
Anterior Cruciate Ligament Injuries
Anterior Cruciate Ligament Injuries http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Printout from Orthoteers.com website, member id 1969. © 2007 All rights reserved. Please refer to the site policies for rules on diseminating site content. Anterior Cruciate Ligament Injuries Anatomy & Biomechanics completely intraarticular anteromedial fibres - tight in flexion - limits anterior translation of tibia on femur posterolateral fibres - tight in extension - limits anterior translation PLUS external rotation ACL strength = 50% PCL strength Load to failure = 1700N strain rate plays a role in the location of ligament failure midsubstance tears occurring at higher rates bone ligament complex tears occurring at lower rates Blood supply - middle genicular artery (post) & synovial vessels (ant) Mechanoceptors with a proprioceptive role Examination: See Knee Examination Mechanism of Injury: substantial anterior tibial shear forces that stress ACL are produced from quadriceps contraction, esp in 0-30 deg of extension Typically, the ACL is torn in a noncontact deceleration situation that produces a valgus twisting injury - when the athlete lands on the leg and quickly pivots in the opposite direction. Associated Injuries: ( Noyes, 1980 ) 1. Meniscal tear - 62% - lateral > medial (Noyes) 2. Capsular tears - 21% 3. Chondral fracture - 10% Natural History: Controversial !? Left untreated, the torn ACL can lead to: 1. Instability (10 years following injury & exploratory arthrotomy) ( McDaniel & Dameron, 1980 ) 1/3 of patients with isolated ACL injuries will show minimal instability, with no pain or discomfort 1/3 have no pain or instability 1/3 will have significant instability & pain 2/3 returned to strenuous sports (1/3 of these had to change their specific sport) 2. Meniscal tears 3. Degenerative joint Disease (DJD) ( Jomha et al., 1999 ) 1 of 6 10/7/2007 12:43 AM Anterior Cruciate Ligament Injuries http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... cartilage damage correlates with length of time from injury; medial compartment > lateral compartment 2-3 giving-way episodes per year has been correlated with DJD most often seen in ACL deficient knees with meniscal injury 4. Quadriceps avoidance gait: between 0 to 45 deg of flexion, contraction of the quadriceps will cause anterior translation of the tibia (which is normally resisted by the ACL); maximum anterior translation of the tibia occurs at 15-25 deg of flexion There is no good evidence that brace wear decreases the rate of re-injury Low demand patients with isolated ACL injury who are willing to moderate their activity will find non-operative treatment to be satisfactory in the majority of cases (over 80%). Non-operative Treatment: Good results if: 1. thigh circumference is equal or better than opp. side 2. stable Poor results if: 1. thigh atrophy 2. meniscectomy performed 3. instability Operative Treatment: 1. Direct Repair For avulsion fractures Not recommended for mid-substance tears due to poor healing potential. 2. Extra-articular reconstruction MacIntosh Procedure: (historical) Pass a mobilised strip of iliotibial band to the posterolateral corner of the knee through a tunnel deep to the lateral collateral ligament 2 of 6 10/7/2007 12:43 AM Anterior Cruciate Ligament Injuries http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... 3. Intra-articular Reconstruction Options: 1. bone patellar bone reconstruction 2. hamstring reconstruction - semitendinosis + gracilis 3. allograft reconstruction 4. Synthetic grafts Isometry: Isometric placement of ACL refers to the concept that a full range of knee can be achieved without causing long-term ligament deformation isometry can not exist because, during ROM, there is no one point on femur that maintains a fixed distance from a single point on tibia; elongation always will occur placement of graft as closely as possible to centers of tibial & femoral attachments of anterior medial band results in least amount of strain (least change in the length of ACL during complete ROM of knee) Technique: See Wheeless 3 of 6 10/7/2007 12:43 AM Anterior Cruciate Ligament Injuries http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Post-op Care: CPM range of motion immediate post-op Closed chain exercises (foot is maintained on the ground or a platform) Running & any activity that involves excessive knee rotation (cutting) is discouraged for the first several months. Complications: 1. Loss of knee extension / Arthrofibrosis more common with early reconstruction incorrect tunnel placement can cause decreased motion and fibrosis (diagnose with x-rays & MRI) 2. Tibial tunnel syndrome incr. size of tibial tunnel over 1yr following surgery 3. Graft failures: 1. Improper placement of graft tunnels 2. Impingement of the graft in the femoral notch: 1. due to improper tunnel placement 2. due to inadequate notchplasty 3. Inadequate graft fixation 4. Associated injuries (varus knee, significant osteochondral defects) 4 of 6 10/7/2007 12:43 AM Anterior Cruciate Ligament Injuries http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... 5. CRPS (0.5%) 6. Infection (<1%) 4. Patellofemoral pain 5. Patella fractures 6. CRPS (0.5%) 7. Infection (<1%) 8. ACL Instability with Degenerative changes Ligamentous stabilisation alone often fails Usually medial compartment OA Rx: combined tibial osteotomy plus extra-articular reconstruction Noyes FR, Bassett RW, Grood ES, Butler DL J Bone Joint Surg Am 1980 Jul;62(5):687-95, 757 Arthroscopy in acute traumatic hemarthrosis of the knee. Incidence of anterior cruciate tears and other injuries. In a prospective study, all injured knees that had traumatic hemarthrosis and absent or negligible instability on clinical examination underwent arthroscopy and examination under anesthesia. Eighty-five knees (eighty-three patients) were examined over a 125-week period. Some degree of disruption of the anterior cruciate ligament was found in sixty-one (72 per cent) of the knees (a partial tear in 28 per cent and a complete tear in 44 per cent), frequently associated with an injury of varying severity to other joint structures. These included minor ligament sprains without laxity in 41 per cent, a major associated ligament injury in 21 per cent, meniscal tears in 62 per cent (partial in 30 per cent and complete in 70 per cent), and a femoral chondral fracture or surface defect in 20 per cent. A popping sensation at injury occurred in 33 per cent of knees with a normal anterior cruciate ligament and in 36 per cent of those with a disruption. One-third of the knees had no to slight pain at the time of injury. The anterior drawer test without anesthesia was positive in only 24 per cent of the knees with a torn anterior cruciate ligament. We concluded that: (1) a traumatic hemarthrosis indicates a significant knee injury; (2) examination under anesthesia plus arthroscopy allows a more accurate diagnosis of injury to joint structures; and (3) such data are required for a rational treatment program to be outlined. Jomha NM, Borton DC, Clingeleffer AJ, Pinczewski LA Clin Orthop 1999 Jan;(358):188-93 Long-term osteoarthritic changes in anterior cruciate ligament reconstructed knees. Australian Institute of Musculo-Skeletal Research, Crows Nest, NSW, Australia. To consolidate the indications for anterior cruciate ligament reconstruction and clarify the long-term prognosis associated with current surgical and rehabilitation techniques, the incidence of osteoarthritis in arthroscopically anterior cruciate ligament reconstructed knees requires investigation. Seventy-two patients with anterior cruciate ligament ruptures who were active in sports requiring sidestepping and pivoting, or who had recurrent episodes of giving way, underwent arthroscopic bone-patellar tendon-bone anterior cruciate ligament reconstruction. These patients were evaluated for meniscal damage and osteoarthritic changes at the time of surgery and followed up for 7 years. Fifty-three patients underwent radiographic evaluation at 7 years, which included anteroposterior, lateral, skyline, and 30 degrees posteroanterior weightbearing views. Radiographic evaluation was performed by three independent surgeons and graded as per International Knee Documentation Committee criteria. Results revealed that knees with chronic anterior cruciate ligament deficiency, even those with intact menisci before reconstruction, suffered early osteoarthritic changes. More severe changes were seen with meniscectomy. Acute anterior cruciate ligament reconstruction with meniscal preservation was shown to have the lowest incidence of degenerative change. Controversy exists regarding the timing of anterior cruciate ligament reconstruction. This study supports early reconstruction of anterior cruciate ligament deficient knees before episodes of giving way occur in individuals intent on continuing activities that involve sidestepping and pivoting. McDaniel WJ Jr, Dameron TB Jr 5 of 6 10/7/2007 12:43 AM Anterior Cruciate Ligament Injuries http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... J Bone Joint Surg Am 1980 Jul;62(5):696-705 Untreated ruptures of the anterior cruciate ligament. A follow-up study. Fifty patients (fifty-three knees) with surgically verified ruptures of the anterior cruciate ligament were evaluated at an average of ten years after injury. There was a high incidence of anterior laxity, rotatory instability, and meniscal tears at follow-up. The roentgenographic incidence of osteoarthritis at follow-up was low. Patients who had regained normal thigh circumference had better results than those with thigh atrophy. Although few of the patients felt that the knee was completely normal, 72 per cent of the patients returned to strenuous sports and 47 per cent felt that they had no restrictions because of the knee. This study of untreated ruptures may provide a baseline for evaluation of procedures to repair or reconstruct the anterior cruciate ligament. [ Close Window ] 6 of 6 10/7/2007 12:43 AM Knee - Osteotomies http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Printout from Orthoteers.com website, member id 1969. © 2007 All rights reserved. Please refer to the site policies for rules on diseminating site content. Knee - Osteotomies 60% of the load of the body weight passes through the medial compartment of the knee Loads up to 4 times body weight are produced on climbing stairs Osteotomy redistributes the force Valgus osteotomy most commonly performed (varus knee) and is indicated in patients that have uni compartmental disease, are less than 60 - 70 years old, are of optimal weight, have an active occupation or lifestyle which they want to maintain and have a good range of motion NB: ROM is not likely to improve with an osteotomy INDICATIONS 1. Age: physiologic age < 60 yrs in an athlete, laborer, or anyone who needs to knee down such as for gardening (TKR will generally not allow the patient to kneel) 2. Weight: > 80 kg are at increased risk for component failure; 3. Angular Deformity: 1. > 15 deg of fixed varus deformity (often patients will have varus laxity) 2. < 15 degrees flexion contracture 3. > 90 degrees flexion 4. Radiologically intact lateral (or medial) and patellofemoral compartments CONTRAINDICATIONS: 1. 2. 3. 4. Tibial Subluxation > 1 cm RA & inflammatory arthritis ACL tear osteochondral injuries with involvement of more than 1/3 the condylar surface or OCD lesion of more than 5 mm deep CLINICAL Observe patient walk (look for varus thrust) Stability Q Angle Compensatory arc of motion - to correct a valgus knee deformity - for a 20-degree varus osteotomy, 20 deg of abduction at the hip is required so pt does not end up with an adduction deformity Examine the foot and ankle to rule out fixed varus deformities which may worsen medial compartment loading Leg length discrepancy Coventry closing wedge osteotomy might be indicated, where as, if the arthritic side is shorter (than the other leg), then consider opening wedge osteotomy INVESTIGATIONS Radiology Standing long-leg film with patellae facing forward (rather than the patient's feet) Mechanical axis = centre of femoral head - medial tibial spine - centre of ankle joint Weight-bearing axis = centre of femoral head - centre of ankle joint Anatomical axis = line along axis of the femur to the intercondylar notch and the line formed by the interspinous region to the centre of the ankle Supine films Arthroscopy METHODS Medial Compartment Disease High Tibial Osteotomy (HTO) above the tibial tubercle Lateral closing wedge & fibular shortening [ Technique, Wheeless ] Overcorrection of the mechanical axis by 3 degrees is ideal 1 of 2 10/7/2007 12:44 AM Knee - Osteotomies http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Complications: 1. Undercorrection - most common 2. Overcorrection 3. Penetration of the articular surface 4. AVN of tibial plateau 5. Patella baja 6. Peroneal nerve injury 7. Anterior compartment syndrome 8. TKR may be more difficult Lateral Compartment Disease < 12 degrees valgus = Varus tibial osteotomy > 12 degrees = Medial closing wedge osteotomy of distal femur (supracondylar) RESULTS Satisfactory results obtained in as many as 70% at 10 years have been reported (study of 51 knees JBJS, 1988) with 30% fair or poor Best results are obtained if slight over correction achieved that is 2 - 3 o beyond the normal 7 o of valgus Results relate to the preoperative knee scores and the degree of correction / over-correction of the mechanical axis Odenbring et al 1990 75% of patients under the age of 50 w/ early medial DJD had at good result at 11 years post surgery Billings et al (JBJS 1999) 64 valgus producing high tibial osteotomies were performed using a calibrated cutting guide w/ plate fixation 43 out of 64 knees had a good to excellent clinical result w/ an average knee score of 94 points at an average of 8.5 years follow up using total knee arthroplasty as an end point, there was 85 % survival at 5 yrs and 53 % at 10 years no patient had patella baja postoperatively (the authors fell that early ROM w/ CPM prevented baja) average initial postoperative correction (and standard deviation) for all knees was to 9.2 - 3.69 degrees of valgus 5 knees were corrected to less than 5 deg of valgus 3 of them were treated with a subsequent arthroplasty (at twenty-four, sixty-five, and sixty-six months) 13 knees had lost more than 2 deg of correction at the time of the latest follow-up average initial postoperative correction for these knees was to 9.4 - 4.12 deg (range, 4 to 17 degrees) of valgus of knees that lost more than 2 degrees of correction, four subsequently had a total knee arthroplasty. [ Close Window ] 2 of 2 10/7/2007 12:44 AM Knee Arthrodesis http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Printout from Orthoteers.com website, member id 1969. © 2007 All rights reserved. Please refer to the site policies for rules on diseminating site content. Knee Arthrodesis Indications: 1. failed knee replacement (most common) better fusion rate following failed condylar components (80%) than failed hinged prostheses (55%) 2. uncontrollable septic arthritis with complete joint destruction 3. young patient with severe articular & ligamentous damage 4. neuropathic joint disease Contra-indications: 1. bilateral knee disease 2. ipsilateral ankle or hip disease 3. severe segmental bone loss 4. contralateral leg amputation Ideal Position: 10-15 degrees flexion 0-7 degrees valgus Techniques of Arthrodesis: 1. External Fixation Ilizarov technique minimal soft tissue dissection allows for late adjustment allows arthrodesis in the presence of active infection 2. Intramedullary Nailing Arthrodesis most reliable for achieving fusion 2 stage technique in the presence of active infection can insert nail antegrade thro the piriform fossa or thro the knee joint complication rates of 20-50% 3. Plate Fixation 2 twelve hole plates Complications: 1. Non-union- 20% 2. Malunion 3. Delayed union 1 of 2 10/7/2007 12:45 AM Knee Arthrodesis http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Ellingsen etal JBJS 76A: 870-877, 1994 18 knees with intramedullary arthrodesis after failed TKR 16/18 united , mean time to union 5.5 mths high rate of complications - 2 AKA (persisting deep infection) 1 rod #, 1 rod migration Ellingsen DE, Rand JA - Intramedullary arthrodesis of the knee after failed total knee arthroplasty. Department of Orthopedics, Mayo Clinic, Rochester, Minnesota 55905. J Bone Joint Surg Am 1994 Jun;76(6):870-7 Eighteen patients (eighteen knees) were managed with an intramedullary arthrodesis after a failed total knee arthroplasty. Twelve knees had had a revision total knee arthroplasty and six, a primary total knee arthroplasty. Three knees had had failure of a hinged prosthesis. In eleven knees, the arthroplasty had failed because of infection. Nine patients had had previous attempts at arthrodesis with external fixation. The average duration of the operation was six hours, and the average blood replacement was 2975 milliliters. A vascularized fibular pedicle graft was used in four patients. At a mean of thirty-seven months after the arthrodesis, sixteen of the eighteen patients had a complete radiographic union. The mean time to union was 5.5 months. Although a high rate of union was achieved in these patients, complications occurred in ten of the eighteen knees and this must be considered. Intramedullary arthrodesis is a successful method of salvage for a failed total knee arthroplasty or one complicated by infection that is not amenable to revision, but it is technically demanding and has frequent complications [ Close Window ] 2 of 2 10/7/2007 12:45 AM Knee Ligament Injuries http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Printout from Orthoteers.com website, member id 1969. © 2007 All rights reserved. Please refer to the site policies for rules on diseminating site content. Knee Ligament Injuries Anterior Cruciate Ligament Posterior Cruciate Ligament Posterolateral Instability & Knee Dislocation Classification of knee joint instability resulting from ligament injury: I. One-plane instability (simple or straight) A.One plane medial B.One plane lateral C.One plan posterior D.One plane anterior II. Rotary instability A.Anteromedial B.Anterolateral 1.In flexion 2.Approaching extension C.Posterolateral D.Posteromedial III. Combined instability A.Anterolateral-anteromedial rotary B.Anterolateral-posterolateral rotary C.Anteromedial-posteromedial rotary Classifications of Ligament Injury / Laxity Testing: O'Donaghue: First Degree Sprain ligament injury with no instability Second Degree Sprain Third Degree Sprain partial tear with some laxity complete tear with marked instability Noyes: Grade 1 0-5mm Grade 2 Grade 3 Grade 4 6-10mm 11-15mm 16-20mm [ Close Window ] 1 of 1 10/7/2007 12:46 AM Knee Mechanics http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Printout from Orthoteers.com website, member id 1969. © 2007 All rights reserved. Please refer to the site policies for rules on diseminating site content. Knee Mechanics KNEE RESTRAINTS - Sectioning Studies Primary Restraints Secondary Restraints 1. 2. 3. 4. 5. 6. iliotibial band: 24% mid medial capsule: 22% mid lateral capsule: 20% MCL: 16% LCL: 12% Meniscii Anterior translation ACL Posterior translation PCL (large anterior bundle more NB progressively from 0 to 90 degrees) LCL Internal rotation ACL POL/PMC has secondary effect within 0 - 45 degrees External rotation Popliteofibular ligament LCL and the posterolateral complex - mainly at 30 degrees POL/PMC flexion MCL - at all degrees of flexion Valgus Superficial MCL is the primary restraint to valgus stress at all angles (least effect at full extension) Posterior Oblique ligament (POL) - especially near or at full Postero-Medial Capsule is tightened at full extension; past extension 30 degrees it slackens ACL Deep MCL (medial capsular ligament) has little resistance to valgus load Varus LCL in all positions of flexion. Greatest effect at 30 degrees, least at full extension Posterolateral structures (Popliteofibular lig.) ACL Posterolateral Structures: 1. Arcuate Ligament 2. Fibular Collat ligament 3. Popliteus tendon 4. Popliteofibular ligament fibers originate from the popliteal tendon and insert onto the fibula deep to the arcuate ligament and its fibers orientation are opposite from the arcuate ligament See Pictures - posterior & lateral Details of Sectioning Studies KINEMATICS Instant Center of Rotation "If one rigid body rotates about another rigid body, its motion at any instant can be described by a point or axis of rotation called the instant center of rotation (ICOR)." (Simon, AAOS Basic Science 1994). Method developed by Reuleaux in 1876. 1 of 3 10/7/2007 12:48 AM Knee Mechanics http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Surface Joint Motion Motion between the tibia and the femur is both rotational and translational. The femoral condyles both roll and glide as they articulate with tibial plateaus. As the knee moves from full extension into flexion the ICOR moves posteriorly relative to both the femur and the tibia Screw Home Mechanism During the normal gait pattern the tibia undergoes internal rotation during the swing phase and external rotation during the stance phase. external rotation of the tibia on the femur occurs during the terminal degrees of knee extension, because of the difference in radius of curvature of the medial and smaller lateral condyle. This screw home mechanism in terminal extension results in tightening of both cruciate ligaments and locks the knee such that the tibia is in the position of maximal stability with respect to the femur . Patellofemoral Joint primary function of the extensor mechanism of the knee is deceleration during the swing phase of gait. Functions: 1. increases the moment arm of the quadriceps 2. allows wider distribution of compressive stress between the patellar tendon & the femur from full extension to full flexion the patella glides caudally 7cm on the femoral condyles. by 20 degrees of knee flexion the patella first begins to articulate with the trochlear groove. Beyond 90 degrees the patella rotates externally & only the medial facet articulates. At extreme flexion the patella lies in the intercondylar groove. Initially the patella contact occurs distally and with increased flexion the contact areas shift proximally on the patella patellofemoral contact pressure is 0.5 times body weight with walking, and increases to 2.5 to 3.3 times body weight with stair climbing and descending 2 of 3 10/7/2007 12:48 AM Knee Mechanics http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Sponsored Links www.biomet.co.uk www.biomet.com www.oxfordknee.net [ Close Window ] 3 of 3 10/7/2007 12:48 AM Meniscal Injuries 1 of 6 http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Printout from Orthoteers.com website, member id 1969. © 2007 All rights reserved. Please refer to the site policies for rules on diseminating site content. Meniscal Injuries Anatomy ANATOMY Function Meniscal Tears Meniscal Cysts Discoid Meniscus [Back To Top] elasofibrocartilagenous crescent shaped; triangular in cross-section anterior horns attached to each other by the small transverse anterior intermeniscal ligament lateral meniscus is more circular; medial meniscus more C-shaped lateral meniscus has twice the excursion of the medial meniscus during knee motion. anterior horn of lateral meniscus & post horns of both meniscii attach to the intercondylar eminence popliteus muscle (not tendon) is attached to lateral meniscus semimembranosis is attached to medial meniscus Blood supply: from branches of the lateral, middle & medial genicular arteries vascular synovial tissue from the capsule supplies the peripheral third of meniscus Frontal section of the medial compartment demonstrates the microvasculature of the medial meniscus. The perimeniscal capillary plexus (PCP) permeates through the peripheral border of the meniscus. F: Femur; T: Tibia. [Arnoczky SP, Warren RF. Microvasculature of the human meniscus. Am J Sports Med. 1982;10:90-95.] Constituents: 1. Type 1 collagen fibres arranged radially & longitudinally (circumferential) longitudinal fibres - dissipate hoop stresses in the meniscus 10/7/2007 12:49 AM Meniscal Injuries 2 of 6 http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... radial fibres & longit fibres - allows meniscii to expand under compressive force 2. Proteoglycans trapped within collagen fibres to absorb energy FUNCTION [Back To Top] 1. Load bearing: at least 50% of the compressive load of the knee joint is transmitted through the meniscus in extension , and approx 85% of the load is transmitted in 90 o flexion. In the meniscectomised knee the contact area is reduced approx 50% Partial meniscectomy also increases the contact pressures 2. Shock absorption: menisci may attenuate the intermittent shock waves generated by impulse loading during gait- the shock absorbing capacity of normal knees is ~ 20% higher than in meniscectomised knees. The ability of a system to absorb shock has been implicated in development of OA ( Radin and Rose " The role of subchondral bone in the initiation and progression of Osteoarthritis" CORR 213:34-40, 1986) 3. Knee joint stability: meniscectomy alone may not seriously affect stability. However, in assoc with ACL tears, meniscectomy increases ant laxity of the knee 4. Lubrication 5. Proprioception: this has been inferred from the finding of type 1 and type 2 nerve endings in the ant and post horns of the menisci MENISCAL TEARS [Back To Top] Meniscal tears can be either traumatic or degenerative in nature. Meniscal tears are uncommon in persons under 10 years of age, but become increasingly common during and after adolescence. Degenerative tears can be found in as much as 60% of the population over age 65 . The majority of these tears, however, are asymptomatic and occur in association with degenerative joint disease. The changing patterns of meniscal injury with chronological age most likely correlate with normal alterations in collagen fiber orientation with aging, as well as increasing intrasubstance degeneration. 10/7/2007 12:49 AM Meniscal Injuries 3 of 6 http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... The majority of meniscal tears affect the medial meniscus and tend to involve the posterior horn. Meniscal tears are either partial or full thickness and stable or unstable. An unstable tear is one where the entire tear or a portion thereof can be displaced into the joint space. There it may become trapped, causing pain by traction at the meniscocapsular junction. It may be responsible for symptoms of catching, locking, and effusion. Meniscal injuries can be further classified based on their tear patterns: Dandy (1990) looked at 1000 meniscal injuries ->70% were medial with a slight increase in the average age (39 years compared to 30 years for lateral meniscus injuries) Occur only when weight is being taken, in the young the knee is flexed and there is a twisting strain, in older patients tears may result from minor force The torn portion may be displaced into the joint ->locking Clinically: Acute history of injury usually with localised pain +/- locking (a locked knee will flex but not extend fully, the history of unlocking is characteristic of a mechanical block) Patients are usually fit and young and symptoms may settle but ->repeated episodes Local signs will depend on the time the joint is examined and whether or not it is still locked (usually locked in 10 o - 20 o flexion) Medial or lateral joint line tenderness and clicking with knee rotation in full flexion ->pain (McMurrays test) Special Tests for Meniscal Tears Investigation (Arthrogram) MRIMackenzie et al. Clin Radiol. 1996 - multicentre review of 2000 patients. Sensitivity 93% Specificity 84% Lat. meniscus- lower sensitivity 76% Post-meniscectomy = <25% accuracy if meniscus has been resected, 25-75% if not resected. Myxoid Degeneration of the post. third of the med. meniscus causes high signal intensity & is commonly reported as a tear. But if the signal of the 'tear' = fluid signal it is more likely to be a tear. Meniscofemoral lig. can resemble a tear of the ant. or post. horns. 60% of people >60yrs have complete meniscal tears. Intrasubstance tears common >40yrs. NB- Tear defn= must extend to articular margin on 3 consecutive slices Problems of MRI - high cost, high false negative rate Elvenes et al. Arch Orthop Trauma Surg 2000 'On the basis of the high predictive value of negative MRI, we conclude that MRI is useful to exclude patients from unnecessary arthroscopy' 10/7/2007 12:49 AM Meniscal Injuries 4 of 6 http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Classification: Grade I tear: small disruption of the homogenous signal Grade II tear: - disruption is more pronounced but does not extend thru either superior or inferior surface - arthroscopically, a grade I or II tear cannot be visualized Grade III tear: - disruption of homogenous signal w/ extension to either superior or inferior surface - is a clinically significant tear Arthroscopy Treatment: Options Conservative ->restrict activity Manipulative to reduce ->conservative treatment Operative ->arthroscopic partial menisectomy or meniscopexy Meniscal transplantation- experimental Meniscal repair Blood supply to the meniscus is age dependent- in the adult the periph 3mm as well as the ant and post horns are well vascularised Repair should be reserved for traumatic tears in the vascular region of the meniscus within 3mm of periphery = vascular ( = red- red tears) 3-5 mm from periphery = grey zone ( = red- white tears) > 5mm from periphery = avascular ( = white- white tears) Techniques: 1. Open Repair: advantage of better preparation of the tear site only the most peripheral of tears in the red-red zone are amenable to this technique because of exposure and accessibility Long-term follow-up of open meniscal repairs has revealed success rates ranging from 84% to 100%. 2. Arthroscopically assisted: 1. Inside-out technique: First described by Henning utilizes zone-specific cannulas to pass sutures through the joint and across the tear. The sutures are swaged onto flexible needles. A small posterior joint line incision is used to retrieve the sutures and tie directly on the capsule. The use of a posterior retractor, such as a gynecologic speculum, is vital in order to protect the posterior neurovascular structures. 2. Outside-in techniques: described by Warren and Morgan and Casscells involve passing sutures percutaneously through spinal needles at the joint line across the tear, and then retrieving the sutures intra-articularly. Mulberry knots can then be tied on the intra-articular free ends of the suture. A small incision is then made at the joint line, where the protruding suture ends are retrieved and tied directly on the capsule. An alternative technique is to retrieve the intra-articular portion of the suture with another pass across the tear using a wire snare and tying the suture back on itself on the capsule. This technique eliminates the need for Mulberry knots. A potential disadvantage of the outside-in technique is difficulty in reducing the tear and opposing the edges while passing the sutures. 3. All-inside technique suitable for repairs of the far posterior horns implantable anchors, arrows, screws, and staples Healing : similar to other connective tissues- exudation, organisation, vascularisation cellular proliferation , remodelling 10/7/2007 12:49 AM Meniscal Injuries 5 of 6 http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... following injury there is formation of a fibrin clot rich is inflammatory cells. Vessels from the perimeniscal capillary plexus proliferate into this fibrin scaffold , followed by mesenchymal cell proliferation forming a cellular fibrovascular scar. Modulation of this scar tissue into normal appearing fibrocartilage requires several months Approx 80% of repairable menisci are found in knees with an acute or chronic tear of the ACL- thus repair of the meniscus is linked to the management of the ACL tear NB risk of injury to peroneal n in lat meniscus repair, saphenous n in medial repair Aftercare: FWB post-op Limit knee flexion to 90 degrees Low impact activity from 3 mths Full activity at 6 mths Results of meniscal sutures: 62% heal, 17% heal incompletely and 21% do not heal 92% are clinically stable 80% return to active sport NB: 30-40% failure rate in 5 yrs in meniscal repair in knees that are ACL deficienttherefore need to reconstruct ACL to protect meniscal repair the success rate in stable knees is ~ 90% at 9 yrs MENISCAL CYSTS [Back To Top] Parameniscal cysts occur relatively infrequently They are usually associated with horizontal cleavage tears . However, isolated cysts without meniscal pathology have also been reported. Usually more common on the lateral side, but some studies report an equal incidence. Incidence ranges from 1% to 22%. Meniscal cysts typically are multilocular and are lined with synovial endothelial tissue. Aetiology theories: traumatic origin purely degenerative origin Barrie performed histopathologic studies & postulated that meniscal cyst formation originated by influx of synovial fluid through microscopic and gross tears in the substance of the meniscus. In 112 cysts, he demonstrated a meniscal tear with a horizontal component, as well as a tract that provided an exchange of fluid between the joint and the cyst. In the absence of a meniscal tear, it has been proposed that a parameniscal cyst may develop from a compression injury to the periphery of a meniscus that has central degeneration. A meniscal cyst may then develop more peripherally, leaving the body of the meniscus abnormal, but not torn. Clnical: A meniscal cyst may present with signs and symptoms consistent with typical meniscal pathology. Intermittent swelling at the joint line is variable, while pain over the area is quite common. Pisani described that a lesion that decreases in size with knee flexion and increases with extension is consistent with a meniscal cyst. Investigations: MRI is valuable for confirming the presence of a suspected meniscal cyst and identifying any concurrent meniscal tear & excluding other pathologies Management: Diagnostic arthroscopy to determine the presence of a meniscal tear. In the presence of a meniscal tear, partial meniscectomy followed by arthroscopic cyst decompression is the treatment of choice. If a tear is not confirmed at the time of arthroscopy, then open-cyst decompression with 10/7/2007 12:49 AM Meniscal Injuries 6 of 6 http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... peripheral meniscal repair becomes the logical treatment option, thereby leaving the body of the meniscus unviolated. In the presence of a small meniscal tear, an arthroscopic limited partial meniscectomy may be performed, and if no tract is identified, then conversion to an open cystectomy may similarly preserve the peripheral meniscal body References: 1. Magnetic resonance imaging of the knee: assessment of effectiveness. Mackenzie R, Dixon AK, Keene GS, Hollingworth W, Lomas DJ, Villar RN [Back To Top] Department of Radiology, University of Cambridge, UK. Clin Radiol 1996 Apr;51(4):245-50 OBJECTIVES: To quantify how magnetic resonance imaging (MRI) influences clinicians' diagnoses, diagnostic confidence and management plans in patients with knee problems. To investigate whether these changes can bring about an improvement in health. METHODS: This was a prospective observational study on all patients referred to a regional unit for MRI of the knee over a 6-month-period. Data on diagnosis, diagnostic confidence and proposed management before MRI was compared with diagnoses and actual management after MRI. In addition, short form 36 item (SF-36) health survey data was collected at referral and again 6 months later. RESULTS: Three hundred and thirty-two patients were entered into the study. MRI led to previously unsuspected diagnosis in 69 of 269 patients with available data. When MRI confirmed the clinical diagnosis, significant improvements in clinicians' diagnostic confidence were found (P < 0.01 for medical meniscus, P < 0.05 lateral meniscus, P < 0.05 anterior cruciate). MRI led to a change in management in 180 (63%) of 288 patients (where data available). There was a significant shift away from surgical management after MRI (P < 0.01). SF-36 results were available in 206 patients. There was a significant improvement over time in five of the eight SF-36 scales (four at P < 0.001, one at P < 0.01). CONCLUSIONS: Magnetic resonance imaging significantly influences clinicians' diagnoses and management plans. These patients, examined by MRI, also recorded an improvement in health related quality of life. 2. Magnetic resonance imaging as a screening procedure to avoid arthroscopy for meniscal tears. Elvenes J, Jerome CP, Reikeras O, Johansen O [Back To Top] Department of Orthopaedics, University Hospital of Tromso, Norway. [email protected] Arch Orthop Trauma Surg 2000;120(1-2):14-6 The objective of this study was to evaluate the role of magnetic resonance imaging (MRI) as a screening procedure before arthroscopy of meniscal tears. Forty-one knees in 40 patients underwent MRI and arthroscopy. Compared with arthroscopy, the sensitivity, specificity, positive predictive value and negative predictive value for MRI for the medial meniscus were 100%, 77%, 71% and 100%, respectively, while the values for the lateral meniscus were 40%, 89%, 33% and 91%, respectively. The overall accuracy for MRI of the medial and lateral menisci combined was 84%. On the basis of the high predictive value of negative MRI, we conclude that MRI is useful to exclude patients from unnecessary arthroscopy. 3. DeHaven and Arnoczky " Meniscal repair- Part 1: Basic science, Indications for repair and open repair" JBJS 76A: 140-152, 1994 4. Dehaven etal " Open meniscal repair. Technique and 2-9 yr results" Am J Sports Med 17:188-795, 1989 5. Cannon and Morgan " Meniscal repair- Part 2: Arthroscopic repair techniques" JBJS 76A: 294-311, 1994 6. Meniscal Lesions: Diagnosis and Treatment. Robert S. P. Fan, MD, Richard K. N. Ryu, MD. [Medscape Orthopaedics & Sports Medicine 4(2), 2000. © 2000 Medscape, Inc.] [ Close Window ] 10/7/2007 12:49 AM Meniscal Special Tests http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Printout from Orthoteers.com website, member id 1969. © 2007 All rights reserved. Please refer to the site policies for rules on diseminating site content. Meniscal Special Tests Numerous rotation tests for meniscal pathology have been described- all have the common purpose of trapping abnormally mobile or torn fragments of menisci between the joint surfaces, causing pain or clicking. McMurray Test ( McMurray, TP: "The Semilunar Cartilages" Br J Surg 29: 407, 1941 ) - intended to diagnose lesions of the posterior horn of the meniscus Pt supine, hip flexed 90o and knee flexed more than 90o. For examining the R knee, the examiner stands to the pts R side with L hand on the knee and R hand holding the foot. The foot is taken from a position of abduction and ER to one of adduction and IR- this is repeated for various angles bw full flexion and 90o- trapping of damaged meniscus is felt as a clunk by the fingers on the jt line Steinmann Test ( Ricklin etal, " Meniscal lesions: Problems of clinical diagnosis , arthrography and therapy", Grune and Stratton, Orlando, FL, 1971) Pt seated and with knee hanging loose over the edge of the table- knee flexed at least 90o, foot grasped and tibia is sharply rotated into IR then ER- a meniscal lesion is demonstrated by pain at the appropriate jt line 1 of 2 10/7/2007 12:51 AM Meniscal Special Tests http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Apley Test ( Apley AG: " The diagnosis of meniscus injuries: some new clinical methods" JBJS 29B:78, 1947) Pt prone , knee flexed > 90o, downward pressure is applied to the foot and the jt surfaces thereby rotated and compressed slightly. The maneuvre is repeated this time with sistraction rather than compression. Meniscal lesions will be demonstrated by clicking or pain in the compression part of the test, while ligamentous injuries cause pain when the jt is distracted Images from - Insall JN. Examination of the knee. In: Insall JN, ed. Surgery of the Knee. New York, NY: Churchill Livingstone; 1984: [ Close Window ] 2 of 2 10/7/2007 12:51 AM Osteochondritis dissecans http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Printout from Orthoteers.com website, member id 1969. © 2007 All rights reserved. Please refer to the site policies for rules on diseminating site content. Osteochondritis dissecans Definition A localised condition affecting an articular surface that involves separation of a segment of cartilage & subchondral bone. Bilateral in 20-30% posterior lateral aspect of the medial femoral condyle in 70% lateral femoral condyle in 20% patella in 10% Guhl Arthroscopic Classification Lesions are classified based on articular cartilage integrity (open or closed) and the stability of the underlying subchondral bone and its bed (stable or unstable). (Clanton & DeLee, CORR 1982); A - Intact lesions B - Lesions showing signs of early separation C - Partially detached lesions D - Craters with loose bodies (salvageable or unsalvageable) Investigations X-rays & tunnel views MRI - to assess the fragment's articular cartilage continuity and the size and viability of its subchondral bone. Natural History The natural history is directly dependent on age at presentation (Pappas Classification): In the juvenile type (patients with completely open distal femoral physis), the prognosis is excellent if the lesion is a closed, stable one. In the adolescent with partial physeal closure, the prognosis is unknown because the lesion may act as either the juvenile or adult type. The adult type (closed physis) has a poorer prognosis because of the limited healing 1 of 3 10/7/2007 12:51 AM Osteochondritis dissecans http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... potential of the lesion. Treatment (based on Pappas) Skeletally Immature Patient (< 12yrs): Non Operative treatment is recommended, since the lesion will frequently heal if the fragment has not detached. Articular cartilage overlying these lesions should be normal & should protect the OCD defect during healing. Protected crutch walking and gentle ROM, since ROM is thought to have beneficial effects on cartilage healing. Skeletally Mature Patient (> 12yrs): Guhl recommends arthroscopic evaluation and treatment of all patients who are 12 years of age or older as determined by bone age roentgenograms, and who have lesions larger than 1 cm in diameter located primarily in a weight-bearing area. Treatment of the lesion is based on the arthroscopic examination. Lesions that are massive (over 3 cm in diameter), lesions having large or multiple loose bodies that are thought to be replaceable, or lesions that are inaccessible to arthroscopic techniques are best treated by open arthrotomy. Arthroscopic method: 30-degree viewing arthroscope through the anterolateral portal and a probe through the anteromedial portal. Removal of any loose bodies Carefully probe the area of OCD. Stable - If the surface is basically smooth, with only an area along the margin of the lesion fissured and loose, the disorder is classified as an early separated lesion. Before overlying articular cartilage has separated, antegrade or retrograde arthroscopic drilling yields successful results Unstable - Pushing on the lesion with the arthroscope or probe will reveal only minor movement of the fragment where the articular surface defect is present. Carefully debride this defect in the articular surface with basket forceps or a small curette through the anteromedial portal. Secure the fragment in its bed using cannulated differential pitch screws (e.g. Herbert), whose low-profile head & compressive effect help prevent iatrogenic articular trauma while promoting chondro-osseous repair.. Kirschner wires introduced under arthroscopic control have been used in the past. Other New & Experimental Treatments for irreparable lesions in the weightbearing zone: 1. 2. 3. 4. 5. 2 of 3 Soft tissue grafts - periosteal / perichondral Chondrocyte transplantation Mosaicplasty (See Maitrise Orthopedique) Artificial matrix - carbon fibre, collagen, polylactic acid Fresh osteochondral grafts (allograft) [Kish et al. Clin Sports Med 1999 Jan;18(1):45-66, vi] 10/7/2007 12:51 AM Osteochondritis dissecans http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Mosaicplasty Patellar OCD Uncommon and presents as mechanical knee pain during adolescence. The lesion occurs in the distal half of the patella. 30% of the lesions are bilateral. The differential diagnosis should include dorsal patellar defect, infection, or tumor. The prognosis for patellar OCD is even less clear than it is for femoral OCD. Subchondral bed sclerosis denotes a poor prognosis, similar to femoral lesions. Osteochondritis dissecans. History, pathophysiology and current treatment concepts. Clanton TO, DeLee JC ; Clin Orthop 1982 Jul;(167):50-64 The past and current status of osteochondritis dissecans suggests that there is still no clear cut etiology. The etiologic mechanism is generally assumed to be multifactorial and related to minor trauma occurring at a susceptible locations. The existence of two clinical patterns is important. Conservative treatment should be emphasized in the young patient who has open physes and a more aggressive approach in the older symptomatic patient. Drilling has a use in the loose unseparated fragment. Free fragments should be replaced when possible if they involve a portion of the weight-bearing articular surface. When replacement is impossible, treatment must be individualized, either by trephining or spongialization followed by joint ranging exercises with nonweight-bearing, or in cases which involve a large portion of the weight-bearing surface of the femoral condyle, a more radical treatment, including osteotomy, hemiarthroplasty, or allograft Arthroscopic treatment of osteochondritis dissecans. Guhl JF; Clin Orthop 1982 Jul;(167):65-74 Forty-nine knees with osteochondritis dissecans were evaluated and in many cases, treated by arthroscopic means. The lesions were classified as to location and degree of separation. Arthroscopic treatment involved drilling, pinning, reduction of fragments, removal and replacement of fragments, and bone grafting. Of the cases, 90% had healed in an average period of approximately five months. The mean follow-up was three years. [ Close Window ] 3 of 3 10/7/2007 12:51 AM Patellofemoral Disorders http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Printout from Orthoteers.com website, member id 1969. © 2007 All rights reserved. Please refer to the site policies for rules on diseminating site content. Patellofemoral Disorders Anatomy & Mechanics Anatomy Clinical Investigations Patellofemoral Trauma Non-arthritic patellofemoral pain [Back To Top] Wiberg's Classification of patella shape: (Descriptive only and has no correlation to pathological conditions) Type I Concave facets, symmetrical and equal in size (10%) Type II Medial facet is smaller. Lateral facet is concave (65%) Type III Medial is distinctly smaller with marked lateral predominance (25%) Patellofemoral kinematics [Back To Top] Patella increases the moment arm of the quadriceps thus increasing quad strength by 33-50% The femur articulates only with a portion of the patella in each position of flexion, moving from proximal to distal with increasing flexion Patellofemoral joint reaction force 0.5 times body weight with walking 3.3 times body weight with stairs CLINICAL [Back To Top] History Determine if complaint is instability or pain Examination (Also see Torsional Profile Assessment ) Standing examination Varus/ valgus alignment Examination of gait Pelvic obliquity and leg length inequality Q-angle Femoral and tibial torsion Miserable malalignment syndrome : internal torsion of the femur, external torsion of the tibia and pronated feet Position of subtalar joint. Pes planus. Sitting examination Grasshopper eyes appearance: high and lateral patellas VMO atrophy Lateral patellar tilt Patellar tracking: pain and crepitation, 'J' sign 1 of 7 10/7/2007 1:01 AM Patellofemoral Disorders http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Position of the tibial tubercle with respect to the midline of the trochlea - Should lie < 20mm lateral to the midline of the femur Supine examination Q angle (Normal M 10 o F 15) Quadriceps mass (VMO atrophy) Hamstring tightness (popliteal angle) Examination for medial plica Tibial torsion Tenderness on quadriceps or patellar tendon insertion, patellar facets, retinaculum tightness hamstrings, or heel cord Crepitation and patellar compression Apprehension test (20-30 o flexion) Clarke's Snatch test (pain on contraction of the quadriceps with the patella fixed) Patellar tilt (evaluates tension of the lateral restraint) Patellar glide test (knee flexed 20 to 30 o ) Decreased: 1 quadrant or less medial glide is indicative of tight lateral restraint increased: subluxable, or dislocatable patella Prone examination Hip motion - femoral neck anteversion (abnormal if IR exceeds ER by more than 30 o ) Quadriceps tightness - Ely test (especially rectus femoris) Leg-heel alignment (Normal 2-3 o of varus) Hindfoot-forefoot alignment: (Normal: long axis of heel 90 o perpendicular to transverse axis of forefoot) INVESTIGATIONS [Back To Top] Radiography AP + True lateral view Blumensaats line Insall / Salvati Ratio Skyline views: Merchant view Laurin view (30deg. flexion) More Detail in Patellofemoral Instability & Summary Table CT More accurate assessment of sulcus and congruence angle Perform with knee in different positions of flexion and with/without quads contraction Magnetic Resonance Imaging 2 of 7 10/7/2007 1:01 AM Patellofemoral Disorders http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Midpatella transverse images with knee flexed 15 o Allows assessment of other areas of the knee: articular cartilage, muscle and supporting retinacular structures Dynamic MRI to assess patella tracking Patellofemoral Trauma [Back To Top] Patella fracture ************** Patellar stress fractures Rare overuse injury reported in endurance runners, volleyball players, fencers and high jumpers (Orava 1996, Iwaya 1985)) Two types: longitudinal and transverse (Iwaya 1985) In cases with delayed diagnosis operative treatment Quadriceps or Patellar tendon rupture Non-arthritic patellofemoral pain [Back To Top] Also see Differential Diagnosis of Anterior Knee Pain 1. Patellar tendonitis (Jumpers knee) Secondary to repetitive trauma: running, jumping and kicking sports Tenderness usually on the inferior pole Classification I Pain only after activity II Some pain with activity, does not interfere with participation III Pain during and after participation. Interferes with competition Treatment Activity modification, warm-up, stretching, ice, NSAID's Initially as above. If fails then: Steroid injection IV Complete tendon disruption 2. Plica syndrome Surgical debridement Primary repair of the tendon [Back To Top] Medial patellar (most common), lateral and suprapatellar Inflammation and impingement on medial femoral condyle Treatment NSAID's, quadriceps exercises Steroid injection Arthroscopic excision if symptoms persist. 3. Chondromalacia [Back To Top] "softening" of the articular cartilage Aetiology 50% idiopathic 15% post traumatic 3 of 7 10/7/2007 1:01 AM Patellofemoral Disorders http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... 20% secondary to maltracking- lateral patellar compression syndrome 15% due to unstable (recurrent dislocaters) patellae Treatment is dependent on cause Classification (Outerbridge) I Articular cartilage softening II Chondral fissures and fibrillation < 1.25mm III Chondral Fibrillation > 1.25 mm (crabmeat changes) IV Exposed subchondral bone 4. Osteochondritis dissecans (OCD) Knee is most common site Typically in teenage athletes Location in the patella is rare Medial facet (70%), lateral facet (30%) More Detail 5. Dorsal defect of the patella Benign lesion - Non-specific fibrous tissue Located along the superolateral aspect of the articular surface of the patella Radiolucency with sclerotic margins and intact overlying articular cartilage Frequently heals spontaneously by sclerosis 6. Bipartite patella [Back To Top] Evident in 15% of people in childhood and 2% in adulthood 57% are unilateral with a male:female ratio of 9:1 Classification (Saupe) Type I Distal pole Type II Lateral Type III Supero-lateral 7. Reflex sympathetic dystrophy see CRPS 8. Patellofemoral Malalignment [Back To Top] Medial patellar subluxation/dislocation Usually iatrogenic, secondary to realignment procedures, but has also been described without previous surgery (Richman 1998) When associated with internal tibial torsion If Tibio-Tubercle distance is decreased: external derotational tibial osteotomy proximal to tibial tubercle If Tibio-Tubercle distance is normal: external derotational tibial osteotomy distal to tibial tubercle Lateral patellar subluxation/dislocation 5% are associated with an osteochondral fracture Treatment First time instability episode with no malalignment and normal radiographs 4 of 7 10/7/2007 1:01 AM Patellofemoral Disorders http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... immobilisation followed by early range of motion and PT If osteochondral loose bodies are present = arthroscopy with removal or anatomical reduction and fixation Classification (Fulkerson) I II III IV Subluxation alone Subluxation and tilt Tilt alone No malalignment Subdivided: A Absence of articular lesion B Presence of minimal chondromalacia C Presence of osteoarthritis Relationship of patellofemoral malalignment to femoral and tibial torsion Internal femoral torsion / Femoral Neck Anteversion Toeing-in if it exists alone and external rotation of hip < 30 o Feet straight : if compensatory external tibial torsion, pes planus, or external hip rotation at o More Detail External tibial torsion Primary or secondary to medial femoral torsion Primary deformity responsible for PF malalignment Gait with normal foot progression angle (straight ahead) but with kneeing-in medial thrust with stance phase. More Detail Treatment Conservative Activity modification, rest, NSAID's and rehabilitation are successful in 90% Supervised exercise program should be continued for at least 6 months Patellar taping (Powers et al, 1997): Average pain reduction of 78% Taping changes the timing of VMO and VL activity in subjects with patellofemoral pain during step-up and step-down tasks When the patellofemoral joint was taped, the VMO was activated earlier. (Guilleard et al 1998) Surgical A. Proximal realignment procedures: 1. Lateral release (open or arthroscopic) Indication: for patellar tilt < 8 degrees or lateral retinacular tightness Do only when it is tight Adequate release should allow inversion of patella to 70-90 degrees 5 of 7 10/7/2007 1:01 AM Patellofemoral Disorders http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... The superficial and deep layers of the retinaculum must be divided. Best results in patients with pain. Worse in patients with instability and severe DJD. 85 % good results in patients with pain and radiographic evidence of tilt and Outerbridge I chondromalacia (Oglivie-Harris 1984) 92% good & excellent results in patients with minimal articular degeneration and tilt (Shea, 1992) 2. Lateral release and medial plication (proximal realignment) Attempt to decrease the valgus quadriceps moment on the patella Indication : retinacular tightness and medial laxity for recurrent lateral subluxation /dislocation in skeletally immature patients 82% good/excellent results in patients with instability (Scuderi 1988) Poor results in patients with significant chondromalacia 3. Galleazi procedure (semitendonosis tenodesis) Reconstruction with semitendonosis tendon Tensioned at 30 o of flexion B. Combined Proximal and distal realignment procedures 1. Lateral release with medialisation of tibial tubercle (Elsmlie-Trillat) Best candidates have recurrent instability, evidence of increased Q angle and minimal, if any articular degeneration 2. Lateral release with antero-medialisation of the tibial tubercle (Fulkerson) Biomechanical studies have shown that the patellofemoral joint reaction force decreases about 50 % after a 2-cm anteriorisation of the tibial tubercle Due to the obliquity of the osteotomy, no bone graft is necessary. Best suited for patients with documented lateral patellar tilt and with Outerbridge grade III-IV chondrosis Summary of distal realignment procedures: 1. Hauser (Abandoned) Tibial tubercle osteotomy with the tubercle moved medial, distal and posterior Complicated by development of patellofemoral DJD in 70 % of patients because of increased PFJ joint reaction forces (Hampson et al, 1975) 2. Goldthwaite-Roux 3. Hemi-patellar tendon transfer Ú ± lateral release/medial reefing 4. Elmslie-Trillat Medialisation of tibial tubercle + lateral release + medial capsular reefing Considered when there is minimal or absent articular injury in patients with lateral instability caused by malalignment Good/excellent results in 81% (Brown, 1984) Best results when postoperative congruence angle < 15 o (Shelbourne et al, 1994) 5. Fulkerson Anteromedial tibial tubercle osteotomy 6 of 7 10/7/2007 1:01 AM Patellofemoral Disorders http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Malalignment and lateral facet chondrosis Slope of cut dependent on amount of subluxation and DJD Not as successful with medial facet chondromalacia 90% good/excellent results (Fulkerson et al.1990) 6. Maquet Elevation (anteriorisation) of tibial tubercle Salvage operation in patellofemoral DJD without malalignment Risk of anterior skin necrosis when anteriorisation > 2 cm C. Patellofemoral arthroplasty Hemiarthroplasty (patellar resurfacing) or total patellofemoral arthroplasty Indicated for OA of the patella and trochlea Great care must be taken to ensure that any malalignment or maltracking is identified and corrected otherwise the procedure will fail Lubinus Avon D. Femoral osteotomy (Albee) For trochlear dysplasia Elevation of the lateral facet of the femoral trochlea with osteotomy and bone graft E. Patellectomy Last resort surgery which may not eliminate pain Complicated by loss of quadriceps strength 30 to 50% Satisfactory results in 77% (Blatter et 1988) Sponsored Links www.biomet.com [ Close Window ] 7 of 7 10/7/2007 1:01 AM Patello-Femoral Instability http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Printout from Orthoteers.com website, member id 1969. © 2007 All rights reserved. Please refer to the site policies for rules on diseminating site content. Patello-Femoral Instability PFJ Mechanics Presentation Anterior Knee Pain Radiology Radiology Summary Treatment Patello-femoral Joint Mechanics Risk Factors [Back To Top] Patella increases moment ( lever ) arm of extensor muscles Slides 7 cm in trochlear groove Patello-femoral contact minimal until 20 deg flexion Contact area moves from proximal -> distal in trochlea & distal to proximal on patella > 90deg flexion quads tendon is in contact with the trochlea 10deg flexion -> lever arm increased 10 % 45deg -> 30 % then decreases Patello-femoral joint reaction force determined by quads force and amount of knee flexion Normal walking -> joint compressive forces = half bodyweight Up stairs -> 2.5 - 3.3 times body wt Deep knee bends -> 7-8 x body wt Presentation [Back To Top] PFJ instability may present as: 1. Anterior Knee Pain 2. Patello-femoral subluxation 3. Patello-femoral Dislocation Anterior Knee Pain [Back To Top] Other causes of anterior knee pain include: 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. Patello-femoral overload (Chondromalacia) Plica Syndrome 'Jump' knee (enthesitis of patella tendon origin) Sindig-Johansson-Larsen's disease (traction tendinitis at lower pole of patella, w/ calcification) Torn Meniscus Discoid Meniscus Osteochondritis Dissecans Patella Bursitis Bipartite Patella Patella cysts or tumours Risk Factors / Causes (Hedden (Toronto); Curr Orth. 9:249-52. 1995): [Back To Top] A. Bony (Static Stability) Shallow femoral trochlea (Dejour et al.) Hypoplastic lateral femoral condyle Patella Shape (Shutzer et al.) Patella Alta B. Malalignment External tibial torsion Incr. femoral anteversion Incr. genu valgum Incr. Q angle (unreliable) C. Soft Tissue (Dynamic stability) Ligamentous laxity contribution of distal oblique portion of vastus medialis muscle is critical (tight hamstring & gastrocnemius w/ pronated feet) Clinical 1 of 4 [Back To Top] 10/7/2007 1:02 AM Patello-Femoral Instability http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Mechanism of injury, acuity, previous treatment, and status of the opposite knee. Q angle The integrity of the ACL (because similar derotation, deceleration mechanisms that cause patellar instability can cause ACL injury) Radiology [Back To Top] Lateral X-ray: Should be with knee at 30deg. flexion (Patella is centered in trochlear groove at 30deg flexion) The superior pole of the patella should not be higher than a line extended form the central part of the distal femoral growth plate = Blumensaat's Line Insall-Salvati index- length of patella tendon to length of patella, normal=1. Patella Baja = < 0.8 Blackburne-Peel index - length of patella articular surface to the distance of its inferior margin from the tibial plateau w/ knee in 30deg. flexion. normal=0.8-1.1. More accurate. Skyline View: See Summary Table Trochlear signs- Crossing sign, 'Bump' sign, Dysplastic condyles, Trochlear depth < 8mm. MERCHANT AXIAL/ SKYLINE X-RAY ( Merchant; JBJS, 56-A:1391-6, Oct 1974 ): = the patient on their back with the knee flexed 45deg. over the end of the table & with the XR cassette resting on the shin & at 90deg. to the XR beam which is angled at 30deg. to the horizontal. From This: 1) Sulcus angle of Brattström : N=126-150deg. (avg. 143deg.). ( Buard et al. / Brattstrom. Acta Orthop Scand. Vol 68. 1969. p 135 ) 2) Congruence angle : betw. a line bisecting the sulcus angle & a line thro the lowest point of the patella articular ridge. = -ve on the medial side, +ve on lateral side. N= -16 to +4deg. 2 of 4 10/7/2007 1:02 AM Patello-Femoral Instability http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... LAURIN LAT. PATELLOFEMORAL ANGLE ( Laurin et al.; CORR, 144:16-26, 1979 ): Taken w/ knee in 20deg. flexion. Lateral PF angle= betw. a line across the tops of the femoral condyles & a line along the lat. facet of patella. If the lines are parallel or open medially = AbN. AP & Tunnel views: for osteochondral fractures. CT Scan CT is helpful in assessing the relationship of the patellofemoral joint in terms of tilt or translation, or both. Arthroscopy Use a suprapatella portal to watch patella centre in trochlear groove betw. 30-60deg. Treatment [Back To Top] Treatment is individualized and is based on the patient's lower extremity alignment, joint motion, ligamentous laxity, muscle strength, and quadriceps competence. The goal of treatment is to prevent recurrence. PROXIMAL REALIGNMENT to alter the tension of tissues attached to the patella.(Lat release & med. reefing) Arthroscopic evaluation of articular surface injury with removal or replacement of osteochondral fragments Lateral retinacular release Direct medial retinacular repair in acute dislocations. Quadriceps transfers, particularly the vastus medialis obliquus are used to restore medial vector balance (Medial plication). Medial hamstring transfer (Galeazzi technique) may be required to provide a tenodesis effect in troublesome cases. DISTAL REALIGNMENT to transpose the tibial tubercle 3 of 4 10/7/2007 1:02 AM Patello-Femoral Instability http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Elmslie-Trillat Procedure: medial tibial tubercle transfer which has no posterior displacement does not involve anterior / posterior displacement of the tuberosity References: 1. Use of a modified Elmslie-Trillat procedure to improve abnormal patellar congruence angle ( Shelborne , 1994). 2. An evaluation of the Elmslie-Trillat procedure for management of patellar dislocations and subluxations. A preliminary report. Cox JS. Americal Journal of Sports Medicine. 4: 72-77, 1976. Goldthwaite-Roux Procedure: The patella tendon is split & the lateral half is passed under the medial half & attached to the periosteum on the tibia in a medial position. Hauser Procedure: (Historical) Involves medialization of the tibial tubercle in order to decrease Q angle. due to the anatomy of the proximal tibia, translating the tibial tubercle medially, will also translate the tubercle posteriorly. Posterior translation of the tibial tubercle will have the effect of increasing patellofemoral contact pressures which leads to pain and OA. Also can produce a low patella (baja) Maquet Procedure: (Historical) Anterior translation of the tibial tubercle which has the effect of decreasing patellofemoral contact forces. Patients with pain due to early patellofemoral arthrosis may expect pain relief following the Maquet Procedure. Disadvantages with this procedure include high incidence of skin necrosis, compartment syndrome and no effect on the Q angle; A combination of tibial tubercle transfer, proximal lateral release, medial capsulorrhaphy and tendon transfer may be required to establish appropriate alignment. Contra-indications to Re-alignment: absence of clear physical examination and radiographic findings of subluxation patellofemoral pain which results from "dashboard" car accident injuries these patients often have significant patellofemoral pain and extensive patellar chondromalacia, but do not tend to improve with surgery Patellar instability associated with abnormal ligamentous laxity; eg, Down syndrome and Ehlers-Danlos syndrome, presents a significant challenge. These patients must be advised of the abnormal nature of their collagen biology and should recognize that surgical reconstruction may not overcome this genetic predisposition for instability. In general, patients with Down syndrome function quite well, despite chronic patellar displacement due to a combination of increased laxity, genu valgum, and hypotonia. Further Reading: D. Dandy; JBJS: 78-B(2):328-35. Mar 1996 [ Close Window ] 4 of 4 10/7/2007 1:02 AM Posterior cruciate ligament injury http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Printout from Orthoteers.com website, member id 1969. © 2007 All rights reserved. Please refer to the site policies for rules on diseminating site content. Posterior cruciate ligament injury Anatomy & Mechanics: orientated vertically blends with post horn lateral meniscus prevents post translation of tibia on femur & prevents hyperextension Secondary constraints are: posterolateral complex & MCL. Twice as strong as ACL: 1. larger cross-sectional area 2. higher tensile strength 3. located closer to the central axis of the knee joint Mechanism of Injury: Direct blow causing posterior displacement of tibia in a flexed knee Hyperextension injury Site of Injury: Femoral avulsions in 25% Tibial Avulsions in 25% Midsubstance tears in 50% Associated Injuries: MCL - When PCL injury occurs with MCL injury, expect large increase in valgus instability when the knee is in full extension Posteromedial Capsule - 10-90% ACL - 50% Meniscal tear - 30% It is important to distinguish one plane PCL posterior instability from posterolateral instability because isolated PCL reconstruction will not correct the rotatory instability Examination: See Knee Examination Natural History: Unknown Most with unidirectional instabillity probably return to pre-injury functional level, but most reports in the literature have relatively short follow-up and include a mix of acute and chronic injuries, as well as isolated and complex ligament injuries. Poor results of non-operative management are associated with: 1. meniscectomy 2. quadriceps insufficiency 3. patellofemoral disease (tibial drop-back shortens the patellar tendon moment arm) 1 of 2 10/7/2007 1:02 AM Posterior cruciate ligament injury http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Management: Traditionally, most authors have recommended nonoperative treatment for isolated posterior cruciate ligament tears. Proven methods for reconstructing this ligament are few most surgeons have had limited experience with these procedures results often are unpredictable no association with OA shown with non-operative treatment [ Close Window ] 2 of 2 10/7/2007 1:02 AM Spontaneous Osteonecrosis of the Knee http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Printout from Orthoteers.com website, member id 1969. © 2007 All rights reserved. Please refer to the site policies for rules on diseminating site content. Spontaneous Osteonecrosis of the Knee First reported by Alback et al. in 1968. They described a radioluscent area in the femoral condyle surrounded by a sclerotic halo and associated with a focally active bone scan. Believed to be an important but underestimated cause of osteoarthritis of the knee Can occur in the medial femoral condyle, lateral femoral condyle or medial tibial plateau Aetiology Unknown Vascular or traumatic lesions are the two main theories Trauma theory: elderly women, who may be relatively osteoporotic, minor trauma causes a microfracture in the subchondral bone; this allows fluids to be expressed through the articular cartilage into the subchondral bone and marrow space, creating increased interosseous pressure and pain. This increased pressure in a closed space interferes with the blood supply and initiates the cycle of compromised circulation and resultant osseous ischaemia. Secondary causes of AVN of the knee: 1. Steroids 2. Alcohol 3. renal transplantation 4. Gaucher disease 5. haemoglobinopathies 6. Caisson disease 7. SLE 8. etc. Spontaneous Osteonecrosis of the Femoral Condyles Clinical Typically female > 60yrs sudden onset of severe pain on the medial side of the knee pain worse at night well localised tenderness over the affected condyle Radiology X-Rays Stage-1 Stage 2 Stage 3 Stage 4 Stage 5 1 of 3 normal (In some patients a radiographically visible lesion never develops, and the symptoms resolve spontaneously) slight flattening on the convexity of the condyle area of radiolucency surrounded by a sclerotic area in the subchondral bone the radiolucency is surrounded by a definite sclerotic halo, of variable thickness and density secondary OA changes 10/7/2007 1:02 AM Spontaneous Osteonecrosis of the Knee http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Bone scans Increased uptake is necessary to make the diagnosis The osteonecrotic lesion appears as a focally intense area of uptake over the affected femoral condyle. MRI extremely valuable in defining osteonecrosis about the knee T1 - discrete low-intensity signal in the femoral condyle T2 - corresponding low signal-intensity area in the central lesion, with a high-intensity signal about the margin (oedema surrounding the lesion) Prognosis Prognosis is related to the size of the lesion at presentation a large lesion (> 50% of the width of the femoral condyle, or > 5cm2) become disabled with increasing pain, deformity, and eventually secondary destruction of the joint. Treatment Making the diagnosis is the most NB as arthroscopy or meniscectomy are initiated before the diagnosis is established. Only later, when the condyle has collapsed, is the correct diagnosis recognized Initially, most patients should be treated conservatively, as the stage of the lesion and the 2 of 3 10/7/2007 1:02 AM Spontaneous Osteonecrosis of the Knee http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... size of the osteonecrotic segment are not clearly defined at the onset of symptoms. If the lesion is small, it will do well and no surgical treatment is required Surgical options for the more advanced stages: arthroscopic debridement proximal tibial osteotomy drilling, with or without bone-grafting Core decompression prosthetic replacement allografting [ Close Window ] 3 of 3 10/7/2007 1:02 AM Antibiotics 1 of 7 http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Printout from Orthoteers.com website, member id 1969. © 2007 All rights reserved. Please refer to the site policies for rules on diseminating site content. Antibiotics Choosing an Antibiotic Choosing an antibiotic Types of Antibiotics Forms of Antibiotic Delivery [Back To Top] Consider patient factors: 1. Allergy 2. Renal and hepatic function 3. Immune status 4. Ability to tolerate oral medication 5. Severity of the illness 6. Pregnancy, breastfeeding, taking oral contraceptive? Consider the organism : 1. What is the likely organism? 2. What is its likely or proven sensitivity? Before starting therapy Always take samples for C+S, do not prescribe blindly before samples taken Dose will vary according to age, weight, renal function and severity of infection Route of administration depends on the severity of the infection, Duration of therapy, for most conditions 5 days is enough but for TB or osteomyelitis relatively long courses required Remember the risk of superinfection (eg pseudomembranous colitis, candida) more likely with broad spectrum antibiotics Prophylaxis against infection Cephalosporin given perioperatively when hardware is inserted (cefuroxime) Grade 1 and 2 open fractures, cephalosporin (cefuroxime) Grade 3A open fractures, cephalosporin and an aminoglycoside (cefuroxime and Gentamycin) Grade 3B open fractures, add in Penicillin to Cefuroxime and Gentamycin and Metronidazole Joint prostheses and dental treatment- The advice of the working party of the British Society for Antimicrobial therapy is that patients with prosthetic joints do not require antibiotic prophylaxis for dental treatment. Joint infections have rarely been shown to to follow dental procedures (BNF) Prior to urinary catheterisation during perioperative period for joint replacement = Gentamycin IM (Controversy about whether it is necessary) Ritter MA, Fechtman RW. Orthopedics 1987 Mar;10(3):467-9. Urinary tract sequelae: possible influence on joint infections following total joint replacement. A total of 277 patients receiving 364 total joint replacements in a period of 2 years were analyzed to determine whether urinary tract sequelae (infections, catheterization, and genitourinary instrumentation) encountered preoperatively or perioperatively had any significant influence on the development of postoperative joint infections. Three of these patients developed joint injections, none as a result of urinary tract infection. None of these infected patients required any catheterizations or instrumentation of the genitourinary system postoperatively. To enhance the previous data, all joint infections encountered in a period of 16 years were analyzed using the same criteria. Only one 10/7/2007 1:03 AM Antibiotics 2 of 7 http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... infection spread hematogenously from a urinary tract infection, and this occurred 20 months after surgery. The results of this study show no correlation between preoperative or perioperative urinary tract sequelae and postoperative joint infections. Bacteriuria should not be considered a contraindication for total joint replacement. Treatment of infection (Common infections seen in orthopaedic patients) Osteomyelitis and septic arthritis Clindamycin alone or Flucloxacillin and Fusidic acid. If Haemophilus influenza (age<5 yrs) add Amoxycillin or Cefuroxime. (decreasing due to HIB vaccine) Treat acute disease for at least 6 weeks and chronic disease for at least 12 weeks Cellulitis Phenoxymethylpenicillin (oral) or Benzylpenicillin (IV) and Flucloxacillin (oral or IV). Or Coamoxiclav alone. If penicillin allergic, use erythromycin alone Animal bites Coamoxyclav (Augmentin) Hospital acquired Pneumonia Broad spectrum cephalosporin- cefatoxime or ceftazidime Or anti pseudomonal penicillin(eg piperacillin) and an aminoglycoside (Gentamycin) Exacerbations of chronic bronchitis Amoxycillin or trimethoprim or tetracycline Uncomplicated pneumonia Amoxycillin Erythromycin if penicillin allergic Add flucloxacillin if staph aureus suspected eg in influenza or measles Urinary tract infection Trimethoprim, amoxycillin or cephalosporin TB Initial phase for 2 months, 4 drugs Continuation phase, 4 months, 2 drugs Isoniazid (Throughout 6 months) Rifampicin (Throughout 6 months) Pyrazinomide (first 2 months only) Ethambutol (first 2 months only) Adult 300mg OD, Child 5-10mg/kg OD Adult 450-600mg OD, Child 10mg/kg OD Adult 1.5-2g OD, Child 35mg/kg OD Adult and child 15mg/kg OD Liver function should be monitored. Septicaemia Initial blind therapy until blood cultures results, Gentamycin + Benzylpenicillin + Flucloxacillin Or cefatoxime/ Ceftazidime alone Add metronidazole if anaerobes suspected Add flucloxacillin or Vancomycin if gram + ve infection suspected TYPES OF ANTIBIOTICS Bactericidal = Kill bacteria Penicillins and Cephalosporins [Back To Top] 10/7/2007 1:03 AM Antibiotics 3 of 7 http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Aminoglycosides Co-trimoxazole Isoniazid, Rifampicin & Ethambutol Vancomycin Eythromycin (high dose) Ciprofloxacin Bacteriostatic = hinder growth of bacteria Sulphonamides Tetracyclines Chloramphenicol Erythromycin PAS Lincamycin / Clindamycin Fucidic Acid Beta Lactam antibiotics (Penicillins & Cephalosporins) Similar structure and action but different spectra of anti microbial activity Bind at various sites in the cell membrane -> growth inhibition and alter protein synthesis ->cell lysis ? exact mechanism Toxicity: (low incidence) Anaphylaxis and cross reactivity in 5 - 20% therefore use cephalosporins with caution in those with penicillin hypersensitivity Some varieties -> bleeding disorders due to inhibition of platelet aggregation (methicillin and ampicillin) Gastrointestinal upset diarrhoea, nausea, vomiting Pseudo membranous colitis Methicillin associated rarely with nephrotoxicity 10% of children -> haematuria (microscopic) less than 1% -> renal insufficiency High dose of penicillin -> seizures Penicillins Penicillins: (Penicillin G, Phenoxymethyl penicillin (oral)) Bactericidal and interfere with bacterial cell wall synthesis Probenecid blocks the renal excretion Most important side effect is hypersensitivity Rare but serious side effect is encephalopathy if given at high dose or in renal failure Natural Penicillin V (Phenoxymethylpenicillin) Oral Gram +ve cocci (streptococci, pneumococcal, gonococcal, meningococcal) anthrax, diptheria, Clostridium , leptospirosis, tetanus Penicillinase resistant penicillins Most staphylococci are resistant to natural penicillin because of the production of B lactamases (penicillinases) Used for staph aureus infections, cellulitis Flucloxacillin Acid stable so can be given IV and Orally Cloxacillin MRSA are resistant and can sometimes only be sensitive to Vancomycin Temocillin New, has activity against penicillinase producing gram â€"ve bacteria except pseudomonas aeruginosa. Not active against gram + ve bacteria Penicillin G (Benzylpenicillin) IV Flucloxacillin Cloxacillin Temocillin Antipseudomonal penicillins Ticarcillin (only available in combination with clavulinic acid) Principally used for infections caused by pseudomonas auruginosa although some activity against other gram neg bacilli 10/7/2007 1:03 AM Antibiotics 4 of 7 http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Azlocillin and piparicillin Broad spectrum penicillins Ampicillin Amoxycillin CoAmoxyclav (Augmentin) More active than ticarcillin against pseudomonas Effective against some gram + and gram - bacteria, but inactivated by penicillinases therefore ineffective against staph aureus, 50% of Ecoli, 15% H. Influenzae Used in UTI, Otitis media, chronic bronchitis Amoxycillin better absorbed Cofluampicil (Magnapen) Pivampicillin Amoxycillin with clavulanic acid which is a penicillinase inhibitor therefore can be effective against staph aureus. Used in cellulitis, animal bites Combination of flucloxacillin and ampicillin Cephalosporins Beta lactam antibiotic Pharmacology similar to penicillins Broad spectrum, gram + and gram Principal side effect is hypersensitivity 10% of penicillin allergic patients have allergy to cephalosporins 1st Generation: (Cephalothin, Cephalexin (oral), Cefazolin) Active against Staph aureus, streptococcus Non hospital acquired E coli, klebsiella and proteus Clostridia Meningococcus Not active against MRSA, haemophillus, pseudomonas Serratia (indole positive proteus) Dose Cephalothin 25 - 30mg/kg IV 6/24 Cephalexin 25 - 50mg/kg/day Oral 6/24 Adults 1 - 4gm/day (divided) Fluclox better for staph if broad spectrum not required Don't use when haemophillus or proteus potential pathogens Has poor penetration of CSF 2nd Generation: (Cephamandole, Cefoxitin, Cefuroxime, Cefaclor (oral)) Active against Enhanced activity against gram negative organisms and many E coli and klebsiella resistant to the 1st generation cephalosporins Less gram positive activity Dose Cephamandole 50 - 100mg/kg/day IV 6/24 Cefaclor 20 - 40mg/kg/day 8/24 3rd Generation: (Cefotaxime, Ceftriaxone) Active against Further increased gram negative activity being active against haemophilus and pseudomonas Only 1/10 to 1/40 activity against staph aureus Not active against pseudomonas Dose Cefotaxime 100 - 200mg/kg/day IV 8/24 (Usually 100 - 150mg/kg/day) 1st generation agents should always be used for sensitive organisms 10/7/2007 1:03 AM Antibiotics 5 of 7 http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... 2nd and 3rd generation agents should be used only for organisms resistant to 1st generation cephalosporins as they are preferable to the more toxic aminoglycosides Duration of administration 5/7 to 6/52 IV and 4/52 to 6/12 oral Other B Lactam antibiotics Aztreonam Activity limited to gram negative aerobes eg pseudomonas, haemophilus influenzea; No activity against gram + organisms Broad spectrum including aerobic and anaerobic gram + and gram - bacteria; Needs to be given with cilastatin to prevent renal metabolism Similar to above except less likely to be metabolised by kidney Imipenem (Primaxin) Meropenem Tetracyclines Broad spectrum but with reducing value due to bacterial resistance Bind to calcium in growing bones and teeth therefore not used for children, pregnant women or breastfeeding mothers Not to be given in renal failure Eg. Tetracycline, Doxycycline, Lymecycline, minocycline, oxytetracycline Aminoglycosides All are bactericidal and active against some gram + and some gram- organisms Inhibit bacterial protein synthesis Not absorbed from the gut, therefore needs to be given IM or IV Accumulation occurs in renal impairment Important side effects- ototoxicity, nephrotoxicity (dose related -> monitor levels) Not to be given with potential ototoxic diuretics eg frusemide Plasma concentration should be measured 1 hour after a dose and just before the next dose Neuromuscular blockade may follow surgery and use of muscle relaxants or may potentiate weakness in myasthenia gravis or botulism Gentamycin Aminoglycoside of choice in UK Active against gram -ve bacilli and strains of pseudomonas Broad spectrum but inactive against anaerobes and poor against haemolytc strep and pneumococci, therefore usually given in conjuction with a penicillin and or metronidazole in undiagnosed serious infections Amikacin For gram -ve bacilli resistant to gentamycin Netilmycin Similar activity to gentamycin but less ototoxicity. Neomycin Too toxic for parenteral adinistration so only used for skin or bowel preparation Macrolides Erythromycin Similar antibacterial spectrum to penicillin Useful in penicillin allergic patients Can cause nausea, vomiting, diarrhoea Azithromycin Clarithromycin Spiramycin Glycopeptides Active against aerobic and anaerobic gram positive bacteria 10/7/2007 1:03 AM Antibiotics 6 of 7 http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Like beta- lactam antibiotics inhibits cell membrane synthesis -> altered cell membrane permeability and inhibition of RNA synthesis Vancomycin Useful in MRSA Used orally in pseudomembranous colitis Beware renal toxicity and ototoxicity Teicoplanin Levels should be monitored Similar to vancomycin, but allows OD administration and can be given IM Clindamycin Limited use because of toxic effects Most serious toxic effect is pseudomembranous colitis Active against gram positive cocci including staphylococci and active against many anaerobes Well concentrated in bone and excreted in bile and urine Recommended for staphylococcal bone and joint infections Chloramphenicol Broad spectrum but associated with severe side effects if given systemically, so reserved for very severe infections Fusidic acid Narrow spectrum Only indication is in infections caused by penicillinase producing staphylococci Used in osteomyelitis as well concentrated in bone A second antistaphyloccoccal antibiotic usually added (fluclox) to prevent emergence of resistance Check LFTs Sulphonamides and Trimethoprim Less used now because of increased bacterial resistance Trimethoprim used for UTI The combination of trimethoprim and sulfametoxazole (cotrimoxazole) are synergistic but its less used now Inhibits formation of folic acid necessary for cell growth, a step which is not required in human cells therefore not toxic Metronidazole High activity against anaerobic bacteria and protozoa Used where anaerobes suspected Effective in pseudomembranous colitis Topically it can reduce the odour of fungating tumours Ciprofloxacin Active against gram + and gram - bacteria but mainly gram â€"ve esp pseudomonas Interferes with DNA gyrase -> bactericidal action Used in septicaemia if organisms sensitive 10/7/2007 1:03 AM Antibiotics 7 of 7 http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... High incidence of staphylococcal resistance so not used in MRSA Forms of antibiotic delivery 1. 2. 3. 4. 5. [Back To Top] Oral IM IV Home IV therapy is possible with a Hickmann or Broviac catheter Antibiotic beads or spacers Polymethylmethacrylate impregnated beads with gentamycin useful in osteomyelitis. Only useful for 6-8 weeks. Tissue concentrations are much higher. They should always be removed as the PMMA beads are foreign bodies Nearly all antibiotics penetrate the synovium well in the presence of inflammation -> 60 -90% serum levels Definitive therapy depends on prolonged administration of the single most effective, least toxic and least costly agent Oral therapy can be used if: 1. 2. 3. 4. 5. Clinical response to parenteral anti microbial therapy Isolation of pathogen that is susceptible to orally administered antibiotic Patient tolerance of the oral agent Adequate serum activity of the oral agent Assurance of patient compliance [ Close Window ] 10/7/2007 1:03 AM Microbiology 1 of 2 http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Printout from Orthoteers.com website, member id 1969. © 2007 All rights reserved. Please refer to the site policies for rules on diseminating site content. Microbiology Gram Positive Cocci: Staph aureus Staph epidermidis Streptococcus Enterococci Characteristics of Gram Positive Bacteria: - gram positive bacteria retain crystal violet after alcohol decolorization Gram Negative Cocci Neisseria gonorrhea Neisseria meningitidis Branhamella catarrhalis Gram Positive Bacilli: Listeria Bacillus anthracis Clostridium tetani Clostridium perfringens Clostridium difficile Cornybacterium diphthiae Actinomyces israeli Nocardia asteroides Gram Negative Bacilli: Enteric Gm Neg Bacilli: Bacteroides fragilis Citrobacter diversus Enterobacteriaceae Escherichia coli Klebsiella Pneumoniae Proteus mirabilis Salmonella typhi Serratia Non Enteric Gm Neg Bacilli: Eikenella corrodens H. influenza Legionella pneumophila Pasteurella multocida Pseudomonas aeruginosa Acinetobacter anitratus Vibrio Characteristics of Gm Neg Bacteria: - cell membrane does not retain crystal-violet indium dye after an alcohol rinse but does retain safrinin O counterstain; lipopolysaccharide is a cell membrane endotoxin which is associated w/ the clinical effects of gm negative sepsis HEPATITIS Hepatitis B: Transmitted via parental, congenital, sexual & blood routes 6 months incubation Contains double stranded DNA coding for 3 surface proteins: 1. surface antigen (HBsAg) 2. core antigen (HBcAg) (not detectable in blood) 10/7/2007 1:04 AM Microbiology 2 of 2 http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... 3. precore protein (HBeAg) HBs Ag = current infection HBe Ag (HBAg) = associated with HBs Ag - high infectivity anti-HBs= Recovery & immunity, developes after vaccine or infection, persists for life anti-HBc (IgM) = current infection anti-HBc (IgG) = recent infection (not due to vaccination) anti-HBe = a good sign and indicates a favourable prognosis More Detail from Hepatitis Central - http://hepatitis-central.com/hbv/hepbfaq/viroligy.html HIV & AIDS [ Close Window ] 10/7/2007 1:04 AM Orthopaedic infections in children http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Printout from Orthoteers.com website, member id 1969. © 2007 All rights reserved. Please refer to the site policies for rules on diseminating site content. Orthopaedic infections in children Acute Haematogenous Osteomyelitis Subacute Haematogenous Osteomyelitis Subacute epiphyseal osteomyelitis Post-Fracture Infection ACUTE HAEMATOGENOUS OSTEOMYELITIS Pathology 1. Inflammation Acute inflammatory reaction with vascular congestion Rise in intra-osseous pressure causing intense pain 2. Suppuration At 2-3 days pus forms within the bone and forces its way down the haversian canals to the surface where it forms a sub-periosteal abscess The pus can spread from here back into the bone, into an adjacent joint or into the soft tissues (Where there is an intra-articular physis) Vertebral infection can spread through the end plate, disc and into the next vertebral body 3. Necrosis At 7 days, rising pressure, vascular stasis, infective thrombosis and periosteal stripping compromise the blood supply to the bone resulting in bone death resulting in a sequestrum 4. New bone formation At 10-14 days this forms from the deep surface of the stripped periosteum forming the involucrum 5. Resolution With release of the pressure and appropriate antibiotics healing can occur There may be permanent deformity Unpublished work (quoted in Dee) shows that experimentally bacteria injected intravenously will settle in the metaphyses of bone preferentially NB - in 10% of cases there is more than one site of infection. 1 of 5 10/7/2007 1:05 AM Orthopaedic infections in children http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Clinical Features Children (invariably) Pain, malaise, fever Limp or not weight bearing Infants Failure to thrive, drowsiness, irritable Adults The commonest site is the thoracolumbar spine (Batson's venous complex from the pelvis) Other bones involved especially in DM, IVDA, immunosuppressed Examination Local erythema, swelling and tenderness indicates that the pus has broken through the periosteum Investigations FBC incr. WCC Differential shows incr. neutrophils ESR may be normal within the first 48 hours but rises rapidly and may exceed 100mm/hr; Its gradual decline indicates effective treatment CRP raised Blood cultures Positive in 50% of cases ASO titres raised in 50% Antibodies to acid cell wall of S.aureus sensitivity 82% in acute osteomyelitis Radiographic studies X-rays essentially normal in the first 10 days 2-3 days deep soft tissue swelling adjacent to the metaphysis, with displaced fat planes 10-14 days demineralisation at the site of the infection and new bone formation at the surface Bone scan 99m Technetium Positive before any x-ray changes (24-48hrs of infection) False positives common in the hands and feet Valueless in the neonate 67 Gallium Uptake related to the local accumulation of PMN and can be used sequentially following a 99m Tc scan to increase the specificity An accumulation of tracer on both scans has an accuracy of 62% Increase also seen in fractures 111 2 of 5 Indium 10/7/2007 1:05 AM Orthopaedic infections in children http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... 111 In labelled white cells can be prepared in a few hours More accurate and easier to interpret than dual isotope scans Reported specificity 86% and sensitivity 83% and accuracy 83% MRI Intra and extra osseous changes will be detected early but are not diagnostic Aspiration and biopsy This will yield a positive culture in 80% of cases Pathogens S. Aureus in 60-90% of cases H. influenza (Hib) makes up 20% of cases under 4yrs Empirical antibiotic therapy Age Most likely pathogen Infant < 1yr Grp B Streptococcus Antibiotic S.aureus H.influenza E.coli Children 1-16 yr & No underlying disease S.aureus Strep.pyogenes H.influenza Sickle cell S.aureus Salmonella Adults S.aureus E.coli Serratia marcescens Pseudomonas aeruginosa Minimum duration of treatment is 6 weeks 20% failure of treatment if antibiotics given for only 3 weeks Blood levels should be 8 times the minimum bactericidal level Surgery If clinical abscess formed or not settling with 48hrs of antibiotics. Incision and drainage of the affected area Drilling of bone is not recommended but any soft areas of bone can be probed Skin closed over a drain Prognosis and complications Recurrence Dependent on the site involved and the time from onset to treatment Metatarsal lesions have the highest rate of failure 50% Distal femur/proximal tibia 20% failure with a more favourable outcome in the upper limb and spine Risk of recurrence in successfully treated osteomyelitis = 4% 1 year following treatment Early diagnosis 92% cured Late diagnosis 25% cured (Cole et al.) In neonates irreversible damage to the physis and joint may occur Damage to the physis may cause either overgrowth or growth retardation with resulting limb length discrepancy Pathological fracture through the abnormal area of bone especially if it has been drilled 3 of 5 10/7/2007 1:05 AM Orthopaedic infections in children SUBACUTE OSTEOMYELITIS http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... [Back To Top] Patient presents with a painful limp, systemically well and may have no signs of local infection There may be signs of a subperiosteal collection, synovitis or pus within a joint X-rays show a well-established lesion in the bone Femur and tibia are by far the most common sites Blood tests WCC and ESR may be raised but in 50% cases tests are normal Brodie's Abscess Commonly occur in the metaphyses of tubular bones but can also occur in flat bones, vertebral body and the diaphysis They are usually manifestations of subacute osteomyelitis Gledhill classification Type s I solitary metaphyseal area lesion that may communicate with the epiphysis II radiolucent lesion metaphyseal lesion not surrounded by sclerotic new bone but with adjacent loss of cortex III diaphyseal lesion associated with cortical hypertrophy and periosteal or endosteal new bone. May be confused with an osteoid osteoma . IV lesion associated with layers of subperiosteal new bone formation giving an onion skin appearance which may be confused with early Ewing's sarcoma Cierney & Mader Classification: Also see Post-fracture Infections SUBACUTE EPIPHYSEAL OSTEOMYELITIS (Green at al.) [Back To Top] The blood supply of the epiphysis has similarities with the metaphysis in that there is sluggish blood flow and vascular loops making it susceptible to infection They identified lesions of the epiphysis that did not communicate with the metaphysis either radiological or at surgery Other presentations identified were patients aggressive lesions that had clinical, radiological and haematological features indistinguishable from primary bone tumours such as Ewing's S.aureus is the only organism causing this pathological entity Treatment IV antibiotics 48hr followed by 6/52 oral therapy Surgery is restricted to those with signs pus Opening and curreting these lesions is successful for healing 4 of 5 10/7/2007 1:05 AM Orthopaedic infections in children http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Curetted tissue shows the characteristics of osteomyelitis but 50% were negative on culture Recovery is usually complete although growth arrest lines and defects in the epiphysis and metaphysis can occur [ Close Window ] 5 of 5 10/7/2007 1:05 AM Orthopaedic infections in children 2 http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Printout from Orthoteers.com website, member id 1969. © 2007 All rights reserved. Please refer to the site policies for rules on diseminating site content. Orthopaedic infections in children 2 SEPTIC ARTHRITIS CHRONIC OSTEOMYELITIS Garr's SPECIAL SITES OTHER ORGANISMS POST-FRACTURE INFECTION SEPTIC ARTHRITIS In children septic arthritis can occur at any age but 50% of cases occur in children under 5years and 30% of cases occur in children under 2years Hip most commonly affected in infants, and knee in older children 10% of cases will have more than 1 joint affected Route of spread 1. 2. 3. 4. Haematogenous Spread from metaphyseal osteomyelitis where the metaphysis is intra-articular Spread from contiguous soft tissue infection Direct inoculation Causative organism 1 of 6 10/7/2007 1:06 AM Orthopaedic infections in children 2 http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Under 2 years 2-16 years 16-30 years over 30 years S.aureus S.aureus S.aureus S.aureus E.coli Strep. Pyogenes Strep. pyogenes Streptococci (A,B,C,G,pneumon) Group B Strep Streptococci (C,G) N.gonorrhoea Haemophilus Haemophilus Since the introduction of the HiB vaccine the incidence of haemophilus infections has dropped dramatically (Personal correspondence from Stepping Hill Hospital microbiology department) Investigations FBC, ESR, CRP USS for detection of hip effusion XR may show subluxation or dislocation Diagnostic aspiration Send sample for Gram stain and microscopy Septic arthritis strongly suspected if the WCC is >50,000mm -3 with 90% PMN , even if the cultures are negative Culture Differential diagnosis Child Irritable hip (transient synovitis) Acute rheumatic fever Henoch-Schonlein purpura Adult Gout Pseudogout Acute RA/OA Acute monarthropy Treatment IV antibiotics broad spectrum aimed at best guess first then adjusted according to microbiology results Length of treatment (minimum) IV 2 weeks Oral child 2-4 weeks Adult 4-6 weeks Anti-staphylococcal antibiotics Anti-streptococcal antibiotics First line Second line Benzylpenicillin Flucloxacillin Vancomycin Clindamycin Fucidin Teicoplanin Rifampicin Clindamycin Rifampicin 2 of 6 10/7/2007 1:06 AM Orthopaedic infections in children 2 http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Anti-haemophilus antibiotics Cefotaxime Surgical drainage Hips should always be drained surgically Best approach anterolateral Arthroscopic washout acceptable in the knee but open drainage may be required Complications Despite alarming XR changes there is a favourable outcome in many children AVN Coxa vara CHRONIC OSTEOMYELITIS [Back To Top] Aetiology Inadequately treated acute osteomyelitis Haematogenous spread Iatrogenic Penetrating trauma Open fractures Contiguous focus infection is the term used when the infection of bone is secondary to a breakdown in the overlying soft tissue e.g. vascular/neuropathic ulcer, DM The adjacent soft tissues are always involved except in Brodie's abscess Causative organism If secondary to acute osteomyelitis the organism is almost always S.aureus Following trauma S.aureus is most common but it may be polymicrobial Gram â€"ve organisms are now isolated from ~50% of patients with osteomyelitis Animal bites - pasturella multocida Human bites - eikenella corrodens Because the sinus tracts can become colonised by many organisms, superficial swabs are unhelpful Classification (Cierny) Type I Medullary Type II Superficial Type III Localised Type IV Diffuse 3 of 6 10/7/2007 1:06 AM Orthopaedic infections in children 2 http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Host Type Risk A : Normal immune system, non-smoker Low B : Local or mild systemic deficiency, smoker Moderate C : Major nutritional or systemic disorders High Treatment Principles Surgical debridement and bony stabilisation Control of dead space Soft tissue cover Antibiotics Surgical debridement Aim is to remove all dead and infected tissue and bone Send samples for Microscopy Culture Histology (0.5% will develop SCC, Marjolin's ulcer) Type I Medullary cortical de-roofing and medullary debridement Type II Superficial shallow decortication back to bleeding bone Type III Localised saucerisation and debridement Type IV Diffuse infected area excised en-bloc and stabilised with ex-fix Antibiotic choice Guided by microbiology department Clindamycin (98% serum level) and vancomycin(14% serum level) have good bone penetration Minimum length 6 weeks with 3 months being the standard treatment course May need to treat for 6-12 months Closure of dead space Local flaps Free flap transfer Up to 40 % failure when these are used for chronic osteomyelitis Open cancellous grafting - Papineau technique Useful for bone deficiencies of less than 4cm Labour intensive Vascularised bone graft Heals as a segmental fracture Indicated when defect is > 6cm Iliac crest for defects > 8cm Fibula 6-35cm can be bridged Bypass graft Involves the establishment of a cross union between the fibula and tibia proximally and distally to the defect which has been debrided and bone grafted Ilizarov technique 4 of 6 10/7/2007 1:06 AM Orthopaedic infections in children 2 http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Acute shortening of the area debrided and the stabilised with ring fixator Coticotomies then performed either above or below and then distraction performed to correct length Amputation Should always be considered especially early in the type "C" host Garr's Chronic Sclerosing Osteomyelitis [Back To Top] Mainly affects children and young adults, average age 16 years No necrosis or pus present but intense periosteal proliferation leading to bone formation Aetiology unclear but may be due to anaerobic organisms such as proprionobacterium acnes Local pain and tenderness in shaft of long bones Clinically and radiologically can be difficult to distinguish from primary osteogenic sarcoma No satisfactory treatment and antibiotic therapy does not affect course Recurrent for years then gradually subsides SPECIAL SITES [Back To Top] Hands Fight bites Animal bites Pelvis S.aureus in 70% of cases Because of excellent blood supply antibiotic treatment alone is usually successful Spine Occurs either in the vertebral body or the disc IV drug abusers Common organisms are S.aureus and pseudomonas Serratia marcescens can cause multifocal osteomyelitis OTHER ORGANISMS [Back To Top] Brucella Associated with the meat trade Treatment doxycycline Salmonella Common in sickle cell disease S.aureus still the most common organism Other diseases affected by salmonella include SLE and the immunocompromised Anaerobic organisms Suspect if foul smelling Care must be taken when taking and transporting the samples as organism may die Fungi Blastomycosis: treatment amphotericin B Coccidiomycosis: treatment amphotericin B Actinomycosis: sulphur granules, treat with penicillin G, IV for 6 weeks then oral for 1 year Cryptococcosis: associated with AIDS, leukaemia, sarcoid and DM. treatment amphotericin B Mycetoma (Madura foot): surgical debridement and ketoconazole Syphilis Treponema pallidum 5 of 6 10/7/2007 1:06 AM Orthopaedic infections in children 2 http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Children - congenital syphilis responds rapidly to antibiotics clutton's joints - late stage of congenital syphilis - large painless joints Adults - involvement of bone and joint in late tertiary stage Painless non tender swelling of long bone or skull Charcot joint may develop Yaws spirochetal infection in tropical countries Similar to syphilis Rx - penicillin TB Think about in cases of immunosuppression and AIDS Spine most common Others - Knee, hip, ankle, SI joints, symphysis pubis, hands and feet ( TB dactylitis) Rx - antituberculous therapy Atypical mycobacteria M. marinarum - fish tank workers M. avium-intracellulare [ Close Window ] 6 of 6 10/7/2007 1:06 AM Poliomyelitis 1 of 2 http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Printout from Orthoteers.com website, member id 1969. © 2007 All rights reserved. Please refer to the site policies for rules on diseminating site content. Poliomyelitis Poliovirus is primarily spread by fecal-hand-oral transmission from one host to another. The virus is shed in oral secretions for several weeks and in the feces for several months. It destroys the anterior horn cells in the spinal cord. Poliovirus infections can be divided into minor and major forms: The minor illnesses occur 1 to 3 days before the onset of paralysis, with gastrointestinal complaints of nausea and vomiting, abdominal cramps and pain, and diarrhea and the systemic manifestations of sore throat, fever, malaise, and headache. The major illness includes all forms of central nervous system (CNS) disease caused by poliovirus, including aseptic meningitis or nonparalytic polio, polioencephalitis, bulbar polio, and paralytic poliomyelitis, alone or in combination Clinical findings: there is fever, stiffness of the neck (nuchal rigidity), and a plecocytosis in cerebrospinal fluid profound asymmetrical muscle weakness develops initial phase is typically followed by some recovery of muscle strength, but permanent weakness results from necrosis of anterior horn cells foot and ankle: 1. calcaneocavus (hindfoot cavus) which occurs as a result of a weak gastrocnemius 2. foot intrinsics are typically spared in polio 3. claw toes: results from relative overactivity of the long toe flexors and extensors (to compensate for weakness of the triceps Rarely, a transverse myelitis with paraparesis, urinary retention, sensory complaints and signs and autonomic dysfunction including hyperhidrosis or hypohidrosis, and decreased limb temperature may occur Post-polio Syndrome: years following a polio infection, develop slowly progressive muscle weakness in the already involved muscles common finding is weakness of the quadriceps and calf muscles when occurring individually, the quadriceps can help compensate for for a weak calf with triceps weakness, the ability to decelerate the tibia is lost and therefore, flexion of the knee will persist throughout stance phase - in order to prevent this, the patient may attempt to compensate with increased quadriceps activity during a larger portion of stance phase in the case of a weak quadriceps and triceps, the occurrence of an equinus contracture or a hinged AFO with dorsiflexion block will both prevent excessive knee flexion and excessive ankle dorsiflexion during stance phase avoid the pitfall of lengthening of the Achilles tendon in these patients these patients may require an ischial bearing, double upright locked knee orthosis, which helps prevent the knee from buckling during gait Diagnostic criteria for post-polio syndrome: 1. A prior episode of paralytic poliomyelitis with residual motor neuron loss (which can be confirmed through a typical patient history, a neurologic examination, and, if needed, an electrodiagnostic exam). 2. A period of neurologic recovery followed by an interval (usually 15 years or more) of neurologic and functional stability. 3. A gradual or abrupt onset of new weakness or abnormal muscle fatigue (decreased endurance), muscle atrophy, or generalized fatigue. 4. Exclusion of medical, orthopedic, and neurologic conditions that may be causing the symptoms mentioned in 3. Links: Lincolnshire Post-Polio Library 10/7/2007 1:06 AM Poliomyelitis 2 of 2 http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... [ Close Window ] 10/7/2007 1:06 AM Tuberculosis 1 of 4 http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Printout from Orthoteers.com website, member id 1969. © 2007 All rights reserved. Please refer to the site policies for rules on diseminating site content. Tuberculosis Tuberculosis is common throughout the world Causes significant morbidity and mortality particularly in Africa and Asia Over 10,000 cases per year occur in United Kingdom Accounts for 1,000 deaths mainly in immigrant Asian population Usually due to Mycobacterium tuberculosis or Mycobacterium bovis infection Primary tuberculosis Usually a respiratory infection that occurs in childhood Infection results in sub-pleural Ghon focus and mediastinal lymphadenopathy Regarded as the primary complex Symptoms are often few Resolution of infection usually occurs Complications include: Haematogenous spread causing miliary TB affecting lungs, bones, joints, meninges Direct pulmonary spread resulting in TB bronchopneumonia Post-primary tuberculosis Occurs in adolescence or adult life Due to reactivation of infection or repeat exposure Results in more significant symptoms Reactivation may be associated with immunosuppression (e.g. drugs or HIV infection) Pulmonary infection accounts for 70% of cases of post-primary TB Usually affects apices of upper or lower lobes Cavitation of infection into the bronchial tree results in 'open' TB Clinical features include cough, haemoptysis, malaise, weight loss and night sweats Infection of lymph glands results in discrete, firm and painless lymphadenopathy Confluence of infected glands can result in a 'cold' abscess Infection of the urinary tract can cause haematuria and 'sterile pyuria' Investigations Large volume specimens should be collected preferably in the early morning Repeated samples may be required Microscopy If Mycobacteria infection suspected samples should be submitted to a Ziehl-Neelsen stain Mycobacteria appear as red acid-alcohol fast organisms Organisms also fluoresce with auramine staining Negative microscopy does not exclude tuberculosis Need supporting histological examination and microbiological culture Photomicrograph of granulomatous tissue obtained from the synovium of a knee joint in a patient with tuberculosis. Many focal giant cells, nodular collections of histiocytes, and an infiltration of chronic inflammatory cells are present (H&E, x 4 obj.). 10/7/2007 1:07 AM Tuberculosis 2 of 4 http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Photomicrograph showing the typical appearance of the giant cells in tuberculosis, with peripherally arranged nuclei - the so-called Langerhans giant cells (H&E, x 10 obj.). Photomicrograph of tissue obtained from a periarticular abscess in a middle-aged male who had renal transplantation and immunosuppressive therapy. Microscopically there is a heavy infiltration of acute inflammatory cells with many admixed large histiocytic cells. No granulomas are recognized. (H&E, x 10 obj.). An acid-fast bacilli (AFB) stain shows an abundance of organisms mostly intracellular. This is a typical microscopic presentation for atypical mycobacterial infection (Ziehl Neelsen, x 50 obj.). Culture Mycobacteria can be difficult to culture Need to: Collect adequate and relevant specimens (e.g. early morning urine x3) Concentration of specimen (e.g. centrifugation) Decontamination to remove other organisms (e.g. Petroff method) Culture on Lowenstein-Jensen method at 35-37o for at least 6 weeks Confirm that any Mycobacteria cultures are pathological Histology Histological examination shows evidence of a delayed hypersensitivity reaction Classical appearance is of caeseating necrosis Tuberculous follicle consists of central caseaous necrosis Surrounded by lymphocytes, multi-nucleate giant cells and epitheloid macrophages Organisms may be identified within the macrophages 10/7/2007 1:07 AM Tuberculosis 3 of 4 http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Caseating necrosis due to tuberculosis Skin tests Delayed hypersensitivity reaction used to diagnose tuberculosis The two commonest tests are the Mantoux and Heaf test In the Mantoux test 0.1 ml of purified protein derivative is injected intradermally Positive reaction is a papule of > 5 mm diameter at 72 hours In the Heaf test purified protein derivative is placed on the skin A gun is used to produce multiple punctures Positive reaction is more than 4 papules at puncture sites at 72 hours Positive skin test are indicative of active infection or previous BCG vaccination Treatment First line chemotherapeutic agents are rifampicin, isoniazid and ethambutol Given as 'triple therapy' for first 2 months until sensitivities available Rifampicin and isoniazid are the usually continued for further 7 months Less than 5% of organisms are resistant to first-line agents Second line treatment includes pyrazinamide MUSCULOSKELETAL INVOLVEMENT pulmonary tuberculosis is evident in only half the patients with skeletal involvement Tuberculous Spondylitis TB Arthritis: although the disease is generally more likely to be chronic, acute mycobacterial arthritis has been reported Hips and knees are affected most frequently may present as gradually worsening arthritis but is often mistaken for some other form of arthritis (such as "mono-articular rheumatoid arthritis" or PVNS) mono-articular joint space will often be maintained (unlike RA) periarticular bone lesions may accompany the synovial involvement peri-articular osteopenia is common Appendicular skeleton: look for metaphyseal lytic lesions with little or no sclerosis, and no periosteal reaction Phalangeal tuberculous osteitis: (TB dactylitis) 10/7/2007 1:07 AM Tuberculosis 4 of 4 http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... look for soft tissue swelling, cortical thinning, medullary destruction, and periosteal reaction involving the middle and distal phalanx [ Close Window ] 10/7/2007 1:07 AM Polarized Light Microscopy http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... Printout from Orthoteers.com website, member id 1969. © 2007 All rights reserved. Please refer to the site policies for rules on diseminating site content. Polarized Light Microscopy from: The Internet Pathology Laboratory Some materials have the property of "birefringence" which is the ability to pass light in a particular plane. Such materials are called "anisotropic" because of this property. These are typically crystals or fibers. Normally, most materials are "isotropic" because any light that passes through them will be scattered in all directions. When viewed under polarized light, however, anisotropic materials will be brightly visible in one plane ("birefringent"), but will be dark in a plane turned 90 degrees. The birefringence observed with polarized light can be further subdivided into "positive" and "negative" birefrigence. This is based upon the property of birefringence in which rays of light travelling through the anisotropic material in perpendicular planes (at right angles) will travel at different velocities through the material. Thus, a birefringent material actually has two refractive indices, a higher one for the "fast" rays of light and smaller refractive index for the "slow" rays travelling through the material. These rays of light can also be called "ordinary" when they are reflected by the material and "extraordinary" when the rays pass straight through the material. A substance is positively birefringent if the "ordinary" reflected ray becomes the "fast" ray that travels faster in parallel with the crystalline structure of the material than the "extraordinary" ray that is "slow" when it traverses the material. Negative birefringence occurs when the "ordinary" ray becomes the "slow" ray when it is reflected and travels across the crystalline structure. For polarized light microscopy, there must be two polarizing filters made of glass or plastic material which will pass light in only one plane. The material is generally made of a thickness that will absorb the "ordinary" or "slow" ray and pass the "fast" rays as "plane polarized" light. One filter (the "analyzer") is placed above the specimen (on top of the slide, or in a filter holder in the turret of the microscope above the lenses). The other (the "polarizer") is placed over the light source below the specimen on the glass slide. Polarizing sets made for a particular microscope can be purchased; however, a polarizing lens for a single lens reflex (SLR) camera can act as a good "polarizer" while 1 of 3 10/7/2007 1:11 AM Polarized Light Microscopy http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... an inexpensive sheet of plastic polarizing material can be cut to size to provide the "analyzer". Properties of positive and negative birefringence can be assessed only with an additional "compensator" plate placed on top of the polarizer (or in the condenser). This compensator is made of a material (quartz or selenite) which magically retards the light a quarter wavelength and produces an interference pattern with a red background on which the properties of positive and negative birefringence can be seen. Thus, the compensator is often called a "red plate". A material is said to be positively birefringent when it appears blue if its axis is aligned parallel to the long axis of the compensator, or "red plate". A negatively birefringent material will appear yellow under the same circumstances. The background will appear dark pink to red. In reality, birefringent materials will be oriented many directions on the slide, so you need to make note of the red plate's axis. A red plate can be purchased (expensive) or you can make your own by applying two layers of clear adhesive tape to a glass slide. You will have to experiment with different tapes to get the right thickness, which you will know when your homemade "red plate" produces the reddest background. The long axis is the same as the long axis of the glass slide. Place the red plate on top of the polarizer over the light source and rotate it for the desired effect. There are a number of usages for polarized light microscopy. These include identification of the following: Exogenous crystalline material (most common example is talc crystals found in subcutaneous injection site, in lungs, and in organs of the mononuclear phagocyte system of persons engaging in injection drug use) Endogenous crystalline material: crystals of sodium urate in gouty tophi, calcium pyrophosphate crystals in persons with calcium pyrophosphate deposition disease Collagen: collagen fibrils are naturally anisotropic and polarize a dull yellow-white Formalin-heme pigment: an artefact of poor fixation, this pigment appears as stippled black material under light microscopy, but has bright white 2 of 3 10/7/2007 1:11 AM Polarized Light Microscopy http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.aspx?ar... birefringence in a stippled pattern with polarized light Amyloid stained with Congo red dye: the structure of amyloid gives it anisotropic properties, and when stained with Congo red, it produces a characteristic "apple green" birefringence For optimal polarized light microscopy, the microscope's light source should be made as bright as possible (remove any other filters, but be careful viewing through the eyepiece). The analyzer filter is placed over the specimen. The polarizer filter is then rotated until the light is extinguished as much as possible. If material on the glass slide has anisotropic properties, it will "bend" the light from the polarizer to pass through the analyzer and appear bright when viewed through the eyepiece. Such materials will be "birefringent". Examples of the use of polarized light microscopy include: Intravenous drug use. Silicosis. Lymph node, silicoanthracosis. Amyloid, cardiac. Sodium urate crystals, negatively birefringent. Calcium pyrophosphate crystals, positively birefringent. Urine, oval fat bodies. [ Close Window ] 3 of 3 10/7/2007 1:11 AM



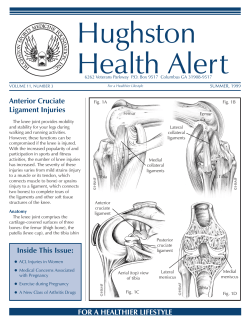








© Copyright 2026