
Managing the watery eye CET 1 FREE CET POINT
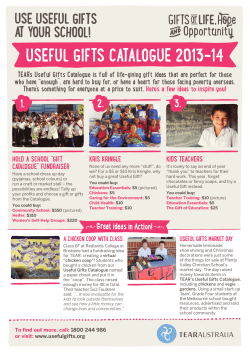
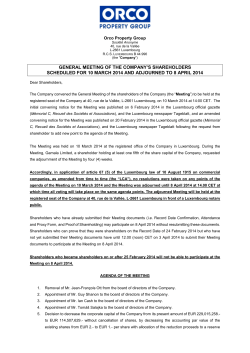
CET CONTINUING EDUCATION & TRAINING PEER REVIEWED 1 FREE CET POINT 4 Approved for: Optometrists OT CET content supports Optometry Giving Sight Dispensing Opticians Having trouble signing in to take an exam? View CET FAQ Go to www.optometry.co.uk 4 Managing the watery eye 40 Anterior eye and oculoplastics Part 3 C-19163 O/D Tristan Reuser, MD, FRCOphth Watery eyes or ‘epiphora’ is a common complaint presenting to eye 29/06 /12 CET and care professionals. amongst patients Surprisingly, dry eyes watery eyes may have common aetiology. There may be Figure 1 MRI scan of the nose, indicating a tumour encroaching the nasolacrimal duct many reasons for epiphora and this article describes the common enter the nasal cavity, just lateral to the types inferior nasal turbinate. Any dye instilled and the most effective examination and management. into the eye may be retrieved from here main Tears which are produced in the main with a small cotton bud, as in Jones’ the lacrimal gland “fall” over the cornea test number one (vide infra) (see later). superolateral part of the anterior orbit. and conjunctiva and end up on the It is divided into two parts by the lower lid. They don’t spill over the lateral horn of the levator aponeurosis eyelid margin, as this is hydrophobic, What’s this patient talking about? – the superolateral orbital lobe and the by virtue of a fatty substance secreted When a patient complains of ‘watering inferomedial palpebral lobe. Accessory by the Meibomian glands. From the eyes’, it is important to establish what tear glands are found in the conjunctiva lower lid, they are actively transported exactly they mean. Sometimes it is the (glands of Krause and Wolfring), as via a lacrimal pump mechanism which feeling of a moist eye, a slight excess well cells. is thought to be controlled mainly by of tears, but they do not spill over From a practical point of view, the blinking. The lacrimal pump mechanism onto the cheek. Epiphora means that accessory play involves contraction of the orbicularis the tears spill onto the cheek. When production. muscle to close the eye, which creates this happens, patients tend to be more There is a distinction between basic tear negative pressure in the lacrimal sac. bothered with it, since apart from secretion, whereby tears are produced Since part of its fibres are connected vision problems (often they complain of continually to replenish the natural to the fascia, which envelops the sac, blurred vision when reading due to an tear film, and reflex tear secretion, this contraction ‘opens up’ the sac by increased tear meniscus) there are also which occurs after stimulation by, for enlarging it. The negative pressure social implications. People think the example, peeling onions, a foreign body sucks in the tears which are located patient is being emotional, which can in the eye, corneal abrasion or cold wind. in the lacus lacrimalis.1 The tears then leave the patient feeling embarrassed. Tears are lacrimal a as role produced gland, by which conjunctival glands in excess don’t tear the sits in goblet ever Not uncommonly, patients complain of Grade of epiphora Degree of epiphora experienced 0 No epiphora 1 Epiphora only outdoors in the wind 2 Epiphora only outdoors but not indoors 3 Epiphora outdoors and indoors Table 1 Sahlin’s3 system for grading the severity of epiphora watering eyes, but during their time in the consulting room, not once do they mop them. If that is the case, is the problem really so bad? A semi-quantitative way of recording the watering is to use Munk’s classification,2 where the number of times per day the patient needs to mop their eyes is recorded. Although this classification implies reasonable quantification, in practice, patients can’t really remember the exact number of Find out when CET points will be uploaded to Vantage at www.optometry.co.uk/cet/vantage-dates times they mop their eyes. Another way of recording the severity of epiphora has been used by Sahlin (Table 1).3 History taking When assessing the cause of epiphora, it is often thought that simply doing 41 a sac washout will tell you enough. History though, is most important, since not only can it give valuable clues might be, it will also indicate how serious it is. If the patient only needs to Figure 2 A lacrimal sac full of mucus (mucocele) wipe their eyes three times a day and of the LeFort type tend to be horizontal uveitis only when outdoors, it may well be that through the middle of the face and lamp examination is, therefore, vital they will be happy to put up with it. may include the nasolacrimal duct. to look for signs of any of these and a The history can provide valuable (through photophobia). Slit systematic approach is best. Start by clues about whether the epiphora is Examination looking for anything which might cause an excess production problem, or a Facial features hypersecretion, blockage in the drainage pathways. Look at the areas in the upper part of position (ectropion) where the tear Soreness and a foreign body sensation the face. A crooked nose may point punctum is not turned towards the tear will point to excess production, due to involve lake. Then instil fluorescein to check the to secretion. the deeper parts of the nose and the tear film break up time (TBUT). Follow This is how dry eye may be a cause nasolacrimal duct too. A swelling in this by instilling dilating drops, since for epiphora if basic tear secretion is the medial canthus may point to a each patient will need a full dilated fundal reduced, causing discomfort, which swollen lacrimal sac full of mucus (a examination. Once any reflex tearing in turn causes reflex tear secretion. mucocele – Figure 2) or mucus mixed from the instillation of tropicamide It is also important to enquire about with purulent material (mucopyocele), has subsided, a drop of 2% fluorescein problems with areas around the eyes, which may cause epiphora. Such a should then be instilled into the lower which excessive reflex tear a fracture, which may eg abnormal eyelid mucocele or mucopyocele must be conjunctival sac for the Jones dye test possible treated before any intraocular operation to be performed. The patient now waits underlying diseases. Nasal history is is considered (eg cataract extraction). 5-10 minutes, after which the remaining important here, since hay fever may If the sac is infected and inflamed fluorescein in the conjunctival sac is cause reflex tear secretion, post-nasal (dacryocystitis), the surrounding area assessed – has there been any dilution of surgery may indicate damage inflicted will also be red, swollen and painful. A the highly concentrated 2% fluorescein by the surgeon to the nasolacrimal duct scar near the area of the medial canthus, drops? If so, it means these drops have (which is located in the lateral wall of may point to previous trauma which either spilt over onto the cheeks, which the nose), with infection of the lacrimal may you can see, or discover from the patient’s sac a possible result. A bloody nasal A have report. If this has not occurred, the discharge may point to a malignant developed, causing an outflow problem. fluorescein will have diluted and drained might regarding the provide cause information and growth (Figure 1) encroaching the have stenosis involved the (narrowing) canaliculi. may into the lacrimal drainage apparatus. meatus, Ocular features and assessment blocking the exit of the distal part of Reflex hypersecretion may be caused one. See whether the dye has reached the nasolacrimal duct into the nose. by blepharitis, trichiasis, distichiasis, the nose. The presence of fluorescein Wegener’s disease is an autoimmune entropion, concretions, may be assessed by applying a cotton disorder which may involve the nasal foreign bodies, dry eyes, eyelashes bud into the nose. The tips used for mucosa and cause symptoms such as ‘stuck’ in the tear punctum, corneal viral swabs are the right size, however, discharge and ‘catarrh’. Facial fractures ulcers, corneal abrasions, and anterior standard cotton buds are too big. The area under the inferior conjunctival It is now time for the Jones test number For the latest CET visit www.optometry.co.uk/cet 29/06 /12 CET as to what the mechanism of watering CET CONTINUING EDUCATION & TRAINING PEER REVIEWED 1 FREE CET POINT Approved for: Optometrists 4 OT CET content supports Optometry Giving Sight Dispensing Opticians 4 Having trouble signing in to take an exam? View CET FAQ Go to www.optometry.co.uk Another aspect of the Jones test two is whether the patient feels something at the back of their nose/throat. However, patients can be unreliable in their responses and so objective observation of the dye is preferred. 42 Advanced assessment Where the optometric investigations described above do not offer conclusive evidence, patients can be referred to the hospital eye service (HES) for more 29/06 /12 CET advanced assessment, as described below. Dacryocystogram (DCG) A DCG is performed in a hospital radiology department, with both eyes tested at the same time. Both inferior canaliculi are cannulated with a small Figure 3 A dacrysocystogram (see text for details) cannula and these are connected to a Y-connector leading to the same syringe. presence of dye on the bud indicates a the dye to appear in the nose increases. In the syringe is a radio-opaque solution, positive Jones test number one result, The Jones test number two is much which is then squirted into the lacrimal such that the dye has gone through a easier to do (and only really done if drainage system. As the solution flows patent lacrimal drainage system. In the the Jones test one was negative). One through the system, x-rays are taken to presence of a positive Jones test one, has to clear all remaining fluorescein locate the solution. This solution blocks epiphora may still be possible as a from the conjunctival sac, and then do x-rays and, therefore, appears black on result of hypersecretion. If there is no a simple washout of the tear apparatus the image. The outlines of this black dye, the result is negative. This can be using a syringe (being careful not to area correspond to where the solution problematic, since 20% of people with cause any damage to the canaliculi). Do is sitting (Figure 3). Modern digital a normal lacrimal drainage will have this with the patient leaning slightly subtraction techniques create shadows a negative test result (false negative). forward so that you will be able to see of the surrounding tissues while the Visualising the inside of the nose can the fluid coming from their nose. It may bones are invisible. Complete blockages reduce this number significantly, hence be either non-coloured or fluorescein of the sac are visible as a stop in the the need for nasal endoscopy. Referral stained. If the fluid is clear, then it nasolacrimal duct; the fluid does not to an ophthalmologist is advisable for means the dye has not gone into the go beyond the block and accumulates this and often the presence of dye in lacrimal system, indicating an ‘upper the nose will confirm a patent drainage system’ failure (vide supra) ie lacrimal system. In addition, it will allow the pump failure, such as in facial palsy, presence of any abnormalities in the punctal stenosis, canalicular block, nose, which might be contributing or punctal eversion. If the fluid is to the tearing, to be detected too. fluorescein stained, then it means that The presence of fluorescein in the nose is the dye has reached the outflow system dependent on the rate of tear production and has collected in the lacrimal sac and how long after instillation of but has not drained normally into the fluorescein the nose is examined.4As nasal cavity. This is called a functional we get older, tear secretion reduces and, block and is due to a partial stenosis, therefore, the “normal” time taken for or narrowing of the nasolacrimal duct. Figure 4 Lacrimal scintillogram to determine the location of a blockage in the lacrimal system Find out when CET points will be uploaded to Vantage at www.optometry.co.uk/cet/vantage-dates above it. Partial blockages can the stenosis is more than 8mm be seen as narrowing, sometimes away from the punctum then a seen dacryocystorhinostomy combination with (DCR) is dilation of the sac just proximal performed following excision of to the block. On other occasions, the stenosis and intubation. DCR one will see contrast in the consists of removing the intervening sac on a ‘late’ x-ray of the face. bone between the tear sac and the nasal cavity, so that the lacrimal sac Lacrimal scintillogram and the nasal mucosa lie directly This test is also performed at next to each other. The tissues are the radiology department, but it involves a radioactive solution. This is instilled into the conjunctival sac and allowed to flow naturally through the Figure 5 Patients often aren’t afraid of being left with small scars following surgical procedures such as DCR it is forced by a syringe). It is, therefore, a physiological test, and very valuable. After every few minutes, an image is taken to determine the location of the radioactivity within the lacrimal drainage system. Once a series of images are created they can be analysed to locate the blockage (Figure 4). This test is complimentary to DCG, where it may be impossible to establish the exact site of a narrowing in functional blocks. connected with sutures and little silicone tubes are then inserted into the canaliculi (not all surgeons use these tubes in all cases), and out into the newly created opening. They are drainage system (unlike in DCG, where left in the tear passages for anything Too little drainage Punctal ectropion due to horizontal eyelid laxity performing an needs eyelid treating by shortening procedure. The lateral tarsal strip operation, where the eyelid is cut in the lateral canthus and shortened at this end, is currently the preferred method. This will often result in an eyelid which is sufficiently tight to correct the punctal position. On other occasions, this may need to be combined with excision of Treatment of watery eyes a diamond of tarsoconjunctiva just Too much tear production inferior to the punctum. This shortening between six weeks and six months. If the block is nearer than 8mm from the punctum, then technically, it is impossible to excise the stenosis. One then has to insert a glass tube (Jones’ tube) through the caruncle and the soft tissues into the nasal cavity. This tube acts simply by gravity and its function is thus position dependent. Sometimes, the canalicular blockages are localised and consist of a little membrane where the common canaliculus enters the tear sac. This can be removed, and intubation with distichiasis, of the back part of the eyelid will then entropion, conjunctival concretions, correctly position the punctum again. foreign bodies, dry eyes, eyelashes Quite often punctal stenosis (narrowing ‘stuck’ in the tear punctum, corneal of the tear punctum) is associated with ulcers, corneal abrasions, and anterior punctal ectropion. It is due to reduced uveitis appropriate tear flow through the punctum, and this treatment if one of these is the cause will return to normal once the duct is of the watery eye. Many of these will correctly positioned again. If the punctal require treatment with ocular lubricants ectropion is due to shortening of the and lid hygiene with baby shampoo or anterior lamella (front part of the eyelid) bypass the block. Several procedures using commercially available products. due to, for example, skin conditions, have been tried, but the gold standard However, there may be more than one then a skin graft may be required. against which all other procedures cause for the epiphora and therefore Canalicular blockages may occur due are judged is the open DCR, which more than one treatment may be to a variety of causes. If the stenosis is has required. Recently, attempts have been only in a short section, then excising The made to treat some patients, who do not the narrowed part of the canaliculus involves expansion of the nasolacrimal want major operations, with injections and intubating this is enough. If the duct with a balloon. The tear duct of botulinum toxin instead, although canaliculi are stenosed over a larger system is then intubated with the this has produced varying results. extent, then several options exist. If silicone tubes again. This procedure Blepharitis, all trichiasis, need their 43 silicone stents done. These silicone tubes prevent the formation of a scar, which would otherwise block the affected part again. Classically, this operation has been done in combination with a DCR, but this may not be necessary.5 More distal blockages, which are in the sac itself, need a procedure to For the latest CET visit www.optometry.co.uk/cet success rates alternative, of over 90%. dacryocystoplasty, 29/06 /12 CET in CET CONTINUING EDUCATION & TRAINING PEER REVIEWED 1 FREE CET POINT Approved for: Optometrists 29/06 /12 CET 44 4 OT CET content supports Optometry Giving Sight Dispensing Opticians 4 Having trouble signing in to take an exam? View CET FAQ Go to www.optometry.co.uk has generally not been as successful the sac. A monitor shows the images The British Journal of Ophthalmology. as DCR, with success rates of 50%. obtained through the little endoscope He is an honorary senior lecturer at Laser procedures include cutting in the probe, while an irrigation Birmingham and Aston Universities. open the soft tissues (the lacrimal cannula and a laser or microdrill sac and nasal mucosa),l but also the for treating stenoses and dacryoliths References bone in between the two. Several (stones 1. Hurwitz JJ. (1996) The lacrimal laser types have been tried, of which available options. This technique has system. the holmium-YAG appears to be mainly been described in the German 2. Munk the most useful for cutting through ophthalmic (1990) Epiphora: treatment by means bone. The other slight difference is success with hundreds of cases treated of that the mucosal surfaces of the tear so far, is claimed. Of importance is dilatation of the nasolacrimal drainage sac and the nose are not sutured, that many patients are not afraid to apparatus. since this is really impossible in be left with small scars after DCR 3. Sahlin S, an endonasal approach. Also, the procedures (Figure 5) and so this gold Lacrimal drainage size of the bony opening is smaller standard will still be hard to beat. symptomatic in the lacrimal literature, sac) and are good than the one used in the external Lippincott-Raven. PL, Lin DT, Dacryocystoplasty Morris with Radiology, Rose DC. balloon 177:687-690. GE. (2001) capacity and improvement dacryocystorhinostomy after in adults approach. Both of these differences About the author perhaps explain the lower success Tristan Reuser is a consultant eye drainage systems. Orbit, 20:173-179. rates achieved with these procedures. surgeon, with a special interest in 4. Hagele Due to advances in technology, it is eye plastics. He works at the Heart of MPH. now possible to visualise the entire England Foundation Trust and at Aspen Age as a factor in Jones testing. lacrimal Eye Care at Midland Eye. He trained in Ophthalmology, Two systems currently on the market the UK, and the Netherlands. He was 5. Fulcher T, O’Connor M, Moriarty allow a probe to be introduced into a clinical director in ophthalmology, P. the canaliculi, and from there into and is a reviewer for both Eye and in outflow system directly. presenting with JE, (1994) (1998) adults. patent Guzek lacrimal JP, Shavlik Lacrimal testing. 101:612-617. Nasolacrimal British intubation Journal Module questions Course code: C-19163 O/D PLEASE NOTE There is only one correct answer. All CET is now FREE. Enter online. Please complete online by midnight on July 27, 2012 – You will be unable to submit exams after this date. Answers to the module will be published on www.optometry.co.uk/cet/exam-archive. CET points for these exams will be uploaded to Vantage on August 6, 2012. Find out when CET points will be uploaded to Vantage at www.optometry.co.uk/cet/vantage-dates 1. Which of the following is TRUE regarding tear production? a) The bulk of tears are produced by the lacrimal gland b) Only a minor component of tears is produced by accessory tear glands c) Meibomian glands perform a very important function in the tear complex d) All of the above 2. Which of the following statements about a patient with a watery eye is FALSE? a) The underlying cause may be due to dry eye and a trial of lubricants is advisable b) All patients will require a dacryocystorhinostomy operation c) It should be distinguished from what is merely a non-bothersome ‘moist eye’ d) It can occur due to punctal stenosis, which reduces tear drainage 3. When establishing the cause of the watering eye problem, which is TRUE? a) History-taking is of minor importance b) Advanced investigations, such as DCG, should always be performed c) The Jones dye test number two should always be performed d) Asking about any recent or previous nose surgery can be useful 4. Which of the following statements about examining the patient with a watery eye is TRUE? a) The Jones dye test differentiates reflex tear secretion from blockage of tear passages b) Eyelid eversion may give useful clues about the cause c) Facial features should be examined for any sign of raised bumps by the inner canthus d) All of the above 5. Which of the following statements about the Jones dye diagnostic test is TRUE? a) It will provide all of the information about the presence and location of a blockage b) A simple ‘sac washout’ (test two) can be diagnostic and could be curative c) The absence of dye in the nose indicates a completely patent drainage system d) 40% of patients with a normal lacrimal drainage system may have a negative test one 6. Which of the following statements regarding the treatment of watery eyes is TRUE? a) If it is due to a drainage problem, it requires a DCR operation b) Dacryocystoplasty is the most successful option available c) It may be that a simple lid tightening operation will be effective d) It should always be conducted before a cataract extraction operation Find out when CET points will be uploaded to Vantage at www.optometry.co.uk/cet/vantage-dates of










© Copyright 2026