
□ PAP
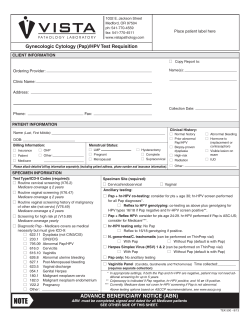
8/1/2013a WOMEN’S HEALTH TEST REQUISITION OFFICE A signed ABN must also be attached for Medicare Screening Paps. Submitting Clinician: Office Location: Name: (Last) ________________________________ (First) ____________________ (Middle) ________________________ PATIENT Date of Birth _________________ Age __________ SSN**_________________________ PT ID# ______________________ Responsible Party (if Minor) _____________________________________ Responsible Party SSN _____________________ Patient Address ________________________________________________________________________________________ □ Thin Prep Vial □ Swab □ Urine Container PAP □ □ □ SOURCE TYPE COLLECTION DATE SPECIMEN City ________________________________ State ____________ Zip code ___________ Phone ______________________ Please attach a printout of information from your EMR if available. ** We are a covered entity under HIPAA regulations. SSN’s are used to aid in linking patient history for optimal patient care. ICD9 Code(s) * Screening Pap (Low Risk Patient) Screening Pap (High Risk Patient) Diagnostic Pap Must be in conjunction with recent Pap (FDA) To Determine Presence of types 16 & /or 18 _____________ _____________ _____________ _____________ ASCCP Guideline GC/CHLAMYDIA/TRICH (check boxes) □ □ □ Chlamydia (CT) rRNA Assay Gonorrhea (GC) rRNA Assay _____________ _____________ Trichomonas (Trich) rRNA Asssay _____________ □ _______________________________ _____________ OTHER CLINICAL HISTORY TESTS ORDERED May be used for over 30 screen. □ Cervix/Endocervix □ ____________________ LMP___________________________ ____________ ____________ ____________ HPV High Risk Screening/Subtyping □ HPV Regardless of Pap Result □ Reflexive Screen for HPV (check one or more) □ if ASCUS □ if ASC-H □ if Low Grade □ if High Grade □ if any abnormal □ HPV Screening only □ HPV Subtyping (check either or both) □ on Postive HPV if Pap Normal □ on all Positive HPV Screens □ Vagina □ Urine □ Routine Exam □ Abnormal Exam (HPV, lesion) * □ Abnormal Bleeding □ Contraceptive: type _______________ □ Estrogen Therapy □ Post Menopausal □ Pregnant _____ weeks □ Post Partum ____ weeks □ Hx of Abnormal Pap □ Hysterectomy—total □ Hysterectomy, intact cervix □ Hx of malignancy; Rx, surgery * □ Pelvic Radiation * □ Other high-risk factors * * Please explain item if checked: __________________________________ __________________________________ * A reference list of ICD-9 codes is shown on the back of this form. Please refer to an ICD-9 manual for a complete list and authoritative information. The ordering practitioner is ultimately responsible for providing medically appropriate ICD-9 codes based on the patient’s signs and symptoms. __________________________________ Primary INS ____________________________________________________________________________________________ INSURANCE Claims Address _________________________________________________________________________________________ Insured’s Name ___________________________________ Policy/Member # ______________________________________ Insured’s DOB ____________________________________ Group #/Employer_____________________________________ Insured’s SSN ____________________________________ MEDICARE #_________________________________________ Insured’s Relation to Patient _________________________ Medicaid # __________________________________________ Secondary INS ______________________________________________ Please attach a copy of each insurance card. CASE # LABEL For SEP Use Only 8/1/2013a ICD-9 SCREENING CODES MEDICARE1 1 V15.89 V22.0 V22.1 M-H N N Screening other specified personal history presenting hazards to health 2 Supervision of normal first pregnancy Supervision of other normal pregnancy V22.2 N Pregnant state, incidental V24.2 N Postpartum (routine postpartum follow-up) V25.49 V69.8 V72.31 V72.32 N M-H M-L N V73.81 N Special screening exam for human papillomavirus (HPV) V73.88 V73.98 V74.5 N N N Special screening exam for other specified chlamydial diseases Special screening exam for unspecified chlamydial disease Special screening exam for sexually transmitted diseases NOS V76.2 M-L Screening for malignant neoplasms of the cervix V76.47 V76.49 M-L M-L Screening for malignant neoplasms of the vagina (post-hysterectomy for non-malignant conditions) Screening for malignant neoplasms of other sites Surveillance of previously prescribed contraceptive methods, other contraceptive method Other problems related to lifestyle Routine gynecological exam with or without Pap test Encounter for Pap cervical smear to confirm findings of recent normal smear following initial abnormal smear M-H This is an allowable code for MEDICARE– High Risk. ABN required for Medicare Screening Paps. Can be repeated after 11 months (Medicare) M-L This is an allowable code for MEDICARE– Low Risk. ABN required for Medicare Screening Paps. Can be repeated at 2 years (Medicare) N This code is not covered for Medicare Screening Paps COMMON ICD-9 DIAGNOSTIC CODES 2 MEDICARE DEFINES HIGH RISK FOR CERVICAL CANCER AS: ▪ Early onset of sexual activity—before age 16 ▪ Fewer than 3 negative Paps in the past 7 years 054.19 054.9 079.4 112.1 131.01 131.09 182.0 183.0 233.1 233.2 616.0 616.10 617.0 622.10 622.11 622.12 623.5 623.8 626.0 626.2 626.4 626.6 626.8 627.1 627.3 795.00 795.01 795.02 795.03 795.04 795.05 795.06 795.07 795.08 795.09 ▪ Multiple sex partners (5 or more in a lifetime) ▪ History of any STD’s ▪ Daughter of a mother who took DES during pregnancy Genital herpes Herpes simplex without mention of complication HPV (human papillomavirus) Candidiasis of vulva and vagina Trichomonial vulvovaginitis Trichomoniasis, Other Malignant neoplasm of body of uterus, corpus uteri / Endometrium / Myometrium /Fundus Malignant neoplasm of ovary and other uterine adnexa Carcinoma in situ of breast and genitourinary system, cervix uteri Carcinoma in situ of breast and genitourinary system, other and unspecified parts of uterus Inflammatory disease of cervix, vagina and vulva, cervicitis and endocervicitis Inflammatory disease of cervix, vagina and vulva, vaginitis and vulvovaginitis Endometriosis of uterus Cervical intraepithelial neoplasia (CIN), unspecified dysplasia, with histologic confirmation Cervical intraepithelial neoplasia (CIN I), mild dysplasia, with histologic confirmation Cervical intraepithelial neoplasia (CIN II), moderate dysplasia, with histologic confirmation Vaginal discharge not otherwise specified Noninflammatory disorders of vagina (e.g. cyst of vagina, hemorrhage of vagina) Absence of menstruation (amenorrhea) Excessive or frequent menstruation (e.g. menorrhagia, menometrorrhagia, heavy periods) Irregular menstrual cycle (bleeding not otherwise specified) Metrorrhagia (bleeding unrelated to menstrual cycle or irregular intermenstrual bleeding) Dysfunctional or functional uterine hemorrhage NOS Postmenopausal bleeding Postmenopausal atrophic vaginitis Abnormal glandular Pap smear of cervix not otherwise specified Abnormal Pap smear of cervix with ASC-US (atypical squamous cells of undetermined significance) Abnormal Pap smear of cervix with ASC-US cannot exclude high grade (ASC-H) Abnormal Pap smear of cervix with low grade squamous intraepithelial lesion (LGSIL) Abnormal Pap smear of cervix with high grade squamous intraepithelial lesion (HGSIL) Cervical high risk HPV test POSITIVE Papanicolaou smear of cervix with cytologic evidence of malignancy Satisfactory cervical smear but lacking transformation zone Unsatisfactory cervical cytology smear (inadequate cervical cytology sample) Cervical low risk HPV test POSITIVE (use also 079.4) This is alist of the ICD-9 codes most commonly received by SouthEastern Pathology for this type of test. Please refer to an ICD-9 manual for a complete list and authoritative information. The ordering physician or practitioner is ultimately responsible for providing medically appropriate ICD-9 codes based on the patient’s signs and symptoms. Clinicians are reminded that tests for which Medicare reimbursement will be sought should only be ordered if medically necessary for the diagnosis and treatment of the patient rather than for screening purposes, except for those screening tests which have been specifically listed as covered by Medicare.








© Copyright 2026