
Malabsorption syndrome due to various causes is associated with antroduodenal hypomotility
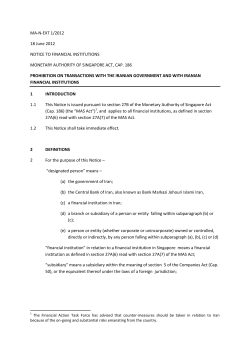
Original Article Malabsorption syndrome due to various causes is associated with antroduodenal hypomotility Kshaunish Das, Sanjeev Sachdeva, Asha Misra, Uday C Ghoshal Department of Gastroenterology, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow 226 014 Background: Patients with celiac disease who present with symptoms of gastrointestinal hypomotility have abnormal antroduodenal manometry. There are no data on antroduodenal manometry in malabsorption syndrome (MAS) due to causes other than celiac disease. Methods: Fasting, post-prandial and post octreotide antroduodenal motility parameters were compared in 18 untreated patients with MAS presenting with chronic diarrhea (tropical sprue 10, small bowel bacterial overgrowth 3, celiac disease 2, common variable immunodeficiency 1, AIDS with isosporidiasis and bacterial overgrowth 1, giardiasis 1) and 8 healthy subjects. Results: Number of patients with MAS and controls having spontaneous migratory motor complexes (MMC) during fasting was comparable (11/18 vs 7/8; p=ns). Fasting contraction amplitude was weaker in MAS than in controls in the gastric antrum (median 42 [range 17-90] vs 80 [31-120] mmHg; p=0.001), proximal duodenum (50 [18-125] vs 72 [48 107]; p=0.013) and distal duodenum (45 [20-81] vs 76 [51-98]; p=0.001). In the fed state too, contraction amplitudes were weaker in patients with MAS in the antrum (32 [15-110] vs 76 [61-103] mmHg, p=0.002), proximal duodenum (57 [20-177] vs 73 [56-113]; p=0.07) and distal duodenum (45 [24-87] vs 75 [66-97]; p<0.0001). Patients with MAS had lower fasting and post-prandial antral and duodenal motility indices than healthy subjects. Intravenous octreotide induced MMC in all patients and controls. Conclusions: MAS due to various causes is associated with antroduodenal hypomotility typical of myopathic disorders. [Indian J Gastroenterol 2006;25:58-61] T he small bowel in patients with malabsorption syndrome (MAS) is frequently dilated and has excessive fluid in the lumen. This has clinical significance as evidenced by reports of patients with celiac disease presenting with intestinal pseudo obstruction that improved with gluten-free diet, 1,2 and frequent finding of secondary small intestinal bacterial overgrowth (SIBO) that may transiently respond to antibiotics in patients with MAS due to various causes. 3,4,5 SIBO in MAS due to another cause may result in refractoriness to treatment directed towards the primary cause. 5,6 Copyright © 2006 by Indian Society of Gastroenterology Though a few reports from Western countries have described multiple abnormalities in both fasting and fed-state antroduodenal manometry (ADM) in patients with MAS due to celiac disease,7,8 most of them had symptoms of gastrointestinal hypomotility instead of chronic small bowel diarrhea. Further, there is no study on ADM in patients with MAS from the tropics, where causes of MAS are heterogeneous. We studied ADM in patients with MAS due to various causes presenting with chronic small bowel diarrhea. Methods Eighteen consecutive patients with MAS due to vari ous causes attending the Luminal Gastroenterology Clinic at our tertiary center and agreeing to partici pate in this study were included. Patients with un controlled diabetes mellitus, chronic renal failure or small intestinal stricture on barium small bowel se ries were excluded. MAS was diagnosed based on clinical presentation, absorption defect of two unre lated substances such as abnormal 5-g D-xylose test (normal <1 g/5 g/5 h) and increased fecal fat excre tion (normal <7 g/d on 72-h estimation using van de Kamer’s method [n=16] or <10/high power field on Sudan III–stain on spot stool specimen [n=10]). The cause of MAS was investigated using a standard protocol described previously. 9 Eight healthy sub jects were studied as controls. Patients and controls underwent ADM after in formed consent. Drugs that may influence gas troduodenal motility and antibiotics were not used within the previous four weeks; none of the patients with MAS received specific treatment before ADM. Our institution’s ethics committee approved the study. Antroduodenal manometry ADM was done after an overnight fast using a wa ter-perfusion system and a low-compliance polyvi nyl catheter (Redtech, Calabasas, CA, USA). The catheter, with eight sideholes placed 3 cm apart from each other, was passed through the nose without any sedation or anesthesia, over a guidewire, and was positioned under fluoroscopy such that at least two proximal ports were in the antrum and the re maining ports were in the duodenum. Das, Sachdeva, Misra, Ghoshal Antroduodenal manometry in malabsorption Fasting motility was recorded for at least 120 min. A meal containing approximately 450 KCal (60% carbohydrate, 15%-20% each of fat and protein) was then given, followed by post-prandial motility recording for at least 90 min. At this stage, 50 μg octreotide (Octride; Sun Pharma, India) was given intravenously over 2-3 min and antroduodenal motil ity was recorded for at least 30 min. The signal was visually scanned to remove ar tifacts (e.g., those due to cough), filtered (9 and 24/ min for antral and duodenal frequency limits, re spectively), and then analyzed (by UCG) using GiPC motility software (Redtech). In the fasting record, presence of spontaneous migratory motor complex (MMC) and its duration was looked for. Post-pran dial record was evaluated for conversion from fast ing to fed pattern. Amplitude of contractions in the antrum and proximal and distal duodenum was mea sured using average of all ports in antrum, proximal two and the remaining ports in duodenum, respec tively. MMC in the duodenal ports after octreotide injection were analyzed similarly. Manometric patterns were defined using estab lished criteria. 10 Motility index (MI) for every 15 minute period during fasting and post-prandial phase was calculated as described previously using the GiPC software. 11 MI in the antrum and proximal and dis tal duodenum was calculated using average values of all ports in antrum, proximal two and the remain ing ports in duodenum, respectively. Average values in the second 15-min period in fasting and post-meal periods were compared between patients and con trols. Statistical analysis Categorical and continuous variables were analyzed using chi-squared test with Yates’ correction and Mann-Whitney U test, respectively. Alpha value of 0.05 was considered as significant. Results Patients with MAS and controls were comparable in age (42 [20-67] vs 33 [26-48] y) and gender distri bution (13 vs 8 males). All patients presented with chronic diarrhea. Causes of MAS included tropical sprue (n=10), SIBO (3; systemic lupus erythemato sus, peripheral vasculitis and jejunal diverticulae in one each), celiac disease (2), common variable im munodeficiency (1), acquired immunodeficiency syndrome with isosporidiasis and SIBO (1), and giardiasis (1). Median urinary D-xylose excretion, number of fat droplets on Sudan III-stained spot stool specimens and 24-h fecal fat excretion were 0.48 g/5 g/5 h (range: 0.16 to 0.79), 16 (6-35) droplets per high power field, and 8.0 g/24 h (4.8 14.4), respectively. Of the 16 patients in whom fecal fat excretion was estimated quantitatively, four had normal value (<7.0 g/d); however, they had abnor mal number of fat droplets on Sudan III staining. Antroduodenal manometry (Table 1, Fig.) The median duration of fasting record in patients with MAS and controls was comparable (160 [range 120-186] vs 147 [120-180] min; p=0.94). Spontane ous MMC was observed as frequently in patients as in controls. The duration of spontaneous MMC in the fasting state in patients with MAS and controls was comparable. Fasting contraction amplitude was weaker in MAS than in controls, in the antrum and duodenum. In the fasting state, discrete clustered contraction (DCC) was observed in one patient with MAS (Fig. 1D) and none of the controls. After meal ingestion, fed pattern was observed in all study subjects except in one patient; this pa tient showed DCC during the fed state (Fig. 1D). In two other patients, the fed pattern was prematurely interrupted after 25 min and 30 min by DCC and a spontaneous MMC, respectively. In the fed state, contraction amplitude in antrum and duodenum were weaker in MAS. Table 1: Manometry parameters in patients with malabsorp tion syndrome (MAS) and controls Parameters MAS (n =18) Healthy subjects p (n = 8) value Presence of spontaneous MMC while fasting 11/18 7/8 ns Duration of spontaneous MMC (min) 6 (2-9) 8 (4 -12) 0.07 Fasting antral amplitude (mmHg) 42 (17-90) 80 (31-120) 0.001 Fasting duodenal amplitude (mmHg) Proximal 50 (18-125) 72 (48-107) 0.013 Distal 45 (20-81) 76 (51-98) 0.001 Conversion to fed pattern after meal 17/18 8/8 ns Post-prandial antral amplitude (mmHg) 32 (15-110) 76 (61-103) 0.002 Post-prandial duodenal amplitude (mmHg) Proximal 58 (21-177) 73 (56-113) 0.07 Distal 45 (25-87) 75 (66-97) <0.0001 Onset of MMC with octreotide 18/18 8/8 ns Duration of post-octreotide MMC (min) 9 (2-21) 15 (6-17) 0.08 Amplitude of post-octreotide MMC (mmHg) Proximal duodenum 30 (12-76) 63 (43-78) 0.003 Distal duodenum 27 (13-59) 64 (45-75) <0.0001 MMC: Migratory motor complex Indian Journal of Gastroenterology 2006 Vol 25 March - April 59 Das, Sachdeva, Misra, Ghoshal Antroduodenal manometry in malabsorption Fig: Tracings of antroduodenal manometry: (A) Healthy subject. Later part of fasting record depicts spontaneous migratory motor complex (MMC). Note that meal resulted in fed pattern and octreotide (oc) induced MMC. “sm” and “em” stand for starting and ending of meal, respectively. (B) Patient with malabsorption syndrome (MAS). Note there is no spontaneous MMC but intravenous octreotide (“oc”) induced MMC. Also note contractions are of lesser amplitude as compared with healthy subject. (C) Patient with MAS (post-prandial record). Though meal resulted in post-prandial pattern, it was for short period and was followed by MMC. (D) Patient with MAS (post-prandial record). Note discrete clustered contractions (DCC) instead of normal post-prandial pattern. Values in X-axis denote time in minutes and in Y-axis denote highest limit of contraction amplitude for respective port in mmHg Octreotide led to induction of MMC in all patients and controls. The amplitude of octreotide-induced MMC was weaker in patients than in controls though the duration of MMC and frequency of contractions during MMC (median: 10 per min) were comparable. In two patients with MAS and none of the controls the duration of post-octreotide MMC was shorter than 5 min. One patient and no control had retrograde contractions with vomiting during the study. Both fasting and fed-state motility indices were Table 2: Motility indices (MI) in patients with malabsorption syndrome and healthy controls Parameters MAS Healthy subjects p (n =18) (n = 8) value 138 (52-268) 191 (153-284) 0.01 Fasting antral MI Fasting duodenal MI Proximal 148 (48-351) Distal 133 (84-340) Post-prandial antral MI 150 (23-408) Post-prandial duodenal MI Proximal 152 (82-285) Distal 142 (81-261) 199 (176-287) 205 (184-274) 0.01 0.002 284 (178-368) 0.001 290 (196-393) 269 (236-398) <0.0001 <0.0001 lower in patients than in controls (Table 2). Discussion This study shows that patients with MAS due to various causes often have abnormalities of ADM in the form of reduced amplitude of contractions in fasting and post-prandial states both in the antrum and duodenum, and reduced motility index. Similar observations have been reported previ ously in two studies, one each in children 7 and in adults. 8 However, all these patients had celiac dis ease. Moreover, most of these patients presented with symptoms of gastrointestinal dysmotility rather than chronic diarrhea. Ours is perhaps the first study from the tropics on ADM in patients with MAS due to other causes, particularly tropical sprue; further, all our patients presented with chronic diarrhea and not symptoms of gastrointestinal dysmotility. The motility abnormalities found in this study are quite expected. The small bowel in patients with MAS is usually atonic with dilatation and increase in luminal fluid. 12 Reduced amplitude of contractions 60 Indian Journal of Gastroenterology 2006 Vol 25 March - April Das, Sachdeva, Misra, Ghoshal Antroduodenal manometry in malabsorption and reduced MI found in the present study are as sociated with myopathic conditions of the gut. 13 Since myopathy is associated with reduced propulsive movement, these results may explain the dilatation of the gut in patients with MAS. We presume that abnormal ADM is associated with diffuse motility abnormality of the whole small bowel.12 This may also explain the prolonged oro-cecal transit time (OCTT) that is known to be associated with sec ondary bacterial overgrowth, in patients with MAS due to tropical sprue 4 and celiac disease. 14 Since previous reports documented that this prolonged OCTT may normalize after specific treatment directed to wards these diseases, 4,14 further work is needed to evaluate whether such normalization is associated with correction of ADM abnormalities. The pathogenesis of this altered antroduodenal motility in patients with MAS is unclear. It may be related to chronic inflammation, immune-mediated changes, alteration in mast cells, or changes in enteric neuropeptides, all of which have been proposed to explain intestinal hypomotility observed in a few patients with celiac disease. 7,8 Induction of MMC in most patients with MAS by intravenous injection of octreotide is another interesting finding in this study. Absence of MMC may be associated with SIBO, 1 5 which often complicates MAS due to various causes 3 and poses special problems in diagnosis and management of these patients. 5,6 In fact, octreotide has been used in the treatment of refractory diarrhea and SIBO. 16,17 Our study documents that even in the presence of marked antroduodenal hypomotility, the gut responds to intravenous octreotide by generating MMC, though somewhat weaker and shorter than in healthy subjects. In conclusion, we have shown that patients with MAS exhibit fasting and fed-state antroduodenal hypomotility; such manometric abnormalities in patients with tropical sprue have not been reported previously. Antroduodenal hypomotility may have pathophysiological significance as prolonged OCTT is common in these patients, which might result in SIBO. References 1. Dawson DJ, Sciberras CM, Whitwell H. Celiac disease presenting with intestinal pseudo-obstruction. Gut 1984;25:1003-8. 2. Stranghellini V, Corinaldesi R, Ghidini C, Ricci Maccarini M, De Giorgio R, Biasco G, et al. Reversibility of gas trointestinal motor abnormalities in chronic intestinal pseudo obstruction. Hepatogastroenterology 1992;39:34-8. 3. Ghoshal U, Ghoshal UC, Ranjan P, Naik SR, Ayyagari A. Spectrum of antibiotic sensitivity of bacteria contaminating upper gut in patients with malabsorption syndrome in the tropics. BMC Gastroenterol 2003;3:9. 4. Ghoshal UC, Ghoshal U, Ayyagari A, Ranjan P, Krishnani N, Misra A, et al. Tropical sprue is associated with con tamination of small bowel with aerobic bacteria and revers ible prolongation of orocaecal transit time. J Gastroenterol Hepatol 2003;18:540-7. 5. Ghoshal UC, Ghoshal U, Misra A, Choudhuri G. Partially responsive celiac disease resulting from small intestinal bacterial overgrowth and lactose intolerance. BMC Gastroenterol 2004;4:10. 6. Tursi A, Brandimarte G, Giorgetti GM. High prevalence of small intestinal bacterial overgrowth in celiac patients with persistence of gastrointestinal symptoms after gluten with drawal. Am J Gastroenterol 2003;98:839-43. 7. Cucchiara S, Bassotti G, Castellucci G, Minella R, Betti C, Fusaro C, et al. Upper gastrointestinal motor abnormalities in children with active celiac disease. J Ped Gastroenterol Nutr 1995;21:435-42. 8. Bassotti G, Castellucci G, Betti C, Fusaro C, Bertotto A, Spinozzi F, et al. Abnormal gastrointestinal motility in patients with celiac sprue. Dig Dis Sci 1994;39:1947-54. 9. Ranjan P, Ghoshal UC, Aggarwal R, Pandey R, Misra A, Naik S, et al. Etiological spectrum of sporadic malabsorp tion syndrome in northern Indian adults at a tertiary hos pital. Indian J Gastroenterol 2004;23:94-8. 10. Kellow JE. Small intestine: Normal function and clinical disorders, manometry. In: Schuster MM, Crowell MD, Koch KL, Eds. Schuster Atlas of Gastrointestinal Motility in Health and Disease. London: BC Decker. 2002: p. 219 36. 11. Camilleri M, Malagelada JR, Brown ML, Becker G, Zinsmeister AR. Relation between antral motility and gas tric emptying of solids and liquids in humans. Am J Physiol 1985;249:G580-G585. 12. Losowsky MS, Walker BE, Kelleher J. Malabsorption in Clinical Practice. New York: Churchill Livingstone. 1974: p. 105-41. 13. Wingate DL. Small bowel manometry. Am J Gastroenterol 1995;90:536-9. 14. Chiarioni G, Bassotti G, Germani UGO, Battaglia E, Brentegani MT, Morelli A, et al.. Gluten-free diet normalizes mouth to-cecum transit of a caloric meal in adult patients with celiac disease. Dig Dis Sci 1997;42:2100-5. 15. Pimentel M, Soffer EE, Chow EJ, Kong Y, Lin HC. Lower frequency of MMC is found in IBS subjects with abnormal lactulose breath test, suggesting bacterial overgrowth. Dig Dis Sci 2002;47:2639-43. 16. Neild PJ, Evans DF, Castillo FD, Newson R, Yasaki ET, Wingate DL, et al. Effect of octreotide on small intestinal motility in HIV-infected patients with chronic refractory diarrhea. Dig Dis Sci 2001;46:2636-42. 17. Soudah HC, Hasler WL, Owyang C. Effect of octreotide on intestinal motility and bacterial overgrowth in scleroderma. N Engl J Med 1991;325:1461-9. Correspondence to: Dr Ghoshal, Associate Professor. Fax: (522) 266 8017, 266 8078. E-mail: [email protected] Received July 15, 2005. Received in final revised form October 22, 2005. Accepted November 8, 2005 Indian Journal of Gastroenterology 2006 Vol 25 March - April 61











© Copyright 2026