
European Commission DG for Energy (ENER/D2)
European Commission DG for Energy (ENER/D2) How to Improve Safety in Regulated Industries What Could We Learn From Each Other Background Material Annex C ENCO FR-(12)-44 July 2012 Specific Contract No. ENER/ 2011/NUCL/SI2.599383 in How w to Im mprove Safety S ndustrie es Regullated In What C Could We W Learrn Frrom Eac ch Othe er Backgground Material Annex C EN NCO FR R-(12)-4 44 July J 201 12 Und der the Fram mework Serrvice Contract forr Technical Assistance TREN/R1/3 350-2008 Lo ot 3 Specific Contract No. ENER R/ 2011/NUC CL/SI2.5993 383 Prepared by: b Prep pared fo or: E European Commissiion DG G for Enerrgy (ENE ER/D2 Nuclear Energ gy) DISCLAIM MER The con ntent of thiis report is the sole ressponsibility y of the Con ntractor andd can in no way be tak ken e views of the Europea an Union. to reflect the Annex C. Overview of Deepwater Horizon oil rig explosion TABLE OF CONTENTS 1. INTRODUCTION .............................................................................................................................4 1.1. EVENT SUMMARY ................................................................................................................................................... 4 1.2. BACKGROUND ....................................................................................................................................................... 4 1.3. REGULATORY AND SAFETY ASPECTS ........................................................................................................................ 5 Safety of the offshore industry ............................................................................................................................ 5 Regulatory aspects .................................................................................................................................................. 6 2. TECHNICAL ASPECTS OF THE DEEPWATER DRILLING ...........................................................7 2.1. DRILLING PROCESS OVERVIEW ................................................................................................................................ 7 Pore pressure and fracture pressure ................................................................................................................... 8 Casing and cement .................................................................................................................................................. 9 The Blowout Preventer .......................................................................................................................................... 9 Setting subsequent casing strings ...................................................................................................................... 10 Float Collar ............................................................................................................................................................ 10 Cementing casing strings ..................................................................................................................................... 11 The production casing .......................................................................................................................................... 12 Well control and barriers .................................................................................................................................... 13 2.2. MACONDO WELL DESIGN AND CONSTRUCTION ........................................................................................................ 14 2.3. PREPARING THE WELL FOR SUBSEQUENT PRODUCTION ............................................................................................ 16 Installation of the production casing ................................................................................................................ 16 The cement design ................................................................................................................................................ 18 Laboratory tests of the cement slurry .............................................................................................................. 19 Cement evaluation log ......................................................................................................................................... 20 Testing of the wellhead seals ............................................................................................................................. 20 Temporary abandonment ..................................................................................................................................... 22 Design features of the Macondo well ................................................................................................................ 24 2.4. OVERVIEW OF THE ACCIDENT ............................................................................................................................... 25 3. INVESTIGATION INTO EXPLOSION ...........................................................................................27 3.1. BP INVESTIGATION REPORT .................................................................................................................................. 28 Annulus cement barrier ....................................................................................................................................... 29 Shoe track barrier ................................................................................................................................................. 29 Negative pressure test ......................................................................................................................................... 30 Recognition of hydrocarbons influx ................................................................................................................... 30 Well control response action .............................................................................................................................. 30 Diversion of blowout to the MGS ....................................................................................................................... 31 The fire and gas systems...................................................................................................................................... 31 The BOP emergency mode ................................................................................................................................... 31 Report summary .................................................................................................................................................... 31 3.2. REPORT OF THE HUMAN RELIABILITY ASSOCIATES .................................................................................................. 32 How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page i Cement slurry design ............................................................................................................................................ 32 Cement placement ................................................................................................................................................ 33 Confirmation of placement ................................................................................................................................. 33 Negative-pressure test ......................................................................................................................................... 33 Failure to timely recognize influx of hydrocarbons ....................................................................................... 34 Failure of well control response ........................................................................................................................ 34 Failure of the Fire and Gas system .................................................................................................................... 34 Failure of the BOP emergency modes................................................................................................................ 35 Report summary .................................................................................................................................................... 35 3.3. FINDINGS OF THE OIL SPILL COMMISSION .............................................................................................................. 36 Report to the President ....................................................................................................................................... 36 Chief Counsel’s investigation report ................................................................................................................. 38 3.4. REPORT OF NAE/NRC COMMITTEE ..................................................................................................................... 41 Interim Report ....................................................................................................................................................... 41 Final Report............................................................................................................................................................ 42 3.5. OBSERVATIONS FROM OTHER SOURCES .................................................................................................................. 43 4. ANALYSIS OF THE DEEPWATER HORIZON ACCIDENT ..........................................................44 4.1. STEP 1 - DEFINITION OF THE PROBLEM ................................................................................................................. 44 4.2. STEP 2 – ANALYSIS OF CAUSES (CAUSAL MAP) ....................................................................................................... 45 4.3. STEP 3. ANALYSIS OF SOLUTIONS ......................................................................................................................... 61 Safety management and safety culture (Causes 1 – 7) ................................................................................... 62 Regulatory oversight (Causes 8 – 10) ................................................................................................................. 63 Procedures and training (Causes 11 – 16) ......................................................................................................... 65 Process safety (Causes 17 – 21) ........................................................................................................................... 66 Equipment design issues (Causes 22 – 26) ......................................................................................................... 66 5. SUMMARY CONCLUSIONS ..........................................................................................................68 5.1. INDUSTRY MANAGEMENT SYSTEM .......................................................................................................................... 68 Risk awareness ....................................................................................................................................................... 68 Communication problems .................................................................................................................................... 69 Safety culture issues............................................................................................................................................. 69 5.2. SAFETY OVERSIGHT OF THE INDUSTRY ................................................................................................................... 70 Regulatory regime of MMS................................................................................................................................... 70 Desired changes ..................................................................................................................................................... 71 6. REFERENCES TO ANNEX C ........................................................................................................73 How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page ii Glossary AMF BOP BSR DOI ECD EDS ETP HAZOP MGS MMS MODU NEPA OPA ppg MOC TA D&C TOC LRMP MUX ROV Automatic Mode Function Blowout Preventer Blind Shear Ram Department of the Interior Equivalent Circulation Density Emergency Disconnect System Engineering Technical Practice Hazards and Operability Mud Gas Separator Minerals Management Service Mobile Offshore Drilling Unit National Environmental Policy Act Oil Pollution Act of 1990 Pounds per gallon Management Of Change Technical Authority Development and Completion Top Of Cement Lower Marine Riser Package Multiplex Remote Operated Vehicle How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 3 1. Introduction 1.1. Event summary On April 20, 2010 at approximately 9:45 pm a huge explosion rocked a semi-submersible Mobile Offshore Drilling Unit (MODU) located about 66 km off the coast of Louisiana in the Gulf of Mexico. The oil rig was called the Deepwater Horizon and was owned by Transocean Ltd and leased to the British Petroleum Company through September 2013. The direct cause of the explosion was that high pressure methane gas from the well expanded into the drilling riser and was released onto the drilling rig, where it ignited and exploded, engulfing the rig. At the time of the explosion, there were 126 crew on board: 7 employees of BP, 79 of Transocean, as well as employees of various other companies involved in the operation of the rig, including Anadarko, Halliburton and M-I Swaco. Most of the workers escaped the rig by lifeboat and were subsequently evacuated by boat or airlifted by helicopter for medical treatment. However, eleven workers were never found despite a three-day Coast Guard search operation, and are believed to have died in the explosion. 16 workers were injured. Efforts by multiple ships to douse the flames were unsuccessful. After burning for approximately 36 hours, the Deepwater Horizon sank on the morning of 22 April 2010. Remotely operated submersible vehicles were used to examine the wellhead. The vehicles were also used in an effort to manually trigger the blowout preventer (BOP), which would close the wellhead and prevent any farther release of oil. The blowout preventer is a 450ton valve installed at the wellhead that is designed to automatically shut to prevent oil leaks in the event of an accident. Attempts to manually close the blowout preventer have not been successful. An oil leak was discovered on the afternoon of 22 April when a large oil slick began to spread at the former rig site. Oil continued to leak from the wellhead more than a mile underwater on the ocean floor at an estimated rate of 42,000 gallons a day. According to the Flow Rate Technical Group, the leak amounted to about 4.9 million barrels (780,000 m3) of oil, exceeding the 1989 Exxon Valdez oil spill as the largest ever to originate in U.S.controlled waters. 1.2. Background The Deepwater Horizon was a semi-submersible mobile offshore drilling rig that could operate in waters up to 2,400 m deep and drill down to 9,100 m. The drilling rig is a mobile, temporary rig that drills the well, identifies that there is a viable reservoir of hydrocarbons, and then makes it safe and ready for a more permanent production rig. This involves drilling a deep bore hole in stages and filling the casing with cement. The rig was built by South Korean company Hyundai Heavy Industries. It was owned by Transocean, operated under the Marshallese flag of convenience, and was under lease to How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 4 BP from m March 200 08 to Septe ember 20133. Transoce ean was pro oviding the rig crew (e.g. the tool pusshers and drillers). Halliburton waas responsible for the cement opperations. At the ttime of the e explosion, the rig w was drilling an explorattory well aat a water depth d of approximately 1,5 500 m in th he Macondoo Prospect, located in the Mississsippi Canyo on Block 252 of tthe Gulf of Mexico in the t United SStates exclu usive econo omic zone aabout 66 km m off the Louisian na coast. BP was the operattor and principal deve eloper of the Macondo Prospect with a 65% % share, while 25 5% was own ned by Anad darko Petrooleum Corpo oration, and d 10% by MO OEX Offshore 2007, a unit o of Mitsui. Th he mineral rights to drrill for oil on o the Maco ondo Prospeect were pu urchased by BP in March 2008 2 at th he Mineralss Management Service e's lease ssale. The platform p commen nced drillin ng in Februa ary 2010 att a water depth of app proximatelyy 5,000 fee et (1,500 m). F FIG. 1-1. Dee epwater Horiizon drilling rig prior to the accidennt. The planned well was w to be drilled d to 188,360 feet (5,600 ( m) below b sea leevel, and was w to be plugged d and suspe ended for su ubsequent ccompletion as a subsea producer . Productio on casing was be eing run an nd cemente ed at the time of the acciden nt. Once thhe cementting was complette, it was due to be e tested fo r integrity and a cem ment plug set to tem mporarily abandon n the well for f later completion ass a subsea producer. p 1.3. R Regulatorry and sa afety asp pects Safety y of the off ffshore ind dustry Modern oil and gas drilling riigs and prooducing plattforms are,, in effect, enormous floating machine es, denselyy equipped with pow werful engin nes and re esponsible ffor keeping g within geologicc formatio ons large volumes of highly y combustible hydroocarbons at a high tempera atures and pressures. For all the eir productivity, the rigs r expose their crew ws to the How to Improve Safety in Regulated Indu ustries om Each Other safety s in EU” What Could We Learn Fro Background Material, ENC CO FR-(12)-44 © ENCO Page 5 risks of injury or death if not properly operated and maintained – risks compounded for operations conducted in progressively deeper waters, ever farther from shore. From its creation until the Macondo well blowout, Minerals Management Service (MMS) was the federal agency primarily responsible for leasing, safety, environmental compliance, and royalty collection from offshore drilling. In carrying out its duties, MMS subjected oil and gas activities to an array of prescriptive safety regulations: hundreds of pages of technical requirements for pollution prevention and control, drilling, well-completion operations, oil and gas major well maintenance, production safety systems, platforms and structures, pipelines, well production, and well-control and -production safety training. As required by the 1978 Act, MMS also attempted to conduct both annual and periodic unscheduled (unannounced) inspections of all offshore oil and gas operations to try to assess compliance with those requirements. Agency officials have tried to meet the requirement for annual inspections of the operation of safety equipment designed to prevent blowouts, fires, spills, and other major accidents. In both annual and unannounced inspections, MMS officials used a national checklist, covering categories such as pollution, drilling, well completion, production, crane, electrical, and personal safety. Most inspections tend to cover a subset of the elements on the list. Roughly 20 percent of the matters for inspection (those for the production meters) are not related to safety. But over time, MMS increasingly fell short in its ability to oversee the offshore oil industry. The agency’s resources did not keep pace with industry expansion into deeper waters and industry’s related reliance on more demanding technologies. And, senior agency officials’ focus on safety gave way to efforts to maximize revenue from leasing and production. Regulatory aspects By the early 1990s, some MMS officials had begun to rethink the agency’s approach to safety oversight of the offshore industry. In the wake of an accumulation of accidents in U.S. waters, and several devastating accidents elsewhere around the globe, they had come to appreciate that a command and control, prescriptive approach to regulation did not adequately address the risks generated by the offshore industry’s new technologies and exploration, development, and production activities, including industrial expansion into deeper waters [C-4]. In March 1980, the Alexander Kielland – built as a drilling rig but under lease to Phillips Petroleum Company to house offshore workers at the Ekofisk Field in the Norwegian North Sea – capsized, killing 123 of the 212 people on board the rig. Two years later, during preparation for an approaching North Atlantic storm, the Ocean Ranger semisubmersible drilling the Hibernia field for Mobil Oil of Canada, sank off the coast of Newfoundland; all 84 crew members were lost in the freezing-cold waters. And in July 1988, the Piper Alpha production platform operated by Occidental Petroleum 120 miles northeast of Aberdeen, Scotland, exploded and sank, killing 167 people, including 2 rescuers. Although the causes of the three accidents varied, they all involved international operations of U.S.-based oil and gas companies. Common contributing factors included inadequate safety assurance, worker training, and evacuation procedures. Poor communication and confusion about lines of authority amplified the death toll in at least two of the accidents. The Norwegian government responded to the loss of the Alexander Kielland by transforming its approach to industry operations. Under the new regime, rather than relying solely on prescribed operational and safety standards, the government required the industry to demonstrate thorough consideration of all risks associated with the structures How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 6 and operations for a drilling or production plan. The regulator no longer “approved” operations. Shifting the burden of demonstrating safety to the operator, the regulator would instead now “consent” to development activity proceding only upon the operator’s demonstration that sufficient safety and risk management systems were in place. The Piper Alpha accident and the subsequent investigation had a similar impact on United Kingdom regulation. As in Norway, the previous prescriptive regulatory approach evolved into one where regulations were supplemented with a requirement for companies to demonstrate to the regulator that they had undertaken a thorough assessment of risks associated with an activity and they had adequate safety and risk management systems to address those risks. All these foreign regulators – the United Kingdom, Norway, and Canada – had previously relied on the kind of prescriptive approach used in the United States, but in the aftermath of these fatal accidents in harsh, remote offshore environments, authorities elsewhere concluded that adding a risk-based approach was essential. They faulted reliance on the “prescriptive regulation with inspection model” for being fundamentally reactive and therefore incapable of driving continuous improvement in policies and practices.[C-4]. According to Magne Ognedal, the Director General of the Norwegian Petroleum Safety Authority, the prescription-only model engendered hostility between the parties and put the risk – legal and moral – onto the regulator to accommodate changing technology, geology, and location, rather than onto the operator, where the responsibility rightly belonged. Under the new safety-management model, minimum standards for structural and operational integrity (well control, prevention of fires and explosions, and worker safety) remained in place. But the burden now rested on industry to assess the risks associated with offshore activities and demonstrate that each facility had the policies, plans, and systems in place to manage those risks. In the United Kingdom, such risk management plans were called a “Safety Case.” 2. Technical aspects of the deepwater drilling This section provides basic information on the deepwater drilling technology that is needed for proper understanding of the course of events in the Deepwater Horizon accident. This information is compiled based on Ref. [C-8] 2.1. Drilling process overview Oil and natural gas are derived from the compressed, heated remains of ancient living organisms like zooplankton and algae. Oil forms deep beneath the Earth’s surface when organic materials deposited in ancient sediments slowly transform in response to intense heat and pressure. The transformed materials can flow through porous mineral layers, and tend to migrate upward because they are lighter than other fluids in the pore spaces. If there is a path that leads to the surface, the hydrocarbons will emerge above ground. If an impermeable layer instead blocks the way, the hydrocarbons can collect in porous rock beneath the impermeable layer. The business of drilling for oil consists of finding and tapping these “pay zones” of porous hydrocarbon-filled rock (reservoirs). How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 7 Offshore drilling is similar in many ways to drilling on land. It uses drill pipe, casing, mud, and cement in a series of carefully calibrated steps to control pressure while drilling thousands of feet below the seafloor. Drilling mud, a sophisticated blend of synthetic fluids, polymers, and weighting agents, is used to lubricate and cool the drill bit during drilling. Like their onshore counterparts, offshore rig crews use drilling mud and rotary drill bits to bore a hole into the earth. The mud is pumped down through a drill pipe that connects with and turns the bit. The mud flows out of holes in the bit and then circulates back to the rig through the space between the drill pipe and the sides of the well (the annulus or annular space). As it flows, the mud cools the bit and carries pulverized rock (called cuttings) away from the bottom of the well. When the mud returns to the surface, rig equipment sieves the cuttings out and pumps the mud back down the drill string. The mud thus travels in a closed loop. Pore pressure and fracture pressure The weight of the rocks above a pay zone can generate significant pressure on the hydrocarbons. Typically, the deeper the well, the higher the pressure – and the higher the pressure the greater the challenges in safely tapping those hydrocarbons. The principal challenge in deepwater drilling is to drill a path to the hydrocarbon-filled pay zone (reservoir) in a manner that simultaneously controls these enormous pressures and avoids fracturing the geologic formation in which the reservoir is found. It is a delicate balance. In addition to carrying away cuttings, drilling mud also controls pressures inside the well as it is being drilled. The mud column inside a well exerts downward hydrostatic pressure that rig crews can control by varying the mud weight. The drillers have to monitor and adjust the mud weight to keep the pressure exerted by the mud inside the wellbore between two important points: the pore pressure and the fracture pressure. The pore pressure is the pressure exerted by fluids (such as hydrocarbons) in the pore space of rock. If the pore pressure exceeds the downward hydrostatic pressure exerted by mud inside the well, the fluids in the pore spaces can flow into the well, and unprotected sections of the well can collapse. An unwanted influx of fluid or gas into the well is called a "kick". An uncontrolled discharge is known as a "blowout". The fracture pressure is the pressure at which the geologic formation will break down or “fracture.” When fracture occurs, drilling mud can flow out of the well into the formation such that mud returns are lost instead of circulating back to the surface. This causes what is known as “lost returns” or “lost circulation.” Both pore pressure and fracture pressure vary by depth. The pore pressure gradient is a curve that shows how the pore pressure in the well changes by depth. The fracture gradient is a curve that shows how the fracture pressure in a well changes by depth. Both gradients are typically expressed in terms of an equivalent mud weight. The drillers must balance the reservoir pressure (pore pressure) pushing hydrocarbons into the well with counter-pressure from inside the wellbore. The mud plays a critical role in controlling the hydrocarbon pressure in a well. The weight of the column of mud in a well exerts pressure that counterbalances the pressure in the hydrocarbon formation. If the mud weight is too low, fluids such as oil and gas can enter the well. But if the mud weight is too high, it can fracture the surrounding How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 8 rock, potentially leading to “lost returns” – leakage of the mud into the formation. Therefore the weight (density) of the drilling mud has to be monitored and adjusted as the well is being drilled – one of many sensitive, technical tasks requiring special equipment and the interpretation of data from difficult drilling environments. Casing and cement At some point as the drilling proceeds, the pore pressure in the bottom of an open hole section will exceed the fracture pressure of the formation higher up in this open hole section. When this happens, the drillers can no longer rely on mud to control pore pressure. If the crew increases the mud weight, it will fracture the formation higher up. If the crew keeps drilling but does not increase the mud weight, hydrocarbons or other fluids in the deeper formation will flow into the well. At this point, the drillers must set casing. Casing is high-strength steel pipe that comes in 20- to 40-foot sections that are screwed together (or “made up”) on the rig to make a "casing string". The casing string serves at least two purposes – (i) it protects more fragile sections of the hole outside the casing from the pressure of the drilling mud inside, and (ii) it prevents high-pressure fluids (like hydrocarbons) outside the casing from entering the well. Once cemented in place, it isolates the wellbore from the previously penetrated formations (and their pore pressures) and serves as a conduit from the wellhead to the bottom of the well for drilling and any subsequent production activity. To cement the casing, a cementing crew pumps cement down the drill string. The cement flows down the drill string, out the bottom of the casing and back up against gravity into the annular space around the casing (between the casing and open hole). When cementing is complete, the cement fills the annular space around the casing, reinforcing the casing and creating the mechanical foundation for further drilling. This process continues as the hole is drilled using progressively smaller diameter casing and cementing each in place. Once set, the cement does two things – it seals the interior of the well (inside the casing) off from the formation outside the casing, and it anchors the casing to the rock around it, structurally reinforcing the wellbore to give it mechanical strength. Cement slurry used in the deepwater drilling is a high-tech blend of dry Portland cement, water, and numerous dry and liquid chemical additives. Operators typically employ specialized cementing contractors to design the slurry, provide the raw materials for the slurry, and pump it into place. Cementing specialists can adjust the cement slurry composition to reflect the needs of each well. For instance, they can add “accelerators” to increase the rate at which the cement sets, or “retarders” to decrease it. The first casing string (so called "conductor casing") serves as part of the structural foundation for the rest of the well. Welded to the top of the conductor casing is a wellhead assembly. The wellhead assembly remains above the seafloor and serves as an anchoring point for future casing strings. The conductor casing is inserted into place using the drill string and a “running tool” that attaches the drill string to the wellhead. The Blowout Preventer The blowout preventer (BOP) is a giant assembly of valves that latches on to the wellhead. The BOP stack serves as both a drilling tool and a device for controlling wellbore pressures. How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 9 The BOP stack is connected back to the rig by the riser. The riser is a sequence of large diameter high-strength steel pipes that serves as the umbilical cord between the rig and the BOP during all remaining drilling operations. Once rig crews lower the BOP and riser system into place atop the wellhead, they perform the rest of their drilling operations through this system. The drill string, drilling tools, and all the remaining casing strings for the well go down into the well through the riser and the BOP. In the completed well, the BOP stack is a potential barrier that can prevent hydrocarbon flow up the well and into the riser. It is done by using either the annular preventers, which can slow or stop the flow, or the blind shear rams (BSR), which shuts it off completely. The annular preventer is a large rubber element designed to close around the drill pipe and seal off the annulus. Upon activation, the annular preventer expands and fills the space within that part of the BOP; if there is something in the annular preventer (such as pipe), the annular preventer seals around it. If no drill pipe is in the hole, the annular preventer can close off and seal the entire opening. The blind shear ram consists of two metal blocks with blades on the inner edges. It is designed to cut the drill string and seal off the annulus and the drill string in the well below. It can withstand and seal a substantial amount of pressure from below. Blind shear rams are designed to cut through drill pipe but will not cut through a tool joint (the place where two pieces of pipe are threaded together), casing hangers, or multiple pieces of pipe. It does not seal the wellbore completely. BOP rams can be activated in several ways: manually from the rig, automatically (when certain conditions are met) or by remotely operated vehicle (ROV). Electrical signals are sent to subsea control pods on the BOP stack. The signals electrically open or close a solenoid valve, which in turn sends a pilot signal that activates the hydraulic system. Setting subsequent casing strings Using the drilling mud system and rotary drill bits, the drilling crew drills ahead through the previously set casing strings. The rig crew extends the open hole below the existing casing strings as far as the pore pressure and fracture gradient allow and then sets subsequent smaller diameter casing strings inside the existing ones. Each new string of casing has a smaller diameter than the previous string because it must be run through the previous string. Some of these subsequent casing strings extend all the way back up to the wellhead. Others, called liners, attach to the bottom segment of previous casing strings. A casing hanger or liner hanger mechanically holds the casing in place. Once the crew drills to a depth where a new casing string is needed, the rig crew removes the drill string from the well in a process called tripping out. Tripping out (or in) with the drill string is time-consuming; it typically takes a drilling crew an hour to trip in or out 1,000 feet, and tripping out of a deepwater well can be a day-long process. After tripping out, the drill crew attaches a running tool to the end of the drill string. The crew attaches the running tool to the casing hanger, which is in turn welded to the top of the casing. The drill crew then lowers the drill string, running tool, and casing string down the riser, through the BOP, and down into the well until the casing hanger is in position. Float Collar A “float collar” is a component installed at the bottom of a casing string. It typically consists of a short length of casing fitted with one or more check valves (called float How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 10 valves). The float collar both (1) stops wiper plugs from traveling farther down the casing string, and (2) prevents cement slurry from flowing back up the casing after it is pumped into the annular space around the casing (Fig. 2-1). During casing installation, the float valves are typically propped open by a short “auto-fill tube.” The auto-fill tube allows mud to flow upward through the float collar as the casing string is lowered. Once the casing is in place, rig personnel “convert” the float collar. By circulating mud through holes in the auto-fill tube, the rig crew creates pressure that pushes the auto-fill tube down so that it no longer props the float valves open. Once the auto-fill tube is removed, the float valves “convert” to one-way valves that allow fluid flow down the casing but prevent fluid flow upward. Cementing casing strings The process for cementing casing strings into place after installing the BOP is slightly different than cementing the early casing strings. Just as in earlier cementing steps, the rig crew pumps cement down the drill string and into place at the bottom of the well. However, because cement is typically incompatible with drilling mud, cementing crews employ two methods to keep the mud and cement separated as they flow down the well. The first involves separating the mud and cement with a water-based liquid spacer that is designed to be compatible with both oil-based drilling mud and water-based cement but that will prevent them from mixing. The second method involves further separating the spacer and cement with a plastic wiper plug that travels down the well between the spacer and the cement. While using the mud-based drilling techniques, the cementing crew starts by pumping spacer, followed by a “bottom” wiper plug, followed by a slug of cement, a “top” wiper plug, more spacer, and then drilling mud. The spacers, wiper plugs, and cement slug travel down in sequence. When the bottom plug reaches the float valve assembly near the bottom of the casing string, it ruptures, allowing the cement behind it to pass through. The cement flows through the float valves and out the bottom of the casing string. It then “turns the corner” and flows up into the annular space around the casing. How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 11 FIG 2-1. Casing C Shoe and Auto-Filll Float Colla ar (Pre- and Post-Converrsion state) When all of the ce ement has made m it thrrough the float valves, the top pplug lands on o top of the bottom plug. Unlike U the bottom plu ug, the top plug is not designed tto rupture. When it lands, it blocks the e flow of mud, m and th he resulting pressure in ncrease signnals the en nd of the cementting processs, at which h time the crew turnss off the pu umps. Cem ment should d fill the annularr space aro ound the bottom b of the casing g string and the porttion of the e casing between the botto om and the float valve es (called th he shoe track). The shhoe track is the end section of the casing. The sho oe track alsso contains cement th at, togethe er with cem ment in the annulus, serves as the prim mary barrie er preventin ng the hydrrocarbons in n the reserv voir from fllowing up the well. In this way, the shoe track k acts as a plug betw ween the inside i of thhe casing and the formation. The prroduction casing If an op perator drills a well pu urely to leaarn about th he geology of an area and assess if oil or gas are present, the t well is called an exploration n well. If the operatoor uses the well to recoverr oil, it is called c a pro oduction w well. The bo ottom-hole sections off exploratio on wells and pro oduction we ells are diffe erent. Once an operatorr is finishe ed drilling an explora ation well, they typiccally fill th he open bottom--hole sectio on with cem ment in a prrocess calle ed plugging and abanddoning. By contrast, c How to Improve Safety in Regulated Indu ustries om Each Other safety s in EU” What Could We Learn Fro Background Material, ENC CO FR-(12)-44 © ENCO Page 12 after drilling the final section of a production well, the operator typically installs a final string of production casing in the open hole section. The production casing extends past any hydrocarbon-bearing zones and down to the bottom of the well. The shoe track also contains cement that, together with cement in the annulus, serves as the primary barrier preventing the hydrocarbons in the reservoir from flowing up the well. In this way, the shoe track acts as a plug between the inside of the casing and the formation. After cementing the production casing into place, the operator can perforate the casing by shooting holes through it and the annular cement. This allows oil to flow into the well. Well control and barriers During drilling, casing, and completion operations, rig personnel must ensure that hydrocarbons do not migrate from the reservoir into the well. Well control is the process of monitoring the well and addressing any hydrocarbon influxes that are detected. To maintain well control, rig personnel must create and maintain barriers inside the well that will control subsurface pressure and prevent hydrocarbon flow. Some barriers are part of the well design itself while others are operational barriers that a drilling crew employs during the drilling process. Drilling mud is a key operational barrier. As long as the column of drilling mud inside the well exerts pressure on the formation that exceeds the pore pressure, hydrocarbons should not flow out of the formation and into the well. If mud pressure exceeds pore pressure, the well is said to be overbalanced. If pore pressure exceeds mud pressure, the well is underbalanced, meaning that the mud pressure is no longer sufficient on its own to prevent hydrocarbon flow. Physical components of the well also create barriers to flow. One is the casing installed in the well, along with the cement system in the bottom of the well. In a production casing string, the cement in the annular space and in the shoe track should prevent hydrocarbons in the formation from flowing up the annular space outside the production casing or up the inside of the well itself. Rig personnel can use additional barriers inside the well to increase the redundancy of the barrier system. For instance, rig personnel can pump cement inside the final casing string of a well to create cement plugs at various depths inside the well. Rig personnel can also install metal or plastic mechanical plugs inside the well. Some mechanical plugs are designed to be removed and retrieved later in the drilling process while others are designed to be drilled out as necessary. A BOP stack is also a potential barrier. By closing various individual rams in a BOP stack, rig personnel can close off the well, thereby preventing hydrocarbon flow up the well and into the riser. When a BOP ram is closed, it becomes a barrier to flow. However, the rams do not close instantaneously—they take anywhere from 40 seconds to a minute to close once activated. If a kick progresses beyond the point where the driller can safely shut it in with an annular preventer or pipe ram, the driller can activate the blind shear ram. When the two elements of the blind shear ram close against each other, they simultaneously shut in the well and sever the drill string. How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 13 2.2. Macondo well design and construction Macondo was an exploration well designed so that it could later be completed for production if sufficient hydrocarbons were found. The initial objective was to evaluate Miocene age formation expected to be found between 18,000 and 19,000 feet below sea level in about 5,000 feet of water. The original well plan was to drill to a total depth of 19,650 feet, but this was modified during drilling and the actual total depth was 18,360 feet. Before the well was drilled, design teams estimated pore pressures and strengths of geologic formations to create a design that included elements such as drilling procedures, drilling mud, drilling bits, casing design, cement and testing. The original plan called for eight casing strings and liners (each consisting of steel casing segments that were screwed together), but the plan was modified to react to conditions that were encountered during drilling [C-3]. Drilling ceased at 18,360 feet (a shallower depth than planned) and involved the use of a total of nine casing strings and liners, rather than the planned eight, including final 9-7/8 x 7-inch tapered production casing (sometimes referred to as a "long string"), as shown in Fig. 2-2. The space between the casing and the wellbore is sealed by pumping cement that secures the casing. FIG. 2.2. Design of Macondo well casing How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 14 The well was to be temporarily plugged and abandoned after the production casing was set and then completed for production at a later date. If a completed well can yield economically valuable oil and gas, the production can be initiated by punching holes through the casing and surrounding cement to allow hydrocarbons to flow into the well. The Macondo well presented a number of technical challenges to the drilling and completion teams, including the deep water, high formation pressures, and the need to drill through multiple geologic zones of varying pore and fracture pressure. In general, many of these problems can be anticipated, but some, such as pore and fracture pressure, are difficult to estimate in advance of drilling the well. This is especially true for the first well drilled in a new area, as was the case for Macondo. Thus, adaptation of the original well plan to the changing conditions encountered with depth when the well is drilled is not unusual. However, it is critical that the design be adapted to the changing conditions with sufficient margin for safety. Wellbore events that necessitated changes to the Macondo well plan included the following [C-1]: Measurement showed the pore pressure were increasing at a faster rate than anticipated, combined with a period of lost circulation of drilling mud at 12,350 feet, indicating that the well could not be continued without setting protective casing. The 16-inch liner was set 915 feet shallower than planned. In the course of drilling at 13,250 feet, a kick occurred, and the lower annular blowout preventer (BOP) was closed in response. During well control operation, the drill string became stuck and was severed at 12,147 feet. The drill string and hole below 12,147 feet were abandoned and subsequent well drilling deviated slightly to go around the abandoned materials left in the original hole. The depth of 13-5/8 inch and 11-7/8 inch were set shallower than planned to allow for the use of higher mud weight to control the well when passing the high pressure reservoir at 15,103 feet. The 9-7/8 inch casing (originally planned as the production casing) was used as a liner at 17,168 feet to drill the final section of the well safely. During drilling at 18,250 feet, severe lost circulation of drilling mud occurred. This problem was handled by the use of mud containing material designed to stop lost circulation and by reducing of mud weight. The lower mud weight was not anticipated in the plan. It was an indication that pore pressure and fracture pressure in part of this interval were considerably less than anticipated. The well was drilled to 18,360 feet, and after 5 days of logging to make a detailed record of the geologic formation, it was determined that hydrocarbon-bearing reservoirs of sufficient quality existed to warrant completion of the well for production at a later time. According to BP investigation report [C-1] there were in fact several reservoirs with decreasing pore pressure with depth. One of the reservoirs containing salt water had a pore pressure exceeding the pore pressure of reservoirs containing hydrocarbons. The difference between the mud weight needed to prevent flow of salt water and the mud weight above which reservoir fracture could occur was very small (only 0.2 pounds per gallon). To continue drilling to the planned final depth of 19,650 feet, the reservoir that had been discovered with decreasing pore and fracture pressures with depth were to be sealed with 9-7/8 x 7-inch combination casing string and cement. However, because the hole diameter that could be drilled below the 7-inch casing was considered to small to be practical, the well was terminated at 18.360 feet. How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 15 2.3. Preparing the well for subsequent production Installation of the production casing At this stage of the Macondo drilling operation the next challenge was to install the production casing and pump the cement into the well without causing additional lost circulation. Based of the BP report [C-1] this was achieved without problems. Relevant details regarding these activities, which could have had a material impact on the accident and seem to be relevant from the point of view of accident causes, are discussed below (based on Ref. [C-4]). Use of long string BP’s design team originally had planned to use a “long string” production casing – a single continuous wall of steel between the wellhead on the seafloor, and the oil and gas zone at the bottom of the well. But after the lost circulation event, they were forced to reconsider this solution. As another option, they evaluated a “liner” – a shorter string of casing hung lower in the well and anchored to the next higher string. A liner would result in a more complex – and theoretically more leak-prone – system over the life of the well. But it would be easier to cement into place at Macondo. The long string implied several difficulties with the cementing job. First, it required the cement to travel through a longer stretch of steel casing – roughly 12,000 feet longer – before reaching its final destination, potentially increasing the risk of cement contamination. Second, because it can require higher cement pumping pressure, a long string design can lead to the selection of lower cement volumes, lower densities, and lower pump rates. Third, the cement job at the bottom of a long string is more difficult to remediate than one at the bottom of a liner. On April 14 and 15, BP’s engineers, working with a Halliburton engineer, used sophisticated computer programs to model the likely outcome of the cementing process. Early results suggested the "long string" could not be cemented reliably. However, changing the original design of a "long string" to a "liner" met resistance within BP. A BP expert assigned to the modelling team determined that certain inputs should be corrected. Calculations with the new inputs showed that a long string could be cemented properly. The BP engineers accordingly decided that installing a "long string" was “again the primary option”. Installing the agreed-upon casing was a major job. More than 18 hours was needed to lower a tool, such as a drill bit, from the rig floor to the bottom of the well, 18,000 feet below sea level. Assembling the production casing section-by-section and lowering the lengthening string down into the well below required roughly 37 hours. Centralizers As the crew gradually assembled and lowered the casing, they paused several times to install centralizers at predetermined points along the casing string. Centralizers are critical components in ensuring a good cement job. When a casing string hangs in the center of the wellbore, cement pumped down the casing will flow evenly back up the annulus, displacing any mud and debris that were previously in that space and leaving a clean column of cement. If the casing is not centred, the cement will flow preferentially up the path of least resistance – the larger spaces in the annulus – and slowly or not at all in the narrower annular space. That can leave behind channels of drilling mud that can How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 16 severely compromise a primary cement job by creating paths and gaps through which pressurized hydrocarbons can penetrate. This issue is known as "channelling" problem. BP’s original designs had called for 16 or more centralizers to be placed along the long string. But on April 1, BP team learned that BP’s supplier (Weatherford) had in stock only six “subs” – (inline centralizers) designed to screw securely into place between sections of casing. The alternative was to use “slip-on” centralizers – devices that slide onto the exterior of a piece of casing where they are normally secured in place by mechanical “stop collars” on either side. These collars can either be welded directly to the centralizers or supplied as separate pieces. However, the slip-on centralizers with separate stop collars can slide out of position or, worse, catch on other equipment as the casing is lowered. Shortly after the BP team decided on the long string, Halliburton ran computer simulations using proprietary software called OptiCem, to predict whether mud channelling would occur. The calculations suggested that the Macondo production casing would need more than six centralizers to avoid channelling. The BP Drilling Engineering Team Leader, obtained permission from senior manager to order 15 additional slip-on centralizers. Haliburton reran their simulations and found that channelling due to gas flow would be less severe with 21 centralizers in place. When the new centralizers arrived, it appeared that they are not custom-designed onepiece units that BP had used on a prior well and would limit the potential for centralizer “hang up”. The earlier decision of using additional centralizers was challenged by the well's team leader. He questioned the need for additional centralizers, and BP drilling engineer on shore finally decided to use only the 6 centralizers of "subs" type. Installation of the long string and preparation for cementing Early on the morning of April 18, with a centralizer plan in hand, the rig crew finally began assembling and lowering the long string into position. The leading end of the casing, the “shoe track,” began with a “reamer shoe” – a bullet-shaped piece of metal with three holes designed to help guide the casing down the hole. The reamer shoe was followed by 180 feet of 7" diameter steel casing. Then came Weatherford-manufactured “float collar,” with two flapper valves, held open by a short “auto-fill tube” through which the mud in the well could flow. As the long string was lowered down the wellbore, the mud passed through the holes in the reamer shoe and auto-fill tube that propped open the float valves, giving it a clear flow path upward. The long string was installed in its final position early on the afternoon of April 19. With the top end of the string seated in the wellhead and its bottom end located just above the bottom of the wellbore, the crew’s next job was to prepare the float-valve system for cementing. During the cementing process, fluids pumped into the well should flow in a one-way path: down the centre of the last casing string, out the bottom, and up the annulus (between the exterior of the steel casing and the surrounding rock formations). To ensure unidirectional flow, the crew needed to convert the float valves (i.e. push the auto-fill tube downward, so it would no longer prop open the float valves). With the tube out of the way, the flapper valves would spring shut and convert from two-way valves into one-way valves that would allow mud and cement to flow down the casing into the shoe track, but prevent any fluid from reversing direction and coming back up the casing. Once the float valves had converted, Halliburton could pump cement down through the casing and up around the annulus; the valves would keep cement from flowing back up the casing once the crew stopped pumping. How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 17 Pressure anomalies in the well To convert the float valves, that evening the crew began pumping mud down through the casing. Based on Weatherford’s specifications, the valves should convert once the rate of flow though holes in the auto-fill tube had reached roughly 6 barrels per minute (bpm), causing a differential pressure on the tube of approximately 600 pounds per square inch (psi). But the crew pumped fluids into the well, eventually pressuring up to 1,800 psi, but could not establish flow. In consultation with BP supervisor on shore and Weatherford staff, the rig team decided to increase the pump pressure in discrete increments, hoping eventually to dislodge the autofill tube. On their ninth attempt, pump pressure peaked at 3,142 psi and then suddenly dropped as mud finally began to flow. Significantly, however, the pump rate of mud into the well and through the shoe track thereafter never exceeded approximately 4 bpm. BP’s team concluded that the float valves had converted, but noted another anomaly. The circulation pressure after converting the float valves (340 psi) was much lower than the drilling-mud subcontractor, M-I SWACO had predicted (570 psi). BP’s well site leader and the Transocean crew switched circulating pumps to see if that made a difference, and eventually concluded that the pressure gauge they had been relying on was broken. Believing they had converted the float valves and re-established mud circulation in the well, BP was ready at last to pump cement down the production casing and complete the primary cement job. The cement design In the days leading up to the final cementing process, BP engineers focused heavily on the biggest challenge: the risk of fracturing the formation and losing returns. If their cementing procedure placed too much pressure on the geologic formation below, it might trigger another lost-returns event similar to the one on April 9. In this case, critical cement – not mud – might flow into the formation and be lost, potentially leaving the annular space at the bottom of the well open to hydrocarbon flow. These concerns led BP to place a number of significant constraints on Halliburton’s cementing design. The first compromise in BP’s plan was to limit the circulation of drilling mud through the wellbore before cementing. Optimally, mud in the wellbore would have been circulated “bottoms up” – meaning the rig crew would have pumped enough mud down the wellbore to bring mud originally at the bottom of the well all the way back up to the rig. Such extensive circulation cleans the wellbore and reduces the likelihood of channelling. And circulating bottoms up allows technicians on the rig to examine mud from the bottom of the well for hydrocarbon content before cementing. But the BP engineers feared that the longer the rig crew circulated mud through the casing before cementing, the greater the risk of another lost-returns event. Accordingly, BP circulated approximately 350 barrels of mud before cementing, rather than the 2,760 barrels needed to do a full "bottoms up" circulation. BP compromised again by deciding to pump cement down the well at the relatively low rate of 4 barrels or less per minute. Higher flow rates tend to increase the efficiency with which cement displaces mud from the annular space. But the increased pump pressure required would mean more pressure on the formation (ECD) and an increased risk of lost How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 18 returns. BP decided to reduce the risk of lost returns in exchange for a less-than-optimal rate of cement flow. BP made a third compromise by limiting the volume of cement that Halliburton would pump down the well. Pumping more cement is a standard industry practice to insure against uncertain cementing conditions: more cement means less risk of contamination and less risk that the cement job will be compromised by slight errors in placement. But more cement at Macondo would mean a higher cement column in the annulus, which in turn would exert more pressure on the fragile formation below. Accordingly, BP determined that the annular cement column should extend only 500 feet above the uppermost hydrocarbon-bearing zone (and 800 feet above the main hydrocarbon zones), and that this would be sufficient to fulfill MMS regulations of “500 feet above the uppermost hydrocarbon-bearing zone.” However, it did not satisfy BP’s own internal guidelines, which specify that the top of the annular cement should be 1,000 feet above the uppermost hydrocarbon zone. Finally, in close consultation with Halliburton, BP chose to use “nitrogen foam cement” – a cement formula that has been leavened with tiny bubbles of nitrogen gas, injected into the cement slurry just before it goes down the well. This formula was chosen to lighten the resulting slurry – thereby reducing the pressure the cement would exert on the fragile formation. The bubbles, in theory, would also help to balance the pore pressure in the formation and clear the annular space of mud as the cement flowed upward. Halliburton is an industry leader in foam cementing, but BP appears to have had little experience with foam technology for cementing production casing in the Gulf of Mexico. Laboratory tests of the cement slurry Cement slurry must be tested before it is used in a cement job. The laboratory tests performed by Haliburton for the Macondo's cement slurry were intended to make sure the cement will work under the conditions in the well. It included evaluating the slurry’s viscosity and flow characteristics, the rate at which it will cure, and its eventual compressive strength. When testing a slurry that will be foamed with nitrogen, the lab also evaluates the stability of the cement that results. Stable foam slurry will retain its bubbles and overall density long enough to allow the cement to cure. The result is hardened cement that has tiny, evenly dispersed, and unconnected nitrogen bubbles throughout. If the foam does not remain stable up until the time the cement cures, the small nitrogen bubbles may coalesce into larger ones, rendering the hardened cement porous and permeable. If the instability is particularly severe, the nitrogen can “break out” of the cement, with unpredictable consequences. On February 10, soon after the Deepwater Horizon began work on the well, Halliburton laboratory personnel run a series of “pilot tests” on the cement blend stored on the Deepwater Horizon that Halliburton planned to use at Macondo. They tested the slurry and the laboratory report was sent to BP on March 8 as an attachment to an e-mail which provided recommended plan for cementing an earlier Macondo casing string. The reported data that Haliburton sent to BP on March 8 included the results of a single foam stability test. To the trained eye, that test showed that the February foam slurry design was unstable. The report did not comment on the evidence of the cement slurry’s instability, and there is no evidence that BP examined the foam stability data in the report at all. How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 19 Documents identified after the blowout reveal that Halliburton personnel had also conducted another foam stability test earlier in February. The earlier test had been conducted under slightly different conditions than the later one and had failed more severely. It appears that Halliburton never reported the results of the earlier February test to BP. Halliburton conducted another round of tests in mid-April, just before pumping the final cement job. By then, the BP team had given Halliburton more accurate information about the temperatures and pressures at the bottom of the Macondo well, and Halliburton had progressed further with its cementing plan. Using this information, the laboratory personnel conducted several tests, including a foam stability test, starting on approximately April 13. The first test Halliburton conducted showed once again that the cement slurry would be unstable. There is no evidence that Halliburton ever reported this information to BP. Instead, it appears that Halliburton personnel subsequently ran a second foam stability test, this time doubling the pre-test “conditioning time” to three hours. The evidence suggests that Halliburton began the second test at approximately 2:00 a.m. on April 18. That test would normally take 48 hours. Halliburton finished pumping the cement job just before 48 hours would have elapsed. Although the second test at least arguably suggests the foam cement design used at Macondo would be stable, it is unclear whether Halliburton had results from that test in hand before it started the cement job. Halliburton did not send the results of the final test to BP until April 26, six days after the blowout. Cement evaluation log The BP team focused on full returns as the sole criterion for deciding whether to run a cement evaluation log. Receiving full returns was a good indication that cement or other fluids had not been lost to the weakened formation. But full returns provided, at best, limited or no information about: (1) the precise location where the cement had ended up; (2) whether channelling had occurred; (3) whether the cement had been contaminated; or (4) whether the foam cement had remained stable. Although other indicators – such as on-time arrival of the cement plugs and observation of expected lift pressure – were reassuring, they too provided limited information. Other cement evaluation tools could have provided more direct information about cementing success. Cement evaluation logs plainly have their limitations, particularly at Macondo. But while many companies do not run cement evaluation logs until the completion phase, BP should have run one here – or sought other equivalent indications of cement quality in light of the many issues surrounding and leading up to the cement job. Testing of the wellhead seals Once the casing and cementing operations were concluded, the focus moved to the installation and testing of the integrity of the wellhead seals and testing of the integrity of the cement, and then to completion of the temporary abandonment process. April 20 was devoted to a series of tests on the rig to check integrity of the well. This included positive- and negative-pressure tests in preparation for “temporary How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 20 abandonment.” During the positive-pressure test, the drill crew increased the pressure inside the steel casing and seal assembly to be sure they were intact. The negative-pressure test, by contrast, reduced the pressure inside the well in order to simulate its state after the Deepwater Horizon had packed up and moved on. If pressure increased inside the well during the negative-pressure test, or if fluids flowed up from the well, that would indicate a well integrity problem – a leak of fluids into the well. Such a leak would be a worrisome sign that somewhere the casing and cement had been breached – in which case remedial work would be needed to reestablish the well’s integrity. The negative-pressure test checks not only the integrity of the casing, like the positivepressure test, but also the integrity of the cement job. At the Macondo well, the negativepressure test was the only test performed that would have checked the integrity of the bottom-hole cement job. Typical procedure for the test is as follows. First, the crew sets up the well to simulate the expected hydrostatic pressure exerted by the column of fluids on the bottom of the well in its abandoned state. Second, the crew bleeds off any pent-up pressure that remains in the well, taking it down to 0 psi. Third, they make sure that nothing flows up from and out of the well and that no pressure builds back up inside of the well. If there is no flow or pressure buildup, that means that the casing and primary cement have sealed the well off from external fluid pressure and flow. A negative-pressure test is successful if there is no flow out of the well for a sustained period and if there is no pressure build-up inside the well when it is closed at the surface. Conduct of these two tests at the Macondo well and their results are briefly overviewed below. Positive-pressure test The crew started the positive-pressure test at noon. They pressured the well up to 250 psi for 5 minutes, and then pressured up to 2,500 psi and watched for 30 minutes. The pressure inside the well remained steady during both tests, showing there were no leaks in the production casing through which fluids could pass from inside the well to the outside. The drilling crew and BP’s well site leader considered the test successful. Negative-pressure test The crew began the negative test of Macondo at 5:00 p.m. Earlier in the day, the crew had prepared for the negative test by setting up the well to simulate the planned removal of the mud in the riser and 3,300 feet of drilling mud in the wellbore. The crew ran the drill pipe down to approximately 8,367 feet below sea level and then pumped a “spacer” – a liquid mixture that serves to separate the heavy drilling mud from the seawater – followed by seawater down the drill pipe to push (displace) 3,300 feet of mud from below the mud line to above the BOP. While drilling crews routinely use water-based spacer fluids to separate oil-based drilling mud from seawater, the spacer BP chose to use during the negative pressure test was a mixture of two different lost-circulation materials left over on the rig. BP wanted to use these materials as spacer in order to avoid having to dispose of them onshore as hazardous waste pursuant to the Resource and Conservation Recovery Act, exploiting an exception that allows companies to dump water based “drilling fluids” overboard if they have been circulated down through a well. At BP’s direction, M-I SWACO combined the materials to How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 21 create an unusually large volume of spacer that had never previously been used by anyone on the rig or by BP as a spacer, nor been thoroughly tested for that purpose. Once the crew had displaced the mud to above the BOP, they shut an annular preventer in the BOP, isolating the well from the downward pressure exerted by the heavy mud and spacer in the riser. The crew could now perform the negative-pressure test using the drill pipe by opening the top of the drill pipe on the rig, bleeding the drill pipe pressure to zero, and then watching for flow. The crew opened the drill pipe at the rig to bleed off any pressure that had built up in the well during the mud-displacement process. The crew tried to bleed the pressure down to zero, but could not get it below 266 psi. When the drill pipe was closed, the pressure jumped back up to 1,262 psi. The crew had noticed that the fluid level inside the riser was dropping, suggesting that spacer was leaking down past the annular preventer, out of the riser, and into the well. This problem was solved by the annular preventer closed more tightly. With that problem solved, the crew refilled the riser and once again opened up the drill pipe and attempted a second time to bleed the pressure down to 0 psi. This time, they were able to do so. But when they shut the drill pipe in again, the pressure built back up to at least 773 psi. The crew then attempted a third time to bleed off the pressure from the drill pipe, and was again able to get it down to 0 psi. When the crew shut the well back in, however, the pressure increased to 1,400 psi. At this point, the crew had bled the drill-pipe pressure down three times, but each time it had built back up. For a successful negative-pressure test, the pressure must remain at 0 psi when the pipe is closed after the pressure is bled off. The results were discussed by Transocean crew and BP Well site leaders and they finally concluded that the 1,400 psi pressure on the drill pipe was being caused by a phenomenon called the “bladder effect.” According to one of the toolpushers this is the effect caused by heavy mud in the riser exerting pressure on the annular preventer, which in turn transmitted pressure to the drill pipe. The negative test was repeated on the kill line as it had been specified in a permit application submitted earlier to MMS. For the second test, the crew opened the kill line and bled the pressure down to 0 psi. A small amount of fluid flowed, and then stopped. Rig personnel left the kill line open for 30 minutes but did not observe any flow from it. The test on the kill line thus satisfied the criteria for a successful negative pressure test – no flow or pressure buildup for a sustained period of time. But the pressure on the drill pipe remained at 1,400 psi throughout. The well site leaders and crew never appear to have reconciled the two different pressure readings. The “bladder effect” may have been proposed as an explanation for the anomaly – but based on available information, the 1,400 psi reading on the drill pipe could only have been caused by a leak into the well. Nevertheless, at 8 p.m., BP well site leaders, in consultation with the crew, made a key error and mistakenly concluded the second negative-pressure test procedure had confirmed the well’s integrity. They declared the test a success and moved on to the next step in temporary abandonment. Temporary abandonment Once BP decided not to run the cement log test, Deepwater Horizon’s crew began the final phase of its work. Drilling the Macondo well had required a giant offshore rig of Deepwater How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 22 Horizon’s capabilities. By contrast, BP, like most operators, would give the job of “completing” the well to a smaller (and less costly) rig, which would install hydrocarboncollection and -production equipment. To make way for the new rig, the Deepwater Horizon would have to remove its riser* and blowout preventer from the wellhead – and before it could do those things, the crew had to secure the well through a process called “temporary abandonment.” Four features of the temporarily abandoned well are worth noting. First is the single 300-foot-long cement plug inside the wellbore. MMS regulations required BP to install a cement plug as a backup for the cement job at the bottom of the well. Second is the location of the cement plug: BP planned to put it 3,300 feet below the ocean floor, or “mud line” (which was deeper than MMS regulations allowed without dispensation, and deeper than usual). Third is the presence of seawater in the well below the sea floor: BP planned to replace 3,000 feet of mud in the wellbore above the cement plug with much lighter seawater (seawater weighs roughly 8.6 ppg, while the mud in the wellbore weighed roughly 14.5 ppg). Fourth is the lockdown sleeve – a mechanical device that locks the long casing string to the wellhead to prevent it from lifting out of place during subsequent production operations. At 10:43 a.m., BP engineer e-mailed an “Ops Note” to the rest of the Macondo team listing the temporary abandonment procedures for the well. It was the first time the BP well site leaders on the rig had seen the procedures they would use that day. BP first shared the procedures with the rig crew at the 11 a.m. pre-tour meeting that morning. The basic sequence was as follows: 1. Perform a positive-pressure test to test the integrity of the production casing; 2. Run the drill pipe into the well to 8,367 feet (3,300 feet below the mud line); 3. Displace 3,300 feet of mud in the well with seawater, lifting the mud above the BOP and into the riser; 4. Perform a negative-pressure test to assess the integrity of the well and bottom-hole cement job to ensure outside fluids (such as hydrocarbons) are not leaking into the well; 5. Displace the mud in the riser with seawater; 6. Set the surface cement plug at 8,367 feet; and 7. Set the lockdown sleeve. The crew would never get through all of the steps in the procedure. BP’s Macondo team had made numerous changes to the temporary abandonment procedures in the two weeks leading up to the April 20 “Ops Note.” For example, in its April 12 drilling plan, BP had planned (1) to set the lockdown sleeve before setting the surface cement plug and (2) to set the surface cement plug in seawater only 6,000 feet below sea level (as opposed to 8,367 feet). The April 12 plan did not include a negativepressure test. On April 14, a different procedure was set forth, which included a negativepressure test but would require setting the surface cement plug in mud before displacement of the riser with seawater. On April 16, BP sent an 'Application for Permit to Modify' to MMS describing a temporary abandonment procedure that was different from the procedure in either the April 12 drilling plan, the April 14 e-mail, or the April 20 “Ops Note.” There is no evidence that these changes went through any sort of formal risk assessment or management of change process. How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 23 Design features of the Ma acondo we ell Fig. 2-3 3 gives a scchematic picture of th he Macondo well (tak ken from thhe BP invesstigation report [C-1]). Thiss shows the e cement b barrier whic ch failed and allowedd hydrocarb bons and mud fro om the rese ervoir to esc cape througgh the drilll pipe (the main pipe tthrough the e middle section)). This figurre also show ws the Blow wout Preven nter (BOP) stack. s Fill lines Kill line F FIG. 2-3. Macondo well ((the source: BP, "Deepwa ater Horizonn Accident A Inveestigation Re eport" [C-1]). How to Improve Safety in Regulated Indu ustries om Each Other safety s in EU” What Could We Learn Fro Background Material, ENC CO FR-(12)-44 © ENCO Page 24 2.4. Overview of the accident Table 1-1 provides timing of relevant events that contributed to the accident. This is a much simplified version of the chronology that aims to give an overview of the events that is accessible to non-specialists, for the purpose of understanding the accident and explaining how safety barriers were breached. Table 1-1. Chronology of the accident Date/Tim e Description of events April 9 -14 The final section of the well is drilled. Total depth of 18,360 ft reached and data collected for five days April 14th Haliburton OptiCem software for cement model confirmed acceptability of using 9 7/8 x 7 inch long string as production casing April 15th OptiCem model updated with 21 centralizers. Decision made to order 15 additional centralizers April 16th Fifteen slip-on bow spring centralizers delivered to rig by helicopter. Mechanical integrity concerns regarding the bow spring centralizers. Decision made not to use bow spring centralizers (instead using 7 inline centralizers) April 19 20 Cement job pumped as planned with full fluid returns observed. Bottom plug burst disk ruptured at higher-than-planned pressure. Cement job completed April 20, at 00:36 hrs April 20th Integrity Test of well carried out: - positive pressure test (successful) - negative pressure test (results interpreted as successful). This test places the well in a controlled underbalanced state to test the integrity of the mechanical barriers. 17:35 Whilst carrying out the negative pressure test, the BP team leader realizes that the rig crew are using a process for negative testing that is not the BP preferred method. Operations are reconfigured to meet the requirements of the permit (a permit is a safety system which only allows work to progress when authorized persons have set out the way the work will be carried out, and defines roles and responsibilities and how risks are being controlled). 18.42 – 20.00 Sea water is pumped into the kill line to confirm that it is full, the fill line is routed to the mini trip tank and flow stops. The line is monitored for 30 minutes and shows no flow. They notice that the drill line pressure is still high and discuss, but this is attributed to the ‘Bladder effect’. The crew assume that the negative pressure test is successful. How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 25 Date/Tim e Description of events 20.00 – 21.01 The crew starts normal activities for temporary abandonment of the well (as it is deemed commercially viable for production drilling) – this involves returning it to the normal ‘overbalanced’ position. However, during the process, at approximately 20.52, the well goes into an underbalanced position – this means that the pressure on drill side is less than in the reservoir and therefore hydrocarbons start to flow. During this time the crew were emptying the trip tank – which may have masked the indication of flow. Drill pipe pressure increases – this should have alerted crew, but it was not noticed. 21.08 The team is busy carrying out a test to check if fluids can be displaced overboard. As part of this test the pumps are shut down. 21.31 approx The differential pressure is discussed – indicating that the drill pipe pressure has been noticed and acknowledged as something that was not expected. 21.40 Mud overflows onto the rig floor. The crew diverts the mud flow to the mud gas separator. Crew close the annular preventer and drill pipe pressure steadily increases. Mud and hydrocarbons discharge onto the rig and overboard 21.45 Assistant driller calls senior toolpusher to report ‘the well is blowing out. [the toolpusher] is shutting it in now’. 21.47 Gas alarms sound. There is a rapid increase in pressure in the drill pipe. 21.48 Gas probably enters the engine room air intake and explosions shake the rig. Extensive damage ensues, possibly damaging the cables which allow the communication of emergency shut-down system with the Blow Out Preventer. Emergency shutdown activation is unsuccessful – the BOP is unable to seal the well – hydrocarbons continue to feed the fire and explosions. 22.00 Order given to abandon the ship. 11 people were determined to be missing and the search and rescue activities commenced: no-one was found. Results of negative-pressure test were incorrectly interpreted by the crew, suggesting that pressure is at a safe level. Apparently the cementing processes failed to provide an effective barrier to hydrocarbon flow. Gas and oil leaked through shoe track barrier and float collar. The crew did not recognize there was a major problem or act to control it until the hydrocarbons were flowing rapidly up the riser. The impact of the decision to proceed to temporary abandonment was compounded by delays in recognizing that hydrocarbons were flowing into the well and riser and by a failure to take timely and aggressive well-control actions. Furthermore, failures and/or limitations of the BOP, when it was actuated, inhibited its effectiveness in controlling the well. The crew closed the blowout preventer and diverter, routing oil and gas to the mud gas separator (MGS) system rather than diverting it overboard. The MGS was overwhelmed by the force of oil and gas which leaked into the rig's ventilation system. The heating, ventilation and air conditioning system is thought to have sent a gas-rich mixture into the engine rooms. How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 26 At about 9:49 p.m., the rig unexpectedly began to shake and a loud surging noise was accompanied by natural gas, drilling mud and sea water that shot high above the floor of the drill ship. The gas exploded and the rig was engulfed in flames. A second explosion followed and the electricity went out. Eleven men died instantly and 115 others rushed to the lifeboats or jumped into the Gulf of Mexico. This all happened so fast that those who died probably had no time to understand what was happening. Two days later, the Deepwater Horizon sank to the bottom of the Gulf of Mexico, and oil has been spilling into the Gulf at rates of at least 5,000 barrels per day since then (there are 42 gallons in a barrel). Attempts to isolate the well using the available equipment were unsuccessful. The BOP designed to work automatically did not control, or recapture control, of the well once it was realized that hydrocarbons were flowing into the well. Also, both the emergency disconnecting system designed to separate the lower marine riser from the rest of the BOP and automatic sequencers controlling the shear ram and disconnect failed to operate. 3. Investigation into explosion The Deepwater Horizon explosion in April 20, 2012 resulted in the loss of life of people and caused one of the worst oil spills in history which had tremendous impact on the environment. Investigation of this accident was conducted by many organizations directly involved in the design and construction of the Macondo well, but also by many other entities representing the government and the public. From industry side it includes BP, which owned the Macondo well, Transocean (rig owner) and Halliburton (cementer), which managed the well-sealing operation. From government side investigations of causes of the accident were undertaken by the National Academy of Engineering (for the Department of Interior), the Chemical Safety Board, the US Coast Guard and the Bureau of Ocean Energy Management. There were also various Congressional inquiries, and Department of Justice criminal and civil probes. The accident was of high interest from the side of media. On May 22, 2010, President Barack Obama announced the creation of the National Commission on the BP Deepwater Horizon Oil Spill and Offshore Drilling: an independent entity, directed to provide a thorough analysis and impartial judgment. The Commission charter was to determine the causes of the disaster, and to improve the country’s ability to respond to spills, and to recommend reforms to make offshore energy production safer. The Commission reviewed thousands of pages of documents, interviewed hundreds of witnesses, and in the autumn conducted a series of public hearings. The intense six-month effort was concluded in the report issued in January 11, 2011 [C-3]. This section summarizes results of selected investigation reports that were released as public domain documents. These include: - British Petroleum Investigation Report Report of Human Reliability Associates Ltd of UK (retrieved from web site) Reports of Oil Spill Commission (including "Report to the President" and "Chief Councel's Report") How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 27 - Report of National Academy of Engineering (NAE) and National Research Council (NRC) prepared for the Department of Interior. The BP report was the first comprehensive investigation report from the industry side published on September 8, 2010 [C-1]. The report included factual information that was used as a starting point for other investigations. The report of Human Reliability Associates is a prompt response to BP report. It provides some views regarding the human factor. It also raises some questions that were not addressed in the BP investigation report. The findings of Oil Spill Commission have been published in two comprehensive reports: "Report to the President" and "Chief Councel's Report". The "Report to the President" focuses on regulatory oversight of leasing, energy exploration and production of oil, human safety and environmental protection. This report includes one chapter devoted to the well blowout and rig explosion. That chapter summarized the results of the investigation by the Commission’s Chief Counsel, Fred Bartlit and his investigative team into the causes of the Macondo well blow out and Deepwater Horizon rig explosion. The "Chief Councel's Report" provide more detailed insights regarding the root causes of the Macondo well blowout and explosion on the Deepwater Horizon. The Report of NAE/NRC presents the consensus view of a committee of 15 experts on the immediate and the root causes that led to loss of well control and the rig accident. It provides observations concerning key factors and decisions that may have contributed to the blowout of the Macondo well, including engineering, testing, and maintenance procedures, operational oversight, regulatory procedures and personnel training/certification. Brief overview of the above mentioned reports are provided in Sections 3.1 – 3.4. 3.1. BP investigation report BP Exploration and Production Inc. – the lease of Mississippi Canyon Block 252 and Macondo well – started investigation of the DH accident immediately in the aftermath of the accident independently from other spill response activities and organizations. BP investigation team was charged with gathering the facts surrounding the accident, analyzing available information to identify possible causes and making recommendations to enable prevention of similar accidents in the future. The team had access to partial real-time data from the rig, documents from various aspects of the Macondo well's development and construction, witness interviews and testimony from public hearings. The team used information that was made available by other companies, including Transocean, Haliburton and Cameron. Over the course of the investigation, the team involved over 50 internal and external specialists from a variety of fields. BP investigation report of 193 pages was released on September 8, 2010. The report states that no one action or inaction was behind the accident. Instead, "multiple companies, work teams and circumstances were involved over time". It blames the combination of "a complex and interlinked series of mechanical failures, human judgments, engineering design, operational implementation and team interfaces". How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 28 The report identified eight interlinked factors that contributed to the accident. They correspond to the existing safety barriers that were intended to ensure safety of the rig. These barriers include three types of safeguards: physical, administrative, and human action type. The following key safeguards are indicated in the BP report: Well integrity was not established or failed 1. Annulus cement barrier did not isolate hydrocarbons 2. Shoe track barriers did not isolate hydrocarbons Hydrocarbons entered the well undetected and well control was lost 3. Negative pressure test was accepted although well integrity had not been established 4. Influx was not recognized until hydrocarbons were in the riser 5. Well control response action failed to regain control of well Hydrocarbons ignited on the Deepwater Horizon 6. Diversion to mud gas separator resulted in gas venting onto rig 7. Fire and gas system did not prevent hydrocarbon ignition Blowout preventer did not seal the well 8. Blowout preventer (BOP) emergency modes did not seal well. The key factors mentioned above are briefly discussed below. Annulus cement barrier The day before the accident cement had been pumped down the production casing and up into the wellbore annulus to prevent hydrocarbons entering the wellbore from the reservoir. The annulus cement was light, nitrified foam cement slurry. Lab tests carried out as part of the investigation suggest that the slurry was unstable at drilling depth pressures and temperatures and there was likely to be nitrogen breakout and migration, resulting in incorrect cement density and allowing hydrocarbons to enter the wellbore annulus. Nitrogen migration would have also contaminated the shoe cement and may have caused the shoe track cement barrier to fail. The slurry was not fully tested before use. The report concludes that there was little focus on other important aspects of design, for example, foam stability, contamination effects and fluid loss potential were not considered. The BP investigation says there were "weaknesses in cement design and testing, quality assurance and risk assessment". It suggests that "improved engineering rigour, cement testing and communication of risk" by Halliburton could have identified those flaws. But the report also says the Houston-based BP staff at the site could have raised awareness of the problems. Shoe track barrier Having entered the wellbore annulus, hydrocarbons passed down the wellbore and entered the space between the 7-inch production casing and the 9 7/8-inch protection casing through the shoe track installed in the bottom of the casing. The BP investigation team concluded that hydrocarbons ingress was through the shoe track rather than through a How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 29 failure in the production casing itself or up the wellbore annulus and through the casing hanger seal assembly. For this to happen, both barriers in the shoe track must have failed to prevent hydrocarbon entry into the production casing. The first barrier was the cement in the shoe track, and the second was the float collar, a device (two flapper valves) at the top of the shoe track designed to prevent fluid ingress into the casing. Negative pressure test A "negative-pressure test" was carried out to check the mechanical barriers (the shoe track, production casing and casing hanger seal assembly). The test involved replacing heavy drilling mud with lighter seawater to place the well in a controlled underbalanced condition. In retrospect, pressure reading and volume bled at the time of the negativepressure test were indications of flow path communication with the reservoir, signifying that the integrity of these barriers had not been achieved. Witnesses state that the toolpusher (rig crew) suggested that the pressure on the drill pipe was due to a phenomenon they (toolpusher and driller) had seen before called ‘annular compression’ or the ‘bladder effect’. Transocean rig crew and BP leaders on the site accepted that and carried on. The report says that they "reached the incorrect view" that the test had been a success and the well integrity had been established. It is stated that the responsible crew did not correctly interpret a pressure test, and both companies neglected ominous signs such as a riser pipe losing fluid. The report also says that while BP did not listen to recommendations by Halliburton for more centralizers, the lack of centralizers probably did not affect the quality of the cement barrier. Recognition of hydrocarbons influx With the negative-pressure test having been accepted, the well was returned to an overbalanced condition, preventing further influx into the wellbore. Later, as part of normal operations to temporarily abandon the well, heavy drilling mud was again replaced with seawater underbalancing the well. Over time, this allowed hydrocarbons to flow up through the production casing and passed the BOP. For an estimated 40 minutes, the influx of gases into the well was apparently not spotted. By this time "hydrocarbons were rapidly flowing to the surface" and, according to witnesses, mud flowed uncontrolled on to the rig platform. The report says that the Transocean rig crew and a team described as "mudloggers" working for Halliburton Sperry Sun may have been distracted by what are described as "end-of-well activities" such as setting a cement plug in the casing, bleeding off the riser tensioners, and transferring mud to the supply vessel and, as a result, important monitoring was not carried out for more than seven hours. The well should have been monitored continuously – however, procedures did not specify how this should be achieved during activities such as in-flow testing, cleaning or other endof-well activities. Well control response action The first well control actions were to close the BOP and diverter, routing the fluid exiting the riser to the mud gas separator (MGS). Closing the BOP was unsuccessful. It did not seal How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 30 properly and was too late as hydrocarbons were already in the riser. Then hydrocarbons were diverted to the mud gas separator (MGS). The alternative of dumping it overboard through 14 in pipe was not chosen. This would (probably) have diverted it safely overboard. Diversion of blowout to the MGS Diversion to the MGS resulted in gas venting onto the rig through the 12 in goosenecked vent exiting the MGS. The high pressure hydrocarbons were diverted through the MGS which was designed for low pressure only – there were several vent points that released the gas onto the rig and into potentially confined spaces with presence of ignition sources. The design of the MGS allowed high pressure carbons to be diverted into the system even though it was outside the design specification and there were vent points onto the rig. The fire and gas systems The fire and gas system did not prevent hydrocarbon ignition. Hydrocarbons migrated beyond areas on Deepwater Horizon that were electrically classified to areas where the potential to ignition was higher. The heating, ventilation and air conditioning (HVAC) system transfer a gas-rich mixture into the engine rooms, causing at least one engine to overspeed, creating a potential source of ignition. The BOP emergency mode There were three different routes to activate the BOP emergency mode. All of them were unsuccessful in sealing the well. The fire is likely to have damaged the cables which provide electronic communication to the pods - prevented the EDS from initiating the blind shear ram (BSR). Automatic Mode Function (AMF) – two independent control pods on the BOP should activate the BSR if certain conditions were met. Subsequent analysis of the control pods showed they were not functioning properly; one had a failed solenoid valve and the other had insufficient battery charge – this would have failed to complete the AMF sequence. Remotely operated vehicle intervention to initiate the auto-shear function, another emergency method of operating the BOP, also failed to seal the well. It is thought that this did activate the blind shear rams, however they failed to seal the well and hydrocarbons continued to flow. The blowout preventer, removed on September 4, had not reached a NASA facility in time for it to be part of the report. Report summary The BP investigation report concludes that no single action caused the incident – it was a culmination of a complex interaction of mechanical failures, human judgments, engineering design, operational implementation and team communication. They use the Reason’s familiar Swiss Cheese metaphor to illustrate the barriers that were breached (Fig. 3-1). How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 31 FIG. 3-1. Barriers bre eached and tthe relation of barriers to the critica cal factors (the source: s "Deep pwater Horizzon Accidentt Investigation Report" [[C-1]) . 3.2. R Report off the Hum man Relia ability Associate A es c Hu uman Relia ability Assoc ciates Ltd1 issued a re eport [COn Septtember 23, 2010 the company 4] on De eepwater Horizon H acc cident that concentratted on human factor aaspects. The report was issu ued 2 week ks after the e publicatioon of BP In nvestigation n Report. Itt was based d on the factual informatio on and anallyses provid ded in BP Investigatio I on Report [[C-1] (publiished on Sept. 8,, 2010). Hu uman Reliab bility Associiate's reporrt was inten nded to proovide a sum mmary of the BP iincident and a comme entary on th he causes frrom a huma an factors pperspective.. Where a appropriate e, the autho ors – Hubbaard and Emb brey – have given theirr own insights from a human factors perspective.. Insights prrovided in the t report are briefly described in terms of prote ective barriiers that faiiled, as pre esented in the BP Invesstigation Reeport [C-1] (Section 2.1]. Cemen nt slurry design d The rep port points out that focus f on prroduction pressures p att the expennse of safe ety is an insidiou us threat for all hazard dous operattions. The safety requirements foor the slurry y design, 1 Human n Reliability Associates Ltd providess human error analysis,, strategic ddevelopment,, incident investiga ation, projectt manageme ent, risk asse essment, pro ofessional de evelopment trraining, and research and deve elopment services. The company c is b based in Daltton, United Kingdom. K How to Improve Safety in Regulated Indu ustries om Each Other safety s in EU” What Could We Learn Fro Background Material, ENC CO FR-(12)-44 © ENCO Page 32 the risks associated with not meeting them should have been explicitly recognized and communicated between Halliburton and BP. It is not mentioned in the BP incident report, but the rig was 41 days over schedule. Each day over schedule cost the company approx $500,000. The authors indicate these pressures as important factor that impacted upon the incident process. It needs to be investigated how these pressures translated into the decisions at different levels of the organization and between BP and Halliburton. Cement placement The equipment supplied (casing string) came with 7 centralizers. Halliburton had identified on the placement model that 21 centralizers would be needed, and sent a further 15 centralizers over to Deepwater Horizon. The BP Macondo team thought they had been sent the wrong centralizers and did not use them. The BP report includes statement that the reduced number of centralizers probably did not contribute directly to the accident. However, Hubbard and Embrey, in their report [C-4], draw attention to two potential issues here – the management of people’s understanding and knowledge, when design and operational parameters change, and poor communication between team members leading to different understandings, perception of risk, and possibly different goals. Confirmation of placement It is not clear why the well team did not follow the guidance in BP’s Engineering Technical Practice (ETP) – they did discuss the situation and developed decision trees to decide that no further evaluation was required. This suggests that they did not have clear guidance regarding the appropriate strategies for different conditions. Possible reasons for not following the BP ETP include: - it was viewed as guidance only, it was difficult to use, it was thought not to be relevant to these circumstances, it did not clearly state the conditions in which it was/not to be applied. Negative-pressure test The rig crew were familiar with a different procedure for the negative pressure test. Hubbard and Embrey [C-4] point out that for complex operations and those carried out infrequently the procedures should be more detailed to compensate for unfamiliarity. It is noted that in Deepwater Horizon case there was a high reliance on leadership and know-how of the crew. However, the procedures that were available were guidelines only and did not provide enough detail. For instance, they did not specify bleed volumes or give success/failure criteria. The information that was available may have been difficult to interpret and this was exacerbated by the crew’s unfamiliarity with the procedure and its lack of detail. There appears to have been a failure to explore other possibilities that would explain why flow did not exit the kill line and a reliance on the explanation of ‘Bladder effect’ without How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 33 considering whether there were other scenarios or risks. Poor decision making is often linked to ‘fuzzy’ symptoms, inadequate information provision, and poor feedback of the consequences when a course of action is taken. This may be due to a combination of other factors that are not explored in the report. Common problems are: time pressure and the pressure to achieve production goals (their immediate goal was to successfully proceed with the temporary abandonment of the well), ambiguity of roles and responsibilities, and possibly poor communications between team members. Failure to timely recognize influx of hydrocarbons The well should have been monitored continuously – however, procedures did not specify how this should be achieved during activities such as in-flow testing, cleaning or other endof-well activities Report of the Human Reliability Associates points out that in control rooms, operations are sometimes assumed to be continuously monitored. However, this is an assumption sometimes used in the design of plant and subsequent risk assessments without proper consideration of its practicality in the production environment. It appears that as the crew were busy with other activities, monitoring drill pipe pressure may not have taken priority and there was nothing to alert them to the unanticipated drill pipe pressure. Again, drill pipe pressure was not indicative of a known problem, and the crew had difficulty assessing the situation and understanding its significance. Appropriate training and job aids would have increased both the speed and accuracy of identification that there was an influx of hydrocarbons and enhanced the probability of appropriate well control actions. Failure of well control response Authors note that it is not clear why the decision to divert flow through the MGS was taken. In their opinion it indicates lack of situational awareness of the suitability of the MGS for large volumes of hydrocarbons and of the risks involved. It may have been motivated by good, but misguided intentions, for instance reducing the impact on pollution of dumping mud overboard with high hydrocarbon content. It is noted that speed of response was crucial. Diverting the flow overboard would have given the crew more time to respond. The BP investigation report [C-1] concludes that Transocean’s protocols did not fully address responding to high flow emergency situations after well control is lost. Their actions suggest they were not adequately prepared to manage an escalating well control situation. The crew had very little time to respond to the influx of hydrocarbons in a rapidly escalating situation. Key members should have been trained and competent. However, the BP investigation report does not give details of the emergency training for the crew. Failure of the Fire and Gas system The high pressure hydrocarbon was diverted through the MGS which was designed for low pressure only – there were several vent points that released the gas onto the rig and into potentially confined spaces. The design of the MGS allowed high pressure carbons to be diverted into the system even though it was outside the design specification and there How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 34 were vent points onto the rig. This indicates that inadvertent operation by operator was not considered in the HAZOP studies of the MGS. Failure of the BOP emergency modes Two independent control pods on the BOP should activate the Blind Sheer Ram if certain emergency conditions were met. Subsequent analysis of the control pods showed they were not functioning properly; one had a failed solenoid valve and the other had insufficient battery charge. This would have failed to complete the Automatic Mode Function sequence. This indicates poor maintenance management system for the pods, possibly linked to a lack of identification of critical components. Report summary The recommendations in the BP report focus on areas very familiar to human factors specialists such as procedure development, training, and proactive risk assessment. Specifically they include; improvements to procedures, competence assurance, Process Safety Performance Management (PSPM), which also extends to monitoring the contractors’ PSPM systems, well control practices, rig process safety, and lastly BOP engineering design and assurance. Similar recommendations have emerged from the analysis of the causes of many high profile medical incidents. While the report answers questions to a certain level, as a human factors specialist the authors would like to know more, particularly about the latent conditions that were prevalent before the incident. After a quick read through these there are burning questions that the BP report leaves unanswered: - - Why were procedures not used – is this typical? What was the effect on decision making and on practice of the pressure to get the well tested and capped? Is there a safety management system in place that includes slurry design? Why was the slurry design not subject to a HAZOP? Why were the changes to centralizers not part of a process that manages the changed specification – if so, why were there communication breakdowns between Halliburton and BP? Why did the crew use the mud gas separator rather than pipework that would have discharged the mud more quickly? What emergency training did the team have? Did they have training or job support to help them identify and respond to escalating situations? How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 35 3.3. Findings of the Oil Spill Commission President Barack Obama established the National Commission on the BP Deepwater Horizon Oil Spill and Offshore Drilling through Executive Order 13543 on May 21, 2010. The Commission examined the relevant facts and circumstances concerning the root causes of the Deepwater Horizon explosion and developed options to guard against, and mitigate the impact of, any oil spills associated with offshore drilling in the future. This included recommending improvements to federal laws, regulations, and industry practices. The Commission’s aim has been to provide the President, policymakers, industry, and the American people a clear, accessible, accurate, and fair account of the largest oil spill in U.S history: the context for the well itself, how the explosion and spill happened, and how industry and government scrambled to respond to an unprecedented emergency. Report to the President On January 11th, the National Oil Spill Commission released its final report to the President, "Deep Water: The Gulf Oil Disaster and the Future of Offshore Drilling" [C-4], which included a chapter on the well blowout and rig explosion. The main conclusions from this report are summarized below. The most significant failure at Macondo – and the clear root cause of the blowout – was a failure of industry management. Most of the failures at Macondo can be traced back to underlying failures of management and communication. Better management of decisionmaking processes within BP and other companies, better communication within and between BP and its contractors, and effective training of key engineering and rig personnel would have prevented the Macondo incident. BP’s management process did not adequately identify or address risks created by late changes to well design and procedures. BP did not have adequate controls in place to ensure that key decisions in the months leading up to the blowout were safe or sound from an engineering perspective. While initial well design decisions undergo a serious peer review process and changes to well design are subsequently subject to a management of change (MOC) process, changes to drilling procedures in the weeks and days before implementation are typically not subject to any such peer-review or MOC process. At Macondo, such decisions appear to have been made by the BP Macondo team in ad hoc fashion without any formal risk analysis or internal expert review. This appears to have been a key causal factor of the blowout. Halliburton and BP’s management processes did not ensure that cement was adequately tested. Halliburton had insufficient controls in place to ensure that laboratory testing was performed in a timely fashion or that test results were vetted rigorously in-house or with the client. In fact, it appears that Halliburton did not even have testing results in its possession showing the Macondo slurry was stable until after the job had been pumped. BP, Transocean, and Halliburton failed to communicate adequately. Information appears to have been excessively compartmentalized at Macondo as a result of poor communication. BP did not share important information with its contractors, or sometimes internally even with members of its own team. Contractors did not share important information with BP or each other. As a result, individuals often found How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 36 themselves making critical decisions without a full appreciation for the context in which they were being made. Transocean failed to adequately communicate lessons from an earlier near-miss to its crew. Transocean failed to adequately communicate to its crew lessons learned from an eerily similar near-miss on one of its rigs in the North Sea four months prior to the Macondo blowout. On December 23, 2009, gas entered the riser on that rig while the crew was displacing a well with seawater during a completion operation. Had the rig crew been adequately informed of the prior event and trained on its lessons, events at Macondo may have unfolded very differently. Decisionmaking processes at Macondo did not adequately ensure that personnel fully considered the risks created by time- and money-saving decisions. Many of the decisions that BP, Halliburton, and Transocean made that increased the risk of the Macondo blowout clearly saved those companies significant time (and money). The problem is that, at least in regard to BP’s Macondo team, there appears to have been no formal system for ensuring that alternative procedures were in fact equally safe. None of BP’s (or the other companies’) decisions in Table 3-1 appear to have been subject to a comprehensive and systematic risk-analysis, peer-review, or management of change process. Government also failed to provide the oversight necessary to prevent these lapses in judgment and management by private industry. Minerals Management Service (MMS) regulations were inadequate to address the risks of deepwater drilling. Many critical aspects of drilling operations were left to industry to decide without agency review. For instance, there was no requirement, let alone protocol, for a negative-pressure test, the misreading of which was a major contributor to the Macondo blowout. Nor were there detailed requirements related to the testing of the cement essential for well stability. Responsibilities for these shortfalls are best not assigned to MMS alone. Efforts to expand regulatory oversight, tighten safety requirements, and provide funding to equip regulators with the resources, personnel, and training needed to be effective were either overtly resisted or not supported by industry, members of Congress, and several administrations. As a result, neither the regulations nor the regulators were asking the tough questions or requiring the demonstration of preparedness that could have avoided the Macondo disaster. But even if MMS had the resources and political support needed to promulgate the kinds of regulations necessary to reduce risk, it would still have lacked personnel with the kinds of expertise and training needed to enforce those regulations effectively. Table 3-1. Examples of decisions that increased risk while potentially saving time. Was Decision Was there a less risky alternative available ? Less time than alternative ? Decision maker Not waiting for more centralizers of preferred design Yes Saved Time BP on shore Not waiting for foam stability test results and/or redesigning slurry Yes Saved Time Halliburton (and perhaps BP) on shore How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 37 Decision Was there a less risky alternative available ? Less time than alternative ? Decision maker Not running cement evaluation log Yes Saved Time BP on shore Using spacer made from combined lost circulation materials to avoid disposal issues Yes Saved Time BP on shore Displacing mud from riser before setting surface cement plug Yes Unclear BP on shore Setting surface cement plug 3,000 feet below mud line in seawater Yes Unclear BP on shore (Approved by MMS) Not installing additional physical barriers during temporary abandonment procedure Yes Saved Time BP on shore Not performing further well integrity diagnostics in light of troubling and unexplained negative pressure test results Yes Saved Time BP (and perhaps Transocean) on rig Bypassing pits and conducting other simultaneous operations during displacement Yes Saved Time Transocean (and perhaps BP) on rig Chief Counsel’s investigation report In addition to the final report to the President [C-4], the Oil Spill Commission has released additional report on the Chief Counsel’s investigation, which provides details of the series of engineering and management mistakes by those responsible for the drilling operations, including BP, Halliburton, and Transocean [C-8]. This additional report was intended to provide the public, policymakers, and industry with the fullest possible account of the investigation into the causes of the well blowout, which was summarized in the Commission’s report. The Chief Counsel’s investigative team uncovered and analyzed far more information than could have been included in the Commission’s report. The report provided comprehensive, coherent, and detailed account of the events leading up to the blowout and explosion. It shows the confusion, lack of communication, disorganization, and inattention to crucial safety issues and test results that led to the accident. It is noted in the report that this was an entirely preventable disaster and that the real cause were poor decisions by management. Among the details presented publicly for the first time in the Chief Counsel’s report are these: BP was aware of problems with Halliburton personnel and work product years before the blowout. In 2007, a consulting firm issued a quality control report warning BP that Halliburton’s lab technicians “do not have a lot of experience evaluating data” and that BP needed to improve communication with Halliburton “to avoid unnecessary delays or errors in the slurry design testing.” BP’s own cementing expert described the “typical Halliburton profile” as “operationally competent and just good enough technically to get by.” And BP’s engineers had been forced to “work around” the Halliburton engineer assigned to Macondo for years – they said that he was “not cutting it” and that he often waited too long to conduct critical tests. But they neither How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 38 reviewed his work at Macondo carefully, nor even checked to see that he conducted testing in a timely manner – even though they knew that their last minute changes to the cement design test could cause problems and that using nitrogen foamed cement could pose “significant stability challenges.” Although testing of the blowout preventer may ultimately reveal flaws in that equipment, BOP failures were not the root cause of the blowout. The rig crew activated the BOP, at best, only moments before the blowout began. By then, hydrocarbons had already gone past the BOP into the riser and were expanding rapidly towards the rig floor. Even if the BOP had functioned flawlessly, the rig would have exploded. A BP engineering reorganization in early 2010 resulted in delays and distractions for the team drilling the Macondo well. The reorganization appears to have had an impact on decision-making in the weeks leading up to the blowout, the time during which virtually all of the decisions identified by the Chief Counsel’s team as increasing the risk of a blowout were made. BP’s own well site leaders accepted facially implausible explanations for the negative test results. Less than a week after blowout, one of the two BP company men who had been on the Deepwater Horizon during the crucial test told senior engineers “I believe there is a bladder effect,” and that this effect – not failed cement – was the source of the problematic test results. Every industry expert the investigative team met with dismissed the so-called bladder effect as a fiction that could not have accounted for the pressure readings the men saw on April 20. If anyone had consulted the BP’s vice president for drilling (who was physically present on the rig during the crucial test) or any other shore-based engineer, the blowout might never have happened. Physical evidence taken from the well shows that hydrocarbon flow almost certainly came to the surface through the “shoe track” of the well and up the production casing. Cement in the shoe track should have blocked this flow, which further calls into question the quality of the cement job. Although BP engineers recognized that the Macondo cement job would be a difficult one, and that Halliburton’s engineer was not doing “quality work,” they did not fully review his cement design. BP’s Macondo team asked an internal cement specialist to provide technical support on an “ad hoc” basis, but he left the country without carefully reviewing the cement design, and never saw any information about the cement slurry design or lab testing results until six days after the blowout. When he reviewed those materials, several aspects of Halliburton’s cement design surprised him. The Transocean crew missed several signs of a “kick” – that is, hydrocarbons in the riser – on the night of a blowout. At 9:27 pm, less than 15 minutes before the blowout began, they did notice an anomaly in pressure data from the well, and shut down operations to investigate. They noticed several anomalies that should have caused serious concern, but showed no hint of alarm. BP’s well design decisions complicated efforts to cap the well. BP was forced to be especially cautious in its capping efforts because it believed that capping the well at the top could cause oil to burst through the sides of the well and flow up through the rocks to the sea floor. BP increased the risks of such problems by installing pressure relief “burst disks” in the well and by choosing not to install a “protective casing” at Macondo. How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 39 Once the Chief Counsel’s team identified serious concerns with Halliburton’s cement slurry design and testing process, Halliburton declined to cooperate with the investigation effort. Halliburton refused to allow the team to conduct further interviews of its cementing engineer and lab personnel. Halliburton has not provided scientific data to support some of its technical assertions, and declined to provide documents regarding lab testing protocols and evaluation criteria. Halliburton also has not used or made available its proprietary cement modeling software to back up its assertions that the Macondo well failed because BP did not use enough centralizers. The Chief Counsel’s team believes that it is reasonable to infer that Halliburton would have provided these materials if they had been favorable to Halliburton. The Chief Counsel’s report settles the confusion over what type of centralizers BP shipped to the rig. BP shipped additional centralizers to the rig to run on the final casing string, but then decided not to use them. Until now, there has been no clear account of what type of centralizers BP shipped to the rig and why they were not used. The Chief Counsel’s report identifies the type of centralizers that were delivered – and includes an actual photograph of them taken by a BP engineer. It also explains why BP’s Macondo team thought they were the wrong type. BP’s on-duty Well Site Leader was not present during preparations for the critical negative pressure test, and may not have been present during the beginning of the negative pressure test itself. Industry experts say that Well Site Leaders should be present on the rig floor during this crucial period. On the Deepwater Horizon rig, fundamental mistakes were made during the negative pressure test, beginning with the test set-up. The misinterpretation of test results was a major factor contributing to the blowout. BP’s penultimate version of its temporary abandonment procedures included not one but two negative pressure tests. BP dropped one of these tests in its final version. According to one expert, this second test would have been less likely to have been misinterpreted by Well Site Leaders and the rig crew. At the very least, it would have given the Deepwater Horizon another opportunity to realize that the cement job had failed. BP and the Macondo team were aware of ways to carry out its temporary abandonment procedure that could have reduced risk. BP decided to set a lockdown sleeve during temporary abandonment operations (rather than later in the well project) to save time (5.5 days) and cost ($2 million). Its engineers also believed that they should set a backup cement plug and a lockdown sleeve as the last steps in the temporary abandonment sequence. Because of these decisions, BP instructed the rig crew to displace over 3000 feet of heavy drilling mud from the well with seawater – severely underbalancing the well – before setting additional backup barriers to hydrocarbon flow. The Macondo team knew this was unnecessary, and that they could use alternative procedures to avoid underbalancing the well before setting additional barriers. They even included such procedures in their plans at various points. But they ultimately rejected those options in favor of an approach that created significant and unnecessary risks. How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 40 3.4. Report of NAE/NRC Committee In response to a request from Department of Interior (DOI) Secretary, NAE and NRC formed Committee to examine the causes of the Deepwater Horizon – Macondo well blowout, explosion, fire, and oil spill and to identify measures for preventing similar incidents in the future. As part of this task, the Committee provided an interim report to the DOI Secretary on November 16, 2010 [C-2]. That report presented preliminary findings and observations concerning key factors and decisions that may have contributed to the blowout of the Macondo well, including engineering, testing and certification. The final report [C-8] presents the Committee's overall findings with regard to causes of the accident and its recommended approaches for improved safety. Interim Report In its interim report the Committee [C-2] pointed out several factors that could have had a material impact on the accident. They are briefly highlighted below. It is noted that the failures and missed indications of hazard were not isolated events during the preparation of the Macondo well for temporary abandonment. Numerous decisions to proceed toward abandonment despite indications of hazard suggest an insufficient consideration of risk and a lack of operating discipline. The decisions also raise questions about the adequacy of operating knowledge on the part of key personnel. Changing key supervisory personnel on the Deepwater Horizon MODU just prior to critical temporary abandonment procedures must have been one of the contributing factors. The Committee noted that the design decision of choosing to use a long-string production casing in a deep, high-pressure well with multiple hydrocarbon zones was inappropriate. Preferable solution would be the use of a cement liner over the uncased section of the well. Deciding that only six centralizers would be used to maintain an adequate annulus for cementing between the casing and the formation rock, even though modeling results suggested that many more centralizers would have been needed was not appropriate. Questionable was also attempting to cement the multiple hydrocarbons and brine zones encountered in the deepest part of the well in a single operational step, despite the fact that these zones had markedly different fluid pressures. Due to this fact, there was only a small difference between the cement density needed to prevent inflow into the well from the high-pressure formations and the cement density at which an undesirable hydraulic fracture might be created in a low pressure zone. Limiting bottoms-up circulation of drilling mud prior to cementing, which increased the possibility of cement contamination by debris in the well, was noted by the personnel but not properly responded. Not running a bond log after cementing to assess cement integrity in the well, despite the anomalous results of repeated negative-pressure tests was an important contributor to the accident. Currently, there are conflicting views among experts familiar with the incident regarding the type and volume of cement used to prepare the well for abandonment. There are also conflicting views on the adequacy of the time provided for the cement to cure. These factors could have had a material impact on the integrity of the well. How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 41 Given the large quantity of gas released onto the MODU and the limited wind conditions, ignition was most likely. Therefore, operation of various alarms and safety systems on the Deepwater Horizon MODU was an important factor potentially affecting the time available for personnel to evacuate. It seems that they failed to operate as intended. The various failures mentioned above indicate the lack of a suitable approach for anticipating and managing the inherent risks, uncertainties, and dangers associated with deepwater drilling operations and a failure to learn from previous near misses. Of particular concern is an apparent lack of a systems approach that would integrate the multiplicity of factors potentially affecting the safety of the well, monitor the overall margins of safety, and assess the various decisions from perspectives of well integrity and safety. The “safety case” strategy required for drilling operations in the North Sea and elsewhere is one example of such a systems approach. Final Report In the Final Report the Committee assessed that the following findings of facts have been established by the available evidence: The flow of hydrocarbons that led to the blowout of the Macondo well began when drilling mud was displaced by seawater during the temporary abandoning process. The decision to proceed to displacement of the drilling mud by seawater was made despite a failure to demonstrate the integrity of the cement job even after multiple negative pressure tests. This was but one of a series of questionable decisions in the days preceding the blowout that had the effect of reducing the margins of safety and that evidenced a lack of safety-driven decision making The reservoir formation, encompassing multiple zones of varying pore pressures and fracture gradients, posed significant challenges to isolation using casing and cement. The approach chosen for well completion failed to provide adequate margin for safety and led to multiple potential failure mechanisms. The loss of well control was not noted until more than 50 minutes after hydrocarbons flow from the formation started, and attempts to regain control by using the BOP were unsucessful. The blind shear ram failed to sever the drill pipe and seal the well properly, and the emergency disconnect system failed to separate the lower marine riser and the Deepwater Horizon from the well. The BOP system was neither designed nor tested for the dynamic conditions that most likely existed at the time that attempts were made to recapture the well control. Furthermore, the design, test, operation, and maintenance of the BOP system were not consistent with a high reliability, fail-safe device. Once well control was lost, the large quantities of gaseous hydrocarbons released onto Deepwater Horizon, exacerbated by low wind velocity and questionable venting selection, made ignition all but inevitable. The actions, policies and procedures of the corporations involved did not provide an effective system safety approach commensurate with the risk of the Macondo well. The lack of a strong safety culture resulting from a deficient overall system approach to safety is evident in the multiple flawed decisions that lead to the blowout. Industrial management involved with the Macondo well Deepwater Horizon accident failed to appreciate or plan for the safety challenges presented by the Macondo well. How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 42 During the course of its investigations, the Committee made several observations with regard to the process and procedures used by industry and government regulators. - While the geologic conditions encountered in the Macondo well posed challenges to the drilling team, alternative completion techniques and operational processes were available that could have been used to prepare the well safely for temporary abandonment. - The ability of the oil and gas industry to perform and maintain an integrated assessment of the margins of safety for a complex well like Macondo is impacted by the complex structure of the offshore oil and gas industry and the divisions of technical expertise among the many contractors engaged in the drilling. - The regulatory regime was ineffective in addressing the risks of the Macondo well. The actions of the regulators did not display an awareness of the risks or very narrow margins for safety. - The extent of training of key personnel and decision makers both in industry and in regulatory agencies has been inconsistent with the complexities and risks of deepwater drilling. - Neither the companies involved nor the regulatory community has made effective use of real time data analysis, information on precursor incidents or near-misses, or lessons learned in the Gulf of Mexico and worldwide to adjust practices and standards appropriately. - Industry's and government's research and development efforts have been focused disproportionally on exploration, drilling, and production technologies as opposed to safety. 3.5. Observations from other sources The Macondo well accident was subject to high interest to the oil drilling industry, the US governmental organizations, the public, individual experts in the field and media. This report is based mostly on the investigation reports described above (Sections 3.1 – 3.4). Opinions related to possible causes and discussions of circumstances could also be found in media and internet forums/ web site pages (e.g. [C-9] – [C-12]). This information was used in drafting this report with caution. However, in many cases it was found to be useful providing new insights and viewpoints that were free of certain biases not necessarily avoided in some of the official materials. How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 43 4. Analysis of the Deepwater Horizon accident This section of the report summarizes the results of causal analysis presented in the available material discussed in Section 3. The results are presented in the form of Cause Map (CM). It displays the whole structure of causes in a graphical form. This form of presentation is believed to facilitate effective communication and documentation of causes of the problem (accident). It is worth noting that communication of findings to experts from different industries and of different professions is an important aspect in this project. The CM for the Deepwater Horizon accident was developed and presented in MS Excel using the worksheet / template prepared by "ThinkReliability" Consulting Company available at web site page http://www.thinkreliability.com. 4.1. Step 1 - Definition of the problem The first step of the Cause Mapping approach is to define the problem by asking the four questions: What is the problem? When did it happen? Where did it happen? And how did it impact the goals? Answers to these questions are provided in Table 4-1. The Deepwater Horizon accident had very severe consequences – safety-related, financial, and environmental. It had also considerable impact on the image of the companies involved and the whole oil industry in the USA. As a direct result of the events at the Deepwater Horizon oil rig 11 workers were killed and 16 injured. This is an impact to the worker safety goal. Financial consequences for the companies involved in the accident were enormous. These consequences are closely related with the environmental impact of the accident and also with the loss of property. Two years after the accident, BP found itself paying out tens of billions of dollars to contain a blowout at the Macondo well, mitigate the damage resulting from the millions of gallons of oil flowing from that well into the Gulf of Mexico, and compensate the hundreds of thousands of individuals and businesses harmed by the spill. BP and its partners (Anadarko and MOEX), and its key contractors (particularly Halliburton and Transocean) face potential liability for the billions more necessary to restore natural resources harmed by the spill [C-4]. Table 4-1. Definition of the problem What Problem(s) Deepwater Horizon oil rig explosion and oil spill When Date April 20, 2010 Time 21:49 Different, unusual, unique Deepwater drilling State, city Gulf of Mexico, Louisiana, United States Where How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 44 28°44′12.01″ N 88°23′13.78″ W Facility, site Macondo well Unit, area, equipment Deepwater Horizon oil rig Task being performed Process of temporary abandoning the well Impact to the Goals Safety 11 fatalities, 16 injured Public Safety Extensive damage to marine and wildlife habitats and to the Gulf's fishing and tourism Environmental Significant release of oil, offshore pollution Production-Schedule Drilling operation in the area suspended Property, Equip, Mtls Complete loss of the rig (appr. cost $700 mln) Labor, Time Massive efforts to terminate the oil spill Frequency Very rare 4.2. Step 2 – Analysis of causes (Causal Map) Property goal was impacted because the oil rig was burned up and sunk. Safety goal was impacted because of the explosion and fire led to 11 fatalities and 16 persons injured. Environmental goal was impacted because the explosion and fire led to significant release of oil to the environment. Production goal was impacted because the drilling operations in the region were suspended for several months. Labor goal was impacted because the release of oil required significant efforts to terminate the spill. The oil rig was burned up and sunk because of the loss of well control and hydrocarbons blowout. Hydrocarbons were released onto the rig because the well integrity was not established during the temporary abandonment process. There were two physical barriers that have been designed to seal the well – the annulus cement barrier and cement plug in the shoe track. Both of these barriers failed to contain hydrocarbons within the geologic formation (reservoir). Influx of hydrocarbons from the formation to the well through the imperfect cement barriers was induced by the end-of-well activities – displacing the mud from the riser and replacing it with seawater. This made the well underbalanced because the mud is much heavier than seawater. Rig crew failed to disconnect the well using the blank shear ram (BSR) because the crew did not recognize gas influx in time. BOP emergency disconnect system also failed to terminate blowout. Flammable gases penetrated the engine area and ignited causing explosion and severe fire. How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 45 Integrity of annulus cement barrier Annulus cement barrier (see Cause Map - Page 2, Cause A) was ineffective in sealing the well because of three potential causes: (i) deficiencies of cement slurry design, (ii) deficiencies of cementing job, and (iii) problems with placing cement in the well. Cement slurry design was critical because of the pore pressure and fracture gradient – however the technical review of the slurry design gave heavy emphasis to preventing lost returns. If cementing procedure placed too much pressure on the geologic formation below, it might trigger another lost-returns event similar to the one on April 9. In this case, critical cement – not mud – might flow into the formation and be lost, potentially leaving the annular space at the bottom of the well open to hydrocarbon flow. BP chose to use “nitrogen foam cement” – a cement formula that has been leavened with tiny bubbles of nitrogen gas, injected into the cement slurry just before it goes down the well. This formula was chosen to lighten the resulting slurry from approximately 16.7 pounds per gallon (ppg) to 14.5 ppg – thereby reducing the pressure the cement would exert on the fragile formation. The bubbles, in theory, would also help to balance the pore pressure in the formation and clear the annular space of mud as the cement flowed upward. Lab tests carried out as part of the investigation suggest that the slurry was unstable at drilling depth pressures and temperatures and there was likely to be nitrogen breakout. The slurry was not fully tested before use. There were several cement slurry design features that could have led to foam instability and contributed to a failure of the cement barrier. These include: the extremely low cement slurry yield point, additive of a defoamer, and lack of fluid loss control additives [C-4]. Potential instability factors were also the possibility of cement slurry contamination because of no bottoms up circulation, relatively low rate of pumping cement, and small volume of cement [C-4]. BP’s plan was to limit the circulation of drilling mud through the wellbore before cementing. Optimally, mud in the wellbore would have been circulated “bottoms-up” – meaning the rig crew would have pumped enough mud down the wellbore to bring mud originally at the bottom of the well all the way back up to the rig. Such extensive circulation cleans the wellbore and reduces the likelihood of channeling (see Section 2.3 for additional explanations). And circulating bottoms-up allows technicians on the rig to examine mud from the bottom of the well for hydrocarbon content before cementing. But the BP engineers feared that the longer the rig crew circulated mud through the casing before cementing, the greater the risk of another lost-returns event. Accordingly, BP circulated approximately 350 barrels of mud before cementing, rather than the 2,760 barrels needed to do a full bottoms-up circulation [C-4]. BP decided to pump cement down the well at the relatively low rate of 4 barrels or less per minute. Higher flow rates tend to increase the efficiency with which cement displaces mud from the annular space. But the increased pump pressure required moving the cement quickly would mean more pressure on the formation (ECD) and an increased risk of lost returns. BP decided to reduce the risk of lost returns in exchange for a less-than-optimal rate of cement flow. BP made another compromise by limiting the volume of cement that would be pumped down the well. Pumping more cement is a standard industry practice to insure against How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 46 uncertain cementing conditions: more cement means less risk of contamination and less risk that the cement job will be compromised by slight errors in placement. But more cement at Macondo would mean a higher cement column in the annulus, which in turn would exert more pressure on the fragile formation below. Why? Effect Possible Solutions: Cause Cause Evidence: Start with the Goals (in red) that have been impacted. Read the map to the right by asking Why questions. Step 2. Cause Map - Page 1 Annulus cement barrier not effective Well integrity not established or failed A AND Shue track barrier not effective B AND Labor Goal Impacted Massive efforts to stop oil spill Environmental Goal Impacted Production Goal Impacted Well underbalanced during the end-of-well activities Drilling operations in area shutdown Hydrocarbons influx onto the rig Rig crew did not disconect the well using BSR AND C Crew failed to recognize gas influx in time D AND Significant release of oil from the well Explosion of hydrocarbons and severe fire Displacing mud from riser before setting plug AND Oil rig burned up and sunk BOP emergency modes failed to seal the well E Property Goal Impacted Gas leaked to the engine area and ignited Safety Goal Impacted E F 11 fatalities, 16 injured Accordingly, BP determined that the annular cement column should extend only 500 feet above the uppermost hydrocarbon-bearing zone (and 800 feet above the main hydrocarbon zones), and that this would be sufficient to fulfill MMS regulations of “500 feet above the uppermost hydrocarbon-bearing zone". However, it did not satisfy BP’s own internal guidelines, which specify that the top of the annular cement should be 1,000 feet above the uppermost hydrocarbon zone. The integrity of cement barriers was also affected by the design of the cement job. There were two important factors that increased potential for channeling: the use of long string casing and a limited number of centralizers (see Section 2.3). How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 47 The 18,300 ft long 400-ton casing string had a 5,800 ft long lower portion with 7-inch diameter. Most of the hole over this portion of casing was 9.875-inch diameter. However, the lowest 180 ft of 7-inch casing with 4 equi-spaced centralizers was squeezed into an 8.5-inch hole with only 56 ft of rathole bottom clearance. Compressed sediment and granular infill in the 0.75-inch wide annulus (Halliburton’s best practices document recommends 1.5 to 2-inch annular gap tolerance) most probably explains the need for much-higher-than-normal pressure of 3142 psi to liquefy it (at the ninth attempt) and allow mud to circulate. The unexpected high pressure and subsequent lower-than-specified mud flow led to problems with conversion of float collar (as discussed in the context of the integrity of shoe track barrier). 17 Questionable stability of nitrified foam Step 2. Cause Map - Page 2 AND/OR Small volume of cement AND 19 Possible contamination by mud/debris Weaknesses of cement slurry design Potential instability of foam cement AND/OR AND A Weaknesses of cement placing TOC less than required in BP ETP AND Reducing risk of lost returns (lower ECD) AND 18 No fluid loss additive Annulus cement barrier not effective No bottoms up circulation Relatively low rate of pumping cement AND/OR Addition of defoamer AND/OR No proven cement evaluation (log) Low yield point AND Placement difficult due to narrow gap Weaknesses of cement job design Potential for channelling Use of long string More convenient system over the life of the well Rig crew do not wait for devices of preferable type Production pressure / delay of the project AND 1 Limited number of centralizers Centralizers are critical components in ensuring a good cement job. The evidence to date does not unequivocally establish whether the failure to use 15 additional centralizers was a direct cause of the blowout. But the process by which BP arrived at the decision to use only six centralizers at Macondo illuminates the flaws in BP’s management and design procedures, as well as poor communication between BP and Halliburton [C-4]. It does not appear that BP’s team tried to determine before April 15 whether additional centralizers would be needed. Had BP examined the issue earlier, it might have been able to secure additional centralizers of the design it favored. Nor does it appear that BP based its decision on a full examination of all potential risks involved. Instead, the decision How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 48 appears to have been driven by an aversion to one particular risk: that slip-on centralizers would hang up on other equipment. BP did not inform Halliburton of the number of centralizers it eventually used, let alone request new modeling to predict the impact of using only six centralizers. Halliburton happened to find out that BP had run only six centralizers when one of its cement engineers overheard a discussion on the rig [C-4]. It needs to be noted that the decisions on the use of long casing string, limited number of centralizers, and Top Of Cement (TOC) lower than in BP's Engineering Technical Practice, which had potential impact on the integrity of cement annular barrier, were convenient from the production point of view or intended to save time and money. The BP team erred by focusing on full returns as the sole criterion for deciding whether to run a cement evaluation log. The BP Macondo team used final lift pressure and returns to confirm successful cement placement and decided no further evaluation was needed. However, this was not in line with procedures which state that more rigorous evaluation is required in some circumstances [C-4]. Cement evaluation logs plainly have their limitations, particularly at Macondo. But while many companies do not run cement evaluation logs until the completion phase, BP should have run one here – or sought other equivalent indications of cement quality in light of the many issues surrounding and leading up to the cement job [C-4]. Integrity of shoe track barrier Potential causes that led to a failure of the shoe track barrier (see Cause Map – Page 3, cause B) include two items: inadequate quality of shoe track cement and failure of flapper valves to seal [C-1]. Inadequate quality of shoe track cement barrier could have been caused by the contamination of shoe track cement due to nitrogen breakout (from the foam cement used for the annular space), contamination of shoe track cement by mud in the wellbore, inadequate design of shoe track cement (tail cement), and swapping of the shoe track cement by mud in the rathole (bottom of the well). Contamination of the shoe track cement by mud was more likely because of the oil-based spacer used by the crew. While drilling crews routinely use water-based spacer fluids to separate oil-based drilling mud from seawater, the spacer BP chose to use during the negative pressure test was a mixture of two different lost-circulation materials left over on the rig – the heavy, viscous drilling fluids used to patch fractures in the formation when the crew experiences lost returns. BP wanted to use these materials as spacer in order to avoid having to dispose of them onshore as hazardous waste1. Material of this type had never previously been used by anyone on the rig or by BP as a spacer, nor been thoroughly tested for that purpose. Two flapper valves, which create additional element of the shoe track barrier, could have failed because of three possible mechanisms: failure to convert the flow collar, damage due to high load needed to establish circulation (see Section 2.3 for discussion of pressure 1 Pursuant to the Resource and Conservation Recovery Act, exploiting an exception that allows companies to dump waterbased “drilling fluids” overboard if they have been circulated down through a well How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 49 anomalies during the preparation of the well for cementing job), and random failure of the two flapper valves. Whether the float valves converted contributing to the blowout, has not yet been, and may never be, established with certainty. But, what is certain is that BP’s team failed to take time to consider whether and to what extent the anomalous pressure readings may have indicated other problems or increased the risk of the upcoming cement job. BP’s team appears not to have seriously examined why it had to apply over four times the 750 psi design pressure to convert the float valves. More importantly, the team assumed that the sharp drop from 3,142 psi meant the float valves had in fact converted. That was not at all certain. The auto-fill tube was designed to convert in response to flow-induced pressure. Without the required rate of flow, an increase in static pressure, no matter how great, would not dislodge the tube. Step 2. Cause Map - Page 3 Contamination of shoe track cement by nitrogen Need to use havier fluid to improve displacement AND/OR 20 Contamination of shoe track cement by mud Inadequate quality of shoe track cement B Use of oil-based spacer AND/OR Disposing lostcirculation material Inadequate design of shoe track cement Shoe track barrier not effectikve AND AND/OR Swapping of shoe track cement with the mud 18 Flow collar not converted Low rate of cement down the well AND/OR Flapper valves do not seal Damage due to high load required to establish circulation AND/OR Random failure of flapper valves While BP’s Macondo team focused on the peak pressure reading that circulation was reestablished, it does not appear the team sufficient mud flow rate had been achieved to convert the float considered this issue. Because of ECD concerns, BP’s engineers How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 of 3,142 psi and the fact ever considered whether valves. They should have had specified a very low © ENCO Page 50 circulating pump rate – lower than the flow rate necessary to convert the float valves. BP does not appear to have accounted for this fact. High load applied to establish circulation could have damage the flapper valves and resulted in their failure to prevent blowout. It is also possible that the failure of flapper valves to seal was a random failure, although likelihood of coincident failures of two valves seems to be low. Displacement of mud from the riser Decision regarding displacement of mud from the riser before setting cement plug (see Cause Map – Page 4, Cause C) was an important factor that have contributed to the blowout. First, it was not necessary or advisable for BP to replace 3,300 feet of mud below the mud line with seawater. By replacing that much heavy drilling mud with much lighter seawater, BP placed more stress on the cement job at the bottom of the well than necessary. BP’s stated reason for doing so was its preference for setting cement plugs in seawater rather than mud. Step 2. Cause Map - Page 4 BP team preference for setting plug in seawater C Displacing mud from riser before setting plug Cement setting in seawater better than in mud Contamination of cement by mud avoided Plug solution consistent with setting lockout sleeve 1 Less risky alternatives not considered The risk of displacing mud not fully realized Focus on production as opposed to safety 4 Lessons from past events not communicated to the rig crew 2 3 No formal system for risk assessment Safety culture at the company level inadequate While industry experts have acknowledged that setting cement plugs in seawater can avoid mud contamination and that it is not unusual for operators to set cement plugs in seawater, BP has provided no evidence that it or another operator has ever set a surface cement plug so deep in seawater (particularly without additional barriers). The risks BP created by its decision to displace 3,300 feet of mud with seawater outweighed its concerns about cement setting better in seawater than in mud. As BP has admitted, cement plugs can be set in mud. BP also could have set one or more non-cement bridge plugs (which work equally well in mud or seawater). No evidence has yet been produced that the BP team ever formally evaluated these options or the relative risks created by removing 3,300 feet of mud [C-4]. How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 51 It is noted in Ref [C-4] that setting the cement plug 3,300 feet below the mud line was not necessary. The BP Macondo team chose to do so in order to set the lockdown sleeve last in the temporary abandonment sequence to minimize the chances of damage to the sleeve. Setting the lockdown sleeve would require 100,000 pounds of force. The BP Macondo team sought to generate that force by hanging 3,000 feet of drill pipe below the sleeve – hence the desire to set the cement plug 3,000 feet below the mud line. BP’s desire to set the lockdown sleeve last did not justify the risks its decision created. BP could have used other proven means to protect the lockdown sleeve if set earlier in the process. It also did not need 3,000 feet of space to generate 100,000 pounds of force. There were some recommendations of BP experts for setting the plug roughly 1,300 feet below the mud line (using heavier drill pipe), rather than 3,300 feet down. That would have significantly increased the margin of safety for the well. The most troubling aspect of BP’s temporary abandonment procedure was BP’s decision to displace mud from the riser before setting the surface cement plug or other barrier in the production casing. During displacement of the riser, the BOP would be open, leaving the cement at the bottom of the well (in the annulus and shoe track) as the only physical barrier to flow up the production casing between the pay zone and the rig. Relying so heavily on primary cement integrity put a significant emphasis on the negative-pressure test and well monitoring during displacement, both of which are subject to human error. BP’s decision under these circumstances to displace mud from the riser before setting another barrier unnecessarily and substantially increased the risk of a blowout. BP could have set the surface cement plug, or a mechanical plug, before displacing the riser. BP could have replaced the mud in the wellbore with heavier mud sufficient to overbalance the well. It is not apparent why BP chose not to do any of these things. Decision making processes at Macondo did not adequately ensure that personnel fully considered the risks created by time- and money-saving decisions. Whether purposeful or not, many of the decisions that BP, Halliburton, and Transocean made that increased the risk of the Macondo blowout clearly saved those companies significant time (and money). It is noted in Ref. [C-4] that choosing a less-costly or less-time-consuming alternative – as long as it is proven to be equally safe – is normal in commercial business. The problem is that, at least in regard to BP’s Macondo team, there appears to have been no formal system for ensuring that alternative procedures were in fact equally safe. None of BP’s (or the other companies’) decisions (shown in Table 3-1) appear to have been subject to a comprehensive and systematic risk-analysis, peer-review, or management of change process. Transocean failed to adequately communicate lessons from an earlier near-miss to its crew. Transocean failed to adequately communicate to its crew lessons learned from a similar near-miss on one of its rigs in the North Sea four months prior to the Macondo blowout. The basic facts of both incidents are the same. Had the rig crew been adequately informed of the prior event and trained on its lessons, events at Macondo may have developed very differently. The above mentioned deficiencies indicate significant weaknesses in safety culture not only within BP, but also within other corporations involved in the Macondo project. Kick detection Failure of the rig crew to recognize influx of hydrocarbons into the well (see Cause Map – Page 5, Cause D) was an important factor that have contributed to the Macondo accident. How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 52 The crew could have prevented the blowout – or at least significantly reduced its impact – if they had reacted in a timely and appropriate manner. What is not now clear is precisely why the drilling crew and other individuals on the rig missed several critical signs indicating that a kick was occurring. There are several potential causes that can explain such behaviour. The rig crew was confident regarding the integrity of the existing cement barriers. There was no systematic monitoring of the important parameters of the well that could help in detecting occurrence of a kick. Important factor was also that at the same time the crew was engaged in several end-of-well activities that could have distracted their attention. The crew was confident that the existing cement barriers are effective based on the negative pressure test, results of which were misinterpreted. The cement evaluation log that could have identified potential barrier integrity problems was not conducted. The crew did not recognised anomalies in the well parameters that could have provided an indication of a kick. How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 53 Cement evaluation log not conducted Safety culture at the company level inadequate No formal system for risk assessment 11 No detailed requirements for the log 10 AND 8 Crew confident of the well integrity AND Safety oversight not effective Negativepressure test mis-interpreted AND G AND Kick symptoms not recognized Crew failed to recognize gas influx in time Crew distracted with end-of-well activities Preparation for setting cement plug in the riser No monitoring of the well parameters AND 9 21 1 Displacement bypassing pits & flow out meter Production pressure due to project delays Saving time and money 16 Pressure anomalies not recognised 13 8 No suitable procedure on well monitoring Regulatory regime not effective in addressing the risk AND Department of the Interior was understaffed Inadequate scope of safety regulations No data on water inflow and mud outflow D 3 2 Step 2. Cause Map - Page 5 Rig crew training not sufficient 10 Department of the Interior was understaffed AND 22 Instrumentation and displays not adequate How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 54 Cement evaluation log was not conducted because the BP team was considering full returns as the sole criterion for deciding whether to run the evaluation log. Receiving full returns was a good indication that cement or other fluids had not been lost to the weakened formation. But full returns provided, at best, limited or no information about (i) the precise location where the cement had ended up, (ii) whether channelling had occurred; (iii) whether the cement had been contaminated; or (iv) whether the foam cement had remained stable. Although other indicators – such as on-time arrival of the cement plugs and observation of expected lift pressure – were reassuring, they too provided limited information. Other cement evaluation tools could have provided more direct information about cementing success. BP team decision of not conducting a cement evaluation log did not fully conform to the intent of its own guidelines ETP GP 10-60 [C-1]. These guidelines require that top of cement (TOC) barrier should be 1000 ft above any distinct permeable zone and centralization should extend to 100 ft above such zone. If these conditions are not met, as in this case, TOC should be determined by a "proven cement evaluation log", which would be done during the completion phase of the well. There is no evidence of a documented risk assessment regarding annulus barriers. It is not clear what is the regulator's position regarding this issue. There are several potential factors that may have contributed to the failure to properly conduct and interpret the negative pressure test that night. There was no standard procedure for running or interpreting the test in either MMS regulations or written industry protocols. The regulations and standards did not require BP to run a negative-pressure test at all. BP and Transocean had no internal procedures for running or interpreting negative-pressure tests and had not formally trained their personnel in how to do so. The crew engaged in conducting and interpreting the test were not fully aware of the associated risk. There were several factors that could have impact on the crew's appreciation of the risk. Although many BP and Halliburton employees were aware of the difficulty of the primary cement job those issues were for the most part not communicated to the rig crew that conducted the negative-pressure test and monitored the well. It appears that BP did not even communicate many of those issues to its own personnel on the rig. BP well site leaders did not consult anyone on shore about the anomalous data observed during the negative-pressure test. Had they done so, the Macondo blowout may not have happened. Due to poor communication, it does not appear that the staff performing and interpreting the test had a full appreciation of the context in which they were performing it. Such an appreciation might have increased their willingness to believe the well was flowing. The rig crew missed several signs of a “kick” – that is, hydrocarbons in the riser -- on the night of a blowout. The Sperry Sun data available to the crew from between 8:00 p.m. and 9:49 p.m. reveal a number of different signals that if observed, should at least have prompted the driller to investigate further, for instance, by conducting a visual flow check, and then shutting in the well if there were indications of flow. For instance, the increasing drill-pipe pressure after the pumps were shut down for the sheen test at 9:08 p.m. was a clear signal that something was happening in the well. Similarly, at roughly 9:30 p.m., the driller and toolpusher recognized an anomalous pressure difference between the drill pipe and kill line. Both of these signals should have prompted action – especially the latter: it was clearly recognized by the crew and coherent How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 55 with the odd pressure readings observed during the negative-pressure test. The crew should have done a flow check and shut in the well, immediately upon confirmation of flow. The crew missed or misinterpreted these signals. One possible reason is that they had done a number of things that confounded their ability to interpret signals from the well. For instance, after 9:08 p.m., the crew began sending fluids returning from the well overboard, bypassing the active pit system and the flow-out meter. Only the mudlogger performed a visual flow check. At 9:27 pm, less than 15 minutes before the blowout began, they did notice an anomaly in pressure data from the well, and shut down operations to investigate. They noticed several anomalies that should have caused serious concern, but showed no hint of alarm. Another factor that prevented correct diagnosis of the problem was the lack of information regarding the flow parameters. Bypassing the active system and flow-out meter resulted in the lack of flow-in and flow-out data that could have indicated the well integrity problem. Had the crew routed the seawater through the active pit system before sending it into the well, such data would have been available. Once the crew began displacing the riser with seawater, they confronted the challenge of dealing with all of the returning mud. The driller repeatedly rerouted the mud returns from one pit to another in order to accommodate the incoming volume. During that time, the crew also sent mud from other locations into the active pit system. It is not clear whether the crew could adequately monitor active pit volume (or flow-in versus flow-out) during that time given all the activity. Important factor was also the lack of a suitable information system that would be capable to alert the crew when anomalies arise. In light of the potential consequences, the system used at the rig, which requires the right person to be looking at the right data at the right time, and then to understand their significance, in spite of simultaneous activities and other monitoring responsibilities, is not adequate. The above mentioned deficiencies and missteps were rooted in systemic failures by industry management (extending beyond BP to contractors that serve many in the industry), and also by failures of government to provide effective regulatory oversight of offshore drilling. These are important root causes that must be properly addressed to prevent recurrence of similar accidents. Failure of BOP emergency mode Blowout preventer (BOP) was the last line of defence in the case of failure of the remaining barriers. The BOP is designed to contain pressure within the wellbore and halt an uncontrolled flow of hydrocarbons to the rig. The Deepwater Horizon’s BOP did not succeed in containing the Macondo well. Witness accounts indicate that the rig crew activated one of the annular preventers around 9:41 p.m., and pressure readings suggest they activated a variable bore ram (which closes around the drill pipe) around 9:46 p.m. Flow rates at this point may have been too high for either the annular preventer or a variable bore ram to seal the well. Earlier kick detection would have improved the odds of success. After the first explosion, crew members on the bridge attempted to engage the rig’s emergency disconnect system (EDS). The EDS should have closed the blind shear ram, severed the drill pipe, sealed the well, and disconnected the rig from the BOP. But none of How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 56 that happened. When the subsea supervisor pushed the EDS button the panel indicators lit up, but the rig never disconnected. Three potential causes can be identified for this failure. They include: failure of the control signal that activate the blind shear ram (BSR), failure of the hydraulic system that operate the shears, and BSR failure to slice through the drill pipe. It is possible that the first explosion had already damaged the cables to the BOP, preventing the disconnect sequence from starting. Even so, the BOP’s automatic mode function (so called “deadman” system) should have triggered the blind shear ram after the power, communication, and hydraulics connections between the rig and the BOP were cut. But the "deadman" system failed too. Another possible cause is unavailability of two redundant control "pods" that control the BOP’s automatic mode function (the “deadman” system). The deadman is designed to close the shear ram if the electronic and hydraulic lines connecting the rig to the blowout preventer are severed. Post-incident testing of the two redundant “pods” revealed low battery charges in one pod and defective solenoid valves in the other. If those problems existed at the time of the blowout, they would have prevented the deadman system from working. This failure may have been due to poor maintenance. Failure of the BSR hydraulic system is a potential single failure that could disable the BSR function. The likely cause is hydraulic fluid leak that may have reduced the ram cutting force. Failure of this system would have also prevented activation of BSR through the use of underwater robot (VOR). Attempt to use VOR was undertaken within the first few days after the explosion. Using a robotic submersible equipped with a hydraulic pump, the crew injected seawater into the blind shear ram, hoping to drive its pistons and blades closed. But the pump did not have nearly the needed strength; it could not pump water at a sufficient rate to budge the blades. It is also possible that BSR was not capable to shear the pipe. Two potential causes can be indicated: BSR blades are positioned on indestructible joint or the BSR cutting force is not sufficient to cut pipe. The first possibility, for the BOP with only one BSR, as used by the Deepwater Horizon, is estimated as 0.10. The possibility of the latter scenario is confirmed by two studies of West Engineering Services of Brookshire, Tex., one of the industry’s premier authorities on blowout preventers (cited in Ref. [C-12]). These studies found a more basic problem: even when everything worked right, some blind shear rams still failed to cut pipe. West’s experts concluded that calculations used by makers of blowout preventers overestimated the cutting ability of blind shear rams. It is noted that modern drill pipe is nearly twice as strong as older pipes of the same size. In addition, the intense pressure and frigid temperatures of deep water make it tougher to shear a pipe. It is worth noting that from the point of view of reliability, BOP is rather a vulnerable device. According to Ref. [C-12] in 2009 Transocean commissioned a "strictly confidential" study of the reliability of blowout preventers used by deepwater rigs. Using the world’s most authoritative database of oil rig accidents, a Norwegian company, Det Norske Veritas, focused on some 15,000 wells drilled off North America and in the North Sea from 1980 to 2006. It found 11 cases where crews on deepwater rigs had lost control of their wells and then activated blowout preventers to prevent a spill. In only six of those cases were the wells brought under control, leading the researchers to conclude that in actual practice, How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 57 blowout preventers used by deepwater rigs had a “failure” rate of 45 percent. The study also revealed that the BOP is vulnerable to a single failure of a control valve in the hydraulic system. An examination by The New York Times [C-12] reveals that the federal agency charged with regulating offshore drilling, the Minerals Management Service, repeatedly declined to act on advice from its own experts on how it could minimize the risk of a blind shear ram failure. How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 58 Step 2. Cause Map - Page 7 VOR failed to activate BSR AND Control signal failed Fire induced damage to BSR control cables? 10 AND Department of the Interior was understaffed None of the two control pods operable ? OR 15 Test and maintenance not adequate BOP did not seal properly 8 Safety oversight not effective AND 9 BSR hydraulic system failed Pressure in the system too low? Leaking valve or untight joint? Inadequate scope of safety regulations 25 E BOP emergency 1 modes failed to seal the well BSR blades on indestructible joint? OR OR 24 BSR unable to shear pipe OR 26 BSR cutting capability overestimated BOP activation too late D How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 Weakness of the BSR design? Crew failed to recognize gas influx in time © ENCO Page 59 Step 2. Cause Map - Page 8 OR Emergency procedures not adequate ? Crew diverted mud & gas flow to MGS Emergency conditions not recognized F Gas leaks to engine area and ignites Gas enters from MGS through HVAC Department of the Interior was understaffed 8 Safety oversight not effective 16 Emergency training not adequate ? AND 10 14 AND 9 Inadequate scope of safety regulations MGS operated beyond design basis AND 23 Connections between MGS and HVAC How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 Weakness of the MGS design © ENCO Page 60 Diversion of flow to the MGS Direct cause of the ignition and explosion of blowout gases was that gas penetrated the engine area that was outside the fire protection area and had electrical equipment containing potential ignition sources. Gas entered the engine area from the mud gas separator (MGS) system through the rig's heating, ventilation and air conditioning system (HVAC). When hydrocarbons flow was finally noted, the Deepwater Horizon crew closed the blowout preventer and diverter, routing oil and gas to the mud gas separator (MGS) system rather than diverting it overboard. The MGS was operated beyond design basis and was overwhelmed by the force of oil and gas which leaked into the rig's ventilation system. Gas was exiting the vents located on the derrick, directly above the rig floor. It is not clear why personnel did not choose to divert the gas directly overboard. While that ultimately may not have prevented an explosion, diverting overboard would have reduced the risk of ignition of the rising gas. Considering the circumstances, the crew also should have activated the blind shear ram to close in the well. Diverting the flow overboard and/or activating the blind shear ram may not have prevented the explosion, but likely could have given the crew more time and perhaps limited the impact of the explosion. There are a few possible explanations for why the crew responded in this way. The crew may not have recognized the severity of the situation, though that seems unlikely given the amount of mud that spewed from the rig floor. They did not have much time to act. The explosion occurred roughly six to eight minutes after mud first emerged onto the rig floor. Perhaps the most significant factor is the lack of appropriate emergency procedure and training. The rig crew had not been trained adequately how to respond to such an emergency situation, including the simulations and drills for such emergencies, and momentous decision to engage the blind shear rams or trigger the EDS. The heating, ventilation and air conditioning system is thought to have sent a gas-rich mixture into the engine rooms. Connections between MGS and HVAC indicate weaknesses of the design. 4.3. Step 3. Analysis of solutions The Cause Map is used to identify all the possible solutions for the problem so that the best solutions can be selected. Potential solutions correspond to those causes which can be controlled by the problem owner so that the problem is prevented from recurring. The following causes, which can be subject of interest in this context, can be identified on the Cause Map for the Deepwater Horizon accident (as developed in Step 2): General issues related to safety management, safety culture, and regulatory oversight 1. 2. 3. Focus on production as opposed to safety / production pressure No formal system for risk assessment of alternative solutions Safety culture at the company level inadequate How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 61 4. 5. 6. 7. 8. 9. 10. Lessons from potential issues or past events not communicated to the rig crew Subcontractors failed to communicate adequately Making ad hoc changes during well development without evaluation of the related risk Well site management not consulting potential issues/anomalies with on shore office Safety oversight of exploration, drilling and production of oil from deepwater formations not effective Inadequate scope of safety regulations for deepwater oil industry Department of the Interior responsible for safety oversight of deepwater oil industry understaffed. Procedures and training 11. 12. 13. 14. 15. 16. No detailed requirements for the cement log test Standard BP procedure for negative-pressure test not detailed enough No suitable procedure on well monitoring Emergency procedures not adequate BOP test and maintenance not adequate Rig crew training not sufficient. Process safety 17. 18. 19. 20. 21. Small volume of cement used in the well cementing process Relatively low rate of pumping cement No bottoms up circulation Use of oil-based spacer Displacement bypassing pits and flow out meter. Equipment design issues 22. 23. 24. 25. 26. Instrumentation and displays for well monitoring not adequate Weakness of the MGS design BSR unable to shear pipe BSR blades on indestructible joint Weakness of the BSR design. The above mentioned causes are arranged in several groups of different type, area of origin and importance. Their numbering corresponds to that used in Cause Map (Step 2, Pages 1 – 8). These causes and corresponding solutions are briefly discussed below. Safety management and safety culture (Causes 1 – 7) Analysis of risks and risk awareness Companies involved in deepwater oil drilling must have in place strict policies requiring rigorous analysis and proof that less-costly alternatives are in fact equally safe (Cause 2). This recommendation also applies to current practice of making ad hoc changes during well development and completion without evaluation of the related risk (Cause 6). When implemented successfully, it would ensure that individual decision makers have a full awareness of the risk associated with the decision. If BP had any such policies in place, it does not appear that its Macondo team adhered to them. Unless companies create and enforce such policies, there is simply too great a risk that financial pressures will systematically bias decision making in favour of time- and cost-savings (Cause 1). How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 62 Regulators need to create suitable framework that support such an approach. One of the important pre-conditions is clear formulation of health, safety and environmental objectives and establishing regulations that require operators, drilling contractors and service companies to work together to meet these safety objectives. Safety management system The most significant failure at Macondo – and the clear root cause of the blowout – was a failure of industry management. Most, if not all, of the failures at Macondo can be traced back to underlying failures of management and communication. Better management of decision making processes within BP and other companies, better communication within and between BP and its contractors, and effective transfer of information among key engineering and rig personnel would have prevented the Macondo incident (Causes 4, 5, and 7). BP and other operators must have effective systems in place for integrating the various corporate cultures, internal procedures, and decision making protocols of the many different contractors involved in drilling a deepwater well. The management system has to clearly define the roles and responsibilities for all parties involved in a given project (operator, drilling contractor and service companies) for health, safety and environmental protection. It should provide detailed project specific information to be shared by key personnel regardless of whether they are employed by the operator, the drilling contractor, or a service company. The system has to facilitate the management of change process and serve as a mechanism to communicate the implications of programme changes to all key personnel. Safety culture It is also critical that companies implement and maintain a pervasive top-down safety culture that reward employees and contractors who take action when there is a safety concern even though such action costs the company time and money (Causes 1 and 3). Long-term proactive improvement programme that ensure effective learning from experience is an integral element of an effective risk management approach reflecting a safety culture (Cause 4). In such a programme “near misses” should provide opportunities to improve, and the reporting of errors, omissions, and questionable results should be highly encouraged. The regulators should establish practices and standards that foster continuous improvement in safety culture within the industry. Regulatory oversight (Causes 8 – 10) Regulatory approach Government agencies1 that regulate offshore activity should reorient their regulatory approaches to integrate more sophisticated risk assessment and risk management practices 1 The Mineral Management Service (MMS) that was the federal agency primarily responsible for regulating the safety of offshore drilling at the time of the Macondo well accident. Since October 1, 2011 the federal entity responsible for safety and environmental oversight of offshore oil and gas activities is the Bureau of Safety and Environmental Enforcement (BSEE). How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 63 into their oversight of energy developers operating offshore (Cause 8). They should shift their focus from prescriptive regulations covering only the operator to a foundation of augmented prescriptive regulations, including those relating to well design and integrity, supplemented by a proactive, risk-based performance approach that is specific to individual facilities, operations, and environments1. This would be similar to the “safety case” approach that is used in the North Sea, which requires the operator and drilling rig owners to assess the risks associated with a specific operation, develop a coordinated plan to manage those risks, integrate all involved contractors in a safety management system, and take responsibility for developing and managing the risk management process. Regulations and standards The regulator agencies working with the International Regulators’ Forum and other organizations, Congress and the DOI should identify those drilling, production, and emergency-response standards that best protect offshore workers and the environment, and initiate new standards and revisions to fill gaps and correct deficiencies. Criteria for high-risk wells and develop methodology to assess those risks should be identified. This process should include input from broad group of experts. Furthermore, the DOI should develop in-house competence to perform such sophisticated risk assessments (Cause 10). Such evaluations could guide the transition to a system where all operators and contractors are required to demonstrate an integrated, proactive, risk management approach prior to leases being granted or receiving permits for exploration wells and major development projects. Coordinated, inter-agency research effort will be needed to develop safer systems, equipment, and practices to prevent failures of both design and equipment in the future. The federal government has relevant expertise in areas that could and should be transferred to the offshore industry. More detailed requirements for incident reporting and data concerning offshore incidents and “near misses” are needed. Such data collection would allow for better tracking of incidents and stronger risk assessments and analysis. Such reporting should be publicly available and should apply to all offshore activities. In addition, DOI, in cooperation with the International Regulators Forum, should take the lead in developing international standards for incident reporting in order to develop a consistent, global set of data regarding fatalities, injuries, hydrocarbon releases, and other accidents. Sharing information as to what went wrong in offshore operations, regardless of location, is a key to avoiding such mistakes. Transparent information and data sharing within the offshore industry and among international regulators is critical to continuous improvement in standards and risk management practices. 1 Proactive, goal-oriented risk management system similar to the systems used in the North Sea by the United Kingdom and Norway has already been instituted by DOI. Implementation of Safety and Environmental Management System (SEMS) in 30 CFR 250 (Federal Register, Vol. 75, No 199, Oct. 15, 2010) began on November 15, 2011. How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 64 Resources and staffing To expand regulatory oversight and tighten safety requirements the regulatory agencies should be provided with adequate funding. Regulators to be more effective should be provided with the resources, personnel, and training. In the past these agencies were not adequately supported by industry, members of Congress, and several administrations. As a result, neither the regulations nor the regulators were asking the tough questions or requiring the demonstration of preparedness that could have avoided the Macondo disaster. The regulator should have a formal training and certification program for its inspectors. The extent of training of key personnel and decision makers in regulatory agencies has to be consistent with the complexities and risks of deepwater drilling. It is also essential that there is better opportunity for higher education and career advancement for inspectors. Individuals involved in regulatory oversight should have qualifications that are appropriate for meeting the challenges of the offshore drilling industry. Procedures and training (Causes 11 – 16) Procedures The Macondo well accident identified several procedures that appear to be inadequate or lacking and require improvement. These include requirements for conducting cement bond log (Cause 11), procedure for conducting negative-pressure test (Cause 12), procedure on well monitoring (Cause 13), and emergency procedure for situations that involve loss of well integrity (Cause 14). These procedures should be carefully reviewed and re-worked. They should clearly define mandatory practices and specify roles and accountabilities for the personnel involved. Procedures should be detailed enough to specify operational steps and decision points as well as the related criteria. Procedures related to tests should include definition of success/failure criteria for the test. Procedures for operations that are more complex and carried out infrequently should be more detailed to compensate for unfamiliarity. So far there was a high reliance on leadership and know-how of the crew. However, the procedures that were available were guidelines only and did not provide enough detail. For instance, the procedure on negative-pressure test did not specify bleed volumes or give success/failure criteria. While initial well design decisions undergo a serious peer review process and changes to well design are subsequently subject to a management of change (MOC) process, changes to drilling procedures in the weeks and days before implementation were typically not subject to any such peer-review or MOC process. At Macondo, such decisions appear to have been made by the BP Macondo team in ad hoc fashion without any formal risk analysis or internal expert review. This appears to have been a key causal factor of the blowout. Such practices are not acceptable and have to be eliminated. These temporary abandonment procedures should be thoroughly and rigorously vetted earlier in the design process. It does not appear that the changes to the temporary abandonment procedures used at Macondo went through any sort of formal review at all. How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 65 Industry staff training Standards for education, training, and professional certification of private-sector decisionmaking personnel involved in drilling operations in force at the time of the Deepwater Horizon accident were relatively minimal compared with other safety-critical industries, such as nuclear or chemical. Personnel on the Deepwater Horizon MODU were mostly trained on the job, and this training was supplemented with limited short courses (such as 1 week of well control school every few years). While this appears to be consistent with industry standard practice and current regulations (such as 46 CFR 10.470 for OIMs), it is not comparable with other safety-critical industries such as nuclear power or chemical manufacturing. The appropriate qualifications of key personnel both on deepwater drilling rigs and ashore need to be assessed and improved, as needed, to provide for safe operations and protect the public interest. Numerous decisions to proceed toward abandonment despite indications of hazard, such as the results of repeated negative-pressure tests, suggest an insufficient consideration of risk and a lack of operating discipline. The decisions also raise questions about the adequacy of operating knowledge on the part of key personnel. Improvement in the awareness of risks and risk management practices should help in resolving this issue. The rig crew has to be trained adequately how to respond to escalating emergency situations, including the simulations and drills for such emergencies, and momentous decision to engage the blind shear rams or trigger the EDS. During the Macondo well accident the crew had difficulty assessing the situation and understanding its significance. Appropriate training and job aids would have increased both the speed and accuracy of identification that there was an influx of hydrocarbons and enhanced the probability of appropriate well control actions. Process safety (Causes 17 – 21) Investigation of causes of the Macondo well accident identified several process-specific decisions that contributed to the risk of blowout. They correspond to the causes 17 – 21 which are associated mostly with the implementation of temporary abandoning procedure. These specific issues should be carefully addressed in the development of appropriate internal procedures and Engineering Technical Practices. Equipment design issues (Causes 22 – 26) Investigation of causes of the Macondo well accident identified several design-specific concerns that contributed to the risk of blowout or had an impact on the severity of accident consequences. These weaknesses correspond to causes 22 – 26. Instrumentation and displays used for well monitoring must be improved (Cause 22). An expert system decision aid should be used to provide timely warning of loss of well control to drillers on the rig (and ideally to onshore drilling monitors as well). If the warning is inhibited or not addressed in an appropriate time interval, autonomous operation of the blind shear rams, emergency disconnect system, general alarm, and other safety systems on the rig should occur. How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 66 Design of the MGS has to be evaluated with regard to consequences of its use beyond design basis, in particular, from the point of view of penetration of flammable gases to non-fire-protected zone through the HVAC system (Cause 23). Arrangement of gas detectors, automatic dampers, and alarms needs to be checked in this context, and eventual design changes introduced. Cutting, sealing and separating capabilities of the BOP system should be specified in the regulations (Causes 24 - 25). Application of specific BOP systems in a well drilling project should be made consistently with the drilling environment to which they are applied and the rigs on which they are installed. Test and maintenance procedures should be established to ensure operability and reliability appropriate to their environment of application. The use of two blind shear rams is also essential issue that needs resolution. Two blind shear rams give an extra measure of reliability, especially, if one shear ram hits on a joint connecting two drill pipes (Cause 25). BOP as well as some other components that are critical to the safety of oil drilling operations should be required to be independently certified by a third party (such as a classification society) or by the relevant regulatory agency. At the time of the Macondo well accident the MMS did not directly oversee the initial and subsequent certifications of BOPs. Instead, the operator was to self-certify the BOP. How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 67 5. Summary conclusions Significant number of issues discussed in Section 4.2 and 4.3 are rather specific to the technology of deepwater oil drilling. They should be carefully addressed by the industry (operators, drilling contractors and service companies) and resolved through appropriate changes in the procedures and training programmes. Regulator agencies have also important role in enforcing appropriate changes. However, most of the issues can be traced back to underlying causes of more general type such as management system, safety culture, and safety oversight. Some of them can be of general interest to different industries and are worth to be discussed during the workshop. Comparisons have to be made and conclusions drawn with care, taking into account significant differences of industries considered in the project. It is important to note that the deepwater oil drilling industry is rather specific area that involves a large number of facilities and was subject to intensive development of technology and rapidly expanding production activities. The Macondo blowout was the product of several individual missteps and oversights by BP, Halliburton, and Transocean, which government regulators lacked the authority, the necessary resources, and the technical expertise to prevent. The extent to which each of these missteps and oversights caused the accident to occur will never be precisely known. What we nonetheless do know is considerable and significant: (1) each of the mistakes made on the rig and onshore by industry and government increased the risk of a well blowout; (2) the cumulative risk that resulted from these decisions and actions was both unreasonably large and avoidable; and (3) the risk of a catastrophic blowout was ultimately realized on April 20 and several of the mistakes were contributing causes of the blowout. Deepwater drilling is an inherently risky business given the enormous pressures and geologic uncertainties. It is now clear that both industry and government need to reassess and change business practices to minimize the risks of such drilling. 5.1. Industry management system The most significant failure at Macondo – and the clear root cause of the blowout – was a failure of industry management. Most, if not all, of the failures at Macondo can be traced back to underlying failures of management and communication. Better management of decision making processes within BP and other companies, better communication within and between BP and its contractors, and effective training of key engineering and rig personnel would have prevented the Macondo incident. Risk awareness BP’s management process did not adequately identify or address risks created by late changes to well design and procedures. BP did not have adequate controls in place to ensure that key decisions in the months leading up to the blowout were safe or sound from an engineering perspective. It should be noted that changes to drilling procedures in the How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 68 weeks and days before implementation were not subject to any peer-review or management of change (MOC) process. At Macondo, such decisions appear to have been made by the BP Macondo team in ad hoc fashion without any formal risk analysis or internal expert review. This appears to have been a key causal factor of the blowout. An obvious example is the last-minute confusion regarding whether to run six or 21 centralizers. Another clear example is provided by the temporary abandonment procedure used at Macondo. That procedure changed dramatically and repeatedly during the week leading up to the blowout. As of April 12, the plan was to set the cement plug in seawater less than 1,000 feet below the mud line after setting the lockdown sleeve. Two days later, the procedure was to set the cement plug in mud before displacing the riser with seawater. By April 20, the plan was to remove 3,300 feet of mud from below the mud line and set the cement plug after the riser had been displaced. It does not appear that the changes to the temporary abandonment procedures went through any sort of formal review. Halliburton and BP’s management processes did not ensure that cement was adequately tested. Halliburton had insufficient controls in place to ensure that laboratory testing was performed in a timely fashion or that test results were vetted rigorously in-house or with the client. In fact, it appears that Halliburton did not even have testing results in its possession showing the Macondo slurry was stable until after the job had been pumped. It is difficult to imagine a clearer failure of management or communication. The story of the foam stability tests may illuminate management problems within BP as well. By early April, BP team members had recognized the importance of timely cement testing. And by mid-April, BP’s team had identified concerns regarding the timeliness of Halliburton’s testing process. But despite their recognition that final changes to the cement design (made to accommodate their concerns about lost returns) might increase the risks of foam instability, BP personnel do not appear to have insisted that Halliburton complete its foam stability tests and report the results to BP for review before ordering primary cementing to begin. Communication problems BP, Transocean, and Halliburton failed to communicate adequately. For example, many BP and Halliburton employees were aware of the difficulty of the primary cement job. But those issues were for the most part not communicated to the rig crew that conducted the negative-pressure test and monitored the well. It appears that BP did not even communicate many of those issues to its own personnel on the rig. Transocean failed to adequately communicate to its crew lessons learned from a similar near-miss on one of its rigs in the North Sea four months prior to the Macondo blowout. Safety culture issues Management and communication issues mentioned above clearly indicate problems with safety culture. Resulting from a deficient overall system approach to safety is evident in the multiple flawed decisions that lead to the blowout. These problems involved the lack of management commitment to safety, lack of the questioning attitude and safety awareness, insufficient level of knowledge of procedures and rules and lack of operating discipline, incompliance with the existing internal procedures or work practices, and inadequate communication on safety matters between individuals and groups. How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 69 BP was aware of problems with Halliburton personnel and work product years before the blowout. Despite that BP’s own well site leaders accepted facially implausible explanations for the negative test results. BP’s on-duty well site leader was not even present during preparations for the critical negative pressure test, and may not have been present during the beginning of the negative pressure test itself. In the light of these facts, the management commitment to safety is questionable. Decision making processes at Macondo well did not adequately ensure that personnel fully considered the risks created by time- and money-saving decisions. None of such decisions appear to have been subject to a comprehensive and systematic risk-analysis, peer-review, or management of change process. The companies are lacking of appropriate organizational and technical framework for a systematic risk assessment, or if such framework existed, it was not used. BP team decision of not conducting a cement evaluation log did not fully conform to the intent of its own guidelines. Introducing ad hoc changes in the temporary abandonment procedure used at Macondo also indicate procedure-related problems at BP. That procedure changed many times during the week leading up to the blowout without any assessment of the related risks. Learning from operational events or near-misses was minimal or non-existing. Also the use of existing expertise and knowledge within the corporation was questionable. 5.2. Safety oversight of the industry Regulatory regime of MMS The oversight system of the deepwater drilling industry in force at the time of the Macondo well accident was based mainly on prescriptive approach. Under that approach specific requirements for equipment and operations were developed and then compliance with the regulations was monitored through auditing. Prescriptive regulations, which are often developed through a multiyear process in response to events and observed trends, were neither timely nor complete and lag behind the development of new technologies [C4]. Over the past few decades, exploration and production companies within the oil and gas industry developed advanced technology that led to a marked increase in deepwater drilling in the Gulf of Mexico. During this period the predominantly prescriptive regulatory system for deepwater drilling used by the Minerals Management Service (MMS) did not keep up with these technological advances. In addition, its level of funding and technical staffing remained static or decreased as industry's offshore drilling activity increased. The Macondo well blowout was precipitated by multiple flawed decisions involving the operator and contractors as they moved toward temporary abandonment of the well despite indications of increasing hazard. This reduced the available margins of safety that take into account complexities of the hydrocarbon reservoirs and well geology discovered through drilling and the subsequent changes in the execution of the well plan. In effect, the industry made important decisions without regulator's review of the impact of the changes on the overall risk with regard to temporary abandonment procedures. MMS’s cursory review of the temporary abandonment procedure mirrors BP’s apparent lack of controls governing certain key engineering decisions. Like BP, MMS focused its How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 70 engineering review on the initial well design, and paid far less attention to key decisions regarding procedures during the drilling of the well. Also like BP, MMS did not assess the full set of risks presented by the temporary abandonment procedure. The limited scope of the regulations is partly to blame. But MMS did not supplement the regulations with the training or the processes that would have provided its permitting official with the guidance and knowledge to make an adequate determination of the procedure’s safety. As noted in the investigation report of NAE/NRC [C-3] the regulatory regime was ineffective in addressing the risk of the Macondo well. The actions of the regulators did not display an awareness of the risk or the very narrow margins of safety. Many critical aspects of drilling operations were left to industry to decide without agency's review. For instance, there was no requirement, let alone protocol, for a negative-pressure test, the misreading of which was a major contributor to the Macondo blowout. Nor were there detailed requirements related to the testing of the cement essential for well stability. Issue of concern is that a flawed, risky well plan for the Macondo well was approved by the MMS, and BP, Anadarko and Mitsui management. Similar or identical plans were undoubtedly approved and used by many operators on other wells drilled in the Gulf of Mexico. A plan that does not include enough cement to overlap the final and previous casing strings, and that does not require running a cement-bond log to ensure the integrity of the seal is a defective plan. The fact that there have not been blowouts on previous wells does not justify the approval and use of an unsafe plan. The extent of training of key personnel and decision makers in regulatory agencies has been inconsistent with the complexities and risks of deepwater drilling. The regulatory community has not made effective use of real-time data, information on precursor incidents or near-misses, or lessons learned from operation to adjust practices and standards appropriately. Desired changes The Deepwater Horizon-Macondo well accident demonstrated the need for changing the existing safety oversight system for a proactive goal-oriented system integrating all aspects of drilling operations that could affect occupational and process safety. The new regulatory system should incorporate a limited number of prescriptive elements into a proactive goal-oriented risk management system for health, safety and the environment. Quantitative risk analysis should be an essential part of such goal-oriented risk management system. With regard to this approach the drilling industry may benefit from lessons learned and practices implemented in the nuclear industry that widely applies the probabilistic risk assessment (PSA) to support both the operators and regulators at various stages of plant design and operation. The regulators should identify safety critical points during well construction and abandonment that warrant explicit regulatory review and approval before operation can proceed and enforce appropriate regulations. The regulator should establish safe operating limits, which, when exceeded, would require regulatory approval for operation to proceed. Appropriate requirements for approval and certification of key steps during well construction should be incorporated into codes and standards. Pre-certification of operators, contractors, and service companies before granting a drilling permit for especially challenging projects could be a useful element of the new oversight system. Consideration should also be given to the possibility of using independent How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 71 well examiners that could help in reviewing well plans and monitoring ongoing activities during drilling, completion and abandonment. How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 72 6. References to Annex C [C-1] British Petroleum, "Deepwater Horizon Accident Investigation Report", Sept. 8, 2010. [C-2] "Interim Report on Causes of the Deepwater Horizon Oil Rig Blowout and Ways to Prevent Such Events", National Academy of Engineering (NAE) and the National Research Council (NRC), prepared for U.S. Department of the Interior, November 16, 2010. [C-3] "Macondo Well Deepwater Horizon Blowout, Lessons for Improving Offshore Drilling Safety", National Academy of Engineering (NAE) and the National Research Council (NRC), prepared for U.S. Department of the Interior, Final Report. http://www.nap.edu/openbook.php?record_id13273 [C-4] "Deepwater, The Gulf Oil Disaster and the Future of Offshore Drilling", Report to the President, National Commission on the BP Deepwater Horizon Oil Spill and Offshore Drilling, January 2011. [C-5] Hubbard, A., Embrey, D., "Deepwater Horizon – Summary of Critical Events, Human Factors Issues and Implications", ©Human Reliability Associates Ltd, Sept. 23, 2010. [C-6] "Oil Spill Reaches Mississippi River". CBS News. 29 April 2010. Retrieved 29 April 2010. [C-7] "Weekly Address: President Obama Establishes Bipartisan National Commission on the BP Deepwater Horizon Oil Spill and Offshore Drilling" (Press release). The Whitehouse. 2010-05-22. Retrieved 2010-06-01. [C-8] Oil Spill Commission, Chief Counsel's Report, http://www.oilspillcommission.gov/chief-counsels-report. [C-9] "Oil spill: BP 'did not sacrifice safety to save money'". BBC. 9 November, 2010. Retrieved 12 November 2010. [C-10] "Gulf oil spill: President's panel says firms complacent". BBC. 9 November, 2010. Retrieved 12 November 2010. [C-11] Leo King (12 November 2010). "Deepwater Horizon modelling software showed BP cement conditions unstable". Computerworld UK. Retrieved 12 November, 2010. [C-12] David Barstow, Laura Dodd, James Glanz, Stephanie Saul and Ian Urbina "Regulators Failed to Address Risks in Oil Rig Fail-Safe Device", New York Times, June 20, 2010. How to Improve Safety in Regulated Industries What Could We Learn From Each Other safety in EU” Background Material, ENCO FR-(12)-44 © ENCO Page 73
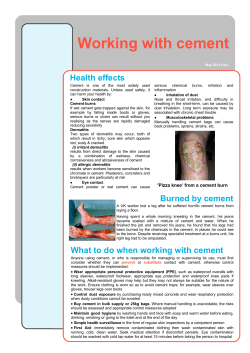









© Copyright 2026