
Neurotic Excoriations and Dermatitis Artefacta
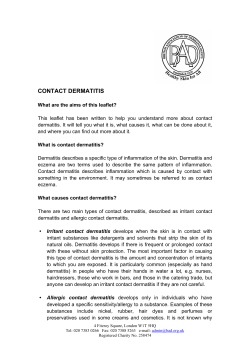
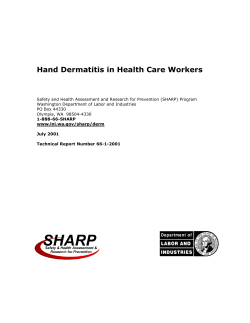
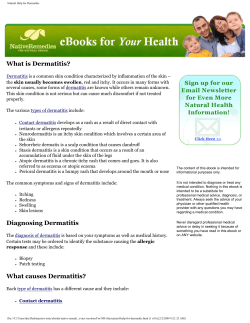
Neurotic Excoriations and Dermatitis Artefacta Caroline S. Koblenzer, MD,* and Rishu Gupta, BS† Neurotic Excoriations is a psychocutaneous disorder that is characterized by an uncontrollable urge to pick at normal skin or skin with mild irregularities. Dermatitis Artefacta is another psychocutaneous disorder that consists of self-induced skin lesions often involving a more elaborate method for damaging the skin, such as the use of a sharp instrument. Both neurotic excoriations and dermatitis artefacta cause significant disfigurement and anxiety for the patient. Since patients often present to dermatologists first, it is important for dermatologists to be aware of the nature of each condition and the available treatment options. This article provides an update on the clinical features, diagnosis, and treatment options for neurotic excoriations and dermatitis artefacta. Semin Cutan Med Surg 32:95-100 © 2013 Frontline Medical Communications KEYWORDS neurotic excoriations, dermatitis artefacta, psychodermatology, psychocutaneous disorder, pathological skin picking, acne excoriée, impulse control disorder, factitial dermatitis T here are 6 clinical conditions in which self-induced lesions cause the patient to consult the dermatologist. Patients with neurotic excoriations, patients with delusional disorders, and those who cut their wrists frankly acknowledge the part that they play in creating lesions. However, those with dermatitis artefacta, those who malinger, and those with Munchausen’s Syndrome completely deny their part.1 This chapter will discuss one syndrome from each group: neurotic excoriations and dermatitis artefacta. Neurotic Excoriations Clinical Picture The patient with neurotic excoriations has an irresistible and uncontrollable urge to pick the skin.2-4 Picking is episodic and may be triggered by anxiety or stress, a focal itching sensation, a pre-existing skin condition, or by the hand encountering an irregularity as it moves unconsciously over the surface of the skin.2,5-7 Once picking is started, there is a build-up of tension, which is relieved only when every lesion has been picked.2,8 Picking is most often accomplished by the fingernails. But it may also be carried out with needles, tweezers, or whatever instrument may come to hand.3,7,9,10 *Private Practice, Moorestown, New Jersey. †Keck School of Medicine, University of Southern California, Los Angeles. Disclosures: The authors have completed and submitted the ICMJE form for disclosure of potential conflicts of interest and none were reported. Correspondence: Rishu Gupta, BS, Department of Dermatology, University of California, 515 Spruce Street, San Francisco, CA 94118. E-mail: [email protected] 1085-5629/13/$-see front matter © 2013 Frontline Medical Communications DOI: 10.12788/j.sder.0008 Lesions are confined to areas within reach of the hands, appearing most numerously on the extensor aspect of the forearms, shoulders, upper back, breasts; buttocks, and the anterior aspect of the thighs. Sparing of the unreachable inter-scapular area in the mid-back, the “butterfly sign” is characteristic.3,10 Lesions may number from one to dozens. Morphologically, active lesions may be round or linear, clean or crusted, scooped-out ulcers (Figure 1). The margins of the older lesions may be thickened from repeated picking. Secondary infection may also occur.3,10 Prurigo nodules may be seen when the condition is ongoing. In the established case, lesions are present in every stage of development (ie, small, newly opened or crusted ulcers, larger and deeper ulcerations with a nodular component, and circular or linear sharply demarcated hypopigmented scars).3,8 Neurotic excoriations can significantly impair the patient’s quality of life.7,11 Time may be spent worrying about picking, resisting the urge to pick, and finally experiencing shame and embarrassment after picking.7 There is a broad spectrum of picking behaviors. For some patients, it occurs almost automatically when the mind is otherwise occupied, while reading, watching television, or driving the car. For others, it may become a daily ritual and may take place behind closed doors for many hours at a time.4,12 Shame and embarrassment usually accompanies this behavior, leading patients to wait many years before seeking treatment.10 Incidence Diagnostic criteria for neurotic excoriations have not yet been delineated by the American Psychiatric Association, making 95 C.S. Koblenzer and R. Gupta 96 Figure 1 Neurotic Excoriations. Lesions have classic morphology and area of distribution for neurotic excoriations. it difficult to determine the true incidence rates.13,14 Indeed, picking is considered to be a part of normal grooming behavior. Children frequently outgrow the common habit of picking insect bites. So it is difficult to determine at what stage the picking behavior should be considered pathological.15 Certainly, it is pathological when it impacts the quality of life.7 Despite this difficulty, studies suggest that there is an incidence of 2%-5% in dermatology patients, with a female to male ratio of 3:1.9,16,17 The average age of onset is reported between the ages of 15 and 35 years in psychiatric literature. In dermatology, we see a second group between 40 and 60 years who are primarily women.3,6,10,16,18,19 Patients complain that an intense focal sensation of itching or burning develops.3 This occurs most frequently in the evening and can be relieved only by picking the exact spot. This then generates an entire cycle of picking.3,20 Unlike the patient with delusions, these patients do not know the cause; they merely seek relief.3,16 Etiology Neurotic excoriations is a psychiatric disorder that most often presents to a dermatologist rather than a psychiatrist.20 The condition has long been considered a part of the obsessive-compulsive spectrum of behaviors. But more recently, because of the absence of an obsessive component, impulsecontrol disorder has been deemed a more accurate diagnosis.4,7,21 Indeed, neuropsychiatric findings would tend to support this diagnosis22 as there is frequent comorbidity with other impulse-control disorders (ie, nail-biting or trichotillomania).4,7,12,23,24 Anxiety and depression are frequently present. The condition is also more common in those who have a family history of similar symptoms of neurotic excoriations.3,6,10 Picking is considered to be a part of normal grooming, which is usually outgrown in childhood. When this is not the case, there have been emotional difficulties in very early childhood. There may also be ongoing stress in the home or school,15 a sign declared in the form of acne excoriée (the uncontrollable urge to pick acne lesions), picking insect bites, or patches of eczema (Figure 2).7,15,25,26 Figure 2 Acne Excoriee. Patient with a form of neurotic excoriations consisting of an uncontrollable urge to pick at acne lesions. Diagnosis The clinical picture is usually diagnostic. However, it is important to consider possible triggers. This means ruling out any underlying primary skin disorder that would generate itching; irregularities in the surface of the skin; or a systemic disorder that may draw attention to the skin by creating an altered sensation.2,3 With this in mind, anemia, hepatic disease, renal disease, thyroid dysfunction and lymphoma should be ruled out. The cultures should be taken to rule out a secondary infection.7 A biopsy should be considered if there is any question of an underlying skin disorder or to reassure a worried patient.2,3,20 Since neurotic excoriations is a psychiatric disorder, it is important to assess the emotional state of the patient. Is the patient experiencing anxiety or depression? Is the patient under significant stress? How is the condition impacting the patient’s life? Is there social withdrawal or isolation? Is the patient able to work? Has the patient had thoughts of hurting himself or others? These issues must be assessed and addressed for the treatment to be successful.27 Treatment A supportive doctor-patient relationship is crucial to help the patient bring the condition under control. A successful relationship cannot be hurried; one cannot become impatient or defensive. Empathize with the patient’s physical discomfort, the embarrassment and the shame that the patient feels, and with the time and expense of treatment. Support the patient’s strengths. Give positive reinforcement for even the smallest advances. See the patient frequently at first to show interest and support. Perhaps see the patient weekly for the first month. Then decrease frequency as their response to treatment allows.28,29 Because the skin is the focus of attention, it is important to prescribe intensive topical treatments that include positive measures to replace the prior destructive activity.28 Depending on the degree of involvement, saline compresses that contain one teaspoon of table salt to one pint of water or soaking for 15 minutes twice daily using a product that Neurotic excoriations and dermatitis artefacta reduces redness, itching, scaling and inflammation (ie, Clorox or Cu tar) are helpful. These can be followed by gentle debridement of the softened crusts with a gauze square. Topical antibiotic ointments, such as a triple antibiotic ointment or a combined antibiotic and steroid ointment (betamethasone, 0.5% with neomycin; or hydrocortisone, 0.5% with neomycin and polymyxin) can then be applied to open areas.1,28 Areas where there is lichenification or nodule formation can be injected with a slow-release suspension of triamcinolone, 10 mg/ml, monthly as needed. When lesions are few, advanced-healing blister band-aids can be applied and left in place until healing has taken place.28 Oral antibiotics should be prescribed as needed, according to the culture findings. Topical retinoids are helpful both in the treatment of acne excoriée and to reduce scarring.25,28 Anxiety and depression should be addressed. Though rare, a multispecialty clinic is ideal for this. If one can help the patient to acknowledge the negative impact of the problem and recognize the presence of anxiety or depression, there is a possibility that they will agree to a psychiatric referral.2,29 The current psychiatric treatments of choice are habit-reversal therapy, cognitivebehavioral therapy or one of the specific serotonin re-uptake inhibitors (SSRI’s).2,19,22,30-34 Sometimes a very low dose of an atypical antipsychotic may be added to boost the impact of the SSRI; and while the oral antihistamines are seldom helpful, opiate antagonists such as naltrexone may help to reduce any altered sensation in the skin.2,35,36 Course and Prognosis Frequently, there is significant improvement in response to the physician’s empathy and interest even after the first visit. If the patient follows instructions and keeps regular appointments, a slow but steady improvement can be expected. The patient should be advised to call at once should any unexpected change take place. They must also be advised never to stop medication unilaterally. Despite positive results when a patient adheres to the regimen, a flare-up may occur during a time of particular stress or peri-menstruation. Some studies in the psychological literature suggest that up to 40% of young people (below the age of 18 years) may continue to pick for the rest of their lives.2,15 From experience in dermatology, this would seem to be an unusually high percentage.6 Dermatitis Artefacta Clinical Picture Dermatitis artefacta refers to a condition in which the patient creates destructive lesions on his or her own skin, secretly and mysteriously, while assiduously denying any part in their creation.37-40 It falls within the spectrum of factitious disorders. The unconscious goal is to gain attention and to be taken care of.14,41-43 The condition generates neither material gain nor avoidance of responsibility; this helps separate it from malingering.14,42,44 Lesions may be single or multiple and are often bilaterally symmetric. The morphology of individual lesions is 97 Figure 3 Dermatitis Artefacta. Patient with severe self-induced lesions. determined by the particular technique by which they are created and are not reconcilable with any known dermatosis.38,45-53 Patients are quite original in their choice of modality. Indeed, lesions may result from picking, gouging, cutting, burning, application of pressure, the pouring on of corrosive liquids, or by any method that one might imagine. Lesions are angulated, geometric or linear; or in the case of burning or suction, they will show the changes characteristic of those injuries. Irregular linear burns, together with the drop sign, may result from the application of caustic liquids. Factitial lesions may be extraordinarily destructive; but the margins of each lesion will be quite distinct with normal surrounding skin (Figure 3).38 What has been termed a “hollow history” is a part of the clinical picture.54 The patient can give no description of the evolution of the lesions. It is as if they had mysteriously appeared, fully formed, perhaps overnight, or during a brief break, and a careful examination will invariably fail to find incipient, early or evolving lesions.38,54,55 When one is consulted by a patient with dermatitis artefacta, an interesting interpersonal dynamic can usually be noted. Despite extensive and often very disfiguring tissue destruction flagrantly exposed, the patient appears remarkably unconcerned, friendly, out-going, and seemingly without great anxiety.56 On the other hand, family members are clearly very anxious, often openly angry and confronting. Most often patients and their family members have consulted a number of physicians in a variety of specialties. The patient has had numerous and repeated tests. But because there have not yet been any answers and no improvement in the patient’s condition, they have a sense that their concerns are unheeded.57-59 In the end, they feel that physicians are incompetent or uncaring and medicine has let them down. A condition called dermatitis artefacta-by-proxy occurs when the lesions are created by one person on the skin of another. The dyad is usually a mother who elicits needed attention by creating lesions on her young child.60-66 Another variant of dermatitis artefacta is pathomimicry in which the patient creates lesions that mimic those of a known dermatosis. They do so either by perpetuating with artificial C.S. Koblenzer and R. Gupta 98 lesions a condition that the patient has previously experienced or by reproducing artificially those encountered on a relative or friend.38,45-53 Incidence The incidence of dermatitis artefacta is difficult to determine as there are few reliable controlled studies, and undoubtedly many cases that are never diagnosed. Accurate diagnostic criteria are not always applied. As a result, confusion with neurotic excoriations and Munchausen’s syndrome sometimes takes place. The condition is significantly more common in women and ratios anywhere from 3:1 to 20:1 are quoted.58 The onset is most commonly in adolescence or early adult life. But short-lived cases may occur in younger patients, which may be triggered by a recent psychosocial stress.37,40,41,67,68 Dermatitis artefacta can also develop in older patients who are predominantly male.58,59,68 It is a common finding that either the patient or a close relative has, or has had, a close relationship with some aspect of the healthcare field. Frequently the patient is a nurse.38,40,56 Etiology Dermatitis artefacta is a primary psychiatric disorder with secondary skin manifestations. The skin lesions are known as a “defense” in that they distract the patient from the underlying psychiatric problem. Most frequently the psychiatric diagnosis is a personality disorder with borderline, paranoid or hysterical features.14,69 These patients usually experience emotional deprivation during childhood, resulting in an unstable body image, a blurring of physical and emotional boundaries, and a need to be cared for.48,70,71 The production of lesions helps to affirm the physical boundary of the self and the need to be cared for.47,66,72-74 The onset of dermatitis artefacta may be triggered by a current psychosocial stress. It is unclear if the patient is aware of creating or perpetuating lesions.74 Some patients apparently create lesions unconsciously, while in a dissociated state. In others, the production of lesions is believed to be a part of the obsessive-compulsive spectrum.75 Diagnosis The clinical picture of the patient with dermatitis artefacta is so characteristic as to raise one’s suspicions. The emotional atmosphere as one first walks into the room—the hollow history, the relative indifference of the patient given the destructive lesions, the bizarre morphology of the lesions, and the sheaf of papers documenting prior studies and prior medications that accompany the patient—should immediately alert the physician.56,57,76 It is important to obtain copies of those prior studies, not to repeat those that are already available. Specific dermatologic diagnostic considerations in each case will be determined by the morphology, distribution of the lesions, and by those prior reports.76 Reportedly, the most common serious considerations are vasculitis, pyoderma gangrenosum, deep fungal infection, arthropod bites and collagen vascular dis- ease.38,52,77-79 One must be alert also to the possibility of pathomimicry.50 Dermatitis artefacta falls under the rubric of somatizing disorders. In this group of patients, comorbidity with other somatizing disorders such as chronic fatigue syndrome, fibromyalgia, irritable bowel disease, is common, as is comorbidity with anxiety and/or depression.13,80 As these patients are disturbed by their body image, it is understandable that other body-image disorders such as an eating disorder or body dysmorphic disorder may also be present.81,82 Dermatitis artefacta is distinguished from malingering because, unlike the malingerer, the patient’s goal is neither material gain nor the avoidance of unpleasant duties, such as perhaps serving in the armed forces.14,44 It is also to be distinguished from Munchausen’s syndrome, which is characterized by peregrination (travelling from doctor to doctor for the treatment of a fabricated condition) and pseudologia fantastica (fabrication of a complex past personal, family, and medical history).58,59,83 Patient’s with this syndrome create false identities and sensational stories about fake symptoms. They also peregrinate from doctor to doctor and from hospital to hospital as they sense that their deceit has been suspected. Occasionally, the patient may undergo unnecessary repeated hospitalizations and major surgical procedures.68 The psychopathology here is a personality disorder with antisocial features.42,68 Treatment As for neurotic excoriations, the treatment of dermatitis artefacta falls into 3 parts: the doctor-patient relationship, topical treatment, and systemic treatment. As with neurotic excoriations, a supportive and trusting relationship is needed for any type of treatment to succeed. Because dermatitis artefacta is a psychiatric disorder, the hope is that one’s approach may ultimately permit either a psychiatric referral or referral to a multi-specialty clinic.58,59,77,84 To prevent further doctor shopping and begin on a path toward treatment, the development of a trusting relationship cannot be hurried. By simply sitting down and making eye contact, one expresses commitment and interest.54 This can be reinforced by looking carefully at the sheaf of papers that the patient brings and documenting what has been done to date.58,85 While taking a careful history, one can empathize with the various aspects of the patient’s prior experience that generates anger and frustration: the expense in time and money of the numerous fruitless consultations and worthless treatments; the negative impact on the quality of life; and the disappointment with seemingly uncaring physicians.39,58,84 See the patient weekly for at least the first month and then extend the interval between visits as the relationship allows.37,40 Be in touch with one’s own feelings and do not permit impatience or defensiveness to emerge in response to the patient’s behavior. Do permit the patient to experience one’s caring through gentle touch. Express a positive attitude and support the patient’s strengths. Stress the need to follow all treatment instructions and to keep appointments.58 Neurotic excoriations and dermatitis artefacta Bearing in mind that the destructive behavior serves as a defense mechanism, it is important not to arouse anxiety by confronting the patient. Anxiety is frequently expressed in anger and may result in further tissue-destruction. However, with children, if one sees the patient separate from the parents, it is sometimes possible to generate a more frank discussion.86 Since the skin is the focus of attention, topical treatment can be instituted in hope that it will take the place of the prior destructive activity. This will be adapted to the specific lesions and may consist, for example, of compresses followed by antibiotic ointment, the packing of deep ulcers with gauze, enzymatic debridement of sloughs, and stimulation of granulation tissue with the application of 10-X sugar. The use of occlusive dressings can permit healing. However, as a treatment, it may result in the appearance of a new lesion at a different site.58,59 Systemic treatment is both dermatologic and psychiatric. Oral antibiotics and anti-fungal agents are prescribed on the basis of culture and laboratory findings, antihistamines (if pruritus is described), and appropriate supplements (ie, iron or B-12).58 Anxiety is common and can be addressed with one of the SSRI family of antidepressants with either buspirone or benzodiazepine. Depression also may be treated with an SSRI, a serotonin and norepinephrine reuptake inhibitor or bupropion. Sometimes it is helpful to add a very low dose of one of the atypical antipsychotics such as aripiprazole, which also has some antidepressant action.58,87 When prescribing one of the psychotropic drugs, it is important to explain to the patient that the drug is not approved by the Federal Drug Administration for this indication — it is an off-label use. It is also important to discuss possible side effects. But during the discussion, stress the positive aspects while putting adequate but not too much emphasis on the possible negatives. Prognosis There are few longitudinal studies of patients with dermatitis artefacta. Therefore, accurate measures of the prognosis are unavailable. However, except in childhood, where the condition may be a transient response to a current psychosocial stress, most observers report a poor prognosis for cure, suggesting that the condition appears to wax and wane with the circumstances of the patient’s life.58,59,71,73,85,88,89 References 1. Koo JYM, Lee CS. Psychocutaneous medicine. New York: Marcel Dekker; 2003. 2. Arnold LM, Auchenbach MB, McElroy SL. Psychogenic excoriation. Clinical features, proposed diagnostic criteria, epidemiology and approaches to treatment. CNS Drugs. 2001;15(5):351-359. 3. Arnold LM, McElroy SL, Mutasim DF, Dwight MM, Lamerson CL, Morris EM. Characteristics of 34 adults with psychogenic excoriation. J Clin Psychiatry. 1998;59(10):509-514. 4. Dell’Osso B, Altamura AC, Allen A,Marazziti D, Hollander E. Epidemiologic and clinical updates on impulse control disorders: a critical review. Eur Arch Psychiatry Clin Neurosci. 2006;256(8):464-475. 5. Calikus¸u C, Yücel B, Polat A, Baykal C. The relation of psychogenic excoriation with psychiatric disorders: a comparative study. Compr Psychiatry. 2003;443:256-361. 99 6. Mutasim DF, Adams BB. The psychiatric profile of patients with psychogenic excoriation. J Am Acad Dermatol. 2009;61(4):611-613. 7. Odlaug BL, Grant JE. Clinical characteristics and medical complications of pathologic skin picking. Gen Hosp Psychiatry. 2008;30(1): 61-66. 8. Koblenzer CS. Psychocutaneous disease. Orlando: Grune & Stratton; 1987. 9. Keuthen NJ, Deckersbach T, Wilhelm S, et al. Repetitive skin-picking in a student population and comparison with a sample of self-injurious skin-pickers. Psychosomatics. 2000;41(3):210-215. 10. Wilhelm S, Keuthen NJ, Deckersbach T, et al. Self-injurious skin picking: clinical characteristics and comorbidity. J Clin Psychiatry. 1999; 60(7):454-459. 11. Flessner CA, Woods DW. Phenomenological characteristics, social problems, and the economic impact associated with chronic skin picking. Behav Modif. 2006;30(6):944-963. 12. Arzeno Ferrao Y, Almeida VP, Bedin NR, Rosa R, D’Arrigo Busnello E. Impulsivity and compulsivity in patients with trichotillomania or skin picking compared with patients with obsessive-compulsive disorder. Compr Psychiatry. 2006;47(4):282-288. 13. American Psychiatric Association. Diagnostic criteria from DSM-IV-TR. Washington, D.C.: American Psychiatric Association; 2000. 14. American Psychiatric Association. Task Force on DSM-IV. Diagnostic and statistical manual of mental disorders : DSM-IV-TR. 4th ed. Washington, DC: American Psychiatric Association; 2000. 15. Odlaug BL, Grant JE. Childhood-onset pathologic skin picking: clinical characteristics and psychiatric comorbidity. Compr Psychiatry. 2007; 48(4):388-393. 16. Fruensgaard K. Neurotic excoriations. A controlled psychiatric examination. Acta Psychiatr Scand Suppl. 1984;312:1-52. 17. Griesemer RD. Emotionally triggered disease in dermatologic practice. Psychiatr Ann. 1978;8:407-412. 18. Gupta MA, Gupta AK, Haberman HF. Neurotic excoriations: a review and some new perspectives. Compr Psychiatry. 1986;27(4):381-386. 19. Simeon D, Stein DJ, Gross S, Islam N, Schmeidler J, Hollander E. A double-blind trial of fluoxetine in pathologic skin picking. J Clin Psychiatry. 1997;58(8):341-347. 20. Gupta MA, Gupta AK. Psychodermatology: an update. J Am Acad Dermatol. 1996;34(6):1030-1046. 21. Grant JE, Odlaug BL, Kim SW. A clinical comparison of pathologic skin picking and obsessive-compulsive disorder. Compr Psychiatry. 2010; 51(4):347-352. 22. Spiegel DR, Finklea L. The recognition and treatment of pathological skin picking: a potential neurobiological underpinning of the efficacy of pharmacotherapy in impulse control disorders. Psychiatry (Edgmont). 2009;6(2):38-42. 23. Lovato L, Ferrão YA, Stein DJ, et al. Skin picking and trichotillomania in adults with obsessive-compulsive disorder. Compr Psychiatry. 2012; 53(5):562-568. 24. Grant JE, Menard W, Phillips KA. Pathological skin picking in individuals with body dysmorphic disorder. Gen Hosp Psychiatry. 2006;28(6): 487-493. 25. Harris SS, Kushon D, Benedetto E. Pathologic grooming behavior: facial dermatillomania. Cutis. 2011;87(1):14-18. 26. Harth W, Taube KM, Gieler U. Facticious disorders in dermatology. J Dtsch Dermatol Ges. 2010;8(5):361-372; quiz 73. 27. Keuthen NJ, Deckersbach T, Wilhelm S, et al. The Skin Picking Impact Scale (SPIS): scale development and psychometric analyses. Psychosomatics. 2001;42(5):397-403. 28. Harth W. Clinical management in psychodermatology. 1st ed. New York: Springer; 2008. 29. Fried RG. Evaluation and treatment of “psychogenic” pruritus and selfexcoriation. J Am Acad Dermatol. 1994;30(6):993-999. 30. Bloch MR, Elliott M, Thompson H, Koran LM. Fluoxetine in pathologic skin-picking: open-label and double-blind results. Psychosomatics. 2001;42(4):314-319. 31. Deckersbach T, Wilhelm S, Keuthen NJ, Baer L, Jenike MA. Cognitivebehavior therapy for self-injurious skin picking. A case series. Behav Modif. 2002;26(3):361-377. 100 32. Pukadan D, Antony J, Mohandas E, Cyriac M, Smith G, Elias A. Use of escitalopram in psychogenic excoriation. Aust N Z J Psychiatry. 2008; 42(5):435-436. 33. Schuck K, Keijsers GP, Rinck M. The effects of brief cognitive-behaviour therapy for pathological skin picking: A randomized comparison to wait-list control. Behav Res Ther. 2011;49(1):11-17. 34. Biondi M, Arcangeli T, Petrucci RM. Paroxetine in a case of psychogenic pruritus and neurotic excoriations. Psychother Psychosom. 2000;69(3): 165-166. 35. Harris BA, Sherertz EF, Flowers FP. Improvement of chronic neurotic excoriations with oral doxepin therapy. Int J Dermatol. 1987;26(8): 541-543. 36. Lienemann J, Walker FD. Reversal of self-abusive behavior with naltrexone. J Clin Psychopharmacol. 1989;9(6):448-449. 37. Cotterill JA. Self-stigmatization: artefact dermatitis. Br J Hosp Med. 1992;47(2):115-119. 38. Lyell A. Cutaneous artifactual disease. A review, amplified by personal experience. J Am Acad Dermatol. 1979;1(5):391-407. 39. Reich P, Gottfried LA. Factitious disorders in a teaching hospital. Ann Intern Med. 1983;99(2):240-247. 40. Sneddon IB. Simulated disease: problems in diagnosis and management. The Parkes Weber Lecture 1982. J R Coll Physicians Lond. 1983; 17(3):199-205. 41. Edlich RF, Tafel JA, Smith JF, Morgan RF. Factitious skin wounds. Compr Ther. 1987;13(8):57-61. 42. Nordmeyer JP. An internist’s view of patients with factitious disorders and factitious clinical symptomatology. Psychother Psychosom. 1994; 62(1-2):30-40. 43. Ugurlu S, Bartley GB, Otley CC, Baratz KH. Factitious disease of periocular and facial skin. Am J Ophthalmol. 1999;127(2):196-201. 44. Wise MG, Ford CV. Factitious disorders. Prim Care. 1999;26(2):315326. 45. Aydin E, Gokoglu O, Ozcurumez G, Aydin H. Factitious cheilitis: a case report. J Med Case Rep. 2008;2:29. 46. Haenel T, Rauchfleisch U, Schuppli R, Battegay R. The psychiatric significance of dermatitis artefacta. Eur Arch Psychiatry Neurol Sci. 1984; 234(1):38-41. 47. Harper JI, Copeman PW. Dermatitis artefacta presenting as a &vasculitis’. J R Soc Med. 1983;76(11):970-971. 48. Levitz SM, Tan OT. Factitious dermatosis masquerading as recurrent herpes zoster. Am J Med. 1988;84(4):781-783. 49. Maurice PD, Rivers JK, Jones C, Cronin E. Dermatitis artefacta with artefact of patch tests. Clin Exp Dermatol. 1987;12(3):204-206. 50. Millard LG. Dermatological pathomimicry: a form of patient maladjustment. Lancet. 1984;2(8409):969-971. 51. Parent DJ, Krafft T, Noel JC, et al. Cutaneous Munchausen syndrome with presentation simulating pyoderma gangrenosum. J Am Acad Dermatol. 1994;31(6):1072-1074. 52. Thomas JR 3rd, Greene SL, Dicken CH. Factitious cheilitis. J Am Acad Dermatol. 1983;8(3):368-372. 53. Gandy DT. The concept and clinical aspects of factitial dermatitis. South Med J. 1953;46(6):551-554. 54. Van Moffaert M. The spectrum of dermatological self-mutilation and self-destruction including dermatitis artefacta and neurotic excoriations. In: Koo JYM, Lee CS, eds. Psychocutaneous Medicine. New York: Marcel Decker; 2003:169-189. 55. Krener P. Factitious disorders and the psychosomatic continuum in children. Curr Opin Pediatr. 1994;6(4):418-422. 56. Koblenzer CS. Psychocutaneous Disease. Florida: Grune & Stratton; 1987. 57. Favazza AR, Conterio K. Female habitual self-mutilators. Acta Psychiatr Scand. 1989;79(3):283-289. 58. Koblenzer CS. Dermatitis artefacta. Clinical features and approaches to treatment. Am J Clin Dermatol. 2000;1(1):47-55. 59. Gattu S, Rashid RM, Khachemoune A. Self-induced skin lesions: a review of dermatitis artefacta. Cutis. 2009;84(5):247-251. C.S. Koblenzer and R. Gupta 60. Epstein MS. Munchausen syndrome: case reports and literature overview. Md Med J. 1995;44(1):39-43. 61. Jones DP. Dermatitis artefacta in mother and baby as child abuse. Br J Psychiatry. 1983;143:199-200. 62. Taylor S, Hyler SE. Update on factitious disorders. Int J Psychiatry Med. 1993;23:81-94. 63. Tumolo J. Making children sick. Munchausen’s syndrome by proxy. Adv Nurse Pract. 2001;9(6):103-106. 64. Klebes C, Fay S. Munchausen syndrome by proxy: a review, case study, and nursing implications. J Pediatr Nurs. 1995;10(2):93-98. 65. Hoorntje TM, Langerak W, Sreeram N. Munchausen’s syndrome by proxy identified with an implantable electrocardiographic recorder. N Engl J Med. 1999;341(19):1478-1479. 66. Plassmann R. The biography of the factitious-disorder patient. Psychother Psychosom. 1994;62(1-2):123-128. 67. Van Moffaert M, Vermander F, Kint A. Dermatitis artefacta. Int J Dermatol. 1985;24(4):236-238. 68. Meadow SR. Who’s to blame–mothers, Munchausen or medicine? J R Coll Physicians Lond. 1994;28(4):332-337. 69. Millard LG, Millard J. Psychocutaneous Disorders. In: Burns DA, Breathnach SM, Cox NH, et al., eds. Rook’s Textbook of Dermatology. Vol 4. UK: Blackwell Publishing; 2010. 70. Fabisch W. Psychiatric aspects of dermatitis artefacta. Br J Dermatol. 1980;102(1):29-34. 71. Kafka JS. The body as transitional object: a psychoanalytic study of a self-mutilating patient. Br J Med Psychol. 1969;42(3):207-212. 72. Doran AR, Roy A, Wolkowitz OM. Self-destructive dermatoses. Psychiatr Clin North Am. 1985;8:291-298. 73. Coid J, Allolio B, Rees LH. Raised plasma metenkephalin in patients who habitually mutilate themselves. Lancet. 1983;2(8349):545-546. 74. Shelley WB. Dermatitis artefacta induced in a patient by one of her multiple personalities. Br J Dermatol. 1981;105(5):587-589. 75. Schaffer CB, Carroll J, Abramowitz SI. Self-mutilation and the borderline personality. J Nerv Ment Dis. 1982;170(8):468-473. 76. Joe EK, Li VW, Magro CM, Arndt KA, Bowers KE. Diagnostic clues to dermatitis artefacta. Cutis. 1999;63(4):209-214. 77. Koblenzer CS. Neurotic excoriations and dermatitis artefacta. Dermatol Clin. 1996;14(3):447-455. 78. Koblenzer CS. Psychiatric syndromes of interest to dermatologists. Int J Dermatol. 1993;32(2):82-88. 79. Harries MJ, McMullen E, Griffiths CE. Pyoderma gangrenosum masquerading as dermatitis artefacta. Arch Dermatol. 2006;142(11):15091510. 80. Gupta MA. Somatization disorders in dermatology. Int Rev Psychiatry. 2006;18(1):41-47. 81. Godt K. Personality disorders in 545 patients with eating disorders. Eur Eat Disord Rev. 2008;16(2):94-99. 82. Paul T, Schroeter K, Dahme B, Nutzinger DO. Self-injurious behavior in women with eating disorders. Am J Psychiatry. 2002;159(3):408411. 83. Newmark N, Adityanjee, Kay J. Pseudologia fantastica and factitious disorder: review of the literature and a case report. Compr Psychiatry. 1999;40(2):89-95. 84. Koblenzer CS. The current management of delusional parasitosis and dermatitis artefacta. Skin Therapy Lett. 2010;15(9):1-3. 85. Sneddon I, Sneddon J. Self-inflicted injury: a follow-up study of 43 patients. Br Med J. 1975;3(5982):527-530. 86. Saez-de-Ocariz M, Orozco-Covarrubias L, Mora-Magana I, et al. Dermatitis artefacta in pediatric patients: experience at the national institute of pediatrics. Pediatr Dermatol. 2004;21(3):205-211. 87. Winchel RM, Stanley M. Self-injurious behavior: a review of the behavior and biology of self-mutilation. Am J Psychiatry. 1991;148(3):306317. 88. Friedman B, Yaffe B, Blankstein A, Rubinstein E, Rieck J. Self-inflicted hand injuries: diagnostic challenge and treatment. Ann Plast Surg. 1988; 20(4):345-350. 89. Murray SJ, Ross JB, Murray AH. Life-threatening dermatitis artefacta. Cutis. 1987;39(5):387-388.







© Copyright 2026