
Intraocular lenses and their potential to inhibit posterior capsule
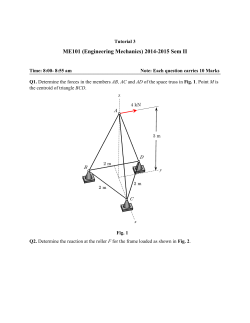
Stability of performance of a handheld radial shape discrimination test in patients at risk of developing neovascular AMD Noelia Pitrelli 1Department Purpose We aimed to assess the performance of the handheld Radial Shape Discrimination (hRSD) test longitudinally in patients at risk of developing neovascular age-related macular degeneration (nAMD) prior to disease development. 1 Vazquez , Simon P. Results 73 participants performed the hRSD test on 5 consecutive visits over a period of 6.5±1.4 months (mean interval between visits 1.6±0.5 months). • • • • The hRSD test1 • Run on an Apple iPod Touch • Stimuli: Radial frequency patterns (sinusoidally modulated circles, frequency = 8 cycles; Fig 1) • Modulation amplitude controlled by a staircase procedure. • Spatial 3AFC • Threshold expressed as a logMAR value. Fig 1: Example of stimuli used in the hRSD test Participants Study eye: • no nAMD or central GA • VA ≥ 0.4 logMAR • no development of nAMD or other sight threatening condition over a period of 5 clinical appointments Fellow eye: • nAMD, being monitored/treated Procedures • hRSD test, using the appropriate near correction2 • Spectralis OCT, assessed at baseline for: • Presence/absence of at least one large druse • Disruption of the ellipsoid zone (EZ) Analysis • • Repeated measures ANOVA for the stability of hRSD threshold over time Regression analyses and t-tests for the effect of age, VA, large drusen, EZ disruption and previous experience with the test on stability. Definitions Large drusen: Disruption to EZ: RPE elevation (≥ 70µm) within 1500µm of the foveal centre Discontinuity of EZ within 1500µm of the foveal centre (with/without drusen) Heinrich 2 Heimann , Paul C. 1 Knox of Eye and Vision Science, University of Liverpool, UK, 2St Paul’s Eye Unit, Royal Liverpool University Hospital, Liverpool, UK Stability over time Methods 1 Harding , • • • • Mean age 78±8y, range 57 to 92, 44 female 38 (52%) had at least one large druse 33 (45%) had some degree of disruption to the EZ 36 (49%) did not have any previous experience with the hRSD test (37 had used the test at least once). hRSD thresholds at each visit were not statistically significant different (F4,288=0.368, p=0.83; Fig 2) Mean thresholds were consistently below the -0.37 logMAR value suggested for detection of nAMD1 The mean difference in hRSD threshold between the first and the last time points was -0.03 logMAR (Bland-Altman 95% limits of agreement: -0.42 and 0.36 logMAR; Fig 3) The mean (±SD) slope of all individual (n=73) regression lines (test result on test visit) was -0.00014±0.000962. For an average follow up time of 189±42 days, this slope represented an improvement in hRSD score of 0.03 logMAR over 6.5 months. Fig 2: Mean plot showing the mean±95%CI for each study visit. Dashed line indicates -0.37 logMAR. The mean (±SD) hRSD thresholds at each time point were : -0.53±0.17, -0.55±0.17, -0.55±0.15, -0.55±0.19 and -0.56±0.21 logMAR Fig 3: Bland Altman plot showing the mean difference (bias) and 95% limits of agreement for visits 1 and 5 Discussion Stable test performance over time prior to the development of disease is an important aspect of any test designed to detect the onset of nAMD and the hRSD test appears to meet this requirement. A number of tests are currently used to monitor patients at risk of developing nAMD. The Amsler Grid is widely used although studies have shown that its sensitivity for detection of nAMD is suboptimal3. The Preferential Hyperacuity Perimeter (PHP), which can be used either in clinic or at home, has shown promise although there is a proportion of patients who struggle to produce reliable results on it4. None of our participants reported any difficulties using the hRSD test. The test does not require a specific room luminance and patients can do it using their usual reading glasses and an eye patch. It can also be implemented on relatively inexpensive handheld devices. The hRSD test is therefore very convenient for use both in the clinic and at home. Future work: We are currently investigating the sensitivity and specificity of the hRSD test for the detection of nAMD by continuing to follow patients until a proportion convert to nAMD in the study eye (the EDiMaD project – see below). Conclusions Effect of age, VA, large drusen, EZ disruption and previous experience on test stability • • the slope of individual regression lines (test result on test visit) was not significantly correlated with age (p=0.99) or baseline VA (p=0.43; Fig 4). • • There was also no difference in mean regression slopes between participants : • with/without large drusen (p=0.53) • with/without ellipsoid zone disruption (p=0.45). • with/without previous experience with the hRSD test (p=0.06) Fig 5: Mean plots showing the mean±95%CI, for groups of participants with/without large drusen (left) and EZ disruption (right). Dashed line indicates -0.37 logMAR. hRSD test performance was stable over a period of approximately six months in eyes at risk of developing nAMD On average, thresholds remained consistently below the cutoff value for the hRSD test previously suggested to be indicative of disease (-0.37 logMAR)1 No significant effects on performance of older age, worse baseline VA or for participants with large drusen or disruption to the EZ References 1. Wang Y-Z et al. Handheld shape discrimination hyperacuity test on a mobile device for remote monitoring of visual function in maculopathy. IOVS 2013;54(8):5497-505. 2. Pitrelli Vazquez N, Knox PC. A handheld radial shape discrimination hyperacuity test: assessment of variability in a clinical population. OPO 2014;34(6):639. Fig 4: Dot plots showing the relationship between individual participant slope (regression line of test result on test visit) and age (left)/ baseline VA (right) Effect of large drusen and EZ disruption on test performance • large drusen did not have a statistically significant effect on hRSD performance (p=0.3) • disruption to the EZ did have a statistically significant effect (p=0.03) however the mean difference of 0.07 logMAR was not clinically relevant (Fig 5). 3. Do DV et al. Detection of new-onset choroidal neovascularization using optical coherence tomography The AMD DOC Study. Ophthalmology 2012;119(4):771-8. 4. Loewenstein A et al. Toward earlier detection of choroidal neovascularization secondary to agerelated macular degeneration. Multicenter evaluation of a preferential hyperacuity perimeter designed as a home device. Retina-J Ret Vit Dis 2010;30(7):1058-64. Poster pdf Links EDiMaD Project Please feel free to scan Acknowledgements This work was supported by a project grant from The Dunhill Medical Trust (grant number: R283/0213). We are also grateful to Vital Art & Science Inc for software and support and Sarah Houston for OCT grading. [email protected]








© Copyright 2026