
Similarities between Congenital Tritan Defects and
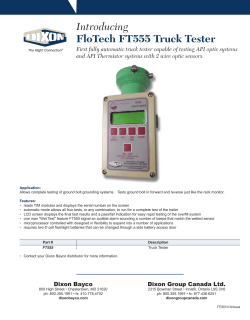
VOLUME 60, NUMBER 8 JOURNAL OF TIHE OPTICAL SOCIETY OF AMERICA AUGUST 1970 Similarities between Congenital Tritan Defects and Dominant Optic-Nerve Atrophy: Coincidence or Identity?* ALEXE. KRILL,VIVIANNEC. SMITH,ANDJOELPOKORNY Eye Research Laboratories, The University of Chicago, Chicago, Illinois 60637 (Received 2 January, 1970) Dominant inherited optic atrophy is usually a stationary disorder with typical findings of optic-nerve pallor, abnormal distance acuity but essentially normal reading vision, minimal visual-field defect, and characteristic color confusions in the blue-green region of the spectrum. The severity of these is extremely variable, even within the same family. In patients with minimal disease, distance acuity may be close to normal and optic pallor may be so subtle that a definitive diagnosis cannot be made unless several affected members of a family are seen. An evaluation of ocular- and color-vision findings are presented for three pedigrees. Color tests included determination of the Rayleigh equation, the American Optical HRR plates, the Farnsworth-Munsell 100-hue test, and determination of netural points and chromaticity confusions. Our results suggest a strong similarity in color vision between previously reported congenital tritan defects and patients with dominantly inherited optic atrophy. Criteria distinguishing the two conditions are suggested. However, a perusal of the literature reveals that most congenital tritanopes were not adequately evaluated to rule out dominantly inherited optic atrophy. Therefore, the almost identical color-vision profiles and pattern of inheritance of the two conditions lead us to question the existence of congenital tritan defect as an independent entity. Vision; Color. INDEXHEADINGS: Many workers with a major interest in color blindness, including ourselves, have never seen a patient with congenital tritanopia. Included in this groupl are Alpern, Linksz, Frangois, Blackwell, and Rubin, who have all written on the subject of color blindness. Trendelenburg,2 who described methods for discovering and testing tritanopes, could not find a single typical case, nor could Pitt, 3 who discussed the properties of tritanopia. This is surprising if the incidence is really somewhere between 1/10 000 and 1/65 000 as Wright, 4 Kalmus, 5 6 and Schmidt claim. Furthermore, since according to Wright, 4 tritanopes know they are color defective, 7 it would be anticipated that at least some of the workers cited above would have seen a tritanope since they have screened populations for color blindness and have searched for color defectives by advertising. A possible explanation may be that there is a subtle retinal or optic-nerve disease with the color-vision defect described for congenital tritanopia, which may visual-field defects. Finally, the condition is usually stationary or only mildly and slowly progressive. The incidence of this disease is close to 1/50 000, which is in the range reported for congenital tritanopia. The inheritance of both conditions is autosomal dominant with frequent intrafamilial and as well as interfamilial variation in manifestation. No other optic-nerve abnormality and only a few retinal abnormalities have dominant inheritance.13-15 Those retinal diseases with this type of inheritance, such as vitelliruptive macular degeneration,' or some cases of retinitis pigmentosa, almost always have obvious visual complaints, if they have a significant color defect, and show obvious progression with time. In hereditary dominant optic atrophy, not only may affected individuals believe that their eyes are normal, but an examiner may miss the diagnosis, particularly in mild cases, which are frequent. This is likely to be so if the examiner relies on the history of the patient and tests only near vision. Distance acuity may be as good as 20/30 or better and therefore not considered to be We intend to explore this possibility in this paper. It is our feeling that the only disease that has all the abnormal. In a few patients, distance acuity may be 8 9 characteristics described for congenital tritanopia is normal. ' Visual fields, tested in the usual clinical hereditary dominant optic atrophy. This condition is manner, frequently show only mild abnormalities, or at characterized by a pallor of the optic nerve. The visual times, appear normal. Even the optic nerve may show acuity and visual fields may be normal or close to only questionable pallor or appear normal in some normal so that the affected individual claims to have individuals. Therefore, it is of vital importance to examine the optic disks of more than one member of an good vision with no eye disease. In his color vision, the patient shows a blue-yellow defect and either he or his affected family (even those who claim to be normal) relatives usually notice this color problem. The patient because some members usually show obvious opticwith hereditary dominant optic atrophy may not be nerve pathology. In the past, it has been emphasized that patients aware of a visual problem, other than a color defect, for several reasons.-- 3 First, the disease usually begins with dominant optic-nerve atrophy often show blueearly in life, possibly even at birth. Often there is very color-vision abnormalities, but usually testing of color little impairment of acuity, particularly for reading. vision was limited to use of the pseudoisochromatic These patients do not complain of nightblindness or plates. We have had the opportunity to determine have been called congenital tritanopia by some workers. 1132 August 1970 TRITAN DEFECTS AND DOMINANT OPTIC ATROPHY 1 133 TABLE I. Visual-screening results. Age Distance vision Near vision IIb hIg IIi 32 39 34 20/25 20/60 20/30 J1 J1 J1 IIIk 14 20/60 J2 III1 Illm IIIn 9 11 13 20/200 20/200 20/80 44 15 24 17 38 12 11 Case Visual fields Optic nerve Defect unknown Family 1 ... ... ... *-. T.P.C N T.P. Yes, Yes, Yes, T.P.? Yese J4 J5 J2 *.. *.. ... T.P. T.P. N Yesf 20/30 20/30 20/200 20/100 J1 J1 J7 J6 Na ... C.S.b C.S. T.P. T.P. RE?d T.P. T.P. RE Yese Yese 20/30, 20/25 20/40 20/60 JP J1 J1 T.P. T.P. RE? P. Yeso Yesf Yes, Family 2 lb Ilc Ild Ile Yesf Family 3 lIb IIIa IIIb a b e Normal. d Central scotoma. Temporal pallor. e N N N Right eye. Visualabnormality detected at eye clinic. f Visualabnormality detected by schoolscreening. neutral points and confusion colors, in addition to some Family 3 was also referred for electroretinography of the usual clinical tests, in several families with this condition. The purpose of this report is to show that the color vision abnormality in some individuals with hereditary dominant optic atrophy is identical to that reported for congenital tritanopia. because the cause of abnormal acuity in subject IIIa was uncertain. She was thought to be normal until she failed a screening examination in school. On initial evaluation, we were uncertain of the diagnosis; however, optic-nerve pallor was obvious in both this girl's sister (IIIb) and her father (.IIb). Most of the subjects who were unaware of abnormal visual acuity and an optic-nerve disease nevertheless SUBJECTS Figure 1 shows pedigrees for three families with dominant optic-nerve atrophy. The visual data are summarized in Table I. Family 1 was first seen because three children (IIIi, HIm, and IIIn) failed visual-screening examinations in school and the referring ophthalmologist wanted confirmation of his impression of optic atrophy in at least two of these three individuals. By history, two of the three individuals (IIIi and IIIm) were known to have had abnormal vision since early childhood. One (IlIn) was thought to be normal until he failed a screening examination in school. Six other members of this family were examined at our clinic and four were considered to have the disease (Fig. 1 and Table I). One member of family 2 (IId) was initially seen in 1958 because of unexplained low acuity. This boy was thought to be normal until he failed a visual test in school. A diagnosis of optic-nerve atrophy in this patient was not made and he was referred for an electroretinogram (ERG) in the hope that some insight would be gained into the cause of the visual loss. It was learned that his sister (IIc) was known to have had abnormal vision since early childhood. The diagnosis of hereditary optic atrophy was uncertain in subject IId until subject IIc was examined. Furthermore, the father was found to have the same condition, although he claimed to be normal. were aware of some color-vision difficulty, or their relatives pointed this out. METHOD Distant visual acuity was tested with Snellen letters projected 6 m from the subject with an American Fcmily No. 1 I a b e-f b a c d e g h , j k Family No 2 I m Family No 3 7 a b b c &> I U a d 3? 5? a becd n e f a b ? 01 b c d L a b c e d? d e ? FIG. 1. Pedigrees for three families with hereditary dominant optic atrophy: *, N, female or male with tritanopia; @, 62, female or male with tritanomaly; 0i, poor vision known; ', color-vision data not reliable; l, G, female or male with optic atrophy, no color-vision testing; \/, examined; ?, status uncertain; = cousin marriage; o sex unknown. KRILL, SMITH, AND POKORNY Optical projection lantern. Near vision was evaluated with a Lebensohn chart. The test distance varied from 23 to 33 cm dependent on the size of the individual.' 7 Both distant and near vision were tested with the bestpossible refractive correction. Visual fields were done in six subjects (Table I) with the Goldmann perimeter. This intrument employs a projection device and a self-recording method with a controlled spot of light as a target. The contrast between target and background illumination can be varied by a series of neutral-density filters. The projected target size can be varied from 1/16 to 64 mm and red, green, and blue filters can be interposed. Fixation of the subject is observed through a peephole in the instrument. In the six subjects tested, only the white light was used and the smallest target size used was 1/4 mm (1.8'). Dark adaptation was evaluated in subjects IlIm of family 1 and IId of family 2. An ERG was obtained from subjects II~m of family 1, IId of family 2, and IIIb of family 3. The methods used for dark adaptation and the ERG are described elsewhere.' 8 -20 The color-vision tests used included the FarnsworthMunsell 100-hue test, the Nagel anomaloscope, the American Optical Hardy-Rand-Rittler pseudoisochromatic plates and the determination of neutral points and confusion colors. The Farnsworth-Munsell 100-hue test was given and evaluated in the usual manner described in the directions that accompany this test. It was administered monocularly under a Macbeth easel lamp that provided a white light with color temperature of 6740 K. In scoring the 100-hue test, we considered both the total errors and the regions of greatest concentration. In general, the number of errors on this test increases with Vol. 60 field, as well as the yellow luminance, was noted. At least five red-green ratios, covering the full range of the instrument, were evaluated. Between each pair of matches the subject was light adapted for 10 s. Our normal subjects were volunteers or patients with normal acuity and color vision. The average midpoint for an equation was a red-green ratio setting of 50 with a range of 44 to 54 on the Nagel scale varying from 0 (green) to 73 (red). Any median setting outside this range was considered to be abnormal, as was a match width greater than 5 units on the Nagel scale. For the determination of color confusions and the neutral point, the patient observed a 30 bipartite field presented within a 10° surround.2 The 3° bipartite field was illuminated by the outputs of two Bausch & Lomb grating monochromators. The 100 surround was illuminated by a tungsten lamp with a color temperature of 2500 K and maintained at a constant retinal illuminance of 16 td. For the determination experimenter of color confusions, the set different wavelengths on each side of the bipartite field. One side was set at a standard retinal illuminance of 16 td and the other side was varied in luminance. The patient was asked to name the colors of the lights on each side, to state whether both sides of the field had the same brightness, and to indicate whether both sides of the field had the same color. Initially, 420 nm at 16 td was set on one half of the field and 530 nm (variable luminance) was set on the other half of the field. If no manipulation of luminance at 530 nm resulted in a judgment of "same color," the wavelength of the 530-nm field was changed to 520 nm age,2 ' but our oldest subject was only 44 (Table I). A total error score greater than 110 was considered to be and the procedure was repeated. Various pairs of wavelengths between 420 and 530 nm were presented in a similar way until the experimenter determined whether a color match could be established. For the determination of the neutral point, the 3° abnormal, for the subjects studied. The axis for a field was filled entirely by the output of a single mono- specific region of errors was a line drawn through the center of this area. According to Farnsworth, 2 2 a tritan axis is centered near the vertical meridian, a protan chromator, and the patient compared the color of the 30 field with that of the 100 surround. The experimenter set a wavelength and the patient was asked to name axis near the horizontal meridian, and a deutan axis in the color of the central field, to state if the central field the oblique meridian bisecting the area between caps and surround were of equal brightness, and to indicate if the central field and surround were of the same color. A number of wavelengths were presented in turn in the central field to establish the reliability of color naming by the patient. 56 and 61. Anomaloscopic evaluation consisted of fixed matches by all patients. In a fixed match, the examiner sets the dial controlling the mixture of red and green and the subject attempts to make brightness, and when possible, color matches by moving the dial controlling the luminance of the yellow half of the bipartite circular field. Five minutes of light adaptation preceded testing. The range of red-green ratios was determined for which the subject matched the two halves of the circular field in color and brightness. The midpoint, as well as the width (range) of the color and brightness-match area, was noted. Where only brightness matches could be made, the subject's color name for both halves of the RESULTS A. Visual Acuity Of the 14 individuals thought to be affected, nine had distance acuity equal to or better than 20/60. None of the nine subjects had 20/20 acuity, but all except one (family 1, IIIk) were able to read the normal line (JI) on the Lebensohn chart at the near test distance. Even this individual was able to read down to J2, a August1970 TRITAN DEFECTS AND DOMINANT OPTIC ATROPHY TABLE F-M 100-hue test Case Age Errors Axis 1135 II. Color-vision findings. AO-HRR plates screen diagnostic BY BY RG Nagel equation RE: 580-585 nm LE: 581 nm 580-585 nm None ... ... RE: None Neutral point Color match Family 1 Ilb 32 ... IIg 39 Iii IlIk 34 14 RE: 447 LE: 318 220 RE: 591 HE11 HIm IIIn 9 11 13 Unreliable Unreliable RE: 245 ... LE: 644 ... Ta 1 0 0 T T 2 2 1 4 1 4 RE: 50-54 LE: 48-53 43-52 RE: 46-S51 0 Unreliable Unreliable RE: 49-54 T LE: 342 Unreliable Unreliable 1 0 LE: 49-53 LE: 51-53 ... ... 4103520 420=510 4209510 420a510 nm nm nm nm ... ... No match LE: 581-585 4503480 nm Family 2 Ib IIc 44 15 IId 24 Ile 17 248 60 RE: LE: RE: LE: 484 655 529 406 T 1 1 0 0 0 0 * RE: 49-52 579-585 nm LE: 51-52 440-510 ... nm ... T+Db 2 2 3 RE: 45-62 LE: 32-62 T+D 1 0 2 52-53 None No match 1 0 0 RE: 48-50 None No match RE: 582-584 nm LE: 575-587 nm 420=530 nm 420=520 nm Family 3 IIb 38 120 T lIla IlIb 12 11 150 190 T+D? T a Tritan axis. b LE: 50-52 0 1 0 0 0 0 51-52 51-52 None 579-582 nm No match 0-530 nm 42 Deutan axis. line above normal. All nine were initially unaware of a visual problem. One was detected on school screening and eight others were detected in our clinic. Two of the other four subjects whose acuities were worse than 20/60 were unaware of a visual problem until they were detected in school screening. B. Visual Fields Four of the six visual fields obtained were normal. The other two showed central scotomas (Table I). C. Optic Nerves Obvious pallor of some portion or all of the temporal portion of the optic nerve was seen in one or both eyes of eight individuals (Table I). A ninth subject had pallor of the entire nerve head. Three individuals had questionable pallor (not all examiners agreed). Normalappearing disks, according to all examiners, were seen in two individuals. D. ERG and Dark Adaptation These tests were normal in the subjects studied. E. Color Vision Table II shows the results of the color-vision tests performed on all patients. Two subjects (family 1, III1 and IIIm) were unreliable. Figures 2-4 show the results of the 100-hue test for three members of family 1 (Fig. 2), two members of family 2 (Fig. 3), and three members of family 3 (Fig. 4). A tritan axis was seen for all individuals for whom testing was performed and considered reliable. In addition, two subjects (family 2, IIc and IId) and possibly a third (family 3, patient IIIa) showed a deutan axis, in addition to the tritan axis. All subjects except one (family 3, patient IIIa) with 20/60 vision or better showed predominately a tritan axis. Subjects considered to be reliable on the anomaloscope gave normal Rayleigh equations, with two exceptions (family 1, IIi and family 2, IId). They had wider than normal match widths (Table II). Neutral points were found in six subjects (Table II). In general, these varied from 579 to 585 nm although one subject (family 2, IId) showed a neutral point for her left eye, extending from 575 to 587 nm (this subject is classified as a tritanope because of the finding of a neutral point and characteristic color match. Obviously her defect extends extensively into the red-green area as well). Confusion color matches varied slightly, but when these were plotted along with the neutral points on a chromaticity diagram, they converged towards the blue end of the spectrum, in the area of the classical tritanopic convergence locus (Fig. 5). In summary, the four subjects who have the colorvision characteristics classically described for congenital tritanopes are subjects IIg and IIi from family 1, subject Ib from family 2, and subject IIIb from family KRILL, Patient i g SMITH, AND POKORNY Vol. 60 Some of our optic-atrophy subjects missed some redgreen pseudoisochromatic plates. In addition, two Putient fi subjecLs with poor vision showed a deutan as well as a tritan axis on the F-M 100-huetest. In pedigrees with a tritanope there are frequently some affected individuals showing evidence of slight red-green abnormalities on the pseudoisochromatic plates and 100-hue test.' 2 a On the anomaloscope, all but two subjects showed normal Rayleigh matches. These two had wider than normal equations. A slight red and rarely a slight green Patientm k FIG. 2. Plot of errors on Farnsworth-Munsell 100-hue test from three patients in family 1. A tritan axis is noted in all three patients. 3. All these subjects had normal reading vision and were unaware of any visual defect other than abnormal color vision. All had classical tritanopic neutral points and color matches and showed only tritan axes on the Farnsworth-Munsell 100-hue test. DISCUSSION A. Comparison with Other Tritan Data The color-vision data of members from these three families and from pedigrees with congenital tritanopia are identical. Almost all affected individuals of both groups showed a tritan axis on the FarnsworthMunsell 100-hue test. Of the 14 affected subjects, all except one missed at least one screening blue-yellow plate on the AO HRR pseudoisochromatic plates. This plate is rarely missed by other types of observers. Walls24 reported that each of his five tritan subjects missed some of these blue-yellow plates. On the other hand, only three of the eight tritans tested by Henry, Cole, and Nathan2 5 missed some of these plates, but the other five tritans reported two or more of the plates to be faint. FIG. 3. Plot of errors on Farnsworth-Munsell 100-hue test from two patients in family 2. Tritan axis is noted in both patients and in addition, a deutan axis is evident in patient Ild. August1970 TRITAN DEFECTS AND DOMINANT OPTIC ATROPHY Patient flb ~ -' I' \ Our pedigrees were characterized \ \I/ Patient ma \ Itritanopia dominance, and the variability ;mon / \ ' >< m<5 m\ 4/tAfound XIn mb B. Comparison with Color-Vision Data from Other Acquired Diseases other acquired diseases we and Verriest31 have a tritan axis on the 100-hue test to be very common in macular disease. However, in our experience and that of Verriest3' and Hong32these patients almost always show a red shift of the Rayleigh equation and, in addition, frequently a widening of the equation, exceeding the normal range. In addition, we have found that patients with minimal or early macular disease may show only anomaloscopic abnormalities without changes in the 100-hue test. In dominant optic atrophy, a tritan axis on the 100-hue test is frequently of acquired optic-nerve disease, a deutan axis is com- mon on the 100-hue test, and a green shift of the 30 32 Rayleight match on the anomaloscope. Therefore, the color vision of patients with hereditary dominant optic atrophy is different from patients with macular and other optic-nerve diseases. FAMILY No.1, PATIENT 100-hue test from three patients in family 3. A tritan axis is evident in patients I1b and IIIb; however, patient ans. axis. seen an anomaloscopic abnormality. In other types |without * FIG. 4. Plot of errors on Farnsworth-Munsell of expression are com- features. / e by variations of the degree of color-vision abnormality in affected members. Similarly, variation is common525 in pedigrees with and even unilateral tritanopes are described.4' Obviously, the hereditary pattern, autosomal / 4 Patient 1 137 Ilg FAMILY No.2, PATIENT lb as 0.8 0. 0.7 ila shows a mixed deutan-tritan \I 0 Oe\\06\\ shift have been reported,5 25' 26 but apprently most tritanopes have normal equations of the anomaloscope. The neutral points reported for our optic-atrophy patients varied from 579 to 585 nm with 2500 K and were in the range reported for tritanopes by Wright4 ; Judd, Plaza, and Farnsworth2 7 ; Cole, Henry, and Nathan2 5 ; Fischer, Bouman, and Ten Doesschate.;2 and Sperling. Only one other study30 evaluated neutral points in dominant optic atrophy. However, both of the patients studied had very poor acuity and matched most of the spectrum to white light. 04 04 03 0.2 0/ / 01 , 0'2 a 0'4 of our subjects were plotted on the chromaticity dia- gram, convergence to the blue end of the spectrum in the area of the tritanopic-convergence found. locus was s a0' O. 0'7 0.' 0.6 07 0 x FAMILY No.1, PATIENTIUi FAMILY No.3 PATIENTII, 0.8 0. O, 07 The color confusions reported for our subjects corre- sponded to those noted in tritanopes. For example, Wright4 most commonly found that tritanopes confused 530 and 420 nm. Our optic atrophy subjects matched 410 nm with 520 nm, 420 nm with 510 nm, \ and other similar combinations. However, the major point is that when the neutral points and color matches / 06 \ \O 05 f I .4 04 05 \F 0X/ /0 0' 02 03 04 0506 07 0.8 \/ 0 0' .3 04 05 06 0 0 FIG. 5. Plot of neutral points and confusion colors from four patients with tritanopia on a chromaticity diagram. Note convergenre of fnertnnyP - --__ nointqin ___the ___airen ____ of __ the ___blue -_ end __ of -1 the - _V_- - 1 138 KRILL, SMITH, AND POKORNY C. Characteristics of Hereditary Dominant Optic Atrophy The subtle nature of the visual defect in hereditary dominant optic atrophy, referred to by many workers8 -1 2 in the past, was emphasized by the data of this study. Six patients were unaware of a visual problem until this was detected at our eye clinic. Five of the six patients were beyond the age of 30 and would therefore be similar to the age range of many of the tritanopes previously reported. It has only been in the last 5 to 10 years that routine visual screening has become a practice in many school systems. Five of our younger patients were discovered to have a visual defect in this manner. None of these five were previously aware of any visual difficulty. Altogether, then, only three of the 14 patients reported in this study were aware of a visual defect since birth, or early childhood. However, most of our patients or their relatives were aware of abnormal color vision (a finding noted by Wright 4 in his study of congenital tritanopia). The original examiners of our patients frequently did not detect the disease if only one member of a family was examined, because of the subtle nature of the optic atrophy. Temporal pallor, the most frequent optic-nerve change, was borderline in some patients. Two patients were originally referred to us because the ophthalmologist was unaware or uncertain of the cause of abnormal distance acuity. In both cases other members of the family who exhibited obvious optic atrophy had not been examined. Obviously, the degree of temporal pallor varies, even within the same family. When of sufficient extent, it is easily recognized and is unlikely to be confused with other anomalies or diseases of the optic nerve by the experienced examiner. The significance of the temporal pallor in these patients is uncertain, but may reflect an absence of some nerve fibers, and accompanying blood vessels, perhaps in most cases, since birth. It should be emphasized that most patients had acuity sufficient to read fine print (J2 or better) without bringing the subject material closer than the test distance customarily used for a normal individual about the same size. This was true of all subjects with distance acuity equal to or better than 20/60. This discrepancy between near and distant vision (assuming the visual angle to be about the same) has been commented on previously by one of the authors3 3 as a frequent finding in certain congenital conditions, such as albinism or rod monochromatism. We have not seen this discrepancy in diseases affecting vision, acquired later in life. Therefore, the frequent finding of this discrepancy in dominant atrophy supports the notion that this disease is usually present since early life, perhaps since birth. Previous reports8'- 3 on dominant optic atrophy emphasize the variability as well as the frequently subtle nature of the disease. Some of the major points Vol. 60 that have been emphasized in these reports are: (a) The optic atrophy varies in extent, but in the majority of patients only the temporal half of the disk is pale; (b) in most cases, it was not difficult to establish the presence of atrophy of the disk, but in some patients the pallor was so slight that the first impression the disk gave was that it was normal. Kjer,8 in his very extensive study of this disease, cites four patients for whom the original examining ophthalomologist had not considered the disk pallor to be pathological. He also emphasized that atrophy was sometimes more apparent by indirect illumination; (c) in doubtful cases, supplementary examinations (determinations of vision, color perception, and visual fields) helped to decide whether a pale disk should be regarded as pathological or merely a physiological variation; and (d) in many patients, there was no direct relationship between optic-disk atrophy and visual acuity. In fact, Kjer8 describes pale disks in some patients with, normal vision, while in other patients optic atrophy was difficult to recognize, whereas vision was obviously impaired. Only two of the six patients we examined showed visual-field defects. However, as pointed out in the Methods section, we did not use the most-sensitive test target of the Goldmann perimeter, nor did we use colored test objects. It has been noted in previous studies8-13 that the majority of patients have minimal visual-field defects that can be detected with small enough white or blue test objects. It is of interest that in two patients with congenital tritan defects,34' 35 visual-field defects were more pronounced with blue than any other-color test object. CONCLUSIONS It is conceivable that congenital tritanopia actually exists and that all of the similar or identical findings mentioned in this report are coincidental. We propose, however, that certain criteria should be met before a case called congenital tritanopia can be accepted as a unique entity, differing from dominant optic atrophy. First, it is necessary to show that both distance and near vision are normal. For example, it is not enough to say that visual acuity was sufficient to read small print, 5 adequate to carry on a certain profession,27 or sufficient to permit reliable results to be obtained from color tests. 25 Second, visual fields must be normal. Third, not only the affected individual, but other members of the family should have normal-appearing optic nerves as well as normal acuity. Further, the ophthalmoscopic examination should be done by some one who has evaluated many pathological optic nerves, because the changes can be quite subtle, as we have noted. Evaluation of previous reports of tritanopes, particularly within the last 50 years, reveals that all these criteria have usually not been fulfilled. This report does not prove that congenital tritanopia does not exist; it serves only to emphasize that there August1970 TRITAN DEFECTS AND DOMINANT OPTIC ATROPHY is a condition, dominant optic atrophy, that presents all the characteristics reported for congenital tritanopia. Therefore, we emphasize that for future subjects in whom congenital tritanopia is suspected, the utmost care should be taken to rule out dominant optic atrophy. REFERENCES * This study was supported in part by Grants EY-0523-09 and EY-00277-05 from the National Institutes of Health, Public Health Service, and also by a grant from the National Society for the Prevention of Blindness. Paper presented at the Chicago meeting of the Optical Society of America, October, 1969 [J. Opt. Soc. Am. 59, 1533A (1969)]. 1 Personal communication. 2 W. Trendelenburg, Klin. Mbl. Augenheilk. 106, 537 (1941). 3 F. H. G. Pitt, Proc. Roy. Soc. (London) B132, 101 (1944). 4 W. D. Wright, J. Opt. Soc. Am. 42, 509 (1952). 5 H. Kalmus, Ann. Hum. Gen. 20, 39 (1955). 6 I. Schmidt, Klin. Mbl. Augenheilk. 109, 635 (1943). 7G. L. Walls, Vision Res. 4, 3 (1964), however, takes the opposing view that tritanopes may not recognize their deficiency. 8 P. Kjer, Acta Ophthalmol. (Suppl. 54) (1959). 9W.Jaeger, Graefes Arch. Ophthalmol. 155, 457 (1954). P. GrUtzner, Deutschen Ophthalmol. Ges. 65, 268 (1963). J. Ruby and J. B. Davey, Brit. J. Ophthalmol. 42, 413 (1958). 12C. V. Londberg and A. Lund, Acta Ophthalmol. 28, 437 (1950). 13P. J. Waardenburg, Genetics in Ophthalmology, Vol. 2 (Royal van Gorkum, Assen, 1963), p. 1623. 14 J. Frangois, Heredity in Ophthalmology (Mosby, St. Louis, 1961), 15A. Franceschetti, J. Frangois, and J. Babel, Les HergdoDigen~rescences Choriordtiniennes (Masson, Paris, 1963), Vols. I and II. 16A. E. Krill, P. A. Morse, A. M. Potts, and B. A. Klien, Am. J. Ophthalmol. 61, 1405 (1966). 17In our experience the arm span of a normal sighted individual is a useful indication of his usual reading distance. Consequently, the tester placed the reading chart at an estimated normal reading distance for each patient. 18A. E. Krill, V. C. Smith, R. Blough, and A. Pass, Invest. Ophthalmol. 7, 701 (1968). 19A. E. Krill and B. A. Klien, Arch. Ophthalmol. 74, 496 (1965). 20 A. E. Krill, Trans. Am. Acad. Ophthalmol. Otol. 70, 1063 (1966). 21 A. E. Krill and A. Schneiderman, Invest. Ophth. 3, 445 (1964). 22 D. Farnsworth, J. Opt. Soc. Am. 33, 568 (1943). 23 The apparatus has been described in J. Pokorny and V. C. Smith, J. Opt. Soc. Am. 60, 562 (1970). 24 G. L. Walls, Am. J. Optom. 36, 169 (1959). 25 G. H. Henry, B. L. Cole, and J. Nathan, Ann. Hum. Genet. 27, 219 (1964). 26B. L. Cole, G. H. Henry, and J. Nathan, Vision Res. 6, 301 (1966). 27 D. B. Judd, L. Plaza, and D. Farnsworth, J. Opt. Soc. Am. 40, 833 (1950). 28F. P. Fischer, M. A. Bouman, and J. ten Doesschate, Doc. Ophthalmol. 5-6, 73 (1951). 19H. G. Sperling, J. Opt. Soc. Am. 50, 156 (1960). 30P. GrUtzner, Graefes Arch. Ophthalmol. 169, 366 (1966). 31G. Verriest, J. Opt. Soc. Am. 53, 185 (1963). 32S. Hong, Arch. Ophthalmol. 58, 505 (1957). 33A. E. Krill, Postgraduate Med. 37, 279 (1965). 34E. Engelking, Graefes Arch. Ophthalmol. 116, 196 (1925). 30H. Hartung, Klin. Mbl. Augenheilk. 76, 229 (1926).









© Copyright 2026