7.
R.
Infantile
in the first
138-41.
normal
Bone
idiopathic
Surg
scoliosis.
orthotics
idiopathic
six months
J
scoliosis
[Br]
1978:
children
and
its
Joint
Surg
[Br]
Boston
brace
system
lumbar
scoliosis
by the
Cliii Orthop
1977:126:87-92.
progression
I 983 :65-A :447-55.
Carlson
JM. Modern
1977: 126: 74-86.
Wynne-Davies
ofjuvenile
Bone
Joint
IV. Curve
[Am]
idiopathic
W. The
RB, Lovell WW,
ofpulmonary
Joint
Surg
Winter
characteristics
treatment.
low thoracic
superstructure.
Surg
in infantile
151-4.
of bone
growth
skeletal
maturation.
SL, Ponseti
Joint
Bone
Winter
its
JE,
treatment
of
girdle
without
(Prenyl)
in the adult
idiopathic
1975:57-A:797-80l.
Craig WA. Three
Instruct
seriatim
10:329-36.
1927;
relationship
1962:44-B:42-67.
stimulation
C/in Orthop
brace
DM,
Surg
cijects
1977:126:67-73.
Harrington
Harrington
instrumentation
scoliosis patient. J Bone
J Bone
its
RE. The first
Anthropol
Tanner
scoliosis.
bracing.
J, Levine DB. A modified
Clin Orthop
Scoliosis:
EG, Drummond
Tupman
curves:
AB.
anatomy
Tolo VT, Gillespie
Effectiveness
of preoperative
of idiopathic
scoliosis.
J Bone
H, Stoll 5, Brown G. The
present.
CH, Norquist
basic
786-92.
Scammon
in
by Harrington
: 1656-7.
A.
for inducing
scoliotic
1975:113:198-211.
and
J Bone
of body casts for the correction
insiruct
Course
Lcet
1955:
history:
a prospective
epidemiological
[Ani] 1978:60-A:
173-6.
Stone
Nilsonne
U,
Lundgren
K-D.
Long-term
prognosis
in idiopathic
scoliosis.
Aeta Orthop
Scand
1968:39:456-65.
Northway
RO Jr, Alexander
RG, Riolo ML. A cephalometric
evaluation
of the old Milwaukee
brace
and
the modified
Milwaukee
brace
in relation
to the normal
growing
child.
Am J Ort/zod
1974:65: 34 1-63.
Olsen
Rogala
126:47-57.
treatment
ofscoliosis
1966:48-A
study
CL Jr. Current
concepts
review:
Surg [Am] 1980:62-A:848-52.
past
AcadOrthop
Am
Roaf R. The
Surg
V, Salsano A. Experimental
scoliosis
minimal
electrical
stimulation
in the
Ito! J Orthop
Traumatol
197:1:39-54.
term
follow-up
I 968:39:466-76.
Ferguson
Risser JC, Lauder
E, Salsano
prolonged
muscles.
JC,
48-B:
Joint
brace treatment
1977;
brace
non-operative
1973 :93: 38-43.
oftreatment
Joint
Surg
J Bone
G, Ascani
induced
paravertebral
AJ. Milwaukee
results.
JH. Indications
for Milwaukee
idiopathic
scoliosis.
Clii: Orthop
instrumentation.
Nash
late
Surg
scoliosis.
167-99.
casts.
MH, Morel G. The
non-operative
treatment
of infantile
idiopathic
scoliosis.
In: Zorab
PA. Siegler
D. eds. Scoliosis
1979.
Based
on the proceedings
of the sixth symposium
on scoliosis
held
at the Cardiothoracic
Institute,
Brompton
Hospital,
London,
on
September
17 and 18. 1979. London:
Academic
Press,
1980:71-84.
Moe
JC. Scoliosis:
Risser
Mehta
of idiopathic
the application
Aead
On/zap
Ani
46-A:
rib-vertebra
angle
in the early
diagnosis
between
resolving
progressive
infantile
scoliosis.
J Bone Joint Surg [Br]
1972:54-B:
230-43.
Mehta MH. The natural
history
of infantile
idiopathic
scoliosis.
In:
Zorab
PA, ed. Scoliosis:
proceedings
of a fifth
.n’mposium
held at
the Cardiothoracic
Institute,
Brompton
Hospital.
London,
on 21st,
22nd September.
1976. London:
Academic
Press,
1977 : 103-22.
Moe
JC. Scoliosis:
in idiopathic
1936: 18:667-70.
management
Joint
Surg
require
B. Prognosis
1950:32-A:38l-95.
scoliosis.
255-9.
The
and
Mellencamp
IV, Friedman
Risser
RP.
Joint
181
SCOLIOSIS
Surg [Am]
scoliosis
in
J Bone Joint
Nelson
J Bone
MJ.
Ponseti
spine
in young
Clin
Ort hop
Lonstein
JE,
Bjorklund
5, Wanninger
MH,
school
screening
for scoliosis
in Minnesota.
1982 :64-A : 48 1-8.
Joint
IDIOPATHIC
Risser
Lloyd-Roberts
GC,
Pitcher
MF.
infancy:
a study of the natural
Surg [Br] 1965:47-B:52&-3.
Bone
FOR
in idiopathic
scoliosis.
thoracic
idiopathic
lordosis
scoliosis.
for spinal
deformities.
scoliosis:
ca usative
of life. J Bone Joint
for the
use of a
J
and loss
J Bone
C/in
factors,
Surg [Br]









© Copyright 2026